

Abstract
Purpose:
This study aims to assess the novel and innovative method of Safe Eye Examination (SEE) technique using the model eye for the purpose of teaching, training, and resident examination.
Methods:
A questionnaire-based study (Descriptive Data) with 53 participants, including ophthalmology residents, fellows in various subspecialties, and trainee optometrists was used. In our study, we used the Reti Eye model, but instead of the usual retina template sheet, we used prominent pathological fundus photographs loaded into the model eye. The study participants were asked to view prominent pathological fundus images printed on a matte finish paper. A circular image was cut and was placed in the Reti Eye model. The candidates were made to perform indirect ophthalmoscopy with a + 20D lens and to fill up a Google image assessment scale questionnaire with characteristics, including pixelation, sharpness, contrast, reflexes, blotchy appearance, and diagnostic confidence, which were then analyzed and depicted. Association between categorical variables was analyzed using Fisher exact test and Chi-square test. A P value of less than 0.05 was considered statistically significant. All data were analyzed with a statistical software package (SPSS, Version 16.0 for Windows).
Results:
The number of positive responses (>90%) obtained for the pixelation, sharpness, contrast, reflexes, blotchy appearance, and diagnostic confidence of the image viewed were statistically more significant than the negative responses (P < 0.05).
Conclusion:
The SEE technique of using the model eye can be incorporated for teaching, training, and skill assessment in the examinations in these difficult times of COVID-19 (coronavirus disease 2019) pandemic.
Keywords: Image assessment scale, Reti Eye model, Safe Eye Examination
The coronavirus disease 2019 (COVID-19) caused by a novel coronavirus (2019-nCoV) that started in late 2019 spread throughout the world leading it to be declared as a global pandemic by the World Health Organization.[1,2] The impact of this outbreak has been severe and has affected millions worldwide.[3] Coming to India, in an effort to curb the spread of the virus, lockdown measures were implemented, and the government directed the hospitals to function only for emergency health care services and stop all nonemergency outpatient department treatments during the lockdown period.[2]
Ophthalmology being more of a nonemergency branch and the subsequent decreased patient inflow because of the fear of the spread of the virus and lockdown measures, ophthalmic training has taken a major hit during these COVID-19 times. Keeping in mind the changes in teaching guidelines incorporated by various medical councils all over the world,[4,5,6,7] the innovative idea of Safe Eye Examination (SEE) technique came into inception aimed at continued teaching and training. The Reti Eye model (Aurolab, Aravind Eye Care, Madurai) is usually utilized in training and teaching laser pan retinal photocoagulation (PHC) or laser indirect ophthalmoscopy.[8] But instead of the template films that come along with it, we modified it by incorporating pathological fundus images. We present the effectiveness of this alternate way of using a nonsurgical simulator for identifying retinal diseases.
Methods
The study was conducted at a tertiary eye care center in South India. Institutional ethics committee approval was obtained before the initiation of the study.
Methodology
The basis of the study was the Reti Eye model (developed by Aurolab, Aravind Eye Care, Madurai) [Fig. 1a], which originally uses an oval-shaped model eye. The front part of the model eye can be unscrewed exposing the interior of the model eye with painted template retinal films on a thin sheet made to fit along the concave curvature of the model eyeball [Fig. 1b].[9] The painted template retinal film can be altered by lesions of the retina being painted on the template for teaching purposes. However, the painted lesions turned out to be indistinct because of preexisting orange background of the template [Fig. 1c]. In our SEE technique, we wanted to give a more realistic fundus appearance in the model eye for better understanding and teaching of the retinal lesions. We replaced the preexisting template in the Reti Eye with pathological fundus photographs of various retinal lesions taken with Topcon TRC-50DX (Topcon Medical Systems, Inc., Japan).
Figure 1.

The Approach for our SEE technique: (a) Reti Eye with wooden holder; (b) Interior of the Reti Eye with template retina; (c) Indistinct painted lesion on template retina; (d) Cutout of printer paper used originally; (e) Calculation of appropriate fit for fundus lesions; (f) Pathological fundus lesions printed on matte finish paper; (g) Nicks in periphery for proper fit; and (h) End result
To start with, we took small printouts of the fundus photos on the printer paper, but the image was too large to fit in the model eye. We used a small cutout that could be placed in the eye, and we could view the target lesion with fair accuracy but with a lot of pixelation [Fig. 1d]. To find the ideal diameter of the printout so that it can best fit the concave curvature of the back of the model eye, we measured the inner diameter of the model eye, which was 30 mm [Fig. 1e]. We took printout of the fundus photo with 25-mm, 30-mm, and 35-mm diameter. The best fit was noted with 30-mm diameter of the printout (600 dots per inch) [Fig. 1f]. To make the image drape along the concave contour of the back of the model eye, four 1- to 2-mm nicks were made in a cross fashion [Fig. 1g and h]. After confirming the dimensions, it was time to conclude on the type of paper to be used for the printout for best visualization with minimal reflexes as possible.
Before the actual initiation of the study, we took high-definition printouts of various retinal lesions (each fundus photo had dimensions of 3 cm × 3 cm) on various forms of paper such as butter paper, glossy paper 180 gross square meter (gsm), matte finish paper 135 gsm, executive bond paper 100 gsm, and JK paper. A panel of experts comprising five ophthalmologists in the hospital were given the model eyes with the photos in situ to visualize and analyze the quality of the image via slit-lamp fundoscopy with the help of a +90D lens and indirect ophthalmoscopy (IDO) with a +20D lens. The matte finish paper with the fundus photograph had the best quality with minimal reflexes, and the same was used for this study [Fig. 2a and b].
Figure 2.
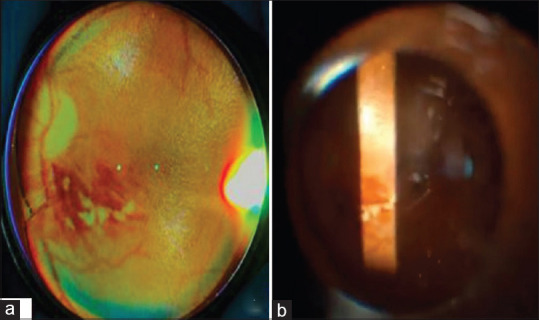
The final images showing clear, distinct fundus lesions viewed through (a) Indirect ophthalmoscopy using +20D lens; (b) Slit-lamp biomicroscopy using +90D lens
Three Reti Eye models were constructed using three Matte finish fundus photographs of various retinal lesions. Each candidate was given two Reti Eye models selected and was allowed to examine the same for 10 minutes using slit-lamp fundoscopy and IDO examination. The candidates were requested to assess the quality of the images using a survey form (Google Form ©2020 Google), which contained six mandatory questions regarding the quality of the image (Arapakis et al.[10]) and subjective assessment along with suggestions and feedback. The characteristics of the retina images studied were pixelation, sharpness, contrast, artifacts/reflexes, blotchy appearance, and diagnostic confidence [Table 1]. Each characteristic was graded from Level 1 being the best or excellent to Level 5 being very poor quality or nondiagnostic.
Table 1.
Characteristics of final images
| Image characteristics | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Noise/Pixelation | Minimal or no noise/pixelation | No significant noise/pixelation | Noisy/pixelation diagnostic | Significant noise/pixelation-affects diagnosis | High-level noise/pixelation-nondiagnostic |
| Sharpness | Excellent sharpness | Good sharpness | Moderate sharpness | Poor sharpness-bad visibility | Zero visibility-nondiagnostic |
| Contrast | Excellent contrast | Very good contrast | Good contrast | Poor contrast-unsatisfactory visualization | Nondiagnostic-image similar to the use of no contrast |
| Diagnostic confidence | Completely confidence | High confidence | Good confidence | Poor confidence | No diagnostic confidence-unacceptable |
| Artifacts/reflexes | No artifacts | Insignificant artifacts/reflexes | Minor artifacts/reflexes | Major artifacts/reflexes-diagnosis still possible | Artifacts/reflexes affecting diagnostic information |
| Blotchy appearance | Absent | Mild | Moderate | Significant-diagnosis still possible | Intense-affecting diagnosis |
Statistical analysis
The association between the categorical variables was analyzed using Fisher exact test and Chi-square test. A P value of less than 0.05 was considered statistically significant. Subjective image data were compared using Wilcoxon signed-rank test. All descriptive data were analyzed with a statistical software package (SPSS, Version 16.0 for Windows).
Results
Responses from 43 (81.1%) trainee ophthalmologists (residents and fellows) and 10 (18.9%) trainee optometrists were tabulated and analyzed. Detailed evaluation of responses for each characteristic of the image is presented in the following sections.
Pixelation
Among the 53 responses, no/nonsignificant/minor pixelation were reported by 52 (98.1%) candidates. Almost all the candidates were able to diagnose the presented lesion using IDO. Only one candidate (2.9%) experienced significant pixelation that affected the diagnosis [Fig. 3a].
Figure 3.

Graphical representation of the analysis of various characteristics of the final image viewed via SEE technique: a. Pixelation; (b) Sharpness; (c) Contrast; (d) Reflexes; (e) Blotchy appearance; and (f) Diagnostic confidence
Sharpness
The sharpness was reported as excellent/good/moderate sharp in 51 (96.22%) responses. Only two candidates (3.7%) reported poor sharpness causing bad visibility. No candidate complained of the lesion in the image being not visible at all [Fig. 3b].
Contrast
Excellent/very good/good contrast responses were reported in 50 (94.30%) responses. Three candidates (5.67%) experienced poor contrast while viewing the fundus image [Fig. 3c].
Artifacts/Reflexes
No/insignificant/minor/major reflexes were reported in 50 (94.30%) responses. Three (5.6%) candidates said that there were reflexes that were affecting the diagnostic information in the image [Fig. 3d].
Blotchy appearance
No/mild/moderate blotchy appearance was reported in 52 (98.11%) responses. Only one candidate (2.9%) responded by saying that the blotchy appearance was significant but even with it rendered the diagnosis still possible [Fig. 3e].
Diagnostic confidence
Very high/good/complete confidence was reported in 48 (90.9%) responses. Five candidates (9.1%) suggested poor confidence in making the final diagnosis [Fig. 3f].
When analyzing the characteristics of each image, the amount of positive (Grades 1–3) responses for this model of IDO training were significantly higher than the negative responses (Grades 4–5) for each characteristic (P < 0.05).
The candidates were encouraged to provide their valuable inputs in the form of feedback/suggestions. Majority of them (>50% responses) wanted the model to be increased in size and placed at a proper height or on an appropriate mound. The second most valuable suggestion (~30% responses) was to mark the laterality of the eye and associated landmarks for better anatomical orientation for saving time during the examination. Approximately 20% candidates wanted the pupillary aperture to be increased in size to simulate a more dilated fundus view.
All the constructive criticisms were well received, and the appropriate changes to incorporate them into this setup have been initiated and are underway.
Discussion
The impact of the COVID-19 pandemic has been noted significantly in the residency training with the current crop of residents not only in ophthalmology but also across various specialties facing the crunch in clinical rotations, surgical cases, and nonoperative patient care.[11] Fewer patients in the coming months may decrease the surgical demands and will in turn lead to decreased surgical rotations for the residents/fellows, which might significantly affect their clinical and surgical skill acquisition.[12] Our survey highlighted the fact that alternate modalities of teaching and training are the need of the hour during these COVID-19 times because the patient–doctor interaction has suffered quite a bit and a sizeable decrease in the patient inflow has been noted. Although there is no substitute for learning and practicing clinical examination techniques on patients and surgical procedures in real life, recent developments in simulation-based training have created new avenues and are providing a breakthrough in imparting knowledge and skills.
The advantages of simulation are that it creates opportunities[13,14] and also allows repetitive practice without affecting patient care.[15] Other notable advantages specifically pertaining to IDO simulation are the lack of requirement to dilate the pupils of patients/students and no phototoxicity secondary to prolonged exposure.[16] Residents/fellows can also get to understand rare or unusual cases with this form of training, which they may not come across in their routine postings.[17]
Chung and Watzke[18] described a simple model of a closed plastic chamber with a 37-mm photograph encased in it and students visualizing it via direct ophthalmoscopy through an 8-mm opening. The associated problems included intense light reflection, low quality, and loss of space perception by the examiners. Pao et al.[19] improvised on the aforementioned technique by using a Styrofoam mannequin head and presented it as THELMA (The Human Eye Learning Model Assistant), which came with the added advantages of better patient–physician relationship and a sense of adequate positioning. Later developments included The EYE Exam Simulator (developed by Kyoto Kagaku Co., Kyoto, Japan) and Eye Retinopathy Trainer® (developed by Adam, Rouilly Limited, Sittingbourne, UK), which are real-size mannequin heads, with an adjustable pupil that allows access to a wider, 35-mm designed, high-quality retina, through a handheld ophthalmoscope. The complexity of this device may cause technical difficulties in the absence of experienced technical staff to assist them.[20] Other direct ophthalmoscopy simulation models studied were the plastic canister, which showed enhanced quality of learning.[21,22]
Other high-end options are virtual reality–based simulation and training. Currently in vogue are the Eyesi® Direct and Indirect Ophthalmoscope simulator, designed by VRmagic providing the added benefits of mapping visualized retinal regions, ability to control physiologic/pathologic functions, and immediate feedback.[20] The cons include the cost and the requirement of expert staff.[15] An additional advantage in our ‘SEE’ technique is that it is very cheap and economical. Any fundus photo, including rare retinal disease presentation can be printed and used for teaching, training, and learning.
The Reti Eye was a practice tool developed by Aurolab (Aravind Eye Care, Madurai) for beginners to learn IDO and laser PHC before starting the same on patients. The kit contains 10 replaceable retinal films for PHC, and the burnt films are used to assess the progress in training. Along with the films, it contains a wooden base on which the model eye can be rotated, and it provides a favorable environment to ophthalmic surgery and also confers protection against mechanical damages.[9]
The SEE technique using the Reti Eye model provides an easy, efficient, and cost-effective alternative to IDO examination with the live participant. More than 90% responses in all were positive or favorable for each characteristic of the image making this modality a feasible option when it comes to teaching and training. The biggest advantage of our technique during the COVID-19 times is getting the model eye disinfected by wiping with 95% isopropyl alcohol after each examination. The SEE technique can also be used for gaining and teaching slit-lamp biomicroscopy by attaching the model eye with an available slit-lamp holder. Our SEE technique is very easy to replicate and highly effective; it does not need any special training to assemble the same except having fair scissors-cutting skills.
Feedback/suggestions collected from the candidates mostly listed our limitations such as the field of view obtained in the final image was less and the image was also magnified to a larger extent. To have a larger field of view, collage of the fundus photos/wide-field fundus photo using various available devices can be considered. A high minus power soft/rigid gas permeable contact lens was placed over the core of the model eye in an attempt to minimize the magnification but that did not help the cause. The orientation of the model eye needs to be checked before initiating the examination because it will ease the technical process by marking the horizontal axis on the model eye. The pupillary area diameter could also be widened for increasing the field of view although keeping in mind on not compromising the quality of the image. The provision for indentation and also the incorporation of media opacities into the model can bring it closer to a real-world experience. These suggestions need to be worked on from our side.
In the COVID-19 times, by conducting and assessing the clinical skills and avoiding undue risk to both the examinee and the participant, we have successfully used the SEE technique with the Reti Eye model for Diplomate of National Board (DNB) ophthalmology final practical examination conducted at our center in evaluating the IDO and slit-lamp biomicroscopy skill demonstration/assessment [Fig. 4a-d]. It was also successfully used in the Bachelor of Science (B.Sc.) Optometry final practical examination for slit-lamp biomicroscopy and IDO skill demonstrations/assessment.
Figure 4.

Ophthalmology practical examination for residents conducted with the help of SEE technique at our center during COVID-19 times
Conclusion
The COVID-19 pandemic has brought about a paradigm shift in the way ophthalmology is functioning. With the current scenario in mind, the SEE technique with the model eye can be used for safe teaching, training, and assessment of IDO or slit-lamp biomicroscopy skills for our residents and trainee optometrists.
Financial support and sponsorship
RETI EYE model, Aurolab, Aravind Eye Care, Madurai
Conflicts of interest
There are no conflicts of interest.
References
- 1.Khanna RC, Honavar SG. All eyes on Coronavirus—What do we need to know as ophthalmologists. Indian J Ophthalmol. 2020;68:549–53. doi: 10.4103/ijo.IJO_516_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nair AG, Gandhi RA, Natarajan S. Effect of COVID-19 related lockdown on ophthalmic practice and patient care in India:Results of a survey. Indian J Ophthalmol. 2020;68:725–30. doi: 10.4103/ijo.IJO_797_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Torales J, O'Higgins M, Castaldelli-Maia JM, Ventriglio A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int J Soc Psychiatry. 2020;66:317–20. doi: 10.1177/0020764020915212. [DOI] [PubMed] [Google Scholar]
- 4.Whelan A, Prescott J, Young G, Catanese VM, McKinney R. Washington, DC: Association of American Medical Colleges; 2020. Guidance on Medical Students'Participation in Direct Patient Contact Activities; pp. 1–6. [Google Scholar]
- 5.Choi BD. A neurosurgery resident's response to COVID-19:anything but routine. J Neurosurg. 2020;133:16–7. doi: 10.3171/2020.4.JNS201028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Patil NG, Chan Y, Yan H. SARS and its effect on medical education in Hong Kong. Med Educ. 2003;37:1127–8. doi: 10.1046/j.1365-2923.2003.01723.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Clark J. Fear of SARS thwarts medical education in Toronto. BMJ. 2003;326:784. doi: 10.1136/bmj.326.7393.784/c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shah PK, Narendran V, Kalpana N. Evolution of ROP screening at Aravind Eye Hospital, Coimbatore-Lessons learnt and the way ahead. Community Eye Health. 2018;31:S23–4. [PMC free article] [PubMed] [Google Scholar]
- 9.Aurolab. [2016] Retieye. [online] Available from: https://www.aurolab.com/retieye.asp .
- 10.Arapakis I, Efstathopoulos E, Tsitsia V, Kordolaimi S, Economopoulos N, Argentos S, et al. Using “iDos.e4“iterative reconstruction algorithm in adults'chest–abdomen–pelvis CT examinations:Effect on image quality in relation to patient radiation exposure. Br J Radiol. 2014;87:20130613. doi: 10.1259/bjr.20130613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mishra D, Nair AG, Gandhi RA, Gogate PJ, Mathur S, Bhushan P, et al. The impact of COVID19 related lockdown on ophthalmology training programs in IndiaOutcomes of a survey. Indian J Ophthalmol. 2020;68:9991004. doi: 10.4103/ijo.IJO_1067_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Potts JR., 3rd Residency and fellowship program accreditation:Effects of the novel coronavirus (COVID-19) Pandemic. J Am Coll Surg. 2020;230:1094–7. doi: 10.1016/j.jamcollsurg.2020.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Weller JM, Nestel D, Marshall SD, Brooks PM, Conn JJ. Simulation in clinical teaching and learning. Med J Aust. 2012;196:594. doi: 10.5694/mja10.11474. [DOI] [PubMed] [Google Scholar]
- 14.Benbassat J, Polak BC, Javitt JC. Objectives of teaching direct ophthalmoscopy to medical students. Acta Ophthalmol. 2012;90:503–7. doi: 10.1111/j.1755-3768.2011.02221.x. [DOI] [PubMed] [Google Scholar]
- 15.Grodin MH, Johnson TM, Acree JL, Glaser BM. Ophthalmic surgical training:A curriculum to enhance surgical simulation. Retina. 2008;28:1509–14. doi: 10.1097/IAE.0b013e31818464ff. [DOI] [PubMed] [Google Scholar]
- 16.Leitritz MA, Ziemssen F, Suesskind D, Partsch M, Voykov B, Bartz-Schmidt KU, et al. Critical evaluation of the usability of augmented reality ophthalmoscopy for the training of inexperienced examiners. Retina. 2014;34:785–91. doi: 10.1097/IAE.0b013e3182a2e75d. [DOI] [PubMed] [Google Scholar]
- 17.Liu A, Tendick F, Cleary K, Kaufmann C. A survey of surgical simulation:Applications, technology, and education. Presence Teleo Virt. 2003;12:599–61. [Google Scholar]
- 18.Chung KD, Watzke RC. A simple device for teaching direct ophthalmoscopy to primary care practitioners. Am J Ophthalmol. 2004;138:501–2. doi: 10.1016/j.ajo.2004.04.009. [DOI] [PubMed] [Google Scholar]
- 19.Pao KY, Uhler TA, Jaeger EA. Creating THELMA –The Human eye learning model assistant. J Acad Ophthalmol. 2008;1:25–9. [Google Scholar]
- 20.Ricci LH, Ferraz CA. Simulation models applied to practical learning and skill enhancement in direct and indirect ophthalmoscopy:A review. Arq Bras Oftalmol. 2014;77:334–8. doi: 10.5935/0004-2749.20140084. [DOI] [PubMed] [Google Scholar]
- 21.Hoeg TB, Sheth BP, Bragg DS, Kivlin JD. Evaluation of a tool to teach medical students direct ophthalmoscopy. WMJ. 2009;108:24–6. [PubMed] [Google Scholar]
- 22.Swanson S, Ku T, Chou C. Assessment of direct ophthalmoscopy teaching using plastic canisters. Med Educ. 2011;45:520–1. doi: 10.1111/j.1365-2923.2011.03987.x. [DOI] [PubMed] [Google Scholar]