

Summary
We propose a weight-neutral strategy for obesity treatment on the following grounds: (1) the mortality risk associated with obesity is largely attenuated or eliminated by moderate-to-high levels of cardiorespiratory fitness (CRF) or physical activity (PA), (2) most cardiometabolic risk markers associated with obesity can be improved with exercise training independent of weight loss and by a magnitude similar to that observed with weight-loss programs, (3) weight loss, even if intentional, is not consistently associated with lower mortality risk, (4) increases in CRF or PA are consistently associated with greater reductions in mortality risk than is intentional weight loss, and (5) weight cycling is associated with numerous adverse health outcomes including increased mortality. Adherence to PA may improve if health care professionals consider PA and CRF as essential vital signs and consistently emphasize to their patients the myriad benefits of PA and CRF in the absence of weight loss.
Subject areas: Obesity medicine, Physical activity, Nutrition
Graphical abstract
Obesity medicine; Physical activity; Nutrition
Introduction
Obesity prevalence has increased dramatically over the past 40 years. Since 1980, the prevalence of obesity has doubled in more than 70 countries (GBD 2015 Obesity Collaborators et al., 2017). National Health and Nutrition Examination Survey (NHANES) data show that obesity prevalence in the United States increased from 30.5% in 1999-2000 to 42.4% in 2017-2018 (Hales et al., 2020). The 42.4% prevalence in 2017-2018 represents a ∼3-fold increase since the 1976-1980 NHANES (Hruby and Hu, 2015). Based on trends in the Behavioral Risk Factor Surveillance System surveys conducted between 1993 and 2016, prevalence of obesity in the United States is projected to reach nearly 50% by 2030, and severe obesity (defined as a body mass index (BMI) > 40 kg/m2) is expected to become the most common BMI category among women, non-Hispanic black adults, and low-income adults (Ward et al., 2019).
During approximately the same period that obesity prevalence increased, so did the prevalence of weight loss attempts (Han et al., 2019; Martin et al., 2018; Montani et al., 2015; Santos et al., 2017; Yaemsiri et al., 2011). Prevalence of weight loss attempts among U.S. adults increased from 34.3% to 42.2% between 1999-2000 and 2015-2016 (Han et al., 2019), and data from 2013-2016 NHANES indicated that 49.1% of U.S. adults tried to lose weight within the past 12 months (Martin et al., 2018). Overall, 66.7% of adults with obesity tried to lose weight (Martin et al., 2018). Since the late 1980s, the prevalence of dieting to lose weight has been at least 40% among U.S. women and at least 25% among U.S. men (Montani et al., 2015). Data from the United States are similar to worldwide prevalence of weight-loss attempts, as a meta-analysis of 72 studies, including 1,184,942 adults, revealed that 42% from the general population and 44% from ethnic-minority populations reported trying to lose weight (Santos et al., 2017). The increased prevalence of weight loss attempts is consistent with NHANES 2003-2008 data indicating that 73% of women and 55% of men reported a desire to weigh less (Yaemsiri et al., 2011).
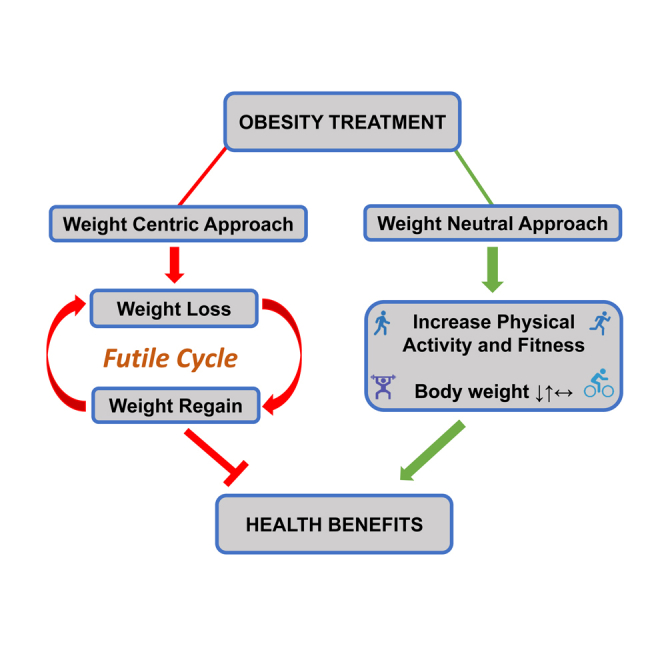
In sum, multiple surveys demonstrate a high prevalence of weight loss attempts over the past 40 years, during which, obesity prevalence has increased approximately 3-fold. Thus, the intense focus on weight loss has not prevented excessive weight gain in recent decades. Moreover, repeated weight loss efforts may contribute to weight gain, and is undoubtedly associated with the high prevalence of weight cycling, which is associated with significant health risks (Montani et al., 2006, 2015; Strohacker et al., 2009). This has created a “weight loss futile cycle” that characterizes the rising prevalence of both obesity and weight loss attempts over the past 4 decades (Figure 1). In addition, the increasing prevalence of obesity and weight loss attempts has been paralleled by an increase in body weight stigma (Tomiyama et al., 2018), which in turn is associated with many adverse health outcomes (Sutin and Terracciano, 2017; Tomiyama et al., 2018; Wu and Berry, 2018), including higher risk of all-cause mortality (Sutin et al., 2015). These risks disproportionately affect individuals with overweight and obesity.
Figure 1.

Weight loss futile cycle
The increased prevalence of obesity during the past 40 years is associated with an increased prevalence of weight loss attempts.
An important question is whether weight loss should be the primary focus of obesity treatment. Alternative approaches to treating obesity and associated comorbidities have been proposed wherein weight loss is not the primary endpoint (Bacon and Aphramor, 2011; Despres, 2015; Gaesser et al., 2011, 2015; Gaesser and Blair, 2019; King et al., 2009; Ross et al., 2015; Shaibi et al., 2015; Thyfault and Wright, 2016). However, the comparative benefits of weight loss vs. increasing physical activity (PA) or cardiorespiratory fitness (CRF) have not been published. Accordingly, the purpose of this review is to address two questions: (1) What is the magnitude of mortality risk reduction associated with intentional weight loss compared to that associated with increasing either PA or CRF? and (2) What is the magnitude of cardiovascular disease (CVD) risk marker reduction associated with weight loss interventions compared with that of PA interventions? Answers to these questions can help clarify the controversies surrounding the healthy obesity phenotype and the “fat but fit” concept (Brown and Kuk, 2015; Eckel et al., 2016; Hsueh et al., 2020; Huang et al., 2020; Kramer et al., 2013, 2014; Lin et al., 2020; Ortega et al., 2013, 2015, 2018; Roberson et al., 2014; Yeh et al., 2019). Answers to these questions are also relevant to the recommendations of the American Heart Association that CRF be considered as an important vital sign (Ross et al., 2016), which may be especially useful in risk classification of individuals with obesity-related comorbidities.
Despite the well documented importance of CRF as a vital sign (Ross et al., 2016), it is not even mentioned in current guidelines for management of overweight and obesity (Jensen et al., 2014; Garvey et al., 2016). Although PA is advocated, it is only in conjunction with a lifestyle program designed to lose weight. In other words, PA is viewed primarily as a means to create a negative energy balance. This overlooks the important health benefits of PA independent of weight loss. Consequently, answers to the two questions stated above are essential to clarify the comparative importance of weight loss and increasing PA and/or CRF for reducing obesity-related mortality and morbidity.
The BMI – mortality relationship: Influence of cardiorespiratory fitness and physical activity
Conventional wisdom holds that a high BMI increases mortality risk, with the BMI range of 18.5-<25 kg/m2 generally associated with lowest mortality risk, and risk increasing as BMI increases throughout the range of BMIs classified as overweight and obese (Aune et al., 2016; Global BMI Mortality Collaboration et al., 2016). However, the relationship between BMI and mortality is by no means clear-cut, as meta-analyses performed during the past 10 years have demonstrated (Aune et al., 2016; Flegal et al., 2013; Global BMI Mortality Collaboration et al., 2016; Jiang et al., 2019; Winter et al., 2017; Winter et al., 2014). Although some meta-analyses have indicated higher mortality risk among adults throughout the range of BMIs >25 kg/m2 (Aune et al., 2016; Global BMI Mortality Collaboration et al., 2016), others have not (Flegal et al., 2013; Jiang et al., 2019; Winter et al., 2014, 2017). In the meta-analysis by Flegal et al. (Flegal et al., 2013), the BMI range 25-<30 kg/m2 was associated with lower risk compared to the BMI range 18.5-<25 kg/m2, and grade I obesity (BMI 30-<35 kg/m2) was not associated with increased mortality risk. Among older adults, BMI associated with lowest mortality typically is observed in the BMI category considered overweight (Jiang et al., 2019; Winter et al., 2014, 2017).
Inconsistent findings from meta-analyses may be because of several behavioral and physical characteristics. Smoking, for example, may confound interpretation of the BMI-mortality relationship. But even restricting analyses to never-smokers does not always show that mortality risk is increased for all BMI >25 kg/m2 (Flegal et al., 2005; Jiang et al., 2019; Winter et al., 2014, 2017). This is consistently evident in older adults, in which lowest mortality risk in never-smokers occurs in the BMI range of ∼23-33 kg/m2 (Jiang et al., 2019; Winter et al., 2014). Failure to account for baseline health status may also confound the BMI-mortality relationship. However, even when restricting analyses to never smokers without pre-existing health conditions and deleting the first 5 years of follow-up, the general shape of the BMI-mortality relationship is similar, with increased risk observed at both the lower and higher ends of the BMI distribution (Flegal et al., 2017; Global BMI Mortality Collaboration et al., 2016; Yi et al., 2015). In addition, BMI does not account for differences in body composition and provides no information on body fat distribution. A recent pooled analysis from 7 prospective cohort studies showed that fat mass and fat-free mass have opposite associations with mortality (Sedlmeier et al., 2021), and regional body fat distribution has considerable impact on health outcomes (Despres, 2012; Piche et al., 2018). Finally, analyses of the association between BMI and mortality rarely consider CRF, which has considerable impact on mortality risk (Ross et al., 2016).
Cardiorespiratory fitness
The major limitation of the meta-analyses described above is that they did not include measures of CRF in their analyses. In studies that have included CRF, the mortality risk associated with high BMI is either eliminated (Barry et al., 2014) or greatly attenuated (Barry et al., 2018). In the first meta-analysis on the influence of CRF on the BMI-mortality relationship, Barry et al. (Barry et al., 2014) demonstrated that low CRF (unfit) is associated with a ∼2-2.5-fold higher risk of all-cause mortality regardless of BMI (Figure 2 top). Importantly, overweight and obesity in conjunction with moderate-to-high CRF (fit) were associated with a lower death rate than adults in the unfit normal-weight category. Of the 10 studies included in this meta-analysis, 6 cohorts included men only, 2 cohorts included women only, and 2 cohorts consisted of both men (∼80%) and women.
Figure 2.

Cardiorespiratory fitness, body mass index, and mortality risk
Joint associations between cardiorespiratory fitness (CRF), body mass index (BMI), and all-cause (top) and cardiovascular disease (CVD) (bottom) mortality. Hazard ratios reflect the pooled data from the meta-analyses of Barry et al. for all-cause mortality (Barry et al., 2014) and cardiovascular disease mortality (Barry et al., 2018). For all-cause mortality, the meta-analysis included 6 cohorts of men only, 2 cohorts of women only, and 2 cohorts of both men (~80%) and women. For CVD mortality, the meta-analysis included 8 cohorts of men only and 1 cohort of both men (89%) and women. Vertical lines for each bar represent 95% confidence intervals. Normal weight (BMI = 18.5-<25.0 kg/m2) and Fit is the referent group. Overweight = BMI 25.0-<30.0 kg/m2, and obese = BMI ≥30 kg/m2. “Fit” includes the top 75%–80% of age-adjusted CRF distribution. See text for details.
It is important to emphasize the definitions of fit and unfit in the meta-analysis of Barry et al. (Barry et al., 2014). Of the 10 studies included, 8 defined “unfit” as either the lowest quintile (7 studies) or quartile of age-adjusted CRF. Thus, the definition of “fit” in these studies was modest, and included the top 75%–80% of the age-adjusted CRF. This meta-analysis also demonstrated the importance of assessing CRF so that low-fit individuals can be identified for interventions to improve CRF.
A subsequent meta-analysis by Barry et al. (Barry et al., 2018), which included 8 cohorts of men only, and 1 cohort consisting of men (89%) and women, demonstrated that CRF greatly reduced CVD mortality risk associated with high BMI, and also highlighted the elevated CVD mortality risk among unfit individuals in the normal-weight BMI category (Figure 2 bottom). The pooled hazard ratios (HR) for the fit-overweight (HR = 1.25, 95% confidence interval 1.07-1.46) and the fit-obese (HR = 1.42, 95% confidence interval 1.01-4.07) categories indicate that CRF does not eliminate the CVD mortality risk associated with high BMI. Nonetheless, the data illustrate that low CRF is more hazardous than is high BMI. In fact, the data in Figure 2 clearly show that risks associated with higher BMI within both unfit and fit groups are much lower than the risks associated with low CRF regardless of BMI.
It is important to note that in the two meta-analyses of Barry et al., all but one of the included studies did not measure CRF directly but rather estimated CRF by time to exhaustion on a maximal exercise test. This is acceptable because correlations between test time on a maximal exercise test and directly measured maximal oxygen uptake (VO2max) are between 0.82 and 0.92 (Ross et al., 2016), respectively. However, measuring CRF directly by analyzing ventilation and gas exchange during a maximal exercise test not only provides a “gold standard” determination of CRF, but with simultaneous assessment of body composition, it also allows for VO2max to be expressed relative to total body weight (ml O2/kg/min) as well as to fat-free mass (FFM; ml O2/kg FFM/min). This is especially important when assessing and comparing CRF across BMI categories (Krachler et al., 2015). For individuals with the same test time on a maximal exercise test, nonobese and obese individuals will have essentially the same VO2max in ml/kg/min, but obese individuals will invariably have a higher VO2max in ml/kg FFM/min because of greater amounts of body fat relative to FFM (Lee et al., 1999). This might reflect “fitter” skeletal muscle and associated health benefits (Booth et al., 2012; Fiuza-Luces et al., 2013), and help explain the greatly reduced mortality risk associated with high CRF in persons with obesity (Figure 2). Importantly, it has been shown that adjustment for FFM increased the prognostic value of CRF in heart failure patients, especially among a subgroup of patients with obesity (Osman et al., 2000). In addition, it was recently reported that CRF in ml/kg FFM/min was a stronger predictor of all-cause mortality than CRF in ml/kg/min in a 19-year follow-up of 2,905 men and women with and without obesity (Imboden et al., 2020).
Even though adjustment for FFM improves the prognostic value of CRF testing, it is not likely that FFM per se is the underlying factor that explains this association. Among 21,925 men in the Aerobic Center Longitudinal Study (ACLS), highest relative risks for all-cause and CVD mortality were observed in unfit (defined as above, Figure 2) men with the highest amount of FFM (Lee et al., 1999). Lowest relative risks were observed for fit men regardless of FFM ranging from <60 kg to >70 kg. One plausible reason for this finding is that fit men are more physically active than unfit men (Ortega et al., 2018), and physical activity strongly affects CRF (Ross et al., 2016). Thus, even though FFM and body fat have opposite associations with mortality risk (Sedlmeier et al., 2021), the “quality” of FFM is more important than the “quantity” of FFM.
In addition to directly measured CRF, simpler estimates of functional capacity indicate that fitness reduces risk associated with high BMI (Zaccardi et al., 2019, 2021). In the UK Biobank cohort, men and women who characterized their usual walking pace as “brisk” had a much lower 7-year all-cause mortality risk and higher estimated 10-year survival compared to adults who characterized their usual pace as “slow,” and this was entirely independent of BMI ranging from ∼20 kg/m2 to ∼44 kg/m2 and body fat ranging from ∼25% to 47% for women and ∼15%–35% for men (Zaccardi et al., 2019).
Muscular fitness
Muscular fitness also is associated with reduced risk of chronic disease and mortality, and this association is independent of BMI (Carbone et al., 2020; Garcia-Hermoso et al., 2018; Kim et al., 2017; Saeidifard et al., 2019). One meta-analysis reported that high levels of handgrip strength and knee-extension strength were associated with lower risk of all-cause mortality (Garcia-Hermoso et al., 2018), and another meta-analysis reported that strength training was associated with lower risk of all-cause mortality (Saeidifard et al., 2019). Neither of these meta-analyses reported HRs for muscular fitness across BMI strata (i.e., as in Barry et al., above), but most of the studies included in these meta-analyses performed multivariate analyses that adjusted for BMI.
In the UK Biobank study, handgrip strength significantly attenuated the higher all-cause and CVD mortality risk associated several measures of adiposity (Kim et al., 2017). In some instances the risk was eliminated. For example, among men and women in the highest quintiles of handgrip strength, HRs for all-cause and CVD mortality were not significantly different when comparing the highest and lowest tertiles of percent body fat. When stratified by BMI, all-cause mortality HRs for the highest quintiles of handgrip strength in men were not different across all BMI categories including normal weight (18.5 - ≤25 kg/m2), overweight (25 - ≤30 kg/m2), and obese (≥30 kg/m2). In women, HRs for both all-cause and CVD mortality in the highest quintiles of handgrip strength were not different across BMI categories ranging from normal weight through grade 1 obesity (30 - <35 kg/m2).
Data on men in the ACLS demonstrated that lower all-cause and cancer mortality risks associated with higher levels of muscular fitness were independent of BMI, waist circumference, and percent body fat, and that the lower risk was observed even after adjusting for CRF (Ruiz et al., 2008, 2009). However, results from the ACLS also demonstrate that CRF has a stronger association with all-cause mortality risk than does muscular fitness.
Physical activity
No meta-analyses have been performed to demonstrate the impact of PA on the BMI-mortality relationship. Although PA is sometimes included in studies of the association between BMI and mortality, meta-analyses generally have avoided examining the impact of this vital behavior. One large meta-analysis did not include PA because the authors viewed it as “over-adjusting” for the contribution of BMI to mortality risk (Global BMI Mortality Collaboration et al., 2016). In another meta-analysis, the authors suggested that PA could attenuate the increased mortality risk observed in the underweight BMI category, but oddly did not acknowledge that the same might be true for the higher risk observed in the overweight or obese BMI categories (Aune et al., 2016). Nonetheless, several cohort studies suggest that PA has a mitigating influence on the BMI-mortality relationship that is qualitatively similar to, but not quantitatively as strong as, that of CRF (Fogelholm, 2010).
A systematic review of 12 cohort studies revealed that BMI was generally unrelated to mortality risk after adjustment for PA (Yerrakalva et al., 2015). Most of the studies reviewed indicated either no association or an inverse association between BMI and mortality after adjustment for PA. In the few studies that showed higher risk with high BMI, the risk generally did not increase until beyond BMI >30 kg/m2. The authors noted that PA measurement methods in all studies were subjective and mostly unvalidated. Therefore, more research utilizing objective PA assessments such as accelerometry is necessary to better capture the influence of PA on the BMI-mortality relationship.
Other epidemiological studies have shown that PA significantly reduces risk for all-cause mortality or CVD associated with high BMI (Bellocco et al., 2010; Crespo et al., 2002; Hu et al., 2005; Zhang et al., 2020). These studies generally show that both high BMI and low PA are associated with increased risk, and that the risk for physically active adults with obesity is comparable to or lower than the risk for inactive adults without obesity. For example, in the 2007-2016 NHANES cohort, compared to the referent group of sedentary adults with obesity, the 10-year CVD odds ratio among physically active adults with obesity (0.50, 95% confidence interval 0.37-0.69) was comparable to that of inactive adults with BMI in the normal weight range (0.42, 95% confidence interval 0.28-0.64) (Zhang et al., 2020). Even “insufficiently active” adults with obesity (i.e., 1-149 min/week of moderate-to-vigorous PA) had a significantly lower 10-year odds ratio of CVD (0.66, 95% confidence interval 0.49-0.89). It is important to note that physically active adults in the normal weight BMI range had the lowest risk (0.22, 95% confidence interval 0.16-0.29), indicating that both PA and BMI contribute to CVD risk. Even so, these NHANES data demonstrate that even modest amounts of PA are associated with significantly lower CVD risk independent of BMI.
Intentional weight loss and mortality
Meta-analyses of observational studies
Several meta-analyses have been published on the relationship between intentional weight loss and mortality risk (Figure 3 top) (Chen et al., 2018; Harrington et al., 2009; Kritchevsky et al., 2015; Ma et al., 2017; Pack et al., 2014; Schellenberg et al., 2013; Singh et al., 2019). In the first meta-analysis on intentional weight loss and all-cause mortality, which was based on results from prospective cohort studies, Harrington et al. (Harrington et al., 2009) reported that intentional weight loss was associated with a 13% lower risk for individuals classified as unhealthy (4 studies), and a 16% lower risk among unhealthy adults with obesity (4 studies). However, intentional weight loss was associated with an 11% higher mortality risk among healthy individuals (8 studies) and a 9% higher risk among mostly healthy adults without obesity (5 studies). Among healthy adults with obesity, intentional weight loss was not associated with a lower mortality risk.
Figure 3.

Intentional weight loss and mortality risk
Meta-analyses of the association between intentional weight loss and risk for all-cause mortality (top) and cardiovascular disease (CVD) mortality or major adverse coronary event (MACE) (bottom). Vertical lines for each bar represent 95% confidence intervals. For both top and bottom graphs, the different colored bars identify observational studies (red bars) and randomized control trials (RCTs) (blue bars).
Two additional meta-analyses of cohort studies that included participants with obesity or type 2 diabetes (T2D) (Chen et al., 2018) or coronary artery disease (Pack et al., 2014), reported that intentional weight loss was not associated with lower all-cause mortality risk (Figure 3 top). These meta-analyses should be viewed with caution owing to the small number of studies included (Chen et al. included 3 studies; Pack et al. included only 1 study). In a meta-analysis that included 4 studies (Pack et al., 2014), “presumed” intentional weight loss was associated with a 33% reduction in a composite outcome of all-cause mortality, CVD mortality, and major adverse cardiac events (MACE) (Figure 2 bottom).
Meta-analyses of randomized controlled trials
Four meta-analyses of randomized controlled trials (RCT) have been published on the effect of intentional weight loss on all-cause mortality (Figure 3 top) (Kritchevsky et al., 2015; Ma et al., 2017; Schellenberg et al., 2013; Singh et al., 2019). Only one showed a significantly lower mortality risk associated with intentional weight loss (Ma et al., 2017). However, the results of this meta-analysis (Ma et al., 2017), as well as that of Kritchevsky et al. (Kritchevsky et al., 2015), should be viewed with considerable caution because of the extremely limited mortality data of most of the studies included in these meta-analyses. Of the 34 intervention studies included in the meta-analysis of Ma et al. (Ma et al., 2017), 23 had 1 or 0 deaths reported in either the intervention group or the control group. Of the 12 lifestyle interventions included in the meta-analysis of Kritchevsky et al. (Kritchevsky et al., 2015), only 3 considered mortality as an endpoint, whereas the remaining studies reported death as an adverse event. Moreover, 7 of the 12 studies included in this meta-analysis reported 2 or fewer deaths in either the intervention or control groups. In fact, only 10 studies included in either meta-analysis reported at least 5 deaths in either intervention or control groups. Of these 10 studies, only one reported a statistically significantly lower all-cause mortality risk associated with weight loss.
For CVD mortality, the one meta-analysis of RCTs showed no benefit of intentional weight loss (Figure 3 bottom) (Ma et al., 2017). Among the 8 RCTs included in this meta-analysis, the Look AHEAD trial (Look Ahead Research Group, 2013) represented 81.7% of the weight in the analysis. This large trial was stopped for futility because results failed to demonstrate a difference in the rate of mortality, nonfatal myocardial infarction or stroke, or hospitalization for angina, among patients with T2D randomized to an intensive lifestyle intervention arm compared to patients randomized to a control arm, despite significantly greater weight loss in the intervention group.
In the most recent meta-analysis, which included 31 RCT lifestyle interventions (Singh et al., 2019), intentional weight loss among adults with overweight or obesity was not associated with a statistically significant reduction in all-cause mortality, although the odds ratio of 0.86 (95% confidence interval 0.73-1.02, p = 0.09) was very close to statistical significance (Figure 3 top). Weight loss averaged 3.63 kg greater than the control group after 1 year, and this decreased over time to a 2.45 kg difference after 3 years. Mortality was not different by amount of weight loss.
Although lifestyle interventions have shown to reduce risk of T2D (Knowler et al., 2002; Tuomilehto et al., 2001), a meta-analysis of lifestyle interventions in patients with, or at risk for, T2D indicated that intentional weight loss did not reduce risk of all-cause mortality (risk ratio 0.75, 95% confidence interval 0.53-1.06; Figure 2 top) (Schellenberg et al., 2013). However, only two studies were included in this meta-analysis.
Overall, data from observational studies and RCTs do not consistently show that intentional weight loss is associated with reduced mortality risk. Even in those studies that demonstrated a benefit of weight loss, it is not clear whether the weight loss itself was the primary factor that reduced the mortality risk. This is because the RCTs included in the weight loss meta-analyses invariably incorporated changes in diet and/or exercise, either as a program that participants could attend or as advice. As discussed in subsequent sections, increases in PA are consistently associated with reductions in mortality risk independently of changes in weight.
Weight loss via liposuction: impact on cardiovascular risk markers
To untangle the effects of lifestyle behaviors vs. weight loss per se, studies examining the cardiometabolic effects of liposuction are instructive. Surgical removal of body fat in the absence of lifestyle changes does not usually improve CVD risk profile, as reported in the three published meta-analyses on this subject (Boriani et al., 2014; Danilla et al., 2013; Seretis et al., 2015a). Although one meta-analysis showed a modest reduction in fasting insulin (Boriani et al., 2014), the other two showed no benefit of liposuction on insulin sensitivity (Danilla et al., 2013; Seretis et al., 2015a). The amount of body fat removed in these liposuction studies (∼1-16 L) is comparable to, or greater than, the amount of weight loss typically observed with lifestyle interventions that improve markers of cardiometabolic health (Gaesser et al., 2011; Gaesser and Blair, 2019). This diminishes the proposition that body fat is the primary cause of elevated CVD risk markers associated with obesity. However, because liposuction is limited to removal of subcutaneous fat, these studies cannot address the significance of ectopic fat and visceral abdominal fat (VAT) for cardiometabolic health (see later section, “Exercise targets ‘unhealthy’ fat”).The lack of improvement in cardiometabolic risk profile after liposuction may be due in part to redistribution of body fat after this procedure. Compensatory increases in VAT have been reported after liposuction (Benatti et al., 2012; Hernandez et al., 2011; Seretis et al., 2015b). Importantly, exercise may prevent this from occurring (Benatti et al., 2012). In a randomized trial of 36 women who underwent small-volume liposuction, removing an average of 1.23 ± 0.36 L of abdominal fat, 18 women who remained sedentary after liposuction experienced a 9.5% increase in VAT at the 6-month follow-up (Benatti et al., 2012). By contrast, 18 women who participated in an aerobic exercise program after liposuction experienced an 11.2% decrease in VAT.
Weight loss via bariatric surgery: impact on morbidity and mortality
Several meta-analyses indicate that bariatric surgery reduces risk of all-cause mortality (Cardoso et al., 2017; Pontiroli et al., 2020; Sheng et al., 2017). Bariatric surgery also reduces risk of macrovascular and microvascular disease, and increases remission rates for T2D (Pontiroli et al., 2020; Sheng et al., 2017). Because bariatric surgery also produces substantial weight loss, these data suggest that weight loss itself may be essential for the observed outcomes.
However, there are several issues that must be considered when interpreting the results of bariatric surgery studies. First, blood glucose and insulin concentrations are rapidly improved within days after surgery, long before appreciable weight loss occurs (Pories et al., 1995; Rubino and Gagner, 2002). Second, in adults with T2D, BMI trajectories after bariatric surgery are not good predictors of remission and relapse (Arterburn et al., 2013). In a study of 4,432 adults with T2D who underwent bariatric surgery, weight loss was virtually identical for those who had durable remissions compared to those who remitted and relapsed (Arterburn et al., 2013). In addition, cases who relapsed their T2D had similar, if not better, BMI maintenance after surgery compared to those who had durable remission. Third, a 2020 meta-analysis reported that the reduction in mortality risk after bariatric surgery was only observed in individuals above the median age in the 9 studies included in the meta-analysis (Pontiroli et al., 2020). The reasons for this finding are not completely understood, but the relatively low overall mortality risk among young persons with obesity may account for this finding. Fourth, two meta-analyses reported that PA levels increased significantly in patients after bariatric surgery (Adil et al., 2019; Herring et al., 2016), and increases in PA after bariatric surgery have been reported to be correlated to improvements in CRF (Bellicha et al., 2019). Increasing PA and CRF are associated with significant reductions in mortality risk, as discussed in the next section. Importantly, it is sedentary individuals (e.g., adults with obesity prior to bariatric surgery) who are likely to experience the greatest reductions in mortality risk by increasing PA and CRF (Kraus et al., 2019; Ross et al., 2016). For these reasons, the extent to which weight loss alone accounts for the improved longevity prospects after bariatric surgery must be interpreted with caution. Finally, it is important to note that the subject populations in bariatric surgery studies are mainly restricted to high-risk individuals with BMI >35 kg/m2 (Cardoso et al., 2017; Pontiroli et al., 2020; Sheng et al., 2017). Thus, results from bariatric surgery studies may not be easily generalizable to most of the population who have BMI <35 kg/m2.
Increasing physical activity or cardiorespiratory fitness: consistent reductions in mortality risk
In contrast to the inconsistent and inconclusive results of intentional weight loss, increasing either PA (Aggio et al., 2020; Gregg et al., 2003; Kieffer et al., 2019; Lewis et al., 2018; Manson et al., 1999; Mok et al., 2019; Ostergaard et al., 2018; Paffenbarger et al., 1993; Petersen et al., 2012; Wannamethee et al., 1998) or CRF (Blair et al., 1995; Ehrman et al., 2017; Erikssen, 2001; Erikssen et al., 1998; Kokkinos et al., 2010; Lee et al., 2011; Prestgaard et al., 2019; Imboden et al., 2019a, 2019b; Laukkanen et al., 2016; Martin et al., 2013; Mikkelsen et al., 2020) is associated with significant reductions in all-cause and CVD mortality risk (Figures 4, 5, and 6). To our knowledge, no meta-analyses have been performed on the association between changes in either PA or CRF and mortality risk. Consequently, data in Figures 4, 5, and 6 represent results from individual cohort studies.
Figure 4.

Increases in physical activity are associated with reduced mortality risk
Observational studies showing the association between increases in physical activity (PA) and relative risks for all-cause mortality (top) and cardiovascular disease (CVD) mortality or coronary event (bottom). Vertical lines for each bar represent 95% confidence intervals. In studies where confidence intervals were not provided, p values are indicated. For Manson et al. (Manson et al., 1999) the p value represents the trend from lowest PA increase to highest PA increase categories. MVPA = Moderate-to-Vigorous PA.
Figure 5.

Increasing cardiorespiratory fitness status is associated with reduced mortality risk
Observational studies showing the association between increases in cardiorespiratory fitness (CRF) status and relative risks all-cause mortality (top) and cardiovascular disease (CVD) mortality or stroke (bottom). Vertical lines for each bar represent 95% confidence intervals. Increases in CRF status were generally defined as improving CRF by enough to no longer be in the “least fit” category of CRF.
Figure 6.

Increases in cardiorespiratory fitness are associated with reduced mortality risk
Observational studies showing the association between increases in cardiorespiratory fitness (CRF) and relative risks of all-cause mortality (top) and cardiovascular disease (CVD) mortality or major adverse coronary event (MACE) (bottom). Vertical lines for each bar represent 95% confidence intervals. For both top and bottom graphs the different colored bars represent risk reduction per 1-MET increase in CRF (orange bars) or per 1 mL/kg/min increase in CRF (green bars). MET = metabolic equivalent of resting metabolism, ~3.5 mL/kg/min.
With few exceptions, increasing PA is associated with a ∼15%–50% reduction in all-cause mortality and a ∼15%–40% reduction in CVD mortality or cardiovascular events (Figure 4). Greater reductions in all-cause mortality risk are typically observed with increases in CRF (Figure 5). When the improvement in CRF is expressed as moving from “unfit” or “low fit” to a higher fitness category, the reduction in all-cause mortality is in the range of 30%–60% (Figure 5 top). Some studies also reported changes in CRF as a continuous variable, either as a 1-MET or 1 mL/kg/min increase in measured or estimated CRF from maximal exercise tests (1 MET = metabolic equivalent of resting metabolism, ∼3.5 mL/kg/min). Each 1-MET increase in CRF was associated with a 14%–29% reduction in all-cause mortality, and each 1 mL/kg/min increase in CRF was associated with a 7%–13% reduction in all-cause mortality risk (Figure 6 top).
Fewer studies have published results on the change in CVD risk associated with changes in CRF. Moving from unfit or low-fit to fit was associated with a 42%–52% reduction in CVD mortality (Blair et al., 1995; Lee et al., 2011) and a 60% reduction in stroke (Prestgaard et al., 2019) (Figure 4 bottom). Increasing CRF by 1 MET was associated with a 19% lower risk of CVD mortality (Lee et al., 2011), and increasing CRF by 1 mL/kg/min was associated with a 15% reduction in risk of CVD mortality (Imboden et al., 2019b) and a 21% reduction in risk of major adverse cardiovascular events (Mikkelsen et al., 2020) (Figure 6 bottom).
In comparison to intentional weight loss, it is evident that the mortality risk reductions associated with increasing PA or CRF are far more consistent and generally of much greater magnitude. This may be attributable to the well-established effects of PA and exercise training on virtually every cell, organ, and system in the body (Booth et al., 2012; Fiuza-Luces et al., 2013). The “polypill” effect of exercise likely benefits individuals across the entire BMI spectrum (Gaesser et al., 2011, 2015). Although the prevalence of the “fit but fat” phenotype is relatively low (Duncan, 2010), this is likely attributable in large part to the lower levels of objectively measured PA in adults with high BMI (Tudor-Locke et al., 2010). Therefore, adults with overweight and obesity would benefit the most from strategies to increase PA, which could also increase CRF (see later discussion).
Does weight loss explain the reduced mortality risk associated with improvements in physical activity or cardiorespiratory fitness?
It is fair to ask whether weight loss could have contributed to the reduced mortality risk associated with increases in either PA or CRF. Unfortunately, most of the studies did not report data on weight change associated with changes in either PA or CRF. However, it is not likely that weight loss would have contributed appreciably to the reduced mortality risk associated with the PA activity or CRF. First, increasing PA typically results in little, if any, weight loss (Donnelly et al., 2009; Donnelly and Smith, 2005; Foright et al., 2018; Pontzer, 2015; Thorogood et al., 2011). In addition, several of the studies that included changes in body weight or BMI in their analyses indicated that weight loss was not a significant contributing factor, as described below.
In the ACLS, for example, the reduced mortality risk associated with an increase in CRF was independent of changes in BMI (Lee et al., 2011). Reductions in all-cause and CVD mortality were linearly related to increases in CRF but unrelated to changes in body weight and body fat percentage. In addition, men in the ACLS who showed a reduction in CRF experienced increases in all-cause and CVD mortality risk regardless of changes in BMI. This further emphasizes the importance of CRF compared to weight loss. In the Oslo Ischemia Study (Prestgaard et al., 2019), among men with low CRF at baseline, change in BMI was not different when comparing men who remained unfit with those who increased CRF, yet those who increased their CRF experienced a 34% lower all-cause mortality risk and a 60% lower risk of stroke during the follow-up.
In men and women from a large UK cohort, an increasing PA trajectory over a ∼10-year period was associated with a 22% lower all-cause mortality risk and a 24% lower CVD mortality risk even when adjusting for baseline BMI and changes in BMI at the final PA assessment (Mok et al., 2019). In a study of Danish adults, those who took up cycling experienced a 22% lower risk of all-cause mortality during a ∼10-13-year follow-up (Ostergaard et al., 2018), even though the initiation of cycling was not associated with reductions in body weight among those with overweight or obesity at baseline, nor did it reduce the incidence of overweight or obesity during the follow-up (Rasmussen et al., 2018). Cycling did, on the other hand, reduce the incidence of abdominal obesity during follow-up. This is important to emphasize because abdominal fat poses a greater health risk than general obesity and represents a relatively small percentage of total body fat (Piche et al., 2018; Despres, 2015) (see later section “Exercise targets ‘unhealthy’ fat”).
Pitfalls of focusing on weight loss: Weight cycling
Because weight loss is rarely sustained (Anderson et al., 2001; Dansinger et al., 2007; Sumithran and Proietto, 2013), and prevalence of weight loss attempts remains high (Han et al., 2019; Martin et al., 2018; McDow et al., 2019; Montani et al., 2015; Santos et al., 2017) and may be increasing (Han et al., 2019), weight cycling is also prevalent (Montani et al., 2015; Syngal et al., 1999; Fildes et al., 2015). There is no universally accepted definition of weight cycling (Montani et al., 2015). In research studies, weight cycling has variously been defined as achieving or exceeding a specified weight loss (in kg or as a percentage of baseline weight) for a specified number of times, or by using coefficient of variation, interpersonal standard deviation, or root-mean-square error of body weight change over time (Atkinson et al., 1994; Mehta et al., 2014; Zhang et al., 2019a, 2019b). Whether weight cycling poses a significant health risk has been debated over the years, with some suggesting no risk (Atkinson et al., 1994; Mehta et al., 2014), and others suggesting that it poses a significant health risk (Bangalore et al., 2017, 2018; Cheng et al., 2015; Cologne et al., 2019; Montani et al., 2006, 2015; Oh et al., 2019; Zhang et al., 2019a, 2019b; Zou et al., 2019). Three meta-analyses have been published on the association between weight cycling and mortality risk (Cheng et al., 2015; Zhang et al., 2019b; Zou et al., 2019). In the largest and most recent of these, Zou et al. (Zou et al., 2019) reported that weight cycling was associated with a 41% higher risk of all-cause mortality and a 36% higher risk of CVD mortality, but was not related to cancer mortality. The risk for all-cause mortality was observed in all BMI categories. Weight cycling was also associated with a 49% higher risk of CVD morbidity and a 35% higher risk of hypertension (Zou et al., 2019). In another recent meta-analysis that included 15 publications (22 cohorts), Zhang et al. (Zhang et al., 2019b) reported that weight cycling was associated with a 45% higher risk of all-cause mortality. Because most of the studies included in the two meta-analyses were the same, it is not surprising that the higher mortality risks (41% and 45%) were similar. In a meta-analysis that focused on older adults, weight cycling was associated with a 53% higher risk of all-cause mortality (Cheng et al., 2015).
In two recent studies not included in these meta-analyses, weight cycling was also associated with a higher risk of all-cause mortality (Cologne et al., 2019; Oh et al., 2019). Body weight variability is also associated with adverse outcomes in adults with T2D and with coronary artery disease (Bangalore et al., 2017, 2018). In patients enrolled in one of three clinical trials of statins, high weight variability was associated with increased risk of coronary events and mortality. Compared to the lowest quintile of weight variability, participants in the highest quintile of weight variability had a 59% higher risk of any coronary event, an 82% higher risk of major coronary event or death, a 75% higher risk of any cardiovascular event, a 99% higher risk of myocardial infarction, and a 92% higher risk of stroke (Bangalore et al., 2017, 2018). The greatest risk was observed in patients with overweight and obesity. It is among these individuals that weight loss attempts (Martin et al., 2018) and weight cycling (Syngal et al., 1999; Fildes et al., 2015) are more prevalent.
The risks associated with weight cycling are very much the same as those associated with obesity (Montani et al., 2006, 2015). Just as few epidemiological studies of the relationship between BMI and mortality have accounted for the influence of CRF, none of the meta-analyses of the BMI-mortality relationship has accounted for the potential contributions of weight cycling to the higher mortality risk observed in the high BMI categories. Severe weight cyclers, for example, are more likely to engage in unhealthy weight loss practices (e.g., vomiting, binge eating, use of laxatives) and less likely to exercise (Field et al., 2004). Because weight cycling is more prevalent among individuals with high BMI (Syngal et al., 1999; Fildes et al., 2015), it is entirely plausible that some of the morbidity and mortality risks associated with high BMI may be because of weight cycling.
Additional support for this plausibility comes from the observations that weight cycling is associated with increased risk for sarcopenic obesity (Rossi et al., 2019), as weight regain following weight loss is typically characterized by greater gain of fat mass compared with fat-free mass (Bosy-Westphal et al., 2013; Goisser et al., 2015; Houston et al., 2019). This may have adverse consequences for weight cyclers because sarcopenic obesity is associated with a 24% higher risk of all-cause mortality, as reported in a meta-analysis of 12 cohorts (Tian and Xu, 2016). Weight cycling in men and women with obesity is also associated with lower handgrip strength (Rossi et al., 2019), which could increase mortality risk as discussed earlier (Garcia-Hermoso et al., 2018).
Cardiometabolic health improvement: Physical activity vs. weight loss
It is well established that weight loss is associated with improvements in obesity-related health conditions, including cardiometabolic risk markers for CVD and T2D. These benefits have been reported in 8 meta-analyses of RCTs on the effects of weight loss on CVD risk factors (Franz et al., 2015; Khera et al., 2018; Mudaliar et al., 2016; Zomer et al., 2016; Neter et al., 2003; Dattilo and Kris-Etherton, 1992; Hasan et al., 2020; Semlitsch et al., 2021). Most of the RCTs included in these meta-analyses have used energy-restricted dietary approaches to achieve weight loss, although some have also included a PA component to enhance the energy deficit. However, the improvements in cardiometabolic risk markers associated with weight loss interventions are generally no greater than exercise training interventions without a specific weight loss target.
Blood pressure
For example, both aerobic exercise training (Cornelissen and Fagard, 2005b; Cornelissen and Smart, 2013) and resistance exercise training (Ashton et al., 2020; Cornelissen and Fagard, 2005a; Cornelissen et al., 2011) reduce systolic and diastolic blood pressures by ∼2-5 mmHg in normotensive individuals, and by ∼5-7 mmHg in those with hypertension (Cornelissen and Fagard, 2005b). These reductions occur despite minimal weight loss and decreases in percent body fat (Cornelissen and Fagard, 2005b; Cornelissen et al., 2011). Although a tendency for larger decreases in blood pressure with greater reductions in weight has been reported (Cornelissen and Smart, 2013), these relationships were not statistically significant. In addition, an earlier review reported clinically insignificant correlations between changes in body weight and changes in either systolic blood pressure (r = 0.09) and diastolic blood pressure (r = 0.07), suggesting that the weight loss contribution to lower blood pressure after exercise training is very small (Fagard, 2001).
By comparison, meta-analyses of weight loss interventions show that weight reduction is typically associated with decreases in systolic and diastolic blood pressure in the range of 1-5 mmHg (Franz et al., 2015; Khera et al., 2018; Mudaliar et al., 2016; Zomer et al., 2016; Neter et al., 2003; Semlitsch et al., 2021). Thus, the blood pressure-lowering effect of exercise training is at least as great as that observed with weight loss interventions.
Glycemic control
Weight loss is routinely advocated for improvements in blood glucose control, and meta-analyses indicate that weight loss is typically associated with lowering of HbA1c in the range of 0.2%–0.9% (Franz et al., 2015; Mudaliar et al., 2016; Zomer et al., 2016). But meta-analyses of exercise training studies show that both aerobic and resistance exercise can lower HbA1c by a similar amount, i.e., ∼0.2%–0.8% (Boule et al., 2001; Jelleyman et al., 2015; Liu et al., 2019; Snowling and Hopkins, 2006). In a meta-analysis by Boule et al. (Boule et al., 2001), exercise training in patients with T2D reduced HbA1c by an average of 0.66% despite no difference in weight change between exercise and control groups. Although a small amount of weight loss may accompany exercise training, weight loss itself does not appear to explain the reduction in HbA1c. A meta-analysis of 27 exercise training studies in patients with T2D showed that HbA1c was reduced by 0.7% after aerobic training and by 0.8% after combined aerobic and resistance exercise training (Snowling and Hopkins, 2006). Although some weight loss was observed after both modes of exercise training, the magnitude of weight loss after combined training (5.1%) was more than three times higher than that after aerobic training alone (1.5%). In addition, resistance training alone reduced HbA1c by 0.5% despite no significant change in body weight (0.5%). These data demonstrate that the relationship between body weight, adiposity, and markers of glycemic control are far from linear and are not likely mediated by weight loss. This complex relationship is best underscored by the observation that gastric bypass surgery routinely results in rapid induction of T2D remission within days, well before any significant weight loss occurs (Rubino and Gagner, 2002).
Blood lipids
Improvements in blood lipids with exercise training are also comparable to those observed with weight-loss interventions. Meta-analyses indicate that exercise training increases high-density lipoprotein cholesterol by 2-5 mg/dL (Kodama et al., 2007; Pattyn et al., 2013; Wewege et al., 2018; Igarashi and Nogami, 2019; Lin et al., 2015), which is comparable to the 1-4 mg/dL improvements observed after weight-loss interventions (Franz et al., 2015; Khera et al., 2018; Mudaliar et al., 2016; Dattilo and Kris-Etherton, 1992; Hasan et al., 2020). In addition, the 3-10 mg/dL reductions in low-density lipoprotein cholesterol after exercise training (Halbert et al., 1999; Igarashi and Nogami, 2019; Lin et al., 2015) are similar to the 1-15 mg/dL reductions reported in meta-analyses of weight loss studies (Dattilo and Kris-Etherton, 1992; Franz et al., 2015; Hasan et al., 2020; Khera et al., 2018; Zomer et al., 2016). Reductions in fasting triglycerides of 5-25 mg/dL reported in meta-analyses of exercise training studies (Ostman et al., 2017; Wewege et al., 2018; Igarashi and Nogami, 2019; Lin et al., 2015) are slightly less than the 11-58 mg/dL reductions observed after weight-loss interventions (Franz et al., 2015; Zomer et al., 2016; Dattilo and Kris-Etherton, 1992).
Average weight loss in exercise training studies is minor, differing by < 0.50 kg from control groups and is not significantly correlated with the improvements in blood lipids (Halbert et al., 1999).
Vascular function
Vascular function has been reported to be impaired in obesity (Arcaro et al., 1999; Ne et al., 2017; Toda and Okamura, 2013) and improved by weight loss (Joris et al., 2015). In a meta-analysis of weight-loss studies that excluded interventions in which weight loss was achieved by exercise alone, weight loss averaging 8.6 kg improved flow-mediated dilation (FMD) by 3.29% in 4 RCTs (Joris et al., 2015). In 33 studies without a control group, a 2.66% improvement in FMD was observed when weight loss exceeded the median level of weight loss (mean weight in these studies = 18.8 kg), and a 0.78% improvement in FMD was observed when weight loss was below the median level (mean weight loss in these studies = 5.7 kg). Meta-regression suggested that a 10-kg weight loss was associated with a 1.11% improvement in FMD.
By comparison, several meta-analyses of exercise training studies indicated that exercise training is associated with an increase in FMD of approximately 1%–4% (Early et al., 2017; Pearson and Smart, 2017; Ramos et al., 2015). Thus, the improvements in FMD reported in exercise training studies are comparable to those observed with weight-loss interventions. The meta-analyses of exercise training studies did not consider the potential contribution of weight loss or fat loss to the improvements in FMD. However, weight loss in exercise training studies is usually minimal (Donnelly et al., 2009; Donnelly and Smith, 2005; Foright et al., 2018; Pontzer, 2015; Thorogood et al., 2011), and certainly less than the median weight loss of 5.7 kg reported for weight-loss interventions (Joris et al., 2015). This strongly suggests that the impact of exercise on vascular function is largely independent of weight loss.
Exercise targets “unhealthy” fat
Ectopic fat, including VAT and fat stores in the liver and other lean tissues, is associated with increased risk of CVD and T2D (Piche et al., 2018; Despres, 2015). Sedentary individuals with obesity typically have high levels of ectopic fat, and this may contribute in large part to the higher mortality risk associated with obesity.
Although exercise training typically does not lead to significant reductions in body weight or total body fat, exercise training can significantly reduce visceral and ectopic fat. This may explain why exercise interventions routinely are associated with improvements in cardiometabolic risk profiles with little, if any, weight loss. Meta-analyses of aerobic exercise training in adults with overweight or obesity demonstrate that exercise significantly reduces VAT and hepatic fat (Ismail et al., 2012; Keating et al., 2012, 2015a, 2015b; Sabag et al., 2017; Vissers et al., 2013). In these studies, weight loss is frequently less than 1 kg.
Weight loss is associated with a reduction in VAT, but exercise training tends to be more effective at reducing VAT despite significantly less total weight loss (Verheggen et al., 2016). Although reduction in VAT is correlated to total weight loss after both exercise training and caloric restriction, the loss of VAT is ∼50% greater with exercise training for a given amount of weight loss (Verheggen et al., 2016). For perspective, consider the lower end of current weight loss recommendations, ∼5% body weight (Garvey et al., 2016; Jensen et al., 2014; Kushner, 2018; Kushner and Ryan, 2014). A 5% weight loss via exercise training is associated with a 21.3% reduction in VAT, whereas the same weight loss achieved via caloric restriction is associated with only a 13.4% reduction in VAT. To achieve the same amount of VAT reduction as a 5% weight loss by caloric restriction, a weight loss of only 2-3% is needed through exercise training.
A meta-analysis of adults with T2D demonstrated that exercise training was associated with a significant reduction in VAT despite minimal overall weight loss (Sabag et al., 2017). Although large weight losses, e.g., with severe energy-restricted dieting or bariatric surgery, are associated with greater reductions in VAT and ectopic fat than occurs with exercise training (Sabag et al., 2017), it is important to identify strategies that are effective for reducing VAT and ectopic fat in the face of minimal weight loss. Most of the studies included in the meta-analyses of exercise training and ectopic fat loss used exercise interventions consistent with current public health guidelines (Piercy et al., 2018). These may be more sustainable than very low-energy-restricted dieting, and are not invasive like bariatric surgery.
Reducing hepatic fat may be more important than loss of VAT for lowering risk of cardiovascular disease and T2D (Fabbrini et al., 2009). For a given amount of VAT, higher amounts of hepatic fat are associated with the dysmetabolism associated with obesity, particularly greater insulin resistance. This is relevant because even in individuals with high amounts of hepatic fat, this fat depot comprises only ∼1% of total body fat (Fabbrini et al., 2009). Although the magnitude of reduction in hepatic fat is correlated with the amount of weight loss, clinically significant reductions in hepatic fat are achieved even with relatively little weight loss (Koutoukidis et al., 2021; Hens et al., 2016). Hepatic fat is reduced via exercise training even when weight loss is negligible (Hens et al., 2016; Keating et al., 2012, 2015a, 2015b; Sabag et al., 2017). Consequently, this may help explain the well-documented beneficial effects of regular exercise for reducing risks of CVD and T2D.
Exercise improves “fitness” of adipose tissue
In addition to reducing levels of VAT and ectopic fat, exercise also has important effects on white adipose (Dewal and Stanford, 2019; Dollet and Zierath, 2019; Lehnig et al., 2019; Lehnig and Stanford, 2018; Stanford and Goodyear, 2018; Stanford et al., 2015; Townsend et al., 2017; Riis et al., 2019). Exercise training induces molecular adaptations in white adipose that increase mitochondrial biogenesis and insulin sensitivity (Dewal and Stanford, 2019; Dollet and Zierath, 2019; Riis et al., 2019). The improved insulin sensitivity in adipose tissue partly mediates exercise training-induced improvements in glucose tolerance (Dollet and Zierath, 2019), and is independent of significant weight loss (Riis et al., 2019; Stanford and Goodyear, 2018). In rodent models, transplantation of white adipose tissue from exercise-trained animals into sedentary animals has been shown to reduce fasting concentrations of blood glucose, insulin, and cholesterol, and increase glucose tolerance (Lehnig and Stanford, 2018; Stanford et al., 2015). Transplant-recipient animals also demonstrate increased insulin-stimulated glucose uptake in their skeletal muscle (Lehnig and Stanford, 2018). These studies indicate that exercise-induced adaptations in white adipose tissue improve whole-body metabolic health, and illustrate that adipose tissue serves as an important endocrine tissue that undergoes beneficial adaptations to exercise (Stanford and Goodyear, 2018). It has been suggested that exercise may increase the secretion of myokines and adipokines that facilitate “cross-talk” between muscle and adipose tissue to improve overall metabolic health (Stanford and Goodyear, 2018). These studies should not be interpreted to reject the effect of weight loss on insulin sensitivity, as weight loss achieved via caloric restriction improves insulin sensitivity in white adipose tissue (Mileti et al., 2021; Eriksson-Hogling et al., 2015). However, as demonstrated by the studies described above, weight loss is not a prerequisite for improvement in insulin sensitivity.
Healthy obesity phenotype: Importance of cardiorespiratory fitness and physical activity
The metabolically healthy obese (MHO) phenotype has been acknowledged since at least 2001 (Sims, 2001). Since then, the number of publications on the metabolically healthy (or unhealthy) phenotype has increased dramatically (Ortega et al., 2018). There has been considerable discussion and debate over the MHO phenotype and whether there is such a thing as “healthy obesity” (Brown and Kuk, 2015; Eckel et al., 2016; Kramer et al., 2013, 2014; Ortega et al., 2013, 2015, 2018; Roberson et al., 2014; Hsueh et al., 2020; Huang et al., 2020; Lin et al., 2020; Yeh et al., 2019).
The MHO phenotype has typically been defined as having no more than one component of the metabolic syndrome or the absence of the metabolic syndrome (which may permit up to two components of the metabolic syndrome). Further complicating interpretation of mortality and chronic disease risk associated with MHO is the fact that criteria used to define the metabolic syndrome also vary across studies (Eckel et al., 2016). The lack of standardized criteria used to define MHO has undoubtedly contributed to confusion as to whether the MHO phenotype is truly healthy and absent of risk relative to metabolically healthy normal weight (MHNW) individuals. Regardless, defining MHO as allowing even one component of the metabolic syndrome is problematic because it could be argued that such a phenotype is not truly metabolically healthy.
Furthermore, dichotomizing obesity phenotypes into “healthy” and “unhealthy” based on cut-points for continuous variables used to define the metabolic syndrome discounts the additive effect of accumulating multiple risk factors used to define the metabolic syndrome. To improve risk stratification of obesity, staging systems such as the Edmonton Obesity Staging System (EOSS) (Kuk et al., 2011; Sharma and Kushner, 2009) and the Cardiometabolic Disease Staging (CMDS) (Guo and Garvey, 2017; Guo et al., 2014) system have been developed. These systems use a 5-point scale that essentially stratifies the risks ranging from individuals having no obesity-related cardiometabolic risk markers (stage 0) to individuals with severe (potentially end-stage) disabilities from obesity-related chronic diseases such as T2D and CVD (stage 4). Both staging systems have been shown to improve risk stratification associated with obesity-related comorbidities and may provide clinicians with a useful approach to identify individuals with obesity who may benefit the most from treatment to reduce risk.
One major limitation of the EOSS and CMDS is that they do not consider PA or CRF in the risk assessment. In fact, virtually all studies to date, including most reviews and meta-analyses, have not included assessments of PA and CRF to characterize MHO (Brown and Kuk, 2015; Eckel et al., 2016; Hsueh et al., 2020; Huang et al., 2020; Kramer et al., 2013, 2014; Lin et al., 2020; Yeh et al., 2019). This is important because individuals with MHO engage in more moderate-to-vigorous PA and have a higher level of CRF than individuals with a metabolically unhealthy obesity (MUO) phenotype, and also spend less time in sedentary behaviors (Ortega et al., 2018). Each of these could contribute to morbidity and mortality risk (Kodama et al., 2009; Kraus et al., 2019; Patterson et al., 2018). Because individuals with the MHO phenotype are more physically active, it is likely that the exercise-induced adaptations in adipose tissue, described in the previous section, contribute to the reduced cardiometabolic risk associated with the MHO phenotype.
Although most reviews and meta-analyses indicate that MHO is associated with reduced mortality and CVD risk compared to MUO, risk is not eliminated, i.e., when compared to MHNW (Hsueh et al., 2020; Huang et al., 2020; Kramer et al., 2013; Lin et al., 2020; Yeh et al., 2019). These studies, however, did not include measures of CRF or PA. In studies that included CRF in their statistical analyses, higher mortality risk associated with MHO was eliminated (Ortega et al., 2015, 2018; Roberson et al., 2014). When PA was accounted for, CVD morbidity and mortality remained elevated by 24% compared to MHNW, but all-cause mortality was not different between the two groups (Ortega et al., 2018). Therefore, as discussed above, PA may not be sufficient to eliminate the higher CVD risk associated with MHO. These studies do, however, highlight the necessity of including CRF and/or PA in risk assessment of MHO.
Optimization of physical activity and cardiorespiratory fitness
The American Heart Association (AHA) recommends that CRF be measured in clinical practice as a vital sign (Ross et al., 2016), and the “Exercise is Medicine” initiative jointly launched in 2007 by the American College of Sports Medicine (ACSM) and the AHA recommends that PA be assessed as a vital sign (Cowan, 2016). Routine assessment of CRF and PA would allow for identification of individuals who would benefit from increased PA. Because individuals with overweight or obesity are generally less active (Tudor-Locke et al., 2010) and have lower levels of CRF (Duncan, 2010) than their thinner counterparts, it is this population of adults with high BMI that stands to benefit the most by increasing PA (Kraus et al., 2019; Ross et al., 2016). Increasing PA, especially if it includes moderate-to-vigorous-intensity activity, would also have the effect of increasing CRF. We have shown that adults with obesity can increase CRF by ≥ 1 MET after just 8 weeks of either moderate-intensity continuous or high-intensity interval exercise training (Sawyer et al., 2016). This occurred despite no loss of body weight or body fat. As discussed above (Figure 6), an increase in CRF of 1 MET is associated with a 14%–29% lower risk of all-cause mortality and a 19% lower risk of CVD mortality. These reductions are equal to, or greater than, the reductions associated with weight loss (Figure 3).
Because of the poor success rates for long-term weight-loss maintenance (Anderson et al., 2001; Dansinger et al., 2007; Sumithran and Proietto, 2013), and because exercise training rarely results in significant weight loss for most adults (Donnelly et al., 2009; Donnelly and Smith, 2005; Foright et al., 2018; Thorogood et al., 2011), it is essential to encourage PA as more than just a tool to produce an energy deficit. Broadly speaking, the ACSM recommendation is to sit less and move more. Further, specific aerobic activity recommendations for adults are to engage in 150-300 min of moderate-intensity PA per week or 75-150 min of vigorous PA per week along with recommendations to engage in muscle strengthening activities such as resistance training at moderate or greater intensities for all major muscle groups for at least two or more, non-consecutive days per week. Before prescribing exercise, health care professionals should risk-stratify their patients based on the ACSM preparticipation screening guidelines (Riebe et al., 2015). Generally, medical clearance is recommended for those with a history of CVD, metabolic or renal disease, or who exhibit signs and symptoms of these conditions. Following risk stratification, health care professionals can provide an exercise prescription or alternatively or provide a PA referral to a qualified exercise professional.
Summary and conclusions
The increased prevalence of weight loss attempts in the United States has coincided with the increased prevalence of obesity. Thus, a weight-centric approach to obesity treatment and prevention has been largely ineffective. It is unlikely that continued focus on weight loss as the primary metric for success will reverse the trends in obesity prevalence or result in sustainable weight loss. In fact, chronic weight cycling is the norm for millions of adults and is likely to remain so for as long as weight loss persists as the cornerstone of obesity treatment. Weight cycling is associated with health risks that are very similar to those associated with obesity, including higher all-cause mortality risk, and may contribute to weight gain.
A weight-neutral approach to treating obesity-related health conditions may be as, or more, effective than a weight-loss-centered approach, and could avoid pitfalls associated with repeated weight loss failure (Bacon and Aphramor, 2011, Brown and Kuk, 2015; Gaesser et al., 2011, 2015, Ross et al., 2015). Table 1 summarizes the major points in support of a weight-neutral strategy for obesity treatment, which focuses on increasing PA and improving CRF. Such an approach does not assume that obesity is entirely benign, or that there are not circumstances that may necessitate weight loss (Guo and Garvey, 2017; Guo et al., 2014; Jensen et al., 2014; Kuk et al., 2011; Kushner, 2018; Kushner and Ryan, 2014; Sharma and Kushner, 2009). However, many obesity-related health conditions are more likely attributable to low PA and CRF rather than obesity per se. Epidemiological studies show that CRF and PA significantly attenuate, and sometimes eliminate, the increased mortality risk associated with obesity. More importantly, increasing PA or CRF is consistently associated with greater reduction in risk of all-cause and CVD mortality than intentional weight loss. In addition, improvements in major cardiometabolic risk markers with exercise training are comparable to those associated with weight loss typically achieved by caloric restriction.
Table 1.
Rationale for a weight-neutral strategy for obesity treatment: shifting the focus from weight loss to increasing physical activity and improving cardiorespiratory fitness
|
|
|
|
|
|
|
|
|
|
We acknowledge that focusing on PA and CRF without establishing a specific weight-loss target is a challenging proposition when nearly three-fourths of women and more than half of men desire to weigh less (Yaemsiri et al., 2011). However, desire is often incompatible with physiology, and this is clearly evident with weight loss. The amount of weight individuals with obesity frequently indicate that they would like to lose (Dalle Grave et al., 2005; Foster et al., 1997) is greater than what is recommended (Garvey et al., 2016; Jensen et al., 2014; Kushner, 2018; Kushner and Ryan, 2014), and considerably greater than the typically observed values with weight loss interventions (Franz et al., 2015; Mudaliar et al., 2016; Zomer et al., 2016). Alternatively, these individuals may be more willing to adopt a weight-neutral PA program if health care professionals promoted this perspective more vigorously and regularly emphasized the health benefits of increasing PA and reducing sedentary behaviors in the absence of weight loss (Bacon and Aphramor, 2011).
Increasing PA and CRF should be a high priority throughout the health care system. In addition to the obvious health benefits, increasing CRF may also substantially reduce health care costs. In the Veterans Exercise Testing Study, annual health care costs for moderately-to-highly-fit men with obesity were ∼$10,000-$27,000 lower than the health care costs for least fit men in the normal BMI category (de Souza de Silva et al., 2019). This suggests that the higher health care costs of obesity may be largely because of low CRF rather than a high BMI.
A weight-neutral approach does not mean that weight loss should be categorically discouraged. Such an approach may not be feasible when so many adults want to lose weight. But shifting the focus away from weight loss as the primary goal, and instead focusing on increasing PA to improve CRF, may be prudent for treating obesity-related health conditions. Weight loss may result from increased PA, but not always (Caudwell et al., 2013; Donnelly and Smith, 2005; King et al., 2009; Lamarche et al., 1992; Sawyer et al., 2015). Even energy restriction approaches do not always lead to predictable weight loss (Dansinger et al., 2005; Gardner et al., 2018). The individual variability in weight change in response to PA and energy restriction interventions is tremendous, with many failing to lose the expected amount of weight based on the energy expenditure of accumulated exercise sessions (Caudwell et al., 2013; Donnelly and Smith, 2005; King et al., 2009; Lamarche et al., 1992; Sawyer et al., 2015) or the energy deficit of the hypocaloric diet (Dansinger et al., 2005; Gardner et al., 2018). This reality has undoubtedly led to countless instances of frustration and discontinuation of lifestyle interventions (Ross et al., 2015). Emphasizing the intrinsic value of PA and CRF—as primary outcomes—may avoid repeating “failures” associated with a weight-centric approach.
Pragmatically, it may be more prudent to focus on PA rather than weight loss. In the Diabetes Prevention Program (DPP) (Knowler et al., 2002) and the Finnish Diabetes Prevention Study (FDPS) (Tuomilehto et al., 2001), up to twice as many participants were able to achieve the PA recommendation (150 min/week in the DPP; 120 min/week in the FDPS) than they were able to achieve the weight loss goal (>7% of initial body weight in the DPP; >5% initial body weight in the FDPS). For purposes of survival, the results of HUNT (Nord-Trøndelag Health Study) are instructive. During a 15.7-year follow-up of adults with coronary heart disease, compared to those who remained sedentary, sustained low PA was associated with 19% lower all-cause mortality risk and sustained high PA was associated with a 36% lower all-cause mortality risk (Moholdt et al., 2018). Weight loss, by contrast, was associated with a 30% increased mortality risk, whereas weight gain was not associated with mortality risk. These results support recommendations to increase or maintain PA and not focus exclusively on weight loss.
Shifting the primary focus from weight loss to fitness via increased PA will undoubtedly be challenging. Whether a weight-neutral paradigm can be fully embraced, and whether increased PA and CRF can be maintained throughout a lifetime, remains to be seen.
Acknowledgments
No funding was provided for this project. The authors thank our colleagues, Dharini Bhammar, Catherine Jarrett, Brandon Sawyer, and Wesley Tucker, for their contributions to previous research projects that helped inform our current work for this review article.
Author contributions
GAG and SSA reviewed the literature and participated in the drafting and writing of the manuscript. Both authors read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Declaration of interests
The authors declare no competing interests.
References
- Adil M.T., Jain V., Rashid F., Al-Taan O., Al-Rashedy M., Jambulingam P., Whitelaw D. Meta-analysis of the effect of bariatric surgery on physical activity. Surg. Obes. Relat. Dis. 2019;15:1620–1631. doi: 10.1016/j.soard.2019.06.014. [DOI] [PubMed] [Google Scholar]
- Aggio D., Papachristou E., Papacosta O., Lennon L.T., Ash S., Whincup P., Wannamethee S.G., Jefferis B.J. Trajectories of physical activity from Midlife to old age and associations with subsequent cardiovascular disease and all-cause mortality. J. Epidemiol. Community Health. 2020;74:130–136. doi: 10.1136/jech-2019-212706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson J.W., Konz E.C., Frederich R.C., Wood C.L. Long-term weight-loss maintenance: a meta-analysis of US studies. Am. J. Clin. Nutr. 2001;74:579–584. doi: 10.1093/ajcn/74.5.579. [DOI] [PubMed] [Google Scholar]
- Arcaro G., Zamboni M., Rossi L., Turcato E., Covi G., Armellini F., Bosello O., Lechi A. Body fat distribution predicts the degree of endothelial dysfunction in uncomplicated obesity. Int. J. Obes. Relat. Metab. Disord. 1999;23:936–942. doi: 10.1038/sj.ijo.0801022. [DOI] [PubMed] [Google Scholar]
- Arterburn D.E., Bogart A., Sherwood N.E., Sidney S., Coleman K.J., Haneuse S., O'connor P.J., Theis M.K., Campos G.M., McCulloch D., Selby J. A multisite study of long-term remission and relapse of type 2 diabetes mellitus following gastric bypass. Obes. Surg. 2013;23:93–102. doi: 10.1007/s11695-012-0802-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashton R.E., Tew G.A., Aning J.J., Gilbert S.E., Lewis L., Saxton J.M. Effects of short-term, medium-term and long-term resistance exercise training on cardiometabolic health outcomes in adults: systematic review with meta-analysis. Br. J. Sports Med. 2020;54:341–348. doi: 10.1136/bjsports-2017-098970. [DOI] [PubMed] [Google Scholar]
- Atkinson R.L., Dietz W.H., Foreyt J.P., Goodwin N.J., Hill J.O., Hirsch J., Pi-Sunyer F.X., Weinsier R.L., Wing R., Hoofnagle J.H. Weight cycling. National Task Force on the prevention and treatment of obesity. JAMA. 1994;272:1196–1202. [PubMed] [Google Scholar]
- Aune D., Sen A., Prasad M., Norat T., Janszky I., Tonstad S., Romundstad P., Vatten L.J. BMI and all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. BMJ. 2016;353:i2156. doi: 10.1136/bmj.i2156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bacon L., Aphramor L. Weight science: evaluating the evidence for a paradigm shift. Nutr. J. 2011;10:9. doi: 10.1186/1475-2891-10-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bangalore S., Fayyad R., Demicco D.A., Colhoun H.M., Waters D.D. Body weight variability and cardiovascular outcomes in patients with type 2 diabetes mellitus. Circ. Cardiovasc. Qual. Outcomes. 2018;11:e004724. doi: 10.1161/CIRCOUTCOMES.118.004724. [DOI] [PubMed] [Google Scholar]
- Bangalore S., Fayyad R., Laskey R., Demicco D.A., Messerli F.H., Waters D.D. Body-weight Fluctuations and outcomes in coronary disease. N. Engl. J. Med. 2017;376:1332–1340. doi: 10.1056/NEJMoa1606148. [DOI] [PubMed] [Google Scholar]
- Barry V.W., Baruth M., Beets M.W., Durstine J.L., Liu J., Blair S.N. Fitness vs. fatness on all-cause mortality: a meta-analysis. Prog. Cardiovasc. Dis. 2014;56:382–390. doi: 10.1016/j.pcad.2013.09.002. [DOI] [PubMed] [Google Scholar]
- Barry V.W., Caputo J.L., Kang M. The joint association of fitness and fatness on cardiovascular disease mortality: a meta-analysis. Prog. Cardiovasc. Dis. 2018;61:136–141. doi: 10.1016/j.pcad.2018.07.004. [DOI] [PubMed] [Google Scholar]
- Bellicha A., Ciangura C., Roda C., Torcivia A., Portero P., Oppert J.M. Changes in cardiorespiratory fitness after gastric bypass: relations with accelerometry-assessed physical activity. Obes. Surg. 2019;29:2936–2941. doi: 10.1007/s11695-019-03932-2. [DOI] [PubMed] [Google Scholar]
- Bellocco R., Jia C., Ye W., Lagerros Y.T. Effects of physical activity, body mass index, waist-to-hip ratio and waist circumference on total mortality risk in the Swedish National March Cohort. Eur. J. Epidemiol. 2010;25:777–788. doi: 10.1007/s10654-010-9497-6. [DOI] [PubMed] [Google Scholar]
- Benatti F., Solis M., Artioli G., Montag E., Painelli V., Saito F., Baptista L., Costa L.A., Neves R., Seelaender M. Liposuction induces a compensatory increase of visceral fat which is effectively counteracted by physical activity: a randomized trial. J. Clin. Endocrinol. Metab. 2012;97:2388–2395. doi: 10.1210/jc.2012-1012. [DOI] [PubMed] [Google Scholar]
- Blair S.N., Kohl H.W., 3rd, Barlow C.E., Paffenbarger R.S., Jr., Gibbons L.W., Macera C.A. Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. JAMA. 1995;273:1093–1098. [PubMed] [Google Scholar]
- Booth F.W., Roberts C.K., Laye M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012;2:1143–1211. doi: 10.1002/cphy.c110025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boriani F., Villani R., Morselli P.G. Metabolic effects of large-volume liposuction for obese healthy women: a meta-analysis of fasting insulin levels. Aesthet. Plast Surg. 2014;38:1050–1056. doi: 10.1007/s00266-014-0386-3. [DOI] [PubMed] [Google Scholar]
- Bosy-Westphal A., Schautz B., Lagerpusch M., Pourhassan M., Braun W., Goele K., Heller M., Gluer C.C., Muller M.J. Effect of weight loss and regain on adipose tissue distribution, composition of lean mass and resting energy expenditure in young overweight and obese adults. Int. J. Obes. (Lond) 2013;37:1371–1377. doi: 10.1038/ijo.2013.1. [DOI] [PubMed] [Google Scholar]
- Boule N.G., Haddad E., Kenny G.P., Wells G.A., Sigal R.J. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials. JAMA. 2001;286:1218–1227. doi: 10.1001/jama.286.10.1218. [DOI] [PubMed] [Google Scholar]
- Brown R.E., Kuk J.L. Consequences of obesity and weight loss: a devil's advocate position. Obes. Rev. 2015;16:77–87. doi: 10.1111/obr.12232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carbone S., Kirkman D.L., Garten R.S., Rodriguez-Miguelez P., Artero E.G., Lee D.C., Lavie C.J. Muscular strength and cardiovascular disease: AN UPDATED STATE-OF-THE-ART NARRATIVE REVIEW. J. Cardiopulm Rehabil. Prev. 2020;40:302–309. doi: 10.1097/HCR.0000000000000525. [DOI] [PubMed] [Google Scholar]
- Cardoso L., Rodrigues D., Gomes L., Carrilho F. Short- and long-term mortality after bariatric surgery: a systematic review and meta-analysis. Diabetes Obes. Metab. 2017;19:1223–1232. doi: 10.1111/dom.12922. [DOI] [PubMed] [Google Scholar]
- Caudwell P., Gibbons C., Hopkins M., King N., Finlayson G., Blundell J. No sex difference in body fat in response to supervised and measured exercise. Med. Sci. Sports Exerc. 2013;45:351–358. doi: 10.1249/MSS.0b013e31826ced79. [DOI] [PubMed] [Google Scholar]
- Chen Y., Yang X., Wang J., Li Y., Ying D., Yuan H. Weight loss increases all-cause mortality in overweight or obese patients with diabetes: a meta-analysis. Medicine (Baltimore) 2018;97:e12075. doi: 10.1097/MD.0000000000012075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng F.W., Gao X., Jensen G.L. Weight change and all-cause mortality in older adults: a meta-analysis. J. Nutr. Gerontol. Geriatr. 2015;34:343–368. doi: 10.1080/21551197.2015.1090362. [DOI] [PubMed] [Google Scholar]
- Cologne J., Takahashi I., French B., Nanri A., Misumi M., Sadakane A., Cullings H.M., Araki Y., Mizoue T. Association of weight fluctuation with mortality in Japanese adults. JAMA Netw. Open. 2019;2:e190731. doi: 10.1001/jamanetworkopen.2019.0731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornelissen V.A., Fagard R.H. Effect of resistance training on resting blood pressure: a meta-analysis of randomized controlled trials. J. Hypertens. 2005;23:251–259. doi: 10.1097/00004872-200502000-00003. [DOI] [PubMed] [Google Scholar]
- Cornelissen V.A., Fagard R.H. Effects of endurance training on blood pressure, blood pressure-regulating mechanisms, and cardiovascular risk factors. Hypertension. 2005;46:667–675. doi: 10.1161/01.HYP.0000184225.05629.51. [DOI] [PubMed] [Google Scholar]
- Cornelissen V.A., Fagard R.H., Coeckelberghs E., Vanhees L. Impact of resistance training on blood pressure and other cardiovascular risk factors: a meta-analysis of randomized, controlled trials. Hypertension. 2011;58:950–958. doi: 10.1161/HYPERTENSIONAHA.111.177071. [DOI] [PubMed] [Google Scholar]
- Cornelissen V.A., Smart N.A. Exercise training for blood pressure: a systematic review and meta-analysis. J. Am. Heart Assoc. 2013;2:e004473. doi: 10.1161/JAHA.112.004473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cowan R.E. Exercise is medicine initiative: physical activity as a vital sign and prescription in adult rehabilitation practice. Arch. Phys. Med. Rehabil. 2016;97:S232–S237. doi: 10.1016/j.apmr.2016.01.040. [DOI] [PubMed] [Google Scholar]
- Crespo C.J., Palmieri M.R., Perdomo R.P., Mcgee D.L., Smit E., Sempos C.T., Lee I.M., Sorlie P.D. The relationship of physical activity and body weight with all-cause mortality: results from the Puerto Rico Heart Health Program. Ann. Epidemiol. 2002;12:543–552. doi: 10.1016/s1047-2797(01)00296-4. [DOI] [PubMed] [Google Scholar]
- Dalle Grave R., Calugi S., Molinari E., Petroni M.L., Bondi M., Compare A., Marchesini G. Weight loss expectations in obese patients and treatment attrition: an observational multicenter study. Obes. Res. 2005;13:1961–1969. doi: 10.1038/oby.2005.241. [DOI] [PubMed] [Google Scholar]
- Danilla S., Longton C., Valenzuela K., Cavada G., Norambuena H., Tabilo C., Erazo C., Benitez S., Sepulveda S., Schulz R., Andrades P. Suction-assisted lipectomy fails to improve cardiovascular metabolic markers of disease: a meta-analysis. J. Plast. Reconstr. Aesthet. Surg. 2013;66:1557–1563. doi: 10.1016/j.bjps.2013.07.001. [DOI] [PubMed] [Google Scholar]
- Dansinger M.L., Gleason J.A., Griffith J.L., Selker H.P., Schaefer E.J. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: a randomized trial. JAMA. 2005;293:43–53. doi: 10.1001/jama.293.1.43. [DOI] [PubMed] [Google Scholar]
- Dansinger M.L., Tatsioni A., Wong J.B., Chung M., Balk E.M. Meta-analysis: the effect of dietary counseling for weight loss. Ann. Intern. Med. 2007;147:41–50. doi: 10.7326/0003-4819-147-1-200707030-00007. [DOI] [PubMed] [Google Scholar]
- Dattilo A.M., Kris-Etherton P.M. Effects of weight reduction on blood lipids and lipoproteins: a meta-analysis. Am. J. Clin. Nutr. 1992;56:320–328. doi: 10.1093/ajcn/56.2.320. [DOI] [PubMed] [Google Scholar]
- de Souza de Silva C.G., Kokkinos P., Doom R., Loganathan D., Fonda H., Chan K., De Araujo C.G.S., Myers J. Association between cardiorespiratory fitness, obesity, and health care costs: the Veterans Exercise Testing Study. Int. J. Obes. (Lond) 2019;43:2225–2232. doi: 10.1038/s41366-018-0257-0. [DOI] [PubMed] [Google Scholar]
- Despres J.P. Body fat distribution and risk of cardiovascular disease: an update. Circulation. 2012;126:1301–1313. doi: 10.1161/CIRCULATIONAHA.111.067264. [DOI] [PubMed] [Google Scholar]
- Despres J.P. Obesity and cardiovascular disease: weight loss is not the only target. Can J. Cardiol. 2015;31:216–222. doi: 10.1016/j.cjca.2014.12.009. [DOI] [PubMed] [Google Scholar]
- Dewal R.S., Stanford K.I. Effects of exercise on brown and beige adipocytes. Biochim. Biophys. Acta Mol. Cell Biol Lipids. 2019;1864:71–78. doi: 10.1016/j.bbalip.2018.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dollet L., Zierath J.R. Interplay between diet, exercise and the molecular circadian clock in orchestrating metabolic adaptations of adipose tissue. J. Physiol. 2019;597:1439–1450. doi: 10.1113/JP276488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donnelly J.E., Blair S.N., Jakicic J.M., Manore M.M., Rankin J.W., Smith B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009;41:459–471. doi: 10.1249/MSS.0b013e3181949333. [DOI] [PubMed] [Google Scholar]
- Donnelly J.E., Smith B.K. Is exercise effective for weight loss with ad libitum diet? Energy balance, compensation, and gender differences. Exerc. Sport Sci. Rev. 2005;33:169–174. doi: 10.1097/00003677-200510000-00004. [DOI] [PubMed] [Google Scholar]
- Duncan G.E. The "fit but fat" concept revisited: population-based estimates using NHANES. Int. J. Behav. Nutr. Phys. Act. 2010;7:47. doi: 10.1186/1479-5868-7-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Early K.S., Stewart A., Johannsen N., Lavie C.J., Thomas J.R., Welsch M. The effects of exercise training on brachial artery flow-mediated dilation: a meta-analysis. J. Cardiopulm Rehabil. Prev. 2017;37:77–89. doi: 10.1097/HCR.0000000000000206. [DOI] [PubMed] [Google Scholar]
- Eckel N., Meidtner K., Kalle-Uhlmann T., Stefan N., Schulze M.B. Metabolically healthy obesity and cardiovascular events: a systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2016;23:956–966. doi: 10.1177/2047487315623884. [DOI] [PubMed] [Google Scholar]
- Ehrman J.K., Brawner C.A., Al-Mallah M.H., Qureshi W.T., Blaha M.J., Keteyian S.J. Cardiorespiratory fitness change and mortality risk among black and white patients: Henry Ford exercise testing (FIT) project. Am. J. Med. 2017;130:1177–1183. doi: 10.1016/j.amjmed.2017.02.036. [DOI] [PubMed] [Google Scholar]
- Erikssen G. Physical fitness and changes in mortality: the survival of the fittest. Sports Med. 2001;31:571–576. doi: 10.2165/00007256-200131080-00001. [DOI] [PubMed] [Google Scholar]
- Erikssen G., Liestol K., Bjornholt J., Thaulow E., Sandvik L., Erikssen J. Changes in physical fitness and changes in mortality. Lancet. 1998;352:759–762. doi: 10.1016/S0140-6736(98)02268-5. [DOI] [PubMed] [Google Scholar]
- Eriksson-Hogling D., Andersson D.P., Backdahl J., Hoffstedt J., Rossner S., Thorell A., Arner E., Arner P., Ryden M. Adipose tissue morphology predicts improved insulin sensitivity following moderate or pronounced weight loss. Int. J. Obes. (Lond) 2015;39:893–898. doi: 10.1038/ijo.2015.18. [DOI] [PubMed] [Google Scholar]
- Fabbrini E., Magkos F., Mohammed B.S., Pietka T., Abumrad N.A., Patterson B.W., Okunade A., Klein S. Intrahepatic fat, not visceral fat, is linked with metabolic complications of obesity. Proc. Natl. Acad. Sci. U S A. 2009;106:15430–15435. doi: 10.1073/pnas.0904944106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fagard R.H. Exercise characteristics and the blood pressure response to dynamic physical training. Med. Sci. Sports Exerc. 2001;33:S484–S492. doi: 10.1097/00005768-200106001-00018. discussion S493-494. [DOI] [PubMed] [Google Scholar]
- Field A.E., Manson J.E., Taylor C.B., Willett W.C., Colditz G.A. Association of weight change, weight control practices, and weight cycling among women in the Nurses' Health Study II. Int. J. Obes. Relat. Metab. Disord. 2004;28:1134–1142. doi: 10.1038/sj.ijo.0802728. [DOI] [PubMed] [Google Scholar]
- Fildes A., Charlton J., Rudisill C., Littlejohns P., Prevost A.T., Gulliford M.C. Probability of an obese person attaining normal body weight: cohort study using electronic health records. Am. J. Public Health. 2015;105 doi: 10.2105/AJPH.2015.302773. e54–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiuza-Luces C., Garatachea N., Berger N.A., Lucia A. Exercise is the real polypill. Physiology (Bethesda) 2013;28:330–358. doi: 10.1152/physiol.00019.2013. [DOI] [PubMed] [Google Scholar]
- Flegal K.M., Graubard B.I., Williamson D.F., Gail M.H. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293:1861–1867. doi: 10.1001/jama.293.15.1861. [DOI] [PubMed] [Google Scholar]
- Flegal K.M., Kit B.K., Orpana H., Graubard B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013;309:71–82. doi: 10.1001/jama.2012.113905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flegal K.M., Graubard B.I., Yi S.W. Comparative effects of the restriction method in two large observational studies of body mass index and mortality among adults. Eur. J. Clin. Invest. 2017;47:415–421. doi: 10.1111/eci.12756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fogelholm M. Physical activity, fitness and fatness: relations to mortality, morbidity and disease risk factors. A systematic review. Obes. Rev. 2010;11:202–221. doi: 10.1111/j.1467-789X.2009.00653.x. [DOI] [PubMed] [Google Scholar]
- Foright R.M., Presby D.M., Sherk V.D., Kahn D., Checkley L.A., Giles E.D., Bergouignan A., Higgins J.A., Jackman M.R., Hill J.O., Maclean P.S. Is regular exercise an effective strategy for weight loss maintenance? Physiol. Behav. 2018;188:86–93. doi: 10.1016/j.physbeh.2018.01.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster G.D., Wadden T.A., Vogt R.A., Brewer G. What is a reasonable weight loss? Patients' expectations and evaluations of obesity treatment outcomes. J. Consult Clin. Psychol. 1997;65:79–85. doi: 10.1037//0022-006x.65.1.79. [DOI] [PubMed] [Google Scholar]
- Franz M.J., Boucher J.L., Rutten-Ramos S., Vanwormer J.J. Lifestyle weight-loss intervention outcomes in overweight and obese adults with type 2 diabetes: a systematic review and meta-analysis of randomized clinical trials. J. Acad. Nutr. Diet. 2015;115:1447–1463. doi: 10.1016/j.jand.2015.02.031. [DOI] [PubMed] [Google Scholar]
- Gaesser G.A., Angadi S.S., Sawyer B.J. Exercise and diet, independent of weight loss, improve cardiometabolic risk profile in overweight and obese individuals. Phys. Sportsmed. 2011;39:87–97. doi: 10.3810/psm.2011.05.1898. [DOI] [PubMed] [Google Scholar]
- Gaesser G.A., Blair S.N. The health risks of obesity have been exaggerated. Med. Sci. Sports Exerc. 2019;51:218–221. doi: 10.1249/MSS.0000000000001746. [DOI] [PubMed] [Google Scholar]
- Gaesser G.A., Tucker W.J., Jarrett C.L., Angadi S.S. Fitness versus fatness: which influences health and mortality risk the most? Curr. Sports Med. Rep. 2015;14:327–332. doi: 10.1249/JSR.0000000000000170. [DOI] [PubMed] [Google Scholar]
- Garcia-Hermoso A., Cavero-Redondo I., Ramirez-Velez R., Ruiz J.R., Ortega F.B., Lee D.C., Martinez-Vizcaino V. Muscular strength as a predictor of all-cause mortality in an apparently healthy population: a systematic review and meta-analysis of data from approximately 2 million men and women. Arch. Phys. Med. Rehabil. 2018;99:2100–2113.e5. doi: 10.1016/j.apmr.2018.01.008. [DOI] [PubMed] [Google Scholar]
- Gardner C.D., Trepanowski J.F., Del Gobbo L.C., Hauser M.E., Rigdon J., Ioannidis J.P.A., Desai M., King A.C. Effect of low-fat vs low-carbohydrate diet on 12-month weight loss in overweight Adults and the association with genotype pattern or insulin secretion: the DIETFITS randomized clinical trial. JAMA. 2018;319:667–679. doi: 10.1001/jama.2018.0245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garvey W.T., Mechanick J.I., Brett E.M., Garber A.J., Hurley D.L., Jastreboff A.M., Nadolsky K., Pessah-Pollack R., Plodkowski R. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr. Pract. 2016;22:842–884. doi: 10.4158/EP161365.GL. [DOI] [PubMed] [Google Scholar]
- GBD 2015 Obesity Collaborators, Afshin A., Forouzanfar M.H., Reitsma M.B., Sur P., Estep K., Lee A., Marczak L., Mokdad A.H., Moradi-Lakeh M. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017;377:13–27. doi: 10.1056/NEJMoa1614362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Global BMI Mortality Collaboration, Di Angelantonio E., Bhupathiraju Sh N., Wormser D., Gao P., Kaptoge S., Berrington De Gonzalez A., Cairns B.J., Huxley R., Jackson Ch L. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388:776–786. doi: 10.1016/S0140-6736(16)30175-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goisser S., Kemmler W., Porzel S., Volkert D., Sieber C.C., Bollheimer L.C., Freiberger E. Sarcopenic obesity and complex interventions with nutrition and exercise in community-dwelling older persons--a narrative review. Clin. Interv. Aging. 2015;10:1267–1282. doi: 10.2147/CIA.S82454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gregg E.W., Cauley J.A., Stone K., Thompson T.J., Bauer D.C., Cummings S.R., Ensrud K.E. Relationship of changes in physical activity and mortality among older women. JAMA. 2003;289:2379–2386. doi: 10.1001/jama.289.18.2379. [DOI] [PubMed] [Google Scholar]
- Guo F., Garvey W.T. Cardiometabolic disease staging predicts effectiveness of weight-loss therapy to prevent type 2 diabetes: pooled results from phase III clinical trials assessing phentermine/topiramate extended release. Diabetes Care. 2017;40:856–862. doi: 10.2337/dc17-0088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo F., Moellering D.R., Garvey W.T. The progression of cardiometabolic disease: validation of a new cardiometabolic disease staging system applicable to obesity. Obesity (Silver Spring) 2014;22:110–118. doi: 10.1002/oby.20585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halbert J.A., Silagy C.A., Finucane P., Withers R.T., Hamdorf P.A. Exercise training and blood lipids in hyperlipidemic and normolipidemic adults: a meta-analysis of randomized, controlled trials. Eur. J. Clin. Nutr. 1999;53:514–522. doi: 10.1038/sj.ejcn.1600784. [DOI] [PubMed] [Google Scholar]
- Hales C.M., Carroll M.D., Fryar C.D., Ogden C.L. Prevalence of obesity and severe obesity among adults: United States, 2017-2018. NCHS Data Brief. 2020:1–8. [PubMed] [Google Scholar]
- Han L., You D., Zeng F., Feng X., Astell-Burt T., Duan S., Qi L. Trends in self-perceived weight status, weight loss attempts, and weight loss strategies among adults in the United States, 1999-2016. JAMA Netw. Open. 2019;2:e1915219. doi: 10.1001/jamanetworkopen.2019.15219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrington M., Gibson S., Cottrell R.C. A review and meta-analysis of the effect of weight loss on all-cause mortality risk. Nutr. Res. Rev. 2009;22:93–108. doi: 10.1017/S0954422409990035. [DOI] [PubMed] [Google Scholar]
- Hasan B., Nayfeh T., Alzuabi M., Wang Z., Kuchkuntla A.R., Prokop L.J., Newman C.B., Murad M.H., Rajjo T.I. Weight loss and serum lipids in overweight and obese adults: a systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2020;105:dgaa673. doi: 10.1210/clinem/dgaa673. [DOI] [PubMed] [Google Scholar]
- Hens W., Taeyman J., Cornelis J., Gielen J., Van Gaal L., Vissers D. The effect of lifestyle interventions on excess ectopic fat deposition measured by noninvasive techniques in overweight and obese adults: a systematic review and meta-analysis. J. Phys. Act Health. 2016;13:671–694. doi: 10.1123/jpah.2015-0560. [DOI] [PubMed] [Google Scholar]
- Hernandez T.L., Kittelson J.M., Law C.K., Ketch L.L., Stob N.R., Lindstrom R.C., Scherzinger A., Stamm E.R., Eckel R.H. Fat redistribution following suction lipectomy: defense of body fat and patterns of restoration. Obesity (Silver Spring) 2011;19:1388–1395. doi: 10.1038/oby.2011.64. [DOI] [PubMed] [Google Scholar]
- Herring L.Y., Stevinson C., Davies M.J., Biddle S.J., Sutton C., Bowrey D., Carter P. Changes in physical activity behaviour and physical function after bariatric surgery: a systematic review and meta-analysis. Obes. Rev. 2016;17:250–261. doi: 10.1111/obr.12361. [DOI] [PubMed] [Google Scholar]
- Houston D.K., Miller M.E., Kitzman D.W., Rejeski W.J., Messier S.P., Lyles M.F., Kritchevsky S.B., Nicklas B.J. Long-term effects of Randomization to a weight loss intervention in older adults: a Pilot study. J. Nutr. Gerontol. Geriatr. 2019;38:83–99. doi: 10.1080/21551197.2019.1572570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hruby A., Hu F.B. The epidemiology of obesity: a big picture. Pharmacoeconomics. 2015;33:673–689. doi: 10.1007/s40273-014-0243-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsueh Y.W., Yeh T.L., Lin C.Y., Tsai S.Y., Liu S.J., Lin C.M., Chen H.H. Association of metabolically healthy obesity and elevated risk of coronary artery calcification: a systematic review and meta-analysis. PeerJ. 2020;8:e8815. doi: 10.7717/peerj.8815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu G., Tuomilehto J., Silventoinen K., Barengo N.C., Peltonen M., Jousilahti P. The effects of physical activity and body mass index on cardiovascular, cancer and all-cause mortality among 47 212 middle-aged Finnish men and women. Int. J. Obes. (Lond) 2005;29:894–902. doi: 10.1038/sj.ijo.0802870. [DOI] [PubMed] [Google Scholar]
- Huang M.Y., Wang M.Y., Lin Y.S., Lin C.J., Lo K., Chang I.J., Cheng T.Y., Tsai S.Y., Chen H.H., Lin C.Y. The association between metabolically healthy obesity, cardiovascular disease, and all-cause mortality risk in Asia: a systematic review and meta-analysis. Int. J. Environ. Res. Public Health. 2020;17:1320. doi: 10.3390/ijerph17041320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Igarashi Y., Nogami Y. Response of lipids and lipoproteins to regular aquatic endurance exercise: a meta-analysis of randomized controlled trials. J. Atheroscler. Thromb. 2019;26:14–30. doi: 10.5551/jat.42937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Imboden M.T., Kaminsky L.A., Peterman J.E., Hutzler H.L., Whaley M.H., Fleenor B.S., Harber M.P. Cardiorespiratory fitness normalized to fat-free mass and mortality risk. Med. Sci. Sports Exerc. 2020;52:1532–1537. doi: 10.1249/MSS.0000000000002289. [DOI] [PubMed] [Google Scholar]
- Imboden M.T., Harber M.P., Whaley M.H., Finch W.H., Bishop D.A., Fleenor B.S., Kaminsky L.A. The influence of change in cardiorespiratory fitness with short-term exercise training on mortality risk from the ball state adult fitness longitudinal lifestyle study. Mayo Clin. Proc. 2019;94:1406–1414. doi: 10.1016/j.mayocp.2019.01.049. [DOI] [PubMed] [Google Scholar]
- Imboden M.T., Harber M.P., Whaley M.H., Finch W.H., Bishop D.L., Fleenor B.S., Kaminsky L.A. The association between the change in directly measured cardiorespiratory fitness across time and mortality risk. Prog. Cardiovasc. Dis. 2019;62:157–162. doi: 10.1016/j.pcad.2018.12.003. [DOI] [PubMed] [Google Scholar]
- Ismail I., Keating S.E., Baker M.K., Johnson N.A. A systematic review and meta-analysis of the effect of aerobic vs. resistance exercise training on visceral fat. Obes. Rev. 2012;13:68–91. doi: 10.1111/j.1467-789X.2011.00931.x. [DOI] [PubMed] [Google Scholar]
- Jelleyman C., Yates T., O'Donovan G., Gray L.J., King J.A., Khunti K., Davies M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: a meta-analysis. Obes. Rev. 2015;16:942–961. doi: 10.1111/obr.12317. [DOI] [PubMed] [Google Scholar]
- Jensen M.D., Ryan D.H., Apovian C.M., Ard J.D., Comuzzie A.G., Donato K.A., Hu F.B., Hubbard V.S., Jakicic J.M., Kushner R.F. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the obesity society. Circulation. 2014;129:S102–S138. doi: 10.1161/01.cir.0000437739.71477.ee. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jiang M., Zou Y., Xin Q., Cai Y., Wang Y., Qin X., Ma D. Dose-response relationship between body mass index and risks of all-cause mortality and disability among the elderly: a systematic review and meta-analysis. Clin. Nutr. 2019;38:1511–1523. doi: 10.1016/j.clnu.2018.07.021. [DOI] [PubMed] [Google Scholar]
- Joris P.J., Zeegers M.P., Mensink R.P. Weight loss improves fasting flow-mediated vasodilation in adults: a meta-analysis of intervention studies. Atherosclerosis. 2015;239:21–30. doi: 10.1016/j.atherosclerosis.2014.12.056. [DOI] [PubMed] [Google Scholar]
- Keating S.E., George J., Johnson N.A. The benefits of exercise for patients with non-alcoholic fatty liver disease. Expert Rev. Gastroenterol. Hepatol. 2015;9:1247–1250. doi: 10.1586/17474124.2015.1075392. [DOI] [PubMed] [Google Scholar]
- Keating S.E., Hackett D.A., George J., Johnson N.A. Exercise and non-alcoholic fatty liver disease: a systematic review and meta-analysis. J. Hepatol. 2012;57:157–166. doi: 10.1016/j.jhep.2012.02.023. [DOI] [PubMed] [Google Scholar]
- Keating S.E., Hackett D.A., Parker H.M., O'Connor H.T., Gerofi J.A., Sainsbury A., Baker M.K., Chuter V.H., Caterson I.D., George J., Johnson N.A. Effect of aerobic exercise training dose on liver fat and visceral adiposity. J. Hepatol. 2015;63:174–182. doi: 10.1016/j.jhep.2015.02.022. [DOI] [PubMed] [Google Scholar]
- Khera R., Pandey A., Chandar A.K., Murad M.H., Prokop L.J., Neeland I.J., Berry J.D., Camilleri M., Singh S. Effects of weight-loss medications on cardiometabolic risk profiles: a systematic review and network meta-analysis. Gastroenterology. 2018;154:1309–1319.e7. doi: 10.1053/j.gastro.2017.12.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kieffer S.K., Croci I., Wisloff U., Nauman J. Temporal changes in a novel metric of physical activity tracking (personal activity intelligence) and mortality: the HUNT study, Norway. Prog. Cardiovasc. Dis. 2019;62:186–192. doi: 10.1016/j.pcad.2018.09.002. [DOI] [PubMed] [Google Scholar]
- Kim Y., Wijndaele K., Lee D.C., Sharp S.J., Wareham N., Brage S. Independent and joint associations of grip strength and adiposity with all-cause and cardiovascular disease mortality in 403,199 adults: the UK Biobank study. Am. J. Clin. Nutr. 2017;106:773–782. doi: 10.3945/ajcn.117.156851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King N.A., Hopkins M., Caudwell P., Stubbs R.J., Blundell J.E. Beneficial effects of exercise: shifting the focus from body weight to other markers of health. Br. J. Sports Med. 2009;43:924–927. doi: 10.1136/bjsm.2009.065557. [DOI] [PubMed] [Google Scholar]
- Knowler W.C., Barrett-Connor E., Fowler S.E., Hamman R.F., Lachin J.M., Walker E.A., Nathan D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002;346:393–403. doi: 10.1056/NEJMoa012512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kodama S., Saito K., Tanaka S., Maki M., Yachi Y., Asumi M., Sugawara A., Totsuka K., Shimano H., Ohashi Y. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301:2024–2035. doi: 10.1001/jama.2009.681. [DOI] [PubMed] [Google Scholar]
- Kodama S., Tanaka S., Saito K., Shu M., Sone Y., Onitake F., Suzuki E., Shimano H., Yamamoto S., Kondo K. Effect of aerobic exercise training on serum levels of high-density lipoprotein cholesterol: a meta-analysis. Arch. Intern. Med. 2007;167:999–1008. doi: 10.1001/archinte.167.10.999. [DOI] [PubMed] [Google Scholar]
- Kokkinos P., Myers J., Faselis C., Panagiotakos D.B., Doumas M., Pittaras A., Manolis A., Kokkinos J.P., Karasik P., Greenberg M. Exercise capacity and mortality in older men: a 20-year follow-up study. Circulation. 2010;122:790–797. doi: 10.1161/CIRCULATIONAHA.110.938852. [DOI] [PubMed] [Google Scholar]
- Koutoukidis D.A., Koshiaris C., Henry J.A., Noreik M., Morris E., Manoharan I., Tudor K., Bodenham E., Dunnigan A., Jebb S.A., Aveyard P. The effect of the magnitude of weight loss on non-alcoholic fatty liver disease: a systematic review and meta-analysis. Metabolism. 2021;115:154455. doi: 10.1016/j.metabol.2020.154455. [DOI] [PubMed] [Google Scholar]
- Krachler B., Savonen K., Komulainen P., Hassinen M., Lakka T.A., Rauramaa R. Cardiopulmonary fitness is a function of lean mass, not total body weight: the DR's EXTRA study. Eur. J. Prev. Cardiol. 2015;22:1171–1179. doi: 10.1177/2047487314557962. [DOI] [PubMed] [Google Scholar]
- Kramer C.K., Zinman B., Retnakaran R. Are metabolically healthy overweight and obesity benign conditions?: a systematic review and meta-analysis. Ann. Intern. Med. 2013;159:758–769. doi: 10.7326/0003-4819-159-11-201312030-00008. [DOI] [PubMed] [Google Scholar]
- Kramer C.K., Zinman B., Retnakaran R. Metabolically healthy overweight and obesity. Ann. Intern. Med. 2014;160:516. doi: 10.7326/L14-5007-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraus W.E., Powell K.E., Haskell W.L., Janz K.F., Campbell W.W., Jakicic J.M., Troiano R.P., Sprow K., Torres A., Piercy K.L. Physical activity, all-cause and cardiovascular mortality, and cardiovascular disease. Med. Sci. Sports Exerc. 2019;51:1270–1281. doi: 10.1249/MSS.0000000000001939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kritchevsky S.B., Beavers K.M., Miller M.E., Shea M.K., Houston D.K., Kitzman D.W., Nicklas B.J. Intentional weight loss and all-cause mortality: a meta-analysis of randomized clinical trials. PLoS One. 2015;10:e0121993. doi: 10.1371/journal.pone.0121993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuk J.L., Ardern C.I., Church T.S., Sharma A.M., Padwal R., Sui X., Blair S.N. Edmonton Obesity Staging System: association with weight history and mortality risk. Appl. Physiol. Nutr. Metab. 2011;36:570–576. doi: 10.1139/h11-058. [DOI] [PubMed] [Google Scholar]
- Kushner R.F. Weight loss strategies for treatment of obesity: lifestyle management and pharmacotherapy. Prog. Cardiovasc. Dis. 2018;61:246–252. doi: 10.1016/j.pcad.2018.06.001. [DOI] [PubMed] [Google Scholar]
- Kushner R.F., Ryan D.H. Assessment and lifestyle management of patients with obesity: clinical recommendations from systematic reviews. JAMA. 2014;312:943–952. doi: 10.1001/jama.2014.10432. [DOI] [PubMed] [Google Scholar]
- Lamarche B., Despres J.P., Pouliot M.C., Moorjani S., Lupien P.J., Theriault G., Tremblay A., Nadeau A., Bouchard C. Is body fat loss a determinant factor in the improvement of carbohydrate and lipid metabolism following aerobic exercise training in obese women? Metabolism. 1992;41:1249–1256. doi: 10.1016/0026-0495(92)90017-5. [DOI] [PubMed] [Google Scholar]
- Laukkanen J.A., Zaccardi F., Khan H., Kurl S., Jae S.Y., Rauramaa R. Long-term change in cardiorespiratory fitness and all-cause mortality: a population-based follow-up study. Mayo Clin. Proc. 2016;91:1183–1188. doi: 10.1016/j.mayocp.2016.05.014. [DOI] [PubMed] [Google Scholar]
- Lee C.D., Blair S.N., Jackson A.S. Cardiorespiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men. Am. J. Clin. Nutr. 1999;69:373–380. doi: 10.1093/ajcn/69.3.373. [DOI] [PubMed] [Google Scholar]
- Lee D.C., Sui X., Artero E.G., Lee I.M., Church T.S., McAuley P.A., Stanford F.C., Kohl H.W., 3rd, Blair S.N. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: the Aerobics Center Longitudinal Study. Circulation. 2011;124:2483–2490. doi: 10.1161/CIRCULATIONAHA.111.038422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lehnig A.C., Dewal R.S., Baer L.A., Kitching K.M., Munoz V.R., Arts P.J., Sindeldecker D.A., May F.J., Lauritzen H., Goodyear L.J., Stanford K.I. Exercise training induces depot-specific adaptations to white and Brown adipose tissue. iScience. 2019;11:425–439. doi: 10.1016/j.isci.2018.12.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lehnig A.C., Stanford K.I. Exercise-induced adaptations to white and brown adipose tissue. J. Exp. Biol. 2018;221:jeb161570. doi: 10.1242/jeb.161570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis Z.H., Markides K.S., Ottenbacher K.J., Al Snih S. The impact of 10-year physical activity changes on 7-year mortality in older Mexican Americans. J. Phys. Act Health. 2018;15:30–39. doi: 10.1123/jpah.2016-0454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin C.J., Chang Y.C., Cheng T.Y., Lo K., Liu S.J., Yeh T.L. The association between metabolically healthy obesity and risk of cancer: a systematic review and meta-analysis of prospective cohort studies. Obes. Rev. 2020;21:e13049. doi: 10.1111/obr.13049. [DOI] [PubMed] [Google Scholar]
- Lin X., Zhang X., Guo J., Roberts C.K., Mckenzie S., Wu W.C., Liu S., Song Y. Effects of exercise training on cardiorespiratory fitness and biomarkers of cardiometabolic health: a systematic review and meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2015;4:e002014. doi: 10.1161/JAHA.115.002014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu J.X., Zhu L., Li P.J., Li N., Xu Y.B. Effectiveness of high-intensity interval training on glycemic control and cardiorespiratory fitness in patients with type 2 diabetes: a systematic review and meta-analysis. Aging Clin. Exp. Res. 2019;31:575–593. doi: 10.1007/s40520-018-1012-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Look Ahead Research Group, Wing R.R., Bolin P., Brancati F.L., Bray G.A., Clark J.M., Coday M., Crow R.S., Curtis J.M., Egan C.M. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N. Engl. J. Med. 2013;369:145–154. doi: 10.1056/NEJMoa1212914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma C., Avenell A., Bolland M., Hudson J., Stewart F., Robertson C., Sharma P., Fraser C., Maclennan G. Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: systematic review and meta-analysis. BMJ. 2017;359:j4849. doi: 10.1136/bmj.j4849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manson J.E., Hu F.B., Rich-Edwards J.W., Colditz G.A., Stampfer M.J., Willett W.C., Speizer F.E., Hennekens C.H. A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. N. Engl. J. Med. 1999;341:650–658. doi: 10.1056/NEJM199908263410904. [DOI] [PubMed] [Google Scholar]
- Martin B.J., Arena R., Haykowsky M., Hauer T., Austford L.D., Knudtson M., Aggarwal S., Stone J.A. Cardiovascular fitness and mortality after contemporary cardiac rehabilitation. Mayo Clin. Proc. 2013;88:455–463. doi: 10.1016/j.mayocp.2013.02.013. [DOI] [PubMed] [Google Scholar]
- Martin C.B., Herrick K.A., Sarafrazi N., Ogden C.L. Attempts to lose weight among adults in the United States, 2013-2016. NCHS Data Brief. 2018:1–8. [PubMed] [Google Scholar]
- McDow K.B., Nguyen D.T., Herrick K.A., Akinbami L.J. Attempts to lose weight among adolescents aged 16-19 in the United States, 2013-2016. NCHS Data Brief. 2019:1–8. [PubMed] [Google Scholar]
- Mehta T., Smith D.L., Jr., Muhammad J., Casazza K. Impact of weight cycling on risk of morbidity and mortality. Obes. Rev. 2014;15:870–881. doi: 10.1111/obr.12222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mikkelsen N., Cadarso-Suarez C., Lado-Baleato O., Diaz-Louzao C., Gil C.P., Reeh J., Rasmusen H., Prescott E. Improvement in VO2peak predicts readmissions for cardiovascular disease and mortality in patients undergoing cardiac rehabilitation. Eur. J. Prev. Cardiol. 2020;27:811–819. doi: 10.1177/2047487319887835. [DOI] [PubMed] [Google Scholar]
- Mileti E., Kwok K.H.M., Andersson D.P., Mathelier A., Raman A., Backdahl J., Jalkanen J., Massier L., Thorell A., Gao H. Human white adipose tissue displays selective insulin resistance in the obese state. Diabetes. 2021;70:1486–1497. doi: 10.2337/db21-0001. [DOI] [PubMed] [Google Scholar]
- Moholdt T., Lavie C.J., Nauman J. Sustained physical activity, not weight loss, associated with improved survival in coronary heart disease. J. Am. Coll. Cardiol. 2018;71:1094–1101. doi: 10.1016/j.jacc.2018.01.011. [DOI] [PubMed] [Google Scholar]
- Mok A., Khaw K.T., Luben R., Wareham N., Brage S. Physical activity trajectories and mortality: population based cohort study. BMJ. 2019;365:l2323. doi: 10.1136/bmj.l2323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montani J.P., Schutz Y., Dulloo A.G. Dieting and weight cycling as risk factors for cardiometabolic diseases: who is really at risk? Obes. Rev. 2015;16(Suppl 1):7–18. doi: 10.1111/obr.12251. [DOI] [PubMed] [Google Scholar]
- Montani J.P., Viecelli A.K., Prevot A., Dulloo A.G. Weight cycling during growth and beyond as a risk factor for later cardiovascular diseases: the 'repeated overshoot' theory. Int. J. Obes. (Lond) 2006;30(Suppl 4):S58–S66. doi: 10.1038/sj.ijo.0803520. [DOI] [PubMed] [Google Scholar]
- Mudaliar U., Zabetian A., Goodman M., Echouffo-Tcheugui J.B., Albright A.L., Gregg E.W., Ali M.K. Cardiometabolic risk factor changes observed in diabetes prevention programs in US settings: a systematic review and meta-analysis. PLoS Med. 2016;13:e1002095. doi: 10.1371/journal.pmed.1002095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ne J.Y.A., Cai T.Y., Celermajer D.S., Caterson I.D., Gill T., Lee C.M.Y., Skilton M.R. Obesity, arterial function and arterial structure - a systematic review and meta-analysis. Obes. Sci. Pract. 2017;3:171–184. doi: 10.1002/osp4.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neter J.E., Stam B.E., Kok F.J., Grobbee D.E., Geleijnse J.M. Influence of weight reduction on blood pressure: a meta-analysis of randomized controlled trials. Hypertension. 2003;42:878–884. doi: 10.1161/01.HYP.0000094221.86888.AE. [DOI] [PubMed] [Google Scholar]
- Oh T.J., Moon J.H., Choi S.H., Lim S., Park K.S., Cho N.H., Jang H.C. Body-weight fluctuation and incident diabetes mellitus, cardiovascular disease, and mortality: a 16-year prospective cohort study. J. Clin. Endocrinol. Metab. 2019;104:639–646. doi: 10.1210/jc.2018-01239. [DOI] [PubMed] [Google Scholar]
- Ortega F.B., Cadenas-Sanchez C., Migueles J.H., Labayen I., Ruiz J.R., Sui X., Blair S.N., Martinez-Vizcaino V., Lavie C.J. Role of physical activity and fitness in the characterization and prognosis of the metabolically healthy obesity phenotype: a systematic review and meta-analysis. Prog. Cardiovasc. Dis. 2018;61:190–205. doi: 10.1016/j.pcad.2018.07.008. [DOI] [PubMed] [Google Scholar]
- Ortega F.B., Cadenas-Sanchez C., Sui X., Blair S.N., Lavie C.J. Role of fitness in the metabolically healthy but obese phenotype: a review and update. Prog. Cardiovasc. Dis. 2015;58:76–86. doi: 10.1016/j.pcad.2015.05.001. [DOI] [PubMed] [Google Scholar]
- Ortega F.B., Lee D.C., Katzmarzyk P.T., Ruiz J.R., Sui X., Church T.S., Blair S.N. The intriguing metabolically healthy but obese phenotype: cardiovascular prognosis and role of fitness. Eur. Heart J. 2013;34:389–397. doi: 10.1093/eurheartj/ehs174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ostergaard L., Jensen M.K., Overvad K., Tjonneland A., Grontved A. Associations between changes in cycling and all-cause mortality risk. Am. J. Prev. Med. 2018;55:615–623. doi: 10.1016/j.amepre.2018.06.009. [DOI] [PubMed] [Google Scholar]
- Osman A.F., Mehra M.R., Lavie C.J., Nunez E., Milani R.V. The incremental prognostic importance of body fat adjusted peak oxygen consumption in chronic heart failure. J. Am. Coll. Cardiol. 2000;36:2126–2131. doi: 10.1016/s0735-1097(00)00985-2. [DOI] [PubMed] [Google Scholar]
- Ostman C., Smart N.A., Morcos D., Duller A., Ridley W., Jewiss D. The effect of exercise training on clinical outcomes in patients with the metabolic syndrome: a systematic review and meta-analysis. Cardiovasc. Diabetol. 2017;16:110. doi: 10.1186/s12933-017-0590-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pack Q.R., Rodriguez-Escudero J.P., Thomas R.J., Ades P.A., West C.P., Somers V.K., Lopez-Jimenez F. The prognostic importance of weight loss in coronary artery disease: a systematic review and meta-analysis. Mayo Clin. Proc. 2014;89:1368–1377. doi: 10.1016/j.mayocp.2014.04.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paffenbarger R.S., Jr., Hyde R.T., Wing A.L., Lee I.M., Jung D.L., Kampert J.B. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N. Engl. J. Med. 1993;328:538–545. doi: 10.1056/NEJM199302253280804. [DOI] [PubMed] [Google Scholar]
- Patterson R., McNamara E., Tainio M., De Sa T.H., Smith A.D., Sharp S.J., Edwards P., Woodcock J., Brage S., Wijndaele K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018;33:811–829. doi: 10.1007/s10654-018-0380-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pattyn N., Cornelissen V.A., Eshghi S.R., Vanhees L. The effect of exercise on the cardiovascular risk factors constituting the metabolic syndrome: a meta-analysis of controlled trials. Sports Med. 2013;43:121–133. doi: 10.1007/s40279-012-0003-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearson M.J., Smart N.A. Effect of exercise training on endothelial function in heart failure patients: a systematic review meta-analysis. Int. J. Cardiol. 2017;231:234–243. doi: 10.1016/j.ijcard.2016.12.145. [DOI] [PubMed] [Google Scholar]
- Petersen C.B., Gronbaek M., Helge J.W., Thygesen L.C., Schnohr P., Tolstrup J.S. Changes in physical activity in leisure time and the risk of myocardial infarction, ischemic heart disease, and all-cause mortality. Eur. J. Epidemiol. 2012;27:91–99. doi: 10.1007/s10654-012-9656-z. [DOI] [PubMed] [Google Scholar]
- Piche M.E., Poirier P., Lemieux I., Despres J.P. Overview of epidemiology and contribution of obesity and body fat distribution to cardiovascular disease: an update. Prog. Cardiovasc. Dis. 2018;61:103–113. doi: 10.1016/j.pcad.2018.06.004. [DOI] [PubMed] [Google Scholar]
- Piercy K.L., Troiano R.P., Ballard R.M., Carlson S.A., Fulton J.E., Galuska D.A., George S.M., Olson R.D. The physical activity guidelines for Americans. JAMA. 2018;320:2020–2028. doi: 10.1001/jama.2018.14854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pontiroli A.E., Ceriani V., Tagliabue E. Compared with controls, bariatric surgery prevents long-term mortality in persons with obesity only above median age of cohorts: a systematic review and meta-analysis. Obes. Surg. 2020;30:2487–2496. doi: 10.1007/s11695-020-04530-3. [DOI] [PubMed] [Google Scholar]
- Pontzer H. Constrained total energy expenditure and the evolutionary biology of energy balance. Exerc. Sport Sci. Rev. 2015;43:110–116. doi: 10.1249/JES.0000000000000048. [DOI] [PubMed] [Google Scholar]
- Pories W.J., Swanson M.S., Macdonald K.G., Long S.B., Morris P.G., Brown B.M., Barakat H.A., Deramon R.A., Israel G., Dolezal J.M. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann. Surg. 1995;222:339–350. doi: 10.1097/00000658-199509000-00011. discussion 350-352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prestgaard E., Mariampillai J., Engeseth K., Erikssen J., Bodegard J., Liestol K., Gjesdal K., Kjeldsen S., Grundvold I., Berge E. Change in cardiorespiratory fitness and risk of stroke and death. Stroke. 2019;50:155–161. doi: 10.1161/STROKEAHA.118.021798. [DOI] [PubMed] [Google Scholar]
- Ramos J.S., Dalleck L.C., Tjonna A.E., Beetham K.S., Coombes J.S. The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: a systematic review and meta-analysis. Sports Med. 2015;45:679–692. doi: 10.1007/s40279-015-0321-z. [DOI] [PubMed] [Google Scholar]
- Rasmussen M.G., Overvad K., Tjonneland A., Jensen M.K., Ostergaard L., Grontved A. Changes in cycling and incidence of overweight and obesity among Danish men and women. Med. Sci. Sports Exerc. 2018;50:1413–1421. doi: 10.1249/MSS.0000000000001577. [DOI] [PubMed] [Google Scholar]
- Riebe D., Franklin B.A., Thompson P.D., Garber C.E., Whitfield G.P., Magal M., Pescatello L.S. Updating ACSM's recommendations for exercise preparticipation health screening. Med. Sci. Sports Exerc. 2015;47:2473–2479. doi: 10.1249/MSS.0000000000000664. [DOI] [PubMed] [Google Scholar]
- Riis S., Christensen B., Nellemann B., Moller A.B., Husted A.S., Pedersen S.B., Schwartz T.W., Jorgensen J.O.L., Jessen N. Molecular adaptations in human subcutaneous adipose tissue after ten weeks of endurance exercise training in healthy males. J. Appl. Physiol. 2019;126:569–577. doi: 10.1152/japplphysiol.00989.2018. [DOI] [PubMed] [Google Scholar]
- Roberson L.L., Aneni E.C., Maziak W., Agatston A., Feldman T., Rouseff M., Tran T., Blaha M.J., Santos R.D., Sposito A. Beyond BMI: the "Metabolically healthy obese" phenotype and its association with clinical/subclinical cardiovascular disease and all-cause mortality -- a systematic review. BMC Public Health. 2014;14:14. doi: 10.1186/1471-2458-14-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross R., Blair S., De Lannoy L., Despres J.P., Lavie C.J. Changing the endpoints for determining effective obesity management. Prog. Cardiovasc. Dis. 2015;57:330–336. doi: 10.1016/j.pcad.2014.10.002. [DOI] [PubMed] [Google Scholar]
- Ross R., Blair S.N., Arena R., Church T.S., Despres J.P., Franklin B.A., Haskell W.L., Kaminsky L.A., Levine B.D., Lavie C.J. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a Scientific Statement from the American heart association. Circulation. 2016;134:e653–e699. doi: 10.1161/CIR.0000000000000461. [DOI] [PubMed] [Google Scholar]
- Rossi A.P., Rubele S., Calugi S., Caliari C., Pedelini F., Soave F., Chignola E., Vittoria Bazzani P., Mazzali G., Dalle Grave R., Zamboni M. Weight cycling as a risk factor for low muscle mass and strength in a population of males and females with obesity. Obesity (Silver Spring) 2019;27:1068–1075. doi: 10.1002/oby.22493. [DOI] [PubMed] [Google Scholar]
- Rubino F., Gagner M. Potential of surgery for curing type 2 diabetes mellitus. Ann. Surg. 2002;236:554–559. doi: 10.1097/00000658-200211000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruiz J.R., Sui X., Lobelo F., Lee D.C., Morrow J.R., Jr., Jackson A.W., Hebert J.R., Matthews C.E., Sjostrom M., Blair S.N. Muscular strength and adiposity as predictors of adulthood cancer mortality in men. Cancer Epidemiol. Biomarkers Prev. 2009;18:1468–1476. doi: 10.1158/1055-9965.EPI-08-1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruiz J.R., Sui X., Lobelo F., Morrow J.R., Jr., Jackson A.W., Sjostrom M., Blair S.N. Association between muscular strength and mortality in men: prospective cohort study. BMJ. 2008;337:a439. doi: 10.1136/bmj.a439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sabag A., Way K.L., Keating S.E., Sultana R.N., O'connor H.T., Baker M.K., Chuter V.H., George J., Johnson N.A. Exercise and ectopic fat in type 2 diabetes: a systematic review and meta-analysis. Diabetes Metab. 2017;43:195–210. doi: 10.1016/j.diabet.2016.12.006. [DOI] [PubMed] [Google Scholar]
- Saeidifard F., Medina-Inojosa J.R., West C.P., Olson T.P., Somers V.K., Bonikowske A.R., Prokop L.J., Vinciguerra M., Lopez-Jimenez F. The association of resistance training with mortality: a systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2019;26:1647–1665. doi: 10.1177/2047487319850718. [DOI] [PubMed] [Google Scholar]
- Santos I., Sniehotta F.F., Marques M.M., Carraca E.V., Teixeira P.J. Prevalence of personal weight control attempts in adults: a systematic review and meta-analysis. Obes. Rev. 2017;18:32–50. doi: 10.1111/obr.12466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sawyer B.J., Bhammar D.M., Angadi S.S., Ryan D.M., Ryder J.R., Sussman E.J., Bertmann F.M., Gaesser G.A. Predictors of fat mass changes in response to aerobic exercise training in women. J. Strength Cond Res. 2015;29:297–304. doi: 10.1519/JSC.0000000000000726. [DOI] [PubMed] [Google Scholar]
- Sawyer B.J., Tucker W.J., Bhammar D.M., Ryder J.R., Sweazea K.L., Gaesser G.A. Effects of high-intensity interval training and moderate-intensity continuous training on endothelial function and cardiometabolic risk markers in obese adults. J. Appl. Physiol. 2016;121:279–288. doi: 10.1152/japplphysiol.00024.2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schellenberg E.S., Dryden D.M., Vandermeer B., Ha C., Korownyk C. Lifestyle interventions for patients with and at risk for type 2 diabetes: a systematic review and meta-analysis. Ann. Intern. Med. 2013;159:543–551. doi: 10.7326/0003-4819-159-8-201310150-00007. [DOI] [PubMed] [Google Scholar]
- Sedlmeier A.M., Baumeister S.E., Weber A., Fischer B., Thorand B., Ittermann T., Dorr M., Felix S.B., Volzke H., Peters A., Leitzmann M.F. Relation of body fat mass and fat-free mass to total mortality: results from 7 prospective cohort studies. Am. J. Clin. Nutr. 2021;113:639–646. doi: 10.1093/ajcn/nqaa339. [DOI] [PubMed] [Google Scholar]
- Semlitsch T., Krenn C., Jeitler K., Berghold A., Horvath K., Siebenhofer A. Long-term effects of weight-reducing diets in people with hypertension. Cochrane Database Syst. Rev. 2021;2:CD008274. doi: 10.1002/14651858.CD008274.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seretis K., Goulis D.G., Koliakos G., Demiri E. The effects of abdominal lipectomy in metabolic syndrome components and insulin sensitivity in females: a systematic review and meta-analysis. Metabolism. 2015;64:1640–1649. doi: 10.1016/j.metabol.2015.09.015. [DOI] [PubMed] [Google Scholar]
- Seretis K., Goulis D.G., Koliakos G., Demiri E. Short- and long-term effects of abdominal lipectomy on weight and fat mass in females: a systematic review. Obes. Surg. 2015;25:1950–1958. doi: 10.1007/s11695-015-1797-1. [DOI] [PubMed] [Google Scholar]
- Shaibi G.Q., Ryder J.R., Kim J.Y., Barraza E. Exercise for obese youth: refocusing attention from weight loss to health gains. Exerc. Sport Sci. Rev. 2015;43:41–47. doi: 10.1249/JES.0000000000000034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharma A.M., Kushner R.F. A proposed clinical staging system for obesity. Int. J. Obes. (Lond) 2009;33:289–295. doi: 10.1038/ijo.2009.2. [DOI] [PubMed] [Google Scholar]
- Sheng B., Truong K., Spitler H., Zhang L., Tong X., Chen L. The long-term effects of bariatric surgery on type 2 diabetes remission, microvascular and macrovascular complications, and mortality: a systematic review and meta-analysis. Obes. Surg. 2017;27:2724–2732. doi: 10.1007/s11695-017-2866-4. [DOI] [PubMed] [Google Scholar]
- Sims E.A. Are there persons who are obese, but metabolically healthy? Metabolism. 2001;50:1499–1504. doi: 10.1053/meta.2001.27213. [DOI] [PubMed] [Google Scholar]
- Singh N., Stewart R.A.H., Benatar J.R. Intensity and duration of lifestyle interventions for long-term weight loss and association with mortality: a meta-analysis of randomised trials. BMJ Open. 2019;9:e029966. doi: 10.1136/bmjopen-2019-029966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snowling N.J., Hopkins W.G. Effects of different modes of exercise training on glucose control and risk factors for complications in type 2 diabetic patients: a meta-analysis. Diabetes Care. 2006;29:2518–2527. doi: 10.2337/dc06-1317. [DOI] [PubMed] [Google Scholar]
- Stanford K.I., Goodyear L.J. Muscle-adipose tissue cross talk. Cold Spring Harb Perspect. Med. 2018;8:a029801. doi: 10.1101/cshperspect.a029801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanford K.I., Middelbeek R.J., Townsend K.L., Lee M.Y., Takahashi H., So K., Hitchcox K.M., Markan K.R., Hellbach K., Hirshman M.F. A novel role for subcutaneous adipose tissue in exercise-induced improvements in glucose homeostasis. Diabetes. 2015;64:2002–2014. doi: 10.2337/db14-0704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strohacker K., Carpenter K.C., Mcfarlin B.K. Consequences of weight cycling: an increase in disease risk? Int. J. Exerc. Sci. 2009;2:191–201. doi: 10.70252/ASAQ8961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sumithran P., Proietto J. The defence of body weight: a physiological basis for weight regain after weight loss. Clin. Sci. (Lond) 2013;124:231–241. doi: 10.1042/CS20120223. [DOI] [PubMed] [Google Scholar]
- Sutin A.R., Stephan Y., Terracciano A. Weight discrimination and risk of mortality. Psychol. Sci. 2015;26:1803–1811. doi: 10.1177/0956797615601103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutin A.R., Terracciano A. Perceived weight discrimination and high-risk health-related behaviors. Obesity (Silver Spring) 2017;25:1183–1186. doi: 10.1002/oby.21845. [DOI] [PubMed] [Google Scholar]
- Syngal S., Coakley E.H., Willett W.C., Byers T., Williamson D.F., Colditz G.A. Long-term weight patterns and risk for cholecystectomy in women. Ann. Intern. Med. 1999;130:471–477. doi: 10.7326/0003-4819-130-6-199903160-00003. [DOI] [PubMed] [Google Scholar]
- Thorogood A., Mottillo S., Shimony A., Filion K.B., Joseph L., Genest J., Pilote L., Poirier P., Schiffrin E.L., Eisenberg M.J. Isolated aerobic exercise and weight loss: a systematic review and meta-analysis of randomized controlled trials. Am. J. Med. 2011;124:747–755. doi: 10.1016/j.amjmed.2011.02.037. [DOI] [PubMed] [Google Scholar]
- Thyfault J.P., Wright D.C. "Weighing" the effects of exercise and intrinsic aerobic capacity: are there beneficial effects independent of changes in weight? Appl. Physiol. Nutr. Metab. 2016;41:911–916. doi: 10.1139/apnm-2016-0122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tian S., Xu Y. Association of sarcopenic obesity with the risk of all-cause mortality: a meta-analysis of prospective cohort studies. Geriatr. Gerontol. Int. 2016;16:155–166. doi: 10.1111/ggi.12579. [DOI] [PubMed] [Google Scholar]
- Toda N., Okamura T. Obesity impairs vasodilatation and blood flow increase mediated by endothelial nitric oxide: an overview. J. Clin. Pharmacol. 2013;53:1228–1239. doi: 10.1002/jcph.179. [DOI] [PubMed] [Google Scholar]
- Tomiyama A.J., Carr D., Granberg E.M., Major B., Robinson E., Sutin A.R., Brewis A. How and why weight stigma drives the obesity 'epidemic' and harms health. BMC Med. 2018;16:123. doi: 10.1186/s12916-018-1116-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Townsend L.K., Knuth C.M., Wright D.C. Cycling our way to fit fat. Physiol. Rep. 2017;5:e13247. doi: 10.14814/phy2.13247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tudor-Locke C., Brashear M.M., Johnson W.D., Katzmarzyk P.T. Accelerometer profiles of physical activity and inactivity in normal weight, overweight, and obese U.S. men and women. Int. J. Behav. Nutr. Phys. Act. 2010;7:60. doi: 10.1186/1479-5868-7-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tuomilehto J., Lindstrom J., Eriksson J.G., Valle T.T., Hamalainen H., Ilanne-Parikka P., Keinanen-Kiukaanniemi S., Laakso M., Louheranta A., Rastas M. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001;344:1343–1350. doi: 10.1056/NEJM200105033441801. [DOI] [PubMed] [Google Scholar]
- Verheggen R.J., Maessen M.F., Green D.J., Hermus A.R., Hopman M.T., Thijssen D.H. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: distinct effects on body weight and visceral adipose tissue. Obes. Rev. 2016;17:664–690. doi: 10.1111/obr.12406. [DOI] [PubMed] [Google Scholar]
- Vissers D., Hens W., Taeymans J., Baeyens J.P., Poortmans J., Van Gaal L. The effect of exercise on visceral adipose tissue in overweight adults: a systematic review and meta-analysis. PLoS One. 2013;8:e56415. doi: 10.1371/journal.pone.0056415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wannamethee S.G., Shaper A.G., Walker M. Changes in physical activity, mortality, and incidence of coronary heart disease in older men. Lancet. 1998;351:1603–1608. doi: 10.1016/S0140-6736(97)12355-8. [DOI] [PubMed] [Google Scholar]
- Ward Z.J., Bleich S.N., Cradock A.L., Barrett J.L., Giles C.M., Flax C., Long M.W., Gortmaker S.L. Projected U.S. State-level prevalence of adult obesity and severe obesity. N. Engl. J. Med. 2019;381:2440–2450. doi: 10.1056/NEJMsa1909301. [DOI] [PubMed] [Google Scholar]
- Wewege M.A., Thom J.M., Rye K.A., Parmenter B.J. Aerobic, resistance or combined training: a systematic review and meta-analysis of exercise to reduce cardiovascular risk in adults with metabolic syndrome. Atherosclerosis. 2018;274:162–171. doi: 10.1016/j.atherosclerosis.2018.05.002. [DOI] [PubMed] [Google Scholar]
- Winter J.E., Macinnis R.J., Nowson C.A. The influence of age the BMI and all-cause mortality association: a meta-analysis. J. Nutr. Health Aging. 2017;21:1254–1258. doi: 10.1007/s12603-016-0837-4. [DOI] [PubMed] [Google Scholar]
- Winter J.E., Macinnis R.J., Wattanapenpaiboon N., Nowson C.A. BMI and all-cause mortality in older adults: a meta-analysis. Am. J. Clin. Nutr. 2014;99:875–890. doi: 10.3945/ajcn.113.068122. [DOI] [PubMed] [Google Scholar]
- Wu Y.K., Berry D.C. Impact of weight stigma on physiological and psychological health outcomes for overweight and obese adults: a systematic review. J. Adv. Nurs. 2018;74:1030–1042. doi: 10.1111/jan.13511. [DOI] [PubMed] [Google Scholar]
- Yaemsiri S., Slining M.M., Agarwal S.K. Perceived weight status, overweight diagnosis, and weight control among US adults: the NHANES 2003-2008 Study. Int. J. Obes. (Lond) 2011;35:1063–1070. doi: 10.1038/ijo.2010.229. [DOI] [PubMed] [Google Scholar]
- Yeh T.L., Chen H.H., Tsai S.Y., Lin C.Y., Liu S.J., Chien K.L. The relationship between metabolically healthy obesity and the risk of cardiovascular disease: a systematic review and meta-analysis. J. Clin. Med. 2019;8:1228. doi: 10.3390/jcm8081228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yerrakalva D., Mullis R., Mant J. The associations of "fatness," "fitness," and physical activity with all-cause mortality in older adults: a systematic review. Obesity (Silver Spring) 2015;23:1944–1956. doi: 10.1002/oby.21181. [DOI] [PubMed] [Google Scholar]
- Yi S.W., Ohrr H., Shin S.A., Yi J.J. Sex-age-specific association of body mass index with all-cause mortality among 12.8 million Korean adults: a prospective cohort study. Int. J. Epidemiol. 2015;44:1696–1705. doi: 10.1093/ije/dyv138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zaccardi F., Davies M.J., Khunti K., Yates T. Comparative relevance of physical fitness and adiposity on life expectancy: a UK Biobank observational study. Mayo Clin. Proc. 2019;94:985–994. doi: 10.1016/j.mayocp.2018.10.029. [DOI] [PubMed] [Google Scholar]
- Zaccardi F., Franks P.W., Dudbridge F., Davies M.J., Khunti K., Yates T. Mortality risk comparing walking pace to handgrip strength and a healthy lifestyle: a UK Biobank study. Eur. J. Prev. Cardiol. 2021;28:704–712. doi: 10.1177/2047487319885041. [DOI] [PubMed] [Google Scholar]
- Zhang X., Cash R.E., Bower J.K., Focht B.C., Paskett E.D. Physical activity and risk of cardiovascular disease by weight status among U.S adults. PLoS One. 2020;15:e0232893. doi: 10.1371/journal.pone.0232893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang X., Rhoades J., Caan B.J., Cohn D.E., Salani R., Noria S., Suarez A.A., Paskett E.D., Felix A.S. Intentional weight loss, weight cycling, and endometrial cancer risk: a systematic review and meta-analysis. Int. J. Gynecol. Cancer. 2019;29:1361–1371. doi: 10.1136/ijgc-2019-000728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang Y., Hou F., Li J., Yu H., Li L., Hu S., Shen G., Yatsuya H. The association between weight fluctuation and all-cause mortality: a systematic review and meta-analysis. Medicine (Baltimore) 2019;98:e17513. doi: 10.1097/MD.0000000000017513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zomer E., Gurusamy K., Leach R., Trimmer C., Lobstein T., Morris S., James W.P., Finer N. Interventions that cause weight loss and the impact on cardiovascular risk factors: a systematic review and meta-analysis. Obes. Rev. 2016;17:1001–1011. doi: 10.1111/obr.12433. [DOI] [PubMed] [Google Scholar]
- Zou H., Yin P., Liu L., Liu W., Zhang Z., Yang Y., Li W., Zong Q., Yu X. Body-weight fluctuation was associated with increased risk for cardiovascular disease, all-cause and cardiovascular mortality: a systematic review and meta-analysis. Front Endocrinol. (Lausanne) 2019;10:728. doi: 10.3389/fendo.2019.00728. [DOI] [PMC free article] [PubMed] [Google Scholar]