

Abstract
Dentigerous cysts are seen in the maxillary canine and third molars. We report a case of dentigerous cysts invading the maxillary sinus, which was managed surgically by endoscopic‐assisted transantral and transnasal approach.
Keywords: dentigerous cyst, endoscopic transantral approach, maxillary sinus
Combined endoscopic‐endonasal approach may be a good method for dentigerous cysts at unusual locations.

1. INTRODUCTION
Dentigerous cysts are the second most common odontogenic cyst after radicular cysts. They are benign in nature and result when fluid accumulates in the space between the reduced enamel epithelium and the crown of the unerupted tooth. The most common location of dentigerous cysts is the third molars of the mandible (70%). 1 Other locations include maxillary third molar and canines. The unerupted tooth, circumvented by the cyst, is often displaced into ectopic positions in the maxillofacial region. When the cyst occurs in the maxilla or upper jaw region, the impacted tooth is often displaced and/or shifted into the maxillary sinus. 2 However, dentigerous cysts invading into maxillary sinus are rare.
The surgical modalities for treatment of maxillary sinus pathologies have changed in recent years. While the radical Caldwell‐Luc approach used to be the standard approach for procedures in the maxillary sinus, it has gradually been replaced by functional endoscopic sinus surgery. 3 Endoscopic‐endonasal middle meatal antrostomy can be used to treat most maxillary pathologies. However, it is difficult to resect huge dentigerous cysts via the endonasal corridor, particularly when there is an impacted tooth involved. A better approach, in such circumstances, might be an endoscopic‐assisted transantral approach coupled with an endonasal approach. A transantral approach allows for easier instrument maneuvering and complete cyst removal while concomitant endonasal approach provides enhanced visualization of the surgical area ensuring complete removal leading to prevent recurrence. Sometimes, dentigerous cyst recurs, leading to contour deformity if not properly removed. We report a case of huge dentigerous cyst of the right maxillary sinus treated concomitantly by both endoscopic transantral and endonasal approaches.
2. CASE REPORT
2.1. Initial presentation
A 10‐year‐old female patient presented with progressively increasing swelling of the right nasofacial region for one month at the Department of Otorhinolaryngology and Head and Neck Surgery (ORL‐HNS) of Gandaki Medical College, a tertiary care hospital in western Nepal. There was no history of pain, fever, or discharge from overlying skin. Our patient denied numbness, tingling, and paresthesia over her face. There was no blurring of vision or diplopia. Patient denied difficulty with mastication and swallowing. She also denied any history of trauma to the face. (Figure 1).
FIGURE 1.
Gross examination showing swelling of right facial region
2.2. Assessment and evaluation
On inspection, her face was asymmetric with diffuse swelling on the right side. Nasal endoscopy shows normal finding at nasal cavity. Computed tomography (CT) scan of nose and paranasal sinus showed a well‐circumscribed cystic lesion around the crown of an unerupted tooth occupying most of the right maxillary sinus. Additional findings included a polypoidal lesion supero‐medially and mucosal thickening infero‐medially within the maxillary sinus, and nasal septum deviation to the left side. (Figure 2) An endoscopic transantral alongside an endoscopic‐endonasal approach surgery under general anesthesia was recommended for excision of the right maxillary sinus dentigerous cyst.
FIGURE 2.
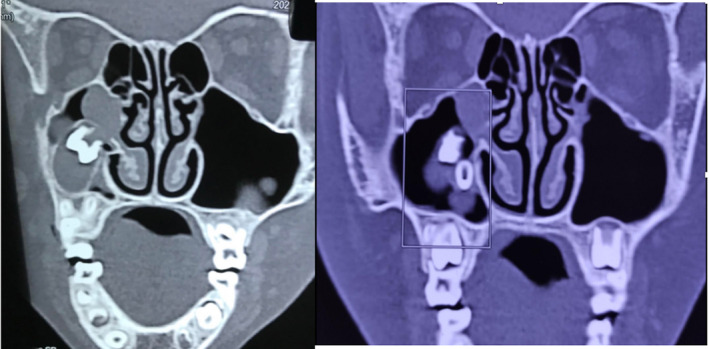
Computed tomography scan of paranasal sinus showing dentigerous cyst in the right maxillary sinus (shown by Arrow and inside box)
2.3. Surgical procedure
Patient was kept in the supine position with the head in neutral position. Endotracheal intubation was performed. Nose was packed with 1:80000 xylocaine with adrenaline for 5 min. After full decongestion of the nose, 0‐degree sinoscope was used to visualize nasal cavity. Local anesthesia was injected at the uncinate process. Uncinectomy was performed, and the middle meatus was widened. For transantral approach, 1 cm incision was made in the upper gingivolabial groove above the canine teeth right side. The upper and lower flaps were retracted. The anterior wall of the maxillary sinus at canine fossae was opened by drilling, but care must be taken not to injure the infraorbital nerve cranially or the tooth bud caudally. A 0‐degree sinuscope was inserted, and maxillary sinus visualized.
After opening of maxillary sinus through transantral approach, we inserted endoscope and instrument either transantral and transnasal endoscopic approach or vice‐versa and both approaches were used to dissect and visualize the dentigerous cyst. (Figure 3) The dentigerous cyst was completely separated from the mucosa of maxillary sinus and removed via the transantral route. The maxillary sinus was then packed with ribbon gauze impregnated with antibiotics. The gingivolabial incision from the transantral approach was sutured in layers with Vicryl 3–0. The maxillary sinus packing was removed postoperative day 3. The postoperative period was uneventful. Histopathology report consists of dentigerous cyst wall with tooth. (Figure 4) The patient was in complete remission at one‐year follow‐up.
FIGURE 3.
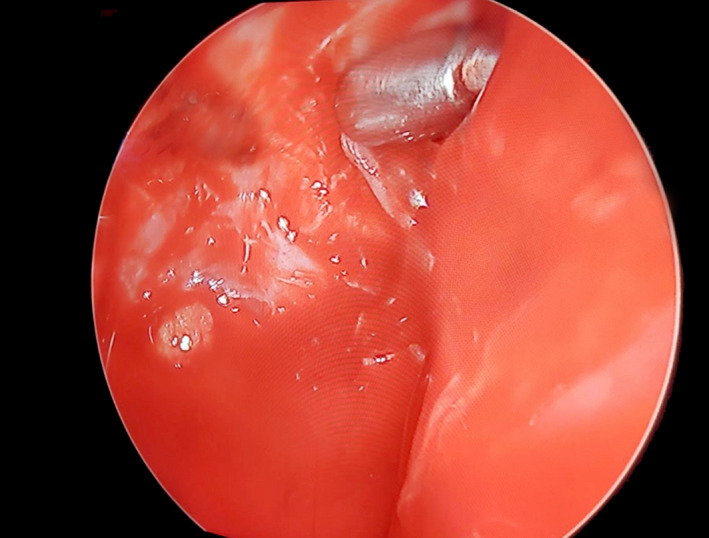
Transantral endoscopic view of maxillary sinus
FIGURE 4.

Resected specimen of dentigerous cyst wall and tooth
3. DISCUSSION
Dentigerous cyst is formed when fluid accumulates in the space between the reduced enamel epithelium and the crown of a partially erupted or impacted tooth. Large cysts can extend up to the ostium of the maxillary sinus. Most of these cysts are diagnosed incidentally, as they are asymptomatic. Dentigerous cysts may be related to supernumerary teeth or ectopically erupted teeth that extend into the maxillary sinus. Dentigerous cysts may present with facial pain, purulent rhinorrhea, epistaxis, external nasal deformity, headache, swelling, and epiphora‐related nasolacrimal duct obstruction. On radiographs, dentigerous cysts appear as well‐defined, round or ovoid, corticated, lucent lesions around the crowns of unerupted teeth. 4
Treatment includes extraction of impacted tooth and enucleation of the cyst. In this case, the ectopic cyst was near the ostium of maxillary sinus. A concurrent transnasal and transantral approach was used for visualization and removal of the cyst, respectively. The transantral approach served as an entrance to the right maxillary sinus and allowed for checking and clearing the pathologies to prevent recurrence. Recurrence is a known problem after marsupialization. It is difficult to remove tooth with huge cyst via transnasal approach only. We take out tooth via endoscopic transantral and transnasal approach. Each bit of diseases cyst wall was removed, and normal maxillary sinus epithelium saved. There are other alternative approach to treat maxillary sinuses pathology like combined inferior meatotomy and middle meatal antrostomy but it needed to make big window at middle wall of maxillary sinus, which jeopardize the nasolacrimal duct and inferior turbinate. So, we prefer endoscopic transantral and endonasal combined approach, which has better visualization and removal of huge dentigerous cyst. This combined approach should be the preferred approach for pathologies around pterygoid region, lateral recesses of sphenoid sinus and retrobulbar orbit too. 5 This approach also helps to deal with posteriorly located maxillary sinus pathology.
4. CONCLUSION
A combined endoscopic transantral and endonasal approach serves as a better method of treatment for large dentigerous cysts circumventing an impacted tooth located within the maxillary sinus compared to other approach. This approach helps in complete removal of disease wall of the cyst, which prevents recurrence.
CONFLICT OF INTEREST
None.
AUTHOR CONTRIBUTIONS
BS conceptualized the study. BS, KS, DK, MK, AM, and AP involved in design, literature review, and writing, seen and approved the final manuscript.
CONSENT
Written informed consent was obtained from the both the patient and her parents for publication of this case reportand any accompanying images.
ACKNOWLEDGEMENT
None.
Sigdel B, Sah K, Kandel D, Karn M, Moran A, Panta A. Endoscopic‐assisted transantral‐endonasal approach to large dentigerous cyst of maxillary sinus. Clin Case Rep. 2021;9:e05027. 10.1002/ccr3.5027
REFERENCES
- 1. Önay Ö, Süslü AE, Yılmaz T. Huge dentigerous cyst in the maxillary sinus: a rare case in childhood. Turk Arch Otorhinolaryngol. 2019;57(1):54‐56. 10.5152/tao.2019.1920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Daley TD, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol. 1994;77(3):276‐280. 10.1016/0030-4220(94)90299-2 [DOI] [PubMed] [Google Scholar]
- 3. Kumar A, Srivastava RK, Saxena A, Khanna R, Ali I. Removal of Infected maxillary third molar from the infra‐temporal Fossa by Caldwell Luc procedure ‐ rare case report with literature review. J Clin Diagn Res. 2016;10(12):Zd01‐zd03. 10.7860/JCDR/2016/17362.8961 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Scholl RJ, Kellett HM, Neumann DP, Lurie AG. Cysts and cystic lesions of the mandible: clinical and radiologic‐histopathologic review. Radiographics. 1999;19(5):1107‐1124. 10.1148/radiographics.19.5.g99se021107 [DOI] [PubMed] [Google Scholar]
- 5. Har‐El G. Combined endoscopic transmaxillary‐transnasal approach to the pterygoid region, lateral sphenoid sinus, and retrobulbar orbit. Ann Otol Rhinol Laryngol. 2005;114(6):439‐442. 10.1177/000348940511400605 [DOI] [PubMed] [Google Scholar]