

Abstract
Objective:
To evaluate longitudinal associations between recreational screen time and sleep in early childhood, and attention-deficit/hyperactivity disorder (ADHD) at age 8 to 10 years.
Method:
Questionnaires from 2,768 mother-child pairs from the Dutch KOALA Birth Cohort Study were used. General estimating equation logistic regression analyses examined associations between screen time and sleep at age 2, 4, and 6, and ADHD at age 8 to 10. Linear regression analysis examined associations between television time, sleep and CBCL/2-3 scores at age 2.
Results:
Longitudinally, neither screen time nor sleep were associated with ADHD. Cross-sectionally, CBCL/2-3 externalizing symptom scores increased by 0.03 with every hour television time (95% CI 0.002–0.05) and increased by 0.02 per hour of less sleep (95% CI −0.03–−0.01).
Conclusion:
Despite an association with externalizing symptoms at age 2, screen time and sleep in early childhood were not associated with ADHD. Carefulness is warranted when extrapolating cross-sectional associations at early age to an ADHD diagnosis.
Keywords: ADHD, child, television, digital media use, externalizing symptoms, sleep
Introduction
Since the introduction of the television (TV) in the 1950s, the use of digital media has become an integral part of the lives of children and adolescents. Although a recent American study by Loprinzi and Davis showed a slow decline in parent reported television use among preschool and primary school children over the past two decades, most parents still reported that their children watched TV, on average, for 2 hr/day (Loprinzi & Davis, 2016). This decrease in watching TV may be explained by a rapid increase in other digital media use, like (game) computers and touch screen telephones and tablets (The Lancet Child Adolescent Health, 2018). Worldwide, both parents and health care workers have concerns about the possible negative effects of screen use, whether TV screens or other digital media use, on the physical and psychological health of children and adolescents. One health-related concern is the potential impact screen use has on attention-deficit/hyperactivity disorder (ADHD) or ADHD-like symptoms (Ceranoglu, 2018; Reid Chassiakos et al., 2016). Several cross-sectional studies showed a positive association between ADHD-like symptoms and different types of screen use (Lingineni et al., 2012; van Egmond-Fröhlich et al., 2012; Zimmerman & Christakis, 2007). A longitudinal cohort study by Ra et al. (2018), indicated, for example, that high-frequency digital media use by high school students was associated with significantly higher odds for ADHD-like symptoms, and emphasized the importance of longitudinal research of the development of ADHD (Ra et al., 2018). As most studies regarding digital media use so far are cross-sectional, and only focus on behavioral symptoms of ADHD, it is extremely difficult to determine whether children who are often exposed to digital media are more prone to actually develop ADHD, or if children with ADHD, for example, tend to use more digital media (Ioannidis et al., 2019; Starcevic & Khazaal, 2017).
When evaluating a possible relationship between hours of screen time and ADHD, sleep is also an important factor to consider. Sleep can be a confounder, mediator, or independent variable. A systematic literature review concerning screen time and sleep among healthy school-aged children found that screen time was adversely associated with sleep outcomes (primarily shortened duration and delayed timing) (Hale & Guan, 2015). Besides that, less sleep duration can cause an increase in ADHD symptoms, and various studies also showed an association between ADHD and sleep problems (Cortese et al., 2009; Owens et al., 2000; van der Heijden et al., 2018).
To date, no longitudinal studies were reported, in which both screen time and total sleep duration were monitored early in life, and in addition data concerning a possible ADHD diagnoses were collected in childhood, considering potential pre, peri- and postnatal confounding factors. The main research question of this study was the longitudinal association between the amount of recreational screen time and sleep duration from age 2 until the age of 6 to 8 years, and an ADHD diagnosis at age 8 to 10 years. In addition, at the age of 2, associations between television time, the total amount of sleep and specific behavioral characteristics (i.e., overactive and externalizing behavior) were analyzed.
Method
Participant Population
Data originated from the prospective KOALA Birth Cohort Study in the Netherlands (Kummeling et al., 2005). Healthy pregnant women were recruited between October 2000 and December 2002 from the general population, by approaching women who participated in an existing study on pregnancy-related pelvic girdle pain (N = 2,343, referred to as conventional recruitment group). In addition, healthy pregnant women with an “alternative lifestyle” with regard to dietary habits (e.g., preferring organic food), vaccination programs and/or antibiotic use were recruited through posters in organic shops, or anthroposophical physician offices and midwives, Steiner schools and magazines (N = 491, referred to as the alternative recruitment group). Mother-infant pairs were excluded from analysis for the current study when the mother had a twin or a multiple pregnancy, when the infant died, or in case the child had a severe congenital disorder leading to intellectual disability, such as Down’s syndrome. All parents signed informed consent, and ethical approval was obtained from the medical ethics committee of the Maastricht University/University Hospital of Maastricht.
Data Collection
Questionnaires especially designed for the KOALA study were completed by parents during pregnancy and at set moments in the child’s life. Information on pre- peri- and postnatal factors, and various lifestyle characteristics were collected. The current study used data from the questionnaires at 14 and 34 weeks of gestation, and at child ages of 2 weeks, 3 months, 2 years, 4 to 5 years, 6 to 8 years, and 8 to 10 years. Questionnaires at age 2 were retrieved throughout the year, at age 4 to 5 and 6 to 8 they were distributed and retrieved during the schoolyear.
Dependent variables
Data regarding an ADHD diagnosis was obtained by questionnaire, filled out by the parents at child’s age 8 to 10 years in 2011. Parents were asked through an open question: “Did a doctor, psychologist, or remedial educationalist diagnose your child with ADHD?” The answer to this question was used as outcome measure of professional based parent-reported ADHD, simply referred to as “parent reported ADHD.” In addition, parents were asked informed consent to approach their general practitioner (GP) for retrieval of medical data. These GPs were mailed in 2014 with a short questionnaire including: “Has the above-named patient ever been diagnosed with ADHD?” Because the diagnosis from GPs was retrieved in a subgroup of the cohort, these data were only used to validate whether results with parent reported ADHD as outcome were confirmed by GP reported ADHD.
At the age of 2, questions from the Child Behavior Checklist/2-3 (CBCL/2–3) for children aged 2 to 3 years, were included in the KOALA questionnaire. The CBCL is a component of the Achenbach System of Empirically Based Assessment (ASEBA), developed by Thomas M. Achenbach (Achenbach & Rescorla, 2001). For this study, the factor structure of the CBCL/2-3 based on the article of Koot et al. (1997) was used, who adapted the structure of the American CBCL/2-3 to the Dutch situation (Koot et al., 1997). This Dutch version of the CBCL/2-3 addressed behavioral problems at a young age, which were subdivided into externalizing problems (overactive, aggressive, and oppositional scale) and internalizing problems (anxious, depressed, and sleep problems scale). Psychometric properties of this Dutch CBCL/2-3 were comparable to those obtained from American samples (Koot et al., 1997). For the current study, only the externalizing scale which included the overactive subscale was selected, as symptoms linked to attention deficit at pre-school age are part of the externalizing scale of the CBCL/2-3. Parents were asked to rate items that described the child’s behavior at that moment or within the past 2 months as 2 if the item was true or often true, 1 if the item was somewhat or sometimes true, and 0 if the item was not true. Mean scale scores were computed by summing the raw scores of 0, 1, and 2 on each CBCL/2-3 item belonging to the Dutch oppositional behavior (17 items), aggression (9 items) and overactive behavior scale (5 items), and dividing total raw scores by the number of items in the specific scale.
Exposure variables and potential confounders
Questions re-garding recreational screen time included questions about daily hours of watching television and playing computer games outside school hours, and were asked at the age of 2, 4 to 5, and 6 to 8 years. The sum of TV time and computer time will hereinafter be referred to simply as screen time. At age 2, both for TV time and computer time, parents could choose between five standardized answers concerning minutes of TV and computer time per day. At ages 4 to 5 and 6 to 8, first parents were asked about the number of days per week, and then about the minutes per day of TV and computer use, using standardized answers. Averages were calculated from these two variables. Data regarding total sleep duration were collected using open ended questions, which asked about average hours of sleep during day- and night-time at ages 2 and 4 to 5. Total sleep duration was measured by adding hours of day- and night-time sleep. At 6 to 8 years, general sleep duration over 24 hr was asked (see Supplemental Appendix 1 for exact questions). Maternal social demographic data were collected at 14 gestational weeks. Data on maternal prenatal smoking and alcohol use came from the questionnaires completed by 14- and 34-weeks’ gestation. Perinatal data, including gestational age, gender of the child and birth weight were collected 2 weeks after birth. Data on marital discord came from the questionnaire 3 months postpartum. Questions on daily family routine were asked in the questionnaire taken at the age of 2 years. Data concerning hours of playing outside were asked at the age of 2, 4 to 5, and 6 to 8 years and analyzed as a possible confounder; results are only shown if significant.
Some determinants had missing values. For education, mode of birth, marital discord and daily family routine the missing values were placed in an “other/unknown” group in the baseline characteristics table, missing values are presented in a separate “unknown” category. For pre-pregnancy BMI the median was imputed and the GHQ missing values were placed in the “GHQ score <3” category. For TV time, computer time, and sleep missing values were not replaced.
Data Analysis
All statistical analyses were performed using SPSS software (IBM SPSS Statistics for Windows). General estimating equation (GEE) logistic regression analyses with an independent correlation structure were performed to examine the longitudinal associations between total screen time (television watching plus playing computer games outside school hours), and total sleep duration (daytime plus nighttime sleep) at ages 2, 4 to 5, and 6 to 8 as the repeated exposure variables, and parent reported ADHD at age 8 to 10 as the outcome variable. The same analysis was done with GP reported ADHD as the outcome variable, these results are presented in the Supplemental Appendix. Persistence of associations over time of follow-up was evaluated by testing for interaction with time (age when the questionnaires of the exposure variables were taken) in the GEE models, which is reported if the p-value for interaction was less than .05. Deviation from linearity was tested by adding quadratic terms to the GEE model for both screen time and sleep and checking for significance (p < .05). To assess whether the longitudinal association were modified by gender or were different between the recruitment groups, results were stratified and only presented if significant (p < .05).
After examining the univariate characteristics of the independent variables, multiple linear regression analysis was used to assess the cross-sectional analysis of the association between the continuous variable’s hours of TV time and total sleep duration at the age of 2 years as independent exposure variables, and mean CBCL/2-3 scores on the overactive scale and externalizing scale as outcome variables, correcting for potential confounding covariates. Television time was used as a separate variable, due to the low amount of computer time and large standard deviations at age 2. Testing for effect modification by gender was performed by adding interaction variables for both gender and television time and gender and sleep. Finally, uni- and multiple logistic regression analysis was performed to examine the longitudinal association between the externalizing and overactive scale of the CBCL/2-3, television time and sleep at age 2 as the exposure variables and an ADHD diagnosis at age 8 to 10 as the outcome variable.
Results
Baseline Characteristics
Of the available 2,834 children from the original KOALA Birth Cohort, 66 were excluded based on exclusion criteria for this study, leaving a total number of 2,768 children. The study flow in Figure 1 shows the available data for the various analyses at the different ages. Baseline characteristics of the total cohort and the subgroups with complete follow-up on parent- and GP reported outcomes are shown in Table 1. Follow-up rates were slightly higher among the families with higher maternal education, non-smoking in pregnancy, and without marital discord, as can be seen from the slight shift between the total cohort and those at follow-up in Table 1. Values for TV time, computer time and total sleep duration were not different in the parent reported ADHD group and the group that was lost to follow-up.
Figure 1.
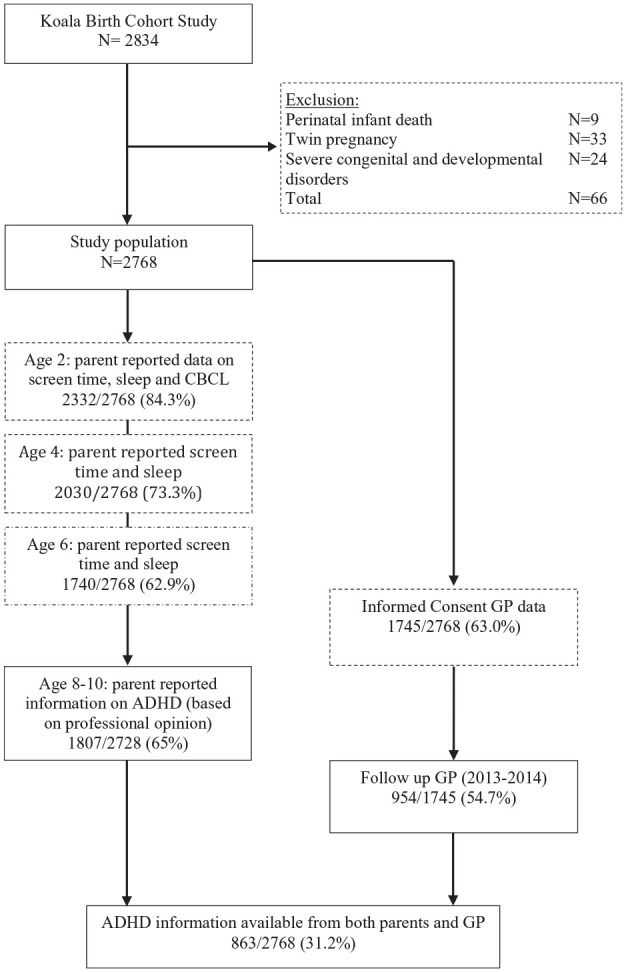
Study flow.
Table 1.
Baseline Characteristics of Maternal, Pre- Peri- and Postnatal Characteristics of the Total Cohort and Follow-Up Subgroups.
| Variable | Total cohort | Follow up parents (8–10 years) | Study cohort with informed consent GP data | Follow up GP (11–13 years) |
|---|---|---|---|---|
| Participants, N (%) | 2,768 (100) | 1,807 (64) | 1,745 (62) | 954 (34) |
| Recruitment group (conventional) N (%) | 2,295 (83) | 1,470 (81.4) | 1,423 (81.5) | 770 (80.7) |
| Maternal education | ||||
| Low | 283 (10.2) | 152 (8.4) | 143 (8.2) | 76 (8.0) |
| Middle | 1040 (37.6) | 665 (36.8) | 672 (35.9) | 328 (34.4) |
| High | 1301 (47.0) | 904 (50) | 898 (51.5) | 512 (53.7) |
| Unknown | 144 (5.2) | 86 (4.8) | 77 (4.4) | 38 (4) |
| Maternal smoking in pregnancy, N (%) | 213 (7.7) | 95 (5.3) | 90 (5.2) | 45 (4.7) |
| Maternal alcohol use in pregnancy, N (%) | 513 (18.5) | 346 (19.1) | 327 (18.7) | 187 (19.6) |
| Gender of child, male N (%) | 1,414 (51.1) | 920 (50.9) | 864 (49.5) | 467 (49.0) |
| Gestational age > 37 weeks, N (%) | 2,688 (97.1) | 1,755 (97.1) | 1,699 (97.4) | 929 (97.4) |
| Birth weight > 2,500 g, N (%) | 2,688 (97.7) | 1,762 (97.5) | 1,707 (97.8) | 932 (97.7) |
| Marital discord, N (%) | ||||
| No | 2,363 (85.4) | 1,621 (89.7) | 1,549 (88.8) | 849 (89) |
| Yes | 220 (7.9) | 135 (7.5) | 142 (8.1) | 76 (8) |
| No partner/unknown | 185 (6.7) | 51 (2.8) | 54 (3.1) | 29 (3) |
| Daily routine of the family 2 years, N (%) | ||||
| (almost) Always | 2,265(81.8) | 1,618 (89.5) | 1,566 (89.7) | 857 (89.8) |
| Seldom or never | 263 (9.5) | 175 (9.7) | 161 (9.2) | 89 (9.3) |
| Missing | 240 (8.7) | 14 (0.8) | 18 (1.0) | 8 (0.8) |
| Television watching, mean minutes/day (SD)* | ||||
| 2 years | 29.4 (25.3) | 28.2 (24.9) | 28.4 (25.1) | 29.1 (25.6) |
| Percentage children who watch TV (age 2) | 92% | 92% | 92% | 92% |
| 4–5 years | 58.3 (33.1) | 57.6 (32.8) | 58.0 (32.8) | 58.3 (32.9) |
| 6–8 years | 67.9 (34.6) | 67.8 (34.5) | 67.9 (34.6) | 68.9 (34.4) |
| Computer games, mean minutes/day (SD)* | ||||
| 2 years | 0.51 (3.4) | 0.51 (3.5) | 0.45 (3.3) | 0.47 (3.3) |
| Percentage children who play computer games (age 2) | 4% | 5% | 4% | 5% |
| 4–5 years | 18.8 (24.7) | 18.2 (24.1) | 18.2 (24.1) | 18.1 (24.0) |
| 6–8 years | 37.1 (27.3) | 36.7 (26.8) | 36.9 (27.1) | 36.7 (27.2) |
| Total sleep duration, mean hours/day (SD) | ||||
| 2 years | 13.3 (1.2) | 13.3 (1.2) | 13.3 (1.2) | 13.3 (1.2) |
| 4–5 years | 11.2 (0.8) | 11.2 (0.8) | 11.2 (0.8) | 11.2 (0.7) |
| 6–8 years | 10.4 (1.5) | 10.4 (1.5) | 10.5 (1.5) | 10.5 (1.6) |
| Playing outside, mean minutes/day (SD) | ||||
| 2 years | 67.6 (39.3) | 66.8 (39) | 66.9 (39.0) | 65.7 (38.4) |
| 4–5 years | 100.4 (42.9) | 100.6 (43.1) | 100.1 (43.0) | 99.6 (41.8) |
| 6–8 years | 107.1 (40.7) | 107.7 (40.7) | 106.8 (40.5) | 107.7 (40.7) |
| CBCL/2-3, mean score overactive scale (SD) † | 0.50 (0.39) | 0.50 (0.38) | 0.50 (0.38) | 0.49 (0.36) |
| CBCL/2-3, mean score externalizing scale (SD) † | 0.44 (0.26) | 0.44 (0.26) | 0.45 (0.25) | 0.44 (0.24) |
| Parent reported ADHD 8–10 years n (%) | 98 (5.4) | 81 (5.3) | 48 (5.6) | |
| GP reported ADHD 9–11 years n (%) | 82 (8.6) | |||
Note. SD = standard deviation; CBCL = Child Behavioral Check List; ADHD = attention-deficit/hyperactivity disorder; GP = general practitioner.
Television watching and computer time measured outside school hours.
Total range of scale is 0 to 2, scales based on items of the Dutch version of the CBCL/2-3 (Koot et al., 1997).
Longitudinal Association Between Screen Time, Sleep Duration, and Parent Reported ADHD
Unadjusted GEE analysis showed a significant association between screen time at the ages of 2, 4 to 5, and 6 to 8 years and parent reported ADHD, which disappeared after adjustment for potential confounders (Table 2). Total sleep duration was unrelated to ADHD in both the unadjusted and the adjusted model. No statistical significance was found when testing for deviation from linearity. Stratification for both recruitment group and gender did not influence the results (conventional group p = 0.5 for screen time and p = 0.9 for sleep; gender only male p = 0.1 for screen time p = 0.8 for sleep). Testing on time interaction was also not significant, indicating no increasing or decreasing trend with age of the strength of the association between screen time or sleep duration with ADHD.
Table 2.
Longitudinal Association Between Screen Time* and Sleep Duration As Repeated Measurements at Age 2, 4, and 6, and Parent Reported ADHD at Age 8 to 9 As the Outcome.
| Variable | Unadjusted |
Adjusted
†
|
||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Screen time (hours/day; age 2, 4, and 6) | 1.4 (1.1–1.7) | 0.004 | 1.1 (0.9–1.4) | .33 |
| Sleep duration (hours/day; age 2, 4, and 6) | 0.9 (0.8–1.1) | 0.22 | 1.0 (0.8–1.1) | .73 |
Note. Odds ratios (OR) with 95% confidence interval (95% CI) from General Estimation Equations logistic regression analysis.
Number of subjects with complete data on screen time and sleep duration at age 2, N = 1,784, age 4 N = 1,647, and age 6 N = 1,603.
Screen time consists of the sum of TV time and computer time outside school hours.
Adjusted for recruitment group, education level of the mother, smoking during pregnancy, alcohol use during pregnancy, gender, gestational age, marital discord 3 months postpartum, and both factors in the table.
Multiple logistic regression analysis with parent reported ADHD as outcome variable showed no independent association with the score on the externalizing scale of the CBCL/2-3 (Table 3). By contrast, a 1-point higher score on the overactive scale of the CBCL/2-3 was associated with a meaningfully higher risk of ADHD at age 8 to 10 (OR 1.8, 95% CI 1.0–3.2); results for screen time and sleep duration were similar as in the GEE model.
Table 3.
Longitudinal Association Between Scores on the CBCL/2-3, Screen Time* and Sleep Duration at Age 2 (and Other Exposures), and Parent Reported ADHD at age 8 to 10 As the Outcome.
| Variable | Unadjusted |
Adjusted
†
|
Adjusted
£
|
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Recruitment group (conventional) | 2.7 (1.3–5.6) | 1.9 (0.9–4.0) | 1.8 (0.8–3.7) |
| Education mother (low) | 5.1 (2.9–8.9) | 3.8 (2.1–7.2) | 3.6 (1.9–6.9) |
| Smoking during pregnancy (yes) | 2.7 (1.4–5.2) | 1.8 (0.9–3.8) | 1.7 (0.8–3.5) |
| Gender (male) | 3.1 (1.9–5.0) | 3.3 (2.0–5.5) | 3.3 (2.0–5.5) |
| Gestational age | 0.9 (0.8–1.0) | 0.9 (0.8–1.1) | 0.9 (0.8–1.1) |
| Marital discord | 1.8 (1.0–3.0) | 1.8 (0.9–3.3) | 1.8 (0.9–3.2) |
| Rhythm in family at age 2 | 0.6 (0.3–0.9) | 0.6 (0.3–1.0) | 0.6 (0.3–1.1) |
| CBCL/2-3 externalizing scale | 3.1 (1.5–6.6) | 1.4 (0.6–3.3) | |
| CBCL/2-3 overactive scale | 2.7 (1.6–4.4) | 1.8 (1.0–3.2) | |
| Screen time (hours/day; age 2) | 1.4 (1.1–1.7) | 1.2 (0.9–1.6) | 1.2 (0.9–1.6) |
| Sleep (hours/day; age 2) | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) | 1.0 (0.8–1.2) |
Note. Odds ratios (OR) and 95% Confidence Intervals (CI) from logistic regression. CBCL Child Behavioral Check List.
Screen time consists of the sum of TV time and computer time outside school hours.
Adjusted for all variables in the model, except for CBCL/2-3 overactive scale.
Adjusted for all variables in the model, except for CBCL/2-3 externalizing scale.
In the GP reported group, both unadjusted and adjusted GEE analysis showed no associations between either screen time or total sleep duration and ADHD (Supplemental Appendix Table B2).
Cross-Sectional Association Between Watching Television, Sleep and the CBCL/2-3 at Age 2
Multiple linear regression analysis showed a significant association between hours of watching TV and the externalizing behavior scale of the CBCL/2-3, but no association with the overactive subscale, as shown in Table 4. A similar result was found for sleep: fewer hours of sleep were only associated with higher scores on the externalizing scale of the CBCL 2/3, but not specifically with the overactive scale. Although statistically significant, effect sizes were small for both screen time and sleep: for example, an increment of 1 h/day of TV watching was associated with a 0.03 higher score on the externalizing scale (scale 0–2, mean 0.44, SD 0.26; effect size = standardized mean difference = 0.03/0.26 = 0.12), and an increment of 1 h/day sleep was associated with 0.02 lower score on the externalizing scale (effect size = 0.08). Furthermore, being male, low education of the mother, no rhythm in family life at age 2 and marital discord showed a significant association with both the externalizing scale and the overactive scale of the CBCL/2-3. No effect modification by the variable gender on watching TV or sleep was found (test for interaction).
Table 4.
Cross-Sectional Association Between TV Time and Sleep Duration (and Other Exposures), and the Mean CBCL/2-3 † Score of the Externalizing Behavior Scale and Overactive Subscale at Age 2 As the Outcome.
| Variable |
CBCL/2-3 externalizing behavior scale
|
CBCL/2-3 overactive subscale
|
||
|---|---|---|---|---|
| Unstandardized B (95% CI) | p | Unstandardized B (95% CI) | p | |
| Watching TV (hours/day) | 0.03 (0.002 to 0.05) | .04 | 0.02 (−0.02 to 0.06) | .3 |
| Sleep (hours/day) | −0.02 (−0.03 to −0.01) | <.001 | −0.01 (−0.23 to 0.002) | .1 |
| Recruitment group (conventional) | 0.01 (−0.02 to 0.04) | .4 | 0.09 (0.04–0.13) | <.001 |
| Maternal education | ||||
| Low | 0.07 (0.03 to 0.1) | .001 | 0.13 (0.07–0.19) | <.001 |
| Middle | 0.05 (0.02 to 0.07) | <.001 | 0.08 (0.05–0.12) | <.001 |
| Smoking during pregnancy | 0.06 (0.02 to 0.1) | .006 | 0.05 (−0.02 to 0.11) | .1 |
| Alcohol use during pregnancy | −0.02 (−0.05 to 0.004) | .09 | −0.03 (−0.07 to 0.01) | .1 |
| Gender (male) | 0.06 (0.04 to 0.08) | <.001 | 0.05 (0.02–0.08) | .005 |
| Gestational age | 0.002 (−0.005 to 0.01) | .6 | −0.02 (−0.01 to 0.01) | .7 |
| Marital discord | 0.07 (0.04 to 0.10) | <.001 | 0.05 (0.001–0.1) | .05 |
| Rhythm in family (yes, age 2) | −0.08 (−0.12 to −0.05) | <.001 | −0.08 (−0.14 to −0.03) | .002 |
| Playing outside (hours/day) | −0.01 (−0.03 to 0.01) | .3 | −0.01 (−0.03 to 0.02) | .5 |
Note. Regression coefficients (B) and 95% confidence intervals (95% CI) from multiple linear regression analysis. N = 2,332; 1,189 males. CBCL = Child Behavior Checklist.
The factor structure of the CBCL/2-3 is based on the article of Koot et al. (1997). This Dutch version of the CBCL 2/3 subdivides behavioral problems at young age in 6 scales (overactive, aggressive, oppositional, anxious, depressed, and sleep problems) and two problem scales (externalizing and internalizing). The externalizing behavior scale consists of the overactive, aggressive and oppositional scales.
Adjusted for all the factors in the table. Constant externalizing scale is 0.6, and for overactive scale 0.67.
Discussion
The current study aimed to examine the longitudinal association between recreational screen time and total sleep duration in early childhood and an ADHD diagnosis at age 8 to 10 years. After correction for possible confounders, no relation between both the amount screen time and total sleep duration at age 2, 4 to 5 and 6 to 8 and a parent reported ADHD diagnosis was found. The absence of this longitudinal association was confirmed in the GP reported ADHD group. By contrast, at the age of 2, both watching television and sleep duration were found to be associated with a higher score of the externalizing scale of the CBCL/2-3.
Screen Time and ADHD
Multiple cross-sectional and longitudinal studies have evaluated the association between TV time, computer time or screen time in general, and symptoms of hyperactivity, inattention, or externalizing behavior (Lingineni et al., 2012; Miller et al., 2007; Ra et al., 2018; Stevens & Mulsow, 2006; Tamana et al., 2019; van Egmond-Fröhlich et al., 2012; Zimmerman et al., 2007). Different from these studies, the current study used an actual ADHD diagnoses instead of ADHD symptoms as outcome variable. In order to diagnose ADHD, a child must meet, in addition to a high score on inattention, hyperactivity, and impulsivity symptoms, also other diagnostic criteria based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Most important, the child must experience serious impairment due to the behavioral symptoms (American Psychiatric Association, 2013). These behavioral symptoms can differ in life due to age, gender or environment (Barkley & Murphy, 2006; Thapar & Cooper, 2016). Most previous studies showed that the environmental factor screen time was associated with increased symptoms of externalizing behavior, hyperactivity, or inattention in healthy preschool and school-aged children (Lingineni et al., 2012; Miller et al., 2007; Ra et al., 2018; Tamana et al., 2019; van Egmond-Fröhlich et al., 2012; Xie et al., 2020; Zimmerman et al., 2007). Our study showed a comparable cross-sectional association between externalizing behavior and time watching TV at the age of 2, but there was no longitudinal relationship between the amount of screen time at a young age and an actual ADHD diagnosis at the age of 8 to 10 years. Finding no association between screen time at age 2, 4 to 5, and 6 to 8 and a professional based parent reported ADHD diagnosis, underlined the importance not to confuse the presence of behavioral symptoms of ADHD with an actual ADHD diagnosis. It showed that the influence of environmental factors like screen time should be considered, when a young child is evaluated because of these ADHD-like symptoms, and stressed the importance of applying all DSM-5 criteria for ADHD when a child is evaluated because of inattention, hyperactivity or impulsivity symptoms. Multiple explanations for this association between externalizing symptoms and screen time could be thought of. Parents may put young children with an overactive temperament in front of the television to get a little bit of rest, as Stevens and colleagues suggested, who also found no meaningful relationship between television exposure at a young age and later symptoms of ADHD (Stevens & Mulsow, 2006). Another explanation may be that watching screens only has a direct effect on behavior; more hours behind screens may result in immediate externalizing behavior or inattention, without long-lasting effects. The positive association at age 2 between more TV time and a higher score on the externalizing scale, could be a result of both of the above explanations. The lack of association between TV time and the overactive subscale of the CBCL/2-3 at age 2 seemed to support this. The 5 items of the overactive subscale are part of the total of 31 items of the externalizing scale of the CBCL/2-3, and overlap with the DSM-5 symptom score for ADHD (American Psychiatric Association, 2013; Koot et al., 1997). This explained the positive association between the overactive subscale of the CBCL/2-3 and an ADHD diagnosis. The externalizing behavioral scale on the other hand, showed no association with an ADHD diagnosis at the age of 8 to 9 years, making it less likely that the externalizing behavioral characteristics were another expression of ADHD.
A recent study of Tamana et al. (2019) showed that in particular a prolonged amount of screen time (including the use of TV, computer, tablet, and mobile phone) was associated with clinically relevant externalizing morbidity and inattention problems (Tamana et al., 2019). Our study did not reveal such a dose effect between hours of screen time early in life and an ADHD diagnosis at the age of 8. The reported amount of screen time in the current study at age 4 to 5 appeared to be only slightly lower than in the study of Tamana et al. (1.3 vs. 1.4 hr/day). However, the total amount of screen time at age 2 was only 30 min in this study, which was much lower than the amount of screen time found in other studies, where screen time or TV time varied between 1.5 and 3.6 hr/day at age 3 (Chaput et al., 2017; Christakis, Zimmerman, et al., 2004; Tamana et al., 2019). Data collection concerning hours of screen time for the current study took place from 2000 to 2009. In 2010 the first touch screen devices were introduced, which could have accounted for an increase in screen time in studies in which data were collected after 2010. Despite the fact that touch screen devices were not yet released when data were collected for this study, the results were useful. Dutch studies showed an enormous increase in medication use for ADHD between 2000 and 2010, the years that data for the KOALA birth cohort were collected (Dutch Health Council, 2014). If this increase in ADHD was linked to an increase in screen time, a positive association would have been found in the current study.
Sleep and ADHD
Total sleep duration also showed no longitudinal association with ADHD. As with screen time, an association between sleep duration and externalizing behavior was found in the analysis at age 2. Cause and effect could not be separated, however. In other words, it was not possible to determine if a child became rebellious due to little sleep, or if externalizing behavior caused decreased sleep time and therefore less sleep duration.
A meta-analysis of subjective and objective studies concerning sleep and ADHD by Cortese et al. (2009), showed many associations between various sleep disturbances and ADHD, but the item “sleep duration” was also not significantly associated with ADHD (Cortese et al., 2009). The authors of this meta-analysis gave as a possible explanation the different interpretation of sleep duration by the parents (e.g., from lights off to wake up time vs. the time a child actually sleeps). Parental perceptions could also have influenced the findings of our study. However, one would expect that if children sleep shorter due to their ADHD problems, parents would notice this over the years (e.g., because children get out of bed), which would become clear with repeated measurements.
Strengths and Limitations
This study has several limitations. Concerning information bias, first, questionnaires that were used measuring both screen time, and sleep were developed specifically for the KOALA study. Screen time and sleep were not measured, but were only parent reported. Especially, the amount of screen time at age 2 was low compared with most other studies (Christakis, Zimmerman, et al., 2004; Tamana et al., 2019). Only few studies which were conducted at the same period as this study, reported on both type and hours of media use. A difference between results shown in this article and other studies, is the country where data were collected, which may be an explanation for the difference in TV time, in addition to the possibility of information bias. Unfortunately, precise data to verify this are missing. Maybe more screen time particularly at this very young age, is associated with ADHD symptoms later in life, as other studies showed (Christakis, Ebel, et al., 2004). In addition, the content of the television and computer programs was not asked. This could have affected study results, as Zimmerman and Christakis (2007) showed that only violent content was associated with attention problems at age 0 to 3 (Zimmerman & Christakis, 2007). It was likely that screen time in our study included violent as well as non-violent content. Second, the ADHD diagnosis was parent reported. Parents where asked whether a doctor, psychologist, or remedial educationalist had ever diagnosed their child with ADHD, but they were not asked in what way this diagnosis was made, and whether this diagnosis fully met DSM-IV-TR criteria (American Psychiatric Association, 2000). Despite the fact that the percentage of children with ADHD and other known relevant factors (like male gender of the child) corresponded with the estimates from the literature, the parent reported group could have given an over- or under estimation of the diagnosis ADHD (Sayal et al., 2018). However, using GP reported ADHD as outcome variable, did not yield differences compared with the results of the analysis with parent reported ADHD as outcome. Only the magnitude of the estimates of the different risk factors was slightly higher in the parent reported group, but also in the GP group no longitudinal association was found between screen time or sleep and ADHD, which supported the results of this study. Selection bias may have occurred due to selective loss-to-follow-up, but the follow-up rates differed only slightly according to baseline characteristics, indicating a limited potential for selection bias.
Finally, a family history of ADHD was not assessed, which might have caused effect modification or confounding. ADHD is both caused by the combined effects of genetic vulnerability and environmental exposures (Faraone et al., 2015; Mill & Petronis, 2008). It is often difficult to separate environmental factors from genetic factors, as genetic studies show that some phenotypes are caused by the same genetic behavioral pathways common to risk-taking propensity, like ADHD and smoking (Strawbridge et al., 2018). Besides that, recent genome-wide-association meta-analysis found genetic correlations between ADHD and phenotypes like education and smoking (Demontis et al., 2019). Known environmental factors that are partly correlated with genetic pathways of ADHD, such as smoking during pregnancy and education level of the mother, were included as confounders in the current study (Faraone et al., 2017; He et al., 2017; Sciberras et al., 2017; Zhu et al., 2014). These factors were indeed associated with both overactive and externalizing symptoms on the CBCL-2/3 at age 2. Only the education level of the mother was associated with an ADHD diagnosis later in the child’s life. Although these factors did not eliminate potential modification of the outcome due to missing data on family history, it is likely that by adjusting for the variables with a known strong correlation with a positive family history, the lack of adjustment for family history was partly corrected for in the analyses.
Conclusion
This birth cohort study showed no longitudinal association between recreational screen time or sleep duration in early childhood and an ADHD diagnosis at age 8. It did find a weak cross-sectional association between time spent watching television, hours of sleep, and higher scores for externalizing behavioral symptoms at the age of 2. Yet, these externalizing behavioral symptoms were not associated with an ADHD diagnosis later in life. The results of the current study showed that it is important to include questions about hours of screen time and sleep when evaluating externalizing, overactive, or inattention symptoms and to include environmental factors into a differential diagnosis before diagnosing ADHD. Furthermore, the study underlines the importance of longitudinal research when examining environmental risk factors for ADHD and other disorders.
Supplemental Material
Supplemental material, Supplementary_material for The Longitudinal Relationship Between Screen Time, Sleep and a Diagnosis of Attention-Deficit/Hyperactivity Disorder in Childhood by Birgit Levelink, Marjolein van der Vlegel, Monique Mommers, Jessica Gubbels, Edward Dompeling, Frans J.M. Feron, Dorothea M.C.B. van Zeben-van der Aa, Petra Hurks and Carel Thijs in Journal of Attention Disorders
Author Biographies
Birgit Levelink is a pediatrician specialised in social pediatrics. She is working as a medical doctor and chief of the social pediatric department at the Maastricht University hospital.
Marjolein van der Vlegel has done her master degree in epidemiology and is currently a PhD student at the Erasmus MC Rotterdam.
Monique Mommers is a biologist and epidemiologist and is appointed as assistant professor at the Department of Epidemiology of Maastricht University. She is a member of the staff of the KOALA team since 2005. Her research focuses around the role of infections and vitamins in asthma development.
Jessica Gubbels is working as a researcher at the Department of Health Promotion of Maastricht University. She is staff member of the KOALA team, and the main focus of her research is to examine environmental influences on dietary intake, physical activity and weight status of young children.
Edward Dompeling is a professor of Paediatrics/Paediatric Respiratory Medicine. The main topic of his professorship is the development of new methods for better diagnosis and monitoring of chronic (lung) diseases in order to achieve better quality of life and prognosis.
Frans Feron is a professor of Social Medicine – in particular Child and Adolescent Health, and head of the department of Social Medicine at Maastricht University. He has a background in medicine (MD) and is officially registered as a medical specialist in Community Health and Social Medicine in the field of Child and Youth Health Care. He holds a PhD in Medicine from Maastricht University, where he completed his dissertation Studies on Neurodevelopmental Issues in Children.
Dorothea M.C.B. van Zeben-van der Aa is a pediatrician, specialised in social pediatrics. She has a had long career in social pediatrics and is recently retiered.
Petra Hurks is an associate professor of neuropsychology and psychopharmacology at the faculty of psychology and neuroscience at the Maastricht University.
Carel Thijs was trained as a medical doctor, epidemiologist and physician in Public Health. He inititiated the KOALA-study and coordinates its many projects and supervises the PhD-fellows and collaborating researchers.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or, publication of this article: this study made use of data collected with financial support of the Netherlands Organisation for Health Research and Development (ZonMw no. 2100.0090); Royal Friesland Foods; Triodos Foundation; Phoenix Foundation; Raphaël Foundation; Iona Foundation; Foundation for the Advancement of Heilpedagogie; Dutch Brain Foundation, and Biobanking and Biomolecular Research Infrastructure Netherlands (BBMRI-nl project RA5) (all in the Netherlands). These organisations were not involved at all in the study design, collection and analysis of data or interpretation of data. They had no influence on the writing process or the decision to submit the paper for publication.
ORCID iDs: Birgit Levelink  https://orcid.org/0000-0001-8238-7031
https://orcid.org/0000-0001-8238-7031
Marjolein van der Vlegel
https://orcid.org/0000-0002-0217-9484
Supplemental Material: Supplemental material for this article is available online.
Reference
- Achenbach M. T., Rescorla L. (2001). Manual for the ASEBA school-age forms & profiles. An integrated system of multi-informant assessment. University of Vermont, Research Center for Children, Youth and Families. [Google Scholar]
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.), text revised ed. (DSM-IV-TR) American Psychiatric Association Publishing. [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.), (DSM-5). American Psychiatric Publishing; . [Google Scholar]
- Barkley R. A., Murphy K. R. (2006). Attention-deficit hyperactivity disorder: A clinical workbook (3rd ed.). Guilford Press. [Google Scholar]
- Ceranoglu T. A. (2018). Inattention to problematic media use habits: Interaction between digital media use and attention-deficit/hyperactivity disorder. Child and Adolescent Psychiatric Clinics of North America, 27(2), 183–191. 10.1016/j.chc.2017.11.009 [DOI] [PubMed] [Google Scholar]
- Chaput J. P., Colley R. C., Aubert S., Carson V., Janssen I., Roberts K. C., Tremblay M. S. (2017). Proportion of preschool-aged children meeting the Canadian 24-Hour Movement Guidelines and associations with adiposity: Results from the Canadian Health Measures Survey. BMC Public Health, 17(Suppl. 5), 829. 10.1186/s12889-017-4854-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christakis D. A., Ebel B. E., Rivara F. P., Zimmerman F. J. (2004). Television, video, and computer game usage in children under 11 years of age. The Journal of Pediatrics, 145(5), 652–656. 10.1016/j.jpeds.2004.06.078 [DOI] [PubMed] [Google Scholar]
- Christakis D. A., Zimmerman F. J., DiGiuseppe D. L., McCarty C. A. (2004). Early television exposure and subsequent attentional problems in children. Pediatrics, 113(4), 708–713. 10.1542/peds.113.4.708 [DOI] [PubMed] [Google Scholar]
- Cortese S., Faraone S. V., Konofal E., Lecendreux M. (2009). Sleep in children with attention-deficit/hyperactivity disorder: Meta-analysis of subjective and objective studies. Journal of the American Academy of Child and Adolescent Psychiatry, 48(9), 894–908. 10.1097/CHI.0b013e3181ac09c9 [DOI] [PubMed] [Google Scholar]
- Demontis D., Walters R. K., Martin J., Mattheisen M., Als T. D., Agerbo E., Team A. R. (2019). Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nature Genetics, 51(1), 63–75. 10.1038/s41588-018-0269-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dutch Health Council, Gezondheidsraad. (2014). ADHD: medicatie en maatschappij [ADHD: medication and society]. http://www.gezondheidsraad.nl/documenten/adviezen/2014/07/03/adhd-medicatie-en-maatschappij
- Faraone S. V., Asherson P., Banaschewski T., Biederman J., Buitelaar J. K., Ramos-Quiroga J. A., Franke B. (2015). Attention-deficit/hyperactivity disorder. Nature Reviews Disease Primers, 1, 15020. 10.1038/nrdp.2015.20 [DOI] [PubMed] [Google Scholar]
- Faraone S. V., Ghirardi L., Kuja-Halkola R., Lichtenstein P., Larsson H. (2017). The familial co-aggregation of attention-deficit/hyperactivity disorder and intellectual disability: A register-based family study. Journal of the American Academy of Child and Adolescent Psychiatry, 56(2), 167–174.e161. 10.1016/j.jaac.2016.11.011 [DOI] [PubMed] [Google Scholar]
- Hale L., Guan S. (2015). Screen time and sleep among school-aged children and adolescents: A systematic literature review. Sleep Medicine Reviews, 21, 50–58. 10.1016/j.smrv.2014.07.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- He Y., Chen J., Zhu L. H., Hua L. L., Ke F. F. (2017). Maternal smoking during pregnancy and ADHD: Results from a systematic review and meta-analysis of prospective cohort studies. Journal of Attention Disorders. 10.1177/1087054717696766 [DOI] [PubMed]
- IBM SPSS Statistics for Windows, version 24, IBM Corp. In. Armonk, N.Y., USA. [Google Scholar]
- Ioannidis K., Hook R., Goudriaan A. E., Vlies S., Fineberg N. A., Grant J. E., Chamberlain S. R. (2019). Cognitive deficits in problematic internet use: Meta-analysis of 40 studies. The British Journal of Psychiatry, 215(5), 639–646. 10.1192/bjp.2019.3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koot H. M., Van Den Oord E. J., Verhulst F. C., Boomsma D. I. (1997). Behavioral and emotional problems in young preschoolers: Cross-cultural testing of the validity of the Child Behavior Checklist/2-3. Journal of Abnormal Child Psychology, 25(3), 183–196. [DOI] [PubMed] [Google Scholar]
- Kummeling I., Thijs C., Penders J., Snijders B. E., Stelma F., Reimerink J., Jansen M. C. (2005). Etiology of atopy in infancy: The KOALA Birth Cohort Study. Pediatric Allergy and Immunology, 16(8), 679–684. [DOI] [PubMed] [Google Scholar]
- Lingineni R. K., Biswas S., Ahmad N., Jackson B. E., Bae S., Singh K. P. (2012). Factors associated with attention deficit/hyperactivity disorder among US children: Results from a national survey. BMC Pediatrics, 12, 50. 10.1186/1471-2431-12-50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loprinzi P. D., Davis R. E. (2016). Secular trends in parent-reported television viewing among children in the United States, 2001-2012. Child Care Health and Development, 42(2), 288–291. 10.1111/cch.12304 [DOI] [PubMed] [Google Scholar]
- Mill J., Petronis A. (2008). Pre- and peri-natal environmental risks for attention-deficit hyperactivity disorder (ADHD): The potential role of epigenetic processes in mediating susceptibility. Journal of Child Psychology and Psychiatry, 49(10), 1020–1030. 10.1111/j.1469-7610.2008.01909.x [DOI] [PubMed] [Google Scholar]
- Miller C. J., Marks D. J., Miller S. R., Berwid O. G., Kera E. C., Santra A., Halperin J. M. (2007). Brief report: Television viewing and risk for attention problems in preschool children. Journal of Pediatric Psychology, 32(4), 448–452. 10.1093/jpepsy/jsl035 [DOI] [PubMed] [Google Scholar]
- Owens J. A., Maxim R., Nobile C., McGuinn M., Msall M. (2000). Parental and self-report of sleep in children with attention-deficit/hyperactivity disorder. Archives of Pediatrics and Adolescent Medicine, 154(6), 549–555. 10.1001/archpedi.154.6.549 [DOI] [PubMed] [Google Scholar]
- Ra C. K., Cho J., Stone M. D., De La Cerda J., Goldenson N. I., Moroney E., Leventhal A. M. (2018). Association of digital media use with subsequent symptoms of attention-deficit/hyperactivity disorder among adolescents. JAMA, 320(3), 255–263. 10.1001/jama.2018.8931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reid Chassiakos Y. L., Radesky J., Christakis D., Moreno M. A., Cross C., Media C. O. C. A. (2016). Children and adolescents and digital media. Pediatrics, 138(5), e20162593. 10.1542/peds.2016-2593 [DOI] [PubMed] [Google Scholar]
- Sayal K., Prasad V., Daley D., Ford T., Coghill D. (2018). ADHD in children and young people: prevalence, care pathways, and service provision. Lancet Psychiatry, 5(2), 175–186. 10.1016/S2215-0366(17)30167-0 [DOI] [PubMed] [Google Scholar]
- Sciberras E., Mulraney M., Silva D., Coghill D. (2017). Prenatal risk factors and the etiology of ADHD-review of existing evidence. Current Psychiatry Reports, 19(1), 1. 10.1007/s11920-017-0753-2 [DOI] [PubMed] [Google Scholar]
- Starcevic V., Khazaal Y. (2017). Relationships between behavioural addictions and psychiatric disorders: What is known and what is yet to be learned? Frontiers in Psychiatry, 8, 53. 10.3389/fpsyt.2017.00053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevens T., Mulsow M. (2006). There is no meaningful relationship between television exposure and symptoms of attention-deficit/hyperactivity disorder. Pediatrics, 117(3), 665–672. 10.1542/peds.2005-0863 [DOI] [PubMed] [Google Scholar]
- Strawbridge R. J., Ward J., Cullen B., Tunbridge E. M., Hartz S., Bierut L., Smith D. J. (2018). Genome-wide analysis of self-reported risk-taking behaviour and cross-disorder genetic correlations in the UK Biobank cohort. Translational Psychiatry, 8(1), 39. 10.1038/s41398-017-0079-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tamana S. K., Ezeugwu V., Chikuma J., Lefebvre D. L., Azad M. B., Moraes T. J., & CHILD Study Investigators. (2019). Screen-time is associated with inattention problems in preschoolers: Results from the CHILD birth cohort study. PLoS One, 14(4), e0213995. 10.1371/journal.pone.0213995 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thapar A., Cooper M. (2016). Attention deficit hyperactivity disorder. Lancet, 387(10024), 1240–1250. 10.1016/S0140-6736(15)00238-X [DOI] [PubMed] [Google Scholar]
- The Lancet Child Adolescent Health. (2018). Growing up in a digital world: Benefits and risks. The Lancet Child and Adolescent Health, 2(2), 79. 10.1016/S2352-4642(18)30002-6 [DOI] [PubMed] [Google Scholar]
- van der Heijden K. B., Stoffelsen R. J., Popma A., Swaab H. (2018). Sleep, chronotype, and sleep hygiene in children with attention-deficit/hyperactivity disorder, autism spectrum disorder, and controls. European Child and Adolescent Psychiatry, 27(1), 99–111. 10.1007/s00787-017-1025-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Egmond-Fröhlich A. W., Weghuber D., de Zwaan M. (2012). Association of symptoms of attention-deficit/hyperactivity disorder with physical activity, media time, and food intake in children and adolescents. PLoS One, 7(11), e49781. 10.1371/journal.pone.0049781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xie G., Deng Q., Cao J., Chang Q. (2020). Digital screen time and its effect on preschoolers’ behavior in China: Results from a cross-sectional study. Italian Journal of Pediatrics, 46(1), 9. 10.1186/s13052-020-0776-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhu J. L., Olsen J., Liew Z., Li J., Niclasen J., Obel C. (2014). Parental smoking during pregnancy and ADHD in children: The Danish national birth cohort. Pediatrics, 134(2), e382–388. 10.1542/peds.2014-0213 [DOI] [PubMed] [Google Scholar]
- Zimmerman F. J., Christakis D. A. (2007). Associations between content types of early media exposure and subsequent attentional problems. Pediatrics, 120(5), 986–992. 10.1542/peds.2006-3322 [DOI] [PubMed] [Google Scholar]
- Zimmerman F. J., Christakis D. A., Meltzoff A. N. (2007). Associations between media viewing and language development in children under age 2 years. The Journal of Pediatrics, 151(4), 364–368. 10.1016/j.jpeds.2007.04.071 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Supplementary_material for The Longitudinal Relationship Between Screen Time, Sleep and a Diagnosis of Attention-Deficit/Hyperactivity Disorder in Childhood by Birgit Levelink, Marjolein van der Vlegel, Monique Mommers, Jessica Gubbels, Edward Dompeling, Frans J.M. Feron, Dorothea M.C.B. van Zeben-van der Aa, Petra Hurks and Carel Thijs in Journal of Attention Disorders