

Abstract
Background
The effect of preadmission metformin usage (PMU) on the mortality of coronavirus disease-2019 (COVID-19) patients with diabetes is conflicting. Most studies have focused on in-hospital mortality; however, mortality after discharge also increases in COVID-19 patients.
Aims
Examining the effect of PMU on all-cause mortality, including the post-discharge period.
Methods
Patients with diabetes who were hospitalised in 2020 due to COVID-19 were included in the study. They were divided into two groups: those with a history of metformin use (MF( +)) and those without such history (MF( −)). Propensity score matching (PSM) was performed at a ratio of 1:1 for age and sex. COX regression analyses were used to demonstrate risk factors for mortality.
Results
We investigated 4103 patients hospitalised for COVID-19. After excluding those without diabetes or with chronic liver/kidney disease, we included the remaining 586 patients, constituting 293 women (50%) with an overall mean age of 66 ± 11.9 years. After PSM analysis, the in-hospital and post-discharge mortality rates were higher in the MF( −) group though not significantly different. However, overall mortality was higher in the MF( −) group (51 (42.5%) vs. 35 (29.2%), p = 0.031). For overall mortality, the adjusted HR was 0.585 (95% CI: 0.371 − 0.920, p = 0.020) in the MF( +) group.
Conclusion
PMU is associated with reducing all-cause mortality. This effect starts from the in-hospital period and becomes more significant with the post-discharge period. The main limitations were the inability to evaluate the compliance with metformin and the effects of other medications due to retrospective nature.
Keywords: Coronavirus disease 2019, Metformin, Mortality, Preadmission, Treatment
Background
COVID-19 has a poor prognosis and the risk of death nearly doubles in people with diabetes mellitus (DM) [1–3]. Hypoglycaemic agents and diabetes itself can affect the course of Covid-19. Although the effects of antidiabetic drugs on COVID-19 are not fully known, new studies are ongoing in this regard. Metformin is one of the most widely used oral hypoglycaemic agents. It also has immunomodulatory effects in animal models via the phosphorylating adenosine monophosphate-activated protein kinase [4]. In addition, some studies reveal that it could have an inhibitory effect, especially on some viruses, by improving insulin sensitivity [5].
Metformin has been used in the past to treat malaria and influenza [6]. Several studies reveal the beneficial clinical results of concomitant use of metformin in respiratory diseases, including chronic pulmonary diseases and pulmonary infection diseases [7–10]. In a comparative study, metformin significantly decreased the mortality rate of chronic lower respiratory tract diseases [11]. In a meta-analysis conducted before the COVID-19 era, five observational studies involving 1282 patients were examined, and preadmission usage of metformin was associated with low mortality in patients with diabetes and sepsis [12]. Given the high worldwide prevalence of type 2 diabetes and the increased risk of COVID-19-related deaths, it is crucial to investigate the safety of hypoglycaemic agents in COVID-19 patients with diabetes [13].
The effect of preadmission metformin usage in patients with COVID-19 was assessed using meta-analyses of various studies. Although most studies reveal results in favour of metformin, there were some methodological differences. Two of these studies employed the propensity score matching (PSM) method while forming the control group, thereby enhancing equality. Moreover, these studies did not evaluate post-discharge mortality data [14, 15]. However, the increase in mortality continued after hospital discharge in COVID-19, with 10% rates reported within a few months after discharge [16, 17]. This prompts the need for more studies to explore the effects of metformin as part of the COVID-19 treatment guidelines [18, 19].
Thus, we aimed at analysing the effect of preadmission usage of metformin on the mortality of COVID-19 by PSM, while including a post-discharge period of at least 90 days.
Material-methods
Our study is a retrospective cohort study. Included participants were patients with diabetes over 18 years of age, hospitalised at the Canakkale Onsekiz Mart University Medical Faculty Hospital with COVID-19 confirmed by radiological and/or PCR between March 12, 2020 and December 22, 2020. Information on the age, sex, medications, comorbidities, laboratory parameters and COVID-19 severity were obtained from participants’ hospital records. Patients with a history of chronic liver/kidney failure and pregnancy were excluded from the study [20]. The study was approved by the Local Ethics Committee of the Canakkale Onsekiz Mart University Medical School (2011-KAEK-27/2021-E.2100041806).
From the records, patients who were found to use metformin regularly in the last 6 months were considered to be using metformin before hospitalisation. They were divided into two groups: those who used metformin (MF) before hospitalisation (MF( +)) and those who did not (MF(–)). Individuals in the MF( +) group were propensity score-matched as 1:1 for age and sex to individuals in the MF(–) group. The patient recruitment scheme is outlined in Fig. 1. The mortality status of the patients included in the study on March 22, 2021 (the first year of the first patient recruitment) was obtained from the Turkish Central Death Registry. Following this date, all cases included in the study had a mortality of at least 90 days. The primary endpoint of our study was at least 90 days of all-cause mortality. Secondary endpoints were in-hospital and post-discharge mortalities.
Fig. 1.
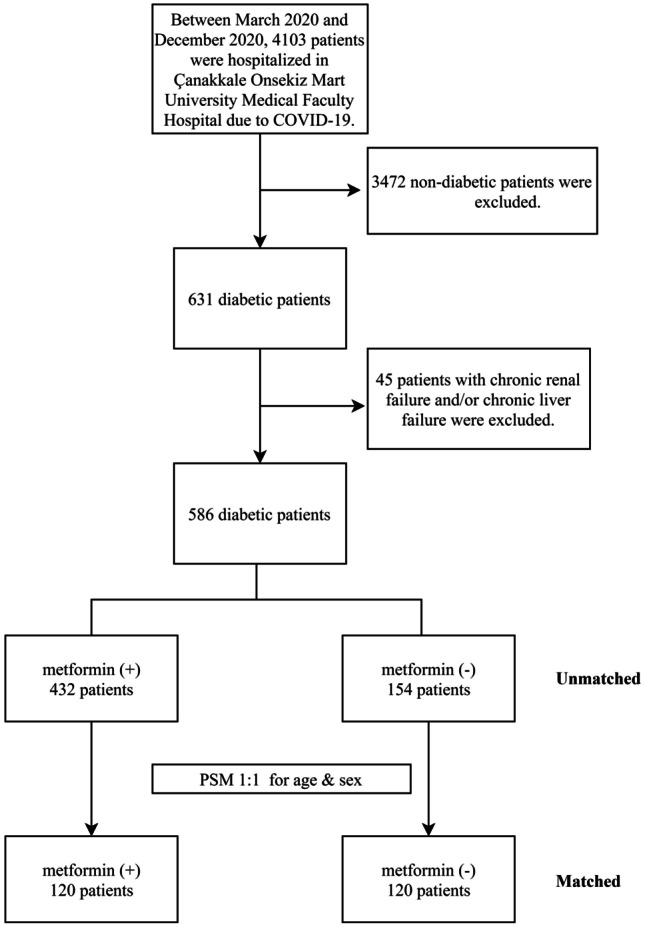
Patient recruitment scheme
Normally distributed continuous variables are presented as mean ± standard deviation, while non-normally distributed as the median and interquartile range (IQR: the difference between the 25th and 75th percentiles). Categorical variables were expressed as numbers and percentages. Student’s t test and Mann Whitney U test were used to compare means between normally distributed and non-normally distributed groups of continuous variables, respectively. Pearson’s chi-square was used to test the significance of the difference between categorical variables. Estimated glomerular filtration rate (eGFR) was calculated according to the CKD-EPI equation [21]. COX regression analyses were used to evaluate the risk factors of COVID-19-related mortality. In the adjusted HR (aHR) analysis, sex, age, glucose, ALT, eGFR, number of hospitalisation days, diabetes duration, chronic pulmonary disease, coronary artery disease, cerebrovascular disease, hypertension and hyperlipidaemia were used covariate variables. Unadjusted hazard ratios (HRs) were calculated by analysis with a single variable. Statistical analysis was performed with SPSS 19 for Windows (IBM, Armonk, NY, USA). A p-value < 0.05 was considered statistically significant.
Results
We included 586 diabetic patients, with a mean age of 66 ± 11.9 years, constituting 293 women (50%). Metformin usage ratio was 73.7% (432).
Analysis of data before PSM (unmatched)
The mean age of the MF ( −) group was significantly higher than the MF ( +) group (68.92 ± 13.47 years vs 64.98 ± 11.19 years, p = 0.001). The MF ( −) group had lower baseline eGFR values (62.2(35.5 − 87.9) vs. 76.5(56.8 − 94.4), p = 0.001) and higher acute renal failure rates (39% vs 19.4%, p = 0.0001). Median number of hospitalization days (IQR) (8(5–16)vs. 6(5–12), p = 0.036), intensive care unit (ICU) admission rate (27.3% vs. 18.1%, p = 0.015), in-hospital mortality rate (26% vs. 11.6%, p = 0.0001), post-discharge mortality rate (20.2% vs. 9.4%, p = 0.002), and overall mortality rate (40.9% vs. 19.9%, p = 0.0001)) were higher in the MF( −) group. Comparison of general characteristics of MF ( +) and MF ( −) groups before PSM is given in Table 1.
Table 1.
Comparison of general characteristics of MF( +) and MF( −) groups before PSM
| MF( +) | MF( −) | p | |
|---|---|---|---|
| Age | 64.98 ± 11.19 | 68.92 ± 13.47 | 0.001 |
| Male (%) | 215 (49.8) | 217 (50.2) | 0.85 |
| Diabetes duration above 10 years (%) | 175 (40.5) | 74 (48.1) | 0.104 |
| Glucose (median (IQR)) | 191 (136 − 267) | 198.5 (152 − 280) | 0.08 |
| eGFR(median (IQR)) | 76.5 (56.8 − 94.4) | 62.2 (35.5 − 87.9) | 0.001 |
| ALT (median (IQR)) | 22 (13 − 32) | 21 (13 − 31) | 0.069 |
| HBA1C (median (IQR)) | 8 (6.8 − 9.9) | 7.7 (6.7 − 10.1) | 0.526 |
| Hypertension (%) | 290 (67.1) | 108 (70.1) | 0.493 |
| COPD-asthma (%) | 63 (14.6) | 30 (19.5) | 0.153 |
| CAD (%) | 143 (33.1) | 62 (40.3) | 0.11 |
| CVD(%) | 37 (8.6) | 16 (10.4) | 0.498 |
| Hyperlipidaemia (%) | 179 (41.4) | 51 (33.1) | 0.07 |
| ARF(%) | 84 (19.4) | 60 (39.0) | 0.0001 |
| ICU admission (%) | 78 (18.1) | 42 (27.3) | 0.015 |
| In-hospital mortality(%) | 50 (11.6) | 40 (26.0) | 0.0001 |
| Post-discharge mortality (%) | 36 (9.4) | 23 (20.2) | 0.002 |
| Overall mortality (%) | 86 (19.9) | 63 (40.9) | 0.0001 |
| Number of hospitalization days (median(IQR)) | 6 (5–12) | 8 (5–16) | 0.036 |
| Follow-up days count | 157.5 (105 − 235.7) | 127.5 (34.2 − 212.7) | 0.001 |
COPD chronic obstructive pulmonary disease, CAD coronary artery disease, CVD cerebrovascular disease, ARF acute renal failure, ICU intensive care unit, eGFR estimated glomerular filtration rate
Analysis of data after PSM (matched)
PSM was performed at a ratio of 1:1 in terms of age and sex, according to the use of metformin. After PSM, 120 MF( +) and 120 MF( −) patients were matched. ALT values (median(IQR)) of the MF ( +) group were higher than those of the MF (–) group (25(16–42) vs 19(11–30), p = 0.003). ICU admission rates, in-hospital mortality rates, and post-discharge mortality rates were higher in the MF( −) group, though not significant. Overall mortality was higher in the MF( −) group than in the MF( +) group (51(42.5%) vs. 35(29.2%), p = 0.031). A comparison of general characteristics of MF ( +) and MF ( −) groups after PSM is presented in Table 2.
Table 2.
Comparison of general characteristics of MF( +) and MF( −) groups after PSM
| MF( +) | MF( −) | p | |
|---|---|---|---|
| Age | 68.72 + 10.04 | 68.72 + 10.04 | 1 |
| Male (%) | 63 (52.5) | 63 (52.5) | 1 |
| Diabetes duration above 10 years (%) | 64 (53.3) | 56 (46.7) | 0.302 |
| Glucose (median (IQR)) | 175.2 (134.5 − 251) | 190 (138 − 259) | 0.507 |
| eGFR(median (IQR)) | 53.9 (38.8 − 80.6) | 61.5 (34.1 − 86.8) | 0.648 |
| ALT (median (IQR)) | 25 (16 − 42) | 19 (11 − 30) | 0.003 |
| HBA1C (median (IQR)) | 8.35 (7.05 − 9.57) | 7.55 (6.57 − 9.65) | 0.214 |
| Hypertension (%) | 89 (74.2) | 88 (73.3) | 0.883 |
| COPD-asthma (%) | 20 (16.7) | 25 (20.8) | 0.408 |
| CAD (%) | 48 (40.0) | 50 (41.7) | 0.793 |
| CVD(%) | 15 (12.5) | 11 (9.2) | 0.406 |
| Hyperlipidaemia (%) | 51 (42.5) | 39 (32.5) | 0.110 |
| ARF(%) | 55 (45.8) | 51 (42.5) | 0.603 |
| ICU Admission (%) | 23 (19.2) | 35 (29.2) | 0.07 |
| In-hospital mortality (%) | 19 (15.8) | 29 (24.2) | 0.107 |
| Post-discharge mortality (%) | 16 (15.8) | 22 (24.2) | 0.148 |
| Overall mortality (%) | 35 (29.2) | 51 (42.5) | 0.031 |
| Number of hospitalization days (median (IQR)) | 7 (5–12.5) | 8.5 (5–16.5) | 0.071 |
| Follow-up days count | 140 (88.7 − 213.7) | 127.5 (39.7 − 211.5) | 0.216 |
COPD chronic obstructive pulmonary disease, CAD coronary artery disease, CVD cerebrovascular disease, ARF acute renal failure, ICU intensive care unit, eGFR estimated glomerular filtration rate
Hazard ratios for overall, in-hospital mortality, and post-discharge mortality
HR for in-hospital mortality, post-discharge mortality, and overall mortality were evaluated with COX regression in matched and unmatched groups.
For overall mortality, the aHR was 0.607 (95% CI: 0.428 − 0.860, p = 0.005) in the unmatched MF( +) group, while the aHR was 0.585 (95% CI: 0.371 − 0.920, p = 0.020) in the matched MF( +) group. For in-hospital mortality, aHR was 0.546 (95% CI: 0.349 − 0.855,p = 0.008) in the unmatched MF( +) group, while aHR was 0.568 (95% CI: 0.306 − 1.052, p = 0.072) in the matched MF( +) group. For post-discharge mortality, aHR was 0.702 (95% CI:0.399 − 1.236, p = 0.22) in the unmatched MF( +) group and 0.652 (95% CI:0.324 − 1.310, p = 0.23) in the matched MF( +) group. All mortality assessments, HR and aHR ratios in the match and unmatch groups, and forest plot graphics are given in Fig. 2. Figure 3 displays the Kaplan − Meier plot showing the risk of overall mortality in the unmatched and matched groups for MF( +) vs. MF( −) patients.
Fig. 2.
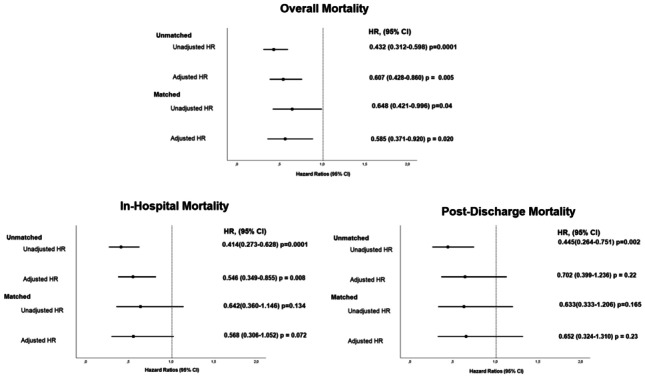
Forest plot showing hazard ratios (HRs) of overall, in-hospital, post-discharge mortality for MF (+) compared to MF (−) patients
Fig. 3.
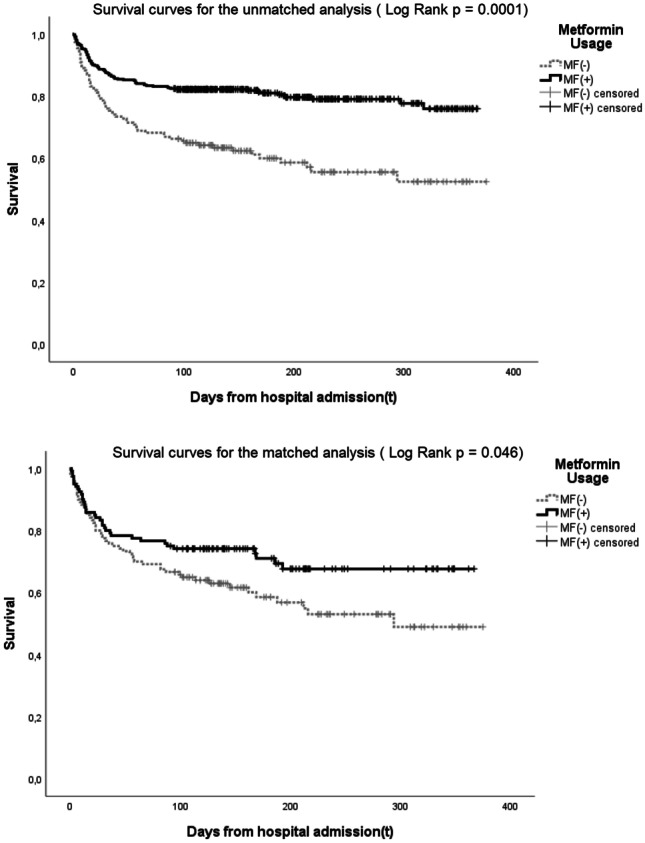
Kaplan–Meier plot showing the risk of overall mortality in the unmatched and matched groups for MF ( +) vs. MF ( −) patients
In the COX regression analysis performed for overall mortality, in addition to metformin, age (95% CI: 1.003 − 1.057, aHR; 1.029, p = 0.031), ALT (95% CI: 1.000 − 1.001, aHR; 1.001, p = 0.001), and eGFR (95% CI: 0.971 − 0.990, aHR; 0.98, p = 0.001) remained statistically significant.
Discussion
Although diabetes is a major risk factor for COVID-19 mortality, the safe use of hypoglycaemic agents in glycaemic control in such patients during the COVID-19 pandemic was unclear [2, 22]. Our study showed that the usage of metformin before hospital admission had a protective effect on mortality. This effect increases over time and becomes more significant on inclusion of the post-discharge period. In our study, the effect remained after PS matching for age and sex. Moreover, after adjusting for comorbidities, metformin provides a decrease in the mortality risk of approximately 45%. Having post-discharge follow-ups distinguishes our study from other related studies, thereby contributing to the literature.
When in-hospital mortality was evaluated, the protectiveness for HR and aHR mortality in the MF( +) group became insignificant after grouped HR matching. Only unmatched HR was protective for mortality in the MF( +) group for the post-discharge period. However, both unmatch and match HR and aHR rates were protective for overall mortality in the MF( +) group.
A recent meta-analysis examining the association between metformin use and overall COVID-19 mortality found an OR of 0.78 (95% CI 0.71–0.86) with PSM studies and 0.75 (95% CI 0.66–0.85) for unmatched studies [23]. The approximately 25% risk reduction found in this meta-analysis was approximately 40% in our study. The fact that we have follow-ups after discharge, our long follow-up period and the inclusion of only hospitalised patients in the study may be the factors affecting this difference.
A meta-analysis in 2020 evaluated nine studies on metformin and COVID-19 hospital mortality. The OR for the non-adjusted model was 0.45 [95% CI: 0.25–0.81], and that for the adjusted model was 0.64 [95% CI: 0.43, 0.97] [24]. However, PSM was not performed in some of the studies evaluated in this meta-analysis. In our study, the preadmission usage of metformin was observed to be protective on in-hospital mortality before PSM, but not after PSM.
Metformin is contraindicated for patients with diabetes having comorbidities such as chronic kidney disease, which has a high risk for mortality. Therefore, metformin-usable patients have a lower diabetic burden [25]. The exclusion of this group in our study provided a more accurate interpretation of the metformin effect. However, some studies did not exclude chronic kidney disease in their analysis [26–28]. In a population-based study involving primary care patients, preadmission usage of metformin had no protective effect compared to in-hospital studies [29]. This could be due to the exclusion of the lower risk group. A recent large cohort exploring the registry containing all patients with diabetes nationwide (in-hospital and out-hospital data) also had results consistent with our study. This study showed that patients on metformin prior to infection had a lower risk of death associated with COVID-19 with an HR of 0.77 (95% CI 0.73–0.81) [13]. Although studies on the COVID-19 mortality of preadmission usage of metformin have different results, the differences in the selection of patient and control groups could impact the results.
Although both groups’ median ALT levels were within the normal reference range, ALT levels were higher in metformin users. In our study, higher ALT levels were associated with mortality. Other studies have also found that ALT can predict increased mortality [30, 31]. Despite the higher ALT levels in the metformin group, a lower mortality rate may support the protective effect of metformin in our study.
Our study has some limitations. Since the deaths of the patients after discharge were evaluated with the national death registration system, the death status at home or in another hospital could also be determined precisely from the system. However, since COVID patients who were hospitalised were evaluated in our study, patients who died before hospitalisation due to peri-hospital cardiac arrest could not be evaluated within the scope of this study. Even though we observed in the prescription records that eligible participants were on drugs, it is possible that the patients were not compliant to their medications. In addition, we evaluated the just efficacy of metformin, not the consequences, complications, or interactions of other hypoglycaemic agents and non-diabetic medications that can be used in combination therapy in diabetes patients. Furthermore, the causality could not be inferred from our observations owing to the study design. Randomised controlled studies are needed to evaluate the mentioned effects more clearly. However, these studies are still ongoing. Although studies show beneficial effects, if the patient had impaired renal/hepatic function, discontinuation of this drug is recommended if there are concerns about acidosis.
Conclusion
Preadmission use of metformin is associated with reducing all-cause mortality following hospitalisation for COVID-19. This effect starts from the in-hospital period, but it becomes significant when evaluated within the post-discharge period. Considering that patients with diabetes have a higher risk of death after COVID-19, this positive effect of metformin is reassuring for clinicians and patients.
Acknowledgements
We acknowledge and are grateful to all health care professionals at Canakkale Onsekiz Mart University, who cared for the patients during the COVID-19 pandemic. Preparation for publication of this article is supported by the Society of Endocrinology and Metabolism of Turkey.
Data availability
The data of the study are available from the corresponding author when a reasonable request.
Declarations
Ethics approval
The study was approved by the Local Ethics Committee of the Canakkale Onsekiz Mart University Medical School (2011-KAEK-27/2021-E.2100041806).
Conflict of interest
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Apicella M, Campopiano MC, Mantuano M, et al. COVID-19 in people with diabetes: understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020;8:782–792. doi: 10.1016/S2213-8587(20)30238-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Barron E, Bakhai C, Kar P, et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. Lancet Diabetes Endocrinol. 2020;8:813–822. doi: 10.1016/S2213-8587(20)30272-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Guo W, Li M, Dong Y, et al. Diabetes is a risk factor for the progression and prognosis of COVID -19. Diabetes Metab Res Rev. 2020;36:e3319. doi: 10.1002/dmrr.3319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kajiwara C, Kusaka Y, Kimura S, et al. Metformin mediates protection against Legionella pneumonia through activation of AMPK and mitochondrial reactive oxygen species. J Immunol. 2018;200:623–631. doi: 10.4049/jimmunol.1700474. [DOI] [PubMed] [Google Scholar]
- 5.Chen Y, Gu F, Guan J-L. Metformin might inhibit virus through increasing insulin sensitivity. Chin Med J (Engl) 2018;131:376–377. doi: 10.4103/0366-6999.223856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bailey CJ. Metformin: historical overview. Diabetologia. 2017;60:1566–1576. doi: 10.1007/s00125-017-4318-z. [DOI] [PubMed] [Google Scholar]
- 7.Ho TW,Huang CT, Tsai YJ et al (2019) Metformin use mitigates the adverse prognostic effect of diabetes mellitus in chronic obstructive pulmonary disease Respir Res 2010.1186/s12931-019-1035-9 [DOI] [PMC free article] [PubMed]
- 8.Wu TD, Keet CA, Fawzy A, et al. Association of metformin initiation and risk of asthma exacerbation A claims-based cohort study. Ann Am Thorac Soc. 2019;16:1527–1533. doi: 10.1513/AnnalsATS.201812-897OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mortensen E, Anzueto A (2018) Association of metformin and mortality for patients with diabetes who are hospitalised with pneumonia. In: Respiratory infections. European Respiratory Society, p PA2639
- 10.Zhang M, He J. Impacts of metformin on tuberculosis incidence and clinical outcomes in patients with diabetes: a systematic review and meta-analysis. Eur J Clin Pharmacol. 2020;76:149–159. doi: 10.1007/s00228-019-02786-y. [DOI] [PubMed] [Google Scholar]
- 11.Mendy A, Gopal R, Alcorn JF, Forno E. Reduced mortality from lower respiratory tract disease in adult diabetic patients treated with metformin. Respirology. 2019;24:646–651. doi: 10.1111/resp.13486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Liang H, Ding X, Li L, et al. Association of preadmission metformin use and mortality in patients with sepsis and diabetes mellitus: a systematic review and meta-analysis of cohort studies. Crit Care. 2019;23:50. doi: 10.1186/s13054-019-2346-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Khunti K, Knighton P, Zaccardi F, et al. Prescription of glucose-lowering therapies and risk of COVID-19 mortality in people with type 2 diabetes: a nationwide observational study in England. Lancet Diabetes Endocrinol. 2021;9:293–303. doi: 10.1016/S2213-8587(21)00050-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hariyanto TI, Kurniawan A. Metformin use is associated with reduced mortality rate from coronavirus disease 2019 (COVID-19) infection. Obes Med. 2020;19:100290. doi: 10.1016/j.obmed.2020.100290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kow CS, Hasan SS. Mortality risk with preadmission metformin use in patients with COVID-19 and diabetes: a meta-analysis. J Med Virol. 2021;93:695–697. doi: 10.1002/jmv.26498. [DOI] [PubMed] [Google Scholar]
- 16.Donnelly JP, Wang XQ, Iwashyna TJ, Prescott HC. Readmission and death after initial hospital discharge among patients with COVID-19 in a large multihospital system. JAMA. 2021;325:304. doi: 10.1001/jama.2020.21465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ayoubkhani D, Khunti K, Nafilyan V et al (2021) Post-covid syndrome in individuals admitted to hospital with covid-19: retrospective cohort study. BMJ 372 10.1136/bmj.n693 [DOI] [PMC free article] [PubMed]
- 18.Do JY, Kim SW, Park JW et al (2020) Is there an association between metformin use and clinical outcomes in diabetes patients with COVID-19? Diabetes Metab 10120810.1016/j.diabet.2020.10.006 [DOI] [PMC free article] [PubMed]
- 19.Zangiabadian M, Nejadghaderi SA, Zahmatkesh MM et al (2021) The efficacy and potential mechanisms of metformin in the treatment of COVID-19 in the diabetics: a systematic review Front Endocrinol (Lausanne) 12 10.3389/fendo.2021.645194 [DOI] [PMC free article] [PubMed]
- 20.Cheng X, Liu Y-M, Li H, et al. Metformin is associated with higher incidence of acidosis, but not mortalitY, in individuals with COVID-19 and pre-existing type 2 diabetes. Cell Metab. 2020;32:537–547.e3. doi: 10.1016/j.cmet.2020.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi: 10.7326/0003-4819-150-9-200905050-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ceriello A, Stoian AP, Rizzo M. COVID-19 and diabetes management: what should be considered? Diabetes Res Clin Pract. 2020;163:108151. doi: 10.1016/j.diabres.2020.108151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Avogaro A, Bonora B, Fadini GP. Managing diabetes in diabetic patients with COVID: where do we start from? Acta Diabetol. 2021 doi: 10.1007/s00592-021-01739-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lukito AA, Pranata R, Henrina J, et al. The effect of metformin consumption on mortality in hospitalized COVID-19 patients: a systematic review and meta-analysis. Diabetes Metab Syndr Clin Res Rev. 2020;14:2177–2183. doi: 10.1016/j.dsx.2020.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dave JA, Tamuhla T, Tiffin N et al (2021) Risk factors for COVID-19 hospitalisation and death in people living with diabetes: a virtual cohort study from the Western Cape Province South Africa Diabetes Res Clin Pract 108925 10.1016/j.diabres.2021.108925 [DOI] [PMC free article] [PubMed]
- 26.Luo P, Qiu L, Liu Y, et al. Metformin treatment was associated with decreased mortality in COVID-19 patients with diabetes in a retrospective analysis. Am J Trop Med Hyg. 2020;103:69–72. doi: 10.4269/ajtmh.20-0375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ghany R, Palacio A, Dawkins E, et al. Metformin is associated with lower hospitalisations, mortality and severe coronavirus infection among elderly medicare minority patients in 8 states in USA. Diabetes Metab Syndr Clin Res Rev. 2021;15:513–518. doi: 10.1016/j.dsx.2021.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Chen Y, Yang D, Cheng B, et al. Clinical characteristics and outcomes of patients with diabetes and COVID-19 in association with glucose-lowering medication. Diabetes Care. 2020;43:1399–1407. doi: 10.2337/dc20-0660. [DOI] [PubMed] [Google Scholar]
- 29.Wang J, Cooper JM, Gokhale K, et al. Association of metformin with susceptibility to COVID-19 in people with type 2 diabetes. J Clin Endocrinol Metab. 2021;106:1255–1268. doi: 10.1210/clinem/dgab067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Salık F, Uzundere O, Bıçak M et al (2021) Liver function as a predictor of mortality in COVID-19 Retrospective study Ann Hepatol 10055310.1016/j.aohep.2021.100553 [DOI] [PMC free article] [PubMed]
- 31.Medetalibeyoglu A, Catma Y, Senkal N et al (2019) The effect of liver test abnormalities on the prognosis of COVID-19. Ann Hepatol 19:614–621. 10.1016/j.aohep.2020.08.068 [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data of the study are available from the corresponding author when a reasonable request.