

Abstract
Background:
Rugby union is a physically demanding sport that carries an inherent risk of injury. Despite being a popular and widely played team sport, little is known about injuries occurring across the male and female amateur game.
Purpose:
To establish and compare injury incidence, nature, and severity in male and female Irish amateur rugby union.
Study Design:
Prospective cohort study.
Level of Evidence:
Level 3.
Methods:
Data were collected prospectively from 25 male teams (959 players) and 8 female teams (234 players) over 2 full seasons. Both time-loss (24-hour time-loss injury definition) and non-time-loss match injury reports were collected, alongside match exposure data.
Results:
Time-loss match injury incidence rates were 49.1/1000 and 35.6/1000 player-hours for male and female players, respectively. Concussion and ankle ligament sprains were the most common diagnoses for male (5.6/1000 and 4.4/1000 player-hours, respectively) and female players (5.5/1000 and 3.9/1000 player-hours, respectively). Anterior cruciate ligament injuries presented the highest injury burden for male and female players with 200.3 and 307.2 days of absence per 1000 player-hours, respectively. In female players, 83% of noncontact injuries occurred in the fourth quarter of match play.
Conclusion:
While female players had a lower overall injury incidence rate compared with male players, concussion and ankle ligament injuries were the most common injuries in both cohorts. In female players, a high rate of noncontact injuries in the second half points to the need for strength and conditioning training programs to reduce fatigue-related injuries.
Clinical Relevance:
Establishing the incidence and burden of rugby-related injuries is an essential step in minimizing injury risk. This epidemiological information will aid the development of future reduction strategies, including education and coaching strategies and strength and conditioning programs, informed by the most common injuries observed and the mechanism of injury.
Keywords: Rugby union, injury risk, epidemiology, injury surveillance, injury prevention
Rugby union, hereafter “rugby,” is an increasingly popular team sport characterized by both high- and low-intensity activities alongside exposure to collisions and contact events.20,30 As with most sports, the majority of participants are amateur with approximately 9.6 million rugby players currently registered across 123 countries worldwide and female players accounting for nearly 30% of all players.2,31
The incidence of rugby-related injury varies from 46.8/1000 to 81/1000 player-hours in the amateur and professional male game, respectively28,33; however, there is a lack of similar research conducted in the female game.18,27 To effectively manage injury risk, comprehensive injury surveillance must be conducted across all levels, to identify injury mechanisms and associated risk factors.15,16 In the current literature, differences in injury definition, reporting, and methods of data collection make comparisons between studies difficult and subsequently affects the design and implementation of effective injury reduction strategies.18,33 In an attempt to manage the risk of rugby-related injury, World Rugby has established a transparent and standardized approach to surveillance and reporting, resulting in comprehensive surveillance conducted at international- or elite-level competitions. 12 Across all levels of the game, a 24-hour time-loss injury definition has been recommended 10 ; however, because of limited resources and medical personnel in the amateur setting, this may not be achievable and therefore a >7-day time-loss (missed-match) injury definition may be used. 4 This “missed-match” definition has resulted in a lower injury rate of 22.8/1000 player-hours reported in the senior male amateur game in comparison with 46.8/1000 player-hours reported in a meta-analysis on amateur rugby.21,33 By only reporting injuries resulting in a >7-day time-loss, overall injury occurrences may not be accounted for and may result in underdiagnosis of minor injuries (eg, minor strains/sprains and lacerations/contusions) and injury recurrences. 8 While these injuries may not result in lengthy absences from matches and/or training, cumulatively throughout the season they may result in a high injury burden to the player and team overall. 22 Therefore, comprehensive injury surveillance, using a 24-hour time-loss injury definition, is required to more accurately reflect the incidence of all injuries.
While injury surveillance has been conducted in some amateur male rugby cohorts, it is often limited to elite-level competitions in the female game with no long-term prospective surveillance strategy in the amateur setting until recently.27,32 A pooled incidence rate of 19.6/1000 player-hours has been reported in the female game, 18 which is lower than the rates reported in meta-analyses in the professional and amateur male game.28,33 This pooled incidence rate included injuries from elite competitions, collegiate teams, and national teams, with the only study 3 reporting on the senior amateur female game excluded because of the methodological differences in study design and injury reporting. While potential sex-related differences in both incidence rates and injury patterns have been recently highlighted, 27 because of a lack of long-term surveillance strategies in amateur female rugby, these differences are yet to be investigated further. Therefore, determining injury risk based on the currently available evidence may not accurately reflect potential differences between male and female players. These potential sex-related differences may influence the subsequent design and implementation of injury prevention strategies, as these strategies may need to be adapted based on differences in injury characteristics.2,27 Therefore, the aim of this study was to describe the incidence, nature, and severity of injuries resulting from match play within Irish male and female amateur rugby.
Methods
This prospective cohort study was conducted over 2 full rugby seasons, running from July 2017 to May 2019. In Ireland, there are approximately 209,000 players currently participating from 224 amateur rugby clubs (130 male clubs, 94 male and female clubs). 31 There is a national league of 58 clubs called the All Ireland League (AIL) representing the highest level of amateur rugby in Ireland. The men’s AIL comprises 50 teams across 2 main divisions (Division 1 and Division 2), whereas the women’s AIL comprises 8 teams in 1 single division. Of the 58 AIL clubs, 21 (16 male clubs, 5 female clubs) were recruited to participate in the Irish Rugby Injury Surveillance (IRIS) Project for the first season of data collection (2017-2018). 32 In season 2 (2018-2019), a further 15 clubs (10 male clubs, 5 female clubs) were recruited, resulting in a total of 26 male clubs and 10 female clubs participating. Both Division 1 and Division 2 men’s AIL teams were included in both seasons, to provide an accurate representation of playing level within the amateur male game in Ireland. In the second season, 2 non-AIL female clubs were recruited, and while these 2 teams played in 1 division lower than the AIL, they would be of similar skill level as they compete each season during the promotion/relegation play-offs for inclusion in the AIL. Ethical approval for this study was granted by the institution’s research ethics committee in compliance with the Declaration of Helsinki.
Participants
At the end of the 2016-2017 rugby season, AIL clubs were contacted and invited to participate in the IRIS Project beginning in the 2017-2018 season. An introductory email and letter were sent to the club secretary and medical staff, outlining the aims of the IRIS Project, support from the Irish Rugby Football Union, incentives, and commitment required from the club staff, players, and medical staff. 32
An injury recorder was nominated in each participating club to act as the main contact point for the IRIS Project. Where possible, the injury recorder was the primary medical professional working with the senior first team; however, some clubs nominated an alternative injury recorder to collect and record injury reports from the match day physiotherapist/physical therapist or doctor. Injury recorders included physiotherapists/physical therapists (n = 27), club welfare officers (n = 7), doctors (n = 1), and team coaches (n = 1). Injuries were recorded on a bespoke web-based injury surveillance platform, IRISweb. 32 All senior first squad players were registered on IRISweb, including player name, date of birth, mass, height, medical history, medications, injury history (within the preceding 12 months), playing position, and number of years playing rugby. 32 Signed informed consent was obtained from each club, injury recorder, and player.
Injury Surveillance
The injury recorder was asked to document any match or training injury occurring in the senior first squad throughout the season, following the World Rugby definition of an injury. 10 Any injury that resulted in a player being unable to fully participate in a future scheduled match or training session for more than 24 hours after the injury was categorized as a time-loss injury. Injuries that did not result in an absence from match or training activities were categorized as non-time-loss injuries. 10 Injury data included injury location and nature, time of occurrence, and the mechanism. 32 Provisional diagnoses, final diagnoses, and number of days of absence from rugby matches and/or training were also recorded. Absences from rugby match play or training due to illness or injuries incurred through other activities (outside rugby match or training activities) were not included. During the season, the main author (C.Y.) conducted a weekly audit of the data collected to ensure accuracy and completeness. 32 All injuries were recorded within 30 days after the last match of the season to give sufficient time to report and clear injuries as appropriate.
Statistical Analysis
Descriptive statistics, including mean ± standard deviation (SD), median (interquartile range), number, and percentages, were used to summarize participant demographics and anthropometrics using SPSS (IBM SPSS Statistics for Windows, Version 25.0, IBM Corp). Data were analyzed and presented separately for male and female players. Injury incidence rates for all match injury variables were calculated according to the following equation 10 :
Using this equation, match exposure was based on 15 players being exposed for 80 minutes. Logistic regression was used to obtain rates of injuries with 95% confidence intervals (CIs). Overall injury incidence rates were reported individually for each season to highlight the potential benefits of continued seasonal prospective surveillance strategies; however, all other variables were reported for both seasons combined. Injury severity was reported as the median (interquartile range) days’ absence. To compare with current literature in amateur rugby, injuries in the current study that resulted in >7 days of absence were also reported separately.4,10 Match injury burden was calculated as days lost per 1000 player-hours to provide an overview of risk. 1
Results
In season 1, 21 clubs (16 male clubs, 5 female clubs) were recruited to participate in the IRIS Project, with 2 clubs (1 male club, 1 female club) failing to give a full season of data and were therefore excluded from analysis. These 2 clubs agreed to participate in the second season of data collection, alongside a further 15 clubs (10 male clubs, 5 female clubs). Four of these 36 clubs were excluded at the end of the second season, with 1 club (female) withdrawing from competitive rugby mid-season and the 3 other clubs (1 male club, 2 female clubs) failing to provide a full season of data. This resulted in an overall compliance rate of 90% over the 2 seasons. A total of 959 male players (mean ± SD of 38 ± 8 players per team) and 234 female players (mean ± SD of 29 ± 13 players per team) were registered over the 2 seasons and monitored for match injuries (Table 1).
Table 1.
Player background information summarized by number or mean ± SD
| Male Players | Female Players | |||
|---|---|---|---|---|
| Total no. of players | 959 | 234 | ||
| No. of clubs | 25 | 8 | ||
| Age, y | 25.1 ± 4.1 | 27.2 ± 5.3 | ||
| Rugby playing experience, y | 14.4 ± 4.7 | 5.8 ± 4.3 | ||
| Division experience, y | 2.8 ± 2.7 | 2.8 ± 2.9 | ||
| Forwards | Backs | Forwards | Backs | |
| Total no. of players | 533 | 426 | 129 | 105 |
| Mass, kg | 103.4 ± 11.9 | 85.7 ± 7.8 | 80.1 ± 14.7 | 67.6 ± 8.7 |
| Height, cm | 185.7 ± 7.4 | 180.2 ± 6.6 | 169.4 ± 7.8 | 164.8 ± 7.5 |
Match Injury Incidence
Over 2 seasons, a total of 1073 injuries were recorded across 1080 matches, with overall time-loss (>24 hours of absence) match injury incidence rates of 49.1/1000 and 35.6/1000 player-hours for males and females, respectively (Table 2).
Table 2.
Match injury incidence rates for seasons 1, 2, and both seasons combined
| Injury Definition | Season | No. of Injuries | Exposure Hours a | IR b (95% CI) |
|---|---|---|---|---|
| Male Players | ||||
| >1-day time-loss | Season 1 | 344 | 6800 | 50.6 (45.2-55.9) |
| Season 2 | 538 | 11,180 | 48.1 (44.0-52.2) | |
| Total | 882 | 17,980 | 49.1 (46.1-52.7) | |
| >7-day time-loss c | Season 1 | 261 | 6800 | 38.4 (33.7-43.0) |
| Season 2 | 423 | 11,180 | 37.8 (34.2-41.4) | |
| Total | 684 | 17,980 | 38.0 (35.4-41.2) | |
| Non-time-loss | Season 1 | 16 | 6800 | 2.4 (1.2-3.5) |
| Season 2 | 38 | 11,180 | 3.4 (2.3-4.5) | |
| Total | 54 | 17,980 | 3.0 (2.2-3.8) | |
| Female Players | ||||
| >1-day time-loss | Season 1 | 72 | 1560 | 46.2 (35.5-56.8) |
| Season 2 | 57 | 2060 | 27.7 (20.5-34.8) | |
| Total | 129 | 3620 | 35.6 (29.9-41.7) | |
| >7-day time-loss c | Season 1 | 55 | 1560 | 35.3 (25.9-44.6) |
| Season 2 | 43 | 2060 | 20.9 (14.6-27.1) | |
| Total | 98 | 3620 | 27.1 (21.7-32.4) | |
| Non-time-loss | Season 1 | 8 | 1560 | 5.1 (1.6-8.7) |
| Season 2 | 0 | 2060 | 0 | |
| Total | 8 | 3620 | 2.2 (0.7-3.7) | |
Each male team competed in 23 ± 2.6 matches in season 1, while the female teams competed in 20 ± 1.9 matches. In season 2, each male team competed in 22 ± 1.5 matches; however, the female teams had fewer matches compared with season 1 competing in 15 ± 1.6 matches. Across both seasons, men had a higher injury prevalence with 51% sustaining at least 1 injury compared with 37% of women and 19% of men sustained more than 1 injury, compared with only 10% of women.
Location and Nature of Time-Loss Match Injuries
The head and face were the most common locations for time-loss injuries for male and female players with respective incidence rates of 7.6/1000 and 6.9/1000 player-hours; however, injuries to the shoulder (men) and knee (women) resulted in lengthier absences from matches and/or training (Table 3). The majority of head and face injuries occurred in the forwards for both the male (4.6/1 000 player-hours) and female players (3.6/1 000 player-hours).
Table 3.
The 3 most common injury locations for seasons 1 and 2 combined.
| Injury Location | IR a (95% CI) | Severity, b Median (IQR) | |
|---|---|---|---|
| Male players | Head/face | 7.6 (6.4-8.9) | 21 (21-27) |
| Shoulder | 7.5 (6.3-8.8) | 22 (7-43) | |
| Ankle | 6.0 (4.9-7.2) | 21 (8-41) | |
| Female players | Head/face | 6.9 (4.2-9.6) | 21 (21-28) |
| Knee | 6.1 (3.5-8.6) | 36 (11-87) | |
| Ankle | 5.2 (2.9-7.6) | 20 (11-73) |
IQR, interquartile range.
IR indicates incidence rate per 1000 player-hours.
Severity is the median days of absence per injury.
Male players had a higher incidence of muscle and tendon strains compared with female players, with respective incidence rates of 14.9/1000 and 6.4/1000 player-hours, whereas women sustained more ligament sprains overall (Table 4). Incidence rates and injury severity for all bodily locations and injury types can be found in the Appendix (S1-S5) (available in the online version of this article). Forwards sustained the majority of injuries compared with backs in both the male (60%) and female (55%) teams. In the male teams, the loose-head prop had the highest injury rate of the overall, with a rate of 5.1/1000 player-hours, whereas the inside center had the highest injury rate in the female teams (5.8/1000 player-hours).
Table 4.
Top 3 most common injury types for seasons 1 and 2 combined
| Injury Type | IR a (95% CI) | Severity, b Median (IQR) | |
|---|---|---|---|
| Male players | Strains | 14.9 (13.1-16.7) | 15 (7-29) |
| Sprains | 12.2 (10.5-13.9) | 22 (10-41) | |
| Hematoma/contusions | 6.6 (5.4-7.8) | 9 (7-21) | |
| Female players | Sprains | 14.1 (10.2-18) | 14 (8-35) |
| Strains | 6.8 (3.8-8) | 10 (4-19) | |
| Concussions | 5.5 (3.1-7.9) | 21 (21-28) |
IQR, interquartile range.
IR indicates the incidence rate per 1000 player-hours.
Severity is the median days of absence per injury.
Time-Loss Match Injury Diagnosis and Burden
Concussion injuries were the most common time-loss injury diagnosis for male (5.6/1000 player-hours) and female players (5.5/1000 player-hours) (Table 5), with 56% of male concussions and 45% of female concussions occurring as a result of tackling the ball carrier. Anterior cruciate ligament (ACL) ruptures carried the highest injury burden for both men and women resulting in a total 200.3 days of absence per 1000 player-hours and 307.2 days of absence per 1000 player-hours, respectively.
Table 5.
The 3 most common injury diagnoses for seasons 1 and 2 combined
| Injury Diagnosis | IR a (95% CI) | Severity, b Median (IQR) | |
|---|---|---|---|
| Male players | Concussion | 5.6 (4.5-6.7) | 21 (21-28) |
| ATFL sprains | 4.4 (3.9-6.0) | 15 (7-35) | |
| Hamstring strains | 4.2 (3.3-5.2) | 21 (14-35) | |
| Female players | Concussion | 5.5 (3.1-7.9) | 21 (20-32) |
| ATFL sprains | 3.9 (1.8-5.9) | 15 (8-21) | |
| MCL sprains | 2.8 (0.9-4.5) | 35 (21-49) |
ATFL, anterior talofibular ligament (ankle); IQR, interquartile range; MCL, medial collateral ligament (knee).
IR indicates the incidence rate per 1000 player-hours.
Severity is the median days of absence per injury.
Timing and Mechanism of Time-Loss Match Injury
Preseason training began in July to August, with AIL matches beginning in September and ending in April (women) or May (men). The majority of injuries reported occurred in the early part of the season (September-November), accounting for 47% and 56% of all male and female injuries, respectively (Figure 1). Muscle and tendon strains and ligament sprains had the highest occurrence during these months for women (62% and 60%, respectively) compared with men (48% and 40%, respectively). These months also resulted in the majority of reported fractures for men (53%) and women (56%). While 52% of joint dislocation/subluxations occurred during the September to November period for men, 75% of dislocation/subluxations occurred later in the season for women (December-February).
Figure 1.
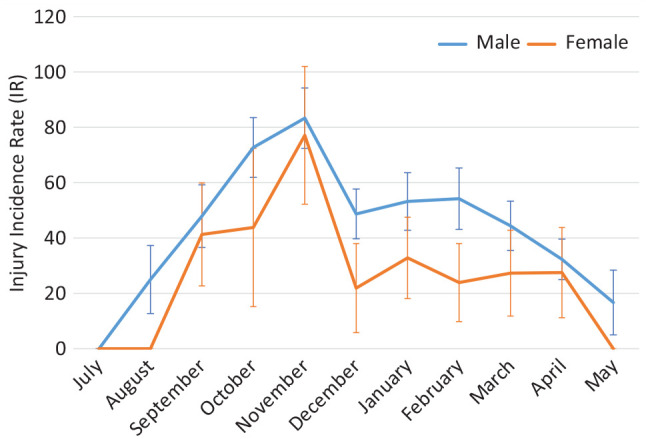
Seasonal variation of match injury occurrence for seasons 1 and 2 combined (IR/1000 player-hours).
During match play, female players had a high incidence of injury in the second quarter, which plateaued out across the third and fourth quarters (Figure 2). In comparison, the male players had a peak of injury occurrence in the third quarter. The fourth quarter of match play resulted in the majority of noncontact injuries in women (83%) compared with men (30%). The tackle event accounted for the majority of injuries for men and women, with 59% (men) and 61% (women) of tackle-related injuries occurring in the third and fourth quarters combined. Injuries occurring due to tackling or being tackled resulted in the same incidence rate for men (14.3/1000 player-hours); however, being tackled resulted in more injuries than tackling in women (11.9/1000 vs 8.8/1000 player-hours). This was followed by noncontact injuries in men (5.1/1000 player-hours) and ruck-related injuries in women (6.1/1000 player-hours).
Figure 2.
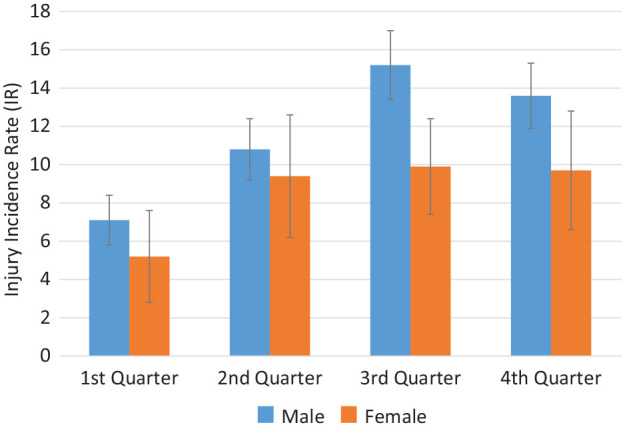
Timing of injury during match play for seasons 1 and 2 combined (IR/1000 player-hours).
Discussion
This study aimed to establish the incidence of injuries in Irish amateur rugby, and compare the incidence, nature, and severity of injuries in senior male and female amateur rugby, over 2 seasons. The high compliance rate of participating clubs allowed for both time-loss and non-time-loss injuries to be recorded and monitored for accurate injury rates and severity measured as total days of absence.
Incidence Rates
Incidence rates in both seasons for men were similar to the pooled incidence rate previously reported in the amateur game (46.8/1000 player-hours) 33 and lower than those of professional male players (81/1000 player-hours). 28 However, these rates were higher than those of previous studies in amateur male rugby (22.8/1000 player-hours), which may be due to the different injury definitions used. 21 Following the recent policy statement from World Rugby, 4 injury incidence rates in the current study were also reported using a >7-day time-loss injury definition and the resultant rate of 38/1000 player-hours remained high in comparison with other research. This may be due to the cohorts used, as the current study used a sample of amateur rugby players from the highest level of amateur play within Ireland, while the cohort used in the Rugby Football Union Community Rugby Injury Surveillance Project includes semiprofessional, amateur, and recreational players. 21 Injury rates may increase with increased levels of competitiveness 28 and therefore using the highest level of amateur players in Ireland may account for the higher incidence rate found here.
A decrease in injury incidence was found for female players during season 2 in comparison to season 1. The IRIS Project is the first longitudinal study to investigate injuries in the amateur female game using a 24-hour time-loss injury definition, and therefore understanding the observed differences in injury rates between male and female players over 2 seasons is a challenge. One possible explanation for the lower injury rate found in women may be due to physiological and anatomic differences between sexes.24,27 Player acceleration and tackler speed increases injury risk, and as female players may have lower levels of speed and power compared to male players, this may influence the forces experienced by players during a tackle-event.7,24 Another explanation may have been the number of matches played during the AIL season. In season 2, the female teams had fewer matches in the AIL as 1 team withdrew from competitive rugby, resulting in less match congestion and longer rest periods between matches. 6
Timing of Injury
Similar to the literature on professional rugby, the third quarter (40-60 minutes) of match play had the highest occurrence of injury for male players, 28 and this may be due to incomplete warm-up at half time, reduced concentration after the break in match play or the introduction of substitute players.19,28 Because of physiological differences observed in women, lower levels of strength and power may result in lower aerobic endurance capacity, particularly leading in to the half-time break may have resulted in the high rate of injuries reported in the second quarter.19,23 All noncontact injuries in the female players occurred in the second half of match play (third and fourth quarters), which may be due to fatigue as the match progressed, 23 particularly as female teams in the current study had smaller squad sizes and therefore less substitute players to use during the season. In the current study, the highest incidence of injury occurred in the first 3 months of the playing season (September-November), similar to recent findings in Rugby League. 9 This may have been due to low levels of participation in preseason training, inadequate preparation for the upcoming season, or potential spikes in training load.9,29 However, injury rates tended to increase once again toward the end of the season, likely due to cumulative fatigue, a smaller pool of available players, and increased competitiveness during the knock-out phases of the competition.6,14,29 The majority of muscle and tendon strains and ligament sprains in female players occurred in the early part of both seasons (September-November), which may be due to inadequate preparation during preseason or low levels of muscular strength.9,14,17 However, in male players, the majority of fractures and dislocations occurred early in the season, perhaps because of a lack of physical robustness, or unrefined tackle technique after the off-season period. 29 Further monitoring of these trends may highlight areas for future injury reduction strategies, focusing on adequate strength and conditioning training and preseason preparation.
Injury Diagnosis and Burden
Concussion and ankle ligament sprains were the most common diagnoses for both male and female players across both seasons. The majority of concussion injuries were to the tackler, which has been previously reported in the professional male game. 7 The mechanism of a concussion injury occurring is multifactorial, with tackle type, player acceleration, tackler speed, fatigue, and head contact type found to be influential.5,7 Modifications to tackle height has been trialed in an attempt to reduce head injury risk; however, the focus has been on the ball carrier and not the tackler.25,26 Further investigation into the effect of tackle height on the tackler is required as a potential avenue to reduce the risk of concussions. 7 Correct tackle technique may also contribute to reducing concussion injury risk7,11 and therefore the relationship between correct tackle technique and fatigue should be investigated. The majority of tackle-related injuries occurred in the second half of match play; thus, player fatigue may influence the tackle technique resulting in an increased risk of injury.5,13,26 Future prevention strategies should incorporate educational and training strategies for correct tackle technique, in conjunction with appropriate strength and conditioning training to ensure tackle technique is not affectes by player fatigue.5,13
Lower limb injuries are commonly reported in the literature on rugby injuries, and the current study recorded high rates of ankle ligament, knee ligament, and hamstring muscle injuries in male and female players. While anterior talofibular ligament injuries were the second most commonly diagnosed injury, ACL injuries carried the highest injury burden for men and women. Previous research has indicated that women are at a higher risk of ACL injury; however, similar incidence rates of ACL injury were observed for male and female players in the current study (0.8/1000 and 0.9/1000 player-hours, respectively). 2 While the rates of ACL injuries were similar, the severity and subsequent burden of ACL injury differed between male and female players, with female players incurring 307.2 days of absence per 1000 player-hours compared with male players (200.3 days of absence per 1000 player-hours).
The physical demands of rugby differ between playing position, with forwards more heavily involved in contact events than backs, 20 which may account for the higher rate of injuries sustained by male and female forwards in the current study. Overall, the female inside centers had the highest incidence rates in the women’s teams. Previous research has indicated that ‘mid-field backs’ (the inside and outside centers) make more tackles per match than “outside backs” (the wingers and fullbacks). 20 The differences in positional demands may be an influential factor in injury occurrence; however, in the current study, no significant associations between player position and injury mechanism were found.
There are many significant limitations to this study. Injury surveillance in amateur sport present additional difficulties compared with professional cohorts; however, the IRISweb system was designed specifically for an amateur cohort allowing both 24-hour time-loss injuries and non-time-loss injuries to be collected, 32 even where access to medical personnel was limited. Nonmedical professionals acting as injury recorders was likely a limitation. However, the ability to record both a “provisional diagnosis” and “final diagnosis” allowed time for the player to seek medical advice outside of the club if no medical professional was available in the club. 32
Conclusion
Concussion and ankle ligament injuries were the most common injuries in both male and female amateur rugby. In the female cohort, the high rate of noncontact injuries in the second half point to the need for strength and conditioning training programs to reduce fatigue-related injuries. Investigation into current warm-up practices, load management, and preseason preparation may assist in reducing the number of muscle strains and ligament sprains occurring early in the season. A high rate of fractures and dislocations were also reported early in the season for male players and further investigation into the physical demands of match play may aid the design of appropriate training regimes. Tailoring injury reduction strategies based on differences in positional demands may influence the effectiveness of the strategy.
Supplemental Material
Supplemental material, sj-docx-1-sph-10.1177_1941738121997145 for Injury Trends in Irish Amateur Rugby: An Epidemiological Comparison of Men and Women by Caithriona Yeomans, Ian C. Kenny, Roisin Cahalan, Giles D. Warrington, Andrew J. Harrison, Helen Purtill, Mark Lyons, Mark J. Campbell, Liam G. Glynn and Thomas M. Comyns in Sports Health: A Multidisciplinary Approach
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
The Irish Rugby Injury Surveillance (IRIS) project is funded and supported by the Irish Rugby Football Union (IRFU).
References
- 1. Bahr R, Clarsen B, Ekstrand J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med. 2018;52:1018-1021. [DOI] [PubMed] [Google Scholar]
- 2. Beynnon BD, Vacek PM, Newell MK, et al. The effects of level of competition, sport, and sex on the incidence of first-time noncontact anterior cruciate ligament injury. Am J Sports Med. 2014;42:1806-1812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bird YN, Waller AE, Marshall SW, Alsop JC, Chalmers DJ, Gerrard DF. The New Zealand Rugby Injury and Performance Project: V. Epidemiology of a season of rugby injury. Br J Sports Med. 1998;32:319-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Brown JC, Cross M, England M, et al. Guidelines for community-based injury surveillance in rugby union. J Sci Med Sport. 2019;22:1314-1318. [DOI] [PubMed] [Google Scholar]
- 5. Burger N, Lambert MI, Viljoen W, et al. Mechanisms and factors associated with tackle-related injuries in South African youth Rugby Union players. Am J Sports Med. 2017;45:278-285. [DOI] [PubMed] [Google Scholar]
- 6. Carling C, McCall A, Le Gall F, Dupont G. The impact of short periods of match congestion on injury risk and patterns in an elite football club. Br J Sports Med. 2016;50:764-768. [DOI] [PubMed] [Google Scholar]
- 7. Cross MJ, Tucker R, Raftery M, et al. Tackling concussion in professional rugby union: a case-control study of tackle-based risk factors and recommendations for primary prevention. Br J Sports Med. 2019;53:1021-1025. [DOI] [PubMed] [Google Scholar]
- 8. Dompier TP, Powell JW, Barron MJ, Moore MT. Time-loss and non-time-loss injuries in youth football players. J Athl Train. 2007;42:395-402. [PMC free article] [PubMed] [Google Scholar]
- 9. Fitzpatrick AC, Naylor AS, Myler P, Robertson C. A three-year epidemiological prospective cohort study of rugby league match injuries from the European Super League. J Sci Med Sport. 2018;21:160-165. [DOI] [PubMed] [Google Scholar]
- 10. Fuller CW, Molloy MG, Bagate C, et al. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Br J Sports Med. 2007;41:328-331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Fuller CW, Raftery M, Readhead C, Targett SG, Molloy MG. Impact of the International Rugby Board’s experimental law variations on the incidence and nature of match injuries in southern hemisphere professional rugby union. S Afr Med J. 2009;99:232-237. [PubMed] [Google Scholar]
- 12. Fuller CW, Taylor A, Kemp SP, Raftery M. Rugby World Cup 2015: World Rugby injury surveillance study. Br J Sports Med. 2017;51:51-57. [DOI] [PubMed] [Google Scholar]
- 13. Gabbett TJ. Influence of fatigue on tackling ability in Rugby League players: role of muscular strength, endurance, and aerobic qualities. PLoS One. 2016;11:e0163161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50:273-280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Gabbett TJ, Ullah S, Finch CF. Identifying risk factors for contact injury in professional rugby league players—application of a frailty model for recurrent injury. J Sci Med Sport. 2012;15:496-504. [DOI] [PubMed] [Google Scholar]
- 16. Holder Y, Peden M, Krug E, Lund J, Gururaj G, Kobusingye O, eds. Injury Surveillance Guidelines. World Health Organization; 2001. [Google Scholar]
- 17. Hulin BT, Gabbett TJ, Lawson DW, Caputi P, Sampson JA. The acute:chronic workload ratio predicts injury: high chronic workload may decrease injury risk in elite rugby league players. Br J Sports Med. 2016;50:231-236. [DOI] [PubMed] [Google Scholar]
- 18. King D, Hume P, Cummins C, et al. Match and training injuries in women’s Rugby Union: a systematic review of published studies. Sports Med. 2019;49:1559-1574. [DOI] [PubMed] [Google Scholar]
- 19. McCall A, Carling C, Davison M, et al. Injury risk factors, screening tests and preventative strategies: a systematic review of the evidence that underpins the perceptions and practices of 44 football (soccer) teams from various premier leagues. Br J Sports Med. 2015;49:583-589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Quarrie KL, Hopkins WG, Anthony MJ, Gill ND. Positional demands of international rugby union: evaluation of player actions and movements. J Sci Med Sport. 2013;16:353-359. [DOI] [PubMed] [Google Scholar]
- 21. RFU CRISP. RFU Community Rugby Injury Surveillance and Prevention Project RFU; 2018. Accessed November 10, 2019. https://www.englandrugby.com/participation/playing/player-welfare-rugby-safe/rugbysafe-research
- 22. Roberts SP, Trewartha G, England M, Stokes KA. Incidence and nature of medical attendance injuries in English community Rugby Union. Orthop J Sports Med. 2014;2:2325967114562781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Salgado E, Ribeiro F, Oliveira J. Joint-position sense is altered by football pre-participation warm-up exercise and match induced fatigue. Knee. 2015;22:243-248. [DOI] [PubMed] [Google Scholar]
- 24. Sekulic D, Spasic M, Mirkov D, Cavar M, Sattler T. Gender-specific influences of balance, speed, and power on agility performance. J Strength Cond Res. 2013;27:802-811. [DOI] [PubMed] [Google Scholar]
- 25. Tierney GJ, Richter C, Denvir K, Simms CK. Could lowering the tackle height in Rugby Union reduce ball carrier inertial head kinematics? J Biomech. 2018;72:29-36. [DOI] [PubMed] [Google Scholar]
- 26. Tierney GJ, Simms CK. Can tackle height influence head injury assessment risk in elite Rugby Union? J Sci Med Sport. 2018;21:1210-1214. [DOI] [PubMed] [Google Scholar]
- 27. Viviers PL, Viljoen JT, Derman W. A review of a decade of Rugby Union injury epidemiology: 2007-2017. Sports Health. 2018;10:223-227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Williams S, Trewartha G, Kemp S, Stokes K. A meta-analysis of injuries in senior men’s professional Rugby Union. Sports Med. 2013;43:1043-1055. [DOI] [PubMed] [Google Scholar]
- 29. Windt J, Gabbett TJ, Ferris D, Khan KM. Training load-injury paradox: is greater preseason participation associated with lower in-season injury risk in elite rugby league players? Br J Sports Med. 2017;51:645-650. [DOI] [PubMed] [Google Scholar]
- 30. World Rugby. Rugby World Cup. World Rugby; 2019. Accessed November 10, 2019. https://www.world.rugby/news/538379
- 31. World Rugby. World Rugby Year in Review 2018. World Rugby; 2018. Accessed November 10, 2019. http://publications.worldrugby.org/yearinreview2018/en/1-1/
- 32. Yeomans C, Kenny IC, Cahalan R, et al. The design, development, implementation and evaluation of IRISweb: a rugby-specific web-based injury surveillance system. Phys Ther Sport. 2019;35:79-88. [DOI] [PubMed] [Google Scholar]
- 33. Yeomans C, Kenny IC, Cahalan R, et al. The incidence of injury in amateur male Rugby Union: a systematic review and meta-analysis. Sports Med. 2018;48:837-848. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-sph-10.1177_1941738121997145 for Injury Trends in Irish Amateur Rugby: An Epidemiological Comparison of Men and Women by Caithriona Yeomans, Ian C. Kenny, Roisin Cahalan, Giles D. Warrington, Andrew J. Harrison, Helen Purtill, Mark Lyons, Mark J. Campbell, Liam G. Glynn and Thomas M. Comyns in Sports Health: A Multidisciplinary Approach