

Abstract
Purpose:
To observe the effect of demodex infection on the ocular surface changes of patients with meibomian gland dysfunction (MGD) and analyze the correlation between the number of demodex and the changes of the ocular surface.
Methods:
Hundred patients with MGD aged 18–70 years who visited the dry eye center of Shanghai Aier Eye Hospital were recruited. All patients were examined with in vivo confocal microscopy to quantify the demodex and divided them into two groups (demodex negative group and demodex positive group) according to the number of demodex mites. The subjects underwent questionnaires of ocular surface disease index (OSDI) and a series of examinations. Parameters including the OSDI score, fluorescein tear film break-up time (FBUT), meibum quality, meibum gland expressibility, meibomian gland dropout (MG dropout), and ocular redness were recorded and compared between the two groups. The correlation between the number of demodex and the ocular surface changes was further analyzed.
Results:
Among 100 patients, 51 were positive for demodex. The demodex-positive group showed significantly increased scores of OSDI (24.41 ± 3.43 vs 20.98 ± 2.31, P = 0.00), ocular redness score (1.38 ± 0.46 vs 1.00 ± 0.30, P = 0.00), and MG dropout (3.00 ± 1.13 vs 2.18 ± 0.64, P = 0.00) and decreased FBUT (6.40 ± 1.63 vs 6.54 ± 1.83, P = 0.00), compared to the demodex-negative group. A significant correlation was noted between the number of demodex and OSDI, ocular redness, and FBUT.
Conclusion:
Ocular demodex infestation might play a role in the ocular surface discomfort, inflammation, and meibomian gland dropout in MGD patients. It is necessary to pay attention to the examination and treatment of demodex mite in patients with MGD.
Keywords: Correlation, demodex infection, MGD, ocular surface
The meibomian glands, found in the upper and lower eyelids, excrete lipids onto the ocular surface that forms the outermost layer of the tear film.[1] Dysfunction of the meibomian gland (MGD) is a common eye surface disorder having a widespread prevalence of 46–70% in Asian populations and 3.5–20% in Caucasian populations with the incidence increasing with age.[2,3,4,5,6] Persistent MGD can lead to various clinical conditions such as altered tear film stability, dry eye symptoms, inflammation, and ocular surface damage.[7,8] The core mechanism of MGD involves obstruction of the meibomian gland, hyperkeratinization of meibomian ductal system, and increased viscosity of meibum. However, the time course of disease progression is uncertain, including the relation between etiologic factors and the development of symptoms of disease, and so far the management of this disease is primarily palliative.
Ocular demodicosis, which is caused by demodex mites residing in eyelids, has been implicated in a number of external eye diseases, such as eyelash loss, abnormal eyelash alignment, blepharitis, and blepharoconjunctivitis.[9] Two distinct species, Demodex folliculorum and D. brevis, have been identified in human eyelids. D. folliculorum tends to reside in clusters in the eyelash follicles,[10,11,12] while D. brevis generally burrow deeper into the sebaceous and meibomian glands.[13,14,15] Liang et al.[16] noted that D. brevis, despite found by lash epilation, was associated with severe MGD that presented with more than one-third of meibomian gland loss in a young population. We thus wonder if ocular demodicosis may also play a role in MGD patients.
Despite the lack of standardization, two techniques are commonly used to detect demodex mite, notably lash epilation and in vivo confocal microscopy (IVCM). Unfortunately, epilation techniques among studies are highly variable,[17,18,19] which makes the mite count comparison between studies challenging. IVCM allows the visualization of the complete content of the lash follicles and meibomian glands, which increases the detection rate of demodex larvae and D. brevis. Randon et al.[20] demonstrated that lash epilation and IVCM had similar mite detection rates, while Jalbert and Rejab found a higher prevalence of mites with IVCM.[21] In this study, we adopted IVCM to quantify the total number of demodex mites and aimed to find out the relationship between demodicosis and the development of MGD.
Methods
Subjects
This is a cross-sectional study. A total of 100 patients with MGD were enrolled in the Dry Eye Center of Shanghai Aier Eye Hospital from January to June in 2020. All subjects were selected by systematic random sampling from new patients aged 18–70 years in outpatient and divided into two groups (demodex negative group and demodex positive group) according to the number of demodex mites. MGD was diagnosed according to the International Workshop on Meibomian Gland Dysfunction 2010 criteria.[22] Exclusion criteria included acute ocular surface inflammation; having undergone eye surgery within 3 months; having ocular trauma within 3 months; having demodex treatment within 3 months; and wearing a corneal contact lens on the day of examination. This research was conducted in accordance with the Declaration of Helsinki, and Institutional Review Board approval was obtained from Shanghai Aier Eye Hospital.
Experimental procedure
All subjects were examined according to the following procedure: ocular surface disease index (OSDI) questionnaire, slit-lamp biomicroscope examination, ocular surface systematic analysis with Oculus Keratograph 5M, and finally demodex examination under IVCM.
OSDI questionnaire
The OSDI is assessed on a scale of 0–100, with higher scores representing greater disability. The index demonstrates sensitivity and specificity in distinguishing between normal subjects and patients with dry eye disease.
Slit-lamp biomicroscope examination
All patients received a general ocular surface checkup for meibomian gland dysfunction using slit-lamp biomicroscope, including assessment of fluorescein tear film break-up time (FBUT), meibum quality, and meibum gland expressibility. The information of the right eyes in all patients was used for statistical analysis in the following study.
(1) FBUT: Subjects were subsequently asked to blink several times after delivery of one drop of 0.5% fluorescein into the conjunctival sac. The time in seconds between the last complete blink and the appearance of the first corneal black spot was measured three times, and the mean value was recorded.
(2) Meibum gland expressibility: Five glands in the central part of the upper eyelid and five on the lower eyelid were assessed by using a meibomian gland evaluator. The degree was recorded on a scale of 0–3: grade 0, all glands expressible; grade 1, 3–4 glands expressible; grade 2, 1–2 glands expressible; and grade 3, no glands expressible.[23] The scores of the two eyelids were summed to obtain an average score.
(3) Meibum quality: The meibum quality was graded on a scale from 0 to 3 as follows: grade 0, clear; grade 1, cloudy; grade 2, cloudy with granular debris; and grade 3, thick, like toothpaste.[23] The scores of the upper eyelid and low eyelid were summed to obtain an average score.
Oculus Keratograph 5M examination
Oculus Keratograph 5M examination was performed to detect ocular redness and meibomian gland dropout.
(1) Ocular redness: The Oculus Keratograph 5M describes ocular redness using a clinical grading scale of 0.0–4.0 in 0.1 steps.[24] A score above 1.0 indicates the presence of ocular surface inflammation. The higher the score, the more severe the ocular surface inflammation.
(2) Meibomian gland dropout: Partial or complete loss of the meibomian glands was scored using the following meiboscore grades: 0, no loss; 1, loss of an area of less than one-third of the total area; 2, loss of an area between one-third and two-thirds of the total area; 3, loss of an area of more than two-thirds of the total area.[25] The scores of the upper eyelid and low eyelid were summed to obtain an average score.
In vivo confocal microscopy
A total of six eyelashes and their follicles per eye in the central part of the upper eyelid and lower eyelid were scanned with in vivo laser confocal microscopy. More than or equal to three demodex were found in any eyelid defined as positive, the number lower than three demodex was negative.[26] The number of demodex from two eyelids was counted and summed to get a total number.
Statistical analysis
The data was analyzed using IBM SPSS25. Data was recorded as mean ± standard deviation. Mann–Whitney U-test was used to compare the difference of variables between the two groups. ANOVA analysis was used to analyze the differences between different age groups, and SNK-q test was used for further comparison. Spearman correlation analysis was performed between Demodex count and ocular surface indexes in MGD patients. Statistical test was performed by bilateral test and P < 0.05 was considered to be statistically significant.
Results
General information
Forty-nine patients (17 men and 32 women) were enrolled in the demodex negative group and 51 patients (22 men and 29 women) were enrolled in the positive group. The general information of the two groups is listed as Table 1. Chi-square test (X2) was used to compare the gender differences between the two groups, and the result has no statistical significant (P = 0.387). Statistical difference was noted in age (P = 0.001) between the two groups. The average age of the demodex positive group (45.53 ± 14.93) was higher than the demodex negative group (36.47 ± 12.43).
Table 1.
General information
| Demodex negative | Demodex positive | P | |
|---|---|---|---|
| Gender* | |||
| Male | 17 (34.7%) | 22 (43.1%) | |
| Female | 32 (65.3%) | 29 (56.9%) | |
| Age | 36.47±12.43 | 45.53±14.93 | 0.001 |
*Compare and analyze the data by Chi-square (χ2) test
Comparison of the indexes between demodex negative group and demodex positive group
As shown in Table 2, the OSDI, redness score, and MG dropout in the negative group were lower than the positive group and the differences were showed statistical significance (P < 0.05). The FBUT of the negative group was higher than the other group and had a significant difference (P < 0.05). The meibum expressibility and meibum quality between the two groups showed no statistical difference (P > 0.05).
Table 2.
The comparison of all ocular surface parameters between two groups
| Parameters | Demodex negative | Demodex positive | P |
|---|---|---|---|
| OSDI | 20.98±2.31 | 24.41±3.43 | 0.000 |
| FBUT | 6.54±1.83 | 6.40±1.63 | 0.003 |
| Redness | 1.00±0.30 | 1.38±0.46 | 0.000 |
| MG dropout | 2.18±0.64 | 3.00±1.13 | 0.000 |
| Meibum expressibility | 2.51±1.04 | 2.78±0.88 | 0.166 |
| Meibum quality | 2.49±1.08 | 2.53±0.88 | 0.496 |
There was a positive correlation between demodex counting and OSDI, redness score (rs = 0.603 P < 0.05, rs = 0.404 P < 0.05). The demodex counting had negative correlation with FBUT (rs = -0.345 P < 0.05). There was no significant linear correlation between demodex counting and MG dropout, meibum expressibility and meibum quality [Table 3 and Figs. 1-6].
Table 3.
Correlation between Demodex count and various examination indexes
| OSDI | Redness | FBUT | |
|---|---|---|---|
| Rs | 0.603 | 0.404 | -0.345 |
| P | 0.00 | 0.00 | 0.00 |
Figure 1.

The scatter plot between FBUT and the number of demodex mite,which has a linear relationship
Figure 6.

The scatter plot between Meibum expressibility and the number of demodex mite,which has no obvious linear relationship
Figure 2.

The scatter plot between Redness score and the number of demodex mite,which has a linear relationship
Figure 3.
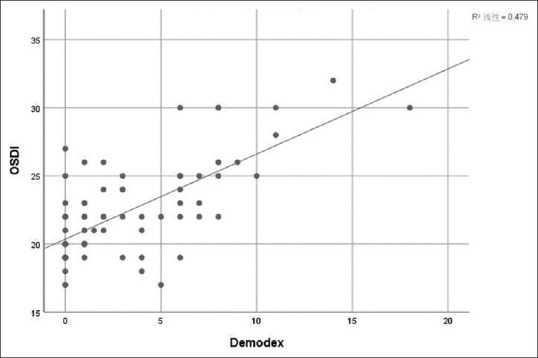
The scatter plot between OSDI and the number of demodex mite,which has a linear relationship
Figure 4.

The scatter plot between MG dropout and the number of demodex mite,which has no obvious linear relationship
Figure 5.

The scatter plot between Meibum quality and the number of demodex mite,which has no obvious linear relationship
Results of comparison between different age groups
Three age groups were divided as follows: group 1: 18–30 years, group 2: 31–50 years, and group 3: 51 years and above. The results [Table 4] showed that there was no significant difference among different age groups in OSDI, FBUT, meibum expressibility, and meibum quality. However, the differences were statistically significant in the demodex count, ocular redness, and meibomian gland dropout (P = 0.019, 0.000, 0.033). Nevertheless, the results of the SNK-q test between each two groups showed that significant differences in demodex count, ocular redness, and meibomian gland dropout were only seen between group 1 and group 3 (P < 0.05), but not between groups with narrower age gaps, i.e., group 1 vs group 2 and group 2 vs group 3.
Table 4.
The comparison of all ocular surface parameters among three age groups
| Group 1 (18-30 yr) n=28 | Group 2 (30-50 yr) n=47 | Group 3 (>50 yr) n=28 | P | |
|---|---|---|---|---|
| Demodex | 2.36±2.88 | 4.05±4.18 | 5.20±3.34 | 0.019* |
| OSDI | 22.04±2.78 | 22.77±3.80 | 23.44±3.18 | 0.324 |
| FBUT | 6.42±1.59 | 5.86±1.89 | 5.63±1.88 | 0.255 |
| Redness | 0.96±0.38 | 1.20±0.40 | 1.46±0.40 | 0.000* |
| MG dropout | 2.29±1.08 | 2.59±0.97 | 3.00±0.87 | 0.033* |
| Meibum expressibility | 2.64±1.19 | 2.62±1.05 | 2.27±1.02 | 0.929 |
| Meibum quality | 2.43±1.17 | 2.56±0.93 | 2.48±0.87 | 0.813 |
Discussion
Demodex is a parasitic mite and mainly lives in eyelash follicles and meibomian glands. The pathogenesis[27] of demodex mites has been debated for a long time and a plausible explanation includes causing direct damage, acting as a carrier of bacteria, and inducing hypersensitivity. MGD is a very common meibomian gland disease and recent studies have shown that demodex infestation can be an important factor in meibomian gland dysfunction.[28,29] Previous study[30] has shown that the rate of demodex infestation increases with age, being observed in 84% of the general population aged 60 years, and 100% of the general population aged above 70 years. Our study also showed that the average age of the positive group is higher than the negative group [Table 1]; it may be related to the poor hygiene habits and relatively low immunity of elderly patients.
Comparison between the demodex-positive group and demodex-negative group showed that the positive group was significantly higher than the negative group in redness score, OSDI and MG dropout, and was significantly lower in FBUT. It revealed that demodex infection may be an important factor to cause or aggravate the damage of the ocular surface and meibomian gland in MGD patients.[31] Xiaobo Zhang et al.[32] have reported that the ocular demodex-positive group showed significantly increased scores of OSDI, lid margin abnormality, and corneal fluorescein staining compared to the ocular demodex-free group, which is consistent with our findings. However, their study adopted light microscopy to recognize the demodex mites and mainly focused on the ocular surface manifestation including the meibum expressibility and meibum quality and did not observed the MG dropout. In this study, we used confocal microscopy to detect demodex mites and added the observation of MG dropout between the two groups, which was more accurate and comprehensive. Meibomian gland dropout, i.e., disappearance of the glandular tissue inside the tarsal plates, was believed to be caused by aging, contact lens wearing, and gland atrophy (as a result of gland obstruction and inflammation).[33] According to our results, we have three hypotheses for this finding. First, we might assume demodex infection as a risk factor for meibomian gland dropout. As a result, demodex mites detection should not be ignored in the MGD patients especially those with obvious ocular surface discomfort symptoms or notable meibomian gland dropout. It is necessary to recognize the importance of the treatment of demodex mite in those patients. Another possibility is that demodex increase was caused by the aggravation of meibomian gland dropout. The static glands might shelter the mites and their eggs. Thus, more attention would be paid to the loss of gland when we are dealing with the mites. There is, however, a third possibility: aging, or some other obscure factor, caused both more demodex and more gland dropout in some way, given the truth that both mite counts and MG dropout were found to be different among three age groups in our study [Table 4]. More evidence would be needed to testify which assumption of the three is more believable, especially interventional study to verify the causal link between the three factors including aging, more demodex, and more gland dropout.
Intriguingly, as is shown in Table 3, we found no significant difference in Meibum expressibility and Meibum quality between the two groups, showing that the mites infestation had no obvious relationship with the meibomian gland expression function. This finding leaves us with two hints. For one thing, in the group of MGD patients, the negative of demodex examination did not mean better meibomian gland function; therefore, the treatment of demodex, if not combined with the treatment of MGD, like physical therapy, would not bring benefits for improving meibomian gland function in patients with both MGD and demodex. For another, opposite to the traditional concept that the occlusion and dysfunction of meibomian gland was a prerequisite for the emergence of gland dropout,[33] demodex infection might directly or indirectly result in the dropout, through inflammation mechanism or some other unclear way.
According to the correlation analysis, the number of demodex was significantly correlated with OSDI, ocular redness, and FBUT and had no correlation with other parameters. It has been shown that the number of demodex folliculorum was proportional to the severity levels of ocular discomfort and the OSDI score.[34] Our study provided a more comprehensive understanding that the more mites, the more serious the discomfort and inflammation of the ocular surface, and the stability of tear film more obviously destroyed. As an ocular surface index, the grade of ocular redness can directly reflect the degree of ocular surface inflammation, so the positive correlation between the number of demodex mites and ocular redness suggested that demodex infestation could be an independent factor to aggravate or cause ocular surface inflammation in MGD patients.
The principal limitation of this study is the cross-sectional design, which illustrates association but not causal link. A prospective study is required in the future for further exploration.
Conclusion
We can probably draw the following conclusions based on the results of this study. First, demodex mite infection might be associated with severer symptoms and signs of patients with meibomian gland dysfunction so that more attention should be paid to the examination and treatment of demodex mites. Second, inflammation played a role in the demodex infestation, and thus antiinflammatory treatment should be highlighted for patients with demodex infestation. Third, there was a link between the demodex and meibomian gland dropout, although the causality was still unknown. The difficult problem worthy of further study in the follow-up work is that the course of mite infection and its relationship with the extent of meibomian gland destruction.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.McCulley JP, Shine WE. Meibomian gland function and the tear lipid layer. Ocul Surf. 2003;1:97–106. doi: 10.1016/s1542-0124(12)70138-6. [DOI] [PubMed] [Google Scholar]
- 2.Uchino M, Dogru M, Yagi Y, Goto E, Tomita M, Kon T, et al. The features of dry eye disease in a Japanese elderly population. Optom Vis Sci. 2006;83:797–802. doi: 10.1097/01.opx.0000232814.39651.fa. [DOI] [PubMed] [Google Scholar]
- 3.Schein OD, Munoz B, Tielsch JM, Bandeen-Roche K, West S. Prevalence of dry eye among the elderly. Am J Ophthalmol. 1997;124:723–8. doi: 10.1016/s0002-9394(14)71688-5. [DOI] [PubMed] [Google Scholar]
- 4.McCarty CA, Bansal AK, Livingston PM, Stanislavsky YL, Taylor HR. The epidemiology of dry eye in Melbourne, Australia. Ophthalmology. 1998;105:1114–9. doi: 10.1016/S0161-6420(98)96016-X. [DOI] [PubMed] [Google Scholar]
- 5.Lekhanont K, Rojanaporn D, Chuck RS, Vongthongsri A. Prevalence of dry eye in Bangkok, Thailand. Cornea. 2006;25:1162–7. doi: 10.1097/01.ico.0000244875.92879.1a. [DOI] [PubMed] [Google Scholar]
- 6.Lin PY, Tsai SY, Cheng CY, Liu JH, Chou P, Hsu WM. Prevalence of dry eye among an elderly Chinese population in Taiwan:The Shihpai Eye Study. Ophthalmology. 2003;110:1096–101. doi: 10.1016/S0161-6420(03)00262-8. [DOI] [PubMed] [Google Scholar]
- 7.Nelson JD, Shimazaki J, Benitez-del-Castillo JM, Craig JP, McCulley JP, Den S, et al. The international workshop on meibomian gland dysfunction:Report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci. 2011;52:1930–7. doi: 10.1167/iovs.10-6997b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wu H, Lin Z, Yang F, Fang X, Dong N, Luo S, et al. Meibomian gland dysfunction correlates to the tear film instability and ocular discomfort in patients with pterygium. Sci Rep. 2017;7:45115. doi: 10.1038/srep45115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lee SH, Chun YS, Kim JH, Kim ES, Kim JC. The relationship between demodex and ocular discomfort. Invest Ophthalmol Vis Sci. 2010;51:2906–11. doi: 10.1167/iovs.09-4850. [DOI] [PubMed] [Google Scholar]
- 10.Coston TO. Demodex folliculorum blepharitis. Trans Am Ophthalmol Soc. 1967;65:361–92. [PMC free article] [PubMed] [Google Scholar]
- 11.Desch C, Nutting WB. Demodex folliculorum (Simon) and D. brevis Akbulatova of Man:Redescription and Reevaluation. J Parasitol. 1972;58:169–77. [PubMed] [Google Scholar]
- 12.English F. Demodex folliculorum and oedema of the eyelash. Br J Ophthalmol. 1971;55:742–6. doi: 10.1136/bjo.55.11.742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.English FP, Nutting WB. Demodicosis of ophthalmic concern. Am J Ophthalmol. 1981;91:362–72. doi: 10.1016/0002-9394(81)90291-9. [DOI] [PubMed] [Google Scholar]
- 14.Lacey N, Kavanagh K, Tseng S. Under the lash:Demodex mites in human diseases. Biochem (Lond) 2009;31:2–6. [PMC free article] [PubMed] [Google Scholar]
- 15.Randon M, Liang H, El Hamdaoui M, Tahiri R, Batellier L, Denoyer A, et al. In vivo confocal microscopy as a novel and reliable tool for the diagnosis of Demodex eyelid infestation. Br J Ophthalmol. 2015;99:336–41. doi: 10.1136/bjophthalmol-2014-305671. [DOI] [PubMed] [Google Scholar]
- 16.Liang L, Liu Y, Ding X, Ke H, Chen C, Tseng SCG. Significant correlation between meibomian gland dysfunction and keratitis in young patients with Demodex brevis infestation. Br J Ophthalmol. 2017;102:1098–1102. doi: 10.1136/bjophthalmol-2017-310302. [DOI] [PubMed] [Google Scholar]
- 17.Gao YY, Di Pascuale MM, Li W, Liu DT, Baradaran-Rafii A, Elizondo A, et al. High prevalence of Demodex in eyelashes with cylindrical dandruff. Invest Ophthalmol Vis Sci. 2005;46:3089–94. doi: 10.1167/iovs.05-0275. [DOI] [PubMed] [Google Scholar]
- 18.Murphy O, O'Dwyer V, Lloyd-McKernan A. The efficacy of tea tree face wash, 1, 2- Octanediol and microblepharoexfoliation in treating Demodex folliculorum ble- pharitis, Cont Lens Anterior. Eye. 2018;41:77–82. doi: 10.1016/j.clae.2017.10.012. [DOI] [PubMed] [Google Scholar]
- 19.Murphy O, O'Dwyer V, Lloyd-McKernan A. Ocular Demodex folliculorum:Pre- valence and associated symptoms in an Irish population. Int Ophthalmol. 2019;39:405–17. doi: 10.1007/s10792-018-0826-1. [DOI] [PubMed] [Google Scholar]
- 20.Randon M, Liang H, El Hamdaoui M, Tahiri R, Batellier L, Denoyer A, et al. In vivo confocal microscopy as a novel and reliable tool for the diagnosis of Demodex eyelid infestation. Br J Ophthalmol. 2015;99:336–41. doi: 10.1136/bjophthalmol-2014-305671. [DOI] [PubMed] [Google Scholar]
- 21.Jalbert I, Rejab S. Increased numbers of Demodex in contact lens wearers. Optom Vis Sci. 2015;92:671–8. doi: 10.1097/OPX.0000000000000605. [DOI] [PubMed] [Google Scholar]
- 22.J Daniel Nelson, Jun Shimazaki, Jose MB, Craig JP, McCulley JP, Den S, et al. The international workshop on meibomian gland dysfunction:Report of the definiton and classification subcommittee. Invest Ophthalmol Vis Sci. 2011;52:1930–7. doi: 10.1167/iovs.10-6997b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lee H, Min K, Kim EK, Kim T-I. Minocycline controls clinical outcomes and inflammatory cytokines in moderate and severe meibomian gland dysfunction. Am J Ophthalmol. 2012;154:949–57. doi: 10.1016/j.ajo.2012.06.009. [DOI] [PubMed] [Google Scholar]
- 24.Downie LE, Keller PR, Vingrys AJ. Assessing ocular bulbar redness:A comparison of methods. Opthalmic Physiol Opt. 2016;36:132–9. doi: 10.1111/opo.12245. [DOI] [PubMed] [Google Scholar]
- 25.Wong S, Srinivasan S, Murphy PJ, Jones L. Comparision of meibomiain gland dropout using two infrared imaging devices. Cont Lens Anterior Eye. 2019;42:311–7. doi: 10.1016/j.clae.2018.10.014. [DOI] [PubMed] [Google Scholar]
- 26.Cheng S, Zhang M, Chen H, Fan W, Huang Y. The correlation between the microstructure of meibomian glands and ocular Demodex infestation:A retrospective case-control study in a Chinese population. Medicine (Baltimore) 2019;98:e15595. doi: 10.1097/MD.0000000000015595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Luo X, Li J, Chen C, Tseng S, Liang L. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea. 2017;36(Suppl 1):S9–14. doi: 10.1097/ICO.0000000000001361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.DRabensteiner DF, Aminfar H, Boldin I, Nitsche-Resch M, Berisha B, Schwantzer G, et al. Demodex mite infestation and its associations with tear film and ocular surface parameters in patients with ocular discomfort. Am J Ophthalmol. 2019;204:7–12. doi: 10.1016/j.ajo.2019.03.007. [DOI] [PubMed] [Google Scholar]
- 29.Sabeti S, Kheirkhah A, Yin J, Dana R. Management of meibomian gland dysfunction:A review. Surv Ophthalmol. 2020;65:205–17. doi: 10.1016/j.survophthal.2019.08.007. [DOI] [PubMed] [Google Scholar]
- 30.Post CF, Juhlin E. Demodex folliculorum and blepharitis. Arch Dermatol. 1963;88:298–302. doi: 10.1001/archderm.1963.01590210056008. [DOI] [PubMed] [Google Scholar]
- 31.Cheng SN, Jiang FG, Chen H, Gao H, Huang YK. Intense pulsed light therapy for patients with meibomian gland dysfunction and ocular demodex infestation. Curr Med Sci. 2019;39:800–9. doi: 10.1007/s11596-019-2108-1. [DOI] [PubMed] [Google Scholar]
- 32.Zhang X, Ding Y, He W. The association between demodex infestation and ocular surface manifestation in meibomian gland dysfunction. Int J Ophthalmol. 2018;11:589–92. doi: 10.18240/ijo.2018.04.08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Knop E, Knop N, Millar T, Obata H, Sullivan DA. The international workshop on meibomian gland dysfunction:Report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci. 2011;52:1938–78.9+. doi: 10.1167/iovs.10-6997c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lee SH, Chun YS, Kim JH, Kim ES, Kim JC. The relationship between demodex and ocular discomfort. Invest Ophthalmol Vis Sci. 2010;51:2906–11. doi: 10.1167/iovs.09-4850. [DOI] [PubMed] [Google Scholar]