

Abstract
Background:
There is limited research regarding the impact of workload on injury risk specific to women’s soccer. Wearable global positioning system (GPS) units can track workload metrics such as total distance traveled and player load during games and training sessions. These metrics can be useful in predicting injury risk.
Purpose:
To examine the relationship between injury risk and player workload as collected from wearable GPS units in National Collegiate Athletic Association (NCAA) Division I women’s soccer players.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Lower extremity injury incidence and GPS workload data (player load, total distance, and high-speed distance) for 65 NCAA Division I women’s soccer players were collected over 3 seasons. Accumulated 1-, 2-, 3-, and 4-week loads and acute-to-chronic workload ratios (ACWR) were classified into discrete ranges by z-scores. ACWR was calculated using rolling averages and exponentially weighted moving averages (EWMA) models. Binary logistic regression models were used to compare the 7:28 rolling average and EWMA ACWRs between injured and noninjured players for all GPS/accelerometer variables. The prior 1-, 2-, 3-, and 4-week accumulated loads for all GPS/accelerometer variables were compared between the injured and uninjured cohorts using 2-sample t tests.
Results:
There were a total of 53 lower extremity injuries that resulted in lost time recorded (5.76/1000 hours “on-legs” exposure time; 34 noncontact and 19 contact injuries). The prior 2-week (7242 vs 6613 m/s2; P = .02), 3-week (10,533 vs 9718 m/s2; P = .02), and 4-week (13,819 vs 12,892 m/s2; P = .04) accumulated player loads and 2-week (62.40 vs 57.25 km; P = .04), 3-week (90.97 vs 84.10 km; P = .03), and 4-week (119.31 vs 111.38 km; P = .05) accumulated total distances were significantly higher for injured players compared with noninjured players during the same time frames. There were no significant differences in player load, total distance, or high-speed distance ACWR between injured and noninjured players for both the rolling averages and EWMA calculations.
Conclusion:
Higher accumulated player load and total distance, but not ACWR, were associated with injury in women’s soccer players.
Keywords: GPS, injury, women’s soccer, workload
Participation in women’s soccer has been growing, as a recent FIFA (Fédération Internationale de Football Association) survey reported that over 13 million girls and women are playing organized soccer worldwide. 19 Increased competition in high-level environments has brought on greater performance expectations for women’s soccer athletes. Players can run over 10 km in a 90-minute game and often play multiple games per week. 27,40
With these increased performance expectations come increased injury risk. 4,16,31,45 –47 While many factors contribute to injury, 56 high cumulative workloads and spikes in player workloads have been associated with increased risk of injury in soccer and other sports. 3,6,7,15,27,29,36 These studies, however, have all been conducted with data from male soccer players or male athletes in other sports, with few studies investigating female athletes.
Technological advances in player load tracking using wearable global positioning system (GPS) units have allowed new avenues for quantifying workload and optimizing player performance to emerge. Wearable GPS units can track metrics such as total distance traveled, distance traveled at high and low speeds, number of accelerations/decelerations, and player load (a calculation based on triaxial acceleration) during games and training sessions. 15 These metrics are not only helpful for monitoring load and planning the intensity of training sessions but may also be useful in predicting injury risk. 6,7
According to the International Olympic Committee Consensus Statement on Load in Sport and Risk of Injury, 50 high accumulated loads have been shown to be a risk factor for injury in multiple sports, including soccer. As such, using metrics collected from GPS units to monitor cumulative load and distance may be valuable for injury prevention. Investigations using GPS data to study injuries in male soccer players have found that injured players had increased cumulative distance and a higher number of accelerations leading up to their injury. 7,15 In addition to cumulative load measurements, the acute-to-chronic workload ratio (ACWR), a measure of an athlete’s relative load, is another way to utilize GPS data to monitor injury risk. 6,7,29,30,36 The ACWR is typically calculated by dividing an athlete’s acute load (between 3 and 7 days in duration) by the chronic load (between 3 and 6 weeks in duration). 27,29,30
Despite the popularity of women’s soccer, there is limited research regarding the impact of workload on injury risk specific to the women’s game, with most studies focusing on men’s soccer. A recent systematic review found 20 articles investigating ACWR across various professional sports, and none of the studies included female athletes. 1 It has been shown that women have different injury risk profiles compared with men. 11 As such, it is valuable to investigate the link between external workload and injuries specific for women’s soccer players. The purpose of this study was to examine the relationship between injury risk and workload as collected from wearable GPS units in National Collegiate Athletic Association (NCAA) Division I women’s soccer players. We hypothesized that a higher player workload measured by wearable GPS devices would be associated with increased injury incidence.
Methods
Participants
Institutional review board approval was obtained prior to conducting the study. A retrospective analysis of prospectively collected data from 74 college women’s soccer players from 1 NCAA Division I team was performed. The players trained on a full-time basis and played their competitive seasons between the months of August and December; 3 separate seasons between 2017 and 2019 were included. Due to the differences in movement and positional requirements, goalkeepers (n = 4) were excluded from this study. In addition, players who were unavailable for an entire season were excluded (n = 5), resulting in 65 individual soccer seasons included for analysis.
Quantifying Workload
Workload was quantified using commercially available GPS units (Catapult OptimEye; Catapult Sports). These units are outfitted with triaxial accelerometers, gyroscopes, and magnetometers that assess full-body acceleration vectors at a sampling frequency 100 Hz. The units also operated in a nondifferential mode at a sampling frequency of 10 Hz. Each player was assigned a GPS unit to wear for all practices and games for the duration of each season. The GPS units were positioned between the scapulae and secured in a custom vest. Following each session, data were downloaded using commercially available software (Catapult Innovations). These GPS have been shown to be a valid and reliable method to track training and game loads. 52
The primary variables of interest included player load, total distance, and high-speed distance, all variables that have been validated for quantifying an athlete’s external load. 43 Based on previous research quantifying running profiles in female soccer players, 39 high-speed distance was defined as accumulated distance where players ran at 8 mph (12.9 km/h) or greater. Player load was calculated from the Catapult analytics platform using a Cartesian formula incorporating triaxial acceleration:
Player load
where a x is the side-to-side acceleration, a y is the anterior-posterior acceleration, and a z represents the vertical acceleration at any given time, t.
All players who were available to participate in training sessions and games were required to wear their GPS unit, and compliance was 95.3% (7654 of 8032 sessions). Based on previous methodology, for training sessions in which data were not available due to a player’s not wearing her GPS monitor or the GPS monitor’s not turning on, we estimated the player’s training session data by calculating the team averages for that day.
Definition of Injury
Injury information was documented by the team athletic trainer or team physician at the time of injury and stored in a local student-athlete injury database or hospital medical records system. Only time-loss injuries affecting the lower extremity, defined as one that caused the athlete to miss at least 1 subsequent practice or game, 20 and lower extremity injuries were included in this study. Injuries were classified based on the consensus statement on injury definitions in soccer, as follows: minimal (1-3 days missed), mild (4-7 days missed), moderate (1-4 weeks missed), or severe (>4 weeks missed). 20 Injuries were also categorized by body part (knee, foot and ankle, thigh, hip, and lower leg). The mechanism in which a participant acquired the injury was classified as contact or noncontact.
Data Analysis
Data were categorized into weekly blocks from Monday to Sunday. Every time a player participated in a training session or game, the data were analyzed in 2 ways. First, for each week throughout the season (August through December in each year tracked), the previous 1-week, 2-week, 3-week, and 4-week cumulative loads were calculated. The loads were then classified into 6 discrete ranges from very low through to very high using z-scores as described previously. 6,7 Second, ACWRs were calculated.
Rolling average ACWRs were calculated by dividing the average acute workload (past 7 days) by the average chronic workload (past 28 days). In addition, an exponentially weighted moving average (EWMA) model was used, which has been shown to be a more sensitive indicator of injury risk than rolling averages. 41 For a given day, the EWMA was calculated as follows:
where is a value between 0 and 1 that represents the degree of decay, with higher values decaying older observations in the model at a faster rate. The λ a was calculated as follows:
where N is the chosen time decay constant, with N = 7 used to represent acute workloads and N = 28 used to represent chronic workloads. The EWMA ACWR value was calculated by obtaining the EWMAtoday for acute workload and dividing this value by the EWMAtoday for chronic workload. To begin the EWMA calculation, the first observation in the series is recorded arbitrarily as the first workload value in the series. From this value, the EWMA calculation can be used for ACWR calculation as previously described. 41,55 For all ACWRs, a value of greater than 1 represents an acute workload greater than the chronic workload and vice versa. The ACWRs were also divided based on z-scores.
Statistical Analysis
Injury incidence was determined by dividing the total number of injuries by the “on-legs” exposure time (defined as the amount of time that a player was actively participating in a training session or game) and reported as rates per 1000 hours. Injury risks were calculated as the number of injuries sustained relative to the number of exposures to each workload classification. Binary logistic regression models were used to compare the ACWRs between injured and noninjured players for all GPS/accelerometer variables. These regression models were performed for both the rolling average and the EWMA ACWR calculations. Odds ratios and 95% CIs were calculated to determine the injury risk for given ACWRs. Correlation among EWMA and simple rolling average ACWR calculations was performed using Pearson correlation coefficient. An a priori sample size calculation was performed with the simple ACWR using an estimated population SD of 1.5. With a minimum of 48 injured players matched to noninjured players by date of injury, this study has 90% power to detect an ACWR difference of 1 point at an alpha of .05 (G*Power version 3.1). 18
As the result of the week-to-week variation in load over the course of the season, each player injury was then matched by season and week to uninjured players for that same week. Shapiro-Wilk tests for normality were conducted on the weekly cumulative loads for all GPS/accelerometer variables, and all data were normally distributed. These variables were compared between the injured and uninjured cohorts using 2-sample t tests with an alpha level of .05 set as significant. R Foundation for Statistical Computing (Version 4.0.0) was used for analysis.
Results
A total of 53 lower extremity injuries that resulted in lost time (5.76/1000 hours “on-legs” exposure time) were recorded for the duration of the study (2017, 5.05/1000 hours; 2018, 7.54/1000 hours; 2019, 4.91/1000 hours), including 34 noncontact and 19 contact injuries. For each game, only those who played in the game were included for analysis. Of the contact injuries, 73.7% occurred in games. The incidence of lower extremity injury during games was over 3.5 times higher than in practice (11.25/1000 hours and 3.07/1000 hours, respectively). There were 10 minimal (1-3 days missed), 17 mild (4-7 days missed), 16 moderate (1-4 weeks missed), and 10 severe (>4 weeks missed) lower extremity injuries. The foot/ankle and thigh were the most common sites for injury over the 3 seasons, with lateral ankle sprains (0.86/1000 hours) and quadriceps strains (0.86/1000 hours) accounting for the highest occurrence during the season (Table 1).
Table 1.
Number of Injuries by Location During the 2017, 2018, and 2019 Seasons a
| Location | No. of Injuries |
|---|---|
| Knee | 12 |
| ACL tear | 2 |
| MCL sprain | 6 |
| Other ligamentous, meniscal, or chondral injury | 4 |
| Foot and ankle | 19 |
| Lateral ankle sprain | 8 |
| High ankle sprain | 1 |
| Ankle fracture | 2 |
| Foot ligament sprain/plantar fasciitis | 6 |
| Other foot injury | 2 |
| Thigh | 19 |
| Hamstring strain | 5 |
| Quadriceps strain | 8 |
| Groin strain | 2 |
| Contusion | 4 |
| Other hip, lower leg, or thigh | 3 |
a ACL, anterior cruciate ligament; MCL, medial collateral ligament.
A total of 28 players sustained 1 injury throughout the season, 9 players sustained 2 injuries throughout the season, and 2 players sustained 3 or more injuries throughout the season. There were 26 players who did not sustain a lower extremity injury during the season. Of the players with multiple injuries within a season, 2 players had recurrent injuries of the same body part (quadriceps strain and foot sprain). Throughout the 3 seasons included in this study, there were 36 players who consistently started and played in the majority of games within a respective season. Within this subgroup, there were 24 players who sustained at least 1 injury during the season compared with 12 players who did not sustain a lower extremity injury during the season.
There were no significant differences in player load, total distance, or high-speed distance ACWR between injured and noninjured players, regardless of the type of ACWR calculation (Table 2). The player load and total distance ACWR calculations were highly correlated using both the EWMA (r = 0.99) and simple moving averages (r = 0.99) calculations. The 2 mechanisms of calculating ACWR, EWMA and simple moving average, were moderately correlated for calculating player load ACWR (r = 0.75) and total distance ACWR (r = 0.75). Players accumulated an average distance of 110.12 km during a 4-week span, with 24.47 km run at a high speed (Table 3). All z-score distributions for accumulated load and ACWRs are presented in Table 3.
Table 2.
Odds of Sustaining an Injury for Each 1-Unit Change of ACWR Calculated Using an EWMA Model or Simple Moving Average Model a
| Load Variable | OR (95% CI) | P |
|---|---|---|
| 7:28 EWMA | ||
| Player load | 0.61 (0.12-2.92) | 0.54 |
| Total distance | 0.83 (0.18-3.85) | 0.81 |
| High-speed distance | 1.24 (0.37-4.10) | 0.73 |
| 7:28 simple moving average | ||
| Player load | 0.53 (0.15 -1.87) | 0.32 |
| Total distance | 0.58 (0.17 -1.95) | 0.38 |
| High-speed distance | 0.69 (0.26 -1.87) | 0.47 |
a ACWR, acute-to-chronic work ratio; EWMA, exponentially weighted moving average; OR, odds ratio.
Table 3.
z-Score Classifications and Distributions for Accumulated Workloads Over 1 to 4 Weeks and 7:28 ACWRs a
| z-Score Classification (range) | Number of Weeks Accumulated | ACWR | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 7:28 EWMA | 7:28 Simple | |
| Player Load, m/s2 | ||||||
| Very low (≤ 2.00) | 0-390 | 0-1451 | 0-2752 | 0-4164 | 0-0.32 | 0-0.21 |
| Low ( 1.99 to 1.00) | 391-1788 | 1451-3912 | 2753-6157 | 4165-8455 | 0.33-0.61 | 0.22-0.59 |
| Moderate-low ( 0.99 to 0.00) | 1789-3186 | 3913-6373 | 6158-9561 | 8456-12,749 | 0.62-0.89 | 0.60-0.96 |
| Moderate-high (0.00 to 0.99) | 3187-4585 | 6374-8835 | 9562-12,965 | 12,750-17,041 | 0.90-1.18 | 0.97-1.34 |
| High (1.00 to 1.99) | 4586-5983 | 8835-11,296 | 12,966-16,370 | 17,042-21,334 | 1.18-1.46 | 1.35-1.72 |
| Very high (≥2.00) | ≥5984 | ≥11,297 | ≥16,371 | ≥21,335 | ≥1.47 | ≥1.73 |
| Total Distance, km | ||||||
| Very low (≤ 2.00) | 0-3.26 | 0-12.56 | 0-24.09 | 0-36.61 | 0-0.32 | 0-0.20 |
| Low ( 1.99 to 1.00) | 3.27-15.39 | 12.57-33.80 | 24.10-53.33 | 36.62-73.36 | 0.33-0.61 | 0.21-0.59 |
| Moderate-low ( 0.99 to 0.00) | 15.40-27.52 | 33.81-55.05 | 53.34-82.58 | 73.37-110.11 | 0.62-0.89 | 0.60-0.96 |
| Moderate-high (0.00 to 0.99) | 27.53-39.65 | 55.05-76.29 | 82.59-111.83 | 110.12-146.86 | 0.90-1.18 | 0.97-1.34 |
| High (1.00 to 1.99) | 39.66-51.78 | 76.30-97.54 | 111.83-141.07 | 146.87-183.60 | 1.19-1.47 | 1.35-1.72 |
| Very high (≥2.00) | ≥51.79 | ≥97.55 | ≥141.08 | ≥183.61 | ≥1.48 | ≥1.73 |
| High-Speed Distance, km | ||||||
| Very low ( 1.99 to 1.00) | 0-2.32 | 0-5.31 | 0-8.46 | 0-11.73 | 0.26-0.57 | 0.17-0.57 |
| Low ( 0.99 to 0.00) | 2.33-6.11 | 5.32-12.23 | 8.47-18.34 | 11.74-24.46 | 0.58-0.89 | 0.58-0.97 |
| Moderate-low (0.00 to 0.99) | 6.12-9.90 | 12.24-19.15 | 18.35-28.22 | 24.47-37.19 | 0.90 -1.20 | 0.98 -1.37 |
| Moderate-high (1.00 to 1.99) | 9.91-13.69 | 19.16-26.07 | 28.23-38.10 | 37.20-49.93 | 0.21 -1.52 | 1.38 -1.77 |
| High (≥2.00) | ≥13.70 | ≥26.08 | ≥38.11 | ≥49.94 | ≥1.53 | ≥1.78 |
a ACWR, acute-to-chronic workload ratio; EWMA, exponentially weighted moving average.
The prior 2-week (7242 vs 6613 m/s2; P = .02), 3-week (10,533 vs 9718 m/s2; P = .02), and 4-week (13,819 vs 12,892 m/s2; P = .04) accumulated player loads were significantly higher for injured players compared with noninjured players during the same time frames (Figure 1). Similarly, the prior 2-week (62.40 vs 57.25 km; P = .04), 3-week (90.97 vs 84.10 km; P = .03), and 4-week (119.31 vs 111.38 km; P = .05) accumulated total distances were significantly higher for injured players (Figure 1). The 1-week accumulated loads for all variables did not differ between injured and noninjured players (player load, P = .18; total distance, P = .24; high-speed distance, P = .35). No differences were detected for high-speed distance at any time point between injured and noninjured players (Figure 1).
Figure 1.
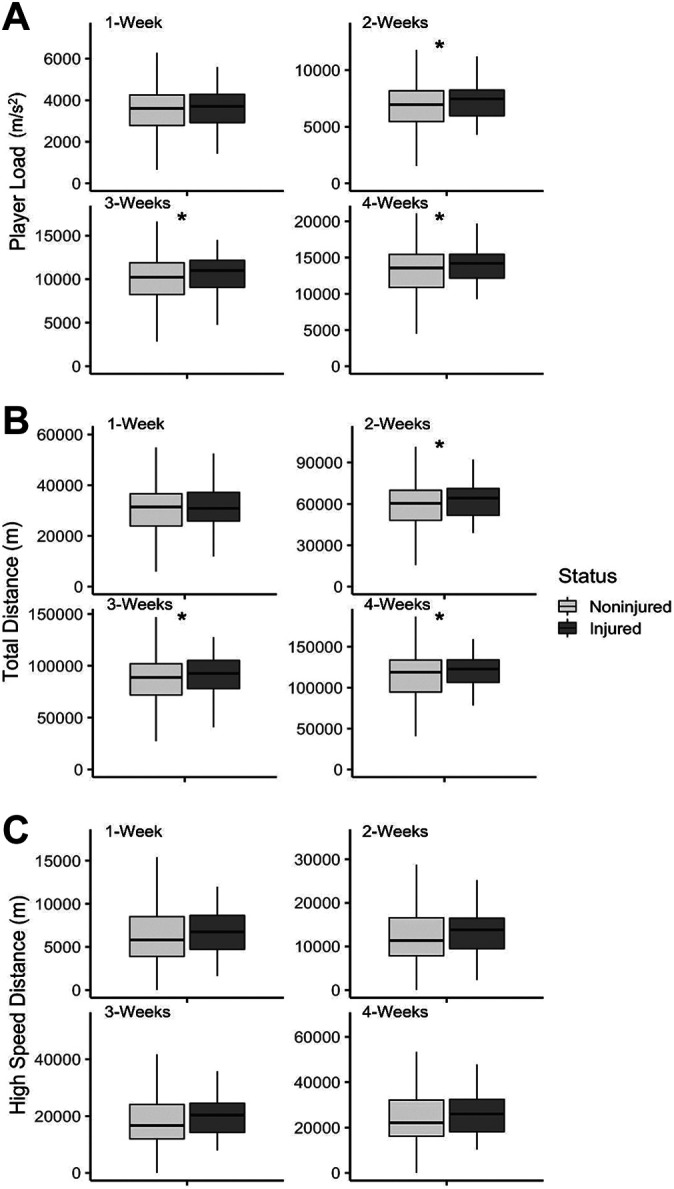
Comparison between noninjured and injured players for 1-, 2-, 3-, and 4-week accumulated (A) player load, (B) total distance, and (C) high-speed distance. *Significant difference between noninjured and injured players (P < .05).
Discussion
In this study, we investigated the relationships of both accumulated workloads collected from wearable GPS units and ACWRs with lower extremity injury risk for an NCAA Division I women’s soccer team. The most important findings of the present study were that injured athletes had significantly higher 2-, 3-, and 4-week accumulated player load and total distance as compared with noninjured players during the same time frame. In addition, there were no associations between player load, total distance, and high-speed distance ACWRs and injuries, regardless of whether an EWMA or simple rolling average model was used.
Although there are a large number of studies investigating risk factors for injury in men’s soccer, fewer studies have focused specifically on the female soccer athlete. To our knowledge, this is the first study to use GPS-derived external workload metrics to evaluate lower extremity injury risk in women’s soccer. Studies comparing men’s and women’s soccer have demonstrated that men are more likely to sustain groin and hamstring injuries, 10,54 whereas women have a higher risk of anterior cruciate ligament (ACL) tears, 28,33 ankle ligament injuries, 35 and concussions. 14 Furthermore, consistent with previous findings, 17,26 the present study found that the incidence of lower extremity injury was over 3 times higher in games than in practices, at rates of 11.25 injuries per 1000 game hours and 3.07 injuries per 1000 practice hours, respectively. While the causes of injuries are multifactorial, the higher intensity of play during games may be one reason for the increased injury incidence. Dupont et al 13 concluded that the injury rate for players playing 2 games per week was significantly higher than for those who played only 1 game per week. Players in the current investigation competed in 2 games per week for the majority of season and had 36 to 72 hours of rest between games. As such, a balance of training and competition with load management and recovery is important for mitigating player fatigue and injury risk.
Many studies of team sports have utilized an absolute load, such as accumulated total distance, to associate with injury risk. 50 High cumulative loads and total distances have been identified as risk factors for injury in soccer and other sports. ‡ Using GPS data, Jaspers et al 32 reported an increased injury risk for players that had higher cumulative 2- to 4-week total distances in professional men’s soccer, and Bowen et al 7 found that high accumulated total distance over 4 weeks was associated with a significant increase in injury risk for male youth soccer players. Other GPS metrics that have been associated with increased injury risk in soccer include increased meters per minute in each session and total number of accelerations. 6,15 The current investigation also supports the finding that absolute load is useful to monitor for athletes, as injured players had significantly higher accumulated player load and total distance as compared with noninjured players.
Another option of measuring load has been with the ACWR, a measure of relative load that is based on the fitness-fatigue model. 29 The ACWR has been used to monitor athlete workload in multiple sports. 2,6,7,29,30,36,42,48,51 Hulin et al 29 first examined the relationship between ACWR and injury risk in elite cricket fast bowlers. The authors calculated 1-week acute and 4-week rolling average chronic workloads by the number of balls bowled and found a 3-fold increase in injury risk when the ACWR was greater than 2. In addition, high ACWRs measured using GPS data are associated with greater risk of injury in rugby, 30 American football, 36,48 and Australian rules football. 42,51
For soccer in particular, investigations in youth and professional men’s soccer players have shown that both higher accumulated and ACWR workloads were associated with greater injury risk. 6,7 While the present study also found that higher accumulated workloads measured by total distance and player load were associated with injury, there was no association between ACWR and injury risk. In the current study, when ACWRs were categorized as moderate to low or moderate to high based on z-scores, the rolling average values ranged between 0.60 and 1.34 for player load and total distance and 0.58 and 1.37 for high-speed distance. Previous studies have concluded that when the ACWR is between 0.8 and 1.3, injury risk is lower. 5,30,50 As the team in the current investigation utilized sports performance staff to monitor player workloads, the majority of the ACWRs fell within the accepted range. Thus, when the ACWR is already controlled, other factors such as accumulated player load and total distance may be more valuable to monitor for injury risk.
Furthermore, there are different variations in the calculation of ACWRs that may affect the sensitivity of injury risk. First, the time frame of acute and chronic windows may vary, with the 7:28 ratio being most used. 27 It is advised that time frames are individualized based on team schedules, and, as such, other ratios such as 3:21, 7:21, and 7:14 have been reported to be associated with significant injury risks. 12,38,48 The current study utilized the 7:28 ratio, as week-to-week training and game intensity were consistent throughout the season. Generally, when calculating ACWR, a rolling average model has been employed and is evidence based. 23 More recently, however, Williams et al 55 proposed an EWMA model for ACWR calculation based on the concept that fitness and fatigue may be better represented as nonlinear decay. Further, Murray et al 41 concluded that the EWMA model for ACWRs may be more sensitive in predicting injury compared with a rolling average calculation. As such, the current study utilized both a rolling averages model and an EWMA to calculate ACWRs. While neither model resulted in significant associations between ACWR and injury risk, there was a moderate correlation between the 2 methods of calculations. Griffin et al 27 conducted a systematic review on monitoring athletes in team sports with the ACWR and found that there is an association between the ACWR and noncontact injuries, but this does not necessarily translate into the ability to predict an injury. With wearable GPS technology becoming more available for soccer players of all levels, monitoring both accumulated loads and ACWRs in combination with other risk factors for injury will be useful for medical and sports performance personnel.
Results from this study can inform clinical care by providing guidance for optimizing metrics of player load, total distance, and high-speed distance specific for women’s soccer to reduce injury risk. Sports performance personnel and medical staff can utilize GPS data to monitor workloads in athletes. In the current study, injured players ran over 7 km more than the team average during a 2-week span. Thus, 2-week average cumulative distances for a team could be calculated, and players who have higher-than-average cumulative distances could be identified and have their training session modified for injury prevention. Future studies should include a larger sample size with women’s soccer players from multiple teams to further investigate which injuries may be more likely to occur due to increased load. Moreover, these studies should also stratify players based on position to identify position-specific injury risks in women’s soccer due to accumulated load.
There were several limitations to the current study. Both contact and noncontact injuries were included in this investigation based on previous findings that higher workloads were strongly correlated with contact injuries. 7,22 However, most studies investigating the relationship between load and injury did so for noncontact injuries. 27 As such, there may be different mechanisms for how load can influence contact and noncontact injuries. Although fatigue can play a role in some contact injuries, such as a contact ACL tear, other contact injuries may have less to do with accumulated load. In addition, this investigation did not find any significant associations between high-speed distance and risk of injury. The authors used 8 mph as the lower-end cutoff for high-speed distance. It has been reported that using fixed thresholds may reduce the sensitivity of the ACWR calculation for high-speed distance, as players vary in their maximum velocity. 9 Moreover, because the majority of injuries occurred during games, substitute players who did not play in as many games may have lower accumulated loads and lower injury risk than starters. Thus, findings from this investigation may be the result of game exposure rather than absolute accumulated loads. Further, the authors only tracked external load with GPS monitoring. Adding in other measures of load, such as rating of perceived exertion, and factoring in injury history, age, and early specialization may be more valuable to detect injury risk. 57 As players wore their GPS units only for trainings and games, other sources of accumulated load for collegiate athletes, such as strength training, were not accounted for. Finally, this study included players from only 1 team. Therefore, the authors did not calculate position-specific risks due to the limited sample size, and the results may not be generalizable to other women’s soccer teams.
Conclusion
Higher accumulated player load and total distance, but not ACWR, were associated with injury in women’s soccer players in this study.
Acknowledgment
The authors thank Brianna Kanz for her help with data collection.
Footnotes
Final revision submitted June 29, 2021; accepted July 19, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.E.H. has received consulting fees from Sideline Sports Doc. G.D.A. has received research support from OrthoFix; education payments from Evolution Surgical; consulting fees from Cytonics, Fidia Pharma, RubiconMD, and Sideline Sports Doc; and other financial/material support from Arthrex and Stryker; and has stock/stock options in Cytonics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Stanford University (eProtocol No. 57358).
References
- 1. Andrade R, Wik EH, Rebelo-Marques A, et al. Is the acute: chronic workload ratio (ACWR) associated with risk of time-loss injury in professional team sports? A systematic review of methodology, variables and injury risk in practical situations. Sports Med. 2020;50(9):1613–1635. [DOI] [PubMed] [Google Scholar]
- 2. Arazi H, Asadi A, Khalkhali F, et al. Association between the acute to chronic workload ratio and injury occurrence in young male team soccer players: a preliminary study. Front Physiol. 2020;11:608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bacon CS, Mauger AR. Prediction of overuse injuries in professional U18-U21 footballers using metrics of training distance and intensity. J Strength Cond Res. 2017;31(11):3067–3076. [DOI] [PubMed] [Google Scholar]
- 4. Bengtsson H, Ekstrand J, Hägglund M. Muscle injury rates in professional football increase with fixture congestion: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med. 2013;47(12):743–747. [DOI] [PubMed] [Google Scholar]
- 5. Blanch P, Gabbett TJ. Has the athlete trained enough to return to play safely? The acute:chronic workload ratio permits clinicians to quantify a player’s risk of subsequent injury. Br J Sports Med. 2016;50(8):471–475. [DOI] [PubMed] [Google Scholar]
- 6. Bowen L, Gross AS, Gimpel M, Bruce-Low S, Li F-X. Spikes in acute:chronic workload ratio (ACWR) associated with a 5-7 times greater injury rate in English Premier League football players: a comprehensive 3-year study. Br J Sports Med. 2020;54(12):731–738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bowen L, Gross AS, Gimpel M, Li F-X. Accumulated workloads and the acute:chronic workload ratio relate to injury risk in elite youth football players. Br J Sports Med. 2017;51(5):452–459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Brink MS, Visscher C, Arends S, Zwerver J, Post WJ, Lemmink KA. Monitoring stress and recovery: new insights for the prevention of injuries and illnesses in elite youth soccer players. Br J Sports Med. 2010;44(11):809–815. [DOI] [PubMed] [Google Scholar]
- 9. Buchheit M. Applying the acute:chronic workload ratio in elite football: worth the effort? Br J Sports Med. 2017;51(18):1325–1327. [DOI] [PubMed] [Google Scholar]
- 10. Cross KM, Gurka KK, Saliba S, Conaway M, Hertel J. Comparison of hamstring strain injury rates between male and female intercollegiate soccer athletes. Am J Sports Med. 2013;41(4):742–748. [DOI] [PubMed] [Google Scholar]
- 11. Crossley KM, Patterson BE, Culvenor AG, Bruder AM, Mosler AB, Mentiplay BF. Making football safer for women: a systematic review and meta-analysis of injury prevention programmes in 11 773 female football (soccer) players. Br J Sports Med. 2020;54(18):1089–1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Delecroix B, McCall A, Dawson B, Berthoin S, Dupont G. Workload and non-contact injury incidence in elite football players competing in European leagues. Eur J Sport Sci. 2018;18(9):1280–1287. [DOI] [PubMed] [Google Scholar]
- 13. Dupont G, Nedelec M, McCall A, McCormack D, Berthoin S, Wisloff U. Effect of 2 soccer matches in a week on physical performance and injury rate. Am J Sports Med. 2010;38(9):1752–1758. [DOI] [PubMed] [Google Scholar]
- 14. Dvorak J, McCrory P, Kirkendall DT. Head injuries in the female football player: incidence, mechanisms, risk factors and management. Br J Sports Med. 2007;41(suppl 1):i44–i46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Ehrmann FE, Duncan CS, Sindhusake D, Franzsen WN, Greene DA. GPS and injury prevention in professional soccer. J Strength Cond Res. 2016;30(2):360–367. [DOI] [PubMed] [Google Scholar]
- 16. Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553–558. [DOI] [PubMed] [Google Scholar]
- 17. Engström B, Johansson C, Törnkvist H. Soccer injuries among elite female players. Am J Sports Med. 1991;19(4):372–375. [DOI] [PubMed] [Google Scholar]
- 18. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. [DOI] [PubMed] [Google Scholar]
- 19. FIFA. Women’s Football Member Associations Survey Report. Accessed July 25, 2021. https://www.fifa.com/womens-football/news/fifa-takes-steps-for-further-development-of-women-s-football
- 20. Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40(3):193–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Gabbett TJ. Influence of training and match intensity on injuries in rugby league. J Sports Sci. 2004;22(5):409–417. [DOI] [PubMed] [Google Scholar]
- 22. Gabbett TJ. The development and application of an injury prediction model for noncontact, soft-tissue injuries in elite collision sport athletes. J Strength Cond Res. 2010;24(10):2593–2603. [DOI] [PubMed] [Google Scholar]
- 23. Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50(5):273–280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Gabbett TJ, Domrow N. Relationships between training load, injury, and fitness in sub-elite collision sport athletes. J Sports Sci. 2007;25(13):1507–1519. [DOI] [PubMed] [Google Scholar]
- 25. Gabbett TJ, Ullah S. Relationship between running loads and soft-tissue injury in elite team sport athletes. J Strength Cond Res. 2012;26(4):953–960. [DOI] [PubMed] [Google Scholar]
- 26. Giza E, Mithofer K, Farrell L, Zarins B, Gill T. Injuries in women’s professional soccer. Br J Sports Med. 2005;39(4):212–216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Griffin A, Kenny IC, Comyns TM, Lyons M. The association between the acute:chronic workload ratio and injury and its application in team sports: a systematic review. Sports Med. 2020;50(3):561–580. [DOI] [PubMed] [Google Scholar]
- 28. Gupta AS, Pierpoint LA, Comstock RD, Saper MG. Sex-based differences in anterior cruciate ligament injuries among United States high school soccer players: an epidemiological study. Orthop J Sports Med. 2020;8(5):2325967120919178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Hulin BT, Gabbett TJ, Blanch P, Chapman P, Bailey D, Orchard JW. Spikes in acute workload are associated with increased injury risk in elite cricket fast bowlers. Br J Sports Med. 2014;48(8):708–712. [DOI] [PubMed] [Google Scholar]
- 30. Hulin BT, Gabbett TJ, Lawson DW, Caputi P, Sampson JA. The acute:chronic workload ratio predicts injury: high chronic workload may decrease injury risk in elite rugby league players. Br J Sports Med. 2016;50(4):231–236. [DOI] [PubMed] [Google Scholar]
- 31. Inklaar H, Bol E, Schmikli SL, Mosterd WL. Injuries in male soccer players: team risk analysis. Int J Sports Med. 1996;17(3):229–234. [DOI] [PubMed] [Google Scholar]
- 32. Jaspers A, Kuyvenhoven JP, Staes F, Frencken WGP, Helsen WF, Brink MS. Examination of the external and internal load indicators’ association with overuse injuries in professional soccer players. J Sci Med Sport. 2018;21(6):579–585. [DOI] [PubMed] [Google Scholar]
- 33. Joseph AM, Collins CL, Henke NM, Yard EE, Fields SK, Comstock RD. A multisport epidemiologic comparison of anterior cruciate ligament injuries in high school athletics. J Athl Train. 2013;48(6):810–817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Knobloch K, Yoon U, Vogt PM. Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int. 2008;29(7):671–676. [DOI] [PubMed] [Google Scholar]
- 35. Larruskain J, Lekue JA, Diaz N, Odriozola A, Gil SM. A comparison of injuries in elite male and female football players: a five-season prospective study. Scand J Med Sci Sports. 2018;28(1):237–245. [DOI] [PubMed] [Google Scholar]
- 36. Li RT, Salata MJ, Rambhia S, Sheehan J, Voos JE. Does overexertion correlate with increased injury? The relationship between player workload and soft tissue injury in professional American football players using wearable technology. Sports Health. 2020;12(1):66–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Macera CA, Pate RR, Powell KE, Jackson KL, Kendrick JS, Craven TE. Predicting lower-extremity injuries among habitual runners. Arch Intern Med. 1989;149(11):2565–2568. [PubMed] [Google Scholar]
- 38. Malone S, Owen A, Mendes B, Hughes B, Collins K, Gabbett TJ. High-speed running and sprinting as an injury risk factor in soccer: can well-developed physical qualities reduce the risk? J Sci Med Sport. 2018;21(3):257–262. [DOI] [PubMed] [Google Scholar]
- 39. Mara JK, Thompson KG, Pumpa KL, Morgan S. Quantifying the high-speed running and sprinting profiles of elite female soccer players during competitive matches using an optical player tracking system. J Strength Cond Res. 2017;31(6):1500–1508. [DOI] [PubMed] [Google Scholar]
- 40. Mohr M, Krustrup P, Andersson H, Kirkendal D, Bangsbo J. Match activities of elite women soccer players at different performance levels. J Strength Cond Res. 2008;22(2):341–349. [DOI] [PubMed] [Google Scholar]
- 41. Murray NB, Gabbett TJ, Townshend AD, Blanch P. Calculating acute:chronic workload ratios using exponentially weighted moving averages provides a more sensitive indicator of injury likelihood than rolling averages. Br J Sports Med. 2017;51(9):749–754. [DOI] [PubMed] [Google Scholar]
- 42. Murray NB, Gabbett TJ, Townshend AD, Hulin BT, McLellan CP. Individual and combined effects of acute and chronic running loads on injury risk in elite Australian footballers. Scand J Med Sci Sports. 2017;27(9):990–998. [DOI] [PubMed] [Google Scholar]
- 43. Nicolella DP, Torres-Ronda L, Saylor KJ, Schelling X. Validity and reliability of an accelerometer-based player tracking device. PLoS One. 2018;13(2):e0191823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Owen AL, Forsyth JJ, Wong DP, Dellal A, Connelly SP, Chamari K. Heart rate— based training intensity and its impact on injury incidence among elite-level professional soccer players. J Strength Cond Res. 2015;29(6):1705–1712. [DOI] [PubMed] [Google Scholar]
- 45. Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of injury incidences in male professional adult and elite youth soccer players: a systematic review. J Athl Train. 2016;51(5):410–424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Rahnama N, Reilly T, Lees A. Injury risk associated with playing actions during competitive soccer. Br J Sports Med. 2002;36(5):354–359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Roos KG, Wasserman EB, Dalton SL, et al. Epidemiology of 3825 injuries sustained in six seasons of National Collegiate Athletic Association men’s and women’s soccer (2009/2010-2014/2015). Br J Sports Med. 2017;51(13):1029–1034. [DOI] [PubMed] [Google Scholar]
- 48. Sampson JA, Murray A, Williams S, et al. Injury risk-workload associations in NCAA American college football. J Sci Med Sport. 2018;21(12):1215–1220. [DOI] [PubMed] [Google Scholar]
- 49. Satterthwaite P, Norton R, Larmer P, Robinson E. Risk factors for injuries and other health problems sustained in a marathon. Br J Sports Med. 1999;33(1):22–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Soligard T, Schwellnus M, Alonso JM, et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 2016;50(17):1030–1041. [DOI] [PubMed] [Google Scholar]
- 51. Stares J, Dawson B, Peeling P, et al. Identifying high risk loading conditions for in-season injury in elite Australian football players. J Sci Med Sport. 2018;21(1):46–51. [DOI] [PubMed] [Google Scholar]
- 52. Theodoropoulos JS, Bettle J, Kosy JD. The use of GPS and inertial devices for player monitoring in team sports: a review of current and future applications. Orthop Rev (Pavia). 2020;12(1):7863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Van Middelkoop M, Kolkman J, Van Ochten J, Bierma-Zeinstra SM, Koes BW. Risk factors for lower extremity injuries among male marathon runners. Scand J Med Sci Sports. 2008;18(6):691–697. [DOI] [PubMed] [Google Scholar]
- 54. Waldén M, Hägglund M, Ekstrand J. The epidemiology of groin injury in senior football: a systematic review of prospective studies. Br J Sports Med. 2015;49(12):792–797. [DOI] [PubMed] [Google Scholar]
- 55. Williams S, West S, Cross MJ, Stokes KA. Better way to determine the acute:chronic workload ratio? Br J Sports Med. 2017;51(3):209–210. [DOI] [PubMed] [Google Scholar]
- 56. Windt J, Gabbett TJ. How do training and competition workloads relate to injury? The workload-injury aetiology model. Br J Sports Med. 2017;51(5):428–435. [DOI] [PubMed] [Google Scholar]
- 57. Xiao M, Lemos JL, Hwang CE, Sherman SL, Safran MR, Abrams GD. High specialization among female youth soccer players is associated with an increased likelihood of serious injury. Med Sci Sports Exerc. 2021;53(10):2086–2092. doi:10.1249/MSS.0000000000002693 [DOI] [PubMed] [Google Scholar]