

Abstract
Objective
To assess the prevalence of patient administrative tasks and whether they are associated with delayed and/or foregone care.
Data Source
March 2019 Health Reform Monitoring Survey.
Study Design
We assess the prevalence of five common patient administrative tasks—scheduling, obtaining information, prior authorizations, resolving billing issues, and resolving premium problems—and associated administrative burden, defined as delayed and/or foregone care. Using multivariate logistic models, we examined the association of demographic characteristics with odds of doing tasks and experiencing burdens. Our outcome variables were five common types of administrative tasks as well as composite measures of any task, any delayed care, any foregone care, and any burden (combined delayed/foregone), respectively.
Data Collection
We developed and administered survey questions to a nationally representative sample of insured, nonelderly adults (n = 4155).
Principal Findings
The survey completion rate was 62%. Seventy‐three percent of respondents reported performing at least one administrative task in the past year. About one in three task‐doers, or 24.4% of respondents overall, reported delayed or foregone care due to an administrative task: Adjusted for demographics, disability status had the strongest association with administrative tasks (adjusted odds ratio [OR] 2.91, p < 0.001) and burden (adjusted OR 1.66, p < 0.001). Being a woman was associated with doing administrative tasks (adjusted OR 2.19, p < 0.001). Being a college graduate was associated with performing an administrative task (adjusted OR 2.79, p < 0.001), while higher income was associated with fewer subsequent burdens (adjusted OR 0.55, p < 0.01).
Conclusions
Patients frequently do administrative tasks that can create burdens resulting in delayed/foregone care. The prevalence of delayed/foregone care due to administrative tasks is comparable to similar estimates of cost‐related barriers to care. Demographic disparities in burden warrant further attention. Enhancing measurement of patient administrative work and associated burdens may identify opportunities for assessing quality, value, and patient experience.
Keywords: access/demand/utilization of services, health care costs, patient assessment/satisfaction, survey research and questionnaire design
What is known on this topic
High administrative complexity is a central feature of the US health care system, with underappreciated implications for patients.
Research examining the administrative costs of health care has primarily focused on clinicians and provider organizations.
Compared to financial barriers to access, evidence examining nonfinancial costs has been limited and not focused specifically on patients' administrative burden.
What this study adds
Using new evidence from a nationally representative survey of nonelderly adults, we find patients frequently do administrative work that can create burdens resulting delays in care and not getting needed care due to difficulties with administrative tasks.
We find the prevalence of delayed or foregone care due to administrative tasks is comparable to similar estimates of cost‐related barriers to care.
Enhancing measurement of patient administrative work and associated burdens may identify opportunities for improving quality, value, and patient experience with the US health system.
1. INTRODUCTION
Health spending in the United States is highest in the world, driven in part by administrative functions. 1 These include billing, documentation, scheduling, compliance, and other nonclinical activities required to coordinate within and across organizations. Estimates of total administrative costs range from 8% to 34% of total health care spending in the United States, substantially greater than other wealthy countries. 2 , 3 Most analyses of health care administration focus on its costs in the provision of care, and there is a paucity of research examining the administrative work borne by patients. 4 , 5 , 6 , 7 No health system in the world is without administrative functions and costs, but the degree of complexity of the US health and insurance systems may impose substantial indirect costs that are rarely systematically measured. These indirect, nonfinancial costs include the time, effort, and stress of navigating the health system to pay for or obtain care.
To illuminate the size and consequences of patients' administrative roles, we used data from a nationally representative survey to assess the annual prevalence of five common types of administrative tasks patients perform: appointment scheduling, obtaining information from an insurer or provider, obtaining prior authorizations, resolving insurance or provider billing issues, and resolving premium problems. We examined the association of these tasks with two important measures of their burden: delayed and forgone care. In addition to prevalence, we examined predictors of experiencing administrative tasks and associated burdens.
Many literatures examine the roles and experiences of patients in the health care system, aspects of which touch on patient administrative work, but none focused exclusively on it. Patient engagement is a ubiquitous term that captures a broad set of activities and attitudes, but the central aim is for patients to participate in their clinical care, for example, through a process of shared decision making. 8 Treatment burden is a newer framework that measures multiple dimensions of chronically ill patients' experience with health care, including clinical, psychological, and administrative burdens. 9 , 10 Patient satisfaction is a widely used quality measure (e.g., Consumer Assessment of Providers and Health Systems [CAHPS]) and is typically oriented to customer service. 11 CAHPS captures some aspects of administrative burden, such as ease of getting an appointment. While the CAHPS instruments for health plans inquire about administrative tasks such as information seeking, billing issues, and ease of filling out paperwork, they do not directly associate these measures of patient administrative functions with access to care. 12
Evidence from public benefits enrollment illustrates that administrative complexity can substantially affect access to care. Prospective Medicare Advantage enrollees are less likely to choose a plan as the number of plan options increases. 13 Medicare beneficiaries with lower cognitive function are less likely to enroll in the plan with the best available benefits. 13 , 14 The introduction of Medicaid work requirements reduced Medicaid coverage in Arkansas, due in part to the program's reporting requirements. 15 But analysis of public benefits enrollment does not capture patient administrative complexity that may be involved in using the health care system once enrolled nor does it capture complexity associated with commercial health insurance.
A rich literature examines financial costs and access to care, but data examining nonfinancial costs have been more limited and not focused specifically on administrative burden. 16 Several surveys, including the National Health Interview Survey (NHIS) and Gallup poll, track the share of patients reporting delayed or missed care due to cost. 17 , 18 Using a similar framework, we assess the prevalence and predictors of patient administrative burden in a nationally representative survey. To our knowledge, ours is the first study to both measure the role patients play in key health care administrative tasks and relate them to the degree to which they affect access to care.
2. CONCEPTUAL MODEL
Timely access is considered foundational to health outcomes. 19 , 20 Factors causing patients to delay or forego needed care are barriers to access potentially threatening health. 19 , 21 Healthy People 2020 identifies barriers related to costs, inadequate or no insurance, unavailable services, and lack of culturally competent care; it does not highlight administrative barriers. 19 Nonfinancial costs, including administration, are recognized access barriers but are understudied relative to financial costs. 16 , 22 The scale of administrative complexity in the health care system overall suggests this aspect of patient experience merits specific attention, especially regarding access.
Administration is not synonymous with burden; it is a neutral, often useful, aspect of management and coordination. While administrative tasks can be necessary, they are not costless. Public policy scholars examining citizens' interactions with the government define administrative burden as the learning, compliance, and psychological costs associated with navigating administrative complexity. 23 Administrative burden can delay or prevent access to services, whether unintentionally or by design. We examine the extent to which patients' administrative burden poses access barriers, measured by delayed or foregone care.
Drawing from evidence on patient experience, access to care, and administrative costs more broadly, we focus on five common types of administrative task.
Appointment scheduling. This is a common patient task, given that most adults have a medical office visit in a given year, and these often require scheduling. 24 The ability to get an appointment when needed is a commonly used access metric appearing in surveys such as the CAHPS and NHIS. 25 , 26
Information seeking. Patient‐facing information is often inaccurate. 27 , 28 Making data accessibility and exchange less burdensome for patients and clinicians has been an ongoing policy priority and is among specific recommendations to reduce systemic administrative costs. 28 , 29 , 30
Prior authorization. Their use is increasing and may pose barriers to access for patients. 31 Simplifying prior authorizations has been recognized as a policy priority by medical and insurance groups. 32 , 33
Billing issues. Evidence shows billing is complex and generates significant administrative work for clinicians and health care organizations; as bill recipients, this complexity likely affects patients, too. 4 , 6 , 34
Insurance premium problems. For individuals not in a group plan with automatic deductions, managing premium payments may be potentially challenging. 35 , 36 , 37
Administrative tasks may be a potential source of inequity because some groups may face larger burdens, and some groups may have fewer resources with which to navigate administrative complexity. 14 , 16 People with complex needs may have more frequent and/or complicated encounters, with more tasks creating more opportunities for burden. 38 Insurance design could affect administrative work required of beneficiaries. 39 Women do a disproportionate share of unpaid caregiving, which may include performing health‐related administrative tasks. 40 People who face racial or other discrimination may experience disparate burdens. 41 , 42
3. METHODS
3.1. Survey sample
We use data from the Health Reform Monitoring Survey (HRMS). Conducted twice annually by the Urban Institute, the HRMS is a nationally representative, probability‐based Internet sample drawn from the Ipsos KnowledgePanel. 43 The KnowledgePanel is a bilingual (English/Spanish) national survey research panel consisting of about 55,000 US adults. 44 The HRMS draws a stratified, random cross‐sectional sample of adults 18–64 years old from the KnowledgePanel and is weighted to be nationally representative. 43 In March 2019, the survey completion rate for the HRMS was 64% (n = 9596). 43 Prior research benchmarking HRMS results against the American Community Survey found the HRMS yielded comparable estimates. 45 (See Appendix A1 for detailed methods.)
The administrative burden question module was administered to a random half of the March 2019 HRMS respondents who reported having health insurance for all of the past 12 months (n = 8305) for a final sample of 4155.
3.2. Survey questions
We defined administrative tasks as nonclinical aspects of care; this definition excludes direct care, such as attending a clinical appointment or self‐administering a treatment. Consistent with this, the survey included questions in five general categories of administrative work: (1) appointment scheduling (one question); (2) information seeking (three questions—one on seeking information about an insurance network, one on seeking other information from a health plan, and one on seeking information from a provider; (3) obtaining prior authorization for care (one question); (4) dealing with insurance premium problems (one question); and (5) addressing insurance‐related or provider‐related billing issues (one question on each). (See Appendix A2 for survey questions.) We asked all respondents eight binary questions about which administrative tasks they had undertaken in the last year, if any. For each task undertaken by a respondent, we asked two follow‐up questions: (1) whether they had delayed needed care because of the task and (2) whether they had foregone needed care because of the task. We modeled questions about burden on the NHIS questions, which ask respondents whether they have delayed or foregone needed care in the past 12 months. 17
3.3. Composite measures
We created binary composite measures for the two task categories with multiple questions: information seeking (three questions) and billing problems (two questions). We also created binary composite measures to aggregate responses across all task categories into summary measures: any task done, any delayed care because of a task, any foregone care because of a task, and combined burden (delayed and/or foregone care because of a task).
3.4. Analysis
We calculated weighted descriptive statistics for each summary measure and for the five task categories (Figures 1 and 2, Table 1, Appendix Exhibits A1–A8). We stratified each measure by the following demographic variables: sex (male/female), age (18–64 years); race/ethnicity (non‐Hispanic white, non‐Hispanic black, other race, and Hispanic ethnicity); educational attainment (high school graduate or less, some college, and college graduate), family income (≤138% of federal poverty level [FPL], 139%–249% FPL, 250%–399% FPL, and ≥400% FPL), insurance type (employer‐sponsored insurance [ESI], public insurance, and direct purchase/marketplace/other coverage), marital status (married/not married), and disability status (disabled/nondisabled). We used two‐sided t‐tests to compare demographic differences between “yes” and “no” respondents for each summary measure and task category. The survey logic asked questions about delayed or foregone care conditional on having undertaken the task. In addition to reporting the conditional responses, we calculated percentages based on the total sample denominator to determine population prevalence of administrative tasks and burden for insured adults 18–64 years.
FIGURE 1.
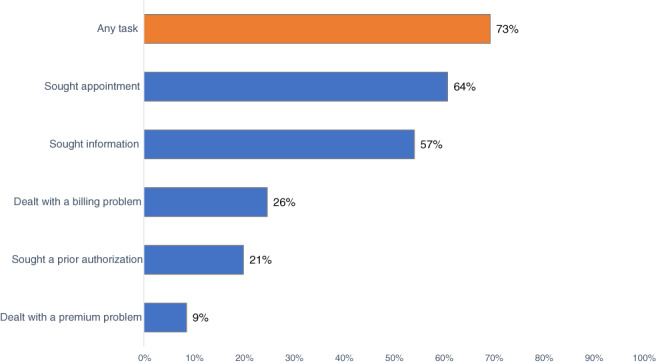
Percent of nonelderly adults who reported doing any of five types health care administrative tasks in the past 12 months. Authors' analysis of Q1 2019 Health Reform Monitoring Survey. Percentages are survey‐weighted, unadjusted descriptive statistics. Denominator for all categories is the total sample (n = 4155) [Color figure can be viewed at wileyonlinelibrary.com]
FIGURE 2.
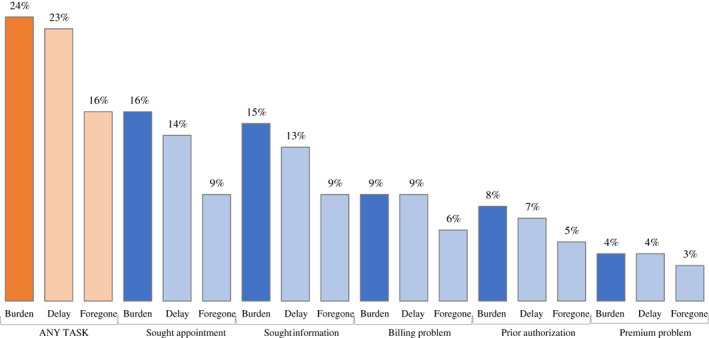
Percent of total respondents who reported any burden, any delayed care, or any foregone care, by administrative task type. Authors' analysis of Q1 2019 Health Reform Monitoring Survey. Percentages are survey‐weighted, unadjusted descriptive statistics. Denominator for all categories is the total sample (n = 4155) [Color figure can be viewed at wileyonlinelibrary.com]
TABLE 1.
Descriptive statistics: demographic characteristics of populations that did administrative tasks, experienced burden
| Any administrative task a | Any burden b | Any delayed care c | Any foregone care d | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Difference | Yes | No | Difference | Yes | No | Difference | Yes | No | Difference | |
| Female (%) | 55 | 39.9 | 15.1**** | 60.7 | 52.2 | 8.4*** | 61 | 52.4 | 8.6*** | 56.4 | 54.7 | 1.7 |
| Age (%) | ||||||||||||
| 18–34 years | 31.4 | 46.4 | −15.0**** | 35.1 | 29.5 | 5.6* | 36.1 | 29.3 | 6.8** | 33.8 | 30.7 | 3.1 |
| 35–49 years | 30.3 | 28.9 | 1.4 | 30 | 30.5 | −0.5 | 29.6 | 30.6 | −1.0 | 30.2 | 30.2 | 0 |
| 50–64 years | 38.3 | 24.7 | 13.6**** | 34.9 | 40 | −5.1** | 34.3 | 40.1 | −5.8** | 35.9 | 39 | −3.0 |
| Race/ethnicity (%) | ||||||||||||
| White non‐Hispanic | 66 | 58.1 | 8** | 58.8 | 69.7 | −10.9**** | 58 | 69.6 | −11.6**** | 59.2 | 67.9 | −8.7*** |
| Black non‐Hispanic | 11.8 | 13 | −1.2 | 13.9 | 10.7 | 3.2* | 14.4 | 10.6 | 3.8** | 13.3 | 11.4 | 1.9 |
| Other race/multiple race non‐Hispanic | 8.9 | 9.4 | −0.5 | 10.3 | 8.2 | 2.1* | 10.5 | 8.2 | 2.3* | 9.5 | 8.7 | 0.8 |
| Hispanic | 13.3 | 19.5 | −6.2** | 17 | 11.4 | 5.5** | 17.2 | 11.6 | 5.6** | 18 | 12 | 6.0** |
| Married (%) | 58.5 | 41.1 | 17.4**** | 51.8 | 61.9 | −10.1**** | 50.7 | 62 | −11.3**** | 52.8 | 60.1 | −7.3*** |
| Disability (%) | 11.3 | 5.4 | 5.9**** | 16.4 | 8.7 | 7.7**** | 16.1 | 9.2 | 6.9**** | 19.2 | 9.2 | 10**** |
| Educational attainment (%) | ||||||||||||
| High school or less | 28.1 | 45.7 | −17.6**** | 31.2 | 26.6 | 4.6* | 31.1 | 26.8 | 4.4* | 34 | 26.5 | 7.5** |
| Some college | 30.3 | 29.7 | 0.6 | 34.3 | 28.2 | 6.1** | 34.9 | 28.2 | 6.7*** | 34 | 29.2 | 4.7* |
| College graduate or more | 41.6 | 24.6 | 17.0**** | 34.5 | 45.2 | −10.7**** | 34 | 45.1 | −11.1**** | 32.1 | 44.3 | −12.2**** |
| Family income relative to poverty (%) | ||||||||||||
| At or below 138% | 18.1 | 28.1 | −10.1**** | 26.4 | 13.9 | 12.5**** | 26.3 | 14.4 | 11.9**** | 28.9 | 15.1 | 13.8**** |
| 139%–399% | 32.4 | 38.2 | −5.8** | 35.3 | 30.9 | 4.4* | 35.7 | 30.9 | 4.8** | 36 | 31.5 | 4.5* |
| At or above 400% | 49.5 | 33.6 | 15.9**** | 38.3 | 55.1 | −16.9**** | 38 | 54.7 | −16.7**** | 35.1 | 53.4 | −18.3**** |
| Health insurance coverage type (%) | ||||||||||||
| Public | 15 | 20.6 | −5.7** | 22.1 | 11.4 | 10.7**** | 21.7 | 11.9 | 9.8**** | 24.5 | 12.4 | 12.2**** |
| Direct purchase, marketplace, other | 10.1 | 15.6 | −5.5** | 10.9 | 9.7 | 1.3 | 11.2 | 9.6 | 1.6 | 9.9 | 10.1 | −0.2 |
| Employer‐sponsored coverage | 74.7 | 62.5 | 12.2**** | 66.6 | 78.8 | −12.3**** | 66.8 | 78.3 | −11.5**** | 64.9 | 77.4 | −12.5**** |
| Sample size (unweighted) | 3273 | 882 | 1015 | 2258 | 921 | 2352 | 661 | 2612 | ||||
Note: Authors' analysis of Q1 2019 Health Reform Monitoring Survey. */**/***/**** Significantly different from zero at the 0.10/0.05/0.01/0.001 level, using two‐tailed tests. Numbers may not sum due to rounding. Percentages are survey‐weighted, unadjusted descriptive statistics.
Comparison of those who reported doing any administrative task and those who did not report doing any tasks.
Comparison of those who did any task and reported delayed and/or foregone care and those who did any task and did not report delayed and/or foregone care.
Comparison of those who did any task and reported delayed care and those who did any task and did not experience did not report any delayed care.
Comparison of those who did any task and reported foregone care and those who did any task and did not experience did not report any foregone care.
We used multivariate logistic regression models to estimate adjusted odds of doing a task, and conditional on doing a task, odds of any burden (combined delayed and foregone care), delayed care, or foregone care. Our primary outcome variables were composite measures of any task, any burden, any delay, and any foregone care. Demographic covariates for all models were sex, age category, race/ethnicity, marital status, disability status, education, income, and insurance type, all as defined above. We estimated odds ratios (ORs) and additionally report predicted probabilities for ease of interpretation.
4. RESULTS
4.1. Respondents
Our sample was 51% female (Appendix Exhibit A1). We grouped respondents by age, namely, 18–34 (35.4%), 35–44 (29.9%), and 45–64 (34.7%) years. Respondents were 63.9% non‐Hispanic white, 12.1% non‐Hispanic black, and 9% another race and 14.9% reported Hispanic/Latino ethnicity. Disability status was 9.7%. Twenty percent of respondents reported family income at or below 138% of FPL, 33.9% from 139% to 399% FPL, and 45.3% at 400% FPL or above. Seventy‐two percent had ESI, 16.5% public insurance, and 11.5% direct purchase/marketplace/other coverage.
4.2. Administrative tasks are common
Administrative tasks are common, with nearly three quarters (73.2%) of insured, nonelderly adults reporting at least one of the five types of administrative task in the past 12 months (Figure 1). Of those adults, most (55.2%) reported undertaking multiple types of tasks, with 5.2% doing all five types of tasks over the year.
The most common task types were contacting a provider to make an appointment (64%) and information seeking, which includes seeking network information, other information from insurers or providers, and gathering information to share between providers (57%). These common tasks are often associated with initiating care. Less common were tasks related to health using care or maintaining health insurance coverage, such as billing problems with either an insurer or provider (26%), prior authorizations (21%), and premium problems (9%).
4.3. Administrative tasks often result in delayed or foregone health care
Among the people who undertook an administrative task, one in three (33.4%) reported either delaying for forgoing needed health care because of an administrative task (Appendix Exhibit A8). Delayed care (30.9%) was more common than foregone care (21.5%), but people often experienced both. The overall population prevalence of administrative burden in our sample, including respondents who did not report doing a task, was 24.4% (22.6% reported delayed care and 15.7% reported foregone care) (Figure 2).
There was an inverse relationship between task prevalence and percent of people doing the task who experienced a burden. About one in four people reported delayed and/or missed care related to common tasks such as seeking appointments (24.7%) or seeking information (25.7%). In contrast, delayed and/or missed care was reported by more than a third of people who dealt with a billing problem (36.4%) or prior authorization (37.6%) and nearly half (45.6%) of people who dealt with a premium problem. While people dealing with premium problems were far more likely to report delayed and/or missed care than people seeking appointments, the prevalence of each of these tasks meant that in absolute terms, more people experienced delayed and/or missed care related to appointment seeking (15.7% of the total sample) than to premium problems (3.9% of the total sample).
4.4. Prevalence of administrative tasks and burdens varies by demographic factors
Those who reported any administrative tasks in the past 12 months were significantly more likely to be female than those who did not report a task (55% vs. 29.9%, p < 0.001), more likely to be aged 50–64 years (38.8% vs. 24.7%, p < 0.001), more likely to be white (66% vs. 58.1%, p < 0.05), more likely to be married (58.5% vs. 41.1%, p < 0.001), more likely to have a disability (11.3% vs. 5.4%, p < 0.001), more likely to be a college graduate (41.6% vs. 24.6%, p < 0.001), more likely to have a family income above 400% FPL (49.5% vs. 33.6%, p < 0.001), and more likely to have ESI than those who did not report a task (74.7% vs. 62.5%, p < 0.001) (Table 1).
Among the subsample of people who did a task, those who reported any burden (delayed and/or missed care) differed from those who completed tasks without either consequence. People reporting a burden remained more likely to be female than people who completed a task without a burden (60.7% vs. 52.2%, p < 0.01) and more likely to have a disability (16.4% vs. 8.7%, p < 0.001). People who reported any burden were less likely to be white than people who did a task without a burden (58.8% vs. 67.9%, p < 0.001), less likely to be married (51.8% vs. 61.9%, p < 0.001), and less likely to be college graduates (34.5% vs. 45.2%, p < 0.001). Those reporting a burden were more likely to have a family income below 138% FPL (26.4% vs. 13.9%, p < 0.001) and to have public insurance than people who completed tasks without a burden (22.1% vs. 11.4%, p < 0.001).
4.5. Characteristics associated with administrative tasks and burdens
After adjusting for demographic covariates, disability status was the variable most strongly associated with doing tasks and experiencing burdens (Table 2). Women had significantly greater adjusted odds of doing any task and experiencing burdens, but burden was driven by delayed care and not foregone care. Having an income above 400% FPL did not significantly increase odds of doing a task but did make people significantly less likely to experience any type of burden. Younger people were significantly less likely to do tasks, but age was not significantly associated with burden. ESI did not significantly affect the odds of doing a task or experiencing delays, but it did significantly decrease odds of foregone care due to an administrative burden.
TABLE 2.
Results of logistic regression models: odds ratios and predicted probabilities of demographic characteristics associated with administrative tasks and burden
| Marginal estimates adjusted prevalence | Any task a | Any burden, conditional b | Any delay, conditional c | Any foregone, conditional d | ||||
|---|---|---|---|---|---|---|---|---|
| Odds ratio | Predicted probability | Odds ratio | Predicted probability | Odds ratio | Predicted probability | Odds ratio | Predicted probability | |
| Sex (%) | ||||||||
| Female | 2.19**** | 80.3% | 1.32** | 35.9% | 1.35**** | 33.6% | 0.97 | 21% |
| Male | ref | 66.6 | ref | 30 | ref | 27.5 | ref | 21.4 |
| Age (%) | ||||||||
| 18–34 years | 0.55**** | 69.6 | 1.17 | 34.6 | 1.25 | 33.1 | 1.05 | 21.3 |
| 35–49 years | 0.63**** | 72.1 | 1.14 | 34.1 | 1.15 | 31.4 | 1.10 | 22 |
| 50–64 years | ref | 79.7 | ref | 31.3 | ref | 28.6 | ref | 20.5 |
| Race/ethnicity (%) | ||||||||
| White non‐Hispanic | ref | 75.2 | ref | 30.6 | ref | 28 | ref | 19.7 |
| Black non‐Hispanic | 0.79 | 71 | 1.23 | 35 | 1.33* | 33.7 | 1.09 | 21 |
| Other race/multiple race non‐Hispanic | 0.8 | 71.3 | 1.60*** | 40.8 | 1.65**** | 38.5 | 1.39* | 25.7 |
| Hispanic | 0.8 | 71.4 | 1.51* | 39.5 | 1.56* | 37.2 | 1.42 | 25.2 |
| Married (%) | ||||||||
| Yes | 1.51*** | 77.2 | 0.85 | 31.8 | 0.82 | 29.1 | 0.95 | 20.8 |
| No | ref | 70 | ref | 35.2 | ref | 33.1 | ref | 21.7 |
| Disability (%) | ||||||||
| Yes | 2.91**** | 87.3 | 1.66**** | 43.2 | 1.60*** | 39.7 | 1.82**** | 20.7 |
| No | ref | 72.1 | ref | 31.9 | ref | 29.7 | ref | 19.8 |
| Educational attainment (%) | ||||||||
| High school or less | ref | 63.5 | ref | 31 | ref | 29.2 | ref | 20.8 |
| Some college | 1.78**** | 74.7 | 1.30* | 3.6 | 1.29 | 34.4 | 1.13 | 22.8 |
| College graduate or more | 2.79**** | 81.8 | 1.07 | 32.4 | 1.01 | 29.5 | 0.96 | 20.2 |
| Family income relative to poverty (%) | ||||||||
| At or below 138% | ref | 71.3 | ref | 41.4 | ref | 37.7 | ref | 28.5 |
| 139%–399% | 1.14 | 73.6 | 0.79 | 35.9 | 0.82 | 33.4 | 0.77 | 24.5 |
| At or above 400% | 1.25 | 75.2 | 0.55*** | 28.2 | 0.58*** | 26.3 | 0.49**** | 16.5 |
| Health insurance coverage type (%) | ||||||||
| Public | ref | 73.7 | ref | 37.4 | ref | 33.5 | ref | 24.4 |
| Direct purchase, marketplace, other | 0.73 | 67.9 | 0.87 | 34.3 | 0.94 | 32.3 | 0.77 | 20 |
| Employer‐sponsored coverage | 1.06 | 74.7 | 0.79 | 32.2 | 0.85 | 30 | 0.80**** | 20.6 |
Note: Authors' analysis of Q1 2019 Health Reform Monitoring Survey. */**/***/**** Significantly different from zero at the 0.10/0.05/0.01/0.001 level, using two‐tailed tests. Numbers may not sum due to rounding.
Regression‐adjusted estimates comparing those who reported doing any administrative task and those who did not report doing any tasks.
Regression adjusted estimates comparing those who did any task and reported delayed and/or foregone care and those who did any task and did not report delayed and/or foregone care.
Regression adjusted estimates comparing those who did any task and reported delayed care and those who did any task and did not experience did not report any delayed care.
Regression adjusted estimates comparing those who did any task and reported foregone care and those who did any task and did not experience did not report any foregone care.
5. DISCUSSION
Administrative complexity in the US health care system has implications for insured nonelderly adults. In a national survey of this population, nearly three quarters of respondents reported doing at least one of five types of health care–related administrative tasks in the past 12 months. Administrative tasks often impose barriers to care: 24.4% of respondents in our sample reported delayed or foregone care due to administrative tasks. Placing our findings in perspective, our estimate of administrative burden prevalence is roughly commensurate with a comparable estimates of financial barriers from a 2019 Kaiser Family Foundation survey, which found that 26% of insured adults of age 18–64 years said that they or a family member had postponed or put off needed care in the past 12 months due to cost. 46 Our estimate of administrative burden was larger than similar NHIS questions related to financial cost: in the 2018 NHIS, 17% of continuously insured adults of age 18–64 years said they or someone in their household delayed care or did not get needed care due to cost. 26
One in three people who undertook a task experienced delayed and/or missed care, ranging from 24.7% of people who sought an appointment to 45.6% of people who had a problem with their premium payment. The most common tasks, appointment seeking and information seeking, were the least onerous, but many more people were exposed to these tasks, so they posed the largest burden in terms of number of people affected. Fewer people experienced insurance or provider billing issues, prior authorizations, and premium problems, but these tasks were relatively more burdensome for those who faced them, compared to other tasks. We are likely undercounting the prevalence and burden of coverage‐related tasks, like dealing with premium problems, because our sample excluded people with coverage interruptions in the past 12 months.
Disability status is the demographic characteristic most strongly associated with administrative burden; people with disabilities are more likely to engage in every type of administrative task and to report every type of burden. This is layered on top of the additional work people with disabilities do related to self‐care and navigating other social services. 47 Our findings likely reflect the fact that people with disabilities use more care—so are more likely to encounter tasks and subsequent administrative burdens. They may also reflect the fact that some disabilities are cognitive and navigating the US health system is especially challenging for persons with cognitive impairments. 14 Similarly, women tend to use more care than men, which may underly relatively higher prevalence of tasks and delayed care among women. 48 Additionally, women disproportionately provide caregiving, which may include administrative tasks. 40
The characteristics of people who reported doing administrative tasks were quite different than the characteristics of people who experienced a burden. White people, older adults, college graduates, and people in high‐income families were all more likely to do a task. But among those doing tasks, nonwhite people, younger people, people with less than a college degree, and people in low‐income families were more likely to report experiencing a burden. In our adjusted estimates, more education was significantly associated with doing a task and higher income was associated with lower odds of experiencing all burdens. Identifying as a race other than black or white and identifying as Hispanic was associated with burden. People with fewer advantages may be less proactive in interacting with the health care system and are less able to avoid or resolve administrative barriers when they do. 49 , 50 , 51 These results may reflect that some people have less experience or knowledge of how to engage the health care system, and/or they may reflect that some people encounter racial or ethnic discrimination that heightens barriers. 42 This raises equity concerns meriting further attention.
Finally, we note that insurance type is not strongly associated with administrative burden. Although descriptive analyses showed people with public insurance (mostly Medicaid given our nonelderly sample) reported more burdens, insurance type was not statistically significant in multivariate analyses, with one exception: ESI is associated with lower odds of experiencing foregone care but is not associated with lower odds of delayed care or delayed/foregone care in combination.
Administration in general is not categorically bad. Indeed, administrative costs and complexity may arise from efforts to increase take‐up, improve quality and efficiency, and to avoid rationing by price (e.g., prior authorization instead of a higher copay) There is strong evidence that cost‐sharing is a blunt instrument for distributing resources and causes attrition from both necessary and unnecessary care. 52 Social policy uses “targeting and ordeals” as a nonprice mechanism to optimize the distribution of finite public resources, targeting populations through the reduction (i.e., auto‐enrollment) or introduction (paperwork) of administrative ordeals. 53 , 54 There is evidence to show that these approaches can direct resources cost‐effectively. 33 , 55 , 56
But using administrative mechanisms to mitigate financial inequities may have unintended consequences: time and knowledge are also unequally distributed resources with consequences for access. 57 Consumerism is a popular approach to insurance and delivery system reform that envisions patients taking the role of discerning customers to drive market efficiencies. 58 But uneven take‐up of financially attractive benefits hints at the presence of potentially inefficient nonprice costs. 59 Consumer‐driven programs have underappreciated implications for patient administrative burden, as patients have to navigate more complex incentives. For example, one high‐deductible health plan made diabetes care free but saw poor uptake of this financially advantageous benefit in low‐income ZIP codes. 60
Our results suggest administrative mechanisms may have equity implications on par with price‐based rationing. We find administrative burden falls disproportionately on people with high medical needs (disability), which raises distributional concerns. And, we find existing racial and socioeconomic inequities are associated with administrative burden. Administrative complexity is endemic to all postindustrial health systems, but there may be opportunity to design administrative tools with greater care to avoid exacerbating or reinforcing inequities.
5.1. Limitations
Survey data are self‐reported and subject to recall bias. However, what constitutes an administrative burden is itself a personal judgment. As such, the sense that one has been burdened by the system is a valid feeling no matter when it occurs. Additionally, estimates of cost‐based delayed or forgone care in the literature, which are widely reported as indicative of underinsurance, are also derived from survey responses. The contribution of our work is to compare administrative‐based access limitations to these cost‐based ones.
Our questions were restricted to adults of age 18–64 years old who were continuously insured over the prior 12 months; the extent of generalizability to older, younger, and uninsured populations is unclear. However, according to the 2018 NHIS, 81.9% of the 18‐ to 64‐year‐old population was continuously insured for 12 months, making these findings widely applicable.
While response rates are a poor proxy for nonresponse bias, response rates for consumer surveys are declining, raising concerns about nonresponse bias. 61 , 62 Bias may be avoidable even with lower response rates if the sample is representative of the study population. 63 Evidence suggests that low response rate surveys with probability sampling and weighting based on established population parameters can produce results similar to high response rate surveys and objective measures. 64 , 65
We do not expect views about administrative burden systematically attracted or dissuaded respondents from completing the survey as this topic was a subset of a larger instrument. Nevertheless, unobservable bias could arise. Our respondents show a propensity to complete surveys and may differ systematically from the general public. Arguably, follow‐through on completing surveys indicates greater administrative capability and may bias our results toward the null, but potential unobserved differences between our sample and the general population are a key limitation of this study.
Our survey items were new questions developed for this study. The tasks we included were necessarily limited by space constraints in the survey, and we acknowledge that ours is not an exhaustive list of administrative tasks. (In particular, it omits work patients may do coordinating between entities, time spent on administrative work, the frequency with which people did each task type/number of delays/foregone care.) We did not know ex ante what the prevalence of tasks or delayed/foregone care would be or which were most important. Modeled on similar questions about cost in the NHIS, our questions asked about delayed or foregone needed care, but we did not assess the nature of need (routine, urgent, or emergent). Our questions were based on a review of consumer survey instruments and ad hoc discussions about administrative tasks with patients. As there is little prior work on any patient administrative tasks, our findings represent a substantial contribution and a foundation for future work, these limitations notwithstanding.
Recent work examining health care “hassles” among Veterans Affairs populations finds hassles are common: ranked by frequency, our studies found the same top two challenges (scheduling and information). 66 Another study using the same hassles framework among women veterans found 29.3% of respondents reported delayed or foregone care. 67 While these studies are not directly comparable to ours, it is reassuring to see broadly consistent patterns.
5.2. Future directions
Patients bear administrative costs in health care, and a priority for researchers and practitioners is to develop a more nuanced understanding of what administrative work patients do and why, as well as its implications for care and outcomes. Clarifying which burdens are intentional (prior authorization) or unintentional (provider billing errors) is one step. Among intentional administrative tasks, examining unintended consequences is key, particularly trade‐offs between degree of complexity and access to care. Out‐of‐pocket spending is rightly a central priority in health policy and reform, but ameliorating the administrative burden of care is a comparatively untapped dimension of Americans' health care experience. Unintentional burdens deserve attention because they impose unintended consequences disproportionately felt by those with greater health care needs and lower knowledge and skills.
Measuring patient administrative work with greater richness and precision is foundational to informing practice and policy. Aggregate measures of health system administration are incomplete without taking into account the share of this work done by patients and their families. Many estimates of delivery‐side administration are based on time costs. The American Time Use Survey is a source of valuable data enabling patients' time costs of care associated with travel to and participation in clinical encounters and/or self‐care, but while it captures household administration generally, it does not specifically capture health administration. 57 , 68 The NHIS, CAHPS, Medicare Current Beneficiary Survey, Health and Retirement Survey, and the National Health and Aging Trends Study currently include some questions related to patient administrative work and are poised to capture richer measures.
While it is a reasonable inference that nonfinancial access barriers pose threats similar to cost‐based barriers, we have not explicitly shown that connection. It remains a worthy topic for future study. Examining administrative burden among children (or their caregivers) and older adults (particularly contrasting Medicare Advantage with traditional Medicare) would be valuable ways to extend this work. Examining the administrative burden of caregiving and dependent relationships more generally merits attention. We did not elicit detail about administrative pathways and how or why barriers arose; this warrants study as multiple barriers can co‐occur. We did not ask about the nature of care that was delayed or foregone (routine, urgent, or emergent), which is an important direction for future inquiry. Future work could explore other tasks and burdens, like psychological burden, life and work disruption, etc. Finally, our dataset did not include measures of health care utilization, which has a causal relationship with task exposure and chance of burdens. This was a descriptive study characterizing prevalence of and demographic characteristics associated with administrative burden in the general population, which we hope will spur causal studies.
6. CONCLUSION
High administrative complexity is a central feature of the US health care system. Largely overlooked, patients frequently report doing administrative tasks and report delayed or foregone care because of difficulties with administrative tasks. Prevalence of administrative burden is comparable to similar estimates of financial barriers to care. Enhancing measurement of patient administrative burdens may identify opportunities for improving quality, value, equity, and patient experience.
DISCLAIMERS
This work does not represent the views of the US Department of Veterans Affairs, the US Government, or any other organization with which the authors are affiliated.
Supporting information
Appendix S1 Supporting information
ACKNOWLEDGMENTS
The Health Reform Monitoring Survey (HRMS) is conducted by the Urban Institute, with funding from the Robert Wood Johnson Foundation. We thank the Urban Institute for allowing us to add questions on administrative burden to the HRMS. We thank Michael Karpman and Sharon Long at the Urban Institute for their help in framing the analysis and developing the survey questions. Michael Anne Kyle was supported by a Harvard Business School Doctoral Fellowship when this work was completed.
Kyle MA, Frakt AB. Patient administrative burden in the US health care system. Health Serv Res. 2021;56(5):755-765. 10.1111/1475-6773.13861
See related Commentary by Herd et al.
Funding information Robert Wood Johnson Foundation
REFERENCES
- 1. Cutler DM, Ly DP. The (paper)work of medicine: understanding international medical costs. J Econ Perspect. 2011;25(2):3‐25. 10.1257/jep.25.2.3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high‐income countries. JAMA. 2018;319(10):1024‐1039. 10.1001/jama.2018.1150 [DOI] [PubMed] [Google Scholar]
- 3. Himmelstein DU, Campbell T, Woolhandler S. Health care administrative costs in the United States and Canada, 2017. Ann Intern Med. 2020;172(2):134–142. 10.7326/M19-2818 [DOI] [PubMed] [Google Scholar]
- 4. Tseng P, Kaplan RS, Richman BD, Shah MA, Schulman KA. Administrative costs associated with physician billing and insurance‐related activities at an academic health care system. JAMA. 2018;319(7):691‐697. 10.1001/jama.2017.19148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Himmelstein DU, Jun M, Busse R, et al. A comparison of hospital administrative costs in eight nations: US costs exceed all others by far. Health Aff. 2014;33(9):1586‐1594. 10.1377/hlthaff.2013.1327 [DOI] [PubMed] [Google Scholar]
- 6. Casalino LP, Nicholson S, Gans DN, et al. What does it cost physician practices to interact with health insurance plans? Health Aff. 2009;28(4):w533‐w543. 10.1377/hlthaff.28.4.w533 [DOI] [PubMed] [Google Scholar]
- 7. Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753‐760. 10.7326/M16-0961 [DOI] [PubMed] [Google Scholar]
- 8. Patient‐centered care: what it means and how to get there|health affairs. Accessed January 8, 2020. https://www.healthaffairs.org/do/10.1377/hblog20120124.016506/full/
- 9. May CR, Eton DT, Boehmer K, et al. Rethinking the patient: using burden of treatment theory to understand the changing dynamics of illness. BMC Health Serv Res. 2014;14(1):281. 10.1186/1472-6963-14-281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Tran V‐T, Barnes C, Montori VM, Falissard B, Ravaud P. Taxonomy of the burden of treatment: a multi‐country web‐based qualitative study of patients with chronic conditions. BMC Med. 2015;13(1):115. 10.1186/s12916-015-0356-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Anhang Price R, Elliott MN, Zaslavsky AM, et al. Examining the role of patient experience surveys in measuring health care quality. Med Care Res Rev. 2014;71(5):522‐554. 10.1177/1077558714541480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. The medicare advantage and prescription drug plan disenrollment reasons survey|CMS. Accessed January 8, 2020. https://www.cms.gov/Research-Statistics-Data-and-Systems/Research/CAHPS/MAPDP_DisenrollmentSurvey [DOI] [PMC free article] [PubMed]
- 13. McWilliams JM, Afendulis CC, McGuire TG, Landon BE. Complex Medicare advantage choices May overwhelm seniors—especially those with impaired decision making. Health Aff. 2011;30(9):1786‐1794. 10.1377/hlthaff.2011.0132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kuye IO, Frank RG, McWilliams JM. Cognition and take‐up of subsidized drug benefits by Medicare beneficiaries. JAMA Intern Med. 2013;173(12):1100‐1107. 10.1001/jamainternmed.2013.845 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Sommers BD, Goldman AL, Blendon RJ, Orav EJ, Epstein AM. Medicaid work requirements—results from the first year in Arkansas. N Engl J Med. 2019;381(11):1073‐1082. 10.1056/NEJMsr1901772 [DOI] [PubMed] [Google Scholar]
- 16. Kullgren JT, McLaughlin CG, Mitra N, Armstrong K. Nonfinancial barriers and access to Care for U.S. adults. Health Serv Res. 2012;47(1 pt 2):462‐485. 10.1111/j.1475-6773.2011.01308.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. QuickStats . Percentage* of adults aged 18–64 years who delayed or did not receive medical care during the past 12 months because of Cost,† by year—National Health Interview Survey,§ United States, 2005–2014. MMWR Morb Mortal Wkly Rep. 2016;65(9):251. 10.15585/mmwr.mm6509a6 [DOI] [Google Scholar]
- 18. More Americans delaying medical treatment due to cost. Accessed January 6, 2020. https://news.gallup.com/poll/269138/americans-delaying-medical-treatment-due-cost.aspx
- 19. Access to health services|healthy people 2020. Accessed December 4, 2020. https://www.healthypeople.gov/2020/topics-objectives/topic/Access-to-Health-Services
- 20. Institute of Medicine (US) Committee on Monitoring Access to Personal Health Care Services . In: Millman Michael, ed. Access to Health Care in America. Washington, DC: National Academies Press; 1993. Accessed December 6, 2020. http://www.ncbi.nlm.nih.gov/books/NBK235882/ [PubMed] [Google Scholar]
- 21. Rahimi AR, Spertus JA, Reid KJ, Bernheim SM, Krumholz HM. Financial barriers to health care and outcomes after acute myocardial infarction. JAMA. 2007;297(10):1063‐1072. 10.1001/jama.297.10.1063 [DOI] [PubMed] [Google Scholar]
- 22. Herd P, Moynihan D. How administrative burdens can harm health. Health Affairs Health Policy Brief; 2020. https://www.healthaffairs.org/do/10.1377/hpb20200904.405159/full/ [Google Scholar]
- 23. Moynihan D, Herd P, Harvey H. Administrative burden: learning, psychological, and compliance costs in citizen‐state interactions. J Public Admin Res Theory. 2015;25(1):43‐69. 10.1093/jopart/muu009 [DOI] [Google Scholar]
- 24. National Center for Health Statistics, CDC . NHIS Early Release—2018. Early release of selected estimates based on data from the 2018 National Health Interview Survey; 2019. Accessed June 18, 2019. https://www.cdc.gov/nchs/nhis/releases/released201905.htm
- 25. CAHPS Clinician & Group Survey. Accessed December 4, 2020. http://www.ahrq.gov/cahps/surveys-guidance/cg/index.html
- 26. Blewett LA, Rivera Drew JA, King M, Williams K. IPUMS Health Surveys: National Health Interview Survey, Version 6.4 [Dataset]. Minneapolis, MN: IPUMS; 2019. 10.18128/D070.V6.4 [DOI] [Google Scholar]
- 27. Haeder SF, Weimer DL, Mukamel DB. Secret shoppers find access to providers and network accuracy lacking for those in marketplace and commercial plans. Health Aff. 2016;35(7):1160‐1166. 10.1377/hlthaff.2015.1554 [DOI] [PubMed] [Google Scholar]
- 28. Lye CT, Forman HP, Gao R, et al. Assessment of US Hospital compliance with regulations for patients' requests for medical records. JAMA Netw Open. 2018;1(6):e183014. 10.1001/jamanetworkopen.2018.3014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Improving the Health Records Request Process for Patients: Insights from User Experience Research. Washington DC: The Office of the National Coordinator for Health Information Technology; 2017. Accessed December 10, 2020. https://www.healthit.gov/sites/default/files/onc_records-request-research-report_2017-06-01.pdf [Google Scholar]
- 30. Cutler DM. Reducing administrative costs in U.S. health care. Washington, DC: The Hamilton Project; 2020. https://www.hamiltonproject.org/assets/files/Cutler_PP_LO.pdf
- 31. Navar AM, Taylor B, Mulder H, et al. Association of prior authorization and out‐of‐pocket costs with patient access to PCSK9 inhibitor therapy. JAMA Cardiol. 2017;2(11):1217‐1225. 10.1001/jamacardio.2017.3451 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Consensus statement on improving the prior authorization process; 2018. https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/arc-public/prior-authorization-consensus-statement.pdf
- 33. Psotka MA, Singletary EA, Bleser WK, et al. Streamlining and reimagining prior authorization under value‐based contracts: a call to action from the value in healthcare initiative's prior authorization learning collaborative. Circ Cardiovasc Qual Outcomes. 2020;13(7):e006564. 10.1161/CIRCOUTCOMES.120.006564 [DOI] [PubMed] [Google Scholar]
- 34. Gottlieb JD, Shapiro AH, Dunn A. The complexity of billing and paying for physician care. Health Aff. 2018;37(4):619‐626. 10.1377/hlthaff.2017.1325 [DOI] [PubMed] [Google Scholar]
- 35. Dague L. The effect of Medicaid premiums on enrollment: a regression discontinuity approach. J Health Econ. 2014;37:1‐12. 10.1016/j.jhealeco.2014.05.001 [DOI] [PubMed] [Google Scholar]
- 36. Gordon SH, Sommers BD, Wilson IB, Galarraga O, Trivedi AN. Risk factors for early disenrollment from Colorado's affordable care act marketplace. Med Care. 2019;57(1):49‐53. 10.1097/MLR.0000000000001020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Drake C, Cai S‐T, Anderson D, Sacks DW. Zero‐Price Effects in Health Insurance: Evidence from Colorado. SSRN Electronic Journal. 10.2139/ssrn.3743009 [DOI] [Google Scholar]
- 38. Yabroff KR, Davis WW, Lamont EB, et al. Patient time costs associated with cancer care. J Natl Cancer Inst. 2007;99(1):14‐23. 10.1093/jnci/djk001 [DOI] [PubMed] [Google Scholar]
- 39. Handel BR, Kolstad JT. Health insurance for “humans”: information frictions, plan choice, and consumer welfare. Am Econ Rev. 2015;105(8):2449‐2500. 10.1257/aer.20131126 [DOI] [PubMed] [Google Scholar]
- 40. Moreira da Silva J. Why you should care about unpaid care work. OECD Development Matters; 2019. Accessed December 4, 2020. https://oecd-development-matters.org/2019/03/18/why-you-should-care-about-unpaid-care-work/
- 41. Wisneiwski J, Walker B. Association of simulated patient race/ethnicity with scheduling of primary care appointments. JAMA Network Open. 2020;3(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Ray V, Herd P, Moynihan DP. Racialized burdens: applying racialized organization theory to the administrative state; 2020.
- 43.Frequently asked questions. Health Reform Monitoring Survey. Accessed February 22, 2020. http://hrms.urban.org/faq.html
- 44. Ipsos KnowledgePanel. Accessed February 13, 2020. https://www.ipsos.com/en-us/solutions/public-affairs/knowledgepanel
- 45. Long SK, Kenney GM, Zuckerman S, et al. The health reform monitoring survey: addressing data gaps to provide timely insights into the affordable care act. Health Aff. 2014;33(1):161‐167. 10.1377/hlthaff.2013.0934 [DOI] [PubMed] [Google Scholar]
- 46. Data Note: Americans' Challenges with Health Care Costs – Appendices – 9316. The Henry J. Kaiser Family Foundation; Accessed February 27, 2020. https://www.kff.org/report-section/data-note-americans-challenges-with-health-care-costs-appendices/ [Google Scholar]
- 47. Deshpande M, Li Y. Who is screened out? Application costs and the targeting of disability programs. AEJ: Economic Policy. 2019;11(4):213–248. 10.3386/w23472 [DOI] [Google Scholar]
- 48. MEPS summary tables. Accessed February 27, 2020. https://meps.ahrq.gov/mepstrends/hc_use/
- 49. Tipirneni R, Politi MC, Kullgren JT, Kieffer EC, Goold SD, Scherer AM. Association between health insurance literacy and avoidance of health care services owing to Cost. JAMA Netw Open. 2018;1(7):e184796. 10.1001/jamanetworkopen.2018.4796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Barnes AJ, Hanoch Y, Rice T. Determinants of coverage decisions in health insurance marketplaces: consumers' decision‐making abilities and the amount of information in their choice environment. Health Serv Res. 2015;50(1):58‐80. 10.1111/1475-6773.12181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Loewenstein G, Friedman JY, McGill B, et al. Consumers' misunderstanding of health insurance. J Health Econ. 2013;32(5):850‐862. 10.1016/j.jhealeco.2013.04.004 [DOI] [PubMed] [Google Scholar]
- 52. Brot‐Goldberg ZC, Chandra A, Handel BR, Kolstad JT. What does a deductible do? The impact of cost‐sharing on health care prices, quantities, and spending dynamics. Q J Econ. 2017;132(3):1261‐1318. 10.1093/qje/qjx013.Advance [DOI] [Google Scholar]
- 53. Nichols AL, Zeckhauser RJ. Targeting transfers through restrictions on recipients. Am Econ Rev. 1982;72(2):372‐377. [Google Scholar]
- 54. Dupas P, Hoffmann V, Kremer M, Zwane AP. Targeting health subsidies through a non‐price mechanism: a randomized controlled trial in Kenya. Science. 2016;353(6302):889‐895. 10.1126/science.aaf6288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Newhouse JP, McGuire TG. How successful is Medicare advantage? Milbank Q. 2014;92(2):351‐394. 10.1111/1468-0009.12061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Maciejewski ML, Wansink D, Lindquist JH, Parker JC, Farley JF. Value‐based insurance design program in North Carolina increased medication adherence but was not cost neutral. Health Aff. 2014;33(2):300‐308. 10.1377/hlthaff.2013.0260 [DOI] [PubMed] [Google Scholar]
- 57. Ray KN, Chari AV, Engberg J, Bertolet M, Mehrotra A. Disparities in time spent seeking medical Care in the United States. JAMA Intern Med. 2015;175(12):1983‐1986. 10.1001/jamainternmed.2015.4468 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Agarwal R, Gupta A, Fendrick AM. Value‐based insurance design improves medication adherence without an increase in total health care spending. Health Aff. 2018;37(7):1057‐1064. 10.1377/hlthaff.2017.1633 [DOI] [PubMed] [Google Scholar]
- 59. Desai S, Hatfield LA, Hicks AL, et al. Offering a price transparency tool did not reduce overall spending among California public employees and retirees. Health Aff. 2017;36(8):1401‐1407. 10.1377/hlthaff.2016.1636 [DOI] [PubMed] [Google Scholar]
- 60. Reed ME, Warton EM, Kim E, Solomon MD, Karter AJ. Value‐based insurance design benefit offsets reductions in medication adherence associated with switch to deductible plan. Health Aff. 2017;36(3):516‐523. 10.1377/hlthaff.2016.1316 [DOI] [PubMed] [Google Scholar]
- 61. Davern M. Nonresponse rates are a problematic indicator of nonresponse bias in survey research. Health Serv Res. 2013;48(3):905‐912. 10.1111/1475-6773.12070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Keeter S, Hatley N, Kennedy C, Lau A. What low response rates mean for telephone surveys. Washington, DC: Pew Research Center Methods; 2017. Accessed February 7, 2019. http://www.pewresearch.org/methods/2017/05/15/what-low-response-rates-mean-for-telephone-surveys/
- 63. Groves RM, Peytcheva E. The impact of nonresponse rates on nonresponse BiasA meta‐analysis. Public Opin Q. 2008;72(2):167‐189. 10.1093/poq/nfn011 [DOI] [Google Scholar]
- 64. Keeter S, Kennedy C, Dimock M, Best J, Craighill P. Gauging the impact of growing nonresponse on estimates from a national RDD telephone survey. Public Opin Q. 2006;70(5):759‐779. 10.1093/poq/nfl035 [DOI] [Google Scholar]
- 65. QuickTake: HRMS benchmarks well against gallup‐healthways and NHIS on changes in health insurance coverage between 2013 and 2015. Accessed July 17, 2019. http://hrms.urban.org/quicktakes/HRMS-Benchmarks-Well-against-Gallup-Healthways-and-NHIS-on-Changes-in-Health-Insurance-Coverage-between-2013-and-2015.html
- 66. Noël PH, Barnard JM, Barry FM, et al. Patient experience of health care system hassles: dual‐system vs single‐system users. Health Serv Res. 2020. 55(4):548‐555. 10.1111/1475-6773.13291 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Brunner J, Rose D, Chuang E, Canelo IA, Yano EM. The role of healthcare system hassles in delaying or forgoing care. Healthcare. 2020;8(2):100411. 10.1016/j.hjdsi.2020.100411 [DOI] [PubMed] [Google Scholar]
- 68. Jonas DE, Ibuka Y, Russell LB. How much time do adults spend on health‐related self‐care? Results from the American time use survey. J Am Board Fam Med. 2011;24(4):380‐390. 10.3122/jabfm.2011.04.100260 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1 Supporting information