

Abstract
Adult mortality increased enormously in Russia and other countries of the former Soviet Union when the Soviet system collapsed 30 years ago. What has happened to mortality in Russia since the fall of the Soviet Union? What explains the wide swings of mortality over time? This paper documents changes in mortality in Russia since 1989, and reviews the research in the economics and public health literature on the causes of the changes. The focus is on the post-2000 period, and the possible role played in recent declining mortality rates by Russia’s alcohol and tobacco control policies. The two themes that emerge are (1) that government policies are critical for understanding both rising and falling male mortality over this period, and (2) that the underlying causes of the mortality crisis and its reversal are difficult to clearly identify empirically and remain, at best, partially understood, leaving much scope for future research on this issue.
Supplementary Information
The online version contains supplementary material available at 10.1057/s41294-021-00169-w.
Keywords: Russia, Transitional economies, Mortality, Health, Alcohol, Policy
Introduction
Extraordinary changes in mortality marked the first three decades after the fall of the Soviet Union. The post-Soviet period began in 1991 with a historic crisis of prime-age mortality in Russia, and ended with more than a decade of rapid and striking improvements in adult mortality. Similar changes occurred across most former Soviet republics over this period. Research on the mortality crisis and its reversal has identified a number of key factors in these changes, but the underlying causes remain at best partially understood. Yet deciphering the causes of these erratic swings in mortality remains an essential research and policy task. A better understanding of the impact of the collapse of the Soviet Union on health and well-being would provide insights into how to best mitigate the mortality impact of economic crisis in other countries. Discerning the causes of the remarkable improvement in mortality in recent years, and the role of government policy in promoting these improvements, surely holds lessons that would be beneficial for many countries.
This paper provides an overview of mortality change in Russia over the last 30 years. The mortality history of the period, although well known, is briefly described. This is followed by a selective review of the literature in economics and public health that has attempted to identify the causes of the mortality crisis of the early 1990s. The remainder of the paper focuses on the mortality reversal that has occurred since 2005, and the possible reasons for this change. The anti-alcohol policies and tobacco control policies of the Russian government play an important role in this discussion, and the evidence to date on the effectiveness of these policies in reducing mortality is evaluated. Several empirical tests of the impact of anti-alcohol policies on mortality are conducted, and provide suggestive evidence of an impact of these policies on reduced male deaths due to external causes. A central theme running throughout the paper is that government policy has played a critical role in Russian mortality trends: government policy contributed to the early mortality crisis, and government policy has facilitated the remarkable mortality improvements of recent years. A second theme is that much remains unknown about the underlying causes of both the mortality crisis and the mortality reversal of recent years, leaving scope for important future research into these questions.
Life Expectancy and Mortality Change in Russia Since 1991
Life expectancy plummeted in the successor states of the former Soviet Union in the early 1990s, with the largest declines occurring in Russia and other countries of the western former Soviet Union (Fig. 1). Male life expectancy at birth in Russia fell by six years between 1991 and 1994, from an already-low 63.4 years to 57.4 years over that period, an almost unprecedented decrease in life expectancy in three years.1 Female life expectancy followed a similar but less extreme pattern, falling from 74.2 to 71.1 years from 1991 to 1994 (Appendix Figure 1). The life expectancy decline reversed in 1995, and mortality rates improved for several years, until the 1998 financial crisis hit the country. Male life expectancy declined by two years between 1998 and 2000, reflecting that—at least in the first decade of transition—life expectancy, especially male life expectancy, appeared to be highly sensitive to changes in real GDP growth. Male life expectancy remained stable at about 59 years from 2000 to 2005 before a new pattern emerged of extended, rapid gains beginning in 2006. Male and female life expectancy reached 68.2 and 78.2 years, respectively, by 2019, by the far the highest life expectancy for men and women in Russia’s history. Many former Soviet countries experienced similar swings in life expectancy over this period (Fig. 1), with the Baltic countries making especially rapid grains. Life expectancy improved significantly in Eastern Europe as well (see Appendix Figure 2), but in recent years the gains in life expectancy in Russia have exceeded those in Eastern Europe. These erratic swings in life expectancy over short periods are unusual in developed countries; more typical is the slowly evolving growth in life expectancy shown in Fig. 1 for France.
Fig. 1.

Source: WHO Health for All Database
Mortality crises tend to disproportionately affect the elderly and infants (Cutler et al. 2002), but the working age population experienced the largest increase in death rates in the mortality crisis of the early 1990s in the former Soviet republics.2 In Russia, the death rate among men age 35 to 44 more than doubled between 1989 and 1994; for women in the same age group the death rate increased by 80 percent. Increased deaths were remarkably high across all working ages for both men and women, as shown in Table 1. Less-educated men and women experienced substantially higher death rates than individuals with higher education (Murphy et al. 2006). By cause, the largest increases in mortality in the early ‘crisis’ period comprised cardiovascular disease deaths (heart attacks, strokes and cerebrovascular diseases), and deaths due to external causes (accidents, injuries, homicides and suicides) (see Appendix Figure 3). The former Soviet Union experienced the highest suicide and homicide rates in the world in some age groups in the early years of transition. As shown in Appendix Figure 4, suicide deaths among men aged 50 to 54 reached 140 deaths per 100,000 population in 1994.3 To put this figure in context, the suicide rate among white, non-Hispanic men aged 45 to 54 in the United States was 39.2 per 100,000 in 2015, a time of notably rising “deaths of despair” (Case and Deaton 2015).
Table 1.
Percentage change in death rates by 5-year age group, Russia
| % change 1989–1994 | % change 1994–1998 | % change 2005–2010 | |
|---|---|---|---|
| Men | |||
| 5–9 | −4.9 | −9.7 | −45.4 |
| 10–14 | 6.7 | −15.7 | −39.1 |
| 15–19 | 40.2 | −12.8 | −40.4 |
| 20–24 | 58.1 | −1.8 | −50.7 |
| 25–29 | 69.8 | −15.8 | −52.1 |
| 30–34 | 92.1 | −24.7 | −37.9 |
| 35–39 | 105.9 | −30.9 | −28.9 |
| 40–44 | 116.0 | −32.7 | −40.4 |
| 45–49 | 91.6 | −31.2 | −44.3 |
| 50–54 | 92.3 | −33.3 | −43.9 |
| 55–59 | 61.4 | 22.5 | −37.0 |
| 60–64 | 54.6 | −24.5 | −31.8 |
| 65–69 | 40.3 | −13.7 | −28.5 |
| 70–74 | 21.5 | −10.0 | −26.6 |
| 75–79 | 20.5 | −13.8 | −24.0 |
| 80–84 | 14.6 | −10.2 | −17.1 |
| Women | |||
| 5–9 | 3.8 | −12.0 | −42.4 |
| 10–14 | 8.4 | −86 | −20.6 |
| 15–19 | 27.1 | −3.2 | −36.3 |
| 20–24 | 42.9 | −0.5 | −42.8 |
| 25–29 | 60.5 | −7.0 | −40.8 |
| 30–34 | 74.1 | −18.2 | −23.1 |
| 35–39 | 76.7 | −26.9 | −18.9 |
| 40–44 | 84.6 | −31.5 | −27.5 |
| 45–49 | 72.0 | −29.1 | −33.3 |
| 50–54 | 71.4 | −28.9 | −38.0 |
| 55–59 | 45.5 | −19.3 | −36.7 |
| 60–64 | 39.7 | −21.5 | −33.2 |
| 65–69 | 25.5 | −11.2 | −29.6 |
| 70–74 | 16.7 | −7.7 | −29.0 |
| 75–79 | 18.7 | −9.3 | −28.5 |
| 80–84 | 15.5 | −5.7 | −18.9 |
Calculated from the Russian Fertility and Mortality Database, Center for Demographic Research, New Economic School, Moscow. http://demogr.nes.ru/index.php/ru/demogr_indicat/data
The rise in all causes of death—and particularly the steep increase in suicide rates—points to the extreme stresses and upheaval that affected the Russian population in the early years of transition. Several other pieces of evidence support the picture of acute psychosocial stress and declining well-being in this early period. As discussed in greater detail below, alcohol consumption increased significantly in Russia and many other former Soviet countries in the early 1990s, which may have been a coping mechanism in response to increased stress (Cornia 2016). There was a large gap in self-reported life satisfaction between residents of transition and non-transition countries in the mid-1990s (controlling for income and other variables), and self-reported happiness declined in Russia until the late 1990s (Guriev and Zhuravskaya 2009). Perhaps most strikingly, individuals born at the start of the transition are on average more than 1 cm shorter than individuals born just before or after that period (Adserà et al. 2019). Adult stature is considered an indicator of the biological standard of living, and a height difference of this magnitude likely reflects nutritional deprivation, inadequate medical care and maternal stress in the early crisis years.4 These indicators collectively suggest a major shock to well-being in Russia and other transition countries in the early 1990s.
Since 2005, there have been significant improvements in mortality and life expectancy in all former Soviet countries, including Russia, primarily due to sharply falling deaths due to cardiovascular disease and external causes (see Appendix Figure 3). Decreased deaths at older ages have also contributed to life expectancy gains in the post-2004 period in Russia (Shkolnikov et al. 2013 and Table 1). Evidence, discussed below, suggests that significant reductions in smoking and drinking among Russian men in part explain these trends; however the increase in life expectancy since the mid 2000s is not fully understood, and is not only due to decreased alcohol consumption (Danilova et al. 2020). Increased investment in advanced medical technology to treat cardiovascular disease and improved management of chronic conditions such as diabetes and hyptertension may have also contributed to declining cardiovascular mortality rates (Kontsevaya et al. 2017). Echoing these positive trends, self-reported happiness in Russia and other formerly socialist countries increased over this period, and the “happiness gap” between residents of post-socialist countries and similar non-transition countries had closed by 2016 (Guriev and Melnikov 2018).
Causes of the Mortality Crisis of the Early 1990s: What Do We Know?
The mortality crisis occurred in the setting of a historic and deep transformational recession, increased job insecurity and poverty, rising income inequality, and unprecedented uncertainty about the future in Russia and other countries of the former Soviet Union. To the casual observer, it might seem obvious that the “cause” of the mortality crisis was the transition to a market economy. But what specifically about the transition caused the mortality crisis?
Attempts to discern the underlying causes of Russia’s mortality crisis have been hampered by the absence of high-quality longitudinal micro data sets that span the years before and after the crisis, which would enable researchers to track the correlates of changes in individual health and mortality over the period.5 Most studies rely on cross-country evidence or regional (oblast)-level data across Russia’s regions by age and cause of death to test hypotheses about the causes of the increased deaths. These aggregate data are unlikely to yield convincing results, and uncovering causal relationships is further hindered by the simultaneity of the changes across economic, political, and social dimensions in the region. Studies of the relationship between alcohol policy and mortality are often plagued by endogeneity problems; for example governments may impose taxes and stricter regulations in response to high mortality. A limited number of studies, discussed below, have succeeded in using quasi-experimental approaches that can credibly identify causal effects, but only one of these studies directly tests a hypothesis about a possible cause of the mortality crisis. In short, although nearly three decades have passed since one of the worse mortality crises of the twentieth century, only limited progress has been made in identifying the causes of the upsurge in deaths.
The findings of the cross-country and cross-regional research studies have helped to rule out possible causes of the crisis, including deterioration of the medical care system, environmental damage and pollution, and material deprivation and inadequate nutrition (Shkolnikov et al. 1998; Cornia and Paniccia 2000; Brainerd and Cutler 2005; Komo 2017). It does not appear that a change in or poor quality of mortality statistics is to blame: the quality of mortality statistics in Russia is reasonably high, although there is likely over-reporting of deaths due to ‘ill-defined conditions’, and underreporting of deaths due to external causes (Gavrilova et al. 2008).
The broad consensus across many studies on the causes of the Russian mortality crisis in the early 1990s is that increased alcohol consumption and psychosocial stress are the most important factors behind the increase in adult male mortality (Shapiro 1995; Shkolnikov et al. 1998; Cornia and Paniccia 2000; Brainerd and Cutler 2005; Cornia 2016; Danilova et al. 2020). Alcohol consumption and male mortality are strongly correlated in Russia, and alcohol consumption soared during the early years of transition (Fig. 2). Increased alcohol consumption was likely fueled by the liberalization of the alcohol market in Russia, with barriers to trade falling and an influx of imported alcohol, coupled with a significant decline in the real price of vodka, which fell by 77% between 1990 and 1994 (Treisman 2010).
Fig. 2.

Source: Russian Fertility and Mortality Database (SDR); Federal State Statistics Service (alcohol consumption per population age 15+, liters of pure ethanol)
Increased alcohol consumption is clearly implicated in the increase in deaths due to external causes in Russia, and is also implicated in increased cardiovascular disease deaths. While moderate alcohol consumption may have a protective effect on the heart, the style of drinking in Russia—binge drinking—leads to increased arrhythmias and heart attacks (McKee and Britton 1998). A small case-control study of deaths in the Udmurt region confirmed this relationship by showing that cardiovascular deaths in Russia are strongly associated with periods of heavy drinking among adult men (Shkolnikov et al. 2001). Another study of men in Novosibirsk found an increased risk of both cardiovascular and external cause mortality among frequent heavy drinkers (Malyutina et al. 2002). An analysis of 25,000 autopsies conducted in Siberia 1990–2004 showed that 21% of autopsied adult male deaths due to cardiovascular disease had lethal or near-lethal levels of ethanol in the blood (Zaridze et al. 2009a). And finally, a case-control study of 48,000 deaths in three Siberian cities by the same authors led the authors to conclude that alcohol consumption may be responsible for more than half of all adult male deaths in Russia from 1990 to 2001, and one-third of adult female deaths (Zaridze et al., 2009b).
Other researchers have noted the important role of ‘surrogate’ alcohol consumption as a cause of premature male mortality in Russia. A significant amount of alcohol is consumed in the form of either homemade alcohol (samogon), which has high ethanol concentrations, or ‘non-beverage’ alcohol, such as after-shave, anti-freeze and lighter fluid, which contain high concentrations of ethanol and toxic ingredients (McKee et al. 2005; Leon et al. 2007). These forms of alcohol are untaxed and, per liter of pure alcohol, are much cheaper than vodka sold in retail stores. The combination of high ethanol concentrations and toxic ingredients also makes these surrogate alcohol products far more lethal than commercially sold vodka. The important role of surrogate alcohol consumption in Russia’s mortality trends is underscored by the strong relationship between life expectancy and mortality from alcohol poisoning over the 1984-2003 period (Danilova et al. 2020). Some of the anti-alcohol policies introduced in Russia in 2006 specifically targeted the consumption of surrogate alcohol and appear to be at least somewhat effective in reducing this consumption (discussed below).
Recent research from the economics literature uses quasi-experimental evidence to add further insights and nuance into earlier analyses of Russia’s mortality crisis. Yakovlev (2018) exploits the kinked structure of the federal excise tax on vodka to identify the price elasticity of demand for heavy drinking in Russia—a key parameter for which previous studies have been affected by endogeneity issues. The paper provides the first evidence of a causal relationship between the price of alcohol and alcohol consumption in Russia, and shows that heavy drinking is relatively elastic with respect to the price of vodka. The paper also demonstrates the importance of peer effects and drinking habit persistence in understanding and modeling alcohol consumption behavior in Russia.
The high price elasticity of heavy drinking in Russia was reflected in the strong response of alcohol consumption and alcohol-related mortality to Mikhail Gorbachev’s anti-alcohol campaign of 1985–1988. The campaign significantly curtailed the production and retail sales of alcohol, and increased alcohol prices in those years. As shown in Fig. 2, this period of reduced alcohol consumption coincided with sharply declining male mortality rates in Russia. Recent research connects this campaign with the mortality crisis of the early 1990s, demonstrating that a large share of the excess deaths in 1990–1994 was due to lagged “catch-up” mortality from the end of the anti-alcohol campaign (Bhattacharya et al. 2013). This study uses the variation in campaign intensity across Russia’s regions to identify the causal relationship between the anti-alcohol regulations and later mortality in Russia. To the best of my knowledge, this is the only paper in the economics literature that uses a quasi-experimental identification strategy to determine the causal effect of any policy or variable on the Russian mortality crisis. As discussed below, Kueng and Yakovlev (2021) further demonstrate that Gorbachev’s anti-alcohol campaign changed the tastes of younger cohorts in favor of beer over vodka. Ironically, while the anti-alcohol campaign helped to create the conditions for the mortality crisis of 1990–1994, the campaign’s enduring impact on tastes has also contributed to the steep declines in mortality in recent years.
The Role of Government Policy in the Post-2005 Mortality Gains
The quasi-experimental studies of Gorbachev’s anti-alcohol campaign provide convincing evidence of the powerful and long-lasting effects of alcohol control policies on alcohol consumption and male mortality in Russia. Although causal evidence is lacking on other causes of the Russian mortality crisis, few observers would dispute that the absence of strong alcohol control policies in the early 1990s contributed to the upsurge in alcohol-related mortality in those years, as well as to the increase in deaths after the 1998 financial crisis. As discussed below, the anti-alcohol policies implemented after 2005 appear to have played a role in recent life expectancy gains. In other words, government alcohol control policies have played, and continue to play, a critical role in male mortality change in Russia.
Tobacco control policies have received less attention in the literature, but these policies also have a significant impact on male mortality rates in Russia. Recent estimates indicate that smoking accounted for 26% of all male deaths in Russia in 2001 (and only 3% of female deaths; see Shkolnikov et al. 2020). Denisova (2010), using individual-level panel data from the Russian Longitudinal Monitoring Survey for 1994–2007, found that the negative impact of smoking on longevity in Russia is comparable to the effect of alcohol consumption on longevity. In light of this, it is unsurprising that the expansive anti-alcohol and tobacco control policies implemented in Russia since the mid-2000s could powerfully combine to reduce alcohol- and tobacco-related deaths. The following section briefly describes these policies and recent studies assessing their effectiveness in reducing mortality. The focus here, and in much of the research, is on male mortality as it is most closely linked with alcohol and tobacco control policies.
Smoking Prevalence and Tobacco Control Policies in Russia
For many years, about 60% of Russian men reported themselves as regular smokers, which was one of the highest male smoking rates in the world. Smoking prevalence is significantly lower among Russian women (10–12 percent), although the share of women who smoke increased from the mid-1990s until the mid-2000s, particularly among less-educated women (Shkolnikov et al. 2020). Male smoking rates started declining around 2007 and, as of 2016, had fallen by more than 10 percentage points, a remarkable decline in smoking prevalence in less than a decade among a population whose smoking rate had not changed in several decades.6
The high prevalence of smoking among Russian men is consistent with the near-absence of regulation of the tobacco market in the Soviet Union and Russia prior to 2010, and with the relatively low price of cigarettes in the country. Russia was a latecomer to ratifying the Framework Convention on Tobacco Control (2008), and subsequently developed its National Strategy on Creation of a Public Policy to Combat Tobacco Consumption in 2010. The first significant legislation passed in Russia to regulate the tobacco market was the Federal Tobacco Control Law, which came into effect on July 1, 2013. This law banned smoking in all public places, banned all types of tobacco advertising and sponsorships, and required pictorial warnings on cigarette packages (Quirmbach and Gerry 2016). These regulations are well-enforced across the Russian Federation (Gambaryan et al. 2018). In conjunction with these regulations, rising excise taxes led the real price of a pack cigarettes to nearly triple between 2008 and 2017, from 11.06 rb/pack (2002 rb) to 30.90 rb, although cigarette prices remain low in comparison with other countries (Zheng et al. 2018).
Did the tobacco control regulations and price increases cause the decline in male smoking prevalence? Given data limitations, it is difficult to conduct empirical tests on the role the smoking bans played, as compared to the rising price of cigarettes. Instead, I examine whether the timing of the change in male smoking prevalence—and its components, declining smoking initiation and increased cessation—is coincident with the earlier increase in cigarette prices or the somewhat later tobacco control regulations.
I use the Global Adult Tobacco Surveys (GATS) of Russia in 2009 and 2016 to estimate smoking prevalence by sex and year since 1990. GATS is a nationally representative survey of individuals aged 15 and older, and it includes questions about the year and age of smoking initiation and cessation, enabling one to form a retrospective panel of smoking history in each year for each individual. Retrospective smoking information is, of course, subject to recall error. However, Krall et al. (1989) find that retrospective accounts of smoking behavior are accurate: comparing longitudinal records with subjects’ recollection of their smoking status 20 (32) years prior shows correct recall among 90 (87)% of subjects, with no differences in accuracy by sex or smoking status at interview. To examine prevalence, initiation and cessation, I form a panel with one observation per person per year, from age 15 to 60.7 Prior to the Tobacco Control Act and the increased price of cigarettes, the annual hazard of smoking initiation was around 4.8% for men, and the hazard rate of cessation was approximately 1.0 percent.8
Figure 3 illustrates that the decline in smoking prevalence among men began two or three years before cigarette prices started to rise, and about six years before the passage of the Tobacco Control Law. The decline in smoking prevalence was due to both increased cessation to 3–4%, and decreased initiation (to less than 1 percent), with both trends starting before the cigarette price increases and the passage of the Tobacco Control Law (Appendix Figure 5a and 5b). It is unclear what might have caused the early decline in male smoking prevalence, but the later declines were likely accelerated by the combined effect of rising cigarette prices and the significant restrictions on smoking behavior embodied in the Tobacco Control Law.
Fig. 3.

Sources: Zheng et al. (2018) (real cigarette price); smoking prevalence calculated from the Global Adult Tobacco Survey for Russia 2009, 2016
Given that the hazard of death associated with smoking is about two times that of nonsmokers, it is worthwhile to investigate whether declining smoking prevalence, contributed to recent mortality declines among men. While it is too soon for lung cancer mortality to decline due to decreased smoking prevalence, as these deaths occur with a lag of several decades after smoking initiation, lower smoking rates may already be contributing to decreased male cardiovascular mortality. The risk of cardiovascular mortality (particularly deaths due to vascular diseases, such as ischemic heart disease (Lopez et al. 1994)) declines rapidly after smoking cessation, and the difference in cardiovascular mortality risk between smokers and non-smokers goes to zero within 10 years of quitting (Shkolnikov et al. 2020). There is already some evidence of the impact of the Tobacco Control Law on the incidence of cardiovascular disease: Gambaryan et al. (2018) use synthetic control methods to demonstrate that hospital discharge rates for cardiovascular disease declined in Russia relative to a synthetic control country after the Tobacco Control Law was implemented. Shkolnikov et al. (2020) estimate that 48,000 male cardiovascular deaths were avoided in 2008–2016 due to the decrease in male smoking rates, which is about 6.2% of all male deaths in that period.
It appears that government policy to reduce smoking prevalence, including increased cigarette prices and a comprehensive ban on public smoking, contributed to declining cardiovascular mortality among men in the post-2005 period (but not among women, as female smoking rates were already low and declined less than male smoking rates). The contribution is relatively modest, but if trends in smoking prevalence continue, it can be expected that cardiovascular and, eventually, cancer mortality will decline substantially in future years.
Anti-Alcohol Policies: Legacies of the Past, into the Present and Future
The anti-alcohol campaign of 1985–1988 provided strong evidence of the impact of alcohol consumption, and alcohol control policies, on male mortality in Russia. Recent research demonstrates that this anti-alcohol campaign had even more far-reaching effects on alcohol consumption and male mortality than first recognized. Kueng and Yakovlev (2021) exploit urban-rural differences in anti-alcohol campaign intensity to identify the causal effect of the campaign on tastes. The results indicate that young adults who had less access to hard liquor developed preferences for light alcohol (beer) over vodka, and these taste differences persist decades later. Most of the change in tastes for beer is driven by cohort effects; in other words, there are much smaller changes in alcohol preferences and consumption patterns within cohorts over time.
The paper also demonstrates that the large expansion of the beer market in the late 1990s had a similar effect on tastes. Individuals who were more exposed to the expansion of the beer market developed stronger preferences for beer over vodka, compared to less-exposed individuals. The authors estimate that the shift in tastes and resulting decline in vodka consumption explains half the decline in male mortality since 2003. A key takeaway from this study is that today’s policy changes can have important long-run consequences for tastes and consumer behavior, implying that the strong alcohol control policies adopted in Russia will also have long-lasting effects.
These alcohol control policies occurred in roughly two phases.9 The first phase began with new regulations on the production, distribution and retail sales of alcohol and non-beverage alcohol products, which took effect on January 1, 2006.10 These regulations included required electronic surveillance systems tracking the movement of alcohol and its raw ingredients through the distribution system, and a costly new licensing system and excise stamps for the production and sale of alcohol products. Producers of non-beverage alcohol products were required to add denaturant to those products to make them unfit for consumption. The increased cost of operating in the alcohol market led to a decline in the number of alcohol producers and distributors in the market, and the major reorganization of the alcohol market led to shortages of alcohol beverages in 2006 due to implementation problems (Levintova 2007; Penina 2017). However, despite the initial problems, these policies appeared to succeed in reducing deaths due to alcohol poisonings (Pridemore et al. 2014).
The second phase of alcohol control policies began in 2010 with policies that targeted alcohol prices and additional restrictions on advertising and alcohol sales. Excise taxes increased by 30% in 2011–2012, and by an additional 80% in 2013–2014 (Penina 2017), resulting in a more than doubling of the price of a half-liter bottle of vodka between 2010 and 2014 (Neufeld and Rehm 2018). The additional restrictions included a ban on the sale of all alcohol at kiosks, and a ban on alcohol sales from 11pm to 8am.11
While implementation and enforcement of the new regulations has been somewhat inconsistent, the evidence suggests that the measures have succeeded in reducing both recorded and unrecorded alcohol consumption—although unrecorded alcohol consumption remains high (Neufeld and Rehm 2018). Nevertheless, these policy measures are by far the most stringent attempts to reduce harmful alcohol consumption in Russia, since the 1985–1988 anti-alcohol campaign.
Have Anti-Alcohol Policies Reduced Deaths in Russia?
It is difficult to credibly test the effect of these anti-alcohol policies because they were largely implemented at the federal level and were multifaceted, involving many regulations that came into effect at the same time. Other changes occurring in the same period—in particular the Tobacco Control Law and increased price of cigarettes, and the improvements in health care access, quality and medical technology—further confound efforts to separately identify the impact of alcohol control policies on mortality.
As a straightforward test of whether Russia’s anti-alcohol policies contributed to reduced death rates, I estimate a difference-in-differences regression comparing the change in death rates in (historically) low-alcohol consuming regions versus high-alcohol consuming regions. If anti-alcohol policies reduce deaths, one should observe greater declines in deaths in regions with high alcohol consumption relative to regions with low consumption. This research strategy is similar to that used in Bhattacharya et al. (2013) for the effects of the anti-alcohol campaign on mortality, and to that of other studies of the impact of disease agents that exploit differential pre-campaign exposure across regions to estimate the impact of population-wide disease eradication campaigns (e.g., Bleakley 2007, 2010).
The data used are regional (oblast-level) death rates by five-year age group and cause for 2000–2018 from the Russian Fertility and Mortality database of the Centre of Demographic Research of the New Economic School.12 The mortality data are supplemented with regional data on economic and social conditions from the Federal State Statistics Service (https://rosstat.gov.ru/). The death rates are age-standardized using the European population, and are grouped into broad causes of death, based on ICD9 and ICD10 codes. “Low” and “high” alcohol consumption are defined by whether a region’s 1990 per capita consumption of pure ethanol was above or below the median consumption level across Russia’s regions. This is admittedly a crude indicator, particularly as it excludes unrecorded alcohol consumption (among other problems), but it nevertheless should group the regions into those that are relatively high alcohol-consuming regions versus low-consuming regions. There were wide regional differences in alcohol consumption in 1990, ranging from 1.4 to 8.6 liters per capita, as well as wide regional differences in mortality rates, as shown in Fig. 4a for male circulatory disease mortality and in Fig. 4b for male mortality due to external causes. Descriptive statistics from the regional mortality data are shown in Table 2 and reflect that regions with lower alcohol consumption have fewer deaths due to external causes and due to cardiovascular disease than do regions with higher alcohol consumption.
Fig. 4.

Author's calculations. Source: Russian Fertility and Mortality Database
Table 2.
Summary statistics, 2000–2018 average. Source: Russian Fertility and Mortality Database
| Low alcohol regions | High alcohol regions | |||||
|---|---|---|---|---|---|---|
| Mean | SD | N | Mean | SD | N | |
| Male death rate per 100K | ||||||
| SDR all causes, 25–64 | 1487.8 | 392.8 | 684 | 1599.4 | 480.1 | 684 |
| Circulatory, 40–54 | 521.7 | 165.7 | 684 | 564.1 | 200.7 | 684 |
| External, 40–54 | 416.8 | 182.6 | 684 | 450.7 | 224.6 | 684 |
| Neoplasms, 40–54 | 164.3 | 31.6 | 684 | 168.3 | 37.8 | 684 |
| Female death rate per 100K | ||||||
| SDR all causes, 25–64 | 476.0 | 129.2 | 684 | 521.0 | 140.0 | 684 |
| Circulatory, 40–54 | 141.5 | 52.2 | 684 | 155.9 | 59.3 | 684 |
| External, 40–54 | 82.3 | 45.4 | 684 | 94.1 | 50.8 | 684 |
| Neoplasms, 40–54 | 115.0 | 17.3 | 684 | 119.8 | 15.3 | 684 |
Weighted by 2000 regional population
The empirical tests using the following regression specification:
Define: Dr = 0 if region has < median alcohol consumption in 1990 (official data)
Dr = 1 if region has >= median alcohol consumption in 1990
Basic specification:
where log(death rate)rt is the age-standardized death rate in region r in year t, γy are year fixed effects, δr are region fixed effects and Xrt are covariates that vary by region and time: log(real gross regional product per capita), log(unemployment rate), poverty rate, net migration rate, share urban population and a measure of air pollution per square kilometer. θt is the coefficient of interest, indicating the percentage difference in mortality rates between high- and low alcohol consumption regions in each year, relative to 2000 (the omitted base year). If the anti-alcohol policies succeed in reducing alcohol-related deaths, this impact should be greater in the high-alcohol consuming regions than in the lower alcohol-consuming regions. This impact should become apparent after the implementation of the anti-alcohol policies in 2006 and/or 2010, and for causes of death that are most correlated with alcohol consumption, such as external causes and cardiovascular mortality. Given the many other changes in public policies and medical care occurring at the same time, these results are suggestive (at best), and cannot be interpreted as showing a causal relationship between mortality and the alcohol control policies.
A representative set of results of the difference-in-differences regressions is shown in Fig. 5, which illustrates the θt coefficients, and their 95% confidence intervals over time for three different causes of death. The top panel show the results for circulatory disease deaths for men aged 25 to 64. Prior to 2006, there was little discernible difference in cardiovascular mortality trends between the high- and low-alcohol consuming regions. After 2006, the death rate started to decline more in high-alcohol consuming regions relative to low-consuming regions, and this difference becomes larger after 2010. However, the confidence intervals are wide, and the difference is not statistically significant over the period.
Fig. 5.
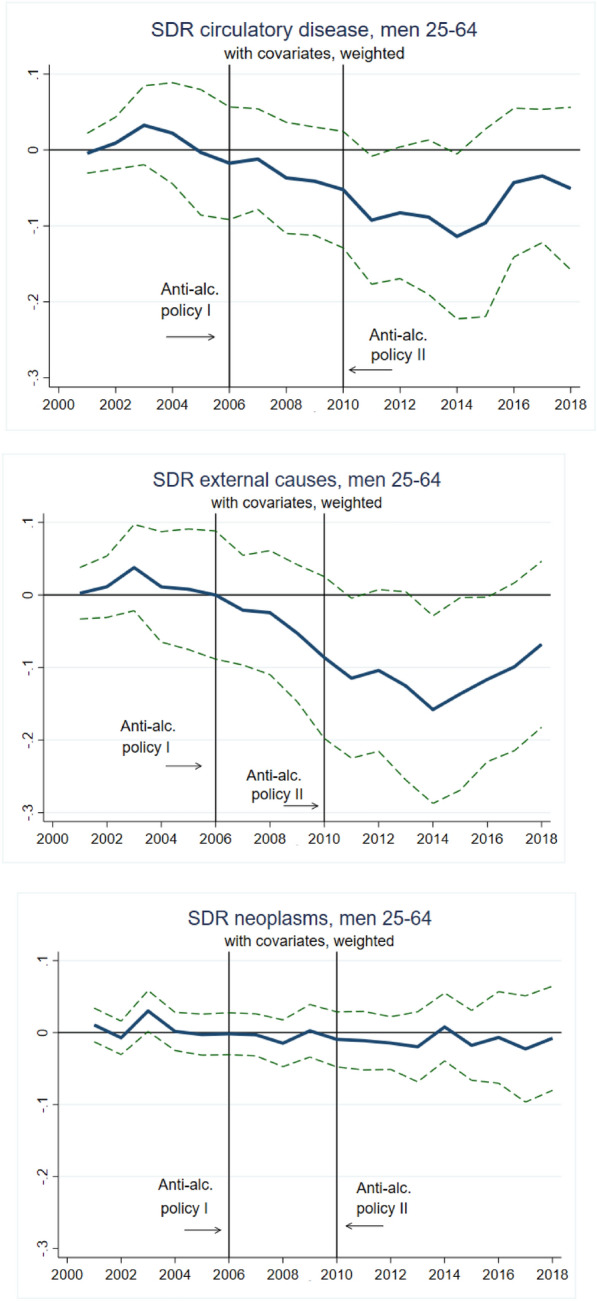
% Difference in mortality rates between high- and low-alcohol consumption regions
The middle panel illustrates the θt coefficients for deaths due to external causes for men aged 25 to 64. The pattern of coefficients is similar to that for circulatory disease deaths, but the difference in trends between high- and low-alcohol consuming regions is sharper, and reaches (marginal) statistical significance in 2014. In contrast to the circulatory disease deaths, the external cause death results would not be affected by the confounding factors of rising cigarette prices and stringent tobacco control regulations that occurred in these years. The third panel illustrates that there is no effect of the policies on the differences in mortality due to neoplasms (cancers) in high- versus low-alcohol consuming regions, as expected. Perhaps surprisingly, the same regressions using the standardized death rate from alcohol poisoning for men aged 25 to 64 as the dependent variable show no differences in the effect of the alcohol control policies on high- versus low-alcohol consuming regions; confidence intervals are wide, and there is no clear trend in coefficient magnitude over time.
To summarize, the evidence is mixed that the anti-alcohol policies caused declining male mortality after 2005. The trends in cardiovascular mortality and especially external cause mortality are suggestive that it is the case, but the lack of any relationship with mortality from alcohol poisoning points to additional factors that are not captured in this empirical approach.
Concluding Remarks
30 years since the demographic catastrophe that afflicted Russia in the early years of its transition from communism, the mortality outlook in that country is almost unrecognizable. Life expectancy gains have been large and rapid, and life expectancy for both men and women reached its highest level in Russia’s history in 2019. Cardiovascular mortality and external cause mortality, both astonishingly high in the early years of transition, have fallen significantly, and are the main factors in declining death rates.
The mortality trends in Russia appear to run in parallel with public policy developments: policies on alcohol and tobacco control have evolved from a near-absence of any regulations in the early 1990s to comprehensive, multi-faceted policies that affect all aspects of alcohol and tobacco pricing, distribution and retail sales. While challenges remain in identifying the causal effects of these policies on mortality, earlier evidence from Gorbachev’s anti-alcohol campaign suggests that the alcohol control measures could have long-lasting and powerfully beneficial effects on adult male mortality in the country. These anti-alcohol policies will likely work in combination with the strong tobacco control policies implemented in the post-2005 period to further reduce cardiovascular death rates and, eventually, deaths due to smoking-related cancers.
Many pressing questions remain for researchers to investigate. For example, few studies have investigated the causes of the remarkable improvements in life expectancy in Eastern Europe, or in other countries of the former Soviet Union. What is the role played by improved quality of medical care, or changing diet and nutrition? How much of the decline in Russian male mortality is due to the expansion of the beer market versus the significant alcohol control policies? Even fewer studies have examined the causes of changing female life expectancy in the region, which would provide insights into factors that are less related to alcohol consumption and high smoking rates. As always, the demographic history of Russia and its neighbors remains a rich and important area for future research.
Supplementary Information
Below is the link to the electronic supplementary material.
Footnotes
For comparison, the increase in mortality due to COVID-19 is projected to decrease US life expectancy by 1.13 years in 2020 (Andrasfay and Goldman 2021).
The infant mortality rate in Russia increased from 17.8 to 19.9 deaths per 1000 births from 1991 to 1993. The infant mortality rate has declined since 1993, and fell to 4.9 deaths per 1000 births by 2019 (Federal State Statistics Service: https://rosstat.gov.ru/).
See Brainerd (2001) for an analysis of the suicide epidemic in the former Soviet Union.
See Brainerd (2010), which uses child and adult stature to assess living standards in the Soviet Union over the 20th century.
The Russian Longitudinal Monitoring Survey (https://rlms-hse.cpc.unc.edu/) is a high-quality panel survey, but the first useable round of the survey is in 1994.
Smoking prevalence in this paper is estimated using the 2009 and 2006 Global Adult Tobacco Surveys for Russia, as described in greater detail below. See Shkolnikov et al. (2020) for a comprehensive overview of smoking prevalence in Russia using multiple data sources.
An upper bound of age 60 is used to avoid the effect of selective mortality of smokers on the estimate of smoking prevalence, which appears to occur at age 60 and over (Shkolnikov et al. 2020). The life-course approach to smoking behavior used here follows that developed in Lillard et al. 2013. See Quirmbach and Gerry (2016) for a life-course approach to smoking among men and women in Russia using the GATS and RLMS.
Hazard rates of initiation and cessation are estimated using a three-year moving average. Hazard rates are much lower for women.
For further details on alcohol control policies in Russia, see Levintova (2007), Pridemore et al. (2014), Grigoriev and Andreev (2015), Radaev (2015), Penina (2017), Neufeld and Rehm (2018), Nemtsov et al. (2019) and Danilova et al. (2020). Yakovlev (2015) provides an overview of alcohol and mortality in Eastern Europe and discusses the effectiveness of various regulatory approaches to reducing alcohol consumption.
Implementation of some of the regulations was delayed until July 1, 2006.
There is some concern and evidence that higher prices and restrictions on legal alcohol sales might lead heavy drinkers to increase consumption of non-beverage alcohol surrogates. Skorobogatov (2021) tests for unintended effects of local strong alcohol sales hours restrictions on the consumption of surrogates using a difference-in-differences approach, exploiting varying hours restrictions introduced at different times across regions in 2005-2010. Results show that the mean hours restriction was associated with 16% higher alcohol poisoning mortality.
I thank Nauro Campos (the editor), two anonymous referees, Louise Grogan, Barry Ickes, Richard Pomfret and participants in the Association for Comparative Economics Studies panel at the ASSA 2021 meetings on “Thirty Years Since the Dissolution of the Soviet Union” for helpful comments and suggestions.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Adserà, Alicia, Francesca Dalla Pozza, Sergei Guriev, Lukas Kleine-Rueschkamp, and Elena Nikolova. 2019. Transition from Plan to Market, Height and Well-Being. CEPR Discussion Paper 14027.
- Andrasfay Theresa, Goldman Noreen. Reductions in 2020 US Life Expectancy Due to COVID-19 and the Disproportionate Impact on the Black and Latino Populations. PNAS. 2021;118(5):1–6. doi: 10.1073/pnas.2014746118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhattacharya Jay, Gathmann Christina, Miller Grant. The Gorbachev Anti-Alcohol Campaign and Russia’s Mortality Crisis. American Economic Journal: Applied Economics. 2013;5(2):232–260. doi: 10.1257/app.5.2.232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bleakley Hoyt. Disease and Development: Evidence from Hookworm Eradication in the American South. Quarterly Journal of Economics. 2007;122(1):73–117. doi: 10.1162/qjec.121.1.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bleakley Hoyt. Malaria Eradication in the Americas: A Retrospective Analysis of Childhood Exposure. American Economic Journal: Applied Economics. 2010;2(2):1–45. doi: 10.1257/app.2.2.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brainerd Elizabeth. Economic Reform and Mortality in the Former Soviet Union: A Study of the Suicide Epidemic in the 1990s. European Economic Review. 2001;45(4–6):1007–1019. doi: 10.1016/S0014-2921(01)00108-8. [DOI] [Google Scholar]
- Brainerd Elizabeth. Reassessing the Standard of Living in the Soviet Union: An Analysis Using Archival and Anthropometric Data. Journal of Economic History. 2010;70(1):83–117. doi: 10.1017/S0022050710000069. [DOI] [Google Scholar]
- Brainerd Elizabeth, Cutler David M. Autopsy on an Empire: Understanding Mortality in Russia and the Former Soviet Union. Journal of Economic Perspectives. 2005;19(1):107–130. doi: 10.1257/0895330053147921. [DOI] [Google Scholar]
- Case Anne, Deaton Angus. Rising Morbidity and Mortality in Midlife Among White Non-Hispanic Americans in the 21st Century. Proceedings of the National Academy of Sciences. 2015;112(49):15078–15083. doi: 10.1073/pnas.1518393112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornia, Giovanni Andrea and Renato Paniccia. 2000. The Transition Mortality Crisis: Evidence. Interpretation and Policy Responses. In The Mortality Crisis in Transitional Economies. Giovanni Andrea Cornia and Renato Panato, eds. Oxford, UK: Oxford University Press, pp. 3-37.
- Cornia, Giovanni Andrea. 2016. The Mortality Crisis in Transition Economies. IZA World of Labor.
- Cutler David M, et al. Financial Crisis, Health Outcomes and Aging: Mexico in the 1980s and 1990s. Journal of Public Economics. 2002;84(2):279–303. doi: 10.1016/S0047-2727(01)00127-X. [DOI] [Google Scholar]
- Danilova Inna, Shkolnikov Vladimir M, Andreev Evgeny, Leon David A. The Changing Relation Between Alcohol and Life Expectancy in Russia in 1965–2017. Drug and Alcohol Review. 2020;39:790–796. doi: 10.1111/dar.13034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Denisova Irina. Adult Mortality in Russia: A Microanalysis. Economics of Transition. 2010;18(2):333–363. doi: 10.1111/j.1468-0351.2009.00384.x. [DOI] [Google Scholar]
- Gambaryan, Marine, Aaron Reeves, Alexander Deev, Marina Popovich, Oxana Drapkina, Andrew Snell, David Stuckler, Kristina Mauer-Stender, Bente Mikkelsen and Sergey Boytsov. 2018. Effects of Tobacco Control Policy on Cardiovascular Morbidity and Mortality in Russia. European Journal of Public Health 28(suppl_2):14-16. [DOI] [PMC free article] [PubMed]
- Gavrilova Natalia S, Semyonova Victoria G, Dubrovina Elena, Evdokushkina Galina N, Ivanova Alla E, Gavrilov Leonid A. Russian Mortality Crisis and the Quality of Vital Statistics. Population Research and Policy Review. 2008;27(5):551–574. doi: 10.1007/s11113-008-9085-6. [DOI] [Google Scholar]
- Global Adult Tobacco Survey. https://nccd.cdc.gov/GTSSDataSurveyResources/Ancillary/Documentation.aspx?SUID=4&DOCT=1
- Grigoriev, Pa el and Evgeny M. Andreev. 2015. The Huge Reduction in Adult Male Mortality in Belarus and Russia: Is It Attributable to Anti-Alcohol Measures? PLoS ONE 10(9): e0138021. [DOI] [PMC free article] [PubMed]
- Guriev Sergei, Melnikov Nikita. Happiness Convergence in Transition Countries. Journal of Comparative Economics. 2018;46(3):683–707. doi: 10.1016/j.jce.2018.07.003. [DOI] [Google Scholar]
- Guriev Sergei, Zhuravskaya Ekaterina. (Un)Happiness in Transition. Journal of Economic Perspectives. 2009;23(2):143–168. doi: 10.1257/jep.23.2.143. [DOI] [Google Scholar]
- Kontsevaya Anna, Sabgaida T, Ivanova A, Leon DA, McKee M. How Has the Management of Acute Coronary Syndrome Changed in the Russian Federation During the Last 10 Years? Health Policy. 2017;121(12):1274–1279. doi: 10.1016/j.healthpol.2017.09.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krall EA, Valadian I, Dwyer JT, Gardner J. Accuracy of Recalled Smoking Data. American Journal of Public Health. 1989;79(2):200–202. doi: 10.2105/AJPH.79.2.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kueng Lorenz, Yakovlev Evgeny. The Long-Run Effects of a Public Policy on Alcohol Tastes and Mortality. American Economic Journal: Economic Policy. 2021;13(1):294–328. [Google Scholar]
- Kumo Kazuhiro. Changes in Mortality: Meta-Analysis. In: Karabchuk Tatiana, Kumo Kazuhiro, Selezneva Ekaterina., editors. Demography of Russia: From the Past to the Present. London: Palgrave Macmillan; 2017. pp. 219–259. [Google Scholar]
- Leon David A, Saburova Lyudmila, Tomkins Susannah, Andreev Evgueny, Kiryanov Nikolay, McKee Martin, Shkolnikov Vladimir M. Hazardous Alcohol Drinking and Premature Mortality in Russia: A Population Based Case-Control Study. The Lancet. 2007;369:2001–2009. doi: 10.1016/S0140-6736(07)60941-6. [DOI] [PubMed] [Google Scholar]
- Levintova Marya. Russian Alcohol Policy in the Making. Alcohol and Alcoholism. 2007;42(5):500–505. doi: 10.1093/alcalc/agm040. [DOI] [PubMed] [Google Scholar]
- Lopez Alan D, Collishaw Neil E, Piha Tapani. A Descriptive Model of the Cigarette Epidemic in Developed Countries. Tobacco Control. 1994;3:242–247. doi: 10.1136/tc.3.3.242. [DOI] [Google Scholar]
- Malyutina Sofia, Bobak Martin, Kurilovitch Svetlana, Gafarov Valery, Simonova Galina, Nikitin Yuri, Marmot Michael. Relation Between Heavy and Binge Drinking and All-Cause and Cardiovascular Mortality in Novosibirisk, Russia: A Prospective Cohort Study. Lancet. 2002;360(9344):1448–1454. doi: 10.1016/S0140-6736(02)11470-X. [DOI] [PubMed] [Google Scholar]
- McKee Martin, Britton Annie. The Positive Relationship Between Alcohol and Heart Disease in Eastern Europe: Potential Physiological Mechanisms. Journal of the Royal Society of Medicine. 1998;91:402–407. doi: 10.1177/014107689809100802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKee, Martin, S. Süzcs, A. Sárváry, R. Ádany, N. Kiryanov, L. Saburova, S. Tomkins, E. Andreev, and D.A. Leon. 2005. The Composition of Surrogate Alcohols Consumed in Russia. Alcoholism: Clinical and Experimental Research, 29(10): 1884-8. [DOI] [PubMed]
- Murphy Michael, Martin Bobak, Nicholson Amanda, Rose Richard, Marmot Michael. The Widening Gap in Mortality by Educational Level in the Russian Federation, 1980–2001. American Journal of Public Health. 2006;96(7):1293–1299. doi: 10.2105/AJPH.2004.056929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nemtsov Alexander, Neufeld Maria, Rehm Jürgen. Are Trends in Alcohol Consumption and Cause-Specific Mortality in Russia Between 1990 and 2017 the Result of Alcohol Policy Measures? Journal of Studies on Alcohol and Drugs. 2019;80(5):489–498. doi: 10.15288/jsad.2019.80.489. [DOI] [PubMed] [Google Scholar]
- Neufeld Maria, Rehm Jürgen. Effectiveness of Policy Changes to Reduce Harm from Unrecorded Alcohol in Russia Between 2005 and Now. International Journal of Drug Policy. 2018;51:1–9. doi: 10.1016/j.drugpo.2017.09.006. [DOI] [PubMed] [Google Scholar]
- Penina Olga. Alcohol-Related Causes of Death and Drinking Patterns in Moldova as Compared to Russia and Ukraine. European Journal of Population. 2017;33(5):679–700. doi: 10.1007/s10680-017-9450-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pridemore, W. A., M. B. Chamlin, M. T. Kaylen, & E. Andreev 2014. The Effects of the 2006 Russian Alcohol Policy on Alcohol-Related Mortality: An Interrupted Time Series Analysis. Alcoholism: Clinical and Experimental Research 38: 257–266. [DOI] [PubMed]
- Quirmbach Diana, Gerry Christopher J. Gender, Education and Russia's Tobacco Epidemic: A Life-Course Approach. Social Science and Medicine. 2016;160:54–66. doi: 10.1016/j.socscimed.2016.05.008. [DOI] [PubMed] [Google Scholar]
- Radaev, Vadim. 2015. Impact of a New Alcohol Policy on Homemade Alcohol Consumption and Sales in Russia. Alcohol and Alcoholism 50(3): 365–372. [DOI] [PubMed]
- Russian Fertility and Mortality Database. Center for Demographic Research, New Economic School, Moscow. http://demogr.nes.ru/index.php/ru/demogr_indicat/data data downloaded on 12 Dec 2020.
- Shapiro Judith. The Russian Mortality Crisis and Its Causes. In: Aslund Anders., editor. Russian Economic Reform in Jeopardy? London and New York: Pinter Publishers; 1995. pp. 149–178. [Google Scholar]
- Shkolnikov Vladimir M, Andreev Evgeny M, McKee Martin, Leon David A. Components and Possible Determinants of Decrease in Russian Mortality in 2004–2010. Demographic Research. 2013;28:917–950. doi: 10.4054/DemRes.2013.28.32. [DOI] [Google Scholar]
- Shkolnikov, Vladimir, France Meslé, and David A. Leon. 2001. Premature Circulatory Disease Mortality in Russia in Light of Population- and Individual-Level Disease. In Weidner, G., Kopp S.M., and Kristenson, M., editors, Heart Disease: Environment, Stress and Gender (NATO Science Series, Series I: Life and Behavioural Sciences).
- Shkolnikov, Vladimir. M., Elena Churilova, Dmitry A. Jdanov,, Svetlana A. Shalnova,, Odd Nilssen, Alexander Kudryavtsev,, Sarah Cook, Sofia Malyutina, Martin McKee, and David A. Leon. 2020. Time Trends in Smoking in Russia in the Light of Recent Tobacco Control Measures: Synthesis of Evidence from Multiple Sources. BMC Public Health, 20(1), 378. [DOI] [PMC free article] [PubMed]
- Skorobogatov, Alexander S. 2021. The Effect of Alcohol Sales Restrictions on Alcohol Poisoning Mortality: Evidence from Russia. Forthcoming, Health Economics. [DOI] [PubMed]
- Treisman Daniel. Death and Prices: The Political Economy of Russia’s Alcohol Crisis. Economics of Transition. 2010;18(2):281–331. doi: 10.1111/j.1468-0351.2009.00382.x. [DOI] [Google Scholar]
- Vladimir Skholnikov, Cornia Giovanni Andrea, Leon David A, Meslé France. Causes of the Russian Mortality Crisis: Evidence and Interpretations. World Development. 1998;26(11):1995–2011. doi: 10.1016/S0305-750X(98)00102-8. [DOI] [Google Scholar]
- WHO Mortality Database. https://www.who.int/data/data-collection-tools/who-mortality-database
- Yakovlev Evgeny. Demand for Alcohol Consumption in Russia and Its Implication for Mortality. American Economic Journal: Applied Economics. 2018;10(1):106–149. [Google Scholar]
- Yakovlev, Evgeny. 2015. Alcoholism and Mortality in Eastern Europe. IZA World of Labor 1.
- Zaridze David, Maximovitch Dimitri, Lazarev Alexander, Igitov Vladimir, Boroda Alex, Boreham Jillian, Boyle Peter, Peto Richard, Boffetta Paolo. Alcohol Poisoning is a Main Determinant of Recent Mortality Trends in Russia: Evidence from a Detailed Analysis of Mortality Statistics and Autopsies. International Journal of Epidemiology. 2009;38:143–153. doi: 10.1093/ije/dyn160. [DOI] [PubMed] [Google Scholar]
- Zaridze David, Brennan Paul, Boreham Jillian, Boroda Alex, Karpov Rostislav, Lazarev Alexander, Konobeevskaya Irina, Igitov Vladimir, Terechova Tatiana, Boffetta Paolo, Peto Richard. Alcohol and Cause-Specific Mortality in Russia: A Retrospective Case-Control Study of 48,557 Adult Deaths. The Lancet. 2009;373:2201–2214. doi: 10.1016/S0140-6736(09)61034-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zheng, Rong, Patricio V. Marquez, Polina Kuznetsova, Xiao Hu and Yang Wang. 2018. Cigarette Affordability in the Russian Federation 2002-2017. The World Bank Group.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.