

Abstract
Introduction
Thalassemia is a genetically diverse group of disease which occurs due to an imbalance in the production of the alpha and beta chains with ensuring chronic hemolysis, ineffective erythropoiesis, and iron overload.
Aim and objective
The main aim of the study is to compare the salivary flow rate, pH, buffer capacity, total antioxidant capacity, and ferritin levels in children with beta thalassemia major and healthy children.
Materials and methods
The present study includes 40 children consisting of 20 beta thalassemia major and 20 healthy children. Unstimulated saliva was collected by the spitting method. The salivary flow rate, pH, buffer capacity, total antioxidant capacity, and ferritin levels were evaluated.
Results
Salivary ferritin levels were found to be higher in children with beta thalassemia major.
Conclusion
Iron overload is also known as hemochromatosis which is one of the complications of thalassemia.
How to cite this article
Rao GV, Preethi V, Daneswari V, et al. A Comparative Study of Salivary Flow Rate, pH, Buffer Capacity, Total Antioxidant Capacity, and Ferritin Levels in Children with Beta Thalassemia Major and Healthy Children. Int J Clin Pediatr Dent 2021;14(3):342-348.
Keywords: Beta thalassemia major, Buffering capacity, Ferritin levels, pH, Salivary flow rate, Total antioxidant capacity
Introduction
Thalassemia are a group of inherited hematological defects in the synthesis of either alpha or beta polypeptide chains of the globulin portion of the hemoglobin molecule and therefore referred to as alpha or beta type.
Thalassemia was first described by two American pediatricians Thomas B Cooley and Pearl Lee. The term thalassemia was coined by George Whipple. Thalassemia roughly translates to “Anemia of the sea” signifying the fact that patients were of Mediterranean origin.1,2
Insight into pathophysiology when Sir David Weatherall and Dr John Clegg and their colleagues were able to isolate and separate the thalassemic globulin chains. They deduced that the culprit was an imbalance in chain synthesis.3 Beta thalassemia is a defect in the synthesis of the beta chain of the hemoglobin leading to an imbalance in the alpha and beta ratio in the red blood cells.4
The distribution of thalassemia worldwide, nearly 15 million people are expected to suffer from thalassemia disorders. The gravity of situation in India, nearly 12,000 infants are born every year with hemoglobinopathy. On average, 1 in every 25 Indians is a carrier of thalassemia. The lack of an easy diagnostic test and its similarity to iron deficiency anemia makes thalassemia one of the most confusing hemoglobinopathies. Whereas both thalassemia and iron deficiency anemia are characterized by microcytic hypochromic anemia, the remedy of iron deficiency anemia lies in iron supplementation, but iron supplementation does not correct the anemia due to thalassemia.5
Saliva offers an alternate to serum as a biologic fluid that can be analyzed for diagnostic purposes. Whole saliva contains locally produced as well as serum derived markers that are useful in the diagnosis of a variety of systemic disorders.6
As there is sparse literature highlighting the salivary ferritin levels in children with beta thalassemia major the purpose of the present study was to compare and evaluate salivary flow rate, pH, buffer capacity, total antioxidant capacity, and ferritin levels in beta thalassemia major with healthy children.
Patients and Methods
The present study was conducted in the Department of Pedodontics and Preventive Dentistry, Mamata Dental College, Khammam, Telangana in association with Sankalpa Voluntary Organization for thalassemic children, Khammam, Telangana. Ethical clearance was obtained from the ethical review committee and Institutional Review Board of Mamata Dental College and Hospital (MDC-R-088244). After explaining the purpose and the procedure of this study to both parents and children, a written consent from the children who were interested in this study were only evaluated.
Inclusion Criteria7
Age-group between 5 and 10 years.
Only those patients who were diagnosed previously for beta thalassemia major were considered.
Matching of age, sex of thalassemia and healthy children.
Exclusion Criteria
Those already undergoing dental treatment.
Those suffering from other diseases known to influence the salivary parameters such as diabetes and CHDs.
The study design consists of 40 children, 20 beta thalassemia major and 20 healthy children. An intraoral examination was conducted by single qualified examiner using sterile set of diagnostic instruments. Unstimulated saliva was collected by the spitting method for biochemical analysis (Fig. 1).8
Fig. 1.

Spitting method
Collection of Saliva Samples
Unstimulated saliva is collected by the spitting method.8 To ensure standardization of samples and minimize the effect of diurnal variation, the saliva collection was carried out at the same time of the day between 9 am and 11 am on a routine basis (Fig. 2). Prior information was provided to the subjects to refrain from eating and drinking at least 60 minutes before the collection.
Fig. 2.

Salivary buffer capacity kit
Salivary samples were collected in a pre-weighed graduated cylinder and the flow rate was calculated immediately (Fig. 3). pH and buffer capacity were measured by saliva check buffer kit (Fig. 2). Total antioxidant capacity is measured by the phosphomolybdenum method (Fig. 4) and calorimeter (Fig. 5).9 Ferritin levels were analyzed by semi-auto-analyzer (Fig. 6).
Fig. 3.
Flow rate
Fig. 4.
Antioxidant capacity (Phosphomolymbenum method)
Fig. 5.
Calorimeter
Fig. 6.
Semi auto analyser
Results
The results of the salivary flow rate, pH, buffer capacity, total antioxidant capacity, and ferritin levels in beta thalassemia major and healthy children were subjected to statistical analysis using IBM SPSS statistics 20.0. Descriptive statistics and Mann-Whitney test were performed (Tables 1 to 5).
Table 1.
Comparison of flow rate (FR) between thalassemia and healthy groups
| Variables | Thalassemia | Healthy | Mann-Whitney | p value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Min | Max | Mean | SD | U | ||
| FR | 0.37 | 1.09 | 0.72 | 0.24 | 0.90 | 2.40 | 1.66 | 0.64 | 0.00 | <0.001 |
SD, standard deviation; p, probability
Table 5.
Comparison of ferritin levels (FL) between thalassemia and healthy groups
| Variables | Thalassemia | Healthy | Mann-Whitney | p value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Min | Max | Mean | SD | U | ||
| FL | 371.4 | 421.9 | 396.04 | 7.56 | 268.0 | 319.3 | 293.56 | 14.7 | 16.12 | <0.001 |
SD, standard deviation; p, probability
The mean difference between both the groups was proved to be statistically significant for salivary flow rate, pH, buffering capacity, antioxidant capacity and ferritin levels. Table 6 and Figure 7 show overall comparison of sialochemistry of saliva where ferritin levels were found to be higher in thalassemia children (396.4) when compared to healthy children (293.56).
Table 6.
Comparison of all variables between two groups
| Variables | Thalassemia | Healthy | Mann-Whitney | p value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Min | Max | Mean | SD | U | ||
| FR | 0.37 | 1.09 | 0.72 | 0.24 | 0.90 | 2.40 | 1.66 | 0.64 | 0.00 | <0.001 |
| PH | 6.20 | 6.60 | 6.42 | 0.17 | 5.50 | 8.5 | 7.00 | 0.13 | 20.00 | <0.001 |
| BC | 3.60 | 6.40 | 5.1 | 1.07 | 9.80 | 12.00 | 10.85 | 0.93 | 0.00 | <0.001 |
| TAC | 76.0 | 99.8 | 87.63 | 7.56 | 69.2 | 151.7 | 110.33 | 35.2 | 0.00 | <0.001 |
| FL | 371.4 | 421.9 | 396.04 | 7.56 | 268.0 | 319.3 | 293.56 | 14.7 | 16.12 | <0.001 |
FR, flow rate; BC, buffer capacity; TAC, total anti oxidant capacity; FL, ferritin levels
SD, standard deviation; p, probability
Fig. 7.
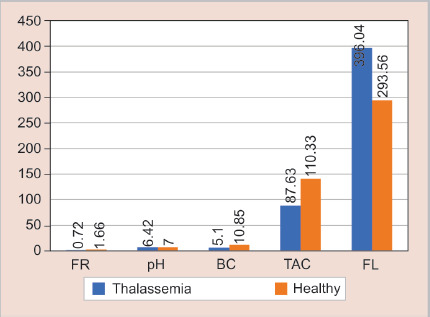
Comparison of all variables between two groups; FR, flow rate; BC, buffer capacity; TAC, total antioxidant capacity; FL, ferritin levels
Discussion
Concentrations of biochemical components in saliva play an important role in oral diseases. The present study salivary flow rate, pH, and buffer capacity were significantly lower among the thalassemia children when compared with that of healthy children, which was in accordance with the previous study conducted by Kuriakose et al.,10 it could be because of increased serum levels of ferritin deposited in salivary glands resulting in inflammatory changes.
As fewer reported studies were assessing the total antioxidant capacity and salivary ferritin levels, the present study focuses mainly on these parameters. Human saliva contains a complex peroxidase system, the major components of which include different forms of lactoperoxidase secreted by salivary glands and myeloperoxidase from polymorphonuclear neutrophils. Cells and biological fluids have an array of protective antioxidant mechanisms, both for preventing the production of free radicals and for repairing oxidative damage. Antioxidant systems include enzymes such as superoxide dismutase, catalase, and glutathione peroxidase, macromolecules such as albumin, ceruloplasmin and ferritin, and an array of small molecules including ascorbic acid, alpha-tocopherol, beta-carotene reduced glutathione uric acid and bilirubin. The sum of endogenous and food-derived antioxidant represent the total antioxidant capacity of the system.11
The total antioxidant levels in thalassemic children are decreased when compared to normal healthy children which were in accordance to Salih et al.12 The unique feature of thalassemia is a defective synthesis of either alpha or beta chain of globulin portion which fails to bounds to iron resulting in the reduced oxygencarrying capacity to the tissues. As a compensatory mechanism ineffective erythropoiesis is initiated in the bone marrow resulting in overproduction of erythroblasts leading to excessive iron load in the serum.
As a part of normal cellular respiration of body tissues, hydrogen peroxide is liberated as a by-product of the mitochondrial oxidative respiratory process results in liberation of OH− (free radicals) as explained by Fenton's reaction.13

These free radicals react with the antioxidant reserves present in the body resulting to reduce oxidative stress (ROS) that leads to vascular tissue damage.
In the present study, salivary ferritin levels were increased in thalassemia children when compared with healthy children which could be due to defective alpha/beta globulin synthesis, ineffective erythropoiesis, and increased peripheral hemolysis of RBC. The qualitative ferritin levels present in saliva are derived from the local vasculature surrounding the salivary glands by passive diffusion or ultrafiltration from the serum. From the acinar and ductal cells, the ferritin reaches the oral cavity.5
Table 2.
Comparison of pH between thalassemia and healthy groups
| Variables | Thalassemia | Healthy | Mann-Whitney | p value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Min | Max | Mean | SD | U | ||
| PH | 6.20 | 6.60 | 6.42 | 0.17 | 5.50 | 8.50 | 7.00 | 0.13 | 20.00 | <0.001 |
SD, standard deviation; p, probability
Table 3.
Comparison of buffering capacity (BC) between thalassemia and healthy groups
| Variables | Thalassemia | Healthy | Mann-Whitney | p value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Min | Max | Mean | SD | U | ||
| BC | 3.60 | 6.40 | 5.1 | 1.07 | 9.00 | 12.00 | 10.85 | 0.93 | 0.00 | <0.001 |
SD, standard deviation; p, probability
Table 4.
Comparison of total antioxidant capacity (TAC) between thalassemia and healthy groups
| Variables | Thalassemia | Healthy | Mann-Whitney | p value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Min | Max | Mean | SD | U | ||
| TAC | 76.0 | 99.8 | 87.63 | 7.56 | 69.2 | 151.7 | 110.33 | 35.2 | 0.00 | <0.001 |
SD, standard deviation; p, probability
Qualitative changes in the salivary composition representing the concentration of biochemical components place an important role in the diagnosis of certain systemic conditions. Thus, saliva can be auxiliary means of non-invasive diagnostic tool for the screening of larger populations.
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Maakaron JE, Cappellini MD, Taher AT. An update on thalassemia intermedia. J Med Liban. 2013;61(3):175–182. doi: 10.12816/0001447. [DOI] [PubMed] [Google Scholar]
- 2.Whipple GH, Bradford WL. Mediterranean disease - “thalassemia” [erythroblastic anaemia of cooley]; associated pigment abnormalities simulating hemochromatosis. J Pediatr. 1936;9(3):279–311. doi: 10.1016/S0022-3476(36)80021-3. [DOI] [Google Scholar]
- 3.Weatherall DJ. Thalassaemia:the long road from the bedside through laboratory to the community. Transfus Med. 2011;21(4):218–223. doi: 10.1111/j.1365-3148.2011.01090.x. [DOI] [PubMed] [Google Scholar]
- 4.Weatherall DJ. The thalassemia syndromes. Tex Rep Biol Med. 1980;40:323–333. [PubMed] [Google Scholar]
- 5.Kaufman E, Lamster IB. The diagnostic applications of saliva—a review. Crit Rev Oral Biol Med. 2002;13(2):197–212. doi: 10.1177/154411130201300209. [DOI] [PubMed] [Google Scholar]
- 6.Madhok S, Madhok S. Dental considerations in thalassemic patients. IOSR-JDMS. 2014;13(6):57–62. doi: 10.9790/0853-13645762. [DOI] [Google Scholar]
- 7.Dhote V, Thosar N, Baliga S. Evaluation of oral hygiene status and salivary biochemistry of patients with thalassemia major: a clinical study. IOSR-JDMS. 2015;14(12):98–102. [Google Scholar]
- 8.Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66(2_suppl):648–653. doi: 10.1177/00220345870660S207. [DOI] [PubMed] [Google Scholar]
- 9.Pierto P, Pineda M, Aguilar M. Spectrophotometric quantification of antioxidant capacity through the formation of a phosphormolybdenum complex; specific application to the determination of vitamin E. Anal Biochem. 1999;269(2):337–341. doi: 10.1006/abio.1999.4019. [DOI] [PubMed] [Google Scholar]
- 10.Kuriakose S, Sundaresan C, Mathai V, et al. A comparative study of salivary buffering capacity, flow rate, resting pH, and salivary immunoglobulin A in children with rampant caries and cariesresistant children. J Indian Soc Pedod Prev Dent. 2013;31(2):69–73. doi: 10.4103/0970-4388.115697. [DOI] [PubMed] [Google Scholar]
- 11.Koracevic D, Koracevic G, Djordjevic V, et al. Method for the measurement of antioxidant activity in human fluids. J Clin Pathol. 2001;54(5):356–361. doi: 10.1136/jcp.54.5.356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Salih KM, AL-Mosawy WF, Faraj YF, et al. Investigation of antioxidant status in Iraqi patients with beta thalassemia major. J Glob Pharma Technol. 2017;7(9):109, 113. [Google Scholar]
- 13.Zubay G. Brown; 4th ed., USA: Wm.C.; 1998. Biochemistry. [Google Scholar]