

Abstract
Lesions to the shoulder rotator cuff may have several configurations, and are divided and classified according to the size of the lesion, the tendon involved, its combinations and whether there is possibility of repair. Irreparable subscapular lesions, as well as irreparable anterosuperior lesions, may generate shoulder dysfunction due to loss of humeral head depressants, causing pain and functional limitation. Myotendinous transfers are among the therapeutic alternatives, and the most studied and widespread in recent decades is the transfer of the pectoralis major to the minor tuberosity. However, some anatomical studies suggest that the latissimus dorsi is a more appropriate alternative for the treatment of these lesions because it presents force vectors more similar to those of the subscapularis, besides presenting promising results in the clinical evaluations with short follow-up. The present work aims to describe the surgical technique developed for transfer of the latissimus dorsi in cases of irreparable subscapular and anterossuperior lesions to the rotator cuff.
Keywords: shoulder/surgery, rotator cuff, tendon transfer, tendon injuries
Introduction
Lesions to the rotator cuff of the shoulder have several configurations, which are classified according to the size of the lesion, as well as the tendons involved and their reparability. 1 2 Initial subscapularis lesions may go clinically unnoticed, causing treatment delay and evolving to a retracted lesion associated with fatty degeneration of the muscular belly, thus becoming irreparable. 1 Their association with lesions to the anterior part of the supraspinatus is not uncommon, and characterize what is called anterosuperior lesions. 3 In these cases, loss of humeral head depressants is observed, leading to anterosuperior instability, generating pain and dysfunction in the shoulder. 3
The surgical treatment alternatives for irreparable subscapularis lesions include muscle transfers such as those of the pectoralis major, pectoralis minor and latissimus dorsi. 2 4 For patients who present the condition associated with glenohumeral osteoarthritis, reverse arthroplasty should be the alternative, acting both in the resolution of joint degeneration and in the treatment of the dysfunction resulted from the cuff injury. 4
The most studied and widespread technique for the treatment of irreparable subscapularis lesions is the transfer of the pectoralis major to the minor tuberosity, presenting favorable and long-term clinical results. 1 5 6 7 However, based on anatomical studies 8 some surgeons believes that the tendon of the latissimus dorsi presents a vector closer to that of the subscapularis because it also originates from the posterior wall of the thorax differently from the pectoralis major, which originates from the anterior wall and presents a vector of almost orthogonal force to that of the anterior part of the rotator cuff. 8 In an anatomical study in cadavers, Elhassan et al. 8 demonstrated that the transfer of the latissimus dorsi to subscapular lesions is anatomically possible and with a low risk of nerve injury. Thus, the purpose of the present work is to describe the surgical technique developed by the Santa Casa de Porto Alegre Shoulder Surgery Group for the transfer of the latissimus dorsi in the subscapularis and/or anterosuperior irreparable lesions to the rotator cuff.
Description of the Technique
Video 1 Transfer technique of the LD in anterosuperior injury of the rotator cuff. Irreparable subscapularis lesion and reparable supraspinatus lesion. Color video.
After performing interscalenic regional block and general anesthesia, the patient is placed in the beach chair position with the aid of elbow support. The deltopectoral approach is performed with an incision of approximately 7 cm in the anterior region of the shoulder to identify the irreparable subscapularis lesion. The coracoacromial ligament is preserved to prevent anterosuperior migration of the humeral head, and, if the long cord of the biceps is intact, tenotomy with or without tenodesis is performed. The tendon of the latissimus dorsi is identified immediately distal to the subscapularis, medial to the long cord of the biceps, and posterior to the pectoralis major. The proximal 2-cm tenotomy of the pectoralis major is performed ( Figure 1 ) for adequate exposure of the distal portion of the latissimus dorsi that often has an arciform insertion ( Figure 2 ). Next, the tendon of the latissimus dorsi of the larger round is released with the aid of a Freer elevator. This stage is important, because the tendons may have an insertion or an almost joined fascia, and if the latissimus dorsi is not well released from the Teres major, this will restrain its proximal excursion to the humerus head. Following this, the disinsertion of the latissimus dorsi from the humerus is made by means of a delicate and sharp osteotome and the preparation of a bone chip in its proximal portion, with care in order not to violate the insertion of the Teres major ( Figure 1 ). Then, the collection of the tendon is performed using a scalpel with a #15 blade adjacent to the bone so there is no graft loss. In this step of the graft collection, it is important that the distal portion of the insertion of the latissimus dorsi is adequately visualized, so that the collection is not finished before its end, consequently avoiding an amputation of the distal part of the graft, which can restrain the excursion and quality of the tendon at the time of insertion ( Figure 2 ). Next, the repair of the tendon of the latissimus dorsi with two Krakow-type sutures with non-absorbable wires (Ethibond 5, Ethicon, Inc., Cincinnati, Ohio, US) is performed at each edge of the tendon, leaving the central part free, avoiding some impairment in vascularization and healing potential ( Figure 3 ). Then, the muscle part of the graft is released with a Cobb elevator to improve the excursion and length of the tendon, taking care not to put at risk the neurovascular structures that are medial and anterior to the latissimus dorsi, like the radial nerve. In the next step, the excursion of the latissimus dorsi is tested, and the most proximal insertion point is delimited. Then, the lesser tubercle and the anterior portion of the greater tubercle (in the anterosuperior lesions) are decorticated with a Leksell Bone Roungeur and the latissimus dorsi graft is transfered and fixated with 2 transosseous stitches at the most proximal point of the decorticated bed of the lesser tubercle, and, in some cases, in the anterior portion of the greater tubercle ( Figure 4 ). A few more transosseous stitches are made by fixing the tendon from the latissimus dorsi to the humeral head if necessary, so that there is adequate coaptation of the graft on its larger surface in the bone bed. The subscapularis stump is repaired at the medial edge or under the tendon of the transferred latissimus dorsi, in an attempt to improve the tension of the anterior wall of the cuff. If possible, other cuff injuries (supraspinatus and infraspinatus) are repaired by the same approach, also with transosseous stitches. ( Figure 5 ). Finally, the proximal part of the tenotomized pectoralis major is sutured ( Video 1 ). After closing by planes and dressing, the patient is immobilized with a sling with abductor cushion developed by the Santa Casa de Porto Alegre Shoulder Surgery Group to maintain the limb in a functional neutral position. A video of the technique is attached ( Video 1 ).
Fig. 1.

Drawing of the irreparable anterosuperior lesion with pectoralis major tenotomy for the adequate exposure of the latissimus dorsi (LD) and its collection with a bone chip.
Fig. 2.

Transoperative photo of deltopectoral pathway showing the distal portion of the LD (black asterisk) with the tenotomized pectoralis major (white arrow).
Fig. 3.

Drawing of the LD graft with passage of two Krakow-type suture lines with Ethibond thread number 5.
Fig. 4.

Transoperative photo showing graft insertion (LD) (white asterisk) in the smaller tube of the humerus (black arrow).
Fig. 5.
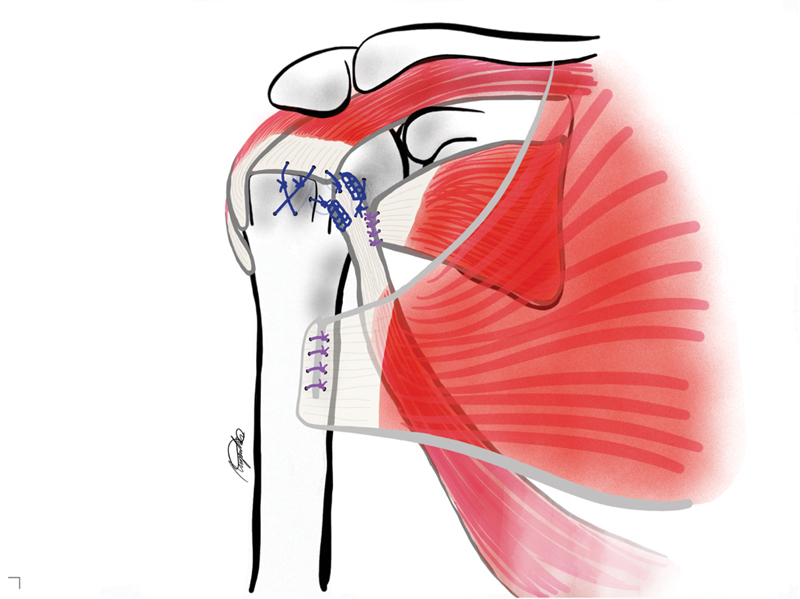
Drawing of the final suture scheme of the graft inserted in the smaller tubercle of the humerus, repair of anterior lesion of the supraspinatus, repair of the subscapularis stump in the LD, and suture of the tenotomized part of the pectoralis major.
The postoperative management is performed with maintenance of the sling for four to six weeks. During this period, the patient is instructed to perform the flexion-extension of the elbow with the arm next to the body already on the first postoperative day. After the removal of the sling, passive movements are recommended, with the patient evolving to active mobility. Muscle-strengthening exercises are recommended only after the 12th postoperative week.
Final Considerations
The transfer of the latissimus dorsi in anterosuperior lesions of the rotator cuff ( Video 1 ) is a new technique that has been shown to be viable, low-cost and without short-term postoperative complications. In addition, patients treated with this technique have reported a high satisfaction rate, and it was also possible to use it for patients with associated posterosuperior lesions. Further studies are needed to evaluate the efficacy and technical reproducibility compared to other treatment methods, as well as their long-term clinical results.
Agradecimentos
Ao dr. Augusto Medaglia, pela elaboração e desenho das ilustrações referentes à técnica cirúrgica, e ao dr. Rodrigo Py Gonçalves Barreto, pela colaboração no processo de revisão e formatação do manuscrito.
Acknowledgements
We would like to thank Dr. Augusto Medaglia for the development and drawingof the illustrations related to the surgical technique, and Dr. Rodrigo Py Gonçalves Barreto for the collaboration in the process of revision and formatting of the manuscript.
Funding Statement
Suporte Financeiro Não houve suporte financeiro de fontes públicas, comerciais, ou sem fins lucrativos.
Conflito de Interesses Os autores declaram não haver conflito de interesses.
Trabalho desenvolvido no Departamento de Ortopedia e Traumatologia, Grupo de Cirurgia do Ombro da Santa Casa de Porto Alegre, Porto Alegre, RS, Brasil.
Work developed at the Shoulder Surgery Group, Department of Orthopedics and Traumatology, Santa Casa de Porto Alegre, Porto Alegre, RJ, Brazil.
Referências
- 1.Resch H, Povacz P, Ritter E, Matschi W. Transfer of the pectoralis major muscle for the treatment of irreparable rupture of the subscapularis tendon. J Bone Joint Surg Am. 2000;82(03):372–382. doi: 10.2106/00004623-200003000-00008. [DOI] [PubMed] [Google Scholar]
- 2.Omid R, Lee B. Tendon transfers for irreparable rotator cuff tears. J Am Acad Orthop Surg. 2013;21(08):492–501. doi: 10.5435/JAAOS-21-08-492. [DOI] [PubMed] [Google Scholar]
- 3.Kany J, Guinand R, Croutzet P, Valenti P, Werthel J D, Grimberg J. Arthroscopic-assisted latissimus dorsi transfer for subscapularis deficiency. Eur J Orthop Surg Traumatol. 2016;26(03):329–334. doi: 10.1007/s00590-016-1753-3. [DOI] [PubMed] [Google Scholar]
- 4.Greenspoon J A, Petri M, Warth R J, Millett P J. Massive rotator cuff tears: pathomechanics, current treatment options, and clinical outcomes. J Shoulder Elbow Surg. 2015;24(09):1493–1505. doi: 10.1016/j.jse.2015.04.005. [DOI] [PubMed] [Google Scholar]
- 5.Konrad G G, Sudkamp N P, Kreuz P C, Jolly J T, McMahon P J, Debski R E. Pectoralis major tendon transfers above or underneath the conjoint tendon in subscapularis-deficient shoulders. An in vitro biomechanical analysis. J Bone Joint Surg Am. 2007;89(11):2477–2484. doi: 10.2106/JBJS.F.00811. [DOI] [PubMed] [Google Scholar]
- 6.Moroder P, Schulz E, Mitterer M, Plachel F, Resch H, Lederer S. Long-Term Outcome After Pectoralis Major Transfer for Irreparable Anterosuperior Rotator Cuff Tears. J Bone Joint Surg Am. 2017;99(03):239–245. doi: 10.2106/JBJS.16.00485. [DOI] [PubMed] [Google Scholar]
- 7.Elhassan B, Ozbaydar M, Massimini D, Diller D, Higgins L, Warner J J. Transfer of pectoralis major for the treatment of irreparable tears of subscapularis: does it work? J Bone Joint Surg Br. 2008;90(08):1059–1065. doi: 10.1302/0301-620X.90B8.20659. [DOI] [PubMed] [Google Scholar]
- 8.Elhassan B, Christensen T J, Wagner E R. Feasibility of latissimus and teres major transfer to reconstruct irreparable subscapularis tendon tear: an anatomic study. J Shoulder Elbow Surg. 2014;23(04):492–499. doi: 10.1016/j.jse.2013.07.046. [DOI] [PubMed] [Google Scholar]




