

Abstract
Background
Burn injuries are a leading cause of morbidity and disability, with the burden of disease being disproportionately higher in low- and middle-income countries (LMIC). Burn prevention programmes have led to significant reductions in the incidence of burns in high-income countries. However, a previous systematic review published in 2015 highlighted that implementation and evaluation of similar programmes has been limited in LMIC. The objective of this scoping review and narrative synthesis was to summarise and understand the initiatives that have been carried out to reduce burn injuries in LMIC and their effectiveness.
Methods
We aimed to identify publications that described studies of effectiveness of burn prevention interventions applied to any population within a LMIC and measured burn incidence or burns-related outcomes. Suitable publications were identified from three sources. Firstly, data was extracted from manuscripts identified in the systematic review published by Rybarczyk et al. We then performed a search for manuscripts on burn prevention interventions published between January 2015 and September 2020. Finally, we extracted data from two systematic reviews where burn evidence was not the primary outcome, which were identified by senior authors. A quality assessment and narrative synthesis of included manuscripts were performed.
Results
In total, 24 manuscripts were identified and categorized according to intervention type. The majority of manuscripts (n = 16) described education-based interventions. Four manuscripts focused on environmental modification interventions and four adopted a mixed-methods approach. All of the education-based initiatives demonstrated improvements in knowledge relating to burn safety or first aid, however few measured the impact of their intervention on burn incidence. Four manuscripts described population-based educational interventions and noted reductions in burn incidence. Only one of the four manuscripts describing environmental modification interventions reported burns as a primary outcome measure, noting a reduction in burn incidence. All mixed-method interventions demonstrated some positive improvements in either burn incidence or burns-related safety practices.
Conclusion
There is a lack of published literature describing large-scale burn prevention programmes in LMIC that can demonstrate sustained reductions in burn incidence. Population-level, collaborative projects are necessary to drive forward burn prevention through specific environmental or legislative changes and supplementary educational programmes.
Keywords: Burns, Prevention, Low-and-middle income countries, Systematic review
Highlights
We have provided an update on the status of burn prevention programmes in low- and middle-income countries.
The majority of studies identified in this review described small-scale education-based initiatives that used knowledge-based outcomes.
Through our updated search, we identified a number of interventions that demonstrated the potential success of environmental initiatives through improving unsafe cookstoves.
Population-level, collaborative projects are necessary to drive forward burn prevention, through specific environmental interventions and supplementary educational programmes.
Background
Burn injuries represent a significant disease burden on the world’s population, with nearly 9 million injuries and an estimated 120,000–180,000 deaths annually [1]. The majority occur in low- and middle-income countries (LMICs), with almost two-thirds in WHO-defined African and South-East Asia regions. This contrasts with many high-income countries, where burn death rates have been decreasing over time. Non-fatal burns are also one of the leading causes of morbidity and disability. Almost 18 million disability adjusted life years (DALYs) can be accounted to burns with a disproportionate 90% of this burden again being borne by LMICs. In Bangladesh, Colombia, Egypt and Pakistan, burn injuries account for up to 18% of permanent disabilities [2]. Additionally, disfigurements cause significant emotional and physical suffering which further ostracise burn survivors from society [3]. Furthermore, burn injuries inflict heavy healthcare costs [4]; by one estimate the life-time health costs of a serious burn are five times that of either HIV or stroke [5].
Burn preventative intervention strategies can be categorized into three domains: education, environmental modification and mixed methods initiatives. Interventions may be applied within sub-populations including schools and local communities, or at population levels [6,7].
Burn prevention programmes, such as public education and environmental modification (including, smoke alarms and fire-retardant fabrics) have had a significant positive impact on incidence of burn injuries in high-income countries (HIC) [8–10]. Well-designed intervention programmes in HICs have also demonstrated cost effectiveness [8]. In this paper we have performed a scoping systematic review and narrative synthesis of research evidence on burn prevention in LMIC. In doing so we build on the systematic review by Rybarczyk et al. [7] and extend it to include studies of interventions where burn evidence was not the primary outcome. Such studies could be of two types: intervention to prevent injuries as a whole where burns were a sub-group and interventions to reduce indoor pollution where burns were a secondary outcome.
Methods
Literature retrieval: overview and review questions
The proposed scoping review will be conducted in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews [11]. The protocol for this review was registered on PROSPERO (registration number: CRD42021229045). We carried out a search specifically for manuscripts describing studies of effectiveness of interventions to prevent burn injury in LMIC (World Bank Classification of Countries [12]). Manuscripts were identified from three sources (Figure 1). Firstly, data was extracted from manuscripts identified in an existing systematic review by Rybarczyk et al. [7]. Secondly, we updated Rybarczyk’s review by performing a search for manuscripts on burn preventive interventions in LMIC, published between January 2015 and September 2020. Thirdly, we scanned the reference list of full text papers as well as utilized knowledge from the senior authors and personal contacts and academic networks to identify papers not identified with the previous two methods. Two other relevant systematic reviews were identified by two senior authors using this method and data extracted fromthem [13,14].
Figure 1.
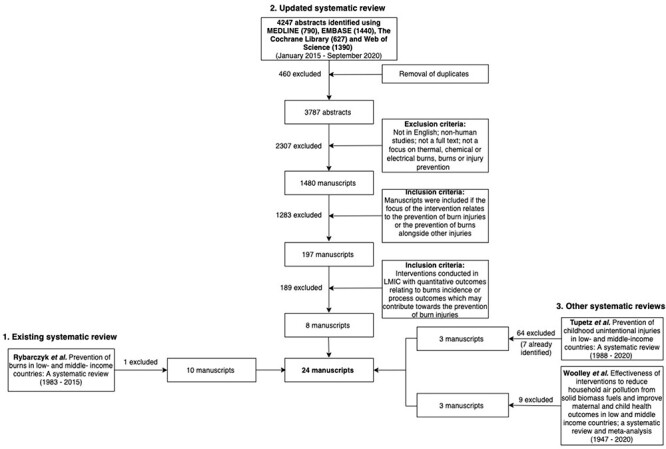
PRISMA flow diagram of the systematic review process. PRISMA Preferred Reporting Items for Systematic reviews and Meta-Analyses, LMIC low- and middle-income countries
We developed a set of research questions that we hypothesized would be useful in the development of future burn prevention initiatives.
(1) What types of burn prevention initiatives have been carried out in LMIC?
(2) What are the characteristics of the targeted populations in these studies?
(3) What methodologies have been used to deliver and study the effectiveness of these burn prevention initiatives?
(4) How effective have these burn prevention initiatives been and are the results sustained?
(5) What evidence gaps exist in the current burn prevention literature?
Inclusion and exclusion criteria
Participants
Participants of all genders and ages were included in this study.
Concept
We applied the following exclusion and inclusion criteria when screening all manuscripts identified from our three sources listed above. Manuscripts were excluded based on the following criteria: not in English language; non-human studies; not a full text; manuscripts that did not cover prevention of thermal, chemical or electrical burns. The inclusion criteria were applied in two stages.
(1) Manuscripts were included if the focus of the intervention relates to the prevention of burn injuries or the prevention of burns alongside other injuries.
(2) Manuscripts were included if the interventions were conducted in LMIC and included quantitative outcomes relating to burns incidence (with or without statistical analysis) or process outcomes that may contribute towards the prevention of burn injuries.
i. Context
All participants from low- and middle- income countries as defined by the World Bank Atlas method were included [12].
Search strategy
Existing systematic review
We identified an existing systematic review published in 2016 by Rybarczyk et al. [7]. This review searched for literature published between 1983 and 2015 on preventative strategies to reduce burn injury in LMIC. They identified 11 manuscripts, however their exact search strategy was not published or made available. We applied our exclusion and inclusion criteria to screen and extract papers from this review.
Update of existing systematic review
The search was performed using MEDLINE, EMBASE, the Cochrane Library and Web of Science. We replicated the search of Rybarczyk et al. [7] as closely as possible. Searches were conducted by combining keywords relating to ‘burns’ with keywords relating to ‘prevention’ or ‘intervention’. Abstracts were limited to English language, human studies and publications between January 2015 and September 2020. Following removal of duplicates, 3787 manuscripts were identified. Two authors [KP, KCL] then reviewed the remaining manuscripts by applying the exclusion followed by the inclusion criteria. Conflicts were resolved by a third author [NM].
Other relevant systematic reviews
We discerned that the scoping review may fail to detect some injury prevention studies where burns were a secondary outcome or studies that alter fuel sources to improve air quality and record burns as a secondary outcome. Using the ‘snowballing’ method, two other systematic reviews were identified by two senior authors which included manuscripts relating to burns prevention in LMIC. One review recorded burns as a sub-group in studies designed to prevent injury as a whole and the other review included burns as a secondary outcome in studies designed to reduce indoor pollution and where respiratory disease was the main outcome. We applied our exclusion and inclusion criteria to screen and extract manuscripts from these additional reviews.
Evidence screening, data extraction and quality assessment
We generated a consolidated list of manuscripts from the above three sources. Full manuscripts were then reviewed in detail, ensuring they fulfilled our inclusion criteria.
Data extracted from the manuscripts retrieved across all three sources included the population studied, study design, sample size, domain of intervention, intervention details, method of data collection, follow-up time, demographic clinical features and outcome measures.
Outcomes included burns incidence and process outcomes, such as burns-related knowledge, and environmental modifications such as the removal of environmental hazards. For the studies involving large populations (education–media-based population level initiatives), aspects of intervention delivery as defined by Steckler et al. including recruitment, reach, intended dose and fidelity were also analysed [15].
Two authors (KP and KCL) conducted a quality assessment for all included manuscripts. We used the following tools to assess quality. (1) For studies with a pre-post design we used the National Institutes of Health (NIH) bias assessment tool. (2) For non-randomized studies we used the Cochrane Risk Of Bias In Non-randomized Studies—of Interventions (ROBINS-I) tool. (3) For randomized studies we used the Risk of Bias I (ROB-I) tool [16–18]. Disagreements were resolved by consensus or based on discussions with senior authors (NM,RL).
Results
Study selection
Across all three sources of search (Figure 1), we identified 24 manuscripts that met our inclusion criteria and describe 24 studies relating to the prevention of burn injuries inLMIC.
Our first source, Rybarczyk’s systematic review, identified 11 manuscripts [7]. One of these manuscripts was excluded from our review as it was a systematic review of epidemiological papers, which failed to clearly describe a burns prevention strategy with outcomes relating to burns incidence or relevant process outcomes [19]. Rybarczyk’s review thus identified 10 of the 24 studies identified in our review.
The second source of papers was our search for burn prevention interventions in LMIC, published between January 2015 and September 2020. This produced 3787 abstracts following removal of duplicates (n = 460). After screening for titles and exclusion criteria, the remaining 1480 manuscripts were then screened using the two-step approach mentioned above, yielding 197 manuscripts that had a primary focus on interventions specifically relating to the prevention of burns or burns in addition to other injuries. Of these manuscripts, 8 described studies of preventative interventions conducted in LMIC with outcomes relating to burns incidence and/or process outcomes and were included in the final analysis.
The third source, the two other systematic reviews, yielded 3 suitable manuscripts from each review. The first review investigated the impact of biomass stoves on respiratory health and included burn injury as an outcome measure [13]. The second focused on childhood injury prevention in LMIC and included studies that described interventions to prevent burn injury [14].
Methodology of studies and outcome types
Of the 24 included studies, seven were from India, four from Iran, three from China, three from South Africa and one each from Zambia, Ethiopia, Rwanda, Malawi, Indonesia, Turkey and Brazil. Studies were categorized according to the three intervention domains identified in the introduction and the population with which the intervention is applied. This left us with five groups (Tables 1–5): (1) education–school-based initiatives (6 studies), (2) education–community-based initiatives (6 studies), (3) education–media-based population level initiatives (4 studies), (4) environmental initiatives (4 studies) and (5) mixed-method initiatives (4 studies).
Table 1.
Educational initiatives—school-based
| Year | Authors | Country of origin | Population studied | Actual sample size | Study design | Intervention method | Follow -up time (post-intervention) | Outcome types | Estimated burn incidence (baseline rates/100,000) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| 2021 | Bagheri et al. [28] | Iran (Tehran) | Primary school children (from 6 mixed public schools) | 180 students | Pre-post | Educational training: An educational scenario (a story that discussed hazardous situations relating to burns and procedures to resolve them) | Immediately after intervention and at 3 months | Knowledge of burn prevention and initial actions when managing burns (measured by pre and post questionnaires) | NA | Students’ knowledge scores relating to burn prevention and initial actions when managing burns significantly increased immediately after the intervention and at 3 months post-intervention (p < 0.05) |
| 2015 | Cao et al. [25] | China (Zunyi) | Children in rural schools, ages 8–16 years | 2342 (baseline) 1502 (follow-up), 5 clusters | Randomized control (cluster) | 16-month multi-level education programme in students: 1. Letter to parents discussing precautions for accidental injuries and management of accidental injuries. 2. Handbook and posters that encourage safety awareness. 3. Lectures and video education about accidental injuries and avoidance of injury-risk behaviours, provided to teachers and students. 4. Teacher training on management of accidental injury | 16 months | Knowledge of injury prevention (measured by pre and post questionnaires) and accidental injury incidence (measured by self-reported pre and post questionnaire) | No burn-specific incidence rate reported | Significant increase in burn-specific knowledge and attitude scores (KAS) in the intervention groups (p < 0.001). Accidental injury incidence rates decreased in the intervention and control group with increasing KAS. At follow-up, injury incidence was 11.04% (intervention) and 12.84% (control); there were no significant differences in injury incidence between the two groups (p > 0.05) |
| 2015 | Wang et al. [29] | China (Shenzhen) | Children in primary and middle classes of 19 kindergartens | 2271 (baseline) 2003 (follow-up) 9 schools (intervention), 10 schools (control) | Non-randomized control | Multi-level intervention applied over 1 year: Parents’ seminars, teacher training, audio and video lectures, graphic material and other methods for injury prevention | 1 year | Injury (including burns) incidence (measured by self-reported pre and post questionnaires) and relevant treatment costs | 31/2271 = 1.37%, 1365 per 100 k | Burns incidence decreased by 63.6% in intervention group (11 baseline, 4 follow-up) compared to 19% in control group (21 baseline, 17 follow-up) (p = 0.027) Per capita injury treatment cost was significantly lower post-intervention (p < 0.05) and significantly different to the control group (p < 0.01) |
| 2013 | Heard et al. [27] | Zambia (Katete) | Elementary school children across 6 schools | 2747 (baseline), 312 (follow-up), | Pre-post | Burn and fire safety presentation and a burn prevention colouring book | 11 months | Knowledge of burn prevention (measured by pre and post questionnaires) | NA | Children performed significantly better in 3 of the 10 questions assessed on the questionnaire. Five questions yielded higher scores post-intervention, but these were not statistically significant. Children performed significantly worse on one question relating to burn first aid and no improvement was observed for one question |
| 2011 | Sinha et al. [26] | India (West Bengal) | Children aged 5–7 years old | 39 children | Pre-post | Comic book that aims to teach students about the burn prevention and ‘stop, drop and roll’ was read out loud in classrooms and students read along with the teacher | Immediately after intervention | Knowledge of burn prevention (measured by pre and post questionnaires) | NA | Pre-test overall score = 66.9%, this increased significantly to 99.1% immediately after the intervention (p < 0.01) |
| 1986 | Keswani et al. [30] | India (Mumbai) | School-aged population of Bombay (Mumbai) | 120 students in intervention, 120 students in control | Non-randomized control | Annual education program in schools (booklets, posters, labels, greeting cards, and the ‘You Can Prevent Burns’ film) | Unclear | Knowledge of burns prevention and management (measured by pre and post questionnaires) and mortality from burns (measured by annual report published by health department for the city) | NA | The children who received the annual education programme scored higher across all questions on the knowledge questionnaire than the control group. Trend toward fewer deaths in women 15–24 and 25–44 years old |
NA not available
Table 5.
Mixed educational and environmental initiatives
| Year | Authors | Country of origin | Population studied | Actual sample size | Study design | Intervention method | Follow-up time (post-intervention) | Outcome types | Estimated burn incidence (baseline rates/100,000) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| 2018 | Chan et al. [42] | China (Nanjiang Village, Guizhou Province) | Ethnic minority rural village community | 64 first intervention. 101 (baseline), 58 (follow up) second intervention | Pre-post | Two-year education-based intervention: face-to-face educational sessions consisting of dramas and interactive games covering general fire and electrical fire risk reduction. Banners and posters with illustrations were used to reinforce messages. Fire blanket and disaster preparedness kits were distributed to subjects | Immediately after and at 17 months | Knowledge of fire-risk perception, prevention and response (measured by pre and post questionnaire) | NA | Increased knowledge of fire prevention and use of equipment (fire blanket knowledge (OR = 3.79, 95% CI = 1.39–10.34) and use increased significantly (OR = 3.56, 95% CI = 1.34–9.49 but not for other items). Only 65.5% of households kept the fire blanket they received. Electrical fire management showed significant increases in confidence post intervention in participants. No significant difference in fire-risk awareness and fire prevention-awareness |
| 2011 | Jetten et al. [43] | India | Families with children <4 years old of Valmiki Nagar, Nai Basti and Aditya Nagar of Indore, Madhya Pradesh | 42 families (baseline) 34 (follow-up) | Pre-post | Educational programme (film with verbal instructions); distribution of barrier or playpen which was present in the house for 1.5 months | 1.5 months | Burns incidence and burns-related hazards (measured by self-reported pre and post questionnaires) | 18/42 = 42.8% = 42,857 per 100 k | Reduction of burns per household (mean number of burns per household 0.53 (pre-intervention), 0.06 (post-intervention) difference 0.47 95% CI 0.06–0.88); reduction in frequency of all dangerous situations in the home (p < 0.01) |
| 2009 | Odendaal et al. [21] | South Africa | Households with children <10 years old in an informal housing area | 211 households (baseline) 192 (follow-up) | Randomized control (individual) | Four home visits (education, enforcement, and engineering using flipcharts, information sharing, printed materials, home inspection, distribution of safety devices, and colouring pages | 1 week | Burns-related hazards and burn safety practices (measured by self-reported pre and post questionnaires) and injury scores for poisoning and falls | 21/211 = 9.95%, 9952 per 100 k (recorded but not used as an outcome measure) | Improvement of household hazard scores for electrical burns (intervention mean score = 3.0, control = 3.9, 95% CI 0.15–1.70) and paraffin safety practices (intervention mean score 2.6, control = 3.3, 95% CI 0.04–1.37); no improvement in overall burn safety practices (intervention mean score = 6.8, control = 7.1, 95% CI −0.31 to 0.80) |
| 2008 | Swart et al. [23] | South Africa | Households with children <10 years old from Slovo Park and Nomzamo, two low- income communities | 410 households (baseline) 377 (follow-up) 26 clusters per trial arm, (average cluster size: intervention = 7.27 households, control = 7.23 households) | Randomized control (cluster) | Four home visits were conducted which focused on injury prevention (child development and injury risks, prevention of burns, poisoning and falls), home inspection/hazard checklist, and caregivers were supplied with safety devices (child-proof locks, paraffin container safety cups) | 2 weeks | Injury risk scores of home hazards for burns, poisoning, and falls (measured by self-reported pre and post questionnaires) | NA | Significant improvement in burn-related safety practices (mean intervention score = 2.5, control = 2.9 p = 0.021, 95% CI −0.76 to 0.07); no significant effect on paraffin (p = 0.911, 95% CI −0.64 to −0.57) or electrical safety practices (p = 0.294, 95% CI −0.54 to 0.16) |
OR odds ratio, CI confidence interval
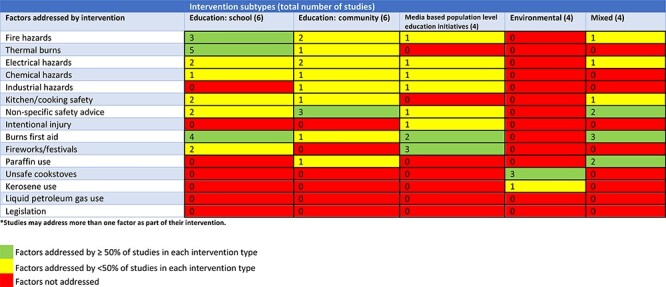
Table 6 provides an overview of factors that may be addressed to reduce burn injury and outlines the frequency with which the studies address each factor as part of their intervention. We identified no studies of the effect of regulation or regulation enforcement in LMICs.
Table 6.
Frequency of burn-related factors addressed by interventions described within studies*
|
Regarding study-design, most studies were,whereby outcomes were measured before and after the intervention was applied (12 studies), followed by randomized control trials (RCTs) (8 studies) and non-randomized trials with concurrent controls (4 studies). Table 7 summarises the measurement methods and outcomes observed in the studies. The majority of studies (67%) utilized self-reported questionnaires (with 3 studies combining both self-reported questionnaires and self-reported environment risk assessments) and the most commonly studied outcomes were the assessment of burn prevention knowledge and burns incidence.
Table 7.
Methodology of studies and outcome types
| Variable | Number of studies |
|---|---|
| Measurement methods | |
| Questionnaires (self-reported) | 16 |
| Hospital records | 4 |
| Environment risk assessment (self-reported) | 3 |
| Environment risk assessment (home survey) | 2 |
| Structured interview | 1 |
| Data registry system | 1 |
| Outcomes | |
| Burn prevention knowledge | 13 |
| Burns incidence | 13 |
| Burn first aid knowledge | 5 |
| Environment risk assessment | 5 |
| Burn mortality | 1 |
| Cost reduction and satisfaction survey | 1 |
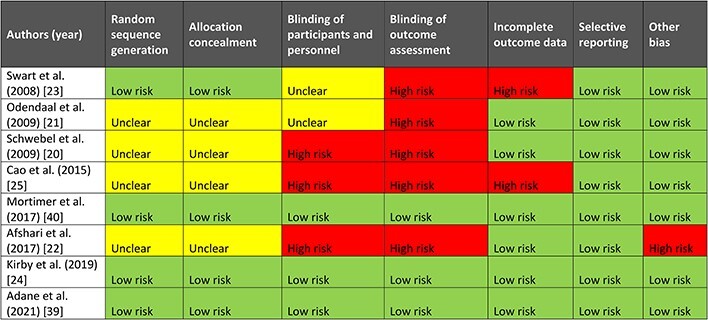
Risk of bias
The risk of bias for the included studies is presented in Tables 8–10, divided according to study design. Due to the heterogeneity of the included studies in terms of intervention, methodologies, population and study design, different tools had to be utilized to analyse the risk of bias across the studies. It was necessary to critique many kinds of study design in contexts where the theoretically optimal study was not practically achievable. We felt that in such instances, the mechanical application of quality criteria was unfair. Adjudicating on RCTs on the basis of the ROB-I tool was relatively straightforward. However, judgement of studies based on other designs has to be more nuanced since they cover topics that impose different constraints. For example, educational interventions in tightly defined populations such as schools pose different issues in terms of blinding/masking and sampling compared to mass media campaigns covering a whole city. We have taken steps to reduce the subjectivity, e.g. by using two authors and adjudication by two senior authors. In general, the studies appear to have many shortcomings, with the quality of studies ranging from moderate to poor but there appears to be a trend of improvement with newer studies.
Table 8.
Summary of risk of bias for pre-post-studies according to the NIH criteria

|
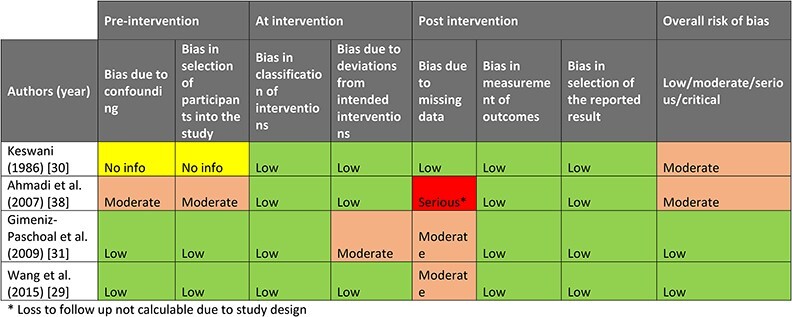
Table 10.
Summary of risk of bias for randomized studies according to the Cochrane ROB-I criteria
|
Table 9.
Summary of risk of bias for non-randomized studies according to the Cochrane ROBINS-I criteria
|
Findings of many school- and community-based education initiatives are compromised as only the success of knowledge acquisition has been reported but not the fidelity of implementation as intended by the study designers. The only study in which the fidelity of implementation was measured was in the study by Schwebel et al. in which a post-intervention survey was conducted to assess the quantity and quality of the safety education provided [20].
A number of issues relating to the quality of the pre-post studies were identified using the NIH criteria [16]. This included the fact that none of the studies performed sample size calculations. In addition, none of the studies stated whether assessors were blinded to the participants’ exposures/interventions, although it is difficult to achieve this with large population interventions.
The quality of the non-randomized studies was generally better than those using a pre-post design. The key concern regarding the quality of these studies was the risk of bias arising from missing end-line data within the post-intervention analyses.
Five of the eight RCTs were cluster trials while three were individual trials (Schwebel et al. [20], Odendaal et al. [21] and Afshari et al. [22]). All three of these individual RCT’s were educational, though Schwebel et al. and Odendaal et al. included elements of enforcement (home inspection hazard checking) and Odendaal et al. included the distribution of safety devices. Adequate randomization methods and allocation concealment were described in only four of eight studies, with none of the individual RCTs achieving this standard. Double-blinding was cited in only three studies. The importance of blinding is arguable in studies where the outcome is objective (e.g. questionnaire scores or burns incidence,) but important where there may be a degree of subjectivity, e.g. home hazard surveys performed by home visitors (e.g. Swart et al. [23], Odendaal et al. [21] and Schwebel et al. [20]). Incomplete outcome data was found in four studies with loss to follow-up (Schwebel et al. [20], Kirby et al. [24], Swart et al. [23] and Cao et al. [25]). In the studies by Schwebel et al., Kirby et al. and Swart et al., the loss to follow-up was small (for Schwebel et al. <15% in both intervention and control groups, for Kirby et al. and Swart et al. <10% in both groups) however the study by Cao et al. had considerable loss to follow-up in the control group (17% in intervention group and 41% in control group) [20,23–25].
Educational initiatives—school-based
Table 1 describes six educational-based initiatives delivered within the school environment. The interventions varied from single modalities such as educational books [26,27] and storytelling [28] to structured multi-modality educational training programmes that combine learning strategies such as lectures, written materials and practical workshops [25,29,30]. Four of the studies aimed to prevent burn injuries alone [26–28,30] and two studies aimed to prevent burns as well as other injuries such as falls and drownings [25,29]. The outcomes measured included knowledge in five studies and the incidence of burns in two studies. As it turned out, the single modality studies [26–28], adopted a pre-post design without contemporaneous controls while the multi-modality training programmes [25,29,30] all used contemporaneous control groups; one of these was a cluster RCT [25]. Five of the six studies used questionnaires to assess children’s knowledge before and after the educational intervention, of which three studies noted significant improvements [25,26,28]. One study found significant improvements in educational outcomes with no associated reduction in injuries overall (they did not report specifically on burn injuries) [25]. The single study that did not include knowledge as an outcome reported a significant reduction in burns incidence in the intervention group [29].
Educational initiatives—community-based
Table 2 describes six educational-based initiatives delivered within the community setting. As with the school-based educational initiatives, half of the included studies used contemporaneous control groups [20,22,31] and the remainder used a pre-post design with no contemporaneous control [32–34]. Three studies directed their interventions at parents with the aim of avoiding child injury [22,31,33], two studies recruited households irrespective of the presence of children [20,32] and one study focused on burns prevention in industrial workers [34]. Five of the studies used knowledge as an outcome measure [20,22,31–33]. This was measured over short follow-up periods, the greatest being 2 months by Afshari et al. [22]. All five studies reported a significant improvement in knowledge-related outcomes. Two of the studies which used knowledge as an outcome also conducted home hazard assessments as an additional measure of burns-related safety practices. They noted significant improvements in burns-related safety practices in the short term [20,33]. Only two of the six studies included burns incidence as an outcome [22,34]. Afshari et al. asked participants to self-report burn injuries and recorded a reduction in burns incidence, although a statistical analysis was not carried out [22]. Sunder and Bharat measured burn rates by observing hospital inpatient and outpatient records over a period of 3 years and found a reduction in burns incidence but again this was not tested statistically [34].
Table 2.
Educational initiatives—community-based
| Year | Authors | Country of origin | Population studied | Actual sample size | Study design | Intervention method | Follow-up time (post-intervention) | Outcome types | Estimated burn incidence (baseline rates/100,000) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| 2019 | Hasibuan et al. [32] | Indonesia (Bandung) | Residents in subdistricts with history of multiple major fires | 61 | Pre-post | One-day community health promotion event: lecture and discussion session (lecture topics: burn prevention in the home, burns incidence, first aid and initial management of burns and burn complications), burn first aid demonstration and discussion session | Unclear | Knowledge of burn prevention and management (measured by pre and post questionnaire) | NA | Significant improvement of knowledge regarding burns prevention and management (pre-test median score = 2, post-test median score = 9, p < 0.001) |
| 2018 | Kahriman et al. [33] | Turkey | Mothers of children aged 0–6 years | 300 mothers | Pre-post | Training of mothers on dangerous situations in the home, posters and brochures. Theoretical training lasted for 16 h, practical training was conducted through a simulation setting, where mothers were asked to identify as many environmental risk factors as possible | Unclear | Knowledge and attitudes towards paediatric injuries including burns (measured by pre and post questionnaire) and environment change (risk assessment form completed by researcher, scoring hazardous situations in the home) | NA | Scores on the identification scale for paediatric injuries increased significantly (p = 0.00). Risk assessment form indicated that there was no significant improvement in overall average score across all paediatric injuries (p = 0.362) but the post intervention burn-specific risk assessment form score was significantly lower (p = 0.00) |
| 2017 | Afshari et al. [22] | Iran (Twiserkan) | Mothers of children <5 years | 72 | Randomized control (individual) | Training programme about the prevention of home-related injuries, formed using the PRECEDE model (Predisposing, Reinforcing & Enabling Constructs in Educational/Ecological Diagnosis & Evaluation). Training manuals were provided, and training consisted of four sessions of 2 weeks and each for 1 hour | 2 months | Knowledge of accidental injury prevention, including burns (measured by pre and post questionnaire) and burns incidence (measured by self-reported pre and post questionnaires) | 5/72 = 6.94%, 6944 per 100 k | Number of burn injuries in intervention group decreased (3 baseline, 1 follow-up) compared to control group (2 baseline, 4 follow-up). Score of knowledge increased statistically significantly in the intervention vs control group |
| 2009 | Schwebel et al. [20] | South Africa | Households in two informal settlement communities—Phillipi and Du Noon | 238 (baseline) 206 (follow-up), intervention = 106, control = 100) | Randomized control (individual) | Intervention: expert trainers trained local professionals to deliver educational materials to the community regarding safe use of kerosene and kerosene-powered appliances | 4 weeks | Knowledge (measured by pre and post questionnaire) and environment change (risk assessment form completed by researcher, scoring kerosene safety in the home) | NA | Significant increase in kerosene-related knowledge in the intervention group compared to the control (p < 0.01) Significant increase in safe kerosene practices in the home and recognition of kerosene injury risk in the intervention group compared to the control group (p < 0.05) |
| 2009 | Gimeniz-Paschoal et al. [31] | Brazil | Families with children <4 years old | 40 relatives of children <four years old | Non-randomized control | Educational talk (30 min), information about the contents of an educational folder about the prevention of childhood burns and a copy of the educational materials | 1 week | Knowledge of burn prevention and management (measured by frequency analysis of interview data) | NA | Prior to the intervention, 62 interview responses on burn risk situations were registered in the intervention group and 60 in the control group. Post-intervention, this increased to 80 and 61 respectively |
| 1998 | Sunder and Bharat [34] | India | Industrial workers at Tata Steel in Jamshedpur, 1993–1996 | 815 patients (142 inpatients, 673 outpatients) with industrial burns treated at a burn centre. The patients were industrial workers at Tata Steel | Pre-post | 75-min audio-visual session for instructors who then distribute safety messages to other employees. Videos were used to highlight burns safety devices, prevention and first aid; annual lectures and discussions were led by instructors; first aid pamphlets and posters were distributed | Incidence first reported in 1993, intervention applied each year from 1994. Incidence rates reported until 1996 | Burns incidence and mortality (measured using hospital records) | Unclear population size | Decline in the incidence of inpatient and outpatient burns admissions after the intervention; no mortality from burns and no burns with >20% total body surface area (TBSA) after the intervention; increase in the number of patients who used water for first aid |
Education–media-based population-level initiatives
Mass media campaigns that utilize multiple media including print (e.g. posters and newspapers), audio, visual media (such as radio and television) and social media have been used commonly in an attempt to influence health related behaviours at a population level. We found four studies describing evaluations of population-level media initiatives (Table 3). In each case a multi-media intervention strategy was used. The interventions were designed to reduce burn injuriesonly.
Table 3.
Education–Media-based population-level initiatives
| Year | Authors | Country of origin | Population studied | Actual sample size | Study design | Intervention method | Follow-up time (post-intervention) | Outcome types | Estimated burn incidence (baseline rates/100,000) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| 2019 | Homaie et al. [36] | Iran (Guilan) | Children and students in Guilan | Not available: population size not reported | Pre-post | Educational materials (pamphlets, posters and banners), radio and television interviews, two media press conferences, 70 educational and preventive messages on social media. The campaign was held between February and March 2016. | 1 year | Burns incidence (measured using a data registry system of a Trauma Research Centre) and incidence of eye, ear and nose injury; injuries were related to a firework event | Unclear population size | Burn injuries reduced from 32 to 10 (68% reduction). Burden of disease (DALY): post-intervention DALY for burn injuries was significantly lower than pre-intervention (p = 0.0460); per injured person, 3.27 years reduction in DALY was reported; mean age of injuries (all injuries) was increased from 27.75 to 32.65 years (but not statistically significant, p = 0.0783); trend in reduction of burn TBSA (21.4 to 17.2, not statistically significant, p = 0.43) but not in incidence of full thickness burns (increased from 62 to 71.4%) |
| 2011 | Sarma [35] | India (Digboi and Guwahati) | Employees and dependents of an oil corporation; high-school students of 14 schools; the populations around Digboi and Guwahati | Oil corporation employees (n = 15,000); population around Digboi and Guwahti (n = ~2 million); high-school students (n = 1240) | Pre-post | Audio-visual aids; annual school programme using audio-visual aids and verbal question and answer sessions/quizzes; articles in house journals/periodicals/newspapers; banners and posters; visits to workers at the refinery; special sessions and a press meet 3 weeks prior to Diwali; books and booklets in local languages; radio and television advertisements | 7 years | Burns incidence (measured using hospital records) | Unclear population size | Reduction of the patients admitted with burns on average per year (p < 0.001); reduction in children (<18 years old) and young adults (19–40 years old) admitted with burn injury (p < 0.001); reduction in 1–20% TBSA (p = 0.007) and 40–60% TBSA (p = 0.048); overall reduction in mean TBSA (p < 0.001); reduction in firecracker burns during Diwali (p < 0.001) |
| 2007 | Ahmadi and Ytterstad [38] | Iran (Gilangharb and Sarpolzahab) | Populations in Gilangharb and Sarpolzahab | Estimated population sizes: Gilangharb 70,000, Sarpolzahab (control) 89,000 | Non-randomized control | Yearly video shown in secondary and high-schools, video clubs and community groups with a booster programme in endemic areas; painting and writing competitions | No post-intervention follow-up: self-immolation burns incidence recorded over 3-year intervention period | Self-immolation burns incidence (measured using hospital records) | Self-immolation attempt rates: Gilangharb: 14.3 per 100 k, Sarpolzahab: 14.9 per 100 k | Self-immolation rates fell by 57% in Gilangharb (not significant) and 27% in Sarpolzahab; Gilangharb all suicide attempt rates were 43% lower than Sarpolzahab (p < 0.001) |
| 1990 | Mohan and Varghese [37] | India (Delhi) | Population of Delhi | Not available: population size not reported | Pre-post | Newspaper articles and advertisements, documentary, television advertisements | No post-intervention follow-up: burns incidence recorded over 2 year intervention period | Burns incidence (measured using hospital records) | Unclear population size | Reduction of burns presenting to two hospitals. Reduction in proportion of burn from ‘anars’, which are highly dangerous fireworks |
DALY Disability adjusted life years, TBSA total body surface area
Three of the four studies [35–37] targeted, either as part of the intervention or as its sole focus, firework-related burns during festivals such as Diwali in India or the Persian firework festival. The remaining study by Ahmadi et al. targeted self-immolation in young women [38]. A combination of interventions were utilised in the studies including printed media such as newspapers, visual media such as banners and posters and audio-visual media such as radio and television in order to reach as wide as an audience as possible with the more recent study by Homaie et al. also utilising social media [36]. In general, these studies showed a positive association between mass media interventions and cause specific burn incidences (e.g. self-immolation rates fell by 57% in the study by Ahmadi and Ytterstad [38]). The study by Homaie et al. was also unique in that it modelled the change in DALY due to the interventions and found a significant reduction of 3.27 years in DALY (p = 0.0460) [36]. The four included studies had variable intervention periods ranging from 1 to 7 years. In terms of follow-up periods, again this was variable, with one study [35] having a follow-up period of 7 years whereas others had a short follow-up period (1 year). One study did not carry out follow-up beyond the 3 year intervention period [38]. Sarma suggests that longer periods of intervention result in better knowledge retention, however as there was no year-by-year analysis in that study this suggestion was not confirmed empirically [35].
Environmental initiatives
Table 4 describes four studies that evaluated modifications to the home environment, such as improved cookstoves and better ambient lighting to reduce household burn injuries. We found three studies of improved cookstoves [24,39,40] where the primary aim of the study was to reduce rates of lower respiratory tract infections and where burns incidence was a secondary outcome. The success of these interventions was variable: Kirby et al. reported a drop in burn injures (3.6 to 1.8%, p < 0.001) [24] which was not replicated in the other two studies [39,40]. Although educational campaigns were used as part of the intervention, they were focused on promoting use of the improved cookstoves rather than burn prevention. Chamania et al. however replaced traditional biomass (kerosene) lamps with non-biomass alternatives (LED or solar lamps) and reported no lamp-related burns in the subsequent 6-month follow-up period compared to 23 burns in the preceding 5 years [41].
Table 4.
Environmental initiatives
| Year | Authors | Country of origin | Population studied | Actual sample size | Study design | Intervention method | Follow-up time (post-intervention) | Outcome types | Estimated burn incidence (baseline rates/100,000) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| 2021 | Adane et al. [39] | Ethiopia | Children<5 | 5508 (baseline) 5333 (follow-up). 50 clusters per trial arm, (Average cluster size: intervention = 53.18, control = 53.48) | Randomized control (cluster) | Replacement of open burning traditional baking stoves with biomass-fuelled improved baking stoves (1-year long intervention) | Every 3 months for 1 year | Cooking-related burn incidence (self-reported by participants), acute lower respiratory tract infections | Baseline rates not recorded. Estimated incidence calculated using post-intervention rates = 92/5333 = 1.73%, 1730 per 100 k | No difference in incidence rates of cooking-related burn events between the intervention (41 events) and control groups (51 events); IRR 0.80 (95% CI: 0.53–1.21) |
| 2019 | Kirby et al. [24] | Rwanda | Children<5 | 2440 children from 1582 households; 87 clusters per trial arm | Randomized control (cluster) | Distribution of a tabletop gravity-based household water filter and portable high-efficient wood-burning cookstove, community and household education and behaviour change messages | 3 follow-up visits at 4-month intervals | Burn prevalence (self-reported by participants), acute respiratory infections, diarrhoeal illness, pneumonia | Baseline rates not recorded. Estimated incidence calculated using post-intervention rates = 163/5940 = 2.74%, 2744 per 100 k | Prevalence of reported burns within the previous 2 months was lower in the intervention (1.8%) compared to control (3.6%) (PR 0.51, 95% CI 0.36–0.74, p < 0.001) |
| 2017 | Mortimer et al. [40] | Malawi | Children<4.5 years | 10,750 (baseline) 10,543 (follow-up) 75 clusters per trial arm (average cluster size: intervention = 70.01, control = 74.57) | Randomized control (cluster) | Biomass burning cookstove- households received two biomass-fuelled cookstoves and a solar panel to charge the battery for the stove fan and user training | 3-month follow-ups for 2 years | Cooking-related burn incidence (self-reported by participants), pneumonia incidence | Baseline rates not recorded. Estimated incidence calculated using post-intervention rates = 508/10,543 = 4.82%, 4818 per 100 k | No difference in the incidence rates of serious adverse events between intervention and control. 19 of the adverse events were cooking-related burns (9 in the intervention, 10 in the control, IRR 0.91 (95% CI 0·37–2·23); p = 0·83. 1505 non-serious burns were reported (549 in the intervention, 956 in the control, IRR 0.58 (95% CI 0·51–0·65); p < 0·0001 |
| 2015 | Chamania et al. [41] | India (Madhya Pradesh) | Households in 18 villages within the Malwa region of Madhya Pradesh | 1042 households | Pre-post | Removal of kerosene lamps in participants homes, replacement with LED or solar lamps | 6 months | Self-reported burns proportions (measured by self-reported pre and post questionnaires), satisfaction of villagers, reduction of the annual cost for household illumination | 23/1042 = 2.21%, 2207 per 100 k | No lamp-related burns reported in 6 months of follow-up (compared to 23 burns in preceding 5 years before intervention). Decreases in cost of illumination; satisfaction of users |
IRR incidence rate ratio, CI confidence interval, PR prevalence rate
Mixed educational and environmental initiatives
Table 5 describes four studies that used a mixture of educational and environmental initiatives to prevent burns. These studies differ from the environmental studies described above in that they included an educational component in addition to the environmental modification. Two studies used educational programmes including face-to-face teaching sessions and film [42,43] whilst the other two used home visits [21,23]. Environmental interventions in the four studies included distribution of safety devices such as fire blankets, barriers and child-proof locks or paraffin safety cups. All but one of the four studies (Jetten et al. [43]) measured only change in knowledge but not actual change in burn incidences. Follow-up post-intervention was short for all studies ranging from 1 week to 17 months. Duration of follow-up is important because effects might not be sustained; the study with the longest follow up showed that only 65.5% of participants were still using the fire safety devices they were supplied with at 17 months [42]. All four studies showed improvement in their measured outcomes of burn prevention knowledge, use of safety devices and burn incidences, though this was not always related to the use of the safety devices. For example, in the study by Swart et al., paraffin safety cups and child-proof locks were provided, however the study showed no significant improvement using paraffin [p = 0.911, 95% confidence interval (CI) −0.64 to −0.57] or electrical safety practices (p = 0.294, 95% CI −0.54 to 0.16) [23].
Discussion
Overview
This scoping systematic review was conducted to identify literature on burns prevention strategies in LMIC. We updated and extended the systematic review published by Rybarczyk et al. in 2016 [7]. We have presented the results of 24 studies describing educational, environmental and mixed-methods initiatives, conducted across 11 LMIC between 1986 and 2020.
Methodology
Half of our 24 studies were before and after designs from which causal inferences cannot be made directly. That said, it is difficult to establish controlled trials for certain types of intervention such as mass media campaigns. One of the many sources of confounding in such studies is temporal effects generally and the phenomenon of regression to the mean in particular. The latter problem arises when an intervention is a response to a sudden, and potentially random, spike in events. Such an example may have explained the dramatic reductions in fire incidence and related fatalities observed in the Oklahoma fire alarm study [8]. One way to mitigate the risk of over-interpreting a temporal trend as an intervention effect is to conduct a time series analysis. Only two of the 12 before and after studies took this form [28,42].
Most educational interventions used knowledge alone as an outcome whereas this is a necessary, but not sufficient, condition for reduced burns incidence [44,45]. Knowledge tests were often conducted immediately following completion of the educational intervention, omitting assessment of long-term knowledge retention.
There is a clear lack of evidence in the included studies on the sustained effect of the interventions used. None of the studies included an explicit definition of sustainability, although some studies have acknowledged their lack of evidence of the sustainability of their interventions and the importance of measuring this in future studies [21,24]. Most of the follow-up periods of studies were too short to gauge whether reductions in burn incidence were sustained (≤1 month) [20,21,23,31] and some studies did not even mention the duration of follow-up [30,32,33]. The longest follow-up period was 7 years in the study by Sarma [35] and even in this study the analysis was done using pre- (6 years) and post- (7 years) intervention blocks and there was a lack of year by year analysis of sustained effect of the interventions. Though not explicably stated, the lack of investigation of the facilitating and hindering factors of the interventions and of long-term follow-up in these studies are likely due to limitations of staff and funding.
Studies with contemporaneous controls also had several limitations. Some do not focus on burns but consider injury prevention as a whole [22,25,29], and for those reporting burns incidence, some do not provide information regarding the severity of recorded burns [22,29].
Intervention types studied
Of the 24 identified studies, 16 aim to reduce burn injury by providing education rather than by environmental modifications, such as substituting liquefied petroleum gas and kerosene for safer alternatives, improving electrical safety systems and enforcing workplace safety [46,47]. The majority of the educational interventions showed that knowledge was improved, at least in the short-term; sustainability and effects on burn rates were inadequately studied as mentioned above. Our review identified only four studies with a sole focus on environmental change and a further four where environmental change was combined with an educational intervention [24,39–41]. Despite not being the primary outcome, two of the three improved cookstove studies reported significant reductions in burns incidence [24,40]. Replacement of the kerosene lamps also yielded a reduction in self-reported proportions of burns; however, this was not statistically assessed [41].
The identified need for evaluation of environmental change interventions
Across many hazards to which humans are exposed, passive interventions that rely on product modification, environmental redesign or control and legislation are more effective than active measures, such as education [6]. Application of environmental initiatives at the population level has been successfully demonstrated in high-income countries. A key example is the widespread introduction and use of smoke detectors and alarms in the USA, with 96% of households reporting that they had a smoke alarm installed by 1993. Death rates from fires reduced by almost 50% between 1981 and 1997 and it is likely that at least some of this improvement was caused by fire alarms [48].
We identified two non-published studies that demonstrate the potential successes of environmental-based initiatives; specifically, the replacement and modification of household cookstoves. The first was a quasi-experimental study conducted in Madagascar in 2011 [49]. The authors noted a significant reduction in burn injuries following the use of ethanol and improved wood stoves compared to their control. The second study took place in Guatemala between 1992 and 1994 [50]. Researchers noted a reduction in burns incidence following the use of improved wood stoves when compared to the use of open stoves, though this was not statistically significant.
There is thus a need for greater emphasis on research into the effectiveness of engineering and environmental modification on burns incidences in LMIC [49–50]. However, it is often easier for researchers to implement and evaluate a community behaviour change intervention than an intervention to enforce regulation or introduce environmental modifications. The solution we propose is collaboration between policy makers and researchers, so that new interventions can be evaluated prospectively. This may provide opportunity for concurrent legislative changes, which have maximized uptake of burns prevention initiatives in HIC [48].
We cite as an example a report published by researchers from the University of Stellenbosch who conducted a pilot project assessing the impact of smoke alarm installation across informal settlements in Cape Town. Authors noted that their collaborative efforts with fire services, local leaders and community members, significantly contributed towards community uptake and resultant improvements in fire protection. Unfortunately the cost of this project was not reported, leaving doubts about the scalability of widespread application of this programme [51]. Future projects should attempt to calculate the intervention costs and offset these against potential savings in terms of health costs, and productivity and health benefit.
Supporting the implementation of environmental interventions
Co-existing educational programmes can improve the application of environmental initiatives [52]. Education can elicit behaviour change, which is beneficial for implementation of user-dependent interventions [53]. For example, it has been suggested that improved education regarding maintenance of smoke detectors and responding to smoke alarms can improve the efficacy of these systems [48,54]. The association between education and behaviour change was explored by two studies included in this review, which noted significant improvements in burns-related safety practices because of educational programmes [21,23].
The media and population-level educational studies described within this review demonstrated that the use of multi-media intervention strategies can be successful when targeting large populations. This has been shown in other non-burn studies that demonstrated greater success where multiple different interventions are used [55] or if policies are designed to motivate behaviour change [56].
Assessing the impact of proposed interventions
Determining causal relations between intervention and effect can be challenging when non-burn specific outcome measures, such as knowledge, are used. We reinforce the recommendation made by Rybarczyk et al. to use burn-specific outcome measures such as burns incidence. Mortality is a rare outcome across a population, and morbidity changes may also fail to reveal the massive quality of life impact of severe burns which are easily lost in the noise at the level of the population at which preventative efforts are inevitably applied [7].
To collect data on burns incidence, self-report questionnaires can be used to record burns acquired over specified time periods. This method can capture self-treated or community managed burns, which may not appear on clinical databases. It also enables data collection in areas where hospital resources may be poor or inaccessible. However, recall bias may dilute effect, especially for the most common small burns. WHO guidance suggests allowing a recall period of up to 3 months for minor injuries and 12 months for more severe injuries [57]. This guidance may be applied in future studies to minimize discrepancies in self-reporteddata.
Population-based interventions may use burn registries based on hospital data to capture incidence over longer periods [58]. The Global Burn Registry provides a standardized template to record the cause of burns and severity measures such as total body surface area, which can be used to estimate burden of disease [36]. However, hospital databases even if complete only capture severe burns. In LMIC large proportions of the population have poor access to formal medical care and may be cared for outside of tertiary centres [59–62] and it is therefore difficult to collect incidences of smaller burns that do not result in referral to major centres.
Limitations
Limitations of this systematic review include our inclusion and exclusion criteria; it is possible that potentially informative qualitative or informal studies may have been excluded. We did not have access to the search strings used by Rybarcyck et al. and therefore we cannot be certain that our search strategy was an exact replica. Other preventative studies or systematic reviews, where burns-related outcomes were not a key focus, may have been missed during screening. Despite some examples being provided in the discussion, due to resource limitations we were unable to complete a comprehensive search for burn prevention studies within the grey literature. Furthermore, exclusion of non-English language studies limits the breadth of literature included in this review.
Conclusions
This review synthesises and provides an update on the status of burns prevention interventions in LMIC. Through our updated review, we have identified several environmental initiatives where burns were recorded as a secondary outcome. We also identified one large-scale population-based study that demonstrated reductions in burns incidence and burden of disease. However, most studies were still restricted to small-scale educational initiatives and lacking in long-term follow-up and clear outcomes to suggest an impact on burns morbidity and mortality. Across all studies included in this review, there is still little focus on legislative or environmental interventions that target the major contributors of burns in LMIC. Population-level, collaborative projects are necessary to drive forward burn prevention through specific environmental interventions and supplementary educational programmes.
Abbreviations
CI: Confidence interval; DALY: disability adjusted life years; HIC: high-income countries; IRR: Incidence Rate Ratio; LMIC: low- and middle-income countries; LPG: Liquid Petroleum Gas; NIH: National Institutes of Health; OR: Odds Ratio; PR: Prevalence rate; RCT: randomized control trial; ROB-I: Risk of Bias I; TBSA: Total Body Surface Area.
Acknowledgements
RL is Director of National Institute for Health Research (NIHR) Applied Research Centre West Midlands (ARC WM), United Kingdom.
NM is Director of the ScarFree Foundation Burns Research centre, Birmingham, United Kingdom.
Conflict of interest
None declared.
Supplementary Material
Contributor Information
Kate Price, College of Medical and Dental Sciences, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK.
Kwang Chear Lee, University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Hospital Birmingham, Mindelsohn Way, Edgbaston, Birmingham, B15 2WB, UK.
Katherine E Woolley, Institute of Applied Health Research, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK.
Henry Falk, Adjunct Professor of Environmental Health, Emory University, Rollins School of Public Health, Atlanta, GA 30322, US.
Michael Peck, Clinical Professor of Surgery, University of Arizona College of Medicine, Phoenix, AZ 85004, US.
Richard Lilford, Institute of Applied Health Research, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK.
Naiem Moiemen, College of Medical and Dental Sciences, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK; University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Hospital Birmingham, Mindelsohn Way, Edgbaston, Birmingham, B15 2WB, UK.
References
- 1. James SL, Lucchesi LR, Bisignano C, Castle CD, Dingels ZV, Fox JT, et al. Epidemiology of injuries from fire, heat and hot substances: global, regional and national morbidity and mortality estimates from the Global Burden of Disease 2017 study. Inj Prev. 2020;26:i36–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. WHO . Burns: key facts 2018updated 06/03/2018. Available from: https://www.who.int/news-room/fact-sheets/detail/burns.
- 3. Kelter BM, Holavanahalli R, Suman OE, Ryan CM, Schneider JC. Recognizing the long-term sequelae of burns as a chronic medical condition. Burns. 2020;46:493–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Entec UK Limited . Department for Communities and Local Government. The economic cost of fire: estimates for 2006 Fire Research Report 2/2011 2011. DCLG, London, UK. [Cited 2020 01 Feb]. Available at:https://webarchive.nationalarchives.gov.uk/20121105004857/http:/www.communities.gov.uk/documents/corporate/pdf/1838274.pdf. [Google Scholar]
- 5. Sanchez JL, Bastida JL, Martínez MM, Moreno JM, Chamorro JJ. Socio-economic cost and health-related quality of life of burn victims in Spain. Burns. 2008;34:975–81. [DOI] [PubMed] [Google Scholar]
- 6. Linares AZ, Linares HA. Burn prevention: the need for a comprehensive approach. Burns. 1990;16:281–5. [DOI] [PubMed] [Google Scholar]
- 7. Rybarczyk MM, Schafer JM, Elm CM, Sarvepalli S, Vaswani PA, Balhara KS, et al. Prevention of burn injuries in low- and middle-income countries: a systematic review. Burns. 2016;42:1183–92. [DOI] [PubMed] [Google Scholar]
- 8. Haddix AC, Mallonee S, Waxweiler R, Douglas MR. Cost effectiveness analysis of a smoke alarm giveaway program in Oklahoma City. Oklahoma. Inj Prev. 2001;7:276–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Reason J. Human error: models and management. BMJ (Clinical research ed). 2000;320:768–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Erdmann TC, Feldman KW, Rivara FP, Heimbach DM, Wall HA. Tap water burn prevention: the effect of legislation. Pediatrics. 1991;88:572–7. [PubMed] [Google Scholar]
- 11. Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Implementation. 2020;18:2119–26. [DOI] [PubMed] [Google Scholar]
- 12. World Bank . Classification of Countries 2021. [cited 2021 Jan 31]. Available from:https://datahelpdesk.worldbank.org/knowledgebase/articles/906519.
- 13. Woolley KE, Dickinson-Craig E, Bartington SE, Oludotun T, Kirenga B, Mariga ST, et al. Effectiveness of interventions to reduce household air pollution from solid biomass fuels and improve maternal and child health outcomes in l low- and middle-income countries: a systematic review protocol. BMC Systematic reviews. 2021;10:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Tupetz A, Friedman K, Zhao D, Liao H, Isenburg MV, Keating EM, et al. Prevention of childhood unintentional injuries in low- and middle-income countries: a systematic review. PLoS One. 2020;15:e0243464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Steckler A, Linnan L, Israel B. Process evaluation for public health interventions and research. San Francisco, California: Jossey-Bass, 2002. [Google Scholar]
- 16. NIH . Study Quality Assessment Tools 2020. [cited 2021 Feb 01]. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality- assessment- tools.
- 17. Sterne JAC, Hernán MA, Mcaleenan A, Reeves BC, Higgins JPT. Chapter 25: Assessing risk of bias in a non-randomized study. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane handbook for systematic reviews of interventions version 6.1 (updated September 2020). Chichester (UK): John Wiley & Sons, Cochrane 2020 [cited 2021 Feb 01]. Available from:www.training.cochrane.org/handbook.
- 18. Higgins JPT SJ, Page MJ, Elbers RG, Sterne JAC. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane handbook for systematic reviews of interventions version 6.1 (updated September 2020). Chichester (UK): John Wiley & Sons, 2020[cited 2021 Feb 01]. Available from:www.training.cochrane.org/handbook.
- 19. Kai-Yang L, Zhao-Fan X, Luo-Man Z, Yi-Tao J, Tao T, Wei W, et al. Epidemiology of pediatric burns requiring hospitalization in China: a literature review of retrospective studies. Pediatrics. 2008;122:132–42. [DOI] [PubMed] [Google Scholar]
- 20. Schwebel DC, Swart D, Simpson J, Hobe P, Hui SK. An intervention to reduce kerosene-related burns and poisonings in low-income south African communities. Health Psychol. 2009;28:493–500. [DOI] [PubMed] [Google Scholar]
- 21. Odendaal W, Niekerk A, Jordaan E, Seedat M. The impact of a home visitation programme on household hazards associated with unintentional childhood injuries: a randomised controlled trial. Accid Anal Prev. 2009;41:183–90. [DOI] [PubMed] [Google Scholar]
- 22. Afshari M, Moghimbeigi A, Hazavehei SMM, Rezapur-Shahkolai F. Effect of a model-based educational program for mothers, on home-related injury prevention among under-five- year children in rural Twiserkan. Turk J Pediatr. 2017;59:648–56. [DOI] [PubMed] [Google Scholar]
- 23. Swart L, Niekerk A, Seedat M, Jordaan E. Paraprofessional home visitation program to prevent childhood unintentional injuries in low-income communities: a cluster randomized controlled trial. Inj Prev. 2008;14:164–9. [DOI] [PubMed] [Google Scholar]
- 24. Kirby MA, Nagel CL, Rosa G, Zambrano LD, Musafiri S, Nagirabega JD, et al. Effects of a large-scale distribution of water filters and natural draft rocket-style cookstoves on diarrhea and acute respiratory infection: a cluster-randomized controlled trial in Western Province. Rwanda. PLoS Med. 2019;16:e1002812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Cao BL, Shi XQ, Qi YH, Hui Y, Yang HJ, Shi SP, et al. Effect of a multi-level education intervention model on knowledge and attitudes of accidental injuries in rural children in Zunyi, Southwest China. Int J Environ Res Public Health. 2015;12:3903–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Sinha I, Patel A, Kim FS, Maccorkle ML, Watkins JF. Comic books can educate children about burn safety in developing countries. J Burn Care Res. 2011;32:e112–7. [DOI] [PubMed] [Google Scholar]
- 27. Heard JP, Latenser BA, Liao J. Burn prevention in Zambia: a work in progress. J Burn Care Res. 2013;34:598–606. [DOI] [PubMed] [Google Scholar]
- 28. Bagheri T, Fatemi MJ, Saberi M, Rahbar A, Momeni M. The effect of education on primary school Students’ knowledge regarding Burn prevention measures and actions to take. J Burn Care Res. 2021;42:220–7. [DOI] [PubMed] [Google Scholar]
- 29. Wang H, Liu YX, Deng WJ, Yang WJ, Wang F. Case-control study of injury intervention for preschool children in Henggang. Pediatr Emerg Care. 2015;31:708–10. [DOI] [PubMed] [Google Scholar]
- 30. Keswani MH. The prevention of burning injury. Burns Incl Therm Inj. 1986;12:533–9. [DOI] [PubMed] [Google Scholar]
- 31. Gimeniz-Paschoal SR, Pereira DM, Nascimento EN. Efect of an educative action on relatives’ knowledge about childhood burns at home. Rev Lat Am Enfermagem. 2009;17:341–6. [DOI] [PubMed] [Google Scholar]
- 32. Hasibuan L, Soedjana H, Hilmanto D, Tarawan V, Muliawan B, Lubis PHA. Knowledge improvement on Burn injury prevention and first management after one-Day health promotion event. Majalah Kedokteran Bandung. 2019;51:233–9. [Google Scholar]
- 33. Kahriman IL, Karadeniz H. Effects of a safety-awareness-promoting program targeting mothers of children aged 0-6 years to prevent Pediatric injuries in the home environment: implications for nurses. J Trauma Nurs. 2018;25:327–35. [DOI] [PubMed] [Google Scholar]
- 34. Sunder S, Bharat R. Industrial burns in Jamshedpur, India: epidemiology, prevention and first aid. Burns. 1998;24:444–7. [DOI] [PubMed] [Google Scholar]
- 35. Sarma BP. Prevention of burns: 13 years’ experience in North- eastern India. Burns. 2011;37:265–72. [DOI] [PubMed] [Google Scholar]
- 36. Homaie Rad E, Kouchakinezhad-Eramsadati L, Mohtsham-Amiri Z, Davoudi-Kiakalayeh A, Yousefzadeh-Chabok S. Effec- tiveness of an educational program on decreasing burns and injuries in Persian festival of fire: a burden of diseases approach. Burns. 2019;45:466–70. [DOI] [PubMed] [Google Scholar]
- 37. Mohan D, Varghese M. Fireworks cast a shadow on India’s festival of lights. World Health Forum. 1990;11:323–6. [PubMed] [Google Scholar]
- 38. Ahmadi A, Ytterstad B. Prevention of self-immolation by community-based intervention. Burns. 2007;33:1032–40. [DOI] [PubMed] [Google Scholar]
- 39. Adane MM, Alene GD, Mereta ST, Wanyonyi KL. Effect of improved Cookstove intervention on childhood acute lower respiratory infection in Northwest Ethiopia: cluster randomized controlled trial. BMC Pediatr. 2021;21:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Mortimer K, Ndamala CB, Naunje AW, Malava J, Katundu C, Weston W, et al. A cleaner burning biomass-fuelled cookstove intervention to prevent pneumonia in children under 5 years old in rural Malawi (the cooking and pneumonia study): a cluster randomised controlled trial. The Lancet. 2017;389:167–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Chamania S, Chouhan R, Awasthi A, Bendell R, Marsden N, Gibson J, et al. Pilot project in rural western Madhya Pradesh, India, to assess the feasibility of using LED and solar-powered lanterns to remove kerosene lamps and related hazards from homes. Burns. 2015;41:595–603. [DOI] [PubMed] [Google Scholar]
- 42. Chan EYY, Lam HCY, Chung PPW, Huang Z, Yung TKC, Ling KWK, et al. Risk perception and knowledge in fire risk reduction in a dong minority Rural Village in China: a health-EDRM education intervention study. Int J Disaster Risk Sci. 2018;9:306–18. [Google Scholar]
- 43. Jetten P, Chamania S, Tulder M. Evaluation of a community- based prevention program for domestic burns of young children in India. Burns. 2011;37:139–44. [DOI] [PubMed] [Google Scholar]
- 44. Rosenstock IM. The health belief model and preventive health behavior. Health Educ Monogr. 1974;2:354–86. [Google Scholar]
- 45. Becker MH. The health belief model and sick role behavior. Health Educ Monogr. 1974;2:409–19. [Google Scholar]
- 46. Ahmed T. Prevention oriented burns epidemiology: the first hospital based study from Bangladesh. J Am Coll Surg. 2016;223:e163. [Google Scholar]
- 47. Dhopte A, Tiwari VK, Patel P, Bamal R. Epidemiology of pediatric burns and future prevention strategies-a study of 475 patients from a high-volume burn center in North India. Burns & Trauma. 2017;5:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Peck MD. Structure fires, smoke production, and smoke alarms. J Burn Care Res. 2011;32:511–8. [DOI] [PubMed] [Google Scholar]
- 49. Consulting P. Ethanol as a household fuel in Madagascar: Helath benefits, economic assessment and review of African lessons for scaling up. Component A- Analysis of household air pollution interventions in Madagascar. 2011. [Google Scholar]
- 50. Dherani M, Pope D, Bruce N. Impact of an improved cookstove on burns in children: findings from the RESPIRE Guatemala Study, 2012.
- 51. Zweig P, Pharoah R, Eksteeen R, Walls R. Installation of smoke alarms in an informal settlement community in Cape Town. South Africa. 2018.
- 52. Mock C, Peck M, Juillard C, Meddings D, Gielen A. L M. Burn Prevention: Success Stories and Lessons Learned. Geneva: World Health Organization, 2011. [Google Scholar]
- 53. Green LW, Kreuter MW. Health Promotion Planning: An Educational and Environmental Approach. Mountain View, CA: Mayfield Publishing Company, 1991. [Google Scholar]
- 54. Runyan CW, Johnson RM, Yang J, Waller AE, Perkis D, Mar-shall SW, et al. Risk and protective factors for fires, burns, and carbon monoxide poisoning in U.S. households. Am J Prev Med. 2005;28:102–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Kotler PGA. Principles of Marketing. 13. Upper Saddle River, NJ: Prentice Hall, 2009. [Google Scholar]
- 56. Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet. 2010;376:1261–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Sethi D, Habibula S, McGee K, Peden M, Bennett S, Hyder A, et al. Guidelines for Conducting Community Surveys on Injuries and Violence. Geneva: World Health Organization, 2004. [DOI] [PubMed] [Google Scholar]
- 58. Peck M, Falk H, Meddings D, Sugerman D, Mehta S, Sage M. The design and evaluation of a system for improved surveillance and prevention programmes in resource-limited settings using a hospital-based burn injury questionnaire. Inj Prev. 2016;22:i56–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Atiyeh B, Masellis A, Conte C. Optimizing Burn treatment in developing low-and middle-income countries with limited health care resources (part 2). Ann Burns Fire Disasters. 2009;22:189–95. [PMC free article] [PubMed] [Google Scholar]
- 60. Atiyeh B, Masellis A, Conte F. Optimizing Burn treatment in developing low-and middle-income countries with limited health care resources (part 3). Ann Burns Fire Disasters. 2010;23:13–8. [PMC free article] [PubMed] [Google Scholar]
- 61. Peck MD. Epidemiology of burns throughout the world. Part I: distribution and risk factors. Burns. 2011;37:1087–100. [DOI] [PubMed] [Google Scholar]
- 62. Stokes MAR, Johnson WD. Burns in the third world: an unmet need. Ann Burns Fire Disasters. 2017;30:243–6. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.