

Abstract
The number of cases of syphilis has increased in the United States and in many high income nations. Otosyphilis is a less recognized complication of syphilis that can lead to irreversible sensorineural hearing loss (SNHL). Different pathophysiological mechanisms have been proposed to explain hearing loss in otosyphilis. We review the literature on otosyphilis in adults and propose the need for future work in this field to identify better ways to diagnose, treat and manage this disease. Patients with syphilis should be screened routinely for hearing loss and all patients with new, sudden, or fluctuating SNHL should be evaluated for syphilis.
Keywords: Syphilis, Otosyphilis, Neurosyphilis, Hearing Loss, Sensorineural hearing loss
Summary:
Otosyphilis is a less recognized complication of syphilis that can lead to irreversible sensorineural hearing loss. We review the literature on otosyphilis to improve awareness and understanding of this disease.
Introduction
Syphilis is a sexually transmitted infection (STI) caused by the organism Treponema pallidum, subspecies pallidum (hereafter T. pallidum). Transmission of this organism is through small breaks in the skin or mucus membranes and is highest in the early stages of disease.1,31s Syphilis infection may cause great morbidity. It can facilitate the transmission of HIV, lead to infant stillbirth in perinatal transmission, and result in uncommon but serious complications such as stroke, blindness and permanent hearing loss1,2,32s. There has been an increase in the number of syphilis cases since the early 2000s in the US and many high-income nations.3,4 Consequently, the incidence of complicated disease has also increased with higher numbers of ocular and congenital syphilis in the last 5 years.4 A recent case series suggests that otosyphilis may also be on the rise.5
Otosyphilis can mimic a variety of audiovestibular conditions.5,6 While sensorineural hearing loss (SNHL) is the main presenting symptom, involvement of the middle ear or ossicles can cause conductive hearing loss.7 Unfortunately, the failure to diagnose otosyphilis in a timely manner can result in permanent and profound hearing loss. We review the literature on otosyphilis in adults and advocate for routine screening for otosyphilis in all patients with a new syphilis diagnosis. We also advocate for a low threshold to test those patients who present with new, sudden, or fluctuating SNHL for syphilis, especially in areas with high prevalence of this disease.
Limitations of previous work
Many reports suffer from imprecision in diagnosis of otosyphilis, primarily because the criteria for inclusion are simply hearing loss in a person with reactive serum treponemal antibody test without identifying those with a history of treated syphilis.8–10, 33s Thus, a person with age or noise related hearing loss and previous treated syphilis could potentially be incorrectly labeled as a case of otosyphilis. Furthermore, reports often do not stage syphilis, routinely evaluate if neurosyphilis is concomitantly present or provide HIV status of patients.9,10 Lumbar punctures (LP) to evaluate for cerebrospinal fluid (CSF) abnormalities are not uniformly done and when CSF is obtained, protein level or white blood cell count (WBC), which are also markers of neurosyphilis, in addition to CSF-Venereal Disease Research Laboratory (VDRL), are not well described.10,33s
There are no randomized controlled trials of otosyphilis treatment, and we are left to rely on case series. Treatment of otosyphilis can be variable even within the same report and often individuals have undergone multiple treatment courses. While most patients are treated according to the CDC 2015 STD Treatment Guidelines1, alternative therapies are sometimes used.9–11,33s There can be a delay in diagnosis when hearing loss is attributed to other audiovestibular conditions and this can influence response to treatment.12,34s,35s Adjunctive steroids are often recommended, although there is variability in the dose and duration.8,10,11,13 Follow up audiograms are often lacking and compromise the interpretation and generalizability of results.5,7,10
In summary, limitations of the literature on otosyphilis include selection bias, misclassification bias and information bias. We take into consideration the limitations of previous work in our review, acknowledging the absence of randomized trials and concentrate on studies we feel most contribute to our understanding of this disease.
Pathophysiology
Early in disease, T. pallidum disseminates throughout the body, including to the central nervous system (CNS).14 It is unclear why some persons develop complications of syphilis and some do not, but host and bacterial factors likely play a role. With respect to the host, neurosyphilis is more common in those with higher serum rapid plasma reagin (RPR) titers and in those with polymorphisms in Toll like receptor genes. Compared to individuals with syphilis who had CSF WBC ≤ 20 cells/ul and nonreactive CSF-VDRL, individuals with WBC > 20/ul or a reactive CSF-VDRL were more likely to have RPR titers 1:32 or greater.15,16 Those with a reactive CSF-VDRL were more likely to have SNPS in TLR1, TLR2 and TLR6 compared to individuals with CSF WBC ≤ 5 cells/ul, nonreactive CSF-VDRL, and no vision or hearing loss.16 Neurosyphilis is also more common in persons living with HIV, and among them, those with CD4 T-cells ≤ 350 cells/ul and not on antiretroviral therapy.16,17 Infection with a unique T. pallidum strain type might increase neurosyphilis risk.18 However, none of these factors have been investigated as risks for otosyphilis.
Hearing loss may develop in congenital or acquired syphilis. Some authors suggest that T. pallidum may affect the 8th cranial nerve within or outside of the CSF space, the cochleovestibular apparatus, or the temporal bone.6,19,20,36s Early in the disease process, spirochetes might directly invade the perilymph of the inner ear, resulting in inflammation confined to the bony labyrinth (Figure 1). If the bacteria are restricted to the cochlea and vestibular system, patients would present with hearing loss and/or vertigo, producing symptoms similar to Meniere’s disease. In these cases, the CSF is usually normal. However, another postulated mechanism begins with treponemal spread through the CSF and the subarachnoid space into the perilymph of the inner ear via the cochlear aqueduct. In this setting, the CSF may be abnormal. Abnormal auditory brainstem responses (ABR) may occur, suggesting dysfunction of the cochlear nerve or upper brainstem pathways.21
Figure 1.
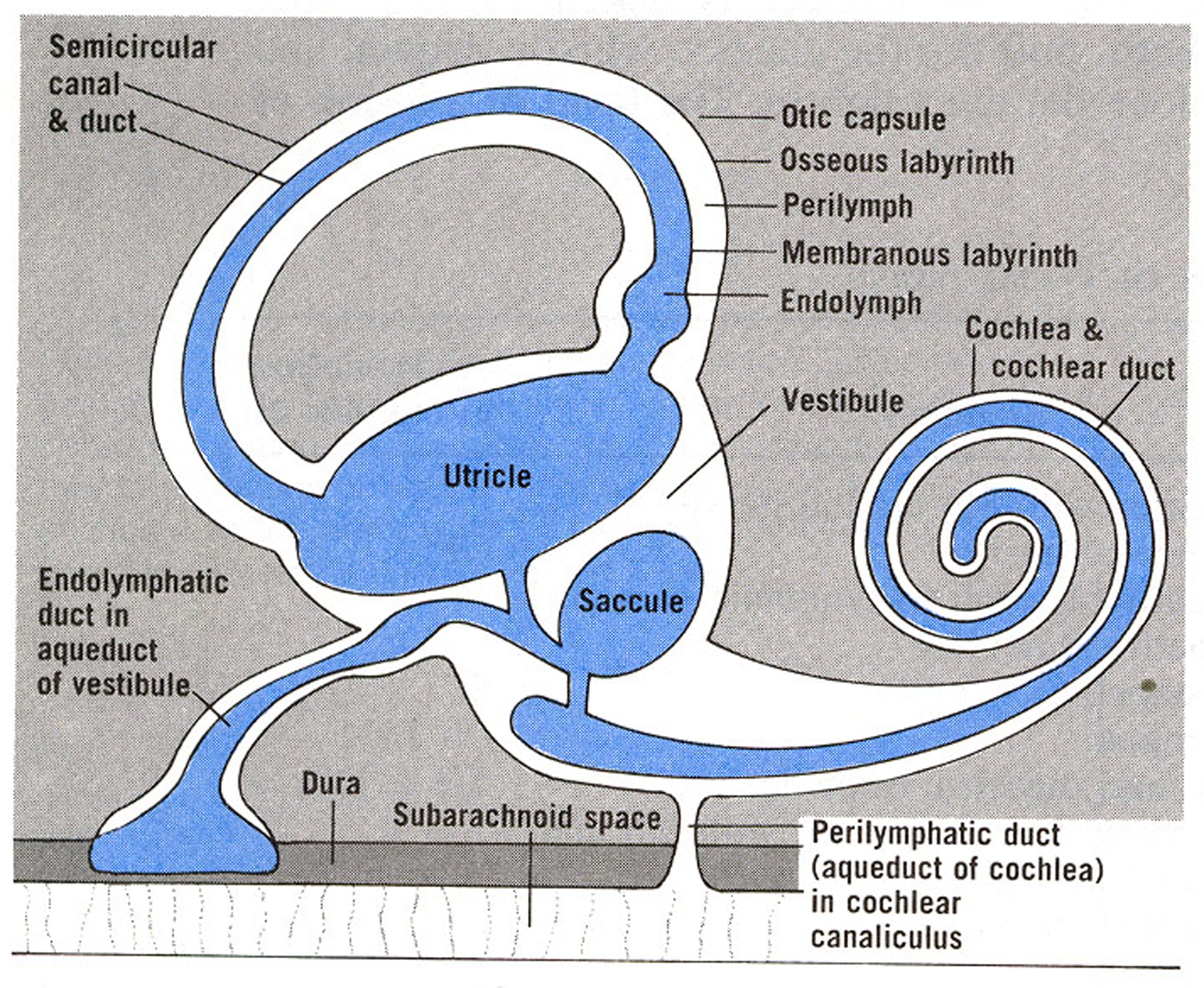
Osseous and membranous labyrinths, showing the basic arrangement and terminology of the internal ear. That the aqueduct of the cochlea communicates with the subarachnoid space is questionable. Taken by permission of the authors from: O’Rahilly, Ronan. Basic Human Anatomy.
In those persons with a history of untreated congenital syphilis or long standing adult infection, osteitis and periostitis of the temporal bone as well as involvement of the ossicles in the middle ear has been noted.6,19,38s Histopathological studies show round cell infiltration with obliterative endarteritis.7,22 This has the potential to compromise the vascular supply leading to bony necrosis of the periosteum.19,38s
The different mechanisms proposed above may result in differences in symptoms, audiometry results, CSF abnormalities, or response to treatment. For example, those patients with inflammation as part of the disease process might be more likely to improve with adjunctive steroid therapy. Therefore, a better understanding of the pathophysiology of hearing loss in individual adult patients with syphilis can help target therapy.
Epidemiology
The 2018 CDC STD Surveillance Report demonstrates a 71% increase in the rate of early syphilis in the US from 2014–2018.4 In 2018, there were >35,000 cases of primary and secondary syphilis cases, 86% of which occurred in men, and primarily in MSM. In parallel, the rate of primary and secondary syphilis among women has also increased in the US, with a 172% increase from 2014–2018. This has led to greater numbers of persons with complicated disease.4,23
Rates of otosyphilis are not nationally reported in the US and there is inconsistency in the number of patients with new syphilis diagnosed with hearing loss reported in the literature. In a series of 289 patients with syphilis seen in the beginning of the penicillin era, hearing abnormalities assessed by audiometry were seen in 102 patients (35%); 17% with early latent, 25% with late latent and 59% of those with neurosyphilis.24 A report of 26 patients with secondary or early latent syphilis who had normal neurological examinations demonstrated abnormal ABRs in 7 individuals (27%).21 On the other hand, a more recent review of 573 patients with syphilis in King County, WA found that only 3.9% complained of hearing loss and 2.7% had tinnitus.23 It is hard to estimate the true incidence or prevalence of hearing loss or vestibular symptoms in patients presenting with syphilis in the current era. New case definitions in the CDC 2018 STD Surveillance Report will help to monitor rates of this disease in the US in coming years.4
Symptoms and Signs
Like ocular and neurosyphilis, otosyphilis can occur at any stage of the disease, and patients with syphilis should be routinely evaluated for otologic symptoms.5,13,23,24,40s Symptoms might include hearing loss, tinnitus or vestibular abnormalities such as vertigo, imbalance or gait instability. In a recent study evaluating a large cohort of 85 individuals with syphilis, 90% of patients with otosyphilis had hearing loss, 73% had tinnitus and 53% had vertigo.10 However, 11% of these individuals had a nonreactive VDRL suggesting they did not have active syphilis at the time of the study. The symptoms of otosyphilis often overlap in the same person, and up to 96% of individuals with abnormal vestibular responses may also have hearing loss.24 Signs of meningitis or ocular manifestations may also be seen in individuals with otosyphilis20,25 and spontaneous and positional nystagmus has been reported.13 Tinnitus or vertigo often resemble Meniere’s disease or other vestibular disorders, and hearing loss due to syphilis can be confused with acoustic neuroma, autoimmune hearing loss, stroke or other otologic processes.
As a general rule, otosyphilis in adults causes SNHL5,8,10 although conductive hearing loss may be present in those with longstanding disease.6,7 Hearing loss can be unilateral or bilateral, often with sudden onset and rapid progression and those patients who report unilateral impairment may have bilateral disease on audiogram.5,12,13,25 Bilateral hearing loss may be symmetric or asymmetric and can present in a variety of ways: mild or moderate and low to high frequency with poor or excellent speech discrimination scores.5,12 There is not one classic type of presentation. In recent case series, the median time between symptom onset to treatment was roughly 1–2 months but can range from a few days to years;5,25,40s it is not clearly reported in many studies.
CSF abnormalities can occur, especially with concomitant neurosyphilis, although we do not know the true proportion of those with otosyphilis who have CSF abnormalities. Among individuals living with HIV and referred for a LP due to concern for neurosyphilis, the odds of a reactive CSF-VDRL were 3 times higher in those with moderate or greater severity symptoms of hearing loss compared to those with no or mild hearing loss.26 In the analysis of 85 patients with syphilis and hearing abnormalities cited above, only 5.4% of individuals had concomitant CSF changes. However, as in most studies, CSF evaluation was not uniformly performed, involving <50% of participants.10 It is possible that a greater number of individuals with otosyphilis have neurosyphilis as small case reports of <20 patients suggest ~50% of patients with otosyphilis have abnormal CSF, and 6 out of 7 patients (86%) with an abnormal ABR pattern had abnormal CSF.5,21,40s
Diagnosis
The clinical manifestations of otosyphilis may mimic other causes of hearing loss and therefore diagnosis of this disease rests on audiological abnormalities in patients with current syphilis and exclusion of other diagnoses. The evaluation of new syphilis requires both treponemal and nontreponemal serologic testing with evaluation of past nontreponemal serologic titers in those with a history of treated disease. Thus, the diagnosis of otosyphilis can be difficult to establish and requires collaboration between public health and infectious diseases specialists, as well as otolaryngologists.
Diagnosis of syphilis
A detailed discussion of syphilis diagnosis is beyond the scope of this review, and the reader is referred to the CDC 2015 STD Treatment Guidelines.1 Briefly, some laboratories and clinics adhere to the traditional syphilis screening algorithm and others follow the reverse screening algorithm, both of which are acceptable methods to establish a serologic cure of syphilis. Once a patient is appropriately treated, the definition of cure includes a 4-fold drop or reversion to nonreactive in nontreponemal serologic titers up to 12 months after treatment for primary, secondary, or early latent syphilis and 24 months for late latent disease. Some patients have a serofast antibody response, in which there is a history of prior treated disease with persistently reactive nontreponemal tests despite demonstrating an adequate fourfold decline in titers. With reinfection, there is an increase in nontreponemal titers by at least fourfold.
Audiology
In a patient with syphilis who presents with tinnitus, hearing loss or vestibular symptoms, the recommended workup includes prompt formal audiologic testing and evaluation by otolaryngology.27 Those with sudden SNHL should be evaluated with an MRI or ABR to rule out other retrocochlear pathology.27 As noted above, patients can have bilateral involvement on audiologic assessment even if only unilateral symptoms, indicating formal audiogram is an important part of the diagnosis and management.
Cerebrospinal fluid
The CDC recommends that all patients with otosyphilis undergo a LP to establish whether there are concomitant CSF abnormalities.1 If CSF abnormalities are present at diagnosis, these can be followed to confirm treatment response. However coordinating the LP should not delay initiating treatment, and some argue that if neurosyphilis treatment will be given regardless of CSF findings, the utility of LP is unproven. Otosyphilis should be treated in the same way as neurosyphilis, regardless of whether CSF is abnormal. However, if the CSF profile is consistent with neurosyphilis (pleocytosis, elevated protein for those without HIV or reactive CSF-VDRL), the diagnosis of otosyphilis is supported.
Other methods to diagnose otosyphilis
There are limited data regarding the utility of methods other than audiology to diagnose otosyphilis. A case report of one patient advocated the use of otoacoustic emissions to measure cochlear function and to follow treatment response.28 Pathological ABR patterns21 or portable screening audiometry (personal communication, Dr. Christina Marra) may be useful to identify otosyphilis. A serum panel at the time of otolaryngology evaluation is warranted to rule out genetic, autoimmune and other infectious diseases associated with sudden SNHL. Other differential diagnosis might include viral cochleitis or neuritis such as those caused by herpesviruses or HIV, bacterial meningitis, ototoxic drugs such as aminoglycosides and vancomycin, trauma, cerebrovascular accident, autoimmune inner ear disease, Cogan’s syndrome, Sarcoidosis and neoplastic conditions such as acoustic neuroma, vestibular schwannomas or carcinomatous meningitis.27, 37s
Neuroimaging
The utility of imaging studies in establishing or supporting a diagnosis of otosyphilis is controversial. Several case reports of patients with long standing disease describe the use of computed tomography (CT) imaging to demonstrate temporal bone changes, notably around the cochlea, vestibule and semicircular canals, suggestive of osteomyelitis.6,19,38s However, similar abnormalities can be seen in unrelated disorders, such as otosclerosis, osteogenesis imperfecta and fibrous dysplasia. These reports suggest that CT imaging might be helpful late in disease when bone manifestations occur, but less useful in early disease.
Magnetic resonance imaging (MRI) of the brain has not been routinely used in the diagnosis of otosyphilis.27 Gadolinium enhancement of the inner ear and the vestibulocochlear nerve and meningeal enhancement can be suggestive of inflammation or infection,29,39s,40s but a normal MRI has also been reported in some individuals as well.12,35s While imaging differences may be related to different pathophysiological mechanisms of otosyphilis, how soon patients are presenting to care and the anatomical location of inflammation, MRI or other neuroimaging techniques are not routinely done and we do not know if it could be helpful in the diagnosis of this disease.
Treatment
Patients with otosyphilis should be treated with the same therapy that is recommended for neurosyphilis:1 intramuscular (IM) aqueous procaine penicillin (APPG) with oral probenecid or intravenous (IV) aqueous crystalline penicillin G (PenG). There are few STD clinics in the US treating patients with neurosyphilis with APPG (personal communication) despite similar outcomes with PenG.30 PenG is time, labor and cost intensive, often requiring inpatient hospitalization or the use of a peripherally inserted central catheter to provide antibiotics as an outpatient. These options might be difficult to coordinate in rural areas where access to specialists and hospitals are scarce, and they can be associated with adverse effects such as catheter related upper extremity venous thrombosis. Some clinicians recommend the use of additional benzathine penicillin G (BPG) 2.4 million units IM weekly for up to 3 weeks after the completion of recommended otosyphilis treatment, however this is not routinely prescribed or recommended.1,40s
A few case series suggest alternative agents to treat adults with otosyphilis. Examples include BPG IM every week for three months;8 BPG IM weekly × 3 weeks for those who don’t have CSF abnormalities;10 or Ampicillin 1.5 grams orally four times daily for four weeks.11 Ceftriaxone (IM or IV) has been suggested as one possible treatment option with limited data in 2 patients who had minimal improvement in tinnitus or hearing defects.12,39s Oral doxycycline 400 mg/day for 21 days has been advocated as treatment for otosyphilis, but it is not clear if hearing loss was due to syphilis vs another etiology in this small case report of 19 patients.9 Imprecision in the diagnosis of syphilis and otosyphilis, lack of a control group, small patient numbers, treatment initiated years after symptoms started, or high rate of loss to follow up for many studies make treatment outcomes difficult to interpret. Therefore, the recommended treatment for adults with otosyphilis is penicillin, either APPG or PenG according to the CDC 2015 STD Treatment Guidelines.1
The use of adjunctive corticosteroids for otosyphilis is often advocated to help reduce inflammation and prevent a Jarisch-Herxheimer reaction with worsening of audiologic symptoms.8,13,20 Typical steroid regimens are prednisone or prednisolone 0.5–1 mg/kg/day orally or IV tapered over 1–2 months, although many case reports do not provide details on the dose and type of steroid used and vary in the treatment length or taper pattern.13,20,40s Prolonged treatment with long term or maintenance oral steroid therapy for 2–3 months, such as prednisone at 5 mg daily, twice a day or every other day has been used in otosyphilis, especially if hearing changes do not improve after antibiotics and a short course of steroids.8,20,41s Besides steroids, adjunctive therapy with oral pentoxifillin 900 mg daily for 2–3 weeks in 2 patients has been suggested to improve hearing.13 Overall, response to adjunctive treatment is difficult to assess because of differences in timing of treatment, dose of adjunctive therapy as well as type and duration of penicillin administered.
Prognosis
While patients may have improvement in hearing after otosyphilis treatment, some do not return to baseline, and it is unclear if hearing deficits persist due to delay in time to treatment, inadequate treatment, irreversible damage or diagnostic imprecision. A recent case series of 7 patients suggest ~40% of patients have improved or stabilized hearing with treatment.25 Patients with longer duration of hearing loss due to syphilis are less likely to respond to treatment and are more likely to have progression of disease.12,34s,35s It is possible that, in late disease, the cochleovestibular system may be irreversibly damaged, arguing for identification of patients with otosyphilis as early in the disease course as possible.
Conclusion
It is important for health care professionals realize that syphilis is still with us and the incidence of otosyphilis in adults may increase in coming years as we see syphilis rates continue to climb upwards. Otosyphilis is one of the few forms of SNHL that can improve with antibiotic treatment, and it is potentially curable. Therefore, routine screening for otosyphilis, such as asking patients about hearing loss, tinnitus or gait imbalance, should be integrated into the work up for a new diagnosis of syphilis regardless of syphilis stage. Missing a diagnosis of otosyphilis has prognostic implications that can lead to irreversible hearing loss. Awareness of otosyphilis needs to be increased health care settings where individuals with otosyphilis may receive care, such as public health, sexual health, otolaryngology, and HIV clinics.
Supplementary Material
Acknowledgments:
We would like to thank Dr. Julie Dombrowski for reviewing the manuscript. We would also like to thank the site editor for the online version of Basic Human Anatomy, Dr. Rand Swenson for permission to use the figure.
Sources of Funding:
Dr. Christina Marra reports grants from the National Institutes of Health [grant number R01 NS082120 and R01 NS034235]. For the remaining authors, none were declared.
Footnotes
Conflicts of Interest: No conflicts of interest are reported by the authors.
References
- 1.Centers for Disease Control Prevention. Sexually Transmitted Diseases Treatment Guidelines. Available from: https://www.cdc.gov/std/treatment/default.htm.
- 2.Wasserheit J Epidemiologic synergy: interrelationships between human immunodeficiency virus infection and other sexually transmitted diseases. Sex Transm Dis 1992;19:61–77. [PubMed] [Google Scholar]
- 3.European Centre for Disease Prevention and Control. Syphilis and congenital syphilis in Europe. A review of epidemiological trends (2007–2018) and options for response. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/Syphilis-and-congenital-syphilis-in-Europe.pdf.
- 4.Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2018. Atlanta: U.S. Department of Health and Human Services; 2019. DOI: 10.15620/cdc.79370. [DOI] [Google Scholar]
- 5.Theeuwen H, Whipple M, Litvack JR. Otosyphilis: Resurgence of an Old Disease. The Laryngoscope 2018. [DOI] [PubMed] [Google Scholar]
- 6.Ogungbemi A, Dudau C, Morley S, et al. Computed tomography features of luetic osteitis (otosyphilis) of the temporal bone. J Laryngol Otol 2014;128:185–8. [DOI] [PubMed] [Google Scholar]
- 7.Karmody CS, Schuknecht HF. Deafness in congenital syphilis. Arch Otolaryngol 1966;83:18–27. [DOI] [PubMed] [Google Scholar]
- 8.Zoller M, Wilson WR, Nadol JB Jr. Treatment of syphilitic hearing loss. Combined penicillin and steroid therapy in 29 patients. Ann Otol Rhinol Laryngol 1979;88:160–5. [DOI] [PubMed] [Google Scholar]
- 9.Chotmongkol V, Sawanyawisuth K, Yimtae K, et al. Doxycycline treatment of otosyphilis with hearing loss. Sex Transm Infect 2012;88:177–8. [DOI] [PubMed] [Google Scholar]
- 10.Yimtae K, Srirompotong S, Lertsukprasert K. Otosyphilis: a review of 85 cases. Otolaryngol Head Neck Surg 2007;136:67–71. [DOI] [PubMed] [Google Scholar]
- 11.Chan YM, Adams DA, Kerr AG. Syphilitic labyrinthitis--an update. J Laryngol Otol 1995;109:719–25. [DOI] [PubMed] [Google Scholar]
- 12.de Goffau MJ, Doelman JC, van Rijswijk JB. Unilateral sudden hearing loss due to otosyphilis. Clin Pract 2011;1:e133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Klemm E, Wollina U. Otosyphilis: report on six cases. J Eur Acad Dermatol Venereol 2004;18:429–34. [DOI] [PubMed] [Google Scholar]
- 14.Lukehart SA, Hook EW 3rd, Baker-Zander SA, et al. Invasion of the central nervous system by Treponema pallidum: implications for diagnosis and treatment. Ann Intern Med 1988;109:855–62. [DOI] [PubMed] [Google Scholar]
- 15.Marra CM, Maxwell CL, Smith SL, et al. Cerebrospinal fluid abnormalities in patients with syphilis: association with clinical and laboratory features. J Infect Dis 2004;189:369–76. [DOI] [PubMed] [Google Scholar]
- 16.Marra CM, Sahi SK, Tantalo LC, et al. Toll-like receptor polymorphisms are associated with increased neurosyphilis risk. Sex Transm Dis 2014;41:440–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ghanem KG, Moore RD, Rompalo AM, et al. Neurosyphilis in a clinical cohort of HIV-1-infected patients. AIDS 2008;22:1145–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Marra C, Sahi S, Tantalo L, et al. Enhanced molecular typing of treponema pallidum: geographical distribution of strain types and association with neurosyphilis. J Infect Dis 2010;202:1380–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kivekas I, Vasama JP, Hakomaki J. Bilateral temporal bone otosyphilis. Otol Neurotol 2014;35:e90–1. [DOI] [PubMed] [Google Scholar]
- 20.Vercoe GS. The effect of early syphilis on the inner ear and auditory nerves. J Laryngol Otol 1976;90:853–61. [DOI] [PubMed] [Google Scholar]
- 21.Lowhagen GB, Rosenhall U, Andersson M, et al. Central nervous system involvement in early syphilis. Part II. Correlation between auditory brain stem responses (ABR) and cerebrospinal fluid abnormalities. Acta dermato-venereologica 1983;63:530–5. [PubMed] [Google Scholar]
- 22.Miller ME, Makary C, Lopez IA, et al. Endolymphatic hydrops in otologic syphilis: a temporal bone study. Otol Neurotol 2010;31:681–6. [DOI] [PubMed] [Google Scholar]
- 23.Dombrowski JC, Pedersen R, Marra CM, et al. Prevalence Estimates of Complicated Syphilis. Sex Transm Dis 2015;42:702–4. [DOI] [PubMed] [Google Scholar]
- 24.Ittkin P, Tamari MJ. Studies of syphilis on the ear and penicillin. Am J Med Sci 1953;225:427–45. [PubMed] [Google Scholar]
- 25.Bradshaw D, Pallawela S, Nelson M, et al. Otosyphilis: missed opportunities for early treatment? Sex Transm Infect 2012;88:573. [DOI] [PubMed] [Google Scholar]
- 26.Davis AP, Stern J, Tantalo L, et al. How Well Do Neurologic Symptoms Identify Individuals With Neurosyphilis? Clin Infect Dis 2018;66:363–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chandrasekhar SS, Tsai Do BS, Schwartz SR, et al. Clinical Practice Guideline: Sudden Hearing Loss (Update). Otolaryngol Head Neck Surg 2019;161:S1–S45. [DOI] [PubMed] [Google Scholar]
- 28.Chun RH, Pinto JM, Blankenhorn R, et al. Recovery of otoacoustic emission function in luetic endolymphatic hydrops: a possible measure of improvement in cochlear function. Int J Otolaryngol 2009;2009:942096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Weder S, Senn P, Caversaccio M, et al. Cochleovestibular Deficit as First Manifestation of Syphilis in a HIV-Infected Patient. Case Rep Neurol 2013;5:62–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dunaway SB, Maxwell CL, Tantalo LC, et al. Neurosyphilis Treatment Outcomes After Intravenous Penicillin G versus Intramuscular Procaine Penicillin Plus Oral Probenecid. Clin Infect Dis 2019; doi: 10.1093/cid/ciz795. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.