

Background: Concerns exist about the efficacy of COVID-19 vaccines against immune escape by viral variants of concern (VOCs): Delta is currently the most common VOC worldwide (1), and nasopharyngeal swabs (NPSs) show that fully vaccinated persons, like unvaccinated persons, harbor infectious viral loads (2). Reports to date have assessed the prevalence of vaccine breakthrough (VBT) infection among health care workers (HCWs), mostly based on spontaneous self-reporting by symptomatic HCWs and hence missing asymptomatic persons, who could nevertheless transmit the pathogen. Once a positive result is identified in an HCW, most countries ask for a 14-day quarantine or 2 consecutive follow-ups after at least 10 days before the HCW is admitted back to the workplace. Such mandatory quarantines can lead to large HCW shortages and cause health crises in hospitals.
Objective: To systematically surveil 2397 HCWs fully vaccinated with BNT162 at the ASST Settelaghi hospitals (Lombardy, Italy) in February 2021.
Methods and Findings: Since March 2021, hospital directive IGG02PG32/2021 has classified wards according to risk for infection from attending patients and mandated surveillance of HCWs. Fully vaccinated HCWs (n = 2397) who worked in 8 wards deemed to be at “high risk” had a mandatory NPS with SARS-CoV-2 polymerase chain reaction (PCR) testing every 2 weeks, and those in 8 “moderate-risk” wards were tested every 4 weeks. The screening used 1 of 2 real-time PCR tests (m2000 RealTime System or Alinity m SARS-CoV-2 Assay [Abbott]). If SARS-CoV-2 RNA was detected, the HCW was tested with daily NPSs until 2 consecutive NPSs were negative for SARS-CoV-2. Positive samples with cycle thresholds below 25 were retested by spike gene sequencing; positive samples with cycle thresholds between 25 and 35 were retested with a VOC-specific multiplex real-time PCR (SARS-CoV-2 Extended ELITe MGB Kit [ELITechGroup]) targeting L452R, E484K, and N501Y. A voluntary postvaccine serologic program was implemented using the LIAISON SARS-CoV-2 S1/S2 IgG assay (DiaSorin).
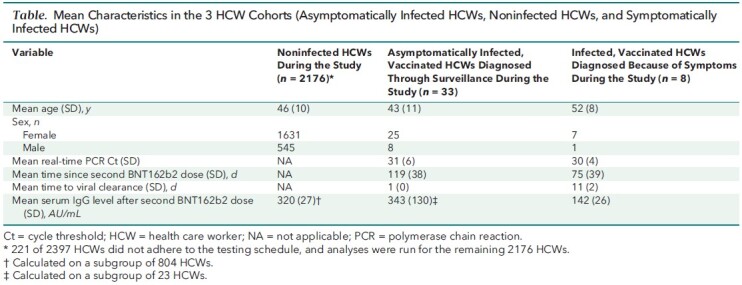
Between 15 March and 17 August 2021, we identified 33 cases of SARS-CoV-2 infection as part of the surveillance program, 17 among 789 HCWs (2.1%) in the high-risk group tested every 2 weeks and 16 among 1387 HCWs (1.1%) in the moderate-risk group tested every 4 weeks; none of these case patients ever developed symptoms, and none had immune deficiency or significant comorbid conditions. Five cases were further characterized by spike gene sequencing and 12 by VOC-specific real-time PCR. The Figure presents cases and background community prevalence of COVID-19 during the study period. During the same interval, 8 HCWs (0.4%) tested positive while symptomatic; only 1 variant could be characterized as Alpha by sequencing. The Table presents characteristics of HCWs according to surveillance results and symptoms. All 33 asymptomatic case patients tested negative the day after the initial positive result, and all negative results were confirmed on a third NPS 2 days afterward. In contrast, symptomatic cases cleared after a mean of 11 days. The mean IgG level was twice as high in the asymptomatic than the symptomatic group.
Figure. PCR Cts for SARS-CoV-2 cases among HCWs and community COVID-19 cases during the study period.
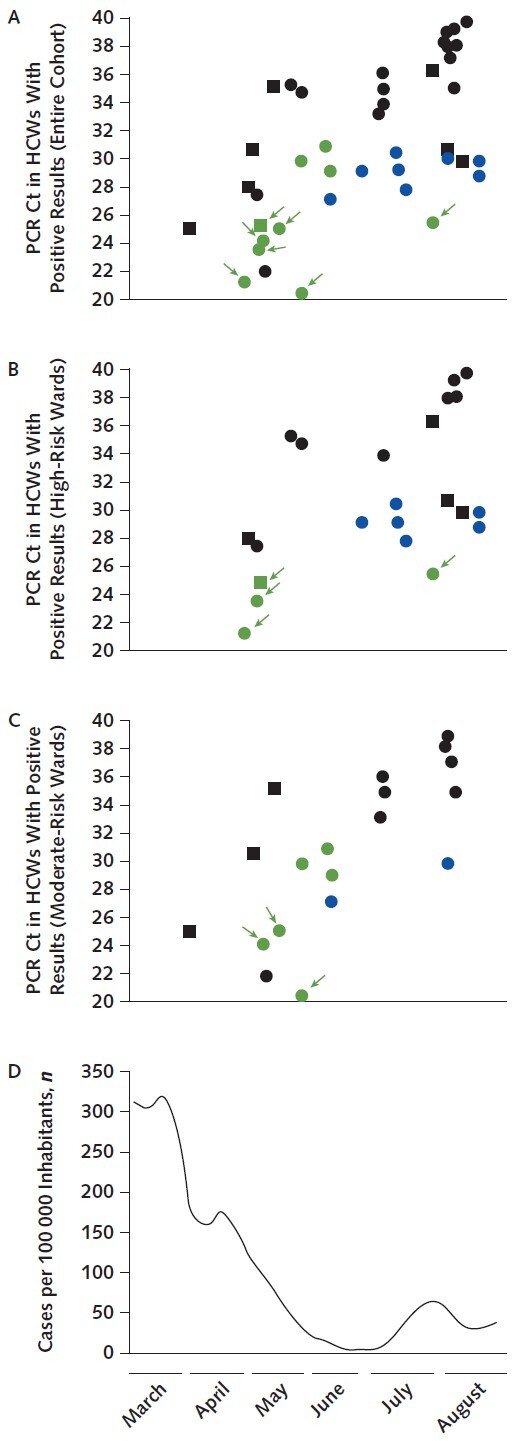
Circles indicate asymptomatic infection, and squares indicate symptomatic infection. The color indicates Alpha variant (green), Delta variant (blue), or undefined strain (black). Arrows indicate attribution based on spike gene sequencing. Ct = cycle threshold; HCW = health care worker; PCR = polymerase chain reaction. A. All asymptomatic and symptomatic cases. B. Cases among HCWs screened every 2 wk working in wards deemed to have high exposure risk (hematology, pediatric oncohematology, general oncology, gynecologic oncology, dialysis and nephrology, general and transplant surgery, infectious diseases, and neonatal intensive care unit). C. Cases among HCWs screened every 4 wk working in wards deemed to have moderate exposure risk (radiotherapy, thoracic surgery, heart surgery, rheumatology, pneumology, COVID hub 1, COVID hub 2, and emergency department). D. Weekly positive SARS-CoV-2 PCR incidence rate in the area of Insubria, Italy (where HCWs resided), during the study period.
Table.
Mean Characteristics in the 3 HCW Cohorts (Asymptomatically Infected HCWs, Noninfected HCWs, and Symptomatically Infected HCWs)
Discussion: Our results indicate that systematic surveillance of asymptomatic vaccinated HCWs uncovers many times more cases of VBT infection than symptom-based testing. The incidence of asymptomatic VBT infections seemed to depend on the frequency of testing and not occupational risk or community prevalence; once corrected for frequency of testing, incidence was similar in the high- and moderate-risk groups. Asymptomatic cases seemed to clear much more quickly and had higher mean antibody levels than symptomatic cases. Because of the rapid viral clearance in asymptomatic VBT infections, our surveillance program likely missed many other such infections.
Benenson and colleagues (3) reported that 689 of 6680 HCWs (10.3%) had VBT infections across 7 weeks of study, but this estimate included HCWs who had received a single dose of BNT162b2. Keehner and colleagues (4) reported 7 cases out of 5455 HCWs at the University of California, San Diego, and 9535s HCWs at the University of California, Los Angeles (0.05%), who were fully vaccinated with BNT162b2 or mRNA-1273. Another study reported 33 cases (16 mildly symptomatic and 17 asymptomatic) among 3694 HCWs fully vaccinated with BNT162b2, without details on time to viral clearance (5)—consistent with our estimates of symptomatic cases. All of these studies were done at times when Alpha was the dominant SARS-COV-2 variant, whereas our study was mostly run during the Delta predominance.
Study limitations include the inability to perform genetic sequencing for more accurate VOC imputation in patients with cycle thresholds above 25 and the lack of viral neutralization assays to assess neutralizing antibody levels. We likely missed a large proportion of asymptomatic VBT infections cleared during intervals between NPSs.
Our findings suggest that regular testing of asymptomatic vaccinated HCWs who tested positive for SARS-CoV-2 may preclude the need for long quarantines, but this requires confirmation in larger studies. Surveillance programs aimed at capturing all VBT infections would need to include frequent testing. In the absence of such frequent surveillance, maintaining vigilant use of personal protective equipment seems to be warranted.
Footnotes
This article was published at Annals.org on 19 October 2021.
References
- 1. Farinholt T , Doddapaneni H , Qin X , et al. Transmission event of SARS-CoV-2 Delta variant reveals multiple vaccine breakthrough infections. med. Rxiv. 2021. [PMID: ] doi: 10.1101/2021.06.28.21258780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Riemersma KK, Grogan BE, Kita-Yarbro A, et al. Vaccinated and unvaccinated individuals have similar viral loads in communities with a high prevalence of the SARS-CoV-2 delta variant. medRxiv. Preprint posted online 31 July 2021. doi:10.1101/2021.07.31.21261387
- 3. Benenson S , Oster Y , Cohen MJ , et al. BNT162b2 mRNA Covid-19 vaccine effectiveness among health care workers [Letter]. N Engl J Med. 2021;384:1775-1777. [PMID: ] doi: 10.1056/NEJMc2101951 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Keehner J , Horton LE , Pfeffer MA , et al. SARS-CoV-2 infection after vaccination in health care workers in California [Letter]. N Engl J Med. 2021;384:1774-1775. [PMID: ] doi: 10.1056/NEJMc2101927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rovida F, Cassaniti I, Paolucci S, et al. SARS-CoV-2 vaccine breakthrough infections are asymptomatic or mildly symptomatic and are infrequently transmitted. medRxiv. Preprint posted online 3 July 2021. doi:10.1101/2021.06.29.21259500