

Abstract
Programs that provide affordable and stable housing may contribute to better child health and thus to fewer missed days of school. Drawing on a unique linkage of survey and administrative data, we use a quasi-experimental approach to examine the impact of rental assistance programs on missed days of school due to illness. We compare missed school days due to illness among children receiving rental assistance with those who will enter assistance within two years of their interview, the average length of waitlists for federal rental assistance. Overall, we find that children who receive rental assistance miss fewer days of school due to illness relative to those in the pseudo-waitlist group. We demonstrate that rental assistance leads to a reduction in the number of health problems among children and thus to fewer days of school missed due to illness. We find that the effect of rental assistance on missed school days is stronger for adolescents than for younger children. Additionally, race-stratified analyses reveal that rental assistance leads to fewer missed days due to illness among non-Hispanic White and Hispanic/Latino children; this effect, however, is not evident for non-Hispanic Black children, the largest racial/ethnic group receiving assistance. These findings suggest that underinvestment in affordable housing may impede socioeconomic mobility among disadvantaged non-Hispanic White and Hispanic/Latino children. In contrast, increases in rental assistance may widen racial/ethnic disparities in health among disadvantaged children, and future research should examine why this benefit is not evident for Black children.
Keywords: Rental assistance, Health inequality, School days, Public housing, United States
Introduction
Rental assistance programs from the U.S. Department of Housing and Urban Development (HUD) offer the potential to break the link between socioeconomic disadvantage and exposure to housing insecurity. However, unlike other safety net programs, HUD assistance is not an entitlement. Currently, roughly one in four eligible families receives assistance (HUD 2019a). In 2019, HUD provided rental assistance to approximately 5 million families, including approximately 4 million children under age 18 (HUD 2019b). HUD assistance represents one of the few sources of affordable housing for families in the bottom income quintile, among whom housing affordability concerns are common. In 2019, 83% of renters in the bottom income quintile spent more than 30% of their income on rent, and 72% spent at least one-half of their income on rent (Joint Center for Housing Studies 2020). Exposure to unaffordable and unstable housing can exacerbate child health problems (Sandel et al. 2018) and disrupt schooling during childhood and adolescence (Allison and Attisha 2019).
Participation in HUD rental assistance programs may have important effects on child health. Improvements in housing stability and quality can reduce exposure to acute illnesses (Sharfstein et al. 2001; Swope and Hernández 2019), and more affordable housing can free up resources for various aspects of child enrichment, including childcare and schooling (Newman and Holupka 2014). By providing access to better and more secure housing, HUD assistance might reduce both the incidence of disease in childhood and the severity of conditions. Evidence is mixed (Slopen et al. 2018), but findings from several recent studies suggest that rental assistance improves mental health and reduces asthma symptoms and hospital use among children (Boudreaux et al. 2020; Fenelon et al. 2018; Gubits et al. 2018; Pollack et al. 2019).
Illness is an important predictor of school absence, and reductions in illness burden are likely to increase attendance (Allison and Attisha 2019). School attendance is a critical driver of human capital accumulation, and an increased number of missed days of school can reduce academic achievement (Gottfried 2011). In many cases, absenteeism is a better predictor of grade completion than are standardized test scores (Allensworth and Easton 2007). Thus, if access to rental assistance improves children’s health in ways that improve school attendance, it could have important long-run impacts. Findings from recent work suggest that receiving rental assistance in childhood can increase adult earnings and decrease incarceration (Andersson et al. 2016; Newman et al. 2009). Improvement in health and schooling outcomes is one plausible mechanism.
This study asks whether access to rental assistance reduces the number of days of school missed due to illness for children in low-income households in the United States. The analysis draws on a unique data set that links nationally representative survey data with longitudinal administrative records on participation in HUD rental assistance. We adjust for selection into rental assistance and consider differences between major housing programs and by the child’s age and race/ethnicity.
Background
HUD Rental Assistance Programs
In 2019, the U.S. Department of Housing and Urban Development (HUD) provided rental assistance to approximately 5 million families, including approximately 4 million children under age 18 (HUD 2019b). HUD funds several rental assistance programs that fall into two major categories: project-based housing and housing choice vouchers. Because these programs differ in their design and physical structure, administration, and typical neighborhood context (Center on Budget and Policy Priorities 2017), we may expect them to have differential effects on child outcomes.
Project-based housing comprises two sets of programs. First, public housing refers to subsidized housing owned and operated by local public housing agencies (PHAs).1 Such housing typically consists of multifamily buildings but may also take the form of single-family, scattered-site units. PHAs receive most of their funds from HUD and must follow HUD issuances of public housing rules and regulations.2 Residents are typically expected to contribute 30% of their income to rent. Second, multifamily housing is largely composed of Project-Based Section 8 housing.3 Under this form of assisted housing, developers receive concessionary financing from HUD to develop units in exchange for providing below-market-rate rents. As for residents of public housing, the assistance is tied to the housing unit—not to the tenant. Therefore, residents of multifamily housing developments cannot transfer their assistance subsidy elsewhere if they decide to move. Although multifamily housing involves a number of different HUD programs and includes roughly one-quarter of all subsidized units in the United States, few studies have examined its impact on child outcomes (Kucheva 2018; Newman and Harkness 2002).
The housing choice voucher program was developed as an alternative to public housing that was intended to give families greater flexibility in where they live (Fischer 2015). A voucher provides a subsidy for families to enter the private housing market, with voucher rent paid directly to landlords on the renter’s behalf (Center on Budget and Policy Priorities 2017). Beneficiaries are expected to contribute approximately 30% of their income to rent, and vouchers cover the remainder up to fair market rent for that housing market, which currently is the 40th percentile of rents in the metropolitan area. Vouchers are intended to be portable, and renters are allowed to take their vouchers to any qualified property in the United States. Although vouchers tend to be located in higher-income neighborhoods than project-based housing, studies have suggested that the program generally falls short of facilitating large-scale racial and economic desegregation (DeLuca et al. 2013; Kleit et al. 2016).
In most housing markets, the demand for rental assistance exceeds the supply of assisted housing units. To manage the excess demand for benefits, PHAs establish waitlists that open periodically for applications (Moore 2017). The mean wait time for rental assistance after being placed on a waitlist is currently 26 months, although it can be more than five years in many U.S. cities (HUD 2019b). PHAs exercise discretion over how to manage the length of the waitlist and whether to prioritize some groups for assistance, such as homeless families or persons with disabilities (McCabe 2017).
Previous Evidence on HUD Rental Assistance and Child Health
Housing has long represented the largest expenditure of the vast majority of U.S. families, and the fraction of income spent on housing has increased over the past three decades (Joint Center for Housing Studies 2020). Children who reside in unaffordable, insecure, or poor-quality housing are more likely to experience health problems and to have difficulty managing existing conditions (Beck et al. 2014; Boudreaux et al. 2020; Ma et al. 2008; McCormack et al. 2009; Sandel and Wright 2006; Warren and Font 2015). Gaining access to assisted housing may protect children in low-income families from these housing-related pressures; it may also help reduce children’s risk of developing chronic health conditions, experiencing hospitalizations, or being exposed to toxins, such as lead (Ahrens et al. 2016; Matte and Jacobs 2000; Rauh et al. 2008).
A systematic review of rental assistance programs and children’s health found mixed results but noted that studies adjusting for unobserved selection were more likely to find positive effects (Slopen et al. 2018). Although some such studies failed to find meaningful effects on child health (Fertig and Reingold 2007; Jacob 2004; Jacob et al. 2015), others showed that children receiving rental assistance experience better health than their counterparts not receiving assistance. One study showed that assisted housing reduced behavior problems among children at low risk for behavior issues (Newman and Holupka 2017a). To address selection bias, several recent studies used future treatment to develop a comparison group; that is, they compared rental assistance recipients with those who will receive rental assistance in the future in order to limit unobservable differences between recipients and nonrecipients (e.g., Elwert and Pfeffer 2019). Two recent studies using this approach demonstrated that rental assistance leads to improvements in mental health and reductions in emergency room visits for asthma, a common measure of uncontrolled asthma symptoms (Boudreaux et al. 2020; Fenelon et al. 2018).
Previous Evidence on HUD Rental Assistance and Educational Outcomes
Negative health effects from exposure to unaffordable, unstable, or poor-quality housing may increase health-related absences from school for low-income children (Abt Associates 2015; Cunningham and MacDonald 2012). HUD rental assistance may reduce the likelihood that children miss days of school due to illness. Few studies have examined the impact of rental assistance programs on school attendance. Evidence from the Family Options Study, an experimental study of rental assistance for homeless families, indicated that both long-term and short-term rental subsidies led to short-term declines in school absences relative to no subsidy (Gubits et al. 2018). However, given that the comparison group in this experiment was homeless families only, it is unclear whether this finding can be generalized to federal rental assistance programs overall. A study comparing New York City children receiving vouchers with those who would receive vouchers in the future found no overall effect of receiving vouchers on school attendance, but children who did not change schools had increased attendance (Schwartz et al. 2020).
Studies of other education-related outcomes found that receiving rental assistance has impacts beyond attendance. For example, Currie and Yelowitz (2000) showed that residence in public housing, compared with other rental accommodations, is associated with an 11 percent percentage point reduction in children being held back by a grade. Schwartz et al. (2020) demonstrated that receiving vouchers led to improvements in children’s test scores but that this effect was not driven by attendance. A study of children in Wisconsin demonstrated that children receiving rental assistance had modestly higher math scores than children who would enter rental assistance in the future (Carlson et al. 2019). Finally, emerging evidence suggests that receiving rental assistance in childhood leads to improved educational attainment and better economic outcomes in adulthood (Andersson et al. 2016; Chyn 2018; Newman and Harkness 2002). Although these studies did not specify the mechanism, improved childhood health is a plausible mediator (Jackson 2009).
Differences by HUD Program
Although project-based housing and vouchers differ in their flexibility, administration, and neighborhood context, each program may improve health and reduce school absences. Several recent studies found that short-term health benefits of rental assistance are more substantial for public housing than for vouchers, particularly for mental health and distress outcomes (Fenelon et al. 2017; Fenelon et al. 2018). Public housing has also shown stronger positive effects on asthma (Boudreaux et al. 2020). Public housing developments may provide access to informal social support networks that promote good mental health or facilitate accessing healthcare (Keene and Ruel 2013; Simon et al. 2017), which may reduce missed school days due to illness.
In contrast, vouchers may provide neighborhood mobility and access to better schools, which could improve educational outcomes. A study of rental assistance and student achievement in Wisconsin found that beneficial effects of rental assistance on math scores were limited to housing choice vouchers (Carlson et al. 2019). In addition, some evidence suggests that the benefits of vouchers—in contrast to public housing—may manifest in the long term (Chetty et al. 2016; Chyn 2018). However, several studies of public housing demolitions in Chicago found no differences in health and schooling outcomes between public housing and housing vouchers (Jacob 2004; Jacob et al. 2015).
Differences by Race/Ethnicity and Age
Non-White children account for the majority of children receiving rental assistance in the United States, with White children accounting for just one-quarter (Fenelon et al. 2018). Limited research has explored whether the benefit of rental assistance for child outcomes varies based on race/ethnicity, although studies have indicated that the protective effects of socioeconomic status indicators (e.g., income, education) on health are smaller for Black and Latino families than for White families (Assari 2018a, 2018b). Given that non-equivalence of the benefits of socioeconomic status can be at least partially explained by racial residential segregation, housing programs that enable families to access better neighborhoods may help to counter this pattern (Williams et al. 2010). Consistent with this idea, one study in Wisconsin indicated that housing vouchers had a significant effect on math achievement for Black children but not for White children, which the authors attributed to improvements in neighborhood and school quality (Carlson et al. 2019). However, research using data from the Panel Study of Income Dynamics (PSID) found that neighborhood disadvantage is significantly higher for Black children receiving rental assistance than for their White counterparts (Newman and Holupka 2017b).
Prior research on neighborhoods and health has suggested potential age-related differences in the impact of rental assistance on school attendance (Nguyen et al. 2016; Schmidt et al. 2017). For example, drawing on data from the Moving to Opportunity (MTO) study, Chetty et al. (2016) reported that moving to a lower-poverty neighborhood significantly improved socioeconomic outcomes in adulthood, but only for children who were younger than 13 years when their families moved. However, other studies from MTO and the PSID suggested that neighborhood context in adolescence has a stronger influence than earlier in life for certain outcomes, such as teen pregnancy and risky behaviors (Schmidt et al. 2017; Wodtke 2013).
Empirical research on the effects of rental assistance on child outcomes has been limited by the dearth of high-quality data in the United States (Slopen et al. 2018). Much of the existing literature has relied on detailed data from a single city or PHA (e.g., Jacob et al. 2015), and studies using national data have often had to rely on respondent self-reporting of rental assistance participation, which has limitations compared with the use of administrative records (Boudreaux et al. 2018; Shroder and Martin 1996). Selection bias is also a particularly important consideration in research on rental assistance because participating families are highly selected on indicators of socioeconomic disadvantage (Helms et al. 2018). As a result, observational studies that compare children receiving rental assistance with those not receiving rental assistance are inadequate in their ability to establish causal effects (Newman and Holupka 2016).
This study overcomes the limitations of previous research using a unique data set that links nationally representative survey data with administrative records on rental assistance participation. We examine the impact of receiving rental assistance on children’s missed school days due to illness. We apply a quasi-experimental waitlist design to account for unobserved factors that select families into rental assistance and isolate the causal effects on children’s outcomes. We examine differences in these effects between project-based housing and housing choice vouchers and by the child’s race/ethnicity and age. We find that access to rental assistance reduces children’s days of school missed due to illness. We demonstrate that this effect is strongest for housing choice vouchers, White and Latino children, and adolescents. We do not find a significant effect for non-Hispanic Black children, who make up 47% of children receiving rental assistance. We also confirm that the relationship between rental assistance and missed school days plausibly represents the impact of rental assistance on child health problems.
Data
We use data from the National Health Interview Survey (NHIS) linked with HUD administrative rental assistance records (Lloyd et al. 2017). Public-use NHIS data were obtained from IPUMS NHIS, which produces a harmonized version of the NHIS (Blewett et al. 2016). NHIS is a multistage, nationally representative household survey that collects a variety of economic, demographic, and health indicators of all members of sampled households. Our measures of missed school days and child health come from the NHIS Sample Child file, which collects detailed information on one randomly selected child per household. The sample covers 1999–2001 and 2004–2012.4 The HUD administrative records cover 1999–2014 and are linked to NHIS based on deterministic matching (Lloyd and Helms 2016). The HUD file provides a longitudinal record of rental assistance entry and exit dates that can be used to generate housing episode histories for each NHIS respondent, including information on housing program (project-based housing and housing choice vouchers). The timing of rental assistance entry is vital to our quasi-experimental approach.
Sample
To be eligible for linkage to the HUD record, NHIS survey respondents must consent to administrative data linking and provide sufficient personally identifiable information: Social Security number, date of birth, and sex. To adjust for potential bias in eligibility for linkage, the National Center for Health Statistics (NCHS) created weights that account for both linkage eligibility and nonresponse to make estimates representative of the civilian noninstitutionalized U.S. population (Lloyd and Helms 2016). The final linked data file includes 28,998 linkage eligible school-aged respondents (aged 5–17) interviewed by the NHIS (1999–2001, 2004–2012) with nonmissing information on the covariates and outcomes. At the time of their interview, 1,485 children (5.1% of the linkage-eligible sample) were current rental assistance recipients: 551 lived in project-based housing, and 934 were using housing choice vouchers. Additionally, 571 respondents would enter rental assistance within two years of their interview, the mean waiting period to enter HUD housing (HUD 2019b).
Missed School Days Due to Illness
Our primary outcome comes from the Sample Child questionnaire, which collects information on the number of missed school days due to illness or injury in the past year for school-aged children (i.e., aged 5–17). The survey asks, “During the past 12 months, about how many days did [SAMPLE CHILD] miss school because of illness or injury?” A knowledgeable adult provides a response that ranges from 0 to 240 days. About 28% of the total sample reported 0 missed school days in the past year, and 10% reported more than 10 missed days. We measure missed school days in two ways: (1) a continuous count of missed days of school due to illness, and (2) a dichotomous measure of whether the child missed at least two weeks of school (10 or more days or fewer than 10 days, consistent with other studies using the NHIS; Classi et al. 2012). Sensitivity analyses in section D of the online appendix examine other thresholds of missed days.
Rental Assistance Status
The primary independent variable of interest is whether the child lives in a household receiving HUD rental assistance, including the specific housing program (housing choice vouchers, project-based housing). To address the potential of selection into rental assistance, we use a quasi-experimental approach that exploits the timing of assistance. We compare children currently receiving rental assistance with children in a pseudo-waitlist comparison group—that is, those who will enter assisted housing within two years. Because waits for rental assistance average about two years, pseudo-waitlist children are likely to resemble those on HUD waitlists.5 This approach accounts for unobserved time-invariant differences between individuals and families that obtain rental assistance and those that do not, given that all pseudo-waitlist individuals eventually enter rental assistance.6 This approach has been applied in previous work on HUD assistance and health (Boudreaux et al. 2020; Keene et al. 2018; Wong et al. 2018) and has been suggested as a means of addressing unobserved selection in other treatments (Elwert and Pfeffer 2019; Schwartz et al. 2020).
Individual and Family Characteristics
Our covariates from the NHIS include (1) the individual characteristics of age (coded as 5–9 or 10–17 years), sex, and race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, or other); and (2) the family characteristics of family structure (one parent or two parents partnered/married), household highest level of education (less than high school, high school, or more than high school), family income-to-poverty ratio (<50%, 50%–100%, 100%–200%, or 200%+), and household employment status (any worker in the household or no workers in the household). We also adjust for census region and the interview year. These covariates are included to improve the precision of our estimates insofar as they are predictive of the outcomes. However, if our pseudo-waitlist design is robust, the coefficient for rental assistance should not change significantly with the inclusion of these covariates.
Contextual Characteristics
To examine the possibility that neighborhood outcomes mediate the relationship between rental assistance and schooling outcomes (Schwartz et al. 2020), we include three indexes of neighborhood socioeconomic and demographic characteristics (Fenelon et al. 2018). These data come from the 2000 Census Summary File 3 and the 2010–2014 American Community Survey and are linearly interpolated for 2001–2009. Individual variables are percentage single-family housing, poverty rate, percentage unemployed, percentage college graduates, percentage on public assistance, percentage in professional occupations, percentage female-headed households, percentage renter, percentage vacant, and percentage living in a different residence five years prior.
We used principal components analysis to generate three neighborhood indexes. The first component—disadvantage—was loaded with the family poverty rate, the percentage receiving public assistance, and percentage female-headed households. The second component—instability—was associated with percentage living in a different residence five years prior and percentage renter-occupied housing, and was inversely associated with the percentage single-family housing. The third component—vacancy—was loaded with percentage vacant housing and percentage living in a different residence (see the online appendix for full component analysis and variable loadings). Research has found that these three measures are related to children’s schooling and health outcomes (Dupere et al. 2010; Leventhal and Brooks-Gunn 2000; Snedker et al. 2009; Wang and Immergluck 2018). Indexes are normalized to have a mean of 0 and a standard deviation of 1. We also include a measure of neighborhood racial composition, categorizing tracts as either mostly White (>80%), mostly Black (>80%), mostly Hispanic/Latino (>50%), or mixed race (all other compositions) (Fenelon et al. 2018).
Health Measures
We examine whether child health represents a plausible mediator of the relationship between rental assistance and missed school days due to illness. We select six parent-reported health measures of child physical health available in each year of the NHIS: fair or poor health status, frequent ear infections, frequent headaches, vision problem, emergency room visit due to asthma attack, and hospitalization in the past year. Previous research has found that these measures respond to housing conditions (Bailie et al. 2012; Boudreaux et al. 2020; Gubits et al. 2018; Sadowski et al. 2009; Smith et al. 2015) and represent health problems that could plausibly lead to missed school days (Allison and Attisha 2019). Correlations among health measures are not high enough for collinearity to be a concern (see section G of the online appendix).
Methods
Our statistical approach involves three steps. First, we examine the relationship between rental assistance and measures of missed school days. Count variables that show evidence of overdispersion violate the assumptions of Poisson regression. Because initial analysis of missed school days indicates overdispersion, we use negative binomial regression to predict the log of the count of missed school days as a function of rental assistance status (Long 1997). Although about 30% of children report no missed school days, Allison (2012) suggested that zero-inflated models should be used only if there is a theoretical reason to expect the inflation model (any vs. none) operates through a different stochastic process than the negative binomial model (number of missed days given any). In the current case, we expect similar processes and prefer the standard negative binomial model.7 These models measure rental assistance status first using a naïve indicator (current assistance vs. no assistance at the time of interview) and then using the pseudo-waitlist approach:
where yi is a count of the number of days of school missed for individual i, R is rental assistance status (naïve or pseudo-waitlist measure), X is a vector of individual and family characteristics, and T is a vector of tract-by-year neighborhood characteristics. In additional models, we use logistic regression models to examine the relationship between rental assistance and whether a child missed at least two weeks of school due to illness.
Second, we consider whether these relationships differ by HUD housing program (housing choice vouchers or project-based housing), race/ethnicity (non-Hispanic White, non-Hispanic Black, or Hispanic/Latino), and age of the child (5–11 years or 12–17 years). We estimate models similar to those presented earlier stratified by subgroup.
Finally, we test whether health problems mediate the relationship between rental assistance and missed school days due to illness. We first predict each health measure as a function of rental assistance status using logistic regression. Then we include health measures in the main negative binomial models to determine whether effects of rental assistance on missed school days are attenuated. All analyses are weighted using NCHS-adjusted weights for linkage eligibility and account for the complex multistage survey design of the NHIS.
To examine the robustness of our pseudo-waitlist approach, we look for any trends in missed school days for pseudo-waitlist children in the months before entering rental assistance. If we see changes in the number of missed school days leading up to entry into rental assistance, then the approach may be biased by preexisting trends. Instead, if changes in missed school days emerge only for children receiving rental assistance, it would increase our confidence in a causal interpretation of our results. We estimate an event study model that predicts the missed days as a function of the timing of the interview relative to entry into rental assistance, examining the outcome in one-year windows before and after entry into rental assistance.
Results
Our total sample includes all children ages 5–17 who were either receiving rental assistance at interview or were within two years of entering rental assistance. Descriptive characteristics of the sample are shown in Table 1, stratified by rental assistance status (current assistance or pseudo-waitlist). Current rental assistance recipients tend to be slightly older than pseudo-waitlist children (42% aged 12–17 vs. 37%; p = .11) and are more likely to live in a single-parent family than pseudo-waitlist children (84% vs. 78%; p = .029). However, no other statistically significant differences are evident between current and pseudo-waitlist children. The current assistance group and pseudo-waitlist group have similar profiles of demographic characteristics and economic disadvantage (see Table A1 in the online appendix for comparisons with children who receive no rental assistance during the period). Among current assistance recipients, 75% are racial/ethnic minorities, 68% have a family income below the federal poverty line, 58% live in families in which the highest level of education is high school or less, and 45% have no current worker in the family. Among pseudo-waitlist children, 75% are racial minorities, 63% are in poverty, 58% have family education of high school or less, and 42% have no worker in the family. The similarity of these two groups provides support for our pseudo-waitlist approach and suggests that the comparison includes similar individuals before and after entry into rental assistance.
Table 1.
Descriptive characteristics of the NHIS-HUD sample by rental assistance status, 1999–2012
| Currenta | Pseudo-Waitlistb | |
|---|---|---|
| n | 1,485 | 571 |
| Male | 0.504 | 0.513 |
| Age Group | ||
| 5–11 years | 0.585 | 0.632 |
| 12–17 years | 0.415 | 0.368 |
| Race/Ethnicity | ||
| Non-Hispanic White | 0.254 | 0.246 |
| Non-Hispanic Black | 0.467 | 0.483 |
| Non-Hispanic other | 0.060 | 0.045 |
| Hispanic/Latino | 0.220 | 0.226 |
| Family Structure* | ||
| Single parent | 0.839 | 0.776 |
| Married/partnered parents | 0.162 | 0.224 |
| Highest Level of Education | ||
| Less than high school | 0.238 | 0.230 |
| High school | 0.341 | 0.346 |
| More than high school | 0.421 | 0.424 |
| Family Poverty Statusc | ||
| Below 50% FPL | 0.309 | 0.299 |
| 50% to 99% of FPL | 0.372 | 0.332 |
| 100% to 199% of FPL | 0.247 | 0.266 |
| 200%+ of FPL | 0.073 | 0.103 |
| Family Employment | ||
| No worker in family | 0.453 | 0.422 |
| Any worker in family | 0.547 | 0.578 |
| Region | ||
| Northeast | 0.182 | 0.191 |
| Midwest | 0.265 | 0.145 |
| South | 0.395 | 0.508 |
| West | 0.158 | 0.157 |
| Census Tract Characteristics | ||
| Disadvantage indexd | 0.867 | 0.909 |
| Instability indexd | −0.106 | −0.017 |
| Vacancy indexd | −0.088 | 0.032 |
| Tract Racial Composition | ||
| >80% White | 0.232 | 0.231 |
| >80% Black | 0.104 | 0.123 |
| >50% Hispanic | 0.129 | 0.137 |
| Mixed race | 0.534 | 0.509 |
Note: All children in the sample received rental assistance at some point during the observation period, 1999–2014.
Receiving rental assistance at interview.
Not receiving assistance at interview, but will enter assistance within two years of the interview.
FPL = federal poverty line.
The index is calculated using principal components analysis and is normalized with a mean of 0 and a standard deviation of 1. See section C of the online appendix for full variable loadings.
Chi-square test of difference between current and pseudo-waitlist significant at p < .05
Naïve and Pseudo-Waitlist Models
Table 2 presents results for missed school days based on (1) a naïve indicator that compares those receiving assistance with those not receiving assistance, and (2) our quasi-experimental pseudo-waitlist model. The naïve negative binomial model indicates that children receiving rental assistance miss more school days due to illness than children who do not receive assistance (incidence rate ratio [IRR] = 1.143; 95% CI = 1.047–1.246). In contrast, the pseudo-waitlist model indicates that children receiving rental assistance miss fewer days of school than their counterparts who will enter within two years (IRR = 0.783; 95% CI = 0.623–0.985). Rental assistance is associated with a 22% reduction in the number of missed days. Thus, after we account for unobserved selection into rental assistance, the results imply that rental assistance leads to fewer missed school days among those who participate in an assistance program. The logistic regression models predicting the odds of missing at least two weeks show a corresponding difference between the naïve and pseudo-waitlist specifications. The naïve model implies that rental assistance is associated with increased odds of missing two weeks (OR = 1.429; 95% CI = 1.193–1.717), and the pseudo-waitlist model implies the opposite result (although not statistically significant) (OR = 0.820; 95% CI = 0.571–1.179). Furthermore, the coefficient in the pseudo-waitlist model does not substantively change after adjustment for covariates, indicating the robustness of the pseudo-waitlist design (see section A of the online appendix for full model results).
Table 2.
Naïve and pseudo-waitlist models predicting missed school days as a function of rental assistance status
| Log Missed School Days (incidence rate ratios)a | Missed at Least Two Weeks of School (odds ratios)b | ||||
|---|---|---|---|---|---|
| Current Assistance | Naïvec | Pseudo-Waitlistd | Naïve | Pseudo-Waitlist | |
| Unadjusted Model | 1.143** (1.047, 1.246) |
0.783* (0.623, 0.985) |
1.429** (1.193, 1.717) |
0.820 (0.571, 1.179) |
|
| Adjusted Model | 1.004 (0.912, 1.108) |
0.795* (0.651, 0.972) |
1.064 (0.819, 1.413) |
0.728† (0.509, 1.042) |
|
Notes: Models predict missed school days outcomes among children aged 5–17. All models adjust for the complex survey design of the NHIS and are weighted to reflect eligibility for linkage to HUD. Unadjusted models contain no covariates. Adjusted models include individual and family characteristics (full covariate results are shown in section A of the online appendix). Values in parentheses are 95% confidence intervals.
Source: Authors’ calculations using NHIS-HUD linkage 1999–2012.
Count of missed school days is modeled using negative binomial regression.
Missed at least two weeks of school is modeled using logistic regression.
The naïve models compare current assistance recipients with all children not receiving assistance at interview.
The pseudo-waitlist model uses as the reference category those children who are not receiving assistance at interview but will enter rental assistance within two years, the mean length of HUD waitlists.
p < .10;
p < .05;
p < .01
Differences by Housing Program
Table 3 compares the effects of rental assistance on missed school days for housing choice vouchers and project-based housing. These models include the full set of individual, family, and neighborhood controls, but the sample is stratified by program. Overall, the effect of rental assistance on missed school days is not significantly different between housing choice vouchers and project-based housing. Children receiving vouchers miss significantly fewer days of school than their counterparts who will receive vouchers within two years (IRR = 0.770; 95% CI = 0.613–0.969)—a 23% difference. The coefficient for children in project-based housing is negative but not statistically significant (IRR = 0.864; 95% CI = 0.639–1.170). Both vouchers and project-based housing predict a reduced likelihood of missing at least two weeks of school, but neither relationship reaches statistical significance. An interaction term between rental assistance status and housing program was not statistically significant for either outcome.
Table 3.
Effects of rental assistance on missed school days comparing housing choice vouchers and project-based housing: Current assistance Versus pseudo-waitlist
| Program Type (vs. pseudo-waitlist) | Log Missed School Days (incidence rate ratios)a | Missed at Least Two Weeks (odds ratios)b |
|---|---|---|
| Housing Choice Vouchers (N = 1,317) | 0.770** (0.613, 0.969) |
0.712 (0.470, 1.079) |
| Project-Based Housing (N = 749) | 0.864 (0.639, 1.170) |
0.636 (0.329, 1.228) |
Notes: Models predict missed school days outcomes among children aged 5–17. All models adjust for the complex survey design of the NHIS and are weighted to reflect eligibility for linkage to HUD. Models are stratified by housing program and adjust for individual, family, and contextual characteristics listed in the Data and Methods section. Each coefficient compares current rental assistance recipients with those in the pseudo-waitlist group. Values in parentheses are 95% confidence intervals.
Source: Authors’ calculations using NHIS-HUD linkage, 1999–2012.
Count of missed school days is modeled using negative binomial regression.
Missed at least two weeks of school is modeled using logistic regression.
p < .01
Child Health Problems
We confirm that child health problems are a plausible mediator of the relationship between rental assistance and missed school days due to illness. First, we assess the effect of rental assistance on each health measure. The models in Table 4 predict the odds of each health outcome as a function of rental assistance status, adjusting for individual, family, and neighborhood characteristics. Children receiving rental assistance tend to be at lower risk of health problems, particularly more severe events. Compared with pseudo-waitlist children, current assistance recipients are less likely to have had an emergency room visit due to an asthma attack (OR = 0.36), to have been hospitalized in the past year (OR = 0.37), and to report frequent ear infections (OR = 0.61). Rental assistance is also associated with reduced odds of fair/poor health status and vision problems, but these differences are not statistically significant. There is no relationship between rental assistance and frequent headaches in children.
Table 4.
Effects of rental assistance on child health problems: Current assistance versus pseudo-waitlist
| Current Assistance Versus Pseudo-Waitlist (odds ratios) | |
|---|---|
| Fair/Poor Health Status | 0.730 (0.436, 1.225) |
| Frequent Headaches | 1.022 (0.710, 1.469) |
| Frequent Ear Infections | 0.610* (0.379, 0.982) |
| Vision Problem | 0.666 (0.379, 1.170) |
| Hospitalized in Last Year | 0.373** (0.182, 0.764) |
| ER Visit Due to Asthma Attack | 0.363** (0.220, 0.601) |
Notes: Each row refers to a separate logistic regression model predicting each health outcome as a function of rental assistance status using the analytical sample. All models adjust for individual, family, and contextual characteristics listed in the Data and Methods sections. Each odds ratio compares current rental assistance recipients with those in the pseudo-waitlist group. Values in parentheses are 95% confidence intervals.
Source: Authors’ calculations using NHIS-HUD linkage, 1999–2012.
p < .05;
p < .01
Next, we adjust for these health measures in our main model predicting missed school days. In Table 5, the first model is our primary adjusted model from Table 2. The second model adds the six health measures. The coefficient for each health measure is positive and significant, indicating that each is associated with an increase in the number of missed school days due to illness. After the inclusion of the health measures, the coefficient on current assistance is attenuated substantially and is no longer statistically significant (IRR = 0.942; 95% CI = 0.79–1.12). This result suggests that 71% of the total effect (IRR 0.79 vs. 0.94) of rental assistance on missed school days due to illness is explained by this specific set of health problems and healthcare utilization events.
Table 5.
Effects of rental assistance on missed school days adjusting for health problems: Current assistance versus pseudo-waitlist
| Log Missed School Days (incidence rate ratios) | ||
|---|---|---|
| Model 1 | Model 2 | |
| Current Assistance | 0.795* (0.651, 0.972) |
0.942 (0.794, 1.117) |
| Health Problems | ||
| Fair/poor health status | 2.452** (1.893, 3.174) |
|
| Frequent headaches | 1.401** (1.184, 1.657) |
|
| Frequent ear infections | 1.370* (1.073, 1.751) |
|
| Vision problem | 1.405* (1.001, 1.972) |
|
| Hospitalized in last year | 1.616** (1.203, 2.171) |
|
| Emergency room visit due to asthma | 2.119** (1.699, 2.641) |
|
| Individual and Contextual Controls | Yes | Yes |
| N | 2,056 | 2,056 |
Notes: Models predict missed school days outcomes among children aged 5–17 using negative binomial regression. The first model replicates the coefficient from the adjusted model in Table 2. The second model adds the six indicators of health problems. Both models include individual, family, and contextual characteristics listed in the Data and Methods section. Values in parentheses are 95% confidence intervals.
Source: Authors’ calculations using NHIS-HUD linkage, 1999–2012.
p < .05;
p < .01
Differences by Race/Ethnicity and Age
Finally, we examine differences in the effects of rental assistance on missed school days by age and race/ethnicity (Table 6). Interaction terms (global F tests) for age and race/ethnicity are statistically significant (p < .05). Rental assistance is associated with a greater reduction in missed school days and a greater reduction in risk of missing at least two weeks among adolescents aged 12–17 years than among children aged 5–11 years. The reduction in missed school days is also greatest for non-Hispanic White children (36%) and Hispanic/Latino children (29%); the association between rental assistance and missed school days is not evident among Black children.
Table 6.
Effects of rental assistance on missed school days comparing effects by child’s age group and race/ethnicity: Current assistance Versus pseudo-waitlist
| Current Assistance | Log Missed School Days (incidence rate ratios) | Missed at Least Two Weeks (odds ratios) |
|---|---|---|
| Age Group | ||
| 5–11 years | 0.875 (0.718, 1.064) |
0.952 (0.625, 1.452) |
| 12–17 years | 0.702* (0.518, 0.951) |
0.533* (0.293, 0.967) |
| Race/Ethnicity | ||
| White, non-Hispanic | 0.640** (0.449, 0.913) |
0.650 (0.319, 1,324) |
| Black, non-Hispanic | 0.989 (0.720, 1.361) |
1.14 (0.569, 2,288) |
| Hispanic/Latino | 0.710* (0.529, 0.951) |
0.540† (0.285, 1.021) |
Notes: Models predict missed school days outcomes among children aged 5–17. All models adjust for the complex survey design of the NHIS, are weighted to reflect eligibility for linkage to HUD, and adjust for individual, family, and contextual characteristics listed in the Data and Methods sections. The first two models are stratified by age group, and the next three models are stratified by race/ethnicity. Each coefficient compares current rental assistance recipients with those in the pseudo-waitlist group. Values in parentheses are 95% confidence intervals.
Source: Authors’ calculations using NHIS-HUD linkage, 1999–2012.
p < .10;
p < .05;
p < .01
The results of an event study model are shown in Figure 1. The graph displays model coefficients for missed school days in one-year intervals relative to entry into rental assistance (i.e., the time before entering housing and the time since entered housing, corresponding to the pseudo-waitlist period and the current assistance period, respectively). Overall, there appears to be no significant trend in missed days before entering rental assistance for pseudo-waitlist children. There also is no evidence of a trend in missed days with greater duration spent in rental assistance, although children in the current assistance group tend to have coefficients below 0 (not all statistically significant). These findings provide some assurance of the robustness of our pseudo-waitlist design and suggest that health-related missed days of school are not changing before entrance into housing.
Fig. 1.
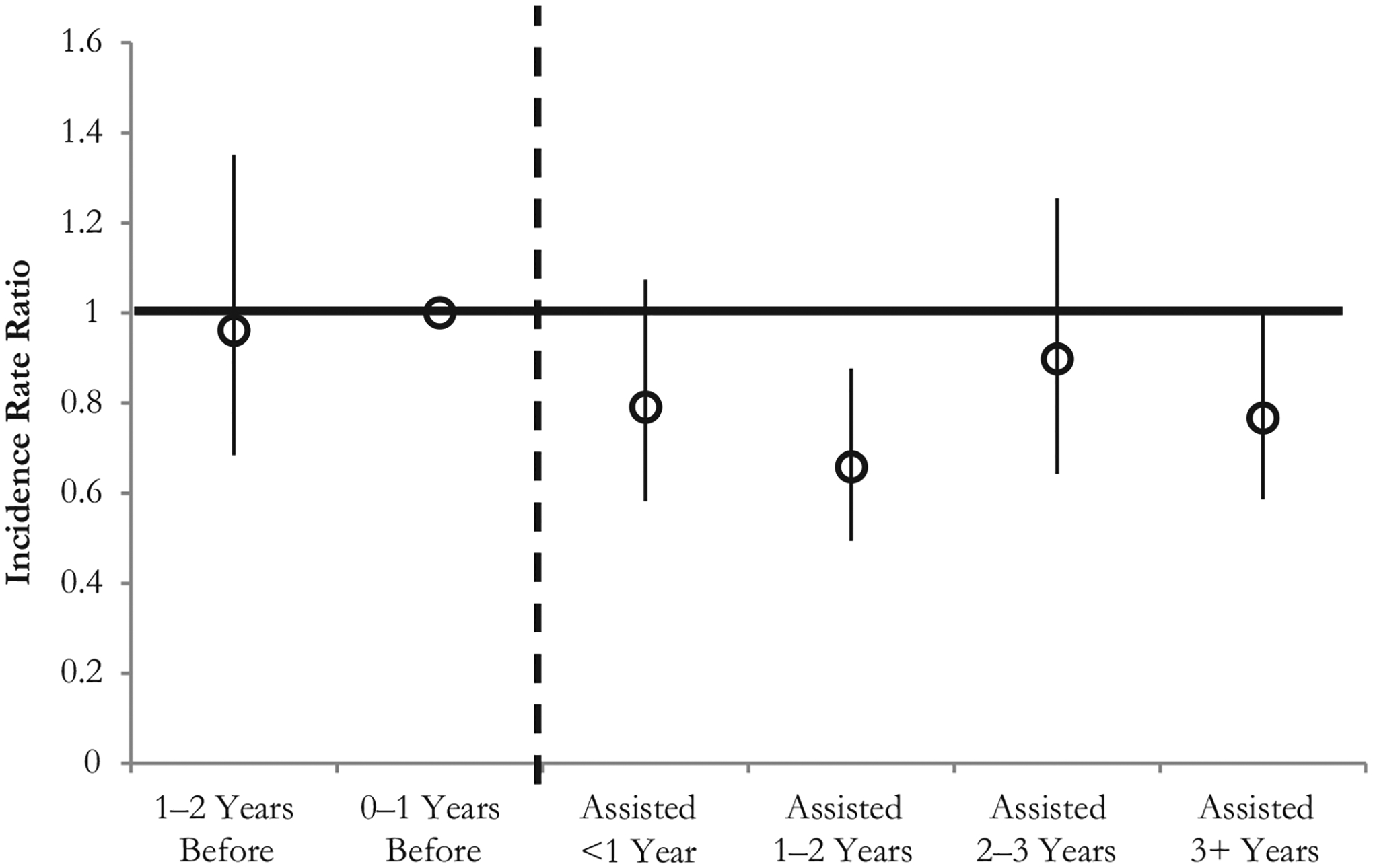
Event study model examining missed school days as a function of time relative to entrance into rental assistance. The graph shows coefficients from negative binomial models by timing relative to entry into rental assistance. “Before” refers to the number of years from the interview to entry into rental assistance. “Assisted” refers to the number of years since entering rental assistance, according to the data linkage. The reference category is children in the year before entry. Models adjust for individual, family, and neighborhood characteristics in Table 3 and the year of interview. The error bars represent 95% confidence intervals.
Discussion
Our focus in this analysis is to examine whether federal rental assistance policies—a $40+ biliion annual federal investment—can reduce the number of school days missed for disadvantaged U.S. children. Our analysis capitalizes on a unique survey-administrative linkage and a quasi-experimental approach to examine the impact of receiving rental assistance on childhood health and schooling outcomes. Our results demonstrate that children receiving rental assistance experience a 22% reduction in the number of days of school missed due to illness. We also confirm that this relationship plausibly represents the effect of rental assistance on children’s health. To our knowledge, this is the first nationwide evidence that investments in affordable and stable housing can improve children’s school attendance through better health, which can be expected to have implications for academic performance and educational attainment. The results provide support for the role of housing inequalities in the production of health inequalities both in childhood and across the life course and the potential for federal rental assistance policies to alleviate these inequalities (Acevedo-Garcia et al. 2008; Hughes et al. 2017).
Reducing inequalities in child health is an important policy goal in and of itself, but it also may affect schooling inequalities (Allison and Attisha 2019). Our study provides evidence that access to rental assistance programs for low-income children can increase school attendance by improving health. These findings have two important implications for child inequalities: (1) rental assistance can reduce socioeconomic inequalities in child health, and (2) rental assistance can reduce inequalities in schooling.
Our results further indicate that rental assistance reduces child health problems. Compared with their counterparts waiting to enter housing, children receiving rental assistance experience fewer ear infections, asthma emergency visits, and hospitalizations. Given that families who receive rental assistance tend to be an extremely disadvantaged subset of the U.S. population (Foster and Rojas 2018; Helms et al. 2017), greater investments in affordable and stable housing represent a valuable policy lever for reducing inequalities in child health. These results are consistent with other recent evidence suggesting that rental assistance provides a health benefit for both children and adults (Boudreaux et al. 2020; Fenelon et al. 2018; Keene et al. 2020).
Our finding that rental assistance leads to a sizable reduction in missed school days due to illness strengthens the notion that housing represents an important platform for investing in children’s educational outcomes (Cunningham and MacDonald 2012). We provide evidence that giving families access to decent, affordable housing reduces health-related school absences among children, which can have lasting effects on educational achievement and attainment (Gottfried 2011). This finding is consistent with experimental evidence among homeless families provided with supportive housing (Gubits et al. 2018) and quasi-experimental evidence that rental assistance improves academic achievement (Carlson et al. 2019; Schwartz et al. 2020). Furthermore, longer-term studies of rental assistance in childhood have found that it increases adult employment and earnings while reducing incarceration risk (Andersson et al. 2016; Newman and Harkness 2002). Future work should attempt to specify whether improved health and school attendance can explain the relationship between rental assistance and longer-term economic benefits.
Differences by Program, Race/Ethnicity, and Age
Our study contributes to the growing literature demonstrating important differences between major rental assistance programs in their impacts on children’s health. Although the stigma historically associated with public housing seems to imply that project-based housing would have negative effects on resident children, past work demonstrated larger gains in mental health from public housing than children in families receiving vouchers (Boudreaux et al. 2020; Fenelon et al. 2018; Keene and Ruel 2013). In this study, we find that housing choice vouchers provide clear benefits in school attendance, whereas benefits associated with project-based assistance are not statistically significant. However, this difference may reflect limited statistical power for project-based housing because coefficients are in the same direction as those for vouchers, and an interaction was not significant. Overall, this finding contrasts with the expectation that vouchers might lead to increased absences if students are forced to change schools following a move (Cunningham and MacDonald 2012). Children in the pseudo-waitlist group may also experience frequent moves and “residential churn” in the absence of rental assistance (Coulton et al. 2009), or it may be that our measure of missed school days due to illness does not capture these types of absences. Furthermore, past studies distinguishing the effects of project-based housing and vouchers on outcomes related to education have found few differences (DeLuca and Rosenblatt 2010; Jacob et al. 2015; Newman and Harkness 2000; Sanbonmatsu et al. 2006). Although voucher recipients tend to live in less disadvantaged neighborhoods than project-based housing residents (Fenelon et al. 2018), evidence that vouchers offer children access to better schools has been mixed (DeLuca and Rosenblatt 2010; Deng 2007; Ellen et al. 2016; Horn et al. 2014). Finally, the affordability benefits provided by rental assistance, whether in the form of project-based assistance or vouchers, may be what drives effects on the lives of children and families (Newman and Holupka 2017a, 2020).
Our results uncover notable racial/ethnic differences in the effects of rental assistance. The beneficial effects of rental assistance for school attendance are most pronounced among adolescents and non-Hispanic White children and Latino children, and they are minimal among Black children. The health and schooling benefits of rental assistance programs suggest that underinvestment in affordable housing may impede socioeconomic mobility among disadvantaged White and Hispanic/Latino children. However, the lack of a benefit for disadvantaged Black children is more concerning because it indicates that the housing affordability and stability benefits of rental assistance do not translate into better school attendance for them as they do for White and Latino children. This finding may suggest that structural racism limits the ability of Black families to capitalize on the nonhousing advantages of rental assistance that White families receive, consistent with the diminished returns hypothesis (Assari 2018b; Williams and Collins 1995). Similarly, vouchers may provide White children with greater access to better schools, whereas Black voucher holders experience higher segregation levels (de Souza Briggs 1998). Although recent evidence showed no significant Black-White differences in the quality of project-based housing (Newman and Holupka 2017b), Black families may live in poorer-quality voucher units or in more disadvantaged neighborhoods, which may limit the health and schooling benefits (Rohe and Freeman 2001). The racial/ethnic difference implies that increased investment in rental assistance may widen racial/ethnic disparities in health and schooling among disadvantaged children, and future research should examine why this benefit is not evident for Black children.
We find that the effect of rental assistance on missed school days due to illness is stronger for adolescents than for younger children. This finding may indicate that adolescent health is more responsive than younger child health to changes in housing conditions or that increased housing stability is more important for adolescents’ management of conditions such as asthma (Schmidt et al. 2014). This finding may also reflect greater duration of rental assistance if adolescents have lived in assisted housing for longer periods than younger children.
Limitations
Although our study makes several novel contributions, it has some limitations. First, we cannot examine changes in school attendance within children over time and instead compare children who differ only in whether they have yet entered HUD housing.
Second, our analytical approach does not involve random assignment, and concurrent changes that are associated with our outcomes (e.g., policy changes related to the supply of housing) may occur alongside entry into rental assistance. Models that control for state of residence to adjust for possible geographic differences in the length of the actual waitlist or in the potential dollar value of housing vouchers (Collinson and Ganong 2018) produce nearly identical results (shown in section B of the online appendix). Additionally, the results of the event study analysis (Figure 1) do not indicate significant changes in missed school days before entering rental assistance.
Third, PHAs may exercise discretion over waitlist priority and may reduce wait times for particularly disadvantaged families (e.g., single parents with children, the homeless, persons with disabilities). To the extent that greater disadvantage is associated with shorter wait times, we may be more likely to observe these families in the current assistance group, which could potentially attenuate any positive effects of rental assistance that we observe.
Fourth, our primary outcome refers to missed school days over the prior year and thus does not correspond exactly to rental assistance status at interview. Our finding in Figure 1 that the coefficient for those in rental assistance for less than one year does not significantly differ from greater durations provides some assurance that this does not bias our results. Models removing children in rental assistance less than one year (section H, online appendix) produce highly similar results. The missed school days due to illness outcomes are also parent-reported and are thus potentially subject to recall bias and social desirability bias. Our finding that missed school days due to illness are correlated with parent-reported child health problems (see Table 5) provides some validity to the parent-reported number. However, the outcome includes only those missed school days that are due to illness or injury and thus does not capture other reasons that children miss school.
Finally, we cannot consider other potential mediators of the relationship between rental assistance and school attendance, including housing quality, exposure to crime, and parenting behaviors. Future work should explore additional mechanisms.
Conclusion
During the Great Recession and mortgage crisis of 2008–2010 and in the years following, the number of rent-burdened U.S. families has grown considerably (Joint Center for Housing Studies 2018), although the difficulty of many families in affording rental housing has been building for at least the last three decades (Joint Center for Housing Studies 2020). Current government policy solutions designed to improve the affordabilty of housing have not been sufficient to curb the tide of the rental crisis. A significant shortfall in the number of subsidized housing units has left roughly 30 million families in need of rental assistance support but unable to receive it (Center on Budget and Policy Priorities 2017). Our findings suggest that the societal underinvestment in affordable housing also likely leads to wider socioeconomic and differences in childhood health among non-Hispanic White and Latino children, which may have implications for longer-term educational outcomes. However, the lack of a school attendance benefit for disadvantaged Black children receiving rental assistance presents another pressing policy problem. If this difference holds, an expansion of rental assistance resources may exacerbate an already sizable racial gap in school outcomes and educational attainment if we do not identify and address the root cause of these differential returns on housing. Unintended effects of social policies on health and economic disparities are important puzzles for population health researchers and policymakers aiming to reduce inequality (Thomson et al. 2018). Thus, future work examining the mechanisms that link rental assistance programs to childhood health and educational outcomes is crucial if we are to identify the reasons for the pronounced racial/ethnic differences in the benefits of rental assistance. A broader understanding of the relationship between access to affordable housing and child outcomes can inform federal funding decisions for HUD rental assistance programs and has implications for scholars studying inequalities in child well-being.
Supplementary Material
Acknowledgments
We are grateful to affiliates of the Hopkins Population Center, Maryland Population Research Center, and Cornell Population Center for helpful comments. Work for this project was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R21-HD095329-01A1). We acknowledge institutional support from the Maryland Population Research Center (P2C-HD041041) and the Population Research Institute (P2C-HD041025).
Footnotes
There are currently more than 3,000 PHAs across the United States.
PHAs may receive funds from sources other than HUD (e.g., foundation grants, other federal agencies), but their primary operating and capital budgets are funded by HUD.
Affordable housing units provided through the Low-Income Housing Tax Credit, a U.S. Department of the Treasury program, are not included in the current analysis unless they house voucher recipients.
Because the NHIS did not obtain identifiable information (including Social Security numbers) from children in the 2002 and 2003 surveys, no respondents under age 18 are eligible for linkage to the HUD record in these years.
The mean length of waitlists for HUD housing was 26 months in 2018. During our analysis period, the length ranges from 18 to 26 months (HUD 2019b).
Respondents in the pseudo-waitlist category are coded based on the program category corresponding with the first HUD program they enter (e.g., pseudo-waitlist for vouchers).
We report results for zero-inflated negative binomial regression models in section B of the online appendix.
Contributor Information
Andrew Fenelon, School of Public Policy and Department of Sociology and Criminology, Penn State University, University Park, PA, USA.
Michel Boudreaux, Department of Health Policy and Management, University of Maryland, College Park, MD, USA.
Natalie Slopen, Department of Social and Behavioral Sciences, Harvard T. H. Chan School of Public Health, Boston, MA, USA.
Sandra J. Newman, Department of Health Policy & Management, Johns Hopkins University, Baltimore, MD, USA
References
- Associates Abt. (2015). Impacts of housing and services interventions for homeless families. Family Options Study: Highlights from the July 2015 report. Bethesda, MD: Abt Associates. [Google Scholar]
- Acevedo-Garcia D, Osypuk TL, McArdle N, & Williams DR (2008). Toward a policy-relevant analysis of geographic and racial/ethnic disparities in child health. Health Affairs, 27, 321–333. [DOI] [PubMed] [Google Scholar]
- Ahrens KA, Haley BA, Rossen LM, Lloyd PC, & Aoki Y (2016). Housing assistance and blood lead levels: Children in the United States, 2005–2012. American Journal of Public Health, 106, 2049–2056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allensworth E, & Easton J (2007). What matters for staying on-track and graduating in Chicago public high schools (Consortium on Chicago School Research). Retrieved from https://consortium.uchicago.edu/publications/what-matters-staying-track-and-graduating-chicago-public-schools
- Allison MA, & Attisha E (2019). The link between school attendance and good health. Pediatrics, 143, e20183648. 10.1542/peds.2018-3648 [DOI] [PubMed] [Google Scholar]
- Allison P (2012, August 7). Do we really need zero-inflated models? Statistical Horizons. Retrieved from https://statisticalhorizons.com/zero-inflated-models [Google Scholar]
- Andersson F, Haltiwanger JC, Kutzbach MJ, Palloni GE, Pollakowski HO, & Weinberg DH (2016). Childhood housing and adult earnings: A between-siblings analysis of housing vouchers and public housing (NBER Working Paper No. 22721). Cambridge, MA: National Bureau of Economic Research. [Google Scholar]
- Assari S (2018a). Diminished economic return of socioeconomic status for Black families. Social Sciences, 7, 74. 10.3390/SOCSCI7050074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Assari S (2018b). Health disparities due to diminished return among Black Americans: Public policy solutions. Social Issues and Policy Review, 12, 112–145. [Google Scholar]
- Bailie RS, Stevens M, & McDonald EL (2012). The impact of housing improvement and socio-environmental factors on common childhood illnesses: A cohort study in Indigenous Australian communities. Journal of Epidemiology and Community Health, 66, 821–831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck AF, Huang B, Chundur R, & Kahn RS (2014). Housing code violation density associated with emergency department and hospital use by children with asthma. Health Affairs, 33, 1993–2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blewett LA, Rivera Drew JA, Griffin R, King ML, & Williams KCW (2016). National Health Interview Survey, Version 6.2 [Data set]. Minneapolis: University of Minnesota. Retrieved from http://www.nhis.ipums.org [Google Scholar]
- Boudreaux MH, Fenelon A, & Slopen N (2018). Misclassification of rental assistance in the National Health Interview Survey: Evidence and implications. Epidemiology, 29, 716–720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boudreaux MH, Fenelon A, Slopen N, & Newman SJ (2020). Association of childhood asthma with federal rental assistance. JAMA Pediatrics, 174, 592–598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson D, Miller H, Haveman R, Kang S, Schmidt A, & Wolfe B (2019). The effect of housing assistance on student achievement: Evidence from Wisconsin. Journal of Housing Economics, 44, 61–73. [Google Scholar]
- Center on Budget and Policy Priorities. (2017). Fact sheet: Federal Rental Assistance. Washington, DC: Center on Budget and Policy Priorities. Retrieved from http://www.cbpp.org/sites/default/files/atoms/files/4-13-11hous-US.pdf [Google Scholar]
- Chetty R, Hendren N, & Katz LF (2016). The effects of exposure to better neighborhoods on children: New evidence from the Moving to Opportunity experiment. American Economic Review, 106, 855–902. [DOI] [PubMed] [Google Scholar]
- Chyn E (2018). Moved to opportunity: The long-run effects of public housing demolition on children. American Economic Review, 108, 3028–3056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Classi P, Milton D, Ward S, Sarsour K, & Johnston J (2012). Social and emotional difficulties in children with ADHD and the impact on school attendance and healthcare utilization. Child and Adolescent Psychiatry and Mental Health, 6, 33. 10.1186/1753-2000-6-33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collinson R, & Ganong P (2018). How do changes in housing voucher design affect rent and neighborhood quality? American Economic Journal: Economic Policy, 10(2), 62–89. [Google Scholar]
- Coulton C, Theodos B, & Turner MA (2009). Family mobility and neighborhood change: New evidence and implications for community initiatives (Report). Washington, DC: Urban Institute. Retrieved from https://www.urban.org/research/publication/family-mobility-and-neighborhood-change [Google Scholar]
- Cunningham M, & MacDonald G (2012). Housing as a platform for improving education outcomes among low-income children (WhatWorks Collaborative report). Washington, DC: Urban Institute. Retrieved from https://www.urban.org/research/publication/housing-platform-improving-education-outcomes-among-low-income-children [Google Scholar]
- Currie J, & Yelowitz A (2000). Are public housing projects good for kids? Journal of Public Economics, 75, 99–124. [Google Scholar]
- DeLuca S, Garboden PME, & Rosenblatt P (2013). Segregating shelter: How housing policies shape the residential locations of low-income minority families. Annals of the American Academy of Political and Social Science, 647, 268–299. [Google Scholar]
- DeLuca S, & Rosenblatt P (2010). Does moving to better neighborhoods lead to better schooling opportunities? Parental school choice in an experimental housing voucher program. Teachers College Record, 112, 1443–1491. [Google Scholar]
- Deng L (2007). Comparing the effects of housing vouchers and low-income housing tax credits on neighborhood integration and school quality. Journal of Planning Education and Research, 27, 20–35. [Google Scholar]
- de Souza Briggs X (1998). Brown kids in White suburbs: Housing mobility and the many faces of social capital. Housing Policy Debate, 9, 177–221. [Google Scholar]
- Dupere V, Leventhal T, Crosnoe R, & Dion E (2010). Understanding the positive role of neighborhood socioeconomic advantage in achievement: The contribution of the home, child care, and school environments. Developmental Psychology, 46, 1227–1244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellen IG, Horn KM, & Schwartz AE (2016). Why don’t housing choice voucher recipients live near better schools? Insights from Big Data. Journal of Policy Analysis and Management, 35, 884–905. [Google Scholar]
- Elwert F, & Pfeffer FT (2019). The future strikes back: Using future treatments to detect and reduce hidden bias. Sociological Methods & Research. Advance online publication. 10.1177/0049124119875958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fenelon A, Mayne P, Simon AE, Rossen LM, Helms V, Lloyd P, … Steffen BL (2017). Housing assistance programs and adult health in the United States. American Journal of Public Health, 107, 571–578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fenelon A, Slopen N, Boudreaux MH, & Newman SJ (2018). The impact of housing assistance on the mental health of children in the United States. Journal of Health and Social Behavior, 59, 447–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fertig AR, & Reingold DA (2007). Public housing, health, and health behaviors: Is there a connection? Journal of Policy Analysis and Management, 26, 831–860. [DOI] [PubMed] [Google Scholar]
- Fischer W (2015). Research shows housing vouchers reduce hardship and provide platform for long-term gains among children (Report). Washington, DC: Center on Budget and Policy Priorities. Retrieved from https://www.cbpp.org/research/housing/research-shows-housing-vouchers-reduce-hardship-and-provide-platform-for-long-term [Google Scholar]
- Foster AC, & Rojas A (2018). Program participation and spending patterns of families receiving government means-tested assistance. Monthly Labor Review, 2018(1), 1–22. [Google Scholar]
- Gottfried MA (2011). The detrimental effects of missing school: Evidence from urban siblings. American Journal of Education, 117, 147–182. [Google Scholar]
- Gubits D, Shinn M, Wood M, Brown SR, Dastrup SR, & Bell SH (2018). What interventions work best for families who experience homelessness? Impact estimates from the Family Options Study. Journal of Policy Analysis and Management, 37, 835–866. [PMC free article] [PubMed] [Google Scholar]
- Helms VE, Sperling J, & Steffen BL (2017). A health picture of HUD-assisted adults, 2006–2012 (Report). Washington, DC: U.S. Department of Housing and Urban Development. Retrieved from https://www.huduser.gov/portal/publications/Health-Picture-of-HUD.html [Google Scholar]
- Helms VE, Steffen BL, Rudd E, & Sperling J (2018). A health picture of HUD-assisted children, 2006–2012 (Report). Retrieved from https://www.huduser.gov/portal/publications/Health-Picture-of-HUD-Assisted-Children.html
- Horn KM, Ellen IG, & Schwartz AE (2014). Do housing choice voucher holders live near good schools? Journal of Housing Economics, 23, 28–40. [Google Scholar]
- Hughes HK, Matsui EC, Tschudy MM, Pollack CE, & Keet CA (2017). Pediatric asthma health disparities: Race, hardship, housing, and asthma in a national survey. Academic Pediatrics, 17, 127–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson MI (2009). Understanding links between adolescent health and educational attainment. Demography, 46, 671–694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacob BA (2004). Public housing, housing vouchers, and student achievement: Evidence from public housing demolitions in Chicago. American Economic Review, 94(1), 233–258. [Google Scholar]
- Jacob BA, Kapustin M, & Ludwig J (2015). The impact of housing assistance on child outcomes: Evidence from a randomized housing lottery. Quarterly Journal of Economics, 130, 465–506. [Google Scholar]
- Joint Center for Housing Studies. (2020). The state of the nation’s housing: 2020 (Report). Cambridge, MA: Joint Center For Housing Studies of Harvard University. Retrieved from https://www.jchs.harvard.edu/sites/default/files/reports/files/Harvard_JCHS_The_State_of_the_Nations_Housing_2020_Report_Revised_120720.pdf [Google Scholar]
- Keene DE, Guo M, & Murillo S (2018). “That wasn’t really a place to worry about diabetes”: Housing access and diabetes self-management among low-income adults. Social Science & Medicine, 197, 71–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keene DE, Niccolai L, Rosenberg A, Schlesinger P, & Blankenship KM (2020). Rental assistance and adult self-rated health. Journal of Health Care for the Poor and Underserved, 31, 325–339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keene DE, & Ruel E (2013). “Everyone called me grandma”: Public housing demolition and relocation among older adults in Atlanta. Cities, 35, 359–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kleit RG, Kang S, & Scally CP (2016). Why do housing mobility programs fail in moving households to better neighborhoods? Housing Policy Debate, 26, 188–209. [Google Scholar]
- Kucheva Y (2018). Subsidized housing and the transition to adulthood. Demography, 55, 617–642. [DOI] [PubMed] [Google Scholar]
- Leventhal T, & Brooks-Gunn J (2000). The neighborhoods they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychological Bulletin, 126, 309–337. [DOI] [PubMed] [Google Scholar]
- Lloyd PC, & Helms VE (2016). NCHS-HUD linked data: Analytic considerations and guidelines (Report). Hyattsville, MD: Office of Analysis and Epidemiology, National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/data/datalinkage/nchs_hud_analytic_considerations.pdf [Google Scholar]
- Lloyd PC, Helms VE, & Simon AE (2017). Linkage of 1999–2012 National Health Interview Survey and National Health and Nutrition Examination Survey data to U.S. Department of Housing and Urban Development administrative records (Vital and Health Statistics, Series 1, No. 60). Washington, DC: National Center for Health Statistics, U.S. Department of Health and Human Services. Retrieved from https://www.huduser.gov/portal/sites/default/files/pdf/Vital-and-Health-Statistics.pdf [PubMed] [Google Scholar]
- Long JS (1997). Regression models for categorical and limited dependent variables. Thousand Oaks, CA: Sage Publications. [Google Scholar]
- Ma CT, Gee L, & Kushel MB (2008). Associations between housing instability and food insecurity with health care access in low-income children. Ambulatory Pediatrics, 8, 50–57. [DOI] [PubMed] [Google Scholar]
- Matte TD, & Jacobs DE (2000). Housing and health—Current issues and implications for research and programs. Journal of Urban Health, 77, 7–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCabe B (2017, November). Waitlists and preferences: Understanding how public housing authorities administer the Housing Choice Voucher Program. Paper presented at the 39th annual research conference of the Association for Public Policy Analysis and Management, Chicago, IL. [Google Scholar]
- McCormack MC, Breysse PN, Matsui EC, Hansel NN, Williams D, Curtin-Brosnan J, … Diette GB (2009). In-home particle concentrations and childhood asthma morbidity. Environmental Health Perspectives, 117, 294–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore MK (2017, November). Getting in line for a housing choice voucher: Waitlist opening dynamics across the US. Paper presented at the Fall Research Conference of the Association for Public Policy Analysis & Management, Chicago, IL. [Google Scholar]
- Newman SJ, & Harkness J (2000). Assisted housing and the educational attainment of children. Journal of Housing Economics, 9, 40–63. [Google Scholar]
- Newman SJ, & Harkness JM (2002). The long–term effects of public housing on self–sufficiency. Journal of Policy Analysis and Management, 21, 21—43. [Google Scholar]
- Newman SJ, & Holupka CS (2014). Housing affordability and investments in children. Journal of Housing Economics, 24, 89–100. [Google Scholar]
- Newman SJ, & Holupka CS (2016). Housing affordability and children’s cognitive achievement. Health Affairs, 35, 2092–2099. [DOI] [PubMed] [Google Scholar]
- Newman SJ, & Holupka CS (2017a). The effects of assisted housing on child well-being. American Journal of Community Psychology, 60, 66–78. [DOI] [PubMed] [Google Scholar]
- Newman SJ, & Holupka CS (2017b). Race and assisted housing. Housing Policy Debate, 27, 751–771. [Google Scholar]
- Newman SJ, & Holupka CS (2020). The effects of assisted housing on children’s healthy development (Working paper). Baltimore, MD: Johns Hopkins Bloomberg School of Public Health, Center on Housing, Neighborhoods and Communities. [Google Scholar]
- Newman SJ, Holupka CS, & Harkness J (2009). The long-term effects of housing assistance on work and welfare. Journal of Policy Analysis and Management, 28, 81–101. [Google Scholar]
- Nguyen QC, Rehkopf DH, Schmidt NM, & Osypuk TL (2016). Heterogeneous effects of housing vouchers on the mental health of US adolescents. American Journal of Public Health, 106, 755–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollack CE, Pollack CE, Blackford AL, Du S, Deluca S, Thornton RLJ, & Herring B (2019). Association of receipt of a housing voucher with subsequent hospital utilization and spending. JAMA, 322, 2115–2124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rauh VA, Landrigan PJ, & Claudio L (2008). Housing and health. Annals of the New York Academy of Sciences, 1136, 276–288. [DOI] [PubMed] [Google Scholar]
- Rohe WM, & Freeman L (2001). Assisted housing and residential segregation: The role of race and ethnicity in the siting of assisted housing developments. Journal of the American Planning Association, 67, 279–292. [Google Scholar]
- Sadowski LS, Kee RA, Vanderweele TJ, & Buchanan D (2009). Effect of a housing and case management program on emergency department visits and hospitalizations among chronically ill homeless adults: A randomized trial. JAMA, 301, 1771–1778. [DOI] [PubMed] [Google Scholar]
- Sanbonmatsu L, Kling JR, Duncan GJ, & Brooks-Gunn J (2006). Neighborhoods and academic achievement results from the Moving to Opportunity experiment. Journal of Human Resources, 41, 649–691. [Google Scholar]
- Sandel M, Sheward R, de Cuba SE, Coleman SM, Frank DA, Chilton M, … Cutts D (2018). Unstable housing and caregiver and child health in renter families. Pediatrics, 141, e20172199. 10.1542/peds.2017-2199 [DOI] [PubMed] [Google Scholar]
- Sandel M, & Wright RJ (2006). When home is where the stress is: Expanding the dimensions of housing that influence asthma morbidity. Archives of Disease in Childhood, 91, 942–948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt NM, Glymour MM, & Osypuk TL (2017). Adolescence is a sensitive period for housing mobility to influence risky behaviors: An experimental design. Journal of Adolescent Health, 60, 431–437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt NM, Lincoln AK, Nguyen QC, Acevedo-Garcia D, & Osypuk TL (2014). Examining mediators of housing mobility on adolescent asthma: Results from a housing voucher experiment. Social Science & Medicine, 107, 136–144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz AE, Horn KM, Ellen IG, & Cordes SA (2020). Do housing vouchers improve academic performance? Evidence from New York City. Journal of Policy Analysis and Management, 39, 131–158. [Google Scholar]
- Sharfstein J, Sandel M, Kahn R, & Bauchner H (2001). Is child health at risk while families wait for housing vouchers? American Journal of Public Health, 91, 1191–1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shroder M, & Martin M (1996). New results from administrative data: Housing the poor, or, what they don’t know might hurt somebody. Washington, DC: U.S. Department of Housing and Urban Development, Office of Policy Development and Research. [Google Scholar]
- Simon AE, Fenelon A, Helms V, Lloyd PC, & Rossen LM (2017). HUD housing assistance associated with lower uninsurance rates and unmet medical need. Health Affairs, 36, 1016–1023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slopen N, Fenelon A, Newman SJ, & Boudreaux MH (2018). Housing assistance and child health in the United States: A systematic review. Pediatrics, 141, e20172742. 10.1542/peds.2017-2742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith NL, Smith TJ, DeSantis D, Suhocki M, & Fenske D (2015). Vision problems in homeless children. Journal of Health Care for the Poor and Underserved, 26, 761–770. [DOI] [PubMed] [Google Scholar]
- Snedker KA, Herting JR, & Walton E (2009). Contextual effects and adolescent substance use: Exploring the role of neighborhoods. Social Science Quarterly, 90, 1272–1297. [Google Scholar]
- Swope CB, & Hernández D (2019). Housing as a determinant of health equity: A conceptual model. Social Science & Medicine, 243, 112571. 10.1016/j.socscimed.2019.112571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomson K, Hillier-Brown F, Todd A, McNamara C, Huijts T, & Bambra C (2018). The effects of public health policies on health inequalities in high-income countries: An umbrella review. BMC Public Health, 18, 869. 10.1186/s12889-018-5677-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Housing and Urban Development (HUD). (2019a). Worst case housing needs: 2019 report to Congress. Retrieved from https://www.huduser.gov/portal/publications/worst-case-housing-needs-2020.html
- U.S. Department of Housing and Urban Development (HUD). (2019b). Assisted housing: National and local: Picture of subsidized households [Data set]. Washington, DC: U.S. Department of Housing and Urban Development. Retrieved from https://www.huduser.gov/portal/datasets/assthsg.html [Google Scholar]
- Wang K, & Immergluck D (2018). The geography of vacant housing and neighborhood health disparities after the U.S. foreclosure crisis. Cityscape, 20(2), 145–170. [Google Scholar]
- Warren EJ, & Font SA (2015). Housing insecurity, maternal stress, and child maltreatment: An application of the family stress model. Social Service Review, 89, 9–39. [Google Scholar]
- Williams DR, & Collins C (1995). US socioeconomic and racial differences in health: Patterns and explanations. Annual Review of Sociology, 21, 349–386. [Google Scholar]
- Williams DR, Mohammed SA, Leavell J, & Collins C (2010). Race, socioeconomic status, and health: Complexities, ongoing challenges, and research opportunities. Annals of the New York Academy of Sciences, 1186, 69–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wodtke GT (2013). Duration and timing of exposure to neighborhood poverty and the risk of adolescent parenthood. Demography, 50, 1765–1788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong MS, Roberts ET, Arnold CM, & Pollack CE (2018). HUD housing assistance and levels of physical activity among low-income adults. Preventing Chronic Disease, 15, 170517. Retrieved from https://www.cdc.gov/pcd/issues/2018/17_0517.htm#1 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.