

Abstract
Background
Oncology patients carry a substantial risk of developing pleural empyema. Here, we report the preliminary results of our early video‐assisted thoracoscopic surgery (VATS) lavage strategy in cases of empyema occurring in patients undergoing (radio‐) chemotherapy.
Methods
This was a retrospective case–control study comparing early VATS lavage (test group, current therapy since January 2018, n = 46) versus VATS pleurectomy (historical control; before January 2018, n = 46).
Results
Five patients in the control group and one in the test group developed recurrence of empyema within 30 days. Complications were more severe and more frequently observed in the historical control group than in the test group (30/46 vs. 12/46 CI: 5%–95%, p = < 0.05). Early VATS lavage saved operating time, allowed a shorter ICU stay (2.6 days CI: 5%–95% vs. 5.1 days CI: 5%–95%, p = ns) and an earlier hospital discharge (6.1 days CI: 5%–95% vs. 13.5 days CI: 5%–95%, p < 0.05). Moreover, radio and/or chemotherapy could be reinitiated earlier (15 ± 20.5 days CI: 5%–95% vs. 40 ± 12 days CI: 5%–95%, p < 0.05).
Conclusions
In this retrospective cohort study, early VATS lavage was found to have a beneficial effect especially on hospital stay and enabling an earlier restart of radio‐ and/or chemotherapy.
Keywords: empyema, pleura, thoracic surgery
How new early and less invasive video‐assisted thoracoscopic surgery (VATS) strategy for the management of empyema in oncology patients could reduce postoperative morbidity? Early VATS lavage and partial decortication seems to safeguard oncology patients with a progressed empyema (ATS phase II and III) from more complex surgical procedures, shortening the hospital stay, reducing the risk of postoperative complications and permitting an earlier restart of oncological therapy.

INTRODUCTION
Infections of the pleural space present in a highly variable manner and affect a heterogeneous population of patients with various underlying etiological conditions. 1 , 2
The increasing number of therapeutic options in oncology has led to a substantial improvement in survival but also to a consequential increase in complications. 3 , 4 , 5 These two risks factors for infections facilitate the development of pneumonia and empyema, especially in those patients undergoing chemotherapy.
Development of an empyema may occur very rapidly and require early surgical treatment to avoid the risk of sepsis, respiratory and multiorgan failure. 5 , 6 Empyema mortality rates, independent of the underlying disease, have been reported to be between 7% and 33%. 2 , 5 , 7 , 8 , 9 Moreover, in elderly patients, morbidity and mortality varies between 50% and 70%. 7 , 8 , 9 , 10 To our knowledge, there are no data in literature regarding empyema morbidity/mortality in oncology patients.
Based on our clinical experience, we introduced a new early and less invasive video‐assisted thoracoscopic surgery (VATS) strategy for the management of empyema in oncology patients and evaluated the success rate focusing on early postoperative results and recurrence of empyema.
METHODS
Study design and population
This was a retrospective case–control study which compared two consecutive surgical management strategies, before and after the introduction of a new treatment algorithm, between January 2015 to December 2017 (control group) and January 2018 to December 2019 (test group).
Algorithm of treatment and surgical procedures
The diagnosis and the classification in both groups was based on microbiological analysis of pleural fluid and a contrast‐enhanced computed tomography (CT) scan.
Patients were classified following the classification drafted by the subcommittee on surgery of the American Thoracic Society (ATS) in 1962. The American Thoracic Society divides pleural empyema pathologically and clinically into three phases reflecting the normal progression. (i) In the exudative phase (stage I) effusion accumulates within the pleural space by extension of the inflammatory process into the pleura: cell count is low and the lung is characteristically re‐expandable. (ii) The fibropurulent‐intermediate phase (stage II) is characterized by pus, invasion of polymorphonuclear leukocytes, and fibrin depositions on the pleural surfaces and within the exudate leading to loculations. While this pathophysiological mechanism prevents extension of the empyema, it inhibits an adequate expansion of the lung. (iii) In the late organized phase (stage III), fibroblast growth produces inelastic membranes and fixes the lung, diaphragm, and chest wall. 11 Contrast‐enhanced CT is considered the most optimal form of imaging to diagnose empyema. CT allows the presence of the thickening and the enhancement of the adjacent pleural layers to be visualized. The thickening and enhancement of the inner visceral and outer parietal pleura are radiological signs of an empyema. 12 CT is also nearly 100% accurate in its ability to distinguish an empyema from an intraparenchymal lung abscess.
Additionally, in some cases, we performed a preoperative ultrasound to find the optimal trocar positioning or “surgical window” for a mini‐thoracotomy.
The procedure was always performed by one qualified thoracic surgeon.
In both groups, patients with empyema in phase I received the similar treatment: thoracentesis (for a sample of pleural fluid to determine pH, lactate dehydrogenase, glucose, protein levels, and blood cell count) and an appropriate antibiotic therapy.
1 Control group (Figure 1)
Phase II: patients initially had a chest tube drain inserted and antibiotic therapy. VATS pleurectomy was performed only in case of clinical worsening within 48 h (fever, increase in inflammatory values, worsening of oxygen saturation).
Phase III: patients received immediate VATS‐pleurectomy. In cases of intraoperative complication, pleural adhesion or decortication requirement, VATS was converted into a posterolateral thoracotomy with dissection of the latissimus dorsi muscle.
FIGURE 1.

Algorithm of surgical treatment in the control group (VATS pleurectomy). Phase II patients all had a chest tube drain inserted and antibiotic therapy. A VATS pleurectomy was only performed if a patient's condition worsened. Phase III patients underwent VATS pleurectomy. The open approach was reserved for cases of decortication, control of bleeding or lung surface control (adhesion). A posterolateral thoracotomy with dissection of the latissimus dorsi muscle is always proposed
2 Test group (Figure 2)
-
Phase II: patients were layered depending on risk factors for empyema and clinical worsening (currently undergoing chemotherapy, leukocytes<3.5 G/L, high inflammatory values ‐CRP > 2 mg/dl; IL‐6 > 20 pg/ml).
Patients with no risk factors had a chest tube drain inserted and appropriate antibiotic therapy.
Patients with one or more risk factors underwent VATS lavage and chest tube drainage.
Phase III: patients received a VATS lavage with removal of membrane and partial decortication (only on not completely expanded pulmonary surface) within 24 h from the first radiological/microbiological diagnosis of empyema. Total extended pleurectomy and decortication was not performed routinely. In stage III, the lung areas not adequately intraoperatively expanded were routinely identified and decortication was performed only in these sites. An extended pleurectomy and decortication (complete pulmonary surface) was performed only in cases of insufficient lung expansion. We switched from VATS into a muscle sparing mini‐thoracotomy or thoracotomy only in the case of complications or intraoperative diagnosis of thickened pleura and diffuse intrathoracic adhesion.
VATS lavage consisted of an extensive debridement and ablation of all septa allowing the entire pleural cavity to be unified and abundant irrigation of the pleural cavity with at least 2 L of physiological solution to be performed.
FIGURE 2.

Algorithm of surgical treatment in the test group (VATS lavage). Phase II patients were stratified into two different treatments arms depending on the risk factors. Phase III patients underwent the invasive surgical option. The open approach (muscle sparing mini‐thoracotomy) was reserved for cases of decortication or adhesion
The visceral and parietal pleura were resected during a total extended pleurectomy/decortication as completely as possible, with attention paid to the visceral pleura in order to avoid air leakage. The adequacy of the decortication in order to achieve sufficient lung re‐expansion was always confirmed during surgery by two‐lung ventilation. Two chest tubes (both 24 Fr) were positioned towards the chest apex and posterior costophrenic angle.
Muscle sparing mini‐thoracotomy is a less invasive open approach, as compared with the posterolateral technique, consisting of a 5–7 cm long thoracotomy performed in the fifth intercostal space without cutting the latissimus dorsi muscle and one or two thoracoscopic trocars located in the sixth and seventh intercostal spaces.
Variables analyzed
Demographics: age and sex
Clinical details: phases of empyema, oncological diagnosis, patients under chemo‐radiotherapy, time between diagnosis of empyema and operative treatment, time between surgery and resumption of oncology therapy, comorbidities;
Type of surgery: conservative treatment (thoracentesis and antibiotics + diuretics), VATS for lavage and chest tube drainage, VATS for pleurectomy and lavage, mini‐thoracotomy for pleurectomy and decortication, posterolateral thoracotomy for pleurectomy and decortication;
Postoperative data: reoperation within 30 days, intraoperative complications, operation time, ICU and hospital stay.
Primary and secondary outcomes
Primary outcome
Recurrence of empyema after surgical procedure was defined as a clinical condition after the fifth postoperative day meeting two or more of the following criteria: increase of inflammatory values, pleural fluids >200 ml/24 h, persistent pleural effusion, septations and loculations at CT‐scan and worsening of the respiratory condition.
Secondary outcome
Postoperative complications were defined as any complication occurring during hospitalization or within the first 30 postoperative days. Postoperative complications were divided into surgical and medical events and classified according to Clavien‐Dindo criteria. 13 Surgical complications were further defined as reoperation, bleeding requiring blood transfusion and surgical site infection. Medical complications were defined as cardiovascular, pulmonary, renal, sepsis, and other events. Events requiring reoperation, intensive care unit admission, or hospitalization longer than 15 days were defined as major complications (Clavien‐Dindo > grade III).
Statistical analysis
Data are presented as median or average ± standard error for continuous variables and number (percentage) for categorical variables. Survival statistics were described with the Kaplan‐Meier method. Matched‐pairs Fisher's exact test was used for the comparative statistics between categorical variables. Between continuous variables, nonparametric comparison of means between independent variables (Mann–Whitney U test) was performed. Survival comparison was analyzed using the log‐rank test. Multivariate analysis was performed using Cox‐regression (inclusion method). A two‐tailed p‐value of ≤ 0.05 was considered statistically significant. Data was entered into an Excel file, exported as .cvs. Survival and multivariate analysis were performed using SPSS version 24. All other analyses were performed using Python and Pandas software (Anaconda Inc.).
RESULTS
The clinical records of 289 consecutive patients with empyema who underwent surgery at the Division of General, Visceral and Thoracic Surgery Feldkirch between January 2015 and December 2019 were analyzed retrospectively. Ninety‐two patients with empyema and associated active malignant disease were included in this study (46 in the control group and 46 in the test group). The clinical characteristics and the risk profile of all 92 patients are summarized in Table 1. Most patients were under chemotherapy (in both groups: 69.5%) or radiotherapy (control group: 26%; test group: 30.4%). The most frequent cancer origin was the lung (control group: 43.4%; test group: 26%) and breast (control group: 26%; test group: 34.7%). At admission, clinical characteristics and the risk profile of both groups were largely comparable. In particular, the empyema stage was similar. The time between admission and the first therapy was short in both groups. No statistical difference was detected in terms of average time between admission and first operative treatment. Table 2 summarizes the surgical approaches in the two different groups depending on the clinical phase. In the control group the highest numbers of operations were a posterolateral thoracotomy for pleurectomy and decortication (43.5%). A switch to a less invasive surgical approach, also in cases of stage III, is documented in the test group: 71.4% of the procedures were mini‐invasive (VATS for lavage, partial decortication and chest drainage) and only eight patients underwent a mini‐thoracotomy or thoracotomy for extended total decortication due to inadequate intraoperative re‐expansion (five patients with massive chronic fibrothorax associated with lung fibrosis and three patients with intrathoracic adhesions).
TABLE 1.
Patient characteristics
| Control group VATS pleurectomy (n = 46) | Test group VATS lavage (n = 46) | Significance | |
|---|---|---|---|
| Sex (M:F) | 42: 4 | 32: 14 | ns |
| Age | 60.5 ± 8.8 | 65.7 ± 12.2 | ns |
| Therapy at admission | |||
| Chemotherapy | 32 (69.5%) | 32 (69.5%) | ns |
| Radiotherapy | 12 (26%) | 14 (30.4%) | |
| Radio‐chemotherapy | 2 (4%) | 0 | |
| Leucopenia <3.5 G/L | 14 (30.4%) | 16 (34.7%) | ns |
| Cancer origin | |||
| Lung | 20 (43.4%) | 12 (26%) | ns |
| Breast | 12 (26%) | 16 (34.7%) | |
| Colorectal | 8 (17.4%) | 8 (17.4%) | |
| Malignant mesothelioma | 6 (13%) | 4 (8.6%) | |
| Others | 0 | 6 (13%) | |
| Comorbidities | |||
| One or more comorbidities | 28 (60.8%) | 30 (65.2%) | ns |
| Cardiovascular | 12 (26%) | 14 (30.4%) | |
| Respiratory | 12 (26%) | 6 (13%) | |
| Diabetes/metabolic | 12 (26%) | 8 (17.4%) | |
| Empyema at admission | |||
| Phase I | 12 (26%) | 10 (21.7%) | ns |
| Phase II | 6 (13%) | 4 (8.6%) | |
| Phase III | 28 (60.8%) | 32 (69.5%) | |
Note: Matched‐pairs comparisons of 46 patients with pleural empyema in oncology patients at the time of hospital admission. Clinical characteristics of patients treated with early VATS (test group) were mostly comparable with those of the historical control. In particular, there was no difference in the empyema stage.
TABLE 2.
Surgical approaches
| Control group VATS pleurectomy (n = 46) | Test group VATS lavage (n = 46) | |
|---|---|---|
| Thoracentesis, antibiotics and diuretics | 14 (30.4%) | 4 (8.6%) |
| VATS lavage and chest tube drainage | 4 (8.6%) | 34 (73.9%) |
| VATS pleurectomy and chest tube | 8 (17.4%) | ‐ |
| Mini‐thoracotomy: pleurectomy, decortication, lavage and chest tubes drainages | ‐ | 6 (13%) |
| Posterolateral thoracotomy: extended pleurectomy, decortication, chest tubes drainages | 20 (43.5%) | 2 (4.3%) |
| Empyem phase I | 12 | 10 |
| Thoracentesis, antibiotics + diuretics | 10 (85%) | 4 (40%) |
| VATS lavage and chest tube drainage | 2 (15%) | 6 (60%) |
| VATS pleurectomy and chest tube | ‐ | ‐ |
| Mini‐thoracotomy: extended pleurectomy, decortication, lavage and chest tubes drainages | ‐ | ‐ |
| Posterolateral thoracotomy: extended pleurectomy, decortication, chest tubes drainages | ‐ | ‐ |
| Empyema phase II | 6 | 8 |
| Thoracentesis, antibiotics and diuretics | 4 (75%) | ‐ |
| VATS lavage and chest tube drainage | 2 (25) | 8 (100%) |
| VATS pleurectomy and chest tube | ‐ | ‐ |
| Mini‐thoracotomy: pleurectomy, decortication, lavage and chest tubes drainages | ‐ | ‐ |
| Posterolateral thoracotomy: pleurectomy, decortication, chest tubes drainages | ‐ | ‐ |
| Empyema phase III | 28 | 28 |
| Thoracentesis, antibiotics + diuretics | ‐ | ‐ |
| VATS lavage and partial decortication and chest tube drainage | ‐ | 20 (71.4%) |
| VATS extended pleurectomy/decortication and chest tube | 8 (28.6%) | ‐ |
| Mini‐thoracotomy: extended pleurectomy, decortication, lavage and chest tubes drainages | ‐ | 6 (21.4%) |
| Posterolateral thoracotomy: extended pleurectomy, decortication, chest tubes drainages | 20 (71.4%) | 2 (7.1%) |
Note: Surgical approaches change between the first and the second era. The treatment of empyema in phase I did not change over time. In the second era a less invasive approach and operation was preferred also in the case of advanced phase.
Primary outcome
With regard to the recurrence of empyema, 10 patients in the control group required a reoperation. Two patients (both with stage III) after a VATS lavage and partial decortication developed an early empyema recurrence and required a total extended decortication/pleurectomy in mini‐thoracotomy. Figure 3 shows the overall empyema free‐survival in the two different groups (Figure 3(a)), depending on the cancer origin (Figure 3(b)). We noted that in the multivariate analysis (Cox‐regression) no factor had an independent significance for recurrence of empyema, but two factors were close, namely the therapy group and the organ of cancer origin (Figure 4).
FIGURE 3.

(a) Empyema‐free survival was longer after VATS lavage in the test group versus the historical control (log‐rank test, p = 0.081). (b) Multivariate analysis showed a higher risk of empyema recurrence for lung and breast cancer patients. Differences did not reach statistical significance, probably due to the small cohort size
FIGURE 4.
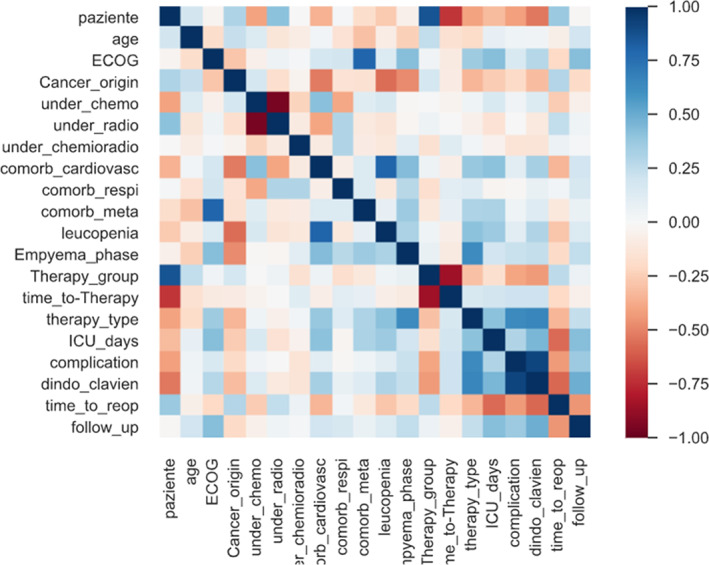
Heat map of the variables considered in the multivariate analysis. This visually highlights the correlations between all parameters considered (input at hospital admission, output at hospital discharge). Positive correlations are represented in red, and negative correlations in blue. A higher color intensity indicates a higher level of correlation
Secondary outcome
Events related to the postoperative period are listed in Table 3. Early VATS lavage saved the operating time (average operating time in the control group: 124 min; in the test group: 26 min), allowed a shorter ICU stay (5.1 days in the control group CI: 5%–95% vs. 2.6 days in the test group CI: 5%–95%, p = ns) and an earlier hospital discharge (13.5 in the control group CI: 5%–95% vs. 6.1 in the test group CI: 5%–95%, p < 0.05). Moreover, (radio‐) chemotherapy could be reinitiated earlier (40 ± 20.5 days CI: 5%–95% vs. 15 ± 12 CI: 5%–95%, p < 0.05). The total number of patients with one or more complications were 30 (65.2%) in the control group and 12 (26.1%) in the test group (CI: 5%–95%, p < 0.05). Six patients in the test group and 20 in the control group developed at least one grade III or IV complication.
TABLE 3.
Outcome data
| Control group VATS pleurectomy (n = 46) | Test group VATS lavage (n = 46) | Significance | |
|---|---|---|---|
| Reoperation within 30 days | |||
| Thoracentesis | 6 (71.4%) | ‐ | ns |
| VATS | 2 (25%)‐ | ‐ | ns |
| Mini‐thoracotomy and VATS pleurectomy | ‐ | 2 (50%) | ns |
| Thoracotomy and open pleurectomy | 4 (20%) | ‐ | ns |
| Intra‐and postoperative data | |||
| Intraoperative bleeding >500 ml | 6 (21.7%) | 2 (4.3%) | p < 0.05 |
| Operating time (min) | 124 ± 60 | 26 ± 35 | p < 0.05 |
| Average ICU stay (days) | 5.16 ± 7.3 | 2.6 ± 2.8 | p < 0.05 |
| Average hospital stay (days) | 13.5 ± 18 | 13.5 ± 6.4 | p < 0.05 |
| Time between surgery and restart (radio‐) chemotherapy (days) | 40 ± 20.5 | 15 ± 12 | p < 0.05 |
| Complications | |||
| Total (Clavien‐Dindo) | 30 (65.2%) | 12 (26.1%) | p < 0.05 |
| Grade I | 0 | 2 (4.3%) | |
| Grade II | 10 (21.7%) | 4 (8.6%) | |
| Grade III a–b | 8 (17.4%) | 4 (8.6%) | |
| Grade IV | 12 (26.1%) | 2 (4.3%) | |
| Grade V | 0 | 0 | |
| Air leak | 14 (46.6%) | 2 (16.6%) | p < 0.05 |
| Pneumonia | 12 (40%) | 4 (33.3%) | ns |
| Cardiovascular | 4 (13.3%) | 2 (16.6%) | ns |
| Others | 8 (26.6%) | 2 (16.6%) | ns |
Note: Patient outcomes after early VATS lavage (test group) versus VATS pleurectomy (control group). There were fewer recurrences of empyema in the VATS group. Complications were more frequent and severe in the historical control group. Early VATS saved operating time, allowed earlier ICU and hospital discharge. Moreover, (radio‐) chemotherapy could be reinitiated earlier.
DISCUSSION
To date, different established classification systems of parainfectious pleural effusions and empyema are available in the literature based on biochemical pleural fluid characteristics, radiological signs and microbiology. 13 , 14 , 15 , 16
Most of them focus exclusively on a parapneumonic pathogenesis, with bacterial pneumonia being the most common underlying disease, without differentiating the clinical condition of patients and ongoing therapy (such as chemotherapy or radiotherapy). These classifications focus on providing an adequate stage‐directed therapeutic management, decelerating the cascade of events leading to sepsis. 17
The first and surgically most relevant classification of “nontuberculous empyema” was drafted by the subcommittee on surgery of the American Thoracic Society (ATS) in 1962 dividing pleural empyema pathologically and clinically into three phases reflecting the normal progression. 11 Progression to empyema, which occurs in three phases, is not sharply defined but consists of a continuous deterioration if patients do not undergo an optimal medical and surgical therapy. 17 , 18 , 19
Whether patients are managed by VATS or thoracotomy is strongly dependent on the center treatment algorithm. There are no randomized studies in the literature which define the optimal timing of treatment or which surgical approach should be used. 20
Whenever drainage therapy alone does not resolve pleural empyema and achieves re‐expansion of the lung, surgical intervention is the gold standard. Moreover, patients with persistent residual sepsis associated with pleural fluid collections despite medical therapy should be considered for surgery. 1 , 2 , 5 Surgery aims at the removal of (infected) septated or loculated pleural fluid collections, debridement of fibrin depositions and decortication of the nonelastic fibrous cortex either by minimally invasive (VATS) or open surgical approaches. The surgical approaches in organized empyema (ATS stage III) are more sophisticated. The current extensive standard is debridement of the pleural cavity and decortication of the visceral and parietal pleura by conventional open surgery with thoracotomy. 9 Nevertheless, with increasing experience within the VATS field, current retrospective case series prove the feasibility of minimally invasive surgical management of late‐stage pleural empyema.
With the improvement in experience In oncological thoracic surgery, some authors have proposed a VATS approach to perform pleurectomy/decortication and have reported better results using VATS in terms of operation time, postoperative pain level, chest tube duration and hospitalization as compared with open surgery. 21 , 22 , 23 , 24 , 25 , 26 , 27
Performed in appropriate candidates, the mortality rate of VATS versus thoracotomy are 1%–3% and 3%–7%, respectively with a median hospital stay of 1–7 days for VATS and 7–10 days for open surgery. 18 , 20 , 28 , 29 Therefore many centers suggest a VATS debridement of the pleural cavity, associated with a routine pleurectomy and decortication, as the first standard surgical approach in stage III cases. 28 , 29 , 30 , 31
The worse outcome of open surgery could be explained by the impaired intraoperative pleural conditions which require thoracotomy to achieve an optimal surgical result by removing pus, adhesions and inelastic membranes20, 27, 30
In our “new concept” we perform “as limited as possible” pleurectomy using the following rationale. (1) In abdominal sepsis with severe peritonitits a peritonectomy is never performed. The peritoneum, an important barrier with potent immunological functions, recovers after control of the septic focus. Based on this observation, we used this approach also in the pleural cavity, avoiding major trauma by pleurectomy and “producing” a big wound surface with a high risk of secondary hematoma. (2) Most of the postoperative complications after a standard VATS pleurectomy occur because of diffuse bleeding on the internal chest surface. Based on this observation, avoiding the risk of bleeding by performing only a VATS lavage, postoperative complications rate should be reduced.
Therefore we perform only lavage and just remove the bacterial membrane on the surface of the pleura. Of note, a thoracoscopic approach does not allow an aggressive debridement in all intrathoracic cavity angles but it seems to be sufficient in term of lavage efficiency.
The previous literature shows that the success rate of VATS versus open surgery is approximately equal for mixed stage II and III empyema populations, as well as in isolated ATS stage III patients. 20 , 29 , 32 , 33 , 34 However, there are no published randomized studies which compare VATS lavage versus VATS pleurectomy.
The delay in surgical intervention has been shown to be the most common predictor of conversion. The conversion rate into open surgery varies from 5% to 60%. 18 The probability of thoracotomy increased from 28% where the operation was performed within 10 days after the onset of symptoms to 81% where the operation was performed with a delay of 30–40 days. 26 , 35 , 36 , 37 , 38
However, whenever thoracotomy is required, open approaches without cutting muscles and rib spread have also become less invasive over the past 20 years. Muscle sparing mini‐thoracotomy also allows surgeons to adequately perform extensive procedures such as a complete decortication. 39
The first recommended choice for a surgical approach, regardless of the empyema phase, should be VATS (VATS pleurectomy or lavage), and conversion to open surgery should only be done if an adequate pulmonary decortication and re‐expansion of the lung are not achieved. 20 , 28
In order to address this surgical trend in the literature and our new hypothesis described above (avoidance of pleurectomy), we started with our new surgical concept in oncology patients undergoing (radio‐) chemotherapy. Those patients have a high risk of sepsis because of their immunosuppressive status. Moreover, patients have a higher rate of intra‐ and postoperative complications, as compared to other nononcology patients, after standard VATS pleurectomy. 3 , 4 , 5 Therefore, we changed our surgical management using an earlier and less invasive surgical strategy.
Our new strategy has shown good results in term of secondary outcomes (postoperative complications risk, ICU stay and hospitalization). Moreover, it also improves overall empyema‐free survival, reducing the number of early recurrences. These results confirm that an early VATS lavage, without the risk of progressing empyema, is mandatory. Furthermore, we noticed that open surgery using the muscle sparing mini‐thoracotomy allows an excellent exposure. The limitation of this study is the small cohort size.
In conclusion, surgical therapy of thoracic empyema, especially in the case of immunosuppressed patients, should be performed early to avoid a rapid progression into a septic condition. Early VATS lavage seems to safeguard oncology patients with a progressed empyema (ATS phase II and III) from more complex surgical procedures, shortening the hospital stay, reducing the risk of postoperative complications and permitting an earlier restart of oncology therapy.
CONFLICT OF INTEREST
All authors have completed the ICMJE uniform disclosure form. The authors have no conflicts of interest to declare.
Girotti PNC, Tschann P, Di Stefano P, Möschel M, Hübl N, Königsrainer I. Retrospective case–control study on the outcomes of early minimally invasive pleural lavage for pleural empyema in oncology patients. Thorac Cancer. 2021;12:2710–2718. 10.1111/1759-7714.14109
REFERENCES
- 1. Ferguson AD, Prescott RJ, Selkon JB, Watson D, Swinburn CR. The clinical course and management of thoracic empyema. QJM. 1996;89:285–9. [DOI] [PubMed] [Google Scholar]
- 2. Davies CWH, Kearney SE, Gleeson FV, Davies RJ. Predictors of outcome and long‐term survival in patients with pleural infection. Am J Respir Crit Care Med. 1999;160:1682–7. [DOI] [PubMed] [Google Scholar]
- 3. Ashbaugh DG. Empyema thoracis: factors influencing morbidity and mortality. Chest. 1991;99:1162–5. [DOI] [PubMed] [Google Scholar]
- 4. Foster S, Maskell N. Bacteriology of complicated parapneumonic effusions. Curr Opin Pulm Med. 2007;13:319–23. [DOI] [PubMed] [Google Scholar]
- 5. Heffner JE. Management of the patient with a malignant pleural effusion. Semin Respir Crit Care Med. 2010;31:723–33. [DOI] [PubMed] [Google Scholar]
- 6. Mandal AK, Thadepalli H, Mandal AK, Chettipally U. Outcome of primary empyema thoracis: therapeutic and microbiologic aspects. Ann Thorac Surg. 1998;66:1782–6. [DOI] [PubMed] [Google Scholar]
- 7. Smith JA, Mullerworth MH, Westlake GW, Tatoulis J. Empyema thoracis: 14‐year experience in a teaching center. Ann Thorac Surg. 1991;51:39–42. [DOI] [PubMed] [Google Scholar]
- 8. Tsai TH, Jerng JS, Chen KY, Yu CJ, Yang PC. Community‐acquired thoracic empyema in older people. J Am Geriatr Soc. 2005;53:1203–9. [DOI] [PubMed] [Google Scholar]
- 9. Farjah F, Symons RG, Krishnadasan B, Wood DE, Flum DR. Management of pleural space infections: a population‐based analysis. J Thorac Cardiovasc Surg. 2007;133:346–51. [DOI] [PubMed] [Google Scholar]
- 10. Finley C, Clifton J, FitzGerald JM, Yee J. Empyema: an increasing concern in Canada. Can Respir J. 2008;15:85–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Andrews NC, Parker EF, Shaw RR, Wilson NJ, Webb WR. Management of non tuberculous empyema: a statement of the subcommittee on surgery. Am Rev Respir Dis. 1962;3:62–6. [Google Scholar]
- 12. Kraus GJ. The split pleura sign. Radiology. 2007;243:297–8. [DOI] [PubMed] [Google Scholar]
- 13. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien‐Dindo classification of surgical complications: five‐year experience. Ann Surg. 2009;250:187–96. [DOI] [PubMed] [Google Scholar]
- 14. Colice GL, Curtis A, Deslauriers J, Heffner J, Light R, Littenberg B, et al. Medical and surgical treatment of parapneumonic effusions: an evidence‐based guideline. Chest. 2000;118:1158–71. [DOI] [PubMed] [Google Scholar]
- 15. Light RW. A new classification of parapneumonic effusions and empyema. Chest. 1995;108(2):299–301. [DOI] [PubMed] [Google Scholar]
- 16. Muers MF. Streptokinase for empyema. Lancet. 1997;349:1491–2. [DOI] [PubMed] [Google Scholar]
- 17. Reichert M, Hecker M, Witte B, Bodner J, Padberg W, Weigand MA, et al. Stage‐directed therapy of pleural empyema. Langenbecks Arch Surg. 2017;402:15–26. [DOI] [PubMed] [Google Scholar]
- 18. Pothula V, Krellenstein DJ. Early aggressive surgical management of parapneumonic empyemas. Chest. 1994;105:832–6. [DOI] [PubMed] [Google Scholar]
- 19. Hamm H. The treatment of parapneumonic effusions and pleural empyemas. Pneumologie. 2005;59:696–703. [DOI] [PubMed] [Google Scholar]
- 20. Mark DR, Tze YC, van Driel M. Surgical versus non‐surgical management for pleural empyema. Cochrane Database Syst Rev. 2017;3:CD010651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Swanson SJ, Herndon JE 2nd, D'Amico TA, Demmy TL, McKenna RJ Jr, Green MR, et al. Video‐assisted thoracic surgery lobectomy: report of CALGB 39802–a prospective, multiinstitution feasibility study. J Clin Oncol. 2007;25:4993–7. [DOI] [PubMed] [Google Scholar]
- 22. Whitson BA, Andrade RS, Boettcher A, Bardales R, Kratzke RA, Dahlberg PS, et al. Video‐assisted thoracoscopic surgery is more favorable than thoracotomy for resection of clinical stage I non‐small cell lung cancer. Ann Thorac Surg. 2007;83:1965–70. [DOI] [PubMed] [Google Scholar]
- 23. Whitson BA, Groth SS, Duval SJ, Swanson SJ, Maddaus MA. Surgery for early‐stage non‐small cell lung cancer: a systematic review of the video‐assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann Thorac Surg. 2008;86:2008–16. [DOI] [PubMed] [Google Scholar]
- 24. Yan TD, Black D, Bannon PG, McCaughan BC. Systematic review and meta‐analysis of randomized and nonrandomized trials on safety and efficacy of video‐assisted thoracic surgery lobectomy for early‐stage non‐small‐cell lung cancer. J Clin Oncol. 2009;27:2553–62. [DOI] [PubMed] [Google Scholar]
- 25. Demmy TL, Nwogu C. Is video‐assisted thoracic surgery lobectomy better? Quality of life considerations. Ann Thorac Surg. 2008;85:S719–28. [DOI] [PubMed] [Google Scholar]
- 26. Chung JH, Lee SH, Kim KT, Jung JS, Son HS, Sun K. Optimal timing of thoracoscopic drainage and decortication for empyema. Ann Thorac Surg. 2014;97:224–9. [DOI] [PubMed] [Google Scholar]
- 27. Chan DT, Sihoe AD, Chan S, Tsang DS, Fang B, Lee TW, et al. Surgical treatment for empyema thoracis: is videoassisted thoracic surgery better than thoracotomy? Ann Thorac Surg. 2007;84:225–31. [DOI] [PubMed] [Google Scholar]
- 28. Davies CW, Gleeson FV, Davies RJ. BTS guidelines for the management of pleural infection. Thorax. 2003;58(Suppl 2):18–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Scarci M, Abah U, Solli P, Page A, Waller D, van Schil P, et al. EACTS expert consensus statement for surgical management of pleural empyema. Eur J Cardiothorac Surg. 2015;48:642–53. [DOI] [PubMed] [Google Scholar]
- 30. Silen ML, Naunheim KS. Thoracoscopic approach to the management of empyema thoracis: indications and results. Chest Surg Clin N Am. 1996;6:491–9. [PubMed] [Google Scholar]
- 31. Solaini L, Prusciano F, Bagioni P. Video‐assisted thoracic surgery in the treatment of pleural empyema. Surg Endosc. 2007;21:280–4. [DOI] [PubMed] [Google Scholar]
- 32. Alfageme I, Munoz F, Pena N, Umbria S. Empyema of the thorax in adults. Etiology, microbiologic findings, and management. Chest. 1993;103:839–43. [DOI] [PubMed] [Google Scholar]
- 33. Thurer RJ. Decortication in thoracic empyema: indications and surgical technique. Chest Surg Clin N Am. 1996;6:461–90. [PubMed] [Google Scholar]
- 34. Lim TK, Chin NK. Empirical treatment with fibrinolysis and early surgery reduces the duration of hospitalization in pleural sepsis. Eur Respir J. 1999;13:514–8. [DOI] [PubMed] [Google Scholar]
- 35. Lardinois D, Gock M, Pezzetta E, Buchli C, Rousson V, Furrer M, et al. Delayed referral and Gram‐negative organisms increase the conversion thoracotomy rate in patients undergoing video‐assisted thoracoscopic surgery for empyema. Ann Thorac Surg. 2005;79:1851–6. [DOI] [PubMed] [Google Scholar]
- 36. Wozniak CJ, Paull DE, Moezzi JE, Scott RP, Anstadt MP, York VV, et al. Choice of first intervention is related to outcomes in the management of empyema. Ann Thorac Surg. 2009;87:1525–30. [DOI] [PubMed] [Google Scholar]
- 37. Stefani A, Aramini B, della Casa G, Ligabue G, Kaleci S, Casali C, et al. Preoperative predictors of successful surgical treatment in the management of parapneumonic empyema. Ann Thorac Surg. 2013;96:1812–9. [DOI] [PubMed] [Google Scholar]
- 38. Divisi D, Gabriele F, Barone M, Zaccagna G, Di Francescantonio W, Crisci R. Clinical history and surgical management of parapneumonic empyema what is the role of video‐assisted thoracoscopic surgery (VATS)? Videoassist Thorac Surg. 2017;2:65. [Google Scholar]
- 39. Andreetti C, Menna C, Ibrahim M, Ciccone AM, D'Andrilli A, Venuta F, et al. Postoperative pain control: videothoracoscopic versus conservative mini thoracotomic approach. Eur J Cardiothor. 2014;46:907–12. [DOI] [PubMed] [Google Scholar]