

Abstract
Introduction: SARS-CoV-2 primarily affects a person's respiratory system and leads to the spread of pathogenicity in the person and therefore this study evaluated the Case Fatality Rate (CFR) and Basic Reproductive Rate (R-naught) of COVID-19. Method: This cross-sectional descriptive study was performed on all people with COVID-19 from the first date of admission of positive PCR patients with SARS-CoV-2 until September 21, 2020, in the area of Markazi Province in Khomein, Iran. Information on the records of definitively discharged and deceased patients due to COVID-19 (having positive PCR) was extracted from 20/2/2020 to 21/9/2020, and Case Fatality Rate (CFR) and Basic Reproductive Rate (R-naught) of COVID-19 were evaluated. The sample size was 691 people. Results: The CFR of the COVID-19 in the current study is 6.65%, and the rate of disease transmission among the sensitive population of Khomein city at the beginning of the study (March) averaged BASIC REPRODUCTIVE RATE= 1.75, and in the last month (September) of the study This value was reduced to BASIC REPRODUCTIVE RATE= 1.306. Conclusion: According to our study on Case Fatality Rate (CFR) and Basic Reproductive Rate (R-naught) of COVID-19, showed that the prevalence of the disease was high in March, which due to lack of proper observance of health protocols, we saw this problem and in the months when people have more problems. Hygiene was reduced, and the rate of transmission and mortality was reduced.
Keywords: SARS-CoV-2, COVID-19, CFR, R-naught
Introduction
Coronavirus 2 is a newfound virus that has caused a great deal of damage and loss of life since its introduction into human societies (with the identification of the first cases in December 2019), which has become a global health concern in general [1,2,3].
Coronavirus is one of the most important pathogens that primarily affects the human respiratory system, including Acute Respiratory Syndrome (SARS)-CoV and Middle East Respiratory Syndrome (MERS)-CoV, which have previously been identified as threatening factors for they were known for their general human health [4].
Some cases of unknown pneumonia that cause were observed in Wuhan, China In December 2019. These cases increased in the coming days and leading to the identification of new human coronavirus from patients. The number of cases and deaths in this part of China increased sharply during July, leading to the virus's introduction as a disease of global concern and concern for the World Health Organization (WHO) [5,6].
In humans, primary coronavirus infections affect the upper respiratory tract and gastrointestinal tract and range from mild and self-limiting infections to severe manifestations such as bronchitis and pneumonia, and renal involvement [7].
Primary symptoms of COVID-19 include fever, cough, dizziness, hemoptysis, hypoxia, dyspnea, lymphopenia, sore throats, rhinorrhea, ARDS, and even heart damage [4,8].
Ways to confronting the outbreak of COVID-19 focused on identifying the treatment and isolation of infected people, tracking and quarantining their close contacts, reducing travel and avoiding undercooked meat, and promoting public participation in breaking the transmission chain that Has been announced [9,10].
Supportive therapies such as oxygen therapy, plasma therapy, Antivirus drugs, and Corticosteroids are also used to treat the symptom of this disease [8].
In the field of health planning, it is essential to pay attention to the amount Case Fatality Rate (CFR) of COVID-19 [11], which in some countries varies from 0 to 8.9%, and the issue of CFR can even indicate economic conflicts in some countries [12].
The Case Fatality Rate (CFR) is an Index that shows the fatality of the disease and includes only the ratio of deaths to patients identified. This rate is used in describing the mortality process and its overall changes, deciding on health priorities, allocating resources, designing intervention programs, and evaluating and refining problems and programs related to public health and the epidemic of disease. Emerging companies can greatly frighten the community if their levels are reported to be high. In Iran and many countries, interpretations were made based on CFR at the beginning or in the middle of the COVID19 epidemic. It was based on various judgments about health systems. On the other hand, the new coronavirus epidemic is more widespread in humans than in previous coronaviruses, which indicates the too high transmission power of this virus. However, the mortality rate from the new coronavirus is much lower than other coronaviruses [13].
A critical component associated with virus transmission is the Basic Reproductive Rate (R-naught). The R-naught is equal to the average number of people at risk of contracting the disease, and the people are not immunized against the virus. Depending on the R-naught, there are three possibilities for the spread or reduction of the disease: A) When the R-naught is less than one, which means the infection causes less than one productive infection. In these cases, this component indicates that the disease Is decreasing. B) When R-naught is equal to one, that it means that the disease has reached relative stability, and C) When R-naught is greater than one, it means that the disease is spreading [14].
According to the explanations provided and the fact that the SARS-CoV-2 has caused an emerging disease, this study evaluated the Case Fatality Rate (CFR) and Basic Reproductive Rate (R-naught) of COVID-19.
Method
This study is a cross-sectional descriptive performed on all people with COVID-19 from the first date of admission until the end of September 2020. In this way, after receiving the ethical code of Khomein University of Medical Sciences (IR.KHOMEIN.REC.1399.004), the information of patients with positive PCR test received and this information was extracted from 20/2/2020 to 21/9/2020 that include the Case Fatality Rate (CFR) and R-naught (R-naught) of COVID-19 The range of age in this study included all age groups, each of which was analyzed separately. The information in the file of each patient was recorded in the relevant checklist and finally analyzed. After collecting data, they were analyzed using descriptive statistics (mean, standard deviation, frequency distribution charts, and tables, disease distribution map) and analytical statistics (independent t-test and chi-square test) by SPSS software version 23. The p-value (p <0.05) was considered as a level of significance. All patient information was confidential and Helsinki ethics were followed at all stages. The sample size was 691 people.
The value of R-naught in the present study was calculated using RStudio software, so that the information of all definite cases (positive PCR) with corona were entered into the software separately each month and then estimated based on specific packages for estimating R and specific commands of this index. The desired was done to calculate the Case Fatality Rate, we were divided the number of deaths due to Covid-19 that had PCR positive by the total number of PC-positive cases and the desired value was obtained. Thus, to estimate CFR by age groups from PCR positive death cases, we used the group of age divided by the number of cases in the same group of age.
Results
Evaluation of Case Fatality Rate (CFR)
The overall Case Fatality Rate of the COVID-19 in the current study is 6.65%, which is 9.09% in men, 5.04% in women, 21.2% in hospitalized patients, 4.35% in urban patients, and 12.9% in rural residents. The highest CFR of the COVID-19 among age groups in both genderes, attributed to the age group of over 90 years, is 33.3% (Table 1).
Table 1.
The Case Fatality Rate of the COVID-19 by Age Groups in both genders
|
Age Groups (year) |
Case Fatality Rate (CFR) (%) |
|
0-9 |
0 |
|
10-19 |
0 |
|
20-29 |
0.85 |
|
30-39 |
0.46 |
|
40-49 |
1.34 |
|
50-59 |
5.62 |
|
60-69 |
8.69 |
|
70-79 |
17.05 |
|
80-89 |
27.90 |
|
=>90 |
33.33 |
Basic Reproductive Rate (R-naught)
The prevalence of the COVID-19 among the susceptible population of Khomein city at the beginning of the study (March) averaged Basic Reproductive Rate=1.745, which varies in different months of the epidemic period according to people's social behaviors and biological characteristics of the virus. Respectively, the R-naught rate in April, May, June, July, August, and September were Basic Reproductive Rate=1.435, Basic Reproductive Rate=1.456, Basic Reproductive Rate=1.15, Basic Reproductive Rate=1.135, Basic Reproductive Rate=1.099, and Basic Reproductive Rate=1.306 (Figure 1).
Figure 1.
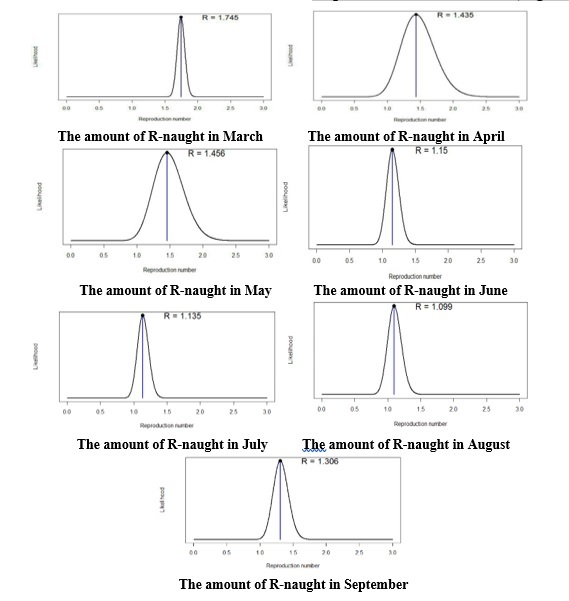
Amount of R-naught (Basic Reproductive Rate) in a variety of months
Discussion
This study aimed to evaluate patients with COVID-19 in Khomein city, which is part of Markazi province in Iran country. According to the results of our study, the Case Fatality Rate (CFR) of COVID-19 was reported to be 6.65%, which according to the results of Tavakoli et al., in their review study in 2020, including, the results are close and similar to this value (4.4) [15].
According to the results obtained from Jiabao Xu et al., the CFR was 9.6 in SARS [16].
According to another research conducted by Awaidy et al. in 2019, it was found that the CFR of the coronavirus is similar to MERS (35.2%), which can be concluded that the CFR of the virus in MERS was significantly more than coronavirus and SARS mortality [17].
According to the study of Yan-Ni-Mi et al., the amount of Case Fatality Rate in China about COVID-19 except Hubei Province was 0.5% to 3.4% in the early stage from February 15 to March 25 [18].
In our study, the CFR rate in women and men was 5.04% and 9.09, respectively. According to the study of Asirvatham et al., the CFR in people over 60 years showed a significant increase, and in women as well, the CFR has been reported less than men, and having underlying diseases has been associated with an increase in the CFR and in general these results are consistent with our study [19].
According to the results of this study, we did not see any mortality in 0 to 19 years. The higher the age, the Case Fatality Rate, according to the patient's clinical condition, such as underlying diseases and old age, was also increasing, which is more reported in the age group over 90 years. These results are consistent with Rahmanian et al. that the CFR in 80-year-olds was reported 14.8% [20].
According to another research conducted by Leiwen Fu et al. in 2020, the total approximation of the Case Fatality Rate was 3.6% (1.1-7.2) and the proportion of severe cases was 25.6% (17.4-34.9) respectively. CFR and laboratory abnormalities were higher in severe cases, but there was no difference in CFR in terms of gender [21].
In another study by Morteza Abdullatif Khafaie, Case Fatality Rate of Italy, the highest of all countries studied for both time points (on March 12, 6.22% versus March 23, 9.26%). The data showed that even though Italy was the only European country reported on March 12, France and Spain had the highest CFR of 4.21% and 6.16% respectively, on March 23, which was strikingly higher than the overall CFR of 3.61%. According to the amounts of CFR in our present study, they are consistent with the results of this study [22].
However, in another study conducted by Pooja Mahajan et al. in 2020, the amounts of CFR per total cases in India were 11.00% and per closed cases is 76.72%, which indicates that the recovery rate of COVID-19 is more than the fatality rate in India [23].
The mysterious SARS-CoV-2 has significant contagious and epidemic power like other similar factors such as SARS and MERS [14,15].
The SARS-CoV-2 Basic Reproductive Rate (R-naught) in our study, which was conducted, was reported to be 1.745 (in March (First month of appearance of this virus) that prevalence was high due to insufficient knowledge of SARS-CoV-2. It means that the virus is spreading and contagious and is consistent with the results of a study by Chih-Cheng Lai et al., which can be considered pandemic [1].
However, in Ying Liu's study, the coronavirus transmission rate was higher than in our study (3.28), which may be justified by the larger sample size in Liu's study than in our study [14].
In the study, Xiao Et al. reported an average R-naught was 2.24 to 3.54, which is higher than our study. The mean Basic Reproductive Rate ranges due to the larger population in China, which naturally has a relatively high R-naught [25].
Because the contagion rate of this virus is related to the observance of hygiene and health protocols, in the months when people used personal protective equipment and hygienic principles, the Reproductive Rate (R-naught) was also lower.
Conclusion
According to our study on Case Fatality Rate (CFR) and Basic Reproductive Rate (R-naught) of COVID-19, showed that prevalence of the disease was high in March, which due to lack of proper observance of health protocols, we saw this problem and in the months when people have more problems.
Hygiene was reduced, and the rate of transmission and mortality was reduced.
The most important strategy for prevention and control of coronavirus is early detection of symptomatic people and timely separation of patients and quarantine of people in contact with the patient.
This is done in Khomein city by health forces in city bases and health houses in cooperation with security forces and entrance to the cities was severely restricted and symptomatic people were prevented from leaving, and people who did not have the facilities and equipment for isolation at home were either referred to a hospital and placed in a convalescent home, thus preventing the spread of the disease in the community and consequently the increase in R-naught was prevented.
Conflict of interests
None to declare.
Acknowledgments
Acknowledgments
The authors would like to appreciate the health center and Imam Khomeini Hospital in Khomein University of Medical Sciences and all the respected colleagues who helped us in this study.
In our study attempted to observe the provisions of ethical codes related to research.
Funding
The funding of this study was from Khomein University of Medical Sciences, Khomein, Iran (No: 99000001).
References
- 1.Lai Ch-Ch, Shih T-P, Ko W-Ch, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19) The epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924–105924. doi: 10.1016/j.ijantimicag.2020.105924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yang P, Li D, Zhao D. Coronavirus Virus Disease 2019, a growing threat to children. J Infect. 2020;80:684–686. doi: 10.1016/j.jinf.2020.02.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zu ZY, Jiang MD, Xu PP, Chen W, Ni QQ, Lu G, Zhang LJ. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology. 2020;296(2):E15–E25. doi: 10.1148/radiol.2020200490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rothan HA. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433–102433. doi: 10.1016/j.jaut.2020.102433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lu H, Tang YW. Outbreak of Pneumonia of Unknown Etiology in Wuhan China: the Mystery and the Miracle. J Med Virol. 2020;92(4):401–402. doi: 10.1002/jmv.25678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Biscayart C, Angeleri P, Lloveras S, Chaves TdSS, Schlagenhauf P, Rodríguez-Morales AJ. The next big threat to global health? 2019 novel coronavirus (2019-nCoV): What advice can we give to travellers?–Interim recommendations January 2020, from the Latin-American society for Travel Medicine (SLAMVI) Travel Med Infect Di. 2020;33:101567–101567. doi: 10.1016/j.tmaid.2020.101567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wevers BA, van der Hoek L. Recently discovered human coronaviruses. Clin Lab Med. 2009;29(4):715–724. doi: 10.1016/j.cll.2009.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Geng Y-J, Wei Z-Y, Qian H-Y, Huang J, Lodato R, Castriotta RJ. Pathophysiological characteristics and therapeutic approaches for pulmonary injury and cardiovascular complications of coronavirus disease 2019. Cardiovasc Pathol. 2020;47:107228–107228. doi: 10.1016/j.carpath.2020.107228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Smith RD. Responding to global infectious disease outbreaks: lessons from SARS on the role of risk perception, communication and management. Soc Sci Med. 2006;63(12):3113–3123. doi: 10.1016/j.socscimed.2006.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sohrabi C, Alsafi Z, O'Neill N, Khan M, Kerwan A, Al-Jabir A, Iosifidis Ch, Agha R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19) Int J Surg. 2020;76:71–76. doi: 10.1016/j.ijsu.2020.02.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Asfahan S, Shahul A, Chawla G, Dutt N, Niwas R, Gupta N. Early trends of socio-economic and health indicators influencing case fatality rate of COVID-19 pandemic. Monaldi Arch Chest Dis. 2020;90(3):451–457. doi: 10.4081/monaldi.2020.1388. [DOI] [PubMed] [Google Scholar]
- 12.Wong JY, Kelly H, Cheung C-MM, Shiu EY, Wu P, Ip KM, Ni MY, Cowling BJ. Hospitalization fatality risk of influenza A (H1N1) pdm09: a systematic review and meta-analysis. Am J Epidemiol. 2015;182(4):294–301. doi: 10.1093/aje/kwv054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rajgor DD, Lee MH, Archuleta S, Bagdasarian N, Quek SC. The many estimates of the COVID-19 case fatality rate. Lancet Infect Dis. 2020;20(7):776–777. doi: 10.1016/S1473-3099(20)30244-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. 2020;27(2):1–4. doi: 10.1093/jtm/taaa021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tavakoli A, Vahdat K, Keshavarz M. Novel coronavirus disease 2019 (COVID-19): an emerging infectious disease in the 21st centur. ISMJ. 2020;22(6):432–450. [Google Scholar]
- 16.Xu J, Zhao S, Teng T, Abdalla AE, Zhu W, Xie L, Wang Y, Guo X. Systematic comparison of two animal-to-human transmitted human coronaviruses: SARS-CoV-2 and SARS-CoV. Viruses. 2020;12(2):244–244. doi: 10.3390/v12020244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Al Awaidy ST, Khamis F. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in Oman: Current Situation and Going Forward. Oman Med J. 2019;34(3):181–181. doi: 10.5001/omj.2019.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mi Y-n, Huang T-t, Zhang J-x, Qin Q, Gong Y-x, Liu S-y, Xue H-m, Ning C-h, Cao L, Cao Y-x. Estimating the instant case fatality rate of COVID-19 in China. Int J Infect Dis. 2020;97:1–6. doi: 10.1016/j.ijid.2020.04.055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Asirvatham ES, Lakshmanan J, Sarman CJ, Joy M. Demystifying the varying case fatality rates (CFR) of COVID-19 in India: Lessons learned and future directions. J Infect Dev Ctries. 2020;14(10):1128–1135. doi: 10.3855/jidc.13340. [DOI] [PubMed] [Google Scholar]
- 20.Rahmanian V, Rabiee MH, Sharifi H. Case fatality rate of coronavirus disease 2019 (COVID-19) in Iran-a term of caution. Asian Pacific Journal of Tropical Medicine. 2020;13:1–3. [Google Scholar]
- 21.Fu L, Wang B, Yuan T, Chen X, Ao Y, Fitzpatrick T, Li P, Zhou Y, Lin y-F, Duan Q, Luo G, Fan S, Lu y, Feng A, Zhan Y, Liang B, Cai W, Zhang L, Du X, Li L, Shu Y, Zou H. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J Infect. 2020;80(6):656–665. doi: 10.1016/j.jinf.2020.03.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Khafaie MA, Rahim F. Cross-Country Comparison of Case Fatality Rates of COVID-19/SARS-COV-2. Osong Public Health Res Perspect. 2020;11(2):74–80. doi: 10.24171/j.phrp.2020.11.2.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mahajan P, Kaushal J. Epidemic Trend of COVID-19 Transmission in India During Lockdown-1 Phase. J Community Health. 2020;45(6):1291–1300. doi: 10.1007/s10900-020-00863-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. 2020;27(2):1–4. doi: 10.1093/jtm/taaa021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zhao S, Lin Q, Ran J, Musa SS, Yang G, Wang W, Lou Y, Gao D, Yang L, He D, Wang MH. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. Int J Infect Dis. 2020;92:214–217. doi: 10.1016/j.ijid.2020.01.050. [DOI] [PMC free article] [PubMed] [Google Scholar]