

Summary
Viral hepatitis is one of the major infectious diseases in Japan and causes liver cirrhosis and liver cancer. Therefore, screening for hepatitis viruses was started in 2002, based on the geriatric health care program. The screening plan has now been transferred to the Health Promotion Project and it is estimated that more than half of the population has been tested for hepatitis viruses. The Basic Act on Hepatitis Measures was enacted in 2009 and the Basic Guidelines for Promotion of Control Measures for hepatitis was issued in 2011. It reported that there were about 770,000 positive people who were unaware that they were infected, and about 0.5 to 1.2 million positive people who knew they were infected but did not continue to receive medical examinations. Ten years have passed since that report and it is estimated that the number of hepatitis virus-positive individuals who need medical examination/treatment is decreasing. Therefore, in order to eradicate viral hepatitis, it is essential to identify areas and age groups in which hepatitis virus testing is inadequate, to encourage people to undergo testing and to promptly send positive patients to hepatologists for continued medical care. This review describes the current status and challenges of hepatitis virus testing measures in Japan, led by the Ministry of Health, Labour and Welfare, and the promotion of visits to medical institutions by positive patients.
Keywords: hepatitis screening test in Japan, follow-up of individuals positive for viral hepatitis, Basic Act on Hepatitis Measures, hepatitis B surface antigen, hepatitis C virus antibody
Introduction
Tests for hepatitis viruses as part of the milestone checkups of the Health Care for Elderly Service began in Japan in 2002. The liver cancer mortality rate in Japan has fallen steadily because of measures such as the establishment of the Basic Act on Hepatitis Measures (1) and Basic Guidelines for Promotion of Control Measures for Hepatitis (2), the Hepatitis Information Center, the establishment of regional core centers (3,4), and subsidization of interferon treatment for hepatitis C virus (HCV). On the other hand, it is estimated that there are about 770,000 individuals who do not know they are persistently infected with hepatitis B virus (HBV) or HCV because they have not yet undergone screening, and about 0.5 to 1.2 million positive individuals who know they are infected but do not continue to visit a hospital care (5,6).
According to a report in 2011(7), the preferred option for hepatitis virus testing was free screening at public health centers, but this had a very low uptake rate of about 6%, because the testing days were limited to one or two per month. Only a further 17.1% were tested for hepatitis viruses in checkups at their workplaces. Many workers have taken mandatory health examinations which did not include screening for viral hepatitis. As a result, they are unwilling to visit a public health center solely for viral hepatitis screening.
On the other hand, 25% of the respondents were tested for hepatitis viruses in hospitals and clinics, the majority (49%) of whom were tested as part of pre-surgery examinations. However, hepatitis virus-positive individuals may not be directed to consultation/treatment because of a lack of awareness by non-specialist doctors and a lack of intra-hospital cooperation.
Considering that the treatments for HBV and HCV infections are now oral antiviral drugs with almost no adverse reactions, new measures are urgently needed for positive patients who do not currently receive medical examinations or treatment.
Current status and issues of viral hepatitis testing through local governments
Hepatitis virus screening was available for individuals between the ages of 40 and 70 for five years from 2002 under the Health Care for Elderly Service, at 5-year intervals (milestone checkup), with additional screening available for those with abnormal liver function, extensive surgical procedures, or a history of heavy bleeding (out with the milestone checkups). As a result, about 87 million people were tested for hepatitis B surface antigen (HBsAg) and HCV antibody (anti-HCV) and about 200,000 positive cases were discovered (Table 1). However, uptake of testing by eligible subjects was only 27% among the recipients of milestone checkups. One of the reasons for the lack of increase in the screening rate was the variable efforts made by local governments. In addition, it is assumed that only National Health Insurance subscribers were eligible to take the test.
Table 1. Number of viral hepatitis screening tests and positive rates from 2002-2006, under the geriatric health care program.
| (a) Hepatitis B surface antigen (HBsAg) | |||||||
|---|---|---|---|---|---|---|---|
| Milestone checkup |
Out of milestone checkup |
Total |
|||||
| Number of tests | Number of positive | Number of tests | Number of positive | Number of tests | Number of positive | Positive rate | |
| FY2002 | 1,291,195 | 15,239 | 631,918 | 9,191 | 1,923,113 | 24,430 | 1.27% |
| FY2003 | 1,382,663 | 15,842 | 466,462 | 6,678 | 1,849,125 | 22,520 | 1.22% |
| FT2004 | 1,279,704 | 13,950 | 356,230 | 4,804 | 1,635,934 | 18,754 | 1.15% |
| FY2005 | 1,205,423 | 12,735 | 341,400 | 4,395 | 1,546,823 | 17,130 | 1.11% |
| FY2006 | 1,145,291 | 11,742 | 604,301 | 6,407 | 1,749,592 | 18,149 | 1.04% |
| total | 6,304,276 | 69,508 | 2,400,311 | 45,207 | 8,704,587 | 100,983 | 1.16% |
| (b) HCV antibody (anti-HCV) | |||||||
| Milestone checkup |
Out of milestone checkup |
Total |
|||||
| Number of tests | Number of positive | Number of tests | Number of positive | Number of tests | Number of positive | Positive rate | |
| FY2002 | 1,298,746 | 14,672 | 624,734 | 16,721 | 1,923,480 | 31,393 | 1.63% |
| FY2003 | 1,375,583 | 13,324 | 454,687 | 10,167 | 1,830,270 | 23,491 | 1.28% |
| FT2004 | 1,271,320 | 10,385 | 347,431 | 6,446 | 1,618,751 | 16,831 | 1.04% |
| FY2005 | 1,196,457 | 8,909 | 331,356 | 5,067 | 1,527,813 | 13,976 | 0.91% |
| FY2006 | 1,138,005 | 7,453 | 596,190 | 6,806 | 1,734,195 | 14,259 | 0.82% |
| total | 6,280,111 | 54,743 | 2,354,398 | 45,207 | 8,634,509 | 99,950 | 1.16% |
Milestone checkup: between the ages of 40 and 70 at 5-year intervals. Out of milestone checkup: abnormal liver function and history of extensive surgical procedures or heavy bleeding.
In 2008, the testing program was taken over by the Health Promotion Service. Many local governments provide opportunities for hepatitis virus testing at the same time as specific medical examinations and cancer screening, for greater convenience. However, most workers did not receive a checkup, even when they received a "Notice of Hepatitis Virus Screening with the annual checkup" from the municipal authorities, because they had health examinations provided by their employers. Individuals of working age rarely took advantage of this program by taking tests for hepatitis viruses.
In order to cope with this situation, in 2008, as an urgent hepatitis virus testing service (specific infectious disease testing service), prefectures, government-ordinance-designated cities, core cities, etc., in cooperation with medical associations, selected medical institutions for commissioned testing, so that testing was more widely available for those who were not able to receive medical checkups conducted under the Health Care for Elderly Service (or Health Promotion Service) from 2008. As a result, about 300,000 people are currently being tested every year as part of the specific infectious disease testing program. From 2010 to 2017, about 10 million people were tested by the projects, and the positive rates in 2017 were 0.64% for HBV and 0.33% for HCV (8) (Figure 1).
Figure 1.
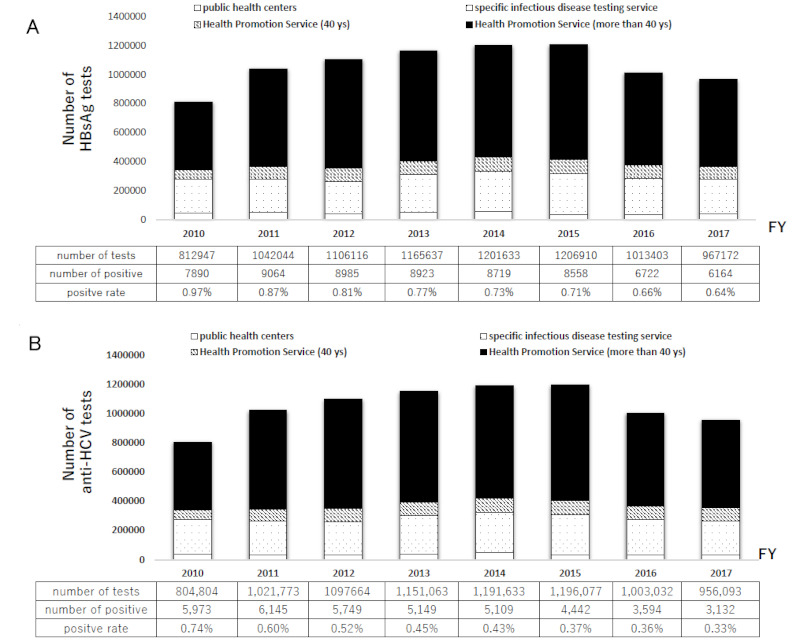
Number of viral hepatitis screening and positive rate from 2010-2017 under urgent hepatitis virus testing project and Health Promotion Project. (A) HBsAg, (B) anti-HCV.
It is not clear how many of those found to be positive for HBV or HCV have been followed up with examinations and hospital treatment. Originally, the purpose of hepatitis virus screening by the Health Promotion Service was stated to be "to spread correct knowledge about the hepatitis viruses and promote medical examinations for hepatitis viruses, so that individuals can recognize their own hepatitis virus infection status, receive health guidance as necessary, and visit medical institutions to avoid health problems caused by hepatitis, reduce symptoms, or delay the progression of the disease". At a time when the number of positive cases is declining, it is of utmost importance that the hepatitis virus screening program not only promotes testing but also directs those found to be positive to medical institutions and monitors their numbers.
Furthermore, if the prefectural government takes the lead in conducting hepatitis virus testing, it will retain the personal information of those who test positive. Because the prefectures are also the main implementers of the subsidies for hepatitis virus testing and treatment, which are unique to Japan, it is easy to monitor the status of positive patients receiving medical examinations and treatment. On the other hand, the burden of examination costs in prefectures is higher than that of hepatitis virus examinations by the Health Promotion Service, and the number of tests conducted by prefectural governments is only 50,000, with Saga, Yamaguchi, and Osaka prefectures accounting for more than 50% of the total (Figure 2). Osaka prefecture is actively confirming the diagnosis of positive patients, and the consultation rate shows that more than 60% are followed up (9).
Figure 2.
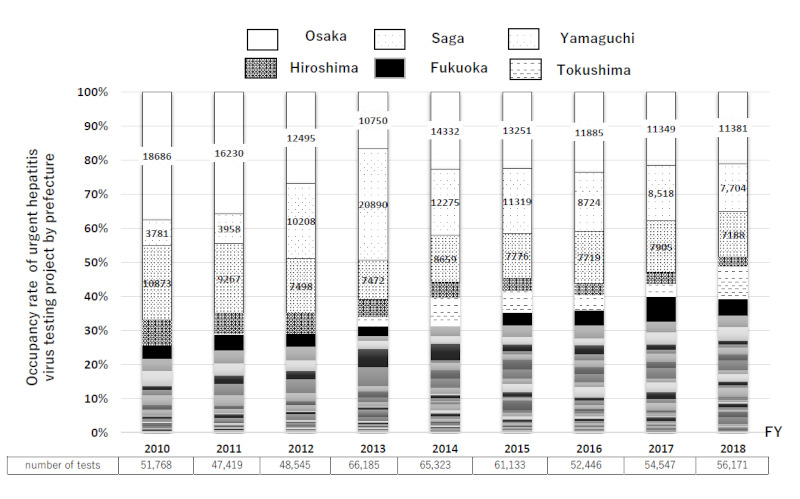
Occupancy rate of urgent hepatitis virus testing project by prefecture from 2010-2018. White column is Osaka prefecture, wide dots in column is Saga prefecture, and narrow dots in column is Yamaguchi prefecture. These three prefectures account for more than 50% of the total.
The Severe Disease Prevention (Follow up) Project for people who test positive for viral hepatitis, through local governments
In the Severe Disease Prevention Project, which started in April 2014, the prefectural government or other authority, after obtaining the consent of the individual, confirms the status of visits to medical institutions and medical treatment by sending a survey sheet once a year and, if the individual has not yet visited a hospital, recommends that the individual visits a specialist and receives medical consultation by telephone or other means (=Follow-up). If an individual is found to be positive for a hepatitis virus and consents to undergo follow-up, with a detailed examination by a specialist designated by the prefectural government within one year of the positive result, the cost of the examination, about 8,000 yen, will be reimbursed (subsidy for the initial detailed examination). In addition, if patients with viral hepatitis were diagnosed with chronic hepatitis or cirrhosis, or post-elimination of HCV following anti- HCV treatment, their medical expenses will be partially reduced twice a year after obtaining the consent of the individual (subsidy for periodic examinations). Recently, the subsidy for the initial detailed examination is being extended, not only to those who are positive for hepatitis virus tests in local governments, but also to those who are found positive at workplace check-ups, preoperative examinations, and prenatal checkups (3,10). Through these subsidy programs, efforts are being made to encourage people to visit specialized medical institutions and to encourage those who are positive to continue to receive examinations; however, the number of first-time specialist examinations and subsidized periodic examinations has been static nationwide.
The situations of local governments with a high consent rate are as follows: i) Advice is given to the patient at the time of hepatitis screening that all applicants should see a specialist in the case of a positive result (consent is obtained before screening, as in Osaka); ii) A physician from the medical institutions for commissioned testing, who is familiar with the provisions of the subsidy system, explains that system to the patient at the time of confirmation of a positive test; and iii) Public health nurses responsible for hepatitis in local areas contact the positive person, as soon as possible after confirmation of the positive result, and visit that person's home or interview him/her at the hepatitis countermeasure department to provide advice.
If the number of positive patients is about ten per year, it is possible to use measure iii. However, if the number of positives is much higher or there is no public health nurse, the burden on the person in charge is heavy and it is better to obtain consent at the time of examination (i and ii). Starting in 2018, the Ministry of Health, Labour and Welfare has also been promoting the follow-up consent for hepatitis virus testing.
Current status and issues of viral hepatitis in the workplace
Although about 20 million community residents have been provided with an opportunity to undergo HBsAg and anti-HCV testing, actions against hepatitis in the workplace in Japan have not yet been fully implemented, and the prevalence of hepatitis virus infections in the workplace remains unknown. Individuals in "the workplace" are non-national insurance subscribers, broadly speaking, who are members of the Japan Health Insurance Association (JHIA) and Union Health Insurance (UHI). The government does not subsidize screening of general workers for viral hepatitis, and the coverage of screening is at the discretion of each health insurance union and company. It would be beneficial if hepatitis virus screening could be conducted by local governments at the time of workplace checkups, but this is not possible in conjunction with the Health Promotion Service. Consequently, it was thought that the hepatitis virus testing system is not sufficiently widespread in the workplace.
We investigated institutions that conducted health screenings in the FY 2016 and reported examination rates of 7.8% and 4.9% for HBsAg and anti-HCV, respectively, in the health insurance association for hepatitis virus testing during workplace checkups in the UHI (11). In this survey, there were many people who are examined every year in same Health Administration Center, and it was revealed that about 70% of the respondents underwent hepatitis screening every year over three years, regardless of whether the test was negative or positive. These results suggest that there remain many UHI members who have not yet been tested.
On the other hand, since 2008 the JHIA has been offering hepatitis virus tests at a partial cost to those who are insured but have never been tested for the viruses. As of 2018, about 19 million people over the age of 40 were insured (12). To date, about two million people have taken the test (Table 2) but, in addition to the fact that less than 10% of subscribers have taken the test, the annual rate in recent years has been as low as 1 to 2%. The JIHA is Japan's largest health insurer and covers the healthcare costs of workers for many small to medium-sized companies in Japan, therefore, there is an urgent need to promote hepatitis virus screening at the JHIA.
Table 2. Number of viral hepatitis screening tests in the Japan Health insurance from 2008-2018.
| Year | The number of hepatitis virus screening recipients | The cumulative number of hepatitis virus screening recipients |
|---|---|---|
| 2008 | 253,840 | 253,840 |
| 2009 | 203,213 | 457,053 |
| 2010 | 194,268 | 651,321 |
| 2011 | 167,451 | 818,772 |
| 2012 | 156,364 | 975,136 |
| 2013 | 147,734 | 1,122,870 |
| 2014 | 143,916 | 1,266,786 |
| 2015 | 146,077 | 1,412,863 |
| 2016 | 137,382 | 1,550,245 |
| 2017 | 205,285 | 1,755,530 |
We simplified the hepatitis virus testing form used by the JHIA using nudge theory, created a leaflet emphasizing the fact that the test can be taken at a reduced cost, and verified the increase of hepatitis virus tests in workplace checkups of JHIA members. In this survey, fully subsidized screening led to the highest hepatitis screening rates, and the leaflet modified using nudge theory significantly increased hepatitis screening uptake at lower costs per person (13). Furthermore, a validation study was conducted at the F branch, which includes about 400,000 people who underwent a workplace checkup in 2017, and the examination rate increased about seven-fold, compared to the previous year (14). The positive rate in F branch was almost the same as the rate from local governments and about 30% of patients positive for anti-HCV were treated with IFN-free direct-acting antivirals. As a result, the Ministry of Health, Labor and Welfare notified insurers and health administration centers to promote hepatitis virus testing during occupational examinations in 2017, (15) and from 2019, the subsidy for the first detailed examination could be used for patients found to be positive from hepatitis virus testing in the workplace (16).
The hepatitis virus tests are non-statutory tests and not included among the mandatory test items for workplace examinations described in Article 66 of the Industrial Safety and Health Act. There is no obligation for business establishments or insurers to add these items. Therefore, when promoting hepatitis virus testing at workplaces, it is desirable to specify which department will manage the results and what recommendations for medical treatment will be made in the event of a positive result. It is critical that results of non-statutory tests are not obtained without the consent of the examinee. Therefore, if the follow-up procedures of a positive test result are not announced before the test, the employer cannot recommend for that person to visit a specialist, even if the result is positive.
It is known that viral hepatitis carriers feel uneasy because they "do not want their workplaces to know about this", so a certain level of consideration must be given to promoting hepatitis virus testing in the workplace.
Viral hepatitis testing before surgery and the consultation status of positive patients
Hepatitis virus testing before surgery is part of routine medical care, as a precautionary measure against infection in hospitals. Nevertheless, not all people who test positive for hepatitis viruses are examined by specialist physicians or receive appropriate treatment. In 2016, the Ministry of Health, Labour and Welfare stated that the results of hepatitis virus tests should be explained to examinees, regardless of the purpose of the test. In addition, they instructed the medical institution (doctor in charge) that conducted the test to refer the patient to a specialist, in the case of a positive result. For this situation, an alert system was developed through an electronic medical record (EMR) order to introduce viral hepatitis-positive individuals to hepatologists, mainly in large hospitals. This system has been reported as useful for promoting appropriate examinations and treatment of individuals with positive results of preoperative and other in-hospital hepatitis virus tests (17,18). However, not all patients with positive hepatitis test results are referred to specialists, solely based on EMR alerts.
We assessed the level of awareness among healthcare professionals about hepatitis virus infection and the electronic medical records alert system and the most common reasons for not referring patients previously were "I had no knowledge and/or interest" and "All I did was explain the results orally" (19).
The doctors who did not respond to the EMR alerts were: i) physicians who were less aware of hepatitis viruses; ii) physicians in departments with more operations and shorter hospital stays (ophthalmology, orthopedics); and iii) physicians with less experience or who were older.
It is thought that more widespread education of healthcare personnel, such as non-specialists and other medical staff, is important to increase the number of individuals receiving appropriate treatment from specialist physicians.
Conclusion
The number of hepatitis virus-positive individuals who need medical examination and treatment is decreasing because viral hepatitis screening by local governments was initiated from 2002. However, when patients received viral hepatitis screening by non-specialist physicians, not all of those with positive hepatitis test results were referred to a specialist.
There are still many patients who are infected with HBV and HCV in workplaces in Japan and promoting hepatitis virus screening for workers at checkups can help detect carriers who are unaware of their infection and require treatment.
Funding: This study was supported financially by the Ministry of Health, Labour and Welfare, Japan (grant number: H26-kansei-ippan-001, H29-kansei-ippan-004).
Conflict of Interest
The authors have no conflicts of interest to disclose.
References
- 1. Ministry of Health, Labour and Welfare. Basic Act on Hepatitis Measures. http://www.japaneselawtranslation.go.jp/law/detail/?id=1995&vm=04&re=01 (accessed May 31, 2021). (in Japanese) .
- 2. Ministry of Health, Labour and Welfare. Basic guidelines for promotion of control measures for hepatitis. http://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou09/pdf/hourei-17e.pdf (accessed May 31, 2021).
- 3. Oza N, Isoda H, Ono T, Kanto T. Current activities and future directions of comprehensive hepatitis control measures in Japan: The supportive role of the Hepatitis Information Center in building a solid foundation. Hepatol Res. 2017; 47:487-496. [DOI] [PubMed] [Google Scholar]
- 4. Setoyama H, Korenaga M, Kitayama Y, Oza N, Masaki N, Kanto T. Nationwide survey on activities of regional core centers for the management of liver disease in Japan: Cumulative analyses by the Hepatitis Information Center 2009-2017. Hepatol Res. 2020; 50:165-173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Tanaka J, Akita T, Ohisa M, Sakamune K, Ko K, Uchida S, Satake M. Trends in the total numbers of HBV and HCV carriers in Japan from 2000 to 2011. J Viral Hepat. 2018; 25:363-372. [DOI] [PubMed] [Google Scholar]
- 6. Tanaka J, Akita T, Ko K, Miura Y, Satake M. Countermeasures against viral hepatitis B and C in Japan: An epidemiological point of view. Hepatol Res. 2019; 49:990-1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ministry of Health, Labor and Welfare. FY2011 hepatitis test examination status. https://www.mhlw.go.jp/stf/houdou/2r9852000002gd4j-att/2r9852000002gd60.pdf (accessed May 31, 2021). (in Japanese) .
- 8. Ministry of Health, Labor and Welfare. About viral hepatitis tests. Available at:. https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou09/hepatitis_kensa.html (accessed May 30, 2021). (in Japanese) .
- 9. Ministry of Health, Labor and Welfare. About 26th Council for Promotion of Hepatitis Measures. https://www.mhlw.go.jp/content/10901000/000781260.pdf (accessed May 20, 2021). (in Japanese) .
- 10. Ministry of Health, Labor and Welfare. About related decree. Released on March 27, 2020. https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou09/pdf/hourei-200327-1.pdf (accessed May 20, 2021). (in Japanese) .
- 11. Tatemichi M, Furuya H, Nagahama S, Takaya N, Shida Y, Fukai K, Owada S, Endo H, Kinoue T, Korenaga M. A nationwide cross-sectional survey on hepatitis B and C screening among workers in Japan. Sci Rep. 2020; 10:11435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Basic information on subscribers and medical fees 2018 in Japan Health Insurance Association. https://www.kyoukaikenpo.or.jp/g7/cat740/sb7200/sbb7204/h30. (accessed May 30, 2021). (in Japanese) .
- 13. Fukuyoshi J, Korenaga M, Yoshii Y, Hong L, Kashihara S, Sigel B, Takebayashi T. Increasing hepatitis virus screening uptake at worksites in Japan using nudge theory and full subsidies. Environ Health Prev Med. 2021; 26:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Korenaga M, Ooe C, Kamimura K, Fukuyoshi J, Ide T, Okada H, Kato F, Mochida S, Inoue T, Akahane T, Kanto T. Tailored message interventions using social marketing approach increase the number of participants in viral hepatitis screening for Japanese workers -multicenter trial of 880,000 general checkup applicants. Hepatology. 2019; 70(Suppl 1):460A. https://aasldpubs.onlinelibrary.wiley.com/doi/epdf/10.1002/hep.30941 (accessed July 17, 2021).
- 15. Ministry of Health, Labor and Welfare. About related decree. Released on May 30, 2017. https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou09/pdf/hourei-170530-1.pdf (accessed May 30, 2021). (in Japanese) .
- 16. Ministry of Health, Labor and Welfare. About related decree. Released on March 27, 2019. https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou09/pdf/hourei-190329-2.pdf (accessed March 27, 2021). (in Japanese) .
- 17. Uchida-Kobayashi S, Enomoto M, Fujii H, et al. Promotion of intra-hospital referral of hepatitis B and C virus carriers to hepatology specialists by electronic medical record-based alert system: a case study at a university hospital. Kanzo. 2016; 57:7-16. (in Japanese with English abstract) [Google Scholar]
- 18. Fujii H, Yamaguchi S, Kurai O, Miyano M, Ueda W, Oba H, Aoki T, Enomoto M, Kawada N, Okawa K. Putting "sticky notes" on the electronic medical record to promote intra-hospital referral of hepatitis B and C virus-positive patients to hepatology specialists: an exploratory study. BMC Infect Dis. 2016; 16:410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hidaka I, Enomoto M, Sato S, Suetsugu A, Matono T, Ito K, Ogawa K, Inoue J, Horino M, Kondo Y, Sakaida I, Korenaga M. Establishing efficient systems through electronic medical records to promote intra-hospital referrals of hepatitis virus carriers to hepatology specialists: A multicenter questionnaire-based survey of 1,281 healthcare professionals. Intern Med. 2021; 60:337-343. [DOI] [PMC free article] [PubMed] [Google Scholar]