

OP01: Surgical Complications 1
1176
A001: The PAD (Post-operative Airway Distress) Score - First Steps to Develop a Post-Surgery Tool for the Assessment of Upper Airway-Related Complications Following Anterior Cervical Spina Surgery
Alexander von Glinski 1,2,3 , Christopher Elias 1 , Basem Ishak 1,2,4 , Sven Frieler , 3 , Ronen Blecher 1 , Clifford Pierre 1,2 , Jospeh Detorri 5 , Steven Deem 6 , Blake Golden 7 , Thomas Schildhauer 3 , Rod Oskouian 1 , and Jens Chapman 1
1 Swedish Neuroscience Institute, Swedish Medical Center, Seattle, Seattle, USA
2 Seattle Science Foundation, Swedish Medical Center, Seattle, Seattle, USA
3 BG University Hospital Bergmannsheil, Ruhr University Bochum, Department of General and Trauma Surgery, Seattle, USA
4 Heidelberg University Hospital, Department of Neurosurgery, Heidelberg, Germany
5 Spectrum Research, Inc., Steilacoom, Steilacoom, USA
6 Neurocritical Care, Swedish Neuroscience Institute, Swedish Medical Center, Seattle, Seattle, USA
7 Division of Head and Neck Surgery, Swedish Cancer Institute, Seattle, USA
Background Context: Anterior cervical discectomy and fusion (ACDF) is a commonly performed cervical spine surgery. While the complication profile is relatively low, a rare and potentially catastrophic complication is acute upper respiratory tract compromise secondary to mass effects created by post-operative hematoma, infection, angiodema, cerebrospinal fluid leaks, and dislodged grafts or hardware. We defined such events as post-operative airway distress (PAD). The aim of this present study was to develop a post-operative airway distress score to identify patients at risk for acute PAD. Materials and Methods: This is an expert consensus (modified Delphi process) and retrospective analysis, single-institution clinical study. All adult patients who received elective anterior cervical discectomy and fusion for degenerative spine disorders (1,466 patients) at a single institution between July 1, 2014 and May 31, 2019 were studied. Outcome Measures: Acute upper airway compromise during hospitalization from primary ACDF operation due to an identifiable structural cause related to surgery requiring readmission to intensive care unit, reintubation, or revision surgery. A list of potential risk factors for acute PAD was created based on our comprehensive literature review and supplemented through a modified Delphi process by a multidisciplinary expert panel. We identified patients with acute respiratory distress affecting the upper airways from the total sample who met inclusion criteria. All non-surgical site related causes were excluded creating our acute PAD-Group. To establish a comparison group for validation of our score we selected patients without acute respiratory failure by a randomized selection process (Non-PAD group). Ultimately, we compared presence or absence of our previously selected risk factors for our PAD and No-PAD group using bivariate analysis retaining factors that showed a P-value ≤ .20. Results: We identified 18 potential risk factors from our Delphi process, of which 9 factors demonstrated a significant association with airway compromise: age >65 years, current smoking status, ASA >2, BMI <18.9 or >25.0, history of a bleeding disorder, intra-operative blood loss >300 ml, surgery including the upper cervical spine (C4 or above), multilevel (≥3 levels) or corpectomy, and duration of surgery >179 min. These nine factors formed the PAD-Score (PADS) which had a range of scores from 0 to 9 giving one point to each factor suggesting a cutoff score of 6 for PADS to balance sensitivity (90.0%) and specificity (90.6%). The mean PADS score comparing those with and without post-operative airway distress was 6.6 ± 1.2 vs 3.0 ± 2.1, respectively (P = .000). Conclusions: Based on our findings, we introduce a tool termed the acute Post-operative Airway Distress Scoring system (PADS) to help identify postoperative patients at risk for heightened awareness towards intensive care admission, reintubation and urgent revision surgery as a result of upper airway compromise caused by surgical site abnormalities.
942
A002: Analysis of Effectiveness of Gelatin Sponge Preperfusion in Vertebral Augmentation: Is It Conductive to Preventing Bone Cement Leakage?
Baoliang Zhang 1 , Zhongqiang Chen 1 , and Guanghui Chen 1
1 Peking University Third Hospital, Beijing, China
Introduction: Bone cement leakage is considered as the most common complication of vertebral augmentation. Emerging researches have reported the application of gelatin sponge for preventing cement leakage, but those results showed inconsistency. Thus, we conducted a meta-analysis to determine whether gelatin sponge preperfusion could effectively reduce the cement leakage rate in the treatment of osteoporotic vertebral compression fractures. Material and Methods: Pubmed, Embase, Cochrane Library, Web of Science, CNKI and Wanfang databases were searched for clinical comparative studies on the effectiveness of vertebral augmentation with or without gelatin sponge preperfusion for thoracolumbar compression fractures. The search time was from inception to August 2020. According to the preestablished criteria, two investigators independently screened the eligible literature, evaluated the methodological quality and extracted the data. The Japanese Orthopaedic Association scores (JOA), Oswestry Disability Index (ODI), visual analogue scale (VAS), anterior height of injured vertebra, Cobb angle and cement leakage rate were compared. Meta-analysis and subgroup analysis were performed by Stata 14. Results: Twelve eligible studies involving 1023 patients were included, including 503 patients in the gelatin sponge group (GS group) and 520 in the conventional surgery group (CS group). Pooled analysis found that there was no difference in postoperative JOA [SMD = .20, 95% CI (-.85, 1.26), P = .707] and ODI at the final follow-up [SMD = .38, 95% CI (-.47, 1.24), P = .381]; Gs group was associated with better improvement of postoperative VAS [SMD = .19, 95% CI (.06, .32), P = .004], but no difference in long-term VAS improvement was observed between two groups[SMD = .10, 95% CI (-.06, 1.26), P = .229]; Regrading radiological outcomes, GS group presented better correction of Cobb angle [SMD = .26, 95% CI (.10, .42), P = .002] while two groups showed similar effectiveness in restoration of the height of injured vertebra [SMD = .04, 95% CI (-.10, .18), P = .579]; Importantly, lower cement leakage rate occurred in GS group than CS group [OR = .41, 95% CI (.29, .59), P = .0001], while the rate of vertebral refracture was similar between the two groups [SMD = .80, 95% CI (.34, 1.88),P = .579]. In addition, there was no significant difference in operation time [SMD = .16, 95% CI (-.23, .55), P = .415] and cement injection volume [SMD = -.1, 95% CI (-.17, .15), P = .884] between the two groups. When stratified by surgical procedures (PKP or PVP), most results were consistent with the aforementioned overall findings, except for no difference in postoperative VAS improvement of patients undergoing PKP and in postoperative Cobb angle recovery of those undergoing PVP. Conclusion: Application of gelatin sponge preperfusion could effectively reduce the rate of cement leakage in vertebral augmentation (PVP and PKP) as well as relieve the early postoperative pain and correct the spinal kyphosis. The operation time, bone cement injection volume, postoperative vertebral height and long-term clinical efficacy were equivalent to those of conventional surgery. Large-sample, multicenter, high-quality randomized controlled trials should be performed to further confirm this conclusion in future.
526
A003: The Use of Table Mounted Retraction Does Not Lead to Higher Incidence of Postoperative Dysphagia After Anterior Cervical Spine Surgery
Athan Zavras 1 , Ali Piracha 1 , Zakariah Siyaji 1 , Talha Qadri 1 , Arash Sayari 1 , Nicholas Shepard 1 , Daniel Caicedo 1 , Mubashir Ahmed 1 , Joana Dhivra 1 , and Matthew Colman 1
1 Rush University Medical Center, Orthopedic Surgery, Chicago, USA
Introduction: Anterior cervical spine surgeries (ACSS), including anterior cervical discectomy and fusion (ACDF), total disc replacement (TDR), and corpectomy, are commonly performedproceduresfor the treatment of numerous pathologies of the cervical spine. Retraction of prevertebral cervical structures is necessary for an anterior approach to the cervical spine, resulting in increased pressure along the pharyngeal and esophageal tissue and potentially leading to dysphagia and damage of local neurovascular structures. Modes of retraction commonly used include non-fixed self-retaining retraction devices or fixed table-mounted retractor arms. However, many surgeons opt against using table-mounted retraction because they believe the fixed construct confers poorer control and may lead to a higher incidence of postoperative dysphagia. Given the scarcity of literature to substantiate this opinion, this study is the first to describe postoperative dysphagia rates in patients after ACSS using table-mounted versus self-retaining retraction. Methods: We retrospectively evaluated all patients who underwent ACSS with a single surgeon between the years of 2014 and 2020. Patients with a minimum follow-up of 6 months were stratified into two cohorts depending on the type of retractor used. Patients in the first group underwent ACSS with self-retaining retraction, whereas a table-mounted retractor arm was used for the second group. Patient outcomes were quantified via retrospective collection of patient-reported outcome (PROs) and the Patient-Reported Outcomes Measurement Information System (PROMIS) questionnaires, including the SWAL-QOL survey for dysphagia, Neck Disability Index (NDI), Visual Analog Scale (VAS) Arm, VAS Neck, Short Form 12-Item Health Survey (SF12), and Veteran’s Rand 12-Item Health Survey (VR12). T-test and chi-square for continuous and categorical variables were performed to compare baseline characteristics. Multivariable regression controlled for baseline characteristics and assessed differences in clinical outcomes associated with the procedure methods. The threshold for statistical significance was set toP< .05. Results: A total of 74 (31 female, 43 male) and 114 (55 female, 59 male) patients receiving either table mounted, or self-retaining retraction were assessed with mean follow-up of 7.897 ± 7.01 and 10.46 ± 8.91 months (p= .074), respectively. Table-mounted retraction patients were significantly younger with a mean age of 62.78 ± 10.3 compared to 58.05 ± 13.1 years in the self-retaining cohort (P= .025). No observed differences in postoperative dysphagia were noted via the SWAL-QOL assessment tool (table-mounted: 83.00 ± 19.0, self-retaining: 81.70 ± 21.0,P= .819). No differences were noted between groups in postoperative PRO or PROMIS surveys. There were no differences in mean time of retraction per operated level (P= .243) or intraoperative blood loss (P= .985). However, mean operative time was significantly shorter with table-mounted retraction compared to self-retaining retraction (table-mounted: 116.6 ± 44.82 minutes, self-retaining: 129.1 ± 49.38 minutes,P= .015). Conclusion: There was no significant difference observed in rates and severity of dysphagia or patient-reported outcomes for neck or arm pain between patients who underwent ACSS with self-retaining and table-mounted retractors. Furthermore, operative time was significantly shortened with the use of a table-mounted retractor arm. These findings indicate that, with proper application, the use of a table-mounted retractor can improve operative efficiency without leading to inferior outcomes.
418
A004: Drivers for Unplanned Readmissions Following Adult Spinal Surgery
Sarthak Mohanty 1 , Sachin Gupta 1 , and Comron Saifi 1
1 University of Pennsyvlania, Department of Orthopaedic Surgery, Philadelphia, USA
Introduction: Unplanned readmissions are not associated with poor patient outcomes but also costly to healthcare systems. The costs of such readmissions has been estimated as high as $17.4 billion 1. Discovering independent predictors of hospital readmission has remained crucial in light of the penalties that hospitals can face 2. Readmission rates have been reported as high as 25% of all hospitalized patients. Therefore, identifying risk factors for readmission within 1 year post-operatively is critical. The goal of this study was to utilize a large, single institution database to assess the incidence of unplanned readmission at 30 day, 90 day, 180 day, and 1 year intervals and risk factors for readmission. Material and Methods: Patients included were those who underwent a spinal procedure as a principal or secondary procedure. They were then compared using baseline characteristics, intraoperative details, and postoperative outcomes. Baseline characteristics consisted of demographics, comorbidities, smoking status, diagnosis, procedures performed and post-operative outcomes. Readmission rates were measured at 30, 90, and 180 days post-operatively. Multivariable logistic regression was performed to establish independent associations with unplanned readmission within one-year post-operatively. Statistical significance was defined as P <.05 (two-sided test). Analyses were conducted with SPSS (IBM Inc., Chicago, IL). Results: 3,079 patients met the inclusion criteria. 22.34% were readmitted within one year. 10.49% of patients were readmitted by 30 days post-op, 3.77% between 30 and 90 days post-op, 3.25% 90 and 180 days, and 4.77% 180 days and one-year post-operatively (Table 1). Those who underwent thoracic procedures (P = .0304) had a higher likelihood of being readmitted. Smokers (P =.0342) had increased odds of being re-admitted compared to non-smokers. Each additional day spent in the hospital during the operative stay resulted in 1.071 higher odds (P < .0001) of readmission. Also, increasing age resulted in 1.021 higher odds (P < .0001) of readmission by one year. Notably, infection was the most common reason for re-admission and was found to correlate with increased rate for readmission within 30 days post-operatively (P = .002). Conclusion: This study was able to successfully identify and analyze risk factors for re-admission across a 1 year time period post-operatively. Older patients and smokers had higher rates for re-admission given their higher risk profile pre-operatively. Thoracic cases had increased readmission rates due to the relative morbidity associated with such procedures. In addition, cases complicated by infection were more likely to be re-admitted in the acute post-operative period most likely in order to treat and eradicate the infection. Surgeons should counsel those high-risk individuals, especially elderly patients and smokers, and patients undergoing thoracic surgery regarding the risks for complications, readmission, and subsequent procedures in addition to increased healthcare costs.
References
1. Jencks, S. F., Williams, M. V & Coleman, E. A. Rehospitalizations among patients in the Medicare fee-for-service program. N. Engl. J. Med. 360, 1418–1428 (2009).
2. Boozary, A. S., Manchin, J. 3rd & Wicker, R. F. The Medicare Hospital Readmissions Reduction Program: Time for Reform. JAMA 314, 347–348 (2015).
1581
A005: Outcomes After Lumbar Disk Herniation Surgery in the Dutch Population
Maike Schepens 1 , Miranda van Hooff 2 , Judith Erkelens, van 3 , Ronald Bartels 4 , Eric Hoebink 5 , Margot Smits 6 , Hans Kuijpens 7 , and Jacques Limbeek, van 6
1 Zorgverzekeraars Nederland, Strategy and quality of care, Zeist, The Netherlands
2 Maartenskliniek, Orthopedics, Ubbergen, The Netherlands
3 Vektis, Research, Zeist, The Netherlands
4 Radboud University Medical Center, Neurosurgery, Nijmegen, The Netherlands
5 Amphia hospital, Orthopedics, Breda, The Netherlands
6 Zilveren Kruis Health Insurance Company, Medical Advisory, Leusden, The Netherlands
7 VGZ Health Insurance Company, Medical Advisory, Eindhoven, The Netherlands
Introduction: Outcomes after surgery for lumbar disk herniation are defined in the International Consortium for Healthcare Outcomes (ICHOM) and include complications, re-operations, mortality, pain, quality of life. For shared-decision making before choosing surgery or conservative treatment patients and doctors need information on the incidence of complications and undesirable outcomes. So far, only limited data is available on the outcomes after primary surgery of this condition in Dutch patients. The objective of this nationwide study is to determine the occurrence of undesirable outcomes after primary surgery, in terms of reoperations, use of opioids and nerve root block treatment. Material and Methods: The Dutch National Claims Database (Vektis) was searched for lumbar hernia disk operations performed in the period between 01-07-2015 and 30-06-2016. Vektis has a nationwide, nearly full (>99%) coverage of all medical care claims that are reimbursed by insurance companies. For all lumbar surgery patients, we examined whether reoperation took place within 18 months. In addition, we investigated whether opioids were prescribed 6 to 12 months after surgery and whether nerve root block was given within one year after surgery. A combined outcome measure was composed of these three outcome measures. 95% confidence intervals (95%CI’s) were calculated with the Agresti-Coull method. Group comparisons between a low-volume hospital group and a high-volume hospital group were done using the Student’s t-test (2-sided). Results: In total 6,895 persons underwent primary lumbar disk herniation surgery during the study period. Lumbar disk herniation surgery was performed in 70 hospitals of which 30 hospitals performed less than 50 operations and 47 less than 100. 23 hospitals performed more than 100 operations per year (range 110 to 690). The reoperations’ weighted mean was 7.3 %, with wide confidence intervals (CI’s) in low-volume hospitals. The percentage of patients with nerve root block within 12 months after surgery was 6.7% and the opioid using patients percentage 6-12 months after surgery was 15.6%. The combined outcome measure showed that 23.0% of patients had one or more undesirable outcomes after surgery. For 14 out of the 30 low-volume hospitals (i.e., less than 50 surgical procedures per year) the 95% CI upper limit exceeded the 50% level for the combined outcome measure. Although the data suggested a volume effect on undesirable outcomes, the t-tests at the volume thresholds 50, 100, 150 and 200 interventions per year did not support this (P-values .07, .08, .13, .11). Conclusion: This unique nationwide study on claims data provides insight into patient-relevant undesirable outcomes such as reoperation, nerve root block and opioid use after lumbar disk herniation surgery. We found that almost one out of four patients had an undesirable outcome within 18 months after surgery that prompted further medical treatment. A wide variation in complication rates is shown between hospitals with a trend that supports a possible effect of volume in lumbar disk herniation care. Additional studies on factors that predict postoperative complications and on factors that prevent these undesirable outcomes are needed.
339
A006: 10k Spinal Cord Stimulation Improves Back and Leg Pain for Patients With Failed Back Syndrome: A Prospective Cohort Analysis With 2y Follow-Up
Simon Weidert 1 2 , Suero Eduardo 2 , Diana Hab 2 , Becker Christopher 2 , Greiner Axel 2 , Böcker Wolfgang 2 , and Ibrahim Richard 1
1 DGS Regional Pain Center Munich - East, München, Germany
2 Ludwig Maximilians Universität Munich, Dpt. for General, Trauma and Reconstructive Surgery, München, Germany
Introduction: Chronic pain as a result of failed back surgery is a difficult to treat condition. Despite advances in surgical techniques and medication strategies, a long-term reduction in pain after failed back surgery may be difficult to achieve, leading to a decrease in quality of life and to permanent disability. Spinal cord stimulation (SCS) implants have been designed to modulate pain signals before they reach the brain, potentially helping patients in which spine surgery has failed to improve pain. In the current study, we prospectively followed 82 patients who received a spinal cord stimulator (Nevro HF10) for chronic pain associated with failed back surgery syndrome. We aimed to determine whether the device would provide significant short- and long-term pain relief for localized back pain and leg pain alike. Material and Methods: This was a prospective series of patients with chronic pain due to failed back surgery syndrome who were operated on by a single surgeon to implant a spinal cord stimulation device. The device (Nevro HF10) consists of two leads placed posteriorly inside the spinal canal at around The attached to a generator that produces an electric constant stimulus at 10kHz frequency. Patients were surveyed pre-implantation and at 6, 12 and 24 months after implantation of the SCS. Using a Visual Analog Scale (VAS), we aimed to quantify pain pre- and post-implantation in the lower back (LB) and both legs (LL & RL) individually. In addition, patients were asked about their pre-implantation functional status, as well as their perception of pain relief. Statistical analyses were conducted using R. Generalized linear models of VAS score as a function of time post-implantation were used to estimate the effect of the SCS on pain. A P-value < .05 was deemed to be statistically significant for all analyses. Results: 82 patients (28 men and 54 women) received a permanent SCS implantation. The mean VAS score pre-implantation was: Lower Back = 8.0, Left Leg = 7.8, Right Leg = 7.6. We found a significant reduction in pain 6 months post-implantation: LB = 3.7, LL = 3.3, RL = 3.3 (P < .05). The reduction in pain persisted until the end of the follow-up at two years after implantation of the SCS. Conclusion: The Nevro HF10 spinal cord stimulator demonstrated to significantly improve pain in patients with failed back surgery syndrome at short- and long-term intervals. With a safe, minimally invasive implantation technique, the spinal cord stimulator may is an additional tool in the management of hard-to-treat chronic pain patients.
587
A007: Hyperlordotic ALIF Cages for the Treatment of Adult Spine Deformity: Incidence of Peri-Operative Radicular Pain and its Correlation with Radiological Outcomes
Domenico Compagnone 1 , Pedro Berjano 1 , Marco Damilano 1 , Riccardo Cecchinato 1 , Andrea Redaelli 1 , Francesco Langella 1 , Daniele Vanni 1 , Carmelo Messina 1 , Giuseppe Peretti 1 2 , and Claudio Lamartina 1
1 IRCCS Istituto Ortopedico Galeazzi, Milan, Italy
2 University of Milan, Department of Biomedical Sciences for Health, Milan, Italy
Introduction: In Adult Spine Deformity cases, the restoration of the ideal lumbar lordosis has positive effects on the clinical outcomes and decreases the risk of adjacent segmental failure. Several surgical strategies are available to reach the ideal spinal alignment. The anterior retroperitoneal approach for interbody fusion (ALIF) offers the possibility to achieve a high degree correction, thanks to cages with 20° and 30°, and to address lordosis restoration in the lower lumbar spine. This study aims to evaluate the incidence of radicular pain and its correlation with radiographic outcomes in patients undergoing hyperlordotic cages to treat Adult Spinal Deformity. Material and Methods: An analysis of a prospective consecutive single-center database was performed to analyze patients who underwent Hyperlordotic ALIF with or without posterior fusion to correct spinal deformity on the coronal and/or sagittal plane. Clinical outcomes were evaluated by the Visual Analog Scale (VAS) back and leg and Oswestry Disability Index (ODI) preoperatively and postoperatively and at 3, 6, and 12 months follow-up. Spinopelvic parameters [Pelvic Incidence (PI), Pelvic Tilt (PT) and Lumbar Lordosis (LL)] and Posterior Disc Height (PDH) and Anterior Disc Height (ADH) were assessed preoperatively and postoperatively on standardized full-standing EOS X-rays. The foraminal area (FA) were measured pre- and postoperatively on CT scan or MRI. Results: Thirty-seven patients (n = 37), with a mean age of 63.2 y/o (SD 8.6 y/o), underwent Hyperlordotic ALIF in our center from January 2016 to December 2019. Seven subjects developed perioperative neurological issues (3 right and 4 left) (Group A), while Thirty did not (Group B). The L5 radicular pain was statistically significant (Pvalue < .05) influenced by the segmental correction magnitude; an average of 26° (SD 11.05) instead of 15.11° (SD 9.93) was obtained with the hyperlordotic cage respectively in Group A and Group B: the higher the correction degrees, the higher the incidence of the symptom. Besides, the average of post-operative L5-S1 PDHs seems to be associated with the occurrence of radicular pain: post-operative PDH in Group A was 5.99 mm (SD 2.68) while in Group B was 8.25 mm (SD 2.62) (Pvalue < .05). Conclusion: The open retroperitoneal approach with hyperlordotic cages allows a good correction of sagittal and coronal imbalance. The radicular pain is a potential perioperative complication of this procedure. A high segmental correction and low post-operative PDH seem to be associated with the occurrence of the symptom; In the larger part of the cases, the radicular pain resolves without other surgical revision in an average time of 3 months.
1364
A008: Association of Duration of Preoperative Opioid Use with Reoperation After One-Level ACDF in Non-Myelopathic Patients
Andre Samuel 1 , Catherine Himo Gang 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
Introduction: Preoperative opioid use before cervical spine surgery has been linked to worse postoperative outcomes. However, no studies have determined the association of duration and type of opioid used with reoperations after anterior discectomy and fusion (ACDF). Methods: Patients undergoing single-level ACDF without myelopathy between 2007 and 2016 with at least 5 year follow up were identified in one private insurance administrative database. Preoperative opiate use was divided into acute (within 3 months), subacute (acute use and use between 3-6 months), and chronic (subacute use and use prior to 6 months) and by the opiate medication prescribed (tramadol, oxycodone, and hydrocodone). Postoperative rates of additional cervical spine surgery were determined at 5 years and multivariate logistic regression was used to determine the association of preoperative opiates with additional surgery. Results: Of 445 patients undergoing single-level ACDF without myelopathy, 66.3% were taking opioid medications prior to surgery. The most commonly used preoperative opioid was hydrocodone (50.3% acute use, 24.7% chronic use). Opioid naïve patients had a 5 year reoperation rate of 4.7%, compared to 25.0%, 15.5%, and 23.3% with chronic preoperative use of tramadol, hydrocodone, and oxycodone. In multivariate analysis, controlling for age, gender, and Charlson Comorbidity Index, chronic use of hydrocodone (odds ratio [OR] = 2.08, P = .05), oxycodone (OR = 4.46, P < .01), and tramadol (OR = 4.01, P = .01) were all associated with increased reoperations. However, acute use of hydrocodone, oxycodone, and tramadol were not associated with reoperations (P > .05). Conclusions: Both subacute and chronic use of common lower-dose opioid medications are associated with increased reoperations after single-level ACDF in non-myelopathic patients. This information is critical when counseling patients preoperatively and developing preoperative opioid cessation programs.
450
A009: Does Minimally Invasive Spine Approach Reduces the Incidence of Dural Tear in Degenerative Lumbar Pathology?
Ayush Sharma 1 , Vijay Singh 1 , Priyank Deepak 1 , Nilesh Mangale 1 , and Ajay Jaiswal 1
1 central railway hospital, department of Orthopaedic and spine surgery, Mumbai, India
Aims and Objectives: To compare the incidence of dural tear (DT) in open vs Minimally invasive spine surgery (MIS) in patients with degenerative lumbar pathologies. Methods: 420 operated cases of degenerative lumbar pathology with prospective follow up of minimum 6 months duration were included in the study. Cases were divided into open and MIS groups. Incidence of DT and various demographic and operative factors were compared across the two groups. Results: 156 patients underwent MIS surgery while open surgery was done in 264 patients. Majority of the study participants were in the age group of 41-60 years (48.0% among MIS patients and 64.4% among open cases). Incidental durotomy was documented in 52(12%) cases. On comparing the two groups, incidence of DT was significantly less in the MIS group (6.4%) compared to (15.7 %) in the open group (p < .05). On further analysis, depending on type of surgery, while the incidence of DT was comparable between the two groups for decompression and fusion surgeries, the MIS group had less incidence of DT for discectomy and in revision surgeries. In the open group, four patients underwent revision for persistent dural leak or pseudo-meningocele but none of the cases in the MIS group had revision surgery due to complications related to dural tear. The distribution of age, gender and risk factors was comparable between the two groups. Incidence of DT was significantly high for patients having high Body Mass Index (BMI) and diabetes mellitus and those undergoing revision surgery (P < .05) irrespective of the approach to surgery. Conclusion: Minimally invasive approach can result in significantly lower incidence of dural tear and complications related to dural tear when compared to open surgery in patients of degenerative lumbar pathology.
OP02: Deformity-Thoracolumbar (Adolescent) 1
943
A010: Is There Evidence of Latent Iron Deficiency in Adolescents Undergoing Spinal Corrective Surgery? An Audit and Quality Improvement Project
Thomas Barker 1 , andrew cook 1 , and Paul Barker 2
1 Norfolk and Norwich University Hospital, Trauma and Orthopaedics, Norwich, United Kingdom
2 Norfolk and Norwich University Hospital, Anaesthetics, Norwich, United Kingdom
Introduction: Spinal corrective surgery can be associated with significant blood loss, which, despite advances in blood loss techniques, can result in significant anaemia post operatively. Latent Iron Deficiency (LID) is a relatively new concept whereby otherwise well individuals have low iron stores but are not anaemic. LID can compound blood loss in surgery by reducing a person’s ability to generate new red blood cells, and has been linked to poor outcomes for other surgical procedures. It is well known that adolescents is a time of increased demand for iron particularly in young females who are common in this cohort. Methods: This audit and quality improvement project reviewed routine pre-operative hemoglobin concentrations and indices to see if there was evidence of latent iron deficiency. Included were patients under 30 presenting to Norfolk and Norwich Hospital for elective correction of adolescent idiopathic scoliosis or Scheuermann’s Kyphosis between January 2017 and March 2020. In addition to preoperative blood tests, we reviewed post-op haemaglobin, need for transfusion, complications, and time to discharge. Patients were excluded if they were undergoing scoliosis correction for other causes (neuromuscular, congenital, degenerative). Results: In our sample of 64 patients, the mean preoperative hemoglobin concentration was normal; 155.1g/L in males and 134.9 g/L in females (p < .005), however the Mean Corpuscular Hemoglobin (MCH) and Mean Cell Volume (MCV) tended to cluster towards and below the lower limits of the normal ranges, and were significantly lower than the population means (MCH p <.05 and MCV p < .01). We have also shown that those with a low MCV preoperatively were statistically more likely to be moderately to severely anemic post operatively, however there was no correlation with length of post-op stay or complications. Conclusion: We believe this data shows a prevalence of latent iron deficiency in this cohort, which may contribute to post operative anaemia. While we accept that ferritin and transferrin saturation are more accurate at identifying iron deficiency, they are not routine tests for otherwise well patients. Our next steps will be to measure the serum ferritin at decision to list for surgery, and if serum ferritin is < 100 mcg/L supplement with oral iron replacement therapy for at least a month prior to surgery.
816
A011: Three Dimensional Correction is Related to Brace Effectiveness in Patients with Adolescent Idiopathic Scoliosis
Kenny Yat Hong Kwan 1 , Amy Cheung 1 , Hui Yu Koh 1 , and Kenneth Man Chee Cheung 1
1 The University of Hong Kong, Hong Kong, Hong Kong
Introduction: Although scoliosis is a three-dimensional (3D) deformity, research in factors determining brace efficacy has not focused on the effects of 3D in-brace curve correction. The purpose of this study was to determine the effect of axial plane parameters on the outcomes of bracing with a thoracolumbosacral orthosis (TLSO) for AIS. Material and Methods: A prospective longitudinal cohort study of AIS patients who fulfilled the Scoliosis Research Society (SRS) criteria for bracing was performed from brace wear initiation and followed through minimum two-year follow-up or surgery. Radiographs using EOS Imaging System were used to reconstruct 3D images of the spine at pre-brace, immediate in-brace, 1 year in-brace and minimum 2 year out-of-brace. Univariate and multiple linear regressions were performed to determine the association between axial rotation correction and curve progression at final follow-up. Logistic regressions were performed to model the probability of risk of progression. Results: Fifty-three patients were enrolled and 46 patients were included in the analysis. At final follow-up, 30 patients did not have curve progression and 16 patients had curve progression. There was no difference in baseline characteristics between the groups. For the transverse plane parameters, significant difference was found between non-progressive and progressive groups in pre-brace apical vertebral rotation (AVR) (4.5 ± 11.2o vs - 2.4 ± 9.8o, p = .044) and 1 year in-brace AVR correction velocity (2.0 ± 5.0o/year vs - 1.7 ± 4.4o/year, p = .016). Logistic regression analysis showed that pre-brace AVR (OR = 1.063; 95% CI:1.000-1.131; p = .050) and AVR CV at 1 year (OR = 1.19; CI: 1.021-1.38; p = .026) were associated with an increased risk of curve progression. There was no difference in SRS-22 scores between patients who experienced curve progression and those who did not. Conclusion: We demonstrate that axial plane parameters and their correction during bracing are related to brace success in this prospective study.
601
A012: Is Fresh Leucodepleted Whole Blood Transfusion Superior to Blood Component Transfusion in Pediatric Patients Undergoing Spine Deformity Surgeries? A Prospective Randomized Study Analyzing Post-Operative Serological Parameters and Clinical Recovery
Keerthivasan J 1 , Shanmuganathan Rajasekaran 1 , Dilip Chand Raja Soundararajan 1 , Ajoy P Shetty 1 , and Rishi Kanna 1
1 Ganga Medical Centre and Hospitals Pvt Ltd, Spine Surgery, Coimbatore, India
Introduction: Major spine surgeries have elevated risks of peri-operative blood loss with significant need for multiple blood transfusions. Many controversies exist on whether fresh whole blood or components transfusion is superior in reducing coagulopathy and inflammatory response. Randomized studies have been done in cardiothoracic and onco-surgeries but can be biased as the primary pathology itself in those studies can confound the coagulation and inflammatory markers. Elective spine surgery is devoid of these confounding factors and study in this condition is an urgent necessity. The primary aim of the study was to compare the effectiveness of fresh whole blood (FWB) and blood component transfusion in improving clinical outcome and serological parameters in early post-operative period following major spine surgery. Methods: A prospective randomized study conducted in tertiary spine deformity centre on patients undergoing spine surgery from September 2017 to August 2018 which involved more than 6 levels of fusion and where expected blood loss was more than 750 ml in two groups. FWB group received fresh whole blood whereas CG group received components transfusion. Outcome measures: Pre-operatively demographics, diagnosis and facial measurements to assess puffiness; intra-operatively level of fusion, type of graft, duration of procedure, volume of transfusion and blood loss; and post-operatively drain collection, vitals, duration of oxygen support and ICU stay, volume of transfusion, complications including facial puffiness and well-being score. In addition, bio-chemical parameters such as PT, ABG, calcium, electrolytes, lactate and interleukin-6 were also compared between the two groups. Results: A total of 65 patients with spinal deformities of different etiologies were included. The mean age was 14.0 and 14.9 years in FWB and CG, respectively. All other pre-operative parameters were comparable. The mean fusion levels and surgical time were 11.1 and 221.20 minutes in FWB, as compared with 10.70 and 208.74 minutes in CG, respectively. Intra-operative blood losses were 929 ml (FWBG) and 847 ml (CG), and the mean volumes of transfusion were 1.90 (FWBG) and 1.65 units (CG). FWBG was significantly superior to CG in the following clinical and laboratory parameters: duration of oxygen dependence [36.43 (FWBG) vs 43.45 hours (CG); P = .0256], mean arterial pH [7.442 (FWBG) vs 7.394 (CG); p < .001], interleukin-6 [30.04 (FWBG) vs 35.10 (CG); p < .019], mean duration of HDU stay [40.6 hours (FWBG) vs 46.51hours (CG); p = .0234] and postoperative facial puffiness [7/30 in FWBG vs 18/35 (CG) (P < .02)]. Conclusion: FWB transfusion can potentially improve the immediate post-operative outcome in patients undergoing major spinal deformity surgeries by reducing the duration of intensive care unit stay and oxygen dependence. The other potential benefits of this practice, based on our study, include a reduced inflammatory response (reduced lactate and IL-6) and post-operative facial puffiness. However, further large-scale validation studies in future are necessary to precisely determine the role of FWB in spine surgeries.
1126
A013: Myelopathic Patients with Severe Pediatric Spinal Deformity can Improve Neurologic Function Close to Non-Myelopathic Patients by 1 year After Surgery
Meghan Cerpa 1 , Scott Zuckerman 1 , Zeeshan Sardar 1 , Lawrence Lenke 1 , Brenda Sides 2 , Michael Kelly 2 , Oheneba Boachie-Adjei 3 , Sumeet Garg 4 , David Bumpass 5 , Paul Sponseller 6 , Suken Shah 7 , Daniel Succato 8 , Burt Yaszay 9 , Peter Newton 9 , Rick McCarthy 5 , Harry Shufflebarger 10 , and Munish Gupta 2
1 Columbia University Medical Center, New York, USA
2 Washington University, St. Louis, USA
3 FOCOS Orthopedic Hospital, Patang West, Ghana
4 Children's Hospital Colorado Aurora, Aurora, USA
5 UAMS Dept. of Orthopaedic Surgery Arkansas Children’s Hospital, Little Rock, USA
6 Johns Hopkins, Baltimore, USA
7 Nemours/Alfred I duPont Hospital for Children, Wilmington, USA
8 Texas Scottish Rite Hospital for Children, Dallas, USA
9 Rady Children's Hospital, San Diego, USA
10 Nicklaus Children's Hospital, Miami, USA
Summary: Severe pediatric spinal deformity patients with myelopathy can expect significant improvement in neurologic function close to neurologic function of non-myelopathic patients by 1 year postoperative. Mean lower extremity motor scores (LEMS) in myelopathic patients increased significantly compared to baseline at every postoperative visit up to 2 years. While non-myelopathic patients had significantly higher postoperative outcomes in SRS mental health, function, and total score, both groups had significantly superior outcomes in every SRS domain compared to baseline. Hypothesis: In severe pediatric spinal deformity, we sought to compare short- and long-term neurologic outcomes in myelopathic versus non-myelopathic patients. Study Design: Prospective multicenter cohort. Introduction: In severe pediatric spinal deformity, ambulatory myelopathic patients are a high-risk population for intraoperative and postoperative neurologic complications. Given the decreased neurologic function before surgery, perioperative and long-term neurologic outcomes in a large series of these patients are unknown. Methods:311 patients with severe pediatric deformity were enrolled in a prospective, multicenter, observational study. Patients were split into two groups: myelopathic and non-myelopathic. Preoperative, perioperative, and postoperative variables and neurologic outcomes were compared. Results: Of the 311 patients, 29 (9.3%) were myelopathic preoperative while 282/311 (90.7%) were non-myelopathic. Both groups were similar in age (P = .18), gender (P = .09), and Risser Stage (P = .06), while more patients in the non-myelopathic group had previous surgery (50 vs 12; P = .03). There were no significant differences in length of surgery (7.4 ± 2.4 vs 6.4 ± 3.6; P = .14), levels fused (12.7 ± 11.9 vs 12.3 ± 12.0; p = .41), or EBL (1209 ± 1041 vs 1307 ± 940; p = .60), however the myelopathic patients had a significantly longer postoperative length of stay (13.0 ± 10.0 vs. 8.6 ± 5.0; P < .01). Mean LEMS in myelopathic patients increased significantly compared to baseline (40.7 ± 9.9) at every postoperative visit (First Erect: 46.0 ± 7.1, P = .02; 1 year: 48.2 ± 3.7, P < .01; 2 year: 47.2 ± 7.7, P < .01), while the non-myelopathic group did not experience any significant postoperative changes. Both groups had significant increases in every SRS domain compared to preoperative, while the non-myelopathic patients had significantly higher outcomes in mental health (P < .01), function (P = .02), and total score (p = .01) compared to the myelopathic group. Conclusion: Severe pediatric spinal deformity patients with myelopathy can expect significant improvement in neurologic motor (LEMS) function postoperative, close to neurologic function of non-myelopathic patients by 1 year follow-up, while both groups had significantly superior outcomes in every SRS domain 2 years postop compared to preoperative scores. Take Home Message: Myelopathic patients with severe pediatric-deformity can expect significant improvement in neurologic motor function postoperatively, close to that of patients without myelopathy. Both groups had superior postoperative outcomes compared to baseline.
927
A014: Can We Stop Distally at LSTV-1 for Adolescent Idiopathic Scoliosis with Lenke 1A/2A Curves?
Yong Qiu 1 , Xiaodong Qin 1 , Zhong He 1 , Zhen Liu 1 , Rui Yin 1 , and Zezhang Zhu 1
1 Nanjing University Medical School, Najing, China
Introduction: Posterior thoracic fusion to save more lumbar mobile segments has become the mainstay of operative treatment for adolescent idiopathic scoliosis (AIS) with Lenke 1A/2A curves. Although previous studies have recommended selecting the last substantially touching vertebra (LSTV-1) as lowest instrumented vertebra (LIV), good outcomes could still be achieved in some cases when LSTV-1 was selected as LIV. We aim to determine in which case one level proximal to LSTV-1 could be a valid LIV, in which case distal fusion should extend to last substantially touching vertebra (LSTV), and to identify risk factors for distal adding-on. Materials and Methods: Ninety-four patients were included in the study with a minimum of 2 year follow-up after posterior thoracic instrumentation, in which LSTV-1 was selected as LIV. Patients were identified with distal adding-on between first erect radiographs and 2 year follow-up based on previously defined parameters. Factors associated with the incidence of adding-on were analyzed. Results: The mean follow-up duration was 37.7 ± 15.8 months. Forty patients (42.6%) with LSTV-1 selected as LIV achieved good outcomes at the last follow-up. Several preoperative risk factors significantly associated with distal adding-on were identified, including lower Risser (P = .001), longer thoracic curve length (P = .005), larger rotation and deviation of LSTV-1 (P < .001) and preoperative coronal imbalance (P = .013). Conclusions: Skeletally immature patients with long thoracic curve, preoperative coronal imbalance, large rotation and deviation of LSTV-1 are at increased risk of distal adding-on when selecting LSTV-1 as LIV. Under this condition, distal fusion level should extend to LSTV; While in other case, LSTV-1 could be a valid LIV.
1589
A015: Selective vs. Non-Selective Thoracic Fusion for Lenke Type 1-4C Curves: Which has More Complications at 5 year Follow-Up?
Jay Reidler 1 , Scott Zuckerman 1 , Meghan Cerpa 1 , Joseph Lombardi 1 , Peter Newton 2 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
2 Rady's Children's Hospital, San Diego, USA
Hypothesis: Selective thoracic fusion is associated with lower rates of complications compared to non-selective fusion. Study Design: Retrospective analysis of prospectively-collected, multicenter data. Introduction: Selective thoracic fusion (STF) is a less invasive option compared to non-selective fusion (NSF) for adolescent idiopathic scoliosis Lenke Type 1-4C curves with significant lumbar deformity. Differences in perioperative and long-term complications between STF vs. NSF remain unknown. Methods: A multicenter, prospective database was queried for Lenke 1-4C curves with minimum 5 year follow-up. Patients were grouped as STF (fusion to L1 or above) vs. NSF (fusion below L1). Perioperative events and complications were compared. Results: In 219 patients (102 STF vs. 117 NSF), NSF had longer surgery (332.3 minutes vs. 231.8 minutes, P < .001), more blood loss ( = 639.9cc, P <.001), and more levels fused (12.1 vs 8.5; P < .001), though no differences were seen in POD1 pain score, days to oral pain meds, or length of stay. NSF had higher complication rates (24.1% vs. 12.7%, P = .032) and a non-significantly higher reoperation rate (8.5% vs 3.9%, P = .164). The most common non-reoperative complications in the NSF group were transient paresthesias (5/18, 27.8%) and pulmonary issues (5/18, 27.8%) within 0-90 days, indicating morbidity associated with longer surgeries. Implant-related reoperations in the STF group included 1 repositioned thoracic pedicle screw causing radiculopathy, and in the NSF group included 3 prominent implants requiring removal/shortening and 1 broken screw requiring replacement. There were 3 cases of residual deformity (1 STF vs. 2 NSF), treated with a heel lift (STF), bracing (NSF), and thoracoplasty (NSF). Infections requiring reoperations occurred in 2 STF cases vs. 5 NSF cases. Conclusion: Selective thoracic fusion for Lenke 1-4C curves is associated with less blood loss, shorter surgery, and a lower overall complication rate at minimum 5 year follow-up than Non Selective Fusion. There were no cases of reoperation for residual deformity in the selective thoracic fusion group. Summary: In this multi-center study with minimum 5 year follow-up, we compared rates of complications following selective vs. non-selective thoracic fusion in Lenke Type 1-4C curves. We found that selective thoracic fusion is associated with less blood loss, shorter surgery, and a lower complication rate. It did not lead to any cases of residual deformity requiring reoperation.
981
A016: Learning Curve in Minimally Invasive Surgery of Adolescent Idiopathic Scoliosis
Ayrat Syundyukov 1
1 Federal State Budgetary Institution Federal Center of Traumatology, Orthopedics and endoprosthesis replacement of Ministry of Health of the Russian Federation (Cheboksary), pediatric orthopedic, cheboksary, Russian Federation
Introduction: Dorsal minimally invasive AIS surgery has an equal degree of correction compared to standard surgical procedure and positive aspects such as low blood loss and fast recovery. The main disadvantage of the technique is the long time of the surgery. The purpose of the study is to assess the dynamics of changes in the magnitude of correction, the amount of blood loss and surgery time over a 4 year period, 2016-2019. Material and Methods: The study provides a retrospective analysis of prospectively collected experience data from one surgeon. Over 4 years, 49 patients were operated using MIS: 2016-12, 2017-10, 2018-16, 2019 - 11. The operation was performed from three skin incisions, with intermuscular approach alternately to the convex and concave sides of the spine, implantation of screws using the hands free technique, correction using minimally invasive devices and with the creation of conditions for fusion. The amount of the time of surgery (min.), the volume of blood loss (ml) and correction (in percent) in dynamics over the years and between the start and end points of study (2016 and 2019) were estimated, determined the Learning Curve. Results: A statistically significant annual decrease in surgery time was revealed (min.), starting from 3 years of observation (P < .05). The differences between the start and end points of observation are statistically significant (356.4; 95% CI: 240-540, P < .0001). Differences in the volume of blood loss (ml) are statistically unreliable in dynamics over the years and significant at the start and end points (221; 95% CI: 50-600; P < .05). The correction value (in percent) for the start and end points of observation did not have statistical differences (79.2; 95% CI: 55-98.3; P > .05). Conclusion: With an equivalent correction of deformations over 4 years, with an increase in the experience of the surgeon, the volume of blood loss and the time of the surgery are reduced. The Learning Curve comprised 38 operations to reduce the duration of surgery by an average of 13.5% annually.
506
A017: Serratus Plane Catheter for Pain Relief in Anterior Spinal Surgery for Idiopathic Scoliosis
Emily Tsang 1 , Alvina Lone 1 , Bisola Ajayi 1 , Jason Bernard 1 , Timothy Bishop 1 , and Darren Lui 1
1 St George's University Hospital NHS Trust, London, United Kingdom
Introduction: Patients having anterior thoracic or thoracolumbar scoliosis surgery may have severe pain postoperatively and require specialised analgesia both intra and post operatively. Intravenous opioid sparing techniques such as intrathecal diamorphine is inconsistent in their results. Morphine and other opioid-based drugs have the disadvantage of nausea, vomiting, constipation, dysphoria and immunosuppression. There is a paucity of data on epidural catheters for muscular blocks in the literature and none for anterior surgery. Various analgesic regimens are used by different anaesthetists including drugs such as morphine, ketamine, gabapentin, paracetamol and non-steroidal anti-inflammatories. The authors believe this is the first study of Serratus Anterior Blockade with Epidural catheR (SABER). Methods: This is a retrospective review of all anterior spinal surgery for adolescent idiopathic scoliosis performed at St Georges’ Hospital NHS Trust from January 2017 to December 2018. An epidural catheter placed in the serratus anterior muscular plane with infusion of 0.125% chirocane in addition to other analgesia was analysed. Analysis included: Demographics, dose and length of anaesthesia (epidural, intravenous, Patient controlled anaesthesia (PCA), oral) peri and postoperatively, transition to oral medication analysis, pain scores at different time point and associated factors or complications. Results: Over this time period, there was a total of 44 patients who underwent anterior spinal surgery, in which 26 patients had thoracic scoliosis surgery, 17 patients had thoracolumbar scoliosis surgery, 1 patient had both. The mean age was 16.4 (11-30 years old), 70% were female, with 100% receiving SABER. There were no early failures of catheter nor catheter site infections. Pain scores reported by the patients steadily reduce from 12 hours to 48 hours post-operatively. Pain scores between Thoracic versus Thoracolumbar scoliosis surgery were not significantly different (P > .05). Significant decrease in Intravenous morphine in both groups occurred on day 1. PCA was discontinued at a mean of 24 hours (20-34 hours). Transition to oral morphine started by mean of day 2.4 (day 2-day 3). Chest drain was removed at mean day 2.4 (day 2-day 4). Average hospital length of stay was 6.1 days. Conclusion: SABER is a novel technique for pain management with the avoidance of intravenous morphine and its well-recognized complications. There is no significant difference regarding the number of levels instrumented or magnitude of correction or anatomical location (thoracic vs thoracolumbar) or presence of costoplasty. There is reduction in PCA in all groups by 12 hours with average transition to oral morphine use by day 2. The use of local anaesthetic infusions in patients having anterior spinal surgery is a safe and effective method of pain relief. Further studies should be conducted to compare its efficacy.
1117
A018: Readmission and Unplanned Surgery After Surgical Scoliosis Correction in Children. A Multivariate Chort Study of 613 Cases
Jorge Nuñez Camarena 1 , Francisco Javier Alonzo González 2 , Caribay Vargas Reverón 3 , Sergio Antonio Castillo Rivera 4 , Jose Luis Do Santos 2 , and Pedro Fernández 5
1 Hospital Mútua Terrassa, Barcelona, Spain
2 Hospital "Ceibal" Accidentes I.G.S.S., Guatemala, Guatemala
3 Hospital Clínic i Provincial, Barcelona, Spain
4 Hospital Dr. Sótero del Rio, Santiago, Chile
5 Hospital La Fe, Valencia, Spain
Introduction: Scoliosis correction procedures in children are technically demanding and complex surgeries that can lead to several complications. Failure of these procedures is reflected in the overall rates of postoperative unplanned readmissions and reinterventions. The purpose of the study was to determine the main factors related to the failure of scoliosis correction surgery that caused unplanned readmissions and surgical reinterventions. Material and Methods: We revised 628 consecutive patients that underwent surgical correction of scoliosis in our center between the years of 2009 and 2017, with complete clinical and radiological records. 613 scoliosis correction surgeries in patients below 18 years of age were analyzed. 15 patients were excluded for having incomplete radiological records. The relevant result taken into consideration was readmission and unplanned reintervention after the primary procedure for scoliosis correction. The primary surgery was considered the initial procedure and patients were followed for a minimum of 12 months. Two orthopaedic spine surgeons were in charge of performing the retrospective revision of the clinical and radiological records. Causes of readmission were categorized as 1. Local complications of surgical wound 2. Implant related complications 3. Medical complications. A descriptive and multivariate logistic regression risk adjustment analysis was performed with the Stata 13 statistical package. Results: 613 patients met inclusion criteria. Middle age was of 13.4 years (Standard deviation 4.0), 66.1% of the patients were female. The most common diagnosis was idiopathic scoliosis (297 patients(P): 54.8%) and neuromuscular scoliosis (171 P: 27.3%). 477 instrumented fusions were performed, 71 surgeries of scoliosis correction with growing rods, 62 VEPTR and 3 other procedures. Global readmission rate per episode was of 18.8% (115/613 P). According to the days of readmission after initial hospital discharge the distribution was: between 0-30 days 4.2%, 30-90 days: 2.0% and 12.6% after the first 90 days from discharge. The main cause of readmission was implant related complications (44.3%). 79.1% of the patients that had an unplanned hospital readmissions were treated with a subsequent surgery. The adjusted model evidenced that the presence of comorbidity was the determining factor for unplanned readmission and surgery with significantly higher odds ratio (OR). Patients with syndromic scoliosis (OR 4.35%, 95% IC: 2.27-8.33) and neuromuscular scoliosis (OR 3.76, 95% CI: 2.13-6.61) presented with higher OR when compared with patients with idiopathic scoliosis. Age was also a significant risk factor. Conclusion: Patients with neuromuscular or syndromic scoliosis presented higher levels of complications and failure. 80% of patients that were readmited to the hospital after their initial discharge were treated with a second surgical intervention. The main cause of readmission was implant related complications.
OP03: Clinical Topics
1890
A019: Comparing Routine Elective Inpatient Spine Surgery to Orthopedic and Non-Orthopedic Surgery Trends
Mustfa Manzur 1 , Andre Samuel 2 , and Sheeraz Qureshi 2
1 Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, USA
2 Hospital for Special Surgery, New York, USA
Introduction: Comparison of relative volume, quality, and facility cost trends across the domains of inpatient elective spine surgery in the USA relative to other routine inpatient elective orthopedic and non-orthopedic surgical procedures have not been previously described in the literature. Material and Methods: Data was extracted from the USA (US) Centers for Medicare & Medicaid Services (CMS) National Inpatient Sample (NIS) using the Healthcare Utilization Project (HCUP) database. The following elements were extracted at the Medicare-severity diagnostic related group (MS-DRG) level: discharges, age, length-of-stay, facility charge, facility cost, mortality rate, and sex. MS-DRG codes were stratified into surgery focus areas. Reported means are all pooled. Threshold for significant difference was P < .05. Results: High volume routine inpatient elective orthopedic procedures included spine fusion and joint replacement. Routine inpatient elective procedure types available for comparison included bariatric surgery, coronary artery bypass graft (CABG) surgery, hernia repair, and extremity-focused vascular surgery. Volumes significantly increased for spine fusion (+1.2% annually, up to 436,745), hip/knee joint replacement (+3.4% annually, up to 1,359,889), and bariatric surgery (+4.4% annually, up to 182,915) [P < .05]. Volumes significantly declined for CABG (-2.3% annually, down to 157,005), hernia repair (-3.8% annually, down to 22,170), and extremity-focused vascular surgery (-4.2% annually, down to 154,600). For spine surgery, LOS increased +0.2 days to 3.7 days and mortality rate decreased 0.40% to 2.36% without significance [P > .05]. For hip/knee joint replacement, length of stay (LOS) decreased -1.3 days to 3.4 days and mortality rate decreased -0.19% to 0.16% without significance [P > .05]. Among comparison elective surgeries, bariatrics LOS decreased the most (-0.4 days to 1.8 days) with a reduction in mortality rate from 0.07% to 0.00% while vascular surgery LOS increased the most (+0.6 days to 6.0 days) along with the highest increase in mortality +0.39% up to 1.90% [p < .05]. In terms of cost, spine fusion procedures facility cost grew +$7,115 to $31,946; however, this cost grew 2.8% annually on average – a rate lower than the US healthcare consumer price index (CPI) over the same period (3.2%). Relative to spine fusion, hip/knee joint replacement surgery facility cost grew slower at 0.9% annually. Among comparable elective surgeries, costs grew the fastest for hernia repair (4.9% annually) and slowest for bariatrics (0.5%). Net change in total cost was greatest for CABG which increased by +$9,819 to $43,854. Conclusion: From 2008 through 2017, inpatient routine elective spine surgery volumes significantly increased. In contrast, only bariatrics net volume grew during the period (+47.2%) while other routine elective procedure net volume declined: CABG (-18.8%), hernia repair (-29.6), and (-32.0%). In contrast, LOS generally increased for comparable elective surgery procedures and with mortality rate significantly increasing for vascular surgery. Despite cost to provide routine inpatient spine surgery consistently increasing yearly, the overall annualized growth rate of this facility cost was both less than (a) the average US CPI growth rate for healthcare expenditure during this period and (b) the average annual growth rate for facility costs of comparable routine elective procedures.
387
A020: Post-Operative Readmission Following Spine Surgery: What Role Do Socioeconomic and Community Factors Play?
Sarthak Mohanty 1 2 , Meeki Lad 3 , David Casper 1 , and Comron Saifi 1
1 University of Pennsylvania, Department of Orthopaedics, Philadelphia, USA
2 Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA
3 Rutgers New Jersey Medical School, Department of Neurological Surgery, Newark, NJ, USA
Introduction: Since its inception in 2012, the CMS Hospital Readmissions Reduction Program (HRRP) has espoused cost-effective healthcare delivery by financially penalizing hospitals with 30 day readmission rates in excess of what would be considered acceptable based on a patient’s age, sex, diagnosis at discharge, and diagnoses prior to admission. However, recent studies corroborating the role of social, economic, behavioral, and environmental factors in a patient’s post-discharge outcomes suggest that this methodology could unduly fault hospitals that serve disadvantaged communities. Given the high cost of spinal surgeries, this present inquiry into the effects of socioeconomic and community factors in spine patient readmission is paramount. Methods: 2830 patients undergoing spinal surgery between 2012-2018 (except for trauma, malignancy, infection, or revision) were identified retrospectively from our institutional database, with readmission status (post-operative day [POD] 0-30, 30-90) as the outcome of interest. Pre-operative health (spinal pathology), demographic data (age, sex, smoking status, race), and neighborhood characteristics (neighborhood income inequality described by the GINI index, personal income, % of families under the federal poverty line, median household value, residents per primary care provider [PCP], prevalence of obesity and diabetes) were abstracted. Income was estimated per patient at the Public Use Micro Area level based on US Census Bureau American Community Survey data, accounting for patient age, race, sex, employment status, insurance status, and educational level. Variance inflation factors were calculated to eliminate collinear variables, followed by univariate and multivariate stepwise regression analyses (using upper quartiles for all continuous variables as reference). Significance was defined as P < .05, with Bonferroni corrections as appropriate for multivariate models. Results: On multivariate stepwise regression, patients under 48 years of age were found to be 0.45 [95% CI: .28-.71] times as likely to be readmitted by POD 30 than patients above 69 years of age. Increased neighborhood obesity prevalence (OR = 1.18 [1.05-1.30]), lower access to healthcare as measured by residents per PCP (OR = 4.24 [2.43-7.40]), population density of the lowest quartile or second-lowest quartile (OR = 9.46 [4.20-21.30], OR = 10.73 [5.07-22.72]), neighborhood median household value of the lowest quartile or second-lowest quartile (OR = 2.13 [1.02-3.24], OR = 2.159 [1.31-3.57]), and income of the lowest quartile or second-lowest quartile (OR = 12.55 [6.75-23.33], OR = 3.68 [1.88-7.23]) were also associated with higher rates of readmission by POD 30. Conversely, patients in neighborhoods with GINI indices ranking in the lower 3 quartiles had reduced odds of readmission by POD 30 (OR1 = .02 [.01-.03], OR2 = .03 [.01-0.06], OR3 = .19 [.10-.27]). Readmission between POD 30-90 was less likely in cervical deformity patients (OR = 0.46 [0.21-0.99]), with socioeconomic factors not demonstrating significant predictive value. Conclusions: Overall, our findings support the notion that surgical centers serving socioeconomically disadvantaged patients are at risk of increased readmissions following spine surgery. Moreover, serving healthier, more socially advantaged patients may not correlate to better surgical care but rather may reflect better access to care, greater financial capital, and less economic inequality within the patient’s neighborhood. Nevertheless, properly identifying at risk populations provides an opportunity to support these patients through better discharge planning and more expansive clinical care pathways.
1551
A021: The Epidemiology of Vertebral Osteomyelitis Requiring Surgical Intervention in the USA From 1998 to 2013
Michael Faloon 1 , Jennifer Kurowicki 1 , Stuart Changoor 1 , Kumar Sinha 1 , Ki Hwang 1 , and Arash Emami 1
1 St. Joseph's University Medical Center, Paterson, NJ, USA
Introduction: Cases of vertebral osteomyelitis (VO) that are refractory to conservative treatment are treated surgically to debride infected segments, decompress and ultimately stabilize affected vertebral segments. There is limited data on the epidemiology of surgical management in VO in the USA (US), and no study to date has evaluated the impact of patient characteristics on surgical outcomes on a large scale. The purpose of this study is to assess the characteristics of patients with VO who underwent surgical intervention. Material and Methods: From the Nationwide Inpatient Sample (NIS) database an estimated 228,044 patients were admitted for VO in the US between 1998 and 2013. Of these, 44,401 underwent surgical intervention. Data were extracted on patient demographics, comorbidities, inpatient mortality, length-of-stay (LOS), and inflation-adjusted hospitalization charges. Sub-analysis included comparisons of length of stay, hospital charges, & mortality rate between operative & non-operative VO cases. Results: The incidence of surgical intervention for patients with VO significantly increased from 0.6 per 100,000 in 1998 to 1.1 per 100,000 admissions in 2013, and is estimated to reach to 1.4 per 100,000 in 2020 based on regression model between calendar year and incidence of VO (R² = 0.9). Majority of patients were white (76%), male (54.5%), had a mean age of 56 years, and 38% carried Medicare insurance. Approximately 22.6% of patients has at least 1 complication during the immediate perioperative time. The comorbidities that significantly (P < .001) increased inpatient mortality were congestive heart failure (CHF) (OR: 6.1), liver disease (OR: 2.9), & renal disease (OR: 1.9). The most common postoperative complications were anemia (6.7%), sepsis (5.6%), superficial infections (4.1%), instrumentation complications (2.8%), pulmonary insufficiency (1.6%), deep venous thrombosis (1.2%), & hematoma (1.1%). The most commonly performed procedures were 2-3 level fusion/instrumentation of lumbar spine (58%), cervical spine (54%), and 4-8 level fusion of thoracic spine (43%). The most common factors that significantly (P < .001) increased length-of-stay were thoracolumbar fusion (OR: 19.9), combined anterior and posterior fusions (OR: 7.5), vertebral resection (OR: 4.4), and fusion of > 9 levels (OR: 3.7). The most common comorbidities that significantly (p < .001) increased length-of-stay were CHF (OR: 8.3), renal disease (OR 8.3), hepatitis C (OR:6.1), & history of drug abuse (OR: 3.2). The most common comorbidities that significantly (P < .001) increased total hospital costs were renal disease (OR: 7.4), liver disease (OR:2.2), CHF (OR: 2.1), psychological illness (OR: 1.6). The mean inflation adjusted total hospital costs increased from $20,355 per patient in 2001 to $39,991 in 2013. Conclusion: VO is an understudied condition with a steady increase in its incidence in the US. It appears that the rate and the need for invasive procedures to salvage this condition is also increasing. We identified certain patient demographics and comorbidities to be associated with higher complications, mortality rate and overall costs. VO is associated with lengthy and expensive hospital stays resulting in a significant burden to patients and the healthcare system.
1279
A022: Sagittal Spinal Alignment Varies with an Individual's Race: Results of the Multi-Ethnic Alignment Normative Study (MEANS)
Zeeshan Sardar 1 , Meghan Cerpa 1 , Jean Charles Le Huec 2 , Stephane Bourret 2 , Kazuhiro Hasegawa 3 , Wong Hee Kit 4 , Gabriel Liu 4 , Denni Hey 4 , Hend Riahi 5 , Michael Kelly 6 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
2 CHU, Bordeaux, France
3 Nigata Spine Surgery Center, Nigata, Japan
4 NUH University Spine Center, Singapore, Singapore
5 Kassab Institute, Tunis, Tunisia
6 Washington University, St. Louis, USA
Summary: Volunteers from 5 countries were enrolled in this radiographic study to provide a global evaluation of spinal alignment in the largest reported Multi-Ethnic cohort of asymptomatic adults. To study the variation of spinal alignment based on race the patients were divided into 3 categories: Asian, Black, and White. Pelvic incidence, sacral slope, pelvic tilt, SVA, and TPA did not differ significantly between the 3 races. However, significant differences in Thoracic Kyphosis and Lumbar Lordosis between the 3 races were found. Hypothesis: We hypothesize that the spinopelvic parameters will vary across the different races. Study Design: Retrospective review of prospectively collected data. Introduction: While we do understand the basics of spinal deformity correction in terms of attaining a globally balanced spine and matching the lumbar lordosis to the pelvic incidence, we still don’t understand the ideal shape an individual’s spine should have based on their unique morphology, age, and race. This study attempts to highlight differences in the spinal alignment of volunteers from 3 main races; Asian, Black, and White. Methods: Radiographic evaluation of full-body low dose stereoradiography in a multiethnic cohort of 488 asymptomatic adult volunteers (Mean age: 40.8; Range: 18-7 years). Patients from 5 countries were included; France, Japan, Singapore, Tunisia, and the USA. Volunteers were grouped into 3 main races; Asian, Black, and White. 3D measurements were performed using a commercially available 2D/3D modeling software. ANOVA and Tukey’s HSD for post-hoc analysis were used to determine the differences between groups. Results: Pelvic parameters including pelvic incidence (P = .38), pelvic tilt (P = .36), and sacral slope (P = .53) were similar amongst the 3 groups (P = .73). Lumbar lordosis (LL) was similar between the Black (60.7 ± 10.7) and White (59.2 ± 11.3; P > .05) races, whereas Asian volunteers (54.4 ± 10.8; P < .001) had lower LL. Thoracic Kyphosis (TK) was similar between the Black (46.5 ± 11.3) and White (47.3 ± 12.1; P > .05) races, but lower in Asians (40.1 ± 9.7; P < .001). The spine length was similar between the Black (565.4 ± 38.2) and Asian (569.7 ± 31.4) races, while it was longer in the White (578.4±31.6) volunteers (P = .0035). Parameters assessing sagittal alignment were similar between the 3 groups; SVA (P = .08), TPA (P = .71). However, T1 tilt was different between White (5.5 ± 2.9) and Asian (4.5 ± 2.3) (P = .0015). Conclusion: Volunteers in the Asian group had lower lumbar lordosis and thoracic kyphosis when compared to the Black and White groups while all groups had similar pelvic morphology. This difference in spinal alignment could possibly be related to different lifestyles. Take Home Message: Pelvic parameters, SVA, and TPA did not differ between the Asian, Black, and White races. However, lumbar lordosis and thoracic kyphosis were lower in the Asian group.
1892
A023: Intraoperative ketamine Use on Intermediate and Long-Term Opioid Utilization Following Spine Surgery
Carol Wang 1 , Ivan Zapolsky 2 , Chelsea Hendow 2 , and Comron Saifi 2
1 University of Pennsylvania, Perelman School of Medicine, Philadelphia, USA
2 University of Pennsylvania, Department of Orthopedic Surgery, Philadelphia, USA
Introduction: Reducing the need for postoperative narcotics may play a key role in curbing the opioid epidemic in the US. Ketamine, an NMDA receptor antagonist, has come to attention as an intraoperative analgesic that has shown promise in decreasing opioid consumption in the immediate post-operative period. However, there have been no objective studies evaluating its potential opioid-sparing effects over longer timeframes, a question arguably more relevant to public health. The purpose of this study is to determine whether intraoperative ketamine reduces long-term outpatient opioid use in patients after spine surgery. Material and Methods: A retrospective review was performed of patients who underwent spine surgery at our institution between August 2016 and June 2018. Opioid prescriptions filled between January 2013 and August 2019 were recorded from the Prescription Drug Monitoring Programs (PDMPs), and cumulative morphine milligram equivalents (MMEs) summed over a given period was used as a metric for comparing opioid consumption. Propensity score analysis was used to evaluate the association between intraoperative ketamine administration and outpatient opioid consumption at 1, 3, 6, and 12 months postoperatively. Patients were further stratified into subgroups based on their exposure to opioids pre-operatively (naïve vs episodic vs chronic use), as well as the magnitude of their pre-operative usage (40-60th percentile, 60-80th percentile, 80th + percentile, <90 MME/day, >90 MME/day). Results: A total of 434 patients were included in this study (118 who received intraoperative ketamine and 316 who did not). There was no statistically significant difference in mean postoperative outpatient opioid consumption between patients who did vs did not receive ketamine at 1 month (ketamine = 2442 MME, 95% CI = [1036-3848], control = 2081 MME, 95% CI = [378-3785]), 3 months (ketamine = 4219 MME, 95% CI = [2505-5933], control = 2548 MME, 95% CI = [-114-5210]), 6months (ketamine = 6337 MME, 95% CI = [3468-9205], control = 3191, 95% CI = [-1614-7997]), or 1 year (ketamine = 10352 MME, 95% CI = [4912-15791], control = 5002 MME, 95% CI = [-4007-14011]). Exposure to intraoperative ketamine was not associated with lower incidence of long-term postoperative opioid use (OR = 1.06, 95% CI = [.964 to 1.16]). Subgroup analysis failed to reveal differences in opioid consumption or incidence of long-term opioid use in any patient subgroup at any time point. Notably, ketamine exposure was not associated with reduced mean opioid consumption in patients with long-term preoperative opioid use (ketamine = 4552 MME, 95% CI = [3362-5742], control = 6011 MME, 95% CI = [5001-7021] at 3 months), despite this being the population theorized to benefit most from intraoperative ketamine. Conclusion: Administration of intraoperative ketamine is not associated with reduced outpatient opioid consumption or decreased incidence of long-term opioid use following spine surgery. Notably, though ketamine exposure has been theorized to have greater opioid-sparing benefits in patients with long-term or high-dose pre-operative opioid use, this was not observed in any subgroup in this study at any time point. Pain management and post-operative opioid consumption in spine surgery patients remain challenging topics that deserve further study.
1877
A024: The Use of Telemedicine for Orthopedic Pathology During the COVID-19 Pandemic
Karen Weissmann 1 2 , Marcelo Perez 1 , and Francoise Descazeaux 1
1 MEDS, Santiago, Chile
2 Universidad de Valencia, Valencia, Spain
Introduction: The use of audiovisual and communication technologies has increased health coverage access in remote areas. During the COVID-19 pandemic an explosive development of this technologies were implemented for orthopedic surgeons. Material and Methods: We analyzed telemedicine benefits at a single medical institution during the COVID-19 Pandemic. Health providers were trained beforehand to use digital platforms and electronic medical records. Health providers were sensed regarding usefulness and outreach. Users were analyzed according to their age, health insurance, geographic distribution and type of service needed. Two quality indicators were analyzed: Net Promoter Score (NPS) which is a fidelization index (promoters minus detractors) and Customer Satisfaction Index (CSI): (Service quality index: % of satisfied customers - % of unsatisfied customers). Both groups were analyzed for interface problems. Results: 1771 synchronous telemedicine episodes were done between April and June 2020: April (242), May (489) and June (840). 59% of the patients were male with a mean age of 41 years (women 40; men 43 years), 73% had private health insurance. 79% of the patients were from the Metropolitan areas. Overall most requested specialists were: Orthopedics (48%), Nutriologist (15%) and Dietician (14%). By gender, women represented 100% of the psychology consultations, 85% of the nutriology and 80% of the endocrinology attention. Men did 67% of the dietician request and 51% of the orthopedic ones. The NPS was 71.70% and ISN 85.71%. Regarding quality of the service, 96.7% of the patients considered their needs and expectations fulfilled and 87.62% reviewed the video-call quality as adequate. 100% of health care providers considered this tool as useful and will continue to do it post-pandemic. The orthopedic surgeons considered that 39.28% of the patients would have benefited from a face to face attention but concluded that 67.72% of the appointments met the requirements to be managed remotely. The most frequently encountered problems were digital literacy of the patients, audio interface problems (19,05%) and video issues (12.29%). 9.52% of patients were dissatisfied with the digital platform. Conclusion: Telemedicine allows remote access to specialists from all over the country and during emergency situations, managing to solve 67% of the orthopedics surgery requests. Patient fidelization with the system is 71.7% and customer satisfaction is 85.71%.
1914
A025: Incidence of Vertebral Fractures by Bone Fragility in Patients with Fractures of the Appendicular Skeleton
Rafael Cabral 1 2 , Rogerio Savoy 1 , Ewerton Galdeano 1 , and Marcelo Munhoz 1
1 University of Jundiai, Orthopedics, Jundiai, Brazil
2 Instituto da Coluna, Orthopedics, Campinas, Brazil
Introduction: Osteoporosis is characterized by decreased bone mineral density and impaired tissue microarchitecture, increasing the risk of fractures due to bone fragility. Some risk factors may be associated, such as: menopause, aging, past history of fracture, smoking, reduced body mass index, reduced bone mineral density, vitamin D deficiency, high blood pressure, diabetes, chronic kidney disease and dysfunction of the thyroid. Osteoporotic fractures represent a public health problem: the Brazilian elderly population is estimated at 23% by the year 2050. Vertebral fracture (VF) are typically related to osteoporosis and represent the first clinical manifestations of the disease, followed by long bone fractures. Patients with VF are five times more likely to have other affected vertebrae and twice as high risk if they suffer fractures of the proximal femur and other appendicular bones. Approximately 2/3 of spinal fractures are asymptomatic. The absence of the diagnosis is shown as a barrier to intervention and early treatment of osteoporosis. Although bone densitometry by double X-ray absorption (DXA) is the method of differential diagnosis, the high cost and availability act as limiting factors for its execution in the public health system. Thus, the presence of VF found on radiographic examination may be a more important clinical finding than quantitative DXA analysis and bioindicators of bone quality. The purpose of this study was to determine the incidence of VF in hospitalized patients with bone fragility fractures in the appendicular skeleton and to correlate with the concentrations of osteometabolic bioindicators and to identify risk factors. Material and Methods: The cross-sectional analytical study included 124 patients admitted to a public teaching hospital in the State of São Paulo, Brazil, from January 2019 to January 2020, with fracture due to bone fragility. Radiographs in the vertebral column profile allowed the quantification of according to the semi-quantitative method of Genant. Information related to previous history and biological material were collected to evaluate bone quality indicators. Statistical analyzes were performed using the Pearson Correlation test, Linear Regression and Student's T test. Results: Fracture of proximal femur was present in 55.65% and VF was identified in 58.87% of the sample. The concentrations of 25 (OH) D and Parathyroidhormone (PTH) were altered and associated with VF. Aging, previous history of fractures, smoking and Diabetes mellitus, were the most identified risk factors, whose fractures were more frequent in the thoraco-lumbar transition of the spine. Conclusion: A high incidence of VF was observed in hospitalized patients with fractures in the appendicular skeleton due to frailty, whose risk factors presented an important association. Among the evaluated bioindicators, hypovitaminosis D established an important relationship with fragility fracture. The identification of individuals with risk factors associated with the systematic radiographic evaluation of the thoraco-lumbar spine, is an important tool for screening and diagnosis of fragility fractures.
1903
A026: Impact of Postmenopausal State on the Distribution of Bone Mineral Density in the Lumbar Spine
Avani Vaishnav 1 , Philip Louie 2 , Chirag Chaudhary 1 , Michael McCarthy 3 , Ryan Lee 4 , Yoshihiro Katsuura 1 , Sravisht Iyer 1 , Steven McAnany 1 , Todd Albert 1 , Catherine Himo Gang 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
2 Virginia Mason Medical Center, Seattle, USA
3 Indiana Spine Group, Carmel, USA
4 George Washington University School of Medicine, Washington, DC, USA
Introduction: Hounsfield units (HU), typically measured at L1-L2, have been identified as a surrogate marker for lumbar Bone Mineral Density (BMD). However, concern remains that L1-L2 BMD may not fully capture BMD differences throughout the lumbosacral spine and inadvertently provide inaccurate assessment. Thus, the purpose of this study was to evaluate the impact of to analyze how conventional HU evaluation relates to local HU at commonly instrumented levels, and to evaluate the impact of age and post-menopausal state on HU in the lumbar spine. Material and Methods: Consecutive female patients presenting to a spine clinic who underwent lumbar CT were selected. Previous lumbar surgery, tumor, fracture or infection were excluded. Patients were divided based on whether they were pre- or post-menopausal. Hounsfield Units (HU) were assessed on lumbar CT by placing an elliptical region of interest confined to the medullary space of the vertebral body, and avoiding cortical bone or sclerosis. HU measurements were performed for L1-S1 in 7 regions: Mid-sagittal; Axial plane - Superior, Waist, and Inferior; Axial plane at the waist – Anterior, Middle and Posterior. HU were compared between the pre- and post-menopausal cohorts using student t-test or Manny-Whitney u-test. The difference between routinely used L1L2 average HU and local HU in each region was calculated and compared between groups. Association of age and menopausal state with HU was assessed using regression analyses. Results: Forty-eight patients, 18 pre-menopausal and 30 post-menopausal were included. The post-menopausal group was significantly older (67 vs 41 years; P < .0001). Post-menopausal women had lower HU in all regions at all levels (P < .05), with the mean difference ranging from 45 to 90 HU. Depending on the region, the L1L2 average was more than 10 units greater than L4 in 30-70% of pre-menopausal and 40-70% of post-menopausal women (P > .05). L1L2 average was also more than 10 units greater than L5 measurements in 17-78% of pre-menopausal and 40-70% of post-menopausal women (P > .05, except Sagittal region P = .038). Age, but not BMI showed a significant negative correlation with HU, which was strong in pre-menopausal and moderate in post-menopausal women. Age and menopausal state account for 35-60% of the variability in HU, except in the Posterior region, where they account for 25-45%. Conclusion: Age and post-menopausal state were negatively associated with HU in the lumbosacral spine, and the conventionally used L1L2 average did not adequately capture local HU variations. Local BMD assessment using HU may provide a more accurate assessment of morphometric characteristics and trabecular milieu in the operative region.
510
A027: Analysis of Industry Payments to Spine Surgeons Using the Open Payments Database
Andrew Platt 1 , Anil Mahavadi 2 , and Martin Herman 1
1 University of Chicago, Chicago, USA
2 University of Alabama at Birmingham, Birmingham, USA
Introduction: Since the 2013 Physician Payments Sunshine Act, all payments to physicians from drug and device manufacturers greater than $10 are required to be publicly disclosed and publicly accessible through the Open Payments Database (OPD). We analyzed differences in payments to academic spine surgeons based on specialty (neurosurgery vs. orthopedics) or geography and how they correlate with academic production. Material and Methods: Payments to academic spine surgeons in 2018 were queried through the OPD. Academic spine surgeons practicing at institutions in Chicago, Los Angeles, New York, Philadelphia, and Houston with both orthopedic and neurosurgical residency programs were included. All payments were recorded and combined to create the total reported payment. Number of publications for each academic spine surgeon for 2018 was taken from PubMed. Results: One hundred and thirty-eight academic spine surgeons were included in analysis including seventy neurosurgeons and sixty-eight orthopedic surgeons. The average total reported payments for all surgeons was $172,366 ± 778,701 (Range $12-7,820,343). The average number of publications in 2018 was 5.39 ± 7.98 (Range 0-46). The average in total reported payments to orthopedic spine surgeons ($311,035 ± 1,093,359) was significantly higher than the average in total reported payments to neurosurgery spine surgeons ($37,659 ± 76,289) (P = .044). The averages in total general payments and consulting fees were also significantly higher to orthopedic spine surgeons. The average number of publications in 2018 was higher from orthopedic spine surgeons (6.00 ± 8.47) compared to neurosurgeons (4.79 ± 7.48) but not statistically significant (P = .385). There were no linear relationships between payment amounts in any category (including royalty or license, consulting, or honoraria) and number of publications. Average payments to academic spine surgeons on the West Coast, East Coast, or Midwest were not significantly different(P = .34). Conclusion: This is the first study to examine payments to spine surgeons using OPD data. This study shows that in 2018, orthopedic spine surgeons received significantly higher industry contributions than neurosurgery spine surgeons. There was no significant correlation between industry payments and research publications. There was no significant difference in industry payments across different regions of the country.
OP04: Tumor and Infections
776
A028: Risk Factors Associated with Infection and Blood Transfusion in Pediatric Population Undergoing Scoliosis Correction
Fernando Alvarado Gómez 1 , María José Bravo Otero 1 , Fabián Armando Gil 2 , and Maria Fernanda Garcia 1
1 Instituto Roosevelt, Bogota, Colombia
2 Pontificia Universidad Javeriana, Bogota, Colombia
Introduction: Scoliosis is a three dimensional structural spine deformity where the deviation in the coronal plane exceeds 10°; 80% of them are idiopathic, the remaining 20% includes congenital, neuromuscular and syndromic etiologies. Scoliosis surgery has improved substantially during the past years, great efforts have been made in order to decrease surgical infections. Nonetheless, deep and superficial wound infections and healthcare-associated infection (HAI) still hind scoliosis patients recovery, lengthen hospital stay and increase scoliosis surgery costs. Current reported scoliosis infection rates ranging from 0.4% to 8.7%, superficial and deep infections occurred in 1.0% and 1.7% of pediatric patients respectively (n = 25,432). Several studies have established the relationship between blood transfusion and higher infection rates, even in idiopathic scoliosis surgery patients. The main object of this study was to determine if there is an association between patient baseline condition including the preoperative hemoglobin and other perioperative variables and the risk of perioperative transfusion and infection, in pediatric population undergoing scoliosis surgical correction. Materials and Methods: A retrospective cohort study was conducted using children undergoing scoliosis correction surgery between January 2014 and December 2016 at Roosevelt Children’s Orthopaedics Institute. Preoperative, intraoperative and postoperative variables were evaluated. A descriptive analysis of the variables was conducted using central tendency statistics and dispersion measurements for quantitative variables. Categorical variables frequency were registered. Separated bivariate analysis were performed between variables and blood transfusion and variables and infection. Multivariate analysis was performed for each outcome variable. Results: A total of 358 patients were included. Risk factors associated with infection were American Society of Anesthesiologists (ASA) III and IV, neuromuscular scoliosis and intraoperative blood transfusion. Risk factors associated with transfusion were preoperative hemoglobin values less than 10g/dl, longer surgical timing and surgical bleeding. HAI were 2.6 more frequent than SSI. Non- transfused patients had on average 1g/dl more preoperative hemoglobin than transfused patients. Conclusions: Ideal preoperative hemoglobin level has not been determined in literature, some authors propose a goal of 5g/dl above the cut-off point for transfusion in idiopathic scoliosis. Low presurgical hemoglobin is a risk factor for transfusion and the latter is a risk factor for infection. Preoperative administration of re-combinant human erythropoietin has been suggested as a measure to decrease BT in spine surgery. Considering that scoliosis correction surgery is an elective procedure, we should evaluate whether increasing hemoglobin levels before surgery decreases complications.
1113
A029: Operative Site Antibiotic Concentrations in Spine Surgery: Do the Prophylactic Antibiotics Reach the Surgical Site in Adequate Concentrations? Systematic Review on Analysis of Wound Concentrations of Various Prophylactic Systemic Antibiotics
Viswanadha Arun-Kumar 1 , J Naresh-Babu 1 , and Jeffrey C. Wang 2
1 Mallika Spine Centre, Department of Spine Surgery, Guntur, India
2 USC Spine Center, Department of Spine Surgery, Los Angeles, USA
Introduction: Prophylactic systemic antibiotic administration prior to any surgery has been a standard of care. One of the major determinants of prophylactic systemic antibiotic’s efficacy is its availability in sufficient concentrations at the surgical site. The drug concentrations achieved at the operative site is critically more important than that achieved in the serum. There are controversial reports in the literature regarding the drug concentrations of antibiotics in the wound. The purpose of this systematic review is to analyze the studies investigating the operative site concentrations of various prophylactic intravenous antibiotics in elective spine surgery. Material and Methods: A systematic review with search limited to English language was conducted of Pubmed/Medline SCOPUS, EBSCO and Cochrane Library using Medical Subject Heading (MeSH) terms. Studies investigating operative site antibiotic concentrations in human subjects who received prophylactic systemic antibiotic prior to elective spine surgery were included. Operative site concentrations were defined as concentrations measured in soft tissue, bone, ligament, intervertebral disc or wound/drain fluid at or near the site of surgery. Search of prophylactic antibiotic was not limited to any specific class. Studies excluded were case reports, animal, in vitro and biomechanical studies. Quality of the studies were assessed by Newcastle-Ottawa Scale. Results: Total number of citations reviewed were 742. After title and abstract exclusion, 48 were selected for retrieval of full text. Out of which 33 were excluded as they did not meet the inclusion criteria of the present study. Fifteen studies were selected and included for final analysis in this study. 13 of the included publications were prospective cohorts, Type of surgery varied from discectomy in 5 studies to short spinal fusion in 6 studies and deformity correction in 4 studies. Majority of the publications estimated the operative site concentrations of Cephalosporins followed by Aminoglycosides, Pencillins, Glycopeptides and Beta lactamase. Overall, antibiotic concentrations in the intervertebral disc ranged from 2.23 - 68.2 μg/g. Pencillins were observed to achieve the least concentrations in IVD. Of all the articles on Cephalosporins, there were considerable differences in tissue concentrations between various Cephalosporins (P value >.05). Highest penetrated antibiotic into IVD was found to be gentamycin followed by sulbactum, clindamycin and ampicillin. Cephalosporins and vancomycin had the least penetrating capacity into the intervertebral disc. The overall quality of the studies seemed to be less than average as only seven studies scored 5 or more out of 9 points on the NOS. Conclusion: Availability of an antibiotic in local tissues depends on various factors such as protein binding capacity of the antibiotic, penetration capability of antibiotics into tissues and seroma or haematoma formed during surgery which may not be accessible to systemic antibiotics and this may limit the availability of the drug in required concentrations at the operative site. This review identifies the lacunae in the literature and there is an urgent need for large prospective trials estimating wound concentrations of routinely used prophylactic systemic antibiotics in spine surgery.
844
A030: Subclinical Propionibacterium Acnes Infection Estimation in the Intervertebral Disc (SPInE-ID): A Prospective Cohort
Nelson Astur ,1,2 , Marcelo Wajchenberg 1,3 , Michel Kanas 1,3 , Andre Mario Doi 4 , Marines Dalla Valle Martino 4 , Mario Lenza 5 , and Delio E. Martins 1,6
1 Hospital Israelita Albert Einstein, Orthopaedics - Spine Group, Sao Paulo, Brazil
2 Santa Casa de Sao Paulo School of Medical Sciences, Department of Orthopaedics and Traumatology, Sao Paulo, Brazil
3 Universidade Federal de Sao Paulo, Department of Orthopaedics and Traumatology, Sao Paulo, Brazil
4 Hospital Israelita Albert Einstein, Department of Microbiology, Sao Paulo, Brazil
5 Hospital Israelita Albert Einstein, Orthopaedics, Sao Paulo, Brazil
6 Universidade Anhembi-Morumbi, School of Medicine, Sao Paulo, Brazil
Introduction: Cutibacterium acnes, formely known as Propionibacterium acnes is an anaerobic bacteria present in the skin flora, hair follicles and sebaceous glands. It has also been related to spine infection and osteomyelitis. Degenerative disc disease and Modic changes were associated to the presence of C. acnes within the intervertebral disc. Modic changes Type I appearance is very similar to spondylodiscitis and sometimes diferential diagnosis cannot be made. Those changes could be secondary to infection by a low-virulent pathogen. We know that subclinical disc infection leads to low back pain, sciatica and endplate abnormalities and C. acnes has been implicated with it. The purpose of this study was to identify if the presence of an infective pathogen within the disc is primary or an intraoperative contamination and if it correlates with low back pain. Material and Method: We prospectively gathered patients from 18 to 65 years old with lumbar disc herniation requiring decompression surgery and sent a disc sample collected during surgery to tissue culturing and pathogen identification. Patients were clinically followed during one year for pain (VAS), disability (ODI) and quality of life (EQ-5D) assessment. Modic changes were assessed comparing preoperative and 1 year postoperative MRI. Infection was also controled with ESR, CRP and Leucogram. During standard fashion microdiscectomy surgery, we first collected samples of the ligamentum flavum, then the herniated disc fragment and finally the muscle. They were sent to microbiology for anaerobic and aerobic culturing and were incubated respectively for 5 and 14 days. After positive culturing, pathogen was identified by MALDI-TOF and molecular analysis. Our primary endpoint was rate of disc infection which we considered as a positive disc culture with both negative muscle and ligamentum culture. Secondary endpoints were the correlation of infection with performance scores, Modic changes and laboratory screening. The protocol of this study was registered at clinicaltrials.gov. Results: We included 108 patients, with most cases being men (58.3%). Mean age was 42 years-old. We had only two cases out of 108 patients that were considered disc infection. Twelve patients also presented positive control tissue cultures and were considered contamination. The vast majority of our patients had no positive culture for any of the collected tissues. Muscle sample was the one with most positive cultures. C. acnes was the most frequent pathogen identified followed by S. aureus. Of the two patients diagnosed with disc infection, one was due to S. aureus and other by C. acnes. Laboratory exams had no significant variance during follow up. There was not a clear pattern of how Modic changed one year after surgery. Mostly, the incidence of Modic increased after surgery presenting types I and II at the same time. Our disc infection rate was 1.8%. We did not find any correlation of infected patients with clinical outcomes, laboratory or Modic changes. Conclusion: Subclinical infection rate of the intervertebral lumbar disc is at 1.8% and may be overestimated in the current literature. Subclinical infection is not related to worst outcomes or worsening of Modic changes over time.
1200
A031: A change in Protocol of Wound Care in Spinal Surgery and its Impact on Postoperative Wound Infections in Neurosurgery
Sara Lener 1 , Granit Molliqaj 2 , Aria Nouri 2 , Karl Schaller 2 , Claudius Thomé 1 , Pierre-Pascal Girod 1 , and Enrico Tessitore 2
1 Medical University of Innsbruck, Department of Neurosurgery, Innsbruck, Austria
2 Geneva University Hospital, Department of Neurosurgery, Geneva, Switzerland
Introduction: Surgical site infections (SSI) are an unfortunate post-operative complication responsible for morbidity. They account for 3% in spine surgery and can increase to 12% with instrumentation. Their treatment usually consists in a surgical revision associated with prolonged antibiotic therapy. This work focuses on wound closure technique, which has an essential influence on SSI. We recently introduced a closed wound dressing (Dermabond or Dermabond + Prineo) that is applied in the operating room. The aim of our study is to determine if a closed dressing protocol reduces SSI. Material and Methods: All patients diagnosed with SSI (based on inspection, clinics and MRI), during the initial stay or at readmission, are prospectively followed. Based on this data, we retrospectively included all primo-operated spine procedures from April 2016 to July 2017 in 2 different centers (Geneva, Switzerland, and Innsbruck, Austria). Data regarding patients, individual infection risk factors, type of surgery and SSI were collected. They were separated in 2 general groups: Closed-Protocol, where we applied the dressing system Dermabond +/- Prineo (a self-adhering mesh with 2-octyl-cyanoacrylate skin glue, removed after 14 days; and Conventional-Protocol, which included dermal, intradermal sutures or staples. Surgical closure of fascia and subcutaneous layer was identical in both groups. For preliminary analysis, we compared the infection rate of each closure type versus all others. Results: 672 patients were included in our study:157 received staples, 122 skin sutures, 101 intracutaneous closure, 78 Dermabond, 217 Demabond+Prineo. The infection rate was 2.4 % (n = 16). The highest infection rate was observed with skin sutures (4.9%) and the lowest was with Dermabond (1.3%) and Dermabond + Prineo (1.4%) compared to an overall infection rate of 2.4%. However, only skin sutures showed a statistically significant difference versus all other closures (4.9% vs 1.8%, P = .05). Despite having lower rates of infection, Dermabond (1.3% vs 2.5 %, P = .43) or Dermbaond+Prineo (1.4% vs 2.9%, P = .24) did not have significantly lower infection rates. Conclusion: Surgical site infections are significanly higher with skin surtures. Dermabond or Dermabond-Prineo had the lowest infection rates, but a larger cohort is necessary to demonstrate a significant superiority versus all other closure types. Further investigation via a multicentric controlled randomized trial is planned.
1672
A032: Malignant Spinal Cord Compression in the Pediatric Population - A Systematic Review, Meta- Analysis and Formulation of National Guidelines
Nigil Palliyil 1 , Nasir Quraishi 1 , Daniel D'Aquino 1 , and David Walker 1
1 Queens Medical Centre, Nottingham University Hospital, Spinal Surgery, Nottingham, United Kingdom
Study Design: Systematic review. Introduction: Malignant Spinal Cord Compression (MSCC) has been noted in 3-5% of children with primary malignant tumours. MSCC can be associated with permanent neurological deficits, hence prompt diagnosis and treatment is necessary. Etio-pathogenesis of spinal cord compression in children is entirely different from that in the adult population and hence the results from adult studies cannot be extrapolated. Our aim was to perform a systematic review on MSCC in children less than 18 years to help formulate national guidelines. Materials and Methods: A systematic review of the English language was undertaken using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Search criteria included ‘MSCC in children, paediatric and metastases’ for papers published between January1999 and September 2019. Isolated case reports/case series with <10 patients were excluded. Results: From a total of 17 articles identified, a final 7 were analysed (Level III/IV). Neuroblastoma constituted the most common cause for MSCC in children (62.7%) followed by sarcoma (14.2%). Soft tissue sarcomas constituted the most frequent cause of MSCC in children >5 years old. The median age at time of diagnosis was 50.9 months (.5-204). The median follow up duration was 50.3 months (14.8-139). Thoracic spinal cord was the most common site of neural compression (45.5%). 95.6% of children presented with motor deficits followed by pain (65.4%) and sphincter disturbance (24%). MRI (Magnetic Resonance Imaging) was the imaging modality of choice. First line steroid therapy was given to all patients before definitive therapy was instituted, resulting in neurological improvement in 75% of cases. 78.6% of patients presenting within 4 weeks of the onset of symptoms showed complete neurological recovery as against 25% of patients making complete recovery amongst those who presented later than 4 weeks. The overall five year survival rate was 72.6% (70.5-79.2%). Definitive treatment modality instituted varied according to the type of primary tumour. Radiotherapy (60%) was associated with the highest incidence of scoliosis as a late sequelae following treatment followed by laminectomy (33%) and chemotherapy (7%). Conclusion: Neuroblastoma is the most common cause for MSCC in children (62.7%) followed by sarcoma (14.2%). Whilst, soft tissue sarcomas constituted the most frequent cause of MSCC in children >5 years old. In children with Neuroblastoma/Lymphoma, chemotherapy was the primary modality of treatment. Early surgery should be a consideration with rapid deterioration of neurology despite chemotherapy. A multimodality approach including chemo-radiotherapy and surgery should be the treatment of choice in metastatic sarcomas. It is worth noting that multi-level laminectomy/decompression and asymmetrical radiation to the spine can lead to spinal column deformity in the future. The prognosis for neurological recovery was found to be inversely proportional to the degree of neurological deficits and duration of symptoms at the time of diagnosis.
1321
A033: ApoE4 Polymorphic Genotype-Associated Neck or Back Pain and Radiculopathy Incidence in Intradural Spinal Cord Tumor Patients in Beijing: A Prospective Clinical Observation
Nicholas Van Halm-Lutterodt 1,2 , Ziyang Ye 3 , Wei-Cheng Chen 4 , Wei-Hsun Huang 2 , Mohamed Kamal Mesregah 1 , Brandon Yoshida 1 , Andrew Mecum 5 , Krishna Mandalia 1,6 , Wenxin Lei 7 , Mercy Bartels-Mensah 8 , Yu Wang 2 , and Yulun Xu 2
1 Keck Medical Center of University of Southern California (USC), Department of Orthopaedics and Neurosurgery, Los Angeles, USA
2 Beijing Tiantan Hospital, Department of Neurosurgery, Beijing, China
3 Wake Forest University, Department of Mathematics and Statistics, Winston-Salem, USA
4 Beijing Tongren Hospital, Department of Clinical Sciences, Beijing, China
5 Emory University, Department of Psychology, Atlanta, USA
6 University of Southern California, Dornsife College of Letters, Arts and Sciences, Los Angeles, USA
7 Melbourne University, Department of Mental Health Nursing, Parkville, Australia
8 University of Debrecen, Department of Clinical Sciences, Debrecen, Hungary
Introduction: One clinical conundrum spine surgeons face is that, after exhausting all potential treatment options, some spine patients recalcitrantly retain or accrue some neurological deficits without any obvious reasons. Currently, Apolipoprotein Eε2 and Eε4 alleles are the most widely studied neurodegenerative and metabolomics genes owing to their reported health- and risk-related properties, respectively. In the spine literature, how ApoEε2 and ApoEε4 impact neurological and patient-related outcomes (PROs) are seldom discussed. We investigated the impacts of ApoEε2 and ApoEε4 genotypes on outcomes of intradural spinal cord tumor (ID-SCT) patients at baseline and 2 year postoperative. Materials and Methods: Following approval by the institutional review board (IRB) of Beijing Tiantan Hospital-Affiliated Capital Medical University, a prospective clinical study of 336 adult (≥18 years) ID-SCT patients who underwent surgical treatment without any prior primary therapy were assessed. ApoE single nucleotide polymorphisms (SNPs) were evaluated for all the ID-SCT patients. Patients within each ApoE2 and ApoE4 categories were then dichotomized into homozygosity-wild type (WT) versus heterozygosity-variant type (VT) as follows: ApoEε2-(rs7412) [WT ( C/C )] vs ApoEε2-(rs7412) [VT ( C/T )] and ApoEε4-(rs429358) [WT ( T/T )] vs ApoEε4-(rs429358) [VT ( C/T )]. Perioperative clinical and PROs were compared between the genotypes. Key primary outcomes comprised of demographics and tumor-related findings as well as W.H.O. classification of the ID-SCTs between the genotypes. Secondary outcomes compared neurological and PROs between the genotypes at baseline and at 2 year postoperative for patient self-reported outcomes that included: visual analogue scale (VAS), Neck Disability and Oswestry Disability Indices (NDI or ODI). Functional measures included: McCormick’s classification and the RAND-36 [Short-Form 36 (SF-36)] health-related quality of life (HRQoL) assessment. Laboratory measures included: Serum glucose, lipids, and protein profiles. Univariate and multivariate analyses were carried out by student t-test, Pearson’s Chi-squared test, Mann-Whitney U test and general linear model (GLM), respectively, with age, gender, body mass index (BMI), and multivitamin intake considered as covariates. Statistical significance was set at P < .05. Results: Of the 336 ID-SCT patients, approximately 85.4% vs 14.6% were ApoEε2-(rs7412)-WT vs ApoEε2-(rs7412)-VT and 81.2% vs 18.8% were ApoEε4-(rs429358)-WT vs ApoEε4-(rs429358)-VT carriers, respectively. The overall average age of patients was 45.0 years, with a female incidence of 53.3%. No significant outcomes were observed for tumor characteristics and W.H.O. grading between the genotypes, (P > .05). At baseline, ApoEε4-(rs429358)-WT carriers showed 300% increase in Neck or Back Pain incidence and 400% increased Neck or Back Pain intensity compared to the ApoEε4-(rs429358)-VT carriers. At 2 Year postoperative, higher significant rates of intractable pain, radiculopathy (paresthesia), and significant inferior social functioning (SF) component score outcome were observed in the ApoEε4-(rs429358)-VT carriers compared to the other 3 genotypes, (P < .05). Conclusion: Findings from this study indicate that the ApoEε4-(rs429358)-WT genotype was significantly associated with increased neck or back pain incidence and intensity at baseline. At 2 year postoperative, the ApoEε4-(rs429358)-VT genotype was significantly associated with increased inferior outcomes of intractable pain, radiculopathy, and social functioning. These outcomes are incentivized value-based information. Our report advocates for genetic-based precision spine practice and warrants further investigation of the possible cost-associated revenues and clinical impacts of ApoE gene in spine patients.
1388
A034: Application of Instrasite Vancomycin for Risk Reduction of Surgical Site Infection After Degenerative Thoracolumbar Posterior Fusion and Idiopathic Scoliosis Surgeries
Zoltan Hoffer 1 , Istvan Klemencsics 1 , Aron Lazary 1 , and Peter Pal Varga 1
1 National Center for Spinal Disorders, Budapest, Hungary
Introduction: Idiopathic scoliosis and degenerative thoracolumbar spinal surgeries can achieve significant improvement in patients’ quality of life. However, surgical site infection can have a significant impact on the final results of surgical treatment. Because of that several preoperative and also intraoperative risk reduction strategies have been developed. The use of intrasite vancomycin is a widely used method. Material and Methods: The aim of our comparative prospective cohort study was to evaluate the effect of local administration of vancomycin on surgical site infection (SSI) after extended degenerative thoracolumbar and idiopathic scoliosis surgeries. Study cohort was made up by patients who underwent surgical treatment between 02/July/2015 and 30/June/2016 because of degenerative thoracolumbal pathologies or idiopathic scoliosis from posterior approach. Patients in the control group were surgically treated because of the same spinal pathologies between 02/July/2015 and 30/June/2016. All of the patients in the study group received both sub- and suprafascially 1g of vancomycin powder before surgical wound closure. Prevalence of SSIs was prospectively analyzed for the two cohorts. Results: The control cohort consisted of a total of 238 patients. The mean age was 50.8 years (8-82 years), with a gender distribution of 172 women (72.3%) and 66 men (27.7%). 175 patients (73.5%) underwent surgery for degenerative thoracolumbar pathology and 63 cases (26.5%) for idiopathic scoliosis. The prevalence of SSI in the control cohort was 13.4%. A total of 199 patients were included in the study cohort. The mean age was 51.1 years (11-84 years), with a gender distribution of 137 women (68.8%) and 62 men (31.2%). 148 patients (74.4%) underwent surgery for degenerative thoracolumbar pathology and 51 cases (25.6%) for idiopathic scoliosis. The prevalence of SSI in the study cohort was 9.5%. Difference in the prevalence of total SSIs proved not to be statistically significant (P = .207) between study and control cohorts, not even in terms of superficial (P = .212) or deep (P = .563) SSIs. Conclusion: The prevalence of SSI was relatively lower in the study cohort during intraoperative local administration of vancomycin. However, the difference between the two cohorts in terms of SSI’s prevalence was not significant regardless of the depth of SSI. Based on our results we can not recommend routinely prophylactic, intraoperative local use of vancomycin.
679
A035: Spinal Infection: Analysis of 600 Patients Over 11-years
Hamdan Abdelrahman 1,2 , Mootaz Shousha 3 , and Heinrich Boehm 3
1 Asiut Universty Hospitals, Asiut, Egypt
2 Helios Hospitals Erfurt, Erfurt, Germany
3 Zentralklinik Badberka, Bad Berka, Germany
Introduction: Spinal infection encompasses a broad range of clinical entities and accounts for approximately 2% to 7% of all cases of osteomyelitis. Primarily, it is a disease of adults affecting predominantly those in their fifth decade of life. The age-adjusted incidence increases with every decade thereafter. The overall incidence of pyogenic spinal infection is on the increase. Methods: Retrospective analysis of prospectively collected data between 2005 and 2015. Data of 600 consecutive patients had been reviewed. The patients previously operated at the spinal region of infection and postprocedual infections had been excluded from the study. In patients with haematogenous spinal infection, the collected demographic, clinical, radiological and laboratory data had been analysed and the effects of various causative organisms on these parameters has been studied. Results: 250 females and 350 males (mean age of 66.1 years). 73.7% of patients were older than 60 years. 67.3% of patients were overweight or obese (P-value .000*). DM in42.2%, Cardiac diseases in 48.2%, renal diseases in 207 (43 patients were on renal dialysis), liver cirrhosis in 34 patients. 56.7% of the patients were in ASA- class III and IV and it had a positive correlation with age (P-value .000*). Other site of infection found in 51.7% as a possible source of infection. 51.2% neurological deficit was found at the presentation; increased with age (P-value .001*), infected spinal region (P-value .000). Lumbar spine in 67%, cervical spine in 7.5% and in 11 patients SIJ. Multifocal was detected in 11.3%; with renal insufficiency in 35 patients (P-value .003*), other sites of infection in (P-value .003*). The commonest type of infection was pyogenic in 95.6%, fungal infection in 6 patients, TB in 14. Mixed infection in 26 patients (4.3%). MRSA in 30 patients of them). Gram-negative organisms in 45 patients (7.5%); E. coli in 20 of them. Discussion: The elderly patients are more susceptible to spinal infections due to the associated comorbidities and immunocompromise than the other age groups. Thanks to the advent of various techniques which helped to improve the diagnostic efficiency to early diagnose these cases and to isolate various causative organisms in spinal infections and hence improve the prognosis of the disease in the recent years. Yet, even with improved diagnosis tools and procedures, the delay in diagnosis remains an important issue. This review aims to highlight the importance of a methodological attitude towards accurate and prompt diagnosis of spinal infections. The introduction of PCR as well as special media for organism culture, especially in patients with low inflammatory parameters, can facilitate the identification of the causative organism and reduce the number of culture with ‘No Growth’.
295
A036: Standardising Post Operative Care Documentation Practices in Spinal Surgery
Raveen Jayasuriya 1 , Lucy Amos 1 , Rye Yap 1 , Michael Athanassacopoulos 1 , Lee Breakwell 1 , Neil Chiverton 1 , Ashley Cole 1 , Marcel Ivanov 1 , Rex Michael 1 , Shreya Srinivas 1 , and James Tomlinson 1
1 Sheffield Teaching Hospitals NHS Foundation Trust, Spinal Surgery Service, Sheffield, United Kingdom
Introduction: In the United Kingdom’s National Health Service the structure of a regular healthcare team is no longer the case. There are an increasing number of junior doctors, nurses and physiotherapists cross-covering speciality teams, and increasing use of locum staff and regular shift changes. Comprehensively documented post-operative care instructions are more imperative than ever to ensure patient safety, enhance recovery, and even potentially reduce length of stay after major spinal surgery.The Royal College of Surgeon’s Good Surgical Practice guide promotes “Detailed post-op care instructions”, but no published standard exists for what minimum “detail” is required. In a speciality as highly litigious as spinal surgery, we as a community should have minimum standard for post-operative care documentation. This quality improvement project demonstrated how we used 4 audit cycles, reviewing 200 operations notes, over a 24 months period to make a simple and effective change to our centre’s post-operative care documentation practices. Methods: 1) identify the minimum dataset expected in post-operative care documentation, 2) audit our current practice, 3) successfully implement a change department wide, 4) re-audit at 3, 12 and 24 months post-implementation, 5) questionnaire to review change implemented. Results: Stage 1: A consensus from all 7 consultant spinal surgeons identified 15 criteria, including important negatives, deemed as mandatory in all major elective and trauma spinal post-operative care documentation. Stage 2: Baseline audit (n = 50 operation notes) observed >75% compliance in only 4 criteria, 50-75% compliance in 1 criterion, and <50% compliance for 10 criteria. This data was presented to the 7 consultants, and the unexpected poor documentation compliance justified Stage 3. Stage 3: A post-operative instruction template was designed based on the 15 key criteria, which could be embedded within the existing IT system. It allowed continued use of existing operative templates, with the addition of a non-overwriting suffix requiring only two mouse clicks. Existing templates were not overwritten to respect autonomy. Template had a “delete as appropriate” format. Stage 4: Re-audit at 3 months demonstrated improved compliance to >75% in 7 criteria, and 50-75% compliance in 7 criteria, and <50% in 1 criterion. Re-audit cycle at 12 months showed that compliance has not only been maintained but continued to improve, with >75% compliance in 8 criteria, and 50-75% compliance in 7 criteria. Feedback from ward staff (Juniors Doctors/Nurses/Physiotherapists) was highly supportive of the template introduced. Re-audit at 24 months demonstrated compliance of >75% in 7 criteria, and 50-75% compliance in 8 criteria. This subtle decline prompted Stage 5. Stage 5: Questionnaire of template usage identified problems criteria response options, and lack of awareness of template by newly appointed consultants and registrars. Conclusion: We successfully changed documentation practices by a) achieving a consensus first, b) a “shock and awe” moment to highlight existing poor documentation, c) implementing a change which fit easily into existing systems, d) respecting autonomy rather than enforcing change and e) an iterative process to ensure template was fit for purpose. We recommend our 15-point template as a step towards standardisation of post-operative care documentation.
OP05: Degenerative Lumbar/Surgical Complications
343
A037: Risk Factors for Reoperation and Joint Replacement Surgery After Short-Segment Spinal Cord Surgeries for Lumbar Degenerative Disc Disease: A Population Based Cohort Study
Meng-Huang Wu 1 , Christopher Wu 2 , Jiann-Her Lin 3 , Ching-Yu Lee 1 , Tsung-Jen Huang 1 , Yi-Chen Hsieh 4 , and Li-Nien Chien 4
1 Taipei Medical University Hospital, Department of Orthopedics, Taipei, Taiwan
2 College of Medicine, Taipei Medical University, Taipei, Taiwan
3 Taipei Medical University Hospital, Neurosurgery, Taipei, Taiwan
4 Taipei Medical University, Taipei, Taiwan
Introduction: Short-segment lumbar spinal surgery is the most commonly performed procedure for treatment of degenerative disc disease. However, population-based data regarding reoperation and joint replacement surgeries after short-segment lumbar spinal surgery is limited. Material and Methods: The study was a retrospective cohort design using Taiwan National Health Insurance Research Database for data collection. Patients diagnosed with lumbar disc disease and first received lumbar discectomy between 2002 and 2013. The Kaplan-Meier method estimated the incidence of 1 year reoperation and joint replacement surgery. Cox proportional hazard regression examined risk factors associated with reoperation. Subgroup analysis were also performed for the reoperation. Results: A total of 90,105 patients received lumbar discectomy surgery (29,719 patients: fusion with fixation group, 2897 patients: fusion without fixation, 57,489 patients: non-fusion group). The incidence of 1 year reoperation and joint replacement surgery for hip and knee was .27, .04, and .04 per 100 person-month, respectively. Compared to fusion with fixation group, fusion without fixation and non-fusion group had a higher risk of reoperation, with an adjusted hazard ratio of 2.3 (95% confidence interval [CI]: 1.76-3.02) and 4.12 (95% CI: 3.57-4.76), respectively. Risk factors for reoperation include fusion without fixation, non-fusion surgery, age >45 years, male gender, diabetes, Charlson Comorbidity Index = 0, lowest social economic status, and steroid use history. Conclusion: Non-fusion surgery and spinal fusion without fixation had higher risk for reoperation compared to spinal fusion with fixation. Higher reoperation risk should be explained to patients who will receive non-fusion surgery even though the risk is low.
680
A038: Prevalence of Occult Infections in Primary Posterior Instrumented Spinal Susion
Jessica Dorilio1, Daniel Alicea1, Christina Dowe1, Tucker Callanan1, Nicole Utah1, Antonio Brecevich1, Fedan Avrumova1, Andrew Sama1, Darren Lebl 1 , Frank Cammisa 1 , and Celeste Abjornson 1
1 Hospital for Special Surgery, Spine Surgery, New York, USA
Introduction: Occult bacteria have been linked to deep and chronic infections in spine surgery. These organisms are commensal to dermal and deeper tissue layers, including the intervertebral disc and bone. This study assesses the colonization rate of occult bacteria from various layers traversed during standard surgical spine exposure. We hypothesize that standard surgical skin preparation nor preoperative antibiotics properly access and eradicate these organisms prior to primary spine surgery. Methods: Fifty-four consecutive patients undergoing primary instrumented lumbar spine surgery were prospectively enrolled. All patients received preoperative antibiotics and skin preparation with povidone-iodine (Betadine) or chlorhexidine-gluconate (ChloraPrep). Culture samples were subsequently obtained from the superficial skin, dermal wound-edge following incision, hypodermis, and the vertebral pedicle prior to instrumentation implantation. Control culture samples were taken from the scalpel prior to incision. Results: A total of 525 culture samples were obtained, and samples were positive in 33.3% of patients (18/54). Culture-positive patients had on average 3.1 positive samples per case. Superficial skin samples were positive in 13.0% (n = 7), dermal layer samples in 16.7% (n = 9), hypodermis samples in 13.0% (n = 7), and vertebral samples in 20.4% (n = 11) of cases. All control samples taken of the scalpel prior to incision were culture-negative. C. acnes was the most common organism isolated, in 83.3% of culture-positive cases. Factors protective against positive culture results included female gender (P = .007; odds ratio, .06; 95% confidence interval, .01-.43) and ChloraPrep utilization (P = .014; odds ratio, .04; 95% confidence interval, .01-.39). Discussion: Occult bacteria was detected in one third of patients undergoing primary instrumented spine surgery. Deep culture samples of the vertebral pedicle were more often positive than dermal layer samples. The data collected supports our hypothesis that occult bacteria persist in the skin and deeper tissue layers perioperatively, regardless of the efforts made by preoperative skin preparation and prophylactic antibiotics.
1193
A039: Reoperation and Long-Term Clinical Consequences Following Single-Segment Surgery for Meyerding Grade 1 Degenerative Lumbar Spondylolisthesis
Andrew Chan 1 , Erica Bisson 2 , Mohamad Bydon 3 , Steven Glassman 4 , Kevin Foley 5 , Christopher Shaffrey 6 , Eric Potts 7 , Mark Shaffrey 8 , Domagoj Coric 9 , John Knightly 10 , Paul Park 11 , Michael Wang 12 , Kai-Ming Fu 13 , Jonathan Slotkin 14 , Anthony Asher 9 , Michael Virk 13 , Panagiotis Kerezoudis 3 , Mohammed Alvi 3 , Jian Guan 2 , Regis Haid 15 , and Praveen Mummaneni 1
1 University of California, San Francisco, San Francisco, USA
2 University of Utah, Salt Lake City, USA
3 Mayo Clinic, Rochester, USA
4 Norton Leatherman Spine Center, Louisville, USA
5 Semmes-Murphey Neurologic and Spine Institute, Memphis, USA
6 Duke University, Durham, USA
7 Goodman Campbell Brain and Spine, Indianapolis, USA
8 University of Virginia, Charlottesville, USA
9 Carolina Neurosurgery & Spine Associates, Charlotte, USA
10 Atlantic Neurosurgical Specialists, Morristown, USA
11 University of Michigan, Ann Arbor, USA
12 University of Miami, Miami, USA
13 Weill Cornell Medical Center, New York, USA
14 Geisinger Health, Danville, USA
15 Atlanta Brain and Spine Care, Atlanta, USA
Introduction: There is conflicting evidence whether surgical approach (decompression alone versus decompression with fusion) impacts reoperation rates following surgery for lumbar spondylolisthesis. Here, we utilize the prospective QOD registry to investigate reoperations following surgery. Material and Methods: We studied 608 patients undergoing elective single-segment spine surgery for degenerative grade 1 lumbar spondylolisthesis. Baseline through latest follow-up data (at least greater than 2 years) were collected. Reoperations were recorded that were deemed related to the index surgery. Results: Four-hundred sixty eight (77.0%) patients underwent fusion [140 (23.0%) underwent decompression alone]. The overall reoperation rate was 6.9% (42 of 608 patients with 44 reoperations). There were a similar proportion of reoperations for decompression and fusion cohorts (9.3% vs 6.2%, P = .21). There were significantly more reoperations within 30 days for the fusion cohort (P = .02), whereas there were significantly more reoperations from 30 days to 1 year for the decompression cohort (P = .01). There were no significant differences at other time points (P > .05). In adjusted analyses, reoperations were independently associated with a decreased odds of reaching ODI minimal clinically important difference (MCID) (defined as 14.3 improvement) (adjusted OR = .4, 95%CI(.2-.7), p = .003), inferior change in ODI (adjusted β = 10.1, 95%CI(4.5-15.7), P < .001), NRS Back Pain (NRS-BP) (adjusted β = 1.1, 95%CI(0.1-2.1), p = .03), NRS Leg Pain (NRS-LP) (adjusted β = 1.6, 95%CI(.6-2.5), P < .001), EQ-5D (adjusted β = -.07, 95%CI(-.14- -.003), P = .04), and NASS Satisfaction (adjusted OR = 3.1, 95%CI(1.7-5.5), P < .001) at latest follow up. In a subgroup analysis of the cohort receiving decompression and fusion, reoperations remained independently associated with a decreased odds of reaching ODI MCID (adjusted P = .001), lower NASS satisfaction (adjusted P = .003), and inferior change in ODI (adjusted p < .001), NRS-BP (adjusted P = .006), NRS-LP (adjusted P < .001), and EQ-5D (adjusted P = .001). For the subgroup receiving decompression alone, reoperation occurrence was not associated with significantly different outcomes at 24 months (adjusted p > .05, all comparisons). Conclusion: Twenty-four months following surgery, decompression surgery alone was associated with a higher reoperation rate (9.3% vs 6.2%) compared to decompression with fusion, though the result was not statistically significant. Fusions had a higher rate of reoperation 30 days following surgery, whereas decompression surgery had a higher rate between 30 days and 1 year. Reoperations, particularly when they occur for patients receiving decompression and fusion, negatively impacted patient satisfaction.
1430
A040: The Effect of Total Hip Arthroplasty on Lumbar Pain and Sagittal Balance of the Spine: A Prospective Observational Study
Helder Fonte 1 , Melissa Silva 2 , Carolina Luísa Lemos 2 , and Ricardo Rodrigues-Pinto 1,2
1 Spinal Unit (UVM), Department of Orthopaedics, Centro Hospitalar Universitário do Porto, Porto, Portugal
2 Instituto de Ciências Biomédicas Abel Salazar, Porto, Portugal
Introduction: Hip-Spine Syndrome (HSS) can occur in patients with back pain symptoms secondary to pathological changes in the hip. Patients develop a fixed flexion of the hip, pelvic anteversion and lumbar hyperlordosis, leading to dislocation or overload on the posterior lumbar facets which is responsible for pain due to the mechanical stress. This paper aims to prospectively evaluate the effect of hip arthroplasty on hip and back pain and to analyze the sagittal balance of the spine in patients submitted to hip arthroplasty. Material: A prospective study was carried out to evaluate the changes in lumbar pain and sagittal balance on patients undergoing total hip arthroplasty. Clinical and radiographic data were collected preoperative and at 2, 6 and 12 months postoperative, using Visual Analog Scale (VAS) to assess hip and low back pain, Harris Hip Score (HHS) and Oswestry Disability Index (ODI). The radiographic evaluation included the measurement of pelvic index (PI), pelvic tilt (PT), sacral slope (SS) and sagittal vertical axis (SVA). Results: Thirty-one patients were included. Hip VAS score decreased from 7.45 ± 1.39 preoperative to 4.58 ± 1.03 (P < .001) at 2 months and to 2.95 ± 2.04 (P = .006) at 12 months. Low back VAS decreased from 5.74 ± 2.02 preoperative to 4.48 ± 1,29 at 2 months (P < .001) and to 3.09 ± 2.37 at 12 months (P = .023). HHS had an average value of 44.35 ± 9.74 preoperative increasing to 55.00 ± 10.81 (P < .001) at 2 months and to 72.25 ± 13.24 (P < .001) at 12 months. ODI revealed a pre-operative average disability of 45.03 ± 11.90 with a decrease to 35.94 ± 10.50 (p < .001) at 2 months and to 21.10 ± 15.94 (P = .001) at 12 months. Radiographic pre-operative evaluation found a mean PI of 58.88° ± 14.36, PT of 18.12° ± 9.95, SS of 40.63° ± 6.95 and SVA of 19.47 ± 30.16 mm. At 2 months, PI (63.91° ± 11.51, P = .015) and SS (45.61° ± 7.85, P = .008) significantly increased. PT was 17.87° ± 7.81 (P = .446) and SVA had a tendency to increase (27.79 ± 28.87, P = .061). One year after the surgery, PI (52.38° ± 13.60, P = .004) and SS (36.89° ± 10.52, P = .001) had significantly decreased, as the vertical sagittal axis (11.57 ± 33.31 mm, P = .023). Conclusion: This study showed that patients suffering for concomitant severe primary hip osteoarthritis and low back pain show a significant improvement of low back pain and disability which continues to improve at 1 year. While no definitive conclusions can be drawn concerning sagittal spine alignment, SVA worsened in the first 2 months after hip arthroplasty, possibly because at this stage patients are still starting to discontinue walking aids, but significantly improved thereafter, obtaining a better sagittal alignment than pre-operatively. In conclusion, hip arthroplasty improves not only hip but also back pain and disability. Improvement in sagittal alignment may contribute to this clinical improvement.
1530
A041: Spinal Alignment Comparison for Lateral Versus Supine L5-S1 ALIF in the Treatment of Patients with Degenerative Conditions of the Lumbar Spine
Kaveh Khajavi 1 , Cristiano Menezes 2 , Brett Braly 3 , and J Alex Thomas 4
1 Georgia Spine & Neurosurgery Center, Atlanta, USA
2 Columna Institute, Belo Horizonte, Brazil
3 The Spine Clinic of Oklahoma City, Oklahoma City, USA
4 Atlantic Neurosurgical and Spine Specialists, Wilmington, USA
Introduction: Anterior lumbar interbody fusion (ALIF) is a widely accepted technique for lumbar fusion. The traditional ALIF (S-ALIF) approach utilizes a supine patient position with the surgeon approaching L5-S1 through a variety of incision starting points. With the introduction of lateral single-position surgery techniques that allow for lateral (e.g., XLIF) procedures from L4 5 and above and posterior pedicle screw fixation without prone patient repositioning, a modified ALIF via an anterolateral retroperitoneal approach (lateral ALIF [L ALIF]) permits access to L5 S1 to extend anterior column access from a single position across the thoracolumbar to sacral spine. Objectives: The objective of this multicenter, retrospective study was to assess differences in spinopelvic parameters (lumbar lordosis, segmental lordosis, restoration of disc space height, and reduction of spondylolisthesis (when present)) following L-ALIF as compared to S-ALIF at L5 S1. Methods: Radiographs from 479 consecutive patients who underwent L5-S1 L-ALIF (n = 317) or S ALIF (n = 162) for degenerative lumbar conditions were included. Patients treated at L4-5 and above with other single-position interbody fusion and posterior fixation techniques were included in the analysis. Lumbar lordosis, L5-S1 segmental lordosis, L5-S1 disc space height, and reduction of L5-S1 spondylolisthesis were measured on preoperative and postoperative lateral X-ray images. Of the 479 patients included in this study, 276 (58%) patients were female, the mean age at surgery was 56.9 years, and the mean body mass index was 29.5 kg/m2. Results: From preoperative to postoperative, mean lumbar lordosis improved by 5.0° and 4.9° in L ALIF and S ALIF groups, respectively (P = .874). Over the same period of time, the mean L5-S1 segmental lordosis also improved by 6.4° and 4.9° in L-ALIF and S ALIF groups, respectively (P = .1149). The L5-S1 disc space height also increased from preoperative to postoperative by 6.5 mm and 6.3 mm in L-ALIF and S-ALIF groups, respectively (P = .596) and the spondylolisthesis slip reduced by 1.4 mm and 2.2 mm in L ALIF and S ALIF groups, respectively (P = .146). Conclusion: The results of this study show that L5-S1 ALIF in both lateral and supine positions led to postoperative improvement in segmental lordosis, overall lumbar lordosis, restoration of disc space height at L5 S1, and reduction of spondylolisthesis. Overall improvement in radiographic outcomes following both L-ALIF and S-ALIF procedures suggests that L-ALIF appears to be a reasonable alternative to S-ALIF for L5 S1 interbody fusions. Further, these results suggest that single-position techniques (e.g., XLIF and ALIF and posterior fixation, all in the lateral position) result in substantially.
678
A042: The Impact of Modifiable Risk Factors on Post-Operative Complications Following Lumbar Spine Fusion
Andy Ton 1 , Shane Shahrestani 1 , Xiao Chen 1 , Alexander Ballatori 1 , Jeffrey C. Wang 1 , and Zorica Buser 1
1 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
Introduction: The increasing prevalence of lumbar spinal fusion has been accompanied by an increase in costly and untimely readmissions. Many studies emphasize perioperative and intraoperative care, few highlight the role of modifiable risk factors on postoperative outcomes in spine surgery. Therefore, this study explores the impact of modifiable risk factors (MRFs) on complications, costs, and readmission rates at 30, 90, and 180 days following lumbar spine fusion. Material and Methods: In a retrospective cohort analysis, patients with lumbar spine fusions were identified within the 2016-2017 Nationwide Readmissions Database (NRD) using ICD-10 codes. Patients were stratified by the following MRFs: Alcohol use, tobacco/nicotine use, malnourishment, dyslipidemia, and primary hypertension. ICD-10 codes for MRFs were confirmed through comparison with prior studies analyzing MRFs. Differences in complications, non-elective readmission rates, costs, and length of stay (LOS) were compared between MRFs and the non-MRF group. Exclusion criteria included surgical indications for trauma and neoplasms and malabsorption syndromes. Statistical analysis was conducted using Tukey multiple comparisons of means, one-way ANOVA, Wald testing, and unpaired Welch two-sample t-tests. Predictive modeling was performed to demonstrate increased risk of readmission per additional MRF. Results: The final analysis included 297,579 patients (56.5% female, 43.5% male) with an overall mean age of 56.72 + 16.53 years. At 30 and 90 days, patients with malnutrition (6.57%, P = .016; 12.87%, P < .001), dyslipidemia (6.26%, P < .001; 10.78%, < .001), and primary hypertension (6.07%, P < .001; 10.26%, P < .001) had significantly greater readmission rates than patients without MRFs (4.84%; 8.01%). At 180 days readmission, all MRFs had significantly greater readmission rates relative to patients without MRFs (11.01%) as shown: alcohol use (18.06%, p = .018), tobacco/nicotine use (13.22%, P = .002), malnourishment (18.47%, P < .001), dyslipidemia (15.37%, P < .001), and primary hypertension (14.50%, P < .001). The dyslipidemia cohort demonstrated significantly greater rates of myocardial infarction (MI) and acute kidney injury (AKI) at 30 days compared to patients without MRFs, primary hypertension, and tobacco/nicotine use (all P < .001) and at 90 and 180 days compared to all MRF groups (all P < .05). Alcohol usage was associated with a significantly greater mortality rate compared to all MRF groups at 90 days (all P < .05). The average LOS and cost of index admission was significantly different between all groups (P < .001) except when comparing dyslipidemia and the non-MRF group. Malnutrition was associated with the highest average LOS (9.07 + 13.29 days) and cost of index admission ($59,936 + $57,341 USD). Predictive modeling showed increases of 0.77%, 1.70%, and 2.44% risk of readmission at 30, 90, and 180 days respectively per additional MRF (all P < .001). Conclusion: These findings highlight the negative impact each MRF has on postoperative outcomes following lumbar spinal fusion. Further longitudinal research using prospective multicenter data is necessary to comprehensively outline the effects of various MRFs on lumbar spine fusion outcomes.
535
A043: Responsiveness of Depression and its Influence on Surgical Outcomes of Lumbar Degenerative Disease
Asdrubal Falavigna 1 , Orlando Righesso Neto 2 , Alisson R. Teles 2 , Sabrina Busnello 2 , and Yan Assunção Bicca 2
1 University of Caxias do Sul (UCS), Health Sciences Postgraduate Program, Caxias do Sul, Brazil
2 University of Caxias do Sul (UCS), Cell Therapy Laboratory and Clinical Studies and Basic Models of Spinal Disorders Laboratory, Caxias do Sul, Brazil
Introduction: an association between spinal disorders and psychological disturbances has been reported in recent years. Also, the presence of preoperative depression has been shown to negatively affect surgical outcomes for spine surgery. Surgical treatment of spine disease may contribute to the capacity to recover from depression. Given the importance of identifying prognostic factors for patients undergoing spine surgery, the present study aims to demonstrate the responsiveness of depression after surgery for lumbar degenerative disease and to verify the impact of this condition on surgical outcomes. Material and Methods: a prospective cohort study with 91 patients with lumbar degenerative diseases who were evaluated preoperatively, at 30 days and 1 year postoperatively. Primary outcome measure was the evolution of depression between the follow-ups and its correlation with satisfaction. Depression was assessed with Beck Depression Inventory. According to depression responsiveness, patients were classified into four groups: NN = no depression; ND = normal during the preoperative period and depression within 1 year; DN = depression during the preoperative period and normal within 1 year; DD = depression during the preoperative period and within 1 year. Results: prevalence of preoperative depression was 28.6 % and 17.6 % within 1 year postoperatively. Most patients (65.4 %) with depression in the preoperative period recovered postoperatively. Poor preoperative health-related quality of life (HRQoL) measures were associated with higher rates of responsiveness of depression during the follow-up. Patients with depression at the 1 year postoperative follow-up had a worse functional outcome. Patients who improved from depression had similar outcome to those without depression. Dissatisfaction within 1 year postoperatively was greater in patients who become depressed after surgery and remain depressed at 1 year follow-up (NN = 8.8 %; ND = 42.9 %; DN = 17.6 %; DD = 44.4 %; P = .012). Conclusion: most patients with depression in the preoperative recover within 1 year postoperatively. Responsiveness of depression is associated with surgical outcomes. The presence of depression after the surgical treatment, independent of when it starts, had a major negative impact on prognosis.
1644
A044: Physical Therapy on Postoperative Day Zero Following Lumbar Spine Surgery Decreases Length of Stay
Blaine Manning 1 , Casey Fogarty 1 , Suryanshi Rawat 1 , Stefan Hanish 1 , Andy Lee 1 , Ahdarsh Vallabhaneni 1 , Nathan Cherian 1 , Muhammad Mirza 1 , Theodore Choma 1 , and Don Moore 1
1 University of Missouri-Columbia, Department of Orthopaedic Surgery, Columbia, USA
Introduction: Postoperative length of stay (LOS) is a major factor in overall cost for lumbar spine surgery, and its duration often depends on discharge clearance from physical therapy (PT). The study goal was to compare postoperative LOS for lumbar spine surgery patients who initiated formal PT on POD 0 versus POD 1. Methods: A retrospective review was conducted of 1870 patients who underwent elective 1-2 level laminectomy +/- posterior lumbar fusion +/- instrumentation by 13 spine surgeons at 1 institution from 2011-2019. Patients were categorized by timing of postoperative PT, with POD 0 defined as within 24 hours after surgery. Patients were excluded if they had incomplete data, admitted under a trauma visit, admitted to the ICU between surgery and discharge for observation or complications, did not see PT before discharge, or had qualifying surgery at >2 levels. Demographics, perioperative variables, and postoperative variables were collected. Statistical methods for categorical bivariate analysis included Chi-square test of independence and Fisher’s Exact test, if Chi-square assumptions were not met. For continuous outcomes, normality was tested using a Shapiro-Wilk test and a two-sample t-test or Wilcoxon Rank Sum test was used to determine differences across POD groups. Data were analyzed using R with two-sided P < .05 considered significant. Results: Of 1870 patients, 336 met inclusion criteria. Formal PT was initiated on POD 0 for 202 patients, and POD 1 for 134 patients. There was no significant difference between POD 0 and POD 1 groups (respectively) regarding: age (57.9 +/- 14.4 years vs 58.4 +/- 14.3 years, P = 1.00), gender (45.5% male vs 52.2% male, P = .28), insurance type (42.1% Medicare vs 44% Medicare, P = .58), BMI (33.2 +/- 7.8 kg/m2 vs 31.7 +/- 5.8 kg/m2, P = .23), or discharge destination (home discharge 88.6% vs 85.1%, P = .61). The difference in LOS (9.9 hours) was large enough to be of statistical and clinical significance (P = .000001214) (median 65.3 hours for POD 0 PT [interquartile (IQ) range, 43.7-74.6] vs 74.2 hours for POD 1 PT [IQ range 51.6-99.8]; p = .000001214). The difference in distribution of postoperative nights spent in the hospital was also clinically and statistically significant between POD 0 and POD 1 groups, respectively (p = .002265922) (1 night stay 21.3 % vs 8.3%, 2-3 night stay 56.4% vs 54.9%, 4 or more nights 22.3% vs 36.8%). Conclusion: Early initiation of PT has been proposed to facilitate discharge following lumbar spine surgery. In our study, lumbar spine patients who initiated physical therapy (PT) on postoperative day (POD) 0 demonstrated clinically and statistically significant earlier discharge than patients who initiated PT on POD 1. Given the role of LOS in quality metrics and reimbursement, it remains important for orthopedic spine surgeons to optimize postoperative LOS. A multidisciplinary approach which includes physical therapists, along with early formal postoperative PT, may facilitate discharge following lumbar spine surgery.
1864
A045: Preoperative Cross-Sectional Area of Psoas Muscle Impacts Short-Term Functional Outcomes After Posterior Lumbar SuSrgery
Hikari Urakawa 1 , Kosuke Sato 1 , Avani Vaishnav 1 , Ryan Lee 1 , Chirag Chaudhary 1 , Jung Kee Mok 1 , Yoshihiro Katsuura 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
Introduction: The decrease of psoas cross-sectional area has been reported to be a predictor of increased risk of mortality and complications in various surgery including spine surgery. However, it is unclear which level should be selected to measure it on MRI and whether the psoas size impacts postoperative functional outcomes in lumbar surgery. The aim of this study was to (1) elucidate the optimal level for the measurement by examining the inter-rater reliability at each level and (2) investigate the impact of psoas cross-sectional area on short-term functional outcomes of posterior lumbar surgery. Material and Methods: Patients who underwent minimally invasive posterior lumbar surgery for degenerative diseases with more than 6 months follow-up were included in this study. The cross-sectional area of psoas muscle was measured at each intervertebral level on T2-weighted axial images of preoperative MRI by 2 observers. Normalized total psoas area (NTPA) was calculated as total psoas area normalized to patient height. Intraclass Correlation Coefficient (ICC) was calculated to evaluate inter-rater reliability of NTPA at each level. Patient reported outcome measures (PROMs) including ODI, VAS (back, leg), SF-12 (PCS, MCS) and PROMIS were collected at pre-op, 2 weeks, 6 weeks, 3 months and 6 months. Results: The total of 215 patients were included in this study. ICC was the highest at L3/4. [ICC .983 (95%CI .973-.989) at L1/2, .991 (95%CI .986-.994) at L2/3, .992 (95%CI .987-.994) at L3/4 and .928 (95%CI .893-.952) at L4/5]. Patients were divided into 2 groups [Lower NTPA group (LG) and Higher NTPA group (HG)] at the point of the sex-specific lowest quartile of NTPA at L3/4 threshold. There were no significant differences in preoperative PROMs except for SF-12 MCS, however they were significantly worse in the Low NTPA group at 6vmonths [ODI: LG 23.4 ± 19.9 vs HG 15.0 ± 15.2, P = .014; VAS back: LG 2.8 ± 2.5 vs HG 2.0 ± 2.3, P = .048; VAS leg: LG 2.5 ± 2.5 vs. HG 1.5 ± 2.2, P = .003; SF-12 PCS: LG 39.7 ± 10.9 vs HG 44.2 ± 10.3, P = .012; PROMIS PF: LG 43.9 ± 9.9 vs HG 47.0 ± 8.7, P = .026)]. In terms of SF-12 MCS, preoperative score was significantly better in the low NTPA group, however, no significant differences were found at all postoperative points. Multivariate logistic regression showed low NTPA was an independent predictor of high ODI (OR = 2.50; 95% CI, 1.23-5.08; P = .011) and VAS leg (OR = 3.85; 95% CI, 1.68-8.81; p = .001) at 6 months. Conclusion: The decrease of psoas cross-sectional area on preoperative MRI had a negative impact on short-term functional outcomes of posterior lumbar surgery for degenerative diseases. Low NTPA was an independent predictor of high ODI and VAS leg at 6 months. NTPA, which is a highly reliable and easy to assess, may be useful for a decision making for more effective treatment based on muscle health in each patient.
OP06: Adult Deformity-Surgical Management
360
A046: Acute Failure of S2-Alar-Iliac Pelvic Fixation Following Adult Deformity Correction
Christopher Martin 1 , David Polly 1,2 , Kenneth Holton 1 , Jose San Miguel-Ruiz 1 , Melissa Albersheim 1 , Paul Lender 1 , Jonathan N. Sembrano 1 , Matthew Hunt 2 , and Kristen Jones 2
1 University of Minnesota, Department of Orthopaedic Surgery, Minneapolis, USA
2 University of Minnesota, Department of Neurosurgery, Minneapolis, USA
Introduction: Pelvic fixation with S2-alar-iliac (S2AI) screws is a widely accepted technique to anchor thoracolumbar constructs in adult deformity surgery. Compared to traditional iliac screws, S2AI screws have been reported to have lower rates of reoperation and wound complications. To our knowledge, there are no prior published reports of acute failure mechanisms of S2AI instrumentation. Material and Methods: We performed a retrospective review of all fusion surgeries extending from L2 or higher with instrumentation to the pelvis in which S2AI screws were placed with at least 6 months follow-up between 3/2017 and 6/2019. We excluded patients under 18 years of age and non-ambulatory patients. Acute instrumentation failure was defined as any case requiring revision of the pelvic fixation within 6 months from the index surgery. We reviewed the demographic and surgical characteristics of each patient, and reviewed pre-operative and 6 week post-operative radiographs to document the change in their deformity parameters as well as for the presence of a transitional lumbo-sacral segment. Results: Failure occurred in 6 of 125 cases (5%), and consisted of either slippage of the rods or displacement of the set screws from the S2AI tulip head, with resultant kyphotic fracture. All occurred within 6 weeks post-operatively. Revision with a minimum of 4 rods connecting to 4 pelvic fixation points was successful. 2 of 3 (66%) patients revised with less fixation sustained a second failure. Failure patients were younger (56.5 years v. 65 years, p = .03). The magnitude of surgical correction was higher in the failure cohort (number of levels fused, change in lumbar lordosis, change in T1-Pelvic Angle, and change in coronal C7 vertical axis, each P < .05). In the multivariate analysis, younger patient age and change in lumbar lordosis were independently associated with increased failure risk (P < .05 for each). There was a trend towards the presence of a transitional S1-2 disc being a risk factor (OR = 8.8, 95% CI .93-82.6). Failure incidence was the same across implant manufacturers (P = .3). Conclusion: All failures involved large magnitude correction and resulted from stresses that exceeded the failure loads of the set plugs in the S2AI tulip, with resultant rod displacement and kyphotic fractures. Patients with large corrections may benefit from four total S2AI screws at the time of the index surgery, particularly if a transitional segment is present. Salvage with a minimum of 4 rods and 4 pelvic fixation points can be successful.
1098
A047: Patient Reported Outcomes After Complex Adult Spinal Deformity Surgery: 5 year Follow-Up Results of the Scoli-RISK-1 Study
Scott Zuckerman 1 , Meghan Cerpa 1 , Lawrence Lenke 1 , Christopher Shaffrey 2 , Justin Smith 3 , Leah Carreon 4 , Kenneth Man Chee Cheung 5 , Michael Kelly 6 , Michael Fehlings 7 , Christopher Ames 8 , Oheneba Boachie-Adjei 9 , Mark Dekutoski 10 , Khaled Kebaish 11 , Stephen Lewis 12 , Yukihiro Matsuyama 13 , Ferran Pellisé 14 , Yong Qiu 15 , and Frank Schwab 16
1 Columbia University Medical Center, New York, USA
2 Duke, Raleigh, USA
3 University of Virginia, Charlottesville, USA
4 Norton Health, Louisville, USA
5 The University of Hong Kong, Hong Kong, China
6 Washington University, St. Louis, USA
7 University of Toronto, Toronto, Canada
8 University of California San Francisco, San Francisco, USA
9 The FOCOS Hospital, Patang West, Ghana
10 Marshfield Clinic Eau Claire Center, Eau Claire, USA
11 Johns Hopkins, Baltimore, USA
12 University of Toronto, Toronto, USA
13 Hamatsu University, Hamamatsu, Japan
14 Hospital Universitari Vall d’Hebron, Barcelona, USA
15 Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, China
16 Hospital for Special Surgery, New York, USA
Summary: Comparing baseline to 5 year data following complex adult spinal deformity (ASD) surgery, significant improvement was seen in ODI, SF-36 PCS/MCS, SRS-22, and NRS-back pain. In long-term follow-up, durable and sustained improvement was seen at 5 years in nearly all PROs however, at 5 years NRS leg pain scores were similar to baseline. Hypothesis: To prospectively evaluate patient-reported outcomes (PROs) up to 5 years after complex ASD surgery. Study Design: Prospective, multicenter, international, observational Scoli-RISK-1study. Introduction: Long-term patient-reported outcomes (PROs) after complex adult spinal deformity (ASD) are important yet sparsely reported. Methods: The Scoli-RISK-1 study enrolled 272 ASD patients undergoing surgery from 15 centers. Inclusion criteria was Cobb angle of >80, corrective osteotomy for congenital or revision deformity, and/or 3-column osteotomy. The following PROs were measured prospectively at intervals up to 5 years: ODI, SF-36 PCS/MCS, SRS-22, NRS back/leg. Comparisons were made from baseline to, 2 years, and 5 years postoperative. Mixed effects models were used for analysis in order to account for those lost to follow-up. Results: Of the 272 patients enrolled, 217 (79.8%) and 77 (28.3%) were seen at 2 years and 5 years. postoperative respectively. 7 Comparing 5 year to baseline data, significant improvement was seen in ODI (31.8 vs 45.7, P < .001), SF-36 PCS (38.3 vs 31.8, P < .001), SF-36 MCS (46.6 vs 42.6, P = .003), SRS-22 (3.46 vs 2.71, P < .001), NRS back pain (3.22 vs 5.99, P < .001). Even though we could see significant improvement in NRS leg pain at 6 weeks, 6 months, and 2 years postoperative (2.46, 2.54, 2.78; P < .001) at 5 years NRS leg pain was similar to baseline (3.53 vs 3.79, P = .844). Conclusion: In long-term follow-up of complex ASD surgical patients, durable and sustained improvement was seen at 5 years postoperative in nearly all PROs, including ODI, SF-36 PCS/MCS, SRS-22, and NRS-back pain; however, at 5 years postoperative NRS leg pain scores were similar to baseline. Take Home Message: 5 years postoperative in complex ASD patients, significant improvement was seen ODI, SF-36PCS/MCS, SRS-22, and NRS-back-pain compared to baseline. Sustained improvement was seen in nearly all PROs except NRS-leg-pain at 5 years.
1106
A048: Lower Extremity Motor Scores (LEMS) After Complex Adult Spinal Deformity Surgery: 5 year Follow-Up of the Scoli-RISK-1 Study
Lawrence Lenke 1 , Meghan Cerpa 1 , Scott Zuckerman 1 , Christopher Shaffrey 2 , Justin Smith 3 , Leah Carreon 4 , Kenneth Man Chee Cheung 5 , Michael Kelly 6 , Michael Fehlings 7 , Christopher Ames 8 , Oheneba Boachie-Adjei 9 , Mark Dekutoski 10 , Khaled Kebaish 11 , Stephen Lewis 12 , Yukihiro Matsuyama 13 , Yong Qiu 14 , Ferran Pellisé 15 , and Frank Schwab 16
1 Columbia University Medical Center, New York, USA
2 Duke, Raleigh, USA
3 University of Virginia, Charlottesville, USA
4 Norton Health, Louisville, USA
5 The University of Hong Kong, Hong Kong, China
6 Washington University, St. Louis, USA
7 University of Toronto, Toronto, Canada
8 University of California San Francisco, San Francisco, USA
9 The FOCOS Hospital, Patang West, Ghana
10 Marshfield Clinic Eau Claire Center, Eau Claire, USA
11 Johns Hopkins University, Baltimore, USA
12 University of Toronto, Toronto, USA
13 Hamamatsu University School of Medicine, Hamamatsu, Japan
14 Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, China
15 Hospital Universitari Vall d’Hebron, Barcelona, Spain
16 Hospital for Special Surgery, New York, USA
Summary: At 5 years postoperative from complex ASD surgery there was no significant changes in LEMS compared to baseline. Mean LEMS remained stable following the 6 months visit at both 2 and 5 years follow-up for all patients reviewed. However, 8/75 (10.7%) patients did experience a worsening in LEMS in the 2-5 year period. These results highlight the importance of long-term follow-up to 5 years postoperative to truly evaluate neurologic motor function following complex ASD surgery. Hypothesis: To prospectively evaluate lower extremity motor function (LEMS) before and at 5 years following surgical correction of complex ASD. Study Design: Prospective, multicenter, international observational study (Scoli-Risk-1). Introduction: Neurologic complications after surgery for complex adult spinal deformity (ASD) are important, yet outcomes are heterogeneously reported and long-term follow-up is sparse. Methods: The Scoli-RISK-1 study enrolled 272 ASD patients undergoing surgery from 15 international centers. Inclusion criteria was Cobb angle of >80°, corrective osteotomy for congenital or revision deformity, and/or 3-column osteotomy (76% of all patients). Change in LEMS over a 5 year follow-up was analyzed. Results: Of the 272 patients, follow-up rates were: 271 (99.6%) discharge, 260 (95.6%) 6 weeks, 255 (93.8%) 6 months, 217 (79.8%) 2 year, and 77 (28.3%) 5 years postoperatively. Comparing all patients who returned for follow-up, rates of postoperative LEMS decline compared to preoperative function were 23.0% at discharge, 17.1% at 6 weeks, 9.9% at 6 months, 10.0% at 2 years and 9.3% at 5 years. At 5 years there was no significant changes in LEMS compared to baseline (49.0 vs 48.4 P = .163). Mean LEMS remained quite stable following the 6 months visit at both 2 and 5 years follow-up (49.0 vs 48.7 vs 49.0). However, 8/75 (10.7%) patients did experience a worsening in LEMS in the 2-5 years follow-up period. Conclusion: After complex ASD surgery, mean LEMS function stabilized after 6 months postoperative until the 5 year follow-up with 10.0% of returning patients still having lower LEMS than preoperatively. In addition, subtle LEMS decline occurred in 10.7% of returning patients during the 2 year to 5 year follow-up period. These results document long-term 5 year follow-up of LEMS following complex ASD surgery and the importance of assessing both individual and group average LEMS. Take Home Message: No significant changes in LEMS were seen at 5 years-postop as mean LEMS stabilized at 6 months, 2 and 5 years follow-up. However, 10.7% of individual patients experienced worsening in LEMS in the 2-5 years-period.
1403
A049: Evaluation of the Reliability and Reproducibility of Roussouly Classification for Lumbar Lordosis Types
Camila Yamazato 1 , Gustavo Ribeiro 2 , Fábio Chaud de Paula 2 , Ramon Soares 2 , Paulo Daniel Sousa Santa Cruz 1 , Nelson Astur 2,3 , Delio E. Martins 2,4 , Marcelo Wajchenberg 1,2 , and Michel Kanas 1,2
1 Federal University of Sao Paulo, Ortopedia, São Paulo, Brazil
2 Hospital Israelita Albert Einstein, Ortopedia, São Paulo, Brazil
3 Santa Casa de Sao Paulo, Ortopedia, São Paulo, Brazil
4 Universidade Anhembi Morumbi, São Paulo, Brazil
Introduction: The type of lumbar lordosis is associated with symptoms, propensity to degeneration and post-surgical prognosis in adult patients. Roussouly et al. proposed a classification for types of lumbar lordosis in 2005, which is widely accepted both in research and in clinical practice. However, there is still a lack of validation for its reliability and reproducibility. The objective of the research was to determine the reliability and reproducibility, intra and interevaluator of Roussouly’s classification for the types of lumbar lordosis. Material and Methods: The measurements were made in 104 panoramic radiographs of the spine in lateral view, of male individuals aged between 18 and 40 years old. Using the Surgimap® software, six examiners with different levels of experience measured the spinopelvic angles and classified the type of lordosis according Roussouly’s classification. After 1 month, the measurements were taken again; intra and interevaluator agreements were calculated using the Kappa Fleiss test. Results: The study showed positive evidence regarding the reproducibility of the Roussouly classification, with the Kappa Fleiss test for intraevaluator agreement between reasonable to almost perfect (.307-.827), and interevaluator between moderate (.43) and reasonable (.369). The most experienced evaluators showed greater interevaluator agreement, ranging from substantial (.619) to moderate (.439). Conclusion: Roussouly et al. classification for lumbar lordosis types, demonstrated good reliability and reproducibility, as intra and interevaluator agreement was considered to be at least reasonable, reaching substantial to almost perfect levels in some situations. Evaluators with higher level of experience showed greater agreement.
1085
A050: Adult Degenerative Scoliosis Shares the Same Spino-Pelvic Alignment as Lumbar Adolescent Idiopathic Scoliosis: A CT-Based and Sex-Age Matched Controlled Analysis
Steven de Reuver 1 , Philip van der Linden 1 , Moyo Kruyt 1 , Tom Schlosser 1 , and René Castelein 1
1 University Medical Center Utrecht, Department of Orthopedic Surgery, Utrecht, The Netherlands
Introduction: The mechanical basis of spinal deformities is becoming better understood. Spino-pelvic morphology is recognized as the key regulator of spinal biomechanics. Recent research indicates that pelvic morphology plays a role in which spinal segments may become part of a scoliotic deformity, especially in different types of Adolescent Idiopathic Scoliosis (AIS). We hypothesize that the same mechanical influences may play a role in the development of Adult Degenerative Scoliosis (ADS), located in the lumbar spine. Therefore, we analyzed an existing database of total-body CTs obtained for indications not related to the spine, to accurately measure the differences in Pelvic Incidence (PI) in ADS patients and a sex-age matched non-scoliotic controls. Material and Methods: CT-scans of 202 subjects were analyzed: 101 ADS patients were matched to a control patient of the same sex and closest age. With multi-planar reconstruction the PI was measured as the angle between the line from the exactly superimposed femoral-heads-axis to the mid-point of the sacral endplate, and the perpendicular line from the mid-point of the sacral endplate. For this method, the intraclass correlation coefficients were .993 for inter- and .998 for intra-observer reliability. Results: Of the sex-age matched included subjects, the median age was 68-69 years and 57% were female. In ADS patients the mean Cobb angle was 21° ± 8° and ranged from 10° to 47. The PI was 54.1 ± 10.8 in ADS patients and 47.7 ± 10.8 in non-scoliotic controls (p < .001). There was no difference between sex, a weak correlation between age and PI in both groups (R = .197-.225; P = .024-.048) and no significant correlation between PI and the level of the apex (P = .880) and the length of the scoliotic curve (P = .440). Conclusion: De novo ADS develops predominantly in the lumbar spine. This current study showed that he PI in ADS patients is higher than in non-scoliotic controls, similarly to what is observed in lumbar AIS. This suggests a similar mechanical basis of both spine deformities. Spino-pelvic alignment predisposes certain areas within the sagittal curvatures of the spine to be more prone to develop a scoliotic deformity. Whether and during which phase in life this will occur, depends on the mechanical properties of the stabilizers of the spine, predominantly the discs.
919
A051: Intra-Operative Neurophysiological Monitoring Alters During Three-Column Osteotomy: Incidence and Risk Factors
Yong Qiu 1 , Benlong Shi 1 , Zezhang Zhu 1 , Dun Li 1 , Zhen Liu 1 , and Yang Li 1
1 Nanjing University Medical School, Najing, China
Introduction: The intra-operative iatrogenic neurological deficits are always essential concerns for patients undergoing posterior three-column osteotomy (3CO). However, the incidence and risk factors for intra-operative neurophysiological monitoring (IONM) alerts during 3CO are not clear. We aim to analyze the incidence and risk factors of IONM alerts in patients undergoing 3CO. Materials and Methods: Retrospective analysis of IONM outcomes in patients undergoing 3CO. Patients sample: A total of 551 patients (340 M, 211 F, 31.9 ± 15.5 years) with severe spinal deformity undergoing posterior 3CO were retrospectively reviewed. The coronal Cobb angle of main curve and sagittal global kyphosis (GK) were measured on pre-operative standing whole spinal x-rays. The neurological status at pre-operation, post-operation and the last follow-up was recorded and the Frankel scores were applied for assessment of neurological status. Surgical procedures and other factors associated with IONM alerts were analyzed. The IONM alerts were defined as somatosensory evoked potentials (SEPs) latency increased >10%, SEPs amplitude decreased >50%, or motor evoked potentials (MEPs) amplitude decreased >80%. Comparison analysis between patients with and without IONM alerts was performed by Chi-square test. Results: A total of 98 (17.8%) IONM alerts were reported during surgery, including 82 SEPs alerts and 91 MEPs alerts. Positive wake-up test was revealed in 57 (10.3%) patients even after prompt managements, and new neurological deficits were observed in 50 (9.1%) patients at immediate post-operation. Of the 50 patients with new neurological deficits at post-operation, the Frankel scores were A in 5 patients, B in 4, C in 9, D in 32. At the last follow-up, the Frankel scores improved from A to C in 1 patient, from B to D in 2, from C to D in 4, from C to E in 2, from D to E in 7. The Chi- square test showed that patients with congenital deformities, GK >90°, vertebral column resection (VCR) procedure, cervicothoracic/thoracic osteotomy, blood loss >3000 ml, pre-operative neurological deficit were at a higher risk of IONM alerts. Conclusions: The incidence of IONM alerts in patients undergoing 3CO was 17.8%. Congenital deformities, GK >90°, VCR, cervicothoracic/thoracic osteotomy, blood loss >3000ml and pre-operative neurological deficit indicated high risk of IONM alerts.
1208
A052: The Efficacy and Safety of Large Diameter Pedicle Screws in Adult Thoracolumbar Deformity
Paul Park 1 , James Lin 2 , Cole Morrissette 1 , Joseph Osorio 3 , Meghan Cerpa 1 , Ronald A. Lehman 1 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
2 Mount Sinai, New York, USA
3 University of California San Diego, San Diego, USA
Summary: With the use of the all-posterior approach, screw pullout strength is a critical factor in adult spinal deformity (ASD) surgical correction. In our series, using large diameter screws (96% ≥6.0 mm diameter) placed transpedicularly or juxtapedicularly can be safe without intraoperative complications. The increased diameter and pullout strength of these screws allows for excellent correction and maintenance over follow-up. Hypothesis: Placement of large diameter pedicle screws (≥6.0 mm) in the thoracolumbar (TL) spine in ASD surgery is safe and can be done without added complication. Study Design: Retrospective, Single-center. Introduction: Pedicle screw instrumentation is the foundation of posterior ASD surgery, and ensuring high screw pullout strength is critical, especially in osteoporotic bone. It is our practice to maximize screw diameter to optimize construct integrity. The operative strategy is to consistently use large diameter (≥6.0 mm) pedicle screws to expand the pedicle or place screws juxtapedicularly; however, placement of larger screws can be dangerous, especially in upper lumbar, upper thoracic, and previously instrumented pedicles, given proximity of adjacent structures. Methods: ASD patients undergoing a primary posterior instrumented fusion were included. Radiographic measurements included: major curve Cobb angle, coronal imbalance (CI), & sagittal vertical axis (SVA). Every implanted screw diameter & length was recorded. Apical pedicle diameters were measured on preoperative CT. Primary outcomes included: 1) intraoperative neuromontoring (IONM) changes and 2) revision surgery. Results: 19 pts and 543 pedicle screws were evaluated (28.6 screws/patient). Mean age was 49.6 years, levels was 13.8, and follow-up was 1.5 years, with 7 patients having >2 years follow-up. Screw analysis revealed: 4% 5.5 mm, 40% 6.0 mm, 24% 6.5 mm, 31% 7.0 mm or greater. Focusing on challenging levels, the average screw diameter at T4 = 6.2 mm, T5 = 6.2 mm, T6 = 6.1 mm, L1 = 6.3 mm. Average screw diameter at the concave apical pedicle was 1.7 mm greater than the pedicle diameter. Mean coronal Cobb of the major curve was 65.4, with Average correction of 75.4%. No IONM changes occurred due to screw placement. There were 2 revision surgeries, both for rod breakage/pseudarthrosis. Conclusion: In a series of 542 consecutive TL pedicle screws placed, 96% of screws were ≥6.0 mm & 56% were ≥6.5 mm. Screws placed at the concave pedicle were on average 1.7 mm greater than the pedicle diameter without any neurovascular complications. Large diameter screws can be safely and consistently placed throughout the TL spine in ASD patients, while achieving and maintaining excellent coronal correction of 75.4%. Take Home Message: In treatment of adult spinal deformity, large diameter screws wider than the native apical pedicle may be safely placed in the thoracolumbar spine for increased pullout-strength and optimal deformity correction.
226
A053: Clinical Outcomes of Cocygectomy for Coccydynia: A Single Institution Series with Mean 5 year Follow-Up
Neha Mulpuri 1 , Nisha Reddy 1 , Kylan Larsen 1 , Ankit Patel 1 , Bassel Diebo 2 , Peter Passias 3 , Lori Tappen 1 , Kevin Gill 1 , and Shaleen Vira 1
1 University of Texas at Southwestern Medical Center, Dallas, USA
2 SUNY Downstate Health Sciences University, Brooklyn, USA
3 NYU Langone Medical Center-Hospital for Joint Disease, New York, USA
Introduction: Coccygectomy is generally reserved for patients who have severe coccydynia despite conservative management. Prior studies consist of small patient groups, heterogenous techniques, and high wound complication rates (up to 22%). This study investigates our institution’s experience with coccygectomy using a novel “off-center” wound closure technique and analyzes prognostic factors for long term success. Material and Methods: Retrospective review of all patients that underwent coccygectomy between 2006 and 2019 at a single academic center was conducted. Demographics, symptomatology, mechanism of injury, attempted conservative management, prior non-operative coccydynia treatment, history of spine surgery prior to coccygectomy, coccyx morphology (Postacchini and Massobrio), and post-operative complications were collected. Pre-operative versus post-operative HRQOLs such as Oswestry Disability Index (ODI), Visual Analog Scale (VAS), PROMIS-29 scores, SF-12, EQ-5D were compared. Risk factors for surgical site infection were identified with logistic regression analysis and similarly, risk factors for failing to meet MCID for ODI, PROMIS-Physical function, and PROMIS-Pain interference were identified. Risk factors for remaining disabled after surgery (ODI <20) were investigated using a stepwise logistic regression. Patient characteristics associated with improvement in post-operative VAS scores and EQ-5D ‘health self-scores’ were identified using stepwise logistic regression and stepwise linear regression, respectively. Results: 173 patients (77% female, mean age = 46.56 years-old, mean follow-up 5.58 ± 3.95 years) underwent coccygectomy between 2006 and 2019. 111 patients had adequate imaging for classification of coccyx morphology. Type IV coccyx morphology (54.05 ± 12.73 years-old) patients were older compared to Type III (41.86 ± 12.03 years-old). The most common etiology of coccydynia was spontaneous/unknown (42.2%), closely followed by trauma/accident (41%). The most common conservative treatments for coccydynia included steroid injections (66.3%), analgesic medications (51.2%), and physical therapy (42.2%). Patients improved from pre-operative to post-operative with respect to ODI, VAS back pain, and several PROMIS-29 domains such as fatigue, sleep disturbance, satisfaction with social role, and pain interference. A patient characteristic identified as a predictor of disability (ODI > 20) post-operatively was older age (OR = 1.054, 95% CI 1.004 to 1.107). Patient characteristics identified as predictors of lower self-reported ‘health scores’ were history of prior spine surgery (ß = .651), coccydynia due to trauma (ß = .363), and women (ß = .264). Having no history of spine surgery to coccygectomy (OR = .161, 95% CI .031 to .844) predicted improved post-operative VAS back pain scores. No clinical outcome differences were demonstrated among the coccyx types (all P < .05). 16 patients (9.25%) had post-operative infections of the incision site. Post-operative infection successfully resolved after management with local wound care and antibiotics. Additionally, no significant association was found between post-operative wound infection and long term improvements in HRQOLs following surgery. Conclusion: This is the largest series of coccygectomy patients to date demonstrating long term improvements in patient-reported outcomes. Our cohort had a significantly lower wound infection rate of 9.42% which we attribute to an “off-center” closure technique. Patients should be counseled that their surgical history, along with age, gender, and etiology of pain can influence their probability of reaching a successful clinical outcome.
1192
A054: Iliac Screw Fixation Revisited: Improved Clinical and Radiological Outcomes Using a Modified Iliac Screw Fixation Technique
Alexander von Glinski 1 , Christopher Elia 1 , James G, Wiginton 1 , Darius Ansari 1 , Clifford Pierre 1 , Ronen Blecher 1 , Joseph R. Dettori 1 , Emre Yilmaz 1 , Thomas A. Schildhauer 1 , Rod Oskouian 1 , and Jens Chapman 1
1 Swedish Neuroscience Institute, Seattle, USA
Introduction: The traditional entry point of an iliac screw often causes post- operative gluteal pain from the prominent screw head. The use of an offset connector also adds a point of weakness to the construct. By choosing a different screw entry point offset connectors. This study aims to describe the modified iliac screw (mILS) technique and compare it to other spinopelvic fixation techniques in terms of wound healing complications, hardware prominence, and failure. Methods: A retrospective analysis was performed of adult patients undergoing lumbopelvic fixation between January 2014 and June 2019. Patients were grouped into one of three groups based on the technique of pelvic fixation: S2 alar-iliac screw (S2AI), traditional iliac screw (tILS), and modified iliac screw (mILS). The primary outcome parameter was the minimal distance from screw head to skin (MDSS). Secondary outcome parameters were instrumentation loosening/failure, adjacent level fractures, pseudoarthrosis, and medial or lateral iliac screw perforation. Results: A total of 190 patients undergoing lumbopelvic fixation were included in the following three groups: mILS group (n = 113), tILS group (n = 40), and S2AI group (n = 37). The mean MDSS in the mILS group was 31.3 mm compared to 23.7 mm in the tILS Group (P < .00199). No statis- tically significant differences were found when comparing the three groups with respect to com- plications. The mILS group did not show any cases of prominent instrumentation and had the lowest rate of instrumentation failure. Conclusions: The mILS technique is an acceptable alternative for lumbopelvic fixation, offering the benefits of iliac screw fixation while avoiding offset connectors and screw prominence complications associated with tILS.
OP07: Spine Biologics and Novel Technologies
677
A055: Intravenous v. Oral Acetaminophen Administration in Perioperative Care of One and Two Level LLIFs With Instrumented Posterior Lumbar Fusion: A Comparative Effectiveness Study
Celeste Abjornson 1 , Jessica Dorilio 1 , Fedan Avrumova 1 , Daniel Alicea 1 , Nicole Utah 1 , Christina Dowe 1 , Antonio Brecevich 1 , Frank Cammisa 1 , Darren Lebl 1 , Alexander Hughes 1 , Andrew Sama 1 , Russel Huang 1 , Matthew Cunningham 1 , Federico Girardi 1 , and Chad Craig 1
1 Hospital for Special Surgery, Spine Surgery, New York, USA
Introduction: Since 2000, the annual death toll from an opioid associated overdose has increased by over 300%. To reduce the opioid consumption, physicians have used alternative approaches, which have proven to be effective and also reduce side effects such as nausea, constipation, and addiction. IV acetaminophen has been shown to successfully reduce opioid usage, however, it is an expensive alternative. Testing the efficacy of IV acetaminophen versus its oral formulation will likely modify future postoperative pain management regimens while also addressing cost-effectiveness. The purpose of the study is to prospectively evaluate clinical outcomes and determine the cost effectiveness of IV vs oral (PO) acetaminophen following lumbar circumferential spine surgery. We hypothesize that IV acetaminophen will perform better than PO in terms of length of stay, morphine equivalence, and change in VAS scores from baseline. Methods: The study is a prospective, single center, randomized control trial. The eligible population included patients between the ages of 18-85 who underwent circumferential lumbar fusion surgery, while failing conservative treatment for more than 6 months. Patients were excluded if they had already undergone lumbar surgery at the index level(s), were diagnosed with osteoporosis, had dysphagia prohibiting oral administration, or had a history of substance abuse. The outcome measures included opioid equivalence, length of hospital stay, Visual Analog Scale (VAS) measurements, and Oswestry Disability Index (ODI) scores. Once enrolled, patients were randomized to either the IV or PO acetaminophen treatment groups. Preoperatively, patients completed a baseline analgesic regimen questionnaire, surveys including VAS, SF-12, and ODI. Patients were administered their first acetaminophen dose within three hours of first incision. Postoperatively, patients received seven subsequent doses of their assigned acetaminophen, with access to supplemental analgesics. Analgesic usage and VAS scores were monitored until discharge. Surveys were completed at 6 weeks and 6 months follow up. Results: The average daily opioid consumption for the IV group was significantly lower than the PO group during the immediate postoperative period. Average length of stay was similar between groups, 3.3 days for PO and 3.6 days for IV. VAS back and leg scores were not statistically different between groups, however, both groups experienced a decrease by more than the minimally clinically important difference (MCID) of 12 points from baseline. ODI also decreased by the MCID at the 6 months follow-up, which was defined as 12.8% for ODI. Discussion and Conclusion: Along with an overall reduction in opioid usage, patient reported outcomes depict successful improvement of pain management with the use of IV acetaminophen following circumferential spinal fusion surgery. Furthermore, despite the large discrepancy between the two formulations in cost-to-perceived-benefit ratio, the significant reduction of opioid usage and, therefore, its associated costs, provides a far less dramatic divergence. The continued testing of the efficacy of IV acetaminophen versus its oral formulation will likely modify future postoperative pain management regimens while also addressing the opioid epidemic plaguing communities across the US.
1881
A056: The Use of Telemedicine as a Rehabilitation Tool for Lower Back Pain (LBP) During the COVID-19 Pandemic
Karen Weissmann 1,2 , Paola Torres 3 , Nicolas Cubillos 1 , Maria Paz Aguilera 4 , Francoise Descazeaux 1 , Nicolas Sepulveda 5 , and Rodrigo Alarcon 5
1 MEDS, Santiago, Chile
2 Universidad de Valencia, Valencia, Spain
3 Fundacion Medica San Cristobal, Santiago, Chile
4 Redsalud, Santiago, Chile
5 Patagonia Spine Foundation, Santiago, Chile
Introduction: Physiotherapy is an important part of the spine pathology treatment. During the COVID-19 pandemic, access to it was limited. The use of tele-rehabilitation increases patient's access to therapists. The objective was to evaluate user's satisfaction and clinical outcomes in patients treated online. Material and Methods: The Delphi method was used. An expert committee of five kinesiologists and four spine surgeons developed a consensus for a telerehabilitation program for lower back pain. 6 synchronic sessions of 40 minutes through digital platforms like Zoom meeting, Microsoft Teams and WhatsApp video. This program was designed at a 42% cost of the original on-site program. Patients were evaluated using the Oswestry Disability Index (ODI) before and after therapy, we considered an MCID (minimally important clinical difference) of at least a 50% change as a positive outcome. User satisfaction was measured with the University of Washington Telemedicine Patient Satisfaction Survey. Happy and very happy were considered as positive answers and unhappy and very unhappy as negative answers. Results: Between April and September 2020, 85 patients accepted to be treated through telerehabilitation: 54 women and 29 men. Of the total of patients, 67 suffered from LBP pathology and were included in this analysis. ODI scores decreased from 39 points pre - intervention to 11.7 points after rehabilitation. Only one patient did not achieve the MCID. Regarding satisfaction surveys, 100% of patients answered, “this is the first time I get treated by a physiotherapist online”. Out of 10 items, 5 items had more than 75% of positive answers and no item had less than 50% positive answers. The average of positive answers was 80%, of neutral answers 16.7% and of negative answers 13.4%. 80% of the users would submit to online physiotherapy treatment again, 15% might use it again and 5% won’t. 68.8% of patients had full insurance reimbursement, the ones that did not had public health coverage. Conclusion: Telerehabilitation offers an alternative to treat LBP increasing easy access to physiotherapy with good satisfaction and outcomes and at lower cost for the patient.
1055
A057: Macrophage Therapy for Intervertebral Disc Herniation: In Vivo Proof-of-Concept
Inês A. Amaral 1,2,3 , Susana G. Santos 1,2,3 , Paulo Pereira 4,5,6 , Mário A Barbosa 1,2,3 , and Carla Cunha 1,2
1 i3S - Instituto de Investigação e Inovação em Saúde, Universidade do Porto, Porto, Portugal, Porto, Portugal
2 INEB - Instituto Nacional de Engenharia Biomédica, Universidade do Porto, Porto, Portugal, Porto, Portugal
3 ICBAS -Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto, Porto, Portugal, Porto, Portugal
4 Centro Hospitalar São João, Porto, Portugal, Department of Neurosurgery, Porto, Portugal
5 Faculty of Medicine, University of Porto, Porto, Portugal, Department of Clinical Neurosciences and Mental Health, Porto, Portugal
6 Neurosciences Center, CUF Porto Hospital, Porto, Portugal, Porto, Portugal
Introduction: Intervertebral disc (IVD) herniation and degeneration is often associated with low back pain, constituting the leading cause of spinal surgery worldwide1. The spontaneous hernia regression is a widely described phenomenon but the underlying mechanisms remain unclear. The main hypothesis is that hernia resorption is associated with a cascade of events, from inflammation to matrix remodeling, and angiogenesis, in which macrophages might be major players2. This study provides a preclinical proof-of-concept of the functional role of macrophages in hernia regression, by their direct administration into the hernia site using a rat model of IVD herniation. Material and Methods: Macrophages were differentiated from syngenic rat bone marrow precursors. Bone marrow was collected by flushing from the femurs and tibias and isolated cells were cultured in RPMI + 10% FBS media, supplemented with M-CSF for 7 days, for macrophage differentiation. Macrophages were administered locally in the hernia site using the previously developed IVD animal herniation and regression model3. A percutaneous needle puncture was performed in male Lewis (LEW/Crl) rats at 10 weeks of age, into coccygeal IVDs Co5/6, Co6/7, and Co7/8 IVDs. Macrophages were collected and 10 × 106 cells administered per hernia 2 weeks after IVD lesion, using a 31-G needle coupled to a microsyringe (Hamilton) and using an adaptor to assure 5 mm depth administration to the center of the IVD. Detailed analysis of in vivo hernia regression was performed by histology and immunohistochemistry and the associated systemic response by flow cytometry for main immune cell populations and cytokine array, at 6w post lesion. Control groups consist in lesioned animals sacrificed at 2w and 6w post lesion, without macrophage administration. Results: A detailed local and systemic analysis was performed to assess the functional potential of macrophage administration for in vivo hernia regression. Histological analysis consisting in delimitation of the hernia area in sections along the IVD for each animal, revealed that the group in which macrophages were administered, the hernia size was significantly smaller than in the untreated group, at 6w post-lesion. Systemically, no significant alterations in the main immune cell populations were found, but a decrease in the circulating levels of GM-CSF, together with increased spleen sizes, was found in the group administered with macrophages. Detailed histological, flow cytometry and cytokine analysis is underway. Conclusion: This study proposes an in vivo functional proof-of-principle of the role of macrophages in hernia regression. The concept of immunotherapy for tissue engineering strategies is still underexplored, but has the potential to provide important breakthroughs to currently unsolved clinical problems.
Acknowledgements
This work was funded by AO Foundation, AOSpine through project no AOSDIA2019-057 and by Portuguese funds through FCT - Fundação para a Ciência e a Tecnologia - CEECIND/00184/2017/CP1392/CT0001 and UID/BIM/04293/2019.
References
1. Weinstein, JN et al. Spine 33, 2789-2800 (2008).
2. Cunha, C. et al. Arthritis Res. Ther. 20, 251 (2018).
3. Cunha, C. et al. J. Orthop. Res. 35, 258–268 (2017).
413
A058: Pedicle Screw Insertion Accuracy Using Intraoperative Computed Tomography Image-Guided Navigation: A Series of 608 Screws
Bastian Stemmer 1 , Benedikt Trnovec 2 , Ertl Sebastian 1 , Bonk Maximilian-Niklas 1 , Ehab Shiban 3 , and Heidecke Volkmar 1
1 University hospital Augsburg, Department of Neurosurgery, Augsburg, Germany
2 Universitätsklinikum Bratislava, Department of Neurosurgery, Bratislava, Slovakia
1 University hospital Augsburg, Department of Neurosurgery, Augsburg, Germany
Objective: The goals of this study were to assess the accuracy of pedicle screw insertion using an intraoperative computed tomography (iCT), and to analyze potential risk factors for screw misplacement. Methods: A retrospective analysis of all patients following iCT navigated spinal pedicle screw placement between November 2016 and February 2019 was performed. Navigated drilling of the pedicle was followed by screw placement. Screw position was checked by a further iCT scan. Screw position was assessed according to the Gertzbein-Robbins classification. Results: 109 consecutive patients were identified (52.3% male, 47.7% female). Median age was 71 years. Screws were placed in all spinal regions: cervical and cervico-thoracal (68), thoracic (118), thoracic-lumbar (126), lumbar (206) and lumbosacral (90). Degenerative spine disease was the most common diagnosis (49.0%). There were 75.3%, 12.0%, 7.4%, 2.5% and 3.1% screws classified as Gertzbein-Robbins A, B, C, D and E, respectively. 30 screws (4.93%) were revised intraoperatively. Lumbar spine, thoracic spine, tumor and infection diagnosis were associated with highest rates of screw misplacement. None of the patients suffered from any neurovascular damage. Conclusion: The all-over revision rate was 4.93%. The highest revision rates were observed for tumor (6.38%), infection patients (6.86%), lumbar spine (6.30%) and thoracic spine (5.90%). None of the patients suffered from any neurovascular damage. No secondary operation to revise the misplaced screws was required. Keywords: pedicle screw, accuracy, intraoperative computed tomography, navigated, malplacement
20
A059: Efficacy of Anterior Vertebral Body Tethering in Skeletally Mature Children with Adolescent Idiopathic Scoliosis - A Preliminary Report
Keyur Akbari 1 , Vignesh Badikillaya 1 , Muralidharan Venkatesan 1 , and Sajan Hegde 1
1 Apollo Hospital, Spine Unit, Chennai, India
Introduction: Anterior Vertebral Body Tethering (AVBT) offers a dynamic fusionless correction option for children with Adolescent Idiopathic Scoliosis (AIS). Fewer existing clinical studies evaluating novel AVBT in skeletally immature children has questioned the mid-term efficacy with concerns of overcorrection and curve progression with remaining growth. The goal of current study is to investigate the safety and efficacy of this novel AVBT technique in the treatment of more skeletally mature children with AIS. Our hypothesis is that novel AVBT technique with maximum intraoperative correction in skeletally mature AIS children with less remaining growth potential can restrict complication of overcorrection, cord breakage, return to theatre or revision to fusion surgery. Material and Methods: We prospectively studied patients with Adolescent Idiopathic Scoliosis (AIS) who were operated between 2018 and2019 with AVBT technique with a minimum of one year of follow up. Our inclusion criteria for this novel technique were skeletally mature children, single structural AIS curve (40-80) with ≥50% flexibility on dynamic radiographs. We do supine awake manual traction and standing side bending dynamic radiographs routinely in all our patients to assess the flexibility of the curve. The curve should correct to ≥50% on dynamic radiographs to be eligible for the option of AVBT. Pertinent clinical and radiographic data collected include skeletal maturity, curve type, Cobb angle, sagittal parameters and patient reported outcome measure SRS-22 questionnaire. Repeated ANOVA test was performed to measure the difference between Cobbs angle. Wilcoxn Signed Rank Test was used to compare pre and post op SRS 22 score. P value < .05 was considered statistically difference. Results: All 10 children were female with mean age of 14.9 years at the time of surgery. Mean follow up was 18.1 months. Mean Rissers and Sander’s score were 4.2 ± .6 and 7.2 ± .64 respectively. 3 patients had Major Thoracic (MT) and 7 patients had Thoraco Lumbar (TL)/Lumbar (L) curves. Cranial and caudal instrumented levels were T5 and L4. Mean pre operative Cobb’s angle was 52˚ ± 11.6˚ and corrected to15.9 ± 6.8o on first erect post op radiograph, with stabilization of corrected curve at one year follow-up (mean Cobb’s 15.3 ± 8.70). Average blood loss during surgery was 112 ± 12.4 ml and average surgical time was 162 ± 13.2 minutes. The average radiation dose during surgery was .6 ± .05 mGy and average radiation exposure time was around 8 ± .6 seconds. Average hospital stay was 3.5 ± .5 days. The average gain in height was 2.7 ±.6 cm. Mean SRS-22 score pre op and post op were 78 and 92.5 respectively (P < .01). No complications were noted till last follow up. Conclusion: AVBT is a safe and effective novel alternative technique to fusion to stabilize progressive idiopathic scoliosis in skeletally mature children. Our short term outcome is promising but it has to stand the test of time.
1826
A060: Lumbar Spine Fusion Outcomes Using a Cellular Bone Allograft with Lineage - Committed Bone Forming Cells in 96 Patients
Hossein Elgafy 1 , Brad Wetzell 2 , Marshall Gillette 1 , Hassan Semaan 3 , Andrea Rowland 1 , Christopher A Balboa 1 , Thomasa Mierzwa 1 , Julie B Mclean 2 , Kimberly Dorsch 2 , and Mark Moore 2
1 University of Toledo, Orthopedic, Toledo, USA
2 LifeNet Health, Virginia Beach, USA
3 University of Toledo, Radiology, Toledo, USA
Introduction: Instrumented posterior lumbar fusion (IPLF) with and without transforaminal interbody fusion (TLIF) is a common treatment for low back pain when conservative interventions have failed. Certain patient comorbidities and lifestyle risk factors, such as obesity and smoking, are known to negatively affect these procedures. An advanced cellular bone allograft with viable lineage-committed osteogenic cells (V-CBA) has demonstrated high fusion rates, but these rates for patients with severe and/or multiple comorbidities remains understudied. The purpose of this study was to assess fusion outcomes in patients undergoing IPLF/TLIF using V-CBA with baseline comorbidities and lifestyle risk factors known to negatively affect bone fusion. Materials and Methods: This was a retrospective study of de-identified data from consecutive patients at an academic medical center. All study patients underwent IPLF procedures with or without TLIF, and with V-CBA. Baseline patient and procedure characteristics were assessed. Radiological outcomes included fusion rates per the Lenke scale. Clinical outcomes were evaluated by the Oswestry Disability Index (ODI) and Visual Analog Scale (VAS) for back and leg pain. Operating room times were also assessed. Results: Data from 96 patients with a median follow-up time of 16 months (range: 4-45 months) were assessed. Successful fusion (Lenke A or B) was reported for 88 of 96 patients (91.7%). Of 24 patients with diabetes, fusion was reported in 22 patients (91.7%). In patients currently using tobacco (n = 21), fusion was reported in 18 patients (85.7%), while in those with a history of tobacco use (n = 61), fusion was observed in 56 patients (91.8%). Successful fusion was reported in all 6 patients with pseudarthrosis at the same level. Mean VAS ratings at the final study visit ranged from 3.5 to 6.0 and mean ODI ranged from 15.2% to 18.3%. The overall mean OR time was 192.7 minutes. Conclusion: The results of this study suggest that V-CBA yields consistently successful fusion despite patient comorbidities and life-style risk factors that are known to negatively affect such bony healing.
398
A061: Development of AOSpine BOnE (Bone Osteobiologics and Evidence) Classification
Jeffrey C. Wang 1 , Timothy S. Yoon 2 , Darrel Brodke 3 , Jong-Beom park 4 , Patrick Hsieh 5 , Hans-Jörg Meisel 6 , and Zorica Buser 1
1 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
2 Emory Spine Center, Emory University, Atlanta, USA
3 University of Utah School of Medicine, Salt Lake City, USA
4 Uijongbu St. Mary’s Hospital, The Catholic University of Korea School of Medicine, Uijongbu, South Korea
5 Keck School of Medicine, University of Southern California, Los Angeles, USA
6 Department of Neurosurgery, Bergmannstrost Hospital, Halle, Germany, Halle, Germany
Introduction: The use of osteobiologics for spine fusion has increased significantly over the years with the expansion of available graft materials. Although various biologics are used frequently, the literature on their effectiveness is inconclusive. The aim of our study was to develop a three-tier classification for the levels of evidence for osteobiologics and provide a description of the principles by which osteobiologics can be evaluated. BOnE (Bone Osteobiologics and Evidence) classification evaluates each osteobiologic based on the available evidence, and if the published evidence is based on clinical, in vivo or in vitro studies. Material and Methods: The process of establishing the BOnE classification included five face-to-face meetings and two web calls among members of the AOSpine Knowledge Forum Degenerative. Initial draft of the BOnE classification was based on a notion that it should be possible to divide osteobiologics into a few categories that are easily recognizable by clinicians, researchers, patients, and industry. Results: The three levels of evidence were determined based on the type of data on osteobiologics, level A for human studies, level B for animal studies, and level C for in vitro studies, with level A being the highest level of evidence. Each level was organized into three sub-groups (e.g., A1, A2 and A3). During the initial testing of the BOnE classification, it was realized that each category required a level 4 sub-group for evidence of very low quality leading to four sub-groups (A1, A2, A3 and A4). The grading principle is very straightforward: evaluation of each osteobiologic would start with the highest level of evidence and it would be downgraded based on the available evidence primarily focusing on peer review publications. Conclusion: The use and the variety of osteobiologics for spine fusion has dramatically increased over the past few decades, however literature on their effectiveness is inconclusive. Several prior systematic reviews developed by AOSpine Knowledge Forum Degenerative reported low level of evidence primarily due to the high risk of bias, small sample size, lack of control groups, and limited patient reported outcomes. BOnE classification will provide a universal platform for research studies and journal publications to classify a new or an existing product, and will allow for creating decision-making algorithms for surgical planning.
1444
A062: Cervical BMP Use is Associated with Increased Fusion Rates Without More Complications in Anterior Cervical Discectomy and Fusion
Colin Haines 1 , Catherine Gorick 2 , Alexandra Thomson 1 , Ehsan Jazini 1 , Thomas Schuler 1 , Rita Roy 2 , and Christopher Good 2
1 The Virginia Spine Institute, Reston, USA, 2 The National Spine Health Foundation, Reston, USA
Study Design: A retrospective review of patients who underwent anterior cervical discectomy and fusion (ACDF) with and without the use of low-dose recombinant human bone morphogenetic protein 2 (rhBMP-2). Objective: To determine whether low dose rhBMP-2 with postoperative oral steroid administration is effective in improving fusion rates and whether the rate of adverse events after ACDF are elevated with low-dose rhBMP-2 use. Background: RhBMP-2 is a naturally occurring human protein shown to promote bone formation. In 2002, the FDA approved its use in anterior lumbar spinal fusion. Despite the potential benefits of its use, concern exists regarding increased risk of dysphasia and retropharyngeal edema with cervical spine use. Materials and Methods: A retrospective review of 164 prospectively collected patients (80 male, 84 female).71 patients received rhBMP-2 during ACDF and 93 patients underwent ACDF without rhBMP-2. Incidence of surgical complications, adverse events, and revision surgeries was compared between the two groups. Fusion was analyzed by flexion and extension radiographs at one year. Results: Patients receiving low dose rhBMP-2 and oral postoperative steroids had significantly higher fusion rates at one year follow up compared to BMP naïve patients (91% vs 82% P = .02, respectively). The rhBMP-2 group averaged more risk factors for pseudarthrosis including tobacco use, prior history of pseudarthrosis, and multilevel fusions compared to non-BMP group (P > .01). There were no statistically significant differences in the rates of graft subsidence, dysphagia, hematoma, or surgical complications between the two groups. No patients experienced post-operative radiculitis, ectopic bone growth, retropharyngeal edema, or wound infection. Conclusions: The use of rhBMP-2 in ACDF with postoperative oral steroids can be a safe and effective approach to improve fusion rates when dosed appropriately. We report a significant increase in fusion rates with low-dose rhBMP-2 and oral postoperative steroids, without a significant difference in complication rates. Keywords: BMP, ACDF, fusion, dysphasia
575
A063: AO Spine Guideline for Using Osteobiologics in Spinal Degenerative Cases: Protocol for AO Spine Guideline Development (AO-GO) - Chapter I ACDF
Hans Joerg Meisel 1 , Zorica Buser 2 , Neha Agarwal 3 , Yabin Wu 4 , Amit Jain 5 , S. Tim Yoon 6 , and Jeffrey C. Wang 2
1 Bergmannstrost Hospital, Halle, Department of Neurosurgery, Halle, Germany
2 Keck School of Medicine, University of Southern California, Department of Neurological Surgery, California, USA
3 Bergmannstrost Hospital Halle, Department of Neurosurgery, Halle, Germany
4 AO Foundation, AO Spine, Davos, Switzerland
5 Johns Hopkins University, Baltimore, MD, Department of Orthopaedic Surgery, Baltimore, USA
6 Emory University, Department of Orthopaedic Surgery, Atlanta, Georgia, USA
Introduction: AO Spine Guideline for Using Osteobiologics in Spine Degeneration (AO-GO) project is an international, multidisciplinary collaborative initiative to identify and evaluate evidence on existing use of osteobiologics in spine degenerative diseases. It aims to formulate precisely defined, clinically relevant and internationally applicable guidelines ensuring evidence-based, safe and effective use of osteobiologics, considering regional preferences and cost-effectiveness. The current focus is the use of osteobiologics in anterior cervical discectomy and fusion surgeries. Methodology: The guideline development is planned in three phases. Phase 1- Evidence synthesis and Recommendation; Phase 2- Guideline with osteobiologics grading and Validation; Phase 3- Guideline dissemination and Development of a clinical decision support tool. The key questions formulating the guidelines for the use of osteobiologics will be addressed in a series of systematic reviews in Phase 1. The evidence synthesized by the systematic reviews will be assessed by Grading of Recommendations, Assessment, Development and Evaluations (GRADE) methodology, including expert panel discussions via web calls and face-to-face meetings to formulate a recommendation. In Phase 2, osteobiologics will be graded based on up-to-date evidence and the grading will be integrated with the recommendation from Phase 1, and thus formulate a guideline for using osteobiologics in anterior cervical discectomy and fusion (ACDF). The guideline will be further validated by using prospectively collected clinical data. In the third phase, dissemination of the proposed guideline and development of a decision support tool is planned. Discussion: AO-GO aims to bridge an important gap between quality of evidence and use of osteobiologics in spine fusion surgeries. Owing to differences in osteobiologics preparation and functional characteristics, respective regulatory requirements for approval may vary, therefore it is highly likely that these products enter market without quality clinical trials. With a holistic approach the guideline aims to facilitate evidence-based, patient-oriented decision-making process in clinical practice, thus stimulating further evidence-based studies regarding osteobiologics usage in spine surgeries.
OP08: Trauma-Thoracolumbar 2
1477
A064: Diagnostic Value of Horizontal Vs Vertical Laminar Fracture for Diagnosis of Posterior Ligamentous Complex Injury in Thoracolumbar Fractures
Mohamed Ali 1
1 Prince Mohamed Bin Abdelaziz Hospital, Neurosurgery, Riyadh, Saudi Arabia
Background Context: According to AO classification, a horizontal laminar fracture (HLF) is a recognized feature of AO type-B injury, whereas a vertical laminar fracture (VLF) is a distinct fracture pattern that typically accompanies a burst fracture and has less likely to disrupt posterior ligamentous complex (PLC). However, the association of these 2 fracture patterns with PLC injury is seldom reported. Purpose: To analyze the diagnostic value of vertical vs horizontal laminar fracture for diagnosis of PLC injury in patients with TLF using MRI as a reference study. Study Design/Setting: A retrospective single-center study conducted in a level 1 trauma center. Patient Sample: Two hundred sixty-two consecutive patients with acute TLF (T1-L5) between 2014 and 2020 who underwent CT and MRI. Patients with translation injury, osteoporotic fracture or pathological fractures were excluded. Methods: Two reviewers evaluated CT for the following findings: Abnormal facet joint alignment (FJA), facet joint widening (FJW), horizontal laminar fracture (HLF), spinous process fracture (SPF), interspinous widening (ISW). Incompetent PLC was defined by supraspinous or ligamentum flavum rupture. Univariate and multivariate association between CT findings and PLC injury was examined. The diagnostic performance (sensitivity, specificity, accuracy, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (+LR), and negative likelihood ratio (-LR) of horizontal and vertical laminar fracture in the diagnosis of PLC injury. Results: In the univariate analysis, VLF showed no significant association with PLC injury (OR 1.5, 95% CI .89-2.5, P = .1) and was therefore not included in the multivariate analysis in which HLF demonstrated an independent association with PLC injury (AOR range 2.5-14.7, P = 000.1). HLF yielded a PPV of 84% (95% CI 72-91) and a +LR of 7.4 (95% CI 4.0-13.3), whereas VLF yielded a PPV of 48% (95% CI 37-58) and a +LR of 1.3 (95% CI .93-1.8). Conclusions: Our study found that HLF was an independent predictor of PLC injury (AOR 6.2), whereas VLF was not associated with PLC injury. Therefore, confusing HLF and VLF might have resulted in an underestimation of the diagnostic value of HLF in previous studies. Keywords: posterior ligamentous complex, thoracolumbar fractures, diagnostic accuracy, computed tomography, MRI, horizontal laminar fracture, vertical laminar fracture
1379
A065: Timing of Surgical Spine Stabilization in Multiple Injured Patients: Introducing Damage Control Spine
Sascha Halvachizadeh 1 , Henrik Teuber 1 , Kai Oliver Jensen 1 , Jakob Hax 1 , Ladislav Mica 1 , Hans Christoph Pape 1 , and Kai Sprengel 1
1 University Hospital Zurich, Trauma, Zurich, Switzerland
Introduction: Timing of definitive surgical treatment in multiple injured patients still is controversial. In these discussions, timing of surgical spine stabilization has only been marginally addressed. The role of Early Spine Stabilization is still unclear. Therefor this study investigates the influence of timing of spinal stabilization on the outcome of multiple injured patients. Material and Methods: This study analyses multiple injured patients treated at one Level 1 trauma center. Inclusion criteria: ages 16 years and older, injury severity score (ISS) ≥16 with injuries to the spine that need surgical stabilization. Group stratification according to first surgical stabilization of the spine: immediate (day of admission), early (within 48 hours) and delayed stabilization (>48 hours). Results: Stratification of 303 multiple injured patients with injuries to the spine with indication of surgical stabilization according time of first surgical procedure to the spine: Immediate (n = 141), early (n = 68) and delayed (n = 94). Group Delayed showed highest total length of stay (LOS) (27 ± 14 days) as well as ICU LOS (15 ± 11 days) and ventilation days (10 ± 11 days). Delayed stabilization of spine injury triples the risk of developing pneumonia (OR 3.0, 95% 1.9-4.8) each day. It further increases the risk of developing sepsis by 1.7 (95%CI 1.0-2.8) each day. There was no significant differences in mortality the groups without injuries to the spine or immediate versus early stabilization. Conclusion: Delayed surgical stabilization of the spine in multiple injured patients increases the risk of developing pneumonia, or sepsis substantially. Therefore, we introduce Damage Control Spine to highlight spinal instability as an important issue in managing multiple injured patients. Stabilization of the spine should be addressed with high priority in the timing of surgical procedures of multiple injured patients.
1229
A066: Systematic Review of RCT: Use of Orthosis in Thoracolumbar Fractures
Daniela Linhares 1 , Bernardo Sousa-Pinto 2 , Manuel Ribeiro da Silva 1 , João Fonseca 2 , and Nuno Neves 1
1 CHUSJ, Orthopedics and Traumatology, Porto, Portugal
2 FMUP, MEDCIDS, Porto, Portugal
Introduction: Although recent studies suggest that orthosis have no benefit, and may have a negative impact in recovery, these devices are traditionally used in conservative treatment of thoracolumbar (TL) fractures. This systematic review and meta-analysis of RCT evaluating radiological and clinical outcomes of treatment of acute traumatic TL fractures in skeletally mature patients with orthosis, compared with no immobilization. Material and Methods: A systematic search was conducted from inception to June 2019, and selection was performed in two phases by two blinded reviewers, based in pre-defined inclusion and exclusion criteria. Two independent reviewers performed data extraction and quality assessment. A previous plan for extraction of radiological (kyphosis progression; loss of anterior height) and clinical (pain; disability; length of stay) outcomes was applied. Meta-analysis were computed. PRISMA guidelines were followed. Results: Five studies, from eight papers, were included. No study reported significant differences in pain, kyphosis progression and loss of anterior height. Only one found a better ODI with orthosis at 12 weeks assessment but not at 24 weeks. No other study reported differences in disability. All authors concluded an equivalence between treatments. Meta-analysis showed a significant increase of 3.47 days (95%CI 1.35; 5.60) in mean admission time in orthosis group. No differences were found in kyphosis at 6 and 12 months; kyphosis progression between 0-6 or 0-12 months; loss of anterior height 0-6 months; VAS for pain at 6 months; and VAS change 0-6 months. Conclusion: This study showed that orthosis seems to add no benefit to conservative treatment of patients with acute TL fractures.
609
A067: Associated Injuries in Patients with Thoracic Spine Fractures
Patrick Curtin 1 , Jay Patel 1 , Jenna Lansbury 1 , Taylor Dickinson 1 , and Michael Stauff 1
1 University of Massachusetts, Orthopedic Surgery, Worcester, USA
Introduction: Thoracic spine fractures (TSFs) are rarely isolated injuries, and they tend to present with a characteristic set of vertebral and non-vertebral injuries based on mechanism of injury. There is limited research on the rates and distribution of injuries that occur concurrently with TSFs. The purpose of this study is to characterize the distributions of these injuries by region of the body and by mechanisms of injury, so that trauma and spine surgeons are able to efficiently evaluate and treat patients presenting with TSFs. Material and Methods: We retrospectively reviewed the trauma database records of 3646 patients presenting with a TSFs at a single institution from 2015 to 2019. We recorded patient demographics, comorbidities, and associated injuries by body region. We characterized the TSFs using the AO classification system, as well as the presenting physical exam and treatment. All associated injuries among the TSF patients were classified into the following categories: head injury (HI), thoracic injury (TI), non-thoracic vertebral injury (NTVI), abdominal injury (AI), upper extremity injury (UEI), lower extremity injury (LEI), and spinal cord injury (SCI). Results: The three leading causes of TSFs were mechanical falls (38%), falls from height (23%), and motor vehicle crashes (MVCs) (21%). TSFs resulting from MVCs had a higher amount of concurrent TI (52.9% vs 38.6%, P = .005), UEI (23.1% vs 14.4%, P = .02), and LEI (24.0% vs 12.6%, P = .002) compared to all other mechanisms. TSF’s after MVCs had a high amount of NTVI (38.8% vs 37.5%) and HI (43.8% vs 40.6%) compared to other mechanisms, but the difference was not statistically different. Need for treatment for TSFs was high with 58.7% requiring a brace, and 11.6% requiring surgical stabilization. TSFs after a fall from height had a higher amount of concurrent NTVI compared to all other mechanisms (51.1% vs 33.7%, P = .0003). There were high rates of TI (48.1% vs 39.7%), and HI (46.6% vs 39.7%) compared to other mechanisms, but the difference was not statistically significant. Need for treatment was high with 61.8% requiring a brace, and 11.5% requiring surgical stabilization. TSFs after mechanical falls had a significantly lower rate of concomitant injury compared to other mechanisms. There was a high rate of other injuries such as TI (25.5%), NTVI (28.8%), and HI (30.7%). TSFs required brace treatment in 51.4% of patients and 2.8% required surgical stabilization. Motor cycle crashes (MCCs) were the mechanism in 4.8% of all TSFs, and were never an isolated injury. Associated injuries and TSFs in MCCs were typically more severe, with 7.4% dying before an exam could be obtained, 7.4% with an ASIA A SCI, and 59.3% requiring bracing for their TSFs. Conclusion: TSFs after MVCs, mechanical falls, and falls from height presented with a predictable pattern of injuries and were rarely an isolated injury. This cross-sectional data may help spine and trauma surgeons better understand patterns of injury associated with TSFs, with the hope of preventing missed injuries and better advising patients with TSFs on severity of injuries.
1579
A068: Venous Thromboembolism in Patients with Thoracic Spine Fractures
Patrick Curtin 1 , Jay Patel 1 , Jenna Lansbury 1 , Taylor Dickinson 1 , and Michael Stauff 1
1 University of Massachusetts, Orthopedic Surgery, Worcester, USA
Introduction: Thoracic spine fractures (TSFs) are rarely an isolated injury. Venous thromboembolism (VTE) management can be increasingly complicated in these patients when trying to balance the risk of VTE against the risk of epidural hematoma or other bleeding complication with chemical prophylaxis. The purpose of this study is to better characterize VTE risk in patients with TSFs. Material and Methods: We retrospectively reviewed the trauma database records of 557 patients presenting with a TSFs at a single institution from 2015 to 2019. We identified 157 patients as having an AO classification B or C TSF. For these 157 patients we recorded patient demographics, comorbidities, and associated injuries by body region. We characterized the TSFs using the AO classification system, as well as the presenting physical exam and treatment. Results: Of the 157 patients, 6 (3.8%) were found to have a VTE event during their hospitalization. Patients with a spinal cord injury (SCI) had 8.2 times the risk (1.73 to 39.06, P = .0081) of having a VTE compared to patients without SCI. Patients with a VTE compared to those without a VTE had high rates of thoracic injury (TI) (48.3% vs 53.6%), non-thoracic vertebral injury (NTVI) (50.0% vs 38.4%), head injury (HI) (67.7% vs 34.4%), abdominal injury (AI) (50.0% vs 17.9%), upper extremity injury (UEI) (16.7% vs 16.6%), and lower extremity injury (LEI) (33.3% vs 14.6%), however none conveyed a statistically higher risk of VTE. Patients who underwent surgery for their TSF had 5.3 times the risk (1.01 to 27.91, P = .049) of VTE compared to patients who did not undergo surgery. Patients with VTE compared to without had similar rates of bracing for definitive treatment of their TSF (83.3% vs 70.2%). Three of the 157 patients died prior to receiving definitive treatment for the TSFs due to the severity of their other injuries. Of the 6 patients found to have a VTE, 5 have prophylactic IVC filters placed prior to discovery of VTE. None of these patients received chemical prophylaxis during their hospitalization, and all had multiple injuries in addition to their TSF. The one patient with a VTE and no IVC filter was placed on SQH prior to discovery of VTE, and had no other injuries besides their TSF. Seven filters were placed in patients who were never found to have a VTE. Conclusion: Although rates of VTE in TSF patients are low, their care is complicated by the presence of additional injuries. SCI and surgery were found to increase relative risk of VTE in this small series. Despite high rate of additional injury in patients with TSF, no body region was clearly associated with increased risk of VTE. The prophylactic benefit of IVF filters in patients in these patients is a consideration given the complexities associated with chemical DVT prophylaxis in the perioperative setting.
911
A069: Thoracolumbar Injuries in Polytrauma: the Importance of the M2 Modifier
Jessica Gilchrist 1 , Michalis Kaminaris 1 , Parker O'Neill 1 , and Darren Lui 1
1 St. George's Hospital NHS Foundation Trust, Department of Orthopaedic and Trauma Surgery, London, United Kingdom
Introduction: Protocol states Major Trauma Centre (MTC) patients receive whole-body CT scans to assess for injuries. The AO Thoracolumbar Injury Classification System (AO TLICS) is used to classify spinal fractures and generate a score delineating if surgery is warranted. Within this AO TLICS, the M2 modifier can be applied to signal a patient specific comorbidity, and carrying no score itself, is useful for arguing both for or against surgery. We evaluate the incidence of thoracolumbar spine injuries in MTC patients with an Injury Severity Score (ISS) >15, with concomitant orthopaedic, visceral, thoracic, head and/or maxillofacial trauma and the importance of the M2 modifier in the justification for or against surgery. Material and Methods: Retrospective analysis of the Trauma Audit Research Network (TARN) data from 1st January to 31st December 2016, with patients of ISS >15. Thoracolumbar injuries and orthopaedic, visceral, thoracic, head and maxillofacial trauma were determined from CT scans, and thoracolumbar fractures classified using AO Spine. Results: 377 patients identified with traumatic spinal injuries from 2433 MTC patients (15.5%). Of these, 186 patients had an ISS >15 (49.3%), with 171 of these patients having CT scans accessible for interpretation (91.9%). 117 of the 171 patients sustained thoracolumbar spine injuries (68.4%). Of these patients 63.2% sustained concomitant orthopaedic trauma, 22.2% sustained visceral trauma, 54.7% sustained thoracic trauma, 38.5% sustained head trauma and 17.1% sustained maxillofacial trauma. 96.6% of the thoracolumbar fractures were A type, 6.8% were B type and 1.7% were C type. Most A type fractures were A0 (56.4%). There were also A1 (33.3%), A3 (12.0%) and A4 (15.4%), with no A2 fractures. There were 4.3% B1 type fractures, 2.6% B2 type fractures and 0% B3 type. The Thoracolumbar AOSpine Injury Score (TL AOSIS) for A3, A4, B1 and B2 injuries indicated 34.2% of these patients should have received surgery. Interestingly, only 57.5% of the recommended patients actually received surgery. Conclusion: In orthopaedic polytrauma, just over 1:3 have spinal fractures that are suitable for surgery according to AO TLICS, but 42.5% of recommended polytraumas did not receive surgery. The M2 modifier may justify no surgery in high TL AOSIS scoring patients with concomitant injuries not suitable for surgery. However, the M2 modifier may also justify surgery in low TL AOSIS scoring fractures in patients with concomitant injuries requiring early mobilisation. The M2 modifier in thoracolumbar spine trauma is particularly important in the context of polytrauma. These patients often have comorbidities making the decision to operate an ambiguous one. To the discerning surgeon, the case-specific nuances indicated by the M2 modifier provide a simple, effective method of communicating and justifying the optimal treatment.
1242
A070: Vertebral Bone Density Variation and the Risk of Subsequent Fracture After Cement Augmentation: A Retrospective Study of Site Specific Computed Tomography Measurements
Alon Grundshtein 1 , Dana Niry 2 , Khalil Salame 1 , Zvi Lidar 1 , Dror Ofir 1 , Morsi Khashan 1 , and Gilad Regev 1
1 Tel Aviv Sourasky Medical Center, The spinal unit, department of neurosurgery, Tel Aviv, Israel
2 Tel Aviv Sourasky Medical Center, Department of Radiology, Tel Aviv, Israel
Introduction: Subsequent vertebral fractures are a common (12-52%) complication of percutaneous cement augmentation procedures for osteoporotic compression fractures. Pre-operative CT scans allow for opportunistic indirect measurement of bone density through the scanned spine through Hounsfield units (HU) values. The study aims to test the hypothesis that low site-specific preoperative HU values can predict a subsequent vertebral fracture after cement augmentation. Material and Methods: Between the years 2007-2017, 66 patients (16 men, 50 women, mean age 77.9 years) were treated by a single level thoraco-lumbar percutaneous cement augmentation (kyphoplasty/vertebroplasty) for a low energy osteoporotic compression. HU values (average and standard deviation) were measured for each vertebra in three different locations in the pre-operative CTs. 22 patients (33.3%) had subsequent vertebral body fractures, within an average of 31.2 months (range 1-79 months). Patient imaging and clinical notes were retrospectively reviewed. Results: Across the cohort, mean HU values were significantly different between the different measurement locations (P < .001) – below the superior endplate (57), the middle of the vertebral body (85.9) and superior to the inferior endplate (81.9). Clinical variables tested including age, gender, steroid treatment, fracture morphology, local kyphosis and augmentation procedure type did not correlate with the risk of subsequent fractures. Mean and minimal HU values were lower in the subsequent level fracture group (47.22 and 74.74 vs 53.86 and 85.11), however that result was not statistically significant (P values of .63 and .36). Fractures of the L2 vertebra correlated significantly with the risk of a subsequent vertebral fracture (P = .012). Conclusion: Bone density was lowest at the cranial part of the cancellous vertebral body, possibly contributing to the common finding of upper endplate compression fractures. This study did not demonstrate statistically significant correlation between low site-specific bone density and the risk of subsequent vertebral fractures. L2 vertebral fractures as a specific risk factor for a subsequent level fracture is a significant finding not previously reported in the literature.
1777
A071: Outcomes of Posterior Short Segment Fixation in AO Type A3 and A4 Thoracolumbar Fractures in Patients with High Occupational Activity
Nihar Shah 1 , Ramavtar Saini 1 , and Mirant Dave 1
1 Geetanjali Medical College and Hospital, Orthopaedics, Udaipur, India
Introduction: With rapid economic development, high velocity trauma and injuries like fall from height are increasing. The inherent anatomy of the thoracolumbar region makes it more susceptible for fractures because the thoracolumbar region is straddled between rigid thoracic spine and mobile lumbar spine. In order to achieve and maintain anatomic reduction, the forces that caused the injury must be counteracted by the instrumentation construct, which should be robust enough to withstand physiologic loads until the injury heals. With posterior fixation becoming the gold-standard treatment of these fractures some surgeons creatively started fixing the fractured vertebra without extension of fixed segments and named the technique short same segment fixation. Managing AO type A3 & A4 thoracolumbar fractures by reinforcing the fractured vertebra by placing additional 1 or 2 screws at the fracture level gives increased stability to the overall construct, maintains anterior vertebral body height, maintaining local kyphotic angle all while sacrificing less segments and helps early return to routine activities. Material and Methods: This study was a prospective study involving 30 patients with single level AO type A3 & A4 thoracolumbar burst fractures with or without neurological deficit between 2016 to 2018 in department of orthopaedics of a tertiary care teaching hospital of southern Rajasthan. All the patients were primarily managed accordingly to ATLS protocol, all the fractures were confirmed by plain radiographs, subsequent CT and MRI were done at surgeon’s discretion. All patients were surgically treated with short same segment fixation using a posterior surgical approach with transpedicular instrumentation. Pedicle screws were placed at one level above and below the fracture site and also inserted at the level of the fracture and connected with rods. Laminectomy done and bone graft was placed post fixation. Rod contouring was done according to the lumbar lordosis and distraction was done to maintain curvature. Results: A total of 30 patients were included in the study with an average age of 43 years (range 30 to 68 year), most common mode of injury was fall from height. All patients were of labour class and high occupational activity. Preoperative AO Classification was A3 in 28 patients A4 in 2 patients. Mean preoperative local kyphosis angle was 9.68 ± 2.11°. Postoperative local kyphosis angle was 2.53 ± 1.17°. Preoperative anterior vertebral body height was 51.64 ± 5.83%, postoperative being 91.68 ± 5.12%. Out of 30, one patient was lost to follow-up. No implant failure was encountered at two years follow up. At 2 years follow-up local kyphosis angle was 2.53 ± 1.12° and anterior vertebral body height was 90.34 ± 4.93%. Conclusion: The team concludes that short same segment pedicle fixation in AO type A3 and A4 thoracolumbar burst fractures provides reliable fixation while sacrificing less motion segments, early return to work and minimal soft tissue handling while maintaining local kyphosis angle and anterior vertebral body height at two-years follow-up. Surgical fixation in A3 and A4 type fractures is the choice of treatment for high occupational activity patients.
1260
A072: Virtual Thoracolumbar Fracture Clinics are a Safe and Effective Alternative to Traditional Clinic Models
Thomas York 1 , Vishal Borse 1 , Mark Nowell 1 , Nigel Gummerson 1 , Almas Khan 1 , and Peter Loughenbury 1
1 Leeds General Infirmary, Leeds Centre for Neurosciences, Leeds, United Kingdom
Introduction: Virtual fracture clinics (VFCs) are an alternative to conventional fracture clinics. There is limited data to support their use for specialist thoracolumbar fracture clinics. Materials & Methods: Lean methodology including process mapping was applied to identify a safe virtual alternative for the existing pathway. First cycle analysis of 100 consecutive referrals to the traditional clinic and second cycle analysis of 100 consecutive referrals to the VFC. Results: First cycle : Mean time to outpatient review 84 days. 240 outpatient appointments; 66 were missed (28% non-attendance). 54% of referrals had 3 or more appointments. 82/100 were AO type A1-3. 9/100 were AO type A4 or B. 1 patient received operative stabilisation (AO type B).Process mapping identified two pathways – virtual review with advice letter and physiotherapy referral (outcome A - AO type A1-3) or face to face review (outcome B - AO type A4 or B). Second cycle : Mean time to outpatient review 10 days. 79/100 received outcome A. 8/79 (10%) made a telephone call for advice and only 2/79 (3%) asked for a face to face appointment. 19/100 received outcome B and all were discharged after one visit. No patients required operative stabilisation. Statistically significant reduction in number of scheduled face-to-face reviews (240 vs 19; P < .001) and mean time to first review (84 days versus 10 days; P < .001). Conclusion: Virtual thoracolumbar fracture clinics are a safe and effective alternative to traditional fracture clinic models. Lean methodology can be uses to extend virtual clinic pathways to specialist spinal trauma clinics.
OP09: Endoscopic Spine Surgery
694
A073: Clinical and Radiographic Outcomes of Cervical Disc Replacement Versus Posterior Endoscopic Cervical Decompression: A Matched-Pair Comparison Analysis
Vit Kotheeranurak 1 , and Taweechai Tejapongvorachai 2
1 Queen Savang Vadhana Memorial Hospital, Sriracha, Thailand
2 Chulalongkorn University, Orthopaedic department, Bangkok, Thailand
Introduction: Cervical disc replacement (CDR) and posterior endoscopic cervical decompression (PECD) are the cervical motion-sparing surgeries to treat cervical radiculopathy. We aimed to compare the clinical and radiographic outcomes between the two procedures. Material and Methods: Eighteen patients, with a single-level unilateral cervical radiculopathy, in each of the CDR and PECD groups were retrospectively recruited as matched pairs. Clinical outcomes included visual analog scale score (VAS) for neck and arm pain, Neck Disability Index (NDI), and satisfaction rates. Radiographic outcomes were index level motion. Intraoperative data, complications, and hospital stay were collected. Patients’ outcomes were compared preoperatively and postoperatively. Results: Matched pairs were compared between 2 groups in terms of demographic data and preoperative measurements; CDR group had less operative time (P< .032), while PECD group has less blood loss PECD (P<.027). The total complication rate was 5% in both groups. VAS for neck and arm, and NDI were significantly improved in both groups, which was no significant difference between 2 groups. Satisfaction rates of the both groups were more than 90%. CDR group was superior to PECD group with respect to its capability to restore DH (P< .001). Early postoperative follow-up periods showed no significant difference in terms of index level motion. PECD group achieved less hospital stay and return-t o-work time significantly (P < .021). Conclusion: PECD may achieve equivalent clinical and radiologic outcomes compared with CDR when certain criteria for surgery are met. Early results showed that both techniques have potential to maintain index level motion. Furthermore, the PECD group showed less blood loss, shorter hospital stays, and faster return-to-work time. While, CDR group had less operative time and better ability to restore disc height.
725
A074: Endoscopic Transnasal Odontoidectomy for Ventral Decompression of the Craniovertebral Junction: Surgical Technique and Clinical Outcome in 18 Cases
Vicki Butenschön 1 , Maria Wostrack 1 , Bernhard Meyer 1 , and Jens Gempt 1
1 Technical University Munich, Department of Neurosurgery, Munich, Germany
Objective: Basilar invagination, odontoid rheumatoid pannus and osteomyelitis result in compression of the brainstem at the cranio-vertebral junction and symptoms of myelopathy. A staged procedure with posterior stabilization and anterior transnasal endoscopic decompression is recently considered a less invasive alternative to the transoral approach. We hereby present a considerably large case series with focus on the operative technique and neurological clinical outcome. Methods: We retrospectively reviewed all patients treated in our neurosurgical department from January 2009 to December 2019. Demographics, pre- and postoperative clinical status as well as operative technique and complications were extracted and analyzed. Results: In total, 21 transnasal operations were performed in 18 patients from 2009 to 2019. All but one patient underwent posterior C1-C2 instrumentation prior to the anterior transnasal CT-navigated full-endoscopic decompression. Median duration of symptoms before surgery was 3 months, only 1 patient suffered from Chiari Malformation Type II. Complications occurred in one patient who died from septic organ failure due to his initial diagnosis of osteomyelitis. Lumbar drains were placed in 19% of the cases, transient swallowing disturbances were observed in 41%, which mostly resolved at follow-up. Postoperative CT imaging showed sufficient decompression in 15 patients, 3 patients underwent a transnasal endoscopic re-decompression (16.7%). Conclusions: Transnasal endoscopic odontoidectomy presents a safe procedure with a satisfying clinical and radiological postoperative outcome compared to the transoral approach.
140
A075: Transforaminal Endoscopic Discectomy. Comparison with Microdiscectomy
Roman Khalepa 1
1 FSBI "Federal Neurosurgical Center", Spinal neurosurgical department, Novosibirsk, Russian Federation
Introduction: The incidence of lumbar disc herniation is 11-25% of all complaints about pain in the lumbar spine. Today microdiscectomy is the gold standard for surgical treatment of lumbar disc herniation. Full endoscopic surgical treatment of lumbar disc herniations has similar results. The aim of this trial was to determine whether endoscopic method leads to equivalent, better or worse outcomes than the current ‘gold standard’ of microdiscectomy. Material and Methods: 210 patients with lumbar disc herniation were operated on with full endoscopic transforaminal technique (TED) and 2205 patients underwent microdiscectomy (Micro). The average age of patients was 39 years (14-76). Standard scales and questionnaires VAS, ODI, SF36 were used to objectify and standardize the clinical manifestations of the disease before and after surgical treatment. MRI, CT, and radiography were used to determine the localization of disc herniations, to determine the consistency of herniated disc, to plan a surgical procedure. Clinical outcome defined during 24 months after surgery by visual analogue scale (VAS), Oswestry Disability Index (ODI) and Short Form 36 (SF36) questionnaires. Results: After the surgery, the leg pain, backpain (VAS), disability (ODI) and quality of life (SF36) were significantly improved (P < .001) in both groups. When comparing the results of TED and standart microsurgical method, it was established that the indices of back (2.4 vs 3.1 respectively) and leg pain (1.7 vs 2.5), disability (ODI 30 vs 31) and quality of life (SF36 MH 42 vs 38; PH 40 vs 36) after endoscopic technique are better but without statistically significant difference (P value > .05). There were 19 (9%) of complications after TED and 104 (4.7%) after microdiscectomy: unintended durotomy (13 (6.4%) vs 79 (3.5% respectively), transitory hypalgesia (3 (2.1%) vs 25 (5%)), retroperitoneal haematoma (1 (0.7%) vs 0 (0%)). Revision surgery (4 (2.1%) vs 11 (0.5%)). Recurrent disc herniations (TED 12 (5.7%) vs microdiscectomy 94 (4.3%)). McNab results: excellent 28% endoscopy vs 26% microdiscectomy; good 56% vs 58%; satisfactorily 16% vs 15%; unsatisfactory 0% vs 1%. Conclusion: Transforaminal endoscopic discectomy and microdiscectomy give comparable outcomes. A less leg and back pain, better parameters of physical ability and quality of life after endoscopic technique due to minimal surgical trauma but are offset by a greater requirement for revision surgery and complications.
250
A076: Comparison of Primary Versus Revision Lumbar Discectomy Using a Biportal Endoscopic technique
Min-Seok Kang 1 , and Hyun-Jin Park 2
1 Bumin Hospital Seoul, Orthopedic Surgery, Seoul, South Korea
2 Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Orthopedic Surgery, Seoul, South Korea
Introduction: The outcomes of the microscopic revision lumbar discectomy (Micro-RLD) are acceptable, but it is known to be inferior to the microscopic primary lumbar discectomy (Micro-LD). The peridural scar formation that inevitably accompanies the primary LD, is the main reason why Micro-RLD is more difficult, increasing the risk of complication such as unintended durotomy, nerve injury, and iatrogenic spinal instability. The biportal endoscopic technique (BE) for primary LD has known to yield similar clinical outcomes and patient satisfaction to Micro-LD, but incurred less bleeding loss, hospital stay and postoperative pain. This study aims to compare the clinical outcomes of patients who underwent the BE-LD and BE-RLD. Material and Methods: A retrospective study of a prospectively collected data was conducted on 81 consecutive patients who underwent BE-LD or BE-RLD and could be follow-up for more than 12 months, between March 2018 and June 2019. Patients were divided into two groups: Group A (BE-LD) and Group B (BE-RLD). Recurrent Lumbar disc herniation (RLDH) was defined as case in which the lumbosacral radicular pain recurs after a pain-free period after primary Micro-LD, and the RLDH was confirmed by magnetic resonance imaging. Clinical outcomes included visual analogue scale (VAS), Oswestry Disability Index (ODI), and modified MacNab’s criteria. In addition, total operation time, length of hospital stay (LOS), amount of surgical drain, and kinetics of serum creatine phosphokinase (CPK) and C-reactive protein (CRP) were recorded. Results: Eighty-one patients were enrolled in this study; 59 from group A and 22 from group B. The demographic data was comparable between the two groups. Both groups were observed to have significant improvement in pain (VAS) and disability (ODI) compared to the baseline values from two days after surgery (P < .05), which lasted until the final follow-up. According to the modified MacNab’s criteria on the follow-up, 88.1 % of the patients was excellent or good in Group A and 90.9% in Group B. There were no significant differences between the two groups in regard to operating time, LOS, amount of surgical drain, and variation of serum CRP and CPK level. There was also no significant difference in improvement of VAS score and ODI score between Group A and B. Two cases of incidental durotomy, one case of epidural hematoma, and one case of local recurrence occurred in Group A. All but one patient who had local recurrence were recovered without secondary surgical treatment. One case of incidental durotomy and one case of epidural hematoma occurred in Group B. Conclusion: BE-RLD showed less postoperative pain, favorable functional improvement, and early laboratory recovery equivalent to BE-LD. Although this study is limited by its retrospective design, the results suggest that even in the BE-RLD, it is useful because of its less invasiveness and clinical results.
1600
A077: Full Endoscopic Lumbar Discectomy f or the Treatment of Lumbar Disc Herniation and Radiculopathy: An Observational Study and Experience of a Single Surgeon in 273 Patients
Wael Chaaban 1
1 Healthpoint Hospital LLC, Spine Unit, Orthopedic department, Abu Dhabi, United Arab Emirates
Introduction: Many endoscopic techniques to treat different spinal motion segment disorders has been described. The Open Lumbar Microdiscectomy has been the Gold standard for the treatment of Lumbar disc Herniation (LDH) with radiculopathy since long time; however, Full Endoscopic Lumbar Discectomy (ELD) is becoming a less invasive surgical alternative with similar benefits and outcomes; with shorter Hosp stay and earlier return to work. Materials and Methods: 273 Patients with LDH and radiculopathy underwent to Full Endoscopic Lumbar Discectomy by a single surgeon between August 2012 and July 2019 with a minimum follow up of 1 year were included in the study. These patients include 177 male and 96 females, with mean age of 37.5 (18-68 years). Patients with other spinal co-morbidities like instability, Lumbar canal stenosis, Discogenic Low Back pain, Deformities and Failed Back surgery syndrome were not included in the study. Either Transforaminal (TELD) or Interlaminar (IELD) approach was decided based on Herniation features on preoperative images and Surgeon experience. Side of approach was decided based on dominant symptoms side. A 25° scope was used to operate all cases. The Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) were measured before the procedure and at 3, 6 and 12 months after the procedure. Length Hospital stay, Return to work, Recurrence/re-intervention rate, Incomplete decompression, overall complication and complication/related factors were also measured in the study. Results: 315 segments were operated, 231 patients underwent a single level procedure and 42 patients underwent 2-levels procedure. Overall satisfaction rate was 89.74% (n:245). The VAS and ODI had both significant improvement after the procedure which keep improved up to 1 year follow up (P < .01). The success rate in patients who underwent a single-level procedure was remarkably higher than those patients who underwent 2-levels procedures (97.40% vs. 47.62%). The overall complication rate was 2.93% (n = 8), Infection 1.10% (n = 3), Incomplete decompression / Residual herniation .73% (n = 2), Recurrence 1.10% (n = 3) but only 1 patient was symptomatic and required a new procedure. Transitory postoperative dysesthesia was seen in 25 patients, where Prolonged operative time (>90 minutes) and Transforaminal approach at L5/S1 level were both significant related factors to present this undesirable post operative outcome. Conclusion: Full Endoscopic Lumbar Discectomy is an effective and safe surgical procedure for the treatment of selected group of patients with Lumbar Disc Herniation and Radiculopathy.
685
A078: A Comparison of Patient Reported Outcomes Between Tranforaminal and Interlaminar Endoscopic Discectomy in Treating Patients with Paracentral Disc Herniation: A Randomized Controlled Trial
Vit Kotheeranurak 1 , Weerasak Singhatanadgige 2 , Worawat Limthongkul 2 , Khanathip Jitpakdee 1 , Wicharn Yingsakmongkol 2 , and Jin-Sung Kim 3
1 Queen Savang Vadhana Memorial Hospital, Conburi, Thailand
2 Chulalongkorn University, Orthopaedic department, Bangkok, Thailand
3 The Catholic University, Seoul St.Mary's Hospital, Neurosurgery, Seoul, South Korea
Introduction: Transforaminal endoscopic lumbar discectomy (TELD) and interlaminar endoscopic lumbar discectomy (IELD) are the minimally invasive procedures that have been increasing in popularity when dealing with surgical cases of herniated nucleus pulposus (HNP) patients. The paracentral disc herniation can be treated with both techniques. We aimed to compare the patient-reported outcomes (PROs) between TELD and IELD in treating patients with paracentral-typed HNP patients. Material and Methods: Fifty-six patients with paracentral-typed disc herniation were randomized into two groups: the transforaminal and interlaminar group. The patients have then received treatment according to their groups and they all completed at least 3 months of follow-up. The patient-reported outcomes were assessed according to the Oswestry Disability Index (ODI), Visual Analog Scale (VAS) score for back leg and wound, and modified MacNab criteria. The operation time, intraoperative radiation time, hospitalization period, returned-to-work time, and complications were obtained. All parameters were compared between the two groups. Student t-test, a Mann-Whitney U test, and a χ 2 were used in statistical analysis. Results: All the patients completed follow up with a mean of 6.8 months (range, 3.1-9.8 months). In the TELD group, the mean operation time was 51.0 ± 7.3 minutes, and the intraoperative radiation time was 4.60 ± 1.32 seconds. While in the IELD group, the mean operation time was 42.2 ± 23.4 minutes, and the intraoperative radiation time was 0.57 ± 2.21 seconds. There were significant differences in operation time and radiation time between the two groups (P < .01) but not in the hospitalization period, return-to-work time, or complication rate (P > .05). There were 2 incidental dural tears, and 1 recurrent herniation in the IELD group and 1 recurrent herniation in the IELD group. Concerning the PROs, patients’ satisfactory rates were 82.6% (19/23) and 87.0% (20/23) owing to the good-to-excellent modified Macnab criteria without a significant difference (P > .05). The postoperative ODI and VAS were significantly improved in the two groups when compared with preoperative status (P < .01) which achieved a minimal clinically important difference (MCID). Early postoperative wound pain was more in the IELD group (VAS = 3.4 ± 1.2 vs 0.8 ± 0.3, P = .047) but not different after 2 weeks follow-up periods. Conclusion: Both IELD and TELD yielded good PROs without statistical difference. The patients in the IELD group experienced a slightly earlier postoperative pain than in the TELD group. However, without any anatomy restriction, IELD provides a more familiar operative orientation associated with shorter operative time and less radiation exposure when compared to the TELD. Skillful needle placement could reduce the operative time and radiation exposure in TELD surgery.
229
A079: Percutaneous Endoscopic Lumbar Discectomy: Presentation of 110 Operated Cases in Argentina and Revision of the Surgical Technique
Guillermo Frucella 1 , and daniel maldonado 2
1 COT, Neurosurgery, Rosario, Argentin
2 HECA, Neurosurgery, Rosario, Argentina
Introduction: Percutaneous Endoscopic Lumbar Discectomy (PELD) is a minimally invasive technique that has been used in different countries since the late eighties for the treatment of Herniated Discs. The purpose of this article is to present the results of the clinical evolution of 110 patients operated on for different lumbar disc herniations by percutaneous endoscopic technique, with a six-months follow-up. Likewise, to describe the technique performed and the most relevant aspects of the preoperative planning, including the percutaneous entry point. Materials and Methods: In a group of 110 patients who together had 141 discs operated on between April 2016 and October 2019, data were collected on patient age and gender, clinical presentation, MRI abnormalities and preoperative Planning (measuring the distance between midline and Skin Entry Point with target in the herniated disc fragment). A directed fragmentectomy was performed in all cases, and then supplemented with the In-Out technique. The main data recorded was the difference in Oswestry scores (ODI) before and after surgery at 6 months after the procedure. The duration of the operation, the length of hospitalization, and the need for reoperation were also verified. All patients were operated awake, receiving epidural anesthesia and sedation. Results: 110 patients and 141 herniated discs were operated on. The average reduction in ODI at 6 months was 47.5 points (SD = 5.7), representing a mean reduction percentage of 85% (SD = 9.5). From the technical point of view, it was possible to average the distance from the midline to the Skin Entry Point, according to the level operated and the chosen approach. Conclusion: Analyzing the results in our series of 110 patients with lumbar herniated discs operated on awake by percutaneous endoscopy, improvements in average pain of 85% were obtained at six months. The endoscopic technique can be considered as an effective procedure for patients with foraminal, extraforaminal and central herniations at the L3L4, L4L5 and L5S1 levels.
32
A080: Partial Pediculotomy, Partial Vertebrotomy Approach for Posterior Endoscopic Cervical foraminotomy and Discectomy
Pang Hung Wu 1 , Hyeun Sung Kim 2 , Ji Yeon Kim 2 , and Il-Tae Jang 2
1 National University Health Systems, Jurong Health Campus, SINGAPORE, Singapore
2 Nanoori Gangnam Hospital, Seoul, South Korea
Introduction: Cervical radiculopathy is a common cervical spine condition. There is paucity of literature in discussing the effect of partial pediculotomy and partial vertebrotomy for posterior endoscopic cervical foraminotomy (PPPV PECF) on cervical radiculopathy. We investigate the radiological and clinical outcome of this approach. Materials and Methods: Retrospective evaluation of 30 cases with cervical radiculopathy underwent PPPV PECF. Preoperative, post-operative roentgenogram for evaluation of stability, Computer Tomography evaluation of foraminal dimensions and area in sagittal view was performed. 3D reconstruction area of decompression evaluations were performed. Clinical outcomes of Visual Analog Scale (VAS), Oswestry Disability Index(ODI) and MacNab’s score were evaluated. Results: There was no complication and recurrence in our PPPV PECF cohort during the study period. At preoperative, 1 week postoperative, and 3 months postoperative and final follow up, the mean Visual Analog Scale had significant improvement with scores of 7.6, 3.0, 2.1, and 1.7 respectively, P < .05; and the mean Oswestry Disability Index with scores of 73.9, 28.1, 23.3, and 21.5 respectively, P < .05. MacNab’s criteria showed all patients scoring good and excellent. Radiological result showed PPPV PECF had significant increase in decompression in the foramen area all CT measured parameters, as compared to the mean preoperative values; 1) sagittal area increased 60.1+/- 23.1 mm², 2) CT Cranio- Caudal length increased 4.0+/- 1.54 mm and 3) CT ventro-dorsal length increased 4.0 +/- 1.97 mm and 4) 3D CT scan reconstruction decompression area increased 996+/- 266 mm², P < .05. Conclusion: PPPV PECF is a safe route of decompression of cervical spine with good clinical and radiological outcome.
34
A081: Comparative Clinical and Radiologic Cohort Study: Uniportal Thoracic Endoscopic Laminotomy with Bilateral Decompression Using One Block Resection Technique and Thoracic Open Laminotomy with Bilateral Decompression for Thoracic Ossified Ligamentum Flavum
Pang Hung Wu 1 , Hyeun Sung Kim 2 , Ji Yeon Kim 2 , and Il-Tae Jang 2
1 National University Health Systems, Jurong Health Campus, Orthopaedic Surgery, Singapore
2 Nanoori Gangnam Hospital, Seoul, Spine Surgery, Seoul, South Korea
Introduction: Thoracic Ossified Ligamentum Flavum is an uncommon cause of thoracic spinal canal stenosis. Symptomatic thoracic myelopathy secondary to Thoracic Ossified Ligamentum Flavum often required decompression spinal surgery. We aimed to evaluate the comparative clinical and radiological outcomes in uniportal endoscopic versus open thoracic decompression for Thoracic Ossified Ligamentum Flavum. Materials and Methods: Retrospective evaluation of all patients who underwent Uniportal Thoracic Endoscopic Laminotomy with Bilateral Decompression Using One Block Resection Technique (TE-ULBD) were compared with Thoracic Open Laminotomy With Bilateral Decompression (TOL) for myelopathic patients with thoracic ossified ligamentum flavum. 3 independent fellowship trained spine surgeon evaluated the radiological and clinical outcomes in computer tomography, magnetic resonance imaging scan and clinical charts. Pre and postoperative MRI parameters of axial cut spinal canal area in upper, middle and lower disc, clinical parameters of VAS, ODI and JOA at preoperative, postoperative 1 week, 6 months and final follow up were compared. Results: 35 levels of TE-ULBD performed in 28 patients were compared with 24 levels of TOL were performed. The overall complication rate of TOL was 8.3% with 2 complications while TE-ULBD was 2.8% with one complication. Both TOL and TE-ULBD cohort had significantly improved their VAS, ODI and JOA score when comparisons were made within their cohort. Comparative analysis of TE-ULBD showed statistically significant improvement than TOL in improvement of final VAS and JOA score. The mean difference+/- standard deviation of VAS and JOA improvement in final follow up when compared with preoperative state of TE-ULBD and TOL were .717+/-.131 and 1.03+/-.2 respectively, P< .05. There was no statistical difference in change in preoperative and final ODI and MRI volume at upper, middle and lower disc canal cross sectional area. Conclusion: Uniportal thoracic endoscopic unilateral laminotomy with bilateral decompression achieved significantly improved pain and neurological recovery with equally sufficient spinal canal decompression as compared to thoracic open laminectomy for patients with myelopathy secondary to ossified ligamentum flavum in our cohort of patients.
OP10: Degenerative Lumbar Surgery 1
1037
A082: 6 Month Outcomes for Patients Undergoing Posterior vs Circumferential Surgical Approach for Isthmic Spondylolisthesis
Paul Arnold 1 , Alexander Vaccaro 2 , James Harrop 3 , Steven Ludwig 4 , Darrel Brodke 5 , Justin Smith 6 , Zach Ray 7 , Michael Fehlings 8 , and Branko Kopjar 9
1 Carle Illinois College of Medicine, Urbana, USA
2 Rothman Institute, Philadelphia, USA
3 Thomas Jefferson University, Philadelphia, USA
4 University of Maryland Medical Center, Baltimore, USA
5 University of Utah, Salt Lake City, USA
6 University of Virginia, Charlottesville, USA
7 Washington University School of Medicine, St. Louis, USA
8 Toronto Western Hospital, Toronto, Canada
9 University of Washington, Seattle, USA
Introduction: There is no consensus on the optimal surgical approach in treating isthmic spondylolisthesis (IS). Both posterior and circumferential surgical approaches are used. Materials and Methods: This is an interim analysis of a prospective, multicenter; observational, comparative study of surgically naïve patients with IS grade I-III at a single level between L4 and S1. Subjects are between 18 and 80 years of age, are enrolled at one of 12 sites in North America, and will be followed for 2 years. Patients with significant scoliosis or cauda equina syndrome are excluded. This interim analysis compares 6 months follow-up outcomes between posterior and circumferential surgical approaches. Results: So far, 161 patients have been enrolled (115 posterior and 46 circumferential). The majority of patients were operated at L5/S1 (74.6% posterior and 95.7% circumferential). 6 month data is available for 112/126 subjects (84 posterior and 28 circumferential). At this time point, there are no differences in age, race, gender, or the baseline score values between the groups. There has been an improvement in all endpoints in both groups. While pain outcomes trend better in the circumferential group and EQ-5D scores in the posterior group, neither of these is significant. There are no differences between the posterior and circumferential groups in change in Oswestry Disability Index (ODI) (20.0 and 15.5 respectively, P = .2277); lumbar pain (2.6 and 3.0 respectively, P = .5817); buttocks and leg pain (3.1 and 3.5 respectively, P = .4701); EQ-5D Index (.23 and .14 respectively, P = .098); SF-36 Physical Component Score (PCS) (10.7 and 11.3 respectively, P = .7347); and SF-36 Mental Component Score (MCS) (7.0 and 3.4 respectively, P = .1855). Conclusion: Patients in both treatment groups have improved in quality of life, pain, and functional outcomes. The extent of improvement is clinically meaningful. There are no differences in outcomes between the posterior and circumferential surgical approaches; however, this is an ongoing study and the current sample size is insufficient to provide confirmatory evidence.
519
A083: Do Organs Change Position In Prone Patients Compared to Supine?
Fauzan A. Hashmi 1 , Peter Loughenbury 1 , Richard Fawcett 2 , and Almas Khan 1
1 Leeds General Infirmary, Spine Surgery, Leeds, United Kingdom
2 Leeds General Infirmary, Radiology, Leeds, United Kingdom
Introduction: The lateral retroperitoneal approach to the spine is a minimally invasive route for performing lumbar interbody fusion, traditionally performed in a lateral decubitus position. Recent interest in single position surgery has led to performing the lateral approach in the prone position, enabling the surgeon to proceed to posterior stabilisation without repositioning the patient. Most spine imaging is performed supine, in a different position to surgery. We sought to define the retroperitoneal anatomical relationships to the intervertebral discs in the prone position compared to supine, so the surgeon may be aware of hazards posed by unexpected changes in anatomy. Materials and Methods: This was a retrospective cross-sectional study conducted at the Department of Spine Surgery, Leeds General Infirmary, Leeds, UK. Patients who had undergone concurrent supine and prone axial CT scans were included. A line drawn between the transverse processes at each vertebral level was named the Inter-transverse process line (ITPL) and the following measurements were recorded in supine and prone positions: 1) the distance and change in ITPL to the anterior border of each Psoas Major muscle at L3, L4 and L5 2) the distance and change from ITPL to the posterior margin of each kidney at of L2/L3 or L1/L2. 3) the distance and change from ITPL to the inferior vena cava. Results: A total of 20 patients were included in the study. The mean displacement of Psoas Major at L3 on left was 2.06 mm ± 1.66 mm (range -1-6.0 mm), on right was 1.77mm ± 1.9 mm (range 0-6.0 mm), at L4, on left was 1.0 mm ± 1.60 mm (range -1-5 mm) and on right was 1.33 mm± 1.60 mm (range -2-4.0 mm). At L5, displacement on left was 1.94 mm ± 2.26 mm (range -2-6 mm) whereas on right it was 1.72 mm±2.19 mm (range -2 - 6.0 mm). The mean kidney displacement at L1 on left was 7.17 mm± 2.2 mm (range 3.0 mm-9.0 mm), on the right 6.57 mm ± 5.38 mm (range .0-15.0 mm), at L2 on left was 9.69 mm ± 7.09 mm (range 1-24.0 mm), on right was 11.44 mm ± 4.83 mm (range 0-20 mm) and at L3, on left was 8.27 mm ± 6.75 mm (range -3-21.0 mm), on right was 14.50 mm ± 7.73 mm (range 4-26 mm). The mean displacement of the inferior vena cava was 1.0 mm at L2 and 2.0 mm at L3. Conclusion: In the majority of patients, the kidney position altered in prone compared to supine. The psoas muscles moved minimally, likely due to its vertebral attachments. The great vessels appeared more static; however, some patients showed posterior movement of the Inferior Vena Cava when prone, bringing the vessel closer to the anterior annulus, potentially increasing the risk of great vessel injury during retractor positioning or ALL release. These findings provide insight into possible alterations in clinical anatomy and must be considered when making the surgical approach.
1337
A084: Morphological Changes in The Major Psoas Position in Relation to the Patient Positioning
Rodrigo Amaral 1 , Luiz Pimenta 1 , Gabriel Porkony 1 , Murilo Daher 2 , and Daniel Arnoni 1
1 Instituto de Patologia da Coluna, São Paulo, Brazil
2 Universidade Federal de Goiânia, São Paulo, Brazil
Introduction: The lateral lumbar interbody fusion (LLIF) is a safe and effective technique to treat a vast range of lumbar disorders. The LLIF is a good option for interbody fusion, as it reduces posterior muscle damage, is capable of relief neurological symptoms through indirect decompression, and promotes more significant gains of segmental lordosis than standard posterior techniques. However, the transient plexus symptoms and the small gain of segmental lordosis still burden the traditional LLIF technique. Therefore, the study aims to assess if a prone decubitus frame is capable of promoting a plexus retraction and the increase of the lumbar lordosis in the surgical table. Methods: Singlecentric, retrospective, non-randomized, comparative, observational study. Inclusion Criteria: The patient had consented to have his/her information collected, with no prior lumbar spine surgery. Exclusion Criteria: Patients with deformities or anatomical variations that impossibilities the evaluation of the key structures of the study, unable to complete MRI at the three proposed positions. The following measures were performed: vertebral body AP size, area of major psoas muscle, a distance of the plexus from the posterior border of the vertebrae, distance from the anterior margin of the psoas muscle from the anterior border of the vertebrae, L1S1 lordosis, and L4S1 lordosis. The difference between the two groups was compared using the T-test with, and the difference between 3 groups was compared using Kruskal-Wallis test, a P < .05 being considered significant. Results: Twenty-four patients were included in the study, 14 female (58%), The area of the psoas muscle significantly increased from L1L2 to L4L5, experiencing a subtle decrease in the L5S1 level. The plexus was located in the first quintile of the vertebrae in all positions for L3L4 and at the beginning of the second quintile for L4L5. A significant increase both in L1S1 and L4S1 was observed in the pone decubitus regarding the other two positions (L1S1-57.6 vs 46.5, P < .001; L4S1-40,4 vs 36.9, P < .01) and Dorsal (L1S1-57.6 vs 47.2, P < .001; L4S1-40.4 vs 36.8, P < .05). Conclusion: The prone position promotes an increase in the lumbar lordosis. However, it did not exert significant effect over the plexus position neither in L3L4 nor L4L5.
603
A085: Low Back Pain Patients With Modic Changes Should not be Treated with Antibiotics
Peter Udby 1
1 Zealand University Hospital, Spine Unit, Køge, Denmark
Introduction: This state-of the-art presentation is based on results from three research groups in Sweden, Denmark and Norway. Independently, studies have been conducted with three different perspectives, but with a focus on treatment of patients with Modic changes. The results of these studies have been published in international journals over the last half of 2019. Material and Methods: In Sweden, a multicenter study with 7 participating clinics, where the presence of bacteria in disci were evaluated in two different patient groups (n = 60) were conducted. DNA technology at two independent university clinics in Gothenburg and Uppsala were used to analyze samples from patients undergoing surgery for respectively lumbar disc herniation and scoliosis. In Denmark, a cohort study with 13 year follow-up on low back patients (n = 204) not undergoing surgery was conducted. The purpose was to evaluate the long-term prognosis of Modic changes in back pain and level of functioning. In Norway the effect of antibiotic treatment for back pain was evaluated, in a multicenter study. The study included patients with chronic low back pain (n = 180), with MC1 or MC2 changes, in a randomized placebo-controlled double-blind study in six hospitals. Results: The Swedish study found no relevant difference in presence of bacteria between the two groups. Also, there was no association between back / leg pain and presence of bacteria. It concluded that findings of bacteria or traces of bacteria, described in previous studies, is likely the result of contamination during the surgical process. The Danish study found that physical function measured by RMDQ was similar in the two groups at baseline, but was statistically significantly better in patients with Modic changes at follow-up, 7.4 vs 9.6 (P = .024). In addition, patients with Modic changes had statistically significantly fewer sick days due to back pain at 13 years follow-up, 9.0 vs 22.9 (number of days per year, P = .003). It concluded, that Modic changes in patients was not negatively associated with the occurrence of back pain or function level at 13 years follow-up. In the Norwegian study, the mean difference in RMDQ score between the Amoxicillin and placebo groups for patients with either MC1 or MC2 was -1.6 (95% CI, -3.1 to .0; P = .04). The difference between the groups in patients with MC1 changes was −2.3 (95% Cl, −4.2 to −.4; P = .02), thus not clinically relevant. Similar results were also found for pain intensity and quality of life. It concluded, that three months treatment with Amoxicillin not associated with a relevant patient-reported clinical effect after one year in terms of function (RMDQ) compared to placebo. Conclusion: Based on the available knowledge, including the three Nordic studies that are reported above, there is currently no basis for recommending treatment with antibiotics for back pain with or without radiculopathy, provided there are no signs of serious infection.
770
A086: What Preoperative Factors are Associated with Achieving a Clinically Meaningful Improvement and Satisfaction After Lumbar Fusion for Degenerative Spondylolisthesis? A Multivariate Analysis of 997 Patients
Graham Goh 1 , and Reuben Soh 1
1 Singapore General Hospital, Singapore, Singapore
Introduction: roper patient selection is key to ensuring good surgical results in spine surgery. Identifying preoperative characteristics that predict postoperative outcomes may guide surgical decision-making and facilitate preoperative counselling. This study aimed to identify characteristics associated with clinically meaningful improvement, patient satisfaction and expectation fulfilment in patients undergoing transforaminal lumbar interbody fusion (TLIF) for degenerative spondylolisthesis. Materials and Methods: Patients who underwent a primary, single-level TLIF for degenerative spondylolisthesis between 2006 and 2015 were identified from our institutional spine registry. Demographic and perioperative characteristics were recorded. Patient-reported outcomes (PRO) such as the Oswestry Disability Index (ODI), 36-Item Short-Form Physical Component Score (SF-36 PCS), Mental Component Score (SF-36 MCS), Visual Analogue Scale (VAS) back pain and VAS leg pain were collected preoperatively and at 2 years postoperatively. Patients also completed the North American Spine Society (NASS) questionnaire for patient satisfaction and expectation fulfilment. Multivariate logistic regression was used to identify preoperative characteristics associated with achieving MCID for each PRO, patient satisfaction and expectation fulfilment using a forward stepwise inclusion algorithm. Results: In total, 997 patients were included. Significant improvements in VAS Back, VAS Leg, ODI, SF-36 PCS and SF-36 MCS were observed. The majority of patients achieved MCID (79.5% for VAS Back, 78.4% for VAS Leg, 85.9% for ODI, 76.8% for SF-36 PCS), satisfaction (87.9%) and expectation fulfilment (85.5%) at 2 years. After adjusting for confounding variables, multivariate analyses showed that increasing age and better preoperative ODI were associated with achieving MCID for VAS Back; increasing age and better preoperative VAS Back were associated with achieving MCID for VAS Leg; lower BMI and better preoperative ODI were associated with achieving MCID for SF-36 PCS. Better preoperative SF-36 MCS was associated with MCID attainment for ODI (OR 1.038, 95% CI 1.019-1.057, P < .001), satisfaction (OR 1.034, 95% CI 1.018-1.049, P < .001) and expectation fulfilment (OR 1.024, 95% CI 1.010-1.039, P < .001). Other preoperative variables such as sex, diabetes, arthritis, comorbidity burden and surgical approach were not associated with postoperative outcomes. Conclusion: Older patients were more likely to experience a clinically significant improvement in back or leg pain after lumbar fusion for degenerative spondylolisthesis, while patients with less disability were more likely to experience an improvement in back pain and quality of life. In particular, a patient’s preoperative mental health was independently associated with multiple outcomes, such as clinically meaningful improvement in functional disability, postoperative satisfaction and expectation fulfilment.
1471
A087: Lumbar Disc Herniation Surgery Preferences Amongst Latin America Spine Surgeons: A Web-Based Survey
Asdrubal Falavigna 1 , Miguel Bertelli Ramos 2 , Carolina Matté Dagostini 2 , Nestor Taboada 3 , Alexandre Iutaka 4 , and Cristiano Menezes 5
1 University of Caxias do Sul (UCS), Health Sciences Postgraduate Program, Caxias do Sul, Brazil
2 University of Caxias do Sul (UCS), Cell Therapy Laboratory and Clinical Studies and Basic Models of Spinal Disorders Laboratory, Caxias do Sul, Brazil
3 Pontificia Universidad Javeriana, Neurosurgery Department, Bogota, Colombia
4 University of São Paulo, Orthopedics Department, São Paulo, Brazil
5 Dr. Cristiano Menezes Institute, Spine Surgery, Belo Horizonte, Brazil
Introduction: Lumbar disc herniation surgery is hallmarked by many technical nuances which may vary according to surgeons’ specialty or experience. Post-operative recommendations may also differ according to surgical strategies adopted. This study aims to evaluate the surgical preferences and post-operative recommendations of Latin American spine surgeons in the lumbar disc herniation setting, assessing possible differences according to surgeons’ specialty, experience, and techniques. Material and Methods: A link containing a 22-item questionnaire was sent to AOSpine Latin America members’ e-mails in June 2020. The survey evaluated: (1) General information; (2) Surgical preferences; and (3) Post-operative recommendations of spine surgeons in the setting of lumbar disc herniation surgery. Results: A total of 438 spine surgeons from 18 different countries answered the questionnaire. Of them, 50.7% were neurosurgeons and 49.3% were orthopedic surgeons. The mean experience of the respondents was 11.7 ± 10.4 years of experience (95%CI 10.7-12.6), and the median was 10.0 years of experience. The majority of surgeons (60.3%) perform ≤5 lumbar disc herniation surgeries per month. Sixty-five (14.8%) surgeons do not use any magnification device. The most commonly used were microscope (51.8%) and magnifying glass (47.5%). Magnification devices were more often used by neurosurgeons (97.2%) than by orthopedic surgeons (72.7%) (OR = 13.09;95%CI = 6.72-38.82;P = .001), especially the microscope (OR = 12.21;95%CI = 7.83-21.31;P = .001). The majority of surgeons (57.3%) perform only open surgery. Specialty and years of experience were not related to the type of surgical technique adopted. Surgeons who performed >5 surgeries per month were more likely to use less invasive techniques (OR = 2.01;95%CI = 1.29-3.36; P = .004). Orthosis or lumbar support devices are never or rarely recommended by 71.9% of surgeons. This recommendation was more frequent among orthopedic surgeons than among neurosurgeons (P < .001). The majority (79.5%) recommended only the restriction of flexion movements and weight-bearing activities in the immediate post-operative period. Mild physical activity is recommended within 30 days and after 30 days following surgery by 44.3% and 55.7% of surgeons, respectively. Unrestricted physical activity is recommended within 3 months of surgery by 28.8%, within 6 months by 48.9%, and after 6 months by 22.4%. Surgeons who perform at least one type of less invasive techniques more often recommended the return to light physical activity within 30 days (50.8%) than those who only perform open surgery (39.4%) (P = .02). Surgeons with ≥10 years of experience also recommended also recommended the return to light physical activity within 30 days (49.8%) more often than less experienced surgeons (38.7%) (P = .02). Conclusion: Some surgical preferences and post-operative recommendations varied among Latin American spine surgeons according to their specialty, years of experience, and number of surgeries per month. The majority of Latin American respondents do not use any less invasive technique for lumbar disc herniation surgery. Neurosurgeons used magnification devices more often than orthopedic surgeons. Surgeons with a higher case volume used less invasive techniques more frequently. Orthosis or lumbar support devices were recommended more often by orthopedic surgeons than by neurosurgeons. Early return to light physical activity was further recommended by more experienced surgeons and by those who performed less invasive techniques.
1285
A088: Early Results of 3D Printed Porous Titanium Thoracolumbar Interbody Cages
Peter Loughenbury 1 , Vishal Borse 1 , Robert Dunsmuir 1 , Almas Khan 1 , Peter Millner 1 , Debasish Pal 1 , Abhay Rao 1 , Greg Rudol 1 , Senthil Selvanathan 1 , and Nigel Gummerson 1
1 Leeds General Infirmary, Leeds Centre for Neurosciences, Leeds, United Kingdom
Introduction: Interbody cages can be used as an adjunct when performing a lumbar spinal fusion. Numerous materials and implant geometries are available. Porous cages aim to improve bone ingrowth and biological fixation. We report early experience of a porous 3D printed titanium interbody cage. Methods: Retrospective review of prospectively collected data entered into the British Spine Registry (BSR). All cases performed with 3D printed titanium cages (November 2016 to December 2019) included. Results: 148 cages implanted into 84 patients by 10 surgeons. Mean age 46.7 years (range 17.7-78.7). 83 were single (70), two level (12) or three level (1) fusions plus one case where cages were used above and below a pedicle subtraction osteotomy. Total 99 levels instrumented with interbody cages – 50 tranforaminal lumbar interbody fusion (TLIF) cages and 49 posterior lumbar interbody fusion (PLIF) cages. Mean Oswestry Disability Index (ODI) score improved from 59.2 (SD 21.2) pre-op to 37.3 (SD 21.1) at one year. Over the same period mean Visual Analogue Scale (VAS) back score improved from 7.8 to 3.8 and mean VAS leg score improved from 8.0 to 3.1. Mean EQ5D score improved from 47.2 to 69.3. Complications – cage subsidence (4), broken cage (1), superficial infection (1), incidental durotomy (1). Conclusion: Early clinical results of 3D printed porous titanium interbody cages demonstrate safety and efficacy when used as an adjunct to lumbar fusion. Patient reported outcomes comparable to alternative cages and posterolateral fusion in our unit. BSR surveillance should allow useful comparison with other implants.
963
A089: Is There a Place for Surgical Repair in Adults with Spondylolysis or Grade I Spondylolisthesis? A Systematic Review and Treatment Algorithm
Sirisha Madhu 1 , Naveen Pandita 1 , Miguel Rafael Ramos 1 , Dinesh Shree Kumar 2 , Colum Patrick Nolan 3 , Barry Wei Loong Tan 1 , Jiong Hao Tan 1 , Keith Gerard Lopez 1 , Andrew Thomas 1 , and Naresh Kumar 1
1 National University Health System, Singapore, Singapore
2 Changi General Hospital, Singapore, Singapore
3 National Neuroscience Institute, Singapore, Singapore
Introduction: Surgical repair is less explored than fusion in adults with spondylolysis/low-grade isthmic spondylolisthesis, due to associated disc-degeneration with increasing age. However, there may be a place for lysis-repair in these adults who have pars defect as the only source of pain with no progressive radiological disc-changes. There are no systematic reviews, exploring direct pars-repair in adults. Hence, we conducted a systematic review to: (1) describe the characteristics of adults suitable for pars-repair, and (2)evaluate the effectiveness and safety of various pars-repair techniques. Materials and Methods: This review is in accordance with PRISMA-P guidelines and registered with PROSPERO(CRD42020189208). Studies in English, including patients>18 years with spondylolysis/grade-I spondylolisthesis treated with standard pars-repair techniques, were considered eligible. A systematic search was performed in June 2020 in PubMed, Embase, Scopus and Web of Science databases. The MeSH terms for search were “spondylolysis” and “spondylolisthesis”, while free-text words included “pars interarticularis”, “pars defects”, “repair”, “pars repair”, “surgical repair”, “Buck*”, “Scott*”, “Scott wiring”, “modified Scott”, “Morscher*”, “pedicle”, “screw”, “pedicle–screw–rod system”, “pedicle–screw–hook system”, “minimally invasive”, “minimal access”, “endoscopic”, “percutaneous”, “navigation”, “image-guided”, and “robot*”. Search strings were developed by combining the MeSH and free-text words using Boolean operators. A two-staged screening process was used. The articles identified in four data bases were screened initially by three independent reviewers by reading title/abstracts and applying eligibility criteria. Full-text of shortlisted articles after removal of duplicates were further screened for eligibility by three independent reviewers. Any conflict in article selection was discussed and resolved. Data was extracted from finalised articles into a data-extraction template and narrative synthesis was conducted. Results: A total of 5813-articles were retrieved. Initial screening resulted in identification of 289-articles. Of these, 111-articles (PubMed,n = 34; Embase,n = 51; Scopus,n = 20; Web of Science,n = 6) were available for full-text review. Further screening resulted in exclusion of 63-articles. A final 48-articles were available for data extraction. The total number of adults across 48-studies was 596. The overall age ranged from 19-60 years, with a high proportion of patients being young/middle-aged adults(19-55 years) (n = 593/596;99.5%). Male:female ratio was 4.2:1. Commonest presentation was persistent low-back-pain (LBP) with duration history of 6-144 months. The lysis defect was primarily bilateral (97.9%). The most involved vertebral level was L5(67.9%) followed by L4(16.2%) and multiple levels (14%). Majority had no disc degeneration (82.9%) and no/<25% slippage (98%). Spondylolysis was the primary diagnosis in 85.5% of patients. Diagnostic pars-infiltration test was conducted in 22-studies. Conservative-therapy prior to pars repair ranged from 3-72 months. Buck’s-repair was the commonest technique (27-studies, n = 365), and pedicle-screw-rod method was the least explored. Successful pars-repair was reported in 78%-100% of adults with high rate of radiological union across all techniques. Greater than 85% returned to regular activity/sport within 3-12 months with positive long-term (≥2 years) outcomes in >80% of patients. The complication-rate was 11.7%, with implant loosening in 3.4%. Conclusion: We have established the feasibility, success, safety, and long-term effectiveness of pars-repair in selected adults with spondylolysis/grade-I spondylolisthesis. We propose the following parameters for optimising selection of adults: (1) age:19-55 years, (2) no/minimal disc-degeneration, (3) no progressive disc-changes on serial-MRI, (4) no/<25% slippage, and (5) positive pars-infiltration test. We present a treatment algorithm for adults and conclude that all standard techniques have comparable clinical outcomes/complications.
260
A090: K-Wireless Robotic and Navigation Assisted Pedicle Screw Placement in Adult Degenerative Spine Surgery
Fedan Avrumova 1 , Kyle Morse 2 , Madison Heath 3 , Roger Widmann 3 , and Darren Lebl 1
1 Hospital for Special Surgery, Spine Surgery, New York, USA
2 Hospital for Special Surgery, Academic Training, New York, USA
3 Hospital for Special Surgery, Pediatric Orthopaedic Surgery, New York, USA
Introduction: K-wireless robotic pedicle screw instrumentation with navigation is a new technology potential to improve spinal instrumentation. Barriers to adoption include registration time with a robotic-navigated system and concern about screw positioning. Understanding the learning curve and limitations is crucial for successful implementation. The purpose of this study was to describe a learning curve of k-wireless robotic assisted pedicle screw placement with navigation, screw position, and risk factors for failure of robotic technique. Material and Methods: Retrospective review of prospectively collected data of 65 adult patients (59.7 ± 13.4 years) underwent robotic-navigated posterior lumbar spinal fusion. Registration, screw placement, and positioning times were recorded. All patients underwent intra-operative 3D fluoroscopy (2019-2020) and screw position was compared to pre-operative CT. Results: A total of 364 instrumented pedicles in 65 adult patients (59.7 ± 13.4 years) were planned robotically, 311 (85.4%) of which were placed robotically. Seventeen screws (4.7%) converted to k-wire, 21 (5.8%) converted to freehand, and 15 (4.1%) planned freehand. Reasons for conversion included morphology of starting point resulting in skive(n = 18), soft tissue pressure on drill guide(n = 9), hypoplastic pedicles causing breach(n = 6), and obstructive reference pin placement(n = 2). A total of 17 (5.5%) critical breaches (≥2-4 mm) were recorded, nine (3.6%) critical breaches were in six patients, from soft tissue pressure. An additional two patients exhibited a total of six (1.9%) critical breaches (>2-4 mm) due to hypoplastic pedicles Three screws (.9%) exhibited lateral breaches in one patient, and isthmic spondylolisthesis in another patient causing skive in one screw (.4%). Two screws (.8%) were abandoned due to interference with the robotic arm. Mean time per screw was 3.6 minutes robotically vs 3.7 minutes freehand (P = .08). Decrease in time per robotic screw was found between first to last ten cases, 5.5 minutes vs 2.3 minutes(P = .0001). Robotic-navigation registration showed a decrease in time between the first to last ten cases, 9.1 ± 2.5 minutes vs 6.0 ± 2.0 minutes, (P = .006). Based on axial plane imaging,143 (46.0%) of screws were placed medial with an average displacement of 1.2 ± .9 mm and 170 (54.0%) of screws were placed lateral with an average displacement of 1.2 ± 1.0 mm. In the sagittal plane, there were 117 (37.9%) screws placed cranial to plan with an average difference of 0.6 ± 0.5 mm, and 193 (62.1%) of screws were placed caudal to plan with an average difference of 1.0 ± .6 mm. Overall, screw positioning was within 1.0 ± .7 mm of the pre-operative template in all planes. No adverse clinical sequelae occurred from implantation. Conclusion: A learning curve for robotic k-wireless screw placement showed improvement in screw times within the first several cases. Additional time per screw was not significantly different between freehand and robotic methods, then converged after the first ten cases. Understanding the learning curve and situations where the robotic technique may be suboptimal can help guide the surgeon safe and effectively for adoption, as well as further refine these technologies.
OP11: Spinal Trauma
308
A091: Validation of the AO Spine Sacral Classification System: Reliability Among Surgeons Worldwide
Gregory Schroeder 1 , Brian Karamian 1 , Jose Canseco 1 , Luiz Vialle 2 , Frank Kandziora 3 , Lorin Michael Benneker 4 , Shanmuganathan Rajasekaran 5 , Jörg Holstein 6 , Klaus Schnake 7 , Mark Kurd 1 , Marcel Dvorak 8 , Emiliano Vialle 2 , Andrei Joaquim 9 , Rishi Kanna 5 , Michael Fehlings 10 , Jefferson Wilson 10 , Jens Chapman 11 , Carlo Bellabarba 12 , Cumhur Oner 13 , AO Spine Sacral Classification Group 14 , Christopher Kepler 1 , and Alexander Vaccaro 1
1 Rothman Orthopaedic Institute, Philadelphia, USA
2 Department of Orthopaedics, Catholic University of Parana, Curitiba, Brazil
3 Center for Spine Surgery and Neurotraumatology, BG Unfallklinik Frankfurt am Main, Frankfurt, Germany
4 Spine Service, Orthopaedic Department, Sonnenhofspital, Bern, Switzerland
5 Department of Orthopaedics, Trauma and Spine Surgery, Ganga Hospital, Coimbatore, India
6 Department of Orthopaedic Surgery, Saarland University Medical Center, Homburg, Germany
7 Center for Spinal Surgery, Malteser Waldkrankenhaus St. Marien, Erlangen, Germany
8 Department of Orthopaedics, Vancouver General Hospital, Vancouver, Canada
9 Neurosurgery Division, Department of Neurology, State University of Campinas, Campinas-Sao Paulo, Brazil
10 Division of Neurosurgery, Department of Surgery, University of Toronto, Toronto, Canada
11 Swedish Neuroscience Institute, Swedish Medical Center, Seattle, USA
12 Department of Orthopaedic Surgery, Harborview Medical Center, University of Washington, Seattle, USA
13 University Medical Center, Utrecht, Utrecht, The Netherlands
14 AO Foundation, Davos, Switzerland
Introduction: Current sacral fracture classification systems are mainly descriptive, lack prognostic correlation, and are non-validated. The lack of an appropriate conceptual framework in classifying sacral fractures has resulted in barriers to communication, research, education, and standardized care. The AO Spine Sacral Classification System, a concise and comprehensive hierarchical classification scheme, has recently demonstrated substantial reliability among expert spine and trauma surgeons. Although promising, these results must be validated in the broader clinical context incorporating surgeons of all types from around the world to evaluate generalizability. Therefore the aims of this study were to 1) demonstrate that the AO Spine Sacral Classification System can be reliably applied by general orthopaedic surgeons, as well as subspecialists, universally around the world, and 2) delineate those injury subtypes which are most difficult to classify reliably in order to refine the classification before evaluating clinical outcomes. Methods: The AO Spine Sacral Classification System was applied to 26 cases by 172 surgeons including orthopaedic spine surgeons, general orthopaedic surgeons, neurosurgeons, and orthopaedic traumatologists from around the world. 2 independent assessments were performed 3 weeks apart. Statistical analysis utilized agreement percentages to evaluate the correct classification of each rating in comparison to the gold standard. Cohen’s Kappa (k) statistic was used for classification agreement and reproducibility. Results: A total of 8,097 case assessments were performed. Overall, 94.0% of assessments were correctly classified by morphology type. When stratifying by morphologic group, 98.3% were correctly classified as type A, 92.5% were correctly classified as type B, and 92.3% were correctly classified as type C fractures. Subtype A1 had the highest agreement percentage (95.4%), while fracture subtypes C1 and C3 had the lowest agreement percentages (67.6% and 77.5%, respectively). The Kappa coefficient for inter-observer agreement for all cases was .72/.75 (Assessment 1/Assessment 2), representing substantial reliability. When comparing classification grading (A/B/C) regardless of subtype, the Kappa coefficient was .84/.85 corresponding to excellent reliability. The Kappa coefficients for inter-observer reliability were .95/.93 for type A fractures, .78/.79 for type B fractures, and .80/.83 for type C fractures. The overall Kappa statistic for intra-observer reliability was .82 (range .18-1.00), representing excellent reproducibility. When only evaluating morphology type (A/B/C), the average Kappa value was .87 (range .18-1.00) representing excellent reproducibility. Conclusion: The AO Spine Sacral Classification System is universally reliable among general orthopaedic surgeons and subspecialists worldwide, with substantial inter-observer and excellent intra-observer reliability.
672
A092: Percutaneous Lumbopelvic Fixation Significantly Decreases Blood Loss, Operating Time, and Return to OR Risk Compared to Open Fixation for Unstable Sacral Fractures
Jimmy Zhu 1 , Carlo Bellabarba 1 , Richard Bransford 1 , and Haitao Zhou 1
1 Harborview Medical Center, Orthopedics and Sports Medicine, Seattle, USA
Introduction: Lumbopelvic fixation is a treatment option for unstable sacral fractures albeit having significant wound complications. Percutaneous lumbopelvic fixation has been developed and increasingly utilized in recent years with hopes of addressing certain complications associated with open lumbopelvic association. However, current literature lacks well designed comparison studies due to the diversity of sacral fractures in pattern and displacement. A key piece of information missing in the reported literature is whether open reduction is necessary to achieve stable fixation when comparing to percutaneous group. The purpose of this study is to carefully identity comparable patient populations and fracture patterns that are either treated with open or percutaneous lumbopelvic fixation to determine if percutaneous fixation provides better outcomes. Material and Methods: This study was a retrospective review of patients at a single academic center between the years 2014 and 2019. Current Procedural Terminology (CPT) codes were used to identity patients requiring lumbopelvic fixation. Patients were included if undergoing lumbopelvic fixation for unstable sacral fractures. Exclusion criteria included subacute injury, insufficiency fractures, pathologic fractures, non-unions, pediatric fractures, concomitant lumbar pathologies, including burst fractures and spondylolisthesis. More importantly, sacral fractures that required open reduction, as indicated by operative report, were excluded. Radiographic features were obtained from preoperative CT imaging to classifying fractures based on AOSpine Sacral Classification system by fellowship trained spine surgeon. Demographic data were collected including age, gender, and mechanism of injury. The utilization of open and percutaneous lumbopelvic fixation was surgeon preference. Clinical measures were collected including operative time, blood loss, intraoperative transfusion, length of stay, return to operating room prior to discharge for wound related complications. Student's t-test and ANOVA were used for statistical analysis. Results: Over 650 patients were identified using CPT codes. 67 patients had unstable sacral fractures. 36 patients were excluded, of which 23 required open reduction methods. For the remaining 31 patients, 15 were treated with open lumbopelvic fixation and 16 were treated with percutaneous technique. There was no significant difference in patient demographics or fracture morphology according to AO classification between the 2 groups. In the percutaneous group, the average estimated blood loss was 168 ml, which was significantly less than 434 ml in the open group (P = .0065). The average OR time in the percutaneous group was 130 minutes compared to 200 minutes in the open group (P = .0094). Length of stay was similar in both groups, 27 days in percutaneous group compared to 24 days in open group. 4/15 patients in the open group developed deep wound infection and required return to OR prior to discharge, all within 30 days. 0/16 patients in the percutaneous group developed infection or wound related complications requiring return to OR prior to discharge (P = .043). The average return to OR in open group was 20 days. Conclusion: Percutaneous lumbopelvic fixation significantly decreased blood loss, operative time, and in-hospital wound complications or infections requiring return to operating room. This conclusion was made with the careful selection of comparable patient populations and fracture patterns in open and percutaneous groups.
136
A093: Spinal Posttraumatic Deformity: An International Expert Survey Amongst AO Spine Knowledge Forum Members
Erin De Gendt 1 , Gregory Schroeder 2 , Andrei Joaquim 3 , Jin Tee 4 , Rishi Kanna 5 , Frank Kandziora 6 , Gaurav Raj Dhakal 7 , Emiliano Vialle 8 , Mohammad El-Sharkawi 9 , Klaus Schnake 10 , R Shanmuganathan 5 , Alexander Vaccaro 2 , Sander Muijs 1 , and Cumhur Oner 1
1 UMC Utrecht, Utrecht, The Netherlands
2 Rothman Institute, Thomas Jefferson University, Philadelphia, USA
3 State University of Campinas, Campinas, Brazil
4 The Alfred Hospital, Melbourne, Australia
5 Ganga Hospital, Coimbatore, India
6 BG Unfallklinik Frankfurt am Main gGmbH, Frankfurt am Main, Germany
7 Bir Hospital, National Academy of Medical Sciences, Kathmandu, Nepal
8 Cajuru Hospital, Catholic University of Paraná, Curitiba - PR, Brazil
9 Assiut University Medical School, Assiut, Egypt
Introduction: There is no clear definition of clinically relevant spinal posttraumatic deformity (SPTD). This leads to a wide variation in characteristics used for diagnosis and treatment indications of SPTD. In order to understand the current concepts of SPTD a survey was conducted among spine trauma surgeons. The aim of this study was to investigate the different views and opinions of spine experts on the different domains (definition, risk factors and management) of clinically relevant SPTD. Material and Methods: The members of the AO Spine Knowledge Forum Trauma participated in an online survey. The survey was divided in four domains: demographics, criteria to define SPTD, risk factors for SPTD and management of SPTD The data was collected anonymously and analyzed using descriptive statistics, absolute and relative frequencies. Consensus on dichotomous outcomes was set to 80% of agreement. Results: Fifteen members with extensive experience in treatment of spinal trauma participated, representing the five AO Spine Regions. Back pain was the only criterion for definition of SPTD with complete agreement. Consensus (≥80%) was reached for kyphotic angulation outside normative ranges and impaired function. 87% and 100% agreed that a full-spine conventional radiograph was necessary in diagnosing and treating SPTD respectively. The ‘missed B-type injury’ was rated at most important by all but one participant. There was no agreement on other risk factors leading to clinically relevant SPTD. Concerning the management, all participants agreed that an asymptomatic patient should not undergo surgical treatment and that neurological deficit is an absolute surgical indication. For most of the participants the preferred surgical treatment of acute injury in all spine regions but the subaxial region is posterior fixation. Conclusion: There is some consensus among leading experts in the field of spine trauma concerning the definition, diagnosis, risk factors and management of SPTD. This study can act as the foundation for a Delphi study amongst the global spine community
1523
A094: Predicting Survival in Elderly Spine Trauma Patients
Catherine Carlile 1 , Andrew Rees 2 , Jacob Schultz 2 , Inamullah Khan 1 , Jacquelyn Pennings 1 , and Byron Stephens 1
1 Vanderbilt University Medical Center, Nashville, USA
2 Vanderbilt University School of Medicine, Nashville, USA
Background: Spine trauma in the elderly population is increasing in prevalence. Given their often extensive medical comorbidities, surgical decision-making in this patient cohort presents unique challenges when compared to younger patients with similar fracture patterns. The marked decrease in physiologic reserve, bone density and increased cognitive and spatial impairment in these patients lead to a weakened response to injury and traditional severity scores can be unreliable in this population. Predictive nomograms have proven useful in other areas of spine surgery; however, there have yet to be any meaningful clinical tools to predict outcomes following the surgical treatment of spine fractures in elderly patients. The goal of this study was to develop a clinical nomogram to better guide patient care and surgical decision-making in this complicated but rapidly-growing population. Methods: Using data extracted from our clinical trauma registry, we conducted a single center retrospective cohort study. All elderly patients (65+) with spine trauma who presented to a single, level I trauma center from 2010 to 2019 who underwent surgical treatment of their spine fractures were included. Outcomes were identified and recorded including in-hospital mortality, mortality after discharge, medical and surgical complications. Retrospective chart review was completed to record comorbidities, presenting injury information, frailty scores, imaging evidence of sarcopenia and osteopenia, presence of spinal cord injury, as well as long-term outcomes for all patients who underwent operative treatment. Operative specifics including site, approach, number of levels, estimated blood loss were recorded as well as trends in lactate at the time of admission and time of surgery. Results from multivariate logistic regression analyses served as the basis for development of the nomogram. Nomogram calibration and discrimination were assessed graphically and by calculation of a concordance index, respectively. LASSO method was used to identify 12 variables which accounted for the majority of the variance in mortality. A subsequent model was developed with those 12 variables including Age, AO/OTA fracture class (A, B, or C), platelet count on admission, lactate on admission, Max AIS, ASIA score, and MFI-5 score. Results: A total of 1760 patients met inclusion criteria over the 9 years period. Patients were primarily male (n = 934, 53%) with an average age of 76. The overall mortality rate within the study period was 36%. The nomogram model was created with outcome variables of 30d, 90d and 365d mortality after traumatic injury. Conclusions: The incidence of spine fractures in the elderly patient cohort secondary to high-energy trauma (eg., motor vehicle collisions) and low-energy trauma (eg., falls) will continue to increase as the population ages. Previous data has described the patient characteristics and preexisting conditions that imply increased morbidity and mortality in these patients, but this is the first study to be able to use a predictive model to guide care and treatment plans in patients with operative spine fractures. Additional prospective research is indicated and planned to internally and externally validate this nomogram to better determine its predictive value.
1788
A095: Baseline, Effect Size of the AO Spine PROST in a Spine Center in The Netherlands
Erin De Gendt 1 , Dino Ahmetagic 1 , Said Sadiqi 1 , Sander Muijs 1 , and Cumhur Oner 1
1 UMC Utrecht, Utrecht, The Netherlands
Introduction: The evaluation of a spine trauma patient is based on the clinicians views, radiological follow-up and preferably a patient’s health and function questionnaire. The questionnaires previously used in the clinic and research were not designed for spine trauma patients specifically. The AO Spine Patient Reported Outcome Spine Trauma (AO Spine PROST) is specifically developed to measure the function and health status of patients after a spinal trauma. The AO Spine PROST validated for a follow-up up to 13 months on content validity and internal consistency. To integrate the AO Spine PROST in the clinic, it is necessary to provide a baseline. The aim of this study was to provide baseline measurements of the AO Spine PROST. Materials and Methods: Consecutive patients after a spine trauma visiting our outpatient clinic were included. Floor and ceiling effects of the AO Spine PROST were analyzed. Effect size was calculated for each time point using the average change in score divided by standard deviation (SD). A baseline of the AO Spine PROST was formed by calculating the mean and corresponding SD for each time point. Differences in baseline score between patients based on fracture type, fracture level and treatment were analyzed. Results: In total, 166 patients completed the AO Spine PROST at different follow-up (FU) visits: 69 at 2 weeks (FU1), 77 at 6 weeks (FU2), 107 at 3 months (FU3), 89 at 1 year (FU4). Baseline scores for the FU point were as followed: FU1 51 (±19.3), FU2 59 (±18.4), FU3 67 (±19.4) and FU4 72 (± 21.1). 43 suffered from an A0-1-2 fracture, 38 from an A3-4 fracture, 50 from a B fracture, 6 from a C fracture and 29 classified as other. The number of patients per fracture region was: 45 with a cervical, 60 with a thoracic and 28 with a lumbar fracture. In total, 106 patients were treated conservatively and 54 surgical. Baseline scores for the subgroups were all within 1 SD of the main baseline. The largest effect size found in consecutive follow-up was .44 between FU2 and FU3. Largest effect size found overall was 1.07 between FU1 and FU4. Analysis showed no floor or ceiling effect. Conclusion: This study provides a baseline of the AO Spine PROST for the use in an outpatient clinic. Baseline measurements fit within expectations as the mean total score increased over time. We expected to see a difference of more than 1SD in the different fractures subgroups, but unfortunately not all patients completed all the FU-point. As this is an ongoing study the results will be more reliable and the duration of follow-up will be increased to 2 years. Also a further differentiation will be applied to detect certain reference groups.
779
A096: Epidemiology of Spinal Trauma in Trauma-Reference Hospitals in Brazilian Metropolis
Francisco Araujo Jr 1 , Anderson Matsubara 1 , Gabriel Luiz De Souza Kondlatsch 2 , Eric Henrique Batista Schmidt 2 , and Luiz Henrique Cardoso Pereira 1
1 Mackenzie Evangelical University Hospital, Neurosurgery, Curitiba, Brazil
2 Mackenzie Evangelical of Paraná University, Curitiba, Brazil
Introduction: The epidemiological profile of patients who are affected by Spinal Trauma is subject to the interference of numerous variables, mainly the demographic profile as well as the lifestyle of the population studied, thus the epidemiological profile of patients affected by this disease suffers specific variations. according to the study site. Therefore, it is necessary to trace the epidemiological profile regionally, since this trauma is a disease that brings with it great morbidity and mortality, and can cause spinal cord injuries to varying degrees of extent, burdening the public system. Objective: To obtain information to trace the epidemiological profile, as well as to identify the main trauma mechanisms for this type of injury, in addition to their possible outcomes (death rate, spinal cord injury, surgical treatment), in order to stimulate public policies focused on prevention of accidents involving spinal trauma and the reduction of morbidity and mortality from this pathology, in the city of Curitiba-Parana, Brazil. Methodology: Retrospective cross-sectional study. All reports of patients who underwent spine computed tomography in 3 trauma centers of Curitiba in 2018 were analyzed, if the patient had a fracture, his medical record was analyzed, with epidemiological data, mechanism of trauma, characteristics of the associated injury, radiological and surgical data collected. Results: Were analyzed 9752 computed tomography reports and medical records; 705 patients had a spinal fracture due to trauma; approximately 36% were female and 64% were male, with a mean age of 48.23 years (± 20.62), the male mean age was nine years lower than female (45 and 54); the number of cases was higher in younger age groups (peak in 21-30 old), decreasing as age increased; the main mechanisms were traffic accidents (33.76%), falls from height (29.08%) and falls from the same level (25.39%); the most affected segment was the thoracolumbar-transition (T10-L2), with an incidence of 45%; followed by lumbar spine (L3-L5) with 17.12% and lower cervical spine (C3-C7), with 15,27%. The first lumbar vertebra was the most affected (226 fractures) followed by the second lumbar vertebra (154 fractures) and the twelfth thoracic vertebra (114 fractures). Death occurred in 2.84%, spinal cord injury in 5.05%. Almost fifteen percent of the admitted patients were treated operatively. Conclusion: The modal profile of the patient victim of spinal trauma in the year 2018 in the City of Curitiba-PR was that of a young man (between 21 and 30 years old), victim of a Traffic Accident with involvement of the thoracolumbar segment without associated spinal cord injury and under conservative treatment. Therefore, these should be the starting points for the development of new preventive measures in that city. Keywords: spinal injuries, spinal fractures, spinal cord injuries, epidemiology, spine.
1803
A097: Percutaneous SI-screw Fixation in High Energy and Low Energy Pelvic Ring Injuries - A 15 years Retrospective Analysis on Over 640 Screws
Oliver Riesenbeck 1 , Moritz Lodde 1 , Jonas Keller 1 , Maria Eveslage 2 , Josef Stolberg-Stolberg 1 , Michael Raschke 1 , and René Hartensuer 1
1 University Hospital Muenster, Trauma-, Hand- & Reconstructive Surgery, Muenster, Germany
2 University of Muenster, Institute of Biostatistics and Clinical Research, Muenster, Germany
Introduction: Percutaneous sacroiliac-screw (SI-screw) fixation is a well-established procedure for the minimal invasive treatment of posterior pelvic ring injuries. There is only limited clinical data available on risk, safety and immediate effects of SI-screw fixation. Materials and Methods: The present retrospective cohort study investigates percutaneous SI-screw fixation over 15 years in a single, level I trauma center. All high energy pelvic ring injuries were classified according to AO classification. All low energy pelvic ring injuries were classified according to fragility fractures of the pelvis (FFP) classification. Groups were compared concerning general epidemiological data, mobilization, complication rates and duration of stay. Multivariable analyses were performed using logistic regression. Results: Between 2005 and March 2020, 448 patients were treated with 642 SI-screws. 124 injuries were classified AO B, 176 AO C, 117 FFP II, 9 FFP III and 22 FFP IV. The high energy traumata were younger (median age AO B 49.3 years, AO C 46.5 years) than low energy traumata (median age FFP II: 80.2 years, FFP III 71.6 years, FFP IV 76.3 years). The sex distribution favored the male in high energy trauma (f/m 39.7/60.3%) and the female in low energy trauma (f/m 87.8/12.2 %). Multivariable regression analysis revealed and increased risk in AO C compared to AO B (OR 3.5), a similar risk in FFP II compared to AO B (OR .8), an increased risk in FFP III/IV compared to AO B (OR 4.1) and an minimal increased risk in FFP III/IV compared to AO C (OR 1.2). In AO B injuries mobilization was not possible in 8.8 % and a wheelchair had to be used in 11.3%. In AO C injuries mobilization was not possible in 16.5 % and a wheelchair had to be used in 26.7%. In all FFP injuries together 6.7 % mobilization was not possible and in 7.4 a wheelchair had to be used. Conclusion: Percutaneous SI-screw fixation of high energy and low energy pelvic ring injuries facilitates mobilization in most of the cases. Considering the injuries FFP II and AO B injuries seem to be comparable considering complications. FFP III/IV seem to have enormous complication risks even compared to AO C injuries. It is reported, that FFP injuries might be progressive in severity, so early surgical treatment might be advisable.
513
A098: An Independent Intra-and Interobserver Agreement Assessment of the AOSpine Sacral Fracture Classification System
Julio Urrutia Escobar 1 , Arturo Meissner-Haecker 1 , Nelson Astur 2 , Manuel Valencia Carrasco 3 , Ratko Yurac 4 , Gaston Camino Willhuber 5 , and Marcelo Alejandro Valacco 6
1 Department of Orthopaedic Surgery, School of Medicine, Pontificia Universidad Catolica de Chile, Santiago, Chile
2 Santa Casa de Misericordia de São Paulo, Sao Paulo, Brazil and Hospital Israelita Albert Einstein, Morumbi, Sao Paulo, Brazil, San Pablo, Brazil
3 Hospital Mutual de Seguridad, Santiago, Chile, Santiago, Chile
4 Department of Orthopaedic Surgery, Clinica Alemana de Santiago, Chile, Santiago, Chile
5 Institute of Orthopedics “Carlos E. Ottolenghi,” Hospital Italiano de Buenos Aires, Buenos Aires, Argentina., Ciudad Autónoma de Buenos Aires, Argentina
6 Hospital Churruca Visca, Ciudad Autónoma de Buenos Aires, Argentina
Introduction: The AOSpine sacral classification scheme was recently described. It demonstrated substantial inter- observer and excellent intra-observer agreement in the study describing it; however, an independent assessment has not been performed. Purpose: To perform an independent inter- and intra-observer agreement evaluation of the AOSpine sacral fracture classification system. Material and Methods: Complete computerized tomography (CT) scans, including axial images, with coronal and sagittal reconstructions of 80 patients with sacral fractures were selected and classified using the morphologic grading of the AOSpine sacral classification system by six evaluators (from three different countries). After a four-week interval, the 80 cases were presented to the same raters in a random sequence for repeat assessment. We used the Kappa coefficient (κ) to establish the inter- and intraobserver agreement. Results: The inter-observer agreement was substantial when considering the fracture severity types (A, B, or C), with κ= .68 (.63-.72), but moderate when considering the sub-types: k= .52 (.49-.54). The intra-observer agreement was substantial considering the fracture types, with κ= .69 (.63-.75), and considering sub-types, κ= .61 (.56-.67). Conclusion: The sacral classification system allows adequate agreement among different raters and by the same rater on separate occasions. Future prospective studies should evaluate whether this classification system allows surgeons to decide the best treatment and to establish prognosis in patients with sacral fractures
434
A099: Vertebral Fractures and Neurological Injury Associated with Increased Recreational Vehicle Use
Sarthak Mohanty 1 , Alex Beschloss 1 , Sachin Gupta 1 , and Comron Saifi 1
1 University of Pennsylvania, Department of Orthopaedics, Philadelphia, USA
Introduction: Recreational vehicle use has become increasingly popular over the past decade both in the USA and around the world. The global all-terrain vehicle market size was valued at 3.9 billion USD in 2018 and is expected to grow at a rate of 3.1% between 2019 and 20251. Men and women who suffer accidents while using such vehicles are prone to spinal injury 2,3,4. However, few studies have examined this relationship at the national scale. The goal of this study was to investigate the trends between recreational vehicle use and spinal injury nationwide. Material and Methods: This study identified spinal injury cases associated with recreational vehicles using the NEISS (National Electronic Injury Surveillance System) database. National estimates, standard errors, and 95% confidence intervals were derived using the provided survey parameters (strata, weights, and primary sampling units) in the NEISS database. Crude rate, defined as number of cases per 100,000 persons was calculated by diving the total number of cases per year by the annual population published by US Census data. Significance for trends were determined using adjusted Wald tests, for which P < .05 (2-sided) were considered significant. Proportions of fracture and nerve injury by recreational vehicle were determined by Pearson’s Chi Squared Test between bicycles, four wheeled ATVs, 2 wheeled ATVs, and other all-terrain, recreational vehicles. Results: 56,349 spine injuries related to recreational vehicle use were isolated from the database. Injuries located in the lower trunk/lumbar vertebrae were most common (47.9%). 78.0% of all spine injuries were experienced by males. Between 2010 and 2019, there was an increase in national cases of spine injury involving recreational vehicles (P < .00001). Nerve injury was more prevalent in four wheeled ATVs (10.2%) when compared to all-terrain vehicles and two wheeled powered vehicles (2.93%) (P < .0001) (Figure 2A). Lumbar spine injury, despite being the most prevalent region of spine injury, showed lower odds (P < .0001) of being admitted. Conclusion: With the increasing popularity of recreational vehicles, there is high concern for traumatic spinal injury. This study was able to identify increasing numbers of spinal injury related to such vehicle use. Such injuries are not trivial and lead to not only life-altering limitations for patients but also increasing healthcare costs. Physicians and patients alike should remain aware and discuss the potential harms regarding the use of recreational vehicles and their high risk for spinal injury.
References
1. National Center for Injury Prevention and Control. CDC Injury Research Agenda, 2009-2018. (2018).
2. Waitt, T., Reddy, V., Grogan, D., et al. A case of dual three-column thoracic spinal fractures following traumatic injury. Surg. Neurol. Int. 11, 150 (2020).
3. Stern, J. & Anand, R. J. Traumatic Decompression of the Jejunum: A Case of Small Bowel Perforation From High-Speed Motor Vehicle Crash. Am. Surg. 3134820933611 (2020). doi:10.1177/0003134820933611
4. Huang, Z., Hu, C., Tong, Y., et al. Percutaneous pedicle screw fixation combined with transforaminal endoscopic spinal canal decompression for the treatment of thoracolumbar burst fracture with severe neurologic deficit: A case report. Medicine (Baltimore). 99, e20276 (2020).
OP12: Spine Surgical Topics
1969
A100: Total Disc Replacement as a Part of Adult Scoliosis Surgical Treatment of 205 Patients with Minimum of 2 years of Follow-Up
Thierry Marnay 1
1 Clinique du Parc, Montpellier, France
Introduction: Surgical scoliosis treatment in adults must face beyond the curve correction, degenerative disc disease, dislocations, spondylolisthesis with sagittal and frontal unbalance and lumbar kyphosis. 2 technical components of the surgery have been used to resolve those difficult problems: the fixation through the pelvis, with a complete loss of lumbar mobility and its consequences. The higher rate of pseudoarthrosis, despite complex contracts, on one hand, and the necessity of posterior lumbar osteotomies to restore an acceptable lordosis with severe risk of complications on the other hand. The purpose of the study was to explore the capacity to maintain or restore part of mobility and lumbar lordosis, using total disc replacement (TDR), by anterior approach (with or without ALIF) in association with the posterior reduction, fixation. Methods: 205 patients (40M, 165F, 18-82 year old, average age 57 years) with scoliosis and lumbar disc degeneration have received 1 or more TDR between 2000 and 2018. 112 idiopathic scoliosis never operated before, 43 degenerative scoliosis in adults never operated on, and 50 cases already operated on by posterior approach (below prior surgery). 286 TDR Prodisc implanted (129-1 level, 71-2 levels, 5-3 levels). The choice of TDR is one of the key points as with the deformity, there is a need for semi-constrained (fixed center) prosthesis, to neutralize the shear forces and compensate the deficit of anterior and posterior longitudinal ligaments. The patients’ analysis includes the perioperative, preoperative, and postoperative VAS and ODI (3, 6, 12, 24 months follow-up), mobility of the disc replacement and the evolution of the curve (Cobb, sagittal parameters). Results: ODI pre-op was 24/50 and declined to 10 in 24 months, VAS lumbar 7.2, radicular 5.7 prep went to 2.6 and 2.1 at 24 months and stabilized at latest follow-up. The mobility measurement at 24 months showed: 151 of 205 patients had a ROM at the TDR level more than 10 in flexion-extension at 24 months. The lordosis capacity of the implants eventually associated to and ALIF with appropriated angulation, allowed the sagittal balance restoration, with T1 axe correction and pelvic tilt reduction. There were no major complications, 4 anterior hematomas (2 drainages, 2 surgical treatments), 2 partial neurological deficits (1 L4, 1 L5). We had no implant TDR complications, no displacements, no explantation required. 2 cases of screw revised, 6 Posterior device removal (2 total, 4 partial), 2 complementary laminectomies, and 2 extension of posterior instrumentation. Conclusion: The choice of TDR, with a semi-constrained prosthesis and loss restoration of motion and sagittal balance in adult scoliosis. It shows interest in the results, as a clinical and mobility point of view that is maintained in long term follow up. That allows to avoid the pelvic fixation in majority of cases, escaping for the clinical bad results and complications of the lawn posterior constructions extend it to the pelvis and also illuminates the risks of posterior transpedicular osteotomies. In elderly people, there is a need for osteodensitometry measurement and eventually cementopalsty of the vertebrae that receive the prosthesis.
References
1. Kim YJ, Bridwell KH, Lenke LG, et al. Pseudarthrosis in primary fusions for adult idiopathic scoliosis: incidence, risk factors, and outcome analysis. Spine. 2005; 30: 468-474.
2. Shaffer AD, Shonuga OA, Hirsch BP, et al. Sclerostin antibody enhances spine fusion in a rat posterolateral transverse process fusion model: preliminary results. Proc 33rd Annual Meeting of the American Society for Bone and Mineral Research, San Diego, CA, 2011, p S517 (Abstract MO0461).
3. Boden SD, Schimandle JH, Hutton WC. An experimental lumbar intertransverse process spinal fusion model. Radiographic, histologic, and biomechanical healing characteristics. Spine (Phila Pa 1976). 1995 Feb 15;20(4):412-20.
1649
A101: Characteristic Features of Cervical Spine Deformity in Dropped Head Syndrome
Yoshifumi Kudo 1 , Ichiro Okano 1 , Koji Ishikawa 1 , Tomoaki Toyone 1 , Akira Matsuoka 1 , Hiroshi Maruyama 1 , Ryo Yamamura 1 , Chikara Hayakawa 1 , Soji Tani 1 , and Yushi Hoshino 1
1 Showa University, Orthopedic Surgery, Shinagawa-ku, Japan
Introduction: Recently, there are several studies focused on whole spine sagittal alignment of Dropped Head Syndrome (DHS). However, few studies have described the details about cervical deformity of DHS ever. The purpose of this study is to investigate the characteristic features of cervical spine deformity in DHS. Materials and Methods: DHS patients who presented to our hospital in 2014-2019 were included in this study. Patients with cervical spondylotic myelopathy (CSM) were also included as control. The following spinal parameters were assessed: C2-7A (C2-5, C5-7), C2-7ROM (Flex and Extension, C2-5, C5-7), C2-7SVA, T1S. We also assessed the degree of cervical degeneration using cervical degenerative index (CDI: Ofiram E, J Orthopaed Traumatol 2009). CDI consists of four factors; Disc space narrow (D), Sclerosis (S), Osteophyte (O), Listhesis (L) with grading 0(normal)∼3(most severe spondylotic change). Student T-tests were used to compare the two groups. The level of significance was set at P < .05. Results: Forty one DHS patients (10 male and 31 female, average 75.8 ± 8.7 years) and 41 CSM patients (10 male and 31 female, average 75.2 ± 7.6 years) were enrolled in this study. The comparison of data of the radiologic parameters were as follows (DHS vs CSM: P value); C2-7A (-35.53 ± 20.94° vs 15.26 ± 13.92°: P < .0001), C2-7ROM(34.34 ± 20.58° vs 42.26 ± 12.47°: P = .029), C2-7SVA(63.90 ± 15.25° vs 23.34 ± 12.18°: P < .0001), T1S(38.8 ± 23.37° vs 28.58 ± 9.78°: P = .013), C2-7F(-43.24 ± 17.39° vs -11.92 ± 16.10° :P < .0001), C2-7E(-8.90 ± 24.98° vs 30.34±14.42° :P < .0001). In every parameter, there was a statistical significance between two groups. In more detailed analysis in DHS cases, there was no significant difference in C2-5A vs C5-7A (-16.07 ± 14.26° vs -19.46 ± 11.63° :P<), and C2-5F vs C5-7F (-23.09 ± 14.16° vs -20.14±12.71° :P = .36). However, there was a significant difference in C2-5E vs C5-7E(-.83 ± 18.29° vs -8.073 ± 10.72° :P = .0079), that means focal kyphosis at C5-7 remains whereas focal kyphosis at C2-5 reduces to 0° in extension. In assessment of CDI, more degenerative changes were seen in lower levels in both groups. In comparison between DHS and CSM, the scores of Disc space narrowing at C3/4/5/6/7, Sclerosis at C5/6/7, Osteophyte at C4/5/6/7 and Listhesis at C2/3/4/5 of DHS group were significantly higher than these of CSM. This means that massive degenerative changes in lower cervical level and slippage in middle cervical level were more obvious in DHS group compared to CSM group. Conclusion: These results suggest that dropped head deformity is not a simple kyphosis, but is a complexed deformity including severe degeneration with irreversible kyphosis at lower level (C5-7) and reducible listhesis at upper and middle level (C2-5). It is not certain that these characteristic features are cause or consequence of this deformity, however, we believe that these are deeply involved with this pathology. Surgeons should take these characteristic features into account in corrective surgery.
297
A102: Does Posterior Scoliosis Correction Improve Respiratory Function in Adolescent Idiopathic Scoliosis? A Systematic Review and Meta-Analysis
So Kato 1 , Jean-Christophe Murray 2 , Yongyao Tan 3 , Mario Ganau 4 , Yasushi Oshima 1 , and Sakae Tanaka 1
1 The University of Tokyo, Tokyo, Japan
2 Laval University, Quebec City, Canada
3 Hospital for Sick Children, Toronto, Canada
4 Oxford University Hospitals NHS Foundation Trust Oxford, Oxford, United Kingdom
Introduction: Pulmonary dysfunction is often advocated among the indications for surgical correction of adolescent idiopathic scoliosis (AIS). Previous studies have discussed the effect of scoliosis correction on respiratory function without reaching a definitive conclusion: some showed that the respiratory function can improve after scoliosis surgery without defining the precise role of anterior, posterior and combined approaches on this improvement; furthermore, the majority of these studies did not take normal growth into account. As a result, the role of surgery remains to be clarified. The object of the present study was to synthesize the current knowledge regarding changes in respiratory function after posterior corrective surgery for AIS. Material and Methods: A comprehensive systematic search was performed to identify all relevant studies in the following electronic databases: MEDLINE, EMBASE, CINAHL and EBSCO. We focused on the studies that discussed 1) posterior fusion surgery for AIS without thoracoplasty, 2) comparisons of pre- and post-operative percent-predicted values of forced vital capacity (%FVC) or forced expiratory volume (%FEV), 3) with minimum 2 years follow-up. Forest plots were depicted and Z value was calculated as a test for overall effect. Results: Ten studies (6 prospective and 4 retrospective studies) met our inclusion criteria. The overall effect showed that there was no significant difference in %FVC or %FEV between pre- and post-operative measurements (very low evidence). Conclusion: Posterior correction surgery for mild to moderate AIS patients showed no significant improvement of post-operative respiratory function measured by relative, percent-predicted values at minimum 2 years follow-up.
1660
A103: Treatment of Acute Spinal Cord Injuries: Use of High-Doses Steroids - Survey Among Ibero-Latinoamerican Spine Surgeons
Ana Ribau 1,2 , Jorge Alves 3 , and Ricardo Rodrigues-Pinto 1,2
1 Spine Unit (UVM). Department of Orthopaedics. Centro Hospitalar Universitário do Porto, Porto, Portugal
2 Instituto de Ciências Biomedicas Abel Salazar, Porto, Portugal
3 Centro Hospitalar do Tâmega e Sousa, Department of Orthopaedics, Penafiel, Portugal
Introduction: The recommendations for the use of a high dose steroids - Methylprednisolone Sodium Succinate (MPSS) in the management of patients with acute spinal cord injury (ASCI) have changed over the years. While initially recommended based on the initial analysis of the National Acute Spinal Cord Injury Studies (NASCIS), in 2013 the Congress of Neurological Surgeons (CNS) and the American Association of Neurological Surgeons (AANS) recommended against its use. However, more recent evidence and clinical practice guidelines have again suggested a potential benefit of its use, particularly when started in the first 8 hours and only during 24 hours. The aim of this study was to evaluate the current practice of use of MPSS in ASCI among spinal surgeons from Ibero-Latinoamerican countries. Material and Methods: A descriptive cross-sectional study design as a survey was conducted. A questionnaire composed of 2 sections: demographic data regarding the surgeons and MPSS administration, was sent by an email to members of SILACO and associated societies. IBM SPSS Statistics 24 was used for the statistical analysis. Results: A total of 182 surgeons participated on the study: 65.4% (119) Orthopaedic surgeons and 24.6% (63) Neurosurgeons. 69 (37.9%) used MPSS in the initial management of ASCI. There was no significant difference between countries (P = .451), specialty (P = .352) or surgeon seniority (P = .652) for the inclusion of steroids in the initial management of ASCI. From those that used MPSS, 45 (65.2%) reported using an initial high-dose bolus (30 mg/Kg) followed by a perfusion (5.4 mg/Kg) and 28 (65.1%) of them maintain the perfusion for 24 hours, while 13 used a high-dose bolus (30 mg/Kg) and 11 performed a low dose steroid bolus or perfusion. Thirty-eight (65.2%) of the surgeons who used MPSS only prescribed them if the patients presented within 8 hours of ASCI. The majority of the surgeons (50.7% (35)) administrated high dose steroids because of the conviction that it has clinal benefits and will improve the recovery. Conclusion: Results from this survey show that MPSS use in ASCI is not widespread within spine surgeons and that the controversy regarding its use remains unanswered. This is probably due to the low level of evidence of the available data, variations over the years, inconsistencies in acute care protocols and health service pathways.
973
A104: The Clinical Course of Disease During Wait Time for Lumbar Spinal Stenosis Surgery and its Effect on Postoperative Outcome: A Retrospective Cohort Study
Thorsten Jentzsch 1,2 , Kala Sundararajan 3 , and Raja Rampersaud 1,3
1 Toronto Western Hospital, University Health Network; University of Toronto, Orthopaedics, Toronto, Canada
2 Balgrist University Hospital, University of Zurich, Zurich, Switzerland
3 Krembil Research Institute, University Health Network, Arthritis Program, Toronto, Canada
Introduction: The purpose of the study is to evaluate the effect of surgical wait times for spinal surgeries on the clinical course of disease during the wait time and its effect of postoperative outcome for patients with lumbar spinal stenosis. Materials and methods: This was a retrospective cohort study between 2007 and 2019 using a convenience sample of patients from several prospective longitudinal studies that provided preoperative Oswestry Disability Index (ODI) data at two different time points. Wait time was defined as the time period between the date of the initial visit at intake and immediately preoperatively. It was categorized into three different time points (short (<6 vs ≥6 months), moderate (<12 vs ≥12 months), and long (<24 vs ≥24 months)). The primary outcome was the total ODI. It was categorized into minimal clinically important difference (MCID) of <30% vs ≥30% improvement for last follow-up. The Spearman correlation, Wilcoxon rank sum test, and robust regression analysis adjusting for age and surgery type were used. Results: 134 patients were analyzed. The median age was 69.0 (interquartile range (IQR) 14.0) years, 66 (49.3 percent (%)) were female, 89 (66.4%) underwent decompression, while 45 (33.6%) underwent decompression and instrumented fusion. The median wait time was 5.9 (IQR 8.2) months and the postoperative follow-up was 19.2 (IQR 8.1) months. In univariate analysis, wait time was borderline associated with worsening of total ODI scores at the short (P = .051) and moderate (P = .064) time point, and significantly associated at the long time point (0 (IQR 11.8) for <24 months vs 8.0 (IQR 16.0) for ≥24 months, P = .026). In the multivariate analysis, wait time was associated with worsening of total ODI scores at each time point (coefficient 2.7 (95% CI .2-5.2), P = .036). In uni- and multivariate analysis, wait time was not associated with absolute postoperative change in ODI scores, but patients with wait times <12 and <24 months were significantly more likely to reach the ODI MCID at last follow-up (OR = .29 (95% CI .12-.75), P= .011 and OR = .24 (95% CI .06-.93), P = .038, respectively). Conclusions: Clinical outcome assessments of disability from the initial visit at intake may become outdated after six months and are very likely to be outdated after two years, after which the level of disability appears to worsen. Although longer wait times do not appear to negatively influence postoperative outcome in patients with lumbar spinal stenosis considering absolute values, but may potentially impact patients when using MCID. Patients may benefit from measures to reduce wait time for surgery to prevent patients from preoperative deterioration in quality of life. Keywords: wait time, outcome, lumbar, spinal stenosis, surgery
1290
A105: Increase in Thoracic Kyphosis with Aging is the Main Factor that Leads to Positive Sagittal Balance: Results of the Multi-Ethnic Alignment Normative Study (MEANS)
Zeeshan Sardar 1 , Meghan Cerpa 1 , Jean Charles Le Huec 2 , Stephane Bourret 2 , Kazuhiro Hasegawa 3 , Wong Hee Kit 4 , Denni Hey 4 , Hend Riahi 5 , Michael Kelly 6 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
2 CHU Bordeaux, Bordeaux, France
3 Niigata Spine Surgery Center, Niigata, Japan
4 NUH University Spine Center, Singapore, Singapore
5 Kassab Institute, Tunis, Tunisia
6 Washington University, St. Louis, USA
Summary: Volunteers from five countries were enrolled in this radiographic study to evaluate spinal alignment. The results showed no significant difference in lumbar lordosis between the different age groups. Thoracic kyphosis was noted to be significantly higher in patients over the age of 50. The increase in TK appeared to be the main driver for increasing SVA. Interestingly, the odontoid remained centered over the knees and not the hips in the sagittal plane in all age groups despite increasing SVA. Hypothesis: We hypothesize that the spinal alignment in adults changes with age. Study Design: Retrospective review of prospectively collected data. Introduction: Adult sagittal spinal alignment can have a significant impact on overall quality of life. While significant advances have been made over the last few decades in better defining normal alignment, predicting the ideal alignment of a specific individual is still a difficult task. Normal variations of the spinal alignment parameters are studied in this asymptomatic cohort in hopes to define patient specific alignment goals. Methods: Radiographic evaluation of Full-body low dose stereoradiography in the largest reported multiethnic cohort of 488 asymptomatic adult volunteers (Mean age: 40.8; Range: 18-79 years). Patients from 5 different countries were included; France, Japan, Singapore, Tunisia, and the USA. 3D measurements were performed using a commercially available 2D/3D modeling software. Results: The lumbar lordosis was similar between the different age groups with means ranging from 56.7 ± 11.9 to 57.8 ± 11.5 (P = .92). Mean T1-T12 thoracic kyphosis (TK) did increase significantly with age increasing from 43.5 ± 11.9 in patients younger than 50 to 48.6 ± 12.1 in those older than 50 (P < .0001). Following the trend of TK, there was an increase in the sagittal vertical axis (SVA) with age (-13.9 ± 23.3 vs 5.3 ± 32.1; P < .0001). The mean distance between the odontoid and the middle of the knees in the sagittal plane range from -3.2 ± 30.7 to 4.5 ± 32.1, and did not vary significantly with age in asymptomatic patients (P = .26). The patients compensated with increased cervical lordosis, increased hip extension, and increased knee flexion as TK and SVA increased with age to maintain the odontoid centered over the knees. Pelvic tilt also increased with age from 10.5 ± 6.8 to 15.9 ± 7.6. Conclusion: Lumbar lordosis was similar across the different age groups, while thoracic kyphosis increased in patients over the age of 50 and accounted for the increase in SVA. Take Home Message: Lumbar lordosis may not decrease with age as previously thought. Thoracic kyphosis was the main parameter that increased with age and led to an increase in SVA.
1339
A106: Outcome and Predictive Factors in Rapid Progressive Cervical Spondylotic Myelopathy: A Retrospective Case-Control Study
Haimiti Abudouaini 1 , and Hao Liu 1
1 West China Hospital, Sichuan University, Orthopedics, Chengdu, China
Introduction: Cervical spondylotic myelopathy (CSM) is a major cause of cervical spinal cord dysfunction in people over 55 years of age. Most patients with CSM usually present with chronic and phased compression, however, some patients with CSM develop rapid severe neurological dysfunction without any trauma. To our knowledge, markers that can be used for early identification of patients with potential to develop rapid neurological deterioration have not been totally identified. Here, we evaluate epidemiological, clinical and radiographic features associated with the development and prognosis of rapid progressive cervical spondylotic myelopathy (rp-CSM). Material and Methods: A retrospective study was carried out for 175 patients diagnosed with CSM between March 2011 and January 2017 at West China Hospital. Patients were divided into rp-CSM group and chronic CSM (c-CSM) group based on the time taken for neurological deterioration to occur and the severity of preoperative neurological dysfunction. The clinical outcomes were assessed using the Modified Japanese Orthopaedic Association (mJOA) score, and imaging parameters such as Torg-Pavlov Ratio (TPR), intervertebral disc level compression ratio and increased signal intensity (ISI) on T2W1. Multivariate analysis was used to compare the outcomes between the 2 groups and identify potential predictors for rapid neurological dysfunction in CSM patients. Results: Out of the 175 patients enrolled in the study, 25 developed rp-CSM (18 males; median age 59.04 ± 12.81 years) and the remaining 75 (54 males; median age 56.88 ± 12.31 years) were used as controls for the study (c-CSM group). The average time taken to develop severe neurological deterioration was .8 months in rp-CSM group and 24 months in c-CSM group (P = .001), while the preoperative mJOA scores were 6 in rp-CSM patients and 12 in c-CSM patients (P = .014). In addition, rp-CSM patients demonstrated worse outcomes than the controls in one year after surgery (mJOA improvement rate 54.5% and 80%, respectively, P = .021). There were no differences in the clinical parameters evaluated between the two groups except for the history of diabetes and smoking. Analysis of radiographic parameters indicated that TPR MRI, intervertebral disc level compression ratio and increased signal intensity (ISI) on T2W1 were poor in rp-CSM patients compared to c-CSM patients. Regression analysis also showed that the history of diabetes, TPR MRI < 0.4, compression ratio ≥50%, and the sagittal diameter of ISI ≥50% of spinal canal diameter on T2W1 were strongly associated with the rapid progressive neurological dysfunction in patients with CSM. Conclusion: The prognosis of rapid progressive CSM is worse than that of common chronic CSM. The rapid neurological deterioration can be identified by TPR MRI (< .4), compression ratio (≥50%), sagittal diameter of ISI (≥50% of spinal canal diameter). Besides, a history of diabetes is a risk factor for the development of rp-CSM.
1466
A107: Indications of Electromyography in Lumbar Spine Surgery, Literature Review
Alejandro Tejera Morett 1 , Michael Dittmar 2 , Francisco Cruz López 1 , Jorge De Haro Estrada 2 , Francisco Javier Sánchez García 1 , and Isaac López Peña 3
1 Reespalda A.C, Zapopan, Mexico
2 Reespalda A.C, Zapopan, Mexico
3 Hospital Versalles, Zapopan, Mexico
Objectives: The objective of this study is to perform a bibliographic analysis of the indications and usefulness of electromyography (EMG) in patients undergoing spinal surgery diagnosed with lumbar disc herniation. Material and Methods: Studies from the last three decades were collected, referring to the use, utility and indications of pre-surgical electromyography in degenerative lumbar spine surgery, in electronic databases Cochrane, Medline, Google Scholar, Pubmed, Scopus and Science Direct, articles that used electromyography as a study to diagnose lesions in the cervical region were excluded. Bibliographic analysis: EMG has been used to study physiological aspects of muscle activity. Two currents were identified, the first that prevailed during the 1990s, in which the combination of EMG with magnetic resonance imaging (MRI) was used for the diagnosis of radiculopathy, in studies of the next two decades, MRI prevailed as a diagnostic method since it has a greater sensitivity and specificity. Currently, electromyography is used as a diagnostic method of post-surgical lesions and sensitivity is affected by the technique performed and the professional interpreting the study. Discussion: It is necessary to emphasize that despite the accessibility and diffusion that was given to this diagnostic method in the early 1990s, it is currently a study that can be dispensed with since non-invasive studies such as magnetic resonance imaging are more effective, without However, in complex cases, where the clinical symptomatology does not correspond to the radiographic diagnosis, or the patient has neuromuscular pathologies that make the clinical diagnosis prior to surgery complex, electromyography has proven to be of help for preoperative planning. EMG has a greater impact on the diagnosis of post-surgical lesions. Conclusions: The EMG, for diagnosis of degenerative lumbar pathology is in disuse, due to the little information it provides prior to surgery, it is suggested to carry out the study after surgical procedures where the evolution has not been the desired one.
1661
A108: Observational Prospective Study of Efficacy of Non-Operative Management of Thoracolumbar Osteoporotic Compression Fractures
Ankit Singh 1 , and Nishat Goda 1
1 K J Somaiya Medical College and Research Centre, Orthopaedics, Mumbai, India
Introduction: Majority of the osteoporotic compression vertebral fractures occur at the thoracolumbar region as it is a zone of structural and functional transition thus vulnerable to injury. These fractures occur most commonly in elderly following trivial trauma prompting disability, debilitating pain and poor quality of life. There has been a noted trend in surgical intervention being employed frantically. To diminish the economic burden in a resource limited and developing region and in patients with significant comorbid conditions, non-operative treatment is of prime significance and we assess its efficacy prospectively. Material and Methods: Consecutive 40 patients with diagnosed thoracolumbar osteoporotic compression fractures excluding those with neurodeficits were subjected to the foreordained protocol of non-operative treatment encompassing analgesics, short period of bed rest, anti-osteoporotic drug therapy (Calcium, Vitamin D3, bisphosphonates, calcitonin intra-nasal spray) orthotic bracing (hyperextension braces) and guided physiotherapy under supervision. Demographics, clinical history and examination findings with relevant radiographic and hematology parameters were recorded. Clinical examination findings, VAS (Visual analogue scale) score, Oswestry disability index (ODI), hematological and radiological findings were assessed at 3 months,6 months and 12 months’ follow up after start of treatment. Counselling regarding compliance was carried at each follow up and whenever deemed necessary. Results: Patients’ mean age was 61.7 +/ - 11.45 years with female preponderance (63.3%) and 90% being postmenopausal. 30% patients had hypertension and 16.7% patients had diabetes mellitus while 10% patients were obese. Back pain followed by deformity were chief complaints with VAS score and ODI score being 6.74 ± .55 and 42.40 ± 16.13 respectively. 6 months following treatment, noteworthy reduction in the VAS score (P < .05) and the ODI scores (P < .05) were found, with VAS score and ODI score improving by 49.1% and 45.50% respectively from the baseline at 12 months post-treatment. Anti-osteoporotic regimen normalised the serum Vitamin D, calcium, phosphorus, alkaline phosphatase and Parathyroid hormone levels. Kyphotic angles were found to be unchanged. None of the patients developed any form of neurodeficit during the course of treatment. Conclusion: With the increasing longevity of the population, the incidence of this age related disease process is increasing. Patients often believe that the pain and impaired mobility associated with these fractures are permanent and that little can be done besides surgical intervention. Resortment and compliance to multifaceted non-operative plan of management is effective in mitigating backache, disability in patients with thoracolumbar osteoporotic compression fractures especially in those with associated co-morbidities and is viable in forestalling further worsening of the disease process. The efficacy was evident on clinical, hematological and radiological examination thus improving quality of life. Keywords: non-operative management, thoracolumbar, osteoporotic compression fractures, efficacy
OP13: Surgical Complications of Adult Deformity
1943
A109: Patients with Severe Baseline Global Alignment and Proportion may Require More Aggressive Age-Adjusted Alignment Goals for Lumbo-Pelvic Mismatch
Peter Passias 1 , Katherine Pierce 1 , Nicholas Kummer 1 , Lara Passfall 1 , Oscar Krol 1 , Sara Naessig 1 , Waleed Ahmad 1 , Bassel Diebo 2 , Renaud Lafage 3 , Virginie Lafage 3 , and Shaleen Vira 4
1 NYU Langone Orthopedic Hospital; New York Spine Institute, Departments of Orthopaedic and Neurologic Surgery, New York, USA
2 SUNY Downstate Medical Center, Department of Orthopaedics, Brooklyn, USA
3 Hospital for Special Surgery, Department of Orthopedics, New York, USA
4 UT Southwestern Medical Center, Department of Orthopedics, Dallas, USA
Introduction: For surgical adult spinal deformity (ASD) patients, the age-adjusted alignment ideals were proposed in order reduce the occurrence of complications such as proximal junctional kyphosis (PJK). The under- and overcorrection of the postoperative age ideal value for the mismatch between pelvic incidence and lumbar lordosis (PI-LL) has yet to be related to the Global Alignment and Proportion (GAP) Score. Materials and Methods: ASD patients with baseline (BL) and 2 years postoperative (2Y) radiographic and HRQL data were included. Age-Adjusted correction groups generated at postoperative follow-up for actual alignment compared to age-adjusted values for PI-LL-adjusted ideal values (Matched, Overcorrected, Undercorrected). GAP Score in the literature includes the four parameters relative pelvic version, relative lumbar lordosis, lordosis distribution index, relative spinopelvic alignment, and an age factor to formulate a sagittal plane score out of 13 (Proportional, Moderately Disproportional, Severely Disproportional). GAP improvement scores were noted as less at 2Y compared to BL, with deterioration as an increase in score at 2Y. Means comparison and chi-squared ANOVA analyses assessed the relationship between pre- and postoperative GAP scores in the PI-LL age-adjusted correction groups. Results: Included: 140 ASD patients (55.5 ± 16.4 years, 81% female, 25.2 ± 4.7 kg/m2). At BL, mean SS: 30.7°, PT: 23.2°, PI: 54.5°, PI-LL: 13.3°, SVA: 61.6 mm, and L1-S1: 40.4°. Assessment of 2Y age-adjusted PI-LL alignment found that 20.3% of patients Matched, 45.1% Overcorrected, and 34.6% Undercorrected. Baseline GAP assessment across the age-adjusted correction groups found that the patients who were Overcorrected, Matched, and Undercorrected groups had similar scores (Over: 6.3, Under: 7.2, Match: 7.6; P = .282). At 2 years, mean GAP score for the Undercorrected group was found to be 7.5 (+0.3), while the Matched group was 4.8 (-2.8) and the Overcorrected group was 3.0 (-3.3), P < .001. 49.1% of Overcorrected patients were Proportional in GAP at 2 years (Under: 15.2%, Matched: 15%, P < .001). The Undercorrected group had significantly more patients who were classified as Severely Disproportional in GAP at 2Y (63%, vs Matched: 25%, Overcorrect: 7%, P < .001). The Overcorrected age-adjusted PI-LL group was found to improve in their GAP score from BL to 2Y more (61.4%, P < .001), while the Undercorrected group was found to remain the same proportionality in their GAP score (74.4%, P < .001) and deteriorate (18.6%, P = .042) significantly more than the Matched and Overcorrected groups. Patients who were Undercorrected in PI-LL and had severe proportionality in GAP at 2Y had more major complications (41.4% vs 22.5%; P = .041) and underwent more reoperations (34.5% vs 16.2%; P = .029) compared to the remainder of the cohort. Conclusion: Patients who are Overcorrected in their PI-LL age-adjusted alignment are more likely to improve and become proportional in their GAP scores at 2 years, implying that certain subgroups require more aggressive realignment.
1247
A110: Prospective Validation of the Spinal Cord Shape Classification System (SCSCS) to Assess the Risk of Intraoperative Neuromonitoring Data Loss with Thoracic Deformity Correction
Meghan Cerpa 1 , Alex Sielatycki 1 , Scott Zuckerman 1 , Earl Thuet 1 , Griffin Baum 2 , Paul Park 1 , Nathan Lee 1 , Joseph Lombardi 1 , Zeeshan Sardar 1 , Ronald A. Lehman 1 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
2 Northwell Health, New York, USA
Summary: We present a prospective validation of the novel spinal cord shape classification system (SCSCS) that is able to identify patients with Type 3 spinal cords (spinal cord deformed against the concave pedicle in the axial plane), have 4x greater odds of losing monitoring data during thoracic deformity correction versus type 1 or 2 spinal cords. Hypothesis: Preoperative morphology of the spinal cord within the spinal canal assessed at the thoracic apical concavity can be used to predict intraoperative loss of intraoperative neuromonitoring (IONM) data. Study Design: Prospective single-center cohort. Introduction: A prior retrospective study of the SCSCS demonstrated increased risk of IONM data loss in type 3 spinal cords, and we now present a prospective study to further validate this novel preoperative SCSCS to identify spinal cords at risk for data loss with correction of thoracic spinal deformity. Methods: 176 consecutive patients undergoing surgical correction of a thoracic deformity with pedicle screw/rod constructs were prospectively enrolled. Spinal cords were classified into 3 types based on the appearance of the cord on the apical axial T2 MRI: Type 1 a circular/symmetric cord with visible CSF between the cord and the apical concave pedicle/vertebral body; Type 2 a circular/oval/symmetric cord with no visible CSF between the concave pedicle and the spinal cord; Type 3 a spinal cord that is flattened/deformed by the apical concave pedicle or vertebral body, with no intervening CSF. Logistic regression was used to assess odds ratios and predictor variables of losing IONM data. Results: Of 176 patients, 93 (53%) had a Type 1 cord; 46 (26%) had a Type 2 cord, and 37 (21%) had Type 3 spinal cord shapes. IONM data changes in trans-cranial motor-evoked potentials (TcMEPs) and/or somatosensory evoked potentials (SSEPs) in 44 (25%; P < .001) cases; 19/93 (20%) in Type 1, 6/46 (13%) in Type 2, and 19/37 (51%) in Type 3. On regression analysis, Type 1 and 2 spinal cords showed a protective effect against IONM data loss (OR = .24, 95%CI: .11-55; P < .001; OR = .14, 95%CI: .05-.42; P < .001). Type 3 spinal cords had a significantly higher odds of IONM data loss (OR = 4.1, 95%CI: 1.8-9.3; P < .001). Vertebral column resection itself was not associated with loss of IONM data (P = .12). Conclusion: This prospective validation of the novel SCSCS to identify patients with increased odds of losing IONM data with thoracic spinal deformity correction, we found that Type 3 spinal cords were 4x more likely to have IONM data changes than types 1 or 2. Take Home Message: We recommend careful review of the axial apical MRI to classify the spinal cord morphology using the SCSCS which demonstrates a markedly increased risk of losing IONM during deformity correction.
1524
A111: The Impact of Preoperative Cross-Sectional Area of Psoas Muscle on Postoperative Outcomes of Adult Spinal Deformity Surgery
Hikari Urakawa 1 , Kosuke Sato 1 , Renaud Lafage 1 , Jonathan Elysee 1 , Avani Vaishnav 1 , Yucheng Yao 1 , Han Jo Kim 1 , Frank Schwab 1 , Virginie Lafage 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
Introduction: Proximal junctional kyphosis (PJK)/ proximal junctional failure (PJF), which is caused by soft tissue or bony failure, is a critical challenge in ASD surgery. The cross-sectional area of psoas muscle has been used as a parameter of sarcopenia and reported to have a negative impact on functional outcomes of lumbar spinal surgery for degenerative diseases. However, it is unclear whether it also impacts outcomes of adult spinal deformity (ASD) surgery. The aim of this study was to examine the impact of preoperative cross-sectional area of psoas muscle on postoperative outcomes of ASD surgery. Material and Methods: ASD patients who were over 18 years old and underwent fusion surgery with >5 levels with > 6 months follow-up were included in this study. The cross-sectional area of psoas muscle was measured at L3/4 on T2-weighted axial images of preoperative MRI. Normalized total psoas area (NTPA) was calculated as total psoas area normalized to patient height. Patient reported outcome measures (ODI, SRS-22), radiographic parameters (PT, PI, SS, LL, SVA, C2-C7 SVA, C2-T3 SVA, TS, TK, TPA and Cobb angle) and prevalence of PJK/ PJF were evaluated at pre-op and 6 months. Results: The total of 65 patients were included in this study. All patients underwent a posterior spinal fusion, if needed, in conjunction with osteotomy. The median of NTPA at L3/4 was 806 (range 482-1194) mm2/m2 in males and 629 (range 315-1129) mm2/m2 in females. It was significantly higher in males than in females (P = .018). Patients were divided into 2 groups [lower NTPA group (LG) and Higher NTPA group (HG)] at the point of the sex-specific lowest quartile of NTPA threshold (male 573 mm2/m2, female 493 mm2/m2). ODI and SRS-22 including all sub-items except for mental health were worse in the LG at 6 months compared to the HG, however, no significant differences were found between groups at all points. In radiographic parameters, C2-C7 SVA was significantly higher in the LG at pre-op and 6 months (pre-op LG 34.2 ± 14.8° vs HG 26.4 ± 11.8°, P = .040; 6M LG 34.5° ± 17.4° vs HG 26.9°±10.3°, P = .044) Additionally, SS at pre-op and 6 months was significantly lower in the LG at pre-op and 6 months (pre-op LG 25.0° ± 11.3° vs HG 33.9° ± 12.7°, P = .013; 6M LG 30.9° ± 7.9° vs HG 37.9° ± 10.8°, P = .025). Prevalence of PJK was significantly higher in the LG, compared to the HG (LG 50.0% vs HG 18.4%, P = .021). There were no patients with PJF in both groups. Conclusion: The decrease of psoas cross-sectional area on preoperative MRI significantly increased prevalence of PJK. It was also associated with higher C2-C7 SVA and lower SS before surgery and at 6 months. This muscle-health related parameter may be useful for a decision making in ASD surgery.
1811
A112: Stratifying Outcome Based on the Oswestry Disability Index for Operative Treatment of Adult Spinal Deformity on patients 60 years of Age or Older: A Multicenter, Multi-Continental Study on Prospective Evaluation of Elderly Deformity Surgery (PEEDS)
Christopher Nielsen 1 , Colby Oitment 1 , Allan Martin 2 , Thorsten Jentzsch 1 , Anna C. Rienmüller 1 , Han Shear Yashuv 1 , and Stephen Lewis 1
1 Toronto Western Hospital, Arthritis Program, University of Toronto, Department of Orthopaedic Surgery, Toronto, Canada
2 Toronto Western Hospital, Arthritis Program, University of Toronto, Department of Neurosurgery, Toronto, Canada
Introduction: Patients with adult spinal deformity suffer from disease related disability as measured by the ODI for which surgery can result in significant improvements. The purpose of this study was to show the change in overall and individual components of the Oswestry Disability Index (ODI) in patients aged 60 years or older following multi-level spinal deformity surgery. Material and Methods: A prospective, multicenter, multi-continental, observational longitudinal cohort study was performed of patients ≥60 years undergoing primary spinal fusion surgery of ≥5 levels for coronal, sagittal or combined deformity. 12 sites participated in this study. Local investigators assessed and included patients for eligibility and performed the surgeries according to their standard of care with techniques according to their discretion. ODI forms were completed at baseline, 10vweeks, 12 months, and 24 months. ODI scores were grouped into deciles. Change was calculated based on total range of ODI scale and improvement or worsening was further categorized from baseline as substantial (≥20%), marginal (≥10% - <20%) or no change (within 10%). Results: Two-hundred nineteen patients met inclusion criteria for the study. Most patients were female (80.1%) and Caucasian (56.6%), and the mean age was 67.5 years. The mean BMI was 26.1 kg/m2 with over 50% of the patients being either overweight (29.7%) or obese (21.5%). Aggregate BMD scores demonstrated that 43% of patients had normal BMD, 45.6% of patients were osteopenic, and 11.4% were osteoporotic. The median number of spinal levels fused was 9 [Q1 = 5.0, Q3 = 12.0]. 2 years mean (95% CI) ODI improvement was 19.3% (16.7%; 21.9%; P < .001) for all age groups, with mean scores improved from a baseline of 46.3% (44.1%; 48.4%) to 41.1% (38.5%; 43.6%) at 10 weeks (P < .001), 28.1% (25.6%; 30.6%) at 12 months (P < 0.001), and 27.0% (24.4%; 29.5%) at 24 months (P < .001). At 2 years, 45.5% of patients showed 20% or greater improvement in ODI, 23.7% improved between 10% and 20%, 26.3% reported no change (defined as ± 10% from baseline), 4.5% of patients reported a worsening between 10-20%, and none reported worsening greater than 20%. 59.0% of patients were severely disabled (ODI >40%) pre-operatively, which decreased to 20.2% at 2 years. Significant improvement was observed across all 10 ODI items at 12 and 24 months. The largest improvements were seen in pain, walking, standing, sex life, social life and traveling. Conclusion: In this prospective, multicenter, multi-continental study of patients 60 years or older undergoing multi-level spinal deformity surgery, almost 70% of patients reported significant improvements in ODI without taking into account surgical indications, techniques or complications.
51
A113: Adult Spinal Deformity Surgery: Instrumentation-Related Complication-Free Survival
Nikita Zaborovskii 1 , Dmitry Ptashnikov 1 , Dmitry Mikhaylov 1 , Oleg Smekalenkov 1 , Sergei Masevnin 1 , and Anton Denisov 1
1 R.R.Vreden National Medical Research Center of Traumatology and Orthopedics, Saint-Petersburg, Russian Federation
Introduction: The surgical management of adult spinal deformity can provide significant improvements in pain, disability, and health-related quality of life. However, these procedures are technically demanding and are associated with a high complication rate. Complications arising from spinal surgery instrumentation present a host of challenges in prevention as well as treatment. We explored the factors that influence the duration of instrumentation-related complication-free (IRCF) survival in adult deformity surgery. Material and Methods: One hundred ninety four patients with spinal deformity (SRS-Schwab type L, sagittal modifiers: 2 grade and more) were included, and the following parameters were studied: age, sex, body mass index (BMI), comorbidities, smoking status, neurological deficit, presence of osteoporosis, Oswestry Disability Index (ODI), Miller frailty index, previous spinal surgeries, type of osteotomy, levels of instrumentation, pelvic fixation, presence of anterior interbody fusion at L5-S1 (ALIF L5-S1), pelvic incidence (PI) and lumbar lordosis (LL) mismatch to evaluate spino-pelvic re-alignment. Instrumentation-related complications were implant instability and proximal junction disorders requiring revision. Multivariate Cox proportional hazard model analysed clinical parameters for their prognostic relevance. Results: The 12 months IRCF rate is 89%. The 24 months IRCF rate is 48%. In patients with instrumentation-related complications, multivariable analysis suggested that severe Miller frailty index (95% CI 1.19-5.87; HR 2.64), ODI less than 40 scores (95% CI 1.16-8.67; HR 3.17), 3-column osteotomy (95% CI 1.46-7.23; HR 3.25), pelvic fixation (95% CI 1.25-13.17; HR 4.21), overcorrection of PI - LL mismatch (95% CI 1.09-6.92; HR 2.74) impacted the probability of shorter IRCF survival. The model found that ALIF L5-S1 was associated with better IRCF survival (95% CI .14-.79; HR .33). Half of adult spinal deformity patients had instrumentation-related complications 2 years following surgery. Individual patient characteristics at baseline as well as surgical invasiveness influence the duration of IRCF survival in adult deformity surgery. Conclusion: Preoperative Miller frailty index, ODI score, type of osteotomy and instrumentation, overcorrection of PI - LL mismatch influence the duration of IRCF survival in adult deformity surgery.
1754
A114: Complications of Multilevel Surgery in Elderly Patients: The Prospective Evaluation of Elderly Deformity Surgery (PEEDs)
Sigurd Berven 1 , Larry lenke 2 , Michael Venezia 3 , Allan Martin 4 , John T. Street 5 , Eric Klineberg 4 , Michael kelly 6 , Justin Smith 7 , Christopher Shaffrey 8 , Yong Qiu 9 , Marinus deKleuver 10 , Kenneth Man Chee Cheung 11 , Ahmet Alanay 12 , Yukihiro Matsuyama 13 , David Polly 14 , and Stephen Lewis 15
1 UC San Francisco, San Francisco, USA
2 Columbia University Medical Center, New York, USA
3 University of Tampa, Tampa Bay, USA
4 UC Davis, Sacramento, USA
5 University of British Columbia, Vancouver, USA
6 Washington University, St Louis, USA
7 University of Virginia, Charlottesville, USA
8 Duke University, Durham, USA, 9 University of Beijing, Beijing, China
10 University of Utrecht, Utrecht, The Netherlands
11 Hong Kong University, Hong Kong, China
12 Acibadem Maslak Hospital, Istanbul, Turkey
13 Hamatsu University School of Medicine, Hamamatsu, Japan
14 University of Minnesota, Minneapolis, USA
15 University of Toronto, Toronto, Canada
Introduction: The appropriateness of surgery for patients with deformity of the spine is based upon the expected risks and benefits. Understanding the risks of spinal deformity surgery in elderly patients is important to empower informed choice for patients and physicians. Complications of surgery in elderly patients with spinal deformity are reported with significant variability in the literature. The purpose of this study is to report the observed complications over a two year period after surgery in elderly patients undergoing multilevel surgery. Methods: The study is a review of data from a prospective multicenter observational longitudinal case series with 12 sites distributed around the world. Patients included were adults over age 60 with spinal deformity who were treated with primary spinal fusion of at least 5 segments. The Adverse Events (AEs) were collected prospectively throughout the study at an individual institutional level, and the collection of data was overseen by on site and remote data monitors. The severity of AEs, and the relationship to treatment was determined by the site investigators. Complications were classified into Medical, Neural, and Surgical complications, and the timing, severity and resolution of complications were recorded. Results: 219 of the 255 patients enrolled from 12 centers met the criteria for inclusion in the study. There were 176 females and 43 males with a mean age of 67.5 (range 60-83 years). 124 patients suffered AEs within the 2 years FU period, and the total number of AEs recorded was 289. AEs were rated as mild in 29 pts (23.4%), moderate in 36 pts (29.0%) and severe in 59pts (47.6%). There were a total of 101 SAEs, of which 81 were treatment related. The most common SAEs were implant failure, junctional pathology, and neural injuries. AEs were classified as Medical, 50pts (23%), Neural in 55 pts (25%), and Surgical in 79pts (36%). Rating complications by intervention required, 44 (15%) required no intervention,162(56%) required Testing and Diagnostic interventions or minimal interventions (transfusion, intraoperative interventions, medicine changes). 7 complications (2%) required invasive non-surgical interventions, and 76 (35%) required a surgical intervention. The outcome of the AEs at patient level was: 66 patients (53% of the patients with AE) recovered without persist damages; 40 patients (32%) were still in the process of recovering at the end of FU; five patients (4%) sustained persistent damages; and five patients (4%) died, and the resolution remains unknown for 8 patients (7%). Conclusions: Complications are common in multilevel fusion surgery for elderly patients with spinal deformity. Understanding the types of complication, rates and severity of complication, interventions required and resolution is important to guide informed choice regarding the appropriateness of surgical interventions in this population. Further work will identify specific risk factors for complications, and correlate complications with changes in health status, and with satisfaction with surgery.
458
A115: Postoperative Complications and Unplanned Readmission After Adult Spinal Deformity Surgery. Multicentric Registry in Latin America
Gaston Camino Willhuber 1 , Alfredo Guiroy 2 , Mariano Servidio 3 , Fernando Nin 4 , Murilo Daher 5 , Bruno Saciloto 6 , Allan Ono 7 , Olavo Letaif 8 , Fernando Alvarado Gómez 9 , Ratko Yurac 10 , Baron Zarate-Kalfopulos 11 , Nelson Astur 12 , Emiliano Vialle 13 , and Marcelo Alejandro Valacco 3
1 Hospital Italiano de Buenos Aires, Institute of Orthopedics “Carlos E. Ottolenghi,”, Ciudad Autonoma de Buenos Aires, Argentina
2 Hospital Español de Mendoza, Mendoza, Argentina
3 Hospital Churruca Visca, Ciudad Autonoma de Buenos Aires, Argentina
4 Medica Uruguaya Casmu, Montevideo, Uruguay
5 Universidade Federal de Goiás, Goiânia, Goiânia, Brazil
6 Clínica Bambina, Guarapuava, Brazil
7 Clínicas da Faculdade de Medicina FMUSP, San Pablo, Brazil
8 Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, San Pablo, Brazil
9 Hospital Universitario Fundación Santa Fe de Bogotá, Bogotá, Colombia
10 Universidad del Desarrollo, Santiago, Chile; Spine Unit, Department of Orthopedic and Traumatology, Santiago, Chile, 11 Instituto Nacional de Rehabilitación, Distrito Federal, Mexico., Mexico, Mexico
12 Hospital Israelita Albert Einstein, Morumbi, San Pablo, Brazil, San Pablo, Brazil
13 Cajuru Hospital, Catholic University of Parana, Curitiba, Brazil., Curitiba, Brazil
Introduction: Postoperative complications in adult spinal deformity surgery is associated with increased morbidity, hospital length of stay and health care costs. The prevalence of complications in adult deformity is heterogenous mainly based of lack of proper registry and consensus of a universally accepted classification of complications. The objective of this study was to register the prevalence of postoperative complications and analyze its risk factors based on two different classifications for postoperative complications. Material and Methods: A retrospective multicentric registry from 8 centers in Latin America was conducted. We included patients of 18 years or older with adult spinal deformity based on at least one of the following parameters: thoracic, thoracolumbar or lumbar scoliosis with a cobb angle of at least 20 degrees, sagittal vertical axis of 5 cm or more, pelvic tilt of 20 degrees or more or thoracic kyphosis of 60 degrees or more treated with spinal fusion of at least three levels. Patients with spinal fracture, infection, tumor or Parkinson disease were excluded. We analyzed the rate of postoperative complications a modified Clavien-Dindo and Glassman classification at 30 days, unplanned readmission and hospital length of stay was also analyzed. Results: 172 patients were included based on our defined criteria (mean age 54.4 ± 7.2). 62% of all cases suffered at least one complication according to Clavien-Dindo system, 18% of complications were considered major. Hospital length of stay was significantly higher in patients with complications (median: 21 days, range 6-142 days) compared with patients without complications (median of 5 days, range 3-9 days). Factors associated with increased risk of complications were age, number of levels fused and postoperative time. Conclusion: Postoperative complications reached a 62% rate in spinal fusion after adult spinal deformity. This is the first multicentric registry of postoperative complications after fusion surgery in Latin America, more studies are required to stablish the real usefulness of Clavien-Dindo Classification when assessing the rate of complications.
714
A116: Predictors of 30 Day Complications in Deformity Correction Surgery: A National Database Study
Yaroslav Gelfand 1 , James Lin 2 , Simon Morr 3 , Meghan Cerpa 3 , Griffin Baum 4 , Joseph Osorio 5 , and Lawrence Lenke 3
1 Montefiore, New York, USA
2 Mount Sinai, New York, USA
3 Columbia University Medical Center, New York, USA
4 Northwell Health, New York, USA
5 University of California San Diego, San Diego, USA
Summary: We analyzed a multi-center operative database for independent predictors of 30 days morbidity and length of stay in spine deformity patients. We found that dependent functional status along with ASA class, age, and operative time were predictors of complications, while transfusions, operative time, dependent functional status, ASA class of 3 or greater, female gender, and anemia were predictors of prolonged length of stay. ASA class over 3 and op-time were predictors of severe complications, but those are often unmodified factors. Hypothesis: Certain pre-operative patient characteristic along with operative parameters are predictive of 30 days postoperative complications and length of stay in deformity surgery. Design: Patients undergoing surgery for adult deformity correction were identified in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2006 to 2016. Introduction: Knowledge of pre-operative patient characteristics that contribute to post-operative morbidity would be helpful in risk stratification and pre-op evaluation. Methods: Inclusion criteria were CPT codes for deformity surgery, a combination of ICD 9 and 10 codes for deformity (kyphosis, scoliosis, proximal junctional kyphosis, etc.) with a combination of CPT codes for a 5 or more level fusion. Multivariate regression model was used to analyze the predictors of non-neurologic complications, severe complications and the length of stay within 30 days of surgical intervention. Results: 2869 cases fit the inclusion criteria. Mean age was 56.4, 36.3% were male, and 63.7% female. Complications occurred in 13.0% of cases, life-threatening complications in 5.2%. Wound infection was the most common complication (3.1%). On multivariate regression predictors of complications were dependent functional status (OR 2.5 95% CI: 1.6-3.8, P < .001), ASA calss of 3 or greater (OR 1.7 95% CI: 1.3-2.2, P < .001), age over 55 (OR 1.6 95% CI: 1.2-2.1, P = .004), and operative time (OR 1.2 95% CI: 1.2-1.3, P < .001), while predictors of severe complications were only ASA category of 3 or greater (OR 1.6 95% CI: 1.0-2.4, P = .031) and operative time (OR 1.2 95% CI: 1.1-1.3, P < .001). Predictors of the length of stay (LOS) were blood transfusion (OR 3.8 95% CI: 3.2-4.5, P < .001), operative time over 7 hours (OR 2.9 95% CI: 2.4-3.8, P < .001), dependent functional status (OR 2.6 95% CI: 1.9-3.5, p<0.001), ASA class of 3 or greater (OR 1.6 95% CI: 1.4-1.9, P < .001), female gender (OR 1.4 95% CI: 1.2-1.6, P < .001), and anemia (OR 1.3 95% CI: 1.1-1.5, P = .001). Conclusion: We identified independent predictors of complications, severe complications, and prolonged length of stay for better patient risks stratification.
357
A117: 30-Day Complications for Deformity Correction Surgery in Patients Older and Younger Than 55
Yaroslav Gelfand 1 , James Lin 2 , Joseph Osorio 3 , Meghan Cerpa 4 , Griffin Baum 5 , Simon Morr 4 , and Lawrence Lenke 4
1 Montefiore, New York, USA
2 Mount Sinai, New York, USA
3 University of California San Diego, San Diego, USA
4 Columbia University Medical Center, New York, USA
5 Northwell Health, New York, USA
Summary: This is a multicenter retrospective review of patients undergoing deformity surgery comparing the complications between those younger and older than 55. Results showed that while severe complications, mortality, and length of stay were not significantly different between the groups, those over 55 suffered more overall complications, were more likely to be discharged to rehab or sub-acute rehab, and more likely to require unplanned return to the operating room. Hypothesis: Older patients (over 55) are generally sicker and are more likely to suffer from post-surgical complications. Design: National database study. Introduction: This is a retrospective review of multicenter national database to compare the complications in deformity surgery for patients older than 55 to those younger than 55. Methods: Patients undergoing surgery for adult deformity correction were identified in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2006 to 2016. Inclusion criteria were CPT codes for deformity surgery, a combination of ICD 9 and 10 codes for deformity (kyphosis, scoliosis, proximal junctional kyphosis, etc.) along with a combination of CPT codes for a 5 or more level fusion. Two groups were established: patients under 55 (group 1) and patients over 55(group 2). Multivariate analysis was used to compare those groups. Results: Total of 2869 cases fit the inclusion criteria. Mean age was 56.4, 36.3% were male, and 63.7% female. 1012 (35.3%) of patients were younger than 55 and 1857 (64.7%) were 55 or older. Complications occurred in 13.0% of cases: 8.4% and 15.6% in group 1 and 2 respectively (OR 1.4 95% CI: 1.1-1.9, P = .018). Severe (life-threatening) complications accounted for 5.2%: 3.5% and 6.2% in groups 1 and 2 respectively, but was not significant on multivariate analysis (OR 1.3 95% CI: .9-2.1, P = .207). Overall mortality was .4% and did not differ between the groups (P = .329). Return to the operating room was more likely in those over 55 (7.0% vs 4.0%), and that remained significant in multivariate regression (OR 1.6 95% CI: 1.1-2.4, P = .027). Discharge to any rehab (OR 4.7 95% CI: 3.7-6.0, P < .001) or subacute rehab (OR 5.7 95% CI: 4.0- 8.1, P < .001) were much more likely in those 55 years of age or older. The length of stay (OR 1.1 95% CI: 1.0-1.3, P = .112) was not significantly different. Conclusion: We found no significant difference in severe complications, mortality, or length of stay between those younger and older than 55. Those over 55 were significantly more likely to suffer from any complication, have unplanned return to the operating room, and had higher rates of discharge to rehab.
OP14: Novel Diagnostics
156
A118: Subclassification of Sanders Stage 7: The Use of Ulna Physis Can Improve Decision-Making for Brace Weaning in Adolescent Idiopathic Scoliosis
Prudence Wing Hang Cheung 1 , and Jason Cheung 1
1 The University of Hong Kong, Orthopaedics and Traumatology, Hong Kong, Hong Kong
Introduction: Adolescent idiopathic scoliosis(AIS) is a three-dimensional deformity which progresses rapidly during pubertal growth spurt and stablizes near skeletal maturity. Previous studies found that curve progression can occur if bracing is weaned at Sanders stage (SS) 7 which represents the early mature stage. A wide range of radiographic appearance occurs from open to fusion of the distal radius and ulna physis between SS7 and SS8. This warrants the investigation of whether subclassification of SS7 allows more accurate identification of skeletal maturity that can lead to an earlier and safe timing for brace weaning. The distal radius and ulna (DRU) classification utilizes the radiographic appearance of the distal radius and ulna comprehensively, and gradings are readily available for assessing decelerating growth and growth cessation. This study aims to investigate whether including the stages of ulnar physeal closure in SS7 aids in more accurate maturity assessment for brace weaning in AIS. Materials and Methods: This was a retrospective analysis of AIS patients at a specialist clinic from June 2016 to Decemeber 2018. Patients who weaned brace-wear at Risser stage ≥4, static standing body height and arm span for at least 6 months and ≥2 years post-menarche were included. Skeletal maturity at weaning was assessed using DRU classification and Sanders staging with SS7 subclassified into SS7a (all phalangeal physes are fused and only distal radial physes are open, with narrowing of medial physeal plate of the distal ulna) and SS7b (those with >50% fusion of the medial growth plate of distal ulna). The relationship of weaning maturity grading and any curve progression was analyzed using Fisher’s exact test, with Cramer’s V and Goodman and Kruskal’s tau. Results: A total of 179 AIS patients (83.2% females) were studied with mean age of 14.8 ± 1.1 years and Cobb angle of 34.6 ± 7.7° at weaning. Follow-up period was 3.4 ± 1.8 years. At post-weaning 6-months, curve progression rates for patients weaned at SS7a versus SS7b were 11.4% and 0% respectively for <40° curves. Similarly, curve progression rate for weaning at U7 was 13.5% vs 0% for weaning at U8. Skeletal maturity assessment at weaning using SS6, SS7a/b, SS8 strongly associated (Cramer’s V: .326, P = .016) with whether curve progressed at post-weaning 6 months. Weaning with SS7 subclassification allowed a significant 10.6% reduction of error in predicting curve progression. For curves ≥40°, post-weaning curve progression rate was not associated with any maturity grading at weaning. Conclusion: The use of SS7a and SS7b allows accurate maturity assessment for guiding brace weaning in patients with AIS. Weaning at SS7b or U8 is more appropriate without any curve progression cases immediately post-weaning for small curves <40°. This makes reaching full fusion of both distal radius and ulna physis (SS8) not necessary and brace weaning can be initiated approximately 9.0 months earlier. This study demonstrates the importance of accurate bone age assessment for more precise timing for weaning, avoiding the overuse of bracing while limiting the risk of curve progression. For large curves, curve progression can occur regardless of the skeletal maturity status at which weaning takes place.
116
A119: Utility of Magnetic Resonance Imaging in Diagnosing the Pathology of Vertebral COmpression Fractures - Comparison of 3 Observers and Radiologist with Biopsy Report
Shaffaf Kareem 1
1 Manipal Hospitals HAL Airport Road Bangalore, Spine Care Department, Bangalore, India
Introduction: Vertebral compression fractures (VCFs) in elderly maybe benign (due to osteoporosis) or malignant. Literature shows inconsistent results with Magnetic Resonance Imaging (MRI) in differentiating between them. Biopsy obtained during cement augmentation procedures (CAPs) like Kyphoplasty or vertebroplasty of such VCFs helps in confirming the diagnosis. This study aims to find the usefulness of MRI in differentiating benign from malignant VCFs when compared to their biopsy obtained during the time of CAP, and to evaluate the clinical outcome of the procedure. Methods: Retrospective observational study was done using the database collected from January2017 to January2020. All patients who underwent CAP for VCFs following no/trivial trauma with a histopathological diagnosis were included in the study. The agreement between MRI and biopsy reports was studied. Each MRI images were also read by 3 spine-fellows for inter-observer agreement. For evaluation of intra-observer agreement, these MRI images were read again by the same fellows after 2 weeks duration. Clinical outcome was assessed by Visual-Analogue-Scale (VAS) and Modified-Oswestry-Disability-Scale (MODS) evaluated pre-operatively and compared with values recorded at 3 months post-procedure. The intra-observer agreement of the spine-fellows (done at zero and at 2 weeks) over the MRI diagnosis, and the inter-observer agreement between the spine fellows and radiologist diagnosis (taken as the gold standard for MRI diagnosis) was assessed by Cohen’s Kappa coefficient (K). Wilcoxon signed-rank test (nonparametric median test) was used to compare pre-procedure and post-procedure VAS & MODS. A P-value≤ .05 was considered statistically significant. Results: The study population included 152patients (218 vertebrae). Mean age was 66.63 years with 92 females and 60 males. Maximum number of VCF was found in thoracolumbar junction. Both MRI and Biopsy-reports showed 118osteoporotic VCFs and 34malignant VCFs. But there were 4unsuspected malignancy in MRI and 4benign VCFs were wrongly suspected as malignant in these. This resulted in a sensitivity, specificity and accuracy of 96.61%, 88.24%, and 94.74% respectively. The agreement between MRI and biopsy, intra-observer agreement and the inter-observer agreement were found to be statistically significant. Mean VAS and MODS reduced from pre-operative scores of 7.86 ± .78 and 31.06 ± 4.33 to 1.74 ± 0.69 and 8.96 ± 8.00 respectively. Conclusion: Diagnosing VCFs is not a major hurdle, but to differentiate benign (osteoporotic) from malignant VCF is a diagnostic challenge as both presents in the same age group of the population and have almost similar clinical characteristics. MRI can safely be used for the diagnosis of VCF and to differentiate the underlying pathology of VCF, with the advantage of being a non-invasive technique compared to biopsy. Evaluating MRI based on the combination of features is the key to increasing diagnostic accuracy. Vertebroplasty/Kyphoplasty significantly improves the pain and functional disabilities associated with the fracture and enable the patients to regain early pain-free mobility. Procuring biopsy concomitantly is easy, accessible, with no increase in morbidity, identifies the unsuspected malignancy and aids in the appropriate staging, planning, and prognostication of the patient. Besides, treatment of a patient depends highly on MRI in whom biopsy report came as inconclusive or insufficient sample was procured.
1868
A120: In Vivo Response to Corrective Spinal Fusion Surgery of Disc Morphology in Adolescent Idiopathic Scoliosis: Initial Response & 1 year Follow-Up
Mary Foltz 1 , Greta Long 2 , Casey Johnson 3 , Tenner Guillaume 4 , Walter Truong 4 5 , David Polly 5 , and Arin Ellingson 1
1 University of Minnesota, Rehabilitation Medicine, Minneapolis, USA
2 University of Minnesota, Computer Science and Engineering, Minneapolis, USA
3 University of Minnesota, Veterinary Clinical Sciences, St Paul, USA
4 Gillette Children's Specialty Healthcare, St Paul, USA
5 University of Minnesota, Orthopaedic Surgery, Minneapolis, USA
Introduction: Adolescent idiopathic scoliosis (AIS) is a 3D deformity of the spine and trunk, primarily identified in coronal radiographs; initially observed as disc wedging and accompanied by nucleus pulposus (NP) migration towards the convexity. Corrective fusion surgery is required to rectify severe scoliosis. Disc degeneration is known to occur at discs adjacent to fusion due to increased mechanical demand; the more levels fused, the higher mechanical demand on the caudal unfused levels. However, the time course of this degeneration is unknown, and understanding the unfused disc’s response to surgery may help to better inform clinical decisions. Aims were to assess discs caudal to lowest instrumented vertebra (LIV), immediately and one-year following surgery. Our hypotheses are: (1) NP will migrate towards disc center in response to surgery and (2) 1 year following surgery there will be a decrease in disc health. Material and Methods: AIS patients indicated for corrective fusion surgery (n = 9F; 14.4 ± 1.13 years; 12-16 years) were enrolled. 3T MRI (T2-weighted images) was used to image caudal adjacent (immediately caudal to LIV) and sub-adjacent (two levels caudal to LIV) discs at 3 time-points: (1) pre-operatively, (2) 3 months and (3) 1 year post-operatively. Axial slices were reconstructed, and scripts were developed to segment disc and NP regions of interest. From segmented regions we evaluated and normalized the (1) NP geometric and weighted (based on signal intensity) centers, (2) NP area, and (3) average NP signal intensity. NP centers inform on NP migration; NP area and signal intensity inform on disc health. Disc angles were manually measured in the coronal plane. Paired t-test were used to compare between time-points (pre-operatively and 3 months post-operative; 3 months and 1 year post-operatively) for each metric. Alpha = .05. Results: Following surgery, at the adjacent disc there was a significant migration of the NP weighted center towards the disc’s center (P = .03); no other significant differences were observed. 1 year post-surgery, a trend was observed, where the adjacent disc’s angle decreased (P = .06); no other significant differences were observed. At the sub-adjacent disc there were no significant differences between the time-points. Conclusion: Our results indicate that in AIS patients the adjacent NP migrates towards mid-line following surgery; however, the disc angle did not change, but one-year post-operation there was a slight decrease in disc angle without a corresponding NP migration. Therefore, NP migration towards mid-line may re-distribute loads more uniformly throughout the disc, followed by a decrease in disc angle. Analysis of the disc health metrics found no significant changes between three-months and one-year following surgery, indicating that the T2-weighted images were unable to detect early signs of degeneration. Limitations include small sample size and one-year follow-up evaluation. Corrective surgery may guide more uniform load transfer through the disc adjacent to LIV. Furthermore, NP migration may be an initial indicator of correction at discs caudal to LIV, since NP migration towards mid-line was detected prior to change in disc angle. Although early signs of degeneration were not observed at 1 year post-surgery, further imaging at two and 5 years time points is planned to track signs of degeneration.
1781
A121: Ossification of Posterior Longitudinal Ligament in Cervical Spine and its Association with Ossified Lesions in the Whole Spine: A Cross-Sectional Study of 2500 CT Scans
Ajoy P Shetty 1 , Neerav Anand Singh 2 , Vibhu Krishnan Viswanathan 2 , and Shanmuganathan Rajasekaran 1
1 Ganga Medical Center and Hospitals, Coimbatore, India
2 Ganga Medical Center and Hospitals, Spine Surgery, Coimbatore, India
Introduction: Cervical ossified posterior longitudinal ligament (c-OPLL) is a rare entity. The current literature evidence regarding the epidemiological data on c-OPLL is scarce. The present study was thus planned to identify the prevalence and characteristics of c-OPLL lesions; and their association with other spinal ligament ossifications. Methods: We performed a retrospective review of whole spine computed tomography (CT) scans of polytrauma patients from 2009 to 2018 using the PACS Database. CT scans were screened for c-OPLL, thoraco-lumbar OPLL, thoracic ossified ligamentum flavum (OLF), cervical and thoracolumbar ossified anterior longitudinal ligament (C-OALL AND T-L OALL), ossified nuchal ligament (ONL) and, diffuse idiopathic skeletal hyperostosis (DISH) and their prevalence and distribution were calculated. Chi square test was used to find out the significance of study parameters on a categorical scale between two groups. Results: Out of 2500 patients, 128 had cervical OPLL with a prevalence rate of 5.12% with mean age of 55.89 years. The most common affected level was C5 followed by C6, and C4. Segmental OPLL was the highest in number 77.7% followed by localized type 14.8%. Thoracic OPLL had prevalence rate of .56% and for OLF 9.90%. The co-existing ossifications with cervical OPLL were thoracic OPLL 7.81%, thoracic OLF 36.71%, cervical OALL 29.68%, thoracolumbar OALL 37.5%, DISH 27.34% and, ONL 7.03%. Conclusion: Our study showed a prevalence of 5.12 % for cervical OPLL, with more than 36% of these patients having co-existing thoracic OLF. We recommend screening MRI analysis of the whole spine for patients with radiographic evidence of OPLL in the cervical spine for the early detection of additional sites of ossification.
709
A122: Prenatal Counselling for Spine Anomalies - Algorithm of Management - From the Genesis to Treatment
Hriday Acharya 1 , Foram Acharya 2 , Rini Sutaria 2 , Prashant Acharya 2 , and Abhay Nene 1
1 Lilavati Hospital and Research Center, Mumbai, India
2 Paras Advanced center for fetal medicine, Ahmedabad, India
Introduction: A lot of spinal anomalies like scoliosis, kyphosis, Hemivertebra, tethered cord anomalies, spina bifida and many more can be diagnosed even before birth. In this era of early diagnosis and prevention, this could be a boon to spine surgeons to educate and counsel the parents minimise the physical deformity before correction and prevent the child’s problem by proper management. Not only that, since we could now followup the child since the very day he/she is born, it gives us a lead time in early management of any disorders or complications, which would develop in the life to come. It can provide the child with a better future. Here, we propose an algorithm in management of these spine anomalies from their diagnosis intrauterine till management after birth. Material and Methods: We studied over 10,000 fetal scans and the most commonly diagnosed spine anomalies were isolated. The management of each of those anomalies ranging from their intrauterine management, postnatal management, treatment in early childhood and adulthood were reviewed. An algorithm was formulated by a team of spine surgeon, fetal medicine specialist and an obstretician which took into consideration the time of diagnosis by a fetal medicine specialist, the follow up till the birth of the fetus by the obstretician and management of those anomalies from an spine surgeons point of view. Results: The algorithm comprised of a team of spine surgeon, fetal medicine specialist and an obstretician each of whom have a defined role to play. Early diagnosis of spine anomalies like hemiverterbra and other segmentation defects along with spina bifida could be easily diagnosed at 12 weeks. Most other anomalies like tethered cord syndrome, kyphosis, scoliosis and any other sydromic association or CNS anomalies can be identified by 20 weeks. After a primary diagnosis of the fetal spine,by pre-set protocols, by the fetal medicine expert the parents are couselled by a team of spine surgeon and an obstretician.The spine surgeon would manage anomalies by either intra uterine surgery (for spina bifida) or post natal management as early as possible, in coordination with the obstretician, to prevent any sequela of the condition. Conclusion:This algorithm gives us a lead time in diagnosing and management of spinal anomalies. This would help in providing the correct treatment to the child in a structured fashion avoiding the delay in diagnosis due to late presentation of symptoms and thereby preventing related complications. It would also,most importantly, help in making the parents prepared for their child’s problems and providing them with an effective plan to managed them.
1042
A123: The Utility of Surgeon-Directed DICOM Manipulation Software as a Preoperative Surgical Planning Tool in Pediatric Craniovertebral Anomalies
Kshitij Chaudhary 1 , Arjun Dhawale 1 2 , Avi Shah 2 , and Abhay Nene 2
1 Sir HN Reliance Foundation Hospital, Mumbai, India, 2 Wadia Children's Hospital, Mumbai, India
Introduction: Rigid instrumentation for complex craniovertebral junction (CVJ) anomalies in children can be challenging. However, orthogonal CT images are inadequate for planning as they are not in the screw trajectory plane. Open source DICOM software, such as Horos, has allowed surgeons to perform multiplanar reconstructions in line with the screw trajectory. This study aims to present a step-by-step preoperative workflow that we have utilized to plan surgery in pediatric CVJ anomalies using Horos. We assessed each site’s suitability for screw anchors preoperatively and correlated the preoperative planning with intraoperative findings and our ability to execute a preoperative plan successfully. We have also evaluated whether this method of preoperative planning can provide additional anatomical information compared to conventional PACS. Methods: The study included 25 consecutive children, less than 12 years old, operated for atlantoaxial instability by two surgeons between 2014 and 2019. The preoperative demographics, presenting symptoms, and the diagnosis were recorded. The preoperative CT angiogram was available on hospital PACS (Picture archiving and communications system), and its findings were noted. The DICOM data was then transferred to the surgeon’s laptop and loaded in Horos. The surgeon manipulated the DICOM images to determine an idealized path of screws at each cervical site in four steps. 3D volume rendering of the pathoanatomy was generated, and anomalies were noted. The surgeon compared the anatomical data obtained using Horos with that from the PACS CT and graded it as; Grade A (substantial new information), Grade B (confirmatory with improved visualization and understanding), Grade C (no added information). Any deviations inconsistent with preoperative planning were recorded. Fusion was assessed on a CT scan. Results: All children presented with a neurological deficit at a mean age of 7.2 years (2-12 years). Etiology was congenital anomalies (n = 11), skeletal dysplasia (n = 7), isolated os odontoideum (n = 5), and Down syndrome (n = 2). Surgeries were occipitocervical fixation (n = 18, 72%), C1-C2 fusion (n = 9, 36%), transarticular screws (n = 5, 20%). The most common cervical anchors used were C2 laminar screw (C2LAM) (n = 20), C2 pedicle screw (n = 10), and transarticular screw (n = 10). In 18 (72%) patients, the surgeon noted substantial new information (Grade A) about CVJ anomalies on Horos compared to PACS CT. Concerning planning for fixation anchors, the surgeon graded the information obtained as Grade A in all patients (100%). In 7 patients with dysmorphic C2 lamina, we used a novel uncrossed trajectory with an ipsilateral entry point for the C2LAM. In 4 (16%) patients, the surgery could not be executed precisely as planned Horos and alternative anchors were used. The average follow up was 25 months. Neurology improved in all except one patient. There were four (16%) complications; VA injury (n = 1), neurological worsening (n = 1), and loss of fixation (n = 1), non-union (n = 1). Conclusion: Horos is a free-to-use, user-friendly DICOM software, which can be a significant value addition to the surgeon’s preoperative workflow in planning complex craniovertebral anomalies. In our experience, surgeon-directed DICOM manipulation gives more anatomical information compared to studying PACS images. We describe a novel alternative entry point and trajectory for C2 laminar screws.
688
A124: Spine Anomalies in Fetus: Diagnosis & Incidence - A Retrospective Study of 10,000 Cinsecutive Fetal Scans
Hriday Acharya 1 , Prashant Acharya 2 , and Abhay Nene 1
1 Lilavati Hospital and Research Center, Mumbai, India
2 Paras Advanced Center for Fetal Medicine, Ahmedabad, India
Introduction: Looking for spinal anomalies is now an integral part of most prenatal ultrasound evaluations worldwide. However, we have very few published figures relating to the incidence and types of spinal anomalies from a prenatal scan. Here we look into how big this spectrum of disease is in the context of India and which anomalies can commonly be identified and how often are they identified at a tertiary care center. The purpose of the study was to find the incidence of various spine anomalies in the fetus and to evaluate the scope of early diagnosis in the management of these anomalies. Material and Methods: We report the results of 10,000 consecutive prenatal ultrasound scans specifically with respect to the incidence and distribution of spinal anomaly. All consecutive scans were done at a tertiary center by a single Fetal Medicine expert, between 2011 and 2019, were studied. Of the data obtained, all patients having spinal bony and cord anomalies were included in the study. Results: Out of 10,000 patients studied,89 (.008%) were diagnosed with spine and Spinal cord anomalies. Of these 89 patients, 57 had spinal dysraphism.10 had one or more level of hemivertebra.9 patients presented with intra-uterine scoliosis and 22 with kyphosis. Sacral agenesis was present in 7 of these patients. Conclusion: This is the first study to evaluate the incidence of prenatal diagnosis of spinal anomaly. Prenatal information will be of great value to spine surgeons as well as parents for counseling and planning treatment. A team approach comprising of a Spine surgeon, a fetal medicine expert and an obstetrician, in all cases should be the order of the day.
1034
A125: High-Resolution Computed Tomography Angiography (CTA) for Diagnosing Blunt Cerebrovascular Injury: Does it Cut the Mustard? A Systematic Review and Meta-Analysis
Charlotte Kik 1 , Willem Bart Slooff 1 , Nizar Moayeri 2 , and Sander Muijs 3
1 University Medical Center Utrecht, Neurosurgery, Utrecht, The Netherlands
2 University Medical Center Utrecht, Utrecht, The Netherlands
3 University Medical Center Utrecht, Orthopaedic surgery, Utrecht, The Netherlands
Introduction: Blunt cerebrovascular injuries (BCVI) collectively describe all non-penetrating traumatic injuries to the extra- or intracranial carotid and vertebral arteries. Screening of patients with BCVI is pivotal as up to 80% of these patients do not display neurological symptoms at presentation. Non-invasive and fast screening modalities, such as computed tomography angiography (CTA), are increasingly being utilized in the acute phase. Previous literature showed that the diagnostic accuracy of CTA is not yet equal to that of the rarely used golden standard of digital subtraction angiography (DSA) in detecting BCVI in trauma patients. However, the recent implementation of higher channel CTA (≥64 channels) may prove more sensitive. This article aims to determine whether high channel (≥64) multidetector CTA is equally or more accurate in diagnosing BCVI than DSA in trauma patients. Methods: An electronic database search was performed in PubMed, EMBASE, and Cochrane Library. Summary estimates of sensitivity, specificity, positive and negative likelihood, diagnostic odds ratio, and their 95% confidence intervals were determined using a bivariate random-effects model. Results: Of the 3293 studies identified, 9 met the inclusion criteria. Pooled sensitivity was 64% (95% CI, 53%-74%) and specificity 95% (95% CI, 87%-99%) The estimated positive likelihood ratio was 11.8 (95%, 5.6-24.9), with a negative likelihood ratio of 0.38 (95%, .30-.49) and a diagnostic odds ratio of 31 (95%, 17-56). Conclusion: CTA has good specificity but poor sensitivity when compared to DSA in diagnosing any type of BCVI. CTA with higher channels (≥16) did not have higher diagnostic accuracy as compared to CTA with lower channels (<16). These results show that the common clinical practice of using DSA only to confirm BCVI for CTA positive cases may pose the risk of underdetection and, consequentially, of undertreatment. However, most of the studies included in this analysis only reported on CTA with channels equal to or lower than 16, while contemporary trauma centers utilize CTA with up to 128 channels. Considering the invasiveness of DSA and common use of high channel CTA as the primary screening modality for BCVI, it begs the question of whether there will ever be enough evidence to replace DSA as the golden standard. Therefore, instead of aiming to replace DSA, we recommend that future research should focus on the harmfulness of undertreatment in BCVI patients, especially with regards to low-grade dissections.
1928
A126: Diagnostic and Treatment Criteria of Craniocervical Instability in Ehlers Danlos Syndrome - A Systematic Review
Laura-Nanna Lohkamp 1 , Nandan Marathe 1 , and Michael Fehlings 1
1 Division of Neurosurgery, Department of Surgery, Toronto, Canada
Introduction: Treatment indications for craniocervical instability (CCI) in patients with Ehlers Danlos syndrome (EDS) remain a matter of debate resulting in inconsistent surgical care availability among various countries. The aim of this systematic review is to summarize the diagnostic and therapeutic criteria currently applied in EDS and to identify consecutive knowledge gaps. Material and Methods: A systematic literature review was performed using the databases Ovid Medline, EMbase, Cochrane Library and PubMed based on the PRISMA guidelines. Search terms were Ehlers Danlos and spine, cervical spine, craniocervical instability or craniocervical junction, respectively. Articles were included if they described the application of diagnostic and/or treatment criteria for CCI in the context of EDS. Reported parameters pertaining to CCI and treatment indication in EDS patients are summarized. Results: Out of 113 articles, 7 met the inclusion criteria, including one case report, research article and editorial each as well as 4 original articles. All of them reported radiographical criteria for diagnosis of CCI, mainly established in lateral flexion and extension x-rays of the cervical spine, followed by dynamic CT imaging. Overall 13 distinct linear and angular morphometric parameters of CCI were recorded and applied according to the type of instability. The most common parameters to define CCI were the atlantodental interval (ADI), the basion-axis interval (BAI), the clivo-axial angle (CXA) and angular displacement of C1 to C2. The choice of diagnostic parameters was inconsistent among the majority of articles. Consistent treatment criteria were proposed in two of the studies, including a total of 42 EDS patients, who underwent cervical instrumentation for CCI. Reported symptoms representing treatment indications were neurological deficits, headache and neck pain or symptoms of cervicomedullary syndrome combined with radiographic signs of instability. In 22 patients the outcome was assessed radiographically, neurologically and via Karnofsky Performance Score (KPS) at 2 and 5 years follow up. The second study additionally used the Short Form Health Survey (SF-36) and patient-reported frequency of symptoms at 12 and 24 months in another set of 20 EDS patients. Postoperative improvement of neurological deficits was observed in all patients. Statistically significant improvement of headache or neck pain as well as of symptoms related to cervicomedullary syndrome were documented in most of the patients in both studies. Conclusions: Based on the current literature there is a significant lack of evidence for the choice and correct application of CCI criteria in EDS patients. The parameters mainly used are the ADI, BAI, CXA and angular displacement between C1 and C2, but warrant further assessment in bigger cohorts. Published outcome data after craniocervical instrumentation in these patients is scarce and univocal, although positive, not yet able to guide us in surgical decision-making. Further studies are required to evaluate a set of dedicated diagnostic criteria and to establish clinical guidelines for craniocervical instrumentation.
OP15: Cervical Surgery
326
A127: Fusion Rate for Combined Antero-Posterior vs Anterior Fixation with Allograft for 3 and 4 level Cervical Spine Pathology
Ekamjeet Dhillon 1 , Celeste Tavolaro 1 , Carlo Bellabarba 1 , and Richard Bransford 1
1 Harborview Medical Center, Orthopaedics and Sport Medicine, Seattle, USA
Introduction: Multilevel cervical spine decompression and fusion is the treatment of choice for patients with advanced degenerative cervical spine pathologies. Two common techniques include an anterior cervical discectomy and fusion (ACDF) or combining the ACDF with posterior spine instrumented fusion (PSIF). The anterior approach is often preferred, however, the rates of pseudoarthrosis is high using an anterior-only approach to 3 or more levels of interbody fusion. This study examines the radiological rates of fusion in patients undergoing an anterior-only vs combined anterior-posterior approach for 3 or more levels of interbody fusion. Material and Methods: We conducted a retrospective study of all patients undergoing three or more levels of interbody fusion between 2006 and 2016. Inclusion criteria included at least one year of radiographic follow-up with either flexion-extension plain radiographs or computed tomography (CT). Demographical, preoperative, and postoperative variables were documented, including BMI, indication for surgery, and rates of revision surgery secondary to pseudoarthrosis. Two orthopaedic surgeons independently reviewed the imaging to determine the levels of interbody fusion or nonunion for each patient. Results: 62 patients were included in our study, with 24 undergoing anterior-only approach with a total 74 interbody levels and 38 undergoing an anterior-posterior approach with a total of 119 interbody levels. The rate of radiographic interbody fusion of all levels was 79.73% (n = 59/74) in the anterior-only approach with 46% (n = 11) having at least one level of interbody nonunion and 17% (n = 4) requiring reoperations to address pseudoarthrosis. The rate of radiographic interbody fusion was 98.32% (n = 117/119) in the anterior-posterior approach with 5% (n = 2) having at least one level of interbody nonunion and 3% (n = 1) requiring reoperation to address pseudoarthrosis. In addition, 11% (n = 4) in the anterior-posterior group underwent reoperation for posterior wound dehiscence, which was not seen in the anterior-only approach. Conclusion: Almost half (46%) of the patients undergoing an anterior-only approach to interbody fusion of 3 or more levels developed a pseudoarthrosis, with one-sixth requiring revision surgery. Alternatively, combined anterior and posterior fixation resulted in a much higher radiographic fusion rate of 98.32%, compared to 79.73% in the anterior-only approach, with only 1 patient requiring a revision. However, this improvement in interbody fusion rate must be weight against the higher rates of wound dehiscence requiring reoperation.
1549
A128: ACDF with Ultra-Low Dose BMP-2 Versus the Posterior Approach in Multilevel Fusions to the Cervico-Thoracic Junction
Daniel Coban 1 , Michael Faloon 1 , Stuart Changoor 1 , Conor Dunn 1 , Michael Pompliano 1 , Ki Hwang 1 , Kumar Sinha 1 , and Arash Emami 1
1 St. Joseph's University Medical Center, Paterson, NJ, USA
Introduction: The cervicothoracic junction (CTJ) is a critical surgical landmark, acting as a mechanical transition point between the cervical and thoracic spine. Multilevel surgery in this region is subject to a number of potential sequelae, including adjacent segment disease (ASD), pseudoarthrosis, and sagittal malalignment. Surgical approach and length of construct can impact the rate of complications, revisions and clinical outcomes; however, there is a paucity of reports comparing the anterior approach with posterior cervical fusion (PCF) and inclusion of the CTJ. Therefore, the purpose of this study was to compare the clinical and radiographic outcomes in multilevel cervical fusion with respect to the approach and inclusion of the CTJ. Material and Methods: Between 2005 and 2013, 155 patients with at least 5 years of follow-up underwent multilevel fusion to the CTJ. Patients were divided into three groups: 1) ACDF to C7, 2) PCF to C7, and 3) PCF to T1/T2. Patients with complete records were included in outcome analysis, and patients with complete preoperative, early (<1 mo postop), and late (>2 years) films were included in radiographic analysis. Standard binomial and categorical comparative analysis were performed. Results: 155 patients were included in the final outcome analysis. Overall re-operation rates were 1) 14.5%, 2) 8.3%, 3) 10.0% (P = .588), respectively. The rate of pseudoarthrosis was 7.2% in Group 1, 2.8% in Group 2 and 6% in Group 3 (P = .869). ASD was seen in 2.9% of patients in Group 1, 2.8% of patients in Group 2 and 2% of patients in Group 3 (P = .951). Group 1 had 4 revisions due to neuroforaminal stenosis, 2 revisions due to persistent radicular pain, 2 hardware removal operations due to dysphagia, 1 revision due to pseudoarthrosis and 1 revision due to ASD. Group 2 had 3 revisions total, one due to ASD, another due to pseudoarthrosis and one due to hardware failure. Group 3 had 4 total revisions. Three due to pseudoarthrosis, 1 due to ASD and one due to persistent pain. Radiographic analysis showed a statistically significant difference (P = <.001) in both mean early and late restoration of lordosis between the ACDF group (-7.0° and -8.0°) and the PCF groups (C7: +8.3° and +6.6°; T1/T2: + 6.6° and + 5.5°). Conclusion: Clinically relevant complication rates leading to reoperation for long cervical fusions were less than anticipated in all groups. Anterior procedures underwent a higher rate of revisions but had better restoration of lordosis and pain scores at 5 years. Stopping at or crossing the CTJ did not result in better overall clinical outcomes.
638
A129: Preoperative and Postoperative Sagittal Cervical Alignment is Predictive of PROMIS Patient Reported Outcomes and Nurick Scores
Sarthak Mohanty 1 , and Comron Saifi 1
1 University of Pennsylvania Health System, Orthopaedic Surgery at the Hospital of the University of Pennsylvania. The Spine Center at Pennsylvania Hospital, Philadelphia, USA
Introduction: Normal lordotic curvature enables fluid motion and functionality for the cervical spine. Cervical spinal deformity causes increased muscular energy expenditure that may contribute to pain. This study explores the impact of cervical sagittal alignment on patient reported outcomes and neurologic function following cervical spine fusion surgery. Methods: A single center, retrospective analysis of 54 cervical spine fusion patients undergoing posterior cervical fusion (PCF) between 2017 and 2018 who had (1) 12 months (12M) of follow-up office visits, and (2) pre- and 12M post-operative cervical X-rays in the lateral view and (3) Patient reported outcomes along a 12 M period. The following parameters were measured: (1) C2-C7 Slope (CL), the C2-C7 Cobb angles which are obtained by drawing a line parallel to the inferior end plate of C2 and another line parallel to the inferior end plate of C7. Perpendicular lines are drawn from each of these lines, and the angle subtended by their intersection is measured; (2) T1 sagittal slope (T1S), the angle between the superior endplate of T1 and the horizontal plane; (3) cSVA, the distance between the C2 and C7 plumb lines. Patient-Reported Outcomes Measurement Information System (PROMIS) physical pain and mental stress scores were assessed at pre- op and 12M post-op. The effect of radiographic and clinical parameters on these scores was analyzed by multiple linear regression modeling. Nurick Grades, for myelopathic disability, were estimated from office visits pre- and post-op and analyzed by multivariable binary logistic regression, with Nurick scores >1 coded as "1" and Nurick scores of 0 or 1 coded as "0". Odds ratios are reported as (OR [95% CI]). Results: The multiple linear regression analysis built significant models for physical pain and mental stress PROMIS scores at 12M post-op (Physical: F (7, 47) = 7.631, P < .0001; Mental: F (7, 47) = 6.6292, P < .0001). Values are reported as (Increase in PROMIS score per unit change in sagittal, cervical parameter, p value). Significant predictors for a higher physical PROMIS score at 12M were pre- operative CL (.4711, P = .0010), cSVA (.3080, P= .0129) and post-op CL (0.3592, P= .0299). Significant predictors for a higher mental PROMIS score were pre-operative CL (.5268, P = .0033), and cSVA (.3444, P= .0299). Higher physical PROMIS scores (OR:1.797, [1.115- 5.840]) and higher post-op cSVA (OR:1.607 [1.054-4.500]) as well as lower pre-op T1S (OR:.4544 [.09399-.9195]) were associated with increased odds of having a Nurick score of >1 at 12M post-op (Table 3). Pre-operative C2-C7 lordosis, pre-op cSVA, and post-op C2-C7 lordosis strongly predicted increase in physical pain and mental stress patient reported, PROMIS scores. Conclusions: We provide meaningful data on the correlation between patient reported pain and cervical alignment parameters. Notably, increased physical pain PROMIS score, lower pre-op T1 slope, lower post-op T1 slope, and higher post-op cSVA were associated with increased odds of developing a Nurick score of >1 at 12M follow up. Pre-operative C2-C7 lordosis, pre-op cSVA, and post-op C2-C7 lordosis may serve as useful measures for surgeons to consider in counseling and caring for patients undergoing PCF.
1724
A130: The effect of the positioning of the screws and plate in anterior cervical fusion
Sara Diniz 1 2 , Ana Ribau 1 2 , Arnaldo Sousa 1 2 , João Esteves 1 2 , and Ricardo Rodrigues-Pinto 1 2
1 Centro Hospitalar Universitário do Porto. Portugal, Spinal Unit, Department of Orthopaedics, Porto, Portugal
2 Instituto de Ciências Biomedicas Abel Salazar, Porto, Portugal
Introduction: Anterior cervical fusion is a standard technique for the treatment of both degenerative and traumatic pathology of the spine. The purpose of this study is to retrospectively evaluate the cases of anterior cervical fusion with plate augmentation and try to relate the positioning of the plate and screws with the development of adjacent disc ossification (ADO). Material and Methods: Were reviewed all patients who underwent single-level anterior cervical fusion with autologous iliac crest graft and plating, between January 2009 and September 2016. Both trauma and degenerative cases were included. For the plate and screw positioning measurements was used the immediate postoperative cervical lateral radiograph. For all patients were measured the plate-to-endplate distance for both the superior and inferior border, the screw-plate angle and the distance from the tip of the screw to the endplate and ADO degree. Results: The disease developed or progressed in 40% (seventeen) of the superior adjacent discs and in 35% (fifteen) of the inferior adjacent discs. The mean superior plate-to-endplate distance was 3.74 +/- 2.60 mm and the inferior plate-to-endplate distance was 4.31 +/- 2.25 mm. The increase of the plate-to-endplate distance was related to the decrease of the ADO progression/development in the level above (P .022). The mean angle of the superior screws was 94.3 +/- 6.4 mm and the mean angle of the inferior screws was 92.4 +/- 5.8 mm. There was no significant relation between screw angle and disease progression for both levels. Conclusion: In this study the increase of the plate-to-endplate distance was related to the decrease of the ADO progression/development in the level above (P = .022). This is in accordance to many studies that defend the closer the plate is to the adjacent disk, the higher the risk of ADO development. This study goes in accordance to the idea that plates should be placed as far as possible from the endplates. However, this study raises the hypothesis that the distance from the screw to the endplate may also have an influence in the disease progression.
698
A131: Clinical Risk Factors Associated with the Development of Adjacent Segment Disease in Patients Undergoing Cervical Spine Procedure
Samuel Broida 1 , Kimihide Murakami 1 , Aidin Abedi 2 , Hans-Jörg Meisel 3 , Patrick Hsieh 4 , Jeffrey C. Wang 2 , Steven Presciutti 1 , Zorica Buser 2 , and Timothy S. Yoon 1
1 Emory Spine Center, Emory University, Atlanta, USA
2 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
3 Department of Neurosurgery, Bergmannstrost Hospital, Halle, Germany, Halle, Germany
4 Keck School of Medicine, University of Southern California, Department of Neurological Surgery, Los Angeles, USA
Introduction: Intervertebral disc disease (IDD) is characterized by progressive degeneration of intervertebral discs, resulting in local inflammation, loss of structural disc integrity, and chronic pain. In IDD of the cervical spine, surgery is often reserved for patients experiencing severe pain or compressive lesions causing myelopathy or radiculopathy. Cervical fusion for IDD carries a known risk of adjacent segment disease (ASD), a complication that often requires surgical intervention to relieve symptoms. Proposed risk factors for development of ASD include both clinical and radiographic patient characteristics, however assessment of the true impact of these risk factors has been limited by small sample sizes and loss to follow-up in individual studies. The aim of this study was therefore to synthesize and critically examine the clinical risk factors associated with development of adjacent segment disease in the cervical spine following fusion. Materials and Methods: We systematically reviewed the literature for cervical ASD according to the Preferred Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and protocol. A total of 6850 unique studies were obtained in the initial search. Of those, screening by title and abstract resulted in 19 articles for full text review. The methodological quality of included papers was evaluated by two reviewers according to the Methodological Index for Non-Randomized Studies (MINORS). A meta-analysis was performed to compute the odds ratio [OR] with corresponding 95% confidence interval [CI] for dichotomous outcome data, and mean difference [MD] with 95% CI for continuous variables. The data were pooled using both fixed and random effects models. Results: Eleven papers met the criteria for final analysis. Congenital /developmental stenosis (OR 1.94, 95% CI 1.06-3.56), age (MD 3.47, 95% CI 2.12-4.81), pre-operative VAS (neck) (MD .54 95% CI .09-.99), pre-operative VAS (arm) (MD .89 95% CI .43-1.34), pre-operative NDI (MD 4.18, 95% CI 2.11 to 6.26), and final post-operative JOA/ recovery rate (MD -.25, 95% CI -.48 to -.02) were found to be statistically significant clinical risk factors for development of ASD following cervical fusion. There were no significant differences in gender (OR .76, 95% CI .57-1.00), smoking (OR 1.03, 95% CI .73-1.44), alcohol (OR 1.07, 95% CI .70-1.64), diabetes (OR .85, 95% CI .56-1.31), number of segments (single vs multi- level) (OR .93, 95% CI .69-1.24), BMI (MD -.09, 95% CI -.46-1.00), and pre-operative JOA (MD -.34, 95% CI -.85-.17). Conclusion: This study provides a comprehensive review of risk factors for ASD development after fusion for cervical IDD. The overall quality of evidence is limited due to a considerable heterogeneity of the current literature as well as moderate to low methodological quality of the available studies.
789
A132: Clinical Outcomes of Patients with Degenerative Cervical Myelopathy Managed Nonoperatively: An Ambispective Longitudinal Cohort Study in 117 Patients
Allan Martin 1,2 , Sukhvinker Kalsi-Ryan 2 , Muhammad Akbar 2 , Anna Rienmueller 2 , Jetan Badhiwala 2 , Jefferson Wilson 2 , Lindsay Tetreault 2 , Aria Nouri 2 , Eric Massicotte 2 , and Michael Fehlings 2
1 University of California, Davis, Neurological Surgery, Sacramento, USA
2 University of Toronto, Toronto, Canada
Introduction: Degenerative cervical myelopathy (DCM) is among the most common pathologies affecting the spinal cord, but its natural history is poorly characterized. Mild DCM is often managed non-operatively, but surgery is recommended by clinical practice guidelines if neurological deterioration occurs. The purpose of this study is to investigate functional outcomes of patients with DCM managed nonoperatively, and study the utility of quantitative clinical measures and MRI to detect neurological deterioration. Material and Methods: Patients with DCM (newly diagnosed or recurrent myelopathic symptoms after previous surgery) who were initially managed nonoperatively were included. Retrospective chart reviews were performed to analyze clinical outcomes and anatomical MRI scans for worsening compression or increased signal change. Quantitative neurological assessments were collected prospectively, including mJOA, QuickDASH, GRASSP-myelopathy (motor, sensory, and dexterity), grip dynamometer, Berg Balance, gait stability ratio, and gait variability index; a deterioration of 10% on each measurement scale was considered positive for deterioration (e.g., 2-point decrease in mJOA). A composite score was considered positive if 3 or more measures worsened by 10%. Results: 117 patients were included (95 newly diagnosed, 22 recurrent myelopathy), including 74 mild, 28 moderate, and 15 severe cases. Over a mean follow-up of 2.5 years, 57% (95% CI = 46-67%) of newly diagnosed and 73% (95% CI = 50-88%) of recurrent DCM patients deteriorated neurologically. In newly diagnosed patients, deterioration occurred in 31/63 mild patients (49%; 95% CI = 37-62%), 15/21 moderate patients (71%; 95% CI = 48-88%), and 8/11 severe patients (73%; 95% CI = 39-93%). Deterioration was best detected with grip strength (60%), GRASSP dexterity (60%), and gait stability ratio (50%), whereas mJOA had low sensitivity (33%) in 50 patients. A composite score had sensitivity = 81% and specificity = 82%. Sensitivity of anatomical MRI was 28% (83 patients). Conclusion: DCM appears to have a poor natural history, even in patients with mild severity, with the majority deteriorating in short to mid-term follow-up. Prospective studies with robust neurological outcome measures are needed to validate these findings and fully characterize the natural history of DCM. Serial assessments to detect deterioration should include mJOA, grip strength, dexterity, balance, and gait analysis, and the use of composite scores shows promise to improve diagnostic accuracy. Lack of worsening on anatomical MRI or mJOA are not sufficient to determine clinical stability.
798
A133: Inter-Rater Reliability of the Modified Japanese Orthopaedic Association Score in Degenerative Cervical Myelopathy: A Prospective Study
Allan Martin 1,2 , Thorsten Jentzsch 2 , Jamie Wilson 2 , Ali Moghaddamjou 2 , Fan Jiang 2 , Anna Rienmueller 2 , Jetan Badhiwala 2 , Muhammad Akbar 2 , Anick Nater 2 , Colby Oitment 2 , Mario Ganau 2 , Eric Massicotte 2 , and Michael Fehlings 2
1 University of California, Davis, Sacramento, USA
2 University of Toronto, Toronto, Canada
Introduction: The modified Japanese Orthopedic Association (mJOA) score is widely accepted as the most important assessment in degenerative cervical myelopathy (DCM); this score has been utilized in clinical practice guidelines and directly influences treatment recommendations, but its reliability has not been established. This study aims to determine the inter-observer reliability of the mJOA in a large cohort of DCM patients. Material and Methods: This prospective cross-sectional study involved blinded administration of a refined version of mJOA to DCM patients by 2 or more experienced clinicians. Inter-rater reliability was measured using intra-class correlation (ICC), agreement, and mean difference for mJOA total score and subscores. Data were also analyzed with ANOVA for differences by mJOA severity (mild: 15-17, moderate: 12-14, severe: <12), assessor, assessment order, previous surgery, age, and sex. Results: 154 DCM patients underwent 322 mJOA assessments (183 paired assessments). ICC was .88 for total mJOA, .79 for upper extremity (UE) motor, .84 for lower extremity (LE) motor, .63 for UE sensation, and .78 for urinary function subscores. Paired assessments were identical across all 4 subscores in 25%. The mean difference in mJOA was 0.93 points between assessors, and this differed by severity (mild: .68, moderate: 1.24, severe: .87, P = .001). Differences of >= 2 points occurred in 19%. Disagreement between mild and moderate severity occurred in 12% of patients. Other variables did not demonstrate significant relationships with mJOA scores. Conclusion: The inter-rater reliability of the mJOA and its subscores is good, except for UE sensory function, which is moderate. However, the vast majority of assessments differed between observers, indicating that this measure should be interpreted carefully and used in conjunction with other neurological assessments for surgical decision-making, particularly when near the threshold between severity categories, or when a patient is reassessed for deterioration. Further efforts to educate clinicians on administration and refine UE sensory subscore may enhance the reliability of this tool.
529
A134: Stand Alone Cages Versus Cage and Plate Constructs for One- and Two-Level Anterior Cervical Discectomy and Fusion: A Prospective Randomized Controlled Trial
Athan Zavras 1 , Zakariah Siyaji 1 , Ali Piracha 1 , Talha Qadri 1 , Michael Nolte 1 , Arash Sayari 1 , Garrett Harada 1 , Bryce Basques 1 , Kern Singh 1 , and Matthew Colman 1
1 Rush University Medical Center, Orthopedic Surgery, Chicago, USA
Introduction:Although anterior cervical discectomy and fusion (ACDF) with interbody spacer and separate plate/screw construct (PLATE) construct is commonly performed, some have suggested this procedure may be associated with higher incidence of postoperative dysphagia, elevated operative time, malpositioned hardware, higher costs, and adjacent segment impingement. To address these concerns, others have opted to utilize an interbody cage with integrated screws and no plate (CAGE) with good results. This study’s purpose was to compare the perioperative and radiographic outcomes between stand-alone and anterior plated 1-2 level ACDF. Methods:This study was a prospective, randomized, controlled trial with minimum 6 months follow-up. Allprocedureswere performed between July of 2017 and February 2020. Patients with 1-2 level degenerative disease were randomized into one of two treatment arms consisting of either PLATE or stand-alone CAGE reconstruction. Measured pre- and postoperative patient-reported outcomes (PROs) included Swallowing Quality of Life (SWAL-QOL), Neck Disability Index (NDI), Visual Analog Scale (VAS) Arm, VAS Neck, Short Form 12-Item Health Survey (SF12), Veteran’s Rand 12-Item Health Survey (VR12). Primary endpoints assessed included clinical improvement, successful arthrodesis, and subsequent revision surgeries. Differences in populations were identified using T-test. Statistical significance was set toP< .05. Results:A total of 46 patients were randomized: 12 patients were treated with 1-level PLATE, 12 with 1-level CAGE, 12 with 2-level PLATE, and 10 with 2-level CAGE. For 1-level ACDF: There were no differences in clinical outcomes as assessed by PROs with the exception of worse swallow function reported on SWAL-QOL in the PLATE cohort at 6 weeks (PLATE: 71.3 ± 14.1, CAGE: 87.8 ± 11.1,P =.049) and 6 months (PLATE: 80.5 ± 9.23, CAGE: 92.0± 7.89,P =.042). Radiographic analysis noted no differences in the degree of changein cervical sagittal alignment, magnitude of disc height correction, arthrodesis, or cage subsidence. Pseudarthrosis requiring revision was observed in 1 PLATE patient. For 2-level ACDF: While there were no differences in baseline PROs, patients in the CAGE cohort reported worse outcomes immediately postoperatively via the VAS Neck PRO metric (PLATE: 1.49 ± 2.15, CAGE: 5.82 ± 2.86,P =.014), and significantly less symptomatic reduction at 1 year on SF12 (PLATE: 8.09 ± 5.98, CAGE -.55 ± 4.15,P =.024) and VAS ARM (PLATE-5.70±3.57, CAGE: .036 ± 3.84,P =.019) questionnaires. On the other hand, PLATE patients reported worse dysphagia on SWAL-QOL at 6 weeks postoperatively (PLATE: 76.5 ± 7.34, CAGE: 91.3 ± 8.22,P =.038). Radiographic cervical sagittal alignment showed significantly greater lordotic correction in the PLATE group at the cephalad index level for 6 months follow-up (PLATE: 2.92 ± 2.77, CAGE: -.56± 3.87,P =.048). No differences were observed in the magnitude of postoperative disc height correction, rate of arthrodesis, or implant subsidence. Conclusion:There was a significantly greater incidence of transient postoperative dysphagia in both the 1-level and 2-level PLATE cohorts. However, postoperative outcomes demonstrated worse results for 2-level CAGE in certain patient-reported metrics, while radiographic assessments of cervical sagittal alignment showed few differences. These findings indicate that although a greater degree of anterior instrumentation corresponds to increased dysphagia, the immediate stability conferred by anterior plating in PLATE may translate to improved symptomatic reduction than CAGE. Further longitudinal follow-up is necessary to fully elucidate these differences.
1926
A135: Predicting Severe Clinically Relevant Distal Junctional Kyphosis Development Following Adult Cervical Deformity Surgery with Further Distinction from Mild Asymptomatic Episodes
Peter Passias 1 , Sara Naessig 1 , Waleed Ahmad 1 , Katherine Pierce 1 , Lara Passfall 1 , Nicholas Kummer 1 , Oscar Krol 1 , Renaud Lafage 2 , Virginie Lafage 2 , Breton Line 3 , Bassel Diebo 4 , Themistocles Protopsaltis 1 , Han Jo Kim 2 , Robert Eastlack 5 , Alex Soroceanu 6 , Eric Klineberg 7 , Robert Hart 8 , Douglas Burton 9 , Shay Bess 10 , Frank Schwab 2 , Christopher Shaffrey 11 , Justin Smith 11 and , Christopher Ames 12
1 NYU Langone Orthopedic Hospital, Department of Orthopedics, New York, USA
2 Hospital for Special Surgery, Orthopaedics, New York, USA
3 Presbyterian St. Luke's/Rocky Mountain Hospital for Children, Spine Surgery, Denver, USA
4 SUNY Downstate Medical Center, Orthopaedics, Brooklyn, USA
5 Scripps Clinic, Orthopaedic Surgery, La Jolla, USA
6 University of Calgary, Orthopaedic Surgery, Calgary, Canada
7 University of California, Davis, Orthopaedic Surgery, Davis, USA
8 Swedish Neuroscience Institute, Seattle, USA
9 University of Kansas Medical Center, Orthopaedic Surgery, Kansas City, USA
10 Denver International Spine Clinic, Presbyterian St. Luke's/Rocky Mountain Hospital for Children, Denver, USA
11 University of Virginia Medical Center, Charlottesville, USA
12 University of California, San Francisco, San Francisco, USA
Background:While advances have been made in the surgical management of distal junctional kyphosis(DJK), complication rates remain high. Although individual factors related to its occurrence have been cited, many of these cases are mild and have no clinical relevance nor have these been combined into a formal predictive model, particularly for cases that are clinically impactful. the aim of this study was to develop a formal predictive model distinguishing between symptomatic and asymptomatic DJK. Methods: CD patients(pts) were stratified into Aysmptomatic (Asym) and Symptomatic (Sym) DJK. DJK angle(DJKA) was defined>10° change in kyphosis between LIV and LIV-2 and a>10° index angle. Asym: ΔDJK to be>10° in the absence neurologic sequelae. Sym: 1)DJKA>10° and either reop due to DJK or>1 new-onset neurological sequelae related to DJK or 2)pts who had either a DJKA>20° or ΔDJKA>20°. Stepwise logistic regressions were used to identify patient-specific, surgical, radiographic, and HRQL factors that were associated with these types of DJK. Decision tree analysis established cut-offs for the continuous variables. Results: 99 CD pts included (60 years, 26.5 kg/m2, 66.7%F). Surgical characteristics: 7.4 ± 4 levels fused, 47.5% posterior, 18.2% anterior, and 34.3% combined. Overall 32.2% developed DJK(34.3% Asym, 65.7% Sym). 37.5% of Asym pts received a reop versus 62.5% Sym pts. At BL, Asym pts had a greater BMI(28.5 vs 23 kg/m2) and NSR back pain(5.2 vs 4.6; all P < .05). Decision tree analysis identified osteoporosis, UIV level, and the apex of the region of the spine where the primary deformity is located to predict Sym pts. Top factors predicting Sym pts over Asym were BL EQ5D>0.65, UIV cephalad to C2, and C2-C7 apex caudal to C5. Multivariate analysis identified independent radiographic and surgical factors for developing Sym DJK: [Radiographic] BL PI(1.02[.9-1.07]), preop cervical flexibility(1.04[1.01-1.07]); [Surgical] combined approach (6.2[1.4-27]; all P < .05). Having abnormal hyper kyphosis in the thoracic spine, more so than abnormal cervical lordosis, was an independent factor for developing Sym when analyzed against Asym pts (1.2[0.01-115]). Predictive modeling identified factors that were predictive of Sym against no DJK pts such as having myelopathy (mJOA score:12-14), combined approach, UIV = C3 or C4, preoperative hypermobility, and >7 levels fused(AUC: .89). A predictive model for Sym versus Asym pts yielded an AUC of 85% and included being frail, having a TS-CL>20, and a PI>46.3. Controlling for BL deformity and disability, Sym pts had greater cSVA(4-8 cm: 47.6%vs 27%) and were more maligned according to their SRS-SVA (.1[.76-.02]) than non DJK pts at 1Y (all P < .05). Despite their symptomatology and higher re-operation rate, outcomes equilibrated in the Sym cohort at 1Y following revision. Conclusions: Overall 32.2% cervical deformed patients suffered from DJK most of which were clinically significant. Severe symptomatic DJK can be predicted with high reliability using combined determinants of baseline spinal cord dysfunction, mobility, frailty, and surgical factors including end levels, number of levels fused and use of a combined approach. It can be further distinguished from asymptomatic occurrences by taking into account pelvic incidence and baseline cervico thoracic deformity severity
OP16: Spinal Tumors
1232
A136: Incidence, Management, and Outcomes of Adult Spinal Chondrosarcoma Patients in the USA
Ravi Nunna 1 , Saavan Patel 2 , Shashank Patil 2 , Darius Ansari 2 , Taylor Burch 2 , Ankit Mehta 2 , Jens Chapman 1 , and Rod Oskouian 2
1 Swedish Medical Center, Seattle, USA
2 University of Illinois at Chicago, Chicago, USA
Objective: Spinal chondrosarcomas are rare primary malignant neoplasms composed of cartilage-producing cells. They are slow growing but locally aggressive lesions that have high rates of recurrence and progression after treatment. Gold standard treatment remains en-bloc surgical resection; however, complete excision is often difficult due to proximity to critical structures. Radiation and chemotherapy are historically ineffective. We have conducted a comprehensive analysis of demographics, treatment modalities, and survival outcomes in spinal chondrosarcoma patients using a large, prospectively-collected national database to investigate prognostic factors for enhanced clinical decision-making. Methods: Patients with diagnosis codes specific for chondrosarcoma of spine, sacrum, and coccyx were queried from the National Cancer Database (NCDB) during the years 2004-2016. Outcomes were investigated using Cox univariate and multivariate regression analyses, and survival curves were generated for comparative visualization. Results: 1843 individuals were identified with a diagnosis of chondrosarcoma, 82.1% of which were at the sacrum or coccyx and 17.9% at the spine. The mean overall survival of patients in our cohort was 7.91 years. Increased age, larger tumor size, dedifferentiated histology, and presence of metastases were associated with worsened overall survival. In regards to management, 77.7% of patients received surgical intervention and both partial and radical resection were associated with significantly improved overall survival (P < .001). Neither radiotherapy or chemotherapy administration improved overall survival; however, amongst patients who received radiation, those who received higher-dose radiation had significantly improved overall survival compared to lower-dose radiation. Conclusion: In the largest analysis to date, surgical resection was found to be significantly associated with improved overall survival in patients with spinal chondrosarcoma. In those patients receiving radiation, those who receive high doses have improved overall survival compared to those who receive lower doses. Further studies into optimal radiation modality and doses are required.

1824
A137: Correlation Between the Spinal Instability Neoplastic Score (SINS) and Patient Reported Outcomes
Anne Versteeg 1 , Arjun Sahgal 2 , Laurence Rhines 3 , Daniel Sciubba 4 , James Schuster 5 , Michael Weber 6 , Aron Lazary 7 , Stefano Boriani 8 , Chetan Bettegowda 4 , Michael Fehlings 9 , Michelle Clarke 10 , Paul Arnold 11 , Ziya Gokaslan 12 , and Charles Fisher 13
1 University of Toronto, Orthopaedics, Toronto, Canada
2 Sunnybrook Odette Cancer Centre, Toronto, Canada
3 MD Anderson Cancer Center, Houston, USA
4 Johns Hopkins University, Baltimore, USA
5 Hospital of the university of Pennsylvania, Philadelphia, USA
6 McGill University, Montreal, Canada
7 National Center for Spinal Disorders and Buda Health Center, Budapest, Hungary
8 IRCCS Istituto Ortopedico Galeazzi, Milan, Italy
9 University of Toronto and Toronto Western Hospital, Toronto, Canada, 10 Mayo clinic, Rochester, USA
11 The University of Kansas Hospital, Kansas, USA
12 The Warren Alpert Medical School of Brown University and Rhode Island Hospital and The Miriam Hospital, Providence, USA
13 University of British Columbia and Vancouver General Hospital, Vancouver, Canada
Introduction: The Spinal Instability Neoplastic Score (SINS) is used to define neoplastic-related spinal instability. Mechanical instability is one of the criteria for surgical intervention in patients with spinal metastases, however there is a paucity of data regarding the association between mechanical instability and patient reported outcomes (PROs). The aim of this study was to investigate the association between the total SINS score, individual SINS components and PROs. Methods: The AO Spine Knowledge Forum Tumor conducted a multicenter prospective observational study on patients undergoing radiation and/or surgical intervention for the treatment of symptomatic spinal metastases. Data regarding patient demographics, diagnostics, treatment, and PROs (SF-36, SOSGOQ) were collected at baseline, 6 weeks, and 12 weeks post-treatment. The SINS score was assessed using routine diagnostic imaging. The Spearman's rank correlation coefficient was used to assess the association between SINS, PRO at baseline and change in PROs. A multivariable analysis of covariance was performed to detect the important factors on SOSGOQ2.0 total score. Results: A total of 307 patients, including 174 patients who underwent surgery+/- radiotherapy and 133 patients who underwent radiotherapy were eligible for analyses. In the surgery+/- radiotherapy group, 18 patients were classified as having a stable lesion (SINS 0-6), 118 as potentially unstable (SINS 7-12), and 38 as unstable (SINS 13-18) as compared to 55 stable, 71 potentially unstable, and 7 unstable lesions in the radiotherapy alone group. At baseline, the total SINS score and the presence of mechanical pain was significantly associated with the SOSGOQ pain domain (r = -.519, P < .001) and the NRS pain score (r = .445, P < .001). The presence of mechanical pain demonstrated to be significantly associated with a positive change in PROs at 12 weeks post-treatment. In a multivariate model, SINS demonstrated to have the greatest impact (P < .001) on the SOSGOQv2.0 at baseline as compared to other variables including ECOG, CCI, gender, age, primary tumor type, duration of symptoms, MESCC, and ASIA AIS score. Conclusion: Spinal instability, as defined by the SINS score, demonstrated to be significantly correlated with PROs at baseline and change in PROs post-treatment. Mechanical pain, as a single SINS component, showed the highest correlations with PROs.
1186
A138: Outcomes of an Enhanced Recovery After Surgery (ERAS) Program for Patients with Metastatic Spine Tumors
Anubhav Amin 1 , Ori Barzilai 1 , Cindy Vuong 1 , Cynthia Correa 1 , Petal-Ann Persaud 1 , Solange Inglis 1 , Lisa Ruppert 1 , Vinay Puttanniah 1 , Anoushka Afonso 1 , Jess Brallier 1 , Brittany King 1 , Joanna Liu 1 , Wayne Quashie 1 , Vivek Malhotra 1 , Mark Bilsky 1 , and Ilya Laufer 1
1 Memorial Sloan Kettering Cancer, New York, USA
Introduction: Metastatic spine tumor surgery generally consists of palliative operations performed on frail patients with multiple medical comorbidities. Perioperative complications that may arise can mitigate any potential benefit in this vulnerable patient cohort. Enhanced recovery after surgery (ERAS) programs involve an evidence-based multidisciplinary approach to improve perioperative outcomes. While ERAS programs have been shown to be beneficial in other surgical fields, there is a paucity of literature evaluating the feasibility, implementation, and outcomes of an ERAS program dedicated to spinal oncology surgery. We present the Spine Tumor ERAS pathway and describe the clinical outcomes of the program. Materials and Methods: The spinal oncology surgery ERAS program went into effect in April 2019. This protocol focused on multimodality analgesia, including preoperative gabapentinoid, NSAID, and acetaminophen administration in combination with local field blocks with liposomal bupivacaine, to minimize opioid consumption; intraoperative goal-directed fluid management, early advancement of diet, and early ambulation with physical therapy. Two hundred and forty consecutive patients enrolled in the ERAS program were compared to 240 consecutive historical pre-ERAS patients. Outcomes measured included: length of hospitalization stay, time to ambulation, urinary catheter duration, time to regular diet, total intraoperative fluid intake, estimated blood loss, intraoperative opioid use, and cumulative postop day 0-5 opioid use. Results: While the case duration was similar in the ERAS vs. pre-ERAS cohort (276 minutes vs 266 minutes) with similar EBL (165.7 mL vs 199.4 mL), the ERAS cohort utilized less intraoperative opioids (34.7 MME vs 43.2 MME), less postop day 0-5 cumulative opioid use (155.0 MME vs 305.0 MME), ambulated earlier (32.7 hours vs 52.1 hours), discontinued urinary catheters earlier (33.1 hours vs 50.9 hours), advanced to a normal diet earlier (21.6 hours vs 28.1 hours), and had a shorter length of stay (6.6 days vs 8.4 days), in comparison to the pre-ERAS cohort. Conclusion: To date, this is the largest study focusing on outcomes of an ERAS program specifically for patients undergoing metastatic spine tumor surgery. The implementation of an evidence-based multidisciplinary ERAS program has led to a significant reduction in opioid consumption, earlier ambulation, improved clinical quality metrics, and shorter hospitalization.
1920
A139: Outcomes in surgically treated patients with symptomatic spinal metastases: results from "EPOSO", a prospective, multi-institutional and international study
Ori Barzilai 1 , Arjun Sahgal 2 , Laurence Rhines 3 , Daniel Sciubba 4 , Aron Lazary 5 , Michael Weber 6 , James Schuster 7 , Stefano Boriani 8 , Chetan Bettegowda 4 , Paul Arnold 9 , Michelle Clarke 10 , Michael Fehlings 11 , Ziya Gokaslan 12 , Ilya Laufer 1 , Charles Fisher 13 , and AO Knowledge Forum Tumor AOKFT 14
1 Memorial Sloan Kettering Cancer Center, Neurosurgery, New York, USA
2 Department of Radiation Oncology, Sunnybrook Odette Cancer Center and University of Toronto, Toronto, Ontario, Canada, Toronto, Canada
3 Division of Surgery, Department of Neurosurgery, The University of Texas MD Anderson Cancer Center, Houston, TX, Houston, USA
4 Department of Neurosurgery, Johns Hopkins University School of Medicine, Baltimore, MD, Baltimore, USA
5 National Center for Spinal Disorders and Buda Health Center, Budapest, Hungary, Budapest, Hungary
6 Division of Surgery, McGill University and Montreal General Hospital, Montreal, Quebec, Canada, Montreal, Canada
7 Department of Neurosurgery, Hospital of the University of Pennsylvania, Philadelphia, PA, Philadelphia, USA
8 Spine Surgery Division, IRCCS Galeazzi Orthopedic Institute, Milan, Italy, Milan, Italy
9 Department of Neurosurgery, The University of Kansas Hospital, Kansas City, KS, Kansas City, USA
10 Department of Neurosurgery, Mayo Clinic, Rochester, MN, Rochester, USA
11 Division of Orthopedic surgery, University of Toronto and Toronto Western Hospital, Toronto, Ontario, Canada, Toronto, Canada
12 Department of Neurosurgery, The Warren Alpert Medical School of Brown University and Rhode Island Hospital and The Miriam Hospital, Providence, RI, Providence, USA
13 Division of Spine, Department of Orthopaedics, University of British Columbia and Vancouver General Hospital, Vancouver, British Columbia, Canada, vancouver, Canada
14 Research Department, AO Spine International, Davos, Switzerland, davos, Swaziland
Introduction: Recent integration of targeted therapies has revolutionized cancer care. Treatment strategies for metastatic spine disease has been redefined with the integration of radiosurgery and minimally invasive surgical strategies. The impact of surgery in this rapidly evolving landscape is not well defined. The goal of this study was to prospectively evaluate clinical, neurological and HRQoL outcomes in patients with symptomatic spinal metastases who underwent surgical management. Methods: This is a prospective, international collaboration from 10 specialist centers as part of the AO Spine Knowledge Forum Tumor titled: 'The Epidemiology, Process and Outcomes of Spine Oncology' (EPOSO, ClinicalTrials.gov identifier: NCT01825161). Adult patients (aged 18 to 75), who underwent surgery for the treatment of spinal metastases with or without adjuvant radiotherapy were included. Clinical data including spine tumor specific, cancer validated, patient reported outcome tools were used and collected for a minimum of 2 years. Results: Two-hundred and eighty patients (51.8% females, mean age 58) were included in the final analysis. At presentation the mean Charleson comorbidity index was 6.0, mean time from diagnosis of primary tumor was 39.1 months, 35.7% had neurologic deficits as defined by ASIA scores, high grade compression (ESCC 2-3) was present in 47.8% and SINS scores of 7 or more (indicating frank or impending instability) were present in 89.6%. Most common primary tumor sites were; breast (20.3%), lung (18.8%), kidney (16.2%) and prostate (6.5%). Of patients who completed the 2 year follow up, median survival after surgery was 500 days, with 90% local control. Significant and durable improvement in HRQoL was seen at 6 weeks, 12 weeks, 26 weeks, 1 year and 2 years follow-up compared to baseline with various patient reported outcome questionnaires including the Spine Oncology Study Group Outcome Questionnaire 2.0 (SOSGOQ), SF-36 V2, EQ-5D and pain NRS. Conclusions: Surgery maintains a key role in the treatment of symptomatic spinal metastases. These broad, multicenter prospective data represent outcomes demonstrating that surgical decompression and/or stabilization provide oncologic benefit as well as rapid and durable improvement in quality of life for patients with metastatic spine disease.
960
A140: Comprehensive Surgical Treatment Strategy for Spinal Metastases: Results of a Single-Center Series
Arthur Wagner 1 , Elena Haag 1 , Ann Kathrin Joerger 1 , Philipp Jost 2 , Stephanie Combs 3 , Maria Wostrack 1 , Jens Gempt 1 , and Bernhard Meyer 1
1 Technical University Munich School of Medicine, Department of Neurosurgery, Munich, Germany
2 Technical University Munich School of Medicine, Department of Oncology, Munich, Germany
3 Technical University Munich School of Medicine, Department of Radio Oncology, Munich, Germany
Introduction: Based on a large consecutive single-center series of patients with spinal metastases (SM), we devised a comprehensive treatment algorithm for surgical strategies and adjunct therapies. Material and Methods: Between January 2007 and December 2018, patients with a SM were screened for study inclusion after an interdisciplinary neurooncological board meeting decided on the treatment plan. We report baseline characteristics, surgical procedures, complication rates, functional status and outcome of a consecutive cohort managed in accordance to a stratified treatment algorithm and adjunct therapy. Results: 667 consecutive patients underwent 989 operations for SMs at our institution. Mean age was 65 years (range 20-94), median preoperative KPS was 80. Most common primary entities were prostate (21.7%), breast (15.9%) and non-small cell lung cancer (10.0%). The thoracic spine was affected in 48.3% of cases, followed by the lumbar spine in 26.7%. We conducted posterior instrumentation with or without vertebral body replacement in a staged approach in 69.5%, sole decompression in 12.4% and vertebral body augmentation in 18.0% of cases. Follow up was available for 58.9% of patients. Median OS amounted to 18.4 months (95% CI 9.8-26.9), OS after 12 months was 56.0% and median KPS improved from 70 to 80 by discharge. Conclusion: Surgical management of SMs should generally represent the first step of a conclusive treatment algorithm. The need to preserve long-term symptom control and biomechanical stability stems from the growing life expectancy of patients with SMs, and requires a staged invasive surgical strategy currently not supported by level I evidence.
216
A141: Cortical Integrity, Lesion's Position and Size as Additional Parameters for the Characterisation of the Mechanical Weakness of Metastatic Vertebrae
Marco Palanca 1,2 , Luca Cristofolini 2 , Enrico Dall'Ara 1 , Daniele Marras 2 , Alessandro Gasbarrini 3 , and Giovanni Barbanti Bròdano 3
1 The University of Sheffield, Dept of Oncology and Metabolism, Sheffield, United Kingdom
2 Alma Mater Studiorum - Università di Bologna, Dept of Industrial Engineering, Bologna, Italy
3 Rizzoli Orthopaedic Institute, Dept of Oncological and Degenerative Spine Surgery, Bologna, Italy
Introduction: In the oncological field, the rational for mechanical stabilization of vertebrae affected by metastasis is still a challenge. The Spine Instability Neoplastic Score (SINS) is a useful scoring system that aims to help the clinicians deciding the best orthopedic solution[1]. It provides a characterization of the entire spine stability, but due to the large possible variations of the metastasis, frequently the biomechanical outcomes could be unexpected[2-4]. The aim of this work was to identify what geometrical parameters are useful for a mechanistic characterization of the metastatic vertebra weaknesses in addition to the clinical spine characterization provided by the SINS. Material and Methods: Twenty spines with metastases (blastic, lytic and mixed) originated by different primary tumors, were obtained through an ethically-approved donation program. Each spine was CT scanned as in the clinical routine (voxel size = 0.9 mm) and two expert surgeons of the Rizzoli Orthopaedic Institute evaluated the SINS and indicated which surgery they would perform. From the twenty spines, thirty-five segments, consisting of four vertebrae each were isolated. Each segment included a healthy and a metastatic vertebra in the middle and two additional cranial and caudal ones. The specimens were CT scanned again with a better resolution (voxel size = 0.2 mm) in order to accurately measure the size and position of the metastases. Each specimen was biomechanically tested in four different loading conditions: flexion, left lateral bending, right lateral bending, and pure compression. Each test was repeated three times, for ensuring the repeatability of the results. The full-field strain distributions were evaluated on the entire vertebral body surface, through a state-of-the-art 4-cameras Digital Image Correlation[5]. The “mechanical ratio” was computed for each loading scenario, as the ratio between the mean strain on the metastatic vertebra and the adjacent healthy vertebra. Results: A total of 372 tests were performed. The SINS of the 31 metastatic vertebrae was in the range 3-13. Poor agreement was found between the surgery suggestions of the clinicians and SINS, as well as between the evaluated mechanical ratio and the SINS. Larger mechanical ratios were observed in lytic metastasis: lesions on the cortical shell and large lesions close to the cortical shell were associated with higher mechanical ratio (lower vertebral strength) also in case of low SINS. In exceptional cases (4/35 specimens) with lesions on the cortical shell, the metastatic vertebra fractured under low loads. Conversely, vertebrae with only blastic lesions did not show any sign of weakness. Conclusion: The quantitative mechanical evidences confirmed what could be qualitatively expected. The extensive collection of quantitative data will be used in multiple regression analysis to build a phenomenological model. Indeed, the encouraging findings support the idea of improving the risk evaluation including mechanical characterization of the metastatic vertebra in combination with the SINS, and paves the way to retrospective and prospective clinical studies.
Acknowledgements
The study was funded by the AOSpine2019 Discovery and Innovation Award (SONS, AOSDIA2019_063) and the Marie Skłodowska-Curie Individual Fellowship (MetaSpine, MSCA-IF-EF-ST, 832430/2018).
References
1. Fisher, et al.Spine2010,35,E1221–E1229
2. Palanca,et al.Materials2020,13,3256
3. Costa,et al.JBMMB2019,98,268–290
4. Costa,et al.Bone Reports2020,12,100257
5. Palanca,et al.MEP2018,52,76–83
45
A142: An Externally Validated Machine Learning Algorithm for Prediction of Ninety-Day and 1 year Mortality After Surgery for Spinal Metastasis
Akash Shah 1 , Aditya Karhade 2 , Howard Park 1 , Arya Shamie 1 , Don Park 1 , Joseph Schwab 2 , and Francis Hornicek 1
1 UCLA Medical Center, Orthopaedic Surgery, Los Angeles, US
2 Massachusetts General Hospital, Orthopaedic Surgery, Boston, USA
Introduction: The spinal column is the most common site of bony metastasis, with up to 5-10% of patients with cancer developing metastatic epidural spinal cord compression. Surgical decompression and stabilization in the setting of spinal metastasis is performed in order to relieve pain, preserve functional status, and improve quality of life. These potential benefits must be weighed against the risks of perioperative morbidity and mortality. Accurate prediction of a patient’s post-operative survival is thus a crucial component of patient counseling. The Skeletal Oncology Research Group (SORG) previously developed machine learning (ML) algorithms to pre-operatively predict risk of ninety-day and one-year mortality in patients undergoing surgery for spinal metastasis. These algorithms are available in an open-access application. Using an independent geographically distinct patient population, we aim to externally validate these algorithms and assess their utility in providing mortality risk scores at key post-operative time points. Materials and Methods: Retrospective review was employed to identify patients 18 years or older at a tertiary care academic medical center who were treated with surgical intervention for spinal metastatic disease between 2004 and 2020. The primary outcomes were 90 days mortality and 1 year mortality from the date of index surgery. Baseline characteristics of the external validation cohort were compared to the derivation cohort for the SORG ML algorithms. The following metrics were used to assess the performance of the algorithms: discrimination, calibration, overall model performance, and decision curve analysis. Results: Overall, 298 patients underwent surgery for spinal metastatic disease. Sixty-one patients (21.9%) died within 90 days of surgery; 133 (52.6%) died within one year of surgery. The external validation cohort differed significantly from the derivation cohort on the following variables: primary tumor histology, performance status, body mass index, medical comorbidities, previous systemic therapy, and preoperative laboratory values (platelet count, platelet to lymphocyte ratio, creatinine). The SORG algorithms for ninety-day mortality and one-year mortality performed excellently with respect to discrimination with AUC 0.84 and .90, respectively. The algorithm for one-year mortality was well-calibrated with intercept = .04 and slope = 1.17. At both post-operative time points, the SORG algorithms showed greater net benefit than the default strategies of changing management for no patients or for all patients. Use of the algorithms thus results in a greater balance of true positives than false positives. Conclusion: With the increasing prevalence of malignancy in the aging population, the incidence of spinal metastasis is likely to increase. Using a contemporary, geographically distinct independent population, we report successful external validation of SORG algorithms for pre-operative risk prediction of ninety-day and one-year mortality after surgery for spinal metastasis. Often difficult to reliably obtain, patient survival is a critical prognostic consideration when weighing the risks and benefits of operative intervention. By providing accurate prediction of intermediate and long-term mortality risk, the externally validated SORG algorithms may inform shared decision-making with patients and families when determining operative versus non-operative management of spinal metastatic disease. To facilitate the use of these algorithms, the open-access SORG ML algorithms have been made available in a digital interface: https://sorg-apps.shinyapps.io/spinemetssurvival/.
1538
A143: High Predictive Value of Spinal Instability Score Following Radiosurgery for Spinal Metastases
Maximilian-Niklas Bonk 1 , and Ehab Shiban 1
1 University Hospital Augsburg, Department of Neurosurgery, Augsburg, Germany
Aim: The aim of this study was to determine the predictability of progression of a pathologic fracture due to spinal metastases applying the spinal instability neoplastic score (SINS) prior to delivery of radiotherapy for spinal metastases. Methods: A retrospective analysis of Patients with a pathologic fracture due to a spinal metastases between January 2018 and December 2018 was performed. We selected patients with a minimum follow up of 12 months and analysed them according to the SINS criteria. The primary endpoint was the progression of fracture following radiotherapy. Results: 117 Patients were identified. Median age was 70. 42% were Female. Median Follow up was 14 months (range 12-27). 6, 104 and 7 Patients presented with low (0-6), moderate (7-12) and high (13-18) SINS, respectively. 0%, 19% and 85% of Patients with low (0-6), moderate (7-12) and high (13-18) SINS developed a fracture progression after Radiosurgery. Of those eight had neurological deterioration. Conclusion: SINS is a very useful tool for predicting the progression of a pathologic fracture due to spinal metastases after radiotherapy for spinal metastases.
530
A144: Expectations of Treatment Outcomes in Patients with Spinal Metastases; What do We Tell Our Patients? A Qualitative Study
Anne Versteeg 1 , Roxanne Gal 1 , Raphaële Charest-Morin 2 , Jorrit-Jan Verlaan 1 , Hester Wessels 1 , Charles Fisher 2 , and Lenny Verkooijen 1
1 University Medical Center Utrecht, Utrecht, The Netherlands
2 University of British Columbia and Vancouver General Hospital, Vancouver, Canada
Introduction: Realistic pre-treatment expectations are important and have been associated with post-treatment health related quality of life (HRQOL). Patient expectations are greatly influenced by physicians, as they are the primary resource for information. This study aimed to explore the communication practices of physicians regarding treatment outcomes for patients with spinal metastases, and physician experiences with patient’s pre-treatment expectations. Material and Methods: An international qualitative study using semi-structured interviews with physicians routinely involved in treating metastatic spine disease (spine surgeons, radiation and medical oncologists, and rehabilitation specialists) was conducted. Physicians were interviewed about the content and extent of information they provide to these patients regarding treatment options, risks and treatment outcomes. Interviews were transcribed verbatim and analyzed using a thematic coding network. Results: After 22 interviews data saturation occurred. The majority of the physicians indicated that they currently do not validate patients pre-treatment expectations, despite acknowledging the importance of these expectations. Spine surgeons often believe that patient expectations are disproportionate. Physicians expressed they manage expectations by detailing the most common risks and providing a broad but nonspecific overview of treatment outcomes. While the palliative intent seems clear to the physicians, their perception is that the implications of a palliative treatment remains elusive to most patients. Conclusion: This study highlights the current gap in patient-physician communication regarding expectations of treatment outcomes of patients with spinal metastases. These results warrant further projects to improve communication practices and determine the effect of patient expectations on patient reported outcomes in this population.
OP17: Minimally Invasive and Novel Surgical Treatments
1706
A145: Preoperative MRI-Based Vertebral Bone Quality (VBQ) Score Assessment in Patients Undergoing Lumbar Spinal Fusion
Stephan Salzmann 1 , Ichiro Okano 1 , Conor Jones 1 , Jiaqi Zhu 1 , Shuting Lu 1 , Ikenna Onyekwere 1 , Venkatesh Balaji 1 , Marie-jacqueline Reisener 1 , Erika Chiapparelli 1 , Jennifer Shue 1 , John Carrino 1 , Federico Girardi 1 , Frank Cammisa 1 , Andrew Sama 1 , and Alexander Hughes 1
1 Hospital for Special Surgery, New York, USA
Introduction: The importance of bone quality assessment in spine surgery is well recognized. The current gold standard for assessing bone mineral density is dual-energy X-ray absorptiometry (DEXA), however the majority of patients undergoing spinal fusion do not have preoperatively available DEXA data. Furthermore, DEXA has been shown to overestimate BMD in patients with spinal degenerative disease and obesity. Consequently, alternative radiographic measurements using data routinely gathered during preoperative evaluation have been explored for the evaluation of bone quality and fracture risk. Opportunistic quantitative computed tomography (QCT) and more recently the MRI-based vertebral bone quality (VBQ) score both have been shown to correlate with DEXA T-scores and predict osteoporotic fractures. However, to date the correlation between those two modalities has not been studied. The objective of this study was to assess whether the VBQ score can predict the prevalence of QCT based osteopenia/osteoporosis and to evaluate the correlation between those two modalities. Material and Methods: Patients undergoing lumbar fusion from 2014 to 2019 at a single, academic institution with available preoperative lumbar CT and T1-weighted MRIs were included. Asynchronous QCT measurements were performed. The average L1-L2 BMD was calculated and patients were categorized as either normal BMD (>120 mg/cm3) or osteopenic/osteoporotic (≤120 mg/cm3). The VBQ score was calculated by dividing the median signal intensity of the L1-L4 vertebral bodies by the signal intensity of the cerebrospinal fluid on midsagittal T1-weighted MRI images. To assess inter-observer reliability of the VBQ measurements, a validation study was performed. Demographic data and the VBQ score were compared between the normal and osteopenic/osteoporotic group. To determine the area-under-curve (AUC) of the VBQ score as a predictor of osteopenia/osteoporosis receiver operating characteristic (ROC) analysis was performed. VBQ scores were compared with QCT BMD using Pearson’s correlation. Results: A total of 198 patients (53% female) were included. The mean age was 62 years and the mean BMI was 28.2 kg/m2. The inter-observer reliability of the VBQ measurements was excellent (ICC of .90). When comparing the patients with normal QCT BMD to those with osteopenia/osteoporosis, no significant differences existed in terms of sex, race, and BMI. However, the patients with osteopenia/osteoporosis were significantly older compared to the patients with normal BMD (64.9 vs 56.7 years, P < .0001). The osteopenic/osteoporotic group had significantly higher VBQ scores (2.6 vs 2.2, P < .0001). ROC analysis revealed that the VBQ score predicts the presence of osteopenia/osteoporosis based on QCT with an accuracy of 71% (P < .0001). The VBQ score showed a statistically significant moderate correlation with QCT BMD (correlation coefficient = -.358, P < .001). Conclusion: This is the first study to correlate MRI VBQ scores with QCT BMD. We found that the VBQ score significantly differentiates patients with normal BMD versus osteopenic/osteoporotic BMD based on QCT. However, the correlation between both modalities was only moderate suggesting that VBQ might not solely be a measurement of bone density, but rather bone quality. Since the two modalities seem to reflect different properties of bone, VBQ may be an interesting adjunct to clinically performed bone density measurements, rather than a substitution.
761
A146: Prospective Study Pf Intraoperative Motor Evoked Potential Monitoring to Identify Lumbosacral Nerve Root Motor Deficits
Kelley McGowan 1 , Hyunmi Choi 1 , Meghan Cerpa 1 , Earl Thuet 1 , Anil Mendiratta 1 , Ronald A. Lehman 1 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
Summary: In a prospective cohort study of 328 thoracolumbar spinal surgeries, EP (MEP+/-SEP) responses reached warning criteria indicative of nerve root dysfunction in 44 patients (13%). Postop exam within the first 24 hours demonstrated 25 patients (7.6%) had new onset of weakness attributable to nerve root dysfunction. Adjusted logistic regression analyses showed that EP status at closure was an independent predictor, with unimproved EP change significantly more likely to be associated with neurological deficit. Hypothesis: Intraoperative MEP changes can predict post-op deficits. Study Design: Prospective. Introduction: The reliability of nerve root monitoring has not been demonstrated. Methods: This was a prospective cohort study of 328 patients over a 12 months period. The primary outcome was a binary variable of new deficit detected post-op within the first 24 hours. 6 independent variables (Table 1) were considered as potential predictors of outcome. Bivariate logistic regression was used to estimate the unadjusted association between potential predictive factors and neurological outcome (Table 1). Stepwise multivariate logistic regression was then used to determine which factors were independent predictors for postop neuro deficit. Results: Of 328 patients, EP changes occurred in 44 patients (13%). 25 patients (7.6%) had new onset of weakness detected during the first 24 postop period. As seen in Table 1, notification of EP change, type of data change, and data at closure were associated with postop weakness. Of 44 patients with EP data change, 32 did not improve by closure with 23 developing new weakness. On the other hand, of 44 patients with EP data change, 12 improved by closure with 2 developing new weakness. Compared to those with EP improvement at closure, patients without improvement in EP were significantly more likely to have postop weakness (adjusted OR 12.8, 95% CI 2.22 - 70.12). Conclusion: During thoracolumbar spine surgeries, EP nerve root warnings occurred in 13% of patients. EP change that did not improve by closure was an independent predictor of postop neurological weakness. Take Home Message: In a prospective cohort study of thoracolumbar spine surgery, EP change that did not improve by closure of surgery was an independent predictor of lumbosacral nerve root motor deficits.
1696
A147: Thoracic Bone Mineral Density Measured by Quantitative Computed Tomography in Patients Undergoing Spine Surgery
Stephan Salzmann 1 , Ichiro Okano 1 , Conor Jones 1 , Eric Basile 1 , Anthony Iuso 1 , Jiaqi Zhu 1 , Marie-jacqueline Reisener 1 , Erika Chiapparelli 1 , Jennifer Shue 1 , John Carrino 1 , Federico Girardi 1 , Frank Cammisa 1 , Andrew Sama 1 , and Alexander Hughes 1
1 Hospital for Special Surgery, New York, USA
Introduction: The thoracic spine is a common location for vertebral fractures as well as instrumentation failure after long spinal fusion procedures. The association between those complications and bone mineral density (BMD) are well recognized. The current gold standard to measure spinal BMD is dual energy x-ray absorptiometry (DXA). However, due to the overlying sternum and ribs in the thoracic spine, DXA is limited to the lumbar spine. Quantitative computed tomography (QCT) circumvents several shortcomings of DXA and allows for level-specific BMD measurements. To the authors’ knowledge, no investigation has comprehensively quantified the BMD of the entire thoracic spine in patients undergoing spine surgery. The objective of this study was to: 1) assess the reliability of thoracic QCT measurements, 2) determine possible level-specific BMD variation and 3) assess the correlation between BMDs of the spinal levels T1-T12. Material and Methods: Patients undergoing spine surgery from 2016-2020 at a single, academic institution with available preoperative thoracic spine CTs were included. Subjects with previous instrumentation at any thoracic level, concurrent vertebral fractures or a Cobb angle of more than 20 degrees were excluded. Asynchronous QCT measurements of T1-T12 were performed. To assess inter- and intra-observer reliability, a validation study was performed on 10 randomly selected patients. The interclass correlation coefficient (ICC) was calculated. A pairwise comparison of BMD was conducted and correlations between each thoracic level were evaluated. Results: 60 patients (men, 51.7%) met inclusion criteria. The study population was 90% Caucasian with a mean age of 62.2 years and a mean BMI of 30.2 kg/m2. The inter- and intra-observer reliability of the thoracic QCT measurements was excellent (ICC of 0.968 and 0.967, respectively). The trabecular BMD was highest in the upper thoracic spine and decreased in the caudal direction (T1 = 182.3 mg/cm3, T2 = 168.1 mg/cm3, T3 = 163.5 mg/cm3, T4 = 164.7 mg/cm3, T5 = 161.4 mg/cm3, T6 = 152.5 mg/cm3, T7 = 43.5 mg/cm3, T8 = 141.3 mg/cm3, T9 = 143.5 mg/cm3, T10 = 145.1 mg/cm3, T11 = 145.3 mg/cm3, T12 = 133.6 mg/cm3). The BMD of all thoracic levels cranial to T6 was statistically higher than the BMD of all levels caudal to T6 (P < 0.001). Nonetheless, significant correlations in BMD among all measured thoracic levels were observed, with a Pearson’s correlation coefficient ranging from .74 to .97. Conclusion: Our results indicate significant regional BMD differences in the thoracic spine. This BMD variation might contribute to several clinically relevant phenomena: First, vertebral fractures have a bimodal distribution and occur most commonly at the thoracolumbar junction (T12-L1), with the midthoracic region (T7-T8) being the second most common site. In addition to mechanical reasons, this might be partially attributed to thoracic BMD that is lowest at T12, followed by T8. Second, optimal upper instrumented vertebra (UIV) for stopping long fusions to the sacrum and pelvis are controversial. The BMD of surgically relevant upper thoracic stopping points (T2-T4) was significantly higher than the BMD of lower thoracic stopping points (T10-T12). Besides stress concentration at the relatively mobile lower thoracic segments, the low BMD at these levels might contribute to previously suggested higher rates of junctional failures with short fusions.
169
A148: Imaging Profile of Subjects with Lumbar Developmental Spinal Stenosis in a Population-Based Cohort
Prudence Wing Hang Cheung 1 , Marcus Kin Long Lai 1 , and Jason Cheung 1
1 The University of Hong Kong, Orthopaedics and Traumatology, Hong Kong, Hong Kong
Introduction: Developmental spinal stenosis (DSS) occurs when there is narrowing of spinal canal due to maldevelopment of posterior elements relating to genetic disturbance during fetal and postnatal period. Lumbar DSS is of clinical significance as the pre-existing narrowed vertebral canal predisposes patients to experiencing neural compression at a lower threshold, as well as symptoms being presented even with milder degree of degenerative changes of the lumbosacral spine. Current knowledge of DSS mainly lies at the level-specific radiographic definition of the smaller canal size, the relationships between the presence of DSS and different spinal tissues remain unknown. This study aims to determine the differences of spinal imagining phenotypes between subjects with lumbar DSS and those without DSS in a population-based cohort. Materials and Methods: This was a radiological analysis of 2387 subjects who underwent L1-S1 magnetic resonance imaging (MRI) in the population-based disc degeneration cohort. Data collection included patient’s age, gender, body mass index and MRI measurements. Differentiation of cases of lumbar DSS from non-DSS was based on the anteroposterior (AP) vertebral canal diameters. The measurement of other imaging parameters included the vertebral body dimensions, spinal canal dimensions, disc degeneration scores and facet joint orientation. Mann-Whitney U and chi-square tests were used to assess for any differences of these parameters between DSS and non-DSS subjects. To identify possible associations between the presence of DSS and various MRI parameters, univariate and multivariate regression analyses were conducted with adjustment for subject demographics. Results: Axial AP vertebral canal diameter, interpedicular distance, AP dural sac diameter, lamina angle and sagittal mid-vertebral body height were significantly different between lumbar DSS and non-DSS subjects (all at P < .05). Lamina angle (OR: 1.127; P = .002) was associated with the presence of lumbar DSS. Narrower interpedicular distance (OR: 0.745, P = .002) and AP dural sac diameter (OR: 0.506, P < .001) as well as right facet joint angulation (OR: 0.022; P = .002) were also associated with lumbar DSS. No association was observed between disc parameters and DSS. Conclusion: In this large-scale cohort, the vertebral canal size is found to be independent of subject body habitus and vertebral body dimensions. A more obtuse lamina angle and smaller dural sac are found associated with the presence of DSS at the lumbosacral spine, whereas no associations between DSS and disc and endplate parameters such as disc herniation, disc degeneration, Schmorl’s notes, endplate irregularity. Other than spinal canal dimensions, abnormal orientations of lamina angle and facet joint angulation may be a result of developmental variations, leading to increased likelihood of DSS. Other skeletal parameters are spared. The lack of relationship between DSS and soft tissue changes of the spinal column suggested DSS is purely a result of bony maldevelopment.
733
A149: Clinical and Radiographic Outcomes MISS Stand-Alone ALIF vs Posterior Approach Surgery (PCO and Transpedicular Fixation) for Adult Degenerative Scoliosis
Anton Denisov 1 , Dmitry Ptashnikov 1,2 , Dmitry Mikhaylov 1 , Oleg Smekalenkov 1 , Nikita Zaborovskii 1 , and Sergei Masevnin 1
1 National Medical Center of Traumatology and Orthopaedics n.a. Vreden R.R., Bone oncology and spinal surgery, Saint-Petersburg, Russian Federation
2 North-Western State Medical University named after I.I. Mechnikov, Traumatology and Orthopaedics, Saint-Petersburg, Russian Federation
Introduction: Despite the effectiveness of various types of Posterior Column Osteotomies (PCO), they are associated with several disadvantages ( high blood loss, long hospital stay, prolonged intraoperative time, post-op neurological deficit). Minimally invasive spinal surgery (MISS) is gaining popularity around the world as an alternative to open interventions. Also, for improving segmental and total lordosis began to applicate interbody cages with high lordotic angles which contribute for appropriate correction degree and induce indirect decompression by increasing of intervertebral heights. For degenerative scoliosis, asymmetric lordotic titanium cages could help not only in sagittal but in frontal balance correction that can improve radiographic and clinical outcomes. Material and Methods: One -center prospective study of 72 patients with lumbar degenerative scoliosis, mean age 64 (95% CI 57-68). 2 groups were formed in accordance with the classification of SRS-Schwab (2012) and randomized using a random numeral table. The first group (control): transpedicular fixation, SPO and deformity correction from posterior approach. The second group (MISS ALIF): interbody fusion with ALIF stand-alone technique. Was measured intraoperative blood loss, surgery time, hospital stay, sagittal and spine-pelvic parameters (PI, PI-PT, LL, SVA). The degree of pain (VAS scale), SRS-22 and Oswestry scale were evaluated at 5 days-3-6-12 months. Observational period from 2018 to 2020 years. Results: Statistically significant differences (P < .05) were observed in the comparison of such parameters: duration of hospitalization (17 ± 5 in the control, 8 ± 2 in the ALIF group), blood loss (730 ± 380 and 288 ± 61), LL (34 ± 6.2 in mis group and 23 ± 7.3, control). At 5 days of post-op: VAS (3.5 ± 1 and 2.8 ± 1.1 for mis group), ODI ( 55.6 ± 2.1 and 27.9 ± 1.3 for mis group) SRS-22 (55.6 ± 2.14 and 82.3 ± 2.7 for mis group).At 3 months of post- op: VAS (4.4 ± 1.2 and 1.8 ± 0.8 for mis group) ODI (69.2 ± 2.4 and 34.0 ± 1.6 for mis group) SRS - 22 (46.3 ± 3.1 and 74.6 ± 1.1 for mis group). In the rest of post-operative period we haven't observed statistically significant differences (P > .05). But clinically for the rest of post-op period it was still being observed tendency of improvement in MISS ALIF group. Conclusion: Our results support our hypothesis that implementation of lordotic cages as stand-alone MISS ALIF could be a best alternative for PCO technique. Hyperlordotic cage provides a significant degree of correction of lumbar lordosis. Despite the clinical and statistical the same degree of restoration of sagittal balance, this technique allows to reduce blood loss, hospital stay days and give better functional results in early post-op period, that can reduce the usage of painkillers and start rehabilitation process much earlier.
239
A150: Rate of Failure of Indirect Decompression in Lateral Single-Position Surgery - Clinical Results
J Alex Thomas 1 , Christopher I. M. Thomason 1 , Brett Braly 2 , and Cristiano Menezes 3
1 Atlantic Neurosurgical and Spine Specialists, Neurosurgery, Wilmington, USA
2 Oklahoma Sports Science and Orthopedics, Orthopedics, Oklahoma City, USA
3 Columna Institute/ H. Ortopedico Lifecenter, Orthopedics, Belo Horizonte, Brazil
Objective: Lateral single-position surgery (LSPS) of the lumbar spine generally involves anterior lumbar interbody fusion (ALIF) performed in the lateral position (LALIF) at L5/S1 with or without lateral lumbar interbody fusion (LLIF) at L4/5 and above, followed by bilateral pedicle screw fixation (bPSF) without repositioning the patient. One obstacle to more widespread adoption of LSPS is the perceived need for direct decompression of the neural elements, which typical requires a flip to the prone position. The purpose of this study is to examine the rate of failure of indirect decompression (ID) in a cohort of patients undergoing LSPS from L4-S1. Methods: A multi-center, post-hoc analysis was undertaken from prospectively collected data of patients who underwent LALIF at L5/S1 with or without LLIF at L4/5 with bilateral PSF the lateral decubitus (LD) position between March 2018 and March 2020. Inclusion criteria were symptoms of radiculopathy or neurogenic claudication, central or foraminal stenosis (regardless of degree or etiology), and indication for interbody fusion at L5/S1 or L4-S1. Skeletally immature patients, those with tumor, trauma, suspicion of infection, needing revision surgery, or greater than two levels of fusion were excluded. Baseline patient demographic information as well as surgical data were collected and analyzed. The number of patients that failed ID was recorded and each individual case of failure was analyzed. Results: 178 consecutive patients underwent LSPS during the time period (105 patients underwent LALIF at L5/S1 and 73 patients underwent LALIF at L5/S1 with LLIF at L4/5.) Average follow up was 10.9 months (±6.5). bPSF was placed in the LD position in 149 patients; there were 29 standalone cases. Average case time was 101.9 minutes (±41.5), 79.3 minutes for single-level cases, and 134.5 minutes for 2-level cases. 2 patients (1.1%) required reoperation for failure of ID. There were no major operative complications. Conclusions: The rate of failure of ID in LSPS from L4-S1 is exceedingly low. This low risk of failure should be weighed against the risks associated with direct decompression as well as the risks of the extra operative time needed to perform this decompression.
1882
A151: The Impact of Posterior Cervical Foraminotomy on Neck Pain: A Systematic Review and Meta-Analysis
Hikari Urakawa 1 , Kosuke Sato 1 , Avani Vaishnav 1 , Bridget Jivanelli 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
Introduction: Posterior cervical foraminotomy (PCF) is a safe and reasonable surgical treatment option for cervical radiculopathy. There are a plethora of studies evaluating the improvement of radiculopathy, but very few studies report on the impact of the procedure on neck pain. The aim of this study was to elucidate the impact of PCF on neck pain. Material and Methods: A systematic review and meta-analysis was performed based on rules set forth by preferred reporting items for systematic reviews and meta-analysis (PRISMA). A comprehensive literature search was performed in PubMed/ MEDLINE, EMBASE and the Cochrane Library, using Medical Subject Heading terms (“neck” and “foraminotomy”) and associated text words. The search strategy was created by one author and one librarian. Two authors independently reviewed all articles and identified studies presenting clinical outcomes including visual analog scale (VAS) at neck or neck disability index (NDI) for patients who underwent PCF for cervical radiculopathy. Exclusion criteria included patients who had surgery for myelopathy or non-degenerative cervical diseases or who underwent PCF in conjunction with laminoplasty or laminectomy with or without fusion. We also excluded studies that did not provide both pre- and postoperative outcomes, were not written in the English language, or were review articles or case reports of less than 10 patients. Meta-analysis was performed with studies that provided means with standard deviations of VAS and NDI. Results: The initial literature search resulted in 766 articles, of which, 30 studies were met inclusion criteria. VAS neck and NDI improved after PCF in all studies. 11 studies (14 cohorts) with 366 patients were included in meta-analysis. The mean follow-up period was 27.1 months. Minimally invasive techniques for PCF (MI-PCF) were used in 9 articles. The mean delta improvement of VAS neck was 3.99 (95%CI 2.92-5.07, P < .001). The mean delta improvement of VAS arm was 5.73 (95%CI 5.25-6.22, P < .001). The mean delta improvement of NDI was 24.72 (95%CI 21.03-28.42, P < .001). While the mean delta improvement of VAS neck in conventional PCF was 3.74 (95%CI 2.89-4.59), that in MI-PCF was 4.07 (95%CI 2.83-5.31) (P = .66). Conclusion: Contrary to popular belief, patients undergoing posterior cervical foraminotomy can expect to have improvement in their neck pain. Moreover, patients undergoing MI-PCF may experience a greater improvement in neck pain compared to open techniques.
1547
A152: Does Obesity Affect Long-Term Outcomes of Lateral Lumbar Interbody Fusion
Stuart Changoor 1 , Michael Faloon 1 , Conor Dunn 1 , Aksha Parray 2 , Kumar Sinha 1 , Ki Hwang 2 , and Arash Emami 1
1 St. Joseph's University Medical Center, Paterson, NJ, USA
2 Rutgers New Jersey Medical School, Newark, NJ, USA
Introduction: Obese patients can pose significant challenges to spine surgeons in lumbar fusion procedures. The increased risk of complications has led surgeons to be wary in pursing operative interventions in these patients. With the increased proportion of obese patients, it is imperative to understand the long-term outcomes in minimally-invasive approaches. The purpose of this study was to evaluate the long-term safety and efficacy of LLIF in the obese. Material and Methods: A retrospective review was performed to identify patients who underwent LLIF with posterior stabilization since 2007 with a minimum of 5 years follow-up. Demographics including BMI were recorded and patients were subdivided into 2 cohorts: (A) nonobese (BMI <30 kg/m2) and (B) obese (BMI >30 kg/m2). Functional outcomes were assessed by comparing pre- and post-operative VAS and ODI scores. Reoperation rates were compared between cohorts. Pelvic incidence (PI) and lumbar lordosis (LL) mismatch was calculated from both pre- and post-operative radiographs. Results: 115 consecutive patients were included (53 nonobese & 62 obese) with a mean follow up of 95.3 months. Mean BMI was 25.3 in cohort A and 35.3 in cohort B (P < .001). There were more females in cohort A. VAS scores decreased by a mean of 5.7 in cohort A, and 5.4 in cohort B (P = .213). ODI improvement was also similar between the cohorts. 5.6% of nonobese patients required reoperation compared to 9.6% of obese patients (P = .503). Both cohorts achieved a similar proportion of PI-LL mismatch correction, 85% in obese vs 78% in nonobese patients (P = .526). Conclusion: Obese patients have similar surgical outcomes to nonobese patients with respect to functional outcome scores, reoperation rates, and correction of PI-LL mismatch after long-term follow-up. With similar outcome and reoperation profiles, minimally-invasive approaches to the spine, such as LLIF, may be an acceptable alternative to traditional open procedures in obese patients.
740
A153: Clinical and Radiological Outcomes for Mini-Open Combined 1 Step Anterior and Oblique Approach for 2 Level Lumbar Interbody Fusion
Pablo Mendivil 1 , Guillermo Vergara 1,2 , Juam Pablo Sirena 1 , William Velázquez 1,2 , Sofia Beltrame 1
1 Unidad de Cirugía Espinal Compleja y Minimamente Invasiva - Neurocentro Salta - IMAC Instituto Medico de Alta Complejidad, Salta Argentina, Departamento de Neurocirugía, Salta, Argentina
2 Hospital San Bernardo, Salta Argentina, Servicio de Neurocirugia, Salta, Argentina
Introduction: Lumbar interbody fusions techniques include anterior (ALIF), posterior (PLIF), transforaminal (TLIF), extreme lateral (XLIF) and oblique lateral interbody fusion (OLIF), each with its own advantages and disadvantages. L4-L5 and L5-S1 arthrodesis is the most common lumbar double fusion association. The objective of this work is to assess the clinical and radiographic outcomes and complications and determine the comparative effectiveness and safety of mini-open combined one step anterior and oblique approach for two level lumbar interbody fusion. Material and Methods: Eleven patients with indication of L4-L5 and L5-S1 arthrodesis underwent mini-open combined one step L5-S1 anterior and L4-L5 oblique interbody fusion and percutaneous posterior pedicle screws. Demographics, fusion rate, Modified Macnab Criteria Outcome and surgical complications were assessed. Visual Analog Scale score, Oswestry Disability Index and spinopelvic parameters, were evaluated before and after surgery. Results: The mean age of the patients was 49 years. Visual Analog Scale mean improved from 6.27 to 1.09 9 months after surgery and Mean Oswestry Disability Index from 42.5 % to 10.36 %.The mean value of the spinopelvic parameters ± SD preoperative and postoperative was pelvic tilt (PT) 12.4 ± 9.36 - 14.9 ± 7.25, sacral slope (SS) 35.9 ± 14.20 - 140.6 ± 7.60, pelvic incidence (PI) 52.3 ± 17.04 - 59.5 ± 13.60 and lumbar lordosis (LL) 55.8 ± 11.68 - 59.1 ± 10.73. Fusion rate was found to be 95,4% at 9 months. There was no spinal nerve or urinary injury, one major vessel (venous) and two peritoneal lesions without clinical consequences and one case of transient retrograde ejaculation. Conclusions: ALIF seems to be the preferred method in L5/S1 for discogenic LBP and lordosis restoration, in L4/L5 alif/olif the second option because increased risk of vascular injury. Combined one step ALIF for L5-S1 and oblique approach through the surgical window between the psoas and the left common iliac vein for L4-L5 interbody fusion seems to be a good option that combines the good results of the anterior technique minimizing the surgical risks.
OP18: Spinal Tumor Surgery 1
495
A154: Surgical Treatment of Spinal Metastases of the Cervicothoracic Junction
Vanessa Hubertus 1 , Michelle Marino 1 , Czabanka Marcus 1 , Arthur Wagner 2 , Nicole Lange 2 , Ann Kathrin Joerger 2 , Jens Gempt 2 , Björn Sommer 3 , Sven Eicker 4 , Martin Stangenberg 5 , Insa Janssen 6 , Christoph Wipplinger 7 , Veit Rohde 3 , Karl Schaller 6 , Claudius Thomé 7 , Peter Vajkoczy 1 , Julia Onken 1 , and Bernhard Meyer 2
1 Charité - Universitätsmedizin Berlin, Neurosurgery, Berlin, Germany
2 Technische Universität München, Neurosurgery, Munich, Germany
3 Universitätsmedizin Göttingen, Neurosurgery, Göttingen, Germany
4 Universitätsklinikum Hamburg-Eppendorf, Neurosurgery, Hamburg, Germany
5 Universitätsklinikum Hamburg-Eppendorf, Traumatology, Hamburg, Germany
6 Hôpitaux Universitaires de Genève, Neurosurgery, Genève, Switzerland
7 Medizinische Universität Innsbruck, Neurosurgery, Innsbruck, Austria
Introduction: Spinal metastases of the cervicothoracic junction (CTJ; C7-Th2) pose a challenge for treatment. The aim of our study is to compare surgical strategies for their treatment with respect to surgical complexity and associated complications. Material and Methods: 238 patients were surgically treated with spinal metastases of the CTJ in 2005-19 at 7 university centers in Europe. SINS, clinical, surgical and outcome data were assessed. Patients were divided into 4 groups: those with high comorbidities were only decompressed (1), decompression and instrumentation from posterior (2) or anterior (3) was performed in case of instability (SINS) dependent on location of myelon compression (2/3). 360° anterior-posterior instrumentation was performed in extensive lytic lesions and in cases with low comorbidities (4). Results: 37 patients were treated in (1) (15%), 127 patients in (2) (53%), 18 patients in (3) (8%) and 56 patients in (4) (24%). Medium SINS was (1) 7, (2 + 3) 11 and (4) 12. In (1-2) patients presented with worse neurological function than (3-4), whereas in (1) systemic tumor burden was highest. In (2-4) 83-89% suffered from mechanical pain, in (1) 50%. Complications occurred in (1) 17%, (2) 43%, (3) 22% and (4) 32%. Hardware failure (HwF) during follow-up occurred exclusively in (2) and led to surgical revision in 6 cases. HwF occurred exclusively in monocortically placed massa lateralis screws (mMLS) in the cervical spine. In case of bicortical massa lateralis screws (bMLS) or pedicle screws (PS) no HwF was observed at 10 months follow-up. Conclusion: The biomechanical loading capacity of dorsal instrumentation alone seems to have a decisive influence on revision rate in metastases of C7-Th2. In patients with favorable comorbidity rate, the extension of life expectancy through new therapy options should play a crucial role in choosing the right surgical strategy. Attention should be paid to the distinct biomechanical properties of the CTJ, with 360° stabilization and placement of bMLS or PS preferable to mMLS in our multicentric cohort.
1687
A155: Multilevel Total en-Bloc Excision of Primary Chondrosarcoma of the Thoracic Spine Through an all Posterior Approach. Case Presentation and Systematic Review of Literature
Nigil Palliyil 1 , Nasir Quraishi 1 , and Kedar Deogaonkar 2
1 Queens Medical Centre, Nottingham University Hospital, Spinal Surgery, Nottingham, United Kingdom
2 Deenanath Mangeshkar Hospital and Research Centre, Pune, India
Introduction: Chondrosarcomas are malignant cartilage forming neoplasms which account for 10% of all the primary bone tumours. As these tumours are resistant to chemotherapy and radiotherapy, en-bloc excision of the tumour with wide margins is the only option that provides maximum disease free survival and possible cure. We present two cases of primary chondrosarcoma of the thoracic spine treated by multilevel en-bloc excision through an all posterior approach and review the literature pertaining to anterior-posterior versus posterior only approaches for multilevel en-bloc excision of primary malignant tumours. Methods: Two cases of multilevel chrondrosarcoma are presented who both underwent posterior only approaches. Further, a systematic review of the English language literature was carried out using search criteria en-bloc primary thoracic spinal tumours/ vertebrectomy/ spondylectomy, for papers published between (January 1999 and September 2019) using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Results: Both our patients tolerated the procedure well without any postoperative neurological deficits and no major perioperative complications. No local tumour recurrence or distant metastasis was observed till last follow up at 36 months. From our systematic review, a total of 48 articles were identified, and final 7 papers (all retrospective reviews, Level III/IV) were analysed. These studies reported the outcome of 135 cases of en-bloc resections of primary malignant tumours with a mean follow up duration of 39 months (3-211). The primary tumours mainly comprised of chondrosarcomas, chordomas, GCTs and osteosarcomas. The local recurrence rate following en-bloc resections was found to be 14.9%. The complication rate was higher in multi-level resections and when combined anterior+posterior approach (48.3%) was performed as against posterior only approach (10.6%, (P < .0001)). The incidence of local recurrence was higher in patients undergoing en-bloc resection for a recurrent tumour than previously untreated tumour (38.9% vs 7.1%, P < .0001), but not affected by the surgical approach. Conclusions: Multilevel en-bloc tumour resection of the spine is a technically demanding procedure, however it remains the treatment of choice in certain primary tumours as they are potentially curative. A posterior only approach appears to show a significantly lower complication rate when compared to combined anterior-posterior approaches. Local recurrence rate is the highest following en-bloc resection for recurrent tumours, emphasising the importance of a meticulously performed primary surgery.
819
A156: Multiple Cavernous Angiomas of Central Nervous System Associated with Neurofibromatosis Type 2 (NF2)
Dimitar Haritonov 1
1 University Hospital Heart and Brain, Neurosurgery and Spine Surgery, Pleven, Bulgaria
Introduction: Cavernous angiomas (CA) represent 5-12% of all spinal vascular lesions and 1% of all intramedullary lesions in pediatric and young adult patients. Intramedullary spinal cavernomas are relatively rare with only 24 cases reported till date to the best of our knowledge. The aim of presentation of this case is findings of multiple cavernous angiomas of central nervous system associated with Neurofibromatosis type 2 (NF 2). Material and Methods: A 35 year-old man presented to the clinic with acute onset motor weakness in lower limbs. He was diagnosed with multiple cerebral cavernomas and an acutely bleeding spinal cavernoma. MRI showed multiple cerebral silent cavernous angiomas, symptomatic spinal cord cavernous angioma with perilesion bleeding in thoracic region and right acoustic schwannoma associated with café au late spots on the back. Results: Complete surgical excision of the spinal cavernoma was done. Postoperatively the patient's weakness gradually improved to a power of 4/5 in lower limbs over a period of 10 days. Conclusion: Only 24 cases of pediatric and young adults spinal cavernomas have been reported in the current literature. Current consensus on management of these rare lesions is based on previously published case reports/series and surgery appears to be the only definitive treatment.
1369
A157: Metastatic Spine Tumor Surgery in Elderly Patients: Analysis of 78 Patients
Ibrahim Hussain 1 , Benjamin Hartley 1 , Anne Reiner 1 , Ilya Laufer 1 , Mark Bilsky 1 , and Ori Barzilai 1
1 Memorial Sloan Kettering Cancer Center, New York, USA
Introduction: Octogenarians living with spinal metastases are a challenging population to treat, given a high incidence of medical comorbidities. Our purpose was to identify the rate, types, management, and predictors of complications and survival in octogenarians following surgery for spinal metastases. Material and Methods: A single-institution retrospective review of a prospectively collected cohort was performed. Patients aged 80 years or older who underwent open or minimally invasive surgery (MIS) with instrumentation for metastatic spinal tumor treatment between 2008 and 2019 were included. Demographic, intraoperative, and postoperative clinical characteristics were collected. Complications were classified into categories such as wound-related, hematoma, venous thrombosis, pulmonary, and cardiac, among others. We also divided complications into 5 grades based on intervention or outcome. Discharge destination was classified as either home, rehabilitation center, hospice, or death in hospital. Cox proportional hazards regression was used to associate variables with overall survival. Logistic regression was used to associate variables with postoperative complications. Results: 78 patients (mean 83.6 years) met inclusion criteria, of which 81% had open surgery. Average operative time, blood loss, and length of stay were 157 minutes, 615 mL, and 9 days, respectively. The overall complication rate was 31% (N = 24). 16% of all patients required an interventional procedure to address a complication and 7% had life-threatening or fatal complications. The most common complications were wound dehiscence/infection (N = 6), pulmonary (N = 4), and hematoma (N = 3). 91% of patients were discharged home or to rehab. 4 patients (5.1%) died the same admission. Blood loss was significantly associated with increased risk of complications (OR = 1.001; P = .048). There was a non-significant trend towards increased mortality when decompression was also performed (OR = 2.12; P = .09). For deceased patients, median survival was 136 days. For patients still alive, median follow-up period was 441 days. Conclusion: Surgery for metastatic spine disease in octogenarians should not be ruled out based on age only as it can be performed with goals of palliation. Octogenarians undergoing surgery for spinal metastases are at increased risk for postoperative complications and mortality particularly when performing decompression in addition to stabilization and with increasing intraoperative blood loss.
1769
A158: Are Vertebral Hemangiomas Always Innocuous? A Retrospective Series of 23 Patients Who Underwent Surgical Treatment Following Aggressive, Symptomatic, Atypical Vertebral Hemangiomata
Ajoy P Shetty 1 , Guna Pradeep 1 , Vibhu Krishnan Viswanathan 1 , and Shanmuganathan Rajasekaran 1
1 Ganga Medical Center and Hospitals, Coimbatore, India
Introduction: Aggressive vertebral hemangiomata are rare forms of vertebral body hemangiomas, which present with significant vertebral expansion, extra-osseous components with extension into epidural space, disturbance of vascularity and compression fractures leading to spinal cord and/or nerve root compression. They constitute 1% of all spinal hemangiomas and are usually symptomatic. Three-fourths of these lesions occur in the thoracic segments between T3 and T9 levels. The literature evidence on this subject till date is scarce. Materials and methods: A single-centre, retrospective observational study was conducted to analyze the clinical presentation and surgical outcome of patients, who presented with aggressive haemangiomas between January 2010 and February 2020. Only patients who underwent surgical treatment and instrumented stabilization, and had at least 6 months follow-up were included. Results: A total of 23 (mean age 46.4 ± 17.1 years; 15 females) patients with symptomatic, aggressive (Enneking stage III) vertebral haemangioma were diagnosed and surgically treated at our Institution during this period. 3 female patients presented during the peri-partum period (2 during antepartum and 1 in the immediate post-partum periods). Gait instability was the most common presenting symptom in 39.1% (n = 9) patients. Pain, radiculopathy and neurodeficit were the presenting symptoms in 30.4% (n = 7), 17.4% (n = 4) and 13.0% (n = 3) of patients, respectively. Two of these patients had associated bowel/ bladder disturbances. The clinical signs of myelopathy was seen in 73.9% (n = 17). The most common site of lesion was the thoracic spine (n = 13), followed by thoraco-lumbar (D11-L2; n = 18) and lumbar regions (n = 2). The lesion was solitary in 56.5% (n = 13). In the remaining patients with multifocal hemangiomas, only one of the lesions was symptomatic. Preoperative embolization was performed in 73.91% (n = 17) of patients. Radiologically, 12 patients had an epidural component, 5 had both epidural and paravertebral components and 2 had paravertebral extension. Three patients had isolated involvement of vertebral body and 1 patient presented with extension of the lesion into the bilateral pedicles. In all the four patients without significant soft tissue extension, the lesion spanned the entire body and led to significant collapse of the vertebra necessitating surgery. Overall, 65.21% (n = 15) underwent posterior-alone surgery, while the remaining underwent combined antero-posterior surgery. The local recurrence rate was 8.7% (n = 2). Preoperatively, 43.4% patients (n = 10) had normal neurology, while 39.1% (n = 9), 13% (n = 3) had ASIA D and ASIA C neurology respectively. One patient presented with ASIA A neurology. During postoperative followup, all patients regained normal power except the one with ASIA A who improved to ASIA C. Conclusion: Vertebral haemangiomas are commonly-encountered, benign vascular malformations. On rare occasions, they can manifest with aggressive lesions causing extracorporeal extension and neurodeficit. These aggressive lesions require aggressive, timely surgical interventions to prevent progressive collapse and neurological catastrophes. Patients who present with neurological deficit benefit significantly from lesion excision, spinal decompression and instrumented stabilisation. Complete excision of the lesions is necessary to reduce the recurrence rates.
1913
A159: Long-Term Result of Sacrococcygeal Chordoma Surgical Management: About 13 Cases
Mouadh Nefiss 1 , Nouira Amine 1 , Bousrih Anis 1 , Saied Abdellali 1 , Ezzaouia Khelil 1 , and Tborbi Anis 1
1 Mongi Slim Hospital, Orthopedic Surgery Department, La Marsa, Tunisia
Introduction: Chordoma is a rare slowly evolving malignant tumour. The sacral location is the most common. The curative treatment is surgical, either by a double approach or by a simple posterior approach. However, surgery is not always possible when the diagnosis is late. The aim of our work is to evaluate the long-term results in the management of sacro-coccygeal chordomas. Material and Methods: We report a series of 13 cases collected over a period of 18 years. Epidemiological, clinical, radiological and therapeutic characteristics were studied. Factors of poor prognosis were investigated. Results: The patients were 9 men and 4 women, ranging in age from 24 to 79 years. The diagnosis was made with an average delay of 2 years from the onset of symptomatology. The surgical biopsy confirmed the diagnosis for all patients. No metastases were found in the extension work-up. The treatment was exclusively surgical for 10 patients. For 3 patients, abstention was chosen because of the extension of the lesions, notably distal and intra-pelvic, preventing any surgical removal. Carcinological resection was performed in 6 cases using a double approach for 5 patients and a single posterior approach for 1 patient. No adjuvant treatment was associated. The average delay was 8 years for the 10 patients operated on. Four patients developed genito-sphincter disorders but without sacral recurrence. These disorders were definitive in only one case. 2 patients died, one by metastasis and the other in immediate post-operation by an uncontrollable bleeding and the two other patients developed a local recurrence at 2 years of age treated by simple curettage. Finally, at 7 years of age, a patient developed a second location in the dorsal spine (D6) complicated by paraplegia. The factors of poor prognosis in our series were the low socio-economic level of the patients, a symptomatology made of constipation and radiculalgia in preoperative period and a proximal localization at the level of S2 on MRI. In the literature the factors of poor prognosis differ according to the studies, however the majority of them incriminate intra-lesional surgery in a non-specialised centre, non-carcinological resection of the tumour and invasion of the rectal wall on MRI. Conclusion: Sacral chordoma is a slow-growing tumour invading noble structures which are difficult to respect during excision. The technique of the double approach for carcinological resection seems to be the safest, allowing a better clinical result and a better quality of life. Diagnostic delay is the most important factor in poor prognosis, which can be addressed especially with improved imaging techniques.
54
A160: Pre-Treatment Expectations of Patients With Spinal Metastases: What Do We Know and What Can We Learn from Other Disciplines? A Systematic Review of Qualitative Studies
Roxanne Gal 1 , Douwe Oostinga 2 , Hester Wessels 3 , Jorrit-Jan Verlaan 2 , Raphaële Charest-Morin 4 , Charles Fisher 4 , Lenny Verkooijen 1 , and Anne Versteeg 1
1 University Medical Center Utrecht, University of Utrecht, Division of Imaging and Oncology, Utrecht, The Netherlands
2 University Medical Center Utrecht, University of Utrecht, Department of Orthopaedic Surgery, Utrecht, The Netherlands
3 University Medical Center Utrecht, Department of Corporate Communications, Utrecht, The Netherlands
4 University of British Columbia, Vancouver General Hospital, Department of Orthopaedics, Division of Spine, Vancouver, British Columbia, Canada
Introduction: Currently, little is known about treatment expectations of patients with spinal metastases undergoing radiotherapy and/or surgery. Assuming that patients with spinal metastases share characteristics with patients who had spinal surgery for non-cancer related conditions and with advanced cancer patients, we performed a systematic review to summarize the literature on patient expectations regarding treatment outcomes of spinal surgery and advanced cancer care. Material and Methods: A comprehensive search was performed in MEDLINE, EMBASE and PsycINFO for studies between 2000 and sep-2019. Studies including adult patients (>18 years), undergoing spinal surgery or receiving advanced cancer care, investigating patients’ pre-treatment expectations regarding treatment outcomes were included. Two independent reviewers screened titles, abstracts and full-texts, extracted data and assessed methodological quality. Results: The search identified 7343 articles, of which 92 were selected for full-text review. For this review, 31 articles were included. Patients undergoing spinal surgery had overly optimistic expectations regarding pain and symptom relief, they underestimated the probability of functional disability, and overestimated the probability of (complete) recovery and return to work. Studies highlighted that patients feel not adequately prepared for surgery in terms of post-treatment expectations. Similarly, advanced cancer patients receiving palliative treatment often had overly optimistic expectations regarding their survival probability and cure rates. Conclusion: Patients tend to have overly optimistic expectations regarding pain and symptom relief, recovery and prognosis following spinal surgery or advanced cancer care. Pretreatment consultation about the expected pain and symptom relief, recovery and prognosis may improve understanding of prognosis, and promote and manage expectations, which, in turn, may lead to better perceived outcomes.
554
A161: Time Between the First Symptoms and the Onset of Neurological Deficits in Patients with Metastatic Spinal Disease
Floris van Tol 1 , Anne Versteeg 2 , Tom Snijders 1 , Cumhur Oner 1 , and Jorrit-Jan Verlaan 1
1 UMC Utrecht, Utrecht, The Netherlands, 2 University of Toronto, Toronto, Canada
Introduction: Spinal metastases are among the most debilitating complications of (untreated) malignant disease. Without timely treatment, patients are at risk for metastatic spinal cord compression, severely hampering their quality of life and survival. It is essential for oncological health-care providers to be aware of the limited time available to diagnose and treat spinal metastases. The primary objective of the current study was to quantify the time between the onset of symptoms related to metastatic spinal disease and the onset of signs of spinal cord dysfunction. Materials and Methods: A retrospective review of 303 patients with an indication for surgical treatment of spinal metastases was conducted. The time to neurological deficits was determined in days by calculating the time between the onset of symptoms related to spinal metastases and the onset of neurological deficits for each individual patient. Multivariate Poisson regression was used to correlate the time to neurological deficits to the primary tumor, the localization of spinal metastases and the oncological history of the patient. Results: Sensorimotor deficits occurred in 113 patients with a median time to neurological deficits of 66.5 days, showing great variation between spinal localization, tumor type and the absence or presence of a preexisting cancer diagnosis. Of all the neurological deficits, 75% occurred while under active medical care for symptoms related to spinal metastases. More than 30% of neurological deficits occurred after the diagnosis of metastatic spinal disease, but prior to initiation of specific treatment. Conclusion: The current study shows the limited time available before the potential onset of spinal cord injury in patients with spinal metastases. These results emphasize the importance of awareness amongst oncological health-care providers on the timely identification and treatment of metastatic spinal disease, thereby potentially improving their outcome considerably.
910
A162: Single-Stage Minimal-Invasive Posterolateral Transpedicular Approach (MITPA) in the Treatment of Metastatic Tumors in Thoracic Spine
Rafal Zaluski 1 , and Wiktor Urbanski 1
1 Medical University of Wrocław, Neurosurgery, Wroclaw, Poland
Introduction: Surgical treatment of spinal metastatic tumors usually consists of combination of neural structures decompression and spinal fixation. If the lesion extends to the vertebral body, the anterior column may require additional support. In these cases, typically open one-stage postero-lateral approach is performed or occasionally combined two-stage posterior and anterior approach. Unfortunately, these extensive open surgeries are associated with high complication rate. In our study we designed a minimally invasive technique of posterolateral transpedicular approach (MITPA) for posterior pedicular fixation and anterior corpectomy in patients with metastatic tumors. The object of the paper is to present the MITPA technique and compare perioperative results with open techniques. Material and Methods: This is a single surgeon series of 35 patients who had posterior pedicular fixation with corpectomy and anterior cage insertion due to metastatic lesion in thoracic spine. In 15 consecutive patients operated between 2017 and 2019 in the Department of Neurosurgery, posterior percutaneous pedicular fixation with additional corpectomy and decompression with minimal invasive posterolateral transpedicular approach (MITPA) were performed (showed in figure 1). The operation time, average blood loss, neurological functions recovery and occurrence of complications were assessed. The measurements on radiographs were preformed pre and postoperatively to assess the restoration of spinal alignment. The group of 20 patients operated between 2015 and 2019 due to metastatic tumors who underwent open procedures of pedicular fixation with corpectomy were assessed similarly and the results compared between open and MITPA groups. Results: The average operation time in MITPA group was 3 hours 27 minutes and was comparable to the duration of the procedure performed using the open technique (3 hours 42 minutes). We have noticed significantly decreased intraoperative blood loss in MITPA group vs open surgery group (313 ± 74 vs 815 ± 257, P = .0016). In both groups, no deterioration of patients' neurological status was observed. In open group there was one deep infection requiring wound debridement and one superficial wound infection treated conservatively, no wound healing problems in MITPA group was noticed. The preoperative kyphosis improved by 7.80 in MITPA group and 8.10 in open group, however difference was not statistically significant with p value of .43. Conclusions: Presented technique of metastatic thoracic spinal tumors management seems to be an efficient and safe method. It has lower complication rate than open surgery, restores spinal stability and alignment comparably to open technique. However, more observation is necessary, particularly showing how the technique affect the general oncologic treatment.
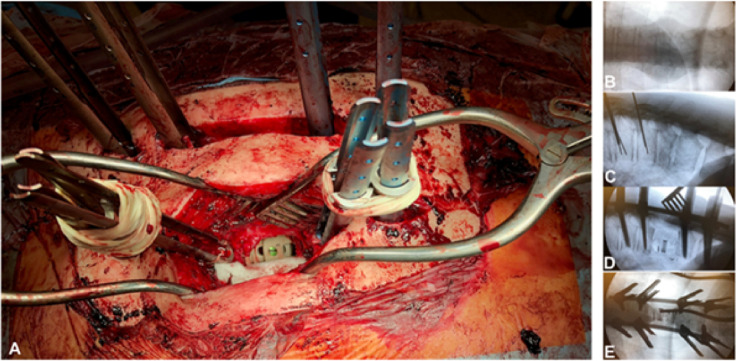
Figure 1. The overview of presented single-stage minimal invasive posterolateral transpedicular approach (MITPA). A - Intraoperative view; shows extenders of percutaneous screws and inserted PEEK intervertebral cage. B,C,D,E - consecutive intraoperative X-rays.
OP19: Degenerative Lumbar Surgery 2
1919
A163: Incremental Clinical Benefit of Adding Layers of Complexity to the Planning and Execution of Adult Spinal Deformity Corrective Surgery
Peter Passias 1 , Katherine Pierce 1 , Waleed Ahmad 1 , Sara Naessig 1 , Virginie Lafage 2 , Renaud Lafage 2 , Gregory Mundis 3 , Jeffrey Gum 4 , Robert Eastlack 5 , Bassel Diebo 6 , Justin Smith 7 , Christopher Ames 8 , Christopher Shaffrey 9 , Douglas Burton 10 , Robert Hart 11 , Frank Schwab 2 , Munish Gupta 12 , Oscar Krol 1 , Lara Passfall 1 , Nicholas Kummer 1 , and Shay Bess 13
1 NYU Langone, Department of Orthopedics Spine Surgery, Manhattan, USA
2 Hospital for Special Surgery, Manhattan, USA
3 University of California, Department of Neurological Surgery, San Diego, USA
4 Norton Leatherman Spine Center, Louisville, USA
5 Division of Orthopaedic Surgery, Scripps Clinic, La Jolla, USA
6 SUNY Downstate Department of Orthopedics, Brooklyn, USA
7 University of Virginia Medical Center, Charlottesville, USA
8 University of California, San Francisco, USA
9 University of Virginia Medical Center, Charlottesville, USA
10 University of Kansas Medical Center,, Kansas City, USA
11 Swedish Neuroscience Institute, Seattle, USA
12 Washington University,, St Louis, USA
13 Denver International Spine Center, Denver, USA
Introduction: For surgical adult spinal deformity (ASD) patients, determining optimal restoration of alignment and spinal shape have been increasingly studied. Temporally, the SRS-Schwab classification system was the first severity categorization system. Next, the age-adjusted alignment was proposed, followed by Roussouly classification, and then a spinal proportionality score to minimize mechanical complications. These additional layers of complexity add to an already technically challenging and high risk case. What hasn’t been determined is the incremental benefit of these. Material and Methods: ASD patients with baseline (BL) and 2-year postoperative(2Y) data included. Patients were classified by the four proposed corrective alignment measures: SRS-Schwab: PT, SVA and PI-LL(0, +, and ++); Age-Adjusted: PT, PI-LL, and SVA-adjusted ideal; Roussouly Type: ‘Match’ or ‘Mismatch’ their theoretical type; Spinal Proportionality: sagittal disproportion score out of 13. Alignment improvement: SRS-Schwab 0 or decrease in severity, Age-Adjusted ideal match, Roussouly theoretical Match, and decrease in proportion. To assess the incremental benefit of layers of complexity, patients were separated into 4 groups: the first layer (1st) solely improving in SRS-Schwab at 2Y, 2nd as Schwab improvement and matching Age-Adjusted, 3rd as the two prior with matching of Roussouly, and 4th improvement in Schwab and proportionality, as well as matching both Age-Adjusted ideals and Roussouly. Comparison was accomplished with means comparison tests and chi-squared analyses. Results: 732 ASD patients (57.5 years, 82.4%F, 27 kg/m2) included. SRS-Schwab BL: PI-LL (++:32.9%), SVA(++: 23%), PT(++:24.6%). At 2Y, 54.9% improved in PT modifier, 71% SVA, 74.3% PI-LL. For Age-Adjusted ideal, 28% met PT ideal, 18.8% PI-LL, and 31.3% SVA. By 2Y, 44.7% matched Roussouly types. At 2Y, 30.8% improved in spine proportion. According to layer of correction complexity groups: 640 (87.4%) met criteria for 1st, 517 (70.6%) 2nd, 176 (24%) 3rd, and 55 (7.5%) 4th. When comparing the incremental adding of the 2nd layer, or age-adjusted ideals to Schwab improvement, complications and HRQLs were similar (P > .05). Addition of Roussouly (3rd) had less mechanical complications and PJK (48.3%), and met MCID for PCS and SRS-Mental (P < .05) more compared to the 2nd tiered. The addition of the spinal proportion score (4th) compared to the 3rd, met MCID for ODI (44.2% vs 3rd: 28.3%, P =.011) and SRS-Appearance (70.6% vs 44.8%, P < .001) more. When assessing baseline components included in the classifications, PI, PT, PI-LL and SVA were smallest in the 3rd group (P < .020). Invasiveness was the greatest in the 4th layer (P < .001). Mechanical complications and PJK occurred to a greater extent in the 1st and 2nd complexity groups (P = .024). According to HRQL follow-up, the 4th layer met MCID more than all other complexity groups for SRS-22 Appearance (P = .002) and ODI (P = .085). Conclusion: Consideration of multiple complex realignment techniques, taking into account deformity severity, age, shape, and spinal proportion, may assist in optimizing patient-reported outcomes following spinal realignment surgery.
1317
A164: Bilateral Radioscopy-Guided Erector Spinae Plane Block for Postoperative Analgesia in Spine Surgery: A Prospective, Randomized Study
Sofia Beltrame 1 , Francisco Fasano 2 , and Pablo Jalon 3
1 Hospital de Clínicas José de San Martin, Buenos Aires, Argentina., Neurosurgery, Ciudad Autónoma, Argentina
2 Hospital de Clínicas José de San Martin, Buenos Aires, Argentina., Ciudad Autónoma de Buenos Aires, Argentina
3 Hospital de Clínicas José de San Martin, Buenos Aires, Argentina., Neurosurgery, Ciudad Autónoma de Buenos Aires, Argentina
Introduction: The erector spinae plane block is a novel technique described recently for neuropathic pain treatment. Although there are a few case reports in the literature about it`s usefulness, it appears to be an effective and simple procedure to manage postoperative pain in spine surgery. It’s the aim of this study to compare two perioperative techniques, the erector spinae plane block with the infiltration of the wound with long lasting local anesthetics, for the management of postoperative wound pain in spinal surgery. Material and Methods: Prospective, single-blind clinical trial, was performed at the Hospital de Clínicas de Buenos Aires, from July 2018 to March 2019. Patients undergoing spinal lumbosacral surgery without fixation were enrolled. 2 perioperative infiltration techniques were compared: pre and postoperative wound infiltration with long lasting analgesics with the interfascial spinae plane erector block. Postoperative results were analyzed in terms of pain relief (VAS), need for opioids, days of immobilization in bed, hours of hospitalization and complications. A P < .05 was considered statistically significant. Results: 40 patients were included. 20 (50%) underwent the standard infiltration technique and 20 (50%) the interfascial spinae plane erector block. The spinae plane erector block was superior in pain wound relief in the first 7 postoperative hours in patients who underwent discectomies or one level decompressions (P = .000). In all the patients with decompressions of 2 or more levels, the new technique proved to be statistically significant superior in all the postoperative variables analyzed: VAS (P = .0004) and number of patients with wound pain after 7 hours of the surgery (P = .000), hours of hospitalization (P = .0007), days of immobilization in bed (P = .0004) and use of opioids (P = .000). Conclusion: The interfascial spinae erector plane is a better technique compare with the standardized infiltration of the wound for postoperative wound pain relief in patients undergoing open spinal surgery. This is the first study that use the blockage with fluoroscopic guideline. It will be the reason for future work to verify its effectiveness in fixation surgeries, minimal invasive spine surgery with anterior or lateral approach, cervicalgia and chronic low back pain management. Keywords: interfascial block, spinal erector muscles, spinal surgery, postoperative pain.
21
A165: Clinical Outcomes in Patients >75-years Undergoing Spine Surgery for Lumbar Degenerative Spine Disease: Impact of Increasing Age and Modified Frailty Index on Surgical Morbidity
Keyur Akbari 1 , Sasidharan M D S 1 , Muralidharan Venkatesan 1 , and Sajan Hegde 1
1 Apollo Hospital, Spine Unit, Chennai, India
Introduction: Surgical procedures are becoming more common in the elderly population, which is likely because of the advancements in surgical technique, improved anesthesia, patient expectations, and increasing longevity. The current study aims to find out the relation between pre operative frail status and post operative complications among patients >75 years undergoing lumbar spine surgery for degenerative disc disease (DDD) using 11 variable modified Frailty Index (mFI). Material and Methods: This is a retrospective study conducted at a tertiary care hospital during the time period 1 May 2017 to 1 May 2019.Consecutive 50 patients > 75 years who met inclusion criteria were included in the study. A match cohort of consecutive 50 patients (age :61-75 years) was also included in the study. The occurrence of perioperative complications and 30 days mortality were analysed in comparison with the modified Frailty Index (mFI) score. Length of hospital stay and 6 months VAS scores for back and leg pain as well as ODI were noted. For the purpose of analysis, we have classified mFI score of 0 has no frail, mFI score of < .27 as pre frail and mFI score of ≥ .27 as frail. ANOVA- test was used to assess statistical significance. P value < 0.05 was considered statistically significant. Results: Demographic metrics included (1) Mean age: 80 years (2) Sex: M:28 F:22. Our study showed that the rates of post operative adverse events increased stepwise as the mFI score increases. In the age group 61-75, as the mFI scored increased from 0 to 0.36, the rate of complications increased from 0 to 100 %. Similarly, for the age group > 75 years, the rate of complications increased from 0 to 100% as the mFI scored increased from 0 to .36. The length of hospital stay with mFI score 0 was 2.5 ± .67 which increased to 8.33 ± 5.77 with mFI score 0.36 in the age group > 75 years. Our study showed that proportion of Clavien Dindo class IV complications (mortality, ICU admissions) was higher in mFI ≥ .27. In our study, there was significant improvement in VAS and ODI scores post surgery in both the age groups and there was no significant difference amongst them despite the mFI being higher in older age group. Superficial infection and delirium were the most common complication in our cohort. Univariate logistic regression analysis showed that age and mFI are associated with any complications in the study group (P < .05) and the association between ASA (American Society of Anesthesiologists) score and any complications was not significant. Conclusion: Our study shows that 11 variable mFI owing to its brevity and practicality is a simple and useful tool for predicting post-op morbidity and mortality in geriatric population undergoing spine surgery for degenerative lumbar spinal condition. Thus, mFI objectively measures risk and might benefit spine surgeons enhancing operative decision making and refining post op care in geriatric population.
456
A166: Efficacy and Feasibility of Percutaneous Transforaminal Endoscopic Surgery (PTES) for Selective Treatment of Responsibility Segments in Multi-Level Lumbar Degenerative Disease
YuTong Gu 1 , Wu Che 1 , Liang Zhang 1 , and Yichao Wang 1
1 Zhongshan Hospital Fudan University, Shanghai, China
Introduction: To evaluate the efficacy and feasibility of selective treatment using PTES for responsibility segments in multi-level (≥2 levels) lumbar degenerative disease including lumbar disc herniation, lateral recess stenosis and intervertebral foraminal stenosis, which needed decompression and fusion for almost each involved level if open surgery was performed. Materials and Methods: From November 2012 to December 2016, 218 patients of multi-level lumbar degenerative disease with unilateral or asymmetric bilateral leg pain or numbness underwent PTES. There were multi-level lumbar disc herniation, lateral recess stenosis or intervertebral foraminal stenosis in MRI or CT. Although the central spinal canal was very narrow in some cases, they should not be diagnosed as lumbar central spinal canal stenosis because there was no symmetric intermittent claudication, and the pain, discomfort, numbness or tiredness during walking relieved by a few minutes of rest occurred in the unilateral leg or more severely in one leg and less in the other, which indicated the symptoms of nerve root compression. In this study, 211 patients were followed for more than 2 years after surgery. There were 64 cases of 2-level, 72 of 3-level, 58 of 4-level and 17 of 5-level. The involved nerve roots and the corresponding responsibility segments were determined according to the location of pain or numbness in the leg. PTES under local anesthesia was performed for the possible responsibility segment. If the patient had obvious relaxation of involved legs during the procedure, which confirmed that the treated segment was exactly responsible for the symptom, it was unnecessary to treat other segments and the operation could be finished. Or other possible responsibility segments should be treated using PTES till the involved legs were relaxed. Results: In 211 cases, 203 patients underwent PTES for 1 segment, 7 cases for 2 segments through one small incision and 1 case for 3 segments. The mean duration of operation was 50.7 ± 9.4 minutes per level. The mean frequency of intraoperative fluoroscopy was 5 (3-11) times per level. The mean blood loss was 5 (2-30) ml. The mean length of incision was 8.1 ± 2.6 mm. The mean stay in the hospital was 3(2-4) days. The patients were followed for an average of 27.4 ± 3.2 months. The VAS score of leg pain significantly dropped from 9 (6-10) before operation to 1(0-3) (P < .001) immediately after the operation and to 0 (0-3) (P < .001) 2 years after operation. However, there were 8 (3.8%) patients with the rebound effect of leg pain 1 week after operation, in which all cases got pain relief during 2 months. At 2 years follow-up, 97.2% (205/211) of the patients showed excellent or good outcomes, 1.9% (4/211) fair and .9% (2/211) poor according to MacNab classification. Two patients underwent reoperation of PTES for recurrence of disc herniation more than 6 months after surgery. No patients had nerve damage and a major complication. Conclusion: The responsibility segments in multi-level lumbar degenerative disease including lumbar disc herniation, lateral recess stenosis and intervertebral foraminal stenosis are selected for surgical treatment using PTES, which is effective, safe and minimally aggressive.
653
A167: Impact of Modic Changes on Functional Outcomes After Microdiscectomy: A Prospective Comparative Cohort Study
Sri Vijay Anand KS 1 , Dinesh Kumarasamy 1 , Shanmuganathan Rajasekaran 1 , Dilip Chand Raja Soundararajan 1 , Ajoy P Shetty 1 , Rishi Kanna 1 , and Pushpa BT 2
1 Ganga Hospital, Department of Spine Surgery, Coimbatore, India
2 Ganga Hospital, Department of Radiology, Coimbatore, India
Introduction: Microdiscectomy is the gold standard procedure performed for lumbar disc herniation with a high success rate (80%). However, in some patients, the preoperative back pain persists after microdiscectomy, and leads to poor functional outcomes after surgery. The presence of pre-operative Modic changes has been correlated to poor outcomes by some authors. This study aims to elucidate the relationship between Modic endplate changes and clinical outcomes after a lumbar microdiscectomy. Methods: A prospective comparative cohort study was performed in consecutive patients undergoing microdiscectomy for lumbar disc herniation (LDH) in a single centre after ethics committee approval. Patients between 18 to 65 years of age with symptomatic single-level disc herniation and failed a trial of conservative management were included. Patients with cauda equina syndrome and significant motor deficits were operated at the earliest and were also included. Patients with prior lumbar surgery, presence of lumbar instability, severe canal stenosis, facetal hypertrophy, high risk for anesthesia, and patients who were lost to follow up during the study period were excluded. Pre-operative clinical and radiological parameters (Presence, location, size and type of Modic changes, Pfirrmann grading, Total endplate score - TEPS) were recorded. The pain was assessed by Numeric pain rating scale (NPRS), and functional assessment by Oswestry Disability Index (ODI). Minimal clinically important difference (MCID) in outcome was calculated for both the groups. Complications related to surgery were studied. Follow-up was done at six weeks, three months, six months and one year. Mac Nab criteria were used to assess patient satisfaction at one year. Statistical analysis was performed to understand the evenness of the distribution of variables across groups and to understand the relationship of Modic changes with functional outcomes. Results: Out of 309 patients, 86 had Modic changes, and 223 had no Modic changes. Both groups had similar back pain (P-value: .07) and functional scores (P-value: .85) pre-operatively. Postoperatively patients with Modic changes had poorer back pain and ODI scores in the third month, sixth month and one year (P-value: .001). However, MCID between the groups were not significant (P-value- .18 for back pain and .58 for ODI scores). Mac Nab criteria at one year were worse in Modic patients (P-value: .001). No difference was noted among Modic types (Type 1 vs Type 2) in the pre-operative and postoperative pain and functional outcomes. Four patients in Modic group (4.7%) and one patient in the non-Modic group (.5%) developed postoperative discitis (p-value: .009). Conclusions: Our study found a negative association between the presence of Modic change in preoperative MRI and postoperative back pain, functional outcomes and patient satisfaction at one year in patients with lumbar disc herniation undergoing microdiscectomy. Modic changes were associated with higher grades of disc degeneration and higher Total endplate scores. However, no difference in clinical outcomes was seen between different types of Modic changes. Our study also found a increased incidence of postoperative discitis and the need for repeat procedures in patients with Modic changes.
1784
A168: Preoperative Community-Based Functional Exercise Training With High-Risk Patients Opting for Lumbar Spinal Fusion: Feasibility and Preliminary Effectiveness
Esther Janssen 1 2 , Ilona Punt 1 3 , Camille Biemans 1 , Lodewijk van Rhijn 1 , Paul Willems 1 , and Nico van Meeteren 4
1 Maastricht University Medical Center+, Department of Orthopedics and Research School Caphri, Maastricht, The Netherlands
2 VieCuri Medical Center, Department of Orthopedics, Venlo, The Netherlands
3 Maastricht University Medical Center+, Department of Surgery and Trauma Surgery, Maastricht, The Netherlands
4 Top Sector Life Sciences and Health (Health∼Holland), the Hague, The Netherlands
Introduction: Preoperative exercise training before major surgery can decrease the risk of adverse postoperative outcomes. This may also apply for patients opting for lumbar spinal fusion (LSF). However, large interindividual differences in risk for negative outcome after LSF exist. Therefore, a focus on deconditioned (a.k.a. “high-risk”) patients is warranted, as these will probably benefit most from preoperative interventions like exercise training. This study aimed to determine the feasibility and preliminary effectiveness of community-based high-intensity functional interval training (HIFIT) program for high-risk patients undergoing LSF. Materials and Methods: In this case control study, a preoperative HIFIT program was implemented into standard care. High-risk patients were identified during a preoperative screening, measuring a patient’s fitness level. A patient was classified as high-risk if they could not achieve 2.5 Wattpeak/kilogram on the Steep Ramp Test (a cycle ergometry test). Feasibility of the HIFIT program was determined by measuring training adherence, training progression, number of adverse events and reached training intensity. A matched Mann-Whitney U test was used to compare trained high-risk patients with untrained high-risk patients on time to functional recovery and length of hospital stay (LoS). In an Interrupted Time Series Analysis (ITSA) the preliminary effectiveness on time to functional recovery and LoS pre- and post-implementation was analyzed. Results: Participation in the HIFIT program was moderate: 47.8% (11/23) of all high-risk patients (after implementation), due logistic reasons (n = 9) or the patient did not want to participate (n = 3). The program was safe and feasible, as no adverse events occurred and only one session was missed (1.35%). Based on the BORG rating of perceived exertion, patients reached on average adequate training intensity in 71% of the supervised sessions. Trained patients increased their preoperative aerobic capacity by 17.6%, and obtained faster time to functional recovery than untrained patients (median 4.5 vs 7.5 (P = .013)). However, this effect was not found for LoS (median 7 vs 8 (P = .575)). The ITSA showed a positive effect of implementation of the HIFIT program on time to functional recovery (relative risk (RR) = .540 (95% Confidence Interval (CI) = .32-.92), P = .023) and but not on LoS (RR = .650 (.41-1.03), P = .070). Conclusion: The HIFIT program is feasible and safe for high-risk patients undergoing LSF. Participation rates of the HIFIT program can be improved by broadening the catchment area of the training network and timely operative planning. The HIFIT program shortened time to functional recovery, but not LoS. This was expected as LoS is largely influenced by logistic and socioeconomic factors. This study can help guide future research endeavors on 1) the effect and 2) the implementation of a preoperative HIFIT program for high-risk patients undergoing LSF.
689
A169: Complication Rates and Onset of Mental Disorders in Patients who Developed Failed Back Surgery Syndrome
Eloise Stanton 1 , Ki-Eun Chang 1 , Blake Formanek 1 , Jeffrey C. Wang 1 , and Zorica Buser 1
1 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
Introduction: Failed back surgery syndrome (FBSS) is a complex and multifaceted condition associated with significant disability and morbidity. FBSS diagnosis is associated with new incidences of further spine complications, as well as mental health disorders. Material and Methods: Data were obtained for patients diagnosed with FBSS from January 2010 to December 2017 from the Mariner insurance database. Patient records were analyzed to determine rates of new lumbar, cervical, and thoracic pathologies, and of new mental health disorders, including tobacco use, depression, anxiety, sleep disorder, bipolar disorder, post-traumatic stress disorder (PTSD), panic disorder, suicidal disorder, and attention-deficit/hyperactivity disorder (ADHD). Rates were determined at 3 months, 6 months, 9 months, and 12 months post-FBSS diagnosis. Results: From 2010 to 2017, 110,097 patients (56% female, 44% male) were diagnosed with FBSS. The most common age group was 70-74 years old. Cumulative incidence rates of new lumbar spine pathology at 3, 6, 9, and 12 months post-FBSS diagnosis were 4.1%, 5.9%, and 7.1%, and 8.0%, respectively. Rates of new cervical spine pathology at 3, 6, 9, and 12 months following post-FBSS diagnosis were 2.9%, 3.9%, and 5.3%, and 6.7%, respectively. Rates of new thoracic spine pathology at 3, 6, 9, and 12 months post-FBSS diagnosis were 1.8%, 3.0%, and 4.0%, and 4.9%, respectively. The rates of new overall mental health disorders within 3, 6, 9, and 12 months post-FBSS diagnosis were 3.4%, 5.8%, 7.8%, and 9.8%, respectively, with rates of anxiety and depression being the highest. The rates of new anxiety diagnosis at 3, 6, 9, and 12 months were 2.3%, 4.0% 5.5%, and 6.8%, respectively. The rates of new depression diagnosis at 3, 6, 9, and 12 months were 2.1% 3.6% 5.0%, and 6.3%, respectively. The rates of new tobacco use at 3, 6, 9, and 12 months were 1.5% 2.6% 3.5%, and 4.2%, respectively. The rates of new sleep disorder at 3, 6, 9, and 12 months were 1.1% 2.0% 2.8%, and 3.5%, respectively. At 12 months, the rate was 0.9% for PTSD, 0.7% for panic disorder, 0.7% for bipolar disorder, 0.5% for suicidal disorder, and 0.2% for ADHD. Conclusion: In our study, patients diagnosed with FBSS experienced subsequent spine-related and mental health complications that continued to increase within the 12 months observational period. The most common spinal complication was lumbar pathology, with its highest incidence rate occurring within the first three months post-FBSS diagnosis. The high rates of both spine pathology and mental health complications observed in this patient population warrants further study into the pathology of FBSS as well as preventative and post-diagnosis treatment paradigm.
1596
A170: Targeting Self-Efficacy More Important Than Dysfunctional Behavioural Cognitions in Patients with Longstanding Chronic Low Back Pain; A Longitudinal Study
Miranda van Hooff 1 2 , Johanna E. Vriezekolk 3 , Robert Jan Kroeze 1 , John O'Dowd 4 , Jacques van Limbeek 5 , and Maarten Spruit 1
1 Sint Maartenskliniek, Orthopedic surgery, Nijmegen, The Netherlands
2 Radboud university medical center, Orthopedic surgery, Nijmegen, The Netherlands
3 Sint Maartenskliniek, Research, Nijmegen, The Netherlands
4 Hampshire hospitals NHS Trust, Basingstoke, United Kingdom
5 Independent epidemiologist, Nijmegen, The Netherlands
Introduction: Multidisciplinary pain management programmes based on cognitive behavioural training principles are recommended to improve daily functioning in patients with chronic low back pain (CLBP). Targeting self-efficacy, i.e. confident in achieving a desired outcome, is suggested to be a more potent determinant for beneficial treatment outcomes than restructuring the patient’s dysfunctional behavioural cognitions (i.e. pain catastrophizing and fear of movement [FoM]), but the evidence is scarce. An evidence-based two-week residential combined physical and psychological (CPP) programme targeting both self-efficacy and dysfunctional behavioural cognitions to improve functional outcome was developed, showed long-term-benefits and was used to evaluate self-efficacy and these behaviourial cognitions. Purpose: To determine whether this CPP programme resulted in post-treatment improvements and maintenance of improvements at one year follow-up in self-efficacy and decreased dysfunctional behavioural cognitions. Subsequently, the unique contribution of self-efficacy to improvement in post-treatment functional status was investigated. Material and Methods: Cohort study including 524 patients with CLBP (727 eligible), aged 18 to 65 years, for whom conservative primary care treatment failed and who were not eligible for an invasive intervention. Primary outcome: functional status (Oswestry Disability Index; minimal clinical important change [MCIC] 10 points). Secondary outcomes: catastrophizing (Pain Catastrophizing Scale; MCIC 5.8 points), FoM (Tampa Scale for Kinesiophobia; MCIC 4.5 points), and self-efficacy (Pain Self-Efficacy Questionnaire; MCIC 5.5 points). Assessments: pre- and post-treatment, 1 and 12-months follow-up (FU). A paired Students’ t-test was used to examine pre- and post-treatment values and post-treatment and 1 year follow-up assessment values. Percentages of patients reaching MCIC at post-treatment were described. Multivariate linear regression techniques were applied to examine the influence of self-efficacy, pain catastrophizing, and fear of movement on the post-treatment functional status. The models' performances were determined by the percentage of variance explained (i.e. Nagelkerke's R 2 ). Results: Participants with incomplete data (12.8%) did not differ from those with complete data (n = 457). 59% were females, mean age 46 (± 9.5) years, mean CLBP-duration 12 (± 10.8) years. All outcomes significantly improved at post-treatment and a slight significant improvement between post-treatment and 12 months FU was observed. Post-treatment relevant improvements in outcomes ranged from 62.4% (FoM) to 68.7% (self-efficacy). After adjustment for baseline values, adding self-efficacy to the basic linear regression model, comprising dysfunctional behavioural cognitions, improved the model explaining post-treatment functional status (basic model R 2 = .49, F(6517) = 83.67, P < .001; final model R 2 = .57, F(8515) = 85.20, P < .001). The relative contribution of self-efficacy, expressed in standardized betas, was 5.67 times higher than catastrophizing and 9.75 times more than FoM. Conclusion: Targeting self-efficacy uniquely contributes to a rapid improvement of functional status in the treatment of selected and motivated patients with longstanding persistent CLBP. Clinically relevant post-treatment improvements and maintenance over time are shown in self-efficacy and dysfunction behavioural cognitions. Targeting patients’ self-efficacy should have a prominent place in treatments for patients with CLBP, such as CPP programmes and (online) self-management programmes.
53
A171: Lordosis Restoration with Midline Minimally Invasive Cortical Trajectory Screws (MiDLF) and Transforaminal Interbody Fusion: A Safe Technique with a Short Stay
Brett Rocos 1 , and Ian Harding 2
1 Toronto Western Hospital, Department of Spine Surgery, Toronto, Canada
2 North Bristol NHS Trust, Department of Orthopaedic Surgery, Bristol, United Kingdom
Introduction: The minimally invasive cortical trajectory screw (MidLIF) technique has been described accompanied with posterolateral interbody fusion (PLIF). We present our 2 years results of a hybrid technique to show that using transforaminal interbody fusion (TLIF) rather than PLIF in conjunction with MidLF is a less invasive and safe technique. Material and Methods: We prospectively identified 25 patients undergoing MidLIF with TLIF from July 2015. The surgical technique was the same for each, with radiological, clinical and patient reported outcome data collected and analysed at 2 years follow up. Results: The cohort showed a mean age of 55 (35-85) years. The length of hospital stay was between 1 and 4 days, with an average of 2.7 days. Post operatively, lordosis across the motion segment fused increased by a mean of 7.3° (0-24), mean pelvic incidence was 53° (31-80°) and pelvic tilt reduced by an average of 3.5° (0-11°). The Oswestry Disability Index improved from 34 pre operatively to 22 post operatively. Visual analogue pain score improved by 5.2 points, from 6 down to 1. One patient showed delayed wound healing. There were no incidences of neurological injury or durotomy. Conclusion: Our data suggests that MidLF with TLIF is both less invasive than traditional techniques and safe. It restores lordosis, requires less exposure and retraction of neural elements than the more widely used PLIF, and shows early discharge and satisfactory medium term patient reported outcomes.
OP20: Basic Science/Cellular Therapy
650
A172: Mesenchymal Stem Cell Secretome: A Potential Anabolic and Immunomodulatory Therapy for Early Intervertebral Disc Degeneration
Sebastian Wangler 1,2 , Amir Kamali 1 , Christina Wapp 1,3 , Karin Wuertz-Kozak 3,4,5 , Sonja Häckel 2 , Claudia Fortes 6 , Lorin Michael Benneker 2 , Lisbet Haglund 7 , R. Geoff Richards 1 , Mauro Alini 1 , Marianna Peroglio 1 , and Sibylle Grad 1,3
1 AO Research Institute Davos, Davos, Switzerland
2 Inselspital, University of Bern, Bern, Switzerland
3 ETH Zürich, Zürich, Switzerland
4 Rochester Institute of Technology, Rochester, USA
5 Schön Clinic Munich, Munich, Germany
6 Functional Genomics Center Zurich, Zurich, Switzerland
7 Mc Gill University, Montreal, Canada
Introduction: Mesenchymal stromal cells (MSCs) have been introduced as promising cell source for intervertebral disc (IVD) regeneration and treatment of low back pain. Besides their multilineage differentiation capacity, MSCs release a wide spectrum of bioactive factors. This secretome holds immunomodulatory and regenerative capacities and has therefore significant therapeutic potential. For clinical translation of secretome-based treatment, characterization of the secretome composition is needed to better understand the induced biological processes and identify the most effective secretomes. The aim of this work was to analyze the secretomes of MSCs stimulated with conditioned medium (CM) from degenerative, traumatic, and healthy IVD tissues. Material and Methods: Degenerative and traumatic human IVD tissue was obtained with written consent from patients undergoing spine surgery. Healthy IVDs were harvested from organ donors after donor and familial consent. IVD tissues were incubated in culture medium for 48h to obtain IVD CM. Human MSCs (n = 12 donors) were isolated from bone marrow aspirates obtained with written consent from patients undergoing spine surgery. MSCs were stimulated with pooled IVD CM (n = 4 for degenerative, traumatic, and healthy IVD groups) for 24 hours. Then, CM was replaced by fresh culture medium to generate MSC secretome during 24 hours. MSCs stimulated with 10 ng/mL IL-1β served as proinflammatory control, and MSCs incubated with culture medium as baseline control. MSC secretomes were analyzed by LC-MS/MS proteomics profiling and cytokine/chemokine immunoassays. Results: Compared to MSC baseline secretome, there were 224 significantly up- or down-regulated proteins following healthy, 179 following traumatic, 223 following degenerative IVD CM, and 160 following IL-1β stimulus. Gene set enrichment analysis revealed different upregulated biological processes depending on the environment the MSCs were exposed to. MSC secretome following stimulation with healthy IVD CM showed upregulation of extracellular structure organization, immune response, and metabolic processes. Degenerative and traumatic IVD CM stimulation revealed common activated processes, including anabolic/catabolic processes, extracellular matrix organization and structure, resulting from upregulated growth factors, enzymes, and enzyme inhibitors. After IL-1β stimulation, immune modulatory and inflammatory processes were enriched. Interestingly, most proinflammatory and immunomodulatory cytokines were undetectable by immunoassay in the secretomes of MSCs incubated with healthy IVD CM. In contrast, the concentration of several chemokines/cytokines like GM-CSF, TNF-α, IL-12p70, IFN- γ, MCP-1, MIP-1β, VEGF, IL-13 and IL-6 was significantly increased in the secretomes of IL-1β primed MSCs (P < .05). In traumatic and degenerative IVD CM, a similar trend was observed for IL-13, IL-8, and IL-6 which were higher than the healthy group (P < .01). Discussion and Conclusion: Stimulation of MSCs with IVD CM induced a more complex MSC secretome, involving more diverse sets of upregulated biological processes, compared to stimulation with IL-1β. Furthermore, the MSCs' response to stimulation with IVD conditioned medium was dependent on the IVD's pathological status. The MSC secretome seemed to match the primary need of the IVD: homeostasis maintenance in the case of healthy IVDs, versus immunomodulation, adjustment of extracellular matrix synthesis, degradation, and (re)organization in the case of traumatic and degenerative IVDs. These findings highlight the significance of MSC preconditioning in the development of tailored and personalized secretome therapies.
1048
A173: Mesenchymal Stem Cell-Seeded High-Density Collagen Gel for Annular Repair: 16 weeks Results from in Vivo Sheep Models
Sertac Kirnaz 1 , Christoph Wipplinger 1 , Stephen Sloan 2 , Franziska Anna Schmidt 1 , Jacob Goldberg 1 , Branden Medary 1 , Fabian Sommer 1 , Lynn McGrath 1 , Lawrence Bonassar 3 , and Roger Härtl 1
1 Weill Cornell Medicine, Department of Neurological Surgery, New York, USA
2 Cornell University, Meinig School of Biomedical Engineering/Sibley School of Mechanical and Aerospace Engineering, College of Engineering, New York, USA
3 Cornell University, Meinig School of Biomedical Engineering/Sibley School of Mechanical and Aerospace Engineering, College of Engineering, Ithaca, USA
Introduction: The objective of the current study was to assess whether performing annular repair in a sheep model of annular injury using high-density collagen (HDC) gel seeded with allogenic mesenchymal stem cells (MSCs) yielded improved histological and radiographic benefits when compared to collagen gel alone. Material and Methods: We performed an anterolateral, retroperitoneal pre-psoas approach to access the IVDs L1-6 in a total of 10 skeletally mature Finn sheep. IVDs were randomized into four groups: 1) intact, 2) injured via 3x10mm box annulotomy and removal of 200 mg of NP, 3) injury and acellular HDC gel patch for AF repair, 4) injury and MSC-seeded HDC gel patch for AF repair. At 16 weeks postoperatively, sheep were sacrificed and underwent post-mortem 3T-MRI scans as well as gross anatomical and histological evaluation. Disc height index (DHI) analysis and modified Pfirrmann grading (PG) were performed on each segment using MR images. Results: Intact control discs showed no degeneration and had an average PG of 1/8 while injured, untreated discs had significant degeneration with an average PG of 5/8. Discs receiving MSC-seeded HDC gel patch for AF repair showed fewer signs of degeneration than the injury only group and equivalent amounts of degeneration as the PG to the acellular HDC gel receiving group. DHI confirmed the trends seen in the PG, where injured discs lost 32% of the intact disc height, the acellular group lost 21% of intact disc height, and the MSC-seeded HDC gel patch preserved 89% of the intact disc height. Conclusion: PG and DHI results demonstrated that HDC gel patch with/without MSCs were able to prevent disc degeneration better than no treatment at all. MSC-seeded HDC gel group was better at preserving DHI than the acellular group.
527
A174: Ex Vivo Priming of Culture-Expanded Mesenchymal Stem Cells (MSCs) with Bone Morphogenetic Protein-2 in a Lumbar Spinal Fusion Model: A Comparative Study of Adipose-Derived and Bone Marrow-Derived MSCs
Alexander Perdomo-Pantoja 1 , Christina Holmes 2 , Ethan Cottrill 1 , Wataru Ishida 1 , Sheng-fu L. Lo 1 , and Timothy F. Witham 1
1 Johns Hopkins University School of Medicine, Neurosurgery - Division of Spine, Baltimore, USA
2 Florida A&M University-Florida State University College of Engineering, Chemical and Biomedical Engineering, Tallahassee, USA
Introduction: In vivo studies have proved that culture-expanded adipose-derived stem cells (ADSCs) enable spinal fusion, especially when combined with bone morphogenetic protein-2 (BMP-2). However, clinical delivery of rhBMP-2 often requires supraphysiological concentrations and has been associated with complications. Therefore, the development of solutions for having successful outcomes of rhBMP-2 without undesired side effects is needed. It has previously reported that a short period of in vitro treatment with BMP-2 prior to transplantation enhanced bone marrow-derived stem cells (BMSC)-mediated bone regeneration in vivo in a calvarial defect model. We hypothesized that this technique might allow spinal fusion using a lower dose of rhBMP-2. The purposes of this study were to examine whether a brief period of in vitro priming with rhBMP-2 can enhance MSC-mediated fusion and to compare the response of adipose-derived and bone marrow-derived cells in a rat model. Materials and Methods: We isolated ADSC and BMSC from the inguinal fat pads and the long bones, respectively, of syngeneic 6-8 weeks old Lewis rats and cultured in vitro. When passage 1 (P1) ADSCs and BMSCs reached 80% confluency, they were primed for 24 hours with 1 ng of rhBMP-2 (Medtronic). After priming, 2x10^6 MSCs (P2) were seeded onto Vitoss (Stryker) bone graft substitute scaffolds for subsequent transplantation. Posterolateral intertransverse spinal fusion surgery at L4-L5 was performed on female Lewis rats divided into 4 experimental groups: [1] Vitoss + rhBMP-2-Primed BMSCsP2; [2] Vitoss + non-primed BMSCsP2; [3] Vitoss + rhBMP-2-Primed ADSCsP2; and, [4] Vitoss + non-primed ADSCsP2. Fusion was assessed eight weeks post-surgery via micro-computed tomography (microCT) imaging, manual palpation, and histology, by two blinded researchers. Manual palpation scoring was estimated as follows: 0 = non-fused; 1 = partial fusion, some motion across operative joint; and, 2 = fused, no motion across the operated joint. MicroCT images were used to measure fusion mass volume (mm^3) and calculate CT fusion score (0 = non-fused; 1 = unilateral fusion; 2 = bilateral fusion). Results: MicroCT imaging data indicate that culture-expanded rhBMP-2-primed ADSCs and BMSCs displayed significantly higher fusion mass volumes than non-primed ADSCsP2 and BMSCsP2, respectively (29.94 mm^3 vs 25.56 mm^3, respectively, P = .04; and 23.8 mm^3 vs 17.79 mm^3, respectively, P = .06). However, fusion mass volumes were not significantly different between primed ADSCsP2 and BMSCsP2. CT fusion scores were not significantly different between primed and non-primed groups. Primed ADSCsP2 also yielded higher manual palpation scores than primed ADSCsP2 (1.9 vs 1.3, respectively, P = .03). Conclusions: In our rat model, rhBMP-2-priming allowed an increased fusion mass volume and manual palpation score among ADSCsP2 compare to non-priming. rhBMP-2 primed BMSCsP2 showed a trend to a higher fusion mass volume compared to non-primed BMSCs. We confirmed our hypothesis that MSC BMP-2-priming enhances spinal fusion in a rat model. Ongoing histological studies will evaluate the characteristics and quality of the new bone formed within the fusion masses.
342
A175: An in Vitro Model of Discogenic Pain. Immunomodulatory Properties of Adipose-Derived Mesenchymal Stem Cells
Marta Esteban Blanco 1 , Elsa Gonzalez Cubero 2 , Jose Garcia Cosamalón 2 , Manuel Fernandez 1 , Maria Elisa Lopez Gonzalez 2 , Maria Luisa Fernandez Gonzalez 2 , and Vega Villar Suárez 2
1 Hospital of Leon, León, Spain
2 University of León, León, Spain
Introduction: Regenerative medicine includes a lot of strategies that comprehend the use of materials and cells generated de novo. The secretome of ASCs (adipose-derived mesenchymal stem cells) released in the medium of cell growth, also called conditioned medium (MC), is being intensively investigated for its therapeutic potential. The main objective was the evaluation of the immunomodulatory properties of the MC obtained from ASCs in discogenic pain. Material and Methods: In this study, it has been developed an in vitro model of discogenic pain in human and rat. Tumor necrosis factor (TNF) was used to induce an inflammatory environment. The ability of the MC to modulate the expression of several pro-inflammatory cytokines and neurotrophins in in vitro model of discogenic pain was analyzed. Results: It was shown the capacity of TNF to induce an inflammatory environment and how the MC is able to modulate the response, showing its paracrine action, both in the proinflammatory genes analyzed and in the neurotrophins that participate in the transmission and in the maintenance of pain. Conclusion: We observed a paracrine action of MC on inflamed cells, carrying out the immunomodulation of pro-inflammatory cytokines and improving their therapeutic efficacy producing an anti-inflammatory effect. These results have a fundamental implication in the treatment of discogenic pain. For this reason, the MC has a great immunomodulatory and neuroprotective capacity. In conclusion, the MC obtained from ASCs presents very promising therapeutic measures for its use in regenerative medicine.
532
A176: Effect of Hypoxia Preconditionated Culture-Expanded Adipose-Derived Mesenchymal Stromal Cells in a Posterolateral Lumbar Spinal Fusion Model
Alexander Perdomo-Pantoja 1 , Christina Holmes 2 , Ethan Cottrill 1 , Wataru Ishida 1 , Sheng-fu L. Lo 1 , and Timothy F. Witham 1
1 Johns Hopkins University School Of Medicine, Neurosurgery - Division of Spine, Baltimore, USA
2 Florida A&M University-Florida State University College of Engineering, Chemical and Biomedical Engineering, Tallahassee, USA
Introduction: Implantation of adipose-derived mesenchymal stromal cells (ASCs) has become a promising strategy for bone regeneration therapies and an attractive alternative to bone marrow-derived mesenchymal stromal cells (BMSCs), particularly in elderly patients. Nevertheless, limited cell survival after implantation due to the in vivo hypoxic environment has been one of the main barriers of the effectiveness of this approach. Hypoxia Inducible Factor-1α (HIF-1α) is a critical mediator of the adaptive cell response to hypoxia and plays an essential role in angiogenic-osteogenic coupling during bone regeneration.1 Dimethyloxaloylglycine (DMOG) treatment has shown to stabilize cellular expression of HIF-1α in cells, as well as enhances osteogenic and angiogenic capacity of MSCs.2 We aimed to demonstrate that hypoxia preconditioning of culture-expanded ASCs before implantation prolongs improve spinal fusion by therapeutically targeting both osteogenesis and vascularization in a rat model. Materials and Methods: ASCs were isolated from the inguinal fat pads of syngeneic 6-8 weeks old Lewis rats and culture-expanded in vitro. When passage 1 (P1) ASCs reached approximately 80% confluency they were preconditioned for 24 hours with 1 ng of DMOG (Fisher Scientific). After preconditioning, 2 × 10^6 ASCs Passage 2 (P2) were seeded onto Vitoss (Stryker) bone graft substitute scaffolds for subsequent transplantation. Posterolateral spinal fusion surgery at L4-L5 was performed on female Lewis rats divided into two experimental groups: [1] Vitoss + DMOG-preconditioned ASCP2s; and, [2] Vitoss + non-preconditioned ASCP2s. Fusion was assessed eight weeks post-surgery via manual palpation, micro-computed tomography (µCT) imaging, and histology. Manual palpation scoring was performed to evaluate the motion across the operated joint by blinded researchers as follows: 0 = non-fused; 1 = partial fusion, some motion across operative joint; and, 2 = fused, no motion across the operated joint. µCT images were used to estimate fusion mass volume (mm^3) and determine CT fusion score (0 = non-fused; 1 = unilateral fusion; 2 = bilateral fusion). Histology was used to assess bone quality and neovascularization within the fusion masses. Results: Preliminary µCT imaging data suggest that DMOG-preconditioned ASCP2 group yielded significantly higher fusion mass volumes than non-preconditioned ASCP2 group (23.49 mm^3 vs 15.39 mm^3, respectively, P =.001). DMOG-preconditioned ASCP2 group showed a trend towards higher rates of µCT fusion and manual palpation scores compared to the non-preconditioned ASCP2 group (1.16 vs 0.50, respectively, P =.06; and 1.25 vs 0.66, respectively, P>.05). Conclusions: In our rat posterolateral fusion model, hypoxia preconditioned culture-expanded ASCs exhibited significant increased fusion mass volumes compared to non-preconditioned ASCs. In addition, µCT fusion scores and manual palpation scores showed to be higher in the group pretreated with DMOG. Ongoing histological studies are evaluating the characteristics, quality, and vasculature of the new bone formed within the fusion masses.
950
A177: Characterisation of Acute Peripheral Inflammatory Responses Identifies Distinct Phenotypes of Circulating Monocytes Following Spinal Cord Injury
Ryan Doig 1 , Sandra Jenkner 1 , Aleesha Searle 1 , Jillian Clark 2 , Brian Freeman 2 , and Stan Gronthos 3
1 South Australian Health and Medical Research Institute (SAHMRI), Neil Sachse Centre for Spinal Cord Research, Adelaide, Australia
2 Royal Adelaide Hospital, Spinal Services, Adelaide, Australia
3 University of Adelaide, Adelaide Medical School, Adelaide, Australia
Introduction: Spinal cord injury (SCI) elicits a cellular inflammatory immune response to protect the host. This acute cellular inflammatory has contrasting characterising: contributing to helpful clearance and repair, but can also exacerbate CNS tissue damage. In addition to resident inflammatory cells, it is well recognised that infiltrating immune cells are active participants in the host response to injury and may exacerbate or counter excess inflammation or promote tissue healing. The next step was to realise that infiltrating inflammatory immune cells may modulate the survival, distribution or differentiation of engrafted pluripotent stem cells. It is important to try to understand these peripheral immunomodulatory events, and the context in which they occur because of the urgent need for viable therapeutics. The aims of this study were: i) to examine the temporal profile of the peripheral blood mononuclear cell (PBMC) response to acute SCI and ii) characterise phenotypic and pathophysiological properties of peripheral immune cells. Material and Methods: In brief, animals received a moderate- severe T10 contusion (200kDyne) injury. At 24 hours, 48 hours, 72 hours, 7, 14, and 28 days after surgery, PBMC were isolated from whole blood samples of Normal (n = 6/group), Laminectomy only (Sham, n = 6/group)) and SCI animals (n = 6/group). PBMCs were isolated from whole blood samples for 9-colour flow cytometry coupled with gated fluorescent activated cell sorting. Isolated hematopoietic cells (CD45) were sorted into T lymphocytes (CD3), B Cells (CD45R), NK Cells (CD161), and monocyte subsets (CD43Lo/CD11bHi and CD43Hi/CD11bInt-Lo). Results: This study examined the temporal profile of T lymphocytes, B cells, NK cells and monocyte subsets represented in peripheral blood from 1-28 days post-injury. Counterintuitive to our hypothesis, we did not detect a significant effect of time on the relative proportion of B, NK cell or monocyte subsets. However, there appeared to be a proportional shift in T lymphocyte subsets; with bi-phasic shifts between the proportion of regulatory and cytotoxic T cells. Interestingly, we identified early shifts in a third sub-population of immature CD45+ monocytes; CD43int/CD11bLo/SSC-A cells during the first 48 hours post-injury with a decrease of the proportion of CD43int/CD11bLo/SSC-A cells in SCI vs SHAM animals, and corresponding increase in CD43Lo/CD11bHi and infiltrating immature M1 CD43Hi/CD11bInt-Lo monocytes. Conclusion: This study characterised peripheral blood monocyte subsets of differing granularity and cell-surface antigen expression in the context acute SCI. Our data point towards the potential for immune cell sub-sets of peripheral origin to participate in the CNS inflammatory response, or modulate the fate of pluripotent stem cells in vitro or in vivo. The findings provide a precedent for examining the immunomodulatory effects of peripheral PBMC subsets on donor stem cells, which may have important implications for regenerative medicine.
1281
A178: What is the Mesenchymal Stem Cell Concentration in the Vertebral Body Compared to the Iliac Crest in Patients Undergoing Posterior Instrumentation?
Robin McManus 1 , Ciara Murphy 2 , Henry Turner 1 , and Patrick Kiely 1
1 Children's Health Ireland at Crumlin, Dublin, Ireland
2 Royal College of Surgeons in Ireland, Dublin, Ireland
Introduction: Spinal fusion is a procedure that is indicated in the management of multiple spinal pathologies. Pseudoarthrosis is a condition where fusion between two or more vertebrae has not been achieved as demonstrated by the presence of intervertebral motion. Following lumbar spine surgery there is up to a thirty five percent chance of the development of pseudoarthrosis. Revision surgery may be required. In order to reduce the chances of fusion failure, the spine is fused using tissue harvested from the patient, a donor or synthetic graft. The iliac crest, (IC), serves as the gold standard for bone graft and bone marrow harvesting, however it can be associated with complications. The vertebral body, (VB), is known to be a good source of bone marrow cells. During spinal procedures the VB is routinely used for instrumentation either by an anterior or posterior approach. The principle aim of this study is to review the literature to determine can the VB serve as a suitable source of mesenchymal stem cells (MSC’s) in patients who require spinal fusion. Methods: A database search was conducted to identify relevant studies for inclusion. Databases searched include Medline, Embase, CINAHL and The Cochrane Library. Search terms were identified by breaking down the question. The only limitation applied to the database search was inclusion of studies published in the English language only. Preferred Reporting Items for Systematic Reviews and Meta-Analyses was used to guide the review. Of the 1032 studies identified following the database search, five of these studies were included in this review paper. Quality appraisal of each of the included studies was completed using the evidence based librarianship checklist. Results: Four of the five included studies scored an overall low validity score of <75%. One article did achieved overall high validity by scoring >75%. However, all studies were included in this review paper in an effort to provide an accurate representation of all of the available literature. Two of five studies reported a higher concentration of progenitor cells in the vertebral body compared to the iliac crest. Two of five studies reported comparable concentrations of progenitor cells in the vertebral body compared to the iliac crest. One study reported a lower concentration of progenitor cells in the vertebral body compared to the iliac crest. Conclusion: There is a paucity of literature in this field and further studies need to be conducted. Based on the included studies it can be concluded that the VB serves as a suitable reservoir for MSC harvest.
606
A179: Exploring the Core matrisome Profile of Fetal Intervertebral Discs in Search of Molecular Targets of Therapeutic Potential
Shanmuganathan Rajasekaran 1 , Chitraa Tangavel 2 , Niek Djuric 3 , Dilip Chand Raja Soundararajan 1 , Sharon Miracle Nayagam 2 , Monica Steffi Matchado 2 , and Sri Vijay Anand KS 1
1 Ganga Medical Centre and Hospitals Pvt Ltd, Spine Surgery, Coimbatore, India
2 Ganga Research Centre, Biotechnology, Coimbatore, India
3 Leiden University Medical Centre, Neurosurgery, Leiden, The Netherlands
Introduction: Intervertebral disc degeneration is accompanied by a loss of Extra-cellular matrix (ECM) content due to an imbalance in anabolic and catabolic pathways. Identifying ECM proteins with anabolic and/or regenerative potential could be the key to developing regenerative therapies. Since human fetal discs grow and develop very rapidly, studying these discs may provide valuable insights on proteins with regenerative potential. The primary aim of this study was to explore fetal intervertebral disc and identify molecules with regenerative potential. Materials and Methods: LC-MS/MC analysis of 9 fetal and 7 healthy adult (age 22-79) nucleus pulposus (NP) was performed to profile the core matrisome. Protein expression was compared between the two groups and a pathway analysis was performed with all proteins that were uniquely expressed or significantly upregulated in fetus, or >2 fold upregulated if the protein was expressed in <3 samples fetus samples. Relevant pathways for ECM assembly were selected and the respective proteins were discussed. Results: Of the 64-expressed core matrisomal proteins in fetus, 22 were unique in > 1 sample,7 were significantly higher expressed compared to healthy adult NP’s, and 4 proteins >2 fold higher. Pathway analysis with these 33 proteins revealed that 20 proteins were integrated in ECM assembly and growth pathways: Fibromodulin, Biglycan, Heparan Sulfate Proteoglycan 2, Chondroitin Sulfate Proteoglycan 4 were involved in Glycosaminoglycan metabolism. In addition, Fibromodulin, Biglycan, procollagen C-endopeptidase enhancer (PCOLCE) and Collagen- type 1a1, 1a2, 6a1,6a3,11a1,11a2, 12a1, 14a1 and 15a1 were involved in Collagen fibril formation, biosynthesis and organization. Regarding the growth pathways: Thrombospondin 1,2,3 and 4, Tenascin C and Collagen- type 1a1, 1a2, 6a1,6a3,11a1,11a2 were involved in ‘PIK3-Akt signaling’ and Matrilin-3 and tenascin C in ‘IGF transport and uptake’. Conclusion: The consistency of the human fetal NP differs greatly from that of a healthy adult. The Core-matrisome of human fetal discs is of great potential for developing future regenerative therapies.
1874
A180: Analysis of 3D-Printed Titanium Porous Scaffolds Using Mesenchymal Stem Cells
Jessica Dorilio 1 , Nicole Utah 1 , Christina Dowe 1 , Antonio Brecevich 1 , Fedan Avrumova 1 , Frank Cammisa 1 , and Celeste Abjornson 1
1 Hospital for Special Surgery, New York, USA
Background: With a reported implant failure rate of 35% in anterior cervical discectomy and fusion (ACDF) procedures, implant design has become more precise. Failed fusion is caused by a number of factors, one of which is the inability to osseointegrate with the surrounding bone tissue. The cellular response to the environment created by an implant is critical when determining short and long-term outcomes. Titanium has been the gold standard biomaterial in implant design because of its hydrophilicity. This fosters an environment that allows for successful cellular attachment and expression of protein factors that drive osteoblast differentiation, such as BMP-2 and osteocalcin. When coupled with implant features, such as porosity, the long-term favorability of titanium is enhanced. Porosity can alleviate the biomechanical drawbacks of titanium, which is its high elastic modulus. A porous structure allows for bone in-growth, on-growth, and through-growth, as well as, vascularization, promoting successful osseointegration. The purpose of the study was to evaluate the mesenchymal stem cell response based on varying levels of porosity. This includes cellular attachment, viability, and protein expression. Materials & Methods: Scaffolds were comprised of a 3D-printed titanium alloy of the FLX lattice in various porosities and sizes, 40, 50, 60, 70, 80% (Centinel Spine, West Chester, PA). The hMSCs were seeded onto replicas of each sample at a density of 25,000 cells/mL in growth media, and were cultured for 3, 7, and 28 days. Using a cytotoxicity assay with a double stain mechanism, live cells were stained. For each sample, images were capturerd on the florescence microscope of the section with the highest live:dead ratio. Cellular attachment, as well as cellular extensions such as filipodia, was visualized on scanning electron microscopy (SEM). Lastly, to assess protein expression driving osteoblast differentiation, individual ELISA assays and a multiplex assay were utilized. Results: As exhibited through scanning electron microscopy, all samples displayed similar stem cell attachment. Fluorescent microscopy showed that viability showed preference to both longer cultures (28 days), and the 70% porous sample, which showed greater live:dead ratio among samples. Total protein concentration at the later time points were greatest after a culture on the 60% porous sample. However, all samples displayed a higher concentration of osteogenic factors BMP-2 and osteocalcin than the interleukins.. Conclusion: Given the many factors that can diminish the success rate of spinal fusion, it is beneficial to mitigate the risk through the optimization of implant design. Microporosity is a feature that can enhance the biocompatibility of titanium implants. As nanotexturing was kept constant between samples, stem cell attachment was similar. However, cellular viability demonstrated that increasingly longer cultures produce the environment sufficient for proliferation and survival of cells. Additionally, the microenvironment promoted by the 70% porous sample enhanced viability. Overall, all samples showed increased expression of factors that encourage osteoblast differentiation and decreased expression of inflammatory cytokines that promote the formation of fibrous tissue, potentially indicating a lower risk of implant failure. Our study has shown that titanium surfaces are better optimized at 60-70% porous size (300-700 micron).
OP21: Cervical Trauma and Spinal Cord Injury
518
A181: Early Versus Late Surgical Decompression for Acute Spinal Cord Injury: A Meta-Analysis of Individual Patient Data
Jetan Badhiwala 1 , Jefferson Wilson 1 , Christopher Witiw 1 , James Harrop 2 , Alexander Vaccaro 3 , Bizhan Aarabi 4 , Robert Grossman 5 , Fred Geisler 6 ,and Michael Fehlings 1
1 University of Toronto, Division of Neurosurgery, Department of Surgery, Toronto, Canada
2 Thomas Jefferson University, Department of Neurological Surgery, Philadelphia, USA
3 Thomas Jefferson University, Rothman Orthopaedic Institute, Philadelphia, Canada
4 University of Maryland School of Medicine, Department of Neurosurgery, Baltimore, USA
5 Houston Methodist Hospital, Department of Neurosurgery, Houston, USA, 6 Independent Consultant, Chicago, USA
Background: Decompressive surgery for acute traumatic spinal cord injury (SCI) involves the mechanical removal of injured tissue (e.g., bone, disc) exerting pressure on the spinal cord. The influence of the timing of surgical decompression for acute SCI remains unclear and there is substantial variability in current clinical practice. Materials and Methods: Patients who underwent decompressive surgery for acute SCI were identified from four independent prospective, multi-center data sources (NACTN SCI Registry; STASCIS; Sygen Trial; NASCIS III). Patients were stratified into early (< 24 hrs) and late (≥ 24 hrs) decompression groups. Neurological outcomes were assessed by American Spinal Injury Association (ASIA) examination. The primary endpoint was change in total motor score at 1 year. Secondary endpoints included ASIA Impairment Scale (AIS) grade and change in upper extremity motor, lower extremity motor, light touch, and pin prick scores at 1 year. One-stage meta-analyses were performed by hierarchical mixed-effects regression adjusting for baseline score, age, injury mechanism, AIS grade, level of injury, and steroids. Effect sizes were summarized by mean difference (MD) for sensorimotor scores and common odds ratio (cOR) for AIS grade, along with corresponding 95% confidence intervals (CIs). As a secondary analysis, Δtotal motor score was regressed against time to surgical decompression (hours) as a continuous variable using a restricted cubic spline and adjusting for the same covariates. Results: The study cohort consisted of 1,548 patients. Mean age was 39.1 years. Patients who underwent early surgical decompression (N = 528) experienced greater recovery than the late surgery group (N = 1,020) at 1 year for total motor score (MD 4.0, 95% CI 1.7-6.3, P = .001), light touch score (MD 4.3, 95% CI 1.6-7.0, P = .002), and pin prick score (MD 4.0, 95% CI 1.5-6.6, P = .002). There was a shift toward better AIS grades, indicating less severe impairment, at 1 year in favor of early decompression (cOR 1.48, 95% CI 1.16-1.89, P = .002). In patients with cervical SCI, early decompressive surgery resulted in disproportionate motor score improvement in the upper (MD 2.2, P < 0.001) over lower limbs (MD 1.3, P = .115). When time to surgical decompression was modeled as a continuous variable, there was a steep decline in Δtotal motor score with increasing time over the first 24 to 36 hours after injury; thereafter, recovery encountered a ‘floor’. This non-linear relationship was statistically significant (P <.001). Conclusion: Surgical decompression within 24 hours of acute SCI improves sensorimotor recovery. The first 24 to 36 hours after injury represent a critical window during which earlier decompressive surgery may augment neurological outcomes. Thereafter, the benefit of timeliness may be lost likely because of irreversible tissue injury. These findings have important implications for guideline recommendations, clinical practice, and healthcare policy, which may need to be revised to support and facilitate the expeditious delivery of surgical care for acute SCI.
615
A182: The Subaxial Cervical AO Spine Injury Score
Jose Canseco 1 , Gregory Schroeder 1 , Taylor Paziuk 1 , Brian Karamian 1 , Frank Kandziora 2 , Emiliano Vialle 3 , Cumhur Oner 4 , Marcel Dvorak 5 , Klaus Schnake 6 , Jens Chapman 7 , Lorin Michael Benneker 8 , Shanmuganathan Rajasekaran 9 , AO Spine Cervical Classification Validation Group 10 , Christopher Kepler 1 , and Alexander Vaccaro 1
1 Rothman Orthopaedic institute, Philadelphia, USA
2 3 Center for Spine Surgery and Neurotraumatology, BG Unfallklinik Frankfurt am Main, Frankfurt, Germany
3 Department of Orthopaedics, Catholic University of Parana, Curitiba, Brazil
4 University Medical Center, Utrecht, Utrecht, The Netherlands
5 Department of Orthopaedics, Vancouver General Hospital, Vancouver, Canada
6 Center for Spinal Surgery, Malteser Waldkrankenhaus St. Marien, Erlangen, Germany
7 Swedish Neuroscience Institute, Swedish Medical Center, Seattle, USA
8 Spine Service, Orthopaedic Department, Sonnenhofspital, Bern, Switzerland
9 Department of Orthopaedics, Trauma and Spine Surgery, Ganga Hospital, Coimbatore, India
10 AO Foundation, Davos, Switzerland
Introduction: The purpose of an effective classification system is to provide distinct and clinically relevant morphological descriptions of injury patterns in a manner that helps guide treatment. The AO Spine Subaxial Cervical Spine Injury Classification System (SCICS) is a compressive classification system has demonstrated adequate inter- and intra-observer reliability in classifying subaxial cervical spine injuries. Establishing a scoring system based on the relative injury severity associated with the classification’s subgroups is the next step in establishing treatment guidelines. By generating a scoring system based on a consensus of relative injury severity, the purpose of this study is to develop an injury score for the AO Spine Subaxial Cervical Spine Injury Classification System. Methods: A survey was sent to the members of the AO Spine Cervical Classification Validation Group composed of spine surgeons from six different world regions (North America, South America, Europe, Africa, Asia, and the Middle East). For each of the subgroups of the AO Spine SCICS, respondents graded each variable of the classification system for severity on a scale from 0 to 100. Each classification subgroup was ranked hierarchically based on relative injury severity, and with limited input from the AO Spine Trauma Knowledge Forum, the Subaxial Cervical AO Spine Injury Score was developed. Results: An A0 injury was assigned an injury score of 0, A1 a score of 1, and A2 a score of 2. Given the significant increase in severity, A3 was given a score of 4. Based on equal severity assessment, A4 and B1 were both assigned a score of 5. B2 and B3 injuries were assigned a score of 6. Unstable C-type injuries were given a score of 7. Stable F1 injuries were assigned a score of 2, with a 2-point increase for F2 injuries. Likewise, F3 injuries received a score of 5, whereas more unstable F4 injuries a score of 7. Neurologic status severity rating scores increased stepwise, with scores of 0 for N0, 1 for N1, and 2 for N2. Consistent with the Thoracolumbar AO Spine Injury Score, N3 (incomplete) and N4 (complete) injuries were given an score of 4. Finally, case-specific modifiers M1 (PLC injury) received a score of 1, while M2 (critical disc herniation) and M3 (spine stiffening disease) received a score of 4. Conclusions: The Subaxial Cervical AO Spine Injury Score is an easy-to-use metric that can help develop a surgical algorithm to supplement the AO Spine Subaxial Cervical Spine Injury Classification System.
1233
A183: Spinal Cord Signal Change on Magnetic Resonance Imaging Predicts Worse Clinical in-and Outpatient Outcomes in Patients with Spinal Cord Injury: A Prospective Multicenter Study in 459 patients
Thorsten Jentzsch 1 2 , Muhammad Akbar 1 , Brett Rocos 1 , Fan Jiang 1 , Jetan H. Badhiwala 1 , David Cadotte 3 , Jefferson Wilson 4 , Robert Grossman 5 , Bizhan Aarabi 6 , James Harrop 7 , and Michael Fehlings 1
1 Toronto Western Hospital, University Health Network, University of Zurich, Toronto, Canada
2 Balgrist University Hospital, University of Zurich, Zurich, Switzerland
3 Hotchkiss Brain Institute, University of Calgary, Calgary, Canada
4 St. Michael’s Hospital, University Health Network; University of Toronto, Toronto, Canada
5 Houston Methodist Hospital, Houston, USA
6 University of Maryland Medical Center and R Adams Cowley Shock Trauma Center, Baltimore, Canada
7 Thomas Jefferson University, Philadelphia, Canada
Introduction: Spinal cord injury (SCI) is a devastating event and prognostic factors for clinical outcome serve an important role in patient management and education. There is a lack of evidence regarding magnetic resonance imaging (MRI) and clinical outcome in the setting of SCI. This study investigated if MRI signal changes predict the clinical course of disease in patients with SCI. Materials and methods: This is an ancillary to the prospective North American Clinical Trials Network (NACTN) registry. Patients were enrolled from 2005-2017. MRI within 72 hours of injury and a minimum follow-up of one year were available for 459 patients. Patients with American Spinal Injury Association impairment scale (AIS) E were excluded. Patients were grouped into those with (n = 354) vs without (n = 105) cord signal change. The primary outcome was any adverse event. Secondary outcomes were the AIS at baseline and final follow-up, length of hospital stay, and mortality. The chi-squared, Wilcoxon rank sum tests and a logistic regression model (adjusting for age and gender) were used. Results: Patients with intrinsic cord signal change were younger (46.0 (interquartile range (IQR) 29.0 vs 50.0 (IQR 20.5) years, P = .039). There were no significant differences in the other baseline variables, gender, body mass index, comorbidities, and injury location. There were more complications in patients with spinal cord signal change (230 (65.0%) vs 47 (44.8%), P < .001). These differences remained significant in a logistic regression model (odds ratio (OR) = 2.01 (95% confidence interval (CI) 1.29-3.32), P = .003). Patients were less likely to be in the AIS D category with SC signal change at baseline (OR = .45 (95% CI .28-.73), P = .001) and final follow-up (OR = 36 (95% CI .16 - .82), P = .015). The length of stay was longer in patients with SC signal change (13.0 (IQR 17.0) vs 11.0 (IQR 14.0), P = .049). There was no difference between groups in mortality (11 (3.2%) vs 4 (3.9%), P = .767). Conclusions: MRI signal change predicts the clinical course of disease in patients with SCI. If present, patients are more likely to have an inferior baseline clinical presentation as well as in- and outpatient clinical outcome. Therefore, patients with SC signal change may benefit from earlier and more aggressive treatment strategies and need to be educated about an unfavorable prognosis. Keywords: Spinal cord injuries, magnetic resonance imaging, MRI, tomography, neurology, paralysis, walking, outcome
Acknowledgements
The NACTN SCI Registry is supported by the US ARMY MEDICAL RESEARCH ACQUISITION ACTIVITY (USAMRAA) under Contract No. W81XWH-16-C-0031 and earlier Department of Defense Awards.
1555
A184: How Does Surgical Approach Affect Outcomes Following Cervical Trauma in the Elderly?
Catherine Carlile 1 , Jacob Schultz 2 , Andrew Rees 2 , Amir Abtahi 1 , and Byron Stephens 1
1 Vanderbilt University Medical Center, Nashville, USA
2 Vanderbilt University School of Medicine, Nashville, USA
Introduction: Both anterior - anterior cervical discectomy and fusion (ACDF) and posterior - posterior cervical fusion (PCF)] approaches are commonly used to treat traumatic injuries of the cervical spine. Some evidence exists to suggest that ACDF may be superior in younger patients with studies demonstrating shorter hospital stays and fewer complications. However, there is a paucity of evidence comparing outcomes between these surgical approaches in elderly patients with cervical spine injuries. With a rapidly aging population in the USA and the corresponding increase in spine trauma in this population, this topic is of increasing importance. Outcome studies comparing ACDF to PCF in the elderly are important to inform surgical management of elderly patients with spinal injury. This study aims to determine if there are outcome differences of ACDF versus PCF in elderly patients - particularly with regard to complication rates and hospital admission length. Methods: Patient demographics, comorbidities, and long-term outcomes were collected into a deidentified institutional spine trauma database. Elderly patients (65+) were age-matched and divided into ACDF and PCF groups. There were no statistically significant difference in the ISS score, injury pattern, or rate of concurrent polytrauma, or comorbidities between these groups (P > .05). Surgical and medical morbidity variables that were evaluated include surgical site and hospital acquired infections, DVT, PE, stroke, pneumonia, and myocardial infarction. A combination of Pearson and t-tests were used to assess correlation between approach and preexisting comorbidities as well as correlations between approach and outcomes (estimated blood loss during surgery, hospital stay length, death during admission, and time to death). Results: A total of 40 patients, 19 anterior and 21 posterior, were included with an average age of 69.8 and 76.6, respectively. There was a significant difference in average age between these cohorts (P < .001). Of intraoperative variables, there was a significantly greater average blood loss (P <. 01) in the PCF group. However, there was no correlation between approach and length of stay (P = .97), medical (P = .58) or surgical (P = .30) complication, in- hospital mortality (P = .52), or death within one year (P = .79). Conclusion: In this cohort, there was no significant difference in morbidity or mortality between ACDF and PCF. Estimated blood loss was found to be significantly lower with patients who underwent ACDF, but this did not translate to a difference in complications or hospital stay. Therefore, our data suggests that ACDF remains a safe option in the appropriate elderly patient with fractures amenable to anterior fixation. However, the benefits of ACDF over PCF may not be as pronounced as in younger populations. Future study, including larger multi-center studies focusing on patient reported outcomes may help elucidate additional differences between the two approaches in this population.
700
A185: Subaxial Spine Arthrodesis in Patients With Spine Fractures and Facet Dislocations: Is Magnetic Resonance Imaging Required to Determine the Optimal Surgical Approach?
Guilherme Finger 1 , Andre Martins de Lima Cecchini 1 , Ericson Sfreddo 1 , Felipe Martins de Lima Cecchini 1 , Otavio Garcia Martins 2 , Tiago Paczko Bozko Cecchini 3 , Alisson R. Teles 4 , and Asdrubal Falavigna 5
1 Cristo Redentor Hospital, Neurosurgery Spine, Porto Alegre, Brazil
2 Federal University of Pelotas,, Pelotas, Brazil
3 Brazilian Lutheran University, Canoas, Brazil
4 McGill University, McGill Scoliosis and Spine Group, Montreal, Canada
5 Caxias do Sul University, Neurosurgery Spine, Caxias do Sul, Brazil
Introduction: The medical literature suggests that facet dislocations (FDs) must be managed surgically, even in the absence of spinal cord injury. In fact, there is no standard guideline for managing FD cases and whether magnetic resonance imaging (MRI) should be utilized for optimizing treatment planning. Methods: Fifteen cases of FD were evaluated twice by nine spine surgeons. The first assessment included computed tomography (CT) images only. Secondarily, original CT studies were supplemented with MRI. In each case, the participating surgeon had to acknowledge whether and what surgical treatment they would offer. Data for the two responses from all nine surgeons were then compared. Results: Based on CT images alone, there was no consensus regarding treatment choices in 13 cases, and a trend toward consensus in just two instances (κ = .01). When MRI scans were added to CT studies, among the 15 cases evaluated, 10 cases demonstrated a trend toward consensus, and in 1 case consensus was achieved. The Kappa interpersonal agreement based on MRI was .13. The analysis of the answers by each contributor in each case demonstrated that in 58.51% of cases the surgical treatment options were changed when analyzed by CT + MRI, in comparison to the options indicated based on CT alone. Conclusion: It appears that obtaining an MRI in addition to a CT before spine surgery for FD is essential mandatory, as it changed the treatment option in nearly 60% of cases.
623
A186: Establishing the Injury Severity of Subaxial Cervical Spine Trauma: Validating the Hierarchical Nature of the AO Spine Subaxial Cervical Spine Injury Classification System
Gregory Schroeder 1 , Jose Canseco 1 , Parthik Patel 1 , Srikanth Divi 1 , Brian Karamian 1 , Frank Kandziora 2 , Emiliano Vialle 3 , Cumhur Oner 4 , Klaus Schnake 5 , Marcel Dvorak 6 , Jens Chapman 7 , Lorin Michael Benneker 8 , Shanmuganathan Rajasekaran 9 , AO Spine Cervical Classification Validation Group 10 , Christopher Kepler 1 , and Alexander Vaccaro 1
1 Rothman Orthopaedic institute, Philadelphia, USA
2 Center for Spine Surgery and Neurotraumatology, BG Unfallklinik Frankfurt am Main, Frankfurt, Germany
3 Cajuru Hospital, Catholic University of Parana, Curitiba, Brazil
4 14 University Medical Center, Utrecht, The Netherlands
5 Center for Spinal Surgery, Malteser Waldkrankenhaus St. Marien, Erlangen, Germany
6 Department of Orthopaedics, Vancouver General Hospital, Vancouver, Canada
7 Swedish Neuroscience Institute, Swedish Medical Center, Seattle, USA
8 Spine Service, Orthopaedic Department, Sonnenhofspital, Bern, Switzerland
9 Department of Orthopaedics, Trauma and Spine Surgery, Ganga Hospital, Coimbatore, India
10 AO Foundation, Davos, Switzerland
Introduction: Classification systems should be simple and reproducible, yet be able to transmit comprehensive information including diagnosis and prognosis to help guide clinical management. Previous subaxial cervical spine injury classifications have been limited by subpar interobserver reliability and clinical applicability. In an attempt to create a universally validated scheme with prognostic value, AO Spine established a subaxial cervical spine injury classification involving four elements: (1) injury morphology, (2) facet injury involvement, (3) neurologic status, and (4) case-specific modifiers. The purpose of this study is to validate the AO Spine Subaxial Cervical Spine Injury Classification System by examining the perceived injury severity by surgeons around the world with various practice experience. Methods: A survey was sent to 272 AO Spine members across six different geographic regions (North America, South America, Europe, Africa, Asia, and the Middle East) with various years of practice experience. Respondents graded the severity of each variable of the classification system on a scale from zero (low severity) to 100 (high severity). The primary outcomewas to assess differences in perceived injury severity for each injury type over geographic regions and level of practice experience. Results: A total of 189 responses were received. Overall, the classification system exhibited a hierarchical progression in subtype injury severity scores. Only three subtypes showed a significant difference in injury severity score among geographic regions: F3 (floating lateral mass fracture, P = .04), N3 (incomplete spinal cord injury, P = .03), and M2 (critical disk herniation, P = .04). When stratified by surgeon experience, pairwise comparison showed only 2 morphological subtypes, B1 (bony posterior tension band injury, P = .02) and F2 (unstable facet fracture, P = .03), and one neurologic subtype (N3, P = .02) exhibited a significant difference in injury severity score. Conclusions: The AO Spine Subaxial Cervical Spine Injury Classification System has shown to be reliable and suitable for patient management. The study shows this classification is substantially generalizable by geographic region and surgeon experience; and provides a consistent method of communication among physicians while covering the majority of subaxial cervical spine traumatic injuries.
47
A187: Odontoid Fracture Extending into the Pars Interarticularis: A Distinct Clinico-Pathological Injury Pattern?
Salvatore Russo 1
1 Imperial College NHS - St Mary's Hospital, Dept of Neurosurgery - Spine division, London, United Kingdom
Purpose: Fractures of the axis can traverse the body of the vertebra below the odontoid process and extend rostrally into the pars interarticularis. The posterior arch of C2, on the side of the fractured isthmus, is often displaced cranially with a contralateral anterior subluxation of the atlantoaxial joint. We investigated clinical and radiological outcomes of this injury pattern specifically addressing the issue of atlantoaxial stability and its impact on consolidation. These aspects have not been sufficiently examined in previous studies. To overcome the surgical challenges related to the morphology of these fractures, we also describe a novel surgical strategy performing an osteotomy of the pars interarticularis and a distraction arthrodesis of the atlantoaxial joints. Methods: We conducted a single centre cohort study of 114 fractures of the axis treated between June 2016 and June 2018 and reviewed the clinical history of 13 consecutive patients with odontoid fracture extending into the pars. Osseous union was defined as osseous bridging across the fracture line on CT while the criteria for a stable fibrous non-union were an Atlanto-Dens Interval (ADI) <3 mm, Posterior-Atlanto-Dens-Interval (PADI) >14 mm and lack of symptomatic motion at the fracture site. Atlantoaxial instability was defined as greater then 50% subluxation across the C1-C2 joint. Return to pre-injury performance status was consider a satisfactory clinical outcome. We used the Barnard exact test for 2 x 2 contingency tables to evaluate statistical correlation for atlantoaxial instability and consolidation. Results: The mean age of the patient population presenting with an odontoid fracture with extension into the pars was 77.2 years (95% CI 70.5-83.9). The mean follow up time was 15 months (95% CI 12-18). 69% had an associated atlantoaxial instability (P-value < .0005) and 54% were displaced. 46% reported an hyperextension injury. The mean time interval from the injury to the hospital presentation was 13.6 days (95% CI 4-23.2). Cervical orthosis treatment was associated with a high non-union rate (70%) (P-value .04) although it did not affect the overall clinical outcome. Fractures causing progressive myelopathy were successfully treated with atlantoaxial distraction arthrodesis. Conclusions: Odontoid fractures extending into the pars interarticularis is a marker of increased injury severity. These fractures are common in the over 70 s and can present after a significant time interval from the initial injury. Hyperextension could be the main injury vector of this fractures. This injury is associated with atlantoaxial instability and non-union when treated with cervical orthosis. The C1-C2 segment can be surgically stabilised with atlantoaxial distraction arthrodesis achieved through an osteotomy of the pars interarticularis. We suggest to consider pars fracture with atlantoaxial subluxation as a risk factor for instability and non-union in odontoid failure.
1642
A188: Fusion Failure Analysis in Anterior Cannulated Screw Fixation of Odontoid Fracture of C2 II Type
Tahir Tamaev 1 , Vadim Manukovsky 1 , Valerii Serikov 1 , and Irina Afanaseva 1
1 Saint-Petersburg I.I. Dzhanelidze Research Institute of Emergency Medicine, Sankt-Petersburg, Russian Federation
Introduction: Anterior fusion with cannulated screw for odontoid fractures of C2 is both minimally invasive and functional technique. Material and Methods: The results of treatment of 40 (20 men and women each) somatically healthy non-smoking patients with anterior cannulated screw fixation using the F. Magerl technique are presented. Patients were divided into 2 age groups 18-44 years old and 45-59 years old. The average age was 36,7 years in the first group and 52.4 years in the second. After surgery, all patients were prescribed to wear a cervical orthosis (Philadelphia type) until signs of consolidation appear. The fusion status was evaluated after 2, 4, 6 months from fixation. Result of treatment was considered unsuccessful, if within 6 months from the moment of injury there was no consolidation or signs of instability of implant appeared. Results: In the studied groups there were no statistically significant differences by gender and age. Signs of consolidation after 2 months were observed in 10% (n = 2) of patients in group 1 and in 10% (n = 2) of patients in group 2. Implant instability at this time was observed only in group 1 in 10% (n = 2) of patients. Within 4 months, fusion occurred in 70% (n = 14) of patients in group 1 and 80% (n = 16) of patients in group 2. After 6 months, fusion occurred in another 5% (n = 1) of patients in group 1 and 5% (n = 1) in group 2. Implant instability up to 6 months developed in another 5% (n = 1) of patients in every group. Over 6 months, fusion occurred in 36 patients, which amounted to 90%. Analysis of the negative results of 10% (n = 4) of cases revealed that common to all of these patients was a violation of the doctor’s prescriptions (total or partial refusal of wearing an orthosis, driving a car, returning to work). Conclusion: Results obtained indicate that anterior cannulated screw fixation of odontoid fractures of C2 II type is a reliable and functional method of treatment, in compliance immobilization until signs of consolidation appear. Patients at least 2 months after the surgery must carefully observe the orthopedic regimen, in the form of restriction of rotational movements and wearing a cervical orthosis. Anterior cannulated screw fixation of odontoid fractures of C2 II type leads to a good orthopedic result in most of the operated patients.
1797
A189: The Impact of HBOT in Spinal Cord Injury
Renate Krassnig 1 , Smolle-Juettner Frayja-Maria 2 , Berzins Uldis 3 , Hohenberger Gloria 3 , and Wildburger Renate 1
1 AUVA Rehabilitation Clinik Tobelbad, Tobelbad, Austria
2 University Hosptial of Surgery, Thoracic Surgery, Graz, Austria
3 University Hospital of Orthopaedics and Trauma, Graz, Austria
Introduction: Spinal cord injury (SCI) represents a central nervous system complication as a result of severe trauma to the spinal column. It often causes neurological disorders of the extremities and the trunk below the injured spinal segments. Due to the increase of traffic accidents and aerial work types, the incidence of SCIs remains at a high level including 130.000 to 500.000 cases per year. SCI represents a significant cause of morbidity and mortality and an immense socioeconomic burden affecting mainly young patients. Material and Methods: All consecutive patients which presented with spinal cord injury (SCI) - edema at the cervical spinal cord - and were treated with or without hyperbaric oxygenation therapy (HBOT) at a level-I university trauma center and which finished their primary rehabilitation at a cooperating rehabilitation clinic between January 1, 2006 and December 31, 2019 were included in the study. The time line was chosen on the base of data accessibility. From this data cohort, two subgroups were built. One involved those patients who had undergone HBOT and the second group included patients who had not received HBOT. All data were collected prospectively in a dedicated trauma database. Specific patient characteristics (age at time of trauma, gender) as well as details on trauma (trauma characteristics, height of SCI, type of surgical intervention) were evaluated retrospectively. Results: Sixteen patients (17.0%; 16/94) presented with either isolated spinal edema or combination of edema and fracture. All of these formations were located at the cervical spine and all of the patients primarily presented with tetraplegia. Ten of the patients (62.5%; 10/16) were treated with, and six (37.5%; 6/16) without HBOT. In the group without HBOT, 20% of all patients (2/10) showed ASIA Score improvements, whereas in the sample that received HBOT, 83.3% (5/6) had improved values at the end of primary rehabilitation (P = ≤. 001). Conclusion: HBOT has a statistically significant impact on recoverage after edema of the cervical spinal cord.
OP22: Deformity-Thoracolumbar (Adult)
1433
A190: Compensation for Standing Posture by Whole-Body Sagittal Alignment in Relation to Health-Related Quality of Life
Kazuhiro Hasegawa 1 , Masashi Okamoto 2 , Shun Hatsushikano 3 , Kei Watanabe 4 , Masayuki Ohashi 5 , Jean-Marc Vital 6 , and Jean Dubousset 7
1 Niigata Spine Surgery Center, 2-5-22 Nishi-machi, Konan-ku, Niigata City, Japan
2 Niigata Spine Surgery Center, 2-5-22 Nishi-machi, Konan-ku, Niigata City, Japan
3 Niigata Spine Surgery Center, 2-5--22 Nishi-machi, Konan-ku, Niigata City, Japan
4 Niigata University Medical and Dental General Hospital, Dept. of Orthop. Surg.,, Niigata, Japan
5 Niigata University Medical and Dental General Hospital, Niigata, Japan
6 Spinal Unit, University Hospital, Bordeaux, France, 7 Académie Nationale de Médecine, Paris, France
Introduction: The aim of this study is to test the hypothesis that three grades of sagittal compensation for standing posture (normal, compensated, and decompensated) correlate with health-related quality of life measurements (HRQOL). Material and Methods: A total of 50 healthy volunteers (normal), 100 patients with single-level lumbar degenerative spondylolisthesis (LDS), and 70 patients with adult to elderly spinal deformity (deformity) were enrolled. Following collection of demographic data and HRQOL measured by the Scoliosis Research Society-22r (SRS-22r), radiological measurement by the biplanar slot-scanning full body stereoradiography (EOS) system was performed simultaneously with force-plate measurements to obtain whole body sagittal alignment parameters. These parameters included the offset between the centre of the acoustic meatus and the gravity line (CAM-GL), SVA), T1 pelvic angle (TPA), McGregor slope, C2-7 lordosis, thoracic kyphosis (TK), lumbar lordosis (LL), pelvic incidence (PI), PI-LL, sacral slope (SS), pelvic tilt (PT), and knee flexion. Whole spine MRI examination was also performed. Cluster analysis of the SRS-22r scores in the pooled data was performed to classify the subjects into three groups according to the HRQOL, and alignment parameters were then compared among the three cluster groups. Results: On the basis of cluster analysis of the SRS-22r subscores, the pooled subjects were divided into three HRQOL groups as follows: almost normal (mean 4.24 (SD . 32)), mildly disabled (mean 3.32 (SD . 24)), and severely disabled (mean 2.31 (SD . 35)). Except for CAM-GL, all the alignment parameters differed significantly among the cluster groups. The threshold values of key alignment parameters for severe disability were TPA > 30°, C2-7 lordosis > 13°, PI-LL > 30°, PT > 28°, and knee flexion > 8°. Lumbar spinal stenosis was found to be associated with the symptom severity. Conclusion: This study provides evidence that the three grades of sagittal compensation in whole body alignment correlate with HRQOL scores. The compensation grades depend on the clinical diagnosis, whole body sagittal alignment, and lumbar spinal stenosis. The threshold values of key alignment parameters may be an indication for treatment.
970
A191: Is There a Heritability Impact on Spinal Sagittal Alignment? A Twin Study in the United Kingdom
Khai Lam 1 and Carlos De La Torre 1
1 London Bridge Hospital, Suite 105, St Olaf's House, London, UK
Introduction and Purpose: Sagittal balance of the spine is a well documented and resounding concept in the understanding and treatment of spinal pathologies. Pelvic incidence (PI) tends to increase linearly with adolescent growing age and becomes a constant anatomical parameter in adulthood. Lumbar lordosis (LL) and thoracic kyphosis (TK) is strongly correlated to the PI. Based on that, Roussouly et al. proposed four types classification for normal sagittal balance depending on the PI, sacral slope and spinal shape. This classification helps in determining the high local stress zones in the spine, vis a vis, the lower lumbar curvature or flat back (low PI) the higher the impact on the disks; the more the lumbar spine is curved or hyper-lordosis (high PI) the more the contact force on the posterior elements (facets in particular). Currently, there are no studies to determine if genetics may act in the causation of a specific sagittal profile, i.e., Roussouly’s classification. The purpose of this study is to study the effects of heritability on measurements in sagittal balance in older adult females based on the classification proposed by Roussouly. Materials and Methods: This is a retrospective observational study on a healthy adult twin population of monozygotic and dizygotic twins obtained from the UK Twins register at King’s College London. The inclusion criteria were twin participants without spine or hip disease or previous spine surgery at the time of enrolment. Each patient underwent simultaneous standing antero-posterior and left lateral full spine radiographs that included the pelvis. The following spinal and pelvic radiographic parameters were then measured: Pelvic parameters consisted of PI to assess sacropelvic morphology, PT and SS. And based on that we classified each individual to a specific spinal shape category based on Roussouly Types 1 to 4. Results: A total of 288 female twins from the general population were included. The average age was 63.2 years. 23% (66) of the individuals were classified as Roussouly Type 1, 33.3% (96) as Type 2, 33.3% (96) as Type 3, and 10.4% (30) as Type 4. Of the 144 pairs of twins, only 50 (34.7%) pairs of twins shared the same Roussouly type of which Type 1 represented 26%, Type 2 represented 38%, Type 3 represented 28%, and Type 4 represented 8%. The remaining pairs of twins had a different Roussouly types between each twin. Conclusion: This study found no strong correlation between heritability and sagittal alignment, regardless of the zygosity of the twins. Only 34.7% of the pairs had the same sagittal spinal phenotype based on the Roussouly’s classification for normal spine sagittal balance.
1054
A192: Optimal Intraoperative Fluid Management in Adult Spinal Deformity Correction Surgery
Meghan Cerpa 1 , Chris Lai 1 , Scott Zuckerman 1 , Joseph Lombardi 1 , Zeeshan Sardar 1 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
Hypothesis: Intraoperative fluid management using liberal amounts of crystalloids and reduced colloids is safe and results in optimal postoperative outcomes in adult spinal deformity correction surgery. Design: Observational cohort. Introduction: Intraop fluid management is a vital component in adult spinal deformity (ASD) surgery that is not standardized nor has consensus on the ideal management. Increased intraop use of crystalloids and colloids is correlated with an increased risk for developing postoperative complications, especially pulmonary complications. This study aims to assess and describe the fluid management protocol for adult deformity surgery at a single-center with minimal pulmonary complications, high intraop extubation rate, and no intraop coagulopathies. Methods: 50 consecutive ASD who underwent corrective surgery at a single institution were included. Preoperative medical records, intraoperative anesthesia and surgical records, and postoperative complications were compiled. Descriptive statistics including means, percentages, and ratios were calculated. Results: The average age was 44 ( ± 17.49) years, 74% (37/50) were female, and 56% (28/50) were revision cases. The average number of levels instrumented was 13 ( ± 4), average number of levels fused was 11 ( ± 5), and an average length of surgery 7.18 ( ± 2.08) hrs. 18% (9/50) of pts had a 3-column osteotomy (PSO or VCR) and the average estimated blood loss was 1316 ( ± 635) ccs. Only 50% of pts received an intraop packed red blood cell transfusion and there were no pts that received platelet or fresh frozen plasma transfusions. Average intraop crystalloids given was 4650 ( ± 1280) mL while the average colloids given was 1556 ( ± 744) mL. The ratio of intraop crystalloids: colloids administered was 2.99:1. 96% (48/50) were extubated intraoperatively. 9 pts had postop pulmonary complications of either pulmonary edema or pleural effusion with an average length of stay of 6.04( ± 2.82) days. Conclusion: Minimizing blood loss and administering a 3:1 ratio of crystalloids:colloids is an optimal intraop fluid management protocol that results in no intraop coagulopathies, a 96% intraop extubation rate, and minimal posto pulmonary complications in ASD surgery.
228
A193: Sagittal Balance Study in Professional Brazilian Football Players
Paulo Daniel Sousa Santa Cruz 1 , Michel Kanas 1 , Nelson Astur 2 , Delio E. Martins 3 , and Marcelo Wajchenberg 1
1 Federal University of Sao Paulo, Ortopedia, Sao Paulo, Brazil
2 Santa Casa de Sao Paulo, Ortopedia, Sao Paulo, Brazil
3 Universidade Anhembi Morumbi, Sao Paulo, Brazil
Introduction: High incidence of postural disorders, mainly in young athletes leads to question the influence of different sport activities in posture and sagittal balance. The study aims to compare spinopelvic angles and sagittal balance of Brazilian professional football players with non-athlete population, classify their lordosis type according Roussouly, and measure the prevalence spondylolysis and spondylolisthesis. Material and Methods: A cross-sectional study was carried out, using standardized panoramic spine radiographs, in lateral view, of 110 Brazilian professional football players, aged between 18 and 40 years, who participated in pre-season evaluation at FIFA Reference Center. Using the Surgimap® software, spinopelvic angles were measured, together with Sagittal Vertical Axis (SVA) and Lumbar Lordosis (LL). The mean values were compared to Brazilian literature data. Lordosis type was classified according Roussouly, and cases with spondylolysis and spondylolisthesis were identified. Results: From de evaluated radiographs, 104 had appropriate measurement quality. Pelvic Tilt (PT) and SVA were statistically lower in professional players when compared to non-athlete population (P = .013 and P = .037). Furthermore, Sacral Slope (SS) tent to be higher in professional football players (P = .054). Most athletes presented type 3 lordosis (54.8%) followed by type 4 (26.9%). Eight athletes (7.7%) presented spondylolysis, from those, seven (6.7%) also had spondylolisthesis. Conclusion: When compared to non-athlete population, significant differences were found in Brazilian professional football players, referring to PT and SVA. Roussouly’s lordosis type 3 was the most common, and the prevalence of spondylolysis and spondylolisthesis was higher than in general population; but lower than found in the literature for professional football players.
757
A194: The Posterior Cranial Vertical Line (PCVL): A Novel Global Sagittal Alignment Parameter that Correlates to Proximal Junctional Kyphosis Following Adult Spinal Deformity Surgery
Paul Park 1 , Cole Morrissette 1 , Nathan Lee 1 , Meghan Cerpa 1 , Ronald A. Lehman 1 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
Introduction: Restoring sagittal alignment has been associated with improved functional status and patient outcomes. While the gold standard for sagittal alignment is the C7-sagittal vertical axis (SVA), this is in fact only a regional measure of sagittal alignment, excluding the position of the skull and lower extremities. We propose a novel radiographic marker of global sagittal alignment, the posterior cranial vertical line (PCVL). The PCVL is a practical, easy-to-implement vertical line drawn from the posterior-most aspect of the occiput down to the floor; its relationship to the thoracic apex, pelvis, and feet are reviewed in this study and its relevance to proximal junctional kyphosis (PJK) is analyzed in adult spinal deformity patients. Methods: Full-length radiographs of 72 adult spinal deformity patients were retrospectively reviewed undergoing posterior spinal fusion (minimum 6 levels) and a minimum radiographic follow-up of 1 year. Average age was 52 years and average follow-up was 1.7 years. The distance of the PCVL to the thoracic apex, posterosuperior S1 endplate, and tibial plafonds were measured and patients were separated into 3 grades according to a previous study in a healthy volunteer population. Radiographic PJK was defined as a sagittal proximal junctional angle (PJA) from the upper instrumented vertebra (UIV) to UIV+2≥10° and/or a change of ≥10° compared to preoperatively. ANOVA, chisquare, logistic regression, and ad-hoc statistical analyses were performed. Results: Of 72 patients included in the study, 47 were preoperatively categorized as PCVL grade 1, 19 as grade 2, and 6 as grade 3. At final follow-up, preoperative PCVL grade was significantly correlated with increased rates of PJK (P = .0027), and a larger PJA (P = .0001). The preoperative PCVL grade differed in 27.8% (20/72) patients when compared to the immediate postoperative PCVL grade. As such, the immediate postop PCVL grade had a significant correlation with radiographic PJK at final follow-up (P = .0097) as well. When the PCVL fell anterior to the cephalad-most extent of the instrumentation on immediate postoperative radiographs, patients were significantly more likely to have radiographic PJK at final follow-up (P = .038), as well as an increased PJA (P = .035). PCVL anterior to cephalad instrumentation at final follow-up was significantly correlated with radiographic PJK (P = .0097) and increased PJA (P = .078); if the PCVL was anterior to cephalad instrumentation at final follow-up, patients were 4.7 (95%CI: 1.4-16.2) times more likely to have radiographic PJK. Discussion and Conclusion: The PCVL is a novel radiographic marker for global sagittal balance in adult spinal deformity patients, in which the preoperative and immediate postoperative PCVL grades are significantly correlated with postoperative rates of radiographic PJK. The PCVL is helpful postoperatively to monitor patients over time, and may highlight patients that are high-risk for developing PJK. A PCVL anterior to the cephalad-most instrumentation is also significantly associated with increased PJA and rates of PJK. The PCVL is a practical, easy-to-implement radiographic marker that provides additional information on sagittal balance that may be used in conjunction with various other factors in determining an appropriate surgical plan in patients that may be more at risk for development of PJK.
394
A195: Multilevel thoracic spine fusion complications for the treatment of idiopathic and neuromuscular scoliosis
Alexander Ballatori 1 , Shane Shahrestani 1 , Xiao Chen 1 , Andy Ton 1 , Jeffrey C. Wang 1 , and Zorica Buser 1
1 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
Introduction: Surgical stabilization for both idiopathic scoliosis (IS) and neuromuscular scoliosis (NMS) is critical to prevent further deformity, chronic pain, restrictive lung disease, as well as many other complications. As technology and surgical technique advances in the field of medicine, one would hope to see improvement in outcomes following scoliosis corrective surgeries. The purpose of this study is to analyze outcomes of IS and NMS patients in the recent years. Material and Methods: We conducted a retrospective cohort study using data from the 2016-2017 National Readmission Database (NRD). Using ICD-10 codes, we identified 1,367 patients under the age of 25 that received multilevel thoracic spinal fusion for diagnosed IS (n = 547) and NMS (n = 820). Mann-Whitney U testing was performed to compare costs, LOS, and 30- and 90-day readmission rates. All statistical analyses were conducted in R. Results: The mean age of our IS group was 14.89 ± 2.99 years old and was 74.4% female. The mean age of our NMS group was 13.09 ± 3.16 and was 51.4% female. We found that multilevel thoracic fusion for NMS was significantly more costly than IS (NMS: $80,735.99 ± 42,097.63, IS: $63,201.46 ± 40,820.19, P < .0001). The NMS group also had longer LOS compared to the IS group following the procedure (NMS: 8.23 ± 9.75, IS: 4.63 ± 2.99, P < .0001). Finally, the NMS group had higher rates of 30- (NMS: 16.0%, IS: 1.34%, P < .0001) and 90-day (NMS: 16.0%, IS: 1.53%, P < .0001) readmissions. Conclusion: Our data showed that NMS patients have higher costs and complications following their surgical correction for scoliosis compared to IS patients. These rates of readmissions are comparable for NMS and lower for IS with respect to studies conducted in the early 2000s, and highlights the need for continued development in the surgical correction of NMS patients.
896
A196: A New Intradiscal 3-Column Osteotomie Technique in Adult Spinal Deformity Using Expandable and Non-Expandable Cages
Sven Frieler 1 2 3 4 , Alexander von Glinski 1 2 3 , Basem Ishak 1 3 , Clifford Pierre 1 3 , Ryan Goodmanson 3 , Rod Oskouian 3 , and Jens Chapman 3
1 Seattle Science Foundation, Seattle, Washington, USA, Swedish Medical Center, Seattle, Seattle, USA
2 BG University Hospital Bergmannsheil, Ruhr University Bochum, Department of Orthopaedics and Trauma Surgery, Bochum, Germany
3 Swedish Medical Center, Swedish Neuroscience Institute, Seattle, USA
4 Swedish Hospital, Seattle, Hansjörg Wyss Hip and Pelvic Center, Seattle, USA
Introduction: Thoracolumbar deformity remains a challenge in spine surgery. Several types of spine osteotomy techniques have been described to maintain sagittal alignment, differing in the invasiveness and degree of possible deformity correction. Intradiscal osteotomy (IDO) is a new and less invasive technique, which can be used in sagittal spinal deformity correction and may be especially beneficial in the lower lumbar region. This retrospective cohort study evaluates the degree of focal and global lordotic changes and emphasized the complications rates as well as cage subsidence achieved with an IDO comparing both static and expandable interbody devices. Methods: A single institutional database was retrospectively reviewed for all patients who underwent IDO with expandable or non-expandable cages in spinal instrumentation. Inclusion criteria were fusion with a minimum of ≥5 motion segments, thoracolumbar and lumbar adult deformity and a follow-up ≥ 6 months. Spinal IDO includes resection of the posterior portions of the surrounding endplates of target disc level including posterior facetectomies, laminaes and spinous processes. Furthermore, an interbody spacer device is placed with posterior instrumentation which allows for lordotic deformity correction. The demographic and surgical data collected includes age, gender, body mass index (BMI), comorbidities, prior surgeries and fused levels. Besides changes in segmental and global lordosis, primary outcome parameters were blood loss and subsidence. Secondary outcome parameters were the presence or absence of intra- and postoperative complications as well as revision surgery. Results: The IDO was performed at 40 levels in total with an average of 2 IDO per case in 20 patients (8 male) with a mean age of 68.5 (range 50-80, SD 8.11). In 11 cases 19 IDO with expandable cages (eIDO) were conducted, while in 9 cases only static cages were used (21 sIDO). The average number of levels fused in the eIDO group was 7.19 (SD 4.0) and a mean blood loss of 1050 ml (SD 898,89) compared to 7.2 levels (SD 1.8) and a mean blood loss of 1283,33ml (SD 440,88) in the sIDO group with no statistical difference. The lumbar lordosis was significantly improved in both groups (eIDO 15° SD 6.8, sIDO 14.9° SD 5.9). The total subsidence rate was 5.0%, while there was no subsidence in the eIDO cohort and two cases in sIDO (9.5%). We encountered overall 6 complications (30.0%) in 5 patients. Two intraoperative complications (dura tear, instrumentation misplacement) within the eIDO cohort and 2 intraoperative complications (dura tear, instrumentation misplacement) in the sIDO group as well as 2 post discharge complication (hardware failure) in both cohorts. Conclusion: Intradiscal osteotomy (IDO) may be a safe and effective intervention for correction of sagittal imbalance. Due to less blood loss and the relatively low complication rate, it might be especially beneficial in elderly patients. Neither the posterior endplate osteotomy, allowing to close the posterior margin as close as possible, is associated with higher subsidence rates nor the use of expandable cages.
949
A197: Variation Patterns of Cervical Alignment in Ankylosing Spondylitis-Related Thracolumbar Kyphosis Following Pedicle Subtraction Osteotomy in Sitting Position: An Eos-Based Investigation
Bangping Qian 1 , Shi-zhou Zhao 1 , Ji-chen Huang 1 , Mu Qiao 1 , Bin Wang 1 , and Yong Qiu 1
1 Nanjing University Medical School, Nanjing, China
Introduction: Both unchanged upper cervical lordosis combined with decreased lower cervical lordosis and decreased upper cervical lordosis combined with decreased lower cervical lordosis have been reported to occur after the correction surgery adult spinal deformity. However, cervical alignment variations following the correction surgery in ankylosing spondylitis (AS) patients have not been investigated. The current study was aimed to investigate the cervical alignment variations following the correction surgery in AS patients with thoracolumbar kyphosis. Materials and Methods: AS patients who underwent pedicle subtraction osteotomy (PSO) for thoracolumbar kyphosis from June 2016 to June 2019 with a minimum of 1-year follow-up were reviewed. Patients were grouped according to the presence (the Ossified group) and absence (the non-Ossified group) of total ossification of anterior longitudinal ligament (ALL) in the lower cervical spine. Radiographic parameters were measured on lateral sitting EOS images including thoracolumbar, craniocervical and global radiographic parameters. Results: Thirty-two patients (27 males and 5 females) with a mean follow-up of 1.5 years were identified. There were 21 patients in the non-Ossified group and 11 patients in the Ossified group. After PSO, both groups showed a decrease in OC7 (P < .001, both). In the non-Ossified group, C2C7 decreased significantly (P < .001) while the OC2 angle remained unchanged (P = .570). In the Ossified group, the OC2 decreased significantly (P < .001) while C2C7 remained unchanged (P = .311). In addition, the change in OC2 was correlated with the osteotomy angle in the Ossified group (R = .776, P = .005). Conclusions: The variation patterns of cervical alignment following correction surgery for AS-related thoracolumbar kyphosis were different based on the patients with / without total ossification of ALL in the lower cervical spine. When planning PSO for patients in the Ossified group, restoration of the physiological upper cervical lordosis angle could be achieved by adjusting osteotomy angle.
420
A198: The Minimally Invasive Interbody Selection Algorithm for Spinal Deformity
Praveen Mummaneni 1 , Ibrahim Hussain 2 , Christopher Shaffrey 3 , Robert Eastlack 4 , Gregory Mundis 4 , Juan Uribe 5 , Richard Fessler 6 , Paul Park 7 , Leslie Robinson 8 , Joshua Rivera 9 , Dean Chou 1 , Adam Kanter 10 , David Okonkwo 10 , Pierce Nunley 11 , Michael Wang 2 , Frank La Marca 12 , Khoi Than 3 , and Kai-Ming Fu 13
1 University of California San Francisco, San Francisco, USA
2 University of Miami, Miami, USA
3 Duke University, Durham, USA
4 Scripps Clinic, San Diego, USA
5 Barrow Neurological Institute, Phoenix, USA
6 Rush University, Chicago, USA
7 University of Michigan, Ann Arbor, USA
8 Enloe Neurosurgery and Spine, Chico, USA
9 University of California, Berkeley, USA
10 University of Pittsburgh, Pittsburgh, USA
11 Spine Institute of Louisiana, Shreveport, USA
12 Henry Ford Health System, Detroit, USA
13 Weill Cornell Medical Center, New York, USA
Introduction: Minimally invasive surgery (MIS) for spinal deformity use interbody techniques for correction, indirect decompression, and arthrodesis. Selection criteria for choosing a particular interbody approach is lacking. We created the minimally invasive interbody selection algorithm (MIISA) to provide a framework for rational decision making in MIS deformity surgery. Methods: A retrospective dataset of circumferential minimally invasive surgery (cMIS) for adult spinal deformity (ASD) collected over a five-year period was analyzed by level in the lumbar spine to identify preferences and evaluate segmental lordosis outcomes. This data was used to inform a Delphi session of MIS deformity surgeons from which the algorithm was created. The algorithm lead to one of four interbody approaches: anterior lumbar interbody fusion (ALIF), anterior column release (ACR), lateral lumbar interbody fusion (LLIF), and transforaminal interbody fusion (TLIF). Preoperative and 2-year postoperative radiographic parameters and clinical outcomes were compared. Results: 11 surgeons completed 100 cMIS for ASD with 338 interbody devices that had minimum 2-year follow-up. The type of interbody approach used at each level from L1-S1 was recorded. The MIISA was then created with substantial agreement. The surgeons generally preferred LLIF for L1-L2 (91.2%), L2-L3 (85.2%), and L3-L4 (80.7%). ACR was most commonly performed at L3-L4 (8.4%) and L2-L3 (6.2%). At L4-L5, LLIF (69.5%), TLIF (15.7), and ALIF (9.8%) were most commonly utilized. TLIF and ALIF were the most selected approaches at L5-S1 (61.4% and 38.6%, respectively). Segmental lordosis at each level varied based upon approach with greater increases reported using ALIF, especially at L4-5 (9.2 degrees) and L5-S1 (5.3 degrees). Substantial increase in lordosis was achieved with ACR at L2-L3 (10.9 degrees) and L3-L4 (10.4 degrees). Lateral interbody arthrodesis without the use of an ACR did not generally result in significant lordosis restoration. There were statistically significant improvements in PI-LL mismatch, coronal Cobb angle, and ODI at 2-year follow-up. Conclusions: The use of the MIISA provides consistent guidance for surgeons who plan to perform MIS deformity surgery. For L1-L4, the surgeons preferred lateral approaches to TLIF and reserved ACR for patients who needed the greatest increase in segmental lordosis. For L4-L5, the surgeons’ order of preference was LLIF, TLIF, and ALIF, however TLIF failed to demonstrate any significant lordosis restoration. At L5-S1 the surgeon team typically preferred an ALIF when segmental lordosis was desired and preferred a TLIF if preoperative segmental lordosis was adequate.
OP23: Cervical Myelopathy
630
A199: Multi-Level Cervical Myelopathy is Associated with Cervical Spinal Deformity
Sarthak Mohanty 1 , Sachin Gupta 1 , David Casper 1 , and Comron Saifi 1
1 University of Pennsylvania Health System, Department of Orthopaedic Surgery, The Spine Center at Pennsylvania Hospital, Philadelphia, USA
Introduction: Understanding changes in sagittal curvature of the cervical spine is crucial in differentiating physiologic and diseased states.Changes in curvature occur during aging and are often asymptomatic. Therefore, discerning the natural progression of the cervical curvature parameters to distinguish changes associated with clinical presentations from those that are asymptomatic is imperative. This study compared baseline and post-operative differences in cervical alignment of patients who underwent cervical fusion to correct multi-level cervical myelopathy (constructs terminating either at C7 or spanning the cervico-thoracic junction (CTJ)) to those of non-surgical, age matched controls. Methods: A single center, retrospective analysis of 52 patients undergoing posterior cervical fusion (PCF) between 2017 and 2018, with 12-month postoperative visits, cervical spine x-rays, and patient reported outcomes was performed. Of these, 22 patients’ fusions terminated at C7, while 30 patients’ fusions crossed the CTJ. A control group comprising of fifty-two age-matched controls with cervical radiographs, no symptoms of myelopathy or radiculopathy, were also analyzed. Pre- and post-operative radiographs were analyzed for cervical lordosis, cervical SVA (cSVA), and T1 slope. Modified Japanese Orthopedic Association (mJOA) scores, which graded functional impairment, were calculated for each subject. A Pearson chi-square test was used to compare incidence of neurological defecits. Differences in radiological parameters were assessed using one-way ANOVAs and post-hoc Tukey's t-tests. Kruskal-Wallis (KW) nonparametric analysis of variance with post-hoc Dunn’s tests were used for mJOA scores. Results: Pre-operatively, patients undergoing fusion showed significant differences in cervical alignment by T1S (21.27 vs 28.43, P < .0001), C2-C7 lordosis (11.58 vs 25.96, P < .0001), and cSVA (36.08 vs 24.93, P < .0001) when compared to non-surgical controls. Despite significant correction post-operatively, patients undergoing fusion remained less lordotic than controls by T1S (25.61 vs 28.43, P < .0001) and C2-C7 lordosis (17.69 vs 25.96, P < .0001). Within the fusion cohort, patients whose fusion constructs spanned the CTJ demonstrated more severe pre-op malalignment than those in the C7 cohort by T1 slope (14.33 vs 21.27, P < .0001), C2-C7 lordosis (9.03 vs 13.07, P < .0001), and cSVA (9.03 vs 13.07, P < .0001). Compared to C7 patients, CTJ patients had more pronounced alignment corrections by T1 slope (28.43 vs 23.26, P < .0001) and C2-C7 lordosis (20.74 vs 15.16), although differences in the mJOA motor and sensory scores showed no significant differences between the CTJ and C7 cohorts at pre- and post-op timepoints. Conclusion: Patients undergoing posterior cervical spinal fusion and decompression for symptomatic cervical myelopathy have a significant cervical malalignment based on T1 slope, cervical lordosis, and cSVA when compared to physiologic, age-matched controls who did not have symptoms of myelopathy. Within symptomatic patients who underwent PCF, extension of the fusion construct across the CTJ resulted in more pronounced corrections of cervical alignment by T1 slope and C2-C7 lordosis when compared to patients whose fusion constructs terminated at C7. Taken together,in cases of elective posterior cervical laminectomy and fusion, fusing across the CTJ may better achieve physiologic cervical alignment and should be evaluated against the trade-offs of increased surgical time, estimated blood loss, and the rates of wound dehiscence reported in literature.
1087
A200: Frailty is a Better Predictor than Age of Mortality and Perioperative Complications After Surgery for Degenerative Cervical Myelopathy: An Analysis of 41,369 Patients from the NSQIP Database 2010-2018
Jamie Wilson 1 2 , Jetan Badhiwala 2 , Ali Moghaddamjou 2 , Albert Yee 2 , Jefferson Wilson 2 , and Michael Fehlings 2
1 University of Nebraska medical center, Neurosurgery, Omaha, USA
2 University of Toronto spine program, Toronto Western Hospital, Toronto, Canada
Introduction: Degenerative Cervical Myelopathy (DCM) is the leading cause of adult spinal cord dysfunction and surgery is typically the accepted treatment. DCM is frequently diagnosed in the elderly and this can present management challenges as older age is associated with increased risk of perioperative adverse events. Frailty may be a more accurate predictor of medical risk than age, therefore we hypothesized that frailty would be a better indicator of surgical risk in DCM than advanced age and that this could guide clinical management. The objective of the current study was to model the effects of frailty and age on the risk of perioperative adverse events for surgical DCM patients in order to produce an accurate predictive tool suitable for clinical use. Material and Methods: The NSQIP inpatient sample database records from 2010-2018 were interrogated for adult patients who underwent surgery with a diagnosis of DCM based on ICD9/ICD 10 codes (721.1, 722.71, M47.12, M50*). MFI11, MFI5, Charlson Co-Morbidity Index (CCI) and the American Society of Anesthesiologists (ASA) scores were calculated using previously published conventions matching variables within the NSQIP database volume. Outcomes of Mortality, major complication, readmission <30 days, reoperation <30 days and length of stay were calculated for each patient and compared initially with univariate analysis. Multivariable modelling of age and frailty with a base model (type of surgical approach, number of operated levels and gender) was performed, with receiver operating characteristic area under the curve analysis to define discriminative ability of each measure. Results: 41,369 patients were included, mean age 56.6 (56.5-56.7), 46% were female. Anterior was the most common approach (80%), with 3% combined anterior/posterior. On univariate analysis, age and MFI5/MFI11 were significantly correlated with mortality, major complication, unplanned readmission, reoperation within 30 days, length of hospital stay and discharge destination other than home (P < .05 for each), whereas CCI and ASA scores showed an inferior correlation. Increasing frailty for both MFI5/MFI11 demonstrated increasing risk for each outcome, and the effect size for frailty (“Frail” & “Severely Frail” patients) was higher compared to age. The multivariable regression model confirms that the MFI5 score is a stronger predictor of all outcome variables compared to age as a continuous variable (P < .05). The discriminative value of the Base model + MFI5 was excellent (.85), and superior to all other measures of frailty. Conclusion: In the one of the largest studies of perioperative complications in DCM, Frailty indices appear to be stronger predictors of adverse events compared to age alone. This has important implications in the pre-operative assessment and counselling of patients undergoing surgery for DCM. The multivariable model presented has the potential for widespread clinical use for perioperative risk stratification.
832
A201: Clinical Impact of OPLL Progression After Cervical Laminoplasty
Kawaguchi Yoshiharu 1 , Taketoshi Yasuda 1 , Shoji Seki 1 , Kayo Suzuki 1 , Kenta Watanabe 1 , Yasuhito Yahara 1 , Hiroto Makino 1 , and Katsuhiko Kamei 1
1 University of Toyama, Toyama, Japan
Introduction: Laminoplasty is a standard operation for the treatment of cervical myelopathy caused by cervical ossification of the posterior longitudinal ligament (OPLL), as cervical OPLL often causes multi-level spinal cord compression. It has been reported that the long-term surgical outcome of laminoplasty is favorable in most of the patients with cervical OPLL.1 However, as OPLL is a progressive disease,2 neurological deterioration is frequently encountered due to the progression of the ossified lesion. However, the incidence and characteristics of neurological deterioration due to OPLL progression after the first posterior surgery have not yet been precisely elucidated. The purpose of this study was 2 fold: 1) To analyze the incidence of patients who required an additional second surgery for the neurological deterioration due to OPLL progression, and 2) To clarify the clinical characteristics and surgical outcome of the patients. Material and Methods: This study was carried out in a single institute with a long-term follow-up. From 1981 to October 2015, 201 patients with myelopathy due to cervical OPLL underwent laminoplasty. One hundred sixty-seven patients who could be followed for more than 2 years were included. The neurological finding was graded by JOA score. If the patients had both neurological deterioration with clinical symptoms and OPLL progression, we judged as the neurological deterioration was caused by the OPLL progression. We retrospectively examined the incidence of the patients who required an additional second surgery. We also evaluated the clinical characteristics and the surgical outcome after second operation. In the patients who required a second surgery due to OPLL progression (the second surgery group), the period from laminoplasty to second surgery was checked. The symptoms requiring the second surgery were evaluated. Clinical characteristics, including sex and age at cervical laminoplasty, were compared with the patients who did not have a second surgery during follow-up (the control group). Results: Nine patients (5.4%) out of 167 patients had the second surgery by neurological deterioration due to OPLL progression. The age in the second surgery group was younger than that in the control. The mixed type of OPLL in the second surgery group was more than that in the control group. The symptoms of neurological deterioration were progressive cervical or thoracic myelopathy in 6 patients and radiculopathy in 3. The neurological recovery was achieved in 6 patients after the second surgery, however, 3 still had the neurological deficit. The patients who showed poor recovery had clear T2 high intensity by MR image in the spinal cord. Conclusion: Young age at laminoplasty and mixed type of OPLL were risk factors for OPLL progression. Revision surgery was effective, but if the patients had clear T2 high intensity in the spinal cord, the recovery was poor. Thus, revision surgery should be considered before irreversible neural damage occurs.
721
A202: Efficacy of Surgical Decompression in Patients with Degenerative Cervical Myelopathy: Results of the Canadian Prospective Multi-Center Study
Syed Mohammed Karim 1 2 , Bradley Jacobs 3 , Michael Johnson 4 , Chris Bailey 5 , Sean Christie 6 , Jerome Paquet 7 , Andrew Nataraj 8 , David Cadotte 3 , Jefferson Wilson 9 , Neil Manson 10 , Hamilton Hall 11 , Ken Thomas 3 , Raja Rampersaud 12 , Greg McIntosh 13 , Charles Fisher 2 , and Nicolas Dea 2
1 Mayo Clinic, Department of Orthopedic Surgery, Rochester, USA
2 Vancouver General Hospital, Combined Neurosurgical and Orthopaedic Spine Program, Vancouver, Canada
3 University of Calgary, Department of Clinical Neurosciences, Division of Neurosurgery, Department of Radiology, Calgary, Canada
4 University of Manitoba, Department of Surgery, Section of Orthopaedics and Neurosurgery, Winnipeg, Canada
5 Western University, Department of Surgery, London, Canada
6 Dalhousie University, Division of Neurosurgery, Halifax, Canada
7 Centre Hospitalier Universitaire de Quebec, Department of Orthopaedics, Quebec, Canada
8 University of Alberta, Division of Neurosurgery, Faculty of Medicine and Dentistry, Edmonton, Canada
9 University of Toronto, Division of Neurosurgery, Department of Surgery, Toronto, Canada
10 Canada East Spine Centre, Saint John Regional Hospital, Saint John, Canada
11 University of Toronto, Department of Surgery, Toronto, Canada
12 University of Toronto, Division of Orthopaedic Surgery and Neurosurgery, Department of Surgery, Toronto, Canada
13 Canadian Spine Society, Toronto, Canada
Introduction: Recent evidence suggests that patients who undergo decompression for degenerative cervical myelopathy (DCM) benefit from surgery regardless of disease severity. The goal of this study was to evaluate the impact of surgery on patient reported outcomes one year after surgery in a prospective cohort of Canadian patients with mild, moderate, and severe DCM. Material and Methods: Patients with a clinical diagnosis of DCM and evidence of spinal cord compression were prospectively enrolled in the Canadian prospective DCM study by 35 surgeons from 7 Canadian centers between 2015 and 2019. The cohort comprised patients who underwent surgical decompression and completed one year of follow-up. Neurologic (mJOA), disability (NDI), health related quality of life (HRQoL) (EQ-5D; SF-12 PCS; SF-12 MCS), and pain related (NRS neck and arm) outcome measures were collected at 3 and 12 months post-operatively. Outcomes at 3 and 12 months were compared to baseline for the whole cohort and were further stratified by baseline disease severity. Results: 391 patients were included in the analyses with 110 patients (28%) classified as mild (mJOA ≥ 15), 163 (42%) as moderate (mJOA 12-14), and 118 (30%) as severe (mJOA < 12). Follow up data at 12 months were available for 298 patients (76%). At 12 months after surgery, the entire cohort saw statistically significant improvements in all outcome measures. Mean mJOA scores improved from 12.82-14.75; NDI scores improved from 40.76-28.72; EQ-5D scores improved from .56-.71; SF-12 PCS scores improved from 34.78 to 40.80; SF-12 MCS scores improved from 47.20 to 50.41; NRS neck pain improved from 5.61 to 3.48; NRS arm pain improved from 5.65 to 3.25 (P < .001 for all comparisons). Only improvements in the NDI, EQ-5D, and SF-12 PCS were clinically significant, however, in terms of meeting their respective MCIDs. When stratified by disease severity, there was a clinically significant improvement in all outcome measures among patients with severe myelopathy. Clinically significant improvements in patients with mild to moderate myelopathy were limited to the NDI, EQ-5D, and SF-12 PCS. Conclusion: Surgical decompression for DCM is associated with improvements in disability and HRQoL outcomes at 12 months after surgery among all patients. Only the subset of patients with severe myelopathy experience clinically significant improvements in mJOA and pain scores, signifying that the magnitude and breadth of improvement are directly related to baseline disease severity.
1895
A203: Cervical Spine Steroid Injections for Delay of Surgery for Cervical Spondylotic Myelopathy
Mustfa Manzur 1 , Andre Samuel 2 , Steven McAnany 2 , Todd Albert 2 , Sravisht Iyer 2 , Avani Vaishnav 2 , and Sheeraz Qureshi 2
1 Sidney Kimmel Medical College at Thomas Jefferson Universit, Philadelphia, USA
2 Hospital for Special Surgery, New York, USA
Introduction: Cervical spine steroid injections are increasingly being used for diagnosis and treatment of degenerative pathology. For cervical spondylotic myelopathy, traditionally treated with surgery, there has been little investigation of the possible therapeutic or preventative effects of targeted injections. As injections may be targeted to the epidural space, the transforaminal region, or the zygapophyseal joints, differing injection modalities may also have variable therapeutic effects. Material and Methods: All patients with a new diagnosis of cervical spondylotic myelopathy, without previous cervical spine surgery or steroid injection treatment, were identified in a large insurance databases. Administration of steroid injections and surgical treatment timing was determined based on Current Procedural Terminology (CPT) codes. Multivariate logistic regression was used to determine the association of steroid injection administration with surgical treatment at various time points after initial diagnosis. Significance at P < .01. Results: A total of 686 surgically managed CSM patients were retrospectively identified in the PearlDiver database. A total of 244 patients underwent pre-surgical spinal steroid injection therapy to manage CSM symptoms. Of these, 185 patients (75.8%) underwent epidural steroid injections, 35 (14.3%) underwent zygapophyseal injections, and 24 (9.8%) underwent transforaminal steroid injections. Median time from initial CSM diagnosis to surgery was 75.5 days (µ = 351.6 days; σ = 544.9 days). In multivariate analysis, both transforaminal injections (OR = .40, P = .20) and zygapophyseal injections (OR = .33, P = .02) were insignificantly associated with decreased odds of surgery within 1 month of diagnosis, while epidural injections were not associated with decreased odds of surgery (OR = 1.17, P = .35). Interestingly, epidural and transforaminal injections were both associated with increased odds of surgery after six months post-diagnosis (P < .01). Only zygapophyseal injections had consistently reduced odds of surgery (without significance). Conclusion: The practice of steroid injection, regardless of approach (epidural, transforaminal, or zygapophyseal), does not prevent treatment of CSM via a surgical modality over the long term. While symptomatic relief may lead to short-term benefits from steroid injection, specifically in the case of transforaminal and zygapophyseal injections, it appears that this short-term benefit only delays definitive surgical treatment. Assessment of diagnostic and treatment decision-making workflow may enable identification of other aspects of CSM management that lead to delays in diagnosis and definitive treatment as well as additional cost burden.
701
A204: Prospective Randomized Control Pilot Study to Compare the Role of Injection Cerebrolysin in Operated Cases of Cervical Myelopathy
Ayush Sharma 1 , Romit Agarwal 1 , Ajay Jaiswal 1 , and Vijay Singh 1
1 central railway hospital, Department of Orthopaedic and spine surgery, Mumbai, India
Introduction: Cerebrolysin which contains a mixture containing 85% free amino acids and 15% biologically active low-molecular weight peptidest and mimics the effects of endogenous neurotrophic factors to interact with the pathologic process cascade of neurodegenerative diseases. Cerebrolysin has been used successfully in a large number of neurologic conditions such as Alzheimer disease, stroke, and other cognitive disorders resulting in significant improvement, with no significant adverse reactions reported. Aim of the study was to compare the effect of injection cerebrolysin in operated cases of cervical myelopathy. Material and Methods: The study commenced after approvalfrom the institutional ethics committee. 60 operated cases of cervical myelopathy were randomly divided into two groups. All the cases were operated by a single team of surgeons. Group one was administered injection cerebrolysin post operatively for 3 weeks while group two was administered placebo for 3 weeks. Modified Japanese orthopedic association scores (mJOA) and visual analog scale (VAS) were used to document functional outcomes at 3 weeks, 3 months, 6 months and 1 year. Recovery of hand function was separately accessed by improvement in hand power and sensations.ASIA (American Spinal Injury Association) scores were used to study the post-operative neurological recovery. Results: The preoperative mJOA and Vas scores were comparable between the two groups(P < .05). Both the group showed significant improvement in both mJOA and Vas scores at 3weeks, 3 months, 6 months and one year follow up (P < .01).On comparing the two groups there was no difference in improvement of mJOA and Vas scores at 3 weeks, 3 months, 6 months and one year follow up(P < .05).On comparing the hand function, the cerebrolysin group showed significant improvement in hand function at one year compared to the placebo group(P = .03). Post-operative neurological recovery was better in the cerebrolysin group with 66.7% patients showing complete neurological recovery compared to 56.7% for the placebo group, but this difference was statistically not significant (P = .318). Conclusion: Use of cerebrolysin in post-operative cases of cervical myelopathy is safe and can result in improved hand function.
16
A205: Do Intra-Operative Neurophysiological Changes During Decompressive Surgery for Cervical Myeloradiculopathy Impact Functional Outcome? A Prospective Study
Keyur Akbari 1 , Sajan Hegde 1 , and Muralidharan Venkatesh 1
1 Apollo Hospitals, Spine Unit, Chennai, India
Introduction: Current safe spine surgery guidelines recommend multimodal intra-operative neuromonitoring (IONM) during spinal surgery as a reliable and valid diagnostic adjunct to assess spinal cord integrity. IONM accurately identifies the topography of neural structures and gives real time alarm to the surgical team about intraoperative surgical insults. There is insufficient evidence on the therapeutic relationship between IONM changes during cervical spinal decompressive surgery for cervical spondylotic myelopathy and neurological outcomes. The primary objective of the present prospective study was to investigate whether IONM positive changes can predict functional outcome after surgical intervention for cervical myeloradiculopathy. Material and Methods: 28 patients who underwent cervical spine surgery with IONM for compressive myelo-radiculopathy were enrolled. During surgery motor evoked potential (MEP) and somatosensory evoked potential (SSEP) at baseline, before and after decompression were documented. A decrease in latency >10% or an increase in amplitude >50% was regarded as a “positive changes”. Patients were subgrouped based on IONM changes into Group A(those with positive changes) and Group B (those with no change or deterioration). Nurick grade and modified Japanese Orthopaedic Association (mJOA) were evaluated before and after surgery. Unpaired t test was used to evaluate the significance of the difference in Nurick grade and the mJOA between the groups. Spearman correlation coefficient was used to ascertain the strength of association. Results: 9 patients (32.1%) showed improvement in MEP. The mean age at the time of surgery, mean duration of symptoms, cord signal changes on MRI preoperatively and type of surgery were equally distributed between the two groups. Hence, there was no major confounding effect of all these factors in the present study. The mean preop Nurick grade and mJOA score of group A and B were (2.55 ± 83 and 11.11 ± 1.65) and (2.47 ± 7 and 11.32 ± 1.24) respectively. The mean postoperative Nurick grade of group A and B at three months was 1.8 ± .97 and 2.0 ± . 67 respectively and this difference was not significant. The mean postoperative Nurick grade of group A and B at 6 months was 1.55 ± .74 and 1.63 ± .46 respectively and this difference was not significant. The mean postoperative mJOA score of group A and B at 3 months was 13.1 ± 1.76 and 12.1 ± 1.39 respectively and unpaired t test concluded that this difference was not significant. The mean postoperative mJOA score of group A and B at six months was 14.3 ± 1.03 and 12.9 ± .98 respectively and this difference was statistically significant (P value = .011). Spearman correlation coefficient showed significant positive correlation between the IONM change and the mJOA score at six months postoperatively (r = .47; P = .01). Conclusion: Intraoperative neuromonitoring is a valuable tool in predicting neurological recovery in patients undergoing decompressive surgery for CCM. Patients with improved MEP after cervical cord decompression have a better prognosis in immediate and long-term neurological function recovery. Improvement in functional mJOA score is more significant at 6 months post surgery in patients with improved MEP changes.
1735
A206: A Multicentric Prospective Study on Cervical Spine Myelopathy Surgery in France
Philippe Bancel 1
1 Institut Arago, Spinal Department, Paris, France
Introduction: It is the first multicentric prospective study on cervical spine surgery realized in France. Material and Methods: Material: It is a Cohort study observational, prospective (inclusion June 2013 to October 2015). This study was multicentric. Inclusion criteria were: older than 18 years, volunteers, cervical myelopathy clinically. The study was composed of 180 patients. Method: Tool of data used was KEOPS software. Clinical evaluation included: general status, previous treatment, neurological examination, comorbidities, etiologic diagnosis. Radiological evaluation: included standard and dynamic X-Ray’s, Cervical MRI. Outcome measures used was: SF12, NDI, Walking test (Crockard) and Prehension test (Pascal-Mousselard). Statistical analysis was done by the: IMER center Lyon. Results: Clinical results: NDI score was 39 before surgery, 22.9 after surgery, mLOA score was 12.4, became 14. Crockard score was 45.6 and became 34.5. SF 12 mental: 43.4 became 46.6, SF12 physical: from 34.3 became 40.2. Radiological results: Diameter was significatively bigger after laminectomy and laminoplasty. but we did not observe correlation between mJOA and canal diameter.,no correlation between mJOA and Hyper T2 signal, No correlation neither observed between Fujiwara and mJOA and NDI pre and post-op. At least nno correlation between mJOA and spine type. Conclusion: Our indication surgical strategy and results are similar to the international literature. But It is the first multicentric prospective study conducted in France
1588
A207: The Role of Nutrition in Degenerative Cervical Myelopathy: A Systematic Review
Celine Partha-Sarathi 1 , Benjamin Davies 1 , and Oliver Mowforth 1
1 Division of Neurosurgery, University of Cambridge, Department of Clinical Neurosciences, Cambridge, United Kingdom
Introduction: Degenerative cervical myelopathy (DCM) is the commonest cause of adult spinal cord impairment worldwide, encompassing chronic compression of the spinal cord, neurological disability and diminished quality of life. Evidence on the contribution of environmental factors is sparse; in particular, the role of nutrition in DCM is unknown. The objective was to assess the effect of nutrition on DCM susceptibility, severity and surgical outcome. Methods: A systematic review in MEDLINE and Embase was conducted following PRISMA guidelines Full-text papers in English, with a focus on cervical myelopathy and nutrition, published between before January 2020 were considered eligible. Quality assessments were performed using the Downs’ and Black’s tool and GRADE assessment tool. Patient demographics, nutritional factor and DCM outcomes measures were recorded. Relationships between nutritional factors and interventions and disease prognosis were assessed. The results were separated depending on whether they discussed effects on spinal cord disease, spinal column disease or adverse, post-operative outcomes. Results: A total of 5835 papers were identified, 38 of which were included in the final analysis. DCM patients with pathological weight pre-operatively were likely to see poorer improvements post-surgically. Obese patients experienced poorer physical and mental improvements from surgery compared to non-obese patients, were more likely to suffer from post-operative complications such as infection, DVT and PE and were also more likely to have comorbidities such as diabetes, hyperlipidaemia and CVD. An unbalanced diet, a history of alcohol abuse and malnourishment were associated with poorer post-operative outcome. Supplementation of vitamins, minerals and proteins reduced disease-severity in malnourished patients with chronic spinal cord injury. Conclusion: Nutritional factors appear important in influencing surgical outcomes and disease progression in DCM patients. Further elucidation of the role of nutritional factors in susceptibility to DCM may be beneficial in disease prevention. In addition, better characterisation of the role of nutritional deficiencies as risk factors may aid DCM diagnosis. Further work on the role of nutrition in surgical outcomes may help inform decisions surrounding peri-operative nutrition and be useful in decisions pertaining to peri-operative optimisation.
OP24: Basic Science/Novel Therapy
854
A208: SERPINs-A Potential Target for Arresting Intervertebral Disc Degeneration
Sri Vijay Anand KS 1 , Shanmuganathan Rajasekaran 1 , Dilip Chand Raja Soundararajan 1 , Chitraa Tangavel 2 , Sharon Miracle Nayagam 2 , Sunmathi R 2 , Ajoy P Shetty 1 , Rishi Kanna 1 , Pushpa BT 3 , and Raveendran M 4
1 Ganga Hospital, Department of Spine surgery, Coimbatore, India
2 Ganga Research Centre, Department of Proteomics, Coimbatore, India
3 Ganga Hospital, Department of Radiology, Coimbatore, India
4 Tamilnadu Agricultural University, Department of Biotechnology, Coimbatore, India
Introduction: The etiology of disc degeneration (DD) is claimed to be multifactorial. Irrespective of the initiating factor, breakdown of extracellular matrix (ECM) is a critical event in DD. This ECM disassembly is brought about by proteolytic enzymes called proteases that cleave the bond holding the ECM. Serine proteases are a large family of proteases whose activities are kept in check by regulators, Serine protease inhibitors (SERPINS). The role of SERPINs in health and disease of IVD has not been studied in detail so far. In this context, we did a systematic study using high throughput proteomics with appropriate healthy control discs and discuss the inferences here. Materials and Methods: After ethical committee approval and consent, twelve intervertebral Nucleus Pulposus tissues each from (1) Normal organ donor volunteers without any sign of low back pain (ND), and patients with (2) herniated discs (DH) and (3) degenerated discs (DD) were harvested under sterile operating conditions and subjected to proteomic analysis. Immunohistochemistry(IHC) was performed to confirm the presence of two SERPINs A1 and E2. Results: Mass spectrometry identified a total protein of 2164 in ND, 1734 in DH, and 2394 in DD groups, respectively. We identified 21 SERPINs present in at least one disc sample out of a total of 37 human serpins already reported in the literature. With stringent cut off (>5 PSM and presence in at least in 2 samples per group) to increase the authenticity, we shortlisted 14 SERPINS, 8 in ND, 12 in DH, and 13 in DD group, respectively. 7 SERPINs were common to all three groups that include SERPINA1, SERPINA3, SERPINA5, SERPINA8, SERPINC1, SERPINE2, and SERPING1. SERPINA4, SERPIND1, SERPINF1, SERPINF2, and SERPINH1 were found common to DH and DD groups. SERPINE1 and SERPINB1 were found unique to ND and DD groups, respectively. SERPINA1, SERPINA5, SERPINE2, and SERPING1 showed higher expression in healthy control NP discs (ND) when compared to diseased discs- DH and DD. SERPINs A1 and E2 are known to play a protective role in maintaining disc homeostasis by inhibiting proteases such as matrix metalloproteinases (MMPs). SERPIN A5, a multifunction protein, inhibits several proteases involved in the coagulation pathway. SERPIN G1 regulates other proteases in the tissue leading to inflammation and has an anti-inflammatory role. SERPIN A3, an acute phase pro-inflammatory protein, was found in abundance in DH. SERPINH1, a procollagen-specific molecular chaperone Hsp47 was found in abundance in DH, the dysregulation of which leads to changes in the expression of ECM proteins such as fibronectin (FN1) and collagen type I. Validation of selected SERPINA1 and E2 IHC staining in the healthy ND and diseased DH and DD IVD confirmed the expression as observed in the proteomics data. Conclusion: Our study confirmed the presence of many SERPINs with various functions in the human intervertebral disc. These SERPINs A1 and E2 with inhibitory effect on MMPs could be utilized as a potential target to arrest disc degeneration.
363
A209: Effects of Single-Dose Versus Hypo-Fractionated Focused Radiation on Vertebral Body Structure and Biomechanical Integrity: Development of an Irradiation Model
Alexander Perdomo-Pantoja 1 , Christina Holmes 2 , Benjamin D. Elder 3 , Sheng-fu L. Lo 1 , Wataru Ishida 1 , Brian C Goh 4 , Chukwuebuka C. Achebe 5 , Ethan Cottrill 1 , Warren L. Grayson 5 , Soojung C. Hur 6 , Thomas L Clemens 4 , and Timothy F. Witham 5
1 Johns Hopkins University School of Medicine, Neurosurgery - Division of Spine, Baltimore, USA
2 Florida A&M University-Florida State University College of Engineering, Chemical and Biomedical Engineering, Tallahassee, USA
3 Mayo Clinic, Neurosurgery, Rochester, USA
4 Johns Hopkins University School Of Medicine, Orthopaedic Surgery, Baltimore, USA
5 Johns Hopkins University School of Medicine, Biomedical Engineering, Baltimore, USA
6 Johns Hopkins University Whiting School of Engineering, Mechanical Engineering, Baltimore, USA
Introduction: The spine is the most frequent bone metastasis site, with 30% of cancer patients developing symptomatic spinal lesions during their illness. Among the treatment armamentarium for spine tumors, spine stereotactic body radiation therapy (SBRT) is one of the main modalities since it allows the precise and accurate delivery of high-intensity radiation to spinal tumors. However, these harmful doses of radiation may be sufficient to cause toxicity in the surrounding vertebrae, resulting in osteoradionecrosis and an increased risk of vertebral compression fracture (VCF). Although a few studies have reported radiation dosage among the predictive factors for VCF, there is little known regarding how radiation treatment affects vertebral integrity and if there is a significant advantage to using hypofractionated therapies instead of a single-dose treatment. Having an in vivo irradiation model is imperative to answer those questions. For that purpose, we aimed to develop a needed, clinically-relevant animal model to analyze the effects of localized, high-dose radiation on vertebral microstructure and mechanical integrity, utilizing the small animal radiation research platform (SARRP). Materials and Methods: Following anesthesia, male New Zealand white (NZW) rabbits, 8-12 weeks old, were positioned into a padded acrylic tube to maintain an “upright” position, exposing the lumbar region. Rabbits were placed inside the Small Animal Research Radiation Platform (SARRP, Xstrahl) to administer the radiation treatment. In all cases, the L5 vertebrae were located using preliminary X-ray imaging, and a customized collimator was used to irradiate the L5 spine level exclusively. According to the radiation protocol applied (220 kVp, 13 mA), rabbits were divided into three experimental groups: (1) Single 24-Gy dose; (2) Hypofractionated in three 8-Gy doses on three consecutive days; and (3) Nonradiated or Control. Rabbits were euthanized at a 6-month time point post-irradiation, and their lumbar vertebrae harvested for radiological, histological, and biomechanical testing. Results: In the CT micro-architectural analysis, we observed that a localized single-dose of 24 Gy radiation led to loss of vertebral bone volume and decreased trabecular number and a subsequent increase in trabecular spacing and thickness at L5. Hypofractionation of the radiation dose (3 x 8 Gy) similarly led to reduced trabecular number and increased trabecular spacing and thickness, yet preserves normalized bone volume at L5. In the biomechanical testing, single-dose irradiated samples showed lower fracture loads and stiffness compared to those receiving hypofractionated irradiation and non-irradiated controls. Interestingly, hypofractionated and control groups exhibited similar means for fracture load and stiffness. For all samples, bone volume, trabecular number, and spacing were positively correlated with fracture loads and Young's modulus (P < .05). Although hypocellularity was histologically observed in both irradiated groups' bone marrow, only the hypofractionated group conserved bone healing features. Conclusions: Single-dose radiation was detrimental to a greater degree than hypofractionation for the micro-architectural, cellular and biomechanical characteristics of irradiated vertebral bodies. The significant correlation between radiological measurements and biomechanical properties confirmed the reliability of this animal model of radiation-induced VCF.
619
A210: The Spatial and Temporal Expression of Sclerostin and Canonical Wnt Signaling Factors in Maturing Posterolateral Spinal Fusions
Thanh Doan 1 , Mesfin Teklemariam 1 , Sreedhara Sangadala 1 , Scott D. Boden 1 , Hicham Drissi 1 , and Steven Presciutti 12
1 Emory University School of Medicine, Orthopaedic Surgery, Atlanta, USA
2 Atlanta Veteran Affairs Medical Center, Decatur, USA
Introduction: Despite state-of-the-art techniques, spinal pseudarthrosis remains common (10-40%) and is associated with significant morbidity and cost.1 One promising strategy is to enhance canonical Wnt signaling locally in the fusion bed because it positively uncouples bone formation/resorption. Anti-sclerostin treatments have also been shown to result in greater bone volume after spinal fusion.2 Very little, however, is known about sclerostin and canonical Wnt signaling during the fusion process. Material and Methods: Twenty-two adult female New Zealand White rabbits underwent a bilateral posterolateral intertransverse process arthrodesis at L5-L6 using autologous iliac crest bone graft (ICBG).3 Rabbits were euthanized at 1-week (N = 5), 2-weeks (N = 4), 3-weeks (N = 4), 4-weeks (N = 4), and 6-weeks (N = 5) after arthrodesis. Immediately following euthanasia, tissue samples were collected from the decorticated transverse processes (TPs), ICBG between the TPs (Inner Zone) and overlying the TPs (Outer Zone), and paraspinal muscle touching the ICBG. Two rabbits did not undergo surgery (controls), whereby ICBG, L5/6 TPs, and paraspinal muscle were harvested. All tissue was immediately snap-frozen within minutes of euthanasia. High-quality RNA was isolated using a cryogenic tissue homogenizer. Expression of sclerostin and canonical Wnt signaling factors (Wnt3a, LRP6, Gsk3b, β-catenin) were measured in duplicate using real-time qPCR and normalized to GAPDH. Immunohistochemistry using an anti-sclerostin antibody was also performed to determine protein levels temporally. Results: Successful fusion was confirmed at 6 weeks via μCT in 3/5 rabbits, which is consistent with the known fusion rate in this model (66%).3 We identified unique temporal trends in sclerostin gene expression and protein levels in the TPs, Outer Zone, Inner Zone, and muscle. The act of harvesting ICBG caused significantly increased expression of sclerostin, with a >6-fold increase in the Outer and Inner Zones at 1-week (P <.05). The surrounding muscle had a >13-fold increase in sclerostin expression at 3-weeks (P < .05). Sclerostin was also significantly expressed in the TPs at 6-weeks (∼5-fold increase, P < .05), which could be a signal to stop forming bone once the fusion is complete. Wnt3a was the most dynamically expressed Wnt factor, with an almost 20,000-fold increase in the muscle at 1 week and a 500-fold increase in expression in the TPs at 6-weeks (P < .05). Conclusion: This is the first description of how sclerostin levels, and levels of various canonical Wnt signaling factors, are both spatially and temporally dynamically controlled during the maturation of a posterolateral spine fusion mass. This fills an important knowledge gap in our understanding of the basic biology of spinal fusion and provides insight into an understudied regulator of osteogenesis in this setting. Sclerostin and canonical Wnt factors seem to play a role in osteogenesis after spinal arthrodesis and their dynamic expression is regulated differently within specific regions of the maturing fusion mass. Understanding these signaling patterns will be critical in aiding in the design of novel local delivery strategies of biologics that modulate canonical Wnt signaling for the purpose of preventing pseudarthrosis (i.e., determining the specific region of the fusion to be targeted with biologics or determining the optimal timing needed for drug release from its carrier).
580
A211: Bilateral Erector Spinae Plane Block-A Promising Protocol For Post-Operative Pain Relief
Sathish Muthu 1 2 and Kartik Kumar Natarajan 1 3
1 Orthopaedic Research Group, Coimbatore, India, 2 Government Hospital, Velayuthampalayam, Karur, India, 3 Lok Manya Tilak Municipal General Hospital, Mumbai, India
Introduction: Although opioids remain the mainstay of perioperative pain management in spine surgery, inclusion of methods to utilize the non-opioid medications into the multimodal pain control regimens helps to avoid opioid-related side-effects. Dorsal rami innervate all the pain generators following lumbar spine surgery. Hence regional anesthetic techniques like Thoraco Lumbar Interfascial Plane (TLIP) Block, Erector Spinae Plane Block (ESPB) have been developed to address them locally and thereby enhancing postop recovery. There was increasing evidence to support their usage for postoperative pain management but no meta-analyses exist so far to give conclusive evidence for their utilization in spine surgery. Hence, we performed this meta-analysis to analyze the efficacy of bilateral ESPB for postoperative analgesia in lumbar spine surgery from the available evidence in literature so far. Materials and Methods: We conducted independent and duplicate electronic database searches including PubMed, Embase and Cochrane Library till February 2020 for comparative studies analyzing the efficacy of bilateral ESPB for postoperative pain relief in lumbar spine surgeries. Post-operative pain scores, total analgesic consumption, number of patients requiring rescue analgesics, first analgesic requirement time and complications were the outcomes analyzed. Analysis was performed in R platform using OpenMeta (Analyst) software. Results: Four studies including 170 patients (ESPB/Control = 80/90) were included in the analysis. There was a significant pain relief in ESPB group compared to placebo across all timelines such as during immediate post-operative period (P < .001), 4 hours (P = .041), 8 hours (P = .001), 12 hours (P = .038) and 24 hours post-surgery (P = .002). ESPB group showed a significant reduction in number of patients requiring rescue analgesic (P < .001) and total analgesic consumption(P < .001) and post-operative nausea and vomiting (P = .012) compared to controls. ESPB group also had significant prolongation of time for rescue analgesic if needed (P < .001). Conclusion: Bilateral ESPB offers prolonged post-operative pain relief compared to controls, thereby reducing the need for opioid consumption and its related complications. Although our meta-analysis establishes the efficacy of ESPB for postoperative pain relief in spine surgeries, future studies investigating the type of local anesthetic with its volume and concentration need to be done to develop a standard protocol for its routine use in multimodal analgesia employed in spine surgeries.
1417
A212: Anti-Inflammatory Effect of BSP-Resveratrol Membrane for the Prevention of Epidural Fibrosis After Laminectomy
Hsuan-Yu Chen 1 , Tsung-Han Yang 2 , Chih-Wei Chen 3 , Tze Hong Wong 2 , Po-Quang Chen 3 , Ming-Hsiao Hu 3 , Shu-Hua Yang 3 , and Feng Huei Lin 1
1 Institute of Biomedical Engineering, National Taiwan University, Taipei, Taiwan
2 National Taiwan University Hospital, Hsin-Chu Branch, Hsin-Chu City, Taiwan
3 National Taiwan University Hospital, Taipei, Taiwan
Introduction: Laminectomy is a surgical procedure required for the treatment of spinal disorders such as lumbar disk herniation, spinal stenosis, or tumor excision. Although the treatment is effective and relieves neural compression, 8-40% patients suffer from failed back surgery syndrome (FBSS) post laminectomy and 4-9% patients received revision surgery. Material and Methods: An CMC-BSP-Reservatrol membrane would be the material of choice for this purpose, since it could fill an irregular surgical defect and be delivered in a minimally-invasive manner. The objective of this study was to evaluate, in vitro and in vivo, the cytocompatibility and anti-adhesive effect of CMC-BSP-Reservatrol membrane. Different cell types present in the spine were used to test the cytocompatibility of the hydrogel. CMC-BSP-Reservatrol membrane extraction medium had no deleterious effects on neural cells (PC-12), but reduced fibroblasts viability (NIH/3T3). Results: Although CMC-BSP-Reservatrol membrane did not change the release of lactate dehydrogenase from myoblasts (C2C12) and Schwann cells (RSC96), the extraction medium concentration slightly affected the mitochondrial activity of these two cell types. qPCR showed that the CMC-BSP-Reservatrol membrane down-regulated S100a and P4hb expression in NIH/3T3 cells, supporting the hypothesis that the CMC-BSP-Reservatrol membrane might inhibit fibroblast activity. Conclusion: The CMC-BSP-Reservatrol membrane is a promising injectable and thermosensitive material for prevention of post-operative epidural fibrosis.
882
A213: Use of NPY Y1 Selective Antagonist to Suppress Neuropathic Pain
Michelle Tucci 1 , Robert McGuire 2 , and Hamed Benghuzzi 3
1 University of Mississippi Medical Center, Anesthesiology, US, USA
2 University of Mississippi Medical Center, Orthopedics, Jackson, USA
3 Mississippi Academy of Sciences, Jackson, USA
Introduction: Severe pain that is chronic (lasting >3 months) represents a major complication associated with tissue or neuronal injury, and it has become clear these types of injuries produce dramatic alterations in the gene expression of peptidergic neurotransmitters and receptors at the level of the primary afferent neuron, spinal cord, dorsal horn, and brain. The chronic pain state is characterized by persistent long-lasting activation of peripheral nociceptors. Such plastic changes are thought to take the subject from acute to chronic pain. Several neuropeptides and their receptors are expressed in these target regions and contribute to modulating the pain signals. One important neuropeptide, NPY, and its receptor, Y1, appears to be an important mediator of NP. Neuropeptide Y and especially the NPY Y1 receptor (Y1-R) are highly expressed at key sites of pain transmission, including lamina II of the spinal cord dorsal horn, and tissue or nerve injury dramatically alters their expression profiles. Currently, several major classes of analgesics are available for the management of NP, and include antidepressants, anticonvulsants, opioids, and adjuvant analgesics, which have shown incomplete effectiveness and do not target NPY or alter Y1-R density. Targeting NPY or the Y1-R could optimize pain management and minimize the occurrence of side effects associated with current pain treatment strategies. Material and Methods: Sixteen male Sprague Dawley rats were randomized into four equal groups, naïve, CCI +saline, CCI + 100 µg/kg/day gabapentin, and CCI + 10 µg/kg/day NPY 1 receptor antagonist. Von Frey filaments were used to obtain the response latencies to mechanical stimuli pre surgery. Animals underwent unilateral sciatic nerve chronic constriction injury (CCI) and assessed with Von Frey filaments 3 days post-surgery, and drug treatments were started. Latency changes were assessed on days 3, 5 and 7 post drug treatment. Results: The results indictated that rat withdrawal latencies were significantly increased in gabapentin and NPY Y1 receptor antagonist treated animals on days 3, 5, and 7 compared to CCI + saline. By 7 days withdrawal latencies for rats treated with NPY 1 receptor anatagonist were similar to naive control. Conclusion: A 10 µg/kg/day dose of a selective Y1 receptor antagonist had a significantly greater capacity to suppress pain in comparison to gabapentin. Targeting NPY or the Y1-R could optimize pain management and minimize the occurrence of side effects associated with current pain treatment strategies (e.g., dependence, abuse liability) and may be an alternative non-opioid pain.
334
A214: Biomimetic Platelet-Derived Growth Factor Delivery System with Osteoinductive Bone Particles and Adipose-Derived Stem Cells in Biodegradable Tissue-Engineered Grafts for Spinal Fusion
Alexander Perdomo-Pantoja 1 , Alexandra N Rindone 2 , Emma Whitehead 2 , Christina Holmes 3 , Warren L. Grayson 2 , and Timothy F. Witham 1
1 Johns Hopkins University School of Medicine, Neurosurgery - Division of Spine, Baltimore, USA
2 Johns Hopkins University School of Medicine, Biomedical Engineering, Baltimore, USA
3 Florida A&M University-Florida State University College of Engineering, Chemical and Biomedical Engineering, Tallahassee, USA
Introduction: Biodegradable biomaterials are a promising graft material for spinal fusion due to their ability to degrade as new bone tissue grows into the graft while also providing mechanical stability during the early stages of bone healing. A newly designed, biodegradable polycaprolactone-decellularized bone (PCL-DCB) hybrid is desirable for spinal fusion due to its mechanical rigidity and osteoinductivity, but it requires a stem cell source for the bone to regenerate into the material. Pre-clinical studies have demonstrated that incorporation of ex vivo expanded adipose-derived stem cells (ADSCs) into grafting materials enables complete spinal fusion, but their approaches require supraphysiological doses of BMP-2, which can lead to undesirable clinical complications.4Platelet‐derived growth factor‐BB (PDGF) is an attractive alternative to BMP‐2, since it directly promotes the osteogenesis of ADSCs when applied at physiological concentrations. Recently, Rindone et al. developeda biomimetic PDGF delivery system using heparin-conjugated, decellularized bone particles (HC-DCB) that enhances ADSC-mediated bone regeneration in critical-sized murine calvarial defects. In this study, we utilized this promising delivery system for the controlled release of PDGF-BB in 3D-printed PCL-DCB spinal fusion grafts in a rat model. Materials and Methods:ADSCs were isolated from the inguinal fat pads of syngeneic 6-8-week-old Lewis rats and culturedin vitro. When passage 1 (P1) ADSCs reached 80% confluency, cultured-expanded ADSCs (P2) were seeded onto PCL-DCB scaffolds along with HC-DCB particles (40 mg/mL in fibrin) and 20 ug/mL PDGF for subsequent transplantation. Dorsolateral spinal fusion surgery at L4-L5 was performed on Lewis rats divided into 5 experimental groups: [1] PCL only; [2] PCL-DCB + HC-DCB particles; [3] PCL-DCB + HC-DCB particles + PDGF; [4] PCL-DCB + HC-DCB particles + 2.5 x 106 ADSCP2/side; and, [5] PCL-DCB + HC-DCB particles + 2.5x106 ADSCP2/side + PDGF. Fusion was evaluated eight weeks post-surgery. Micro-computed tomography (microCT) images were evaluated to determine CT fusion status and fusion mass volume. Histology and immunohistochemistry were performed to assess new bone quality. Results: MicroCT imaging analyses revealed bone formation along the scaffolds struts for all PCL-DCB groups. Additionally, all PCL-DCB groups created fusion masses between the L4-L5 transverse processes (TPs). By contrast, [1] PCL only scaffolds did not form bone. Of all the PCL-DCB groups, the [3] PCL-DCB + HC-DCB particles + PDGF group significantly displayed a higher CT volume (P < .05). Furthermore, histological staining demonstrated that PCL-DCB grafts were well-integrated with the host TPs in all groups. A more significant bone deposition was found in the graft-TP interface in the treated groups ([3], [4], and [5]) compared to [2] PCL-DCB + HC-DCB particles, being more remarkable in the [3] PCL-DCB + HC-DCB particles + PDGF group. Expression of Runx2, osteocalcin, and CD31 was observed in the treated groups ([3], [4], and [5]). Conclusions: We demonstrated that biodegradable PCL-DCB grafts enable spinal fusion when combined with osteoinductive HC-DCB particles. Although the presence of both cells and growth factors was not required to achieve spinal fusion in PCL-DCB + HC-DCB grafts,PDGF-BB enhanced bone formation when added to these grafts.
800
A215: Validity of Scoliotic Discs as Controls for Molecular Research in Intervertebral Disc Disorders
Sri Vijay Anand KS 1 , Shanmuganathan Rajasekaran 1 , Dilip Chand Raja Soundararajan 1 , Chitraa Tangavel 2 , Sharon Miracle Nayagam 2 , Sunmathi R 2 , Raveendran M 3 , Ajoy P Shetty 1 , and Rishi Kanna 1 , Pushpa BT 4
1 Ganga Hospital, Department of Spine Surgery, Coimbatore, India
2 Ganga Research Centre, Department of Proteomics, Coimbatore, India
3 Tamilnadu Agricultural University, Department of Biotechnology, Coimbatore, India
4 Ganga Hospital, Department of Radiology, Coimbatore, India
Introduction: Despite being a highly researched subject, the studies on etio-pathogenesis have been inconclusive. One of the primary reasons for elusiveness being, lack of appropriate controls for making a precise comparison with degenerated discs. Discs from scoliosis surgery is a common control used in molecular studies of disc disorders. This study aims to compare the validity of scoliotic discs as controls by comparing it against MRI normal discs from voluntary organ donors and establish 'True Controls' that can be utilized for future Intervertebral disc (IVD) research. Materials and Methods: After appropriate ethical clearance and consent, nucleus pulposus of Eight MRI normal discs from eight brain dead voluntary organ donors (ND) and eight scoliotic discs (SD) from three patients who underwent anterior surgery for adolescent idiopathic scoliosis were harvested under sterile precautions. After protein extraction, prefractionation and in-gel tryptic digestion, the extracted peptides were subjected to tandem mass spectrometry. The raw data were subjected to further bioinformatic analysis to understand the patho-mechanisms involved. Results: Mass spectrometry identified a total of 235 proteins in ND and 438 proteins in the SD group and 157 proteins common to both group. About 78 (15.31%) proteins were found only in the ND group, and 281 (54.45%) were found only in the SD group. Proteins involved in Extracellular matrix integrity (Versican, Keratins KRT6A, KRT14, KRT5 and KRT 13A1, A-kinase anchor protein 13, Coagulation factor XIII A chain, Proteoglycan 4) and proteins involved in transcription and DNA repair (Von Willebrand factor A domain-containing 3B, Eukaryotic initiation factor 2B, Histone H4, Leukocyte Cell-Derived Chemotaxin 2) were found to be down-regulated in SD. Inflammatory proteins (C3, C1S), and oxidative stress response proteins (Peroxiredoxin-2,6, Catalase, Myeloperoxidase, Apolipoprotein E) were found to be up-regulated in SD. These changes were reflected at the pathway level also. Conclusion: Our study found that scoliotic discs have an abundance of inflammatory, oxidative stress response proteins. Whereas, these proteins were either absent or downregulated in the MRI normal discs from voluntary organ indicating a more biologically inert state. These findings establish MRI normal discs from voluntary organ donors as the 'true' control for molecular studies in IVD research and recommend it for future studies.
569
A216: Intra-Operative Topical Vancomycin Powder Application-Is the Practise Safe in Paediatric Spine Surgeries?
Sathish Muthu 1 2 and Girinivasan Chellamuthu 1 3
1 Orthopaedic Research Group, Coimbatore, India
2 Government Hospital, Velayuthampalayam, Karur, India
3 Ganga Hospitals, Orthopaedic Trauma Surgery, Coimbatore, India
Introdcution: Various methods have been developed and implemented to prevent SSI in the paediatric population. The practices vary among different groups of surgeons based on their training and expertise. One such practice is the application of Topical Vancomycin Powder (TVP) in the surgical wound before closure. Vancomycin powder is increasingly used off-label as TVP to prevent infection in spine surgeries. Uncertainty exists on its safety and usefulness in pediatric population. Hence, we aim to systematically review the available articles on TVP use in pediatric spine surgeries exploring the usefulness and safety of such practice. Materials and Methods: We conducted independent and duplicate electronic database search in PubMed, Embase and Cochrane Library till March 2020 to identify all relevant literature on the use of TVP for pediatric spine surgeries. Surgical Site Infection (SSI) rate, specific reported complications, reoperation rate, microbial flora pattern in reported SSI and safety profile were the outcomes analyzed. Analysis was performed in R platform using OpenMeta[Analyst] software. Results: No prospective studies were available to evaluate the use of TVP in pediatric spine surgeries for the prevention of SSIs. Neither standardized protocol nor drug dosage or safety profile was established for pediatric use. Three retrospective cohort studies including 824 patients (TVP/Control = 400/424) were included in the meta-analysis. There was a low-quality evidence suggesting no significant difference between the two groups in SSI rate (RR = .474, 95% CI [0.106, 2.112], P = .327) with significant heterogeneity (I2 = 70.14, P = .035). TVP group showed a significant benefit on cost-analysis in one of the included studies. However, TVP did not prevent gram-negative co-infection on SSI in the TVP group. Conclusion: TVP does not qualify to be recommended as a safe and useful option to prevent SSI following pediatric spine surgeries from the literature available at present. High-quality prospective interventional studies are needed to arrive at a consensus on its use along with appropriate dosage and method of application.
OP25: Lumbar Degeneration
799
A217: Lessing PROM Burdens Via Machine Learning
Gregory Schroeder 1 , Andrea Wood 2 , and Otho Plummer 2
1 The Rothman Institute at Thomas Jefferson University, Philadelphia, USA
2 OBERD, Columbia, USA
Introduction: Clearly and concisely understanding patient conditions is a universal goal of physicians. Patient Reported Outcomes Measures (PROMs) are employed as tools to scientifically gain this insight as efficiently as possible in order to optimize medical consultations. While PROMs alone are generally not burdensome, they are often administered directly following a substantial amount of other registration, past medical and history of present illness paperwork. Attempts to improve the situation have been made by administering shorter PROM forms. Computer Adaptive Testing (CAT) is a strategy that dynamically selects the most appropriate next question based on previous response and in turn, reduces the amount of questions required to complete the form session. Unnecessary questions are omitted based on the patient’s unique current condition and a valid score is still effectively assigned via this more concentrated technique. Examples of CAT include PROMIS and PediCat instruments, both of which rely on Item Response Theory (IRT). Recent publications have validated a machine learning (ML) method which voids the need for calibrated item banks and permits CAT application to historically popular PROM instruments. Our aim is to expand on such ML approaches to further explore question reduction. Material and Methods: ML CAT methods have yielded up to fifty-percent savings in questions, while having a correlation coefficient >.98 with the full questionnaire. The algorithms sought maximum accuracy, and question reduction occurred as a collateral benefit. This work may be extended by focusing on lowering question count to the absolute extent possible while still maintaining score integrity for the Neck Disability Index (NDI) and Oswestry Disability Index (ODI) instruments. Data analysts examined the ML algorithm and CAT results for NDI and ODI, honing in on questions revealed to be less significant for score accuracy. The ML CAT model was adjusted based on new findings and reapplied to the data set. The resulting system, in view of its increased speed of use, is informally called CAT+ or Cheetah. Results: The full form NDI asks 10 questions. The NDI (ML) CAT managed to obtain a correlation coefficient >.97 with an average of 5.92 questions per session. The NDI Cheetah obtained a correlation coefficient >.96 with an average of 4.97 questions per session. See Table 1 for statistical details. The full form ODI asks 10 questions. The ODI (ML) CAT averaged 5.53 questions per session with a correlation coefficient >.98. The ODI Cheetah averaged 4.36 questions per session with a correlation coefficient >.96. See Table 2 for statistical details. Conclusion: The CAT method verified for a number of legacy PROMs shows consistent findings when applied to NDI and ODI instruments. Still, our research demonstrates that previously used ML methods ask questions that produce minimal gains in terms of score accuracy. These questions can also be eliminated to further shorten NDI and ODI form sessions through careful analysis and advanced ML CAT techniques, thus lessening patient form burden.
1360
A218: Preoperative Sagittal Imbalance Associated with Improved Radiographic and Clinical Outcomes After MIS TLIF for Degenerative Spondylolisthesis
Andre Samuel 1 , Catherine Himo Gang 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
Introduction: Existing literature demonstrates the importance of restoring sagittal balance for long-segment lumbar fusion. However, it remains to be seen how sagittal balance relates to outcomes after short segment minimally invasive fusions. Specifically no previous studies have stratified patients based on preoperative PI-LL mismatch to identify differences in radiographic and clinical outcomes. Methods: 56 consecutive patients undergoing 1- or 2- level MIS TLIF for degenerative spondylolisthesis were grouped based on preoperative PI-LL mismatch greater than or less than 10°. Postoperative improvement in radiographic sagittal parameters and patient reported outcome measures (PROMs) were assessed compared between groups at mean follow up of 41 weeks. Results: A total of 25 patients (44.6%) had a preoperative PI-LL (pelvic incidence - lumbar lordosis) mismatch of > 10°. Preoperative pelvic incidence (67.3° vs 53.3°) and pelvic tilt (30.0° vs 17.5°) were greater in patients with preoperative PI-LL mismatch (P <. 05). There were no significant differences in preoperative PROMs between groups. Postoperatively, there was a greater decrease in PI-LL mismatch (-7.2° vs + 1.7°) and SVA (-16.4mm vs +12.6mm) in patients with preoperative sagittal imbalance (P < .05), but not with pelvic tilt (PT). Patients had statistically significant improvements in all PROMs in both groups, with no significant differences between groups. In multivariate analysis, preoperative SVA > 40mm was associated with increased odds of achieving MCID (minimum clinically important difference) in PROMIS® (odds ratio: 14.38, P = .03). However, preoperative PI-LL > 10° and PT > 20° were not associated with increased MCID for any measured PROMs. Conclusion: MIS TLIF results in good clinical outcomes despite preoperative radiographic sagittal parameters. However, patients with preoperative sagittal imbalance may benefit from greater improvement in both radiographic and clinical outcomes.
1559
A219: Sagittal Balance in Short-Segment Decompression and Fusion for the Management of Degenerative Lumbar and Sacral Spine Stenosis
Valerii Serikov 1 , Vadim Manukovsky 1 , Vissarionov Sergey 2 , Irina Afanaseva 3 , and Tahir Tamaev 1
1 Saint-Petersburg I.I. Dzhanelidze Research Institute of Emergency Medicine, Neurosurgery, Saint-Petersburg, Russian Federation
2 H.Turner National Medical Research Center for Сhildren’s Orthopedics and Trauma Surgery, Pushkin, Saint-Petersburg, Russian Federation
3 Saint-Petersburg I.I. Dzhanelidze Research Institute of Emergency Medicine, Diagnostics and Imaging, Saint-Petersburg, Russian Federation
Introduction: The role of the sagittal balance in surgical treatment of diseases and injuries of spine becomes more and more actual and important every year. Sagittal profile balance influence on quality of patients life has been noted in many studies. We assessed the effect of sagittal profile parameters correction during short-segment decompression with stabilization on quality of patients life with degenerative stenosis of the lumbar and sacral spine. Material and Methods: We present the results of a retro-prospective cohort study of 60 patients with clinically significant degenerative stenosis (Schizas grade C-D) at L3-S1 levels. The follow-up period was 12 months. Patients were divided into 2 groups. The control retrospective group consisted of 30 people. These patients underwent treatment of degenerative stenosis with stabilization without taking into account the sagittal balance. In the second group, when stabilizing spine, lordosis and sagittal profile were corrected according to the FBI formula (FBI = C7TA + FOA + PTCA). The average age in the groups was 47.1 and 50.3, respectively. All patients assessed pain syndrome on a VAS scale before surgery, in the first 10 days and at 1.5, 3, 6, 9, 12 months after surgery. Patients life quality was assessed using the ODI and RDQ scales at the same time as assessment of pain syndrome. Results: There were no statistically significant differences in gender, age, levels and number of affected levels of spine in the study groups. During the analysis, average correction volume in the second group was 13,4 degrees. There were statistically significant differences in pain syndrome dynamics and life quality between study groups during entire observation period. After 12 months of observation in the second group of the study, there was a significant decrease in the level of pain syndrome according to VAS (H = 215,5 P < .001), an improvement of life quality according to the RDQ (U = 238 P < .001) and ODI (U = 158,5 P < .001) scales. Conclusion: Correction of lumbar lordosis and sagittal profile even with short-segment fixation in patients with degenerative lumbar and sacral spine stenosis leads to a significant improvement in life quality and a decline of patients pain syndrome in up to 12 months.
1859
A220: Isovue Contrast for Intraoperative Assessment of Discectomy Quality in Tlif: A Preliminary Report of A Prospective Randomized Controlled Trial
Athan Zavras 1 , David Rossi 1 , Michael Nolte 1 , Nicholas Shepard 1 , Kern Singh 1 , and Matthew Colman 1
1 Rush University Medical Center, Orthopedic Surgery, Chicago, USA
Introduction: Transforaminal lumbar interbody fusion (TLIF) allows for increased fusion biology, stability, and the capacity to provide intersegmental manipulation when treating instability and deformity of the lumbar spine. Certain TLIF techniques rely on interbody arthrodesis as the primary source of arthrodesis, making the extent and quality of endplate preparation and discectomy critical to successful fusion. However, prior studies have demonstrated that even under ideal ex-vivo conditions, the extent of discectomy is surprisingly low. This study aimed to develop an effective technique for intraoperative quantitative and qualitative feedback during discectomy and endplate preparation in TLIF. Materials and Methods:This study is a prospective, randomized, controlled trial that began enrolment in 2019 of patients undergoing 1-2 level TLIF for low-grade spondylolisthesis with the same surgeon. Patients included in this report had a minimum 6-month follow-up. The surgeon completed the endplate preparation and discectomy via standard technique, at which time ISOVUE-300M contrast was administered via spinal needle into the disc space and orthogonal radiographs were obtained. Patients were randomized into a control (OBSERVATION) and investigational group (FEEDBACK). The case proceeded as usual with grafting and cage insertion in OBSERVATION, while contrast imaging guided further disc preparation in FEEDBACK, after which the disc was re-imaged with ISOVUE. The surface area and clearance density of preparation was calculated from intraoperative radiographs. The ABC/2 formula was applied for volumetric measurements of the ellipsoid disc preparations. Other primary endpoints included clinical improvement on patient-reported outcomes (PROs), disc height correction, parameters of spinopelvic alignment, and radiographic or CT evidence of arthrodesis. Differences between cohorts were identified using univariate statistics. Significancewas set toP <.05. Results: Twelve patients were randomized into OBSERVATION and 10 into FEEDBACK. Initial preparation showed no differences between cohorts in the surface area or clearance density of the prepared superior or inferior endplates. The volume of disc space cleared did not differ. After additional preparation in FEEDBACK, final pre-fusion status differed significantly. Clearance density was greater in FEEDBACK compared to OBSERVATION at the superior (90.39 ± 2.41% vs 71.62 ± 7.47%,P <.001) and inferior endplates (89.92 ± 3.13% vs 73.92 ± 6.03%,P <.001). The percent of endplate surface area prepared was also greater in FEEDBACK at the superior (61.49 ± 14.58% vs 37.30 ± 15.63%,P =.001) and inferior endplates (62.28 ± 8.86% vs 42.60 ± 14.04%,P =.001), while the percent of disc volume cleared showed superior results in this group (90.89 ± 6.53% vs 57.63 ± 22.82%,P <.001). Arthrodesis was observed in 100% of FEEDBACK compared to 83.30% of OBSERVATION patients (P =.296), as assessed using Bridwell radiographic criteria, or CT when available. There were no differences in subsidence, spinopelvic correction, or postoperative PROs. Conclusion:Additional endplate preparation and discectomy following ISOVUE in TLIF showed several benefits. There were significant increases in superior and inferior endplate clearance density, percent of endplate surface area prepared, and percent of disc volume cleared. Although the higher percentage of arthrodesis in FEEDBACK was not statistically significant, further investigation of a larger data set may elucidate the impact on arthrodesis and other important clinical endpoints.
731
A221: Long-term outcomes in in cauda equina syndrome. Measurement of core outcomes using validated questionnaires
Thomas Barker1, Lennel Lutchman1, Nick Steele1, am rai1, andrew cook1, girish swamy1, and robert crawford1
1 Norfolk and Norwich University Hospital, Trauma and Orthopaedics, Norwich, United Kingdom
Introduction: Cauda Equina Syndrome (CES) is a relatively uncommon condition that can be associated with long-term autonomic dysfunction and chronic severe lower back pain. Historical studies have had either small numbers of patients, short periods of follow up, or did not use validated methods of assessing patient reported outcomes. In January 2020 a core outcome set (COS) for CES were defined by international consensus among key stakeholders. These measures include autonomic function (bowel, bladder, sexual function, and genital/perineal sensation), non-autonomic function (strength, pain, complications) and quality of life. This study aims to assess the long-term outcomes of patients treated for CES, using validated questionnaires. Material and Methods: Institution approval and Caldecott approval was granted for the study. A retrospective review of a prospectively collected database of patients treated for CES was performed. All patients had undergone surgical decompression for acute CES secondary to intervertebral disc prolapse at our institution between January 2007 and December 2019. Patients were included only of they presented with clinical features compatible with Incomplete Cauda Equina Syndrome (CESI) or Cauda Equina Syndrome with retention (CESR) and had MRI confirmation of a large lumbar disc herniation which was occluding the majority of the spinal canal. The time from onset of autonomic dysfunction symptoms to time of surgery and the reason for any delay was recorded. All patients provided written consent of their willingness to participate in the study and completed a series of validated questionnaires that evaluated the core outcome set. These included the Oswestry Disability Index (ODI), EQ-5D, Qualiveen urinary function questionnaire, Neurogenic Bowel Dysfunction score and Arizona Sexual Experiences Scale. Results: A cohort of 86 patients was identified over the study period. 42 were male and 44 female. 61 patients had CESI and 25 CESR. The average duration of follow-up was 59.7 months (range 11 to 182, SD 42.4). Only twenty-five patients had surgical decompression within 48 hours of symptom onset. The most frequent reason for delay was a delay in patient presentation, with only a few exceptions. Persistent severe back pain was a frequent complaint. Many patients had undergone further MRI imaging or pain intervention treatment for chronic, severe back pain. Persistent autonomic dysfunction was present in some patients and we analysed the distribution of these symptoms between the CESI and CESR groups. Conclusion: To our knowledge, this study reports the longest follow-up of patients with CES and is the first to use validated patient-reported outcome measures to assess the Core Outcome Set for CES. Persistent severe back pain and on-going autonomic dysfunction was frequently noted in this cohort of 86 patients at a mean follow-up of five years.
1197
A222: Body Mass Index Impact on Clinical Outcomes After Minimally Invasive Extreme Lateral Interbody Fusion
Carlos De La Torre 1 and Khai Lam 1
1 London Bridge Hospital, London, United Kingdom
Introduction and Purpose: The minimally invasive extreme lateral interbody fusion (ELIF) has increasingly been used in the treatment of lumbar pathology. The perceived benefits suggest it will continue to play an important long-term role in the treatment of these disorders. It has been proposed that patients baseline anthropomorphic characteristics may influence the clinical outcomes following ELIF. The purpose of this study was to determine the effect of Body Mass Index (BMI) on the clinical outcomes in patients treated with ELIF. Materials and Methods: Between January 2013 and January 2020, we identified 142 consecutive patients undergoing ELIF for lumbar pathology. Patient related outcome measures (PROMS) were collected in 104 patients preoperatively, and up to 12 months postoperatively. PROMS included Oswestry Disability Index (ODI), Visual Analog Scale (VAS) for both back (BP) and leg pain (LP) and SF-36. Based in the WHO nutritional status classification we categorised patients as Normal, Pre-obese and Obese according to their BMI (18.5-24.9, 25-29.9, >30 kg/m2 respectively). Results: There were 56% female and 44% male patients with a mean age of 56 (26-84) years. 37 patients were identified as normal, 40 as pre-obese and 27 as obese. For ODI, statistically significant mean improvements from pre-operative to last follow-up were 23.9 ± 21.2 (P < .0001) for normal weight, 17.8 ± 23.8 (P < .0001) for pre-obesity weight and 16.2 ± 4.32 (P < .0001) for obesity weight. For VAS BP, significant mean improvements from pre-operative to last follow-up were 3.4 ± 3.1 (P < .0001) for normal weight, 3.7 ± 3.13 (P < .0001) for pre-obesity weight and 3.6 ± 3.5 (P < .0001) for obesity weight. For VAS LP the mean improvements were 3.4 ± 3.14 (P < .0001) for normal weight, 3.7 ± 3.08 (P < .0001) for pre-obesity weight and 3.5 ± 3.3 (P < .0001) for obesity weight. For the PCS domain of SF-36 the mean improvements were 10.7 ± 14.2 (P < .0007) for normal weight, 6.14 ± 12.3 (P < .02) for pre-obesity weight and 7.2 ± 10.7 (P < .01) for obesity weight. For the MCS domain 7.7 ± 12.4 (P < .003) for normal weight, 4.5 ± 13.3 (P < .04) for pre-obesity weight and 5.7 ± 9.6 (P < .02) for obesity weight. Based on a previous study1 the percentage of patients that met the MCID for ODI was 62%, 50% and 60% for normal, pre-obese and obese respectively. For VAS BP was 75%, 79% and 72% for normal, pre-obese and obese respectively. For VAS LP was 54%, 51% and 60% for normal, pre-obese and obese respectively. Conclusions: Our analysis revealed that BMI did not affect the mean outcome scores in patients who underwent surgery of the lumbar spine using the ELIF approach. Comparison between baseline and last follow-up results demonstrated a similar improvement in all BMI groups and showed statistically significant improvements in all aspect of PROMS and MCID. These results corroborate that the ELIF approach is an effective and safe treatment for lumbar pathology regardless of BMI.
624
A223: Post-Operative Outcomes After Degenerative Lumbar Spine Surgery in Rheumatoid Arthritis Patients - A Propensity Score Matched Analysis
So Kato 1 , Hideki Nakamoto 1 , Yasushi Oshima 1 , Yuki Taniguchi 1 , Yoshitaka Matsubayashi 1 , Toru Doi 1 , Naohiro Kawamura 2 , Nobuhiro Hara 3 , Akiro Higashikawa 4 , Takashi Ono 5 , and Yujiro Takeshita 6
1 The University of Tokyo, Tokyo, Japan
2 Japanese Red Cross Medical Center, Tokyo, Japan
3 Musashino Red Cross Hospital, Tokyo, Japan
4 Kanto Rosai Hospital, Kawasaki, Japan
5 JCHO Tokyo Shinjuku Medical Center, Tokyo, Japan
6 Yokohama Rosai Hospital, Yokohama, Japan
Introduction: Despite that treatment options for rheumatoid arthritis (RA) have significantly evolved with the introduction of biologic agents, degenerative lumbar disease in RA patients still remains a major challenge. The risk of adverse events and reoperation is known to be high in RA patients. However, well-controlled comparisons between RA patients and non-RA counterparts have not yet been conducted in the literature and the current evidence is scarce. The object of the present study was to compare post-operative outcomes after lumbar spine surgery between RA and non-RA patients using propensity score matched analysis. Material and Methods: Patients who underwent primary posterior spine surgery for degenerative lumbar disease in our prospective multicenter study group between 2017 and 2019 and completed pre- and post-operative questionnaires for patient-reported outcome measures were enrolled. Demographic data including age, sex, body mass index (BMI), American Society of Anesthesiologists Classification (ASA), diabetes mellitus, steroid use, smoking, operative spinal level, fusion surgery were investigated and these factors were used to calculate propensity score for RA diagnosis. One-to-one matching was performed and 1-year post-operative outcomes (numerical rating scale [NRS] for back pain, Oswestry Disability Index [ODI], EuroQOL [EQ5D], Short Form-12 [SF-12], Core Outcome Measures Index for theback [COMI]) and 30-day complication rates were compared between RA and non-RA patients. Results: Among 4545 patients included, 78 had RA (1.7%). In comparison to non-RA patients, RA patients were older (71 vs 64 yrs, P < .01), leaner (BMI 23 vs 24, P = .02) and more likely to be female (82% vs 40%, P < .01), diabetic (22% vs 14%, P < .01), and steroid user (51% vs 2%, P < .01). ASA was greater (2.0 vs 1.9, P < .01) and fusion surgery was more commonly performed (55% vs 27%, P < .01) with greater spinal levels involved in surgery (3.5 vs 2.7, P < .01). Propensity matching generated 62 pairs of RA and non-RA patients who underwent posterior lumbar surgery. After background adjustment, it was revealed that there were no statistically significant differences in post-operative NRS (2.8 vs 3.5, P = .32), ODI (24.6 vs 26.9, P = .79), EQ5D (0.68 vs 0.71, P = .43), SF-12 physical component score (32.1 vs 32.7, P = .71) or COMI (3.2 vs 3.2, P = .98). 30-day complication rate (10% vs 8%, P = .75) did not differ either between the two groups. Conclusion: Diagnosis of RA was found not to have negative impact by itself on post-operative outcomes after posterior surgery for degenerative lumbar disease.
1632
A224: Relation Between Patient Perceived Surgical Indication, Fullfilment of Expectations and Functional Outcome in Patients Undergoing Spine Surgery
Sara Diniz1 2, Pedro Manuel Mendes dos Santos2, Carolina Luísa Lemos2, and Ricardo Rodrigues-Pinto1 2
1 Centro Hospitalar Universitário do Porto. Portugal, Spinal Unit, Department of Orthopaedics, Porto, Portugal
2 Instituto de Ciências Biomedicas Abel Salazar, Porto, Portugal
Introduction: Patient expectations regarding surgery have been shown to affect self-reported clinical outcome. In spinal surgery, misconceptions about surgery outcome are frequent which may lead to patient dissatisfaction. The objective of this study was to understand patient misconceptions relatively to the self-perceived surgical indication and how they can influence patient satisfaction and functional outcomes. Material and Methods: From an initial pool of 316 patients, 149 were included in the study. A questionnaire was retrospectively applied to assess patient-perceived surgical indication, fulfilment of expectations and subjective improvement with surgery. Additionally, two validated questionnaires (Neck Disability Index (NDI) and Oswestry Disability Index (ODI) for were also used to assess objective clinical outcome. Results: Patients submitted to lumbar surgery were 2984 times more likely to report fulfilment of expectations and those reporting appendicular symptoms were 2675 times more likely to report fulfilment of expectations than those submitted to cervical surgery or reporting axial symptoms, respectively. Being male was the only factor associated with subjective improvement. Among cervical pathologies, patients with cervical myelopathy reported higher subjective improvement than patients with cervical disc herniation. NDI was significantly lower in patients reporting fulfilment of expectations with cervical surgery. Patients undergoing lumbar surgery with predominant appendicular symptoms had lower disability than those with predominant axial symptoms (39.34 vs 29.98). Patients who reported fulfilment of expectations had lower disability as did those who reported a subjective improvement after surgery. Conclusion: This study showed that patients with appendicular symptoms and those undergoing lumbar surgery were more likely to report subjective improvement with spinal surgery. A surprisingly high percentage of patients reported axial symptoms as the main indication for undergoing surgery (38.26%). Misconceptions about spine surgery can lead to unrealistic expectations towards treatment and ultimately lead to dissatisfaction with surgery. This underlines the importance of the communication between surgeons and patients.
247
A225: Nose to back: spheroids derived from human nasal chondrocytes for nucleus pulpous repair
Jesil Kasamkattil 1 2 , Anna Gryadunova 2 3 , Max Hans Peter Gay 1 2 , Vladimir Mironov 3 , Stefan Schären 1 , Ivan Martin 2 , Andrea Barbero 2 , Olga Krupkova 1 2 , and Arne Mehrkens 1
1 Spine Surgery, University Hospital Basel, Basel, Switzerland
2 Tissue Engineering, Department of Biomedicine, University of Basel & University Hospital Basel, Basel, Switzerland
3 Institute for Regenerative Medicine, I.M. Sechenov First Moscow State Medical University, Moscow, Moscow, Russian Federation
Introduction: Autologous nasal chondrocytes (NC) could be an excellent source for nucleus pulposus (NP) repair/regeneration. Indeed, NC possess large cartilage-regenerative capacity and survive in harsh NP microenvironment better than traditionally used MSCs (Gay et al., 2019). We aim this in vitro study at analyzing the therapeutic potential of NC spheroids (NCS), namely their capacity for injectability, NP-like matrix accumulation, and integration in conditions simulating degenerative disc disease (DDD). Material and Methods: Human NC (n = 5) were cultured as spheroids with different culture supplements for 1-7 days. Injectability (size, shape) and biosynthetic potential of NCS (biochemical content, gene expression, proliferation, elastic modulus) were evaluated at each time point. Human NP cells (n = 3) were cultured as spheroids for up to 14 days. DDD mimicking conditions (inflammation, acidity, low glucose, hypoxia) were introduced and NCS-NP fusion kinetics was monitored for 4 days (microscopy/image analysis). Anabolic and catabolic responses of NCS vs NC single-cell suspension were assessed histologically, biochemically, and by ELISA. Results: Non-adhesive technology allowed the fabrication of NCS compatible with a common spinal needle (<600 µm). NCS cultured with different supplements for 1-7 days upregulated aggrecan and collagen type II expression and accumulated GAG and total collagen (P < .05). In DDD mimicking conditions, NCS performed superior to NC single-cell suspension in terms of cell viability and catabolic shift (IL-8 release, P < .05). The kinetics of NCS-NP fusion was not impaired by the DDD mimicking conditions. Interestingly, “growth” culture supplements facilitated fusion with NP tissue, while “chondrogenic” supplements increased elastic modulus (P < .05). Conclusion: Our data indicate that NC cultured as spheroids can produce NP-compatible matrix, develop biomechanical properties similar to NP tissue, and possess the capacity to integrate within degenerated NP. Moreover, specific NCS properties are potentially tunable by culture supplements. These results need to be verified in a whole disc organ culture bioreactor, towards demonstration of the functionality of NC for scaffold-free NP repair.
OP26: Trauma-Thoracolumbar 1
1463
A226: AO Spine PROST (Patient Reported Outcome Spine Trauma) - Validation of the English and Dutch Versions
Said Sadiqi 1 , Cumhur Oner 1 , and AO Spine Knowledge Forum Trauma 2
1 University Medical Center Utrecht, Department of Orthopaedics, Utrecht, The Netherland
2 AO Foundation, Davos, Switzerland
Introduction: No outcome instrument was specifically designed for traumatic spinal column injury patients, making it difficult to measure the effect size of various treatment options. The AO Spine Knowledge Forum Trauma initiated a project and developed the Patient Reported Outcome Spine Trauma (AO Spine PROST) consisting of 19 items. The psychometric properties of the English (ENG) and Dutch (NL) language versions of the tool were investigated in an international multicenter validation study. Material and Methods: Patients were recruited from four level-1 trauma centers from North America and the Netherlands. The study consisted of 3 parts: cross-sectional, test-retest, and responsiveness. For concurrent validity, next to AO Spine PROST also SF-36 was filled out by patients. Patient characteristics were analyzed using descriptive statistics. Floor and ceiling effects as well as the number of inapplicable and missing questions were analyzed for content validity. Cronbach’s α and item-total correlation coefficients (itcc) were calculated for internal consistency. Spearman correlation tests were performed within AO Spine PROST items and in correlation to SF-36. Test-retest reliability was assessed using Intraclass Correlation Coefficients (ICC). Responsiveness of the Dutch version was assessed by calculating effect sizes (ES) and standardized response mean (SRM). Factor analysis was performed to explore any dimensions within AO Spine PROST. Results: Out of 179 and 196 enrolled patients, 163 (91.1%) and 162 (82.7%) were included in the ENG and NL validation study, respectively. Content validity showed good results, and no floor and ceiling effects were seen. The internal consistency was excellent (ENG: Cronbach’s α = .97; itcc 0.50-0.90, NL: Cronbach’s α = .96, itcc 0.50-0.86), with also good Spearman correlations (ENG: 0.29-0.85, NL 0.25-0.79). Also test-retest reliability was excellent (ENG: ICC = .97, NL: ICC = .92). The strongest correlations of AO Spine PROST with SF-36 were seen with the physical components (0.69-0.82; P < .001). Factor analysis revealed 2 possible dimensions (Eigenvalues >1), explaining 75.7% (ENG) and 65.4% (NL) of variance. Concerning responsiveness analysis, very good results were seen with ES = 1.81 and SRM = 2.03 (P < .001). Conclusion: Very satisfactory results were obtained for reliability, validity and responsiveness of the English and Dutch versions of the AO Spine PROST, a disease-specific patient-reported outcome measure for traumatic spinal column injury patients. It is considered as a valuable tool, and has the potential to contribute to the reduction of ongoing controversies in spine trauma care.
224
A227: Ability and Limits of Kyphoplasty to Stabilise Post Traumatic Segmental Instability
Oliver Riesenbeck 1 , Niklas Czarnowski 1 , Michael Raschke 1 , and René Hartensuer 1
1 University of Muenster, Department of Trauma-, Hand- and Reconstructive Surgery, Muenster, Germany
Introduction: Several case series in the literature suggest that kyphoplasty may be an option to stabilize segmental instability after traumatic vertebral body fractures. However, this approach contradicts the classical biomechanical idea of segmental instability after injury to the central column. The aim of this study is to investigate the effect of intravertebral vertebral reconstruction using kyphoplasty to stabilize posttraumatic segmental instability with a robotic spine tester. Material and Methods: The intact kinematic values of 14 osteoporotic human spine (TH11-L3) were recorded using a robot-based spinal cord tester in combination with active 3D motion tracking with and without tracking bias and used as a baseline. After standardized induction of incomplete burst fracture (AOS A3) of L1, the kinetic test was repeated to assess posttraumatic values. The fractured vertebra (L1) was then treated by kyphoplasty. Kinematic values of each FSU were examined after kyphoplasty. The following results focus on the injured plane (TH12 - L1). Results: The experimental fracture situation resulted in a significantly increased range of motion (ROM) of the TH12 - L1 level for extension/flexion, lateral bending, and axial rotation. The increase in ROM for axial rotation was 201% (P = .001), for extension/flexion 132% (P = .0002), and for lateral bending 277% (P = .0002) of intact kinematic values. After kyphoplasty a significant decrease of the posttraumatic instability TH12 - L1 was observed for all three directions of movement. The ROM reduced to 80% (P = .002) for axial rotation, 90% (P = .0002) for extension flexion, and 71% (P = .0002) for lateral bending. However, for all three directions of movement, the original intact values could not be restored, and there was a significant remaining increase in the ROM compared to the values before the injury. Compared with intact values, ROM increased by 161% (P = .002) with axial rotation, 120% with extension flexion (P = .001), and 197% with lateral bending (P = .0002). Conclusion: Kyphoplasty seems to have the potential to reduce segmental instability after trauma. However, in the model presented, intravertebral reconstruction failed to restore intact levels and significant instability persisted. These observations may help understand the stabilizing effect of kyphoplasty, but they do not answer how much stabilization gain is needed to achieve good clinical outcomes. The observed residual instability after kyphoplasty suggests that this treatment offers limited opportunities to stabilize traumatic segmental instability.
1721
A228: Is the AO Spine Thoracolumbar Injury Classification System Reliable and Practical? A Systematic Review
Zion Hwang 1 , James Houston 2 , Evangelos Fragakis 2 , Cristina Lupu 2 , Jason Bernard 2 , Timothy Bishop 2 , and Darren Lui 2
1 St. George's University of London, London, United Kingdom
2 St. George's Hospital, Trauma and Orthopaedics, London, United Kingdom
Introduction: Controversy surrounding the classification of thoracolumbar injuries has given rise to various classification systems over the years, including the most recent AOSpine Thoracolumbar Injury Classification System (ATLICS). This systematic review aims to provide an up-to-date evaluation of the literature, including assessment of a further three studies not analysed in previous reviews. In doing so, this is the first systematic review to include a mixed adult and paediatric (age range: 9-96) subject cohort in their dataset and, more importantly, the reliability among non spine-subspecialty professionals; something that is essential in validating the classification as an inter-disciplinary communication tool. Also detailed in this review is the wide variety between reliability across studies, particularly with regard to sub-type classification, documenting findings that have not been previously published. The final goal of this up-to-date and accurate analysis of the ATLICS is to comment on its characteristics and whether it should be adopted by the spinal community, taking into account aspects that could be further improved. Material and Methods: In this systematic review, electronic searches of PubMed, EBESCO, Cochrane, and Web of Science databases were conducted. Data extraction and quality assessment were in accordance with Cochrane Collaboration guidelines. Results: Twelve articles assessing the reliability of ATLICS were included in this review. The overall inter-observer reliability varied from fair to substantial, but the three additional studies in this review, compared to previous reviews, presented on average only fair reliability. Least reliably classified were A1, A4 and B subtypes. The overall intra-observer reliability was reported in seven studies, of which six studies presented substantial reliability. Excluding subtypes improved both overall inter- and intra- observer reliability. Only one study assessed the reliability of the neurological classification, yielding substantial reliability, and no studies were found on patient-specific modifiers. Conclusion: This systematic review concludes that ATLICS is reliable for the majority of injuries, but the variability within subtypes suggests the need for further research in assessing the needs of users in order to increase familiarity with ATLICS or perhaps the necessity to include more subtype-specific criteria into the system. Further research is also recommended on the reliability of modifiers, neurological classification and the application of ATLICS in a paediatric context.
1537
A229: Posterior Stabilisation of Fractures of the Thoraco-Lumbar Junction: Does the Inclusion of the Fracture-Level Pedicle Screw Affect Functional and Radiological Outcomes?
Riaz Mohammed 1 , Roberto Carrasco 2 , Rajat Verma 1 , Irfan Siddique 1 , Saeed Mohammad 1 , and Mahmoud Elmalky 1 3
1 Salford Royal NHS Foundation Trust, United Kingdom, Department of Complex Spine Surgery, Salford, United Kingdom
2 Salford Royal NHS Foundation Trust, Division of Population Health, Health Services Research and Primary Care, Salford, United Kingdom
3 Menoufia University, Faculty of Medicine, Shibin el Kom, Egypt
Introduction:The thoracolumbar junction representing the transition zone between the rigid thoracic and the mobile lumbar spine, is subjected to greater loading stresses. Fractures of this area are therefore common and associated with neurological deficit, instability and deformity. The optimal construct for fractures of the thoraco-lumbar junction is debatable, with no high-quality evidence to support the superiority of one method over any other. Though posterior pedicle screw fixation is the gold standard for unstable thoracolumbar fractures, instrumenting the fractured level in the construct is a relatively new technique. Our study assesses both functional and radiological outcomes of this construct in single level fractures of the thoracolumbar junction (T11-L1). Methods:Radiological parameters and functional outcomes (hospital registry database) were prospectively collected for 53 consecutive thoracolumbar junction fractures operated between the years 2010-2018. Patients where the fracture level was instrumented (FL group: 34 patients) were compared with the group where fracture level was not instrumented (NFL group: 19 patients).Radiological parameters analysed were sagittal index, bi-segmental kyphosis (Cobb) angle and the degree of vertebral height restoration. Outcomes were compared between pre-operative, immediate post-operative and final follow up study periods. To counter for small numbers and unequal groups, stepwise regression analysis adjusted by age at the time of intervention, gender and functional scores were performed. Only those variables with P value≤0.2 were selected in the stepwise regression model. Results:Post-operative back pain score was significantly lower in the FL group(P< .025)compared to NFL group.Core Outcome Measures Index (COMI) scores and leg pain scores, though low in theFLgroup, were not statistically significant. Stepwise regression analysis showed that inclusion of fracture-level screw is independently associated with a greater change in sagittal angle from pre-operative to immediate post-operative measurement after intervention and also from pre-operative to final measurement. Also the FL group was associated with a greater change in vertebral height ratio from pre-operative to immediate post-operative measurement. There was no significantdifference between the groups for revision surgery, deep infection, implant failure or post-operative length of hospital stay. Conclusion: The inclusion of the fracture-level pedicle screw in the fixation construct seems to significantly improve the immediate and final measured radiological parameters along with better functional scores in patients with single level unstable vertebral fractures of the thoracolumbar junction.
1045
A230: Reliability of Thoracolumbar Injury Classification System (TLICS) in Predicting the Outcome Following Thoracolumbar Fractures
Nishanth Ampar 1 and Shyamasunder Bhat 1
1 Kasturba Medical College, Manipal, Manipal Academy of Higher Education, Orthopaedics, Manipal, India
Introduction: Thoracolumbar spine fractures are common injuries that can result in significant disability, deformity and neurological deficit. An effective classification system is required for classifying thoracolumbar injuries that not only includes all the essential elements guiding therapeutic management, but accurately predicts the neurological outcome. Thoracolumbar injury classification system (TLICS) includes all the essential elements required for classifying, planning the modality of treatment. The aim of this study was to assess the clinical utility of this scoring system in classifying thoracolumbar spinal injuries, selection of treatment modality and assessment of the neurological outcome. Material and Methods: In this single-centre retrospective study, 85 consecutive cases of thoracolumbar spine injury over the age 17 admitted between 2015 and 2018 with a minimum follow-up time of 2 years were included. The Fractures were then assigned a TLICS score after review of CT and MRI scans. All the pathological fractures were excluded from the study. Patient-specific clinical confounders collected and examined included: age, sex, and neurological status according to the American Spinal Injury Association (ASIA) impairment grading at time of presentation was documented. As per guidelines of TLICS scoring system all fractures with score of less than 4 were managed non-operatively, those with more than 4 were managed operatively (decompression and posterior instrumentation) and the patients with TLICS score 4 were managed either non -operative /operative based on the decision taken following the members of the spinal team. At the end of two years the neurological status was documented as per ASIA impairment grade and compared to the ASIA Impairment grade at the time of presentation and documented as completely improved, partially improved and not improved with objective of assessing the reliability of TLICS score in selection treatment modality and to predict the prognosis following thoracolumbar spine injury. Results: The normality of data was assessed using Kolmogorov-Smirnov (K-S) and Shapiro-Wilk test. We also used non-parametric Kruskal-Wallis test to obtain the mean TLICS values. Out of 85 patients, 58 patients completely improved, whereas in 12 cases partial improvement was recorded and in 15 cases there was no neurological improvement post treatment. Out of 15 patients who showed no neurological improvement, 13 patients had TLICS score of >4. Overall, among 38 patients with TLICS score of >4, 13/38 cases showed improvement, 12/38 cases showed partial improvement and 13/38 did not show any improvement. High mean score of 6.933 ± 1.624 was associated with cases which did not show any neurological improvement. Those who showed partial neurological improvement had a TLICS mean score of 6.000 ± 0.853 and a very low score of 3.897 ± 1.507 was observed in case of patients who showed complete improvement. A statistically significant association between neurological improvement and TLICS score was observed (Chi square = 37.530, P < .01). Conclusion: We conclude that TLICS score can aid in selection of treatment modality and can be a reliable predictor of neurological outcome following thoracolumbar spine injuries.
175
A231: Single-Stage Short-Segment Posterior Fixation and Anterior Decompression with Inter-Body Fusion as a Management Approach for Unstable Thoracolumbar Burst Fractures
Shaffaf Kareem 1
1 Vardhman Mahavir Medical College & Safdarjung Hospital, Spine Care Unit, New Delhi, India
Introduction: In unstable thoracolumbar spine injuries, surgical intervention is necessary for decompressing the cord and stabilizing the spine. In literature, various strategies for the same have been described. When either posterior alone approach or anterior stabilization alone are used, there is a high risk of failure, instability or loss of deformity correction. Hence combined approach is useful in providing direct decompression of the cord as well as stabilization of the spine. Along with that flexibility of the spine is also not compromised. Hence, this study explores the clinical and radiological outcomes of one-stage short-segment posterior pedicle screw fixation and anterior decompression with fusion using a titanium cage. Material and Methods: The study was conducted in 30 consecutive patients of traumatic thoracolumbar unstable burst fractures with evidence of spinal cord compression and neurological deficit. After appropriate clinical and radiological diagnosis, all underwent single-stage short-segment posterior fixation and anterior decompression with fusion using a titanium cage filled with bone graft. Results: In our study, the majority of the patients were of male sex; with a mean age of 30.2 years. Falls from height constituted the commonest mode of injury. The most common vertebra involved was L1. The mean timing of surgery from incision to application of dressing was 249 minutes. The mean blood loss was 1149 ml. Average follow-up of 3 years, showed that those (6 patients) reported with cord discontinuity had no neurological recovery. Out of the rest, 22 patients had improvement of at least 1 grade in frankel grading. No patients showed deterioration of neurology. The mean value of canal compromise reduced from the pre-operative value of 43.47- 0 postoperatively. Mean anterior vertebral height compression (AVHC) % was corrected from 37.77% preoperatively to 18.53% in the immediate postoperative period, and at 6 months it was 22.27% with a mean loss of correction of 2.93%. There was a decrease in lateral Cobb's angle from a mean pre-operative angle of 23.93°- 6.63°. None had post-operative complications like hardware failure, spinal instability, cage subsidence or progression of the deformity. Evidence of fusion was seen in 90%. Conclusion: Adding anterior stabilization to unstable thoracolumbar burst fracture prevents posterior implant failure, preserves the number of motion segments and provides a larger area for a fusion of the segments anteriorly. However, a randomized control study with larger population size and longer follow-up is necessary to look for actual fusion rates as well as the occurrence of complications.
1837
A232: Post-Traumatic Thoracolumbar Kyphosis: A Major, Challenging, Late Complication Following Tl Spinal Injuries - A Retrospective Analysis of its Clinical Presentation, Surgical Management and Long-Term Outcome Following Surgical Intervention
Ajoy P Shetty 1 , Rohit Kavishkar 1 , Rishi Kanna 1 , Vibhu Krishnan Viswanathan 1 , and Shanmuganathan Rajasekaran 2
1 Ganga Medical Center and Hospitals, Spine surgery, Coimbatore, India
2 Ganga Medical Center and Hospitals, Coimbatore, India
Introduction: Post-traumatic kyphosis (PTK) is a challenging complication following TL spinal trauma. It usually develops consequent to missed or conservatively managed AO type B2 injuries (posterior ligamentous complex disruption), injuries to the inter-vertebral discs or vertebral end-plates, severe osteoporosis, pseudoarthrosis, or iatrogenic causes including implant failure or loosening. Progressive kyphosis can lead to recalcitrant symptoms including pain, progressive deformity and neurological deterioration. The aim of the current study was to retrospectively analyze the long-term radiological and clinical outcomes of patients who underwent surgical correction of PTK. Material and Methods: A retrospective analysis of the clinical and radiological data of PTK patients who presented to our Out-Patient clinics or Emergency Department between January 2016 and August 2018 was performed. Only surgically treated patients with adequate (at least 2 year) follow-up were included. For deformity correction we performed one of the following osteotomies - Ponte’s osteotomy, pedicle subtraction osteotomy (PSO), disc-bone osteotomy (DBO) and closing opening wedge osteotomy (COWO). Radiological evaluation of kyphosis was performed using Cobb’s angle. The functional outcome at the final follow-up was assessed using Oswestry Disability Index (ODI), visual analogue scale (VAS), and SF-12 score. The statistical analysis was performed using “student t test”. Results: A total of 22 cases (male to female ratio 2.3; mean age 30.3 years) with PTK treated by posterior spinal deformity correction and instrumented fusion were included for this study. The most common presenting symptom was instability-type, axial back pain [n = 22(100%)]. 9.1% of patients presented with neurological deficit. The mean time of presentation from initial injury was 16.5 ± 7 weeks. The apex of kyphosis was located between T11 and L2 in all our patients. Ponte’s osteotomies, PSO, DBO and COWO were performed in 9, 9,2 and 2 patients, respectively. The mean pre-operative Cobb’s angle was 33.3°. Post-operatively, the mean correction, which was achieved, was 23.85° (P < .05). The mean surgical time was 275 ± 40 minutes, and the mean intra-operative blood loss was 445 ± 71 ml. The mean VAS score for back pain improved from 7.2 to 2, and ODI score decreased from 58.1 to 24.1 at the last follow-up. Conclusion: Symptomatic PTK is a rarely encountered, delayed complication following TL traumata. They usually develop at the junctional levels of TL spine and most commonly present with axial, instability-type back pain. A certain proportion of these patients present with significant neurological deficit. Surgical deformity correction is a safe and effective method for treating this condition. Such procedures can enable the surgeons to achieve adequate correction of the kyphosis and also provide ameliorated, long-term functional outcome for the patients. Keywords: PTK (post-traumatic kyphosis), kyphosis, osteotomy
1400
A233: Classifications and Therapy Recommendations for Thoracolumbar Spinal Injuries: A Comparison Between AO Magerl, TLICS, and AOSpine
Fady Khamis 1 , Philipp Schleicher 1 , Pingel Andreas 1 , and Frank Kandziora 1
1 BGU Frankfurt, Frankfurt am Main, Germany
Introduction: To determine the efficiency or reliability of a new classification system, a direct comparison with existing classification systems should be performed. The aim of the present work is a comparative evaluation of the interobserver reliability of the three international classification systems for thoracolumbar spine injuries (AO Magerl, Thoracolumbar Injury classification score “TLICS”, Thoracolumbar AO Spine classification “TL AOSpine”) and the determination of modification possibilities with regard to reliability, usability as well as therapy recommendation of the currently common TL AOSpine classification system. Materials/Method: This is a monocentric, prospective analysis of patients with fractures of the thoracolumbar region. Only cases with traumatic fractures were included, pathological fractures were excluded. The available x-rays, CT and MRT images were classified by 5 spine surgeons with different degrees of experience using the three classification systems AOSpine, AO Magerl and TLICS, and the associated treatment recommendation according to Thoracolumbar AO Spine classification injury score “TL AOS IS”, German society for trauma surgery “DGU” and TLICS. For the statistical evaluation, the interobserver reliability according to Cohen's kappa was calculated. Results: Radiological and clinical data of 100 patients were included. AO Magerl showed moderate Interobserver reliability (κ = .46) for morphological classification and substantial agreement (κ = .71) for DGU therapy recommendations. TLICS showed fair Interobserver reliability (κ = .35) for morphological classification, substantial agreement (κ = .69) for therapy recommendations according to TLICS. TL AOS showed substantial Interobserver reliability (κ = .69) for morphological classification and a substantial agreement (κ = .77) for therapy recommendations (TL AOS IS). Discussion: In the present study it could be shown that TL AOS is a reliable classification, with superior interobserver reliability compared to AO Magerl and TLICS. The treatment recommendations of TL AOSIS have higher interobserver reliability compared to other treatment recommendations (DGU and TLICS).
1732
A234: Burst Fractures Without Neurological Injury. Predictive Factors for Surgical Treatment
Ana Ribau1, Tiago Barbosa1, Manuel Carrapatoso1, Ricardo Rodrigues-Pinto1, and Pedro Neves2
1 Spinal Unit (UVM). Department of Orthopaedics. Centro Hospitalar Universitário do Porto., Porto, Portugal, 2 Centro Hospitalar e Universitário do Porto, Porto, Portugal
Introduction: The optimal treatment of burst thoracolumbar fractures without neurological injury remains controversial. Numerous classifications have been developed with the goal of guiding the treatment decision however none is completely accepted. On the other wise, there are some factors indicating instability such as height loss greater than 50% and angulation greater than 30°. This work aims to identify the factors that were associated with the decision between surgical or conservative treatment. Material and Methods: All patients treated for burst thoracic and/or lumbar fractures, without neurological injury, in the period of 1 year, in a single institution, were retrospectively evaluated using clinical and image records. Demographic data, type of treatment, TLICS classification, height loss and angulation were analyzed. Results: Of the 97 patients, 27 men and 70 women, with a mean age of 71 years, 79 (81%) were treated conservatively and 18 (19%) underwent surgery. The average age was 52 years for those that underwent surgical treatment and 75 years for the group that was conservatively treated. Seventy-two patients were TLICS 2, of these 67 were treated conservatively and 5 surgically. There were 25 patients with TLICS 4, 12 of which were treated conservatively and 13 surgically. The average angulation for patients treated conservatively was 10° and for those treated surgically 15°. In the univariate analysis, age (P < .001), angulation (P = .007) and TLICS (P < .001) were associated with the type of treatment performed. However, when multivariate analysis was performed, only age (P = .001) and TLICS (P < .005) maintained the association. The TLICS classification was associated with the decision made, however there are patients with same classification that are oriented differently (e.g., 5 patients with TLICS 2 treated surgically). Age is also an independent factor associated with the treatment decision, with a trend towards surgical treatment decision in younger patient. The angulation despite being associated with the treatment decision is not an independent factor and is therefore a confounding factor. Conclusion: Our results are in line with those found in the literature. Although there are some guides for the treatment decision, there is no algorithm and burst fractures without neurological injury still represent a decision dilemma for the surgeon.
OP27: Spinal Infections
582
A235: Relapses, Complications and Mortality with Hematogenous Vertebral Osteomyelitis
Alexander Bazarov 1 , Konstantin Sergeev 2 3 , Aleksei Farion 3 , and Roman Paskov 2 4
1 Tyumen regional hospital
2, Traumatology and Orthopedic Department
3, Tyumen, Russian Federation, 2 Tyumen State Medical University, Department of Traumatology and Orthopedics with a course in Pediatric Traumatology, Tyumen, Russian Federation, 3 Tyumen regional hospital No2, Traumatology and Orthopedic Department No1, Tyumen, Russian Federation, 4 Tyumen regional hospital No2, Tyumen, Russian Federation
Introduction: Hematogenous pyogenic vertebral osteomyelitis is a disease that requires a multidisciplinary approach. The rarity and severity of this pathology requires focusing on relapses, complications and mortality. The number of complications can reach 12.5%. Recurrences are a potential problem for spondylodiscitis, especially when instrumentation is used. The number of relapses according to different studies varies from 1 to 22%. Mortality rates in most publications do not exceed 5.0%, however, it can increase up to 20.0% with late diagnosis. Material and Methods: a retrospective analysis of 209 PVO cases was conducted in the Tyumen Regional hospital #2 in 2007-2017 (Russia) with a diagnosis of “Pyogenic vertebral osteomyelitis”. 68 patients (32.5%) were treated conservatively, 141 (67.5%) operatively. Risk factors for relapse, complications and mortality with various treatment methods were analyzed. A statistical analysis was performed. Results: Recurrent disease was observed in 21 patients (10.0%). Relapses after surgical treatment amounted to 12.8% (n = 18), conservative - 4.4% (n = 3). The main causes of complications were: diabetes mellitus, drug abuse, gross violation of the treatment regimen. 17 patients were operated on again (12.0%), remission was achieved in nine of them (52.9%). The risk of relapse was significantly higher among drug-addicted patients (P = .015), but only in the surgical group. Complications accounted for 15.8% (n = 33) of the total number of patients. In the surgical group: intraoperative - 5.0% (n = 7), postoperative - 19.8% (n = 28). The number of complications is significantly higher in the group of operated patients who underwent volumetric surgery and treatment in the intensive care unit for other diseases (P = .028). Hospital mortality of 4.3% (n = 9) was significantly higher in patients with diabetes mellitus (P = .039), among those who were operated on (P = .023). Conclusion: The risk of relapse was significantly higher among drug-addicted patients (P = .015), but only in the group of operated patients. With conservative treatment the rate of relapses was 4.4% compared to surgical treatment - 12.0%. Complications are significantly more common in patients who have been treated in the intensive care unit and operated on for other diseases (P = .028). Hospital mortality (n = 9) was 4.3% and significantly higher in patients with diabetes mellitus (P = .039).
381
A236: Tuberculosis of the Cranio-Vertebral Junction: Its Altered Biomechanics and Treatment Strategy
Sudhir Srivastava 1 , Nandan Marathe 1 2 , Sunil Bhosale 1 , Aditya Raj 1 , and Ashraf Shaikh 1
1 Seth GS Medical College and KEM Hospital, Orthopedics, Mumbai, India
2 Toronto Western Hospital, Orthopedic Surgery, Toronto, Canada
Introduction: TB of the Craniovertebral junction (CVJ) is a not so common form of spinal TB, accounting for less than 1% of all forms of spinal TB. Usually, diagnosis gets delayed because of non-specific nature of symptoms and difficulty in interpreting screening X-rays at the initial stages of the disease. Neurological deficit in such a situation can be catastrophic. Peculiar anatomy of this region further compounds the problem. CVJ has a Y-shaped beam for load transmission and has no anterior loading structure at C1. Stabilizing structures mainly include the ligaments and destruction secondary to TB causes instability which in turn leads to neural dysfunction. The authors have designed a protocol based management strategy for TB of the CVJ. This study will assess functional outcomes of patients with CVJ Koch treated using this protocol. Materials and methods: 108 patients with TB of the CVJ were managed at a tertiary care University Hospital in India over a period of 12 years. A treatment algorithm was developed for these patients based on the clinical and radiological classification. Patients were divided radiologically into 3 grades depending on the severity of involvement. Group A included patients with presence of pre-vertebral shadow, no instability and only lytic lesion in the bone. Group B had patients with instability and osseous destruction. This group was further subdivided into patients with early involvement of one lateral mass/ joint and those in whom lateral mass was bilaterally affected. Group C included patients with significant destruction of lateral mass complex, irreducible C1- C2 dislocation and persistent AAD in paediatric age group. Patients were treated either conservatively or surgically using the treatment algorithm. Conservative management strategies included Anti- tuberculosis chemotherapy, Orthosis and Traction. Surgeries performed included occipito-cervical fixation and fusion, Trans-articular screw fixation and fusion, C1-C2 separate fixation (Pedicle screw/ Lateral mass screw/ Laminar screw). Results: 60 patients were treated conservatively, 28 patients required OCP, 18 patients needed trans-articular screws, 2 patient was treated with C1-C2 separate fixation. 6 patients had clinically appreciable tilt and 10 patients had axial settling in the conservatively treated group. However, there was no functional impairment. There was no neurological deterioration in any conservatively treated patient. In the surgically treated group of 48 patients not a single patient had neurological deterioration. Out of the 8 patients who were clinically grade 3, 7 patients were ambulatory at 18 months follow-up. 1 patient remained paraplegic. Fusion was achieved in all cases. Conclusion: Though the bacteria and the chemotherapy are the same, TB of the CVJ needs special attention because of the complex anatomy of the region and presence of vital structures in the vicinity. Early detection, initial rigid orthosis for adequate healing and protocol base surgical intervention when warranted will give a long lasting fruitful outcome. Keywords: Cranio- vertebral, tuberculosis, trans-articular, orthosis, occipito-cervical
710
A237: Current trends of drug resistance in spinal tuberculosis: a single centre experience
Aditya Raj 1 , Sudhir Srivastava 1 , and Nandan Marathe 2
1 Seth G.S Medical College & K.E.M Hospital, Orthopaedics, Mumbai, India
2 Toronto Western Hospital, Toronto, Canada
Introduction: Spinal tuberculosis accounts for about 50% of cases amongst extra pulmonary osteoarticular tuberculosis. Resistance to drugs in spinal tuberculosis patients is on a rise and there is inadequate literature concentrating on the precise pattern of resistance in Indian subcontinent which harbours 24% of global prevalence. The aim is to study the pattern of drug resistance in spinal tuberculosis among first and second-line drugs. Drug resistance is common in spinal tuberculosis and we intend to find the prevalence of various drug resistance patterns. Methods: This study represents a retrospective observational analysis. Patients with spinal tuberculosis visiting a tertiary centre were assessed. Samples were taken from the affected vertebrae and sent for BACTEC Mycobacterium Growth Tube Indicator(MGIT) 960 culture. Patients with a positive growth in MGIT were included in the study. All previously treated patients (Relapse, Treatment after failure, Treatment after loss to follow-up and other previously treated patients) were excluded. We routinely perform MGIT, Gene Xpert (Cartridge based nucleic acid amplification technique) and histopathological examination in all the patients undergoing a biopsy for suspected tuberculous spondylodiscitis. Results: 150 patients with a positive growth in MGIT report were included in the study, of which 43 patients had some kind of drug resistance. Seven were multidrug resistant (MDR), 9 had pre-extensive drug resistance (pre XDR) and 4 had extensive drug resistance (XDR). Among the 9 patients who had Pre XDR TB, 6 (13.95%) had resistance to FQ and 3 (6.97 %) had resistance to an injectable 2nd line. Mono-drug resistance was present in 17 cases (39.5%) and polydrug resistance was present in 6 (13.95%) patients. The most common drug resistance among the first line agents was encountered was with Isoniazid (74.4%) and least with pyrazinamide (30.23%). Among the second line agents the drug resistance was more common with the FQ group as compared to second line injectables. Resistance to RIF in the study was less as compared to that of INH, showing that INH resistance is more prevalent and examining patients with Gene Xpert for RIF resistance alone will not prevent amplifier effect. Conclusion: Drug resistance in spinal tuberculosis was found to be 28.6%. Out of these MDR was in 16.2 %, pre XDR in 20.9% and XDR in 9.3% patients. In recent years, new drug regimens are being evaluated for drug resistant pulmonary tuberculosis based on drug sensitivity pattern, while no such study has been performed for spinal tuberculosis. This study provides pattern of drug resistance in patients with drug resistant spinal TB.
661
A238: Instrumented Fusion in Tubercular Spondylitis in Low Middle Income Country, Nepal
Subin Byanjankar 1 and Dipak Maharjan 1
1 Green Pastures Hospital and Rehabilitation Center, Orthopedics and spinal disorder, Pokhara, Nepal
Introduction: While Tuberculosis is rare in developed countries, it is rampant in Low Middle-Income countries. Even though there is an improvement in diagnosis with improved laboratory services, radiology, a significant number of patients present late with complications of advanced disease. Tubercular Spondylitis is primarily a medical disease. Surgery is indicated for neurological complications, pain, diagnostic dilemma and correction/prevention of deformity. Material and Methods: We prospectively followed up 29 adults operated for Tubercular spine from May 2009 to April 2019. 19 patients underwent instrumented Fusion in thoracic and lumbar Spine from T5- L5. The mean follow up was 34 months. Indications for surgery included neurologic complication 10, recalcitrant pain unresponsive to Anti-tubercular therapy (ATT) - 11. All the patients were assessed clinically with American Spinal Injury Association (ASIA) Impairment Scale and Oswestry Disability Index (ODI) preoperatively and follow up at 6 weeks, 3 months and then at 3 months interval. Anterior debridement, decompression and Anterior Column Reconstruction (ACR) using Iliac Crest Bone Graft or Titanium cage filled with bone graft followed by Posterior Spinal Instrumentation (PSI) were performed in 11 patients. Posterior Spinal Instrumentation, circumferential debridement, decompression, and Anterior Column Reconstruction through an Extended Posterior Approach - 10 patients. Other surgeries included open transpedicular biopsy in 5 patients with the diagnostic dilemma and anterolateral decompression and Biopsy in other 2 and Anterior Cervical Fusion 1. All patients received 12 months of Anti-tubercular therapy. 3 proven Multidrug-Resistant (MDR) TB received MDR regimen. Results: 21 patients were reviewed. 1 paraplegic patient who had recovered to ambulation with support, died at 6 months. Another patient with Tuberculosis of L3L4L5 with pain and deformity was fully ambulatory died after 3 years due to Alcoholic Liver Disease. Mean duration of surgery was 5.3 hours (4 - 7 hours), mean blood loss 820 ml (400 - 1200 ml) and mean hospital stay was 20 days (12 - 40 days) in Anterior Debridement, Decompression and Column Reconstruction followed by Posterior Spinal Instrumentation and in the Singe stage Extended Posterior Approach mean duration of surgery 3.5 (3 - 5 hours), mean blood loss 550ml (300 - 800ml) and mean hospital stay12.6 days (8-14 days). Neurological recovery was seen in all 5 complete paraplegics and 3 incomplete paraplegics. There was a significant improvement of ODI - mean 89.2% pre-operative to 19.1 % (Range 13 - 40) at 6 months follow up and 6.1 % (Range 0 - 18) at 1 year follow up. 2 patients developed surgical site infection requiring debridement, 2 patients developed cold abscesses who were later diagnosed to have MDR. 1 patient developed drug-induced Hepatitis. 1 patient developed unhealed sinus and Implant breakage. Conclusion: Surgical treatment when indicated for active Tubercular Spondylitis with Anterior Debridement, Decompression, Anterior Column Reconstruction and Posterior and Spinal instrumentation along with Anti-tubercular therapy offers good clinical and neurological recovery. Single-stage Extended Posterior approach for circumferential decompression and column reconstruction has an advantage of reduced operative time, operative blood loss and shorter hospital stay.
718
A239: Modern Tactics and Surgical Treatment of 338 Patients with Purulent Spondylitis
Maxim Goncharov 1 , Vadim Manukovsky 2 , and Evgeni Levchik 3
1 Ural State Medical Universitet, Neurosurgery, Ekaterinburg, Russian Federation
2 Saint-Petersburg I.I. Dzhanelidze Research Institute of Emergency Medicine, Neurosurgery, Saint-Petersburg, Russian Federation
3 ural State Medical Universitet, Ekaterinburg, Russian Federation
Introduction: In the treatment of purulent spondylitis, there are many problems, such as-the timing of specialized care, indications for surgical treatment, one or two-stage surgical interventions, isolated arthrodesis, or with instrumental fixation. We operated on 338 patients with purulent spondylitis. Active surgical tactics in patients with purulent spondylitis, together with the choice of low-traumatic and radical approaches, as well as postoperative antibacterial therapy, allows achieving good surgical outcomes in the majority (90%) of patients. Material and Methods: During the period from 2007 to 2017, 338 patients were operated on. The average age of patients was 47.6 ± 2.8 years. 38 (11.24%) were diagnosed with HIV infection. The average duration of the disease from the first signs to surgical treatment was 47.9 ± 23.3 days. Patients were also divided into 3 groups according to the clinical classification of E. Pola (2017): А1-4 - 0, В1-4 -10(2,9%), С1-4-328 (97,1%). Neurological disorders of varying severity were detected in 256 (75.7%) patients. Systemic inflammatory response syndrome was diagnosed in 141 (41.7%) patients. Results: Performed the following operations: decompression and debridement in 132 (39.05%) patients, decompression, debridement and fusion in 198 (58.6%), and fusion in 8 (2.3%). To evaluate the results of surgical treatment, we took into account the dynamics of pain (according to VAS), neurological disorders (according to the ASIA/ISNCSCI scale), systemic inflammatory response syndrome, indicators of quality of life and patient satisfaction with treatment (Karnovsky, Oswestry scale), and the presence of postoperative complications. Good and satisfactory results of surgical treatment at the time of discharge from the hospital were observed in 320 (94.6%) patients. These patients reported high postoperative quality of life scores on the Karnovsky scale (average 81.2 ± 7.4 points) and low Oswestry disability scores (ODI 20.3 ± 2.3). The majority of unsatisfactory outcomes in patients were due to: fatal outcomes in 7 (2,07%), residual gross neurological disorders, repeated vertebral operations in 6 (1.7%); repeated vertebral operations due to infection of the autosteal graft or bone migration in 5 (1.5) patients. Conclusion: Surgical treatment of purulent spondylitis is a complex and multi-factorial task. Reducing the duration of the disease, active surgical tactics, taking into account the syndrome of a systemic inflammatory response, is accompanied by good outcomes in the majority (94%) of operated patients.
676
A240: Can Intra-Operative Irrigation with Antibiotics Reduce Bacterial Load at the Surgical Site? An in-Vitro Study
Rawan Masarwa 1 , Ofir Uri 1 , and Eyal behrbalk 1
1 Hillel Yaffe Medical Center, Orthopaedic Department, Hadera, Israel
Purpose: Intra-operative surgical site irrigation with antibiotics and may reduce risk of infection in spine surgeries involving instrumentation. Nevertheless, this common practice lacks supporting evidence. This prospective in-vitro study evaluated short-term exposure to antibiotics on growth of common pathogens involved in wound site infection in spine surgery. Methods: A suspension of one of three micro-organisms: (1) Staphylococcus Aureus, (2) Staphylococcus Epidermidis, or (3) Pseudomans Aeruginosa was added to 2-ml vials of enriched medium, containing one of three antibiotics: (a) Vancomycin, (b) Gentamicin, or (c) Cefazolin. The final inoculum of each micro-organism was 103 CFU/ml, representing a contaminated surgical wound in spine surgery. Antibiotics were washed out from the suspension by centrifugation technique after: (i) 5 minutes, or (ii) 8 hours, representing time of tissue exposure to antibiotics after intra-operative surgical site irrigation or applying antibiotic powder to the surgical field before wound closure, respectively. Recovery growth of micro-organisms was monitored for 24h by laser light scattering technology and compared to control vials containing micro-organisms without antibiotics. Results: Pseudomans Aeruginosa inoculated in vials with Gentamicin, showed no 24-hour bacterial growth after 5-minute and 8-hour exposure to the antibiotic. Vials of all other bacteria-antibiotic combinations showed bacterial growth curves similar to the control vials after both 5-minute and 8-hour exposure to antibiotics, with no signs of bacterial growth inhibition. Conclusion: Our findings demonstrate that a 5-minute exposure to Gentamicin may inhibit Pseudomonas Aeroginosa growth in enriched medium vials and support surgical wound irrigation with Gentamicin in spine surgery.
484
A241: Outcomes of surgical treatment of spondylitis in HIV-infected patients
Maxim Goncharov 1 , Evgeni Levchik 1 , and Arkadiy Vishnevsky 1
1 URAL State Medical Universitet, Ekaterinburg, Russian Federation
Introduction: Currently, Russia ranks 4th in the world after South Africa, Nigeria, and Mozambique in terms of the growth rate of new cases of HIV-infected patients [WHO, 2018]. The total number of HIV-infected patients in the Russian Federation is more than 1 million people. The goal of the study was to improve the outcomes of surgical treatment of purulent spondylitis in HIV-infected patients. A personalized approach to the patient, taking into account the level of CD4 cells, is accompanied by favorable outcomes of surgical treatment, comparable to the indicators of the control group. Material and Methods: A monocenter group-control study was conducted between 2005 and 2018. The catamnesis of 365 patients with pyogenic spondylitis was studied. 64 (17.5%) had HIV infection. The average duration of HIV infection at the time of hospitalization was 6.5 ± 2.2 years. Patients were also divided into 3 groups according to the clinical classification of E. Pola (2017): А1-4 - 0, B1-4 - 2 (3,1%), C1-4 - 62 (96,8%). Neurological disorders of varying severity were detected in 52 (81.3%) patients with HIV infection. Results: Patients were operated on: 22 (34.4%) had decompression and debridement, 42 (65.6%) had decompression, debridement and fusion. Good and satisfactory results of surgical treatment at the time of discharge from the hospital were observed in 57 (89.1%) patients. These patients reported high postoperative quality of life scores on the Karnovsky scale (average 79.2 ± 5.4 points) and low Oswestry disability scores (ODI 23.3 ± 4.5). 2 (3.1%) patients had unsatisfactory treatment outcomes due to increased neurological symptoms in the immediate postoperative period. When evaluating outcomes and complications in HIV-positive patients with different levels of CD4 + lymphocytes, the prevalence of early infectious complications (in 10 patients - 66.6%) was revealed in the group of patients with CD4 cell levels less than 200 cells/µl (P < .05). Conclusion: Patients with HIV infection are at risk for developing purulent spondylitis. The choice of conservative or surgical treatment of purulent spondylitis depends on the stage of the disease, the type of vertebral destruction, the presence of spinal instability and neurological disorders.
743
A242: Risk Factors for Revision Surgery in Infectious Spondylitis Patients: Prospective Cohort Analysis
Gereyhan Kaibov 1 , Denis Naumov 1 , and Alexander Mushkin 1
1 Saint-Petersburg State Research Institute of Phisiopulmonology, Spine surgery, Saint-Petersburg, Russian Federation
Introduction: The rate of postoperative complications for infectious spondylitis is about 20%. A health related quality of life analysis shows the significant increase of a patient’s disability index after revision surgery. The risk factors evaluation of a postoperative failure produces a relevant data for treatment results improvement. Materials and Methods: Prospective cohort analysis from January to December 2019. During the evaluation period 227 consecutive infectious spondylitis patients were operated. Pathological tissue debridement, anterior fusion with titanium mesh cage and posterior fusion with transpedicular screw or laminar hooks fixation was performed in all cases. 58 cases of postoperative complications were detected, included 38 cases in patients with pyogenic spondylitis and 20 cases - with chronic tuberculosis spondylitis. The average age of patients was 52 years (min-21 years, max-76 years), 35 male and 23 female were suffered post-op complications. The Charlson Comorbidity index was 2.2 ± 1.3 for pyogenic spondylitis and 3.2 ± 2 - for tuberculosis spondylitis. Next evaluation parameters were analysis as potential risk factors: primary disease etiology, level of spondylitis, length of anterior / posterior fusion, Charlson Comorbidity index, sex and patients age, primary surgery time and blood loss. Results: The rate of postoperative complications in our cohort was 13%. Complications at early post-op period (less than 30 days after initial surgery) were detected in 14 patients, at delay post-op period (from 30 to 90 days) - in 8 patients, and at late post-op period (more than 90 days) - in 36 patients. The average period for post-op complications development was 7 ± 3 months (min - 7 days post-op, max - 9 months post-op). Primary disease recurrence was finding in 2 cases, anterior fusion failure - in 12 cases, posterior fusion failure - in 21 cases, surgical site infection - in 23 cases (superficial - 5 cases, deep - 18 cases). The primary disease etiology, length of posterior instrumentation, sex and patient age, primary surgery time and operation blood loss weren’t influence on a risk of post-op complications. The rate of post-op complications was higher in patients with lumbar spondylitis (OR = 2.384, CI = 95%, P = .038). The most of complications was detected at delay post-op period (OR = 4.549, CI = 95%, P = .025). Conclusion: The anterior and posterior fusion failures are the most common post-op complications in patients with infectious spondylitis. The late post-op period related with complications. The decrease of a complication rate is correlate with catamnesis.
220
A243: Recovery of Long Standing Neurological Deficit in Paediatric Dorsal Spinal Tuberculosis
Sudhir Srivastava 1 , Aditya Raj 1 , and Nandan Marathe 2
1 Seth G.S Medical College & K.E.M Hospital, Orthopaedics, Mumbai, India
2 Toronto Western Hospital, Toronto, Canada
Introduction: Neurological deficit among patients of spinal tuberculosis is still frequently found in the developing countries. Patients in developing nations do have a protracted course of this disease and patients are frequently neglected in the low socioeconomic strata group. These patients may have an onset of neurological deficit and still present quite late in the course of disease. It is not uncommon for these patients to remain non ambulatory for a long period of time before approaching a clinician. The aim is to study the recovery of neurological deficit in paediatric spinal tuberculosis cases presenting to us more than 6 months after onset of motor weakness in lower limbs. Material and Methods: This is a retrospective analysis of 13 consecutive patients of paediatric spinal tuberculosis presenting to us at least 6 months after the onset of neurologic deficit. All these patients underwent surgical intervention at our centre and their neurological recovery was noted in terms of improvement in Frankel grading and spasticity improvement by modified Ashworth scale. All the patients were followed up to at least 18 months post op and final neurologic status was assessed at that time. Results: The mean age of the patients at presentation was 8.5 years. The mean duration of neurologic deficit at the time of presentation was 10.23 months (6-24 months). Seven patients had a Frankel grade B at presentation out of which six improved to Frankel grade D and one improved to Frankel C at final follow up. Out of the other 3 patients with Frankel A at presentation, 2 improved to Frankel grade D and 1 to Frankel grade C. The remaining 3 patients presented with Frankel grade C at presentation, two improved to Frankel D and one improved to Frankel E at the time of final follow up. Six of these patients underwent a single incision transthoracic versatile approach and supplemented with hartshill rectangle and sublaminar wire fixation. The anterior reconstruction of the destroyed vertebrae was done with iliac crest bone graft and rib graft harvested during the exposure in these patients. Four patients were treated with hybrid fixation by posterior approach. The distal part of the construct comprised of pedicle screw system and the proximal part of the construct comprised of sublaminar wire over the rod. A single connecting rod was bent and contoured in an inverted U shape to achieve this construct. The remaining three patients were operated with a pedicle screw and rod based system only with anterior reconstruction by locally harvested autograft. Conclusion: This study provides evidence in support of late surgical decompression in paediatric patients with dorsal spinal tuberculosis presenting after extended periods of neurological deficit and a chance for neurological recovery still exists. The surgical decompression should not be deferred only on the basis of time elapsed since the onset of deficit and an optimum neurological environment should be provided for recovery.
OP28: Clinical Biomechanics 1
1927
A244: Biomechanical Study of the Behaviour of the Intervertebral Disc: Intact Lumbar Spine Versus Lumbar Arthrodesis
Khalil Habboubi 1 , Hassen Makhlouf 1 , Meddeb Mehdi 1 , Chaker Mohamed 1 , Lanouar Bouzid 1 , and Mondher Mestiri 1
1 Kassab Institute, Tunis, Tunisia
Background: Arthrodesis is the most common solution for the treatment of degenerative pathology of the lumbar spine but it can expose to adjacent syndrome in the long term. The aim of our study was to make numerical simulations on finite element model of the lumbar spine, to analyze the behaviour of the adjacent upper and lower intervertebral discs after an arthrodesis. Methods: It was a prospective evaluative study comparing the distribution of pressure on intervertebral disks between two models of lumbar spine (from L2-L5): the first model of a 40 year-old healthy man and a second model, of the same subject, having an L3-L4 arthrodesis. The model was constructed from high resolution computed tomographic images. The dimensions and the material properties were chosen from previous studies in the literature. We used SOLIDWORKS 2018 to create the model and the simulation. We fixed the inferior surface of L5 vertebral body and applied increasing loads in axial compression and flexion on the upper surface of L2 vertebral body for the two models, with and without arthrodesis. Results: The lumbar spine model was validated by comparing the data of literature. The numerical results showed that the intervertebral disc was exposed to higher pressure if the applied charges increase; therefore a risk of disc degeneration. Our results showed that L4-L5 disc support the maximum of pressure of the lumbar spine. Comparing the distribution of pressure in the two models, with and without arthrodesis, we found that the Vons Mises stress in the adjacent discs increase, especially for the upper level, causing an accelerated degeneration of the disc responsible of adjacent syndrome. Conclusion: The finite element method allows us to create a reliable numerical model. The results of our study showed increasing pressure in the discs adjacent to an arthrodesis, whose clinical and radiological involvement will be the development of an adjacent syndrome.
158
A245: Exploring the Effect of Different Implant Materials on the Active Apex Correction Technique: A Finite Element Study Simulating 6-Month Growth
Daksh Jayaswal 1 , Aakash Agarwal 1 , Alaaeldin Ahmad 2 , Amey Kelkar 1 , Manoj Kodigudla 2 , andVijay Goel 1
1 University of Toledo, Toledo, USA, 2 Annajah Medical School, Nablus, Palestine
Summary: Selection of implant material has a significant implication on both the outcome and the economics of spinal surgeries done around the world. This study compares the correction achieved by the active apex correction technique (APC) for constructs made with stainless-steel (SS), titanium (Ti) and cobalt-chromium (CoCr) respectively. Minimal variation in the clinical parameters indicate the flexibility available to surgeons when planning surgery for early onset scoliosis (EOS) cases. Hypothesis: Clinical outcome of implant constructs with different materials could impact surgical planning for surgeons using the APC technique. Study Design: Finite element study simulating APC with a 6-month follow-up period. Introduction: Modern-day surgical planning for EOS requires an understanding of biomechanical aspects of implanted materials along with the associated economics (amongst other factors), in order to best service the patient needs. This finite element (FE) study explores the correction across different material constructs, simulating the modified SHILLA/ active apex correction technique (APC) over a 6-month follow-up period. Methods: A FE model simulating coronal (T5-T11 cobb angle: 44° & T11-L1 secondary curve) of 36° and sagittal deformity (T4-T12 kyphosis: 36° & L1-S1 lordosis: 46°) was compressed (30N) above and below the apex to simulate APC technique. The model simulated the effect of gravity and muscle forces, with 6-month spinal growth. 3 versions models were created to simulate the effect of different materials (SS, Ti, CoCr) construct. Chosen scoliotic parameters were measured and compared for these models at various time points. Results: Compared to the base model with no instruments, all instrumented models showed a reduction in the coronal and sagittal angles, apical vertebral translation and wedging at the end of the 6-month growth period. All values showed negligible variance when compared across different material cases (Table 1). Conclusion: The excellent results across SS, Ti and CoCr constructs indicate multiple intra-operative options while performing the active apex correction technique from an implant (material) perspective. Take Home Message: The study shows that the apical compression through a posterior approach, can be adopted across most facilities around the world, adaptable to operative resources available locally.[fx9]
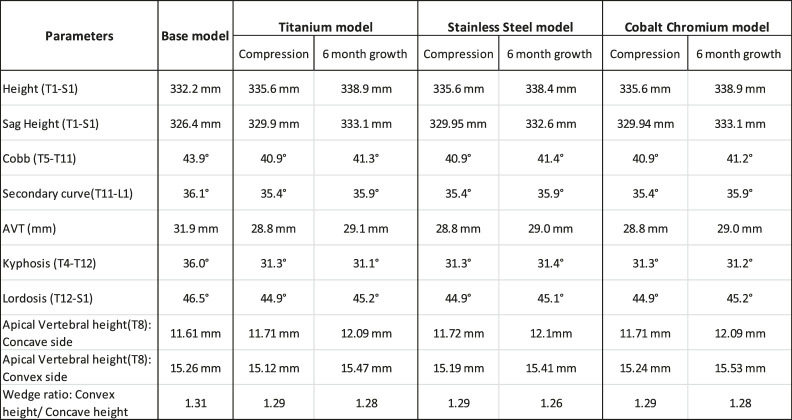
Table 1. Output parameters from the finite element model simulating the Active Apex Correction technique with different implant material cases
1808
A246: Biomechanics of Different Cage Shapes and Positions in Transforaminal Lumbar Interbody Fusion (TLIF) - A Finite Element Analysis
Gael Dreher 1 , Wilfried Matthis 2 , and Timo Biedermann 2
1 Biedermann Motech GmbH & Co. KG, Karlsruhe, Germany
2 Biedermann Motech GmbH & Co. KG, Villingen-Schwenningen, Germany
Introduction: Clinical outcome of transforaminal lumbar interbody fusion (TLIF) is dependent on segmental stabilization as well as sagittal alignment and disc height restoration, which are directly related to cage subsidence. While TLIF cages are available as straight devices placed in oblique fashion (OC) and banana-shaped devices to be placed medially in more or less anterior positions (BC), there is limited research on the biomechanics of each cage type. Our study aims to better understand the influence of cage type and positioning on bone loading, cage subsidence and of pedicle screw loading/loosening. Material and Methods: A nonlinear finite element (FE) model of a lumbar spine with reduced bone strength was developed and validated by comparing its range of motion with literature data. A TLIF with facetectomy, discectomy and posterior pedicle screw instrumentation was modelled in segment L4L5. The implanted cages were an OC implanted obliquely and a BC with three different positions ranging from central to anterior. Both cage types were given identical endplate contact surface area. The spine was subjected to a follower load (FL) of 400N and a flexion of 7.5 Nm, which is the expected maximum loading condition. We then reviewed the correlation between the results of our FE model and outcomes of retrospective studies comparing TLIF with OC and BC. Results: With 0.42 mm, sinking into the superior L5 endplate was highest for the OC, while for the BC it decreased further with more anterior cage positions, the maximum value being 0.15 mm. For the OC, plastic deformation of bone occurred below the endplates and in the vicinity of the pedicle screws, an indicator for risk of subsidence and screw loosening. The volume of plastically deformed bone was smaller for the BC and it decreased further with more anterior cage positions while the stress and moments on the posterior instrumentation were reduced as well. An improved segmental stabilization was also noted for the BC. The fact that the highly loaded anterior portion of the OC is asymmetric, narrow and discontinuous and that the lever arms between BC and posterior instrumentation are higher explain these different results. Various retrospective studies [Rice 2016, Kim 2015] compared the outcome of TLIF procedures with OC and BC. It was found that restored disc height and segmental lordosis were significantly higher in the BC group than in the OC group. Conclusion: Sagittal alignment and disc height following TLIF are intimately connected to cage subsidence. A higher loading of the bone surrounding intervertebral cages increases the risk for cage subsidence. Based on our FE model, when compared to OC, BC can increase segmental stability, reduce bone loading, cage subsidence, loading on posterior instrumentation and the risk of screw loosening under combined FL and flexion. This further improves with more anterior cage positions. This finding is in line with retrospective studies comparing TLIF with OC and BC, where restored disc height and segmental lordosis were significantly higher in the BC groups than in the OC groups.
1571
A247: Biomechanical comparison of two fixation techniques for B2 fractures of the sacrum according to the AO Spine Sacral classification system
Moritz Lodde 1 2 , Christoph Katthagen 1 , Clemens Schopper 2 , Ivan Zderic 2 , R. Geoff Richards 2 , Boyko Gueorguiev 2 , Oliver Riesenbeck 1 , Michael Raschke 1 , and René Hartensuer 1
1 Department of Trauma-, Hand- and Reconstructive Surgery, Münster, Germany
2 AO Research Institute Davos, Davos, Switzerland
Introduction: Pelvic ring fractures including Os sacrum fractures occur with an incidence of 0.3 to 8% Klicken oder tippen Sie hier, um Text einzugeben., which have increased during the last four decades together with the number of operative treatments, particularly in the older population [2, 10]. In young patients, they are mainly caused by high energy trauma, whereas in older patients - by low energy falls [1]. Several systems classifying Os sacrum fractures exist. The primarily descriptive classification system according Denis [3] is well established. However, the AO Spine Sacral classification system can be used uniformly, has been validated and is associated with a treatment algorithm [9, 11]. Different fixation methods are described as stabilization methods including Sacroiliac (SI-) screw and S1/S2-alar-ilium-screw [4]. The aim of the present study was to investigate the biomechanical competence of two fixation techniques for B2 fractures of the sacrum. It was hypothesized that the S1/S2-alar-ilium-screw would be biomechanically superior to the SI-screw. Methods: A B2 fracture of the sacrum according to the AO Spine Sacral classification system was simulated in 20 artificial pelvises, assigned to two study groups of 10 specimens each (n = 10) for fixation with either a SI-screw or S1/S2-alar-ilium-screw. The B2 fracture of the sacrum was simulated by a transalar osteotomy. The specimens were tested under progressively increasing cyclic loading. The specimens were aligned to the machine axis so that an axial compression force was applied through the center of the S1 vertebral body. Axial stiffness and displacement at the fracture site were analyzed. The hypothesis was examined by comparisons among the two groups using the Kruskal-Wallis test with Bonferroni correction for multiple comparisons. The level of significance was set at 0.05 for all statistical tests. Results: Axial stiffness [N/mm] was significantly greater (P < .05) in the group of the S1/S2-alar-ilium screw (Median: 18.52 N/mm) compared to the group of the SI-screw (Median: 3.66 N/mm). Furthermore, the displacement (cm) was significantly (P < .05) lower in the group of the S1/S2-alar-ilium screw (Median: 0.02 cm) than in the group of the SI-screw (Median: 0.41 cm). Discussion: The hypothesis that the S1/S2-alar-ilium-screw would be biomechanically superior to the SI-screw for the treatment of a simulated B2 sacrum fracture was confirmed. Stabilization of the posterior pelvic ring and the sacrum via the SI-screw is a safe, effective and feasible [5]. Additionally, the SI-screw can be used minimally invasive. Surgical treatment complications are mainly approach-related and occur in up to 30% of the cases, especially in the elderly patient [8]. However, the results of the present study correspond to previous studies showing, that the SI-screw only provides little vertical stability [6]. From a biomechanically point of view, the S1/S2-alar-ilium screw can provide this stability. Clinically, the S1/S2-alar-ilium screw and similar spinopelvic fixation methods are used successfully [5-7]. Conclusion: The S1/S2-alar-ilium screw is biomechanically superior to the SI-screw and presents a successful alternative for treatment of fractures of the posterior pelvic ring and the spinopelvic junction.
348
A248: Biomechanical Effects of Changes in Cervical Alignment Following Single-Level ACDF Using 3d Motion Capture
Darren Lebl 1 , Kathleen Meyers 2 , Hamidreza Jahandar 2 , and Timothy Wright 2
1 Hospital for Special Surgery, Spine Surgery, New York, USA, 2 Hospital for Special Surgery, Biomechanics, New York, USA
Introduction: Alignment of the cervical spine likely has significant effects on the clinical longevity of the subaxial motion segments. The biomechanical effects of changes in alignment on the cervical spine remain to be understood. Single-level ACDF is a commonly performed procedure and cervical alignment may influence motion transfer to adjacent and non-contiguous subaxial motion segments. To better understand the role of alignment on unfused cervical motion segments, the present study was designed to evaluate the biomechanical effects on the subaxial cervical spine (C2 to T1) of: 1) changes in T1 tilt 2) single-level ACDF and 3) combined effects of ACDF and changes in T1 tilt. Materials and Methods: Six cadaveric cervical spines (C2-T1) were screened fluoroscopically and placed with retro-reflective markers. Computed tomography (CT) scans with sagittal/coronal reformats were performed and degeneration was graded. Specimens were tested to 30° flexion and 30° extension in the intact state and following single-level ACDF(C5-C6). Motions of each vertebral body were tracked using a 3D-motion capture system and input into an inverse kinematics model to correlate the 3D reconstruction and motion capture data. A customized testing apparatus was developed to alter the T1 slope in human cervical cadaveric spines to neutral, +15degrees, and -15degrees. Generalized estimating equation modeling was used to analyze the main effects as well as the interaction effects of fusion and while we also controlled for the clustered nature of the data. Parameter estimates of the model are reported as mean change in range of motion and standard error, with statistical significance defined as p-value =.05. SAS software was used for all statistical analyses. Results: In the intact specimen, increase in T1 tilt (0 to +15) did not result in increased ROM at any motion segment (C2-3,C3-4,C4-C5,C5-6,C6-C7,C7-T1: P = NS). In the intact specimen, decrease in T1 tilt (0 to -15) resulted in significantly increased ROM at C2-C3 (P <.0001), C3-C4 (P <.0001), C5-C6 (P <.01), C6-C7 (P <.005), and C7-T1 (P <.02), but not at C4-C5 (P = NS). The effects of ACDF on the unfused segments at various cervical alignments was: Neutral T1 tilt, ACDF did not result in significantly increased ROM at any level (C2-3, C3-C4, C4-C5, C6-C7, C7-T1: P = NS). At increased T1 Tilt (+15deg), motion was significantly increased at C2-C3 (P <.05), however, not at any other segment (P = NS). At decreased T1 tilt (-15deg), there was a trend toward increased motion at C7-T1 (P = .06), and no significant increase in motion at any other level (P = NS). The GEE model did not show significant cumulative effects for the interaction of tilt and fusion on range of motion (P = NS). Conclusion: Changes in cervical alignment have a biomechanical influence on the observed patterns of motion in both the intact state and following ACDF. In the unfused specimen, increased T1 tilt resulted in no significant hypermobility whereas decreased T1 tilt resulted in significantly increased hypermobility at five motion segments. Following ACDF, hypermobility was transferred to non-contiguous segments, cranially when T1 tilt was increased and trended caudally when T1 tilt was decreased.
1626
A249: Analysis of Implants of Lumbosacral Spinal Fusion Using FEM
Hiroyuki Tachi 1 and Yuiciho Abe 1
1 Eniwa Hospital, Orthopedic surgery, Eniwa, Hokkaido, Japan
Background: In correction surgery for patients with adult spinal deformity (ASD), iliac fixation was often performed to prevent loosening on S1 pedicle screws (S1PS) and subsequent pseudarthrosis. Although Iliac Screws (IS) or Sacral Alaa Iliac Screws (SAI) was frequently used to reduce the strain on the caudad S1PS, the implant breakage could occur around caudal side. From the biomechanical viewpoints, it is important to evaluate the effect of SAI and IS on reducing the stress of S1PS. This study aimed to analyze the stress of lumbosacral implants in correction surgery for ASD using Finite Element Model (FEM). Materials and Methods: Three patients who underwent ASD correction using SAI were enrolled. The preoperative and postoperative CT DICOM data was used to simulate sacrum, ilium, sacroiliac joint, screws and rods in FEM. The merge of the DICOM data, and Finite Element Analysis (FEA) were performed using the Software with the program code. Three model were created; S1PS only model (S1 model), S1PS and IS model (IS model), and S1PS and SAI model (SAI model). The forward bending loaded force of 500 N was applied on the proximal of rods under the fixation of iliac side. We analyzed stress on the S1PS and the cortical bone, and distribution effect of IS and SAI on stress of S1PS by comparing with each model. Results: The stress on the S1PSs was concentrated on their screw neck, and significantly reduced to 39.5% in IS model and to 30.6% in SAI model (both; P < .001). ISs and SAIs played a role in distributing the stress on S1PSs. The stresses on the ISs and SAIs were mainly distributed on the lateral connector (53.9%) and the screw surface around sacroiliac joint (69.2%), respectively. The stress on the cortical bone was also significantly reduced to 21.2% in IS model and 16.6% in SAI model (both; P < .001). Although there wasn’t significant difference between distributed stress of SAIs (2.8 MPa) and one of ISs (3.9 MPa), the stress tended to be lower in SAI model than IS model (P = .08). Conclusion: The stress on the S1PS was reduced in IS and SAI model, indicating that ISs and SAIs can prevent loosening or breakage of S1PS, which lead to pseudoarthrosis. Main stress areas are located at the lateral connector in IS model and the screw surface around sacroiliac joint in SAI model, indicates that the center of the moment may be position at the lateral connector in IS model and the screw surface around sacroiliac joint in SAI mode, where mobile segments were controlled by implant fixation. Furthermore, the risk of breakage may be higher in IS model than SAI model, because distributed stress of SAIs tended to be lower.
931
A250: Reduced Dynamic Stability in Simulated Scoliosis
Fraje Watson 1 , Rui Loureiro 1 , and Julian Leong 1 2
1 University College London, London, United Kingdom
2 Royal National Orthopaedic Hospital, London, United Kingdom
Introduction: Adolescent Idiopathic Scoliosis (AIS) is known to affect standing balance. Measuring dynamic balance could lead to new objective outcome measures for monitoring individuals with AIS. The Margin of Stability (MoS) has been used to measure stability in pathologic populations. The aim is to collect pilot data in a simulation of scoliosis in healthy, adult volunteers prior to investigations in an adolescent, clinical population. We hypothesise that the MoS will be different between scoliosis simulation groups and controls, and that speed and incline will impact these differences. Materials and Methods: A custom thoracolumbosacral orthotic brace was designed and developed to simulate a right thoracic scoliosis with a left truncal shift. An upper and lower section were joined at the front and back by a hinge joint (XROM2, ChanecoTM; Northampton, UK) that could be used to set the two sections in a straight position (Brace-Straight) or at a 30 angle (Brace-Tilt). Ten healthy volunteers walked for 1-minute each at 3 speeds with 0% incline (0.8 m/s, 1.0 m/s, 1.6 m/s) and 3 inclines at 1.0 m/s (0.0%, 4.5%, 9.0%). Volunteers completed these walks under 3 conditions; Control, Brace-Straight and Brace-Tilt. Volunteers underwent gait analysis in a Gait Real-time Analysis Interactive Laboratory (GRAIL; Motekforce Link, Amsterdam, The Netherlands) with a dual-belt instrumented treadmill, surrounded by 10 Bonita motion-capture cameras (100Hz; Vicon, Oxford, UK) to capture the location of 46 reflective markers on their body. Gaps were filled using Nexus 2.7 (Vicon, Oxford, UK) and data was imported into Visual 3D v6 student edition (C-Motion Inc., Maryland, USA) to create a 14-segment model for each participant. Pipelines calculated the average mediolateral MoS (MoSml) for left and right heel strikes during the middle 30s of each walk. Results: For the speed walks, a linear mixed model showed that brace group significantly predicted left MoSml F (2, 65.90) = 19.31, P < .001, but did not significantly predict right MoSml. Left MoSml was significantly bigger for the Brace-Tilt group compared to Control (P < .001) and Brace-Straight (P < .001) groups. Speed did not predict left MoSml, but did predict right MoSml F (2, 65.39)=11.80, P < .001. Right MoSml was significantly bigger for 0.8m/s (P < .001) and 1.0 m/s (P < .001) compared to 1.6m/s. For the incline walks, a linear mixed model showed that brace group significantly predicted left MoSml F (2,71.53) = 22.74, P < .001 and right MoSml, F (2, 63.47) = 14.29, P < .001. Left and right MoSml was significantly smaller for the Brace-Tilt group compared to Control (P < .001) and Brace-Straight (P < .001) groups. Incline significantly predicted left MoSml. Conclusion: Left MoSml for the Brace-Tilt (scoliosis simulation) group was significantly different to the Control and Brace-Straight groups for speed and incline trials. Right MoSml for the Brace-Tilt group was significantly different to the Control and Brace-Straight groups during incline trials only. The effect of speed and incline on left and right MoSml was variable. If these results were replicated in a clinical population, then use of the MoS as an objective outcome measure in monitoring and treatment of AIS is feasible, and this could be done with a wearable device at home.
1107
A251: Biomechanics Following Two Special Constructs Of 3-Level Hybrid Surgery with Cervical Disc Arthroplasty and Anterior Cervical Discectomy and Fusion: A Finite Element Analysis
Kangkang Huang 1 , Beiyu Wang 1 , Hao Liu 1 , Tingkui Wu 1 , Xin Rong 1 , and Chen Ding 1
1 West China Hospital, Sichuan University, Orthopedics, Chengdu, China
Introduction: To analyze the biomechanical characteristics of two special constructs of 3-level hybrid surgery through a finite element analysis. Material and Methods: A finite element model of a healthy cervical spine (C0-T1) was constructed. Five surgical models were developed. They were FAF model (C4/5ACDF+C5/6CDA+C6/7ACDF), AFA model (C4/5CDA+C5/6ACDF+C6/7CDA), FFF model (C4/5ACDF+C5/6ACDF+C6/7ACDF), F model (C5/6ACDF) and A model (C5/6CDA). A 75-N follower load and 1.0-N·m moments were applied to the top of the cervical spine model to produce flexion, extension, lateral bending and axial rotation in the intact model. The ROMs of cervical spine, facet pressure, intradiscal pressure and prosthesis pressure were recorded. Results: In FAF model, the ROMs of the total cervical spine and the FSU decreased by 34.54%, 54.48%, 31.76%, 27.14% and 56.56%, 59.17%, 62.04%, 53.57% in the flexion, extension, lateral bending and axial rotation directions, respectively, compared with the intact cervical spine model. In FFF model, the ROMs of the total cervical spine and the FSU decreased by 55.96%, 54.58%, 46%, 46.87% and 90.79%, 89.7%, 88.14%, 85.36% in the flexion, extension, lateral bending and axial rotation directions, respectively, compared with the intact cervical spine model. In AFA model, the ROMs of the total cervical spine and the FSU decreased by 20.97%, 16.74%, 12.75%, 15.45% and 33.68%, 30.4%, 26.6%, 32.75% in the flexion, extension, lateral bending and axial rotation directions, respectively, compared with the intact cervical spine model. In FAF model, the ROMs of the C5/6 level was 7.48°, 5.35°, 8.33° and 7.47°in the flexion, extension, lateral bending and axial rotation directions, respectively. In A model, the ROMs of the C5/6 level was 7.36°, 5.25°, 8.2° and 7.32°in the flexion, extension, lateral bending and axial rotation directions, respectively. The ROMs of the adjacent segments, the intradiscal pressure and the facet contact force in FAF model and AFA model were lower than FFF model in all directions. The maximum prosthesis pressure of Prestige-LP in FAF model was similar compared with A model in all directions. The maximum prosthesis pressure of screws in FAF model was higher compared with FFF model in all directions except left lateral bending. The maximum prosthesis pressure of screws in AFA model was higher compared with F model and FFF model in neutral, flexion and extension. Conclusion: The two special constructs of 3-level hybrid surgery could remain more ROMs of cervical spine, while has fewer biomechanical effects on the adjacent segments compared with ACDF. The CDA segments of two special constructs was safe and effective, but the prosthesis pressure of screws increased.
469
A252: Framingham Cohort Adjacent Segment Biomechanics Following T10-Pelvis Spinal Fusion: A Computational Study
Christian Rodriguez 1 , Rachit Kumar 1 , and Comron Saifi 1
1 University of Pennsylvania, Department of Orthopaedic Surgery, Philadelphia, PA, USA
Introduction: Proximal junctional kyphosis (PJK) and failure (PJF) are challenging complications of long fusion constructs for the treatment of adult spinal deformity (ASD). Few studies have investigated the biomechanics of long spinal fusions, none of which accounted for anatomical variation. This study seeks to use a large cohort to understand the biomechanical stresses proximal to the upper instrumentation of a T10-pelvis fusion depending on the type of simulated motion. Material and Methods: The pre-fusion models were subject-specific thoracolumbar spine models that incorporate the height, weight, spine curvature, and muscle morphology measurements of 250 individuals from the Framingham Heart Study Multidetector CT Study. To create post-fusion models, the subject-specific models were further modified to eliminate motion between the intervertebral joints from T10 to the pelvis. Simulated motion included neutral standing, axial rotation, trunk flexion, and ‘pushing a force’. Due to an absence of in vivo data on kinematic changes following long spinal fusion, both increased segmental mobility and unchanged segmental mobility were modeled for each simulated motion. OpenSim analysis tools were used to calculate the medial lateral shear force, anterior posterior shear force, and compressive force on the T9 vertebra during the simulated motions. A paired sign rank t-test was used to compare the pre-fusion and post-fusion models. Results: Differences between pre-fusion and post-fusion T9 biomechanics were consistent between increased segmental mobility and unchanged segmental mobility conditions. Unchanged segmental mobility results are reported. During trunk flexion, compression decreased from 1583 N pre-fusion to 1170 N post-fusion (t [249] = 36.61, P < .001). Axial twist had a compression decrease from 889.2 N-735.4 N (t [249] = 21.28, P < .001). Standing (t [249] = 9.33, P < .001) and ‘pushing a force’ (t [249] = 29.46, P < .001) motions also saw significant decreases in compression. Anterior-posterior shear force significantly decreased from 74.69 N-33.98 N (t [249] = 22.21, P < .001) during ‘pushing a force’. Anterior-posterior shear force significantly increased from 23.16 N-204.2 N (t [249] = 34.99, P < .001) during trunk flexion and significantly increased from 93.35 N-143.7 N (t [249] = 18.08, P < .001) during axial twist. Changes in medial-lateral shear forces were clinically insignificant for the simulated motions of standing, axial twist, and ‘pushing a force’ due to force changes being less than 1 N. During trunk flexion, medial lateral shear force significantly increased from 115.8 N-157.1 N (t [249] = 20.92, P < .001). Conclusion: This computational study provided the first use of subject-specific models to investigate the biomechanics of long spinal fusions. Patients undergoing T10-Pelvis fusion were predicted to have increased shear forces and decreased compressive force at the T9 vertebra, independent of change in segmental mobility. The results suggest that more research is needed to understand how shear forces affect vertebral body integrity. Despite its limitations, this computational model shows potential for the investigation of spinal fusion biomechanics in order to reduce the risk of PJK or PJF.
OP29: Novel Technologies
1709
A253: Comparing Hyper-Lordotic and Less-Lordotic Cages for Achieving Segmental Lumbar Lordosis During Transforaminal Lumbar Interbody Fusion in Adult Spinal Deformity Surgery
Justin Mathew 1 , Meghan Cerpa 1 , Nathan Lee 1 , Venkat Boddapati 1 , Gerard Marciano 1 , Zeeshan Sardar 1 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
Introduction: Transforaminal lumbar interbody fusion (TLIF) is a posteriorly-based interbody fusion approach used to improve both lower lumbar segmental sagittal alignment and fusion rates in adult spinal deformity surgery. The interbody cages used in TLIF procedures have evolved, with newer hyper-lordotic cages now available, which are assumed to provide more segmental lordosis; however, the evidence on this remains scant. Material and Methods: 38 consecutive patients who received open TLIF procedures performed by a single surgeon between 2017 and 2018 were reviewed. 20 patients had “hyper-lordotic cages” (20°lordosis), while 18 patients had “less-lordotic” cages (6°lordosis). 23 patients had single-level TLIF procedures and 15 had two level TLIF. Standard radiographic measurements, including Cobb angles and SLL were assessed preoperatively, postoperatively, and at one year follow up. Changes in SLL were compared using Student’s and paired t-tests. Results: In one and two-level open TLIF, both hyper-lordotic and less-lordotic cages produced significant improvement in SLL. Among those receiving a one-level TLIF, SLL increased 9.6° (P = .006) in those with less-lordotic cages; it increased 9.2° (P = .004) in those with hyper-lordotic cages. Among those receiving a two-level TLIF, SLL increased 12.4° (P = .045) in those with less-lordotic cages; it increased 11.5° (P = .006) in those with hyper-lordotic cages. However, the improvement in SLL was not significantly different between the two cage types in either one or two-level TLIF procedures (P = .907, P = .877). At one year follow up, there remained no significant difference in the change in SLL between the hyper-lordotic and less-lordotic cages (P = .55). Conclusion: Although it is theorized that hyper-lordotic cages would increase SLL during open TLIF procedures greater than less-lordotic cages, our data failed to
demonstrate that. As our study examined cases performed by a single surgeon immediately before and after adoption of these lordotic cages, it is likely that surgical technique is of equal or greater importance in improving SLL than the amount of lordosis designed into interbody cages. Hyper-lordotic cages do not produce significantly more SLL than less-lordotic cages in posterior open TLIF procedures.
1159
A254: Safe and Improved Bone Removal Using a New Curved Device: Four Center Experience with 624 Patients
John Peloza 1 , Hani Malone 2 , Larry Khoo 3 , Michael Millgram 4 , Scott Kutz 5 , Richard Guyer 6 , Jean Charles Le Huec 7 , Ely Ashkenazi 4
1 Center For Spine Care, Dallas, TX, USA
2 Scripps Clinic Torrey Pines, La Jolla, CA, USA
3 The Spine Clinic of Los Angeles, Los Angeles, CA, USA
4 Assuta Medical Center, Israel Spine Center, Tel Aviv, Israel
5 Minimally Invasive Neurosurgery of Texas, Plano, TX, USA
6 Texas Back Institute, Plano, TX, USA, 7 Bordeaux University School of Medicine, Bordeaux, France
Introduction: Spinal procedures often require the removal of bony tissues to prevent nerve compression and reduce pain. In order to reach difficult-access spinal regions such as the foramen, the surgeon is often required to remove healthy supporting bone structures, therefore increasing the risk of spinal instability. This study describes the authors’ experience with a recently developed, FDA-approved, curved shielded drill, designed to efficiently remove bone from difficult-access areas. Material and Methods: 653 patients were treated using the device by six experienced surgeons in four centers since 2013. Procedures included lumbar, cervical and thoracic decompressions and fusions, 108 of which were minimally-invasive. Device-use duration was recorded and surgeon assessment was obtained using questionnaires. TLIF (transforaminal lumbar interbody fusion) surgery duration, length of stay and complication rates were compared with same-institution controls (65 procedures). Data from the literature and the financial department was used to calculate the estimated cost reduction due to the use of the device. The rate of device-related dural tears was calculated and compared with global device-related dural tear rate associated with the device, calculated from 1417 safety-records of procedures and with the literature. Results: One device-related dural tear (< .2%) was reported, a similar rate to the global device-related dural tear rate of the device (0.2%) and lower than previously published device-related tear rate of 2.9% associated with the Kerrison rongeur and high-speed drill. Surgeon satisfaction rate was 99%. Surgery time reduction was the most common comment in surgeon questionnaires. Lumbar foraminotomy using the device required, on average, 2 minutes and in some cases enabled the surgeon to avoid a spinal fusion since the improved access eliminated the need for excessive bone removal. Length of stay in these cases was shorter by 0.6 and 3.4 days compared with control decompressions and fusions, respectively. An average of 1.7 device passes was required for each foramen. Cervical osteophyte removal required on average 3 minutes and often enabled the surgeons to avoid additional level surgery. TLIF procedures required, on average, 23 minutes less than control procedures, after controlling for patient characteristics and procedure year (P < .01). A 0.5 days reduction in length-of-stay and a reduction of 55% in complication rates, were also noted. The estimated cost reduction was approximately $2000/procedure. Conclusion: The device is safe and effective for performing spinal surgery in various settings. Procedure time reduction was noted as the most significant advantage by the surgeons.
1801
A255: Digital and Sensor-Based Training in Spine Surgery-The Future of Education?
Hans-Jörg Meisel 1 2 , Werner Korb 3 , Philipp Gernerth 3 , Lukas Panzenboeck 4 , Alvaro Cordoba 5 , Oliver Muensterer 6 , Hubertus Feussner 7 , and Christoph Mehren 8
1 BG Klinikum Bergmannstrost Halle, Neurosurgery and Spine Surgery, Halle, Ger
many 2 Danube University Krems, Krems, Austria
3 Vocationeers, Hallein, Austria
4 Orthopaedic Hospital Vienna-Speising, Spine Surgery, Vienna, Austria
5 Uruguay British Hospital, Montevideo, Uruguay
6 Ludwig-Maximilians-Universität, Haunersches Kinderspital, Munich, Germany
7 Technical University Munich (TUM), University Hospital rechts der Isar, Munich, Germany
8 Schoen Clinic München Harlaching, Spine Surgery, Munich, Germany
Introduction: New training and simulation concepts need to hold up with rapidly emerging technologies. To support these steady developments and the unstoppable digitalization, a new training concept with sensors was introduced in spine training. In preliminary studies a simulation system was used and extended with a sensor system. Five medical specialists and five medical resident medical staff from the area of orthopedic, trauma, and neurosurgery performed a microsurgical discectomy on this system (cf. Mehren C: Global Spine Journal, 1-8, 2020). Based on these results a new study was performed and the web-based technology MySebastian was developed and analyzed to integrate these sensor data into training. Material and Methods: Based on the results of the study (Mehren C, 2020), a cognitive task analysis (ACTA) was performed. For this study a qualitative research design, based on a guided expert interview, was chosen. As preliminaries for this study the pains and gains, as well as the specific difficulties, but also the chances in terms of training in medicine and surgery were modelled. Based on these results a first version of a semi-structured questionnaire was drafted. With this first version the first two experts were interviewed. All interviews were recorded with a handy recorder and afterwards transcribed with an analytics software. Afterwards the transcript was analyzed and all relevant statements made by the expert were collected. Then the first codes were defined inductively and the collected statements were assigned to the appropriate code. After every interview the authors discussed the transcripts and the collected statements to improve the questionnaire. With every interview this process was repeated and also the codes were in constant change. This circular and iterative research approach (the Flick-approach) was chosen to retrieve a maximum of information and do the generation of a first theory. Results: We derived iteratively five different Code Categories, which include (1) Issues of Training in Medicine (total: 62; 27,43 %), (2) Tools / Apps / Social Media in Training (55; 24,34 %), (3) Assessment, Sensor Data and Benchmarking in Training (44; 19,47 %), (4) Videos in Training (42; 18,58 %), (5) Workflows and Procedures in Training (23; 10,18 %) and in TOTAL (226; 100,00%). In total this shows that most of the experts agreed on (1) limited budgets for courses and technologies in education; (2) structural problems (generation issues, limited research for training/education); and (3) not enough time for training and limited personnel. As a further result a first prototype of the web-platform (Beta version) of MySebastian was developed for surgical training and expertise management: https://beta.mysebastian.at. Conclusion: Based on the findings we can summarize that training in surgery is insufficient. Therefore, the path to implement successful educational concepts goes over the experts more than the trainees. Consequently, a solution (mySebastian web platform) was developed for the experts that save time and money, facilitate the training process as well as introduce state of the art educational concepts. Future work and validation of the software will show whether this first steps are going into the right direction.
375
A256: Patient perspectives on artificial intelligence in healthcare decision making
Matthew Parry 1 , Edward DelSole 1
1 Geisinger Health System, Scranton, USA
Introduction: Artificial intelligence (AI), specifically, machine learning is a powerful tool that can in many cases improve diagnostic accuracy, treatment decisions, and outcome prediction for patients presenting with an orthopaedic issue. The goal of this study is to evaluate patient perspectives on AI in healthcare and seeks to identify patient characteristics that influence those perspectives. Material and Methods: A 37-question survey was randomly distributed to 2101 orthopaedic surgery patients in a large integrated health system with 184 patients as the final analytical population. The primary outcome, average level of comfort with AI, was assessed by thirteen questions using a Likert scale graded from 1 through 10. Secondary outcomes included categorical measures of perceived impact of AI in orthopaedic care, perceived impact of AI on healthcare costs, whether patients would refuse AI if it increased healthcare costs, and whether patients believe it’s acceptable for a doctor to sell health data to a third party for the purpose of building intelligent computers for use in healthcare. Descriptive statistics were calculated for baseline demographic, education, orthopaedic, and technology use data as well as on data relating to patients’ perspectives on the use of AI in healthcare. Generalized linear multivariable regression models were run to predict differences in average AI comfort level. Bivariate analyses were also performed between the secondary outcomes and demographic, orthopaedic, and technology use predictors. Results: The average AI comfort level among the analytical population was 6.3 (SD: 2.5). Average AI comfort level differed significantly between age groups (P = .0022), with older participants having the highest average comfort level and younger patients with the lowest, (55+ years old, mean 6.9; SD: 2.3, 45-<55 years, mean 6.0; SD: 2.4, 30-<45 years, mean 5.6; SD: 2.6, 18-< 30 years, mean 4.1; SD: 2.1). Comfort level differed as a function of education (P = .0004), with patients with a graduate degree having the highest average (mean: 7.4; SD: 2.0) and patients with less than high school having the lowest average (mean: 2.8; SD: 2.0). Secondary outcomes relating to patients’ perspectives on AI in healthcare were all significantly associated with average AI comfort level in the expected directions (P < .05). In the multivariable model, only perceived impact of AI in orthopaedic care and survey format remained significantly associated with average AI comfort level. Conclusion: Older orthopaedic patients are on average more comfortable with AI being integrated into their healthcare team, when compared to younger patients. Similarly, patients with a higher degree of education were more comfortable with AI incorporation, as compared to patients with a lower education level. Patients who had a high primary outcome of average comfort level also saw AI as a positive improvement, felt AI would decrease the healthcare cost, would not refuse care if AI increased the cost, and were comfortable with physicians selling data to third parties to create intelligent computers. These results indicate that younger and more uneducated patients may be apprehensive to the use of AI in their healthcare team, while older and more educated patients will likely view the addition as beneficial.
875
A257: Development of a Non-Opioid Biodegradable Sustained Release Formulation for Local Postoperative Analgesia
Jasper Steverink 1 2 , Susanna Piluso 1 2 , Jos Malda 1 3 , Marianna Tryfonidou 3 , Raymond Schiffelers 4 , Floris van Tol 1 2 , Bas Oosterman 2 , and Jorrit-Jan Verlaan 1 2
1 University Medical Center Utrecht, Orthopedics, Utrecht, The Netherlands
2 SentryX B.V., Austerlitz, The Netherlands
3 Utrecht University, Clinical Sciences, Utrecht, The Netherlands
4 University Medical Center Utrecht, Clinical Chemistry & Haematology, Utrecht, The Netherlands
Introduction: Instrumented spinal surgery ranks amongst the most painful surgeries overall. Most pain is likely elicited by local damage and pressure to the periosteum induced by spinal implants. This severe pain is conventionally treated systemically with opioids. The frequency and severity of opioid-related adverse events are actual topics of societal debate and spark the development of non-opioid alternatives. In this study, a hydrogel-based biodegradable sustained release formulation (BSRF) is developed to provide local sustained release of an anesthetic to the periosteum with minimal systemic effects. Following release, the BSRF is degraded in situ. The BSRF is co-implanted with pedicle screws during surgery, providing analgesia at the source of pain. Its robustness and flexibility ensure excellent adaptation to the bone surface and the BSRF can be implanted without changing the current surgical workflow. The BRSF aims to decrease opioid consumption and shorten hospital stay following spinal surgery. Material and Methods: A gelatin-based biopolymer wa\s functionalized with photo-crosslinkable chemical moieties and used to prepare hydrogels by exposure to visible light. Hydrogels were characterized by swelling measurements, rheometry and dynamic mechanical analysis. The morphology of the hydrogels was assessed by scanning electron microscopy. In vitro drug release and drug loading efficiency was studied for 168 hours and quantified by UPLC. Furthermore, in vitro cytotoxicity was evaluated using human mesenchymal stem cells and NIH3T3 mouse fibroblasts by performing Live/Dead and Alamar blue assays after 24 and 48 hours in culture in standard growth medium. Hydrolytic and enzymatic degradation was assessed in vitro. Implantability combined with pedicle screws and in vivo release was assessed in a sheep model for instrumented spinal surgery. Results: The hydrogel was sufficiently robust (maximal compressive force >500 N, elastic modulus ∼300 kPa) to allow implantation during pedicle screw placement and also displayed self-healing properties. The hydrogel encapsulated 52.5 mg/mL bupivacaine, and provided >120 hours of sustained drug release in vitro. Release was characterized by a slight initial burst, followed by a more linear phase. The hydrogel did not lead to major in vitro cytotoxicity (cell viability >80%) and enzymatically degraded within four weeks. The BSRF released bupivacaine up to 72 hours in vivo. Conclusion: A BSRF for postoperative analgesia was developed and displayed promising characteristics, such as sufficient mechanical robustness, good cytocompatibility and prolonged drug release in vitro and in vivo. Animal studies are currently conducted to investigate safety of the BSRF and analgesic efficacy. The hydrogel could also serve as a platform for other types of drugs and is easily combined with various other orthopedic implants.
1647
A258: The “Raising Roof” Cervical Expansive Laminoplasty with Preservation of Bilateral Muscular-Ligament Complex
Yu Sun 1
1 Institute of Spine Surgery, Peking University Third Hospital, Department of Orthopaedic Surgery, Beijing, China
Objective: To evaluate the clinical outcome of “Raising Roof” cervical expansive laminoplasty using customized 3D printed artificial lamina through inter-muscular space with preservation of bilateral muscular-ligament complex. Method: The current procedures of cervical expansive laminoplasty like open-door and French-door laminoplasty have achieved satisfactory outcome in terms of thorough spinal cord decompression and good neurological recovery. At the meantime, some complications, such as destruction of muscular ligament complex, limited enlargement of spinal canal, door re-closing and hinge fracture..., have existed all the time. Many surgeons developed modified procedures but can only solved the problems from certain point of view. This procedure takes the approach through the muscle space between semispinalis cervicis and capilis. The bilateral laminae are cut through at the junction of laminar and lateral mass. The lamina is lifted up with all the muscles and ligaments attached to the lamina and spinal process. The customized 3D printed artificial lamina are inserted into the gap of cutting edge of laminar and lateral mass and fixed with screws. The laminar is raised like the roof of spinal canal. The bilateral muscular ligament complex are well preserved. Results: 22 cases received this procedure between June and September 2019. The operation included C4-C6, C3-C6 and C4-C7. The operating time is 100-180 minutes. The blood lose is 50-300 ml. The post-operative drainage is 110-150 ml. Patients are encouraged to start neck mobilization including flexion, extension and rotation. No collar applied. The average hospital stay is 2.2 days. The JOA score improved 1-3 on discharge. The VAS for neck pain was 1-3. The spinal canal enlarged significantly. Cervical spinal cord decompressed thoroughly. Conclusion: The “Raising Roof” procedure of cervical expansive laminoplasty using customized 3D printed artificial lamina through inter-muscular space has showed satisfactory outcome in the early post-operative stage. The muscular ligament complex have been well preserved with good spinal cord decompression. This procedure may have the better application prospects in clinical practice.
1635
A259: Nano Topography is More Important than the Coating Itself: Titanium Versus CaP Nanocoated Cages
Willems Karel 1 ,AmélieWillems 1
1 AZ Delta Roeselare, Orthopaedic Surgery, Roeselare, Belgium
Introduction: Posterior interbody fusion is frequently used to treat degenerative low back pain. Titanium (Ti) cages are considered the gold standard, but the more elastic PEEK cage seems to result in better clinical and radiological outcome. PEEK is an inert material that does not promote bony ingrowth. A micro surface is created by glas blasting and this engineered topography is important to orientate cells, to increase the wettability of the surface to blood, to promote adhesion of cells to the surface and to facilitate binding of fibrins, matrix proteins, growth and differentiation factors. Several types of nano coating have been used to combine the mechanical characteristics of PEEK with a bioactive layer. A randomized controlled, double blind multicenter parallel three arm study the clinical and radiographic outcome of posterior lumbar interbody fusion (PLIF) at one level was assessed for implantations of PEEK cages, with Ti coating (TSC) or CaP coating (osteoCon) or uncoated (reCreo) cages. Material and Methods: Patients between 18 and 75 years with chronic mechanical low back pain with or without radiation into the leg (>6 months) refractory to pharmacological and non-surgical conservative treatment scheduled for stabilization and decompression via PLIF approach utilizing supplemental posterior fixation were randomly assigned to receive implantation of PEEK cages, with Ti coating (TSC) or CaP coating (osteoCon) or uncoated (reCreo) cages. The primary radiological outcome was the implant stability and fusion status assessed with X-ray, standing A/P and lateral radiographs and CT-scan at 6 and 12 months. The CT-scans were evaluated by an independent experienced spine radiologist, blinded to the used spacer. The primary clinical outcome was the evolution from baseline in pain, disability and quality of life. Clinical evaluation was performed pre-operatively, and at 6 weeks, 3 months, 6 months and 12 months. Patients were asked to report pain for the leg and for the back on a 10-point visual analogue scale (0 no pain and 10 the worst imaginable pain), and to fill out the Oswestry Disability Index (ODI) and the SF-36 was used pre-operatively and after 12 months. Results: An engineered surface topography is important in developing nano coated PEEK cages. The created micro roughness of the surface is in the micro meter range, and this surface is covered by a coating layer of 250 nm(with variation of 45 nm). In our clinical study there is no clinical and no radiographic statistical difference between thv CaP and Ti nano group. Titanium is more bioactive than CaP. Conclusion: We conclude that the engineered topography is the fundamental for nano-coated PEEK cages.
1397
A260: Shape Memory Polymer Added with Monitoring System for the Invention of Intelligent Brace
Dechun Wang 1 and Weidong Liu 2
1 Qingdao Municipal Hospital, Qingdao, China
2 Jilin University, Changchun, China
Introduction: The shape memory polymer (SMP) can be designed and used for bracing. The brace wearing situation can be monitored by the intelligent system composed of force sensor, printed circuit board (PCB) and PC or mobile phone. Up to seven force sensors could be attached on the inner surface of the brace to collect the forces being imposed by the brace and connected to the PCB by thin wires. The force would be transferred to the cloud storage by the mobile phone app. The thoracolumbosacral orthosis (TLSO) were usually used to prevent worsening of the condition. Accurately evaluating the effectiveness and compliance of bracing is an on-going challenge for physicians. Material and Methods: To better monitor the effectiveness and compliance of bracing, the platform of the custom-designed hardware, mobile phone app as well as cloud storage on the web were developed. The hardware consists of thin and flexible force sensor, PCB with CPU, Li-ion battery, plug-in software, data storage, Bluetooth etc. Results: A kind of rigid SMP for brace production was specially designed to ensure no shrinkage and superior fixation for increasing the likelihood of comfort. Any part of the SMP brace could be changed from one shape to another at a low temperature, 75°C. Further, the SMP had better mechanical properties, such as tensile strength and hardness etc., which could make the brace thinner and lighter compared with the normally used materials, for example, polyethylene (PE) and polypropylene (PP). The intelligent system results demonstrated that it could be able to accurately detect the real time of brace wear and force imposed by the brace. Conclusion: SMP provides more opportunities than other usually used materials to adjust the brace during the treatment. The intelligent monitoring system establishes a quantitative relation of the wearing time and the force imposed by brace, which dramatically helps the physician to monitor and analyze the effectiveness and compliance of bracing.
1799
A261: Early Minimally Invasive Surgery is Associated with Improved Clinical Outcomes in Patients with Traumatic Spinal Fractures and Ankylosing Spondylitis
Fahid Rasul 1 , Mathew Sewell 1 , Fady Sedra 1 , Syed Aftab 1 , Suresh Pushpananthan 1 , Jonathan Bull 1 , Arun Ranganathan 1 , and Alexander Montgomery 1
1 Royal London Hospital, Department of Spinal Surgery, London, United Kingdom
Purpose: Patients with ankylosing spondylitis (AS) have a high propensity for spinal fractures following relatively minor trauma. These fractures are inherently unstable and require surgical stabilisation to allow early rehabilitation. We report our unit’s experience of managing this complex patient cohort focussing on the role of early surgery and minimally invasive surgery (MIS). Methods: Retrospective review of prospectively collected electronic database. All patients with a diagnosis of spinal fracture and AS who underwent spinal surgery between December 2017 and July 2020 at Royal London Hospital (RLH) were included. Patient demographics, radiological fracture characteristics, surgical procedure details and clinical outcomes were extracted by case note review. Study methods were compliant with the STROBE checklist. Results: 22 consecutive AS patients with traumatic spinal fractures were admitted to RLH during the study period. 20 operations were performed and one patient was managed non-operatively. Male:Female = 20:2. Mean age = 73.1 years (range 45-90 years). Median number of spinal levels fixed = 6 (range 4-14) with one reported metalwork failure. Mortality at 30 days = 22.7% (5/22) all of which were related to respiratory complications. 10 patients experienced post-operative complications (10/20 = 50%). Patient reported back pain improved following surgery (P < .0001 t-test 95% CI = 4.25-5.62). 5 patients underwent MIS. The MIS subgroup experienced a statistically significant lower rate of post-operative complications (0 vs 10 P = .0396, Chi-squared), shorter length of inpatient hospital stay (8 days vs 31 days P = .0148, paired t-test) and reduced operative time (138.8 mins vs 249.6 mins P = .0111, paired t-test) compared to the open surgery subgroup. Those patients who had early surgery (<3 days after admission) experienced less complications compared to those that waited >6 days prior to intervention (17.6% vs 80% P = .0207 Chi-squared test). Conclusion: Spinal fractures in patients with ankylosing spondylitis are challenging fractures to manage mainly due to associated medical comorbidities and poor bone quality. Surgical stabilisation at the earliest opportunity improve chances of recovery and reduces the risk of complications. Long segment construct and circumferential fusion when feasible are advised. Minimally invasive techniques are potentially beneficial and may improve patient’s clinical outcomes.
OP30: Deformity-Thoracolumbar (Adolescent) 2
1097
A262: Risk Factors for Implant Failure in Spinal Deformity Correction Surgery. A Cohort Study of 365 Cases
Francisco Javier Alonzo González 1 , Jorge Nuñez Camarena 2 , Rudolf Herrera 1 , Sergio Antonio Castillo Rivera 3 , Salvador Fuster 4 ,and Pedro Fernández 5
1 Hospital "Ceibal" Accidentes I.G.S.S., Guatemala, Guatemala
2 Hospital Mútua Terrassa, Terrassa, Spain
3 Hospital Dr. Sótero del Rio, Santiago, Chile
4 Hospital Clínic i Provincial, Barcelona, Spain
5 Hospital La Fe, Valencia, Spain
Introduction: Implant failure (pull out, loosening or breakage) is a common complication after spinal deformity correction surgery in pediatric patients that can cause loss of the correction achieved in the primary surgery or reintervention. The objectives of our study were: 1. Determine the current incidence of implant failure in pediatric deformity correction surgery 2. Analyze protective and risk factors for implant failure in pediatric deformity correction surgery. Material and Methods: We analyzed 365 patients that underwent surgical treatment in our center for spinal deformity correction. 15 patients with radiological or clinical incomplete records were excluded from the study. All our patients were 18 years old or younger at the time of the intervention. Retrospective revision of clinical and radiological records were performed by two orthopaedic spine surgeons. Variables included in the study were type of scoliosis, Cobb angle (pre-operative and post-operative), type of surgery, indication for surgery, implant type, number of implants included in the fixation, implant density, use of iliac screws, and demographic variables. Results: 365 patients were analyzed. 68.8% of the patients were female. Middle age was 13.1 years (Standard deviation of 4.3). The overall implant failure rate was of 11.5%. Between these patients the most common type of failure was the pull out (71.4%). Risk factors for implant failure were neuromuscular scoliosis and syndromic scoliosis, higher number of levels included in the fixation, reintervention with a change of implant choice, use of iliac screws, use of growing rods and VEPTR. Documented protective factors against implant failure were higher age and higher density of implants, both presenting with significantly lower rates of implant failure. Conclusion: Our study showed an overall rate of implant failure of 11.5% in pediatric deformity correction surgery, being the implant pull out the most common type of failure. Protective factors against implant failure were higher patient age and implant density in the fixation. Risk factors for implant failure were neuromuscular or syndromic scoliosis, longer fixations, iliac fixation, reintervention with implant change and the use of growing rods or VEPTR.
1173
A263: Is isolated Pulmonary Function Test (PFT), sufficient to asses the pulmonary status in scoliosis deformity correction cases?
Jvaghar Jill 1 , Nalli Ramanathan Uvaraj 2 , and Sathish Muthu 3
1 Madras Medical College, Orthopaedic Spine Surgery, Chennai, India
2 Madras Medical College, Orthopaedic Spine Surgery, Chennai, India
3 Madras Medical College, Orthopaedics, Chennai, India
Introduction: Scoliosis is a three-dimensional deformative abnormality of the spine. There is substantial interest in the relationship between spinal deformity and pulmonary function due to potentially high rates of morbidity and mortality. The deformed structures compress the lung parenchyma causing a decrease in lung volume and its compliance. These changes along with the increased effort to breathe may result in alveolar hypoventilation, hypercapnia, and hypoxemia leading to cor-pulmonale and right-sided heart failure. Since poor pulmonary function may lead to a higher incidence of postoperative pulmonary complications, preoperative pulmonary function tests (PFT) have commonly been used to predict postoperative complications concerning the severity of scoliosis. The objective of this study was to assess whether PFT was sufficient to evaluate the improvement in pulmonary function pre and post-deformity correction. Materials and methods: This was a retrospective analysis among patients with thoracic or thoracic lumbar scoliosis who were admitted to our institution for deformity correction between June 2014 to June 2019. The patients enrolled in the study were aged between 10-17 years, had a preoperative diagnosis of predominant thorasic scoliosis with a pre-operative PFT available for analysis. All the included patients were followed up radiographically along with the pulmonary function tests to measure total lung capacity (TLC), forced vital capacity(FVC), and forced expiratory volume in one second (FEV1) along with a functional assessment of the lung capacity. Each test was repeated three times and the single best effort was recorded. We focussed on percent predicted values of FVC and FEV1 to asses restrictive lung disease. Results: 17 patients were included in the study, with a mean age of 13.7 (10-17 years) at deformity correction. 8 patients had congenital scoliosis and 9 had adolescent idiopathic scoliosis. The mean preoperative FVC was 1.552 and percent predicted FVC was 63%. After posterior instrumentation corrective surgery, the mean FVC was 1.803 and percent predicted FVC was 66.5%. At 2years follow-up, PFT did not show any improvement for the correction of curves involving 5 levels or more. Patients with severe scoliosis with preoperative severe restriction showed a significant improvement of percent predicted FVC from 37% to 59% (P < .05). However, functional improvement was noted in the rest with significant improvement in right heart pressure with no significant improvement in PFT. Conclusion: Despite demonstrating a significant improvement in their functional status corresponding improvement in their pulmonary function was not noticed which raises the question that whether these cases had a lung compromise, to begin with, or whether pulmonary compensation was established before the surgery. Since PFT was the only measure utilized to assess the status of the lung, we probably could not essentially establish the extent of the lung compromise pre-operatively. We recommend additional measures to asses on going right heart compensation with echocardiography and pulmonary artery pressure to objectively establish the pre-operative pulmonary status beforehand.
809
A264: Comparison of Flexibility Assessments in Adolescent Idiopathic Scoliosis (FLEXIS)
Kenny Yat Hong Kwan 1 , Caglar Yilgor 2 , Ahmet Alanay 2 , and Kenneth Man Chee Cheung 1
1 University of Hong Kong, Hong Kong, Hong Kong
2 Acibadem University School of Medicine, Istanbul, Turkey
Introduction: There is no consensus as to which type of dynamic radiograph is optimal in predicting the true flexibility of a curve in adolescent idiopathic scoliosis (AIS) or the final behavior of the curve post-surgical correction. This study aims to investigate the flexibility equivalence of different bending methods. Material and Methods: Patients diagnosed with AIS who had reached the threshold for surgical correction were prospectively recruited in two centres. Data regarding demographics, concomitant treatment and curve characteristics were obtained. Radiographs of standing whole spine, supine side-bending, awake traction, supine traction under general anaesthesia (STUGA) and fulcrum bending were performed preoperatively. The following formulae were calculated to determine which type(s) of flexibility films were most accurate in predicting the final behavior of the curve post-surgical correction: Flexibility index (%) = [(Pre-operative Cobb angle - Bending Cobb angle)/Pre-operative Cobb] x 100% Correction rate (%) = [(Pre-operative Cobb angle-Post-operative Cobb angle)/Pre-operative Cobb angle] x 100% Correction index (%) = (Correction rate/Flexibility) x 100%. Results: 132 patients (19 male and 113 female) with a mean age at the time of surgery of 14 ± 1.74 years were recruited from Turkey and Hong Kong. Patients were analysed according to curve patterns. 90 patients had thoracic major curves. The correction indices were 508.9 ± 159.2%, 183.0 ± 193.5%, 135.5 ± 97.4%, 153.1 ± 21.1% and 139.6 ± 22.9% for supine, supine side bending, fulcrum bending, awake traction and STUGA respectively. For lumbar major curves (n = 42), the correction indices were 342.4 ± 209.6%, 138.4 ± 72.3%, 121.5 ± 39.6%, 131.6% and 136.5 ± 67.6% respectively. Conclusion: The correction index takes into account the inherent curve flexibility, and an index close to 100% suggests that the instrumentation has taken up all the flexibility revealed by the dynamic radiograph. This study showed that for thoracic curves, the fulcrum bending radiograph most accurately predicted post-operative curve correction, whereas for lumbar curves, all dynamic radiographs apart from supine films showed similar predictability for curve correction. Fulcrum bending radiographs can help preoperative planning for AIS surgeries including the need for intraoperative releases and fusion level determination, particularly for thoracic curves.
975
A265: Changes in shoulder balance and prediction of final shoulder imbalance during growing-rod treatment for early-onset scoliosis: a case series
Ziyang Liu 1 , Tie Liu 1 , and Yong Hai 1
1 Department of Orthopedic Surgery, Beijing Chaoyang Hospital, Capital Medical University of China, Department of Orthopedic Surgery, Beijing, China
Introduction: Achieving and maintaining shoulder balance after the entire growing-rod (GR) treatment is essential for early-onset scoliosis (EOS) patients. However, few studies have reported the outcomes of shoulder balance after the entire GR surgery in EOS patients, and the risk factors for shoulder imbalance after final fusion in EOS patients have been understudied. This study investigated changes in shoulder balance of early-onset scoliosis (EOS) patients during the GR treatment, analysed risk factors for final shoulder imbalance, and evaluated the satisfaction of patients' parents with shoulder balance after the treatment. Material and Methods: In total, 24 consecutive 'growing-rod graduates' were studied. Demographic data, surgical-related factors, and radiographic parameters were analysed to identify risk factors for final shoulder imbalance, and shoulder balance changes from GR implantation to last follow-up after fusion were analysed. The satisfaction of parents was evaluated by an adapted questionnaire. Results: Early postfusion shoulder imbalance (odds ratio (OR): 19.500; 95% confidence interval (CI)=1.777-213.949; P = .015) was identified as an independent risk factor for final shoulder imbalance at the last follow-up. Radiographic shoulder height (RSH) was significantly improved after GR implantation (P = .036), and further improved during the postfusion period (P = .021). Through the whole treatment, from GR implantation to the last follow-up after fusion, the value of RSH showed significant improvement (P = .011). Similar trends were also found in other parameters, including clavicle angle (CA), coracoid height difference (CHD), and T1 tilt (T1T). The postimplantation shoulder balance and imbalance patients had no significant difference in final RSH (P > .05), while the shoulder balance significantly improved in patients with prefusion shoulder imbalance after fusion (P = .045). All parents (100%) were satisfied with the final shoulder condition and entire treatment. Conclusion: GR surgery improved shoulder balance. Shoulder balance status after GR implantation did not determine the final status, but final fusion could further adjust the shoulder balance of patients with prefusion shoulder imbalance. For patients with early shoulder imbalance after final fusion, there was a high probability of shoulder imbalance at the final follow-up. Postfusion spontaneous adjustment after final fusion significantly improved shoulder balance.
1587
A266: Should Selective Thoracic Fusion be Reserved for Non-Structural Compensatory Lumbar Curves? Radiographic and Clinical Results from Propensity Matched Patients at Minimum 5-Year Follow-Up
Jay Reidler 1 , Scott Zuckerman 1 , Meghan Cerpa 1 , Joseph Lombardi 1 , Peter Newton 2 , and Lawrence Lenke 1
1 Columbia University Medical Center, New York, USA
2 Rady's Children Hospital, San Diego, USA
Hypothesis: Selective thoracic fusion results in worse radiographic outcomes compared to non-selective fusion for Lenke 1-4C curves, but similar patient reported outcomes for Lenke 1-2C curves. Study Design: Retrospective analysis of multicenter, prospectively collected data. Introduction: For adolescent idiopathic scoliosis (AIS) Lenke Type 1-4C curves, controversy exists whether selective thoracic fusion (STF) is sufficient or non-selective fusion (NSF) should be used to treat the associated lumbar curves. Methods: A prospective, multicenter database was queried for Lenke 1-4C curves (min 5-yr follow up). Patients were dichotomized to STF (fusion L1 or above) vs NSF (fusion below L1). We analyzed two subgroups: 1) non-structural lumbar curves (1-2C), and 2) structural lumbar curves (3-4C). After propensity score matching within each subgroup for age and preop thoracic and lumbar Cobb angles, we conducted within and between group comparisons of radiographic data and SRS-22 scores. Results: Of 124 patients with 1-2C curves, 74 matched (37 STF, 37 NSF). At 5 years postop, both STF and NSF led to improvement in main thoracic (MT) and compensatory lumbar (CL) Cobb angles as well as coronal balance (C7-CSVL), but NSF values were better than STF (P < .05). While SRS total and self-image scores improved for each procedure (P < .05), there were no significant differences in STF and NSF patient reported outcomes (PROs). Of 95 patients with 3-4C curves, 36 matched (18 STF, 18 NSF). At 5 years postop, both STF and NSF led to improvement in MT and CL cobb angles, but again NSF values were better than STF (P < .05). NSF reported better total SRS (P < .02) and self-image (P = .05) scores when compared to STF. Conclusions: In propensity score matched patients treated for Lenke Type 1-2C curves, STF results in slightly less radiographic correction but similar patient reported outcomes as NSF at 5 years. In contrast, matched patients treated for Lenke Type 3-4C curves with NSF have both better radiographic and patient reported outcomes when compared to STF. Summary: In this multicenter study with minimum 5-year follow-up, we performed propensity score matching to compare patients treated with selective thoracic fusion and non-selective fusion for Lenke 1-2C curves vs 3-4C curves. We found that selective thoracic fusion resulted in slightly less radiographic improvement compared to non-selective fusion for all curves. While STF led to similar patient-reported outcome scores as NSF for Lenke 1-2C curves, NSF led to better scores for Lenke 3-4C curves.
78
A267: Fusing to the Pelvis in the Correction of Scoliosis Associated with Rett Syndrome
Brett Rocos1 and Reinhard Zeller1
1Hospital for Sick Children, Toronto, Canada
Introduction: Rett syndrome is a rare disorder characterised by severe, C shaped scoliosis in up to 80% of cases. In the past, posterior spinal fusion has been the mainstay of treatment, most often including the pelvis. However, fusing to the pelvis has been shown to influence function of the spinopelvic relationship, which has been hypothesised to reduce the ability to ambulate in these patients. In this study, we sought to show the results of the surgical treatment of scoliosis in patients with Rett syndrome and analyse the impact of fusing to the pelvis on ambulation. Materials and Methods: A retrospective case series methodology was used to analyse the radiographic, clinical and functional outcomes of consecutive patients treated for Rett syndrome associated scoliosis treated surgically between the ages of 10 and 8 years in a single tertiary referral paediatric spinal unit. Cases were identified through departmental and neurophysiological records, and patients were excluded if the diagnosis of Rett syndrome was not confirmed. Results: Seven eligible cases were identified. The mean coronal Cobb angle was 90.9°, mean sagittal Cobb 72.0° and pelvic obliquity 24.5°. The mean post-operative improvement in coronal Cobb was 53.2° and pelvic obliquity was not significantly improved. These did not change during a mean follow up of 2.7 years. None showed any post-operative complications and of the 4 patients fused to the pelvis, only 1 was able to ambulate preoperatively, and this ability was lost postoperatively. Conclusions: Our data suggests that with modern technology, severe curves can be safely treated, and that fusion to the pelvis is not necessary to prevent curve progression, which may be important in preserving patient mobility post operatively.
1618
A268: Anterior vs Posterior Approach for the Treatment of Lenke 5c Curves in Patients with Idiopathic Scoliosis; Results from the Swedish Spine Registry
Anastasios Charalampidis 1,2 , Hans Möller 1,3 , and Paul Gerdhem 1,2
1 Department of Clinical Sciences, Intervention and Technology (CLINTEC), Karolinska Institutet, Stockholm, Sweden
2 Department of Reconstructive Orthopaedics, Karolinska University Hospital, Stockholm, Sweden
3 Stockholm Center for Spine Surgery, Stockholm, Sweden
Introduction: Adolescents with severe idiopathic scoliosis may be treated with anterior or posterior fusion surgery, although there is no consensus as to which is associated with the best outcome. Moreover, studies with longer term follow-up are limited. Material and Methods: We used data from the Swedish spine registry and identified 59 patients with idiopathic scoliosis treated with fusion for Lenke 5C type curves; 27 patients underwent anterior surgery and 32 underwent posterior surgery. All patients had pre- and postoperative radiographic data and postoperative clinical data at a minimum of 2 year after surgery. Patient reported outcomes measures included the SRS-22r, EQ-5D-3L, EQ-VAS and VAS for back pain. Radiographic assessment included measurement of the Cobb angle of the major curve, curve flexibility, rate of curve correction, any difference in sagittal parameters, number of fused vertebrae and length of fusion. Results: The mean age at surgery was 16 years in both groups. The mean follow-up time was 3.8 years. There were no significant differences in the SRS-22r score and EQ-5D-3L index at follow-up (all P ≥ .1). Postoperatively, both the anterior and posterior fusion group demonstrated a significant correction of the major curve (P ≤ .001) with no significant difference of the correction rate between the groups (P = .4). The posterior fusion group had shorter operative time (P < .001) and higher perioperative blood loss (P = .004) while the anterior group had lower number of fused vertebrae (P < 0.001). Conclusion: The type of surgical approach for Lenke 5C curves is not associated with any measurable differences in health-related quality of life, despite the lower number of fused vertebrae after anterior surgery.
1185
A269: Effect of Tranexamic Acid Dosing on the Percent of Total Blood Lost During Adolescent Idiopathic Scoliosis Surgery
Katherine Krenek 1 , Kristen Jones 2 , Christopher Vara 3 , Natalie Scholz 1 , Allison Wolf 1 , and David Polly , 3
1 University of Minnesota, Department of Orthopaedic Surgery, Minneapolis, USA
2 University of Minnesota, Department of Neurosurgery, Minneapolis, USA
3 Shriners Children’s Twin Cities, Department of Orthopaedic Surgery, Woodbury, USA
Introduction: Posterior spinal fusion (PSF) for adolescent idiopathic scoliosis is associated (AIS) with significant intraoperative blood loss. Tranexamic acid (TXA) is an antifibrinolytic agent that is known to reduce the percent of total blood volume lost during posterior spinal fusion, however the optimal dosing regimen has not been defined. Material and Methods: Fifty-three AIS patients underwent PSF in 2011-2019; 18 received no-TXA, 18 received low dose TXA (10 mg/kg loading 1 mg/kg/hr infusion), and 17 received high dose TXA (30 mg/kg loading, 10 mg/kg/hr infusion). We retrieved relevant demographic, hematologic, intraoperative, and outcomes information from medical records. The primary outcome was percent total blood volume lost (%TBVL) per level fused, calculated from estimates of intraoperative blood loss, estimated total blood volume per patient (via Nadler’s equations), and number of levels fused. Unadjusted outcomes were compared using standard statistical tests. Results: The %TBVL per level fused was significantly lower in the high dose TXA vs no-TXA group (0.9% vs 1.8%; P = .003) and in the low dose TXA vs no-TXA group (1.1% vs 1.8%; P = .03). There was no significant difference in %TBVL per level fused between the high dose TXA and low dose TXA groups (1.1 vs 0.9; P = .75). No patients had documented seizures, DVTs, or PEs. Conclusion: Both high and low dose TXA significantly reduced the percentage of total blood volume lost per level fused when compared to no-TXA in AIS patients who underwent PSF using a standardized blood loss measure. No significant difference in percentage of total blood volume lost per level fused was found when comparing high dose TXA to low dose TXA. There were no documented complications of seizure, DVT, or PE in any of the patients in the study.
1917
A270: VCR-Based and Non-VCR-Based Surgical Maneuvers in Deformity Correction for Achieving Spinal Balance in Severe Rigid Scoliosis Patients: Weighing the Odds
Nicholas Van Halm-Lutterodt 1,2 , Mohamed Kamal Mesregah 1 , Ziyang Ye 3,4 , Krishna Mandalia 1 , Andrew Mecum 5 , Wei-Hsun Huang 2 , Wei-Cheng Chen 6 , Brandon Yoshida 1 , Yu Wang 2 , and Yulun Xu 2
1 University of Southern California, Department of Orthopaedics and Neurosurgery, Los Angeles, USA
2 Beijing Tiantan Hospital, Department of Neurosurgery, Beijing, China
3 University of Chicago Graham School of Continuing Liberal and Professional Studies, University of Chicago, Department of Business and Analytics, Chicago, USA
4 Wake Forest University, Department of Mathematics and Statistics, Winston-Salem, USA
5 Emory University, Department of Psychology, Atlanta, USA
6 Beijing Tongren Hospital, Department of Clinical Sciences, Beijing, China
Introduction: Severe rigid scoliosis defined as Cobb of ≥80° in spine patients can result in significant neurological deficits, cardiopulmonary complications as well as psychological and social stigmatization based cosmetic appearance. When the deformity is severe and rigid in patients, aggressive surgical approaches are sometimes considered to achieve desired corrective outcomes. Vertebral column resection (VCR-based) has the potential of about ≥60 degree of correction while other surgical osteotomy techniques (non-VCR-based) may range from 15-45° of correction while attempting to establish spinal balance in these patients. We evaluated the corrective rates of spinal balance and radiographic parameters between VCR-based and non-VCR-based surgery in severe rigid scoliosis patients. Materials and Methods: A comprehensive literature review was performed from January 2000-December 2019. The selection criteria for included studies included: average major curve Cobb angle of ≥80 o , case series of ≥10 patients, reported coronal and sagittal parameters with information on both coronal (CB) and sagittal balance (SB) at preoperative and final follow-up, with a 2-year minimum follow-up period. Primary outcomes compared between the two surgical technique groups included: baseline averages of demographics, etiological diagnoses, estimated blood loss (EBL), mean surgery duration, average fusion length (FL), major curve (MC) Cobb angle, MC apical vertebral translation (AVT), MC flexibility, thoracic kyphosis (TK), lumbar lordosis (LL), CB and SB. Secondary outcomes included: final follow-up (FFU) averages of MC Cobb angle, MC correction rate, MC AVT, MC AVT correction rate, TK, LL, CB, CB correction rate, SB and SB correction rate. Results: A total 303 patients from 11 retrospective studies and 1 prospective study were observed. Of 303 severe rigid scoliosis patients observed, 41.25% (n = 125) and 58.75% (n = 178) were VCR-based and non-VCR-based, respectively. The averages of age: 17.80 years and 21.63 years, female incidence: 58.10% and 68.20%, idiopathic etiology: 65.24% and 63.50%, congenital etiology: 23.96% and 19.5%, estimated blood loss: 2943.33 ml and 1125.22 ml, mean operation time: 510.27 mins and 649.78 mins were observed for VCR-based and non-VCR-based patients, respectively. The baseline average MC Cobb angles of 101.65o and 109.20o were corrected at rates of 64.70% and 60.80% at FFU for VCR-based and non-VCR-based patients, respectively. The average correction rates of MC AVTs were 66.18% and 70.70% in VCR-based and non-VCR-based groups, respectively. The baseline outcomes for CB: 1.52 cm and 1.42 cm and SB: 1.74 cm and 1.73 cm for respective VCR-based and non-VCR-based patients were corrected at respective rates of 38.83% and 28.90% for CB and 32.20% and 43.93% for SB. Postoperative cardiopulmonary complications, were higher in the Non-VCR-based patient group at a rate of 18.63% compared to an incidence rate of 5.10% in the VCR-based group. Other medical and implant-related complications between the two surgical groups were comparable. Conclusion: Findings from this study indicate that both VCR-based and non-VCR-based surgical spinal fusion technique maneuvers for the correction of severe rigid curves of ≥80 degrees are equally effective and can achieve correction rates of ≥60% at 2-year following corrective surgery. VCR-based surgery achieved higher CB correction rates while non-VCR-based surgery achieved higher SB correction rates.
OP31: Surgical Complications 2
1269
A271: Spinal Surgery Complications. An unsolved problem. Is the world health organization safety surgical Checklist an Useful Tool to Reduce Them?
Giovanni Barbanti Bròdano 1 , Cristiana Griffoni 1 , Giuseppe Tedesco 1 , Silvia Terzi 1 , Stefano Bandiera 1 , riccardo ghermandi 1 , Gisberto Evangelisti 1 , Marco Girolami 1 , valerio pipola 1 , Carlotta Cavallari 1 , Asdrubal Falavigna 2 , and Alessandro Gasbarrini 1
1 IRCCS Istituto Ortopedico Rizzoli, Oncological and Degenerative Spine Surgery, Bologna, Italy
2 University of Caxias do Sul, Department of Neurosurgery, Caxias do Sul, Brazil
Introduction: To face the problem of surgical complications, which is generally relevant in surgical fields, an intraoperative checklist (Safety Surgical Checklist, SSC) was elaborated and released by the World Health Organization in 2008, and its use has been described in 2009 [1]. In our Institution, the WHO SSC was introduced in 2011. In spinal surgery, many preventive measures were investigated to reduce complications, but there is no report on the effectiveness of the WHO checklist in reducing complications. The aim of this study was to compare the incidence of complications between the two periods, from January to December 2010 (without checklist) and from January 2011 to December 2012 (with checklist), in order to assess the checklist effectiveness. Material and Methods: A retrospective and single center study was carried out on patients who underwent spinal surgery during the three-year period from January 2010 to December 2012. Patients were classified according to the spine pathology and the different presentation of the complication. According to the pathology treated, there were oncological, degenerative, traumatic and infectious groups. Complications were divided into seven categories:(1). post- surgical hematoma. (2). surgical site infection. (3) cerebrospinal fluid (CSF) leakage or fistula. (4). mechanical complications (misplaced instrumentation and/or failure). (5). neurological complications. (6). systemic complications. (7). surgery related death. The complications’ classification and the patients’ inclusion into the categories were performed by independent investigators, i.e. non-MD clinical researchers (1 research nurse and 1 clinical research assistant) not directly involved in the care of the patients. The WHO Safety Surgical was introduced for the first time in our center in 2011. We registered the complications arising in patients treated from 2010 to 2012 during a 3 years follow up period for each patient, assessing the possible differences before and after the checklist's introduction. Results: The sample size was 917 patients, the mean age was 52.88 years. The majority of procedures were performed for oncological diseases (54.4%) and degenerative diseases (39.8%). 159 complications in total were detected (17.3%). The overall incidence of complications for trauma, infectious pathology, oncology, and degenerative disease was 22.2%, 19.2%, 18.4%, and 15.3%, respectively. No correlation was observed between the type of pathology and the complication incidence. We observed a reduction of the overall incidence of complications following the introduction of the SSC: in 2010 without checklist, the incidence of complications was 24.2%, while in 2011 and 2012, following the checklist introduction, the incidence of complications was 16.7% and 11.7%, respectively (mean 14.2%). Conclusion: Despite the limitations of the study, in particular the impossibility to carry out a randomized study,SSC seems to be an effective tool to reduce complications in spinal surgery. We propose to extend the use of checklist system also to the pre-operative and post-operative phases in order to further reduce the incidence of complications.
References
1. Haynes A.B., Weiser T.G., Berry W.R., et al (2009) Asurgical safety checklist to reduce morbidity and mortality in a global population. NEngl J Med 360:491-499.
939
A272: Outcomes in Spinal Surgery During theCOVID-19 Pandemic
Christine Scarsbrook 1 , Maheswaran Archunan 1 , Anand Shah 1 , Nick Steele 1 , Andrew Cook 1 , Lennel Lutchman 1 , Am Rai 1 , and Girish Swamy 1
1 Norfolk and Norwich University Hospital, Norwich, United Kingdom
Introduction: The COVID-19 pandemic has had a hugely detrimental impact on hospital services worldwide. There has also been increasing evidence about the higher patient mortality and morbidity associated with contracting SARS-CoV-2 in the peri-operative period. This is supported by a study carried out in China, which revealed that patients in the incubation phase of COVID-19 had a higher rate of ITU admission and mortality following elective surgery. A multicentre international cohort study recently published in the Lancet looked at the outcomes of 1128 patients with peri-operative COVID-19 infection. The results showed that 51.2% patients developed pulmonary complications and the 30 day mortality was 23.8%, highest in male patients aged 70 or over. These increased risks to patients during COVID-19 have been recognised by the British Association of Spinal Surgeons (BASS) who produced a COVID-19 information leaflet for patients to sign. We analysed the risk/benefit ratio of surgery for individual patients, and we have continued our emergency and urgent spinal operating services. This study describes the measures and pathways taken in our university hospital to protect patients and staff, and our outcome measures during COVID-19. Material and Methods: This is a prospective single-centre study of all patients who underwent spinal surgery in a four month period during the pandemic. All spinal surgical patients’ data were collected to identify demographics, co-morbidities, ASA grade, surgical indication and procedure, time to surgery, length of stay, need for ITU admission, COVID-19 swab result, complications and outcomes including mortality. Hospital theatre systems, intra-operative notes, patient pathways, both national and local, for elective and emergency patients [blue, green or yellow] were also reviewed. We compared the outcomes of patients under each pathway with our historic database over preceding years. Results: 72 patients underwent spinal surgery during this four month period; this was significantly lower than the 167 patients in the equivalent period in 2019 due to bed restrictions to accommodate COVID-19 patients. Emergency operating took up a higher proportion of the workload - with 37.5% spinal operations being emergency surgery, and 62.5% operations classified as urgent. None of the patients required ITU admission. There were 11 complications; 4 dural tears treated intra-operatively with no sequelae, 4 superficial wound infections, 1 post-operative chest infection (normal chest x-ray), 1 patient with mild dysphagia (following ACDF) and 1 ongoing urinary dysfunction (following cauda equina compression). None of the patients contracted COVID-19. There were three mortalities post-discharge in the community; none were related to surgery or to COVID-19. Conclusion: There was no variation in clinical outcomes in patients operated on before and during COVID-19 in our hospital. This is likely to be in part due to the procedures brought in on our wards and in our theatre complex as a response to the virus, as well as the new ‘blue’ pathway designed for urgent elective patients. These results should encourage other departments worldwide to adapt their surgical pathways to protect their patients and to restart their spinal elective service when their hospitals have the capacity to do so.
1077
A273: Adverse Events Occurring up to 5-Years After Complex Adult Deformity Surgery: A Scoli-RISK-1 Analysis
Meghan Cerpa 1 , Scott Zuckerman 1 , Lawrence Lenke 1 , Christopher Shaffrey 2 , Justin Smith 3 , Leah Carreon 4 , Kenneth Man Chee Cheung 5 , Michael Kelly 6 , Michael Fehlings 7 , Christopher Ames 8 , Oheneba Boachie-Adjei 9 , Mark Dekutoski 10 , Khaled Kebaish 11 , Stephen Lewis 7 , Yukihiro Matsuyama 12 , Ferran Pellisé 13 , Yong Qiu 14 , and Frank Schwab 15
1 Columbia University Medical Center, New York, USA
2 Duke, Raleigh, USA
3 University of Virginia, Charlottesville, USA
4 Norton Health, Louisville, USA
5 University of Hong Kong, Hong Kong, China
6 Washington University, St. Louis, USA
7 University of Toronto and Toronto Western Hospital, Toronto, Canada
8 University of California San Francisco, San Francisco, USA
9 The FOCOS Hospital, Patang West, Ghana
10 Marshfield Clinic Eau Claire Center, Eau Claire, USA
11 Johns Hopkins, Baltimore, USA
12 Hamamatsu University School of Medicine, Hamamatsu, Japan
13 Hospital Universitari Vall d’Hebron, Barcelona, Spain
14 Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing, China
15 Hospital for Special Surgery, New York, USA
Summary: Following complex ASD surgery at 5-years postoperative, 77.9% of patients experienced an adverse event (AE). Of patients with an AE, 20.2% had a severe complication, while 59% of patients that experienced an AE required surgical treatment. 75.9% of neurologic deficits were transient and improved over time. Common etiologies for neurologic AEs were nerve root retraction, compression, direct injury, and distraction. Most common spine complication in years 2-5 was implant failure, followed by sensory and motor deficit. Hypothesis: Prospectively evaluate neurologic and non-neurologic adverse events (AEs) occurring up to 5-yrs postop following surgical correction of complex ASD. Study Design: Prospective/multicenter/international/observational, Scoli-Risk-1. Introduction: Surgical treatment for complex adult spinal deformity (ASD) is associated with a variety of postop complications. Rates of perioperative complications following complex ASD surgery are well established, while reports of long-term postop complications remain unclear. Methods: 272 ASD pts undergoing surgery from 15 centers were enrolled. Inclusion criteria: Cobb>80, corrective osteotomy for congenital or revision deformity, and/or 3-column osteotomy (76% of all patients). At each follow-up visit any neurologic or non-neurologic AE was documented & categorized. Results: Of the 272 patients, follow-up rates were: 271 (99.6%) discharge, 260 (95.6%) 6-weeks, 255 (93.8%) 6-months, 217 (79.8%) 2-year, and 77 (28.3%) at 5-years. By 5-years postop, 212/272 patients (77.9%) experienced an AE. Of those that experienced an AE, 20% had a severe AE, 24% mild, and 33% moderate. A total 190/272 (69.9%) experienced a non-neurologic AE & 101 (37%) experienced a neurologic AE. Of all patients with complications, conservative management or no action was taken in 87 patients (41%), whereas 125 (59%) of the patients that experienced AEs required some form of surgical treatment (either revision spine or other surgery). 3 deaths occurred, none of which were directly related to surgery: ileus 3.2 months postop, cardiac arrest 9.8 months postop, and suicide 1.2 years postop. Specifically in the 2-to 5-year period, a total of 58 complications occurred that were related or possibly related to surgery, including: 27 (47%) implant failure, 6 (10%) sensory deficits, 3 (5%) loss of correction, 3 (5%) cord/motor deficits, and 2 (3%) deep infections. Conclusion: At 5-years postop following complex ASD surgery with prospective assessment, 77.9% of patients experienced an AE, with 20% having a severe complication and 59% requiring surgical treatment either spine or non-spine. 75.9% of neurologic deficits were transient and improved over time. The most common spine complication in the 2- to 5-year period was implant failure, followed by motor and sensory deficits.
667
A274: The influence of hospital type, insurance type, and patient income on 30-day complication and readmission rates following lumbar fusion
Xiao Chen 1 , Michael Collins 1 , Shane Shahrestani 1 , Alexander Ballatori 1 , Andy Ton 1 , Jeffrey C. Wang 1 , and Zorica Buser 1
1 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
Introduction: Several studies have shown that factors such as insurance type and patient income are associated with different readmission rates following certain orthopaedic procedures. However, no studies have investigated how 30-day complication and readmission rates vary by hospital type, insurance type, and patient median income following lumbar spine fusion. Material and Methods: A retrospective cohort study was conducted using the National Readmissions Database (NRD) from 2010-2016 using ICD-9 and ICD-10 codes, which identified 596,568 patients with primary lumbar fusion. Statistical analysis was conducted in R. Kruskal-Wallis tests with Dunn’s pairwise comparisons were performed to analyze differences in 30-day readmission and complication rates in patients who underwent lumbar spine fusion. Complications analyzed included infection, wound injury, hematoma, neurological injury, thromboembolic event, and hardware failure. Results: The hospital types analyzed were metropolitan non-teaching (212,131 patients), metropolitan teaching (364,752 patients), and rural (19,685 patients). 30-day readmission was significantly higher in rural and metropolitan teaching hospitals compared to metropolitan non-teaching hospitals (P < .01). Patients treated at rural hospitals were also more likely readmitted at 30 days than those treated at metropolitan teaching hospitals (P < .001). Compared to those treated at metropolitan non-teaching hospitals, patients from metropolitan teaching hospitals had significantly higher rates of infection (P < .0001), wound injury (P < .0001), hematoma (P = .018), and hardware failure (P < .002). The insurance types analyzed included Medicare (213,534 patients), Medicaid (78,520 patients), private insurance (196,648 patients), and out-of-pocket (45,025 patients). Privately insured patients were significantly less likely to be readmitted at 30 days than those paying with Medicare or Medicaid (P < .01). Infection, hematoma, and hardware device failure rates were significantly higher in out-of-pocket payers compared to all other groups (P < .0001). Infection, wound injury, and hematoma rates were significantly lower in Medicare payers compared to all other groups (P < .0001). Patient income was separated into quartiles, with 112,083, 145,755, 156,276, and 147,289 patients placed in quartiles 1 to 4, respectively. No difference in readmission rates were found between any of the income groups, although patients in quartile 4 were significantly more likely to develop hematomas compared to those in quartiles 1 and 2, and were more likely to experience a thromboembolic event compared to all other groups. Conclusion: Patients undergoing lumbar spine fusion at metropolitan non-teaching hospitals and paying with private insurance had significantly lower 30-day readmission rates than their counterparts. Complications within 30 days following lumbar spine fusion were significantly higher in patients treated at metropolitan teaching hospitals and in patients paying out-of-pocket. However, aside from a few exceptions, patient income was generally not associated with differential complication rates.
1915
A275: Endplate Volumetric Bone Mineral Density is a Predictor for Cage Subsidence Following Lateral Lumbar Interbody Fusion: A Risk Factor Analysis
Conor Jones 1 , Ichiro Okano 1 , Stephan Salzmann 1 , Erika Chiapparelli 1 , Marie-jacqueline Reisener 1 , Jennifer Shue 1 , Andrew Sama 1 , Frank Cammisa 1 , Federico Girardi 1 , and Alexander Hughes 1
1 Hospital for Special Surgery, New York, USA
Introduction: Lateral lumbar interbody fusion (LLIF) is a common procedure used for various spinal conditions. One of the common complications of this procedure is subsidence, which is the sinking of the interbody device into adjacent vertebrae. Previous work has shown that a decreased BMD as measured by DXA is a risk factor for subsidence, but emerging data suggests a lower endplate volumetric BMD (EP-vBMD) as measured by Quantitative Computed Tomography is a risk factor for subsidence following standalone LLIF. However, it remains unclear if this is the case for LLIF with posterior screws. Additionally, there is interest in the role that patient factors, such as BMI and diabetes status, plays on bone quality. The purpose of this study is to investigate risk factors for subsidence following LLIF. Materials and Methods: We reviewed the data of consecutive patients undergoing LLIF from 2014-2019 at a single academic institution who radiological imaging between 5 and 14 months after surgery. We excluded levels with previous instrumentation, previous fractures, and poor imaging quality. Cage subsidence was measured using the grading system devised by Marchi et al.1 We collected preoperative body mass index (BMI) along with diabetes status. We measured both EP-vBMD and the trabecular volumetric BMD measurement of the vertebral body (VB-vBMD). EP-vBMD was the average of the upper and lower endplate vBMDs measured in cortical and trabecular bone with a 5mm region of interest beneath the cage contacting surfaces. Univariable analysis and multivariable logistic regression analyses with a generalized mixed model were conducted. Multivariable analysis included BMI, diabetes status, EP-vBMD, VB-vBMD, and all trending (P < .20) factors in univariable analyses as explanatory variables. Ad hoc analysis, including receiver operative characteristic curve analysis, identified the cut-off values in significant continuous variables for subsidence. The statistical significance level was set at P < .05. Results: 567 levels in 347 patients were included in the final analysis. Mean age (±SD) was 61.7 ± 11.1 yrs. 50.3% of the patients were male. 134 (38.7%) patients were overweight, 114 (32.9%) were obese, and 45 (13%) were diabetic. Subsidence with a grade of at least 1 was observed in 160 levels (28.2%). After adjusting for age, American Society of Anesthesiologists Physical Status, Charlson comorbidity index, LLIF level, and VB-vBMD, standalone status (P = .001) and EP-vBMD (P = .032) were associated with subsidence. ROC curve analysis demonstrated a cutoff of 211 kg/m2 for EP-vBMD. Ad hoc analysis demonstrated patients with no risk factors had subsidence at 18.3% of levels, 31.1% of levels with one risk factor, and 44.9% of levels with both risk factors (P < .0001). Conclusion: A decreased local EP-vBMD and the absence of posterior screws are risk factors for subsidence following LLIF. When performing LLIF, the preoperative EP-vBMD measurement should be considered, and in patients with a low EP-vBMD, the addition of pedicle screws could be included to limit the risk of subsidence.
References
1. Marchi L, Abdala N, Oliveira L, Amaral R, Coutinho E, Pimenta L. Radiographic and clinical evaluation of cage subsidence after stand-alone lateral interbody fusion. J Neurosurg Spine. 2013;19(1):110-118. doi:10.3171/2013.4.SPINE12319
1873
A276: Severe short-term complications after cerebrospinal fluid leakage following lumbar spine surgery. A retrospective single-centre study
Michal Krakowiak 1 , Tomasz Szmuda 1 , Justyna Fercho 2 , Zuzanna Maliszewska 2 , and Paweł Słoniewski 1
1 Medical University of Gdansk, Neurosurgery Department, Gdansk, Poland
2 Medical University of Gdansk, Scientific Circle of Neurology and Neurosurgery, Gdansk, Poland
Introduction: Cerebrospinal fluid (CSF) leak as a result of an incidental durotomy is a relatively common complication associated with spine surgery. It may lead to more serious conditions such as meningitis or intracranial hypotension. This study aims to assess the severe complication rate followingCSF leakage. Material and Methods: The authors conducted a retrospective study on patients who underwent lumbar spine surgery and were readmitted due to postoperative CFS leak in one of the Neurosurgery Departments in Poland. The clinical data of spine surgeries from January 2015-September 2020 was collected from the local hospital database. Factors included into the analysis were: age, Body Mass Index (BMI), nicotinism, comorbidities, lenght of hospitalization, initial spine surgery, dural tear recognition during revision surgery, usage of external lumbar drainage. Patients treated for emergency spine cases were excluded from this study. Results: Out of 3080 patients after spine surgery 73 cases were included. The male-to-female ratio was 50:50. The mean age was 55 years (range 24-86 years) among women and 58.8 years (range 31-80 years) among men. The overal incidence of CSF leakage was 2.37% of which 12% had other severe complications. Meningitidis was the most common one (n = 7, 9.5%). No correlation was found between meningitidis and nicotinism, BMI or previous spine surgery. There was 1 (1.36%) case of pneumocephalus and 1 case of an acute subdural heamatoma (1.36%) induced by intracranial hypotension. Surgical management of CSF leaks correlated with shorter hospital stay (P < .05). Conclusion: Unintended durotomy is a common complication in spine surgery. As presented in this study, griveous complications may occur due to postoperative CSF leakage. The surgeon and patient need to be aware of these potentially fatal conditions in order to reduce them.
1793
A277: Comparison of Implant-Related Complications Between the Magnetically Controlled Growing Rod and The Spring Distraction System for the Treatment of Early Onset Scoliosis
Justin Lemans 1 , Casper Tabeling 1 , René Castelein 1 , and Moyo Kruyt 1
1 University Medical Center Utrecht, Orthopaedic Surgery, Utrecht, The Netherlands
Introduction: Traditional Growing Rod surgery for Early Onset Scoliosis (EOS) is associated with high complication rates, which are attributed to the need for frequent re-operations. Although this need can be mitigated by using the Magnetically Controlled Growing Rod (MCGR), recent literature shows that complications are still frequent, possibly owing to MCGRs mechanical complexity. We developed the Spring Distraction System (SDS), which continuously distracts the growing, scoliotic spine through a compressed titanium spring that is positioned around a standard growing rod. Although it offers a theoretical favorable biomechanical stress profile, its effect on complications has not yet been studied. Therefore, the current study aims to compare the complication rate and complication profile of the MCGR and the SDS. Material and Methods: We performed a retrospective cohort study to compare consecutive EOS patients between 2013 and 2018 who underwent primary implantation with either a hybrid MCGR construct or the SDS implant. Patient- and disease-related variables were collected and 2 observers independently scored and graded complications in all included patients. Complication rate was reported as complications/patient/year and a Kaplan-Meier survival analysis with the Log-Rank method was performed to compare the time to complications between the groups. Results: We included 32 EOS patients, 14 MCGR and 18 SDS patients. Mean age at surgery was 7.9 ± 1.6 and 8.4 ± 1.9 years for MCGR and SDS respectively. Mean follow-up was 4.1 ± 1.6 (MCGR) and 3.0 ± 0.4 (SDS) years. The MCGR group showed 18 complications (1.3/patient), which corresponded to 0.31 complications/patient/year. Ten patients (71%) had at least 1 complication. There were 4 anchor failures, 2 rod fractures and 8 actuator malfunctions in which the MCGR failed to lengthen any further (after a mean of 3.4 years) and had to be replaced to allow for further spinal lengthening. In addition, there were 3 cases of proximal junctional kyphosis and 1 case of post-operative neurological injury. The SDS group showed 17 complications (0.9/patient), corresponding to 0.31 complications/patient/year. Eleven patients (61%) had at least 1 complication. There were 3 anchor failures, 3 rod fractures, 1 case of rod slippage, 3 side-to-side connector complications and 2 wound complications (1 wound dehiscence and 1 deep surgical site infection). There were no cases where the SDS implant failed to lengthen during the study period. However, there were 5 cases of implant kyphosis resulting in implant prominence. Across all patients, median complication survival (i.e. the point where half of the patients suffered a complication) was 2.8 years. The Kaplan-Meier analysis showed no significant difference (P = .408) in median complication survival between the MCGR (3.0 years) and SDS (2.5 years) group. Conclusion: Although complication rate normalized for follow-up was similar between MCGR and SDS patients (0.31 complications/patient/year), complication profile was different between groups. In the MCGR group, failure to lengthen occurred in >50% of patients, while the SDS group showed no patients in whom spring lengthening stalled during growth. However, SDS patients had a higher rate of implant kyphosis. The median complication survival for all patients was 2.8 years, with no differences between the groups.
388
A278: Complication Rates Following Posterior Lumbar Fusion in Osteoporotic Patients Taking Bisphosphonates
Sidney Roberts 1 , Ryan Murphy 1 , Blake Formanek 1 , Zorica Buser 1 , and Jeffrey C. Wang 1
1 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
Introduction: Osteoporosis has been shown to have negative effects on outcomes of spine surgery and is associated with increased post-operative complication rates. Bisphosphonates are one of the most commonly prescribed drug classes for osteoporosis, and the current body of literature has mixed results with regards to the effect of bisphosphonates on spinal fusion and post-operative complications. The present study aims to elucidate the effects of bisphosphonates on complications following posterior lumbar fusion (PLF) with a large database study. Material and Methods: The PearlDiver patient record database was queried to identify adult patients (over 18 years of age) who had undergone posterior lumbar fusion (PLF) using Current Procedural Terminology (CPT) codes. Those patient cohorts were divided based on a diagnosis of osteoporosis prior to surgery and bisphosphonate usage. This yielded three groups: Osteo+Bisph+, Osteo+Bisph-, and Osteo-Bisph-. The surgery groups were matched according to age, sex, and Charlson Comorbidity Index (CCI). Incidence of post-operative complications were analyzed and statistical analysis was conducted using Pearson chi-square analysis. Results: Patients with osteoporosis (both groups Osteo+Bisph+ and Osteo+Bisph-) had higher rates of revision surgery than patients without osteoporosis at 6 months and 1 year but these results were not statistically significant. Patients with osteoporosis (both groups Osteo+Bisph+ and Osteo+Bisph-) also had higher rates of instrumentation complications and post-operative vertebral fractures with Osteo+Bisph- having the highest rate of both complications. These results were also not statistically significant. There was no statistically significant difference in pseudarthrosis between the three groups. Osteo-Bisph- had significantly higher rates of post-operative leg pain than Osteo+Bisph- (P = .0036) and significantly higher rates of post-operative back pain than both groups Osteo+Bisph+ and Osteo+Bisph- (P = 0.00349) (Table 1). Conclusion: Patients with osteoporosis had higher rates of post-operative revision, instrumentation failure and post-operative fracture than patients without osteoporosis, however these results were not statistically significant. There was also no significant difference in the aforementioned complications between osteoporotic patients taking bisphosphonates and those who did not. Patients without osteoporosis had higher rates of post-operative back pain and leg pain than patients with osteoporosis regardless of bisphosphonate usage.
1312
A279: Safety and efficacy of magnetically controlled growing rods in an early onset scoliosis population
Henry Turner 1 , Patrick Carroll 1 , Robin McManus 1 , Jim Kennedy 1 , Jacques Noel 1 , and Patrick Kiely 1
1 Children's Health Ireland at Crumlin, Trauma and Orthopaedic Surgery, Dublin, Ireland
Introduction: There has been controversy surrounding the safety and efficacy of magnetically controlled growing rods (MCGR) for the treatment of patients with early onset scoliosis (EOS). The primary aim of our study was to evaluate the efficacy of MCGR in correcting and controlling spinal deformity progression. The secondary aim was to evaluate the number of patients that needed additional unplanned surgery in the follow-up period. Material and Methods: All 88 patients who had MCGR inserted from 2014 onwards in our institution were included in this study. This cohort comprised of 41 Females and 47 Males and were sub classified according to the C-EOS classification system. This revealed 19 Congenital, 23 Idiopathic, 16 Syndromic and 30 Neuromuscular origin patients. The following outcomes were measured: Pre- and post-operative Scoliosis Major Cobb (MCA) and Major Kyphosis (MKA) angles, space available for lung ratios (SALR), T1- T12 heights, rod length changes, additional unplanned surgeries, and implant failures. Results: (Our data is represented as means with SD in brackets) The mean age at surgery was 8.14 years (±2.81) and mean follow up after surgery was 35 months ( ± 15). The pre- and immediate postoperative MCA’s were 76 (±21)° and 36 (±19)°, respectively. The latest MCA was 44° (±21). Pre- and immediate postoperative MKA’s were 43 (26) degrees and 28 (±16)°, respectively. The latest MKA was 32 degrees ( ± 17).The preoperative and latest SALR’s were 86% (±13) and 95% (±9) respectively, an increase of 9%.The pre- and immediate postoperative T1-T12 heights were 168mm (±30) and 193 mm (±30) respectively. The latest T1-T12 height was 209 mm (±33), an increase of 16mm (8.3%) from the immediate postoperative measurement. The increase in rod lengths were 17 mm (±10) and 18 mm (±10) for right and left side rods, respectively. Macroscopic evaluation of implants and radiographic evaluation revealed bilateral actuator pin failure in 2 patients (2.27%) and there was no evidence of end cap failure. 24 patients (27%) had additional unplanned surgery due to infection, inadequate deformity control and rod or anchor point failure. Conclusion: Our findings suggest that MCGR can achieve success in controlling significant deformity in the EOS population over the short to medium term. As with other treatment options, additional unplanned surgery may be needed and this must be communicated to the affected individuals and their guardians. Further research continues to define long term outcomes for the EOS population.
OP32: Clinical Biomechanics 2
1036
A280: Spine Stability After Treatment of Degenerated Intervertebral Discs with Percutaneous Cement Discoplasty
chloe techens 1 , sara montanari 1 , Ferenc Bereczki 2 , Peter E. Eltes 2 , Aron Lazary 2 , and Luca Cristofolini 1
1 University of Bologna, Department of Industrial Engineering, Bologna, Italy, 2 National Centre for Spinal Disorders, Budapest, Hungary
Introduction: Low back pain can be caused by nerve compression due to stenosis of the foramen associated with intervertebral disc degeneration. Invasive surgical solutions are not suitable for old patients with comorbidities. A minimally invasive approach, percutaneous cement discoplasty, has been recently developed for the polymorbid patients [1]. The mechanical impact on the spine stabilization and surrounding tissues have not been investigated yet. This in vitro study aimed at: (1) testing the stabilization of human spine segments after discoplasty by monitoring the disc height and the range of motion (ROM), (2) preventing complications by assessing the strains on the specimen surface, (3) relating the surgery quality to the biomechanical stability of the spine segments. Material and Methods: 27 fresh-frozen human cadaveric lumbar FSUs were obtained from 15 donors (35-86 y.o., 63-132 kg) after ethical approval. The soft tissues were removed, leaving the ligaments intact. The specimens were potted with the intervertebral disc horizontal and prepared with a water-based white-on-blue speckle pattern in order to measure surface strains with Digital Image Correlation (DIC) [2]. The specimens were mechanically tested in flexion and extension under 50% body weight axial load combined to an offset. The ROM, the stiffness, and the disc height were measured. Disc surface images were recorded and analysed by a 3D-DIC system using optimized parameters. Cement distribution within the disc and surface contact with the endplates were analysed from CT scan segmentations. The specimens were tested under two conditions: (1) Simulated degeneration: the intervertebral disc manually emptied through an incision in the annulus. (2) Discoplasty: after acrylic cement injection (Mendec Spine, Tecres, Italy). Results: Discoplasty increased the disc height by 34% in flexion and 35% in extension compared to the degenerated conditions, thus increasing the width of the foramens. On the contrary, discoplasty only impacted the ROM in flexion with a 27% reduction with respect to nucleotomy condition. Discoplasty was associated with a 37% increase of stiffness in flexion and a reduced neutral zone. The highest strains were exhibited in the disc after nucleotomy. Cement injection resulted in a restrained gradient over the disc, with a localization of compressive strains along the endplates. Conclusion: Similarly to clinical observations, discoplasty recovered the disc height, thus rehabilitating the neuroforamen area. The large volumes of cement improved spine stability in flexion resulting in stiffer segments. Disc tissue underwent reduced deformations which concentrated on the endplates.
References
1. Varga et al, Der Ortho, 44:1-8,2015.
2. Palanca et al, MEP, 52: 76-83, 2018.
Acknowledgements
European Union’s Horizon 2020 Marie Skłodowska-Curie ITN grant SPINNER No. 766012 and the Hungarian Scientific Research Fund (OTKA FK123884).
Ethical approval
The entire study was approved by the bioethical committee of University of Bologna, protocol 76497 of 1st June 2018. The specimens were obtained through ethically-approved International donation programs.
1702
A281: Analysis of the Largest Database of Anthropometric Measurements of the Occipito-Atlantoaxial Joints
Karim Bayanzay 1 , Matthew Nudelman 2 , and Mayar Abbasi 3
1 Jersey Shore University (Perth Amboy), Internal Medicine, Perth Amboy, USA
2 Stanford University, Emergency Department, Palo Alto, USA
3 McGill Unviersity, Center for Intelligence Machines, Quebec, Canada
Introduction: The complex geometrical and biomechanical dynamics of the occipito-atlantoaxial joints remain unparalleled in the human body. The atlantal (C1) joint plays a central role in the craniocervical junction, which is comprised of the occipito-atlantal joint (C0-C1) and the atlantoaxial joint (C1-C2). Due to complexities related to its anatomy, there is no consensus on the precise biomechanics of the occipito-atlantoaxial spine. For further clarification, many anatomists have endorsed developing a quantitative database measuring key anatomical landmarks of the cervical spine to provide a better understanding of its geometry and kinematics. This report presents an analysis of the largest database describing the atlas' radiographic measurements and their relationship to surrounding structures. Material and Methods: KKT Orthopedic Spine Centers provide wave treatments to manage chronic back and neck pain. As part of their treatment process, three x-ray images (lateral, frontal, and top skull) of the patient's cervical spine are obtained in a uniform manner and stored in a centralized database. The data is then analyzed by a proprietary software, Spinalytics®, which calculates distances and angles between key landmarks on the cervical spine x-rays. This study included all patients visiting any of the KKT Orthopedic Spine Centers with x-rays analyzed by Spinalytics® between November 2006 and June 2019. Data regarding the occipito-atlantal angle, atlas angle, antlanto-cervical angle, and atlas rotation were extracted from the database and included in this study. The occipito-atlantal angle describes the angle between the skull line and the true vertical through the atlas midpoint. The atlas angle is the acute angle formed between the mastoid line and the true horizontal line through the atlas midpoint. The atlanto-cervical angle is between the spinal line and true vertical through the atlas midpoint. The atlas rotation is the angle between the vertical line and the lateral mass line on the side of the atlas' acute angle on the top skull X-ray. Results: This study included 49,937 patients in 25 centers in 14 countries. The average patient age was 45 (SD: 16) years old, with 49% male. The mean deviation of the occipito-atlantal angle is 2.37o to the right, the mean atlas angle is 1.86o to the right, and the mean atlanto-cervical angle deviation is 2.20o to the left. The average atlas rotation angle is tilted 87.86o anteriorly. Linear regression models suggest that the atlas influences the angles between the skull and cervical spine, bi-directionally. However, deviations in the skull do not impact the cervical spine and vice versa. Conclusion: This study's results show a clockwise rotation of the axis with a higher degree of rotation in the occipito-atlantal angle than the atlanto-cervical angle. The atlas angle appears to influence deviations in occipito-atlantal and atlanto-cervical angles; therefore, deviations' primary foci appear to be the atlas. Further studies amongst healthy volunteers and correlation with clinical data are required to clarify the clinical significance of these anthropometric measurements.
1625
A282: A Simple Biomechanical Study, Reveals that a Reversal in Direction of Compression, Could Greatly Improve Restoration of Lordosis in Lumbar Fusion
Shay Menachem 1,2 , and Kevin Seex 1,2
1 Macquarie University, Department of Clinical Medicine, Faculty of Medicine, Health and Human Sciences, Sydney, Australia
2 Macquarie University Hospital, Macquarie Neurosurgery, Sydney, Australia
Introduction: Lumbar lordosis is usually lost in the degenerative process, and when lumbar fusion is required, restoration of the correct shape of the spine is one of the modern metrics of a successful operation. However, operations regularly fail to achieve adequate lordosis and one of the reasons why, is one that is rarely discussed, namely that achieving lordosis can be difficult. We sought to investigate this. Study of the anatomy, normal vertebral motion, and current techniques, led to the hypothesis that simply changing direction of compression during surgical fusion, would gain more lordosis. Method: Using a biomechanically validated Sawbones ™ model we inserted standard polyaxial pedicle screws (Nuvasive™, ‘Reline’) from S1-L4 in a surgically correct, well aligned position. A standard lordotic rod was placed in the screws without requiring rod reduction, and the caps attached but left unlocked. Markers were attached to L4 and S1 spinous processes to allow photographic analysis of lordosis. Two techniques of compression were compared. A-Standard, whereby caudal screws were locked first and compression proceeded sequentially in a cranial direction prior to locking. B-Alternate, whereby cranial screws were locked first and compression proceeded caudally. A standard parallel compressor was used. Both methods were repeated to confirm consistent reproducibility, and after increasing levels of surgical invasiveness; intact, add interbody cage, add inferior facet resection, add Ponte resection. Standardised photographs were analysed to measure change of lordosis with each technique. The methodology was also tested for accuracy against a previously validated digital multicamera system similar to image guidance systems. Compression was done by the same surgeon to the same ‘white knuckle’ force. Results: There was an increase in the lordosis gained using method B of 300% for an intact model, 195% after a cage insertion, 60% after adding inferior facet resection and 33% for a full Ponte osteotomy. Statistical analysis of the results demonstrated a significant difference (P = .002) between the two methods for all levels of model integrity. Conclusion: In this biomechanical model, locking the top screws first was a consistently superior method of compression to gain lordosis. If confirmed clinically, without changing instrumentation, surgeons should consider reversing direction of compression to a “Top down” technique. No previous literature regarding this matter was found. Our pre-experiment hypothesis was that intact and possibly inferior facet resection would favour technique B. This was based on the following observations; the initial locking of one tulip also fixes the position of the rod and so the moving tulip has to follow this rod, the alignment of the normal facet joints forms about a 90 degree angle with moving superior screw, while the moving inferior screw forms about a 45° angle. The moving superior screw could thus be expected to block earlier i.e. produce less lordosis than a moving inferior screw. What was unexpected was that “Top Down” was superior after Ponte resection, (i.e. total facet resection) indicating additional unknown factor(s) were dictating the results.
92
A283: Biomechanics of the Active Apex Correction Technique of Early Onset Scoliosis: A Parametric Finite Element Study Simulating 6-Month Growth
Daksh Jayaswal 1 , Aakash Agarwal 1 , Alaaeldin Ahmad 2 , Amey Kelkar 1 , Manoj Kodigudla 1 , and Vijay Goel 1
1 University of Toledo, Toledo, USA
2 Annajah Medical School, Nablus, Palestine
Summary: The active apex correction (APC) technique demonstrates the possibility of effective remodulation of the wedging at the apex using a modified SHILLA approach. This may in turn nullify the complications inherent with SHILLA by avoiding apical fusion. The current finite element (FE) study explores the parametric effect of compression during APC with a 6-month follow up. Results show the magnitude of the initial compressive force dictates the degree of correction, while maintaining the correction. Hypothesis: Clinical outcome of implant constructs with different materials could impact surgical planning for surgeons using the APC technique. Study Design: Finite element study simulating APC with a 6-month follow-up period. Introduction: Newer, modified techniques like the active apex correction (APC), aim to nullify the complications inherent with SHILLA by avoiding apical fusion. This study evaluates the effect of the correction achieved by the APC technique (or APC). Additionally, we explored the effect of the compression force applied during the surgery. Methods: A FE model simulating coronal (T5-T11 cobb angle: 44° & T11-L1 secondary curve) of 36° and sagittal deformity (T4-T12 kyphosis: 36° & L1-S1 lordosis: 46°) was compressed. 3 models with the APC construct were simulated with compression varying from 1 mm-5 mm displacement (6-30N) applied between screws proximal and distal to the apex(T8). The model simulated the effect of gravity and muscle forces and 6-month epiphyseal spinal growth (Figure 1). The clinical output parameters were measured and compared for these models at various time points. Results: Compared to the base model with no instruments, the instrumented models achieved a reduction in the coronal and sagittal angles, apical vertebral translation and wedging at the end of the 6-month growth period, across the different compressive force cases (Table 1). Conclusion: The output parameters showed consistent maintenance of the correction achieved by the APC, with the magnitude of the initial compressive force dictating the degree of correction. Take Home Message: The results show that tethering through a posterior approach, which is the gold standard for spine surgeons tackling EOS, we can perform this active apex correction technique to get excellent results.
Figure 1. Schematic showing the modified SHILLA approach with active apex correction used in this study
Table 1. Output parameters from the finite element model simulating the Active Apex Correction technique with different compressive force cases

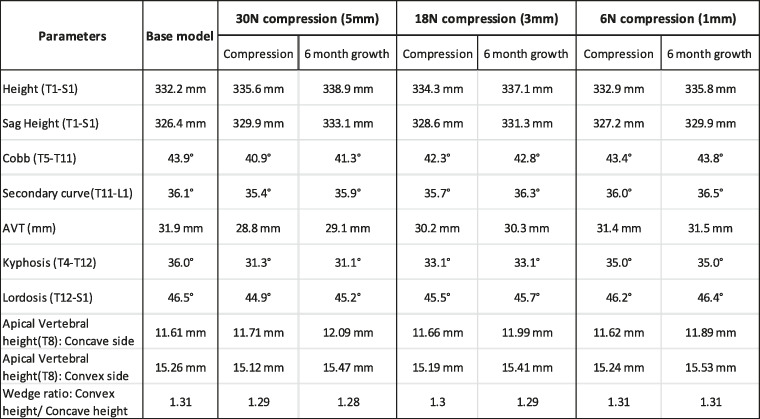
640
A284: Update on the Biomechanics of the Transverse Atlantal Ligament in the Elderly
Basem Ishak 1 , Emre Yilmaz 2 , Alexander von Glinski 2 , Rod Oskouian 3 , and Jens Chapman 3
1 Heidelberg University Hospital, Department of Neurosurgery, Heidelberg, Germany
2 BG University Hospital Bergmannsheil, Department of Trauma Surgery, Bochum, Germany
3 Swedish Neuroscience Institute, Complex Spine Surgery, Seattle, USA
Introduction: The transverse ligament is the strongest ligament of the craniocervical junction and therefore, plays a critical role in atlanto-axial stability. However, several clinical studies have questioned this ligament’s strength in the elderly. The goal of this biomechanical study was to reevaluate the force required for the transverse ligament to fail in a more physiological biomechanical model in elderly specimens. Material and Methods: Twelve C1-2 specimens were harvested from fresh-frozen Caucasian cadavers with a mean age at death of 81 years (range 68-89 years). Only the transverse ligament was preserved, and the bony C1-2 complex was left intact. The dens was pulled away from the anterior arch of C1 using a strength test machine that applies controlled increasing force. After testing, the axis was split in half to check for hidden pathologies and osteoporosis. The differences in the failure force between sex and age groups (group 1: < 80, group 2: > 80 years) were compared. Results: The mean force required for the transverse ligament to fail was 236.2 ± 66 N (range 132-326 N). All but two specimens had significant osteoporotic loss of trabecular bone. No significant differences between sex and age groups were found. Conclusion: The transverse ligament’s failure in elderly specimens occurred at an average force of 236 N, which was lower than that reported in the previous literature. The ligament’s failure force in younger patients differs and may be similar to the findings published to date.
974
A285: Influence of Pelvic Incidence on the Segmental Lordotic Parameters in Normal Adults
Kalyan Kumar Varma Kalidindi 1 , Gururaj Sangondimath 1 , and Kuldeep Bansal 1
1 Indian Spinal Injuries Centre, New Delhi, India
Introduction: We performed this study to understand the spectrum of sagittal spino-pelvic parameters, segmental lumbar parameters and the location of lumbar apex in asymptomatic adult population and analyse their correlations with each other. Materials and Methods: Hundered asymptomatic adult volunteers (Mean age of 29.1 (±7.9) years; 69 males, 31 females) who satisfied the selection criteria were enrolled for the cross sectional study. Standing antero-posterior and lateral whole spine and pelvis X-rays were performed and the radiographic parameters were analyzed. We introduced a “segmentation line” bisecting the apical vertebra/disc to divide the ULL (upper arc of lumbar lordosis) &LLL (Lower arc of lumbar lordosis). Results: The mean PI (Pelvic incidence) was 48.02, ULL was 29.12, LLL was 16.02, TLL (Total lumbar lordosis) was 45.14, LTA (Lumbar tilt angle) was4.73 and LLA (Location of lumbar apex) was 4.11. As the PI increases, the location of the lumbar apex moved higher. The PI had a significant positive correlation with the LLL(r = .582, P < .001) and TLL(r = .579, P < .001) but not with the ULL(r = .196, P = .05). The LLA is strongly correlated positively with the ULL(r = .349, P < .001), negatively with the LLL(r= -0.63, P <.001) and not correlated with the TLL(r=-0.177, P = .078). Conclusions: The PI influences the location of the lumbar apex, the lower arc of lordosis and the total lordosis but not the upper arc of the lordosis. The location of lumbar apex does not influence the total amount of lumbar lordosis but the segmental lordosis is strongly influenced by its location.
863
A286: Novel Biomechanical Model for Proximal Junctional Kyphosis
Timothy OConnor 1 , Mary O'Hehir 1 , Jennifer Mao 1,2 , Brandon Mariotti 1 , Daniel Rathbone 3 , John Pollina 1 , Munish Gupta 4 , David Polly 5 , Asham Khan 1 , Sigurd Berven 6 , and Jeffrey Mullin 1
1 University at Buffalo Neurosurgery, Neurosurgery, Williamsville, NY, USA
2 Rothman Orthopaedics, Philadelphia, PA, USA
3 Jacobs Institute, Buffalo, NY, USA
4 Washington University Physicians, Orthopaedics - Back and Spine, Saint Louis, MO, USA
5 University of Minnesota Medical School, Orthopedic Surgery, Minneapolis, MN, USA
6 University of California San Francisco, Orthopaedic Surgery, San Francisco, CA, USA
Introduction: A biomechanical model was created to evaluate repetitive fatigability testing on long thoracolumbar constructs. Material and Methods: An explanted spine was instrumented from T3-Sacrum and secured to a rigid frame constructed from aluminum t-slot extrusion. A 20 cm rod was attached to bilateral pedicle screws placed on the level immediately rostral to the upper instrumented vertebrae of interest (UIV+1), and spectra cord was secured to the rod. The explanted spine was oriented in a lateral position to avoid unintended moment applied by the remaining rostral spine. The rostral aspect of the spine was then suspended from above to allow largely unrestricted movement in the medial plane. The cord was deflected by a pulley 90 degrees to run vertical to the floor and secured to a water-filled container that could be filled or emptied to adjust the load applied. A pneumatic actuator raised and lowered the loading weight to cyclically flex the spine, while a counterweight provided a constant extension force of 5 N. Circular markers were placed on separate metal rods secured to the pedicles of the UIV and UIV+1 to allow measurements of change in angle. A python script using the Hough Circle Transformation tracked the circular markers via a Logitech webcam and used the marker positions to calculate change in angle between UIV and UIV+1. To evaluate the reliability of the tracking script, a series of measurements were taken without moving the markers and the standard deviation of these measurements were assessed. An electrical solenoid valve allows programmable control of repeated loading cycles. Results: This biomechanical model was able to successfully apply repetitive forces with a variety of moment arms and shear forces that can be increased independently from one another. Moment can be increased independent of shear force by increasing the rod length attached to the UIV + 1; adjusting the water level in the loading weight will modulate moment and shear in tandem. The Python angle measurement script was able to successfully interact with a commonly available Logitech webcam to act as an optical tracker, and successfully record the relative angles of the UIV and UIV + 1 endplates. Evaluation of 46 measurements of the same marker position showed a standard deviation of 0.16 degrees suggesting that this method is adequate for measuring angle changes less than half a degree. Conclusion: This is the first description of a novel biomechanical model that can successfully test long thoracolumbar constructs with repetitive flexion and accurately measure the relative change of angles of individual endplates. This model can be used to provide information regarding optimal tension parameters in junctional tethers, as well as fatigability testing for a variety of spine applications.
899
A287: Association of Facet Tropism at the Last Mobile Segment with Sacralisation of the L5 Vertebrae
Sasidharan M D S 1,2 , and Davis John Thelekatt 1
1 KMC Manipal Hospital, Spine Surgery, Mangaluru, India
2 Apollo Hospital, Spine Surgerty, Chennai, India
Introduction: An association between asymmetry of the lumbar facet joints and disc pathology has been studied previously. Researchers have shown a relationship between facet tropism and disc herniation. The present study aims at finding an association between facet tropism at the last mobile segment with sacralisation of L5 vertebrae. There have been many literatures on facet joint degeneration at the L5 vertebrae as well as sacralisation of L5 vertebrae but limited knowledge on its association with the mobile segment or transition segment of a sacralised L5 and facet joint asymmetry. Materials and Methods: The sampling was done by dividing the total study group into two on the basis of the MRI findings. Group A included patients with sacralisation of the lumbar vertebrae (L5) and Group B included the patients with normal lumbosacral vertebral morphology, all who had low back pain. The sample study included 230 patients and divided into 115 patients in each group. Analysis is done by using Chi square test, Odds Ratio, Kappa ratio and Student’s t test. A statistical analysis is conducted using IBM, SPSS 17.0 and P < .05 is considered as significant. Results: Among the 230 patients selected for the study 53% of the patients were males and 47% were females. Among the females in the study 65.4% of them had sacralised vertebrae and 36.5% males had sacralised vertebrae. 27% of the total patients suffered from both low back pain and sciatica. 70% of the total patients suffered from disc degeneration. All patients in the age group 30-40 years who presented with low backpain were found to have facet tropism. 90.9 % of the total study group who had facet tropism in the sacralised vertebrae were in the age group less than 40years. In the group B, the patients who had sacralised vertebrae 83 % of them had developed disc degeneration, but facet tropism was found to be 79% of the total study group. The association of facet tropism with sacralisation using chi square test of independence was found to be highly significant at X2 (1, N = 230) = 53.010 P < .001. The association of facet tropism with disc degeneration and age was also found to be significant. Conclusion: This study showed significant association of facet tropism at last mobile segment with sacralisation of L5 vertebrae. The statistical analysis shows that facet tropism is eight times more likely to be seen in sacralised vertebra when compared with non sacralised vertebra. The age group less than 40 years who had low back pain showed higher incidence of facet tropism and disc degeneration. Similar to literature, our study also found significant association between facet tropism and transitional vertebra with disc degeneration. Using regression coefficient the study also found to have statistical significance for transitional vertebra to predict disc degeneration. Patients with sacralised vertebrae showed early disc degenerative disease when compared with patients who did not have sacralisation of L5 vertebrae.
1726
A288: Implant Surface Functionalization Technologies and the Need af a Transparent Quality Evaluation System
Dietmar Schaffarczyk 1 and Helmut Cölfen 2
1 surgeSupply GmbH, Research, Regulatory and Quality Assurance, Kreuzlingen, Switzerland
2 University of Konstanz, Physical Chemistry, Konstanz, Germany
Introduction: For bone implants, osseointegration resulting in a good and fast bone-implant contact is of primary importance to secure a proper implant function and to avoid implant loosening or inflammation resulting in necessary revision surgeries causing pain to the patients and immense costs. Especially Polyetheretherketone (PEEK) is a promising implant material due to the close mechanical properties to bone but it is completely bio-inert hindering osseointegration and making surface functionalization necessary. Many different surface functionalization technologies have been reported both of physical and chemical nature. The same is true for the other prominent implant materials titanium and ceramics although they already have a naturally better osseointegration than PEEK but are much harder and stiffer than bone and brittle in case of ceramics. Surface functionalization, which can be subdivided into surface coating and material modification needs to be judged from a quality and safety viewpoint. Material and Method: However, a literature research resulted in the fact, that no quality standard yet exists for implant surface functionalization. This makes it difficult to impossible to compare the safety and performance of different surface functionalized bone implants clearly showing the need to establish a transparent quality evaluation system for bone implants. Results: In this perspective article, we give the state of the art and then develop a quality evaluation system, which is based on 6 main categories as important benchmarks for the quality of a surface functionalized bone implant material. A simple catalogue of questions can be answered and from the resulting scores, the Safety Performance Evidence Level (SPEL) representing the safety and quality of a given implant can be calculated in %. This simple SPEL system allows an easy and transparent judgement and comparison of bone implants, which will hopefully assure the easy identification of safe and well performing high-quality bone implants in the future. Keywords: bone implant, polyetheretherketone (PEEK), surface functionalization, quality evaluation, safety and performance evaluation level (SPEL)
OP33: Robotics, Navigation and VR
1310
A289: Learning Curve in Pedicle Screw Insertion Using an Intraoperative Computertomography (ICT) Guided Navigation
Benedikt Trnovec 1 2 , Bastian Stemmer 3 , Heiko Mueller 3 , Svorad Trnovec 4 , Ehab Shiban 3 , Kamil Kolejak 1 , and Volkmar Heidecke 3
1 University Hospital Bratislava Ruzinov, Neurosurgical department, Bratislava, Slovakia
2 National Institute of Children's Diseases, Neurosurgical department, Bratislava, Slovakia
3 Universitätsklinikum Augsburg, Neurosurgical department, Augsburg, Germany
4 University Rostock, Neurosurgical department, Rostock, Germany
Introduction: iCT navigation guided screw placement has an extraordinary low misplacement rates. There is a lack of evidence concerning the learning curve in this technique. Aim of this single center retrospective study is to show the effect of learning curve in the first year of use. Methods: A retrospective analysis of all patients undergoing pedicle screw instrumentation within the first year (October 2015 and December 2016) of introducing iCT navigated spinal instrumentation was done. In each surgery, an intraoperative CT scan for referencing the navigation was performed and subsequently one or more CT scans for intraoperative control of screw placement accuracy where performed. The cases were divided into three equal intervals for analysis. Results: Sixty five patients were identified. There were 55.4% female and 44.6 male patients. Median age of 68 years. According to the Gertzbein and Robbins classification grades, there was proper placement (A + B grade) in 85,5%, 88.8% and 87%in the first, second and third time interval, respectively. The intraoperative revision rate was 10.5%, 6.5% and 5.8% in the in the first, second and third interval, respectively. None of the patients required secondary surgery caused by screw misplacement or had any neurovascular damage. Conclusion: The learning curve for iCT was evident after 3 months. There was no difference in accuracy or revision rates between the second and third interval.
852
A290: The trends in robot-related complications, operative efficacy, radiation exposure, and clinical outcomes after robot-assisted spine surgery: a multicenter study of 722 patients and 5,005 screws from 2015 to 2019
Nathan Lee 1 , Ian Buchanan 1 , Venkat Boddapati 1 , Justin Mathew 1 , Paul Park 1 , Eric Leung 1 , Avery Buchholz 2 , John Pollina 3 , Ehsan Jazini 4 , Colin Haines 4 , Thomas Schuler 4 , Christopher Gooed 4 , Joseph Lombardi 1 , and Ronald A. Lehman 1
1 The Och Spine Hospital at New York-Presbyterian, New York, USA
2 University of Virginia Health System, Charlottesville, USA
3 State University of New York, Buffalo, USA, 4 Virginia Spine Institute, Reston, Reston, USA
Introduction: With the arrival of robot-assisted spine surgery nearly twenty years ago, there has been a growing amount of literature that suggests robots are safe and can achieve comparable outcomes to conventional techniques. However, much of this literature is limited by small sample sizes and single-surgeon or single center series. Furthermore, it is unclear what the impact of robotic technology has made on operative and clinical outcomes over time. This is the first and largest multicenter study to examine the trends in outcomes and complications after robot-assisted spine surgery over a five-year period. Material and Methods: We included adult (≥18 years old) patients who underwent robot-assisted (Mazor Renaissance, X, and Stealth) spine surgery from 2015-2019. Several perioperative factors were compared across the years of surgery. Outcomes of interest included operative efficiency (robot time per screw), radiation exposure (fluoroscopy time per screw), robot complications (e.g. screw exchange, robot abandonment), and clinical outcomes (e.g., length of stay, 90-day reoperations). The minimum follow-up was 90 days after the index surgery. Chi-square/fisher exact test and t-test/ANOVA were used for categorical and continuous variables, respectively. The Cochran-armitage test was used to examine statistically significant trends. Results: A total of 722 adult patients were included in this study (117 Renaissance, 477 X, 128 Stealth). The mean (standard deviation) Charlson comorbidity index was 1.5 (1.5) and 54.4% of patients were female. The most common diagnoses included high grade spondylolisthesis (40.6%), degenerative disc disease (18.4%), and degenerative scoliosis (17.6%), and the mean number of instrumented levels was 3.8 (3.4). Most patient and operative factors (e.g. gender, smoking status, total instrumented levels, and pelvic fixation,) were similar across the years. From 2015 to 2019, the mean robot time per screw decreased from 7.2 minutes to 5.5 minutes (P = .004, R2 = .65) and the mean fluoroscopy time per screw decreased from 15.2 seconds-9.4 seconds (P = .002, R2 = .83). Similarly, the rates of both intraoperative screw exchange for misplaced screw (P = .0115, R2 = .13) and robot abandonment (P = .011, R2 = .22) improved significantly over time. The incidence of other intraoperative surgical complications (e.g., dural tear, loss of motor/sensory function, blood transfusion) remained consistently low, but similar between years. The length of stay decreased by nearly 1 day from 2015-2019 (P = .007, R2 = .78), even though the mean Charlson comorbidity index worsened with time (P = .036). The 90-day reoperation rate did not change significantly over the last five years. Conclusion: Current trends demonstrate that robot screw accuracy, reliability, operative efficiency, and radiation exposure have improved significantly over the last five years. This is likely the result of increased surgeon experience with robots and the recent advances in robotic technology. The 90-day surgical complication rates remain consistently low and the mean length of stay has reduced significantly with time. These findings further validate continued usage of robot-assisted spine surgery and the potential path toward improved value-based care.
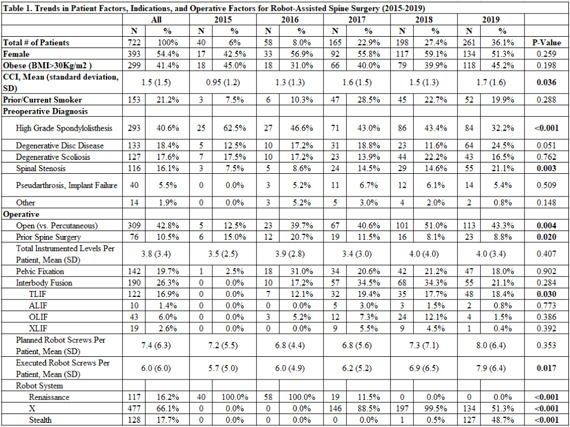

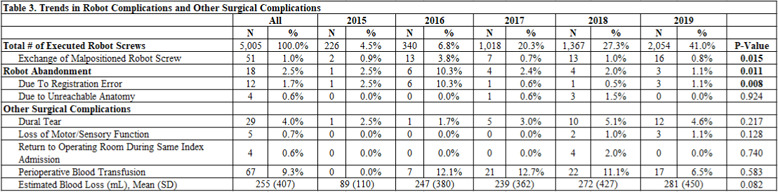

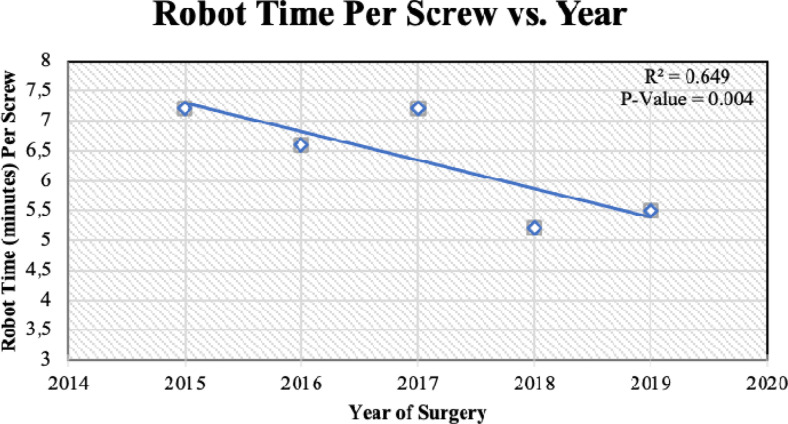
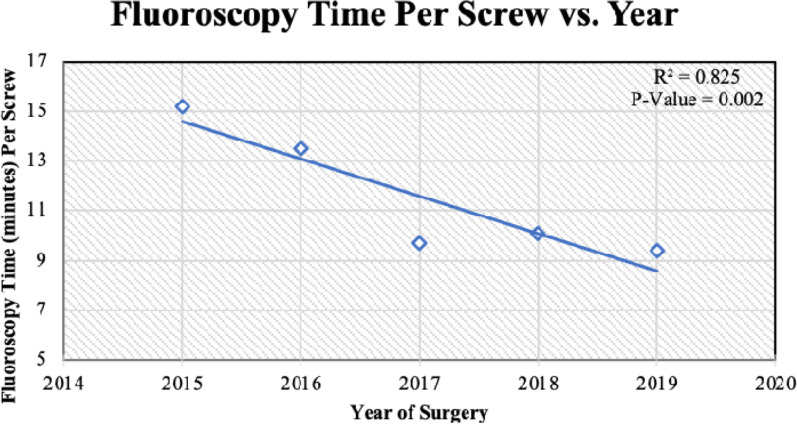

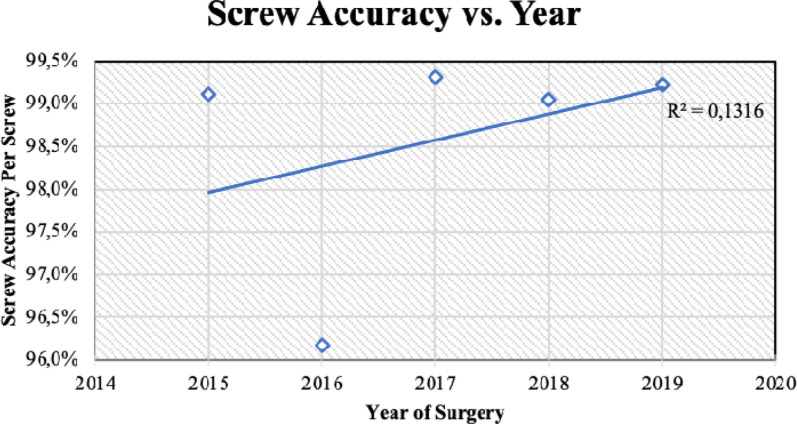
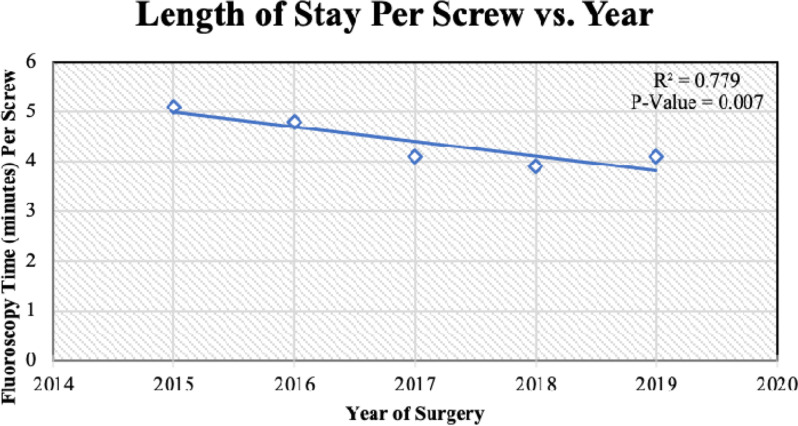
1301
A291: The iliac kickstand screw: a novel pelvic screw for correction of coronal spinal imbalance
James Lin 1 , Jun Kim 2 , Joseph Lombardi 2 , Meghan Cerpa 2 , and Lawrence Lenke 2
1 Mount Sinai, New York, USA
2 Columbia University Medical Center, New York, USA
Summary: The “iliac kickstand screw” is a novel pelvic screw that facilitates correction of coronal spinal imbalances. It has a uniquely lateral starting point which creates a longer lever arm for distraction. It was placed in 24 consecutive patients using the free hand technique with no neurovascular or visceral complications. The mean starting point is 6cm lateral to midline on the iliac crest. The screw trajectory is approximately 10 degrees of lateral angulation and 60 degrees cephalocaudal angulation. Hypothesis: The iliac kickstand screw can be placed safely and reliably. Study Design: Retrospective radiographic study. Introduction: The goal of spinal deformity surgery is to restore spinal alignment in both sagittal and coronal planes. While there has been significant emphasis placed on sagittal plane correction, coronal imbalance can also be debilitating. However, correction of large coronal deformities is challenging. We recently described the “kickstand rod” technique for correction of coronal imbalance. This technique utilizes powerful “construct-to-construct” distraction between a fixed multi-screw thoracic construct and the ilium, facilitated by a novel “iliac kickstand screw”. The technique for freehand placement of the “iliac kickstand screw”, as well as screw trajectories and parameters, have not been previously described. Methods: Consecutive adult patients who underwent spinal deformity surgery and coronal imbalance correction using the “kickstand rod” by the senior surgeon were identified. All screws were placed using the free hand technique. The starting point for the screw is near the most cephalad surface of the iliac crest, approximately 6cm lateral to midline. Screw accuracy was assessed using intraoperative O-arm imaging and screw trajectories and breaches were analyzed using 3D visualization software. Results: Twenty four consecutive screws were analyzed. The mean patient age was 50.1 years. 20 were female. 12 were left sided screws and 12 were right sided screws. The mean starting point was 59.5 mm lateral to midline. The mean horizontal angle was 10.8°, and the mean caudal angle was 57.9 . The mean screw size was 7.88 mm (range 7.5-8.5mm) and screw length was 74.2mm (range 70-90mm) 6 of 24 screws had cortical breaches, 5 of which perforated medially and 1 of which perforated inferiorly. There were zero clinically notable neurovascular or visceral complications. Conclusion: The “iliac kickstand screw” is a novel pelvic screw that facilitates correction of coronal spinal imbalances. It was placed in 24 consecutive patients using the free hand technique with no neurovascular complications. Take Home Message: We describe a novel “iliac kickstand screw” which facilitates correction of coronal imbalance.
338
A292: The “Unfair Advantage” of Mixed-Reality Simulation for Percutaneous Pedicle Screw Placement Makes it as Effective as Cadaver Training: a Prospective Randomized Study with Novice Volunteers
Simon Weidert 1 , Jonathan Bischoff 1 , Becker Christopher 1 , Kammerlander Christian 1 , Greiner Axel 1 , Mayr Matthias 1 , and Böcker Wolfgang 1
1 Ludwig Maximilians Universität Munich, Dpt. for General, Trauma and Reconstructive Surgery, München, Germany
Introduction: Becoming proficient in percutaneous pedicle screw placement requires training several skills such as correct c-arm adjustment, determining an ideal entry point and advancing the trocar using the projection images. The recommended gold standard training model is the cadaver. Its disadvantages are availability, cost and radiation dose. A hybrid simulator co-developed at the LMU Munich uses a clever combination of 3D printed specimens with virtual imaging and guidance to train these skills. This study will investigate the hypothesis that a mixed-reality simulator can be used to train the skill of percutaneous pedicle screw placement as effectively as with the cadaver and real C-arm imaging. Material and Methods: The mixed-reality simulator consists of a torso with an exchangeable spinal segment (lumbar and thoracic models were used). All instruments are electromagnetically tracked and the software can generate x-rays in all projections as well as CT and 3D rendering images in real-time. The study design is a randomized prospective study with a simulator group and a control group training on cadavers. The study is divided into a training day followed by a test day. Initially, theoretical training was given in a common seminar format. While the control group was then intensively trained in teams of two on the cadaver itself by an experienced surgeon for > 1 hour per individual trainee, the simulator group initially received only peer-teaching by a trained student on the simulator. On the test day, the simulator group participants were individually trained by the expert for 30 minutes before the test. All participants then implanted 2 percutaneous pedicle screws on the cadaver without further assistance. After each session, a CT was performed and the screw positions were evaluated. Time, number of images and radiation dose were recorded. Results: 12 medical students were equally randomized to both groups. All participants completed the training and test day. The main outcome parameter quality of pedicle screw placement was evaluated on CT according to Gertzbein-Robbins (GR). The simulator group achieved GR grade A or B (under 2 mm pedicle breach) in 93% of cases, the control group only in 58%. The stat. significance was slightly missed with P = .059. With regard to time, there was a tendency towards superiority of the simulator group that further showed a significantly reduced radiation personal dose over both days. Conclusion: The simulator group showed no inferiority but a clear tendency towards superior performance. Especially compared to day 1 of the control group, a strong effect of the simulator on skills is measurable. This is probably due to the “unfair advantage” of the constant availability (training immediately before the “real intervention” is possible), the repeatability as well as the visualization (to train projection thinking) and realistic haptics of the simulator. At least for the learning of percutaneous pediculation, the simulator shows excellent transfer learning and is at least an equivalent substitute for cadaver training.
1214
A293: Procedural Metrics for Minimally Invasive Lumbar Stenosis Decompression Using a Lumbar Astenosis Simulation Model to Improve the Skills and Accelerate the Learning Curve in Orthopedic and Neurosurgical Trainees
Carolin Melcher 1 , Andreas Korge 2 , Kevin Foley 3 , Rodrigo Navarro- Ramirez 4 , Ibrahim Hussain 5 , and Roger Härtl 5
1 University Hospital Ulm, Department of Orthopedic Surgery (RKU), München, Germany
2 Schoen Klinik Harlaching, Wirbelsäulenzentrum, München, Germany
3 University of Tennessee, Semmes-Murphey Neurologic and Spine Institute, Memphis, USA
4 McGill University Health Centre, Neurosurgery, Montreal, Canada, 5 Weill Cornell Medical College, New York Presbyterian Hospital, Center for Comprehensive Spine Care, New York, USA
Introduction: Surgical training as a resident or fellow as well as during specialization on master level depends on theoretical knowledge as well as the manual ability to perform a specific task skillfully, reliable and safely. Many experienced surgeons who expertly perform a specific procedure are able to identify and agree on the essential “steps” to be completed and “ errors” to be avoided, whereas they rarely think about the procedures they perform with the level of detail needed to identify those key features. Previous studies demonstrated that repetition of surgical tasks and using real surgical instruments while training on a simulator can help trainees to improve their surgical skills, performance and level of comfort during surgery. This might even be enhanced by a step-by-step guide performance metrics for a minimal invasive unilateral laminotomy for bilateral decompression (ULBD) of lumbar spinal stenosis with and without spondylolisthesis were defined in an earlier study. Material and Methods: In a prospective two-armed comparative study simultaneously performed at 2 centers, one in the US (Neurosurgery) and one in Germany (Orthopedic surgery) 6 trainees from each center performed three identical decompression procedures on a spinal simulator using the metrics for ULBD. The learning curve was evaluated regarding technical skills, timing and occurrence of errors and sentinel errors using the metrics sheet as well as instructor and personal surveys and a gap analysis. Furthermore, video recordings of all procedures were rated by 3 individual experts using a global rating scale and a video specific checklist. Results: Within all residents the quantity of errors and sentinel errors were significantly reduced from procedure 1 to procedure 3 with a concomitant reduction of surgical time and skipped steps. Not only did the participants report progress in subjective perception with the personal survey, but the improvement of the surgical skills with better surgical outcome, higher economy of motion and instrument use was accredited by all evaluation tools (instructor survey, gap analysis, video analysis) and within all levels of experience. Conclusion: Procedural metrics for ULBD in combination with a surgical simulator can be successfully used in surgical training to improve the surgical skills of surgeons of all levels.
1907
A294: Evolution of image guidance in minimally invasive transforaminal lumbar interbody fusion (MI-TLIF): comparing the learning curves of fluoroscopy, navigation and robotics
Avani Vaishnav 1 , Jung Kee Mok 2 , Hikari Urakawa 1 , Kosuke Sato 3 , Ryan Lee 4 , Chirag Chaudhary 1 , Catherine Himo Gang 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
2 Weill Cornell Medical College, New York, USA
3 University of Tsukuba, Tsukuba, Japan
4 George Washington University School of Medicine, Washington, DC, USA
Introduction: Intra-operative image-guidance has undergone tremendous advancements in recent years, evolving from two-dimensional modalities such as 2D fluoroscopy or serial radiography to 3-dimensional computer assisted navigation, and more recently robotics. Despite these advances, concern regarding the learning curve of new technologies remains a deterrent to greater adoption. Thus, the purpose of this study was to evaluate the learning curve of fluoroscopy, intraoperative navigation (ION) and robotic navigation for minimally invasive TLIF (MI-TLIF). Material and Methods: A retrospective review of prospectively collected data on consecutive patients who underwent single-level MI-TLIF by a single surgeon using fluoroscopy, intra-operative navigation or a robot was performed. Outcomes of interest were operative time, estimated blood loss, intra-operative complications, radiation exposure, length of stay (LoS) and reoperations. Chronologic case number for each modality was plotted against each outcome of interest. The derivative of a nonlinear association or dissociation curve fit to the dataset was solved for the point at which the slope of the curve equaled the linear slope. At this point, average rate of change equals the instantaneous rate of change on the nonlinear curve. Therefore, rate of change after this case will be less than the average rate of change, suggesting a plateau in learning had occurred. Results: Of the 225 patients included, 109 underwent MIS-TLIF using fluoroscopy, 77 using ION and 39 using robotic navigation. There was no learning curve for estimated blood loss, length of stay or operative complications in any cohort. Fluoroscopy. Median operative time was 112 minutes, fluoroscopy time 144seconds and radiation dose was 62.7 mGy. There were no intra-operative complications; 11(10.0%) patients required reoperation (2 epidural hematoma, 2 failed hardware, 2 pseudarthrosis, 2 recurrent stenosis, 3 ASD).Operative time: Proficiency: 38 cases (Before vs after proficiency = 137 vs 104minutess, P < .0001). Fluoroscopy time: Proficiency: 51 cases (Before vs after proficiency = 168 vs 126 seconds, P < .0001). Radiation dose: Proficiency: 51 cases (Before vs after proficiency = 72.05 vs 53.95 mGy, P = .008). Reoperations: Proficiency: 43 cases. (Before vs after proficiency = 18 vs 5%; P = .023). Intra-operative 3D Navigation. Median operative time was 88minutes, fluoroscopy time 25seconds and radiation dose 47 mGy. There were no intra-operative complications; 5(6.5%) patients required a repeat spin intra-operatively and 7(9.1%) underwent a reoperation (1 each - SSI, screw repositioning, cage displacement, superficial hematoma, ASD, recurrent stenosis, pseudoarthrosis with painful hardware). Operative time: Proficiency: 31 cases (Before vs after proficiency = 95 vs 80 minutes, P < .0001) Fluoroscopy time, radiation dose, repeat spin and reoperations: No learning curve. Robotic Navigation. Median operative time was 103 minutes, fluoroscopy time 18seconds and radiation dose 38.1 mGy. There were no intra-operative complications; the first patient required intra-operative manual repositioning of one screw (2.6%), and 1 (2.6%) required a revision surgery for residual stenosis. Operative time, fluoroscopy time and radiation dose: No learning curve. Intra-operative screw repositioning and reoperations: Could not be assessed due to low incidence. Conclusion: Our results suggest that newer intra-operative image-guidance modalities have the potential to reduce or even eliminate the learning curve for minimally invasive procedures and may thus allow for greater adoption of these techniques.
856
A295: Does Robot-Assisted Spine Surgery Achieve Better Patient - Reported Outcomes than Freehand Techniques?
Nathan Lee 1 , Ian Buchanan 1 , Venkat Boddapati 1 , Justin Mathew 1 , Paul Park 1 , Eric Leung 1 , Joseph Lombardi 1 , and Ronald A. Lehman 1
1 The Och Spine Hospital at New York-Presbyterian, New York, USA
Introduction: It is well-known that robot-assisted spine surgery can achieve similar pedicle screw accuracy as conventional freehand techniques. However, the literature comparing the patient-reported outcomes remains relatively sparse. Material and Methods: We included adult (≥18 years old) patients who underwent robot-assisted spine surgery from 2016 to 2018. The minimum follow-up was 2-years after the index surgery. Patients with missing values were excluded. A propensity-score matching algorithm accounted for several perioperative factors (gender, Charlson comorbidity index, preoperative diagnoses, instrumented levels, interbody fusion, and pelvic fixation) to control for the potential selection bias between freehand and robot-assisted surgery. Patient reported outcomes were measured using the Oswestry Disability Index (ODI). The minimum clinically important difference (MCID) rates between groups were assessed at each follow-up period (6-weeks, 6-months, 1-year, and 2-years). Chi-square/fisher exact test and t-test/ANOVA were used for categorical and continuous variables, respectively. Results: After propensity score matching, a total of 70 patients remained. The mean (standard deviation) Charlson comorbidity index was 1.4 (1.0) and 57% of patients were female. The most common diagnoses included degenerative disc disease (37.1%), degenerative scoliosis (27.1%), and high grade spondylolisthesis (19%), and the mean number of instrumented levels was 4.6 (4.4). Rates for intraoperative complications, postoperative complications, and any reoperation within 2 years after surgery were low and similar between groups. The baseline ODI scores were similar between freehand (39.1) and robot-assisted surgery (40.5, P-value = .736). By two years, substantial improvements in both groups (mean ODI - freehand: 4.6, robot-assisted: 1.5; and MCID% - freehand:77.1%, robot-assisted: 82.9%) were achieved, but not significantly different. Similarly, no differences were observed for the other follow-up periods. When comparing individual component scores, the robot-assisted group scored higher in “Lifting,” “Sitting,” and “Standing;” however, the magnitudes of these differences were less than 1 point. Conclusion: In this single-surgeon series, robot-assisted spine surgery can achieve excellent and similar patient-reported outcomes to conventional freehand techniques. Future studies should include large, prospective randomized controlled trials as well as the inclusion of other patient reported outcome measures.
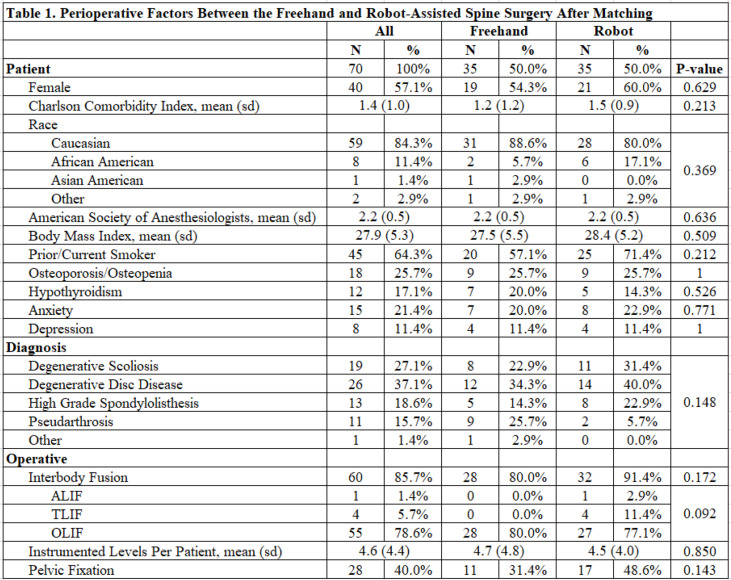
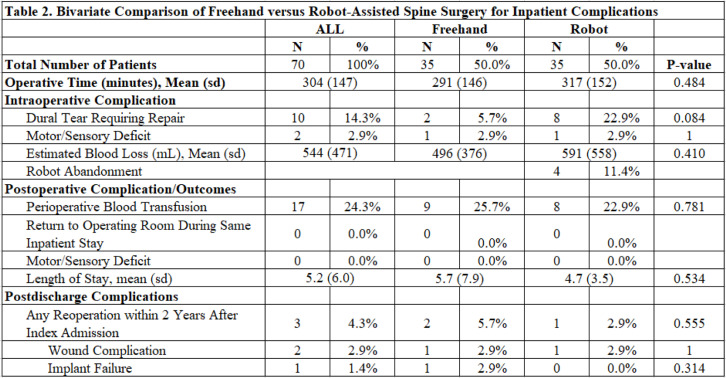
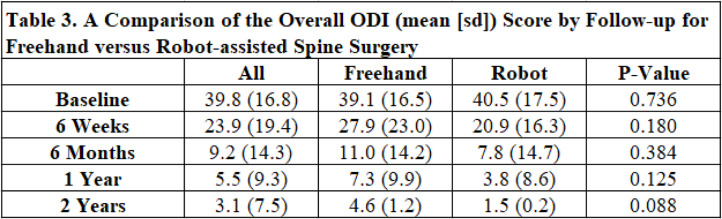
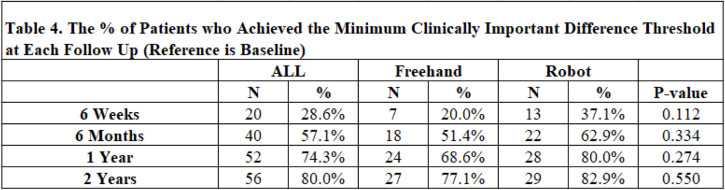
1199
A296: Clinical Outcomes and Complications of Computer Navigated Minimal Invasive Postero-Lateral Sacro-Iliac Joint Fusion Using a Threaded Bolt System
Carlos De La Torre 1 and Khai Lam 1
1 London Bridge Hospital, London, United Kingdom
Introduction and Purpose: We report the clinical and radiological outcomes or a retrospective case series (novel postero-medial approach) to perform a minimal invasive SIJ fusion using a threaded bolt system performed under computer navigation. Materials and Methods: Between September 2017 and August 2020, we identified 27 consecutive patients undergoing SIJ fusion. The diagnosis of SIJ pain was made following a detailed clinical history, examination, CT and MRI scans, followed by positive diagnostic injections. Patient related outcome measures (PROMS) were collected preoperatively, 3 months, and 6 months postoperatively. PROMS included Oswestry Disability Index (ODI), SF-36, EQ5-D, Visual Analog Scale (VAS) for both back (BP) and leg pain (LP). We collected estimated blood loss (EBL), duration of surgery (DOS) and length of hospital stay (LOS). Technique: In a prone position, a 2 cm skin incision is made 2 cm lateral and superior to the postero-superior iliac crest. Then 2 implants were threaded across the SIJ via a postero-medial ‘tubular’ approach under 3D computer navigation, aimed parallel to the S1 endplate or pointed toward the sacral promontory, and crossing just proximal to the SIJ sulcus into the subchondral bone. Appropriate length threaded hollow bolts that was packed with local bone autograft and allograft (human DBM) before final insertion through the pilot hole. Results: There were 77% female and 23% male with mean age 53 (24-85) years, average LOS 2.1 days (range 1-3), mean EBL <20 ml, and DOS 60 minutess (range 40-120). For ODI, statistically significant mean improvements from pre-operative at 3 and 6 months follow-up were 11.9 ± 9.1 (P < .001) and 18.2 ± 13.7 (P < .001) respectively. For VAS BP, similar significant mean improvements of 2.6 ± 2.1 (P < .0001) and 3.5 ± 2.2 (P < 001), and for VAS LP of 2.8 ± 2.8 (P < .0001) and 3.3 ± 2.5 (P < .0001). The PCS and MCS domains of SF-36 and EQ-5D will be presented at the congress. 14 patients had history of previous lumbar spine surgery.Based on a previous study 1 the percentage of patients that met the MCID at 6 months for ODI, VAS BP and VAS LP were 66%, 85% and 77% respectively. No serious adverse events occurred, and no one required a return to the operating theatre for revision surgery. Conclusions: Surgery using this threaded Titanium hollow bolt system performed via a novel postero-medial approach under 3D computer navigation allows for a truly safe minimal invasive surgery to fuse the SIJ. The technique results in minimal blood loss, rapid patient mobilization and early discharge home within 48 hours. Early 6 months results show statistically significant improvements in all aspect of PROMS and MCID. Further follow-up at 1 and 2 years will continue to confirm the durability of this technique.
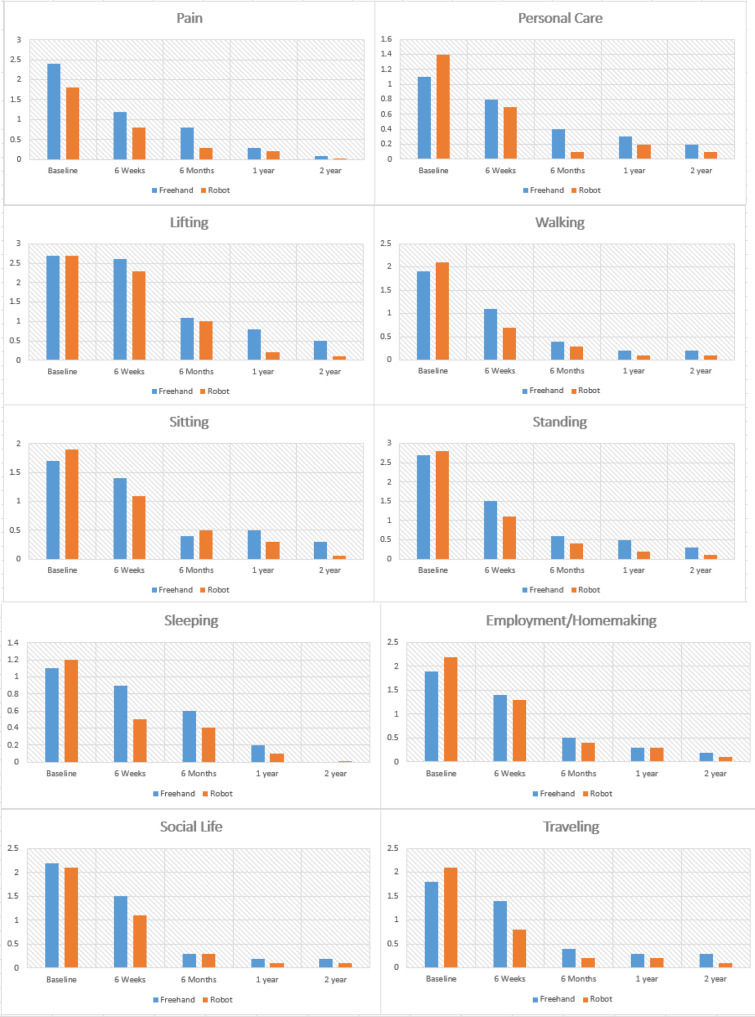
1128
A297: First Experiences With a Reinforced Lumbopelvic Fixation Technique with 6 Months Follow-Up
Schippers Philipp 1 , and Jacques Dominik Müller-Broich 1
1 Orthopedic University Hospital Friedrichsheim, Frankfurt am Main, Germany
Introduction: Lumbopelvic fixation is a common procedure in primary and revision spinal surgery but leads to high biomechanical stress on adjacent segments and the SIJ, resulting in implant failure such as breakage and loosening and pain. This frequently results in further surgery. For patients showing clinical and radiological signs of SIJ affection/arthrosis who fail conservative therapy, lumbopelvic fusion may be considered. The Bedrock™ technique has been described as a new option for reinforced lumbopelvic fixation, fusing the SIJ with additional triangular titanium implants, thereby reducing biomechanical loads off the S2AI screws. We share our first experiences with this new technique with a mean follow-up of 6.6 (SD = 6.6) months. Materials and Methods: Six patients suffering from persisting low back pain (LBP) with indication for reinforced lumbopelvic fixation and SIJ fusion were treated with this new technique. All surgeries were carried out by a single surgeon at our orthopedic university hospital. Data was gathered retrospectively. Results: Since January 2019, six patients (3f, 3m) were treated with reinforced lumbopelvic fixation and SIJ fusion with a mean follow up of 6.6 months (SD = 6.6). Walking distance was reduced to an average < 100 m. Standard treatment involved S2AI screws and triangular titanium implants (SIBone, iFuse 3D™) Five patients had prior lumbar or lumbosacral fusion but persistent LBP and significant SIJ arthrosis. Three patients had screw loosening and/or low grade infection of the screws. One patient suffered from multisegmental osteochondrosis/SIJ arthrosis. Mean age was 72.5 years (SD = 10.2), mean length of stay in hospital was 15.7 days (SD = 9.4). Average number of fused lumbar/thoracic segments 3.8 (SD = 2.1). Sagittal balance improved from (PI-LL) pre-OP 32.2° (SD = 22°) to post-OP 20.6° (SD = 11.5°). Average implant length was 65 mm bilaterally. There were no intraoperative or implant associated adverse events (AE) or serious adverse events (SAE). Postoperative imaging demonstrated good implant positioning and function. At time of article submission, all patients regained walking ability for distances > 1000 m and were satisfied with the result. All patients reported significant reduction of SIJ pain. One revision case had prior suspicion of infection that was treated conservatively via i.v. and oral antibiotics. One dural tear occurred at the lumbar level. One patient had a L5 screw misplacement requiring revision surgery six months later. Conclusion: We report our results of six patients with a new reinforced lumbopelvic fixation and fusion by S2AI screws augmented by one parallelly placed triangular titanium implant fusing the SIJ bilaterally with a mean follow-up of 6.6 months. Intra- and postoperatively we experienced no implant associated adverse event. Patients regained significant walking ability and significant reduction of SIJ pain. Radiologically no signs of implant loosening or failure were detected at the end of follow-up. Our first results seem to demonstrate a safe and efficacious surgical technique for reinforced lumbopelvic fixation with fusion of SIJ with significant improvement of the health care related quality of life. Further studies need to be conducted in order to obtain additional evidence.
OP34: Trauma-Cervical
1080
A298: Long Term Proms (Patient Reported Outcome Measures) for the Non-Operative Management of Odontoid Peg Fractures in the Elderly
Andreas Demetriades 1 and Henry Searle 2
1 Royal Infirmary Edinburgh, Department of Neurosurgery, Edinburgh, United Kingdom
2 Edinburgh University Medical School, Edinburgh, United Kingdom
Objectives: Controversy persists on the best management of C2-peg fractures in the elderly. The aim of this study was to investigate the effect of conservative treatment with a neck brace using patient-reported outcome measures. Design: This was a questionnaire-led, prospective cohort study. Subjects: Elderly patients with a type II C2-peg fracture who were managed in a brace for three months between June 2015 and March 2019 were divided into three age groups: 65-75, 75-85 and >85. Methods: Participants were invited to complete COMI and NDI questionnaires. Results were collated, stored on a database and analysed using descriptive statistics. Means are reported with standard deviation, and medians with interquartile range. Results: 110 patients completed the NDI and 107 patients completed the COMI. The mean age for the COMI and NDI was 78.3 (±8.0) and 78.2 (±8.1) years. The median examination interval was 6.4 (5.3) and 6.3 (4.0) months for the COMI and NDI respectively. Whilst 29% of the whole cohort reported no problems, 50% reported some neck pain but only 15% describing this pain as severe. 34% reported no pain. 77% experienced nil, slight or infrequent headaches. 62% had sleepless nights only lasting 0-2 hours. Mean neck pain was rated 3.5 (±2.9)/10, with mean arm/shoulder pain rated 2.4 (±2.9) /10. Pain decreased as examination interval increased in groups 65-75 and 75-85, but not in those aged >85 where pain slightly increased. Overall 75% described their quality of life (QoL) as very good, good or moderate. These results were maintained across all age groups, with 50% aged >85 experiencing no pain and 69% rating their QoL as very good, good or moderate. Conclusion: Neck brace management of C2-peg fractures for three months avoids the risks of surgery and has a clear benefit with a good patient-reported QoL and minimal effect on the functional aspects of patients’ lives.
316
A299: Variation in Global Treatment Practices of Subaxial Cervical Facet Fractures
Brian Karamian 1 , Gregory Schroeder 1 , Jose Canseco 1 , Martin Holas 2 , Andrei Joaquim 3 , AO Spine Knowledge Forum Trauma 4 , Cumhur Oner 5 , Christopher Kepler 1 , and Alexander Vaccaro 1
1 Rothman Orthopaedic institute, Philadelphia, USA
2 Teaching Hospital F. D. Roosevelt, Banská Bystrica, Slovakia
3 Neurosurgery Division, Department of Neurology, State University of Campinas, Campinas-Sao Paulo, Brazil
4 AO Foundation, Davos, Switzerland, 5 University Medical Center, Utrecht, Utrecht, The Netherlands
Introduction: The management, including the workup and treatment, of unilateral subaxial facet fractures remains controversial. Given this uncertainty, it is important to understand the effects of regional bias on the treatment of facet fractures and elucidate what surgeon characteristics influence treatment preferences. The goal of this study, therefore, is to determine the variation in the global treatment practices for unilateral facet fractures, and to determine how surgeon experience, practice setting, and subspecialty affect the work-up and treatment of subaxial cervical spine facet fractures. Methods: A 22-question survey was sent to 272 members of the AO Spine Cervical Classification Validation Group. These spine surgeons represent six world regions: North America, Latin and South America, Europe, Africa, Asia, and the Middle East. Clinical vignettes consisted of fracture types F1-F3 with various associated neurologic injuries (N0-N2) classified using the AO Spine Subaxial Cervical Classification System. Questions surveyed surgeon preferences with regards to diagnostic workup and management. Results: A total of 161 responses were received. The AO Spine Subaxial Classification system remains the most widely used classification system among surgeons globally, preferred by 71.9% of all surgeons, with no statistically significant differences between world regions, surgeon experience, practice setting, or surgical subspecialty. Academic surgeons use the facet portion of the AO Spine classification system less frequently (61.6%) compared to hospital employed and private practice surgeons (81.1% and 81.8%, respectively) (P = .029). The overall consensus was for the operative treatment of any facet fracture with radicular symptoms and for any fractures categorized as F2N2 and above (ie F3N0, F3N1, F3N2). For F3N0 fractures, significantly less surgeons from Africa/Asia/Middle East (49%) and Europe (59.2%) chose operative treatment than from North/Latin/South America (74.1%) (P = .025). For F3N1 fractures, significantly less surgeons from Africa/Asia/Middle East (52%) and Europe (63.3%) recommended operative treatment than from North/Latin/South America (84.5%) (P = .001). For fractures treated non-operatively, the preferred method by the majority of surgeons was immobilization in a hard collar. No consensus could be made regarding anterior versus posterior surgical approach for operative management. Greater than 95% of surgeons included CT in their work-up of facet fractures, regardless of type. No statistically significant differences were seen in the need for MRI to decide treatment. Conclusion: This is the first study to evaluate global variation in the management of subaxial facet fractures. This study demonstrates considerable agreement between surgeon preferences with regards to facet fracture management despite differences in geographic region, surgeon experience, practice setting, or subspecialty with few exceptions.
522
A300: Posterior Atlantoaxial Fusion: Technique and Retrospective Case Series
Andrew Platt 1 , Mena G. Kerolus 2 , Brian T. David 2 , and Vincent C. Traynelis 2
1 University of Chicago, Chicago, USA
2 Rush University Medical Center, Chicago, USA
Introduction: The most common indications for posterior atlantoaxial fusion are trauma and degeneration, which can encompass a spectrum of pathologies including atlantoaxial arthrosis and atlantoaxial instability. This study is a description of technique with accompanying operative video and retrospective case series of patients undergoing posterior atlantoaxial fusion. Material and Methods: All patients who underwent atlantoaxial posterior fusion by one surgeon at an academic medical center between 2010 and 2018 were included. Primary outcome measures included number of levels instrumented, estimated blood loss (EBL), complications, reoperations, length of stay, destination upon discharge, and rate of postoperative fusion which was assessed by computed tomography (CT) at the 12 month postoperative visit. Patient reported outcomes, prospectively collected and retrospectively analyzed, including Short Form Survey (SF-12), Modified Japanese Orthopedic Association Scale (mJOA), Neck Disability Index (NDI), and Visual Analogue Scale (VAS) were also assessed. Results: The key aspects of the employed operative technique include: positioning of the patient under live fluoroscopic x-ray to ensure adequate visualization of C1 and C2, coagulation and division of the C2 nerve roots proximal to the ganglion, placement of bilateral machined cortical allografts into the C1-2 facet joint space, placement of bi-cortical guide holes into each C1 lateral mass using a 0.63mm K-wire and drill prior to placement of C1 lateral mass screws, passage of a suture beneath the lamina of C1 tied to an Atlas cable that is then looped around the spinous process of C2 and used to tightly secure a rib graft in place. Forty-seven patients (mean age 65.4 ± 15.8 years) were included in analysis following C1-2 fusion with mean follow-up 13.8 ± 11.4 months. The most common surgical indications were C1-2 instability, C1-2 arthrosis, and type II odontoid fracture. The mean total number of instrumented levels was 2.6 ± 1.2. Mean estimated blood loss was 351.1 ± 390.4cc. The minor complication rate was 12.8%, with the most common complication being postoperative hyponatremia, and major complication rate was 2.1%, a single postoperative mortality related to multisystem organ failure. The reoperation rate was 8.5% and the average time to reoperation was 436.3 ± 576.5 days. Average length of stay was 7.6 ± 9.1 days. Seventy-four percent of patients were discharged to home. The postoperative fusion rate was 81%. Postoperatively, SF-12 mental health and physical health scores increased from 40.8 ± 11.3 and 33.8 ± 9.9 to 48.1 ± 10.3 and 36.0 ± 11.1, respectively. The increase in the SF-12 mental health was statistically significant(P = .002). NDI decreased from 43.4 ± 16.4 to 38.5 ± 24.3. VAS-neck scores significantly decreased from 6.4 ± 2.5 to 4.2 ± 2.8 (P = .002). There were no significant changes in mJOA or VAS-arm scores. Conclusion: The above technique for C1-2 fusion has shown to be safe with a major complication rate of 2.1% and reoperation rate of 8.5% and effective with a high rate of postoperative fusion (81%) likely related to the fastidious operative technique. During the course of the study patients showed significant improvements in SF-12 mental health and VAS-neck scores. Although there was a decrease in NDI postoperatively, the difference was not statistically significant.
1172
A301: Risk Factors Associated with 90-Day Readmission Following Odontoid Fractures - A Nationwide Readmissions Database Study
Alexander von Glinski 1 , Christopher Elia 1 , Tye Patchana 1 , Ariel Takayanagi 1 , Varun Arvind 1 , Clifford Pierre 1 , Basem Ishak 1 , Jens Chapman 1 , and Rod Oskouian 1
1 Swedish Neuroscience Institute, Seattle, USA
Introduction: Hospital readmissions represent a large financial burden upon our healthcare system. Management of odontoid fractures, which are the most common isolated spine fracture in the elderly, continues to be debated. We used the Nationwide Readmission Database (NRD) to identify readmission rates and factors related to readmission after surgical and non-surgical management of odontoid fractures. Methods: A retrospective study was performed using the 2016 Healthcare Utilization Project (HCUP) NRD. Demographic information and factors associated with readmission were collected. Readmission rates, complications, length of hospital stay were collected. Patients treated operatively, non-operatively, and patients who were readmitted or not readmitted were compared. Statistical analysis was performed using open source software SciPy (Python v1.3.0) for all analyses. Results: We identified 2,921 patients who presented with Type II dens fractures from January 1st 2016 to September 30th 2016, 555 of which underwent surgical intervention. The readmission rate in patients who underwent surgery was 16.4% (91/555) and 29.4% (696/2366) in the non-operative group. Hospital costs for readmitted and non-readmitted patients were $353,704 and $174,922, and $197,099 and $80,715 for non-operatively managed patients, respectively. Medicaid and Medicare patients had the highest readmission rate in both groups. Charlson and Elixhauser comorbidity indices were significantly higher in patients who were readmitted (P < .0001). Conclusion: We report an overall 90-day readmission rate of 16.4% and 29.4%, in operative and non-operative management of type II odontoid fractures, respectively. In the face of a rising incidence of this fracture in the elderly population, an understanding of the comorbidities and age-related demographics associated with 90-day readmissions following both surgical and non-surgical treatment are critical.
1263
A302: Diagnostic Imaging in Subaxial Discoligamentous Injury - Is CT Sufficient?
Svorad Trnovec 1 , Benedikt Trnovec 2 , Christian Henker 1 , Steffen Sola 1 , Kamil Kolejak 2 , and Thomas Freiman 1
1 Universitätsmedizin Rostock, Neurosurgery, Rostock, Germany
2 Slovak medical university, University hospital Bratislava, Neurosurgery, Bratislava, Slovakia
Introduction: Traumatic injuries of the cervical spine can be accompanied by significant neurological deficits and an impaired prognosis. Choosing the best therapy and prevention of secondary injuries relies on an adequate and reliable diagnostic. Discoligamentous injuries are often concomitant to cervical fractures or can appear as solitary lesions and still are diagnostic challenging. The aim of our study was to assess the sensitivity and specifity of CT and MR imaging for diagnosis of discoligamentous injuries. Methods: In this retrospective study, only patients after subaxial cervical spine injuries with abnormal findings on initial CT or MR imaging were included. Vertebral body burst fractures and luxation injuries were excluded. Clinical data was extracted from in-house medical charts. Results: In this retrospective study, a total of 34 patients, treated between 2010 and 2018 at our department, were included. 31 cases were examined with initial CT and followed MRI scan, 3 cases had only an MRI scan. Neurological status was unaffected within 13 patients, 8 showed injuries of cervical nerve roots, incomplete tetraplegia was observed in 10 patients, complete paraplegia/tetraplegia in 2. Primary CT was suspicious for discoligamentous injuries in 24 cases, MRI scan was followed in all these patients. Within 3 of these, no lesion was detected within MRI and flex/ext. x-ray films. In 7 cases, CT finding was primary negative, but MRI was performed due to neurological deficits, radicular pain or severe neck pain. In all of these cases, MRI revealed a discoligamentous injury. A total of only one MRI was confirmed false negative with gross instability in flex/ext. x-ray films and complete disc rupture shown during surgery. 3 CT scan were rated false positive and another 6 as false negative. 29 cases were treated surgically, one with external bracing and 4 patients with conservative therapy. Conclusions: Beside an accurate diagnostic quality of CT for bony injuries of the cervical spine after trauma, for the detection of discoligamentous injuries MRI is still superior. Despite the higher sensitivity of MRI, some cases will still need a further clinical evaluation or dynamic motion studies via flexion-extension X-ray films. A clinical neurological symptomatic, also pain too, should be indication for MRI.
1259
A303: Traumatic Cervical Spine Injuries in Rugby Players: A South American Trinational Case Series
Juan José Zamorano 1 , Ratko Yurac 1 , Alfredo Guiroy 2 , Juan Pablo Guyot 3 , Fernando Nin 4 , and Marcelo Alejandro Valacco 5
1 Clínica Alemana de Santiago, Spine Unit-Department of Orthopedics and Traumatology, Santiago, Chile
2 Hospital Español de Mendoza, Department of Orthopedics, Mendoza, Argentina
3 Fundación Favaloro, Buenos Aires, Argentina
4 Medica Uruguaya, Montevideo, Uruguay
5 Sanatorio Finochietto, Buenos Aires, Argentina
Introduction: Traumatic cervical spine injuries may carry catastrophic consequences to patients and their families. Although infrequent, their incidence after rugby-related trauma has increased in recent years, as reported mainly in literature from the UK, France and New Zealand. Until the year 2000, most of these lesions were produced by traumatic mechanisms to the cervical spine occurring during a scrum, leading to modifications in scrumming regulations, which helped to reduce the injury risk in forwards. Recent literature has reported a higher incidence of injuries among backs and during tackling. There is still no consensus regarding return to rugby practice after a traumatic cervical spine injury. We describe a case series of rugby players from three Latin American countries with traumatic cervical spine injuries due to game-related trauma, focusing on injury mechanism, treatment modality and return to play. Material and Methods: Retrospective, descriptive case series. We collected cases of rugby-related traumatic cervical spine injuries using the authors’ network of spine surgeons in Argentina, Chile and Uruguay. We used an electronic spreadsheet format to collect several variables (demographics, player position, injury mechanism and type, diagnostic study, treatment and return to sport, particularly return to rugby). The information was filled in by the collaborating spine surgeons and all the collected data was pooled into one file for statistical analysis. Results: We collected a total of 38 male patients (63.2% from Argentina, 21% from Chile and 15.8% from Uruguay), injured between 1993 and 2019. Mean age 22 years (range 15-35 years) and 57.9% were backs. Regarding the mechanism, 52.6% of the patients were injured during tackles (even distribution of tacklers and tackled players), 28.9% in scrums and 18.4% during other formations. All the patients presented single-level injuries, with fracture-dislocations as the most frequent type of lesion (57.9%), followed by fractures (26.3%) and traumatic cervical disc herniations (15.8%). The most affected levels were C5-C6 and C6-C7 (23.7% each). Under one third of the patients (31.6%) was able to continue playing after the injury and 55.3% presented some type of neurological impairment, ranging from complete tetraplegia (7.9%) to transient radicular symptoms. Thirty-one patients (81.6%) required surgical treatment, mainly in the form of an anterior cervical discectomy and fusion (45.2%), while 25.8% required a combined anterior/posterior approach. Regarding return to sports, 73.7% was able to resume some type of sport, while 78.6% of them (22/28 patients) returned to rugby, with a median of 314 days after the accident (range 55-609 days). Conclusion: Traumatic cervical spine injuries must be ruled-out in rugby players presenting neck pain and/or neurological symptoms after a game-related trauma. In line with recent literature, in our case series the incidence was higher among backs and during tackling and their treatment usually required surgery. Although over 50% was able to return to rugby, there is still no consensus regarding this topic.
604
A304: Regional and Experiential Differences in Surgeon Preferences for the Treatment of Cervical Facet Injuries
Jose Canseco 1 , Gregory Schroeder 1 , Brian Karamian 1 , Parthik Patel 1 , Giovanni Grasso 2 , Michael Chang 1 , Frank Kandziora 3 , Emiliano Vialle 4 , Cumhur Oner 5 , Klaus Schnake 6 , Marcel Dvorak 7 , Jens Chapman 8 , Lorin Michael Benneker 9 , Shanmuganathan Rajasekaran 10 , AO Spine Cervical Classification Validation Group 11 , Christopher Kepler 1 , and Alexander Vaccaro 1
1 Rothman Orthopaedic institute, Philadelphia, USA
2 Neurosurgical Unit, Department of Biomedicine, Neurosciences and Advanced Diagnostics, University of Palermo, Palermo, Italy
3 Center for Spine Surgery and Neurotraumatology, BG Unfallklinik Frankfurt am Main, Frankfurt, Germany
4 Department of Orthopaedics, Catholic University of Parana, Curitiba, Brazil, 5 University Medical Center, Utrecht, Utrecht, The Netherlands
6 Center for Spinal Surgery, Malteser Waldkrankenhaus St. Marien, Erlangen, Germany
7 Department of Orthopaedics, Vancouver General Hospital, Vancouver, Canada
8 Swedish Neuroscience Institute, Swedish Medical Center, Seattle, USA
9 Spine Service, Orthopaedic Department, Sonnenhofspital, Bern, Switzerland
10 Department of Orthopaedics, Trauma and Spine Surgery, Ganga Hospital, Coimbatore, India
11 AO Foundation, Davos, Switzerland
Introduction: The management of cervical facet dislocation injuries remains controversial. There is persistent debate among surgeons regarding imaging modalities, the appropriateness of nonoperative management, as well as surgical approach. The main purpose of this investigation was to identify whether a surgeon’s geographic location or years in practice influences their preferred management of traumatic cervical facet dislocation injuries. Methods: A 25-question survey was sent to 272 AO Spine members located in six different geographic regions (Africa, Asia, Europe, Latin/South America, the Middle East and North America) with various years of practice experience. The survey included clinical case scenarios of cervical facet dislocation injuries and asked responders to select preferences among various diagnostic and management options. Results: A total of 189 complete responses were received. Over 50% of responding surgeons in each region elected to initiate management of cervical facet dislocation injuries with an MRI, with 6 case exceptions. Overall, surgeons that chose operative management were more likely to intervene with an anterior cervical discectomy and fusion (ACDF) for either bilateral (43.3%) or unilateral (46.0%) jumped facets status post-reduction. There was considerable agreement between American and European responders regarding management of these injuries, with only 3 cases exhibiting a significant difference. Additionally, results also exhibited considerable management agreement between those with ≤ 10 and > 10 years of practice experience, with only 2 case exceptions noted. Conclusion: More than half of responders, regardless of geographical location or practice experience, identified MRI as a screening imaging modality when managing cervical facet dislocation injuries, regardless of the status of the spinal cord and prior to any additional intervention. Additionally, a majority of surgeons would elect an anterior approach for the surgical management of these injuries. The study found overall agreement in management preferences of cervical facet dislocation injuries around the globe.
1420
A305: Unstable Jefferson Burst Fractures: Intraoperative Stability Testing After Posterior Atlas Ring Osteosynthesis (C1-Ro) Regardless of Dickman Type Transverse Atlantal Ligament (Tal) Lesion Allows Determination of The Extent of the Surgical Procedure
Andy Ottenbacher 1 , Rizk Ahmed 1 , and Bettag Martin 1
1 Krankenhaus der Barmherzigen Brüder Trier, Neurosurgery, Trier, Germany
Introduction: Atlas ring osteosynthesis (C1-RO) is a motion preserving operative option in unstable Jefferson burst fractures (JBF). Dickman type II transverse atlantal ligament (TAL) lesion is a commonly accepted indication for C1-RO. There is one biomechanical and one clinical report that Dickman type I TAL lesions may also be treated with C1-RO. In 2017, we introduced an intraoperative stability test to assess craniocervical and C1-C2 stability in posterior C1-RO. The objective of this work is to present mid-to longterm results of posterior C1-RO vs C1-C2 stabilization in unstable JBF based on the results of the intaoperative stability test after C1-RO -regardless of Dickman type TAL lesion. Material and Methods: The clinical findings (pain and clinical ability to rotate the head) and radiological results (CT-scan and flexion-extension-views postoperatively and at last observation) of 5 consecutive cases (47-75 years age, mean age 61) with unstable JBF (two Dickman type I, three Dickman type II lesions) from 2017-2019 with posterior C1-RO or C1-C2 osteosynthesis with therapy decision after reduction, C1-RO and intraoperative stability test, were retrospectively analyzed. Results: Surgical procedures were completed as C1-RO in 4 patients, as sufficient stability could be assessed intraoperatively. One C1-RO (a JBF with a Dickman Type II lesion) was converted intraoperatively to a C1-C2 osteosynthesis with a cross connector because of assessment of significant instability C1-C2 in the intraoperative stability test by means of tilting C1 over C2. In all cases of C1-RO, bony stabilization of the atlas ring could be demonstrated during the follow-up period (3.5-21 months postoperatively). No morbidity was observed. The anterior atlanto dental interval (AADI) in the flexion-extension x-ray views did not increase during follow-up period (mean 12 months postoperatively) and all patients were free of significant pain. Therefore, no case with C1-RO had to undergo further surgical stabilization procedure. Conclusion: The intraoperative stability test in treatment of unstable JBF by means of posterior C1-RO with reposition enables the determination of the extent of the surgical procedure. Dickman type I TAL lesions may also be treated with C1-RO, if found stable in the test after lifting up C0 and restoring longitudinal stabilizers, as the assessed intraoperative stability remains. Furthermore, we suggest that any attempted posterior C1-RO in unstable JBF should undergo intraoperative stability testing after initial C1-RO to assess individual resulting stability. Hence we think that the ability to test stability intraoperatively is an advantage of the posterior over the anterior C1-RO.
1807
A306: Isolated C1 Fixation for Traumatic Jeffersons Fractures Using a Novel Surgical Technique
Fahid Rasul 1 , Thomas Doke 1 , Amy Macneil 1 , and Jonathan Bull 1
1 Royal London Hospital, Royal London Hospital, E1 1FR, United Kingdom
Introduction: Isolated C1 fractures are commonly managed non-operatively. Patients report severe neck pain and often treatment involves prolonged use of a hard collar for immobilisation. The traditional operative approach for unstable C1 fractures involved a C1-2 fixation causing significant reduction in patient’s rotational movement of the neck. Here the authors describe their novel technique of C1 fixation and report the clinical outcomes in our cohort of patients. Material and Methods: Retrospective review of prospectively collected electronic database. All patients with a diagnosis of C1 fracture who underwent spinal surgery between January 2017 and July 2020 at Royal London Hospital (RLH) were included. Patient demographics, radiological fracture characteristics, surgical procedure details and clinical outcomes were extracted by case note review. Study methods were compliant with the STROBE checklist. Results: 11 consecutive patients with traumatic C1 fractures underwent surgery using our novel technique at RLH during the study period. Male:Female = 9:2. Mean age = 59.1 years (range 23-84 years). Patient reported neck pain improved significantly following surgery (P = .0008 95% CI = 1.74-4.26; paired t-test). One patient returned to theatre for re-positioning of metalwork. All patients maintained their neurological function post-operatively. Mean length of inpatient hospital stay = 8.25 days (range 1-30 days). Rotational movement was generally well preserved. Conclusion: We report a novel technique of C1 fixation that allows early removal of a collar and effective fracture reduction thereby facilitating fusion. We report good clinical outcomes with patients maintaining functional rotational movement and improvements in pain scores following surgery. Our series suggests that in carefully selected cases isolated C1 fixation may be used to treat traumatic C1 fractures effectively.
OP35: Arthroplasty-Cervical
1032
A307: Preoperative Ossification and Range of Motion were Risk Factors for High-Grade Ossification
Han Wang 1 , and Hao Liu 1
1 West China Hospital, Sichuan University, Department of Orthopaedic Surgery, Chengdu, China
Introduction: Heterotopic ossification (HO) was one of the main postoperative complications following TDR, however, the etiology of HO remains unclear. As we all know, mild HO such as McAfee I or II was considered not clinically relevant, but severe HO which grades III or IV was of great clinical significance. Although it was widely accepted that HO will progress as times goes by, direct studies about risk factors for high-grade HO are still limited. Additionally, the impact of HO on clinical outcomes remains controversial. The present study included the largest sample size among any known HO studies and the objective of this study was to explore the risk factors for HO and high-grade HO, as well as their effect on clinical outcomes. Material and Methods: Overall, 286 patients with TDR or hybrid surgery were involved in the present study. The sex, age, clinical symptoms, surgical procedures, involved levels, follow-up period, preoperative ossifications, and preoperative operative range of motion of replacement level were collected as the potential risk factors for HO. The JOA, NDI, VAS scores and range of motion of replacement levels and the cervical spine were collected to evaluate the impact of HO on clinical outcomes. Preoperative ossifications including (1) ossification of anterior/posterior longitudinal ligament; (2) bubble osteophytes; (3) ROM-limiting osteophytes; (4) ligamentum nuchae ossification. Results: There were 125 patients with single-level TDR, 21 patients with double-level TDR, 72 patients with double-level hybrid surgery and 68 patients with three-level hybrid surgery involved in this study. HO was found in 186 (65.03%) patients while high-grade HO was observed in 26 (9.09%) patients. The preoperative ossification signs (P < .001, OR: 2.991, 95%CI: 1.759-5.085) and ROM of replacement levels (P = .017, OR: .934, 95%CI: .884-.988) were shown to be significant factors of HO occurrence in logistic regression. No significant differences were found in JOA(P = 0.123), NDI(P = 0.925) and VAS(P = .074) scores between patients with and without HO. Although more ROM was found in patients without HO, no statistical differences were found between them at the final follow-up. And the logistic regression showed that the preoperative ossification signs (P = .022, OR: 3.282, 95%CI: 1.183-9.108) and ROM of replacement levels (P = .005, OR: .830, 95%CI: .729-.944) were risk factors for high-grade HO. The ROM of replacement levels in high-grade HO group were significantly lower than those without high-grade HO (3.96° vs 10.06°, P < .001), as well as the ROM of C2-7 (44.44° vs 52.43°, P = .004). Conclusion: Preoperative ossification signs and preoperative ROM of replacement levels were considered as the risk factors of HO and high-grade HO. No differences were observed on clinical outcomes and postoperative ROM between patients with and without HO. However, the ROM of replacement levels and the cervical spine were significantly limited in patients with high-grade HO. The results of this study might provide more evidence that HO is likely a reflection of the patients’ own characteristics rather than an unnatural phenomenon and unpredictable postoperative complication.
1001
A308: Comparison of Two Anterior Hybrid Techniques for Three-Level Cervical Degenerative Disc Disease
Han Wang 1 , Hao Liu 1
1 West China Hospital, Sichuan University, Department of Orthopaedic Surgery, Chengdu, China
Introduction: In recent years, novel hybrid surgery that incorporate anterior cervical discectomy and fusion, and total disc replacement has clinically been widely in use. Based on the number of the implanted disc, three-level hybrid surgery is categorized into two groups including, single fusion combined double replacement (1F2R) and single replacement combined double fusion (1R2F). Previous studies have primarily focused on fusion versus hybrid or replacement versus hybrid. However, limited studies have directly compared the clinical characteristics of different hybrid techniques. Herein, we aimed to compare the clinical and radiological outcomes between the two groups and assess the characteristics and benefits of both operations. Material and Methods: Sixty-four consecutive patients who underwent three-level hybrid surgery by single fusion combined with double replacement or single replacement combined with double fusion were retrospectively evaluated. The clinical outcomes such as VAS, JOA score, and JOA recovery rate was collected. And radiological evaluation including range of motion and cervical lordosis were analyzed. Heterotopic ossification was assessed according to the McAfee classification and dysphagia was quantified using Bazaz scoring system. The reoperation rate and other complications were all collected. Results: In total, 32 patients were involved in 1F2R group and 32 patients in 1R2F group, and all the patients had a satisfactory clinical outcome. The JOA recovery rate of 1F2R and 1R2F group was 76.47% and 76.09%, respectively. And no significant differences were observed on VAS scores between two groups at the last follow-up. The C2-7 cervical lordosis was similar between two groups at the last follow-up, however, there was a statistical difference in the 1R2F group when compared to the preoperative level (pre 6.48° vs last 10.12°, P = .003). The range of motion decreased in both two groups, but 1F2R group showed a better range of motion at the final follow-up (38.25° vs 29.17°, P = .001). Heterotopic ossification was observed in 10 segments (15.63%) in 1F2R group and 17 levels (53.13%) in 1R2F group, but severe heterotopic ossification was only observed in 2 and 1 patients in 1F2R and 1R2F group, respectively. Additionally, one patient underwent the re-operation for the fourth level in 1F2R group and no spinal cord injury, wound infection or hoarseness were observed. Conclusion: This study indicated that the two kinds of hybrid surgery incorporating fusion and non-fusion are safe and effective in the treatment of three-level CDDD. The 1R2F operation was better in correcting the cervical lordosis irrespective of higher incidence of HO. On the other hand, 1F2R operation was superior in maintaining cervical ROM. However, the biomechanical characteristics for different HS were complex. Therefore, further randomized controlled studies on HS groups are indispensable.
287
A309: The Impact of Physical Therapy After Cervical Spine Surgery for Degenerative Spine Disorders: A Systematic Review
Justin M. Lantz 1 , Aidin Abedi 2 , Frances Tran 1 , Rafael Cahill 1 , Kornelia Kulig 1 , Lori Michener 1 , Raymond Hah 2 , Jeffrey C. Wang 2 , and Zorica Buser 2
1 University of Southern California, Division of Biokinesiology and Physical Therapy, Los Angeles, USA
2 University of Southern California, Department of Orthopedic Surgery, USC Spine Center, Los Angeles, USA
Introduction: Cervical spondylosis is a chronic degenerative disorder affecting both the discs and joints of the cervical spine which can result in a combination of neck pain, cervical radiculopathy, and/or cervical myelopathy. Once symptoms become recalcitrant to conservative management or there is progressive deterioration of neurological status, surgical intervention may be indicated. There is paucity of evidence concerning post-operative management of these patients, specifically the use of physical therapy (PT). Physical function deficits can be present up to 14 years after cervical surgery. It is important to determine if the literature indicates a need for post-operative PT, that may improve patient outcomes and decrease healthcare costs. The aim of this systematic review was to identify the impact of PT after cervical spine surgeries regarding complications, patient-reported outcomes (PROs), physical function and cost-effectiveness. Material and Methods: The following bibliographic databases were searched electronically from the date of inception until July 2019: PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Physiotherapy Evidence Database (PEDro), and the Web of Science. Four reviewers independently reviewed the titles, abstracts and full texts of identified records based on the eligibility criteria. Inclusion criteria: peer-reviewed, English language, at least ten adult patients (diagnosed with degenerative spine disorders) who had undergone cervical spine surgery with post-operative PT. Exclusion criteria: poorly defined surgical/PT protocols, outcome measures, trauma, cancer or infection. The Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) assessed risk of bias. Meta-analysis was not performed due to study heterogeneity and limited data for comparisons. The findings were described narratively and the GRADE approach was used to define the certainty of evidence. Results: 10,743 studies were screened on the title and/or abstract level. Twenty studies were selected for full-text review and six studies met the inclusion criteria, including two randomized controlled trials (RCTs) None of the RCTs or longitudinal studies had a lone surgical comparator group. Both RCTs were at moderate risk of bias overall. Methodological concerns included potential for bias in the outcome measurement and lack of blinded assessment for PROs. RCTs included 63 and 201 patients with cervical radiculopathy. Surgeries included 1-3 level anterior cervical discectomy and fusion or posterior foraminotomy with or without laminectomy. Post-operative PT consisted of exercise, cognitive behavioral therapy and optional vestibular rehabilitation. PROs: studies demonstrated reduction in Neck Disability Index, Visual Analog Scale for pain and improvement in the Global Assessment, EuroQol-5D, and Modified Odom Scale. Physical function: studies demonstrated improvement in cervical active range of motion, manual dexterity, hand strength, and neck muscle endurance. Between-group comparisons were generally insignificant. No studies reported complications, adverse events or cost-effectiveness relating to PT with or without surgery. Conclusion: PT after cervical surgery for spondylosis appears to be tolerated without notable adverse effects and may lead to improvements in pain, disability, and physical function. However, due to limited availability of studies, heterogeneity in study design and lack of lone surgical control groups in current literature, it is difficult to determine the true effect of the addition post-operative PT to cervical surgery.
1358
A310: Assessment of the Self-Reported Dysphagia in Patients Undergoing One-Level Versus Two-Level Cervical Disc Replacement with the Prestige-LP Prosthesis
Haimiti Abudouaini 1 and Hao Liu 1
1 West China Hospital, Sichuan University, Orthopedics, Chengdu, China
Introduction: Incidences of dysphagia in cervical disc replacement (CDR) are lower than those reported in anterior cervical discectomy and fusion (ACDF). Surgical CDR is has a clinical importance due to its complicated outcomes. It has been documented that surgery may lead to high dysphagia rates in ACDF. There is paucity of documented information on the differences in post-operative dysphagia of CDR between one-level and two-level CDR. This paucity, therefore, necessitated this retrospective study on post-operative dysphagia after one- and two-level CDR. Material and Methods: The prevalence and severity of post-operative dysphagia between one-level and two-level CDR was evaluated by the Bazaz grading system during the follow-up time. Regression analyses were done to identify confounding factors associated with post-operative dysphagia after CDR. Results: One hundred and fourteen patients in one-level CDR group and forty eight patients in two-level CDR group were recruited. The overall dysphagia occurrences in the one- and two-level CDR groups were 17.54% and 35.41% at week one, 12.28% and 25% after one month, 9.65% and 18.75% after three months, 6.14% and 14.58% after six months, 4.39% and 6.25% after one year, and 3.51% and 4.17% at the final follow-up, respectively. The identified risk factors for dysphagia after CDR were advanced age, C4/5 surgery, two-level surgery, dC2-C7 angle ≥ -5° and ≥ 6 mm changes in the prevertebral soft tissue swelling (dPSTS). Conclusion: It was revealed that patients who experienced two-level CDR may have weak swallowing functions in the early post-operative term. However, after mid-to-long-term follow-ups, these patients exhibited better improvements in post -operative swallowing compared to those who had undergone one-level CDR.
1968
A311: Management of Cervical Spondylotic Myelopathy with Total Cervical Disc Replacement: Analysis of Patients with Clinical and Radiological Signs of Cervical Myelopathy
Christoph Mehren 1 , Franziska Heider 2 , and Tuna Pehlivanoglu 3
1 Schön Klinik München Harlaching, Spine Center, Munich, Germany
2 Schön Klinik München Harlaching, Spine Center, München, Germany
3 Sağlık Bilimleri Universitesi Istanbul, Istanbul, Turkey
Introduction: Over the past decade, total cervical disc replacement (cTDR) has been established as a viable treatment option for cervical degenerative disc disease. Especially patients with radiculopathy due to certain disc pathologies have been treated successfully with excellent clinical long-term results in the past. The aim of this study was to question the clinical and radiographic efficacy of Pro Disc Vivo cervical disc arthroplasty in patients with clinically and radiographically documented myelopathy due to degenerative changes at the index level. Material and Methods: 18 consecutive patients (10 males, 8 females) with documented clinical and radiological signs of myelopathy, as part of an ongoing prospective non-randomized single center study, were included in this investigation. All of the patients underwent the same procedure through an anterior cervical approach and a ProDisc Vivo cervical disc prosthesis was inserted within strict inclusion criterias (e.g. no instability, no kyphotic deformity, residual motion of the index segment, no distinct bony osteophytes, no osteoporosis). MRIs were taken routinely to confirm the diagnosis of spinal stenosis with myelopathy. Conventional x-rays of the cervical spine were taken in ap and lateral as well as in flexion/extention to determine the global lordosis as well as the range of motion (ROM). Patients without radiographic (MRI) evidence of myelopathy were excluded. Enrolled patients were calculated Nurick grade together with VAS, NDI and JOA scores preoperatively and also during the follow-up appointments. Results: The study population had a mean age of 52.4 years and a follow up period of 20.3 months in average(range 3-48 months). Cervical disc arthroplasty was performed in 15 patients for one, in 2 patients for two and one patient for three levels. The mean range ROM of the index level stayed consistent with 9.4° preoperatively and 9.6° (P = .637) at the last follow up, the global lordosis in neutral position changed from 5.8° to 14.2° significantly (P = .002). The JOA score improved from 11.3 (Grade I: 9 patients, Grade II: 9 patients) to 16.62 (all patients: Grade I) (P < .001/P = .003) as well as the NDI 36.71 (73.43%) to 10.3 (P < .001) and the VAS score from 5.71/6.07 (arm/neck) to 1.3/2.0 (P < .001/P < .001). The mean Nurick grade was 1.33 pre-operatively and dropped down in all cases to Nurick grade of 0 (P < .001). At the latest follow-up visit all patients were highly satisfied by means of social functioning and pain. They were all able to return to work, daily activities and recreational sports. Conclusion: This study proved that Pro Disc Vivo cervical disc arthroplasty was a viable treatment option with excellent outcomes even in management of cervical myelopathy with regard to pain scores (VAS) and neck disability index by improving the neurologic deficit, arm pain and local neck symptoms together with scores of functional outcome (JOA and NDI scores). Considering the Nurick grades our clinical results revealed that, anterior decompression and implantation of cTDR could improve the severity of myelopathy within strict inclusion criterias as well. This study also concluded that cTDR was improving the pre-operative ROM and lordosis with great statistical significance.
References
1. Kim YJ, Bridwell KH, Lenke LG, et al. Pseudarthrosis in primary fusions for adult idiopathic scoliosis: incidence, risk factors, and outcome analysis. Spine. 2005; 30: 468-474.
2. Shaffer AD, Shonuga OA, Hirsch BP, et al. Sclerostin antibody enhances spine fusion in a rat posterolateral transverse process fusion model: preliminary results. Proc 33rd Annual Meeting of the American Society for Bone and Mineral Research, San Diego, CA, 2011, p S517 (Abstract MO0461).
3. Boden SD, Schimandle JH, Hutton WC. An experimental lumbar intertransverse process spinal fusion model. Radiographic, histologic, and biomechanical healing characteristics. Spine (Phila Pa 1976). 1995 Feb 15;20(4):412-20.
1119
A312: Effect of Changes in Postoperative Intervertebral Space Height on Clinical and Radiological Outcomes After Cervical Disc Replacement
Haimiti Abudouaini 1 and Hao Liu 1
1 West China Hospital, Sichuan University, Orthopedics, Chengdu, China
Introduction: Narrowing of intervertebral space height (ISH) is an important pathological change in degenerative spinal disease, and ideal intraoperative distraction and postoperative intervertebral space maintenance is one of the most expectant goals pursued by spinal surgeons. It has been reported that the distraction of intervertebral space height has a close association with axial symptoms, adjacent segment degeneration, and neurologic recovery after cervical surgery. However, compared with cervical intervertebral space distraction, which has received considerable attention in previous studies, limited studies analyse the relationship between the maintenance of ISH and clinical and radiological outcomes after CDR. Material and Methods: In this study, the height variation and general trend of postoperative ISH in all patients were analysed. The patients were divided into three groups based on the change of postoperative intervertebral space height (ISH); group A (ISH < 2 mm), group B (ISH 2-4 mm), and group C (ISH >4mm) and the clinical and radiographic results compared among the three groups. A total of 120 consecutive patients with symptomatic cervical disc disease were included in this study. Results: The results showed that the mean ISH increased significantly from 0.729 mm before surgery to 1.143 mm at one week, then gradually decreased to 1.032 mm at three months, 0.980 mm at six months, 0.760 mm at one year, and 0.750 mm at the final follow-up. The average postoperative Neck Disability Index (NDI) was 19.73 ± 0.81, 13.74 ± 4.94, 17.19 ± 4.22 in the three groups at one year after surgery and the average range of motion (ROM) was 5.44 ± 3.85° in group A, 9.34 ± 4.38° in group B and 6.51 ± 4.38° in group C. The mean diameter of the intervertebral foramen (IVF) was 6.54 ± 1.86 mm in group A, 9.63 ± 2.38 mm in group B and 9.31 ± .68 mm in group C. Degeneration at the superiorly adjacent disc level was observed in 13.51% patients in group A, 9.37% in group B and 21.05% in group C. Degeneration at the inferiorly adjacent level was radiographically identified in 21.62% in group A, 14.06% in group B, and 26.32% in group C. Conclusion: This study revealed that cervical disc replacement cannot maintain the intervertebral disc height obtained immediately after surgery. There is no obvious correlation between the change in intervertebral space height and clinical efficacy in the early postoperative stage. However, the intervertebral disc height may affect the NDI index one year after surgery. If the postoperative intervertebral space height change can be maintained at 2-4 mm in a year, satisfactory ROM, intervertebral foramen diameter, and relatively low ASD may be obtained after cervical disc replacement.t
1026
A313: Effect of disc height and degree of distraction on heterotopic ossification after cervical disc replacement
Xiaofei Wang 1 , Han Wang 1 , and Hao Liu 1
1 West China Hospital, Sichuan University, Department of Orthopaedic Surgery, Chengdu, China
Introduction: Heterotopic ossification (HO) is a potential and severe complication of cervical disc replacement (CDR). However, the underlying mechanism of CDR and its association with preoperative disc height loss (DHL) and postoperative degree of distraction (PDD) remain unclear. We hypothesized that DHL and PDD could predict HO after CDR. Material and Methods: Data were obtained from 127 patients who underwent single-level CDR with a minimum follow up of two years. DHL and PDD were obtained from lateral radiographs and HO was evaluated at the last follow up appointment. Receiver operating characteristic (ROC) curves were calculated to verify the diagnostic value of DHL and PDD in predicting HO. Results: Both DHL and PDD were significantly larger in the HO group than the non-HO group (P < .05). DHL ≥ 24.97% increased the risk of HO by 5 times (P = .003, 95% CI: 1.62-15.49), and PDD ≥ 36.67% increased the risk of HO by 3.87 times (P < .001, 95% CI: 1.81-8.27). A combined DHL and PDD (combined parameter) cut-off of 60.36 had a sensitivity of 87.18%, specificity of 67.35%, and area under the curve of 0.77 for predicting HO. Conclusion: DHL and PDD are associated with the development of HO after CDR. The cut-off value of DHL may narrow criteria for CDR with the aim of reducing HO formation. The combined parameter may help surgeons to select the most suitable implant height to reduce the prevalence of HO.
1356
A314: Outcomes Following Cervical Disc Replacement vs Anterior Cervical Discectomy and Fusion in Patients with Predominantly Neck Pain Complaints
Andre Samuel 1 , Catherine Himo Gang 1 , and Sheeraz Qureshi 1
1 Hospital for Special Surgery, New York, USA
Introduction: Although cervical disc replacement (CDR) continues to increase in popularity for the treatment of cervical radiculopathy, the presence of preoperative neck pain is often cited by surgeons as a reason for choosing anterior cervical discectomy and fusion (ACDF) instead.1 The origin of neck pain is often multifactorial and there is some literature that suggests comparable results between CDR and ACDF in patients who have both neck pain and upper extremity radiculopathy.2-5 The purpose of our study was to compare outcomes between CDR and ACDF in patients who presented with predominantly neck pain complaints. Methods: A retrospective review of prospectively collected data was performed on patients undergoing one or two-level CDR or ACDF by three surgeons at a single academic institution. Patients who had presented with predominant complaints of neck pain (pNP; VAS-neck>VAS-arm) were initially identified and subsequently stratified into two cohorts by procedure: CDR (n = 41) and ACDF (n = 83). Outcome data was collected at preoperative visits and at each of the following postoperative visits: 2 weeks, 6 weeks, 12 weeks, 6 months, 1 year, and 2 years. The following MCID-threshold values were used, based on previous studies in the literature: NDI: -15.0, VAS-Neck: -2.5, VAS-Arm: -2.5, SF-12: PCS +8.1, SF-12 MCS: +4.6. Differences in PROMs were analyzed with Wilcoxon-Signed-Ranks-Tests within each cohort and Mann-Whitney-U-Tests to compare PROMs between groups. Rates of MCID achievement were analyzed for each PROM with Fischer’s-Exact-Tests. Results: 124 total patients presenting with pNP were included (mean age: 49.93 ± 11.73 years, mean BMI: 26.65 ± 4.05 kg/m2). In those with minimum six-month follow-up, both the CDR (median follow-up: 336.5 days) and ACDF (median follow-up: 336.5 days) cohorts demonstrated significant improvements in NDI (P < .001), VAS-neck (P < .001), and SF-12 PCS (P < .001). While both cohorts demonstrated improvements postoperatively in these three PROMs, the degree of improvement was not significantly different between the two cohorts in any PROM (all P ≥ .185). In addition, the CDR cohort demonstrated significant improvement in SF-MCS (P = .022). There were no significant differences in any of the final PROMs (all P ≥ .320) between CDR and ACDF patients with a minimum six-month follow-up. When comparing cumulative percentages of patients achieving MCID at each post-operative time point, no significant differences were observed between the two cohorts at any time point (all P ≥0.236) with 90.2% (n = 37) of CDR patients and 84.1% (n = 69) of ACDF patients achieving MCID in ≥1 PROM by the 2-year follow-up. Discussion and Conclusion: Historically, surgeons have favored ACDF in patients presenting with a primary complaint of neck pain in the setting of cervical radiculopathy. While the presence of neck pain and significant radiographic facet arthritis should continue to be a contraindication to CDR, our findings suggest that disc replacement may be a viable surgical option in an appropriately indicated subset of patients who present with a predominant.
1018
A315: Cervical Sagittal Alignment After Prestige Lp Cervical Disc Replacement: Radiological Results and Clinical Impacts
Xiaofei Wang 1 , Han Wang 1 , and Hao Liu 1
1 West China Hospital, Sichuan University, Department of Orthopaedic Surgery, Chengdu, China
Introduction: Cervical disc replacement (CDR) has been widely used to treat one- and two-level cervical degenerative disc disease. Studies have shown the effectiveness of CDR in preserving range of motion (ROM) and delaying adjacent segment degeneration (ASD). Cervical sagittal alignment is an important factor affecting favorable clinical outcomes in cervical spine surgery. This study aimed to explore whether cervical sagittal alignment can be maintained after CDR and to identify the impact of cervical sagittal alignment on outcomes after CDR. Material and Methods: This was a single-center, retrospective study. 132 patients who underwent one-level CDR were included. Cervical sagittal alignments, including cervical lordosis (CL), segmental alignment (SA), sagittal vertical axis (SVA), T1 slope (T1s), and T1s minus CL (T1s-CL), were measured. The effects of cervical sagittal alignment on the CDR outcomes were analyzed. Patients were divided into the heterotopic ossification (HO) group and ASD group to determine the potential impacts of cervical sagittal parameters. Results: The cervical sagittal alignment parameters, except for the SVA, were significantly improved after CDR and showed decreasing trends at the last follow-up. Significantly higher CL and T1s were found in patients with better ROM after CDR. SVA ≥ 20 mm increased the risk of anterior HO (odds ratio = 2.945, P = .007). Significantly kyphotic SA and lower T1s values were found in the ASD patients than in the non-ASD patients (P < .05). Patients with ASD at the inferior level showed significantly worse CL (P < .05). Conclusion: CDR had limited function of improving cervical sagittal alignment. Poor cervical sagittal alignment after CDR was associated with HO, ASD, and less ROM.
OP36: Spinal Tumor Surgery 2
597
A316: Analysis of unplanned hospital readmissions up to two-years after metastatic spine tumour surgery
Andrew Thomas 1 , Sirisha Madhu 1 , Miguel Rafael Ramos 1 , Liang Shen 2 , Yong Hao Joel Tan 3 , and Naresh Kumar 3
1 National University Health System, Singapore, Singapore
2 National University of Singapore, Biostatistics unit, Singapore, Singapore
1 National University Health System, Singapore, Singapore
Introduction: Unplanned hospital readmissions (UHR) after discharge following metastatic spine tumour surgery(MSTS) adversely affect quality of life of these patients. Majority of studies on UHR focus on assessment of readmissions within 30 days following index-discharge. The aim of this study was to investigate rates, causes, and risk factors of UHR within 30 days, 90 days, 1 year and 2 years after MSTS to augment multi-disciplinary treatment planning and improve patient education. Materials and Methods: We retrospectively reviewed 272-patients (age ≥18 years) who underwent MSTS between 2005-2016 with a follow-up for minimum two-years or until their demise, whichever was earlier. Institutional review board approval was obtained prior to commencement of study. Hospital records were utilised to obtain demographics, oncological and procedural details, and postoperative outcomes. All UHR within 2years were reviewed. UHR were defined as unscheduled hospitalisations after index-discharge and did not include planned follow-up/readmissions for radiotherapy/chemotherapy. Primary outcomes were rates and causes of UHR. Four-time frames were considered with regards to UHR: (1 < 30 days, (2) 30-90 days, (3) 90days-1year, and (4) 1-2years. UHR rate was calculated as number of patients being readmitted divided by total number of surviving patients within each timeframe. Risk factors for UHR were evaluated using multivariate logistic regression analysis. Results: A total of 204-patients were included in the final analysis. The mean age was 60+12 years; 49% were females. An Eastern Cooperative Oncology Group Performance Status (ECOG-PS) score of 0-2 was noted in 88% of patients. Median Charlson Comorbidity Index (CCI) and Tokuhashi scores were 7 and 8, respectively. Most common primary tumour type was lung (24.5%), followed by breast (19.1%). Majority underwent open surgery (72.1%). Overall, perioperative complication rate was 46%. A total of 425-UHR occurred across all four studied timeframes in 151-patients. Thirty-day, 90-day, 1year, and 2year UHR-rates after MSTS were 17.2%, 31.1%, 46.2%, and 52.7%, respectively. Majority of patients had their first UHR between 30-90days (32.5%). The highest number of readmission-events occurred after one year from discharge (n =153/425). Lung cancer primaries had the highest UHR-events (24.7%) whilst renal/thyroid displayed the least (6.6%). Disease-related causes (16.2%) were the most common reason for readmissions across all timeframes, followed by respiratory (13.7%) and progression of metastatic spine disease (12.7%). Urological conditions accounted for majority of readmissions within 30days (25%); disease-related causes (27.9%), symptomatic spinal metastases (16.7%), and respiratory conditions (19.6%) represented the most common causes at 30-90 days, 90 days-1year, and 1-2 years, respectively. An ECOG >1 (P = 0.057), CCI >7 (P = .01), and primary lung tumour (P = .02) significantly increased UHR-risk on multivariate analysis. Conclusion: Our study findings offer useful insights into UHR during the overlooked timeframe of beyond 90days. Overall, 74% of patients had at least one UHR within 2years of MSTS and majority were secondary to disease-related causes. Majority of first UHR occurred between 30-90 days after surgery. Local disease progression and overall disease progression accounted for the highest UHR-events at 90 days-1 year and 1-2 year timeframes, respectively. This information allows clinicians to anticipate causes of UHR within specific timeframes, thereby enabling better surveillance and prevention of MSTS-related morbidity.
736
A317: Symptomatic Ventriculus Terminalis in a 64-Year-Old Female: A Case Report
Mahmoud Ben Messaoud 1 , Kais Maamri 1 , Nessrine Nessib 1 , Mohamed Boukhit 1 , ines cherif 1 , Maher Hadhri 1 , Souheil Khalfaoui 1 , Atef Ben Nsir 1 ,and Mehdi Darmoul 1
1 Neurosurgery department, Fattouma Bourguiba University Hospital, Monastir, Tunisia
Introduction: Ventriculus terminalis (VT) or the "fifth" ventricle is an embryological remnant consisting of an ependyma-lined cavity located in the conus medullaris. VT is extremely rare in adults and asymptomatic in the vast majority of cases; but may occasionally become symptomatic if cystic dilation occurs. Surgical treatment is still matter of debate. Material and Methods: We report a case of 64-year-old female. Results: We report the case of a 64-year-old female, who was referred to our department with a 6 months history of sphincter dysfunction made of urinary incontinence and chronic constipation. On physical examination, muscle strength was normal in both lower limbs, deep tendon reflexes were weak with bilateral Babinski sign. Magnetic resonance imaging (MRI) of the spine showed a cystic lesion at D10-D12. (length: 4 cm; volume 4.5 cm3) similar to CSF in both T1 and T2-weighted images with no contrast enhancement which then was reported as VT. This lesion was associated to a 3 mm large hydromyelia extending from D2 to D8. Decision was to address the VT with posterior approach, D9-D12 laminectomy, myelotomy and cyst fenestration. Post-operative course was uneventful and the patient was discharged three days following surgery. Six-months control MRI showed significant cyst size reduction and a marked improvement in sphincter dysfunction was noted starting 9 months after surgery. Conclusion: Microsurgical fenestration is a safe and effective treatment strategy for symptomatic VT and can be associated with a good clinical outcome even in elderly patient.
1367
A318: Clinical Outcomes in 91 Patients Treated with Hybrid Spinal Surgery for Metastatic Renal Cell Carcinoma
Ibrahim Hussain 1 , Jacob Goldberg 1 , Joseph Carnevale 1 , Samuel Hanz 2 , Anne Reiner 1 , Yoshiya Yamada 1 , Ilya Laufer 1 , Mark Bilsky 1 , and Ori Barzilai 1
1 Memorial Sloan Kettering Cancer Center, New York, USA
2 Weill Cornell Brain and Spine Center, New York, USA
Introduction: The management of renal cell carcinoma (RCC) spinal metastases is controversial in regards to extent of resection and adjuvant radiation dosing. We present outcomes of patients with RCC spinal metastases treated by hybrid spinal surgery which consists of an initial posterior transpedicular approach for circumferential decompression of the neural elements plus instrumented stabilization, followed by adjuvant radiation therapy. Methods: A retrospective study of a prospectively collected cohort of patients undergoing hybrid surgery for pathology-proven spinal metastases from renal cell carcinoma between 2003 and 2017 was performed. Radiation therapy was either single fraction, hypofractionated with high dose per fraction, or hypofractionated with low-dose per fraction. Patient demographic, clinical, and surgical data were collected. The degree of systemic disease was at time of surgery was divided into solitary metastasis, oligometastatic disease (2-5 metastatic lesions regardless of organ system involved), or widespread metastatic disease (greater than 5 metastatic lesions regardless of organ system involved). Complications were divided into major and minor complications, with major complications requiring invasive measures or those resulting in permanent disability or death. Results: A total of 91 patients were included (84% male). Median age was 62.2 years old. 89% involved the thoracolumbar spine. 56% of patients had widespread disease, 33% had oligometastatic disease, and 11% had a solitary metastasis. Median operative time and blood loss were 162 minutes and 1000 mL, respectively. 25 patients received SRS in a single fraction. 56% of patients had hypofractionated PORT with high-dose per fraction (3 fractions with 800-900 cGy per fraction). 15 patients had hypofractionated with low-dose per fraction (5 fractions with 600-900 cGy per fraction). 16 patients had complications related to treatment, of which 11 were major. The median length of stay was 5 days and 87% of patients were discharged home. There was an overall 92% PFS rate. The median time to POD requiring treatment was 422 days. At 12-month follow-up, 44% of patients had died, with 44% demonstrating ECOG scores ranging from 0-2. The mean overall survival for the cohort was 686 days. For patients still alive, median time to last follow-up was 1163 days. For patients that died during the study, mean survival was 543 days. When stratifying patients by degree of systemic disease, there was an expected increased risk of death (1.09x) and progression (1.21x) with widespread disease. Patients with a solitary metastasis received a higher median dose of PORT (2850 cGy). Patients with oligometastatic disease were 11% less likely to die and 9% less likely to progress than patients with a solitary metastasis. There was increasing risk of POD with hypofractionated regimens (1.5x for high-dose, and 5x with low-dose). Conclusion: Patients treated with hybrid spinal surgery for metastatic RCC demonstrate a PFS rate of 92%, mean OS of 686 days, and 12% risk of major complications. The median time to POD requiring treatment was 422 days. There was a 1.5-5x increased risk for POD with for hypofractionated regimens. Patients with widespread disease at the time of surgery had a 1.1-1.2x increased risk for POD and death.
723
A319: Neurological Outcome and Respiratory Insufficiency in Intramedullary Tumors of the Cervical Spine
Vicki Butenschön 1 , Jens Gempt 1 , Bernhard Meyer 1 , and Maria Wostrack 1
1 Technical University Munich, Department of Neurosurgery, Munich, Germany
Objective: Intramedullary tumors of the upper cervical spine are challenging entities with a high risk of postoperative neurological deterioration. As the levels above C4 are responsible for volitional ventilatory control, patients are at risk of permanent respiratory dysfunction with the need of long-term ventilation. Methods: We retrospectively reviewed all patients treated for intramedullary lesions including the upper cervical spinal cord above the C4 level in our neurosurgical department from January 2008-December 2019. Patient’s demographics, pre- and postoperative clinical status as well as operative technique and complications were extracted and analyzed. Results: In total, 34 patients underwent a surgical treatment for intramedullary lesions including or above the C4 level from 2008 to 2019. Median age was 44 years, and 56% of the patients were male. The most common entity was ependymoma (n: 22, all WHO II), 7 patients were treated for intramedullary glioma (WHO I-IV) and 5 patients for a hemangioblastoma. In total, 22 patients presented with neurological deficits preoperatively (65%). Respiratory dysfunction was observed in only one patient requiring tracheotomy (2.9%). Postoperative neurological worsening was observed in 56% (motor function deterioration in 35% of the cases, sensory deficits in 50%), but the majority of patients recovered, and was independent at follow-up (median McCormick grade 2, 76.7% of the cases with McCormick grade 1 or 2). Conclusions: Intramedullary tumors of the upper cervical spine remain challenging neurosurgical entities. Despite its high-risk location, respiratory insufficiency seems to remain a rather are complication, while transient postoperative neurological deterioration is observed in more than half of the cases.
1750
A320: Apolipoprotein E4 (rs429358) Variant Genotype: A Risk Gene Associated with Higher Serum Lipid Profile and Spine-Related Neck or Back Pain
Nicholas Van Halm-Lutterodt 1,2 , Krishna Mandalia 2,3 , Ziyang Ye 4.5 , Wei-Cheng Chen 6 , Mohamed Kamal Mesregah 2 , Brandon Yoshida 2 , Andrew Mecum 7 , Wei-Hsun Huang 1 , Wenxin Lei 8 , Mercy Bartels-Mensah 9 , Yu Wang 1 , and Yulun Xu 1
1 Beijing Tiantan Hospital, Department of Neurosurgery, Beijing, China
2 Keck Medical Center of University of Southern California (USC), Department of Orthopaedics and Neurosurgery, Los Angeles, USA
3 University of Southern California, Dornsife College of Letters, Arts and Sciences, Los Angeles, USA
4 Wake Forest University, Department of Mathematics and Statistics, Winston-Salem, USA
5 University of Chicago Graham School of Continuing Liberal and Professional Studies, University of Chicago, Department of Business and Analytics, Chicago, USA
6 Beijing Tongren Hospital, Department of Clinical Sciences, Beijing, China
7 Emory University, Department of Psychology, Atlanta, USA
8 Melbourne University, Department of Mental Health Nursing, Parkville, Australia
9 University of Debrecen, Department of Clinical Sciences, Debrecen, Hungary
Introduction: The apolipoprotein E (ApoE) gene that is implicated in regulating serum metabolic and lipid species is also reportedly associated with vertebral column and neurological degeneration. Increasing ApoE genetic polymorphic studies indicate that the wild-type (WT) genotypes of apolipoproteins Eε2 and Eε4 specifically hold metabolic health and risk gene properties, respectively. Nevertheless, as to whether their variant (VT) genotypes carry the same functional properties in the transportation and regulation of serum lipids in spine patient outcomes remain elusive. To this end, we evaluated the relationship(s) between WTs and VTs of ApoEε2 and ApoEε4 genotypes on serum lipid profile as well as the associated clinical outcomes in spine patients perioperatively. Materials and Methods: Following approval by the institutional review board (IRB) of Beijing Tiantan Hospital-Affiliated Capital Medical University, a prospective clinical study of 336 adult (≥18 years) intradural spinal cord tumor (ID-SCT) patients who underwent surgical treatment without any prior primary therapy were assessed. Patients within each ApoE2 and ApoE4 categories were then dichotomized into homozygosity-wild type (WT) and heterozygosity-variant type (VT). We compared patient outcomes of ApoEε2-(rs7412) [WT ( C/C )] versus ApoEε4-(rs429358) [WT ( T/T )] and ApoEε2-(rs7412) [VT ( C/T )] versus ApoEε4-(rs429358) [VT ( C/T )]. The impact of WT and VT genotypes on serum metabolic and lipid profiles associated with perioperative clinical outcomes were evaluated. Key primary outcomes comprised of demographics, daily dietary outcomes, and serum metabolic panel. Secondary outcomes compared neurological and PROs between the genotypes at baseline and at 2-year postoperative for patient self-reported outcomes that included: visual analogue scale (VAS), Neck Disability and Oswestry Disability Indices (NDI or ODI), Chinese national daily foods frequency questionnaire (FFQ). Functional measures included: McCormick’s classification and the RAND-36 [Short-Form 36 (SF-36)] health-related quality of life (HRQoL) assessment. Laboratory measures included: Serum glucose, lipids, and protein profiles. Univariate and multivariate analyses were carried out by student t-test, Pearson’s Chi-squared test, Mann-Whitney U test and general linear model (GLM), respectively, with age, gender, body mass index (BMI), and multivitamin intake considered as covariates. Statistical significance was set at (P < .05). Results: Of the 336 ID-SCT patients, approximately 85.4% vs 81.2% were ApoEε2-(rs7412)-WT vs ApoEε4-(rs429358)-WT and 14.6% vs 18.8% were ApoEε2-(rs7412)-VT vs ApoEε4-(rs429358)-VT carriers, respectively. At baseline, the ApoEε4-(rs429358)-VT carriers showed significantly higher average serum total cholesterol (TC), low-density lipoprotein (LDL-c), LDL-c/HDL-c ratio, cholesterol ratio (CR), and apolipoprotein B (Apo-B) than ApoEε2-(rs7412)-VT carriers. The ApoEε4-(rs429358)-VT carriers also demonstrated 390% increase in Neck or Back Pain incidence and 390% increased Neck or Back Pain intensity compared to the ApoEε2-(rs7412)-VT carriers at baseline (P < .05). Conclusion: Findings from this study indicate that the WTs of both ApoEε2 and ApoEε4 genotypes were potentially comparable at regulating serum lipid species. ApoEε4-(rs429358)-VT genotype was a risk gene and associated with potential lipid-induced systemic inflammation and significantly increased neck or back pain incidence and intensity preoperatively. Further studies are encouraged to assess how the ApoEε4-(rs429358)-VT genotype impacts preoperative prescriptions of pain medications including opioids and to extrapolate the potential impact(s) of this gene is affecting opioid dependency and crisis following surgical treatment in spine patients.
614
A321: Responder-analysis of pain relief after surgery for the treatment of spinal metastatic tumors
Robert Rothrock1,2,3, Anne Reiner4, Ori Barzilai2, Shahiba Ogilvie2, Eric Lis5, Yoshiya Yamada6, Mark Bilsky2, and Ilya Laufer2
1 Mount Sinai Icahn School of Medicine, Neurosurgery, New York City, USA
2 Memorial Sloan Kettering Cancer Center, Neurosurgery, New York City, USA
3 University of Miami Miller School of Medicine, Neurosurgery, Miami, USA
4 Memorial Sloan Kettering Cancer Center, Biostatistics, New York City, USA
5 Memorial Sloan Kettering Cancer Center, Radiology, New York City, USA
6 Memorial Sloan Kettering Cancer Center, Radiation Oncology, New York City, USA
Introduction: The current analysis focused on the patient pain experience after surgery for the treatment of spinal metastatic tumors. Responder analysis was carried out to capture patient-level pain experience and to study the variability of pain improvement. Materials and Methods: The patient population included 174 patients who underwent surgery for the treatment of metastatic spine tumors. Brief Pain Inventory (BPI) and MD Anderson Symptom Inventory-Spine Tumor (MDASI-SP) instruments were used to measure patient reported outcomes. Logistic regression modeling was used to associate preoperative characteristics with “treatment success” defined as rating the BPI worst pain item 0-4. Linear regression modeling was used to associate preoperative characteristics with minimal clinically important improvement (MCI) in physical functioning defined by distribution as a one-point decrease in the BPI Interference Construct score from preoperative (baseline) to 6 months postop. Results: Patient-level analysis of pain response revealed that 60% of patients experienced at least a minimally important decrease in pain. At least one-third of the patients experienced a substantial reduction in pain and twelve percent experienced complete resolution of pain. At least half of the patients experienced a decrease in pain sufficient to result in minimal clinically important improvement in physical functioning, evidenced by a 1-point decrease in the BPI Pain Interference construct. Cutpoint analysis revealed that 48-49% were classified as responders based on the change from more severe to less severe pain categories in the Worst Pain BPI and Average Pain BPI items and BPI Pain Severity Construct. Increasing scores on all of the preoperative pain intensity BPI items, the MDASI Core Symptom Severity, the MDASI Spine Tumor Specific Construct and the presence of preoperative neurologic deficits were associated with lower probability of pain treatment success. Postoperative complications were also associated with decreased probability of pain treatment success. On the other hand, increasing severity in all BPI pain items and MDASI constructs was associated with increased probability of a minimal clinically important improvement in physical function. Conclusions: The current analysis confirms that a significant proportion of patients experience significant and clinically important pain relief after surgery for the treatment of spinal metastatic tumors. Patients with milder preoperative symptoms are more likely to reach a “low pain” or pain treatment success outcome after surgery, suggesting that earlier intervention may lead to improved postoperative outcomes. However, patients with higher preoperative symptom severity also benefit from surgery through the attainment of adequate pain relief to achieve an improvement in physical function.
1296
A322: Clinical Outcomes of Symptomatic Spinal Metastases Treated with Hybrid Therapy (Separation Surgery Followed by Radiosurgery) for Colorectal Adenocarcinoma
Benjamin Schachner 1 , Anubhav Amin 1 , Yoshiya Yamada 1 , Ilya Laufer 1 , Mark Bilsky 1 , and Ori Barzilai 1
1 Memorial Sloan Kettering Cancer Center, New York, USA
Introduction: Twenty-seven percent of patients with colorectal cancer (CRC) develop bone metastasis. There is a paucity of evidence regarding the outcomes of patients who undergo surgery for spinal metastasis from colorectal origin. Treatment of symptomatic spinal metastases is palliative and achieved through surgery, radiotherapy, or a combination of both. Over the past decade, Hybrid therapy (i.e., separation surgery followed by radiosurgery) has become a widely accepted treatment paradigm for metastatic spine disease regardless of histologic subtype. Understanding histology specific outcomes facilitates informed decision making in a rapidly evolving field of multimodality therapies including targetable mutations. This study evaluates outcomes of CRC patients who underwent hybrid therapy for spinal metastases. Material and Methods: A retrospective chart review of all patients at a single institution who underwent surgery for spinal metastasis followed by SRS with a confirmed diagnosis of CRC was performed. Fifty CRC patients were identified. Data collected for this study included patient demographics, tumor histology, type and extent of spinal intervention, radiation data including treatment dose and field, molecular diagnostic pathology (EGFR exon 19, Her2, KRAS, tp53, and APC exon 16) and outcomes were measured and evaluated included survival, local control, complications including reoperations, repeat irradiation, and/or postoperative kyphoplasty at previously treated level. Results: Fifty CRC patients were identified with 32 male, 18 female patients with a mean age of 55.06 (25-83). Fifty-five of these patients were treated with open decompression and stabilization, and 2 were treated with minimally invasive surgery. Average survival from the time of surgery was 288 days (31-1422). Ten patients (20%) had local progression of disease with an average time to progression of 365 days (30-840). Twelve patients (24%) required a reoperation; 6 for local tumor recurrence, 1 for tumor progression at an adjacent level, 3 for wound complication and 1 for progressive spinal instability. Tumor mutations (exon 19, her2, KRAS, TP53, APC exon 16) had no impact on local control. Twenty-one patients (42%) had progression of disease to other spinal levels. Of note, those who survived over 1 year from the day of surgery (DOS), the odds of local progression of disease needing reoperation, RT, and/or kyphoplasty was markedly increased (OR 28.5. 95% CI: 4.2487-191.1784) and statistically significant (P = .0006). Conclusion: Hybrid therapy provides a safe and effective therapy for treatment of symptomatic spine metastases for CRC patients. Local control rates of 80%, lower than previously reported for other histologies, suggest a more challenging disease to treat in the context of spinal cord compression. These outcomes were not significantly affected by the genomic landscape of the primary cancer. Patients surviving beyond one year after surgery had higher odds of requiring further interventions for local progression.
1297
A323: Outcomes of Surgery Followed by Radiosurgery for Treatment of Spinal Metastases from Non-Small Cell Lung Cancer: Do Targetable Mutations Matter?
Benjamin Schachner 1 , Anubhav Amin 1 , Yoshiya Yamada 2 , Ilya Laufer 1 , Mark Bilsky 1 , and Ori Barzilai 1
1 Memorial Sloan Kettering Cancer Center, Neurosurgery, New York, USA
2 Memorial Sloan Kettering Cancer Center, Radiation Oncology, New York, USA
Introduction: Spine metastases occur in 30-40% of all patients with cancer. Because of their relative resistance to radiation, non small cell lung (NSCLC) metastases causing epidural spinal cord compression are challenging to treat. Over the past decade, Hybrid therapy (i.e. separation surgery followed by radiosurgery) has become a widely accepted treatment paradigm for metastatic spine disease regardless of histologic subtype. Understanding histology-specific outcomes is key to informed decision-making in a rapidly evolving field of multimodality therapies including targetable mutations. The advent of new biologics and small molecules that target specific mutations has extended overall survival for multiple cancers and is a rapidly changing landscape. This study evaluates patients who underwent hybrid therapy for NSCLC spinal metastases to determine if targetable mutations affect outcomes. Material and Methods: A retrospective chart review of patients who underwent surgery followed by stereotactic body radiation therapy (SBRT) for symptomatic spinal metastases from NSCLC at a single, tertiary, cancer center was performed. One hundred and five NSCLC patients were included in this analysis. Data evaluated included patient demographics, surgical details, radiation data including dose and fractionation, adjuvant chemotherapy, molecular diagnostic pathology, targeted therapies (immunotherapy, targeted small molecule therapy, and chemotherapy), and outcomes including overall survival (OS), progression free survival (PFS), local tumor control, reoperations, repeat irradiation, and/or postoperative kyphoplasty at previously treated level. Results: One hundred and five NSCLC patients were identified with 56 male, and 49 female patients with a mean age of 65 (32-85.4). This cohort had an average SINS score of 9.5 (5-15), and a construct length of 5.9 (3-12) with an average of 2.6 levels decompressed (1-6). Ninety-four of these underwent open decompression and stabilization, while 11 were treated with minimally invasive surgery. Average survival from the time of surgery was 414.7 days (30-2572). Local control was obtained in 89.5% of patients. 11 patients had local progression of disease; the average time to progression was 366 days (26-2305). Sixteen patients returned to the OR: 4 for tumor recurrence at the index level, 4 for progression at adjacent levels, 2 wound complications, 5 for pathological fracture or hardware failure, and 1 for hematoma evacuation. Twenty-nine of the 105 patients received PD-1 immunotherapy (28%), 35 out of 105 received VEGF immunotherapy (33%), 81 out of 105 received anti-neoplastic agents (77%), and 40 out of 105 received small molecule therapy in the form of kinase inhibitors (38%). Exon 19 mutation significantly increased the odds of local progression (OR 4.8,4 95% CI: 1.08-21.74, P = .04). Average pack years for this cohort was 22.1 (0-102); current smoker status at time of surgery and SBRT significantly increased the risk of PFS and OS. Conclusion: Hybrid therapy is a safe and effective method for treatment of symptomatic spine metastases from NSCLC origin providing durable local control with low complication profiles. Our data demonstrate that EGFR exon 19 mutations increase the odds of local progression of disease. These data provide initial insight to the possible role of mutational analyses for prognostication and informed decision making in the management of spinal metastases.
1295
A324: Spinal Cord Compression and Spinal Instability in Multiple Myeloma - A Shifting Paradigm Towards Non-Operative Management
Nikki Shah 1 , Roozbeh Shafafy 1 , Susanne Selvadurai 1 , Adam Benton 1 , Jan Herzog 1 , and Sean Molloy 1
1 The Royal National Orthopaedic Hospital NHS Trust , Spinal Surgical Unit, Stanmore, United Kingdom
Introduction: Patients with metastatic spinal cord compression (MSCC) or unstable spinal lesions warrant early surgical consultation. In multiple myeloma, chemotherapy and radiotherapy have the potential to decompress the spinal canal effectively in the presence of epidural lesions. Mechanical stability conferred by bracing may potentiate intraosseous and extraosseous bone formation, thus increase spinal stability. With this in mind, this study aims to review the role of non-operative management in myeloma patients with a high degree of spinal instability, in a Specialist Tertiary Centre. Material and Methods: Retrospective analysis of a prospectively collected database of 83 patients with unstable myelomatous lesions of the spine, defined by a Spinal Instability Neoplastic Score (SINS) of 13-18. Data collected include patient demographics, systemic treatment, neurological status, radiological presence of cord compression, most unstable vertebral level and presence of intraosseous and extraosseous bone formation. Post-treatment scores were calculated based on follow-up imaging which was carried out at 2 weeks for cord compression and 12 weeks for spinal instability. A paired t-test was used to identify any significant difference between pre- and post-treatment SINS and linear regression was used to assess the association between variables and the change in SINS. Results: A significant reduction in SINS was observed from a pre-treatment average score of 14 to a score of 9, following treatment for myeloma (P < .001). A higher initial score and a younger age were associated with a larger overall reduction in SINS (P < .001 and P = .02 respectively). Not one particular variable (bisphosphates, chemotherapy, radiotherapy and steroids) had a significant association in SINS reduction. 25 (30%) patients had spinal cord compression, all of which showed radiological resolution of cord compression at 2 weeks. No patients developed neurological deterioration during treatment and all patients had an improvement in their pain scores. 64 (77%) patients had evidence of intraosseous and/or extraosseous bone formation on their follow-up scan. Conclusion: Non-operative management in the form of bracing and systemic therapy is a safe and effective treatment for spinal instability and spinal cord compression in myeloma. The decision to adopt a non-operative approach in this cohort of patients should be made in a tertiary centre with expertise in multiple myeloma and in a multidisciplinary setting.
OP37: Surgical Complications 3
592
A325: Human lumbar Discs are not Sterile! - Defining the Normal Intervertebral Disc Microbiome
Shanmuganathan Rajasekaran 1 , Dilip Chand Raja Soundararajan 1 , Chitraa Tangavel 2 , Sri Vijay Anand KS 1 , Monica Steffi Matchado 2 , and Sharon Miracle Nayagam 2
1 Ganga Medical Centre and Hospitals Pvt Ltd, Spine Surgery, Coimbatore, India
2 Ganga Research Centre, Biotechnology, Coimbatore, India
Introduction: Traditionally, Central Nervous System, spinal cord, eye, fetus and Intervertebral Disc were considered to be to be sterile and immune privileged. With the advent of 16SrRNA sequencing, it has been proved that each of the above have a microbiome which plays an essential role in maintaining homeostasis. With increasing reports of sub-clinical infection as an etiology of disc degeneration and Modic changes, it remains unknown, whether lumbar discs are truly sterile. The primary aim of the study was to investigate the presence of Disc microbiome and its microbial composition. Materials and Methods: In order to obtain true normal controls, intervertebral discs were collected from MRI normal brain-dead voluntary organ donors with no history of back pain. The study was performed after the approval of IRB. The discs were dissected in surgical sterile conditions and were snap frozen immediately to -160 C and the processed samples were subjected to total DNA extraction using QIAamp® DNA Mini Kit and enrichment using NEBNext® Microbiome DNA Enrichment Kit (Cat # E612S/L; New England BioLabs, Ipswich, MA). The purified DNA was amplified using v1-V9 specific primers and the sequencing was performed using Illumina MiSeq platform. Raw data was analysed using Bioinformatic tools such as Greengenes database and kraken2. Proteomic analysis was also performed to confirm bacterial presence. Results: All the eight normal disc samples had bacteria. 42.75% OTUs were classified at the Kingdom level, 44% at Phylum level, 22.62% at Genus level and 5.5% at Species level. A total of 355 bacterial species were identified in normal discs which were distributed under five major phyla- Proteobacteria, Parcubacteria, Firmicutes, Cyanobacteria and Actinobacteria. 21 abundant genera including Pseudomonas, Acinetobacter, Anoxybacillus, Sphingomonas, Bordetella, and Brevundimonas were identified. At species level, the five most abundant bacteria identified were Anoxybacillus kestanbolensis, Acinetobacter lwoffii, Sphingomonas yabuuchiae, Stenotrophomonas acidaminiphila and Pseudomonas veronii. The much-discussed Propionibacterium acnes ranked ninth in abundance in the normal discs. Bacterial presence was confirmed through proteomics data by identification of bacteria specific proteins and vital enzymes. Conclusion: This is the first metagenome study in world literature to document the entire microbiome of MRI normal disc. The results of this study prove that lumbar discs are not sterile structures as traditionally thought. This brings out the question of what spectrum of organisms could invoke sub-clinical infection and disc degeneration. In addition, the presence of Propionibacterium acnes in normal disc samples raises a doubt in its etiopatholgical role in disc degeneration. It would be interesting to analyze the microbiome of degenerated discs to analyze whether a differential microbial composition is associated with disc degeneration.
884
A326: Highly Concentrated Bupivacaine Does not Lead to Increased Local Toxicity Following Skeletal Surgery: a Proof of Concept
Jasper Steverink 1,2 , Floris van Tol 1,2 , Suzanne Bruins 2 , Andre Smorenburg 2 , Marianna Tryfonidou 3 , Bas Oosterman 2 , and Jorrit-Jan Verlaan 1,2
1 University Medical Center Utrecht, Orthopedics, Utrecht, The Netherlands
2 SentryX B.V., Austerlitz, The Netherlands, 3 Utrecht University, Clinical Sciences, Utrecht, The Netherlands
Introduction: Skeletal surgeries are generally perceived as exceptionally painful. Currently, postoperative pain is treated in a multimodal fashion with a prominent role for opioids. The recent societal debate regarding opioids and their frequent adverse effects have sparked the development of non-opioid alternatives. A number of non-opioid analgesics aim to provide a local, sustained release of the amino-amide anesthetic bupivacaine. To obtain extended pain relief, incorporation of a high bupivacaine dose is necessary. The local toxicity induced by high concentrations of bupivacaine is unknown. This study describes local toxicity thirty days following infusion of ascending concentrations of bupivacaine in a rat model of spinal and femoral surgery. Material and Methods: Wistar rats (n = 16) underwent either spinal or femoral implantation of a screw using established approaches. A custom-made cannula for bupivacaine infusion was attached under the screw-head close to the periosteum. Next, either the clinically used concentration of 0.5%, or higher concentrations of 2.5% or 5% bupivacaine was administered, leading to cumulative doses of .67, 3.3 and 6.7 mg/kg bupivacaine, respectively. Half of the rats received the complete dose as bolus infusion. immediately to simulate a dose-dumping scenario. The other half received the dose over 72 hours of pump-controlled infusion, resulting in 12 different treatments. Body weight, leukocyte and creatinine kinase (CK) levels were monitored during the postoperative period. Thirty days after surgery, rats were killed and the implantation site was collected. Hematoxylin-eosin slides were assessed by a blinded pathologist for signs of inflammation, fibrosis, bone reaction, periosteal reaction, osteoclast activity, necrosis and muscle damage. A cumulative histology toxicity score was calculated. Data were analyzed using a multivariate regression analysis. Results: All but two rats recovered uneventfully. Weight, leukocyte counts and CK-levels normalized in all rats during the postoperative period. Bupivacaine concentration, implantation location and speed of administration did not affect postoperative weight gain, leukocyte counts and CK-levels. No difference in histology toxicity score between bupivacaine concentrations was observed, non between administration speeds. Histology toxicity score was significantly higher for spinal implantation compared to femoral implantation, probably corresponding to the more invasive dissection during the procedure. Conclusion: This animal study found no concentration-dependent local toxicity of bupivacaine for skeletal surgery. The toxic effects of even the highest bupivacaine concentration used appear minor/negligible in light of the surgical intervention sustained. The current results might facilitate orthopedic application of sustained-release formulations, containing high concentrations of bupivacaine.
1102
A327: The influence of frailty on the outcomes of spine surgery; a systematic review
Jamie Wilson 1,2 , Vivien Chan 2 , Jetan Badhiwala 2 , Robert Ravinsky 3 , Albert Yee 2 , Jefferson Wilson 2 , and Michael Fehlings 2
1 University of Nebraska medical center, Omaha, USA, 2 University of Toronto Spine Program, Toronto, Canada, 3 University of Arizona College of Medicine, Orthopedics, Phoenix, USA
Introduction: With an aging population, there is an increasing number of elderly patients undergoing spine surgery. Recent literature in other surgical specialties suggest frailty to be an important predictor of outcomes. The aim of this review was to examine the association between frailty and outcomes after spine surgery. Material and Methods: A systematic review was performed registered with PROSPERO (ID:129928). Search strategies 1946 to 2020 with subject headings and keywords for “frailty”, “elderly” and “spine surgeries” and conditions of interest were defined for three databases (Ovid Medline and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid Embase Classic + Embase and Ovid Cochrane Central Register of Controlled Trials). Filters for human studies were used, and were not limited by date or language. The search results were filtered by abstract, and relevant articles were then graded by 3 authors independently. Articles were grouped by index applied, and where possible classified into disease-specific partitions. The primary outcome measure reported was adverse events. Secondary outcomes included other measures of morbidity, mortality, and patient outcomes. Sample size, mean age, age limitation, data source, study design, primary pathology, surgical procedure performed, follow-up period, assessment of frailty used, surgical outcomes, and impact of frailty on outcomes were extracted from eligible studies. Quality and bias was assessed using the PRISMA 27-point item checklist and the QUADAS-2 tool. Results: Initial search returned 4727 results, which were narrowed to 189 after screening by abstract. 30 full text articles were graded and included in the final analysis (total of 127 813 patients). The measure most frequently cited was the 11-point Modified Frailty Index (n = 18), calculated from inpatient diagnostic codes. The most common pathology was degenerative disease followed by adult spinal deformity (ASD), metastatic disease and trauma/spinal cord injury. Pooled quantitative analysis was possible for only 2 articles (ASD). Frailty was universally associated with increased perioperative complications, mortality, length of stay and non-home discharge destination. Only ASD showed correlation with long-term patient-reported outcomes. Morphometric analysis has suggested that measures of sarcopenia may have better acuity for predicting complications compared to frailty. Conclusion: There is strong evidence that frailty is associated with increased risk of morbidity and mortality in patients who received spine surgery. However, it remains inconclusive whether frailty impacts patient outcomes and quality of life after surgery.
1181
A328: Pedicle Screw Stacking: A Technical Note on Instrumentation of Lumbar Spine with a Broken Pedicle Screw
Jvaghar Jill 1 and Nalli Ramanathan Uvaraj 1
1 Madras Medical College, Orthopaedic Spine Surgery, Chennai, India
Introduction: With a substantial increase in the number of pedicle screw breakage in failed spine surgeries, it becomes imperative to instrument the involved level to attain maximum stability to enhance fusion following revision surgeries. We present a novel, feasible bailout procedure called Pedicle Screw Stacking (PSS) to instrument lumbar pedicles with a broken screw inside them. Materials and Methods: Five patients with nine broken pedicle screws at the screw-shaft junction were preoperatively assessed to determine the position of the broken screw within the pedicle. Based on location, they were classified into Type I, Type II, and Type III when they occupied superior, middle, and inferior zones in the pedicle respectively. Stack screws were inserted inferiorly in Type I, superiorly in Type III, and by a tricortical method in Type II. Results: One inferior stack screw at L5 (Type I), five superior stack screws at S1 (Type III), and three tricortical pedicle screws at L5 (Type II) were placed in five patients during revision surgeries. All patients had improvement in functional scores without post-operative neurological deficit or implant failure or screw related complications at a follow-up of not less than two years. Conclusion: PSS is a safe method to instrument the index level, without removal of the broken screw while revising a failed lumbar spine surgery. This technique potentially avoids the instrumentation of additional segments and improves the stability of the revision construct. However, meticulous pre-operative assessment of anatomy is needed to assess the feasibility of the technique based on pedicle anatomy on a case-to-case basis.
1137
A329: Tranexamic Acid in Elective Spine Surgery: A Randomised Controlled Trial Analysing the Efficacy of Intravenous, Local Infiltration and Topical Administration of Tranexamic Acid
Viswanadha Arun-Kumar 1 and J Naresh-Babu 1
1 Mallika Spine Centre, Deparment of Spine Surgery, Guntur, India
Introduction: Intravenous tranexamic acid (ivTXA) has almost become a standard for bleeding management in spine surgery. However, the systemic complications associated with it may be rare but not uncommon. To negate these effects, topical application of tranexamic acid (tTXA) has been used recently with good amount of success. Although local infiltration of tranexamic acid (loTXA) has been used in trauma related haemorrhages, till date there is no literature available examining its efficacy in spine surgery. The purpose of the study is to evaluate the safety and efficacy of tranexamic acid administered through various routes in instrumented spine surgeries. Material and Methods: 104 people undergoing instrumented spine surgery were randomly assigned to 4 groups. Groups included (1) ivTXA-intravenous administration of TXA one hour prior to surgery. (2) loTXA-local infiltration of TXA bilaterally into the paraspinal musculature prior to incision. (3) tTXA-Topical application of TXA just before wound closure. (4) Control group. Outcome measures include intraoperative blood loss, post-operative blood loss, need for blood transfusion, length of hospital stay, blood parameters. Results: All the three groups with different modes of TXA administration were found to be effective in reducing blood loss compared to control group. Intra-operative blood loss was significantly reduced in ivTXA(223.6 ± 40.1 ml, P-< .0001) and loTXA (256.07 ± 119 ml, P-0.0039) groups when compared to controls(344 ± 88.5 ml).Whereas, the post-operative blood loss was least in tTXA followed by ivTXA, loTXA and controls. There was 67% reduction in need for blood transfusion in tTXA group, 55.5% reduction in ivTXA group, and 33% reduction in loTXA group when compared to control group. Conclusion: In instrumented spine surgery, ivTXA and loTXA were found to be equally effective in reducing the intra-operative blood loss. Whereas, the tTXA has better post-operative blood conserving effects. This is the first study to detail about safety and efficacy on local infiltration of TXA in spine surgery, which is an effective and safe method for reducing intra-operative blood loss.
1125
A330: Risk Factors for Post-Operative Venous Thromboembolic Events in Patients Undergoing Thoracic Spine Surgery
Wesley Cooperman 1 , Blake Formanek 1 , Jeffrey C. Wang 1 , and Zorica Buser 1
1 Keck School of Medicine, University of Southern California, Orthopaedic Surgery, Los Angeles, USA
Introduction: Venous thromboembolic events (VTEs), including pulmonary embolism and deep vein thrombosis, are preventable postsurgical complications that are associated with high morbidity and mortality in addition to increased hospital costs and prolonged hospital stays. There is a need for preoperative criteria to identify risk factors for postoperative thromboembolism in patients undergoing thoracic spine orthopedic procedures. This study aimed to elucidate the relative rates and temporal trends of VTEs after various thoracic spine procedures, and the comorbidities and demographics that were independent predictors of VTE. Material and Methods: This is a retrospective study utilizing the PearlDiver insurance database to identify patients who underwent primary single- or multilevel thoracic spine surgery from 2010-2018. Procedures evaluated included fusion, laminectomy/decompression, corpectomy, osteotomy, and kyphoplasty/vertebroplasty. Patients undergoing these procedures were identified using Current Procedural Terminology (CPT) codes. International Classification of Diseases (ICD), Ninth and Tenth Revision diagnosis codes were used to determine the incidence of postoperative VTEs and identify patient comorbidities. Complication codes for VTEs were queried at postoperative day (POD) 0, 1, 7, 30, and 90. Summary statistics, including VTE incidence rates and odds ratios (ORs), were calculated for patient risk factors and demographics. Results: A total of 41,689 patients who underwent thoracic spine surgery from 2010-2018 were identified (52.0% female). Within the entire patient population, the incidence of VTE was 1.40% within a 90-day follow-up period, with an incidence of thromboembolism of 0.21%, 0.46%, and 1.06% by POD 1, 7, and 30, respectively. Patients aged 70-74 represented the most common age group to undergo thoracic spine surgery (17.7%) and experienced the greatest incidence of VTE of any age group (1.79%). Males had an increased incidence of VTE compared to females (1.43% vs 1.38%). Fusion was the most common procedure performed (59.4%) and was associated with the greatest incidence of VTE (1.52%). Osteotomy and laminectomy were associated with VTE incidence rates of 1.40% and 1.34%, respectively. Among individuals with one or more of the queried risk factors, the incidence of VTE was 1.79%, compared with an incidence of 1.20% in individuals without these factors. Risk factors associated with the highest incidence of postoperative VTE were extremity paralysis (7.25%), central venous lines (3.84%), heart failure (3.36%), arrhythmia (3.34%), and hypertension (1.88%). The lowest incidence of VTE was seen in patients with a history of tobacco use (1.25%). Conclusion: Our preliminary data suggests there are identifiable risk factors associated with increased risk of postoperative VTE in patients undergoing thoracic spine surgery. The highest incidence of VTE was observed following fusion. Patients aged 70-74 experienced the highest rate of VTE, and males had a higher incidence of VTE than females. Individuals with one or more queried risk factors had a higher incidence of VTE than those without any factors. These findings regarding the incidence and timing of VTEs have the potential to guide clinician assessment of patient risk and screening practices prior to thoracic spine surgery.
395
A331: Post-Operative Complications Following Sacroiliac Joint Fusion to Treat Sacrum Pain, Sacroiliitis, Sacral Instability, or Spondylosis
Alexander Ballatori 1 , Shane Shahrestani 1 , Andy Ton 1 , Xiao Chen 1 , Zorica Buser 1 , and Jeffrey C. Wang 1
1 Keck School of Medicine, University of Southern California, Department of Orthopaedic Surgery, Los Angeles, USA
Introduction: The sacroiliac joint has been implicated as a source of chronic low back pain. Many have turned to sacroiliac joint fusion after failure of conservative care to relieve symptoms. However, identifying patients who will respond positively from the sacroiliac joint fusion is still unclear. This study examines the postoperative outcomes of sacroiliac joint fusion based on the primary diagnoses of sacrum pain, sacroiliitis, sacral instability, or spondylosis. Material and Methods: Using the 2016 National Readmission Database, we conducted a retrospective cohort analysis of 1,272 patients who received a sacroiliac joint fusion for diagnosed sacrum pain (n = 288), sacroiliitis (n = 536), sacral instability (n = 135), or spondylosis (n = 155) using ICD-10 coding. We then collected all of the individuals that had a non-elective readmission, separated them by their primary diagnosis, and analyzed for postoperative complications including infection, urinary tract infection, pain, osteomyelitis, thromboembolisms, sepsis, pneumonia, pseudoarthrosis, novel lumbar pathology, nervous system complications, and need for revision surgery. Statistical analysis was conducted in R. Tukey multiple comparisons of means was used to compare complications by diagnosis. Results: Sacroiliitis had the highest rate of non-elective readmissions (17.1%), followed by those diagnosed with sacrum pain (14.2%), spondylosis (11.6%), and sacral instability (9.6%), but these rates were not significant between any groups on pairwise comparison. However, those with a primary diagnosis of sacroiliitis had a significantly higher average number of readmissions (1.80 ± 1.16 readmissions) than those with a primary diagnosis of sacrum pain (1.24 ± 0.58 readmissions, P = .013), but no differences existed between other groups. After comparing the different categories of postoperative complications, significant differences in postoperative infection rates were noted between patients with a primary diagnosis of sacroiliitis and those with a primary diagnosis of sacrum pain (P = .008). Conclusion: Patients diagnosed with sacroiliitis had the highest rate of non-elective postoperative readmissions following sacroiliac joint fusion, and patients diagnosed with sacral instability had the lowest rates of non-elective postoperative readmission. The reasons for readmission were not significantly different across each group, except for infection rates of those with a primary diagnosis of sacroiliitis being significantly higher than those diagnosed with sacrum pain.
1861
A332: Short Term Complications Related to the Lumbar Interbody Fusion Approach
Mouadh Nefiss 1 , Ayari Sakr 1 , Bousrih Anis 1 , Ben Ayed Mehdi 1 , Ezzaouia Khelil 1 , Bouzidi Ramzi 1 , and Tborbi Anis 1
1 Mongi Slim Hospital, Orthopedic Surgery Department, La Marsa, Tunisia
Introduction: Lumbar interbody fusion is a therapeutic option that has demonstrated its efficacy in the treatment of various degenerative discal pathologies. However, this technique requires a learning curve and, in some cases, a longer operating time, which may expose the patient to complications that differ depending on the technique chosen. The main objective of our work was to study the rate and type of short term complications related to the lumbar interbody fusion approach. Material and Methods: We conducted a retrospective study of 42 lumbar interbody fusions operated in our department. We used the Eurospine “Spine Tango” form for the fellow, the collection of clinical and epidemiological data. All patients underwent standard pre-operative radiological explorations with magnetic resonance imaging (MRI). Complications were divided into non-specific such as non-fusion, recurrence of clinical symptoms and surgical site infection; specific complications related to the approach such as meralgia for the anterolateral approach. Risk factors for complications were analyzed using SPSS version 20. Results: The average age of our patients was 53 years with a female predominance (sex ratio of 3.6). The main pathologies were degenerative disc disease (38%), degenerative spondylolisthesis (29%) and lumbar spinal stenosis (26%).23 patients were operated by posterior approach (12 PLIF and 11 TLIF) and 19 patients were operated by anterior or anterolateral approach (4 ALIF and 15 OLIF). The operating time was between 2 and 3 hours in 60% of cases. Blood loss was estimated between 100 and 500ml in 66% of cases. An intraoperative transfusion was performed for 2 patients. The overall complication rate was 28,6%. For the posterior approach, we found one case of dural tear which was sutured, one case of spondylodiscitis which was treated with debridement washing and antibiotics with no post-operative clinical impact and 4 cases of clinical recurrence of sciatica. For patients who had an anterior approach, 5 presented a post-operative meralgia and 1 patient with hypoesthesia around the approach. There were no cases of non-fusion or instability. No patient presented a thromboembolic complication. Conclusion: The advantages of lumbar interbody fusion compared to the classical posterolateral fusion technique are well known. However, the complication rate of this technique remains high and must be considered during decision making regarding the approach choice.
1727
A333: Comparing Clinical Outcomes from Pedicle Screw Insertions with Robotic Guidance vs Freehand vs Computer Navigated Techniques: A Systematic Review
Joachim Starup-Hansen 1 , Sherief Elsayed 2,3 , and Roozbeh Shafafy 4
1 Brighton Sussex Medical School, Brighton, United Kingdom
2 Brighton and Sussex University Hospitals, Brighton, United Kingdom
3 NMC Spine, Dubai, United Arab Emirates
4 Royal National Orthopaedic Hospital, Stanmore, United Kingdom
Introduction: The placement of pedicle screws is now common practice in spinal surgery. The freehand method (FH) is a well-established technique of screw insertion where anatomical landmarks and surface topography of the posterior spine are used in order to safely instrument the spine with pedicle screws. Due to the proximity of the pedicle to the neural elements as well as the arrangement of vascular structures adjacent to the spine, inaccurately placed screws can result in significant neurological and vascular complications. Accurate screw placement using the FH method is therefore reliant on the skill and experience of the surgeon. In recent years, significant effort has been placed into the development of surgical tools such as image guided spinal navigation (NV) and more recently robotic assisted guidance (RG) in order to improve the accuracy of screw placement. Whilst the literature thus far has shown that RG improves the accuracy of pedicle screw placement, it remains unclear whether this translates into improved clinical outcomes for patients. We aimed to provide a systematic review of the available literature, comparing clinical outcomes from pedicle screws placed via RG versus NV versus the conventional FH approach. Material and Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. A literature review was conducted in the Medline, Embase, SCOPUS and Cochrane databases from the year 2000 onwards using predetermined search terms. All peer reviewed English language human studies were included. Both prospective and retrospective studies were eligible for analysis. The primary outcome was the rate of post-operative revision surgeries due to misplaced screws. Secondary outcomes were intra-operative screw revision rates, radiation exposure, length of hospital stay, operation duration, blood loss, changes in leg and back pain, changes in disability and complication rates. Results: Among 19 studies, intraoperative revision rates, post-operative revision rates, blood loss and radiation exposure were improved by RG compared to the FH approach. Complication rates, neurologic injury rates, length of hospital stay, length of operations, changes in disability and changes in pain were equivalent between RG and the FH approach. There is lack of available literature comparing RG to NV techniques. Conclusion: Based on the available literature, RG has the potential to minimize the incidence of clinically important adverse events compared to the FH technique. Given the evidence, RG may reduce intra-operative screw revision and the need for post-operative revision. Additionally, RG is associated with reduced blood loss compared to FH, likely due to its minimally invasive nature. Radiation exposure is also reduced with RG compared to FH, yet it should be noted that in cases of osteolytic spinal disease, the benefit in this domain may be limited. Overall, although it is clear that RG does provide benefit across multiple domains compared to the FH approach, it remains questionable whether the size of these benefits is clinically significant. Future research should evaluate whether the improved patient outcomes can justify the costs associated with RG systems.
OP38: Cervical Trauma
1522
A334: Comparing Outcomes of Subaxial and Alantoaxial Trauma in Elderly Patients
Catherine Carlile 1 , Jacob Schultz 2 , Andrew Rees 2 , and Byron Stephens 1
1 Vanderbilt University Medical Center, Department of Orthopedic Surgery, Nashville, USA
2 Vanderbilt University School of Medicine, Nashville, USA
Introduction: In contrast to younger patients, the elderly are more likely to sustain severe cervical spine trauma from relatively low energy mechanisms of injury. The presence of pre-existing spine pathology such as osteoporosis, cervical stenosis, ankylosis, spondylosis, and degenerative changes can predispose elderly patients to fractures and neurologic injury. To date, there has been little research comparing outcomes and mortality rates of patients with upper cervical (occiput-C2) versus subaxial (C3-C7) cervical spine injuries. Given this paucity of data on this subject, we sought to compare mortality rates and outcomes between using our prospective trauma database. Materials and Methods: All elderly trauma patients (65+) with cervical spine injuries who presented to a single, high-volume, level I trauma center between 2010-2019 were identified via an institutional trauma database. Retrospective chart review was performed to assess treatment rendered, complication, and outcome measures and then stored in a deidentified database. Imaging characteristics of patients including psoas index (a marker for sarcopenia) and L3 Hounsfield Unit (an indicator of osteoporosis) were calculated using standard technique and recorded. Patients were sorted into upper cervical (occipital condyle, C1, and C2 vertebral fractures and ligamentous injuries) and subaxial (C3-7) cohorts and by treatment (operative vs non-operative management). Surgical and medical morbidity variables recorded include surgical site infection, pneumonia, STEMI, DVT/PE and stroke. Pearson's Chi-squared tests were used to compare rates of mortality and complications between groups. Results: A total of 922 patients were identified, with 545 upper cervical (59%), and 377 subaxial (41%) trauma patients. Patients with upper cervical spine trauma were significantly older (P < .001), more sarcopenic (P = .002), osteoporotic (P = .002), and had higher rates of dementia (P = .003). There was no significant difference in cardiac or pulmonary comorbidities between the two groups (P = .7). Patients with subaxial injuries had a higher injury burden, with significantly higher Injury Severity Scale (ISS) scores (P = .008), non-contiguous spine injuries (P = .016), closed head injury (P = .04), and pelvic fractures (P = .04). Comparing operative cohorts, there was a higher proportion of medical and surgical complications in the upper cervical group (P = .006), and specifically higher incidence of pneumonia (P = .009). There was also found to be higher overall mortality in all upper cervical injuries both operative and nonoperatively managed as compared to the subaxial cohort (P = .015). There was no significant difference in in-hospital mortality between the two groups (P = .25). Conclusion: Although patients with subaxial injuries were found to be more severely traumatized with higher energy mechanisms and more severe associated injuries, our data demonstrates that patients with upper cervical trauma are at higher risk for medical and surgical complication and mortality, regardless of need for operative intervention. This is likely secondary to poor reserve given their older age, advanced sarcopenia, and increased morbidity associated with both operative management and nonoperative immobilization. In conclusion, we have demonstrated in the largest study to date that patients with upper cervical injuries, although less severely traumatized, should be critically evaluated given their increased risk for morbidity and mortality, especially during discussions with the patient and family about expected outcomes and functional status.
1552
A335: Complications of Anticoagulation Therapy for Thromboembolic Event Prophylaxis in Patients with Cervical Spine Fractures
Michael Faloon 1 , Jennifer Kurowicki 1 , Stuart Changoor 1 , Conor Dunn 1 , Charles Long 1 , Kumar Sinha 1 , Ki Hwang 1 , and Arash Emami 1
1 St. Joseph's University Medical Center, Paterson, NJ, USA
Introduction: The role and timing of anticoagulation (AC) therapy for thromboembolic event (TEE) prophylaxis in patients with cervical fractures is an ongoing debate in the literature with poor evidence dictating guidelines specific to these injuries. The risk of TEE must be weighed against the risk of bleeding complications from the therapy itself. Patients with cervical fractures may be at greater risk of bleeding complications. Therefore, the purpose of this study was to evaluate comorbidity burden, rate of thromboembolic events, rate of anemia and transfusion events, and utilization rates of various forms of pharmacologic prophylaxis following cervical spine fracture. Material and Methods: A retrospective review of the Humana insurance database from 2007 to 2016 was performed to identify patients with cervical spine fractures. Patients were subdivided by AC therapy prescribed within 6 months of cervical spine fracture. Each cohort was longitudinally tracked for incidence of thromboembolic events, anemia, or transfusion at 2 weeks, 4 weeks, 12 weeks, and 6 months following cervical fracture. Demographics analysis and Charleston Comorbidity Index (CCI) was recorded. Sub-analysis by comorbidity was performed between cohorts. Chi-squared test was used to determine significance and compound annual growth rate was used to analyze utilization. Results: Five thousand eight hundered and seventy one patients were identified as having AC therapy with aspirin/anti-platelet, heparin/LMWH, warfarin or factor Xa inhibitors within 6 months of cervical spine fracture. Patients on aspirin/anti-platelet therapy were the least likely cohort to have any TE (2.1%, P < .5), particularly DVT (1.3%) and PE (0.6%). There was no difference found between cohorts in regards to incidence of stroke, proportion of transfusion, and anemia. Conclusion: Aspirin and anti-platelet anticoagulation therapy after cervical fracture had the least number of thromboembolic events when used within 6 months compared to other common forms of anticoagulation. Further research is needed to better understand the relationship between timing of specific anticoagulation therapy with the risks of the specific patient (cervical fracture pattern, medical comorbidities, etc.) and these significant complications to create a more individualized protocol.
1964
A336: Results in Dorsal Percutaneous C1/C2-Screw-Osteosynthesis in Instable Odontoid Fracture Type Anderson 2 and Combined Facture C1/C2 in the Elderly
Stefan Hauck 1
1 Trauma Center Murnau, Spine Surgery, Murnau, Germany
Question: For the surgical treatment of unstable odontoid fractures or combined fracture of C1/C2 (“unhappy triad”) in old age several surgical procedures are possible:(1) direct anterior screw fixation of the odontoid, (2) dorsally by C1/C2-screw-osteosynthesis, open with iliac crest bone graft and cerclage (n.Gallie) or, (3) dorsally by C1/C2-screw-osteosynthesis percutaneously with two C1/C2-screws. The anterior direct screw osteosynthesis in osteoporotic bone metabolism is not successful, the dorsal C1/C2-screwing in open technique with iliac crest bone graft and cerclage is very stressful for the elderly. The percutaneus C1/C2-screw-osteosynthesis can lead to healing of the odontoid fracture; after completion of the fracture healing the screw fixation can be removed. Methodology: In a prospective study 32 patients with unstable odontoid fracture and an age over 60 years were stabilized with percutaneous posterior dorsal screw fixation C1/C2. The surgery was performed with 3D image converter for documentation of the reposition preoperatively and postoperatively to control the screw position. Intraoperative the percutaneous approach was documented with the exact image converter in two planes, ap and strictly laterally. Postoperative clinical controls were performed and CT inspection to document the stability and he healing of the fracture of the odontoid within a year. Results: In the period from January 2007 to December 2012 was carried out in 32 patients with unstable odontoid fractures with percutaneous screw fixation C1/C2 posterior stabilization. 17 women, 15 men with a mean age of 81.8 years / - 7.5 (median 84, min 57, max 91) were stabilized. The mean OR-time was 50.0 min / - 24.3 (median 44.5, Min 16, Max 123). In the mean follow-up of 117 days / - 244 (median 29.5), all patients had a stable course. In 12/32 patients the healing of the fracture could be demonstrated by CT, in 3/32 the metal was removed. Conclusions: The C1/C2 dorsal percutaneous screw fixation of unstable odontoid fractures is a safe and promising, the patient little burdensome procedure. With the help of 3D-imaging operating profit can be improved. Especially the older patients benefit from this supply strategy with high healing rate of the fractures. The metal removal can be effected by fracture healing of the odontoid, and thus the C1/C2-joint can be given free again.
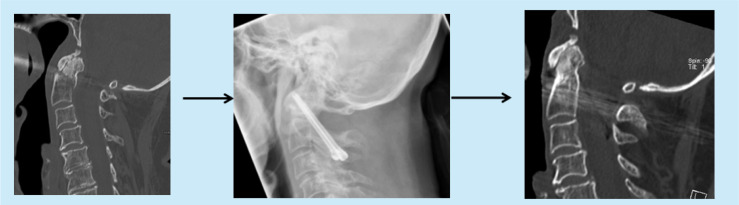
1764
A337: Timing of Surgery and Pre-Operative Physiological Parameters as Clinical Outcomes in Traumatic Subaxial Cervical Spine Fractures and Dislocations
Aman Khanna 1 , and Hari Menon 1
1 New Civil Hospital Surat, Orthopaedics, Surat, India
Introduction: The burden of disability and rehabilitation with Spinal Cord Injury is immense and increasing with the advent and easier availability of high-speed vehicles in developing countries. Primary insult to spinal cord caused by compression due to dislocation or burst is irreversible. This injury further leads to progressive and continuous compression leading to hypoperfusion of the injured segment increasing the oedema and cord contusion. Pre-clinical studies have suggested direct co-relation between the period of compression of the cord and the extent of the structural irreversible damage to the cord. This finding has led spine surgeons to offer early surgical intervention to mitigate the damage and promote neurological recovery in such patients. An early surgical decompression targets to attenuate a secondary hit mechanism cascade including ischemia which ultimately leads to permanent loss of function for spinal cord. Despite the world-wide use of early decompression in patients with sub axial cervical fracture dislocation as a standard, it’s role in improving neurology and decreasing mortality/morbidity remains controversial. There is a lacunae in the data of the surgical and functional outcomes of sub axial cervical spine fractures and dislocations in terms of patient’s pre-operative physiological profile and surgical timing. Also there has been a considerable difference in the studies performed in the developing world and the developed world with respect to the surgical and functional outcomes, disability and mortality. This may be due to constraints of resources, sporadic health infrastructure, disregard for aggressive rehabilitation of the patients with permanent disabilities, lack of research funding and prioritization of other communicable and curable diseases with respect to the spinal cord injuries in developing countries. In this study, we have aimed to evaluate the risk factors associated with sub axial cervical spine fractures and dislocations in terms of patient’s pre-operative physiological parameters and surgical timings. Material and Methods: Twenty six patients with sub axial cervical spine fractures and dislocations were enrolled. Demographic data of patients, appropriate radiological investigation and physiological parameters like respiratory rate, blood pressure, heart rate, PaO2 and ASIA impairment scale were documented. They were divided pre-operatively into 2 groups. Group U with patients having abnormal physiological parameters and Group S including patients having physiological parameters within normal range. They were further sub divided into early and late groups according to the timing of surgery as Uearly, Ulate, Searly and Slate. All the patients were called for follow up at 1, 6 and 12 months. Results: Patients in Group S had neurological improvement by one ASIA grade and a good outcome irrespective of the timing of surgery. Patients in Group U having unstable physiological parameters and undergoing early surgical intervention had poor outcomes. Conclusion: This study concludes that early surgical intervention in physiological unstable patients had strong association as a risk factor in the final outcome of the patients in terms of mortality and morbidity. Also, no positive association of improvement in physiological stable patients with respect to timing of surgery could be established.
1676
A338: YouTube as a Source of Patient Information on Cervical Spine Fractures: A Content-Quality and Optimization Analysis
Michal Krakowiak 1 , Justyna Fercho 2 , Zuzanna Maliszewska 2 , Shan Ali 2 , Tomasz Szmuda 1 , and Paweł Słoniewski 1
1 Medical University of Gdansk, Neurosurgery Department, Gdansk, Poland
2 Medical University of Gdansk, Scientific Circle of Neurology and Neurosurgery, Gdansk, Poland
Introduction: Due largely to its convenience, the internet allows patients to search the web for health information. For this reason, it is critical to check the quality and adequacy of information published online. In this paper, we evaluated the information available on YouTube concerning cervical spine fractures. Material and Methods: The first 35 videos for each of the following search terms were considered for analysis: cervical spine fracture, cervical spine injury, broken cervical spine, broken neck, neck trauma and c spine trauma. All the videos were searched on October 4, 2020. The search was conducted under the default “relevance” sorting in “incognito mode” without being logged to any personal browser account. Videos were assessed by two independent evaluators using the DISCERN scoring system, the Journal of the American Medical Association (JAMA) score and the Global Quality Score (GQS). “VidIQ Vision for YouTube” plugin was used to investigate the quantitative information the analysed videos. The discrepancy between individual videos and the 2 evaluators (a 6th year medical Student and a 4th year neurosurgery resident) was statistically evaluated and compared. Non-English videos, videos greater than 60 minutes and videos containing irrelevant information (e.g., music videos and pranks) were excluded. Results: Out of the 210 videos considered, only 65 (31%) met the inclusion criteria. The DISCERN score ranged from 18 to 53 while the mean between the raters was 32 points which indicates an overall poor quality of videos on cervical spine fractures. Qualitative analysis showed that the vast majority of videos had clear information (n = 59, 90.77%). Most of the videos included anatomy (n = 44, 67.69%), mechanisms of injury (n = 43, 66.15%) and symptoms of cervical trauma (n = 34, 52.31%). 66.15% (n = 43) of videos had a doctor speaking. Most videos were uploaded by physicians (27.69%). The absolute agreement for the intraclass correlation coefficient was .97 for DISCERN, .86 for JAMA and 0.74 for GQS. Videos explaining cervical spine anatomy, treatment options, treatment procedures and risks had a statistically significant higher DISCERN, GQS and JAMA score. Videos containing: clear information, radiographs, diagrams and a doctor speaker had a higher DISCERN, GQS and JAMA score. Patient speakers correlated with lower video scores. No correlation was found between the length of video, words per minute or the number of likes, animation and the JAMA/GQS/DISCERN scores. Videos uploaded by patients had a statistically significant lower scores in all three scales. Conclusion: The quality of cervical spine fracture videos on YouTube is poor. Considering the extent to which patients rely on YouTube as a source of information, the educational quality of videos on this topic can be much improved. We have highlighted specific topics that are commonly omitted so that future content creators may use it as a guide to make more robust educational videos.
544
A339: Epidemiological and Surgical Aspects of Post-Traumatic Syringomyelia in A Rehabilitation Hospital
Vitor Viana Bonan de Aguiar 1 , Giovani Rodrigues Batista 1 , ricardo de amoreira gepp 1 , and Asdrubal Falavigna 2
1 Sarah Network of Rehabilitation Hospitals, Brasilia, Brazil
2 Universidade de Caxias do Sul, Caxias do Sul, Brazil
Introduction: Patients who are victims of traumatic spinal cord injury (SCI) may develop late neurological signs and symptoms directly related to the initial trauma, or even worsening of the pre-established neurological symptoms. In these cases, differential diagnoses should be investigated including syringomyelia. Post-traumatic syringomyelia (PTS) is the development of a spinal cord cyst caused by changes in the CSF flow. The incidence of symptomatic PTS is observed in 4-40% of cases of SCI, but the literature is heterogeneous and scarce. The objective of this study is to analyze the cases of PTS in terms of prevalence, prognostic factors and results of surgical therapy. Material and Methods: A retrospective study was carried out using electronic records from the hospital database of patients with PTS. Clinical and radiological data were extracted from January 2000-December 2018. Prevalence, patient demographic data, information about the traumatic event, clinical and radiological factors, and the impact of different surgical techniques adopted for the treatment of PTS were analyzed. Results: A total of 920 patients diagnosed with SCI were recorded and 85 patients met the inclusion criteria for diagnosis of PTS. Traffic accidents were the most common cause (N = 58; 68.2%), the thoracic segment was the most affected (N = 56; 65.9%) and upper limb paresis was the most common clinical alteration that motivated surgery (N = 27; 45%). Surgical treatment was indicated in 48 patients distributed among the following types of surgery: syringo-pleural shunt (N = 29; 60.4%), adhesiolysis (N = 17; 35.4%) and syringo-subarachnoid shunt (N = 2). The prevalence of PTS in the hospital was 9%, being more frequent in ASIA A patients. The majority of patients with PTS (63 patients; 74.1%) were operated in the first SCI approach. Specific surgical treatment for syringomyelia significantly reduced the cyst, both in the number of levels (P = .05) and by reducing a large part of the cyst (P = .001). The reoperation rate after using the adhesiolysis technique was 47%, while the cyst derivation technique showed a rate of 38%. Conclusion: The follow-up and monitoring of patients with spinal trauma are important for the diagnosis of syringomyelia, especially the late neurological symptoms. Surgery has a positive impact on the radiological reduction of the syringomyelia cyst.
1601
A340: Standard Set of Network Outcomes for Traumatic Spinal Cord Injury: A Consensus-Based Approach Using the Delphi Method
Martin Pouw 1,2 , Thomas van Schaik 1 , Henk van de Meent 3,4 , Armin Curt 5 , Ilse van Nes 3 , Allard Hosman 1 , Marinus De Kleuver 1 , Helma Bongers-Janssen 3 , Marije Vos-van der Hulst 3 , and Miranda van Hoff 1 6
1 Radboud University Medical Center, Orthopaedic Surgery, Nijmegen, The Netherland
2 Sint Maartenskliniek, Orthopaedic Surgery, Nijmegen, The Netherlands
3 Sint Maartenskliniek, Rehabilitation Medicine, Nijmegen, The Netherlands
4 Radboud University Medical Center, Rehabilitation Medicine, Nijmegen, The Netherlands
5 Balgrist University Hospital, Spinal Cord Injury Center, Zurich, Switzerland
6 Sint Maartenskliniek, Research, Nijmegen, The Netherlands
Introduction: In the acute care for patients with traumatic spinal cord injury (t-SCI), the primary focus is to prevent and reduce secondary damage. The focus during the rehabilitation phase is to regain the best level of participation. At the moment, large practice variation in treatment exists in level one-trauma centers and in rehabilitation centers. To understand and reduce practice variation, standardization of treatment outcomes is warranted. With systematic and continuous outcome monitoring during both the clinical and rehabilitation phase, it is possible to assess the value of provided care. The data can be used to describe care patterns, including suitability of care and inequalities in care provision. Purpose: to define a standardized (network) outcome set for t-SCI, including patient-relevant outcomes, adequate measurement instruments, as well as case-mix and risk factors. Material and Methods: Based on peer-reviewed literature and (inter-)national databases as the EMSCI (European Multicenter Study about Spinal Cord Injury) and the Dutch SCI database (Nederlandse Dwarslaesie Database; NDD), a preliminary set of outcomes, casemix and risk factors, and adequate measurement instruments was composed. A multidisciplinary panel participated, consisting of 19 health-care professionals (orthopaedic and neurosurgeons, rehabilitation physicians, physiotherapists, occupational therapists, psychologists, nurses) with experience (average 14 years) in t-SCI management. A modified Delphi method was performed to reach formal consensus and consisted of two web-based surveys and one face-to-face meeting (threshold for consensus: 70%). Results: In the first two Delphi rounds, 18/19 invited panelists (94.7%) responded and 10 panelists participated in the final meeting. The prefinal set was confirmed by all panelists. The standard set encompasses the three-tiered outcome hierarchy and consists of patient-reported and clinician-reported outcome domains, covering the surgical and rehabilitation phase. It includes survival (survival rate, trauma severity), degree of health or recovery (functional status; neurological status [ASIA], walking ability [e.g. SCIM-III, 10MWT, WISCI], quality of life [EQ5D5L, AOSpine PROST]), time to recovery and to return to normal activities (time of injury, admission, surgery, rehabilitation and discharge), disutility of care or treatment process (operative mortality, re-operations, adverse events), sustainability of health and nature of recurrences (participation, caregiver burden), and long-term consequences of therapy (pneumonia, decubitus, surgical interventions). The panelists reached consensus on a measurement schedule (acute [<72 hours], sub-acute and chronic [1, 3, 6 and 12 months] phase) and on the proposed casemix and risk factors, including demographics (e.g. age, gender), clinical status (e.g. physical status, co-morbidities), and treatment process ((non-)surgical treatment and rehabilitation program). Conclusion: A standard set for network outcomes is developed and can be implemented in hospitals and rehabilitation centers involved in the treatment of t-SCI. The set facilitates pooling of data and can be used to compare casemix and risk-adjusted outcomes across regions, studies, and registries in order to improve the quality in clinical practice in t-SCI. Using the standard set, prognostic prediction of outcomes of treatment is feasible, so each patient receives the right care at the right time in the right place. In future, this supports patient-specific decision-making, and ultimately improved outcomes and value of care for patients with t-SCI.
13
A341: Pedicle Screw in Lower Cervical Spine
Pashupati Chaudhary 1 , Raju Rijal 1 , Dipendra Mishra 1 , and Pramod Baral 1
1 BPKIHS, Dharan, Nepal
Background: Pedicle screw fixation of lower cervical spine is a new technique that provides an alternative to posterior lateral mass plating. Although biomechanical studies suggest the use of pedicle screws to reconstruct the cervical spine, placing screw in small cervical pedicle poses a technical challenge. Penetreation of screw in pedicle is a primary complication associated with screw insertion in the lower cervical spine. Aim and Objective: To manage the cervical spine injuries by pedicle screw presented to department of Orthopaedics, BPKIHS, Dharan. Materials and methods: This is retrospective interventional study done at the department of Orthopaedics,B.P.Koirala Institute of Health Sciences, Dharan, Nepal over a period of 7 years from March 2012-April 2019. A total of 55 patients with cervical spine injuries were treated by pedicle screw. The patient’s age ranged from 20 to 60 years and the mean follow-up was 12 weeks. Results: The study comprised of 55 patients with cervical spine injuries were treated by pedicle screw The age incidence in this series ranged from 20 years-60 years. 40 patients were males and 20 was female. All had fractures or fracture dislocation at different levels of lower cervical spine.The mechanism of injury included falls from height (80%), motor vehicle accidents (18%) and sports related injury (2%). Discussion: Pedicle screw insertion into the pedicles in the lower cervical spine is technique that requires a solid knowledge of 3-dimensional anatomy of cervical spine and experience of pedicle screw fixation in thoracolumbar spine. The biomechanical advantages of pedicle screw fixation in cervical spine is obvious, but data are limited. However, safety and role of pedicle screw fixation in reconstruction in the lower cervical spine have not been defined. Conclusion: It is indicated in patients with osteoporotic bone or when rigid internal fixation can not be achieved by conventional techniques. Keywords: Cervical pedicle screw, lower cervical spine, lateral mass
499
A342: Modern Guerilla Warfare and Penetrating Missile Injuries of the Cervical Spine: Characteristics of Penetrating Missile Injuries to the Cervical Spine in a Large War Time Cohort of Modern Guerrilla Warfare
Thamer Hamdan 1 , Bisola Ajayi 1 , Mohsen Raza 1 , Angelo Fragkakis 1 , Timothy Bishop 1 , Jason Bernard 1 , and Darren Lui 1
1 St George's Hospital, Complex spine surgery, London, United Kingdom
Introduction: Missile injuries are very serious injuries particularly in the cervical region. They are classified into high and low missile injuries when it involves the cervical spine. In modern guerrilla warfare, one must be aware of ballistic pathology with bullets as well as from explosives. In particular, improvised explosive devices commonly known as IED's play a new and important pathophysiology whether they are suicided vests or roadside bombs. They usually produce severe or lethal injuries and serious neurovascular deficit is frequent. We present the details of 40 patients with local experience on how to handle serious penetrating cervical missile injuries. Methods: All cases were collected from the record of Basrah University Hospital, Iraq. Healthy military gentlemen with ages ranging between 20-35 years were included. Results: 11 patients had bullet injuries and 29patients had fragments of shell injuries. The sites of injuries were 9: C2-C3, 12: C5-C6,12: C4-C5 and 7: C7-T1. Bullet entrance was anterior in 23 patients, posterior in 7 patients and lateral in 10 patients. The cervical vertebrae were injured in 37 patients at body or lamina level while in 3 patients it was only neural tissue injuries. Missiles were retained in 13 patients. All injuries showed some degree of neurological deficit with quadriplegia in 26 patients. 9 patients presented with very serious injuries. No relation was found between the size of the missile and the extent of damage. Outcome of treatment in all patients was poor. Conclusion: Gunshot wounds only account for approximately one third of penetrating missile injuries in patients who survive and are well enough to receive medical treatment. 62% of patients’ cohort were from explosive devices, consistent with data from 2010, where 58% of fatalities were from IED's occurring in foreign soldiers in Afghanistan. We discuss the importance of general supportive measures, generous wound excision, removal of the retained missiles and heavy cover of antibiotics.
OP39: Minimally Invasive Spine Surgery
384
A343: Minimally Invasive vs Open Surgery for Lumbar Spinal Stenosis in Patients with Diabetes - A CSORN Study
Kalpesh Hathi 1 , Erin Bigney 2,3 , Eden Richardson 2,3,4 , Dana El-Mughayyar 3 , Amanda Vandewint 3 , Tolu Alugo 1,5 , Neil Manson 1,3,6 , Edward Abraham 1,3,6 , CSORN Investigators 4 , Najmedden Attabib 1,3,7
1 Dalhousie Medicine New Brunswick, Saint John, New Brunswick, Canada
2 Horizon Health Network, Saint John, New Brunswick, Canada
3 Canada East Spine Center, Saint John, New Brunswick, Canada
4 Canadian Spine Outcomes and Research Network, Markham, Ontario, Canada
5 Saint John Regional Hospital, Anesthesiology and Pain, Saint John, New Brunswick, Canada
6 Saint John Orthopaedics, Saint John, New Brunswick, Canada
7 Saint John Regional Hospital, Neurosurgery, Saint John, New Brunswick, Canada
Introduction: Patients with diabetes experience worse outcomes following spine surgery. It is important to optimize the outcomes of patients with diabetes as they are at greater risk of complications and comorbidities. Studies comparing MIS vs OPEN spine surgery for patients with diabetes are lacking. This study compares the outcomes of patients with diabetes undergoing MIS vs OPEN surgery for lumbar spinal stenosis (LSS). Material and Methods: This is a multi-center retrospective cohort study. Baseline, surgical, 6-12 week and 12 month follow-up data were obtained for patients with diabetes diagnosed with LSS from the Canadian Spine Outcomes and Research Network (CSORN) registry. Exclusion criteria were American Society of Anesthesiologists (ASA) scores >3 or >3 levels operated on. Primary outcomes of interest were blood loss, length of hospital stay, adverse events, modified Oswestry Disability Index (ODI) and the Numerical Rating Scales (NRS) for leg and back pain. Two separate analyses were run to compare the effects of MIS vs OPEN surgery for two treatment cohorts: (1) patients undergoing decompression without fusion (N = 116; MIS n = 58; Open n = 58), (2) patients undergoing decompression with fusion (N = 108; MIS n = 54; Open n = 54). A 2 (MIS vs OPEN) x 3 (baseline; 6-12 weeks; 12 months) mixed measures analysis of co-variance (ANCOVA) with ASA scores as a co-variate were run for each cohort. Categorical variables were analyzed with 2x2 chi-square tests and continuous variables were analyzed with t-tests. Significance was set at P < .05 and mean differences were compared against published values for minimal clinical important difference (MCID). Results: All patients had significant improvements on ODI and pain scores from baseline to 6-12 weeks and 12 months which met MCID, regardless of surgical technique. There was no significant difference between MIS and OPEN surgery on long-term outcomes in the decompression without fusion cohort. The MIS group who underwent decompression with fusion had significantly lower ODI (mean difference 14.25; P < .001) and back pain (mean difference 1.64; P = .002) compared to OPEN surgery at 12 months post-operation, the difference exceeded the MCID. The MIS groups in both cohorts had significantly less blood loss (without fusion mean difference 99.77 ml, P = .002; with fusion mean difference 244.23 ml, P < .001) and significantly shorter length of stay in hospital (without fusion mean difference 1.15 days, P = .008; with fusion mean difference 1.23 days, P = .026). There were no statistical differences in adverse events for either cohort (without fusion P = .485; with fusion P = .079). Conclusion: Patients with diabetes benefit long-term from decompression with and without fusion for LSS regardless of surgical technique. MIS surgery for LSS is associated with significantly less blood loss and shorter length of hospital stay. MIS decompression with fusion for LSS provides patients with diabetes with less disability (ODI) and back pain one year post-operation compared to OPEN procedures. To optimize outcomes, MIS approaches should be promoted for patients with diabetes undergoing decompression with fusion for LSS.
1342
A344: Patient Reported Outcomes of Patients that Fail to Reach Minimum Clinically Important Differences: Comparison of MIS to Open TLIF
Oliver Ayling 1 , Nicolas Dea 1 , and Charles Fisher 1
1 University of British Columbia, Spine Surgery, Vancouver, Canada
Introduction: Treatment of degenerative lumbar diseases has been shown to be clinically effective with open or minimally invasive transforaminal lumbar interbody fusion (TLIF), with equivalent clinical outcomes between the two modalities. Despite this, a substantial proportion of patients will not meet minimal clinically important differences (MCID) on patient reported outcomes (PROs). Previous studies have not compared subsets of patients that fail to reach MCIDs after open (O-TLIF) or minimally invasive (MIS-TLIF) TLIF in order to identify clinical variables associated with poor outcome. Material and Methods: Patients undergoing O-TLIF or MIS-TLIF for lumbar degenerative disorders enrolled in the Canadian Spine Outcomes and Research Network prospective registry. The outcomes of patients not meeting MCID on the Owestry Disability Index (ODI of 15) at 2 years post-operatively were analyzed at 24 months post-operatively on the ODI, SF-12 Physical (PCS) and Mental (MCS) scales, numeric rating scale (NRS) leg and back pain, and Euroqol-5D (EQ5D). Results: 41.4% (181 of 437) and 42.1% (53 of 126) of patients in the O-TLIF and MIS-TLIF, respectively, did not reach a MCID of 15 on the ODI at 2 years. Patients undergoing MIS-TLIF were younger (55.0 ± 14.9 vs 59.7 ± 13.0, P = .041) but otherwise had similar demographic characteristics. Operative time was similar between the groups (P = 0.16), however blood loss was significantly greater in the O-TLIF cohort (635.0 ± 625.5 ml vs 179.3 ± 159.44 ml, P < .001). There were no significant differences between any baseline PROs. The 2-year post-operative NRS-leg scores were significantly lower in each group than the baseline scores (O-TLIF: 7.12 ± 2.06 vs 2-year, 4.84 ± 3.09; MIS-TLIF: baseline, 6.45 ± 2.73 vs 2-year, 4.38 ± 3.17, < .001), however, the proportion of patients meeting MCID on the NRS-leg at 2 years was significantly higher in the O-TLIF group (75.63% vs 56.52%, P = .015). On the NRS back pain scale, 2-year post-operative scores were significantly lower than baseline in both groups (P < .001) but the proportion of patients reaching MCID was not different (48.62% and 47.06%, P = .99). The 2-year scores and rates of reaching the MCID on the EQ5D, PCS, and MCS were not different. Multivariable regression analysis for the MIS-TLIF cohort demonstrated higher baseline back pain scores were independently associated with worse ODI (P = .0096). In the O-TLIF cohort, higher baseline back pain scores, symptom duration > 6 months, and increasing blood loss (in millilitres) were associated with worse ODI scores (P < .0001, P = .036, P = .039). Single level fusion operations were independently associated with improved ODI scores (P = .001). Conclusion: Similar rates of patients fail to reach MCID at 2-years on the ODI after open or MIS TLIF (∼40%). Of these patients, MIS-TLIF operations were associated with significantly fewer patients achieving MCID on NRS leg pain scores at 2 years. Higher baseline back pain, longer symptom duration, and increasing blood loss were independently associated with worse ODI scores after open TLIF while higher baseline back pain was an independent predictor of worse ODI scores after MIS TLIF. These data provide novel insights into patient counseling as well as surgical selection when deciding which patients will derive the most benefit from MIS or open operations.
1586
A345: Open vs Minimally Invasive Transforaminal Lumbar Interbody Fusion: A Matched Cohort Analysis with Five-Year Follow-Up
Daniel Coban 1 , Stuart Changoor 1 , Conor Dunn 1 , Michael Pompliano 1 , Kumar Sinha 1 , Ki Hwang 1 , Michael Faloon 1 , and Arash Emami 1
1 St. Joseph's University Medical Center, Paterson, NJ, USA
Introduction: Transforaminal lumbar interbody fusion (TLIF) is a widely performed procedure that has evolved as a treatment option for addressing conditions such as spinal stenosis, disc herniation and spondylolisthesis of the lumbar spine. With the advent of new minimally invasive techniques, minimally invasive TLIF (MI-TLIF) has gained popularity as a surgical option and offers potential advantages of reduced tissue trauma, blood loss, medication use and cost. Despite numerous reports on short-term outcomes comparing the open versus the minimally invasive technique, a paucity of literature exists comparing outcomes with long-term follow-up of matched cohorts. Therefore, the purpose of this study was to determine the overall revision rates, rates of fusion, and functional clinical outcomes of open versus MI-TLIF with five-year follow-up. Material and Methods: A retrospective review was performed to identify all patients between 2012-2015 with at least 5-year follow-up who underwent single-level open or minimally invasive TLIF. Each cohort was matched for age, sex, BMI and levels operated. Revision rates, time to revision, graft subsidence and fusion rates in each group were compared. Graft subsidence was defined as cage migration into one vertebral endplate >3 mm on plain radiographic measurement. Bony fusion was defined as the absence of a radiolucent gap between the cages and endplates and the presence of trabeculation and bony bridging between cages and adjacent endplates. Functional outcomes were assessed with ODI, VAS-l and VAS-b measurements at follow-up visits. Standard binomial and categorical comparative analyses were performed. Results: A total of 90 patients were included in this study, 45 in the open TLIF cohort and 45 in the MI-TLIF cohort. Mean follow-up of the open and MI-TLIF cohorts were 90.3 and 97.9 months, respectively. The overall revision rates were 13.3% for the open TLIF group and 15.6% for the MI-TLIF group (P = .764). Mean time to revision was 1,281.3 and 718.1 days for the open and MI-TLIF groups, respectively (P = .015). The most common reason for revision surgery was pseudarthrosis (57.1%) in the MI-TLIF cohort and hardware failure with accompanying adjacent segment degeneration (33.3%) in the open TLIF cohort. At the 5-year mark postoperatively, 11.1% of patients in the open TLIF group and 8.9% of patients in the MI-TLIF group had radiographic signs of subsidence (P = .725). Successful spinal fusion at 5 years was 89.1% and 91.1% in the open and MI-TLIF cohorts, respectively. There were 18 females and 27 males in each cohort matched for age, sex, BMI and levels operated (1: L3-4, 28: L4-5, 16: L5-S1). Average blood loss was 235.6 ± 40.1 and 83.2 ± 28.1 ml in the open and MI-TLIF groups, respectively (P = < .001). Both groups experienced significant improvements in their functional outcome scores (ODI, VAS-leg, VAS-back) compared to their pre-operative values. Conclusion: MI-TLIF is a safe and effective alternative to the open transforaminal approach in the treatment of single-level lumbar spinal disease, demonstrating long-lasting benefit. After five-year follow-up, MI-TLIF demonstrated similar improvements in functional outcome scores without increased rates of revision or subsidence. Larger, prospective studies are required to corroborate these findings.
1002
A346: Minimally Invasive Scoliosis Surgery with Trans-Kambin Posterior Oblique Lateral Lumbar Interbody Fusion: Single Surgeon Feasibility Study
Hamid Abbasi 1
1 Inspired Spine, Neurosurgeon, Burnsville, USA
Introduction: Degenerative deformities of the spine have traditionally been treated with extensive open surgeries. However, these open procedures are associated with a high degree of surgical morbidity. In this study, we explore whether clinical improvement in patients with spinal deformities can be achieved using a new minimally invasive surgery (MIS) called oblique lateral lumbar interbody fusion (OLLIF). OLLIF is a MIS single surgeon procedure in which the disc is approached through Kambin’s triangle. OLLIF can achieve correction of spinal deformities through careful cage placement. Material and Methods: This study is a retrospective review of 37 OLLIF surgeries in 36 patients with symptomatic degenerative spinal deformity. Collected perioperative data included surgery time, blood loss, and hospital stay. Follow-up was conducted at least 150 days post surgery. We recorded complications and patient reported outcomes such as Oswestry Disability Index (ODI) and pain scale. Imaging was conducted pre- and post-surgery. Fusion rates and changes in Cobb angle were also measured. Results: A total of 37 surgeries that treated 100 vertebral levels were performed. For two and three level procedures, respectively, the mean blood loss was 83 and 178 ml, the average surgery time was 74 and 158 minutes and the average hospital stay was 2.6 and 3.3 days. The patients ambulated within 24 hours in all but two cases. The patients reported pain improvements on the ten-point pain scale from 8.3 to 3.7 (P < .001) and on the ODI from 53% to 32%. Cobb angles decreased from 16° to 9.3° (P < .001), amounting to 2.5° of correction per level of surgery. Detailed imaging was reviewed by independent radiologists for 24 cases and 100% interbody fusion was achieved along with 71% right posterolateral and 74% left posterolateral fusion. There were three cases of mild nerve irritation/neuropraxia and no infections. Conclusion: OLLIF is a safe and effective MIS technique to correct adult degenerative scoliosis. Unlike alternative procedures, OLLIF is technically less complex than comparable procedures and can safely be used from the thoracolumbar junction to S1.
765
A347: Minimally invasive versus open transforaminal lumbar interbody fusion in obese patients: a propensity score matched study on perioperative, functional and subjective outcomes
Graham Goh 1 , Adriel Tay 1 , Reuben Soh 1
1 Singapore General Hospital, Singapore, Singapore
Introduction: The perioperative benefits of minimally invasive surgery in obese patients have been described. However, there is a paucity of literature on the patient-reported outcomes (PROs), satisfaction and return to work following minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) and Open TLIF in this subgroup of patients. This study aimed to compare the clinical outcomes of obese patients undergoing MIS and Open TLIF. Materials and Methods: Patients who were obese (BMI ≥30.0 kg/m2) and underwent a primary, one- to two-level TLIF were retrospectively reviewed and stratified into two cohorts: Open TLIF and MIS TLIF. The cohorts were matched in a 1:1 ratio for age, sex, body mass index, comorbidity burden, number of levels fused and preoperative PROs using propensity scoring. Operative time, length of stay and perioperative outcomes were recorded. Differences in PROs, including Oswestry Disability Index (ODI), 36-Item Short-Form Physical Component Score (SF-36 PCS), Mental Component Score (SF-36 MCS), Visual Analogue Scale (VAS) back pain, and VAS leg pain, at each postoperative time point were compared between the cohorts using independent sample t-tests. Achievement of minimal clinically important difference (MCID), patient satisfaction assessed using the North American Spine Society questionnaire, and return to work were compared using Chi-square analysis. Revision procedures were recorded at mean follow-up of 10 ± 3.3 years. Results: In total, 236 obese patients were included: 118 Open TLIF and 118 MIS TLIF. The two cohorts were closely matched in terms of demographics, perioperative variables and preoperative PROs. Length of stay was longer in the Open TLIF cohort (7.0 ± 5.2 vs 4.4 ± 2.5 days, P < .001) and there was a trend towards a higher complication rate (14.4% vs 8.5%, P = .075). However, there was no difference in operative time, transfusions or readmissions. Patients who underwent Open TLIF reported worse ODI (P = .043) and VAS leg pain at 2 years, although the latter did not reach statistical significance (P = .095). Achievement of MCID for each PRO, patient satisfaction and return to work were comparable between the cohorts. A total of 8 Open TLIFs and 6 MIS TLIFs were revised (P = .582). Conclusion: Obese patients who underwent MIS TLIF had less perioperative complications, shorter length of stay and improved functional disability compared to a matched group who underwent Open TLIF. However, a similar proportion achieved a clinical meaningful improvement. Patient satisfaction and return to work were also comparable at 2 years.
579
A348: Percutaneous Kyphoplasty Vs Percutaneous Vertebroplasty for Neurologically Intact Osteoporotic Kümmell’s Disease: A Systemtic Review and Meta-Analysis
Baoliang Zhang 1 , Zhongqiang Chen 1 , and Guanghui Chen 1
1 Peking University Third Hospital, Beijing, China
Introduction: Kümmell’s disease (KD) is a relatively rare entity secondary to vertebral compression fracture (VCF), characterized by delayed vertebral collapse and kyphosis. Percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) are widely-used minimally invasive techniques for the treatment of neurologically intact osteoporotic KD, but which one is preferable choice remains controversial. Therefore, a systematic review and meta-analysis should be performed to shed light on the facts regarding the efficacy and safety of both procedures for neurologically intact KD, providing evidence-based medical support for clinical decision-making. Material and Methods: The PubMed, Embase, Web of Science, Cochrane library, Wanfang, CNKI were searched from inception to September 1, 2020, for all randomized controlled trials or cohort studies that compared PVP and PKP in treating KD patients without neurological deficits. All eligible studies were selected based on predesigned screening criteria. Two investigators independently conducted the quality assessment and extracted the data. Fixed-effect and random-effect models were used for pooled analysis according to the heterogeneity. All statistical analysis was performed by Stata software 14.0. Results: Eight eligible studies with a total of 438 KD patients (195 undergoing PKP and 243 undergoing PVP) were included in the final analysis. Patients were followed up for at least one year. Pooled results showed no difference between PKP and PVP in clinical outcomes (short-term and long-term visual analogue scale and Oswestry disability index) and perioperative complications (overall complications, bone cement leakage and new vertebral fracture). Regarding radiographic outcomes, PVP was associated with better improvement in short-term and long-term Cobb’s angle compared to PKP [SMD = -.37, 95% CI (-.64, -.10), P = .007; SMD = -0.34, 95%CI (-.61, -.07), P < .012]. Even though the restoration of vertebral height in PKP group was slightly better than PVP group in the short run [SMD = 0.43, 95%CI (0.14, 0.71), P = .003], there were no significant differences between two groups at the final follow-up (P = 0.186). In addition, PKP required more consumption, including bone cement injection volume [SMD = .50, 95%CI (.27, .73), P < .001], operating time [SMD = 1.80, 95%CI (.67, 2.93), P < .001], fluoroscopy times [SMD = 1.02, 95%CI (1.62, 1.43), P < .001], intraoperative blood loss [SMD = 0.96, 95%CI (.41, 1.91), P < .001] and operation cost [SMD = 31.12, 95%CI (1.48, 60.77), P < .040]. Conclusion: This study demonstrated that PVP was as similar as PKP in clinical outcomes and perioperative complications, which indicated both procedures are effective and safe for treating neurologically intact osteoporotic KD. In addition, PVP could provide better correction of spinal kyphosis and less consumption. Based on the current evidence, we recommended PVP as the superior technique. The future directions of KD treatment relies on the results of randomized controlled trials with higher quality and larger sample sizes.
1700
A349: Prospective Comparative Study of Functional Outcome in Open vs Minimally Invasive Tubular Discectomy for Lumbar Disc Herniation
Akash Shakya 1
1 Dr BAM Hospital, Orthopaedics and Spine Surgery, Mumbai, India
Aim: Aim of the study was to compare the functional outcome of open vs minimally invasive tubular discectomy for lumbar disc herniation. Material and Methods: All patients undergoing discectomy for lumbar disc herniation were prospectively followed for one year. VAS (Visual analogue score), ODI (Oswestry Disability Index) were used to analyse the functional outcome at post-operative period day one, two weeks, One month, three months, Six months and one year. Data was divided into open and minimally invasive group (MIS) and analysed. Result: 218 patients were included in the final analysis. 82 were from MIS group and 136 underwent open discectomy. While pre-operative mean VAS scores were comparable for both the groups, follow up VAS scores were significantly better for MIS group at post-operative day one(P = .001), two weeks(P = .001), One month(P = .001), three months(P = .003) and six months (P = .023). Similarly ODI scores were also significantly better for MIS group at post-operative day one(P = .004), two weeks(P = .001) and one months(P = .003). No significant difference was found between one year VAS scores and ODI scores between the two groups (P > .05). Incidence of dural tear was significantly less (6%) in minimally invasive group compared to open surgery (13.9%) (P = .001). Conclusion: Functional outcome of minimally invasive tubular discectomy for lumbar disc herniating are comparable with open discectomy with significantly improved VAS scores up to 6 months and significantly better ODI scores up to one month and with significant less chances of dural tear.
1265
A350: Stable Low Grade Spondylolisthesis Does not Compromise Clinical Outcomes of Minimally Invasive Tubular Decompression in Patients with Spinal Stenosis
Morsi Khashan 1 , Gilad Regev 1 , Dror Ofir 1 , Khalil Salame 1 , and Zvi Lidar 1
1 Tel Aviv Medical Center, Tel Aviv University, Tel aviv, Israel
Background: Surgical decompression has been shown to be superior to conservative management in lumbar spinal stenosis (LSS) patients. The purpose of the present study is to compare the clinical outcome and complication rates following minimally invasive (MIS) tubular decompression without arthrodesis in patients suffering from LSS with or without concomitant stable low grade degenerative spondylolisthesis. Methods: Ninety six consecutive patients who underwent elective MIS lumbar decompression with a mean follow-up of 27.5 months were included in the study. The data was collected prospectively to our data base. The spondylolisthesis (S) group comprised 53 patients who suffered from LSS with stable degenerative spondylolisthesis, and the control (N) group included 43 patients suffering from LSS without spondylolisthesis. Outcome measures included complications, and revision surgery rates. Pre- and post-operative visual analog scale (VAS) for both back and leg pain was analyzed, and theOswestryDisability Index (ODI) was used to evaluate functional outcome. Results: The two groups were comparable in most demographic and preoperative variables. VAS for back and leg pain improved significantly following surgery in both groups. Both groups showed significant improvement in their ODI scores, one and two years postoperatively. The average length of hospital stay was significantly higher in patients with spondylolisthesis (P-value< .01). There was no significant difference between the groups in terms of post-operative complications and revision surgeries. Conclusions: Our results indicate that MIS tubular decompression may be an effective and safe procedure for patients suffering from LSS, with or without degenerative stable spondylolisthesis.
769
A351: Lumbar Interbody Fusion in Adult Isthmic Spondylolisthesis: Does Minimally Invasive Surgery Benefit Patients Compared with Open Surgery?
Graham Goh 1 and Reuben Soh 1
1 Singapore General Hospital, Singapore, Singapore
Introduction: Isthmic spondylolisthesis is common in younger patients and can be treated with Open or Minimally Invasive transforaminal interbody lumbar fusion (MIS TLIF). While technical and approach-related considerations have received much attention for this pathology, few studies have directly compared the clinical effectiveness between Open and MIS TLIF. This study aimed to compare the patient-reported outcomes (PROs), satisfaction and return to work in patients following Open and MIS TLIF for isthmic spondylolisthesis at minimum 2-year follow-up. Materials and Methods: Patients who underwent a primary single-level TLIF for low-grade isthmic spondylolisthesis were retrospectively reviewed and stratified into two cohorts: Open TLIF and MIS TLIF. The cohorts were matched in a 1:1 ratio for age, sex, body mass index, comorbidity burden and preoperative PROs using propensity scoring. Operative time and length of stay were recorded. Differences in PROs, including Oswestry Disability Index (ODI), 36-Item Short-Form Physical Component Score (SF-36 PCS), Mental Component Score (SF-36 MCS), Visual Analogue Scale (VAS) back pain, and VAS leg pain, at each postoperative time point were compared between the cohorts using independent-sample t-tests. Achievement of minimal clinically important difference (MCID), patient satisfaction assessed using the North American Spine Society questionnaire, and return to work were compared using Chi-square analysis. Results: In total, 136 patients were included: 68 Open TLIF and 68 MIS TLIF. The two cohorts were closely matched in terms of demographics, perioperative variables and preoperative PROs. Operative time was similar, but the MIS TLIF cohort had a shorter length of stay (3.3 ± 1.2 vs 5.4 ± 3.0 days, P < .001). There was no difference in PROs between the cohorts at all time points. The Open TLIF cohort had a higher rate of MCID achievement for SF-36 PCS at 24 months (83.8% vs 64.7%, P = .018), but both cohorts demonstrated similar achievement of MCID for ODI, VAS back pain, VAS leg pain. Patient satisfaction and return to work were also comparable. The Open TLIF cohort took 82.8 ± 66.7 days to return to work while the MIS TLIF cohort took 89.2 ± 76.8 days (P = .695). Conclusion: Patients with low grade isthmic spondylolisthesis who underwent MIS TLIF had a shorter length of stay. However, both MIS and Open techniques produced similar improvements in pain, disability and quality of life. Patient satisfaction and return to work was also comparable at 2 years.
OP40: Deformity-Thoracolumbar (Adolescent) 3
1778
A352: The Analysis of Progression of Disc Degeneration in the Unfused Segments in Post-Operative Adolescent Idiopathic Scoliosis - A 10 Year Follow-Up MRI-Based Study
Ajoy P Shetty 1 , Sridhar J 2 , Rishi Kanna 2 , and Shanmuganathan Rajasekaran 1
1 Ganga Medical Center and Hospitals, Coimbatore, India
2 Ganga Medical Center and Hospitals, Spine Surgery, Coimbatore, India
Introduction: The impact of long-segment fusions on the distal mobile vertebral segments is of major concern. There is currently a paucity of literature on the progression of disc degeneration in the distal un-fused segments in patients with strategic pedicle screw instrumentation. The current retrospective study was thus planned to analyse the progression of the Pfirrmann’s grade in the distal un-fused lumbar segments in postoperative Adolescent Idiopathic Scoliosis (AIS). Methods: A total of 58 patients who underwent surgery for AIS with minimum 6.5-year follow-up (5-15) were included. Coronal Cobb’s angle (CCA), apical translation, lower instrumented vertebra tilt (LIV tilt), lower instrumented vertebra-sacral angle (LIV-Sacral angle), sagittal spinal parameters [Thoracic kyphosis (TK) and lumbar lordosis (LL)]; and pelvic parameters were measured. Disc health was assessed in Magnetic Resonance Imaging (MRI) by Pfirrmann’s grading, Total endplate score (TEPS) and facet degeneration were measured by Fujiwara’s grading. Functional evaluation was performed using SRS 22 score. Results: A total of 58 patients were included in the study. The mean follow-up was 10 years. Based on MRI scan, 43 were included in Pfirrmann’s grade static (PGS) group and 15 in Pfirrmann’s grade progressed (PGP) group. Of the15 patients in PGP group, LIV was L4 in 8, L3 in 3, L1 in 3 and L2 in 1. Fifteen patients in our cohort had a progression of Pfirrmann’s grade. Among these patients, 11 (73.3%) progressed from grade 1 to grade 2; but in 4 patients (26.6%), Pfirrmann’s grade progressed to more than 3. The progression of degeneration did not significantly correlate with the preoperative and postoperative TEPS score, coronal or sagittal parameters. Conclusion: The analysis of progression of the Pfirrmann’s grade in distal un-fused segments did not show any significant correlation with the pre-operative and post-operative coronal or sagittal parameters and the number of unfused segments.
1250
A353: Studies on the Influence of Growth Friendly Implants Used in Eos Treatment on Titanium Ion Release into the Tissue
Anna Danielewicz 1 and Michał Latalski 1
1 Medical University, Childrens' Orthopeadic, Lublin, Poland
Introduction: The long-term cumulative effects of the presence of implants after surgical treatment of Early-Onset Scoliosis (EOS) may be harmful.The aim of the study is to evaluate the influence of different growth-friendly systems used for surgery in EOS on the level of titanium ions (Ti) in samples tissues taken intraoperatively. Material and Methods: The study group included 77 patients (mean 13,5 yo) who were surgically treated with implants made of Ti-6Al-4V titanium alloy. The stabilization covered on average 11 segments. Mean observation time was 3,25 ± 1,14 years. Patients were divided into 5 groups: traditional growing rods (TGR), guided growth system, VEPTR, revision group (patients who had a fracture of the implant) and a control. The concentration of Ti was examined on Inductively Coupled Plasma Optical Emission Spectrometry. Results: There was a higher content of Ti in clean tissue and in the blood in boys vs girls (0.0068 mg/g vs 0.0035 mg/g and 4, 1962 μg/L vs 3.6465 μg/L respectively). Ti in contaminated tissue was the highest in the GGS group than VEPTR, revision group and TGR (3.855 mg/g, 1.456 mg/g, 1.022 mg/g and 0.52 mg/g respectively). Ti in the blood increases was the highest in the GGS group than VEPTR, revision group and TGR (14.12 ± 0.12 μg/L, 8.875 ± 3.65 μg/L, 4.435 μg/L and 3.454 μg/L respectively). There was no correlation with the number of implanted anchors and the observation time. Conclusion:(1). Movement between implants affects the number of Ti released. (2). The duration of implants in the child's body doesn’t affect the content of Ti, putting this aspect of treatment among arguments for not delaying the start of surgical treatment of patients with EOS. (3). Mechanical failure to the implant has no significant effect on increasing the content of Ti.
1015
A354: What a Stranded Whale with Scoliosis can Teach us About Human Idiopathic Scoliosis
Steven de Reuver 1 , Lonneke IJsseldijk 2 , Jelle Homans 1 , Dorien Willems 3 , Stefanie Veraa 3 , Marijn van Stralen 4 , Marja Kik 2 , Moyo Kruyt 1 , Andrea Gröne 2 , and René Castelein 1
1 University Medical Center Utrecht, Department of Orthopedic Surgery, Utrecht, The Netherlands
2 Utrecht University, Division of Pathology, Department of Biomolecular Health Sciences, Faculty of Veterinary Medicine, Utrecht, The Netherlands
3 Utrecht University, Division of Diagnostic Imaging, Department of Clinical Sciences, Faculty of Veterinary Medicine, Utrecht, The Netherlands
4 University Medical Center Utrecht, Imaging Division, Utrecht, The Netherlands
Introduction: Scoliosis is a deformation of the spine that may have several known causes, but only humans can develop scoliosis without any obvious underlying cause. This is called ‘idiopathic’ scoliosis and is the most common type. Recent observations showed that human scoliosis, regardless of its cause, has a uniform three-dimensional anatomy. We hypothesize that scoliosis is a universal compensatory mechanism of the spine, independent of cause and/or species. Material and Methods: We had the opportunity to study the rare occurrence of scoliosis in a whale that stranded in July 2019 in the Netherlands. A multidisciplinary team of biologists, pathologists, veterinarians, taxidermists, radiologists and orthopedic surgeons conducted necropsy and CT-imaging analysis. In areas of the spine that did not show underlying anatomical changes, we analyzed the compensatory curves in 3D and compared the morphology with the non-scoliotic spine of 10 control whales. Results: The stranded animal was a common minke whale (Balaenoptera acutorostrata) and was a 403 cm long, 530 kg female juvenile, with an estimated age between 0.5-4 years. The most likely cause of death was considered to be acute recent blunt trauma. Visual inspection showed epiphysiolysis at the left-side of the lower endplate of vertebra L3, a burst upper endplate at the right-side of vertebra L4, fractured spinous processes of vertebrae L1 to L6, severely wedged vertebrae T11 and T12 and detachment of the transverse processes at multiple levels. Two traumatically deformed vertebrae had led to an acute post-traumatic scoliosis, which had initiated the development of compensatory curves in regions of the spine without anatomical abnormalities. The 3D analysis of the compensatory curves showed a rotation of the vertebral bodies in the transverse plane into the convexity of the curve. The mean anterior-posterior length discrepancy (AP%) of the total compensatory curvature was +9.4% in the whale, indicating a lordosis. This is significantly different from the kyphosis in the same part of the spine in the non-scoliotic control group, with a total AP% of -2.1 ± 0.4% (P < .001). On the contrary, the bony morphology of the vertebral bodies was similar to the controls; the vertebral body AP% of the whale was -2.5%, which was comparable to the kyphotic shape of the vertebral bodies in controls with -1.8 ± 0.8% (P = .429). Almost all anterior lengthening was present in the intervertebral discs, as the disc AP% in the compensatory curvature of the whale was +99.5%, which meant a lordotic shape of the intervertebral discs with an anterior length almost twice the posterior length. This is in sharp contrast to the kyphosis in the discs of controls with -4.6 ± 5.0% (P < .001). Conclusion: Three-dimensional analysis of these compensatory curves showed strong resemblance with different types of human scoliosis. This indicates that any decompensation of spinal equilibrium can lead to a uniform response, regardless of underlying cause or species. The unique biomechanics of the upright human spine, with significantly decreased rotational stability, explains why only in humans this universal mechanism of scoliosis can occur in an ‘idiopathic’ way.
1116
A355: Management of Progressive Neuromuscular Scoliosis and Respiratory Distress in a Child with Nemaline Rod Myopathy
Balamurugan Thirugnanam 1 , Ajay Kumar Shetty Papanna 1 , and Vidyadhara Srinivasa 1
1 Manipal Hospitals, Spine Care, Bengaluru, India
Introduction: Nemaline Rod Myopathy (NRM) is the commonest among non-dystrophic congenital myopathies. Clinical presentation is highly variable due to variable mutations in large number of genes. Variable clinical presentations ranging from normal lifespan with mild symptoms to neonatal death have been reported. Children with NRM have generalized muscle weakness with predilection to neck, face, axial and proximal extremity muscles. Respiratory muscle weakness is the most prominent feature and affects the overall prognosis and survival. Even ambulant and mildly affected patient may develop unsuspected hypoxia especially during night and hence requires assisted mechanical ventilation. Materials and Methods: Eleven-year-old wheelchair bound girl presented with progressive breathing difficulty, deformity of back, and worsening sitting balance of 2 years duration. Following an uneventful normal delivery to a non-consanguineously married couple, the parents had noticed the child to grow normally except for delayed motor milestones. The child from the age of 3-years started developing repeated respiratory difficulties and was started on nocturnal BiPAP ventilator support. In view of generalized motor weakness and respiratory difficulty, the muscle biopsy done revealed NRM. The child had multiple episodes of respiratory worsening and admission to ICU. The child presented to Spine Care for the management of progressive spinal deformity affecting the sitting balance on wheel chair. Results: We corrected the rigid right Thoracolumbar Scoliosis T3-L1 (Cobb angle 87°) successfully using multi-modal intra-operative neuromonitoring with multiple Ponte osteotomies and instrumented fusion T2-ilium. Following surgery she was able to sit independently, able to breathe better and requiring less BiPAP support. At 2-years follow up, her breathing reserve improved significantly and not even requiring nocturnal ventilator support. Conclusion: To the best of our knowledge this is the first reported case of a severe rigid scoliosis in a child with NRM managed surgically successfully. Surgical management of these patients requires multidisciplinary approach for successful outcome in view of respiratory failure. Deformity correction will improve the respiratory reserve of child and may even obviate the need of nocturnal mechanical ventilation support.
1213
A356: Leaving Out Often Difficult to Place Proximal Thoracic Concave Apical Screw(S) in Adolescent Idiopathic Scoliosis: Are these Screws Necessary?
Joseph Osorio 1 , Meghan Cerpa 2 , James Lin 3 , Simon Morr 2 , Griffin Baum 4 , Scott Zuckerman 2 , and Lawrence Lenke 2
1 University of California San Diego, San Diego, USA
2 Columbia University Medical Center, New York, USA
3 Mount Sinai, New York, USA
4 Northwell Health, New York, USA
Summary: Proximal thoracic (PT) concave apical screw placement in AIS patients are challenging due to pedicle morphology, wound depth, concavity trajectory and spinal cord location directly adjacent to the medial pedicle wall. We evaluated 40 patients with Lenke Type 1-2 AIS curves, 63% of which had PT concave apical screw(s) purposely left out. The most common levels left out were T5 (30%) and T6 (53%). No difference in correction of PT (P = 0.44) and main thoracic(MT) (P = .93) curves between groups was seen. Hypothesis: Proximal thoracic (PT) concave apical screw(s) in AIS patients are often difficult to place, carries high neurologic risk, and adds operative time with little to no benefit seen in deformity correction. Thus these screws can be left out of AIS constructs involving the PT region. Study Design: Retrospective, single-institution. Introduction: In AIS patients, the concave PT pedicles are often small (Type C or D) and rotated, making placement challenging. The spinal cord is also draped along the concave pedicle-vertebral body junction thus rendering even a slight medial trajectory/breach a potential neurologic complication. Additionally, concave PT curve correction occurs with distraction distributed away from the apex, making the apical screw unnecessary. We sought to evaluate whether leaving these concave apical PT screw(s) out affected overall curve correction. Methods: AIS patients with Lenke Type 1-2 curves with UIV of T4 or cephalad were identified. Mean age was 15.3 yrs, 27 (68%) had Type 1 curves, and 13 (33%) had Type 2. The UIV was T1 in 1 (3%), T2 in 11 (28%), T3 in 14 (35%), and T4 in 14 (35%) pts. The levels where PT apical screws were left out were analyzed using Cobb angles for PT and main thoracic (MT) curves (pre- and postop standing radiographs). Results: Of 40 AIS patients, 25 (63%) had PT concave apical screw(s) left out: 59% of Type 1, and 69% of Type 2 curves. Screws were left out at the following levels: T4-15%, T5-30%, T6-53%, T7-3%. Preoperative PT and MT Cobb angles of both groups were similar preoperatively. Postoperative PT correction was similar between both groups: screws left out 10° (2-26) vs all screws 9° (3-23), P = .44. Postoperative MT correction was also similar between both groups: screws left out 10° (1-31) vs all screws 10° (1-18), P = .93). Conclusion: Leaving out the proximal thoracic concave apical pedicle screw(s) in Lenke Type 1-2 AIS showed no difference in correction compared to all levels instrumented. Leaving out screws theoretically minimizes risk of neurologic complications and decreased OR time to place these challenging screws without sacrificing coronal correction. Take Home Message: Leaving out the PT concave apical pedicle screw(s) in Type 1/2 AIS patients has no effect on coronal correction while avoiding unnecessary risks of these challenging and neurologically risky screws.
69
A357: The Use of 3 Rods in Correcting Severe Scoliosis
Brett Rocos 1 , Eliane Rioux-Trottier 1 , Masayoshi Machida 1 , Amit Sigal 2 , Jim Kennedy 3 , David Lebel 1 , and Reinhard Zeller 1
1 Hospital for Sick Children, Department of Orthopaedic Surgery, Toronto, Canada
2 Dana Children's Hospital, Tel Aviv, Israel
3 Children's Health Ireland at Crumlin, Dublin, Ireland
Introduction: The three rod technique, utilising a short apical concavity rod is an option to achieve controlled correction in severe scoliosis. We describe this technique, the complications encountered, and the long term outcomes. Materials and Method: All paediatric patients who underwent corrective surgery for scoliosis ≥ 100° using 3 parallel rods were included. Radiographs were assessed to evaluate the correction and clinical records examined for any loss of correction, complications, revision procedures or neuromonitoring events. Results: 27 patients met the inclusion criteria. All underwent posterior instrumented fusion, 5 underwent a circumferential fusion to prevent crankshaft phenomenon and 3 underwent preoperative halogravity traction. The main thoracic curve (MT) measured 112° (100- 145°), the proximal thoracic (PT) 48° (20- 75°) and thoracolumbar (TL) 22° (2- 97°). 4 patients with an MT not significantly different to the remainder of the group (P = 0.73) underwent anterior fusion. Eleven patients showed loss of motor evoked potentials, all of which returned to within 25% of baseline. All patients had normal postoperative neurology. One patient underwent removal of hardware for late infection. The cohort showed a 47% (95% CI 42-53%) correction of their MT. PT was corrected by 15° (95% CI 10- 19) and TL 23° (95% CI 16- 31°). There was no significant loss of correction at 2 years. Conclusion: Our series suggests that three rod constructs lead to a 50% correction of severe curves, that three column osteotomies may not be necessary, and that the technique is safe and effective for the correction of severe scoliosis.
28
A358: Development of Thoracic Kyphosis After High Implant Density Posterior Correction and Fusion for Adolescent Idiopathic Scoliosis
Peter Obid 1 , Andreas Conta 2 , Philipp Drees 3 , and Thomas Niemeyer 1
1 Asklepios Paulinen Klinik, Spine and Scoliosis Center, Wiesbaden, Germany
2 University of Mainz, Mainz, Germany
3 University of Mainz, Department of Orthopaedics and Traumatology, Mainz, Germany
Introduction: Posterior correction and fusion provides good results in the coronal plane. But pedicle screw based instrumentations tend to flatten the spine. Previous studies on thoracic kyphosis (TK) restoration have produced mixed findings on the ability of posterior instrumentations to achieve that goal. With derotation the anterior column is lengthened which sacrifices kyphosis. Although there is a paucity of evidence to prove that this affects long-term outcome and quality of life, it is logical to assume that TK restoration may optimize global sagittal alignment and slow down lumbar and cervical disc degeneration. Material and Methods: Radiographs of 100 consecutive patients that underwent posterior correction and fusion for adolescent idiopathic scoliosis (AIS) at a single center were analyzed. 5.5 mm titanium or cobalt chromium rods were used. Thoracic Kyphosis (TK) was measured preoperatively and two years postoperatively for the whole group, and separately for hypo-, normo- and hyperkyphotic patients (according to the Lenke classification). A one-sided one-sample t-test was performed to compare pre- and postoperative values. Results: For all patients mean TK significantly decreased by 3.8° ± 3.4 (P = .005). For hyperkyphotic patients (n = 9) mean TK significantly decreased by 18.9° ± 3.8 (P = .006). For normokyphotic patients (n = 75) mean TK significantly decreased by 3.9° ± 3.2 (P = .001). For hypokyphotic patients (n = 16) mean TK significantly increased by 4.9° ± 2.4 (P = .005). Conclusion: The results are ambivalent which is consistent with the literature. Except for the hyperkyphotic group the differences are within or close to the range of a measurement error. The main conflict of implant stiffness versus lengthening the anterior column with derotation remains unsolved. Additionally, it is difficult to define an optimal TK for any given patient. TK restoration remains a challenge. Even with translation maneuvers and the use of cobalt chromium rods, creation of kyphosis is difficult. However, in patients that are already hypokyphotic it is possible to achieve good coronal correction without sacrificing additional kyphosis.
1274
A359: How Close are We to “Complication Free” Adolescent Idiopathic Scoliosis Fusion Surgery?
Jay Reidler 1 , Meghan Cerpa 1 , Joseph Lombardi 1 , Zeeshan Sardar 1 , and Lawrence Lenke 1
1 Coluia University Medical Center, New York, USA
Summary: This study examines recent rates of complication and readmission following posterior spinal fusion for adolescent idiopathic scoliosis (AIS). We observed no readmissions, reoperations, or major medical or surgical complications in this series of 76 consecutive cases. Hypothesis: We hypothesized that posterior spinal fusion for treatment of AIS currently has lower complication and readmission rates than previously reported. Study Design: Consecutive single surgeon series. Introduction: Historically, rates of complication associated with posterior spinal fusion for AIS have been reported to range between 5 to 10%, with 30-day unplanned readmission rates around 3%. With the development of improved intraoperative techniques and perioperative care protocols, one would expect these rates to have improved in recent years. Yet, little is known about current rates of complication and readmission. Methods: We collected surgical and postoperative data on 76 consecutive cases of posterior spinal fusion for AIS using pedicle screw constructs in patients aged 11-18 years who underwent surgery between 2015 and 2019. All surgeries were performed in a tertiary children’s hospital (43%) or in a tertiary spine-focused hospital (57%) by a single surgeon with greater than 25 years experience in deformity surgery. Results: Mean age was 15.8 ± 1.8 yrs and time since surgery was 2.1 ± 1.2 yrs. An average of 11 ± 2 levels were instrumented/fused per case and the distribution of Lenke classification types was: 1 = 39%, 2 = 26%, 3 = 12%, 4 = 1%, 5 = 12%, 6 = 9%. The mean surgical time was 4.3 ± 0.8 hour, estimated blood loss was 565 ± 291 cc, and length of stay was 3.6 ± 0.8 days. The rates of readmission and/or reoperation were 0%, with up to 4 year follow up for the earliest patients. There were no major medical or surgical perioperative complications. There were two minor complications (3%) including 1 durotomy and 1 transient postoperative ileus. Seventeen patients (22%) received blood transfusions. In 4 cases (5%), there were concerning neuromonitoring changes that resolved following corrective maneuvers and there were no postoperative neurologic deficits. Conclusion: In this consecutive series of AIS spinal fusion patients over a 4 year period, we observed no readmissions, reoperations, or major medical or surgical complications. This current state of the art information will be important for patient counseling and comparison as newer techniques, such as non-fusion options, become available. Take Home Message: Surgeons can potentially achieve extremely low complication rates when treating AIS with posterior spinal fusion. This must be considered as alternatives to this gold-standard treatment are investigated in the future.
729
A360: Radiographic Outcomes of 3-D Alif Stand-Alone Cages Implementation for Ads Patients (Retrospective Study)
Anton Denisov 1 , Dmitry Ptashnikov 1 2 , Nikita Zaborovskii 1 , Sergei Masevnin 1 , and Dmitry Mikhaylov 1
1 National Medical Center of Traumatology and Orthopaedics n.a. Vreden R.R, Bone oncology and spinal surgery, Saint-Petersburg, Russian Federation
2 North-Western State Medical University named after I.I. Mechnikov, Traumatology and Orthopaedics, Saint-Petersburg, Russian Federation
Introduction:Is well known that the usage of minimal invasive surgery (MIS) techniques for adult degenerative scoliosis (ADS) require correct placement of interbody cages.For the purpose of improving segmental and total lordosis were invented interbody cages with certain lordotic angles which contribute not only to appropriate correction degree but although to indirect decompression by increasing of intervertebral heights. Implementation of 3D printing in nowadays practice has allowed more individualize preoperative planning and implant preparation for achieving definite goals of spinal surgery. In case of ADS, asymmetric lordotic titanium cages could help not only in sagittal but in frontal balance correction that can improve radiographic outcomes. The goal of this study is to evaluate changes of radiographic parameters at patients with ADS whom performed anterior correction with asymmetric titanium lordotic cages. Material and Methods:This is a single center retrospective study of 50 patients (19 men, 31 women) who underwent oblique and anterior interbody fusion using titanium custom asymmetric lordotic cages for ADS correction. Were formed 2 groups according to SRS-Schwab classification (2012): first group 25 patients with PI-LL mismatch moderate and second group 25 patients with PI-LL mismatch severe.Period of observation from april 2018 to august 2020. Standing full spine and conventional radiographs at pre-op and 1-6-12-mounth follow-up were performed. Observed radiographic parameters: SVA, LL, PT, central line and Cobb angle for frontal deformation. Intragroup results were compared using t Student test. And intergroup results were evaluated with U Mann-Whitney test. Results:21patients underwent 3-level MIS ALIF, OLIF, and 29 underwent 2-level. The mean age was 58 years, with prevalence of 64% women. In both groups, frontal deformation correction was achieved. Was found statistical difference between pre-op and post-op radiographic parameters in first (P = .019,P <.05) and the second (P = .042,P <.05) group. Comparing results entre groups we found that mean post-op values of SVA, PT, LL were significantly higher in the first group (mean SVA1= 25 ± 8 mm, mean SVA2= 87 ± 19 mm,P = .018; mean PT1=14 ± 30, mean PT2= 28 ± 40,P = .032; mean LL1=47 ± 20mean LL2=31 ± 10,P = .024). In addition, 74% of patients of the second group subsequently required posterior transpedicular fixation and Smith-Peterson Osteotomy (SPO) performing for achieve full sagittal correction. Wherein in the first group only 18% patients were held second stage surgery. Conclusion:Titanium custom asymmetric lordotic cagesprovided significant increase in sagittal balance correction among patients with moderate deformity (first group), instead of the second group where the majority of patients with severe deformations for reasons of non-achieved significant improvement of correction required additional surgery.
References
1. Kim YJ, Bridwell KH, Lenke LG, et al. Pseudarthrosis in primary fusions for adult idiopathic scoliosis: incidence, risk factors, and outcome analysis. Spine. 2005; 30: 468-474.
2. Shaffer AD, Shonuga OA, Hirsch BP, et al. Sclerostin antibody enhances spine fusion in a rat posterolateral transverse process fusion model: preliminary results. Proc 33rd Annual Meeting of the American Society for Bone and Mineral Research, San Diego, CA, 2011, p S517 (Abstract MO0461).
3. Boden SD, Schimandle JH, Hutton WC. An experimental lumbar intertransverse process spinal fusion model. Radiographic, histologic, and biomechanical healing characteristics. Spine (Phila Pa 1976). 1995 Feb 15;20(4):412-20.