

Abstract
Thyroid pathology is characterized by abnormal values of thyroid hormones that can affect the brain and can lead to cognitive impairment (attention, memory, mood), depression and anxiety. The aim of the study is to evaluate the association between the cognitive disorders and thyroid disease and the link between thyroid hormone levels FT4 and TSH in depression and anxiety. We included 130 individuals from Endocrinology Clinic of Craiova, over a period of 6 years (2014-2020), none of whom was taking thyroid medication and antidepressants. The most important symptom found in thyroid pathology is depression, which occurs in those with long-lasting illness. We obtained that 45.38% of the cases were diagnosed with depression and 46.92% with anxiety. Depressive symptoms were assessed with Hamilton scale and anxiety symptoms with the Beck scale. Regarding the impaired cognitive function, we found it in 34.7% of cases of hypothyroidism (loss of memory / lack of concentration) and for the cases with hyperthyroidism, we found changes in 51,42%.
Keywords: Hyperthyroidism, hypothyroidism , depression, anxiety, memory
Introduction
Thyroid pathology is characterized by abnormal values of thyroid hormones that can affect the brain and can lead to cognitive impairment (attention, memory, mood), depression and anxiety [1].
Thyroid hormones play a very important role in the whole body, especially in the brain, where thyroid hormone receptors are found. Thyrotropin and thyroliberin, are involved in neuronal synapses, enhancing synaptic transmission through direct effect, neuromodulator, and indirectly through catecholamines [2].
A particular importance is the diagnosis of disthyroidism started with psychiatric disorders or which aggravates an already existing psychiatric pathology. The frequency of hyper/hypothyroidism among patients with psychiatric pathology is increasing, it is a reason to study them together [3].
Among the most common symptoms in hyperthyroidism are emotional lability, loss of memory, impaired intellect, mood alterations, concentration disorders, panic attacks, loss of concentration capacity, agitation, psychosis [1]. Clinical hypothyroidism is characterized by levels of Thyroid-stimulating hormone (TSH) and low levels of Thyroxine (T4) and Triiodothyronine (T3). There are certain changes in cognitive alibies in hypothyroid patients like memory, anxiety, executive function, attention as well as depression [4].
The most important symptom found in thyroid pathology is depression, which occurs in those with long-lasting illness. Its characteristics are apathy and lethargy and it is also called apathetic thyrotoxicosis [5].
The basis for the development of depression in autoimmune thyroiditis is a pathophysiological mechanisms very well known, immune dysregulation [3].
The mechanism of depression appears to be autoimmune, whether we are talking about dysthyroidism or euthyroidism [4].
Also genes encoding certain neuronal components and neurotrophins are altered by thyroid hormones [5].
Thyroid pathology is characterized by abnormal values of thyroid hormones that can affect the brain and can lead to cognitive impairment (attention, memory, mood), depression and anxiety [6,7].
The severity of clinical symptoms in thyroid pathology appears to be related to the age of the patient, the duration of the disease and the patient’s individual susceptibility to thyroid hormones [8].
The Aim of the Study is to find out if there is an association between the cognitive disorders and thyroid disease and the link between thyroid hormone levels FT4 and TSH in depression and anxiety.
Materials and Methods
Subjects
We included 130 individuals from Endocrinology Clinic of Craiova, over a period of 6 years (2014-2020).
Our patients weren`t treated for depression or thyroid diseases. We observed the values of Thyrotropin (TSH), free thyroxine (FT4), antibodies against thyroperoxidase (TPOAb) and TG (TGAb) for every patient.
The approval and informed consent have been obtained, from each participant. For the conduct of the study we used the principles of the Declaration of Helsinki
Assessment of depression and anxiety
Depressive symptoms were assessed with Hamilton scale and anxiety symptoms with the Beck scale.
The Hamilton Depression Rating Scale is a questionnaire used to diagnose the severity of depression and it is also helpful to evaluate the recovery process.
This Scale use 17 to 21 items, depending of the type and the severity of depression, scored on 3 to 5 point scale.
The most important items are: the depressed mood, anxiety psychic, agitation, loss of weight, feelings of guilty, depersonalization, insomnia, compulsive symptoms.
Interpretation for the 17 items scale is (a er total score indicate a more pronounced degree of depression): the total score between 0-7 indicates normal, 8-17 is frequently associated with mild depression, also a score between 17-25 should be considered moderate depression and a score higher than 25 shows us a severe depression [9].
Beck and his team undertook a sequential analysis of the items that could possibly be included in this instrument from a table of 86 items.
Each item describes a symptom characteristic of anxiety and the subject must assess how much he is bothered by these symptoms on a scale from 0 (not at all) to 3 (very much).
The variation of the score can be between 0-63 and the authors provide certain threshold scores to assess the severity of anxiety: 0-9 should be considered normal or lack of anxiety; a score between 10-18 is frequently associated with mild to moderate anxiety; also a number between 19-29 shows moderate to severe anxiety and range 30-63 is severe anxiety [10].
Biochemical and Hormone Assays
Hormonal and antithyroid antibody dosages were performed using the electrochemoluminescence method (ECLIA).
The limits of the hormonal and antibodies values are: for TSH values, between 0.4-4.0mIU/ml; for FT4 the normal value is between 0.89-1.76ng/dl; also TPOAb must be under 35 IU/ml and TGAb (age<20 years) >115UI/mL.
Through patients with subclinical thyroid dysfunction we understand those patients who had FT4 values within normal limits, in association with the presence of normal TSH values (in cases with subclinical hypothyroidism) or low (present in subclinical hyperthyroidism).
Statistical analysis
The results of the study were analyzed with the SPSS statistical program.
We used the standard deviation to find out the variation of the data compared to the mean value.
According to this deviation, a difference of plus or minus 1 from it will include 68.2% of the total parameters analyzed.
The median was found to be the sum of the patchy distributed values. P's value is considered to be statistically significant when it is <0.05.
Results
We enrolled 130 cases in the study, 50 with hypothyroidism and 80 with hyperthyroidism. (Figure 1).
Figure 1.
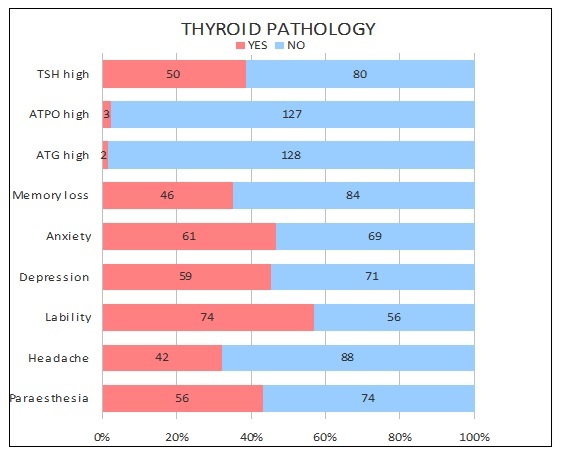
The distribution of cases for patients with thyroid pathology, depending on the presented symptoms
Gender distribution indicates a predominance of female patients in the studied group.
For thyroid pathology, a very percentage of female patients is observed 86.92% (113 cases out of 130), respectively 13.07% men (17 cases).
From the analysis of the environment of origin of the patients analyzed, we note that they come mainly from urban areas.
Thus, it is concluded that 111 out of 130 patients with thyroid impairment come from urban areas (totaling 85.35%).
Mean of TSH values for our patients was 2,24±2,73 and for FT4 was 22,5±13,15.
The mean age was in our study 40,95±13,18 (Table 1).
Table 1.
The descriptive analysis of TSH and FT4 values
|
Statistic |
Age |
FT4 (pmol/l) |
TSH (mUI/ml) |
|
No. of observations |
130 |
130 |
130 |
|
Minimum |
19,00 |
2,00 |
0,01 |
|
1st Quartile |
30,00 |
9,55 |
0,17 |
|
Median |
38,00 |
24,85 |
0,22 |
|
3rd Quartile |
51,00 |
29,00 |
4,98 |
|
Maximum |
72,00 |
50,20 |
9,00 |
|
Mean |
40,95 |
22,50 |
2,24 |
|
Variance (n-1) |
173,84 |
172,83 |
7,44 |
|
Standard deviation (n-1) |
13,18 |
13,15 |
2,73 |
Less than half of the study group for patients with thyroid pathology had elevated levels of TSH (50 cases out of 130 cases with thyroid pathology, amounting to approximately 40%).
It is also noted that only 2 and 3 cases identified increased levels of ATPO and ATG.
In our study emotional lability had the highest percentage (74 cases, 56.92%) and anxiety (46.92%-totaling 61 cases).
These are followed, at a short distance from depression (59 cases-45.38%), paresthesia (56 cases 43.07%) and memory loss (46 cases 35.6%)
The least common manifestation is headache in these patients (35.38%-42 cases) (Figure 1).
After using Hamilton and Beck Scales, we obtained the following results: for depression-71 patients were normal, 38 with mild depression, 13 with moderate depression and 8 patients with severe depression.
For anxiety, we identified 87 patients which were normal, 28 with mild to moderate anxiety, 9 with moderate to severe anxiety and 6 with severe anxiety.
For the patients with hyporthyroidism form this study group was clearly dominated, equally, by the depression and headache (31 cases out of 50, representing 62%). These were followed by the memory loss/lack of concentration in 17 cases (4%) and anxiety in 2 cases (4%).
Regarding the hyperhyroidism, the dominant clinical feature was anxiety (24 cases out of 80-representing 30%), followed by memory loss/lack of concentration (19 cases-23,75%), depression and headache (15 cases each-18.75%) (Figure 2).
Figure 2.
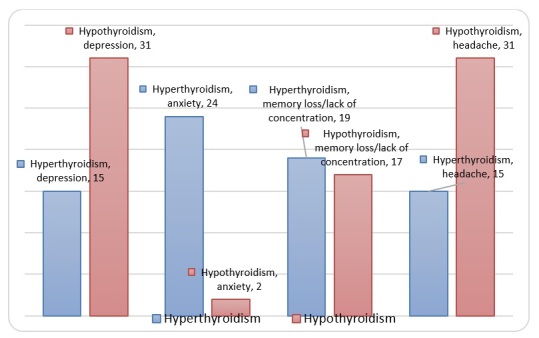
Neuropsychiatric symptoms of hyper/hypothyroidism
In our study, 56% of cases had subclinical hyperthyroidism and only 44% overt hyperthyroidism (Figure 3).
Figure 3.
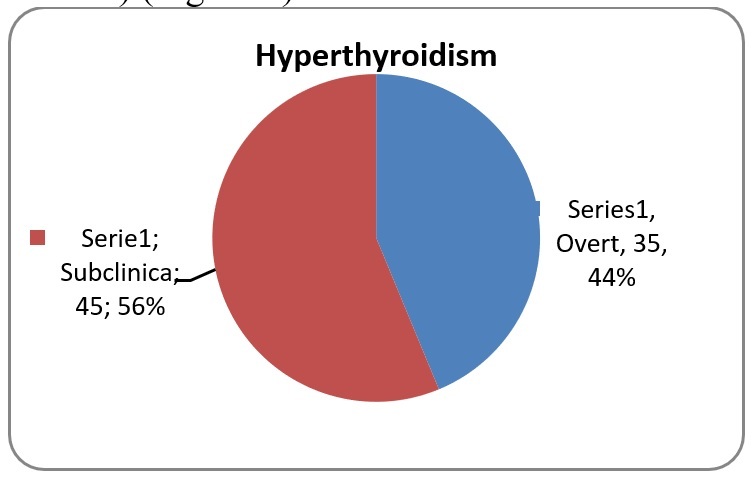
The distribution of cases with hyperthyroidism, depending on the clinical picture
We analyzed in patients with overt and subclinical hypertyroidism anxiety, depression and concentration/memory disorders.
From all cases of subclinical hyperthyroidism, 6.67% of patients presented anxiety.
For the patients with overt hyperthyroidism, we found that it was present in 65.71%.
The difference on anxiety was statistically significant (p<0.0001) (Figure 4).
Figure 4.
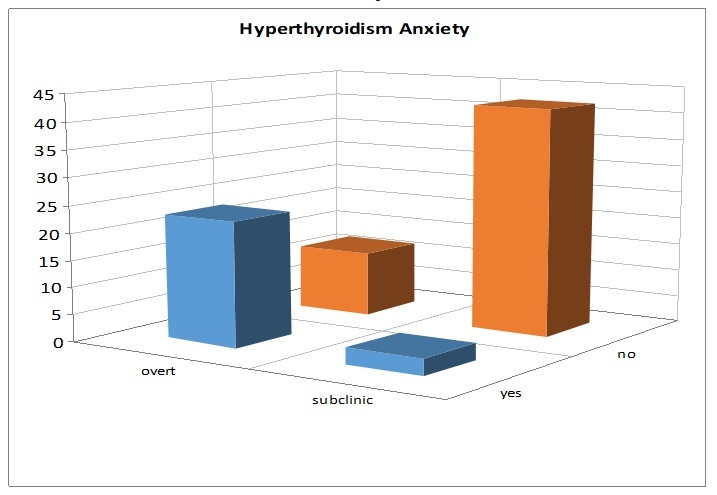
The distribution of anxiety in overt/subclinical hyperthyroidism
Of the 45 cases with subclinical hyperthyroidism, 6.67% presented depression and of the 35 cases with overt hyperthyroidism, 40% had depression.
The difference is statistically significant. (p<0.0184) (Figure 5).
Figure 5.
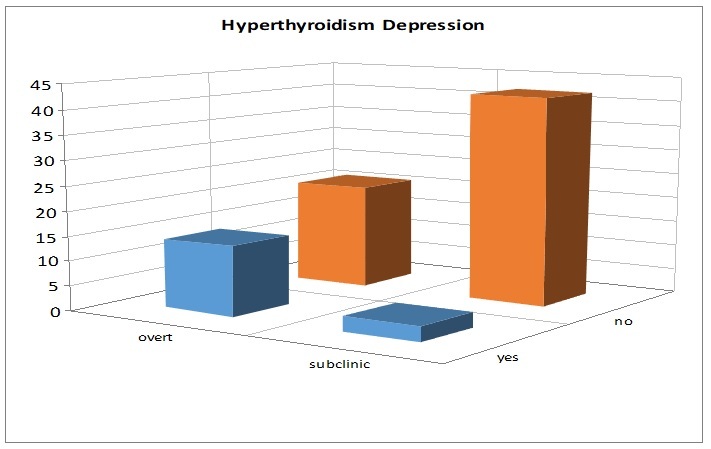
Depression as a symptom in overt/subclinical hyperthyroidism
Memory loss/lack of concentration affected 51.43% from 35 cases with overt hyperthyroidism and 6.67% from 45 cases with subclinical hyperthyroidism.
The difference is statistically significant (p<0.0028) (Figure 6).
Figure 6.
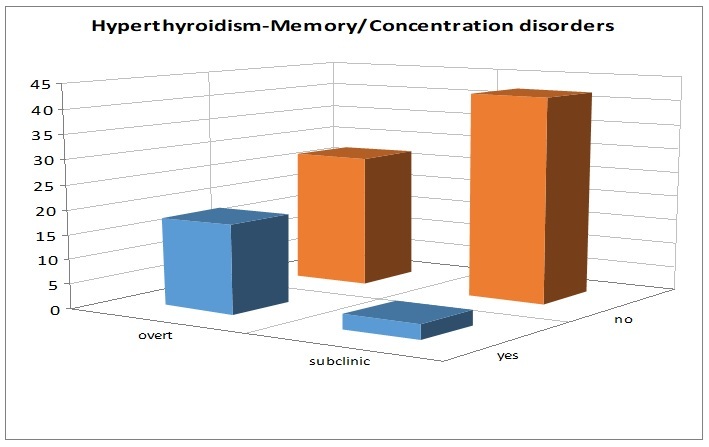
Memory loss/ lack of concentration in Hyperthyroidism
From the 50 cases with hypothyroidism, 30 were overt and 20 were subclinical (Figure 7).
Figure 7.
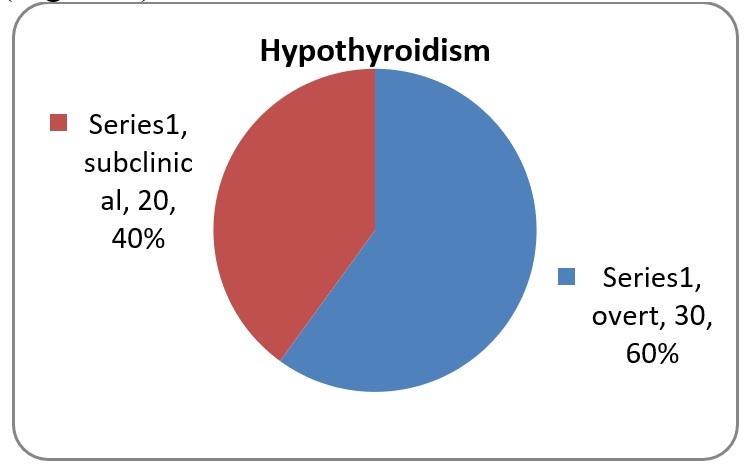
The distribution of cases with hypothyroidism, depending on the clinical picture
The distribution of neuro-psychiatric manifestations in patients with hypothyroidism shows a predominance of depression and memory loss, with a small number of cases with anxiety (Figure 8).
Figure 8.
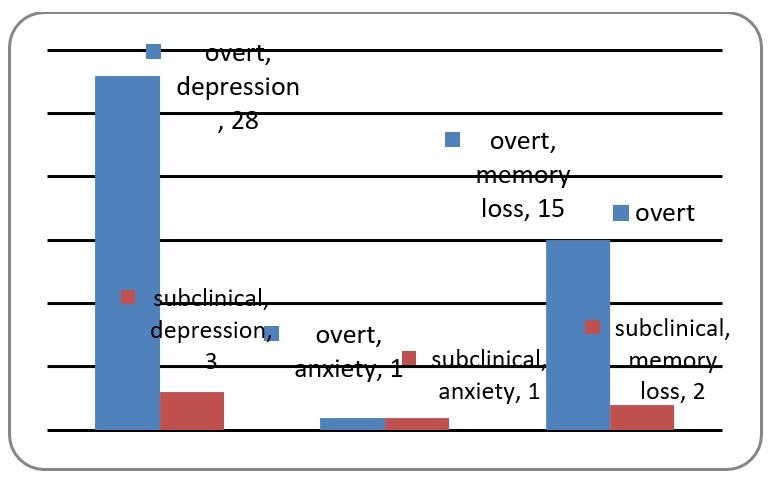
The distribution of neuro-psychiatric manifestations in patients with hypothyroidism
We found 1 case each of anxiety (Figure 9) and 15 cases (43%) of memory loss/lack of concentration in overt hypothyroidism (Figure 10), versus 3 cases each (20%) in subclinical hypothyroidism.
Figure 9.
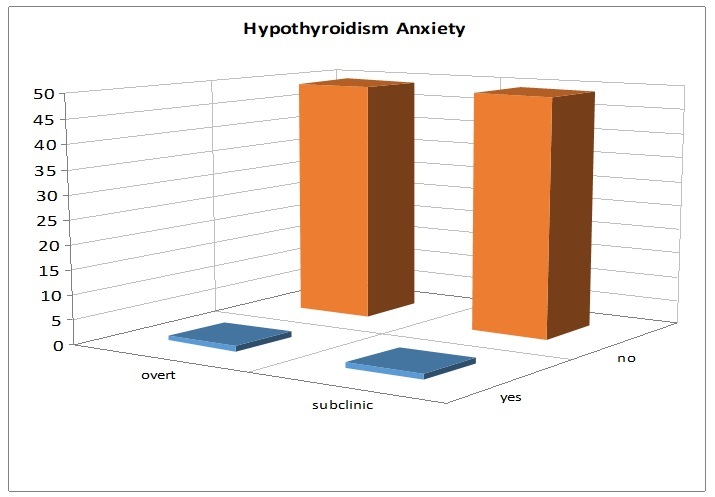
The distribution of anxiety in overt/subclinical hypothyroidism
Figure 10.
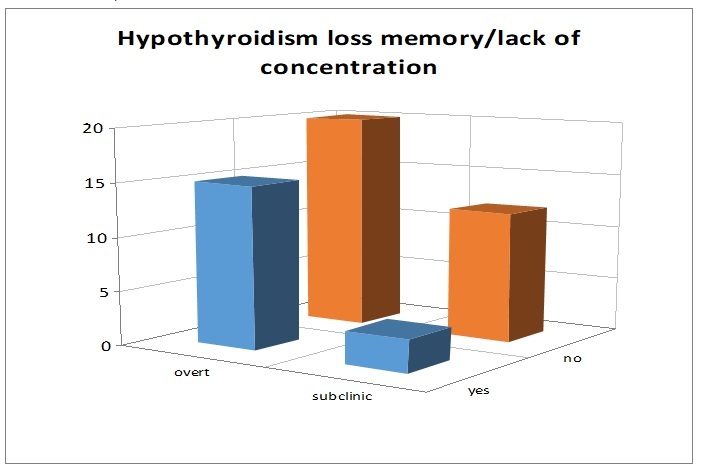
Loss memory/lack of concentration in hypothyroidism
The difference is statistically significant, both for anxiety (p<0.0021) and memory loss (p<0,009).
In our study, we identified 28 cases of depression (80%) in overt hypothyroidism, versus 3 cases (20%) in subclinical hypothyroidism patients (Figure 11).
Figure 11.
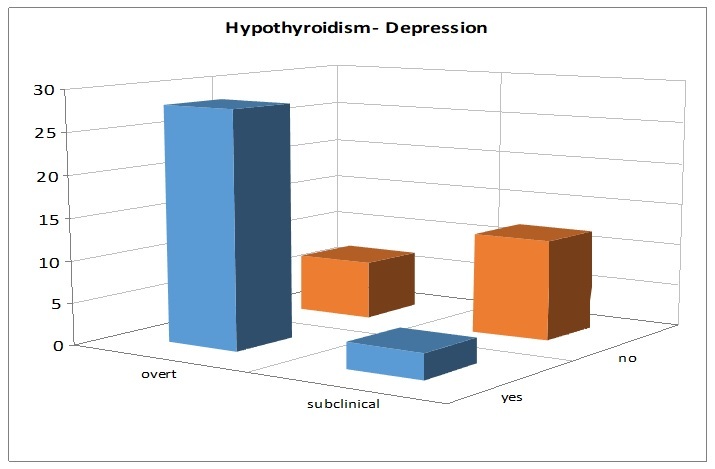
Distribution of depression in Hypothyroidism
The difference is statistically significant (p<0.0034).
Discussion
The connection between the thyroid function and mood is well known for years [11].
Some authors even recognize the link between thyroid diseases and psychiatric pathology like anxiety, depression or abnormal cognitive function [12,13,14].
Others consider thyroid hormones a routine check for every patient with psychiatric disorders [15].
In our study, we examined the neuro-psychiatric symptoms (depression, anxiety, memory loss and lack of concentration) and laboratory abnormalities of thyroid disorders in adults.
We found out that 45.38% of the cases were diagnosed with depression and 46.92% with anxiety. A similar observation was made in a study by Kafle B. and collab. which identified 46.00% cases of depression [16].
Also, Ghorkali B. and collab. found depression in 50.4% of cases and anxiety in 42.6% [14,17].
On the other hand, the same study appreciate that 69.8% of cases were diagnosed with hypothyroid function [13].
In our study, TSH values were lower in 38.46%, while 61.53% were higher.
We observed that the patients with subclinical hyperthyroidism had 6.67% anxiety and same for depression and memory loss/lack of concentration.
For those with overt hyperthyroidism, we found 65.71% anxiety, 40% depression and 51.43% loss of memory/lack of attention.
P values were statistically significant each time.
Also, we observed patients with subclinical hypothyroidism and we found that 20% had anxiety and same for depression and memory loss/lack of concentration.
For those with overt clinical picture, 43% had anxiety and memory loss/lack of concentration, 80% depression.
P value was statistically significant each time.
Another study by Bahls S-C and de Carvalho G.A. confirms the laboratory changes in patients with hypotalamus-pituitary-thyroid axis abnormalities.
They notified that the patients diagnosed with depression had er T4 levels and that the response of TSH to TRH was inappropriate for these patients [17].
Other studies show that depression was observed in 64% in patient’s hypothyroidism [18] and in 63% of cases with hyperthyroidism [19] plus impaired cognitive function in 37% of cases [20].
According to the latest studies [21], thyroid hormones protect the brain areas involved in learning and memory. In a clinical trial by Boxtel and collab., they observed that an elevated TSH level is linked with an inappropriate memory performance [22].
Also, Rivas R. and Naranjo J.R. noted that the abnormalities in the thyroid gland function will lead to changes of behavioral changes, memory and neurological changes [13].
Regarding the impaired cognitive function, we found it in 34.7% of cases of hypothyroidism (loss of memory/lack of concentration) and for the cases with hyperthyroidism, we found changes in 51,42%.
According to Samuels M., the significant changes in cognitive function are improved after the patients are diagnosed and receive treatment [12].
This was proved by a clinical trial from 2006 [23] which shows that it has been a significant improvement of verbal memory after 3 months of treatment in patients with hypothyroidism.
Conclusion
Hypo and hyperthyroidism occupy a well-deserved place among endocrinological conditions because they are not rare and because of their frequent association with symptoms like anxiety and depression.
Regarding patients with anxiety, this may be the only one of the symptoms of a subclinical disease, but which could have a particular impact on the patient.
For this reason, it is required to evaluate all this patients, ensuring that the clinical examination is correct and complete.
Since the time of onset of thyroid disease, clinical manifestations are not suggestive for diagnosis and patients are referred to psychiatric/neurology services, where is establishing the symptomatic treatment, we considered useful to know these feature deduct to guide patients to a endocrinology service for etiological treatment.
Conflict of interests
None to declare.
Glossary
ABBREVIATIONS
- TSH
Thyroid-stimulating hormone
- T4
thyroxine
- T3
triiodothyronine
- TPOAb
antibodies against thyroperoxidase (TPOAb)
- TGAb
antibodies againstthyroglobulin (TGAb)
- SD
standart deviation
References
- 1.Gibney SM, Drexhage HA. Evidence for a dysregulated immune system in the etiology of psychiatric disorders. J Neuroimmune Pharmacol. 2013;8(4):900–920. doi: 10.1007/s11481-013-9462-8. [DOI] [PubMed] [Google Scholar]
- 2.Apostol M, Keeran M, Klempf N, McCoskey V, Ernst AA, Weiss SJ, Sarangarm D. Thyroid stimulating hormone testing in ED evaluation of patients with atrial fibrillation and various psychiatric diagnoses. Am J Emerg Med. 2019;37(6):1114–1117. doi: 10.1016/j.ajem.2018.08.076. [DOI] [PubMed] [Google Scholar]
- 3.Fardella C, Gloger S, Figueroa R, Santis R, Gajardo C, Salgado C, Barroilhet S, Foradori A. High prevalence of thyroid abnormalities in a Chilean psychiatric outpatient population. J Endocrinol Invest. 2000;23(2):102–106. doi: 10.1007/BF03343687. [DOI] [PubMed] [Google Scholar]
- 4.Davis JD, Tremont G. Impact of frontal systems behavioral functioning in dementia on caregiver burden. J Neuropsychiatry Clin Neurosci. 2007;19(1):43–49. doi: 10.1176/appi.neuropsych.19.1.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bauer M, Szuba MP, Whybrow PC. In: Psychoneuroendocrinology: The scientific basis of clinical practice. Wolkowitz OM, Rothschild AJ, editors. Washington: American Psychiatric Publishing; 2003. Psychiatric and behavioral manifestations of hyperthyroidism and hypothyroidism; pp. 419–444. [Google Scholar]
- 6.Kirim S, Keskek SO, Köksal F, Haydardedeoglu FE, Bozkirli E, Toledano Y. Depression in patients with euthyroid chronic autoimmune thyroiditis. Endocr J. 2012;59(8):705–708. doi: 10.1507/endocrj.ej12-0035. [DOI] [PubMed] [Google Scholar]
- 7.Bauer M, London ED, Silverman DH, Rasgon N, Kirchheiner J, Whybrow PC. Thyroid, brain and mood modulation in affective disorder: insights from molecular research and functional brain imaging. Pharmacopsychiatry. 2003;36(Suppl 3):S215–221. doi: 10.1055/s-2003-45133. [DOI] [PubMed] [Google Scholar]
- 8.Educatie Medicala Continua, 2004, Tulburări endocrine asociate bolilor psihice [Online] Available from: http://www.emcb.ro/article.php?story=20050201164157553 [ Accessed 01.04.2021]
- 9.Suflet linistit, 2017, Scala de depresie Hamilton [Online] Available from: www.suflet-linistit.ro/scala-de-depresie-hamilton/[ Accessed 14.03.2021]
- 10.Suflet linistit, 2017, Inventar de depresie beck test profesional [Online] Available from: www.suflet-linistit.ro/inventar-de-depresie-beck-test-profesional/[ Accessed 14.03.2021]
- 11.Yuan L, Zhang Y, Luan D, Xu X, Yang Q, Zhao S, Zhou Z. Reversible Affective Symptoms and Attention Executive Control Network Impairment Following Thyroid Function Normalization in Hyperthyroidism. Neuropsychiatr Dis Treat. 2019;15:3305–3312. doi: 10.2147/NDT.S227386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Samuels MH. Thyroid disease and cognition. Endocrinol Metab Clin North Am. 2014;43(2):529–543. doi: 10.1016/j.ecl.2014.02.006. [DOI] [PubMed] [Google Scholar]
- 13.Rivas M, Naranjo JR. Thyroid hormones, learning and memory. Genes Brain Behav. 2007;6(Suppl 1):40–44. doi: 10.1111/j.1601-183X.2007.00321.x. [DOI] [PubMed] [Google Scholar]
- 14.Gorkhali B, Sharma S, Amatya M, Acharya D, Sharma M. Anxiety and Depression among Patients with Thyroid Function Disorders. J Nepal Health Res Counc. 2020;18(3):373–378. doi: 10.33314/jnhrc.v18i3.2499. [DOI] [PubMed] [Google Scholar]
- 15.Dickerman AL, Barnhill JW. Abnormal thyroid function tests in psychiatric patients: a red herring? Am J Psychiatry. 2012;169(2):127–133. doi: 10.1176/appi.ajp.2011.11040631. [DOI] [PubMed] [Google Scholar]
- 16.Kafle B, Khadka B, Tiwari ML. Prevalence of Thyroid Dysfunction Among Depression Patients in a Tertiary Care Centre. JNMA J Nepal Med Assoc. 2020;58(229):654–658. doi: 10.31729/jnma.5296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bahls SC, Carvalho GA. The relation between thyroid function and depression: a review. Braz J Psychiatry. 2004;26(1):41–49. doi: 10.1590/s1516-44462004000100012. [DOI] [PubMed] [Google Scholar]
- 18.Moreau T, Manceau E, Giroud-Baleydier F, Dumas R, Giroud M. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18(10):687–689. doi: 10.1046/j.1468-2982.1998.1810687.x. [DOI] [PubMed] [Google Scholar]
- 19.Gold MS, Pottash AL, Extein I. Hypothyroidism and depression. Evidence from complete thyroid function evaluation. JAMA. 1981;245(19):1919–1922. doi: 10.1001/jama.245.19.1919. [DOI] [PubMed] [Google Scholar]
- 20.Monzani F, Del Guerra P, Caraccio N, Pruneti CA, Pucci E, Luisi M, Baschieri L. Subclinical hypothyroidism: neurobehavioral features and beneficial effect of L-thyroxine treatment. Clin Investig. 1993;71(5):367–371. doi: 10.1007/BF00186625. [DOI] [PubMed] [Google Scholar]
- 21.Accorroni A, Chiellini G, Origlia N. Effects of Thyroid Hormones and their Metabolites on Learning and Memory in Normal and Pathological Conditions. Curr Drug Metab. 2017;18(3):225–236. doi: 10.2174/1389200218666170116112407. [DOI] [PubMed] [Google Scholar]
- 22.van Boxtel MP, Menheere PP, Bekers O, Hogervorst E, Jolles J. Thyroid function, depressed mood, and cognitive performance in older individuals: the Maastricht Aging Study. Psychoneuroendocrinology. 2004;29(7):891–898. doi: 10.1016/j.psyneuen.2003.08.002. [DOI] [PubMed] [Google Scholar]
- 23.Miller KJ, Parsons TD, Whybrow PC, van Herle K, Rasgon N, van Herle A, Martinez D, Silverman DH, Bauer M. Memory improvement with treatment of hypothyroidism. Int J Neurosci. 2006;116(8):895–906. doi: 10.1080/00207450600550154. [DOI] [PubMed] [Google Scholar]