

Abstract
Aim
A laboratory study to determine the apical pressure generated by seven canal irrigation methods in an anterior tooth with an open apex.
Methodology
Canal irrigation was performed on a 3D‐printed central maxillary incisor with an open apex (maximum diameter of 2.1 mm). Ultrasonically activated irrigation (UAI), sonic activation (EDDY), negative pressure irrigation (EndoVac), the self‐adjusting file (SAF) and the XP‐endo Finisher were employed at tooth length (TL), TL—1 mm, TL—2 mm and TL—3 mm. UAI was tested at three intensity levels additionally. Hydrodynamic irrigation with RinsEndo was performed in the pulp chamber, at the canal orifice, the coronal third, the middle of the canal and at TL. Er:YAG laser activation, at four frequency settings, was performed in the pulp chamber and at the orifice of the canal. The pressure of the fluid towards the canal terminus generated by activation was directly transferred to a pressure sensor with a range of 0 to 120 mmHg and a response time of ≤0.5 ms. The critical threshold for apical extrusion of the irrigant was set at 5.73 mmHg (lower limit of the central venous pressure: 5.88 ± 0.15 mmHg). Each experiment was repeated ten times. The tests were followed by descriptive analyses (maximum, mean, standard deviation, 95% confidence interval).
Results
EndoVac, the SAF, the XP‐endo Finisher, and UAI never exceeded the critical threshold at any insertion depth or intensity level. Er:YAG laser activation exceeded the critical threshold exclusively at frequency settings that varied from the manufacturer's recommendation. EDDY at TL and RinsEndo at any insertion depth exceeded the critical threshold in 100% of the measurements. EDDY at TL—1,—2, and—3 mm crossed the critical threshold in 30%, 10%, and 20% of the measurements, respectively.
Conclusions
In a simulated maxillary central incisor with an open apex, irrigation with EndoVac, Er:YAG laser activation, UAI, the SAF, and the XP‐endo Finisher generated apical pressures below the critical threshold of 5.73 mmHg. By contrast, using EDDY and RinsEndo for irrigation produced higher apical pressures that exceeded the critical threshold.
Keywords: apical extrusion, endodontics, immature tooth, NaOCl accident, root canal treatment, sodium hypochlorite
INTRODUCTION
Irrigation is an essential part of the chemo‐mechanical preparation of root canals aiming to remove dentine debris, pulp tissue, and microbes (Gulabivala et al., 2005; Haapasalo et al., 2005). Sodium hypochlorite (NaOCl) is the most commonly used irrigant owing to its excellent chemical properties (Dutner et al., 2012; Haapasalo et al., 2005; Zaugg et al., 2019). It has the potential to dissolve organic tissue, to act effectively against a broad range of microorganisms and to neutralize their products (Buttler & Crawford, 1982; Zehnder, 2006).
On the other hand, NaOCl has toxic effects on vital tissues, potentially leading to necrosis, haemolysis, and ulceration (Pashley et al., 1985). It is therefore important to avoid irrigant extrusion into the periapical region. The frequency of such an extrusion is unknown but it is considered to be rare (Spencer et al., 2007). Nonetheless, the extrusion of NaOCl followed by severe symptoms has been described in several case reports (Boutsioukis et al., 2013). Possible symptoms include severe pain, tissue necrosis, oedema, profuse interstitial bleeding with haemorrhage or bleeding from the root canal, anaesthesia or paraesthesia, irritation of the throat and secondary infection (Hülsmann & Hahn, 2000).
In vivo and ex vivo studies as well as reviews of case reports have attempted to identify factors that determine irrigant extrusion (Boutsioukis et al., 2013; Dutner et al., 2012; Hülsmann & Hahn, 2000). Although some factors remain unclear, technical aspects have been investigated fully. For example, wedging of the syringe tip can inhibit the coronal outflow of the irrigant and thus increase the pressure of the fluid towards the foramen (Shen et al., 2010). A larger apical preparation size or the presence of apical ramifications have been reported to result in less extrusion in vitro (Boutsioukis et al., 2010; Lorono et al., 2020). In addition, an open apex is considered to be a significant factor favouring extrusion of irrigants. In a survey among board‐certified endodontists (diplomates of the American Board of Endodontics), an open apex was named the most common reason for a NaOCl accident (Kleier et al., 2008).
Severe NaOCl accidents such as extensive ecchymosis around the periorbital region and at the angle of the mouth and the neck are likely due to penetration of NaOCl into the facial venous system. Since anatomical variations in the venous system are not uncommon (Hollinshead, 1968), drainage from the anterior teeth may occur into the facial vein via tributaries. More frequently, the drainage occurs into the pterygoid plexus. For NaOCl to enter the venous system, the central venous pressure must be exceeded (Baumann et al., 2005; Lyons & Burwell, 1938; Zhu et al., 2013). This critical threshold corresponds to 5.73 mmHg (mean: 5.88 mmHg ± SD of 0.15 mmHg) and has been chosen in several studies investigating apical irrigant extrusion (Charara et al., 2016; Goode et al., 2013; Khan et al., 2013). The apical tissue pressure countering an extrusion is a crucial factor, but it is considered to be individual and dependent on the clinical situation (Lorono et al., 2020).
Syringe irrigation is indispensable and remains the most commonly used method (Peters, 2004; Zaugg et al., 2019). However, several irrigation methods aiming to improve irrigation are available. Ultrasonically activated irrigation (UAI) as well as sonic irrigation transmit acoustic energy from the file within the canal to the irrigant to enhance the efficacy of the irrigation process (Neuhaus et al., 2016; van der Sluis et al., 2007). UAI works at a frequency of 28 to 36 kHz and at an amplitude of 4 to 200 µm whereas sonic irrigation works at a frequency of up to 6000 Hz and at an amplitude of 240 µm. The sonic irrigation device EDDY (VDW) is a flexible, noncutting polyamide tip of 28 mm length with an ISO size of 20 and a 0.02 taper that can be coupled to an air scaler (Conde et al., 2017; Eggmann et al., 2020; Neuhaus et al., 2016).
Laser activation works via laser pulses vaporizing the irrigant. The resulting bubbles collapse, creating shockwaves, and generating cavitation effects (de Groot et al., 2009). Besides activation of the irrigant, novel methods for affecting fluid dynamics by suction have been developed. RinsEndo (Dürr Dental) is a hydrodynamic irrigation method rinsing with alternate sequences of suction and pressure (Rodig et al., 2010). EndoVac (Kerr Dental) brings the irrigant into the pulp chamber by a master delivery tip. The irrigant reaches the apical regions because of negative pressure created by suction of a cannula that is placed within the main root canal close to the canal terminus (Nielsen & Baumgartner, 2007). The macrocannula has a size of 55, a taper of .02 and is used for irrigation of the pulp chamber and the coronal and middle segments of the canal during initial instrumentation. The microcannula has asize of 32 and enables irrigation of the apical parts of the root canal system (Desai & Himel, 2009).
In addition, coreless shaping instruments have been developed to perform more minimally invasive root canal preparations. The Self‐Adjusting‐File (SAF; ReDent NOVA, Berlin, Germany ) adapts to the shape of the root canal and thus causes little alteration to its original form (Lacerda et al., 2017; Metzger et al., 2010). SAF works with simultaneous irrigation, the irrigant flows continuously through the hollow file, which produces favourable cleaning results (De‐Deus et al., 2011). SAF ejects 4 mL of irrigant per minute and works at a speed of 5000 rpm. The XP‐endo Finisher (FKG dentaire SA, LaChaux‐de‐Fonds, Switzerland) with its hook‐shaped tip was designed for the final preparation and cleaning of complex root canal shapes (De‐Deus et al., 2019).
Only a few studies have analysed irrigant extrusion using new irrigation devices. EndoVac appears to reduce extrusion compared with conventional irrigation in extracted mature teeth (Romualdo et al., 2017). By contrast, the results in terms of extrusion for other devices such as RinsEndo, UAI, laser activation, SAF and the XP‐endo Finisher are inconclusive (Azim et al., 2018; Boutsioukis et al., 2013; Desai & Himel, 2009; Iriboz et al., 2015; Mitchell et al., 2011). Evidence on NaOCl extrusion in teeth with open apices is limited (dos Reis et al., 2020). The open apex situation is clinically relevant not only in immature teeth but also in resected teeth, teeth with root fractures, in teeth with extensive apical resorption and in teeth with an iatrogenically overprepared root canal beyond the apex when these teeth have to be root canal treated or retreated (Boutsioukis et al., 2013).
Therefore, the aim of this laboratory study was to evaluate the impact of seven methods of irrigant agitation on the apical pressure of NaOCl generated in teeth with an open apex. The research hypothesis was that all tested irrigation methods would never produce maximum pressure values exceeding the critical threshold of the central venous pressure (5.73 mmHg).
MATERIALS AND METHODS
Experimental setup
Experiments were performed on a 3D‐printed central maxillary incisor. The printed tooth was based on micro‐computed tomography imaging data of an immature tooth 21. The cross‐section of the canal terminus had a minimal diameter of 1.57 mm, a maximal diameter of 2.11 mm, a circumference of 5.84 mm and an area of 2.49 mm2. The total distance from the incisal edge to the canal terminus, henceforth referred to as tooth length (TL), was 17 mm. A 3D rendered (itk‐SNAPE, University of Pennsylvania) image of the micro‐computed tomography data and a photography of the immature tooth is shown in Figure 1.
FIGURE 1.
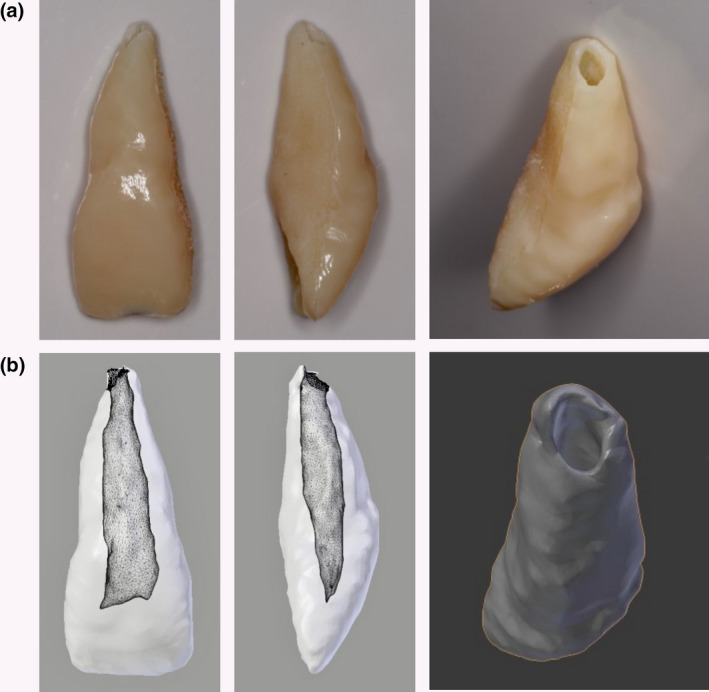
(a) 3D‐printed immature tooth 21 and (b) 3D rendered image of the micro‐computed tomography data in different aspects
The printed tooth was mounted in a threaded cylinder using C‐silicone putty material (Coltoflax; Coltène/Whaledent AG, Altstätten, Switzerland). The cylinder was placed on a pressure sensor, the enclosed chamber between apex and the membrane of the sensor was filled completely with water. The generated pressures during irrigation were thus transferred directly and without any alteration to the sensor owing to the lack of compressibility of water under the conditions in this laboratory setup. The pressure sensor (IMP 320; ICS Schneider Messtechnik GmbH, Hohen Neuendorf, Germany) had a measurement range of 0 to 120 mmHg. At an analogue output signal of 20 mA, the sensor registered with a precision of 0.1% and had a response time of ≤0.5 ms. Measurement data were transformed by an analogue‐digital converter (12bit, RedLab 1208FL USB Mini‐Messlabor; Meilhaus Electronic GmbH, Alling, Germany) and transferred via USB cable to a personal computer. Data were processed with a laboratory software (LabVIEW; International Instruments AG, Austin, TX, USA) with a customized written protocol to read and save the obtained data. Figure 2 shows the experimental setup.
FIGURE 2.
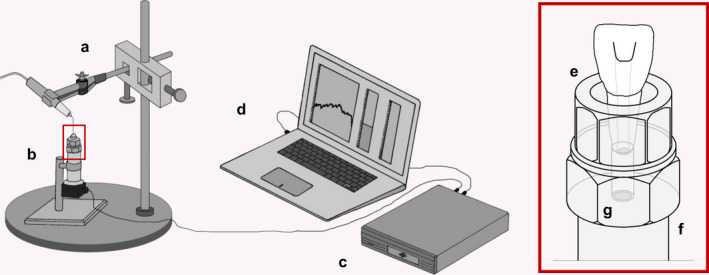
Experimental setup: (a) Irrigation device in an adjustable clamp. (b) 3D‐printed central incisor on the pressure sensor. (c) analogue‐digital converter. (d) Computer with laboratory software. (e) 3D‐printed central incisor embedded in a threaded cylinder by silicone. (f) Pressure sensor with (g) pressure membrane
Irrigation protocols
Irrigation was performed with seven irrigation devices. The activation time of each measurement was 10 s since preliminary tests had shown maximum pressure values to be reached within this time period. The measurement per group was repeated ten times. Before irrigation, the root canal and the pulp chamber were completely filled with 0.1 mL 1% NaOCl (Hänseler AG), Herisau, Switzerland. During the irrigation period of 10 s, no additional NaOCl was added to the root canal system except for the irrigation with EndoVac. The hand pieces were fixed in a solid and adjustable clamp.
UAI was performed using smooth wire irrigation instruments, Irri S files and the VDW.ULTRA unit (both VDW). Files with a size 25 and a length of 25 mm were used. Intensity levels of 10, 20 and 30 were employed (28–36 kHz).
Sonic irrigant activation was performed with EDDY, coupled to an air scaler handpiece, the SONICflex 2003 L handpiece (Kavo), which was connected to a dental unit (Teneo; Dentsply Sirona, York, PA, USA). The air scaler handpiece used to drive the EDDY tips was employed at its highest power setting at all times (Eggmann et al., 2020).
EndoVac was tested with the macrocannula and the microcannula. Since EndoVac creates negative pressure by suction, NaOCl was added during the irrigation process. Following the manufacturer's instructions, this was accomplished by a syringe. To monitor the force applied on the syringe plunger and to keep it as constant as feasible, the plunger of the syringe was equipped with a force sensor (KM25; Transmetra GmbH). The force sensor had a measurement range of 0 to 100 N. Data were converted, processed, read and saved as described above. The force applied on the syringe plunger never exceeded 20 N throughout the experiment. Irrigation with the macroannula required 2.5 mL additional NaOCl during the 10 s irrigation period, the microcannula required 0.3 mL additional NaOCl.
XP‐endo Finisher files with a length of 25 mm and size 25 were used. A torque of 1 Ncm and the rotation speed of 1000 rpm was chosen according to the manufacturer's recommendation.
The SAF was tested with a file of 21 mm in length and a diameter of 1.5 mm.
The five irrigation methods described above were tested at the following insertion depths: TL (i.e. flush to the canal terminus), TL—1 mm, TL—2 mm and TL—3 mm.
LiteTouch‐Induced Photomechanical Irrigation (LT‐IPI) was performed by using the Orcos medical litetouch III laser (Orcos medical AG, Küsnacht, Switzerland), an Er:YAG laser working at a wavelength of 2940 nm. Four different modes were tested, namely 20 mJ/10 Hz, 20 mJ/20 Hz, 20 mJ/50 Hz and 40 mJ/10 Hz. Laser activation was done with a bent handpiece and a tip with a length of 17 mm and a diameter of 0.4 mm. Each mode was performed at an insertion depth of 7 mm, which correlated with a position inside the coronal pulp chamber, and 11 mm, which correlated with the cementum‐enamel junction/the root canal orifice.
RinsEndo, a hydrodynamic irrigation system working at a frequency of 1.6 Hz and ejecting 105 µL of irrigant per second, was used at an insertion depth of 7, 11, 12.5 mm (the coronal third of the root canal), 14 mm (the middle of the root canal) and at TL.
The workflow of the experiments is summarized in Figure 3.
FIGURE 3.
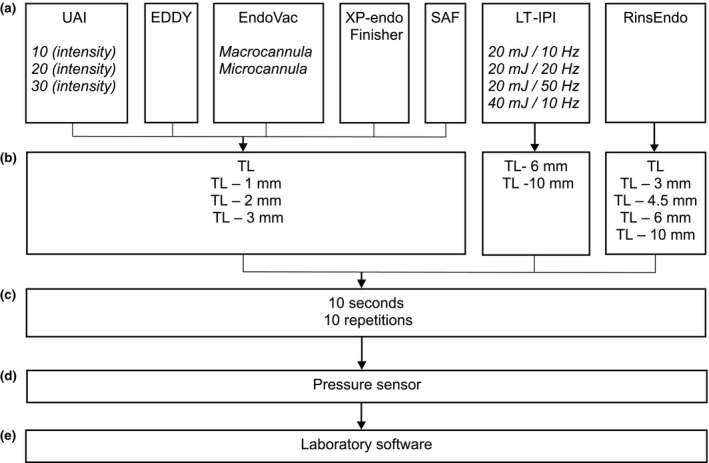
Workflow: setting and insertion depth of the seven irrigation methods. (a) Irrigation method and setting. (b) Insertion depth. (c) Irrigation. (d) Measurement. (e) Data processing
Data for irrigation by syringe were obtained from another study where irrigation by syringe was performed in the same experimental setup as described above (Jäggi et al., 2021). Irrigation by syringe was performed with a 30G side‐vented cannula, an applied pressure on the syringe plunger of 40 N and at an insertion depth of TL—1 mm.
Critical value and statistics
A descriptive statistical analysis was performed. The maximum pressure values of each measurement and the 95%—confidence intervals were subjected to the analysis. To gauge the risk of apical NaOCl extrusion, the lower limit of the mean central venous pressure of 5.73 mmHg (mean: 5.88 mmHg ± SD of 0.15 mmHg) was defined as the threshold. Pressure values exceeding this critical threshold were considered indicative of potential apical NaOCl extrusion.
RESULTS
Irrespective of the insertion depth, EndoVac, the SAF, the XP‐endo Finisher and UAI, across all its intensity levels (28–36 kHz), never exceeded the threshold value of 5.73 mmHg.
LT‐IPI did not exceed the threshold value at any insertion depth when used at frequencies ≤20 Hz (the manufacturer recommends a frequency of 10 to 15 Hz for irrigant activation). Irrigant activation at an intensity level of 20 mJ/50 Hz and an insertion depth to the pulp chamber resulted in the threshold value being exceeded in 10% of the measurements. At 20 mJ/50 Hz and an insertion depth to the root canal orifice, 50% of the measurements were above the threshold value.
EDDY used at TL exceeded the upper limit of the central venous pressure of 6.03 mmHg in 100% of the measurements. Pressure values above the threshold value of 5.73 mmHg were observed in 30%, 10% and 20% of the measurements when the EDDY tip was placed at TL—1 mm, TL—2 mm and TL—3 mm, respectively.
Hundred percent of the measurements with RinsEndo lay over the upper limit of the central venous pressure of 6.03 mmHg, irrespective of the insertion depth.
Table 1 shows the detailed results of all irrigation methods in relation to the lower and upper limit of the central venous pressure (5.73 mmHg/6.03 mmHg). Also, data for irrigation by syringe are shown in Table 1.
TABLE 1.
Results: Maximum values, mean, standard deviation (SD), 95% confidence interval (CI), percentage of measurements exceeding 5.73 mmHg per irrigation method; maximum value above 6.03 mmHg (red) and maximum value above 5.73 mmHg (orange)
| Irrigation | Setting | Insertion depth | Maximum (mmHg) | Mean (mmHg) | SD | 95% CI | Percentage >5.73 mmHg (%) |
|---|---|---|---|---|---|---|---|
| UAI | 10 (intensitiy) | TL | 0.47 | 0.28 | 0.13 | 0.19–0.38 | 0 |
| TL—1 mm | 0.41 | 0.19 | 0.10 | 0.11–0.26 | 0 | ||
| TL—2 mm | 0.23 | 0.08 | 0.06 | 0.04–0.13 | 0 | ||
| TL—3 mm | 0.29 | 0.17 | 0.08 | 0.12–0.23 | 0 | ||
| 20 (intensitiy) | TL | 1.17 | 0.77 | 0.32 | 0.54–0.98 | 0 | |
| TL—1 mm | 0.77 | 0.42 | 0.17 | 0.30–0.54 | 0 | ||
| TL—2 mm | 0.35 | 0.17 | 0.08 | 0.12–0.23 | 0 | ||
| TL—3 mm | 0.41 | 0.17 | 0.18 | 0.03–0.23 | 0 | ||
| 30 (intensity) | TL | 1.23 | 0.91 | 0.26 | 0.73–1.13 | 0 | |
| TL—1 mm | 1.00 | 0.67 | 0.23 | 0.50–0.83 | 0 | ||
| TL—2 mm | 0.47 | −0.01 | 0.40 | −0.29 to 0.28 | 0 | ||
| TL—3 mm | 0.65 | 0.09 | 0.50 | −0.26 to 0.44 | 0 | ||
| EDDY | TL | 9.79 | 8.48 | 0.90 | 7.80–9.15 | 100 | |
| TL—1 mm | 6.56 | 4.82 | 1.28 | 3.90–5.78 | 30 | ||
| TL—2 mm | 6.39 | 3.77 | 1.37 | 2.78–4.73 | 10 | ||
| TL—3 mm | 6.44 | 4.99 | 0.92 | 4.28–5.55 | 20 | ||
| EndoVac | Macrocannula | TL | 0.12 | −0.14 | 0.13 | −0.23 to −0.05 | 0 |
| TL—1 mm | 0.06 | −0.16 | 0.11 | −0.24 to −0.08 | 0 | ||
| TL—2 mm | 0.00 | −0.12 | 0.08 | −0.17 to −0.06 | 0 | ||
| TL—3 mm | 0.00 | −0.17 | 0.08 | −0.23 to −0.07 | 0 | ||
| Microcannula | TL | 1.88 | 1.45 | 0.20 | 1.28–1.58 | 0 | |
| TL—1 mm | 2.05 | 1.64 | 0.32 | 1.35–1.80 | 0 | ||
| TL—2 mm | 2.64 | 1.82 | 0.50 | 1.43–2.18 | 0 | ||
| TL—3 mm | 2.46 | 2.21 | 0.38 | 1.65–2.25 | 0 | ||
| RinsEndo | TL | 107.65 | 96.71 | 11.66 | 88.36–105.08 | 100 | |
| Middle of root canal | 107.30 | 96.94 | 10.72 | 89.26–104.63 | 100 | ||
| Coronal third of root canal | 64.46 | 56.19 | 4.28 | 53.10–59.25 | 100 | ||
| Root canal orifice | 71.90 | 57.10 | 7.65 | 51.60–62.56 | 100 | ||
| Coronal pulp chamber | 46.59 | 37.77 | 7.23 | 32.55–42.83 | 100 | ||
| LT‐IPI | 20 mJ/10 Hz | Root canal orifice | 1.94 | 1.52 | 0.24 | 1.35–1.65 | 0 |
| Pulp chamber | 1.17 | 0.91 | 0.14 | 0.83–0.98 | 0 | ||
| 20 mJ/20 Hz | Root canal orifice | 4.04 | 3.31 | 0.44 | 3.00–3.60 | 0 | |
| Pulp chamber | 2.81 | 2.13 | 0.47 | 1.80–2.48 | 0 | ||
| 20 mJ/50 Hz | Root canal orifice | 6.62 | 5.66 | 0.68 | 5.18–6.15 | 50 | |
| Pulp chamber | 5.80 | 4.35 | 0.84 | 3.75–4.95 | 10 | ||
| 40 mJ/10 Hz | Root canal orifice | 4.34 | 3.83 | 0.29 | 3.60–4.05 | 0 | |
| Pulp chamber | 2.64 | 2.17 | 0.34 | 1.95–2.40 | 0 | ||
| SAF | TL | 1.23 | 0.82 | 0.23 | 0.66–0.98 | 0 | |
| TL—1 mm | 0.88 | 0.69 | 0.12 | 0.61–0.75 | 0 | ||
| TL—2 mm | 1.00 | 0.70 | 0.17 | 0.59–0.83 | 0 | ||
| TL—3 mm | 1.00 | 0.71 | 0.16 | 0.60–0.83 | 0 | ||
| XP‐endo Finisher | TL | 0.53 | 0.20 | 0.16 | 0.09–0.32 | 0 | |
| TL—1 mm | 0.12 | 0.08 | 0.04 | 0.05–0.10 | 0 | ||
| TL—2 mm | 0.12 | 0.09 | 0.04 | 0.07–0.11 | 0 | ||
| TL—3 mm | 0.17 | 0.11 | 0.04 | 0.08–0.14 | 0 | ||
| Syringe | 40 N (force) | TL—1 mm | 2.64 | 1.10 | 0.51 | 0.88–1.31 | 0 |
Data for syringe irrigation were obtained from a previous study (Jäggi et al., 2021).
Figure 4 A representative graph for each irrigation method outlining the changes in the apical pressure through the irrigation period of 10 s.
FIGURE 4.
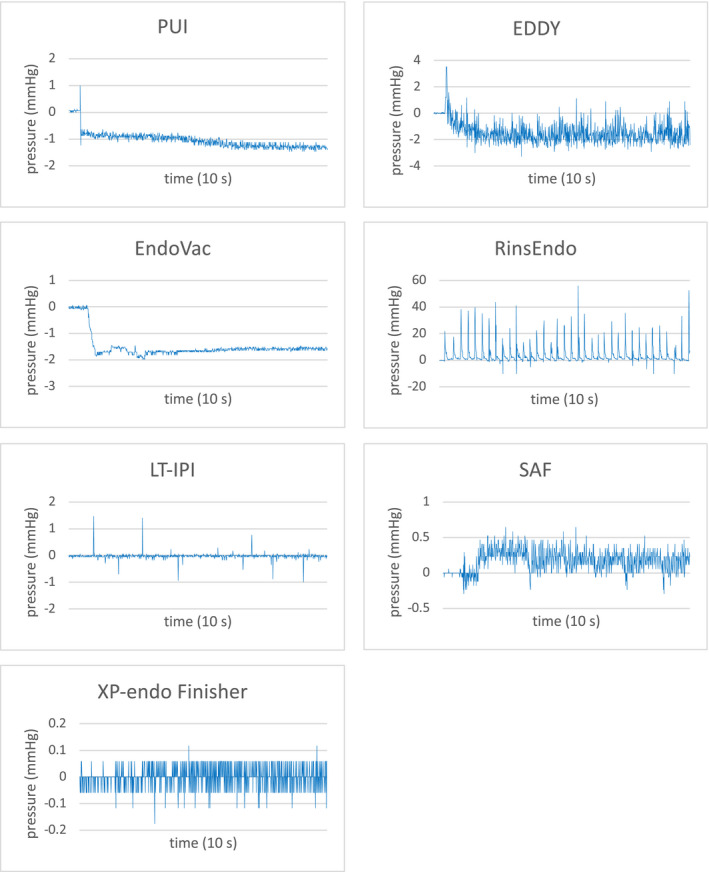
Representative graph for each irrigation method. The pressure values are not true to scale for a better understanding of the pressure gradients
DISCUSSION
This laboratory study evaluated the apical pressure of NaOCl generated during irrigation with seven irrigation methods in a simulated tooth with an open apex. EndoVac, the SAF, the XP‐endo Finisher and UAI produced pressures below the critical threshold. Laser activation (LT‐IPI) produced pressures below the critical threshold as long as the intensity level is chosen according to the manufacturer's recommendation. Irrigation with RinsEndo, by contrast, produced pressures far above the critical threshold. Likewise, sonic activation with EDDY created pressures exceeding the threshold. Thus, irrigant activation using RinsEndo and EDDY may lead to irrigant reaching the periapical tissue, potentially causing NaOCl extrusion accidents in teeth with open apices. Consequently, irrigant activation using RinsEndo and EDDY should be used with caution in immature teeth.
It remains elusive which apical pressure threshold needs to be exceeded for irrigant extrusion to occur to an extent that is clinically relevant (Park et al., 2013). The present investigation, in accordance with previous studies, chose the central venous pressures as a reference. It is, however, important to bear in mind that different threshold values may be applicable. Threshold values used in other studies are 25 mmHg representing the capillary pressure, 20–30 mmHg representing the interstitial pressure and 30 mmHg representing the intraosseous blood pressure (Charara et al., 2016; Goode et al., 2013; Khan et al., 2013; Lorono et al., 2020; Park et al., 2013; Zhu et al., 2013). The lowest reference value reported in the literature was chosen in the present study in order to err on the side of caution when providing recommendations. The results differ when shifting the threshold to other values mentioned in the literature (20–30 mmHg). Sonic activation with EDDY, in particular, generated maximal values that seem to be acceptable when considering critical values that are above the central venous pressure.
Theories concerning the conditions enabling serious ecchymotic NaOCl accidents have been discussed in several studies. As a necessary condition, the apical foramen has to be patent for the irrigant to extrude (Zhu et al., 2013). The setup in the present study, using a simulated tooth with a wide open apex, replicated this condition. Furthermore, due consideration must be given to individual conditions that may affect the periapical pressure. In maxillary teeth as well as in females in general, the counterpressure may be affected by lower bone density (Boutsioukis et al., 2013). The periapical pressure may thus likely be lower. In addition, the location of the root apex in the maxillary sinus or towards other soft tissues may favour extrusion. The pulp and periapical status prior to the extrusion have been reported to have an influence. Presumably, situations with periapical pathosis and situations with healthy periapical tissues are dissimilar (Boutsioukis et al., 2013; Kleier et al., 2008).
Other studies examining irrigant extrusion neglected the presence of periapical tissues, for instance by surrounding the apical foramen only by atmospheric air (Boutsioukis et al., 2013). In the present study, extrusion was quantified as pressure in mmHg. This may be methodologically advantageous because the reference point can be adjusted if and when new evidence on periapical pressures emerges.
The generated pressures were recorded at an interval of 10 ms by a high‐precision pressure sensor with a metering precision of 0.1% and a response time of ≤0.5 ms within a measuring range of 0–120 mmHg. Negative pressures were recorded (irrigation using EndoVac), too. Negative pressure readings must, however, be treated with caution as the pressure sensor was not calibrated to register negative pressures.
As the recommendations of the manufacturers concerning, the insertion depths of the irrigation device into the root canal system varied and are related to the so‐called working length (WL) in teeth with fully formed apices, several insertion depths were tested. The respective manufacturers recommend to insert EDDY one millimetre short of full WL, to insert EndoVac, the XP‐endo Finisher and SAF to WL, to insert the special cannula of RinsEndo to the coronal third of the root canal and to insert the tip of the LT‐IPI into the coronal pulp chamber. The insertion depths in the present study were on one hand chosen to comply with the manufacturer's recommendations but also to induce potential outliers (e.g. insertion of RinsEndo to TL). Owing to these considerations, LT‐IPI was not only tested at 10 and 15 Hz in accordance with the manufacturer's recommendation but also at 20 and 50 Hz. Mounting the irrigation devices into a solid and adjustable clamp provided constant defined and reproducible insertion depths.
There are only a few previous studies investigating irrigant delivery and activation with different irrigation devices in immature teeth. The results of the current study are in agreement with the results of previous studies. dos Reis et al. (2020) reported higher extrusion values when sonic agitation with the EDDY instrument was performed. On the contrary, the XP‐endo Finisher produced less irrigant extrusion than EDDY, comparable to the extrusion when irrigating by syringe (dos Reis et al., 2020).
Irrigation by syringe was tested in the same setting in another study (Jäggi et al., 2021). The apical pressures were dependent on the diameter of the cannula (G25 versus G30), the needle tip design (open‐ended versus side‐vented), the insertion depth (TL, TL—1 mm, TL—2 mm, TL—4 mm) and the applied pressure on the syringe plunger (10 N, 20 N, 40 N, 80 N). When considering conditions realistic to daily practice (applied pressures on the syringe plunger: 40 N, irrigation with an G30 side‐vented cannula, insertion depth: TL—1 mm) the maximum value amounted 2.64 mmHg and the mean 1.71 mmHg. Conventional irrigation performed as mentioned results in higher apical pressures than EndoVac, UAI, the SAF and the XP‐Endo finisher at an insertion depth of TL—1 mm. Nevertheless, the critical value of 5.73 mmHg was never exceeded when performing conventional irrigation as mentioned above.
Although severe NaOCl accidents are considered to be rare, the issue of irrigant extrusion is of crucial importance. NaOCl accidents can have grave consequences, first and foremost for the patients who are affected, but also for the dentists involved (Zhu et al., 2013). In a survey, almost half of the endodontists in the United States reported to have experienced at least one accident in their practice (Kleier et al., 2008). The present study may provide information to help to minimize the risk for such accidents.
The present study indicates that, in immature teeth and in other cases with open apices, the various irrigant methods tested have little risk for apical irrigant extrusion. These laboratory data suggest that NaOCl, with its numerous advantageous properties, can be used as irrigant in teeth with open apices when one of the recommended methods (EndoVac, UAI, SAF, XP‐Endo finisher) is employed for improving disinfection and cleaning of the root canal without risk of apical extrusion when used cautiously.
CONCLUSION
In a maxillary central incisor with an open apex, irrigation with LT‐IPI respecting the manufacturer's recommendation, EndoVac, UAI, the SAF and the XP‐endo Finisher generate periapical pressures that were below the critical threshold of the central venous pressure (5.73 mmHg).
Performing irrigation with RinsEndo or EDDY in teeth with an open apex produced pressures higher than the critical threshold. The safety of these devices in immature teeth therefore warrants further investigation.
ETHICAL APPROVAL
Ethical approval was obtained from the local Research Ethics Committee (EKNZ UBE‐15/111).
CONFLICT OF INTEREST
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
AUTHOR CONTRIBUTION
E. Magni: Conceptualization, Visualization, Data curation, Investigation, Formal analysis, Writing –original draft, Writing –review & editing. M. Jäggi: Conceptualization, Visualization, Writing –review & editing. F. Eggmann: Formal analysis, Writing –original draft, Writing –review & editing. R. Weiger.: Conceptualization, Writing –review & editing. T. Connert: Conceptualization, Visualization, Data curation, Formal analysis, Writing –review & editing.
Magni, E. , Jäggi, M. , Eggmann, F. , Weiger, R. & Connert, T. (2021) Apical pressures generated by several canal irrigation methods: A laboratory study in a maxillary central incisor with an open apex. International Endodontic Journal, 54, 1937–1947. 10.1111/iej.13575
REFERENCES
- Azim, A.A. , Aksel, H. , Margaret Jefferson, M. & Huang, G.T. (2018) Comparison of sodium hypochlorite extrusion by five irrigation systems using an artificial root socket model and a quantitative chemical method. Clinical Oral Investigations, 22, 1055–1061. [DOI] [PubMed] [Google Scholar]
- Baumann, U.A. , Marquis, C. , Stoupis, C. , Willenberg, T.A. , Takala, J. & Jakob, S.M. (2005) Estimation of central venous pressure by ultrasound. Resuscitation, 64, 193–199. [DOI] [PubMed] [Google Scholar]
- Boutsioukis, C. , Gogos, C. , Verhaagen, B. , Versluis, M. , Kastrinakis, E. & Van der Sluis, L.W. (2010) The effect of root canal taper on the irrigant flow: evaluation using an unsteady Computational Fluid Dynamics model. International Endodontic Journal, 43, 909–916. [DOI] [PubMed] [Google Scholar]
- Boutsioukis, C. , Psimma, Z. & van der Sluis, L.W. (2013) Factors affecting irrigant extrusion during root canal irrigation: a systematic review. International Endodontic Journal, 46, 599–618. [DOI] [PubMed] [Google Scholar]
- Buttler, T.K. & Crawford, J.J. (1982) The detoxifying effect of varying concentrations of sodium hypochlorite on endotoxins. Journal of Endodontics, 8, 59–66. [DOI] [PubMed] [Google Scholar]
- Charara, K. , Friedman, S. , Sherman, A. , Kishen, A. , Malkhassian, G. , Khakpour, M. et al. (2016) Assessment of apical extrusion during root canal irrigation with the novel gentlewave system in a simulated apical environment. Journal of Endodotics, 42, 135–139. [DOI] [PubMed] [Google Scholar]
- Conde, A.J. , Estevez, R. , Loroño, G. , Valencia de Pablo, Ó. , Rossi‐Fedele, G. & Cisneros, R. (2017) Effect of sonic and ultrasonic activation on organic tissue dissolution from simulated grooves in root canals using sodium hypochlorite and EDTA. International Endodontic Journal, 50, 976–982. [DOI] [PubMed] [Google Scholar]
- De‐Deus, G. , Belladonna, F.G. , de Siqueira Zuolo, A. , Perez, R. , Carvalho, M.S. , Souza, E.M. et al. (2019) Micro‐CT comparison of XP‐endo Finisher and passive ultrasonic irrigation as final irrigation protocols on the removal of accumulated hard‐tissue debris from oval shaped‐canals. Clinical Oral Investigations, 23, 3087–3093. [DOI] [PubMed] [Google Scholar]
- De‐Deus, G. , Souza, E.M. , Barino, B. , Maia, J. , Zamolyi, R.Q. , Reis, C. et al. (2011) The self‐adjusting file optimizes debridement quality in oval‐shaped root canals. Journal of Endodontics, 37, 701–705. [DOI] [PubMed] [Google Scholar]
- Desai, P. & Himel, V. (2009) Comparative safety of various intracanal irrigation systems. Journal of Endodontics, 35, 545–549. [DOI] [PubMed] [Google Scholar]
- dos Reis, S. , Cruz, V.M. , Hungaro Duarte, M.A. , da Silveira Bueno, C.E. , Vivan, R.R. , Pelegrine, R.A. et al. (2020) Volumetric analysis of irrigant extrusion in immature teeth after different final agitation techniques. Journal of Endodontics, 46, 682–687. [DOI] [PubMed] [Google Scholar]
- Dutner, J. , Mines, P. & Anderson, A. (2012) Irrigation trends among American Association of Endodontists members: a web‐based survey. Journal of Endodontics, 38, 37–40. [DOI] [PubMed] [Google Scholar]
- Eggmann, F. , Vokac, Y. , Eick, S. & Neuhaus, K.W. (2020) Sonic irrigant activation for root canal disinfection: power modes matter! BMC Oral Health, 20, 102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goode, N. , Khan, S. , Eid, A.A. , Niu, L. , Gosier, J. , Susin, L.F. et al. (2013) Wall shear stress effects of different endodontic irrigation techniques and systems. Journal of Dentistry, 41, 636–641. [DOI] [PubMed] [Google Scholar]
- de Groot, S.D. , Verhaagen, B. , Versluis, M. , Wu, M.K. , Wesselink, P.R. & van der Sluis, L.W. (2009) Laser‐activated irrigation within root canals: cleaning efficacy and flow visualization. International Endodontic Journal, 42, 1077–1083. [DOI] [PubMed] [Google Scholar]
- Gulabivala, K. , Patel, B. , Evans, G. & Ng, Y.‐L. (2005) Effects of mechanical and chemical procedures on root canal surfaces. Endodontic Topics, 10, 103–122. [Google Scholar]
- Haapasalo, M. , Endal, U. , Zandi, H. & Coil, J.M. (2005) Eradication of endodontic infection by instrumentation and irrigation solutions. Endodontic Topics, 10, 77–102. [Google Scholar]
- Hollinshead, W.H. (1968) Anatomy for surgeons: volume 1—the head and neck, 3rd edition. Jagerstown: Harper and Row. [Google Scholar]
- Hülsmann, M. & Hahn, W. (2000) Complications during root canal irrigation—literature review and case reports. International Endodontic Journal, 33, 186–193. [DOI] [PubMed] [Google Scholar]
- Iriboz, E. , Bayraktar, K. , Turkaydin, D. & Tarcin, B. (2015) Comparison of apical extrusion of sodium hypochlorite using 4 different root canal irrigation techniques. Journal of Endodontics, 41, 380–384. [DOI] [PubMed] [Google Scholar]
- Jäggi, M. , Magni, E. , Eggmann, F. , ElAyouti, A. , Connert, T. & Weiger, R. (2021) Apical pressure generated using conventional syringe irrigation in immature teeth—an in vitro study. Materials, 14, 2580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan, S. , Niu, L. , Eid, A.A. , Looney, S.W. , Didato, A. , Roberts, S. et al. (2013) Periapical pressures developed by nonbinding irrigation needles at various irrigation delivery rates. Journal of Endodontics, 39, 529–533. [DOI] [PubMed] [Google Scholar]
- Kleier, D.J. , Averbach, R.E. & Mehdipour, O. (2008) The sodium hypochlorite accident: experience of diplomates of the American Board of Endodontics. Journal of Endoddontics, 34, 1346–1350. [DOI] [PubMed] [Google Scholar]
- Lacerda, M. , Marceliano‐Alves, M.F. , Perez, A.R. , Provenzano, J.C. , Neves, M.A.S. , Pires, F.R. et al. (2017) Cleaning and shaping oval canals with 3 instrumentation systems: a correlative micro‐computed tomographic and histologic study. Journal of Endodontics, 43, 1878–1884. [DOI] [PubMed] [Google Scholar]
- Lorono, G. , Zaldivar, J.R. , Arias, A. , Cisneros, R. , Dorado, S. & Jimenez‐Octavio, J.R. (2020) Positive and negative pressure irrigation in oval root canals with apical ramifications: a computational fluid dynamics evaluation in micro‐CT scanned real teeth. International Endodontic Journal, 53, 671–679. [DOI] [PubMed] [Google Scholar]
- Lyons, R.H. , Kennedy, J. & Burwell, C. (1938) The measurement of venous pressure by the direct method. American Heart Journal, 16, 675–693. [Google Scholar]
- Metzger, Z. , Teperovich, E. , Zary, R. , Cohen, R. & Hof, R. (2010) The self‐adjusting file (SAF). Part 1: respecting the root canal anatomy—a new concept of endodontic files and its implementation. Journal of Endodontics, 36, 679–690. [DOI] [PubMed] [Google Scholar]
- Mitchell, R.P. , Baumgartner, J.C. & Sedgley, C.M. (2011) Apical extrusion of sodium hypochlorite using different root canal irrigation systems. Journal of Endodontics, 37, 1677–1681. [DOI] [PubMed] [Google Scholar]
- Neuhaus, K.W. , Liebi, M. , Stauffacher, S. , Eick, S. & Lussi, A. (2016) Antibacterial efficacy of a new sonic irrigation device for root canal disinfection. Journal of Endodontics, 42, 1799–1803. [DOI] [PubMed] [Google Scholar]
- Nielsen, B.A. & Baumgartner, C.J. (2007) Comparison of the EndoVac system to needle irrigation of root canals. Journal of Endodontics, 33, 611–615. [DOI] [PubMed] [Google Scholar]
- Park, E. , Shen, Y. , Khakpour, M. & Haapasalo, M. (2013) Apical pressure and extent of irrigant flow beyond the needle tip during positive‐pressure irrigation in an in vitro root canal model. Journal of Endodontics, 39, 511–515. [DOI] [PubMed] [Google Scholar]
- Pashley, E.L. , Birdsong, N.L. , Bowman, K. & Pashley, D.H. (1985) Cytotoxic effects of NaOCl on vital tissue. Journal of Endodontics, 11, 525–528. [DOI] [PubMed] [Google Scholar]
- Peters, O.A. (2004) Current challenges and concepts in the preparation of root canal systems: a review. Journal of Endodontics, 30, 559–567. [DOI] [PubMed] [Google Scholar]
- Rodig, T. , Sedghi, M. , Konietschke, F. , Lange, K. , Ziebolz, D. & Hulsmann, M. (2010) Efficacy of syringe irrigation, RinsEndo and passive ultrasonic irrigation in removing debris from irregularities in root canals with different apical sizes. International Endodontic Journal, 43, 581–589. [DOI] [PubMed] [Google Scholar]
- Romualdo, P.C. , de Oliveira, K.M.H. , Nemezio, M.A. , Küchler, E.C. , Silva, R.A.B. , Nelson‐Filho, P. et al. (2017) Does apical negative pressure prevent the apical extrusion of debris and irrigant compared with conventional irrigation? A systematic review and meta‐analysis. Australian Endodontic Journal, 43, 129–137. [DOI] [PubMed] [Google Scholar]
- Shen, Y.A. , Gao, Y. , Qian, W. , Ruse, N.D. , Zhou, X. , Wu, H. et al. (2010) Three‐dimensional numeric simulation of root canal irrigant flow with different irrigation needles. Journal of Endodontics, 36, 884–889. [DOI] [PubMed] [Google Scholar]
- van der Sluis, L.W. , Versluis, M. , Wu, M.K. & Wesselink, P.R. (2007) Passive ultrasonic irrigation of the root canal: a review of the literature. International Endodontic Journal, 40, 415–426. [DOI] [PubMed] [Google Scholar]
- Spencer, H.R. , Ike, V. & Brennan, P.A. (2007) Review: the use of sodium hypochlorite in endodontics–potential complications and their management. British Dental Journal, 202, 555–559. [DOI] [PubMed] [Google Scholar]
- Zaugg, L.K. , Savic, A. , Amato, M. , Amato, J. , Weiger, R. & Connert, T. (2019) Endodontic treatment in Switzerland. A National Survey. Swiss Dental Journal, 130, 18–29. [DOI] [PubMed] [Google Scholar]
- Zehnder, M. (2006) Root canal irrigants. Journal of Endodontics, 32, 389–398. [DOI] [PubMed] [Google Scholar]
- Zhu, W.‐C. , Gyamfi, J. , Niu, L. , Schoeffel, G.J. , Liu, S.‐Y. , Santarcangelo, F. et al. (2013) Anatomy of sodium hypochlorite accidents involving facial ecchymosis—a review. Journal of Dentistry, 41, 935–948. [DOI] [PMC free article] [PubMed] [Google Scholar]