

Abstract
Background:
US Latino men who have sex with men (LMSM) are a group at highest risk for HIV. One driver of HIV among LMSM is inadequate access to pre-exposure prophylaxis (PrEP) information. The social network theory of homophily suggests that sharing similar sociodemographic factors could influence PrEP conversations within networks. This study aimed to determine how the effects of homophily across sociodemographic, immigration, cultural, and PrEP-related factors, is associated with PrEP-related communication.
Setting:
This study was conducted in Miami-Dade County, FL.
Methods:
Data collected between August 2018 and October 2019 included ten sociocentric friendship groups of 13 LMSM (N=130). Participants were recruited using respondent-driven sampling by a community-based organization in Miami. We used the Multiple Regression Quadratic Assignment Procedure (MRQAP) to identify the effects of homophily and relationship characteristics, on PrEP-related conversations using R software.
Results:
More frequent PrEP-related conversations were associated with dyadic friendships characterized by homophily on knowledge of PrEP effectiveness, heterophily on depressive symptom severity, home addresses proximity, friend closeness, and interaction frequency. Past PrEP-related conversation frequency also increased based on heterophily on the Latino cultural value of familism (i.e. emotional support to family). Racial homophily, heterophily on severity of depressive symptoms, home addresses proximity, friendship closeness, and frequency of interactions increased likelihood to encourage a friend to use PrEP.
Discussion:
Social and spatial closeness, and homophily play a role in PrEP-related conversations. Information from social networks contextualized in geographic settings can be elucidated to contribute towards the design of novel opportunities to end HIV.
Keywords: Men who have sex with men, PrEP, Hispanic Americans, Risk Reduction Behavior, Respondent Driven Sampling, Social network analysis
INTRODUCTION
In the US, there were approximately 38,000 new HIV infections in 2018. Of these, Latino men who have sex with men (LMSM) were identified as a group at highest risk for HIV, representing 21% of new HIV diagnoses.1 In 2019, Miami Dade County (MDC) reported the highest US rate of new infections: an incidence four times the national average (42.7 vs. 11.5 per 100,000 residents).1,2 From 2014–2018 in MDC, Latinos experienced an increase of 9.7% new HIV diagnosis, and LMSM experienced an increase of 7.9% new infections: this highlights a continuing HIV-related health disparity that urgently needs to be addressed.2
One potential contributor to LMSM HIV disparities is their access to information about pre-exposure prophylaxis (PrEP)—the best preventive measure against primary HIV infection.3–7 Latino gay and bisexual men consistently continue to report disparities in PrEP information and access relative to White gay and bisexual men (87% versus 95% for access to PrEP information, and 30% versus 42% for access to PrEP, respectively).8 As health-related information has the potential to spread within social groups in a manner that can result in the uptake of health-related behaviors, the source of where individuals first hear about PrEP can determine PrEP self-referrals and uptake.9,10 Hearing about PrEP through a friend network or sexual partner network is highly associated with becoming a self-referral for PrEP.9,10 To the best of our understanding, there is a gap in previous research in characterizing relationship factors that are associated with PrEP-related conversations among LMSM.
The spread of information within networks can be partially explained by the social network theory of homophily. Homophily, the interaction of individuals with other “individuals similar to themselves in respect to a variety of qualities and characteristics,” occurs in the context of sociodemographic and contextual factors, such as location and group membership.11,12 As such, dyads who are similar on some characteristic such as race or country of birth may be more likely to share information relative to dyads who are dissimilar. Associations of homophily and PrEP-related conversations have been noted in other sexual and racial minority groups.13 Due to the Latino community’s heterogeneity in MDC, it is important to understand how sociodemographic and contextual similarities and differences between individuals can influence the spread of health-related messaging between dyads within social networks. This is a current gap in the literature.
For Latinos in the US, the incorporation of cultural values can influence the success of health promotion programs.14 These cultural values can include respeto (construct which values showing respect to elder and/or authority figures),15 religiosidad/ espiritualidad (construct which values religion), and familismo (construct consisting of emotional support, family as referent, and familial obligation, which values individuals accepting responsibility of their families and closer group of friends).16,17 Accordingly, Latinos may be more likely to promote conversations about PrEP with members of their friendship networks based on homophily on endorsement of these cultural values. However, limited information exists on the detailed characteristics of the dissemination of PrEP information within social networks. Disclosing one’s PrEP use with sexual partners has been shown to be positively associated with condom use, suggesting that PrEP conversations among LMSM may have an additive impact on HIV prevention.18
Migration has previously been identified to drive the HIV epidemic.19 Latino immigrants tend to settle in communities where they have social ties with high levels of homophily—such as LMSM in MDC.20 Higher levels of geographic segregation related to homophily could sustain elevated HIV incidence within specific populations.21 For this, it is important to understand how geospatial factors in social networks can influence PrEP information dissermination within networks. In MDC, foreign-born Latinos experience a higher HIV incidence relative to US-born Latinos and account for 85% of new HIV diagnoses among Latinos.22 As most HIV infections among foreign-born Latinos occur after immigrating to the US,23 it is important to understand how immigration-related factors, such as acculturation stress, negatively influence health behaviors. In addition to acculturation-related stressors, psychiatric comorbidities have been shown to drive the HIV epidemic.20 Latinos experiencing immigration stress may create relationships with other individuals experiencing this stress.24 Thus, homophily on immigration-related factors (e.g., country of nativity and acculturation stress) may positively influence health-related conversations, like conversations about PrEP.
Previous PrEP research has largely focused on implementing traditional random sampling. To address this lack of network studies, this study uses a sociocentric network approach to explore how factors associated with PrEP communication within networks. More specifically, this study aims to address the gap of how homophily is associated with PrEP knowledge and communication within LMSM friendship networks. More specifically, we hypothesized that homophily on race, being US born, Latino cultural values (i.e. familism support, familism obligations, familism referent, respect, and religiosity), acculturation stress (i.e. immigration stress and discrimination stress), and PrEP knowledge factors is positively associated with previous PrEP-related conversations, future PrEP-related conversations, and encouraging someone to use PrEP.
METHODS
Participants and inclusion criteria
This study analyzes 130 LMSM participants. LMSM were a part of one of ten sociocentric networks. Each of the 130 LMSM participants could identify up to 12 LMSM within their sociocentric friendship social network, for a total of 13 LMSM members in each network. Inclusion criteria included the following: 1) identifying as Hispanic/Latino/Latinx, 2) identifying as a cis gender man, 2) having sex with another man in the past six months, 3) being between ages 20–39 years (a group at highest behavioral vulnerability to HIV),1 and 4) qualifying for PrEP in accordance with the Centers for Disease Control and Prevention clinical practice guideline.25 Data were collected from August 2018 to October 2019.
Recruitment and Enrolment
Participants were recruited using respondent-driven sampling. A local LMSM-centric community-based HIV service organization recruited participants from two sites in MDC. To address potential network overlaps, seeds were randomly drawn from the [BLINDED ORGANIZATION] clientele by randomly selecting day/time intervals when potential seeds could be found at one of two [BLINDED ORGANIZATION] MDC sites. To configure each sociocentric network, the Project Coordinator first recruited 10 seeds. Of these 10 seeds, five reported using PrEP, and five reported not using PrEP. Using respondent-driven sampling, each of the 10 seeds each invited three friends (referred to as first-order friends). These first-order friends then each invited three friends (second-order friends). If any friends declined participation, the seed/friend was asked to invite a substitute friend. If a participant was able to recruit only one or two friends, seeds and/or other first-order friends were asked to recruit a fourth friend, who recruited additional friends using the respondent-driven sampling approach until 13 LMSM were enrolled into one sociocentric network. Respondent-driven sampling can reach previously unreached communities than traditional outreach methods.26 We chose to enroll networks of 13 members as it may increase social capital with groups while increasing HIV prevention knowledge.27 Participants could only be a part of one social network, and those participants who overlapped in networks were assigned to the network they were first recruited into.
Once networks were established, the Project Coordinator scheduled assessments. Study staff provided written and verbal informed consent to participants then delivered a two-hour long assessment to participants in either English or Spanish. Assessments were conducted by trained, bilingual LMSM interviewers using tablet computers. Each participant received a $50 gift card as compensation for their time during interviews and a $10 gift card for each friend that enrolled in the study.
Dependent Measures
Sociodemographic variables include race (Black, White, Multiracial, Other), home address, and country of origin (collected as country of birth then recoded as US-born or foreign-born).
PrEP Knowledge was assessed by asking, “How effective is PrEP when taken as prescribed in preventing HIV?” with the options, “I don’t know,” “Less than 50% effective,” “Less than 75% effective,” “Less than 90% effective,” and “90% or more than 90% effective.” Responses were scored for the correct answer as a binary variable (1=“90% of more than 90% effective,” 0=all other responses).
PrEP use was assessed by participants self-reporting their current PrEP use (0=not currently using PrEP, 1=currently using PrEP).
Endorsement of Latino Cultural Values constructs were measured using the Mexican American Cultural Values Scale.17 This is a 35-item 5-point Likert scale that measures adherence to nine types of Latino Cultural Values (α = 0.88).17 This study examined the effects of five of the subscales: Familism Support (6 items), Familism Obligations (5 items), Familism Referents (5 items), Religiosity (7 items), and Respect (8 items). We found the mean score for each of these subscales (range: 1–5). Higher mean scores indicated high endorsement of each of these cultural values. Cronbach’s alpha for each subscale was as follows; Familism Support α=0.9; Familism Obligations α=0.8; Familism Referents α=0.79; Religiosity α=0.86, and Respect α=0.66.
Immigration and discrimination stress was assessed using the Hispanic Stress Inventory Version 2.28 The Hispanic Stress Inventory has high reliability for measuring immigration and discrimination stress experienced by foreign-born and US-born Latinos through the Immigration Stress and Discrimination Stress subscales (respectively, 9 items, α=0.88; 11 items, α=0.88). To capture immigration and discrimination stress, respondents were prompted, “Please indicate how worried or tense you feel in response to the following statements” then provided with 9 statements to measure immigration stress and 11 statements to measure discrimination stress. We found the mean score for each of these two scales (range: 1–5). A mean score of 5 indicated higher immigration stress, while a mean item score of 1 indicates lower immigration stress. An example of an item included, “I have thought that if I went to a social or government agency, I would be deported.”
Depressive symptoms were assessed using the 9-item Patient Health Questionnaire (PHQ-9).29 Participants indicated on a scale of 0–3, how often they were bothered by a list of 9 problems over the last two weeks.30 We added the scores for each item together (range: 0–27) to calculate participants’ raw PHQ score. Examples of problems include, “Feeling down, depressed, or hopeless.”
Distance between participants’s homes were assessed by using ArcGIS Pro (Esri, Redlands, CA). First, we geocoded participants’ home addresses.31 The Euclidian distances between participants’ home addresses were calculated using the “Generate Near Table” tool for dyads with friendship ties. R was then used to configure the distance table (in meters) into an adjacency matrix of distances between egos, per social network.32 To protect participants’confidentiality, network visualizations were rotated and layers protraiting specific locateions were removed.
Social network measures
Friendship ties were assessed by asking participants if they knew each of member of their sociocentric friendship group (i.e. “Do you know this person? By “know” I mean that you know his name, he knows your name, the two have spoken before, and you know how to contact him if necessary (for example, by telephone, visiting his house, or by internet” as a binary outcome). Frequency of meeting was assessed by asking, “In the last six months, how frequently did you meet with this person, in person, for example, went out to do a job or went out together?” with options 1=“Never,” 2=“Once a month,” 3=“Once a week,” and 4=“Almost every day.” Emotional closeness/attachment was assessed by a 5-item Likert scale “On a scale of 1 to 5, how close do you feel to this person?” (1=“Not at all close” to 5=“Extremely close”).
Dependent PrEP conversation measures
PrEP conversation frequency was assessed by asking “In the past, how frequently did you have a conversation about PrEP with this person?” with options 1=“Never,” 2=“Sometimes,” and 3=“Frequently.” Likelihood to talk about PrEP was assessed by asking, “In the next six months, how likely is it that you will talk about PrEP with this person?” with options, 1=“Not likely,” 2=“Not very likely,” 3=“A little likely,” and 4=“Very likely.” Likelihood to encourage PrEP use was assessed by the following question, “In the next six months, how likely is it that you will encourage this person to begin using PrEP?” with options, 1=“Not likely,” 2=“Not very likely,” 3=“A little likely,” and 4=“Very likely.”
Analysis
Homophily was calculated separately for each dependent measure by finding the absolute difference in scores among all dyad combinations of the 130 participants. For the measure of homophily, ordinal items have ordinal homophily scores and categorial items have binary homophily scores. This process creates a measure of similarity for each variable. For ordinal measures (e.g., acculturation-related stress), a score of 0 indicated homophily, while a larger score indicated increasing heterophily, or decreasing homophily. For categorical measures (e.g., for country of nativity) participants who both provided the same answer were assigned the value 1 for homophily and 0 for heterophily.
To identify if dyadic homophily of dependent measures were associated with 1) PrEP conversations, 2) likelihood to talk about PrEP in the future, and 3) encouragement to use PrEP, we used the Multiple Regression Quadratic Assignment Procedure (MRQAP) using R software.32,33 The QAP is a resampling-based method which corrects for the expected dependencies among egos within the same network to provide the correct standard errors.34 As such, MRQAP does not rely on assumptions of independence and are commonly used for sociocentric network analyses.35–37 MRQAP allows for the individual analysis of each network, and then conducts an aggregate analysis. The MRQAP network meta-analysis used the R igraph package and an adapted version of the functions rmperm and netlm.32,38 The rmperm function ensured that when separate networks were combined for the permutation tests, only indices that refer to a specific network were permuted by the function. The second function changed the MRQAP estimation by correcting permutation scores to allow input matrices to incorporate a combination of individual networks. The present study permuted each analysis 1,000 times. Networks were visualized using Cytoscape software.39
Sociocentric friendship networks were stratified by the seed’s PrEP use status for visualization purposes, then each network’s home address directional distribution (i.e., standard deviation ellipse) was calculated using ArcGIS Pro software.31 This descriptive spatial analysis summarizes the central tendency, dispersion, and orientation of the participants’ home addresses within each network by creating a standard deviational ellipse polygon covering 63% (1 standard deviation) of participant home addresses.40
Ethical approval
This study was approved by the [BLINDED INSTITUTION]. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
RESULTS
A total of 130 LMSM were grouped into ten sociocentric social networks. Data were incomplete for 3 participants, and our sample total was 127 participants. There were 400 unique dyads and 800 ties sent within the entire sample. Participants’ mean age was 28 years (±4 years), and were majority white (72%), single/never married (87%), and lived in Miami-Dade County (87%). Approximately half of the participants were either US or Latin American born, spoke English or Spanish, and were college educated. Table 1 includes additional information surrounding participants.
Table 1:
Participant sociodemographic information, stratified by PrEP use (n=127)
| PrEP non-user (n=89) | PrEP user (n=38) | Total sample (n=127) | ||||
| Categorial | N | % | N | % | N | % |
|
| ||||||
| Race | ||||||
| Black | 3 | 3.37 | 2 | 5.26 | 5 | 3.94 |
| White | 68 | 76.40 | 23 | 60.53 | 91 | 71.65 |
| Multiracial | 14 | 15.73 | 10 | 26.32 | 24 | 18.90 |
| Other | 4 | 4.49 | 3 | 7.89 | 7 | 5.51 |
| Region of Nativity | ||||||
| US | 50 | 56.18 | 21 | 55.26 | 71 | 55.91 |
| Latin America | 39 | 43.82 | 17 | 44.74 | 56 | 44.09 |
| Education | ||||||
| High School or less | 14 | 15.73 | 4 | 10.53 | 18 | 14.17 |
| Some College | 44 | 49.44 | 21 | 55.26 | 65 | 51.18 |
| College or More | 31 | 34.83 | 13 | 34.21 | 44 | 34.65 |
| Relationship/Marital Status | ||||||
| Single/Never Married | 81 | 91.01 | 29 | 76.32 | 110 | 86.61 |
| Married/Domestic partner | 8 | 8.99 | 9 | 23.68 | 17 | 13.39 |
| County of residency | ||||||
| Miami-Dade County | 79 | 88.76 | 31 | 81.58 | 110 | 86.61 |
| Broward County | 8 | 8.99 | 7 | 18.42 | 15 | 11.81 |
| Other county | 2 | 2.25 | 0 | 0.00 | 2 | 1.57 |
| Native Language | ||||||
| English | 48 | 53.93 | 21 | 55.26 | 69 | 54.33 |
| Spanish | 41 | 46.07 | 17 | 44.74 | 58 | 45.67 |
| PrEP Knowledge Score * | ||||||
| Correct | 58 | 68.24 | 31 | 93.94 | 89 | 75.42 |
| Incorrect | 27 | 31.76 | 2 | 6.06 | 29 | 24.58 |
|
| ||||||
| PrEP non-user | PrEP user | Total sample | ||||
| Continuous | Mean | SD | Mean | SD | Mean | SD |
|
| ||||||
| Age | 28.5 | 4.41 | 27.7 | 3.77 | 28.22 | 4.22 |
| Discrimination Stress score | 2.02 | 1.15 | 2.08 | 1.21 | 2.04 | 1.16 |
| Immigration Stress score | 1.72 | 1.23 | 1.65 | 1.22 | 1.7 | 1.22 |
| Family emotional support score † | 3.32 | 1.23 | 3.811 | 0.97 | 3.48 | 1.17 |
| Family Obligation score † | 3.26 | 1.19 | 3.81 | 0.89 | 3.43 | 1.13 |
| Family as referents score † | 3.02 | 1.14 | 3.46 | 0.93 | 3.15 | 1.1 |
| Religiosity score | 2.28 | 1.29 | 2.45 | 1.43 | 2.33 | 1.33 |
| Respect score | 3.24 | 1.17 | 3.61 | 0.93 | 3.35 | 1.11 |
| Raw PHQ Score | 3.74 | 5.10 | 4.00 | 4.78 | 3.82 | 4.99 |
indicates significant relationship association of p<0.05 using chi-square analyses between PrEP users and nonusers
indicates significant relationship association of p<0.05 using t-tests between PrEP users and nonusers
Table 2 displays the results of the MRQAP analysis. The estimates presented in the table are standardized regression coefficients. In models 1a, 2a, and 3a, we excluded the social network factors of frequency of seeing each other and perceived closeness. These initial models explained much less of the variance in PrEP conversation outcomes (Multiple R2 = 6%, 7%, and 6%, respectively for PrEP conversation frequency, likelihood to talk about PrEP in the next six months, and likelihood to encourage PrEP use in the next six months). In models 1b, 2b, and 3b, we introduced the social network variables of frequency of seeing each other and perceived closeness, and these models explained much more of the variance in PrEP conversation frequency, likelihood to talk about PrEP in the next six months, and likelihood to encourage PrEP use in the next six months (Multiple R2 = 75%, 65%, and 60%, respectively).
Table 2:
MRQAP of PrEP conversations based on LMSM homophily
| PrEP conversation frequency | Likelihood to talk about PrEP in the next six months | Likelihood to encourage PrEP use in the next six months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Model 1a ** | Model 1b † | Model 2a ** | Model 2b † | Model 3a ** | Model 3b † | |||||||
|
| ||||||||||||
| Dependent measure | Estimate | Pr(>=|b|) | Estimate | Pr(>=|b|) | Estimate | Pr(>=|b|) | Estimate | Pr(>=|b|) | Estimate | Pr(>=|b|) | Estimate | Pr(>=|b|) |
| Intercept | 0.674 | 0.000 | 0.052 | 0.289 | 1.045 | 0.000 | 0.274 | 0.002 | 1.026 | 0.000 | 0.260 | 0.005 |
| Race | 0.086 | 0.137 | 0.002 | 0.953 | 0.055 | 0.451 | −0.045 | 0.367 | −0.005 | 0.930 | −0.106 | 0.044 |
| Both born in US or Latin America | −0.083 | 0.110 | −0.037 | 0.213 | −0.067 | 0.326 | −0.010 | 0.833 | −0.090 | 0.200 | −0.033 | 0.493 |
| Both have PrEP knowledge | 0.233 | 0.000 | 0.090 | 0.004 | 0.291 | 0.000 | 0.122 | 0.008 | 0.241 | 0.010 | 0.072 | 0.162 |
| Difference in discrimination Stress | −0.069 | 0.092 | 0.013 | 0.536 | −0.115 | 0.027 | −0.012 | 0.743 | −0.093 | 0.080 | 0.009 | 0.780 |
| Difference in immigration Stress | 0.033 | 0.352 | −0.007 | 0.728 | 0.040 | 0.372 | −0.011 | 0.749 | 0.048 | 0.292 | −0.003 | 0.925 |
| Difference in Family emotional support | 0.292 | 0.000 | 0.090 | 0.010 | 0.369 | 0.001 | 0.114 | 0.062 | 0.360 | 0.000 | 0.107 | 0.102 |
| Difference in Family Obligation | −0.076 | 0.199 | −0.053 | 0.089 | −0.089 | 0.251 | −0.062 | 0.241 | −0.109 | 0.146 | −0.081 | 0.133 |
| Difference in Family as referents | −0.252 | 0.002 | −0.008 | 0.824 | −0.315 | 0.005 | −0.011 | 0.843 | −0.248 | 0.024 | 0.053 | 0.380 |
| Difference in Religiosity | 0.002 | 0.942 | −0.008 | 0.504 | −0.021 | 0.545 | −0.031 | 0.111 | −0.019 | 0.574 | −0.029 | 0.148 |
| Difference in Respect | 0.004 | 0.971 | −0.034 | 0.477 | −0.042 | 0.775 | −0.087 | 0.175 | −0.073 | 0.592 | −0.118 | 0.085 |
| Difference in PHQ Score | 0.140 | 0.014 | 0.123 | 0.000 | 0.309 | 0.000 | 0.289 | 0.000 | 0.344 | 0.000 | 0.324 | 0.000 |
| 1 Mile distance btwn homes | 0.000 | 0.028 | 0.000 | 0.002 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.003 | 0.000 | 0.000 |
| Both use PrEP | −0.021 | 0.830 | −0.010 | 0.836 | −0.095 | 0.477 | −0.087 | 0.288 | −0.008 | 0.958 | 0.002 | 0.979 |
| Both do not use PrEP | 0.134 | 0.048 | −0.005 | 0.878 | 0.031 | 0.724 | −0.140 | 0.005 | 0.086 | 0.392 | −0.084 | 0.145 |
| Frequency of seeing each other | 0.206 | 0.000 | 0.207 | 0.000 | 0.215 | 0.000 | ||||||
| Closeness/Attachment | 0.255 | 0.000 | 0.350 | 0.000 | 0.341 | 0.000 | ||||||
|
| ||||||||||||
| Multiple R squared | 0.060 | 0.754 | 0.074 | 0.651 | 0.061 | 0.596 | ||||||
| Adjusted R squared | 0.048 | 0.751 | 0.062 | 0.646 | 0.050 | 0.590 | ||||||
Does not include the social network factors of frequency of seeing each other and perceived closeness
Includes social network factors of frequency of seeing each other and perceived closeness
For frequency of PrEP conversation, our final model found that homophily on PrEP knowledge (β=0.090; p<0.01), a higher difference in family emotional support (β=0.090; p<0.01), a higher difference in PHQ score (β=0.123; p<0.001), living further away from each other (β=0.000; p<0.01), seeing each other more frequently (β=0.206; p<0.001), and higher perceived closeness (β=0.255; p<0.001) were associated with higher frequency of conversations.
For likelihood to talk about PrEP in the next six months, our final model found that homophily on PrEP knowledge (β=0.122; p<0.01), a higher difference in PHQ score (β=0.289; p<0.001), living further away from each other (β=0.000; p<0.001), both not being PrEP users (β=−0.140; p<0.01), seeing each other more frequently (β=0.207; p<0.001), and higher perceived closeness (β=0.350; p<0.001) were associated with higher likelihood of talking about PrEP in the next six months.
For likelihood to encourage PrEP use in the next six months, our final model found that racial homophily (β=−0.106; p<0.05), a higher difference (heterophily) in PHQ score (β=0.324; p<0.001), living further away from each other (β=0.000; p<0.001), seeing each other more frequently (β=0.215; p<0.001), and higher perceived closeness (β=0.341; p<0.001) were associated with higher likelihood of encouraging friend to use PrEP in the next six months.
Figure 1 shows the ten sociocentric friendship networks in the present analyses. The color of the egos (circles) symbolizes PrEP use: egos who were not PrEP users are represented by white circles, egos who were using PrEP are represented by black circles, and egos with missing PrEP use information are represented by gray circles. The lines (ties) between egos symbolize the frequency of PrEP conversations between egos (directed, participant provided a score for each nominated friend). The lightest color denotes never having talked about PrEP, and the darkest color denoting having talked often about PrEP.
Figure 1: PrEP conversation frequency, no spatial consideration.
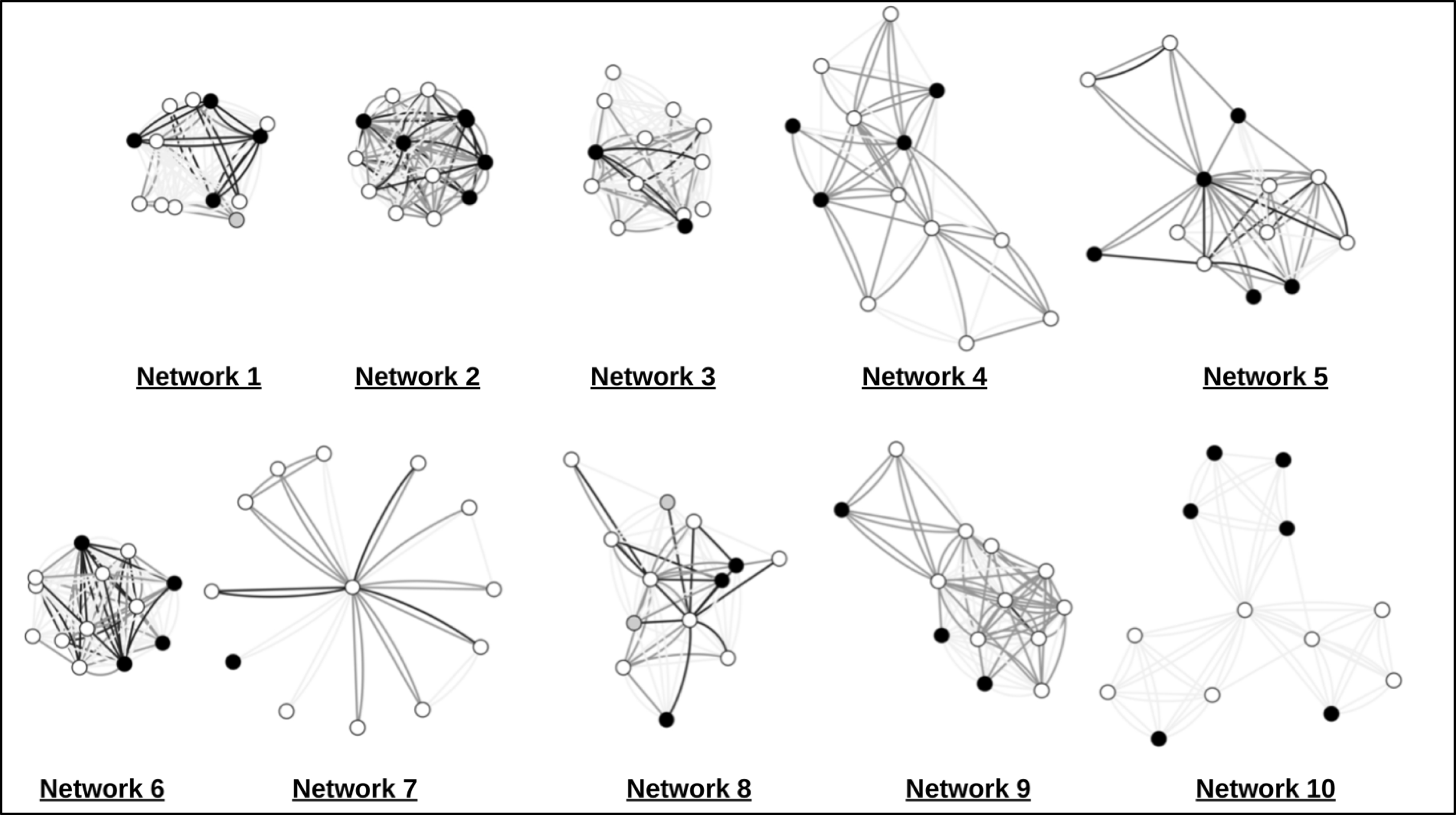
Figure 1 shows the ten sociocentric friendship networks in the present analyses. The color of the egos (circles) symbolizes PrEP use: egos who were not PrEP users are represented by white circles, egos who were using PrEP are represented by black circles, and egos with missing PrEP use information are represented by gray circles. The lines (ties) between egos symbolize the frequency of PrEP conversations between egos (directed, participant provided a score for each nominated friend). The lightest color denotes never having talked about PrEP, and the darkest color denoting having talked often about PrEP.
Figure 2 visualizes the same ten sociocentric networks, with the line (tie) length representing the distance between the home addresses of egos (not to scale for networks with an asterick by a tie). The asterisk symbolizes those egos whose home addresses were further relative to egos within their network and whose home address distance was truncated as to prevent distorting the network visualization. The color of the egos (circles) symbolizes PrEP use: egos who were not PrEP users are represented by white circles, egos who were using PrEP are represented by black circles, and egos with missing PrEP use information are represented by gray circles. The lines (ties) between egos symbolize the frequency of PrEP conversations between egos (directed, participant provided a score for each nominated friend). The lightest color denotes never having talked about PrEP, and the darkest color denoting having talked often about PrEP.
Figure 2: PrEP conversation frequency, with spatial consideration.
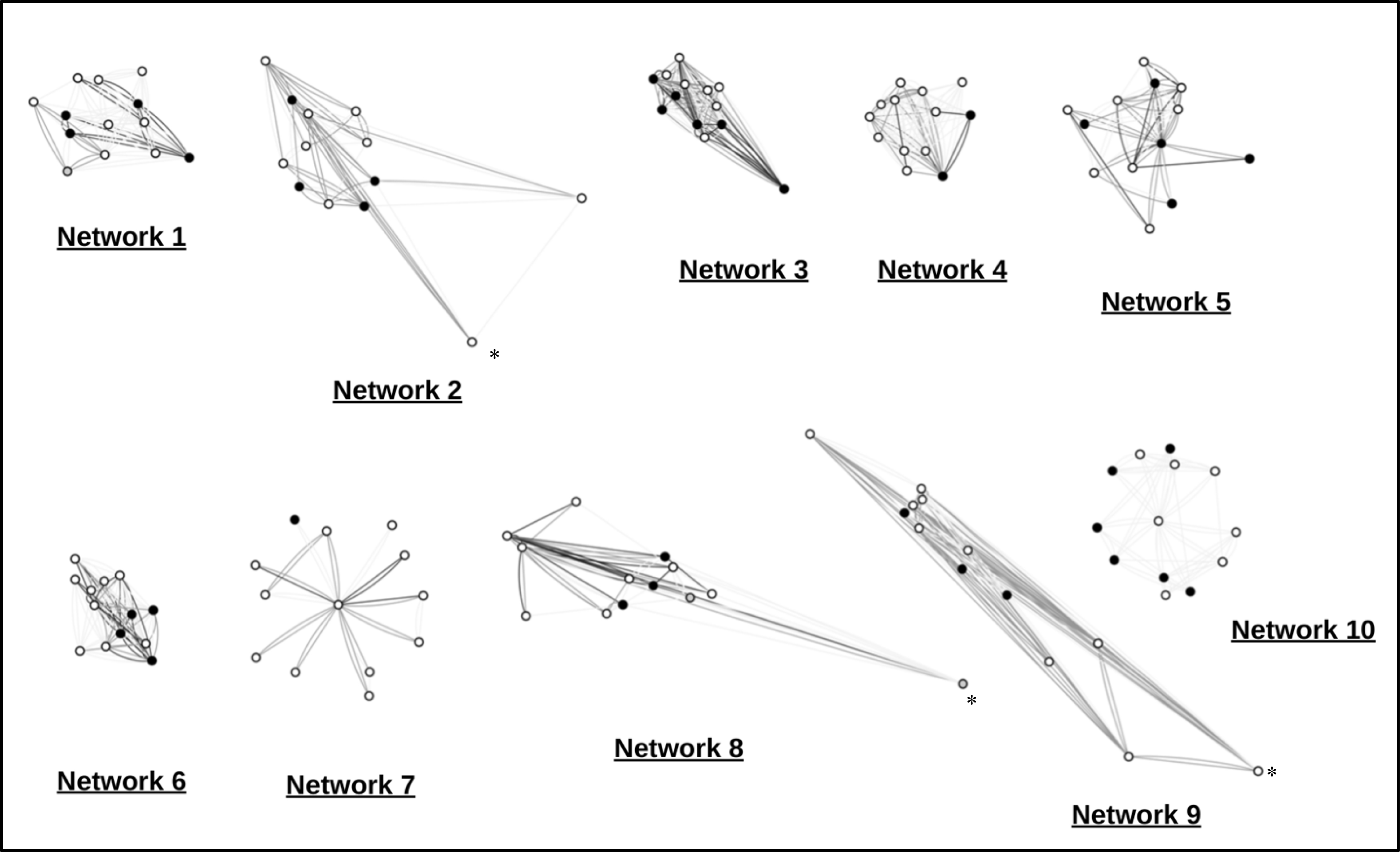
Figure 2 visualizes the same ten sociocentric networks, with the line (tie) length representing the distance between the home addresses of egos (not to scale for networks with an asterick by a tie). The asterisk symbolizes those egos whose home addresses were further relative to egos within their network and whose home address distance was truncated as to prevent distorting the network visualization. The color of the egos (circles) symbolizes PrEP use: egos who were not PrEP users are represented by white circles, egos who were using PrEP are represented by black circles, and egos with missing PrEP use information are represented by gray circles. The lines (ties) between egos symbolize the frequency of PrEP conversations between egos (directed, participant provided a score for each nominated friend). The lightest color denotes never having talked about PrEP, and the darkest color denoting having talked often about PrEP.
The directional distribution analyses show that networks are dispersed around Miami-Dade County, Florida (Figure 3). Participants from the majority of networks are primarily distributed throughout Miami Dade County (N01-N04; Y01-Y04), while one network is distributed across both Miami Dade County and Broward County (YN05), and one network is distributed across Broward County (Y05).
Figure 3: Standard Deviation Ellipses of participant home addresses, stratified by seed’s PrEP use.
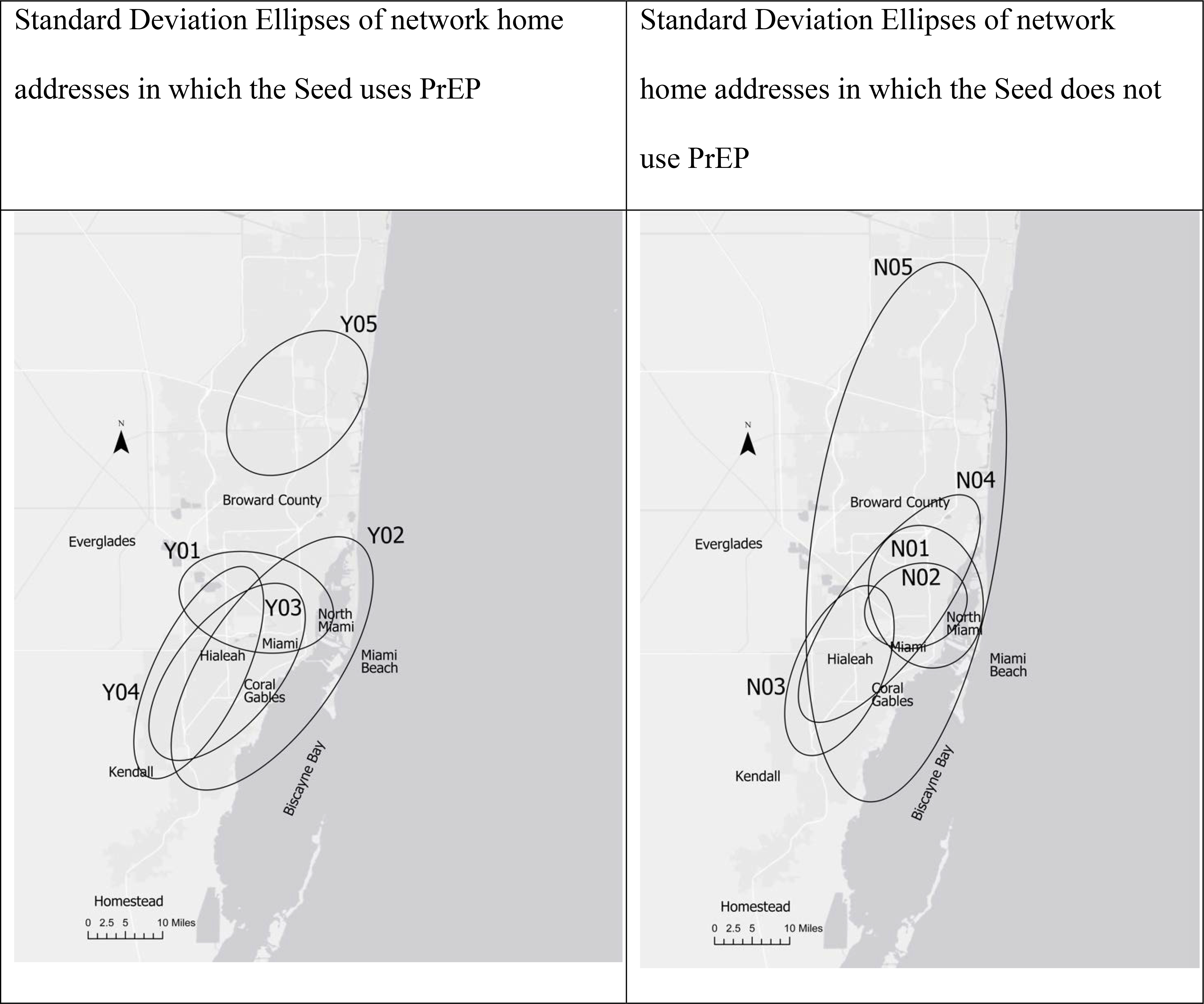
The directional distribution analyses show that networks are dispersed around Miami-Dade County, Florida (Figure 3). Participants from the majority of networks are primarily distributed throughout Miami Dade County (N01-N04; Y01-Y04), while one network is distributed across both Miami Dade County and Broward County (YN05), and one network is distributed across Broward County (Y05).
DISCUSSION
We found that LMSM demonstrated a preference to have more frequent past and future PrEP-related conversations with a friendship dyad characterized by homophily on knowledge of PrEP effectiveness, heterophily on severity of depressive symptoms, further proximity of home addresses, feeling closer to this friend, and seeing this friend more often. Frequency of past PrEP-related conversations also increased based on heterophily on the Latino cultural value of familism (i.e. emotional support to family). Frequency of future PrEP-related conversations also increased between dyads if both LMSM were not using PrEP. LMSM reported an increased likelihood to encourage a friend to use PrEP based on a friendship dyad characterized by racial homophily, heterophily on severity of depressive symptoms, proximity of home addresses, feeling closer to this friend, and seeing this friend more often. Additionally, there was great variety in conversations about PrEP between the networks- while some networks had much discussion about PrEP, other networks did not discuss PrEP as extensively.
While discrimination stress was significant in our initial models for PrEP-related conversations, when social network factors were introduced (such as frequency of seeing each other and closeness), this relationship was no longer significant. This may be explained by personalismo, an important Latino cultural construct promoting conversations about sensitive topics, such as HIV prevention and PrEP, only once trust, support, and empathy are established within friendships.41,42 Network-related factors can further explore the construct of personalismo which could influence PrEP-related conversations more than other more traditional cultural values. Future research can identify how network factors such as betweenness, density, and centrality may influence PrEP-related conversations. There is significant heterogeneity among MDC Latinos regarding country of origin/birth and immigration status.43 Future research can consider investigating the role of these factors on LMSM friendship formation and network configuration using social network analyses such as exponential random graph modeling.
Our findings suggest that LMSM have a higher likelihood of having PrEP-related conversations and encouraging friends to use PrEP when when they feel closer to their friend and when they saw their friend more often. This finding is especially important in MDC, the epicenter of the US HIV epidemic that is a majority Latino hub.1,2 Our findings suggest that LMSM may only feel comfortable enough having PrEP-related conversations with friends they feel attached to or see more often: this also aligns with the Latino cultural value of personalismo.41,42 This finding that emotional closeness and physical interactions is associated with PrEP-related conversations is novel and important. Social network-based interventions designed to increase PrEP uptake among LMSM friends can include educational programs centered on PrEP promotion scripts. Future research can identify how those LMSM who are isolated or not as connected to the LMSM community can be reached for PrEP promotion strategies using non-convential gay-oriented settings. For example, pharmacy chains are neutral environments for providing PrEP and PrEP service information, which could allow us to reach LMSM not engaged in the gay scene.
Heterophily, or lower homophily, in family emotional support (e.g., lower homophily on family emotional support), was positively associated with previous conversations and a higher likelihood of talking about PrEP in the next six months. According to the Mexican Cultural Values scale, family emotional support is described as desirability to maintain close relationships with family members, or in our context, LMSM friends.17 Interestingly, homophily on other Latino cultural values such as family as referent (reliance on communal interpersonal reflection to define the self) or family obligation (perceived importance of tangible caregiving), were not significantly associated with PrEP-related conversations. Although culture may be an important predictor of sharing health-related information, heterophily on emotional support of the family, was found to be important as well. As some LMSM may have immigrated to the US alone, future qualitative research should consider investigating the role of heterophily on familism in health-related communications among LMSM to explore this finding.
In addition to heterophily on emotional support to family, heterophily on depressive symptoms, as measured by the PHQ was found to be associated with more frequent PrEP conversations. This may be due to one of two reasons. First, friendships may be more mismatched in depressive symptoms, and conversations may occur more in these mismatched friendships. Previous studies have found that nondepressed individuals make friendships without regard to depressive symptoms;44 however, depressive individuals have been found to find depressed individuals less attractive as friends.45 This mismatch in depressive symptoms in friendships, facilitates social interactions such as PrEP-related conversations. Alternatively, as depressive symptoms has been shown to be associated with increased sexual compulsivity,46 nondepressed LMSM may be more likely to engage in PrEP-related conversations with their depressed and higher sexual risk-taking friends (or vice versa).
Previous studies have found that homophily on race and ethnicity are the strongest drivers of group affiliation.11 We did not find this to be the case for PrEP-related conversation; instead we found that homophily on race had decreased associations with encouraging a friend to use PrEP. Notably, our sample consisted of only MSM with Latino ethnicity. Our findings only somewhat support previous research which suggests that there is ease of conversation between similar races: among Latinos, the relationship between racial homophily and conversation ease contrasts previous findings conducted with mixed-ethnicity groups.11 Among nationally heterogenous Latino subgroups, race and skin color plays an important role in friendship formation, with the sending society having a stronger influence on preference than US culture.47 This suggests that cultural and societal racial views from Latinos’ country of origin may affect the formation of Latino friendships in the US, which will then influence the type of information shared between mixed-race Latino friendship dyads. In addition, we found that LMSM have a higher likelihood of having PrEP-related conversations and encouraging friends to use PrEP when their friends live further from them. Although the estimates for this significant relationship were small (Effect Estimates <0.000), this identified a positive relationship between further distance and more PrEP conversations. This finding could suggest that LMSM may be less likely to discuss sensitive topics such as PrEP with friends of the same race or who live closer together due to the opportunity for more overlapping networks discouraging conversations around taboo topics such as sex, HIV, and PrEP. Otherwise, our findings could suggest that participants may have more frequent conversations from friends whom they perceive to be geographically isolated, as they are further from their home address. Additionally, our findings must be interpreted with caution as this is a pilot study: future studies with larger samples can be conducted to provide additional power.
In the era of COVID-19, our findings are especially important for HIV prevention. To surmount geographic isolation as a determinant, future studies should explore the use of technology-based HIV prevention strategies. Technology-based HIV prevention strategies could include the use of theory-based mobile phone apps,48 telemedicine/telehealth for PrEP delivery,49 HIV self-testing,50 or recruitment using technology such as social media, among others.51 Another option is to use geographic fencing to identify and recruit participants. Geographic fencing includes having a virtual perimeters for a geophysical area.52 For example, future studies should assess the feasibility of using a mobile phone app including setting up wireless “fences” in high HIV risk zip codes or areas: when individuals enter these areas, an app could send an alert to engage in protective behavior or alert individuals of the nearest HIV prevention services.52 Distance may be less relevant in technology-based strategies, as they can be implemented virtually anywhere with adequate wireless connectivity. Interventions to address geographic isolation could also include mobile PrEP clinics, which can attract potential PrEP candidates on a neighborhood-by-neighborhood basis.53 Future research could consider calculating the spatial mismatch of neighborhoods using the proxy of census tracts through a PrEP-to-Need ratio (number of PrEP prescriptions divided by number of new HIV diagnoses), as has been previously done with other health topics.54
It is interesting to note that the sociocentric visualizations reveal that one network did not discuss PrEP at all (Network 10). This network also appears to be spatially close. This emphasizes the importance of reaching LMSM who may not be in networks which discuss PrEP. Mass media interventions can reach these individuals utilizing strategies such as bilingual PrEP advertising, sexual health clinics, and community based organizations with PrEP navigators. Additionally, future interventions can address structural factors that may impact PrEP access, such as the guidelines in Miami around PrEP for those without documentation and who are un/underinsured. Future research questions could also include those surrounding the informal economy around PrEP (i.e. pill-sharing), which our study did not measure.
There were several limitations to our study. First, our study was cross-sectional, and no causality can be inferred. In addition, mediation analyses cannot be conducted with confidence. Second, due to the lack of established knowledge of the distributional properties of parameter estimates in LMSM social networks, a conventional power analysis could not be conducted to estimate needed sample size for this project.55 However, previous successful social network studies with non-LMSM have been conducted with similar sample sizes.27,56,57 Finally, we offered our survey bilingually, meaning that each survey prompt, question, and response options were offered in English and Spanish in tandem. As a result, we cannot accurately assess the proportion of people who took the survey in English or Spanish. Finally, we only assessed whether LMSM received PrEP information from their social networks: a future study will assess additional sources where LMSM get PrEP information from and describe the PrEP provider and navigator landscape in MDC.
Conclusions
Our findings suggest that both homophily and heterophily play a role in PrEP-related conversations. Homophily was not associated with all cultural values when examining health communication, and future interventions can include only those values which are important. Geographic closeness was salient in associations with PrEP-related conversations. The HIV epidemic is far from ending: people are multidimensional, and the power of social networks must be harnessed to illuminate novel opportunities to end HIV. Future studies and interventions must strive to incorporate network stru ctures and dynamics to eradicate HIV.
Acknowledgments
Funding:
We would like to acknowledge the efforts and contributions of our participants, our community partner Latinos Salud, and our mentors. Research reported in this publication was supported by the National Institute on Drug Abuse (awards #K99DA041494; #R00DA041494), the National Institute on Minority Health and Health Disparities (awards #F31MD015988; #P20MD002288; #U54MD002266), the National Institute of Allergy and Infectious Diseases (award #P30AI050409) and the National Institute of Mental Health (awards #R01MH125727, #R01MH100021, #P30MH116867) of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse, the National Institute on Minority Health and Health Disparities, the National Institute of Allergy and Infectious Diseases, the National Institute of Mental Health or the National Institutes of Health.
ABBREVIATIONS
- HIV
Human Immunodeficiency Virus
- LMSM
Latino men who have sex with men
- PrEP
Pre-exposure prophylaxis
Footnotes
Conflict of Interest:
The authors disclose they have no perceived or real conflicts of interest.
References
- 1.Centers for Disease Control and Prevention. HIV Surveillance Report, 2018 (Updated). November 2019 2020. [Google Scholar]
- 2.HIV/AIDS Section, Florida Department of Health. HIV/AIDS Epidemiological Profile, EMA 011A: HIV Diagnoses from 2014 to 2018. In: Division of Disease Control and Health Protection, ed2020. [Google Scholar]
- 3.Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. New England Journal of Medicine. 2010;363(27):2587–2599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bangsberg D, Haberer J, Psaros C, Baeten J, Katabira E, Tumwesigye E. High adherence and high effectiveness observed in HIV discordant couples: Partners PrEP Study, adherence monitoring and counseling substudy. Paper presented at: 19th Conference on Retroviruses and Opportunistic Infections (CROI)2012. [Google Scholar]
- 5.Thigpen MC, Kebaabetswe PM, Paxton LA, et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. New England Journal of Medicine. 2012;367(5):423–434. [DOI] [PubMed] [Google Scholar]
- 6.Choopanya K, Martin M, Suntharasamai P, et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. The Lancet. 2013;381(9883):2083–2090. [DOI] [PubMed] [Google Scholar]
- 7.HIV prevention pill not reaching most Americans who could benefit – especially people of color [press release]. 2018–03-23T06:52:05Z 2018. [Google Scholar]
- 8.Centers for Disease Control and Prevention. 2019 Conference on Retroviruses and Opportunistic Infections: PrEP use has increased among gay and bisexual men at risk for HIV. https://www.cdc.gov/nchhstp/newsroom/2019/croi-2019.html. Published 2019. Accessed September 7, 2020.
- 9.J. F Lessons learned from the US PrEP Demonstration Project: Moving from the “real world” to the “real, real world.”. 2015; San Francisco, CA. [Google Scholar]
- 10.Algarin AB, Shrader CH, Bhatt C, Hackworth BT, Cook RL, Ibañez GE. The Pre-exposure Prophylaxis (PrEP) Continuum of Care and Correlates to Initiation Among HIV-Negative Men Recruited at Miami Gay Pride 2018. J Urban Health. 2019;96(6):835–844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McPherson M, Smith-Lovin L, Cook JM. Birds of a feather: Homophily in social networks. Annual review of sociology. 2001;27(1):415–444. [Google Scholar]
- 12.Monge PR, Contractor NS. Theories of communication networks. Oxford University Press, USA; 2003. [Google Scholar]
- 13.Young LE, Jonas AB, Michaels S, Jackson JD, Pierce ML, Schneider JA. Social-structural properties and HIV prevention among young men who have sex with men in the ballroom house and independent gay family communities. Social Science & Medicine. 2017;174:26–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Antshel KM. Integrating culture as a means of improving treatment adherence in the Latino population. Psychology, Health & Medicine. 2002;7(4):435–449. [Google Scholar]
- 15.Villarruel AM, Jemmott LS, Jemmott JBI. Designing a Culturally Based Intervention to Reduce HIV Sexual Risk for Latino Adolescents. Journal of the Association of Nurses in AIDS Care. 2005;16(2):23–31. [DOI] [PubMed] [Google Scholar]
- 16.Cauce AM, Domenech-Rodriguez M. Latino families: Myths and realities. Latino children and families in the United States: Current research and future directions. 2002:3–25. [Google Scholar]
- 17.Knight G, Gonzales N, Saenz D, et al. The Mexican American Cultural Values scales for Adolescents and Adults. J Early Adolesc. 2010;30(3):444–481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shrader CH, Arroyo-Flores J, Skvoretz J, et al. PrEP Use and PrEP Use Disclosure are Associated with Condom Use During Sex: A Multilevel Analysis of Latino MSM Egocentric Sexual Networks. AIDS Behav. 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Deane KD, Parkhurst JO, Johnston D. Linking migration, mobility and HIV. Trop Med Int Health. 2010;15(12):1458–1463. [DOI] [PubMed] [Google Scholar]
- 20.Carrico AW. Getting to Zero: Targeting Psychiatric Comorbidities as Drivers of the HIV/AIDS Epidemic. International Journal of Behavioral Medicine. 2019;26(1):1–2. [DOI] [PubMed] [Google Scholar]
- 21.Mustanski B, Birkett M, Kuhns LM, Latkin CA, Muth SQ. The role of geographic and network factors in racial disparities in HIV among young men who have sex with men: an egocentric network study. AIDS and Behavior. 2015;19(6):1037–1047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.HIV/AIDS Surveillance, Florida Department of Health in Miami-Dade County. HIV Among HIspanics/Latinos in Miami-Dade - 2016. Paper presented at: Hispana Iniciativa2017; Miami, FL. [Google Scholar]
- 23.Valverde EE, Oster AM, Xu S, Wertheim JO, Hernandez AL. HIV Transmission Dynamics Among Foreign-Born Persons in the United States. J Acquir Immune Defic Syndr. 2017;76(5):445–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brondolo E, Brady Ver Halen N, Pencille M, Beatty D, Contrada RJ. Coping with racism: a selective review of the literature and a theoretical and methodological critique. J Behav Med. 2009;32(1):64–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Centers for Disease Control and Prevention. Preexposure prophylaxis for the prevention of HIV infection in the United States—2017 Update: a clinical practice guideline. In: US Public Health Service, ed. Atlanta, GA: 2018. [Google Scholar]
- 26.Salganik MJ, Heckathorn DD. Sampling and estimation in hidden populations using respondent-driven sampling. Sociological methodology. 2004;34(1):193–240. [Google Scholar]
- 27.Kanamori M, De La Rosa M, Shrader C-H, et al. Progreso en Salud: Findings from Two Adapted Social Network HIV Risk Reduction Interventions for Latina Seasonal Workers. International Journal of Environmental Research and Public Health. 2019;16(22):4530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cervantes RC, Fisher DG, Padilla AM, Napper LE. The Hispanic Stress Inventory Version 2: Improving the assessment of acculturation stress. Psychological assessment. 2016;28(5):509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gilbody S, Richards D, Brealey S, Hewitt C. Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): a diagnostic meta-analysis. Journal of general internal medicine. 2007;22(11):1596–1602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Association AP. Diagnostic and statistical manual of mental disorders (DSM-5®). American Psychiatric Pub; 2013. [DOI] [PubMed] [Google Scholar]
- 31.ArcGIS Pro [computer program]. 2019.
- 32.R: A language and environment for statistical computing [computer program]. Vienna, Austria: 2019. [Google Scholar]
- 33.Dekker D, Krackhardt D, Snijders TA. Sensitivity of MRQAP tests to collinearity and autocorrelation conditions. Psychometrika. 2007;72(4):563–581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Prell C Social network analysis: History, theory and methodology. Sage; 2012. [Google Scholar]
- 35.Everett MG, Borgatti SP. The dual-projection approach for two-mode networks. Social Networks. 2013;35(2):204–210. [Google Scholar]
- 36.Borgatti SP, Mehra A, Brass DJ, Labianca G. Network analysis in the social sciences. science. 2009;323(5916):892–895. [DOI] [PubMed] [Google Scholar]
- 37.Hanneman RA, Riddle M. Introduction to social network methods. In: University of California Riverside; 2005. [Google Scholar]
- 38.Csardi G, Nepusz T. The igraph software package for complex network research. InterJournal, complex systems. 2006;1695(5):1–9. [Google Scholar]
- 39.Shannon P, Markiel A, Ozier O, et al. Cytoscape: a software environment for integrated models of biomolecular interaction networks. Genome Res. 2003;13(11):2498–2504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.ESRI. Directional Distribution (Standard Deviational Ellipse) (Spatial Statistics). https://pro.arcgis.com/en/pro-app/latest/tool-reference/spatial-statistics/directional-distribution.htm. Published 2020. Accessed December 29, 2020.
- 41.Añez LM, Paris M Jr., Bedregal LE, Davidson L, Grilo CM. Application of cultural constructs in the care of first generation Latino clients in a community mental health setting. J Psychiatr Pract. 2005;11(4):221–230. [DOI] [PubMed] [Google Scholar]
- 42.Acevedo V Cultural competence in a group intervention designed for Latino patients living with HIV/AIDS. Health Soc Work. 2008;33(2):111–120. [DOI] [PubMed] [Google Scholar]
- 43.US Census Bureau, Population Estimates, American Community Survey. Race and Hispanic Origin: Hispanic or Latino, percent. In:2019. [Google Scholar]
- 44.Schwartz-Mette RA, Lawrence HR, Shankman J, Fearey E, Dueweke A. Birds of a feather want to talk together: The impact of depressive symptoms on initial stages of friendship formation in older adolescence. Journal of Social and Clinical Psychology. 2018;37(10):769–793. [Google Scholar]
- 45.Schaefer DR, Kornienko O, Fox AM. Misery does not love company: Network selection mechanisms and depression homophily. American Sociological Review. 2011;76(5):764–785. [Google Scholar]
- 46.Parsons JT, Grov C, Golub SA. Sexual compulsivity, co-occurring psychosocial health problems, and HIV risk among gay and bisexual men: further evidence of a syndemic. American journal of public health. 2012;102(1):156–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Roth WD, Marin A. The Role of Skin Color in Latino Social Networks: Color Homophily in Sending and Receiving Societies. Sociology of Race and Ethnicity. 2020:2332649220940346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Biello KB, Marrow E, Mimiaga MJ, Sullivan P, Hightow-Weidman L, Mayer KH. A mobile-based app (MyChoices) to increase uptake of HIV testing and pre-exposure prophylaxis by young men who have sex with men: protocol for a pilot randomized controlled trial. JMIR research protocols. 2019;8(1):e10694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Touger R, Wood BR. A review of telehealth innovations for HIV pre-exposure prophylaxis (PrEP). Current HIV/AIDS Reports. 2019;16(1):113–119. [DOI] [PubMed] [Google Scholar]
- 50.LeGrand S, Muessig KE, Horvath KJ, Rosengren AL, Hightow-Weidman LB. Using Technology to Support HIV Self-Testing Among Men Who Have Sex with Men. Current Opinion in HIV and AIDS. 2017;12(5):425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.MacCarthy S, Barreras JL, Mendoza-Graf A, Galvan F, Linnemayr S. Strategies for Improving Mobile Technology–Based HIV Prevention Interventions With Latino Men Who Have Sex With Men and Latina Transgender Women. AIDS Education and Prevention. 2019;31(5):407–420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Besoain F, Perez-Navarro A, Aviñó CJ, Caylà JA, Barriga NA, de Olalla PG. Prevention of HIV and Other Sexually Transmitted Infections by Geofencing and Contextualized Messages With a Gamified App, UBESAFE: Design and Creation Study. JMIR mHealth and uHealth. 2020;8(3):e14568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Doblecki-Lewis S, Kobetz E, Byrne, et al. 1965. PrEP On the Go! Implementation Mobile PrEP, STI, and HIV Prevention Services in South Florida. Open Forum Infect Dis. 2019;6(Suppl 2):S65–S65. [Google Scholar]
- 54.Williams J, Petersen N, Stoler J. Characterizing the spatial mismatch between intimate partner violence related healthcare services and arrests in Miami-Dade County, Florida. BMC Public Health. 2018;18(1):1085–1085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kolaczyk ED, Krivitsky PN. On the question of effective sample size in network modeling: An asymptotic inquiry. Statistical science: a review journal of the Institute of Mathematical Statistics. 2015;30(2):184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Fujimoto K, Williams ML. Racial/ethnic differences in sexual network mixing: A log-linear analysis of HIV status by partnership and sexual behavior among most at-risk MSM. AIDS and Behavior. 2015;19(6):996–1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Kuhns LM, Hotton AL, Schneider J, Garofalo R, Fujimoto K. Use of Pre-exposure Prophylaxis (PrEP) in Young Men Who Have Sex with Men is Associated with Race, Sexual Risk Behavior and Peer Network Size. AIDS Behav. 2017;21(5):1376–1382. [DOI] [PMC free article] [PubMed] [Google Scholar]