

Key Points
Question
What is the role of lung cancer screening in survivors of head and neck cancer?
Findings
In this ad hoc secondary analysis of a large randomized clinical trial, 171 head and neck cancer survivors with a long smoking history were identified. These individuals had 2.5 times the rate of lung cancer as those without prior head and neck cancer.
Meaning
These results support annual low-dose computed tomography chest screening for lung cancer in head and neck cancer survivors who have a significant smoking history and are fit to undergo curative treatment.
This randomized clinical trial uses data from the National Lung Screening Trial to investigate the role of lung cancer screening—specifically, low-dose computed tomography vs chest radiography—in head and neck cancer survivors.
Abstract
Importance
In head and neck cancer survivors, lung cancer screening may aid in detecting a second primary lung cancer or metastatic head and neck cancer earlier in the course of disease, which may improve treatment outcomes. However, no randomized data exist to assess the value of lung cancer screening in this population.
Objective
To evaluate the incidence of second primary lung cancer in survivors of head and neck cancer survivors with screening low-dose computed tomography (CT) vs chest radiography (CXR).
Design, Setting and Participants
For this ad hoc secondary analysis of a randomized clinical trial, head and neck cancer survivors were identified from the National Lung Screening Trial, which enrolled participants from August 2002 to April 2004. This randomized clinical trial compared screening using low-dose CT chest vs CXR in patients aged 55 to 74 years with at least a 30 pack-year history of cigarette smoking and who were current smokers or had quit within the past 15 years and who were at high risk for lung cancer. The incidences of second primary lung cancer and second primary head and neck cancer were compared with screening using low-dose CT vs CXR. Data were analyzed from December 1, 2020, to June 30, 2021.
Interventions
Screening low-dose CT of the chest vs CXR.
Main Outcomes and Measures
The primary outcome was the incidence of a second primary lung cancer.
Results
Among 53 452 enrolled participants, we identified 171 survivors of head and neck cancer, of whom 82 were screened with low-dose CT of the chest and 89 with CXR. Participants’ mean (SD) age was 61 (5) years, and 132 were men (77.2%). The incidence of lung cancer was higher among head and neck cancer survivors compared with participants without head and neck cancer (2080 per 100 000 person-years [2.1%] vs 609 per 100 000 person-years [0.6%]; adjusted rate ratio, 2.54; 95% CI, 1.63-3.95). In head and neck cancer survivors, the incidence of second primary lung cancer was 2610 cases per 100 000 person-years in the low-dose CT group vs 1594 cases per 100 000 person-years in the CXR group (rate ratio, 1.55; 95% CI, 0.59-3.63). In head and neck cancer survivors, overall survival was 7.07 years with low-dose CT vs 6.66 years with CXR (log-rank P = .48).
Conclusions and Relevance
The results of this ad hoc secondary analysis of a randomized clinical trial suggest that head and neck cancer survivors are at especially high risk for a second primary lung cancer. These findings underscore the importance of low-dose CT screening in head and neck cancer survivors with significant cigarette smoking history who are fit to undergo treatment with curative intent.
Introduction
Imaging after cancer treatment is used to identify residual cancer, recurrent initial cancer, and/or screen for second primary cancers at an earlier stage to hopefully provide curative treatment and improve subsequent outcomes. Among survivors of head and neck cancer (HNC), to our knowledge, no randomized data exist to help guide surveillance imaging beyond 6 months after treatment, and approaches to posttreatment imaging surveillance for HNC vary widely. As a result, the National Comprehensive Cancer Network Guidelines and American Society of Clinical Oncology HNC Survivorship Care Guideline do not recommend routine surveillance imaging for HNC beyond 6 months after treatment unless there are concerning signs or symptoms,1,2 whereas the American College of Radiology Neck Imaging Reporting and Data Systems white paper recommends surveillance imaging for the first 2 years after treatment.3
Survivors of HNC are at high risk of second primary cancers such as lung cancer, as 70% to 80% of HNC is associated with prior tobacco use.4,5,6 Current US Preventive Services Task Force (USPSTF) guidelines recommend low-dose computed tomography (CT) lung cancer screening annually for those aged 50 to 79 years with 20 pack-years or more, regardless of prior cancer status.7 However, USPSTF guidelines do not mention HNC as a risk factor for lung cancer.7 Furthermore, adherence to lung cancer screening recommendations is low, with only 14% of eligible individuals completing recommended screening.8
To examine the effects of lung cancer screening in survivors of HNC, we performed an ad hoc secondary analysis of a randomized clinical trial of lung cancer screening. Our primary goals were to (1) compare the rate of abnormal imaging findings in survivors of HNC vs participants without prior HNC, (2) compare the incidence of a secondary primary lung cancer (SPLC) in survivors of HNC vs participants without prior HNC, and (3) examine the benefits of low-dose CT vs chest radiography (CXR) lung cancer screening in survivors of HNC.
Methods
Data Source
For this ad hoc secondary analysis of a randomized clinical trial, we used data from the National Lung Screening Trial (NLST), the details of which have been previously published.9 Briefly, this trial randomized participants at high risk for lung cancer in a 1:1 ratio to screening low-dose CT of the chest vs CXR for lung cancer detection conducted at 33 medical centers in the US. This trial enrolled individuals aged 55 to 74 years with at least a 30 pack-year history of cigarette smoking and who were current smokers or had quit within the past 15 years. Participants underwent 3 screening examinations (times T0, T1, and T2) starting soon after randomization at 1-year intervals. Participants were randomized using a centralized system stratified by age, sex, and screening center. Enrollment took place from August 2002 through April 2004. Importantly for this subgroup analysis, participants were excluded from the NLST if they had a previous cancer diagnosis in the past 5 years. The NLST was funded by the National Cancer Institute. The trial protocol is available at the ClinicalTrials.gov website10 and in Supplement 1. The NLST was approved by the institutional review board at each participating institution, and this secondary analysis of trial data was approved by the Wayne State University institutional review board. Written informed consent was obtained from all participants. Our study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
Study Population
We identified a subset of participants in the NLST who were diagnosed with HNC before randomization (eFigure in Supplement 2). Race was self-reported by participants during study eligibility screening as required by the funding agency. We defined HNC survivors as any NLST participant who reported a history of oral cavity, pharynx, larynx, and/or nasal and sinus cancer. We made 2 sets of comparisons. First, we compared HNC survivors with participants without prior HNC to examine the incidence of abnormal imaging findings and examine the incidence of lung cancer. Second, in HNC survivors who were randomly assigned to low-dose CT chest vs CXR screening, we compared the incidence of SPLC and overall survival.
Outcomes
Our primary outcome was the incidence of SPLC in HNC survivors after randomization to either low-dose CT of the chest or CXR. Our secondary outcomes were the incidence of a second primary HNC (SPHNC), combined SPHNC or SPLC, and overall survival in HNC survivors. Additional secondary outcomes included the incidence of abnormal imaging findings suggestive of lung cancer and the incidence of lung cancer when comparing HNC survivors and participants without prior HNC history.
Statistical Analysis
We used unadjusted statistical models for comparisons in the group of HNC survivors randomized to either low-dose CT or CXR using the intention-to-screen principle. The primary outcome was a comparison of the incidence of SPLC after randomization to either low-dose CT or CXR. Event rates for the primary outcome were defined as in the primary analysis of the NLST based on the ratio of events to the person-years at risk for the event.11 We calculated CIs for the incidence of SPLC and used a log-rank test to compare survival of participants with prior HNC randomized to low-dose CT or CXR. For comparisons between HNC survivors and participants without prior HNC, there was a potential for confounding. Thus, we used a Cox proportional hazards model to test the relationship between prior HNC and development of lung cancer over time after adjusting for age, sex, race, and smoking pack-years. We performed statistical analyses using SPSS, version 26 (IBM Corp). Data were analyzed from December 1, 2020, to June 30, 2021.
Results
Cohort Description
Among the cohort of 53 452 participants in the NLST, we identified 171 HNC survivors who were enrolled a median of 9 years (range, 1-54 years) after HNC diagnosis. Of those survivors, 132 (77.2%) were men and 39 (22.8%) were women; 7 (4.1%) were Black; 154 (90.1%) were White; and 9 (5.6%) were of other race or ethnicity, including American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, multiple races, or unknown. Median follow-up after enrollment and randomization was 6.7 years (range, 0-8.2 years). Compared with all other patients, HNC survivors were more likely to be male (77.2% vs 58.9%; difference, 18.3%; 95% CI, 11.6-24.2) and had a more extensive cigarette smoking history (59 median pack-years [IQR, 44-80 pack-years] vs 48 median pack-years [IQR, 39-66 pack-years]; difference, 11 pack-years; 95% CI, 10-12 pack-years) (Table 1).
Table 1. Characteristics of Study Cohort at Enrollment.
| Characteristic | No. (%) | |||||
|---|---|---|---|---|---|---|
| Survivors of head and neck cancer | All other patients | |||||
| All (n = 171) | Low-dose CT chest (n = 82) | CXR (n = 89) | All (n = 53 281) | Low-dose CT chest (n = 26 551) | CXR (n = 26 505) | |
| Age at randomization, y | ||||||
| <55 | 0 | 0 | 0 | 5 (<0.1) | 2 (<0.1) | 3 (<0.1) |
| 55-59 | 37 (21.6) | 16 (19.5) | 21 (23.6) | 22 724 (42.8) | 11 382 (42.9) | 11 342 (42.8) |
| 60-64 | 52 (30.4) | 24 (29.3) | 28 (31.5) | 16 249 (30.5) | 8121 (30.6) | 8128 (30.7) |
| 65-69 | 44 (25.7) | 20 (24.4) | 24 (27.0) | 9432 (17.8) | 4722 (17.8) | 4710 (17.8) |
| 70-74 | 38 (22.2) | 22 (26.8) | 16 (18.0) | 4643 (8.8) | 2324 (8.8) | 2319 (8.7) |
| ≥75 | 0 | 0 | 0 | 4 (<0.1) | 1 (<0.1) | 3 (<0.1) |
| Sex | ||||||
| Male | 132 (77.2) | 69 (84.1) | 63 (70.8) | 31 275 (58.9) | 15 646 (58.9) | 15 629 (59.0) |
| Female | 39 (22.8) | 13 (15.9) | 26 (29.2) | 21 782 (41.1) | 10 906 (41.1) | 10 876 (41.0) |
| Race | ||||||
| Black | 7 (4.1) | 2 (2.4) | 5 (5.6) | 2364 (4.5) | 1191 (4.5) | 1173 (4.4) |
| White | 154 (90.1) | 76 (92.7) | 78 (87.6) | 48 353 (91.1) | 24 192 (91.1) | 24 161 (91.2) |
| Othera | 9 (5.8) | 4 (4.8) | 5 (6.7) | 2342 (4.4) | 1171 (4.4) | 1171 (4.4) |
| Cancer history | ||||||
| Nasal/sinus cancer | 21 (12.3) | 11 (13.4) | 10 (11.2) | NA | NA | NA |
| Oral cancer | 103 (60.2) | 51 (62.2) | 52 (58.4) | |||
| Pharyngeal cancer | 8 (4.7) | 3 (3.7) | 5 (5.6) | |||
| Laryngeal cancer | 46 (26.9) | 20 (24.4) | 26 (29.2) | |||
| Time since HNC diagnosis, median (IQR), y | 9 (6-13) | 10 (6-17) | ||||
| Tobacco use | ||||||
| Pack-years smoking, median (IQR) | 59 (44-80) | 60 (45-76) | 56 (44-83) | 48 (39-66) | 48 (39-66) | 48 (39-66) |
| Former smoker | 87 (50.9) | 40 (48.8) | 47 (52.8) | 27 504 (51.8) | 13 781 (51.9) | 13 723 (51.8) |
| Current smoker | 84 (49.1) | 42 (51.2) | 42 (47.2) | 25 553 (48.2) | 12 771 (48.1) | 12 782 (48.2) |
Abbreviations: CT, computed tomography; CXR, chest radiography; HNC, head and neck cancer; NA, not applicable.
Other included American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, multiple races, or unknown.
Results of Lung Screening Examinations
Among the 171 HNC survivors, 82 were screened with low-dose CT of the chest, and 89 were screened with CXR. At least 1 screening examination was suspicious for lung cancer in 35 participants (42.7%) in the low-dose CT group and 24 participants (27.0%) in the CXR group (Table 2). Survivors of HNC in the low-dose CT group were also more likely to have significant abnormalities identified at first screening that were not suspicious for lung cancer (15 participants [18.3%] vs 2 participants [2.2%]). Invasive procedures were performed in 8 HNC survivors (9.8%) in the low-dose CT group vs 2 (2.2%) in the CXR group. In the original NLST, lung cancer screening resulted in false-positive rates of 26.3% at baseline, 27.2% at year 1, and 15.9% at year 2.
Table 2. Results of Screening.
| Screening examination result | No. (%) | |||
|---|---|---|---|---|
| Survivors of head and neck cancer | All other patients | |||
| Low-dose CT chest (n = 82) | CXR (n = 89) | Low-dose CT chest (n = 26 551) | CXR (n = 26 505) | |
| T0a | ||||
| No or minor abnormalities | 41 (50.0) | 71 (79.8) | 16 368 (61.7) | 22 775 (85.9) |
| Significant abnormalities, not suspicious for lung cancer | 15 (18.3) | 2 (2.2) | 2677 (10.1) | 783 (3.0) |
| Positive screen suspicious for lung cancer | 24 (29.3) | 14 (15.7) | 7161 (27.) | 2372 (8.9) |
| Inadequate or other | 2 (2.4) | 2 (2.2) | 346 (1.3) | 575 (2.2) |
| T1b | ||||
| No or minor abnormalities | 46 (56.1) | 66 (74.2) | 16 238 (61.1) | 22 092 (83.4) |
| Significant abnormalities, not suspicious for lung cancer | 5 (6.1) | 1 (1.1) | 1509 (5.7) | 428 (1.6) |
| Positive screen suspicious for lung cancer | 20 (24.4) | 9 (10.1) | 6877 (25.9) | 1472 (5.6) |
| Inadequate or other | 11 (13.4) | 13 (14.6) | 1928 (7.3) | 2513 (9.5) |
| T2c | ||||
| No or minor abnormalities | 49 (59.7) | 66 (74.2) | 18 583 (70.0) | 21 727 (81.9) |
| Significant abnormalities, not suspicious for lung cancer | 5 (6.1) | 1 (1.1) | 1403 (5.3) | 359 (1.4) |
| Positive screen suspicious for lung cancer | 12 (14.6) | 5 (5.6) | 4027 (15.2) | 1168 (4.4) |
| Inadequate or other | 16 (19.5) | 17 (19.1) | 2539 (9.6) | 3251 (12.3) |
| Any time | ||||
| Positive screen suspicious for lung cancer | 35 (42.7) | 24 (27.0) | 10 115 (38.1) | 4008 (15.1) |
| Procedures related to screening | ||||
| Any procedure related to screening | 28 (34.1) | 20 (22.5) | 8785 (33.1) | 3660 (13.8) |
| Invasive procedure related to screening (biopsy, surgery) | 8 (9.8) | 2 (2.2) | 1096 (4.1) | 390 (1.5) |
Abbreviations: CT, computed tomography; CXR, chest radiography.
T0 indicates first screening examination performed soon after randomization.
T1 indicates second screening examination performed 1 y after first screening.
T2 indicates third screening examination performed 1 y after second screening.
Incidence of Lung Cancer Based on Prior Cancer History
We then compared the incidence of lung cancer in survivors of HNC and other forms of cancer vs participants with no prior cancer. After adjustment for age, sex, race, and pack-years of cigarette smoking, the incidence of lung cancer was highest in HNC survivors when compared against participants with history of a non-HNC or no prior cancer (2080 per 100 000 person-years [2.1%] vs 609 per 100 000 person-years [0.6%]; adjusted rate ratio, 2.54; 95% CI, 1.63-3.95) (Table 3).
Table 3. Incidence of Lung Cancer Based on Prior Cancer History.
| Prior cancer | No. of participants | Lung cancers identified | Incidence lung cancer per 100 000 person-years |
|---|---|---|---|
| HNC | 171 | 20 | 2080 |
| No HNC | 53 057 | 2038 | 609 |
| Cervical | 767 | 32 | 656 |
| Breast | 748 | 40 | 301 |
| Bladder | 240 | 18 | 1224 |
| Colorectal | 230 | 10 | 694 |
| Thyroid | 83 | 3 | 579 |
| Kidney | 68 | 4 | 996 |
| Transitional cell (kidney) | 32 | 3 | 1486 |
| Stomach | 27 | 1 | 610 |
| Esophageal | 20 | 1 | 845 |
| Pancreas | 7 | 0 | 0 |
Abbreviation: HNC, head and neck cancer.
Lung Cancer Screening With Low-Dose CT vs CXR
We next compared results in the subgroup of 171 HNC survivors who were randomized to either low-dose CT of the chest or CXR. In our primary analysis, the incidence of SPLC was 2610 cases per 100 000 person-years (12 cancers) in the low-dose CT group, compared with 1594 cases per 100 000 person-years in the CXR group (8 cancers, rate ratio, 1.55; 95% CI, 0.59-3.63). The incidence of either SPHNC or SPLC was 3659 cases per 100 000 person-years in the low-dose CT group, whereas there were no additional HNC diagnoses made after randomization in the CXR group, which had a total incidence of 1594 cases per 100 000 person-years (adjusted rate ratio, 1.95; 95% CI, 0.83-4.61). Notably, HNC survivors who were diagnosed with lung cancer after randomization were more likely to have squamous cell carcinoma histology (9 of 19 [47.4%] vs 447 of 2003 [22.3%]; difference, 25.1%; 95% CI, 4.9%-46.1%) (Table 4). In the low-dose CT group and CXR group, 7 of 11 (63.6%) and 4 of 8 (50.0%) participants were diagnosed with stage I SPLC, whereas 1 of 11 (9.1%) and 2 of 8 (25.0%), respectively, were diagnosed with stage IV. There was a 20% reduction in overall survival among HNC survivors who were randomized to CXR as compared with participants randomized to low-dose CT (hazard ratio, 0.79; 95% CI, 0.42-1.52) (Figure). In HNC survivors, overall survival was 7.07 years with low-dose CT vs 6.66 years with CXR (log-rank P = .48). The wide CI associated with the hazard ratio prevents making definitive conclusions regarding the effect of low-dose CT vs CXR.
Table 4. Second Primary Cancers Identified With Low-Dose CT Chest vs CXR.
| Type of cancer | No. (%) | |||||
|---|---|---|---|---|---|---|
| Survivors of head and neck cancer | All other patients | |||||
| All (n = 171) | Low-dose CT chest (n = 82) | CXR (n = 89) | All (n = 53 281) | Low-dose CT chest (n = 26 551) | CXR (n = 26 505) | |
| HNC diagnosed after randomization | 6 (3.5) | 6 (7.3) | 0 | 273 (0.5) | 150 (0.6) | 123 (0.5) |
| Lung cancer diagnosed after randomization | 20 (11.7) | 12 (14.6) | 8 (9.0) | 2038 (3.8) | 1077 (4.1) | 961 (3.6) |
| Other cancer diagnosed after randomization | 19 (11.1) | 10 (12.2) | 9 (10.1) | 4495 (8.5) | 2212 (8.3) | 2283 (8.6) |
| Stage and type of lung cancer | ||||||
| I | 11 (57.9) | 7 (63.6) | 4 (50.0) | 817 (40.3) | 521 (48.7) | 296 (30.9) |
| II | 2 (10.6) | 0 | 2 (25.0) | 144 (7.1) | 72 (6.8) | 72 (7.5) |
| III | 3 (15.8) | 3 (27.3) | 0 | 453 (22.4) | 216 (20.2) | 237 (24.7) |
| IV | 3 (15.8) | 1 (9.1) | 2 (25.0) | 589 (29.0) | 244 (22.8) | 345 (36.1) |
| Missing or other | 0 | 0 | 0 | 25 (1.1) | 18 (1.7) | 7 (0.7) |
| Histology of lung cancer | ||||||
| Squamous cell carcinoma | 9 (47.4) | 5 (45.5) | 4 (50.0) | 447 (22.3) | 239 (22.6) | 208 (22.0) |
| Bronchioalveolar carcinoma | 3 (15.8) | 2 (18.2) | 1 (12.5) | 153 (7.6) | 115 (10.9) | 38 (4.0) |
| Adenocarcinoma | 6 (31.6) | 4 (36.4) | 2 (25.0) | 652 (32.5) | 347 (32.8) | 305 (32.2) |
| Large cell carcinoma | 0 | 0 | 0 | 84 (4.2) | 40 (3.8) | 44 (4.6) |
| Non–small cell carcinoma or other | 0 | 0 | 0 | 355 (17.7) | 168 (15.9) | 187 (19.7) |
| Small cell carcinoma | 1 (5.3) | 0 | 1 (12.5) | 285 (14.2) | 134 (12.7) | 151 (15.9) |
| Carcinoid | 0 | 0 | 0 | 28 (1.4) | 14 (1.3) | 14 (1.5) |
Abbreviations: CT, computed tomography; CXR, chest radiography; HNC, head and neck cancer.
Figure. Kaplan-Meier Incidence and Survival Analysis in Survivors of Head and Neck Cancer.
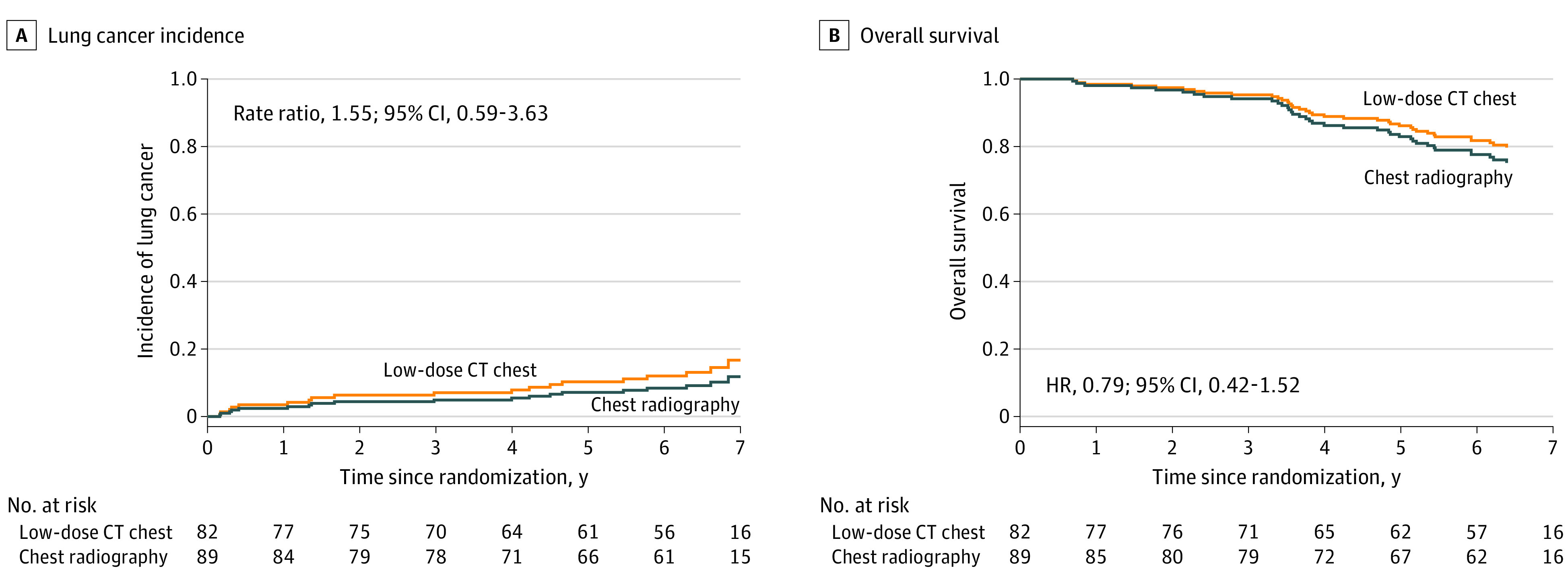
A, Incidence of lung cancer in survivors of head and neck cancer randomized to low-dose computed tomography (CT) chest vs chest radiography. B, Overall survival in survivors of head and neck cancer randomized to low-dose CT chest vs chest radiography. HR indicates hazard ratio.
Discussion
In this secondary analysis of the NLST examining HNC survivors, we identified 3 principal findings. First, we demonstrated that HNC survivors were more likely to have abnormal screening results. Second, in the setting of a randomized clinical trial, we confirmed that HNC is an especially high-risk feature for development of secondary lung cancer. Importantly, the risk of developing SPLC persists for many years after treatment for HNC. Third, in a cohort of 171 HNC survivors, we identified a potential benefit of lung cancer screening with low-dose CT of the chest vs CXR. Together, these results underscore the importance of low-dose CT screening in HNC survivors.
Results of Lung Screening Examinations
Pulmonary nodules are frequently detected on CT in HNC survivors. Previous retrospective single institutional studies have reported an 11% to 52% rate of pulmonary nodules in patients with HNC.6,12 However, these reports were single-arm analyses of HNC survivors, and it is difficult to compare the results to those of people with other forms of cancer. We found that HNC survivors in the NLST were more likely to have significant abnormalities identified with screening, and 42.7% had at least 1 low-dose CT screening test suspicious for lung cancer. Furthermore, 9.8% of HNC survivors who were screened with low-dose CT of the chest underwent an invasive procedure related to screening. This finding suggests that individuals with a history of HNC may be more likely to experience the risks associated with screening, including subsequent invasive procedures.
Head and Neck Cancer as a High-risk Feature for Lung Cancer Screening
Previous retrospective research has demonstrated that HNC survivors have a widely varying risk of developing SPLC, ranging from 0.6% to 8.0%.13,14 An analysis of a Taiwanese national cancer database found that 5.7% of 63 720 HNC survivors developed a second primary cancer, although in that series, only 0.6% of patients developed SPLC.14 In contrast, an analysis of the Surveillance Epidemiology and End Results database found that 8.0% of HNC survivors developed SPLC an average of 6.7 years after treatment, most frequently after supraglottic or hypopharyngeal cancer.13 Another study15 found that the risk of SPLC was higher after HNC than after other cancers. That study compared HNC survivors in the Surveillance Epidemiology and End Results database with the control group of the NLST and estimated that cancers of the larynx, oropharynx, hypopharynx, and tonsils were among the highest demonstrated cumulative incidence of SPLC.15 However, the wide range in incidence of SPLC leaves some doubt as to the true incidence. In this prospective cohort enrolled in a randomized trial a median of 9 years after HNC, we confirm that HNC survivors are at high risk for developing SPLC. We found that 2.1% of participants with prior HNC will develop lung cancer per year of follow-up (2080 per 100 000-person-years), well above the incidence seen for survivors of other forms of cancer.
Increased Detection of SPLC, Overall Survival, and Costs of Low-Dose CT
We observed that HNC survivors had a nonsignificant trend for increased detection of SPLC and improved overall survival with low-dose CT of the chest. The wide CIs, presumably due to the small sample size and number of outcome events, prevent definitive conclusions. A larger sample of HNC survivors and outcome events will provide a more precise estimate of the true effect of low-dose CT lung screening when compared with CXR. Importantly, results from the well-powered full sample of 53 452 participants showed a significant 6.7% improvement in overall survival and 20% improvement in lung cancer mortality with low-dose CT chest screening.9 The incidence of lung cancer in HNC survivors was 2.5 times higher than that in the overall trial, suggesting that low-dose CT screening was more effective at diagnosing SPLC than CXR; this effect may be even greater in HNC survivors.
The differences in incidence of SPHNC (6 cases of SPHNC in the low-dose CT group vs 0 cases in the CXR group) further hint that low-dose CT screening may also lead to detection of SPHNC. The mechanisms are likely multifactorial and not fully discernible from the present data. We hypothesize that low-dose CT chest screening may detect some findings in the lower cervical lymph nodes, larynx, and hypopharynx that may lead to a diagnosis of SPHNC. Furthermore, many patients who undergo low-dose CT chest screening require positron emission tomography (PET)/CT to investigate suspicious lesions; these images include the entire head and neck, which may lead to the diagnosis of SPHNC. Thus, we hypothesize that in addition to screening for SPLC, low-dose CT chest screening may contribute to the diagnosis of SPHNC.
Implications
The frequency of surveillance imaging of the neck after HNC is controversial, with differing opinions and guideline recommendations. The National Comprehensive Cancer Network and the American Society of Clinical Oncology HNC Survivorship Care Guidelines do not recommend routine surveillance imaging for HNC beyond 6 months after treatment unless there are concerning signs or symptoms.1,2 In contrast, the American College of Radiology Neck Imaging Reporting and Data Systems white paper recommends that HNC patients undergo a PET/CT screening 3 months after treatment, followed by a contrast-enhanced CT of the neck and chest or PET/CT 6 months later. If contrast-enhanced CT is negative, the American College of Radiology white paper recommends another contrast-enhanced CT scan of the neck and chest 12 months later.3 Our study does not examine surveillance neck imaging but does provide some perspective on the risks and benefits of chest imaging after HNC.
Survivors of HNC are at high risk of second primary cancers such as lung cancer. The National Comprehensive Cancer Network guidelines recommend annual low-dose CT chest screening for individuals aged 50 years or older with at least a 20 pack-year smoking history and importantly include prior HNC as a high-risk feature.16 Similarly, recently updated USPSTF guidelines recommend annual low-dose CT chest screening for those aged 50 to 80 years with at least a 20 pack-year smoking history who currently smoke or have quit within the past 15 years.7 These guidelines have decreased the number of pack-years necessary to warrant screening from the 30 pack-years or more used in the NLST to 20 pack-years or more based on modeling data showing likely benefit in this group.17 Significantly, USPSTF guidelines do not mention prior HNC as a risk factor for lung cancer. However, USPSTF guidelines do state that screening should stop if a patient has not smoked in 15 years or if they develop a health problem that substantially limits life expectancy or the ability to undergo curative lung treatment. Based on the data presented here and in the other reports of the NLST,9,18 we would advocate that HNC survivors aged 50 years or older with a 20 pack-year or more smoking history who are fit enough to undergo curative lung cancer treatment should undergo annual low-dose CT screening for lung cancer.
Although this conclusion is not practice-changing, it does emphasize the importance of adhering to lung cancer screening recommendations in HNC survivors. Adherence to USPSTF lung cancer screening guidelines is estimated to be only 14% nationally.8 Lung cancer screening rates are even lower in current smokers, non-White individuals, and those with less education.8,19 Our results show that HNC survivors are at especially high risk for SPLC and may warrant special consideration to boost adherence. Given the especially high rates of SPLC in HNC survivors, we believe that all lung cancer screening guidelines, including those by the USPSTF, should include prior HNC as a high-risk feature for the development of lung cancer. We would recommend incorporating lung cancer screening into standard HNC survivorship and recommend integration of quality metrics to optimize adherence in this population. However, implementing routine lung cancer screening into HNC survivorship will require a concerted approach, as clinicians who treat patients with HNC have raised concerns about incorporating lung cancer screening into cancer clinics related to workflow, shared decision-making, and competing priorities.20
Limitations
There are several limitations to consider when interpreting our results. First, the NLST was not specifically designed to address our study question, and the data collected were not optimized for our study question. Prior HNC was self-reported, and no data on the stage or treatment for HNC were collected. In addition, we were unable to identify or differentiate human papillomavirus–related cancers, which are associated with different smoking rates. Second, the group of HNC survivors was small, and our results may reflect imprecision in effect size estimates, which prevents definitive conclusions. Third, participants with previous cancers diagnosed within 5 years were excluded from the NLST. If prior HNC within 5 years was not an exclusion criterion, the incidence of both SPHNC and SPLC would have been even higher.21 However, owing to the mortality risk in HNC survivors within 5 years of treatment, the benefits of SPLC diagnosis may be decreased owing to competing risks of mortality.22 Fourth, the results presented were limited to the results of screening, the incidence of SPLC and SPHNC, and overall survival. Additional oncologic and quality-of-life outcomes may help to better define the risks and benefits of low-dose CT screening. Fifth, differentiating pulmonary head and neck squamous cell carcinoma metastases from squamous cell SPLC relies on clinical impression, radiologic imaging, and histology. However, in cases with squamous cell histology, it is not always possible to determine definitively whether this finding represents a second primary or pulmonary metastases; this uncertainty may explain some of the differences in observed rates. Nonetheless, we believe that this secondary analysis of a randomized clinical trial provides important insight into the risk of SPLC among HNC survivors.
Conclusions
In this secondary analysis of a randomized clinical trial, we evaluated HNC survivors enrolled in the NLST and found a 2.5 times greater rate of lung cancer compared with patients with no previous cancer. Adherence to lung cancer screening recommendations in the real world is low, and our results underscore the importance of lung cancer screening in HNC survivors. In total, these results support routine annual low-dose CT chest screening for lung cancer in HNC survivors with prior significant tobacco use who are fit enough to undergo treatment with curative intent.
Trial Protocol
eFigure. Flow Diagram of Cohort Selection
Data Sharing Statement
References
- 1.National Comprehensive Cancer Network . NCCN guidelines. Accessed June 9, 2021. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1437
- 2.Nekhlyudov L, Lacchetti C, Davis NB, et al. Head and neck cancer survivorship care guideline: American Society of Clinical Oncology Clinical Practice Guideline Endorsement of the American Cancer Society Guideline. J Clin Oncol. 2017;35(14):1606-1621. doi: 10.1200/JCO.2016.71.8478 [DOI] [PubMed] [Google Scholar]
- 3.Aiken AH, Rath TJ, Anzai Y, et al. ACR Neck Imaging Reporting and Data Systems (NI-RADS): a white paper of the ACR NI-RADS committee. J Am Coll Radiol. 2018;15(8):1097-1108. doi: 10.1016/j.jacr.2018.05.006 [DOI] [PubMed] [Google Scholar]
- 4.Argiris A, Karamouzis MV, Raben D, Ferris RL. Head and neck cancer. Lancet. 2008;371(9625):1695-1709. doi: 10.1016/S0140-6736(08)60728-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jethwa AR, Khariwala SS. Tobacco-related carcinogenesis in head and neck cancer. Cancer Metastasis Rev. 2017;36(3):411-423. doi: 10.1007/s10555-017-9689-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Piersiala K, Akst LM, Hillel AT, Best SR. CT lung screening in patients with laryngeal cancer. Sci Rep. 2020;10(1):4676. doi: 10.1038/s41598-020-61511-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Krist AH, Davidson KW, Mangione CM, et al. ; US Preventive Services Task Force . Screening for lung cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(10):962-970. doi: 10.1001/jama.2021.1117 [DOI] [PubMed] [Google Scholar]
- 8.Zahnd WE, Eberth JM. Lung cancer screening utilization: a behavioral risk factor surveillance system analysis. Am J Prev Med. 2019;57(2):250-255. doi: 10.1016/j.amepre.2019.03.015 [DOI] [PubMed] [Google Scholar]
- 9.Aberle DR, Adams AM, Berg CD, et al. ; National Lung Screening Trial Research Team . Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365(5):395-409. doi: 10.1056/NEJMoa1102873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.National Lung Screening Trial (NLST) Screening . (NLST). Clinicaltrials.gov identifier: NCT00047385. Updated May 20, 2014. Accessed July 1, 2021. https://clinicaltrials.gov/ct2/show/NCT00047385
- 11.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi: 10.3322/caac.21492 [DOI] [PubMed] [Google Scholar]
- 12.Green R, King M, Reid H, Murchison JT, Evans A, Nixon IJ. Management of pulmonary nodules in head and neck cancer patients—our experience and interpretation of the British Thoracic Society Guidelines. Surgeon. 2017;15(4):227-230. doi: 10.1016/j.surge.2016.10.002 [DOI] [PubMed] [Google Scholar]
- 13.Crippen MM, Brady JS, Burke LA, Eloy JA, Baredes S, Park RCW. Second primary lung malignancy following head and neck squamous cell carcinoma. Laryngoscope. 2019;129(4):903-909. doi: 10.1002/lary.27422 [DOI] [PubMed] [Google Scholar]
- 14.Chen MC, Huang WC, Chan CH, Chen PT, Lee KD. Impact of second primary esophageal or lung cancer on survival of patients with head and neck cancer. Oral Oncol. 2010;46(4):249-254. doi: 10.1016/j.oraloncology.2010.01.002 [DOI] [PubMed] [Google Scholar]
- 15.Donin NM, Kwan L, Lenis AT, Drakaki A, Chamie K. Second primary lung cancer in United States Cancer Survivors, 1992-2008. Cancer Causes Control. 2019;30(5):465-475. doi: 10.1007/s10552-019-01161-7 [DOI] [PubMed] [Google Scholar]
- 16.National Comprehensive Cancer Network . Lung cancer screening. Accessed June 9, 2021. https://www.nccn.org/patients/guidelines/content/PDF/lung_screening-patient.pdf
- 17.Meza R, Jeon J, Toumazis I, et al. Evaluation of the benefits and harms of lung cancer screening with low-dose computed tomography: modeling study for the US Preventive Services Task Force. JAMA. 2021;325(10):988-997. doi: 10.1001/jama.2021.1077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Black WC, Gareen IF, Soneji SS, et al. ; National Lung Screening Trial Research Team . Cost-effectiveness of CT screening in the National Lung Screening Trial. N Engl J Med. 2014;371(19):1793-1802. doi: 10.1056/NEJMoa1312547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lopez-Olivo MA, Maki KG, Choi NJ, et al. Patient adherence to screening for lung cancer in the US: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(11):e2025102. doi: 10.1001/jamanetworkopen.2020.25102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dukes K, Seaman AT, Hoffman RM, et al. Attitudes of clinicians about screening head and neck cancer survivors for lung cancer using low-dose computed tomography. Ann Otol Rhinol Laryngol. 2020;129(1):23-31. doi: 10.1177/0003489419868245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hall SF, Groome PA, Rothwell D. Time to first relapse as an outcome and a predictor of survival in patients with squamous cell carcinoma of the head and neck. Laryngoscope. 2000;110(12):2041-2046. doi: 10.1097/00005537-200012000-00012 [DOI] [PubMed] [Google Scholar]
- 22.Pagedar NA, Jayawardena A, Charlton ME, Hoffman HT. Second primary lung cancer after head and neck cancer: implications for screening computed tomography. Ann Otol Rhinol Laryngol. 2015;124(10):765-769. doi: 10.1177/0003489415582259 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eFigure. Flow Diagram of Cohort Selection
Data Sharing Statement