

Abstract
Purpose
The “Act on Hospice and Palliative Care and Decisions on Life-Sustaining Treatment for Patients at the End-of-Life” was enacted on February 3, 2016 and went into effect on February 4, 2018 in Korea. This study reviewed the first year of determination to life-sustaining treatment (LST) through data analysis of the National Agency for Management of Life-Sustaining Treatment.
Materials and Methods
The National Agency for Management of LST provided data between February 4, 2018 and January 31, 2019 anonymously from 33,549 patients. According to the forms patients were defined as either elf-determinants or family-determinants.
Results
The median age of the patient was 73 and the majority was male (59.9%). Cancer patients were 59% and self-determinants were 32.1%. Cancer patients had a higher rate of self-determinants than non-cancer (47.3% vs. 10.1%). Plan for hospice service was high in cancer patients among self-determinants (81.0% vs. 37.5%, p < 0.001). In comparison to family-determinants, self-determinants were younger (median age, 67 years vs. 75 years; p < 0.001) and had more cancer diagnosis (87.1% vs. 45.9%, p < 0.001). Decision of withholding or withdrawing of LSTs in cancer patients was higher than non-cancer patients in four items.
Conclusion
Cancer patients had a higher rate in self-determination and withholding or withdrawing of LSTs than non-cancer patients. Continued revision of the law and education of the public will be able to promote withdrawing or withholding the futile LSTs in patients at end-of-life. Further study following the revision of the law should be evaluated to change of end-of-life care.
Keywords: Terminal care, Hospices, Advance directives, Withholding treatment
Introduction
With the advancement of medical treatment and technology, life-sustaining treatment (LST) such as cardiopulmonary resuscitation, mechanical ventilation, hemodialysis, and anticancer drugs have also developed. However, these LSTs are often applied to patients with chronic diseases who have no possibility of a fundamental recovery, resulting in situations that merely extend the duration of the end-of-life process. Starting with the United States. ‘Natural Death Act’ in 1976, other countries around the world have established guidelines through the social agreement on the advance directives (ADs) and the cessation of meaningless LST [1,2]. However, in South Korea, even if the patient’s condition deteriorated and the possibility of recovery was low despite active treatment, there was little shared decision-making for LST between the physician and the patient [3]. The end-of-life decision including do-not-resuscitate (DNR) is usually made between the physician and family-caregivers without patients in practice [4–7]. There is still controversy about withholding or withdrawing LST in South Korea. Since the so-called Boramae hospital case in 1997, there have been fierce pros and cons regarding the LST at the end-of-life [8]. The LST decisions law has been triggered by an event commonly referred to as the ‘Grandmother Kim case’ [9]. Based upon the decisions, the public had come to recognize the right to die with dignity and the right to self-determination of life. In clinical practice, informed consents and shared decision-making have become more important to patients. Finally, the “Act on Hospice and Palliative Care and Decisions on Life-Sustaining Treatment for Patients at the End-of-Life” was enacted on February 3, 2016 and went into effect on February 4, 2018 in South Korea [10].
Two years post enactment we conducted this study to investigate the first-year status of determination to LST through data analysis of National Agency for Management of Life-Sustaining Treatment. This study is the part of the result of a research project (task number: NA19-008) conducted by the National Evidence-based Healthcare Collaborating Agency, funded by the government (Ministry of Health and Welfare) in 2019.
Materials and Methods
1. Data sources
The database of the National Agency for Management of Life-Sustaining Treatment is a national registration system of legal forms, which are included in the enforcement decree of the act on decisions on LST for patients at the end-of-life. Data was obtained from February 4, 2018 to January 31, 2019 after de-identification. The legal forms in the system consists of LST plan (appendix form No. 1), determination of whether the patient is at the end-of-life process (appendix form No. 9), confirmation of the patient’s intention by advanced directive (appendix form No. 10), confirmation by consistent statements of two or more of the patient’s family members (appendix form No. 11), confirmation by unanimous consensus of the patient’s family (appendix form No. 12), and the paper of implementation of LST (appendix form No. 13) [10]. Data used for analysis in each form are shown in S1 Table.
2. Term definition
The definitions of the following terms in this study were taken from the first edition of the law [10]. LSTs were limited to cardiopulmonary resuscitation (CPR), mechanical ventilation, hemodialysis, and the administration of anticancer drugs. Withholding LST was defined as not beginning LST for the patient at the end-of-life. Withdrawing LST were defined as discontinuing LST for the patient at the end-of-life, who has been receiving the LSTs.
The terminal patient was defined as a patient who has been diagnosed as expected to die within a few months with no possibility of a fundamental recovery, and where symptoms gradually worsened despite proactive treatment. The diagnosis of terminal illness was confined to four types of disease: cancer, acquired immune deficiency syndrome (AIDS), chronic obstructive pulmonary disease (COPD), and chronic liver cirrhosis (LC) by the ordinance of the Ministry of Health and Welfare. The patient in dying periods was defined as a patient in a state of imminent death, in which there is no possibility of revitalization or recovery despite treatment and where symptoms worsen rapidly.
The scope of a patient’s family was defined as either spouse of the patient, lineal descendants, or lineal ascendants that are 19 years or above. If no family member falls under the above, siblings will take over.
3. Process of decision of LST according to the law
The decision process of withdrawal or withholding LST can begin after a patient or family member requests to the attending physician about LST processing. Form 1 (LST plan) is filled out only after a patient is either diagnosed with a terminal illness or is in the dying process by the attending physician and a specialist in the field (herein after referred to as “the two physicians”). When the two physicians agree that a patient is on the verge of death, they fill out form 9. The patient can express their will about the type of LST and the use of hospice service on form 1. In case of dying process, the decision of LST is recorded on form 1, 10, 11, or 12.
4. Classification of patients
A patient’s diagnosis was collected from form 9 and categorized as either cancer or non-cancer. Cancer diagnosis was classified according to the causes of death statistics in Korea [11]. Non-cancer diagnosis was categorized into three non-cancer terminal diseases (AIDS, COPD, and LC) which can diagnose the terminal illnesses by the law. The other top 10 causes of death statistics in Korea 2018 except suicide: heart diseases, pneumonia, cerebrovascular diseases, diabetes mellitus, liver diseases, chronic lower respiratory diseases, Alzheimer’s disease, hypertensive diseases, sepsis and respiratory tuberculosis [11].
Patients were also categorized by form completed either as self-determinants or family-determinants. Patients who filled out form 1 were grouped as self-determinants and forms 11 or 12 were named family-determinants.
5. Statistical analysis
This is a descriptive study to evaluate demographics and clinical characteristics of patients, plan for hospice service, method of LST decision-making, and four items of LST decisions (CPR, mechanical ventilation, hemodialysis, and anticancer drugs). To draw a comparison between the two groups, t test for mean differences, chi-squared test or Fisher’s exact test for frequencies was used. A two-sided p-value less than 0.05 was considered statistically significant. All analyses were conducted using SAS ver. 9.4 (SAS Institute Inc., Cary, NC).
Results
1. Study population
Between February 4, 2018 to January 31, 2019, 44,381 cases were registered in the system. 10,774 for form 1, 33,549 for form 9, 10,740 for form 11, 12,035 for form 12 and a total of 33,549 were registered with form 13 (S2 Table). Among them 33,549 patients who had the forms for LST decision (1, 11, or 12), form 9, and form 13 were included in the analysis (Fig. 1).
Fig. 1.
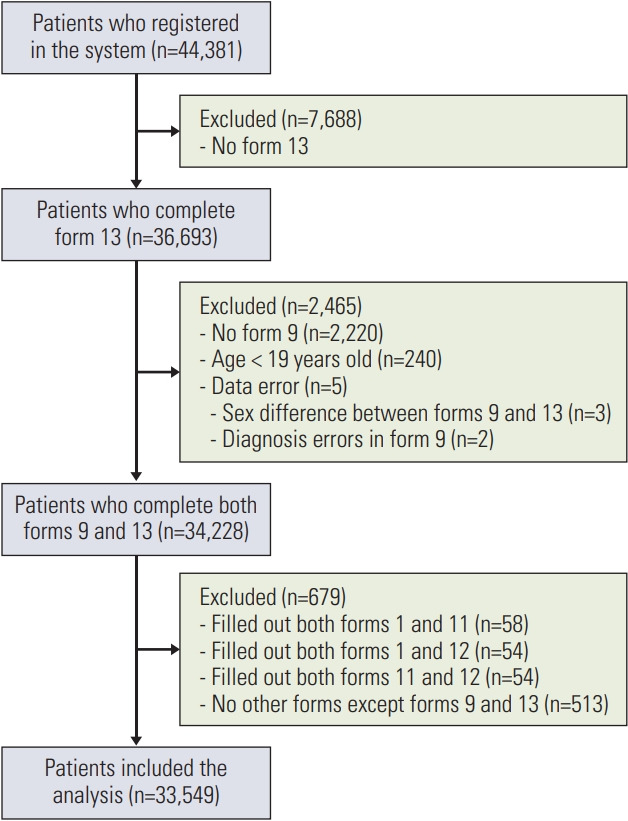
Patient cohort.
Patients’ characteristics are shown in Table 1. The median age was 73 years (interquartile range [IQR], 62 to 81). Cancer patients were 59.0% and self-determinants were 32.1%. Among self-determinants, patients at terminal illness were 66.2%, and marked LST items, which were more than 99%, were CPR and mechanical ventilation. Among family-determinants in form 11 were 10,740 (47.2%) and form 12 were 12,035 (52.8%). The ratio of LST decision papers according to the age was detailed in Table 2. The median number of family members with form 11 were 3 (IQR, 2 to 4; range, 1 to 47) and most common family members were lineal descendants (n=6,650, 61.92%) followed by the spouse and lineal descendants (n=3,376, 31.43%) (S3 Table). The median number of family members in form 12 were 3 (IQR, 2 to 4; range, 1 to 21). Most of the LST decision papers were written in the advanced general hospitals and general hospitals (96.3%). The patients who filled out residence on form 1 and location of hospitals in which LST decision papers were concentrated in Seoul and capital areas (Fig. 2). The patients with terminal illness who filled out form 1 were 66.2% (7,135) while 33.8% (3,639) were in dying process. Plan for hospice service among self-determinants were 8,117 (75.3%). The mean period between form 13 and one of the LST decision forms (form 1, form 11, form 12) were 8.6 days (±23.6 days), 1 day (±8.9 days), and 1.4 days (±9.2 days), respectively.
Table 1.
Characteristics of patients
| Characteristic | No. (%) (n=33,549) |
|---|---|
| Age (yr) | |
| Median (IQR) | 73 (62–81) |
| Sex | |
| Male | 20,112 (59.9) |
| Female | 13,437 (40.1) |
| Diagnosis | |
| Cancer | 19,827 (59.0) |
| Non-cancer | 13,772 (41.0) |
| Subject of decision | |
| Self-determinants | 10,774 (32.1) |
| Family-determinants | 22,775 (67.9) |
| Disease status a) | |
| Terminal illness | 7,135 (66.2) |
| Dying periods | 3,639 (33.8) |
| Marked LST items in the form 1 a) | |
| CPR | 10,750 (99.8) |
| Mechanical ventilation | 10,696 (99.3) |
| Hemodialysis | 10,104 (93.8) |
| Anticancer drugs | 8,502 (78.9) |
| Plan for hospice service a) | |
| Yes | 8,117 (75.3) |
| No | 2,060 (19.1) |
| Unmarked | 597 (5.5) |
| Patient residence a) | |
| Seoul | 2,776 (25.8) |
| Gyeonggi-do | 2,408 (22.4) |
| Incheon | 881 (8.2) |
| Gyeongsangnam-do | 657 (6.1) |
| Busan | 622 (5.8) |
| Daegu | 526 (4.9) |
| Jeollanam-do | 460 (4.3) |
| Ulsan | 459 (4.3) |
| Gyeongsangbuk-do | 366 (3.4) |
| Chungcheongnam-do | 302 (2.8) |
| Chungcheongbuk-do | 293 (2.7) |
| Gangwon-do | 286 (2.7) |
| Jeollabuk-do | 278 (2.6) |
| Jeju Island | 208 (1.9) |
| Gwangju | 153 (1.4) |
| Daejeon | 67 (0.6) |
| Sejong | 32 (0.3) |
| Type of hospitals | |
| Advanced general | 20,567 (61.3) |
| General | 11,753 (35.0) |
| Hospital | 1,089 (3.2) |
| Nursing hospital | 112 (0.3) |
| Clinic | 28 (0.1) |
| Hospital location | |
| Seoul | 12,354 (36.8) |
| Gyeonggi-do | 5,398 (16.1) |
| Incheon | 2,538 (7.6) |
| Daegu | 2,200 (6.6) |
| Gyeongsangnam-do | 1,861 (5.5) |
| Jeollabuk-do | 1,699 (5.1) |
| Busan | 1,482 (4.4) |
| Jeollanam-do | 1,048 (3.1) |
| Ulsan | 970 (2.9) |
| Chungcheongbuk-do | 884 (2.6) |
| Chungcheongnam-do | 866 (2.6) |
| Gangwon-do | 762 (2.3) |
| Gwangju | 610 (1.8) |
| Jeju Island | 552 (1.6) |
| Gyeongsangbuk-do | 163 (0.5) |
| Daejeon | 162 (0.5) |
CPR, cardiopulmonary resuscitation; IQR, interquartile range; LST, life-sustaining treatment.
Available for self-determinants only (n=10,774).
Table 2.
Age distribution according to the LST decision type
| Age (yr) | Self-determinants | Family-determinant |
|---|---|---|
| 19 | 0 | 6 (100) |
| 20–29 | 41 (22.8) | 139 (77.2) |
| 30–39 | 207 (41.1) | 297 (58.9) |
| 40–49 | 826 (49.1) | 857 (50.9) |
| 50–59 | 2,143 (47.8) | 2,340 (52.2) |
| 60–69 | 2,894 (41.0) | 4,168 (59.0) |
| 70–79 | 2,944 (29.5) | 7,027 (70.5) |
| 80–89 | 1,527 (19.0) | 6,505 (81.0) |
| ≥ 90 | 192 (11.8) | 1,436 (88.2) |
Values are presented as number (%). LST, life-sustaining treatment.
Fig. 2.

Distribution of patient residence and hospital location.
2. Difference of LST decision according to the disease
Patients were categorized as cancer and non-cancer according to the diagnosis. Lung cancer is the most common malignancy and pneumonia is the most common benign disease (Table 3). COPD, AIDS, and LC which are diagnosed as terminal illnesses by law, were only 7.9% (1,089/13,722) of all benign disease.
Table 3.
Diagnosis in non-cancer patients and cancer patients
| Rank | Cancer | No. (%) | Non-cancer | No. (%) |
|---|---|---|---|---|
| 1 | Malignant neoplasm of trachea, bronchus and lung (C33–C34) | 4,463 (22.5) | Pneumonia | 3,622 (26.4) |
| 2 | Malignant neoplasm of liver and intrahepatic bile ducts (C22) | 2,726 (13.7) | CVD | 1,389 (10.1) |
| 3 | Malignant neoplasm of colon, rectum and anus (C18–C21) | 1,804 (9.1) | Sepsis | 1,244 (9.1) |
| 4 | Malignant neoplasm of stomach (C16) | 1,746 (8.8) | Heart diseases | 1,208 (8.8) |
| 5 | Malignant neoplasm of pancreas (C25) | 1,689 (8.5) | LC | 600 (4.4) |
| 6 | Malignant neoplasm of breast (C50) | 742 (3.7) | COPD | 474 (3.5) |
| 7 | Non-Hodgkin lymphoma (C82–C86) | 617 (3.1) | Liver diseases | 208 (1.5) |
| 8 | Leukemia (C91–C95) | 617 (3.1) | Respiratory tuberculosis | 159 (1.2) |
| 9 | Malignant neoplasm of ovary (C56) | 355 (1.8) | Chronic lower respiratory diseases | 73 (0.5) |
| 10 | Malignant neoplasm of esophagus (C15) | 330 (1.7) | Diabetes mellitus | 57 (0.4) |
| 11 | Malignant neoplasm of prostate (C61) | 316 (1.6) | Hypertensive diseases | 38 (0.3) |
| 12 | Malignant neoplasm of bladder (C67) | 283 (1.4) | Alzheimer’s disease | 16 (0.1) |
| 13 | Multiple myeloma and malignant plasma cell neoplasms (C90) | 278 (1.4) | AIDS | 15 (0.1) |
| 14 | Malignant neoplasms of lip, oral cavity and pharynx (C00–C14) | 272 (1.4) | Other | 4,619 (33.7) |
| 15 | Malignant neoplasm of meninges, brain and other CNS (C70–C72) | 267 (1.3) | ||
| 16 | Malignant neoplasm of cervix uteri (C53) | 231 (1.2) | ||
| 17 | Secondary malignant neoplasm (C76–780) | 145 (0.7) | ||
| 18 | Malignant melanoma of skin (C43) | 95 (0.5) | ||
| 19 | Malignant neoplasm of corpus uteri and uterus unspecified (C54–C55) | 94 (0.5) | ||
| 20 | Malignant neoplasm of larynx (C32) | 44 (0.2) | ||
| 21 | Other and unspecified malignant neoplasms (Re. C00–C97) | 2,713 (13.7) |
AIDS, acquired immune deficiency syndrome; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular diseases; LC, liver cirrhosis.
More than half of the patients were male in both groups. Cancer patients were younger than non-cancer patients (p < 0.001). The rate of self-determination was significantly higher in cancer patients than non-cancer patients (47.3% vs. 10.1%, p < 0.001) (Table 4). Among the patients with terminal illness, self-determinant was 93.6% (6,680/7,135) in cancer patients while it was 6.38% (455/7,135) in non-cancer patients (p < 0.001). For the question, if they were willing to use hospice service in the near future, only 521 (37.5%) non-cancer patients answered yes, while 7,596 (81.0%) cancer patients answered yes (p < 0.001). The decision of withholding or withdrawing the LSTs on each items was higher in cancer patients than non-cancer patients (p < 0.001).
Table 4.
Comparison between cancer and non-cancer patients (n=33,549)
| Variable | Cancer | Non-cancer | p-value |
|---|---|---|---|
| No. of registrations | 19,827 (59.1) | 13,722 (40.9) | |
| Age (yr) | 69 (59–77) | 73 (62–81) | < 0.001 |
| Sex | |||
| Male | 12,378 (62.4) | 7,734 (56.4) | < 0.001 |
| Female | 7,449 (37.6) | 5,988 (43.6) | |
| Status of patient’s disease | |||
| Terminal illness | 6,680 (71.2) | 455 (32.7) | < 0.001 |
| Dying periods | 2,703 (28.8) | 936 (67.3) | |
| Subject of LST decisions | |||
| Self-determinants | 9,383 (47.3) | 1,391 (10.1) | < 0.001 |
| Family-determinants | 10,444 (52.7) | 12,331 (89.9) | |
| Plan for hospice service a) | |||
| Yes | 7,596 (81.0) | 521 (37.5) | < 0.001 |
| No | 1,354 (14.4) | 706 (50.8) | |
| Unmarked | 433 (4.6) | 164 (11.8) | |
| Marked LST items in the form 1 a) | |||
| CPR | 9,732 (99.9) | 1,378 (99.1) | < 0.001 |
| Mechanical ventilation | 9,333 (99.5) | 1,363 (98.0) | |
| Hemodialysis | 8,948 (95.4) | 1,156 (83.1) | |
| Anticancer drugs | 7,669 (81.7) | 833 (59.9) | |
| Patient’s residencea),b) | |||
| Seoul | 2,379 (85.7) | 397 (14.3) | < 0.001 |
| Busan | 554 (89.1) | 68 (10.9) | |
| Daegu | 467 (88.8) | 59 (11.2) | |
| Incheon | 805 (91.4) | 76 (8.6) | |
| Gwangju | 143 (93.5) | 10 (6.5) | |
| Daejeon | 57 (85.1) | 10 (14.9) | |
| Ulsan | 406 (88.5) | 53 (11.5) | |
| Sejong | 29 (90.6) | 3 (9.4) | |
| Gyeonggi-do | 2,109 (87.6) | 299 (12.4) | |
| Gangwon-do | 232 (81.1) | 54 (18.9) | |
| Chungcheongbuk-do | 241 (82.3) | 52 (17.7) | |
| Chungcheongnam-do | 248 (82.1) | 54 (17.9) | |
| Jeollabuk-do | 209 (75.2) | 69 (24.8) | |
| Jeollanam-do | 416 (90.4) | 44 (9.6) | |
| Gyeongsangbuk-do | 337 (92.1) | 29 (7.9) | |
| Gyeongsangnam-do | 569 (86.6) | 88 (13.4) | |
| Jeju Island | 182 (87.5) | 26 (12.5) | |
| Hospital type | |||
| Advanced general | 11,735 (59.2) | 8,832 (64.4) | < 0.001 |
| General | 7,049 (35.6) | 4,704 (34.3) | |
| Hospital | 946 (4.8) | 143 (1.0) | |
| Nursing hospital | 69 (0.3) | 43 (0.3) | |
| Clinic | 28 (0.1) | 0 | |
| Hospital location b) | |||
| Seoul | 7,874 (63.7) | 4,480 (36.3) | < 0.001 |
| Busan | 1,096 (74.0) | 386 (26.0) | |
| Daegu | 1,382 (62.8) | 818 (37.2) | |
| Incheon | 1,571 (61.9) | 967 (38.1) | |
| Gwangju | 119 (19.5) | 491 (80.5) | |
| Daejeon | 82 (50.6) | 80 (49.4) | |
| Ulsan | 643 (66.3) | 327 (33.7) | |
| Gyeonggi-do | 3,057 (56.6) | 2,341 (43.4) | |
| Gangwon-do | 368 (48.3) | 394 (51.7) | |
| Chungcheongbuk-do | 457 (51.7) | 427 (48.3) | |
| Chungcheongnam-do | 437 (50.5) | 429 (49.5) | |
| Jeollabuk-do | 586 (34.5) | 1,113 (65.5) | |
| Jeollanam-do | 772 (73.7) | 276 (26.3) | |
| Gyeongsangbuk-do | 58 (35.6) | 105 (64.4) | |
| Gyeongsangnam-do | 1,006 (54.1) | 855 (45.9) | |
| Jeju Island | 319 (57.8) | 233 (42.2) | |
Values are presented as number (%) or median (IQR). CPR, cardiopulmonary resuscitation; IQR, interquartile range; LST, life-sustaining treatment.
Only for whom wrote the form 1,
Percentages were summation within the region.
All reviewed patients’ most common place of residence and location of hospitals were Seoul and capital area. The types of hospitals were mostly in advanced general hospitals and general hospitals in both cancer patients and non-cancer patients (94.7% and 98.6%, respectively).
3. Comparison of features according to self-determinants and family-determinants
The number of family-determinants was more than twice the number of self-determinants 22,775 (67.9%) and 10,774 (32.1%), respectively (Table 5). Self-determinants had more a diagnosis of cancer and were more male than family-determinants. Self-determinants were also younger than family-determinants (p < 0.001). Both self-determinants and family-determinants mainly prepared the LST decision forms in advanced general and general hospitals (61.3% and 35.0%, respectively). The national average rate of self-determinants across the nation was 28.3%. The regions higher than the national average were as follows: Ulsan (51.8%), Jeollanam-do (48.8%), Busan-si (37.4%), Jeju island (36.2%), Incheon (35.7%), Gyeonggi-do (34.5%), Gyeongsangnam-do (34.0%), Daegu (33.4%), and Seoul (32.6%). Of the regions below the national average, less than 10% were Gwangju and Gyeongsangbuk-do with 2.1% and 3.7%, respectively.
Table 5.
Comparison of characteristics according to the LST decision-making
| Total | No. (%) | p-value | ||
|---|---|---|---|---|
| Self-determinants | Family-determinants | |||
| No. of registrations | 33,549 | 10,774 (32.1) | 22,775 (67.9) | |
| Diagnosis | ||||
| Non-cancer | 13,772 | 1,391 (12.9) | 12,331 (54.1) | < 0.001 |
| Cancer | 19,827 | 9,383 (87.1) | 10,444 (45.9) | |
| Sex | ||||
| Male | 20,112 | 6,822 (63.3) | 13,290 (58.4) | < 0.001 |
| Female | 13,437 | 3,952 (36.7) | 9,485 (41.6) | |
| Age (yr) | 73 (62–81) | 67 (58–76) | 75 (65–82) | < 0.001 |
| Hospital type | ||||
| Advanced general | 20,567 | 5,816 (54.0) | 14,751 (64.8) | < 0.001 |
| General | 11,753 | 4,430 (41.1) | 7,323 (32.2) | |
| Hospital | 1,089 | 480 (4.5) | 609 (2.7) | |
| Nursing hospital | 112 | 26 (0.2) | 86 (0.4) | |
| Clinic | 28 | 22 (0.2) | 6 (0) | |
| Hospital location a) | ||||
| Seoul | 12,354 | 4,027 (32.6) | 8,327 (67.4) | < 0.001 |
| Busan | 1,482 | 555 (37.4) | 927 (62.6) | |
| Daegu | 2,200 | 734 (33.4) | 1,466 (66.6) | |
| Incheon | 2,538 | 905 (35.7) | 1,633 (64.3) | |
| Gwangju | 610 | 13 (2.1) | 597 (97.9) | |
| Daejeon | 162 | 32 (19.8) | 130 (80.2) | |
| Ulsan | 970 | 502 (51.8) | 468 (48.2) | |
| Gyeonggi-do | 5,398 | 1,861 (34.5) | 3,537 (65.5) | |
| Gangwon-do | 762 | 206 (27.0) | 556 (73.0) | |
| Chungcheongbuk-do | 884 | 211 (23.9) | 673 (76.1) | |
| Chungcheongnam-do | 866 | 180 (20.8) | 686 (79.2) | |
| Jeollabuk-do | 1,699 | 199 (11.7) | 1,500 (88.3) | |
| Jeollanam-do | 1,048 | 511 (48.8) | 537 (51.2) | |
| Gyeongsangbuk-do | 163 | 6 (3.7) | 157 (96.3) | |
| Gyeongsangnam-do | 1,861 | 632 (34.0) | 1,229 (66.0) | |
| Jeju Island | 552 | 200 (36.2) | 352 (63.8) | |
Values are presented as number (%) or median (IQR). IQR, interquartile range; LST, life-sustaining treatment.
Percentages were summation within the region.
4. Comparison of decision on each LST items
We compared four items of LST decisions in patients who wrote both the form 1 and form 13 (S4 Table). Although the number is small, not all of the patient’s intention has been declared. The inconsistency rate between form 1 and form 13 on each LST items was not different according to the disease. However, inconsistency rate of anticancer drugs had a higher tendency than other items (Fig. 3, S4 Table).
Fig. 3.

Forest plots of inconsistency rate of four items of LST decisions between form 1 and form 13. CI, confidence interval; CPR, cardiopulmonary resuscitation; CTx, anticancer drugs; HD, hemodialysis; LST, life-sustaining treatment; MV, mechanical ventilation.
The withholding or withdrawing of CPR was not different in both self-determinants and family-determinants (p=0.820) (Fig. 4). The rate of withholding or withdrawing of mechanical ventilation, hemodialysis, and anticancer drugs was significantly higher in self-determinants than family-determinants (p < 0.001) (Fig. 4).
Fig. 4.

Comparison of implementation of four items of life-sustaining treatment decisions between self-determinants and family-determinants. CPR, cardiopulmonary resuscitation.
Discussion
In our study, withholding or withdrawing the LST were more than twice as high as in the family-determinants than the self-determinants. 87.1% of self-determinants had diagnosis of cancer. Before law enforcement, most of the hospitals used the DNR form to withhold or withdraw the CPR. Two studies in the oncology inpatient clinic by Oh et al. [4] and Kim et al. [6], reported the practice of the LST under using the CPR form. In these two studies almost all decisions of DNR have taken among the physician and family members, except in only one case that did not have a family member. Patients were completely excluded from the decision process of LST determination intentionally or unintentionally. However, patients’ involvement of LST decision-making was different according to the clinical situation and using the ADs. Approximately 35.5% patients in the hospice center completed the ADs while others could not complete the ADs because of poor physical and mental status [12]. The median date between the date of ADs and death (median, 22 days) were longer than previous studies (7–8 days). Changing the form from the DNR to ADs might be a reason because a following study by Hong et al. [13] in the same center reported that patients’ participation of end-of-life care discussion has been increased after adopting ADs in their clinical practice (30% to 51%, p < 0.001). In our study, 32.1% of study population and 47.3% of patients with cancer were self-determinants. It is quite higher than the periods using the DNR form for LST decision and similar to the studies by Hong et al. [13]. It is also similar to the study of single center reviewing individual patient’s data which reported that 29% (231/809) patients completed the LST forms by themselves [14]. Considering that two studies using ADs in the end-of-life discussion, physician’s interest and using the ADs could have a positive effect increasing the participation of patients in the discussion [12,13]. However, the law also has a positive effect enforcing the use of legal forms of LST to some extent because most of the hospitals that completed the legal forms were not hospice centers.
In our study, self-determinants were higher in cancer patients than non-cancer patients. During our study periods, the first edition of the law allowed “terminal illness” as a diagnosis in cancer patients and only three kinds of non-cancer diagnosis including AIDS, LC, and COPD [10]. Most of the non-cancer patients could start the LST decision process when they were diagnosed in the dying process. LST discussion during the dying process might have been impossible because of rapid deterioration of their mental or physical conditions [15,16]. For cancer patients, diagnosis of terminal illness is relatively easier than benign disease by the nature of disease trajectory [17] where as it is hard to differentiate terminal illness from the reversible condition in benign disease. Continuous revision of the law allows the diagnosis of “terminal illness” regardless of the type of disease [18]. It is hoped that only a revision of the law reflecting this reality will give the patients at end-of-life an opportunity to prepare for and face death.
In our study, the mean duration between form 1 and form 13 was longer than the mean time for form 11 and 12. When patients think over and make decisions of LST, they need enough time to think over their conditions and to understand withholding or withdrawing any type of futile treatment. However, when family members decided to withhold or withdraw LSTs it could be due to the difficulty to think and judge due to the shock of the sudden exposure of their family member approaching death [19]. We also could not exclude the possibility that patients might receive more LSTs based on family’s opinion rather than patients’ will. Earlier discussion of LST with patients and family members could give them the time to fully think about LST and make decisions properly.
LST items of the decision, except CPR, were different between self-determinants and family-determinants. The withholding or withdrawing rate of CPR were the same in both groups (99.6%, p=0.820). Other items including mechanical ventilation, hemodialysis, and anticancer drugs were higher in the self-determinants than family-determinants (98.9% vs. 79.4%, 93.2% vs. 80.4%, 78.4% vs. 56.0%; p < 0.001, respectively). The difference of LST items in form 13 between self-determinants and family-determinants might reflect differences of their clinical situation or less time for decision.
The LST decision forms were mainly prepared at advanced general hospitals (61.3%) and general hospitals (35.0%). In contrast, registration rate of LST decision was very low at 3.2% and 0.3% in the hospitals and nursing hospitals, respectively. In Korea, most patients who have no more effective treatment are often transferred to hospitals or nursing hospitals and finish the disease trajectory there. However, these hospitals seldom establish an ethics committee, which is a prerequisite for the law process of LST decision. As of January 2019, the registration rate of the institutional ethics committee was 0.6% (9/1,465), and 1.4% (22/1,560) in the hospitals, and nursing hospitals, respectively [20]. A common ethics committee is being proposed as an alternative, but in reality, it is not easy. The law was implemented without a clear distinction between withholding or withdrawing LSTs in patients with terminal illness or at the end-of-life and withholding or withdrawing LSTs in patients in vegetable states. So the law was strictly enacted, as if to withhold or withdraw LSTs for patients in vegetable conditions. This might be one of the hurdles of settling the LST decision process.
Among non-cancer patients, a benign disease that could be diagnosed as a terminal illness was about eight percent and most of non-cancer patients completed the legal forms at the end-of-life process. Continuous revision of the law could expand the number of diseases permitted for legal LST forms as well as preliminary discussions about LSTs between physicians and patients.
The study has some limitations. First, we could not differentiate the dead and the alive in the database of the National Agency for Management of Life-Sustaining Treatment. The personal information protect act did not allow to merge the data with Statics Korea’s death data. To overcome this limitation, we included the individual data, which has form 13. The second limitation is the uncertainly of diagnosis we collected. The diagnosis of form 9 was not from the Korean Standard Classification of Disease, nor was the code of the diagnosis in the reimbursement system. Non-cancer diagnosis of form 9 might be a direct cause of death in cancer patients. This could explain the high rate (56%) of selecting anticancer treatment as a LST in non-cancer patients. However, we could not deny the possibility of confusion between patients and physicians during the LST decision process (published elsewhere by Baik et al.).
In conclusion, our study showed that 32.1% were self-determinants and 67.9% were family-determinants during the first year after the law was enacted. Self-determinants were 47.3% in cancer patients and 10.1% in non-cancer patients. The legal forms of LSTs were written mainly in Seoul and capital areas, advanced general and general hospitals. A future revision of the law to overcome the problems currently faced in hospitals will permit a change in the LST decision process. Future studies regarding the status of LST decision-making could assist in understanding the status of LST decision-making and future directions.
Acknowledgments
This study was supported by a grant from the National Evidence-based Healthcare Collaborating Agency (NA19–008).
Footnotes
Ethical Statement
This study was approved by the Ethics Committee of the National Evidence-Based Healthcare Collaborating Agency (NA19-008) and the Kangdong Sacred Heart Hospital (2019-12-013), which waived the need for informed consent because this was a descriptive study and no personal information included in the data set provided. The study was conducted in accordance with the Principles of the Declaration of Helsinki.
Author Contributions
Conceived and designed the analysis: Lee HY, Kim HJ, Kwon JH, Baek SK, Won YW, Kim YJ, Baik SJ, Ryu H.
Collected the data: Lee HY, Kim HJ, Kwon JH, Baek SK, Won YW, Kim YJ, Baik SJ, Ryu H.
Contributed data or analysis tools: Lee HY, Kim HJ, Kwon JH, Baek SK, Won YW, Kim YJ, Baik SJ, Ryu H.
Performed the analysis: Lee HY, Kim HJ, Kwon JH, Baek SK, Won YW.
Wrote the paper: Lee HY, Kim HJ, Kwon JH.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
Supplementary Information
Supplementary materials are available at Cancer Research and Treatment website (https://www.e-crt.org).
References
- 1.Heo DS. Overview and current issues. Korean J Med. 2009;77(Suppl 4):S1026–34. [Google Scholar]
- 2.Koh Y, Heo D, Yun YH, Moon JL, Park HW, Choung JT, et al. Characteristics and issues of guideline to withdrawal of a life-sustaining therapy. J Korean Med Assoc. 2011;54:747–57. [Google Scholar]
- 3.Heo DS. Patient autonomy and advance directives in Korea. J Korean Med Assoc. 2009;52:865–70. [Google Scholar]
- 4.Oh DY, Kim JH, Kim DW, Im SA, Kim TY, Heo DS, et al. CPR or DNR? End-of-life decision in Korea cancer patients: a single center’s experience. Support Care Cancer. 2006;14:103–8. doi: 10.1007/s00520-005-0885-5. [DOI] [PubMed] [Google Scholar]
- 5.Yun YH, Lee CG, Kim SY, Lee SW, Heo DS, Kim JS, et al. The attitudes of cancer patients and their families toward the disclosure of terminal illness. J Clin Oncol. 2004;22:307–14. doi: 10.1200/JCO.2004.07.053. [DOI] [PubMed] [Google Scholar]
- 6.Kim DY, Lee KE, Nam EM, Lee HR, Lee KW, Kim JH, et al. Do-not-resuscitate orders for terminal patients with cancer in teaching hospitals of Korea. J Palliat Med. 2007;10:1153–8. doi: 10.1089/jpm.2006.0264. [DOI] [PubMed] [Google Scholar]
- 7.Lee JK, Keam B, An AR, Kim TM, Lee SH, Kim DW, et al. Surrogate decision-making in Korean patients with advanced cancer: a longitudinal study. Support Care Cancer. 2013;21:183–90. doi: 10.1007/s00520-012-1509-5. [DOI] [PubMed] [Google Scholar]
- 8.Supreme Court Decision 2002Do995 decided Jun 24, 2004[Internet] Seoul: Supreme Court of Korea; 2002. [cited 2021 Feb 17]. Available from: https://glaw.scourt.go.kr/ [Google Scholar]
- 9.Supreme Court Decision 2009Da17417 decided May 21, 2009[Internet] Seoul: Supreme Court of Korea; 2009. [cited 2021 Feb 17]. Available from: https://glaw.scourt.go.kr/ [Google Scholar]
- 10.National Law Information Center. Act on Decisions on Life-Sustaining Treatment for Patients in Hospice and Palliative Care or the End-of-life [Internet] Sejong: Korea Ministry of Government Legislation; 2016. [cited 2021 Feb 17] Available from: https://law.go.kr. [Google Scholar]
- 11.Vital Statistics Division, Statistics Korea. Shin HY, Kim J, Lee S, Park MS, Park S, et al. Cause-of-death statistics in 2018 in the Republic of Korea. J Korean Med Assoc. 2020;63:286–97. [Google Scholar]
- 12.Kong BH, An HJ, Kim HS, Ha SY, Kim IK, Lee JE, et al. Experience of advance directives in a hospice center. J Korean Med Sci. 2015;30:151–4. doi: 10.3346/jkms.2015.30.2.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hong JH, Kwon JH, Kim IK, Ko JH, Kang YJ, Kim HK. Adopting advance directives reinforces patient participation in end-of-life care discussion. Cancer Res Treat. 2016;48:753–8. doi: 10.4143/crt.2015.281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kim JS, Yoo SH, Choi W, Kim Y, Hong J, Kim MS, et al. Implication of the Life-Sustaining Treatment Decisions Act on End-of-Life Care for Korean Terminal Patients. Cancer Res Treat. 2020;52:917–24. doi: 10.4143/crt.2019.740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Heo DS. End-of-life decision in Korea. J Korean Med Assoc. 2008;51:524–9. [Google Scholar]
- 16.Oh DY, Kim JE, Lee CH, Lim JS, Jung KH, Heo DS, et al. Discrepancies among patients, family members, and physicians in Korea in terms of values regarding the withholding of treatment from patients with terminal malignancies. Cancer. 2004;100:1961–6. doi: 10.1002/cncr.20184. [DOI] [PubMed] [Google Scholar]
- 17.Amblas-Novellas J, Murray SA, Espaulella J, Martori JC, Oller R, Martinez-Munoz M, et al. Identifying patients with advanced chronic conditions for a progressive palliative care approach: a cross-sectional study of prognostic indicators related to end-of-life trajectories. BMJ Open. 2016;6:e012340. doi: 10.1136/bmjopen-2016-012340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.National Law Information Center. Act on Hospice and Palliative Care and Decisions on Life-Sustaining Treatment for Patients at the End-of-life [Internet] Sejong: Korea Ministry of Government Legislation; 2018. [cited 2021 Feb 28]. Available from: https://law.go.kr. [Google Scholar]
- 19.Wiegand D. In their own time: the family experience during the process of withdrawal of life-sustaining therapy. J Palliat Med. 2008;11:1115–21. doi: 10.1089/jpm.2008.0015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Monthly statistics [Internet] Seoul: National Agency for Management of Life-sustaining Treatment; 2020. [cited 2020 Dec 17]. Available from: https://www.lst.go.kr/comm/monthlyStatistics.do. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.