Abstract
Objective The present paper aims to evaluate the use of a 5% lidocaine patch to treat neuropathic pain after orthopedic procedures in comparison with therapeutic massage over surgical incisions.
Methods This is a prospective, randomized clinical trial with 37 patients who underwent orthopedic surgery from January 2015 to February 2017. The study included subjects aged 13 to 70 years old who underwent foot and ankle orthopedic surgery and presented neuropathic pain or hypersensitivity at the surgical incision site for at least 90 days after the procedure. All patients were assessed for pain (using the visual analog scale [VAS]) and quality of life (with the SF-36 questionnaire) at the beginning of the treatment and after 30, 60, and 90 days.
Results Although the treatment improved pain in both groups, subjects using the lidocaine patch presented greater pain reduction over time. There were no statistically significant differences in the SF-36 questionnaire, with no significant evidence regarding functional capacity, physical aspects, vitality, emotional aspects, social aspects, general health condition, and mental health. The great advantage of the patch was the degree of personal satisfaction of the patients, with statistical relevance, probably due to the easy application and psychological effect of a drug therapy.
Conclusion Lidocaine patches and massages are effective treatment methods for reducing scar tissue pain, with similar outcomes. The patches improved the degree of patient satisfaction. Level of Evidence 1. Prospective randomized clinical trial.
Keywords: orthopedic procedures, pain, neuralgia, lidocaine, massage
Introduction
Chronic postoperative pain, defined as persistent pain at surgical incision sites for 3 months after the procedure, is a frequent complaint in orthopedic practice. 1 Virtually 50% of patients undergoing orthopedic surgery are affected by this syndrome. Arthrodesis, knee arthroplasty, and osteosynthesis for leg fractures are the surgeries with the highest risk of development of chronic postoperative pain. However, any orthopedic surgery may result in this condition; 2 its treatment constitutes a challenge for the surgeon, since it requires knowledge on the several pain mechanisms and pharmacological options available. Most patients end up not receiving adequate treatment and present with chronic pain, which directly affects the doctor-patient relationship, leading to dissatisfaction, lower adherence to complementary therapies, and worse clinical outcomes and parameters.
Several pharmacological modalities have been proposed as alternatives for chronic postoperative pain treatment, including tricyclic antidepressants, selective serotonin reuptake inhibitors, gabapentin, pregabalin, and opioids. 3 A recently introduced 5% lidocaine patch acts as a mechanical barrier and pharmacologically inhibits sodium channels. Its use is associated with a medium- to long-term desensitization of pain receptors. Lidocaine patches are considered a first-line medication in patients with neuropathic pain or post-herpetic neuralgia (PHN), and it was superior to pregabalin in these subjects. 3 4 5
Nonpharmacological measures have also been successful in the treatment of chronic scar tissue pain, especially manual massage, performed by the patient using circular movements over the scar area for 10 minutes, 2 or 3 times a day. 6 A recent literature review reported the positive effect of massage on surgical scars in 90% of the patients treated for 30 to 180 days. 7 The present study aims to evaluate the use of a lidocaine patch to treat localized neuropathic pain in scar tissue of patients submitted to orthopedic procedures in comparison with therapeutic massage over surgical incisions; in addition, the social impact of the treatment was assessed through satisfaction scales and functional classifications.
Material and methods
This is a prospective, randomized clinical trial with 37 patients who underwent orthopedic surgery from January 2015 to February 2017 after approval by the Ethics Committee under the number CAAE 64900217000005488. Patients aged between 13 and 70 years old, submitted to foot and ankle orthopedic surgeries and presenting with neuropathic pain or hypersensitivity at the surgical incision site for at least 90 days after the procedure were included. Patients outside this age range, presenting allergy to lidocaine, skin conditions and/or lesions, altered bone consolidation (delayed consolidation or pseudarthrosis), or incision site infection, in addition to those who abandoned outpatient follow-up, were excluded. Patients were selected and evaluated from April to August 2017. All individuals were included after signing the informed consent form and then were randomly allocated into two groups: (a) use of a 5% lidocaine patch (700 mg) for 12 hours per day; (b) manual massage with circular compression over the entire length of the scar for 10 minutes, twice a day. The patients were assessed for pain using the visual analog scale (VAS), the personal satisfaction index (excellent = 1, good = 2, regular = 3, or poor = 4) and the quality of life questionnaire SF-36 ( Appendix 1 ) in 4 moments: at the beginning of the treatment, and after 30, 60, and 90 days. There was no loss to follow-up or treatment abandonment. All patients were instructed to use paracetamol, 750 mg, as a rescue medication; alternatively, the patient could use dipyrone, 1 g, in case of atopy with paracetamol. The use of analgesic agents was not considered an exclusion criterion for the study.
The effects of the treatment were analyzed by comparing mean values in each group. Tests were performed with analysis of variance (ANOVA) models with repeated measures and group and moment as factors, and/or combining unpaired and paired Student t-tests or their nonparametric equivalents if the model assumptions were not satisfied. The significance level was set at 5% when using the statistical model; otherwise, it was adjusted by the general Bonferroni correction. All statistical analyzes were performed using the statistical software R 3.4.1 (R Foundation, Vienna, Austria) and NCSS 8.0 (Teikoku Seiyaku Co., Ltd 567 Sanbonmatsu, Higashikagawa, Kagawa – Japão Embalado por: Grünenthal GmbH Zieglerstraße 6 - Aachen - Alemanha).
The present study was registered at International Standard Randomised Controlled Trial Number (ISRCTN) under ID ISRCTN59332544.
Results
Pain assessment using the visual analog scale
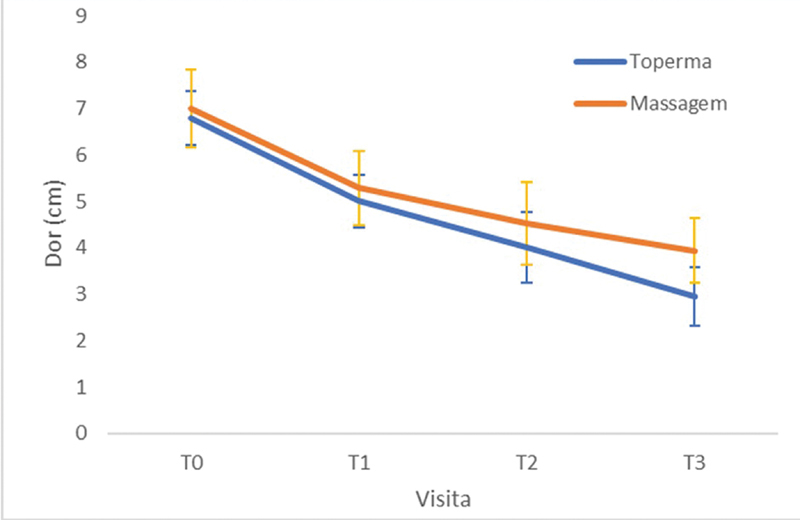
In total, 148 pain assessments using the VAS were recorded in 37 patients at 4 moments: pretreatment visit (t0), and visits at 30 (t1), 60 (t2), and 90 (t3) days after treatment. Pain variations were determined by subtracting the baseline score from the value obtained at each subsequent visit. An analysis at the t0 visit was carried out to verify whether Toperma and Massage treatment groups were comparable with each other regarding the pain measured by the VAS. A Student t-test was performed and found no significant evidence that the groups had different mean pain scores ( p = 0.697).
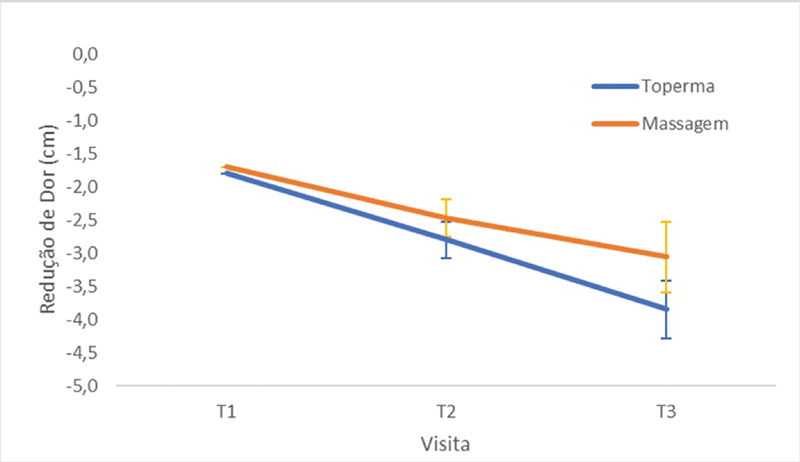
Both groups reported a reduction in pain over time. This decrease was statistically relevant at the first visit ( p < 0.05). Both groups showed statistically similar results ( Figure 1 ). An ANOVA model with repeated measures was used to test differences between groups and over time. The mean pain variations at each visit were distinct from each other ( p < 0.001), but with no significant difference between treatment groups ( p = 0.158); however, there seems to be a trend that each group presents a different pain reduction pattern from the other, since an interaction effect with a borderline p-value ( p = 0.060) was observed ( Figure 2 ).
Fig. 1.
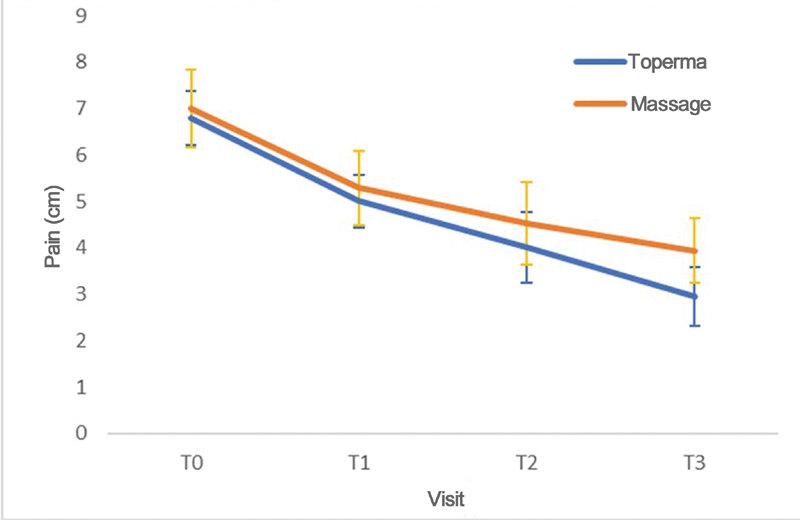
Mean pain profiles according to the visual analog scale (VAS) for each group at each visit (t0, t1, t2, and t3).
Fig. 2.
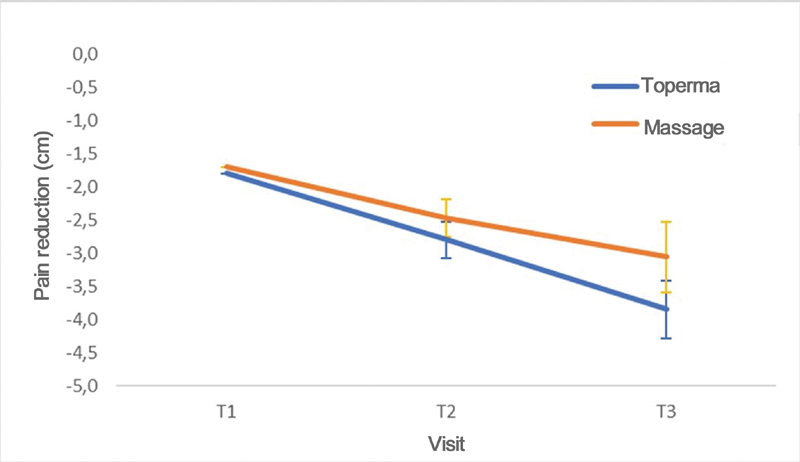
Mean pain reduction profiles according to the visual analog scale (VAS) for each group at each visit (t0, t1, t2, and t3).
None of the analyzed variables showed that the groups were not comparable at baseline. These data were verified using Student t-tests and Mann-Whitney tests, which revealed p-values > 0.098. Three comparative tests for outcome variations at t1, t2 and t3 were performed separately to determine group and time effects, showing a global significance level of 5%.
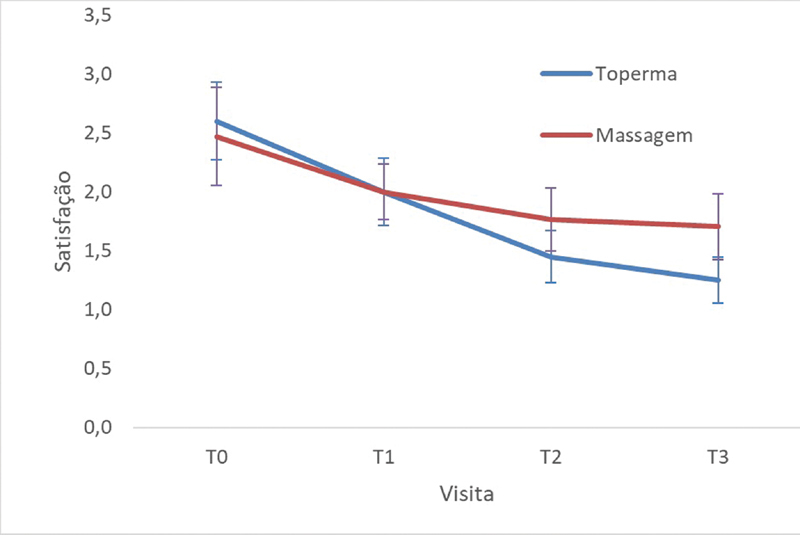
Mann-Whitney nonparametric tests analyzed the group effect over mean satisfaction values and showed a difference between the median values of the groups at t3 (Toperma versus Massage at t1, p = 0.677; at t2, p = 0.064; and at t3, p = 0.009). Since there was a difference between groups, the time effect was analyzed using the Wilcoxon nonparametric test within each group. For the Toperma group, the difference between visits ( p = 0.001 for t1 versus t2; p < 0.001 for t1 versus t3; p = 0.048 for t2 versus t3) was determined, concluding that satisfaction variation in t1 was different when compared with t2 and t3; however, these 2 last visits were not different from each other. For the Massage group, the difference between visits ( p = 0.049 for t1 versus t2; p = 0.027 for t1 versus t3; p = 0.347 for t2 versus t3) was analyzed, revealing the lack of evidence for a time effect in satisfaction variation ( Figure 3 ).
Fig. 3.
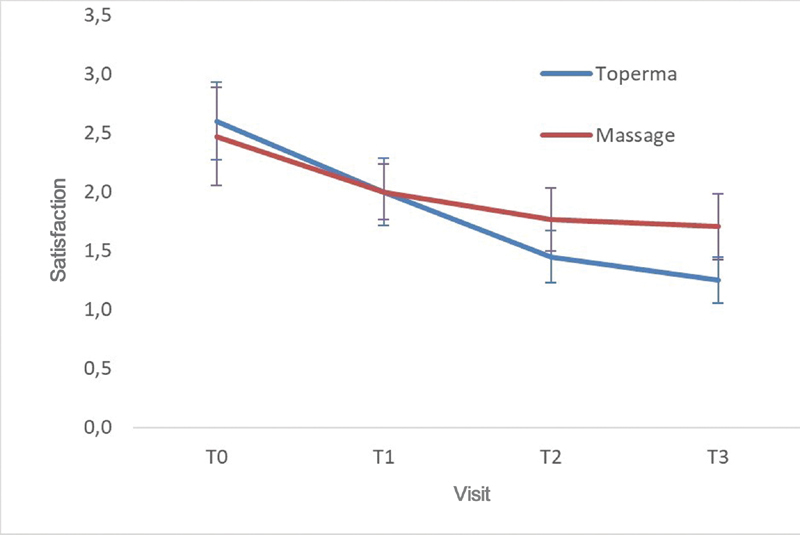
Mean personal patient satisfaction profiles for each group at each visit (t0, t1, t2, and t3).
For functional capacity variation, nonparametric Mann-Whitney tests determined the group effect, revealing no differences between the median values of the groups during visits ( p = 0.110 for t1; p = 0.269 for t2; p = 0.480 for t3). Since there was no difference between groups, the time effect on the total sample was analyzed. Differences between visits were determined using the Wilcoxon nonparametric test ( p < 0.001 for t1 versus t2; p < 0.001 for t1 versus t3; p = 0.003 for t2 versus t3) and concluded that functional capacity variation is different between visits ( Table 1 ).
Table 1. Summary measures for functional capacity in each group and each visit [t0, t1, t2 and t3] and variation among t1, t2, and t3 visits.
| Group | t0 | t1 | t2 | t3 |
|---|---|---|---|---|
| Toperma | ||||
| n | 20 | 20 | 20 | 20 |
| Mean (SD) | 61.0 (12.8) | 65.5 (12.2) | 74.8 (12.4) | 76.8 (12.1) |
| 95%CI | [55.4; 66.6] | [60.1; 70.9] | [69.3; 80.2] | [71.5; 82.0] |
| Median [Q1; Q3] | 62.5 [55.0; 70.0] | 70.0 [60.0; 70.0] | 75.0 [60.0; 85.0] | 80.0 [71.3; 85.0] |
| Minimum; Maximum values | 35.0; 90.0 | 30.0; 90.0 | 55.0; 95.0 | 55.0; 95.0 |
| Massage | ||||
| n | 17 | 17 | 17 | 17 |
| Mean (SD) | 58.5 (9.8) | 50.6 (18.8) | 66.5 (8.8) | 69.7 (9.9) |
| 95%CI | [53.9; 63.2] | [41.7; 59.5] | [62.3; 70.7] | [65.0; 74.4] |
| Median [Q1, Q3] | 60.0 [55.0; 65.0] | 55.0 [30.0; 70.0] | 60.0 [60.0; 70.0] | 70.0 [60.0; 80.0] |
| Minimum; Maximum values | 25.0; 70.0 | 30.0; 80.0 | 55.0; 85.0 | 55.0; 85.0 |
| Group | Group | Group | Group | |
| Toperma | ||||
| n | 20 | 20 | 20 | |
| Mean (SD) | 4.5 (13.4) | 13.8 (15.5) | 15.8 (15.0) | |
| 95%CI | [- 1.4; 10.4] | [6.9; 20.6] | [9.2; 22.3] | |
| Median [Q1; Q3] | 2.5 [0.0; 10.0] | 5.0 [5.0; 16.3] | 12.5 [5.0; 21.3] | |
| Minimum; Maximum values | - 35.0; 30.0 | - 5.0; 50.0 | - 5.0; 50.0 | |
| Massage | ||||
| n | 17 | 17 | 17 | |
| Mean (SD) | - 7.9 (19.0) | 7.9 (10.2) | 11.2 (11.1) | |
| 95%CI | [-17.0; 1.1] | [3.1; 12.8] | [5.9; 16.5] | |
| Median [Q1, Q3] | 0.0 [-30.0; 5.0] | 5.0 [0.0; 15.0] | 15.0 [0.0; 20.0] | |
| Minimum; Maximum values | -35.0; 25.0 | -5.0; 30.0 | -5.0; 30.0 |
Abbreviations: CI, confidence interval; SD, standard deviation.
Nonparametric Mann-Whitney tests determined the group effect over the mean values of physical aspects, revealing a difference between medians from t1 and t3 visits ( p = 0.007 for t1; p = 0.066 for t2; and p = 0.016 for t3). The Wilcoxon test analyzed the time effect separately on each group. For the Toperma group, there was no difference in physical aspects between visits ( p = 0.778 for t1 versus t2; p = 0.027 for t1 versus t3; p = 0.021 for t2 versus t3); the Massage group, however, presented a difference when t1 was compared with the 2 other visits ( p = 0.006 for t1 versus t2; p = 0.003 for t1 versus t3; p = 0.588 for t2 versus t3) ( Table 2 ).
Table 2. Summary measures for physical aspects in each group and each visit [t0, t1, t2 and t3] and variation among t1, t2, and t3 visits.
| Group | t0 | t1 | t2 | t3 |
|---|---|---|---|---|
| Toperma | ||||
| n | 20 | 20 | 20 | 20 |
| Mean (SD) | 35.0 (38.4) | 63.8 (32.9) | 65.0 (30.8) | 73.8 (27.5) |
| 95%CI | [18.2; 51.8] | [49.3; 78.2] | [51.5; 78.5] | [61.7; 85.8] |
| Median [Q1; Q3] | 25.0 [0.0; 56.3] | 50.0 [25.0; 100.0] | 62.5 [50.0; 100.0] | 75.0 [50.0; 100.0] |
| Minimum; Maximum values | 0.0; 100.0 | 25.0; 100.0 | 0.0; 100.0 | 25.0; 100.0 |
| Massage | ||||
| n | 17 | 17 | 17 | 17 |
| Mean (SD) | 52.9 (29.2) | 51.5 (28.6) | 69.1 (20.8) | 70.6 (20.2) |
| 95%CI | [39.1; 66.8] | [37.9; 65.1] | [59.2; 79.0] | [61.0; 80.2] |
| Median [Q1, Q3] | 50.0 [25.0; 75.0] | 50.0 [25.0; 75.0] | 75.0 [50.0; 75.0] | 75.0 [50.0; 75.0] |
| Minimum; Maximum values | 0.0; 100.0 | 25.0; 100.0 | 25.0; 100.0 | 25.0; 100.0 |
| Group | t1 | t2 | t3 | |
| Toperma | ||||
| n | 20 | 20 | 20 | |
| Mean (SD) | 28.8 (24.7) | 30.0 (23.8) | 38.8 (26.3) | |
| 95%CI | [17.9; 39.6] | [19.6; 40.4] | [27.2; 50.3] | |
| Median [Q1; Q3] | 25.0 [18.8; 50.0] | 25.0 [0.0; 50.0] | 50.0 [25.0; 50.0] | |
| Minimum; Maximum values | - 25.0; 75.0 | 0.0; 75.0 | 0.0; 75.0 | |
| Massage | ||||
| n | 17 | 17 | 17 | |
| Mean (SD) | - 1.5 (35.9) | 16.2 (21.5) | 17.6 (23.0) | |
| 95% CI | [- 18.5; 15.6] | [5.9; 26.4] | [6.7; 28.6] | |
| Median [Q1, Q3] | 0.0 [- 25.0; 25.0] | 0.0 [0.0; 25.0] | 0.0 [0.0; 25.0] | |
| Minimum; Maximum values | - 50.0; 75.0 | 0.0; 75.0 | 0.0; 75.0 |
Abbreviations: CI, confidence interval; SD, standard deviation.
Nonparametric Mann-Whitney tests analyzed the group effect over mean pain variations and detected no differences between the median values of the groups ( p = 0.554 for t1; p = 0.734 for t2; and p = 0.091 for t3). At the SF-36 questionnaire, pain variations were different among visits ( p < 0.001 for t1 versus t2; p < 0.001 for t1 versus t3; p < 0.001 for t2 versus t3).
The group effect over the general health condition was determined with nonparametric Mann-Whitney tests, revealing the following p-values: p = 0.347 for t1; p = 0.621 for t2; and p = 0.666 for t3. With the lack of difference between groups, differences between visits were confirmed using the Wilcoxon test, obtaining the following p-values: p < 0.001 for t1 versus t2; p < 0.001 for t1 versus t3; p < 0.001 for t2 versus t3 ( Table 3 ).
Table 3. Summary measures for general health condition in each group and each visit [t0, t1, t2 and t3] and variation among t1, t2, and t3 visits.
| Group | t0 | t1 | t2 | t3 |
|---|---|---|---|---|
| Toperma | ||||
| n | 20 | 20 | 20 | 20 |
| Mean (SD) | 61.3 (19.3) | 64.5 (16.4) | 74.1 (10.2) | 77.6 (9.6) |
| 95%CI | [52.8; 69.7] | [57.3; 71.6] | [69.6; 78.5] | [73.4; 81.8] |
| Median [Q1; Q3] | 62.0 [42.0; 77.0] | 67.0 [54.5; 77.0] | 77.0 [67.0; 80.0] | 78.5 [74.5; 80.5] |
| Minimum; Maximum values | 32.0; 95.0 | 37.0; 100.0 | 57.0; 100.0 | 62.0; 100.0 |
| Massage | ||||
| n | 17 | 17 | 17 | 17 |
| Mean (SD) | 59.6 (21.8) | 66.9 (12.7) | 71.2 (10.2) | 75.1 (9.0) |
| 95%CI | [49.2; 70.0] | [60.8; 72.9] | [66.4; 76.1] | [70.8; 79.4] |
| Median [Q1, Q3] | 62.0 [50.0; 77.0] | 67.0 [52.0; 77.0] | 77.0 [62.0; 77.0] | 80.0 [62.0; 80.0] |
| Minimum; Maximum values | 27.0; 82.0 | 52.0; 82.0 | 57.0; 85.0 | 62.0; 85.0 |
| Group | t1 | t2 | t3 | |
| Toperma | ||||
| n | 20 | 20 | 20 | |
| Mean (SD) | 3.2 (11.4) | 12.8 (11.2) | 16.4 (12.6) | |
| 95%CI | [- 1.8; 8.2] | [7.9; 17.7] | [10.8; 21.9] | |
| Median [Q1; Q3] | 0.0 [- 1.3; 5.0] | 9.0 [4.5; 25.0] | 15.5 [5.0; 27.8] | |
| Minimum; Maximum values | - 13.0; 30.0 | 0.0; 30.0 | 0.0; 35.0 | |
| Massage | ||||
| n | 17 | 17 | 17 | |
| Mean (SD) | 7.3 (11.0) | 11.6 (14.7) | 15.5 (14.2) | |
| 95%CI | [2.1; 12.5] | [4.6; 18.7] | [8.7; 22.2] | |
| Median [Q1, Q3] | 0.0 [0.0; 17.0] | 5.0 [0.0; 27.0] | 7.0 [3.0; 27.0] | |
| Minimum; Maximum values | - 3.0; 25.0 | 0.0; 35.0 | 0.0; 35.0 |
Abbreviations: CI, confidence interval; SD, standard deviation.
For vitality, the group effect was analyzed with Mann-Whitney nonparametric tests, which revealed the following p-values: p = 0.173 for t1; p = 0.652 for t2; and p > 0.999 for t3. With no difference between groups, differences between visits were detected by the Wilcoxon test, with the following p-values: p < 0.001 for t1 versus t2; p < 0.001 for t1 versus t3; p < 0.001 for t2 versus t3 ( Table 4 ).
Table 4. Summary measures for vitality in each group and each visit [t0, t1, t2 and t3] and variation among t1, t2, and t3 visits.
| Group | t0 | t1 | t2 | t3 |
|---|---|---|---|---|
| Toperma | ||||
| n | 20 | 20 | 20 | 20 |
| Mean (SD) | 60.0 (28.4) | 63.3 (23.9) | 71.8 (16.9) | 74.5 (17.8) |
| 95%CI | [47.5; 72.5] | [52.8; 73.7] | [64.4; 79.1] | [66.7; 82.3] |
| Median [Q1; Q3] | 62.5 [40.0; 77.5] | 67.5 [48.8; 80.0] | 77.5 [57.5; 86.3] | 80.0 [61.3; 90.0] |
| Minimum; Maximum values | 10.0; 95.0 | 20.0; 95.0 | 45.0; 95.0 | 45.0; 100.0 |
| Massage | ||||
| n | 17 | 17 | 17 | 17 |
| Mean (SD) | 56.8 (16.5) | 65.3 (9.8) | 67.9 (8.5) | 70.0 (7.3) |
| 95%CI | [48.9; 64.6] | [60.7; 69.9] | [63.9; 72.0] | [66.5; 73.5] |
| Median [Q1, Q3] | 55.0 [40.0; 75.0] | 65.0 [55.0; 70.0] | 65.0 [65.0; 75.0] | 65.0 [65.0; 75.0] |
| Minimum; Maximum values | 30.0; 80.0 | 50.0; 85.0 | 55.0; 85.0 | 65.0; 85.0 |
| Group | t1 | t2 | t3 | |
| Toperma | ||||
| n | 20 | 20 | 20 | |
| Mean (SD) | 3.3 (7.7) | 11.8 (16.7) | 14.5 (17.2) | |
| 95%CI | [- 0.1; 6.6] | [4.4; 19.1] | [7.0; 22.0] | |
| Median [Q1; Q3] | 2.5 [-1.3; 10.0] | 5.0 [0.0; 21.3] | 10.0 [3.8; 26.3] | |
| Minimum; Maximum values | - 10.0; 20.0 | - 10.0; 40.0 | - 10.0; 45.0 | |
| Massage | ||||
| n | 17 | 17 | 17 | |
| Mean (SD) | 8.5 (11.8) | 11.2 (13.1) | 13.2 (13.8) | |
| 95%CI | [2.9; 14.2] | [5.0; 17.4] | [6.7; 19.8] | |
| Median [Q1, Q3] | 5.0 [0.0; 20.0] | 10.0 [5.0; 25.0] | 10.0 [5.0; 25.0] | |
| Minimum; Maximum values | - 10.0; 25.0 | - 10.0; 40.0 | - 10.0; 45.0 |
Abbreviations: CI, confidence interval; SD, standard deviation.
The group effect over social aspects variations was defined using nonparametric Mann-Whitney tests, which showed the following p-values for Toperma versus Massage: p = 0.371 for t1; p = 0.411 for t2; and p = 0.318 for t3. With no difference between groups, differences between visits were confirmed with the Wilcoxon test, which revealed the following p-values: p = 0.003 for t1 versus t2; p = 0.060 for t1 versus t3; p = 0.047 for t2 versus t3 ( Table 5 )
Table 5. Summary measures for social aspects in each group and each visit [t0, t1, t2 and t3] and variation among t1, t2, and t3 visits.
| Group | T0 | t1 | t2 | t3 |
|---|---|---|---|---|
| Toperma | ||||
| n | 20 | 20 | 20 | 20 |
| Mean (SD) | 70.6 (21.9) | 76.3 (21.8) | 80.6 (18.8) | 78.8 (19.1) |
| 95%CI | [61.0; 80.2] | [66.7; 85.8] | [72.4; 88.9] | [70.4; 87.1] |
| Median [Q1; Q3] | 75.0 [50.0; 87.5] | 75.0 [62.5; 100.0] | 81.3 [75.0; 100.0] | 75.0 [71.9; 100.0] |
| Minimum; Maximum values | 25.0; 100.0 | 37.5; 100.0 | 50.0; 100.0 | 50.0; 100.0 |
| Massage | ||||
| n | 17 | 17 | 17 | 17 |
| Mean (SD) | 61.5 (24.5) | 75.0 (11.7) | 76.5 (12.4) | 75.7 (12.1) |
| 95%CI | [49.8; 73.1] | [69.4; 80.6] | [70.6; 82.4] | [70.0; 81.5] |
| Median [Q1, Q3] | 50.0 [40.0; 75.0] | 75.0 [75.0; 75.0] | 75.0 [75.0; 75.0] | 75.0 [75.0; 75.0] |
| Minimum; Maximum values | 25.0; 100.0 | 50.0; 100.0 | 50.0; 100.0 | 50.0; 100.0 |
| Group | t1 | t2 | t3 | |
| Toperma | ||||
| n | 20 | 20 | 20 | |
| Mean (SD) | 5.6 (16.0) | 10.0 (16.0) | 8.1 (14.8) | |
| 95%CI | [- 1.4; 12.6] | [3.0; 17.0] | [1.6; 14.6] | |
| Median [Q1; Q3] | 0.0 [0.0; 12.5] | 6.3 [0.0; 15.6] | 0.0 [0.0; 15.6] | |
| Minimum; Maximum values | - 25.0; 37.5 | - 12.5; 50.0 | - 12.5; 37.5 | |
| Massage | ||||
| n | 17 | 17 | 17 | |
| Mean (SD) | 13.5 (20.6) | 15.0 (20.0) | 14.3 (20.3) | |
| 95%CI | [3.7; 23.3] | [5.5; 24.5] | [4.6; 23.9] | |
| Median [Q1, Q3] | 0.0 [0.0; 35.0] | 12.5 [0.0; 35.0] | 12.5 [0.0; 35.0] | |
| Minimum; Maximum values | - 25.0; 50.0 | - 25.0; 50.0 | - 25.0; 50.0 |
Abbreviations: CI, confidence interval; SD, standard deviation.
Nonparametric Mann-Whitney tests analyzed the group effect over mean emotional aspects, resulting in the following p-values: p = 0.091 for t1; p = 0.057 for t2; and p = 0.018 for t3. With no difference between groups, differences between visits were confirmed with the Wilcoxon test, which showed the following p-values: p = 0.033 for t1 versus t2; p = 0.001 for t1 versus t3; p = 0.252 for t2 versus t3.
The group effect over mental health variation was defined by nonparametric Mann-Whitney tests, with the following p-values: p = 0.250 for t1; p = 0.763 for t2; and p = 0.740 for t3). With no difference between groups, differences between visits were confirmed using the Wilcoxon test, obtaining the following p-values: p < 0.001 for t1 versus t2; p < 0.001 for t1 versus t3; p = 0.018 for t2 versus t3. Thus, the variation in the mental health assessment in t1 is statistically different when compared with other visits ( Table 6 ).
Table 6. Summary measures for mental health in each group and each visit [t0, t1, t2 and t3] and variation among t1, t2, and t3 visits.
| Group | t0 | t1 | t2 | t3 |
|---|---|---|---|---|
| Toperma | ||||
| n | 20 | 20 | 20 | 20 |
| Mean (SD) | 67.0 (26.1) | 68.0 (25.7) | 77.6 (17.4) | 80.6 (16.2) |
| 95%CI | [55.5; 78.5] | [56.7; 79.3] | [70.0; 85.2] | [73.5; 87.7] |
| Median [Q1; Q3] | 56.0 [55.0; 100.0] | 64.0 [52.0; 100.0] | 72.0 [63.0; 100.0] | 80.0 [69.0; 100.0] |
| Minimum; Maximum values | 28.0; 100.0 | 32.0; 100.0 | 56.0; 100.0 | 56.0; 100.0 |
| Massage | ||||
| n | 17 | 17 | 17 | 17 |
| Mean (SD) | 64.9 (20.9) | 69.4 (16.2) | 76.2 (11.9) | 76.9 (11.9) |
| 95%CI | [55.0; 74.9] | [61.7; 77.1] | [70.6; 81.9] | [71.3; 82.6] |
| Median [Q1, Q3] | 64.0 [48.0; 80.0] | 64.0 [56.0; 80.0] | 76.0 [64.0; 80.0] | 76.0 [64.0; 80.0] |
| Minimum; Maximum values | 40.0; 100.0 | 52.0; 100.0 | 64.0; 100.0 | 64.0; 100.0 |
| Group | t1 | t2 | t3 | |
| Toperma | ||||
| n | 20 | 20 | 20 | |
| Mean (SD) | 1.0 (6.9) | 10.6 (12.2) | 13.6 (13.6) | |
| 95%CI | [- 2.0; 4.0] | [5.3; 15.9] | [7.7; 19.5] | |
| Median [Q1; Q3] | 0.0 [0.0; 5.0] | 8.0 [0.0; 18.0] | 14.0 [0.0; 24.0] | |
| Minimum; Maximum values | - 16.0; 8.0 | 0.0; 32.0 | 0.0; 32.0 | |
| Massage | ||||
| n | 17 | 17 | 17 | |
| Mean (SD) | 4.5 (5.8) | 11.3 (10.6) | 12.0 (11.7) | |
| 95%CI | [1.7; 7.2] | [6.3; 16.3] | [6.4; 17.6] | |
| Median [Q1, Q3] | 0.0 [0.0; 12.0] | 12.0 [0.0; 24.0] | 12.0 [0.0; 24.0] | |
| Minimum; Maximum values | - 4.0; 12.0 | 0.0; 24.0 | - 4.0; 32.0 |
Abbreviations: CI, confidence interval; SD, standard deviation.
Discussion
Chronic postoperative neuropathic pain is a challenge for orthopedic surgeons, affecting up to 50% of patients. 2 Although the therapeutic arsenal is extensive, encouraging results are scarce. New therapeutic modalities, including a 5% lidocaine patch, have been tested for neuropathic pain such as PHN. 3 4 5 The 5% lidocaine patch has a dual action, providing a mechanical barrier effect and inactivating sodium channels. Compared with other drugs used for neuropathic pain treatment, its main advantage is the lack of systemic effects, with reports of only local skin reactions or application site pain. Therapeutic massage has been described in several studies as a treatment method for postoperative scar tissue pain, with variable outcomes. 6 7
The present study analyzed and compared effects from these two therapeutic modalities in randomized groups of patients undergoing foot and ankle surgery who continuously presented with surgical scar tissue pain after a minimum of 3 months. Patients were analyzed for pain (measured with the VAS), degree of personal satisfaction, and components from the SF-36 questionnaire.
Both groups showed a pattern of pain improvement over the 3 months of treatment, with equivalent outcomes in 90 days. However, the group treated with lidocaine showed a greater pain reduction over time. The analysis of the variation curve ( Figure 2 ) suggests that, with a longer application time, the patch becomes superior to therapeutic massage. Outcomes in 90 days are consistent with the literature. There are no comparable studies on lidocaine patches.
In the SF-36 questionnaire, no parameter showed a statistically significant difference between groups, which revealed a similar improvement in pain in both groups. Regarding functional capacity, physical aspects, vitality, emotional aspects, social aspects, general health conditions, and mental health, there was no significant evidence to affirm that any of the two treatment modalities had a positive or negative influence; in addition, no difference between groups was detected.
A major advantage of the patch is the degree of personal satisfaction of the patient, with greater, statistically significant improvement. This effect is believed to be due to the easy application and to the psychological effect of drug therapy in comparison with a nondrug treatment. When analyzing the variation of personal satisfaction ( Figure 3 ), there was a tendency for better results over time favoring the patch.
Satisfaction, determined with a simple scale, is an important standard of assessment, since neuropathic pain is a common reason for reports of unsuccess despite the excellent surgical result. Our study demonstrates that the patch increases the satisfaction of the patients with the surgical result, favoring the doctor-patient relationship. Despite its cost, the patch has the benefits of easy adherence and a need for a lower degree of knowledge to comply with the treatment compared with the massage, which requires good understanding and practice.
Although this is a randomized clinical trial, our study evaluated a small number of patients ( n = 37) during a 90-day follow-up period. Our findings suggest that the treatments would differ with longer monitoring, with better results for the patch. Due to these limitations, it is difficult to transport these data to a general population. New studies with a longer evaluation period are required to confirm the applicability of the patch as a treatment method for surgical scar-related neuropathic pain, as well as to verify whether these effects are permanent or temporary.
Conclusion
The present study shows that the lidocaine patch and manual desensitization with massage are two effective treatment methods for pain reduction, with similar outcomes. The lidocaine patch was also associated with an improved satisfaction with the surgical result. Further studies are required to evaluate the applicability of these methods, as well as to verify the duration of the analgesic effects.
Appendix 1 Brazilian Version of the Quality-of-Life Questionnaire – SF-36
1- In general, would you say your health is:
| Excellent | Very Good | Good | Fair | Poor |
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 |
2- Compared with one year ago, how would you rate your health in general now?
| Much better | Somewhat better | About the same | Somewhat worse | Much worse |
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 |
3- The following items are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much?
| Activities | Yes, it limits a lot | Yes, it limits a little | No, it does not limit at all |
|---|---|---|---|
| a) Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports. | 1 | 2 | 3 |
| b) Moderate activities, such as moving a table, using vacuum cleaner, playing ball, sweeping the floor. | 1 | 2 | 3 |
| c) Lifting or carrying groceries | 1 | 2 | 3 |
| d) Climbing several flights of stairs | 1 | 2 | 3 |
| e) Climbing one flight of stairs | 1 | 2 | 3 |
| f) Bending, kneeling, or stooping | 1 | 2 | 3 |
| g) Walking more than a kilometer | 1 | 2 | 3 |
| h) Walking several blocks | 1 | 2 | 3 |
| i) Walking one block | 1 | 2 | 3 |
| j) Bathing or dressing yourself | 1 | 2 | 3 |
4- During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your physical health?
| Yes | No | |
|---|---|---|
| a) Cut down the amount of time you spent on work or other activities? | 1 | 2 |
| b) Accomplished less than you would like? | 1 | 2 |
| c) Were limited in the kind of work or other activities. | 1 | 2 |
| d) Had difficulty performing the work or other activities (for example, it took extra effort) | 1 | 2 |
5- During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (such as feeling depressed or anxious)?
| Yes | No | |
|---|---|---|
| a) Cut down the amount of time you spent on work or other activities? | 1 | 2 |
| b) Accomplished less than you would like? | 1 | 2 |
| c) Didn't do work or other activities as carefully as usual. | 1 | 2 |
6- During the past 4 weeks, how your physical health or emotional problems interfered with your normal social activities with family, friends, or groups?
| Not at all | Slightly | Moderately | Severe | Very severely |
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 |
7- How much bodily pain have you had during the past 4 weeks?
| None | Very Mild | Mild | Moderate | Severe | Very severe |
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 |
8- During the past 4 weeks, how much did pain interfere with your normal work (including housework)?
| Not at all | Slightly | Moderately | Severe | Very severe |
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 |
9- These questions are about how you feel and how things have been with you during the last 4 weeks. For each question, please give the answer that comes closest to the way you have been feeling.
| All of the time | Most of the time | A good bit of the time | Some of the time | A little bit of the time | None of the time | |
|---|---|---|---|---|---|---|
| a) Did you feel full of pep? | 1 | 2 | 3 | 4 | 5 | 6 |
| b) Have you been a very nervous person? | 1 | 2 | 3 | 4 | 5 | 6 |
| c) Have you felt so down in the dumps that nothing could cheer you up? | 1 | 2 | 3 | 4 | 5 | 6 |
| d) Have you felt calm and peaceful? | 1 | 2 | 3 | 4 | 5 | 6 |
| e) Did you have a lot of energy? | 1 | 2 | 3 | 4 | 5 | 6 |
| f) Have you felt downhearted and blue? | 1 | 2 | 3 | 4 | 5 | 6 |
| g) Did you feel worn out? | 1 | 2 | 3 | 4 | 5 | 6 |
| h) Have you been a happy person? | 1 | 2 | 3 | 4 | 5 | 6 |
| i) Did you feel tired? | 1 | 2 | 3 | 4 | 5 | 6 |
10- During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities (like visiting with friends, relatives, etc.)?
| All of the time | Most of the time | A good bit of the time | Some of the time | A little bit of the time |
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 |
11- How true or false is each of the following statements for you?
| Definitely true | Mostly true | I do not know | Mostly false | Definitely false | |
|---|---|---|---|---|---|
| a) I seem to get sick a little easier than other people | 1 | 2 | 3 | 4 | 5 |
| b) I am as healthy as anybody I know | 1 | 2 | 3 | 4 | 5 |
| c) I expect my health to get worse | 1 | 2 | 3 | 4 | 5 |
| d) My health is excellent | 1 | 2 | 3 | 4 | 5 |
QUALITY-OF-LIFE SCORING CALCULATION
Phase 1: Data ponderation
| Question | Score | |
|---|---|---|
| 01 | If the answer was 1 2 3 4 5 |
Score 5.0 4.4 3.4 2.0 1.0 |
| 02 | Keep the same value | |
| 03 | All values are added | |
| 04 | All values are added | |
| 05 | All values are added | |
| 06 | If the answer was 1 2 3 4 5 |
Score 5 4 3 2 1 |
| 07 | If the answer was 1 2 3 4 5 6 |
Score 6.0 5.4 4.2 3.1 2.0 1.0 |
| 08 | The answer to question 8 is based on the score from question 7 If 7 = 1 and if 8 = 1, the score is (6) If 7 = 2 to 6 and 8 = 1, the score is (5) If 7 = 2 to 6 and if 8 = 2, the score is (4) If 7 = 2 to 6 and if 8 = 3, the score is (3) If 7 = 2 to 6 and if 8 = 4, the score is (2) If 7 = 2 to 6 and if 8 = 3, the score is (1) If question 7 was not answered, question 8 score will be the following: If the answer was (1), the score will be (6) If the answer was (2), the score will be (4.75) If the answer was (3), the score will be (3.5) If the answer was (4), the score will be (2.25) If the answer was (5), the score will be (1.0) |
|
| 09 | For this question, the score for items a, d, e, and h should follow these guidelines: If the answer was 1, the score will be (6) If the answer was 2, the score will be (5) If the answer was 3, the score will be (4) If the answer was 4, the score will be (3) If the answer was 5, the score will be (2) If the answer was 6, the score will be (1) For the remaining items (b, c, f, g, and i), the score should be the same |
|
| 10 | Consider the same score. | |
| 11 | For this question, items should be added; however, items b and d should follow these guidelines: If the answer was 1, the score will be (5) If the answer was 2, the score will be (4) If the answer was 3, the score will be (3) If the answer was 4, the score will be (2) If the answer was 5, the score will be (1) |
|
Phase 2: Raw Scale Calculation
In this phase, transform the values from previous questions into scores for eight domains, ranging from 0 (zero) to 100 (one hundred), where 0 = worst and 100 = best score for each domain. This is called a raw scale because the final score has no unit of measure.
Domain:
Functional capacity
Limitation due to physical aspects
Pain
General health condition
Vitality
Social aspects
Emotional aspects
Mental health
To do so, apply the following formula to calculate each domain:
Domain:
For this formula, the lower limit and score range are fixed and stipulated at the following table.
| Domain | Score at corresponding questions | Lower limit | Score range |
|---|---|---|---|
| Functional capacity | 03 | 10 | 20 |
| Limitation due to physical aspects | 04 | 4 | 4 |
| Pain | 07 + 08 | 2 | 10 |
| General health condition | 01 + 11 | 5 | 20 |
| Vitality | 09 (only for items a + e + g + i) | 4 | 20 |
| Social aspects | 06 + 10 | 2 | 8 |
| Limitation due to emotional aspects | 05 | 3 | 3 |
| Mental health | 09 (only for items b + c + d + f + h) | 5 | 25 |
Funding Statement
Suporte Financeiro Não houve suporte financeiro de fontes públicas, comerciais, ou sem fins lucrativos.
Conflito de Interesses Os autores declaram não haver conflito de interesses.
Trabalho realizado no Serviço de Ortopedia e Traumatologia, Hospital Ipiranga, São Paulo, SP, Brasil
Study performed at the Orthopedics and Traumatology Service, Hospital Ipiranga, São Paulo, SP, Brazil .
Contribuição dos Autores
Cada autor contribuiu individual e significantemente para o desenvolvimento deste artigo. Macedo R. R. (0000-0002-2563-2085)*, Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* e Mendes Júnior J. P. (0000-0003-1514-5029)* foram os principais colaboradores para a elaboração do manuscrito. Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* e Mendes Júnior J. P. (0000-0003-1514-5029)* seguiram os pacientes e reuniram dados clínicos. Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* e Mendes Júnior J. P. (0000-0003-1514-5029)* avaliaram os dados da análise estatística. Macedo R. R. (0000-0002-2563-2085)*, Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* e Mendes Júnior J. P. (0000-0003-1514-5029)* conduziram a pesquisa bibliográfica. Ikemoto R. Y. (0000-0001-7718-1186)* e Rodrigues L. M. R. (0000-0001-6891-5395)* revisaram o manuscrito e contribuíram para o conceito intelectual do estudo. *ORCID (Open Researcher and Contributor ID).
Authors' Contribution
Each author contributed individually and significantly to the development of the present article. Macedo R. R. (0000-0002-2563-2085)*, Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* and Mendes Júnior J. P. (0000-0003-1514-5029)* were the main collaborators for manuscript preparation. Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* and Mendes Júnior J. P. (0000-0003-1514-5029)* performed the follow-up of the patients and collected clinical data. Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* and Mendes Júnior J. P. (0000-0003-1514-5029)* evaluated the data for statistical analysis. Macedo R. R. (0000-0002-2563-2085)*, Santos J. P. G. (0000-0002-1086-9872)*, Lobato E. S. (0000-0002-7181-6133)* and Mendes Júnior J. P. (0000-0003-1514-5029)* conducted the literature review. Ikemoto R. Y. (0000-0001-7718-1186)* and Rodrigues L. M. R. (0000-0001-6891-5395)* reviewed the manuscript and contributed to the intellectual concept of the study. *ORCID (Open Researcher and Contributor ID).
Referências
- 1.de León-Casasola O A, Mayoral V. The topical 5% lidocaine medicated plaster in localized neuropathic pain: a reappraisal of the clinical evidence. J Pain Res. 2016;9:67–79. doi: 10.2147/JPR.S99231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tornetta P, 3rd., Court-Brown M, Heckman J D. 8 th ed. . Philadelphia: Wolters Kluwer Health; 2015. Rockwood and Green's fractures in adults. [Google Scholar]
- 3.Nayak S, Cunliffe M. Lidocaine 5% patch for localized chronic neuropathic pain in adolescents: report of five cases. Paediatr Anaesth. 2008;18(06):554–558. doi: 10.1111/j.1460-9592.2008.02491.x. [DOI] [PubMed] [Google Scholar]
- 4.Liedgens H, Obradovic M, Nuijten M. Health economic evidence of 5% lidocaine medicated plaster in post-herpetic neuralgia. Clinicoecon Outcomes Res. 2013;5(01):597–609. doi: 10.2147/CEOR.S51776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hadley G R, Gayle J A, Ripoll J. Post-herpetic neuralgia: a review. Curr Pain Headache Rep. 2016;20(03):17. doi: 10.1007/s11916-016-0548-x. [DOI] [PubMed] [Google Scholar]
- 6.Masanovic M G. [Physical therapy for scars] Soins. 2013;(772):41–43. [PubMed] [Google Scholar]
- 7.Shin T M, Bordeaux J S. The role of massage in scar management: a literature review. Dermatol Surg. 2012;38(03):414–423. doi: 10.1111/j.1524-4725.2011.02201.x. [DOI] [PubMed] [Google Scholar]