

Abstract
Objective
This study aimed to investigate the clinical effects of abdominal aortic balloon occlusion followed by uterine artery embolization for the treatment of pernicious placenta previa complicated with placenta accreta during cesarean section.
Methods
We performed a retrospective analysis of the clinical data for 623 patients who experienced pernicious placenta previa complicated with placenta accreta and received treatment in our hospital from January 2013 to January 2019. All patients underwent abdominal aortic balloon occlusion before their cesarean section. Seventy-eight patients received bilateral uterine artery embolization, and among them, placenta accreta was found at the opening of the cervix in 13 patients. Due to suturing difficulty after the removal of the placenta, gauze packing was used to temporarily compress the hemorrhage. As soon as the uterus was sutured, emergent bilateral uterine artery embolization was performed. Active bleeding was noted in the remaining 65 patients when the lower part of the uterus was pressed after the placenta was removed and the uterus was sutured, therefor, bilateral uterine artery embolization was performed urgently.
Results
Of the 623 patients, 545 patients underwent only abdominal aortic balloon occlusion and 78 patients underwent additional emergent bilateral uterine artery embolization due to hemorrhaging during or after their cesarean section. No hysterectomies were performed. In the 78 patients, the amount of bleeding was 800-3,200 ml with an average of 1,650 ml during the operation; the volume of blood transfused was 360-1,750 ml (average: 960 ml). The fetal fluoroscopy time was 3–8 s (average: 5 s). The dose of radiation exposure was (4.2 ± 2.9) mGy. Fetal appearance, pulse, grimace, activity, and respiration (Apgar) score were normal. No serious complications were observed during or after the operation in the follow-up visits. Conclusion: For patients with pernicious placenta previa complicated with placenta accreta who experience active bleeding after cesarean section and abdominal aortic balloon occlusion, bilateral uterine artery embolization can effectively reduce blood loss and requirement of blood transfusion during the operation, and lowers the risk of hysterectomy.
Keywords: Pernicious placenta previa, Placenta accreta, Abdominal aorta, Balloon, Uterine artery, Embolism
The placenta previa that occurs after cesarean section is called dangerous placenta previa.1 With the liberalization of the policy of second birth in China, the proportion of women with a history of cesarean section has increased significantly, and the incidence of pernicious placenta previa has increased yearly.2 During cesarean section, 90% of the patients experience intra-operative bleeding more than 3,000 ml, 10% more than 10,000 ml,3 and some patients had to received hysterectomies to preserve the life of the parturient and fetus. In recent years, cesarean section combined with abdominal aortic balloon occlusion can effectively reduce the amount of intraoperative bleeding and reduce the rate of subsequent hysterectomies.4,5 However, active bleeding is still observed after abdominal aortic balloon occlusion in some patients. In this study, we performed a retrospective analysis of 623 patients who experienced pernicious placenta previa complicated with placenta accreta and received treatment in our hospital from January 2013 to January 2019. All patients underwent abdominal aortic balloon occlusion before their cesarean section, which effectively reduced the amount of intraoperative bleeding, number of transfusions, and the risk of hysterectomy.
Materials and methods
General data
From January 2013 to January 2019, 623 patients with pernicious placenta previa complicated with placenta accreta were enrolled at our hospital. All patients were diagnosed with pernicious placenta previa complicated with placenta accreta by color Doppler ultrasound and magnetic resonance imaging (MRI) before their operations (Fig. 1). The gestational age was more than 28 weeks. All patients agreed to cesarean section combined with abdominal aortic balloon occlusion. The abdominal aortic balloon catheter was temporarily blocked in 623 patients, and the fetuses were delivered uneventfully in all patients. No massive bleeding occurred during or after the operation in 545 patients. Seventy-eight patients underwent emergency sequential uterine artery embolism due to intraoperative or postoperative bleeding which successfully preserved the uterus. The mean age of the 78 patients was (30.6 ± 4.5) years, all with single fetuses and with an average of 4 pregnancies and 1 to 2 births. All parturients had a history of multiple pregnancies and one or more cesarean sections with the infant’s, average gestational age of 36 weeks.
Fig. 1.

In placenta previa complicated with placenta accreta, the boundary between the placenta and the myometrium is unclear.
Methods
Of the 623 patients, the procedures for 363 cases were performed in an interventional operating room with digital subtraction angiography machine (Artis zeego, Germany); the patients were then sent to the obstetrical operating room setup for the cesarean section combined with balloon occlusion. The procedures for 260 cases were performed in the compound operating room of our hospital equipped with a digital subtraction angiography (DSA) machine (Philips Allura Xper FD20, Holland). A finger oximeter was placed on the right big toe of each patient before her surgery to determine whether the balloon catheter had effectively blocked the abdominal aorta according to the indices of blood oxygen and heart rate during the surgery. Prior to the cesarean section, the right thigh artery was punctured under local anesthesia and a 7/8-Fr vascular sheath was inserted. A guide wire and balloon catheter were introduced through the sheath (Bard peripheral Vascular, Inc. along guide wire USA), and, under fluoroscopy, placed in the abdominal aorta with the main body of the balloon located at the level of the chest (thoracic 12 and lumbar 1) (Fig. 2).
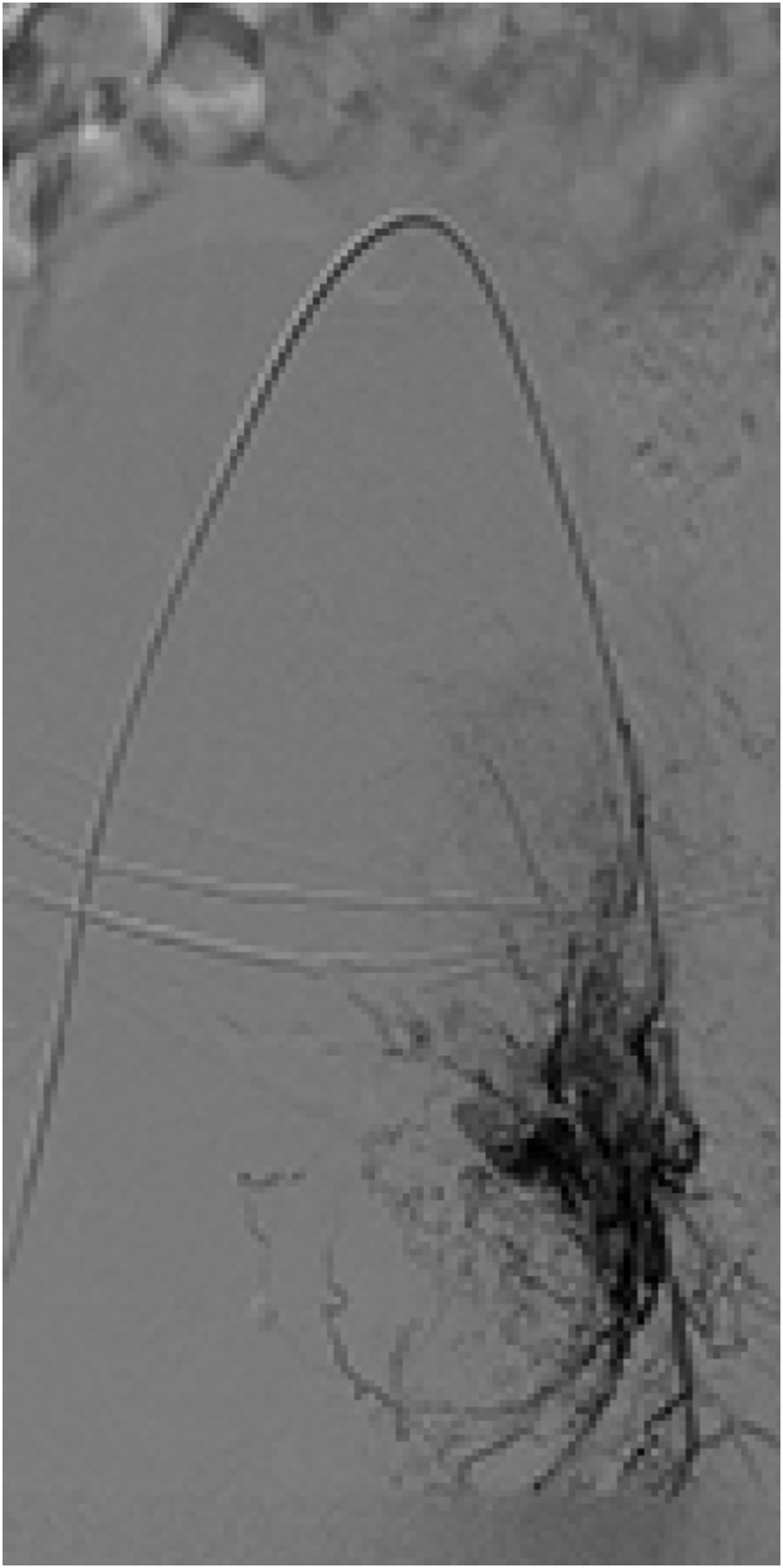
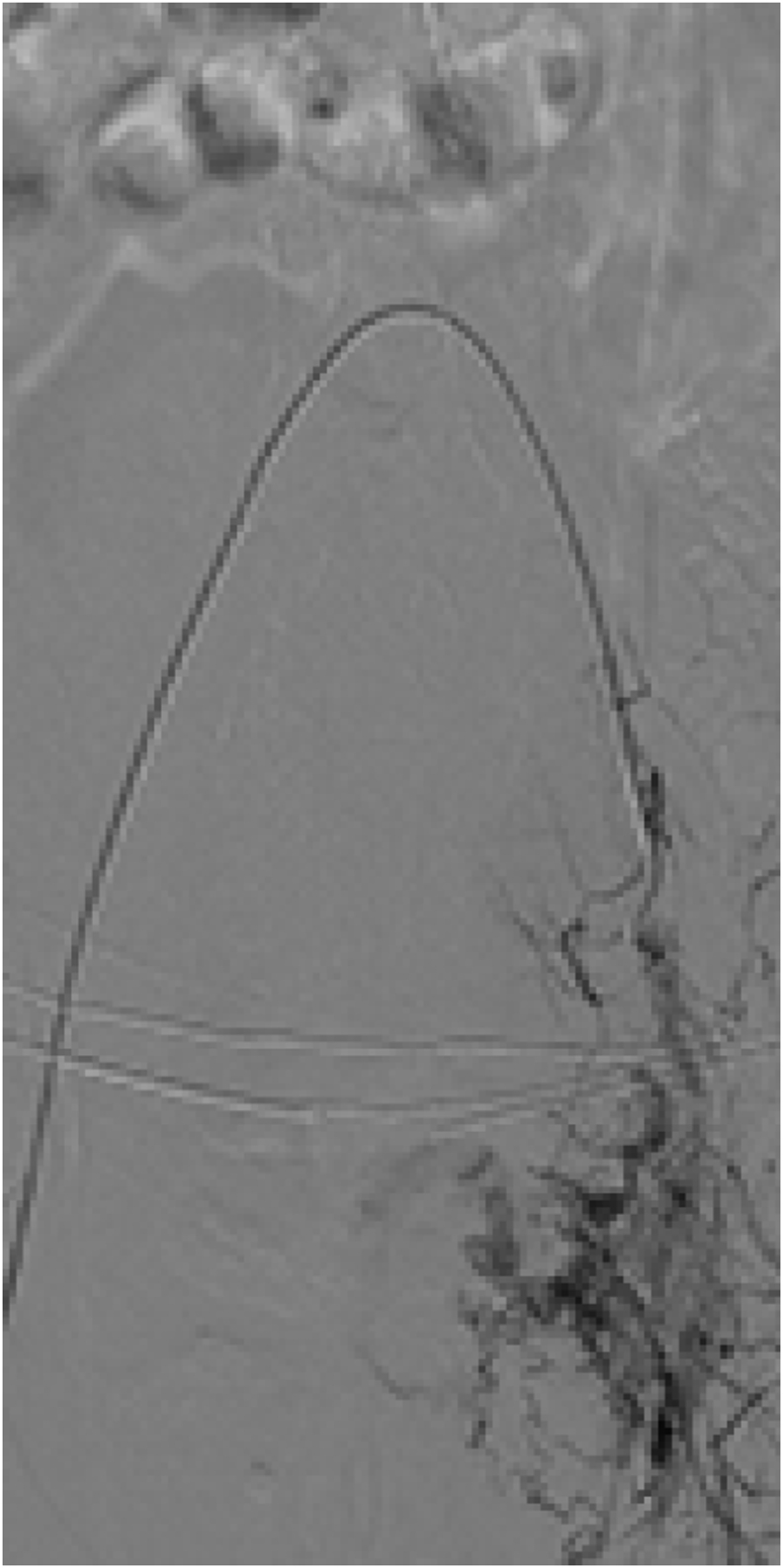
Fig. 2.

The balloon was inflated to occlude the abdominal aorta.
After the obstetrician cut the umbilical cord of the fetus, the interventional doctor immediately filled the balloon with saline to block the abdominal aortic artery, and monitored the balloon occlusion index to ensure that the blood oxygen of both toes decreased slowly to 0, blood oxygen curve was flat, and the heart rate gradually cannot be monitored. The obstetrician peeled the placenta at the same time, and balloon inflation time was selected according to the intraoperative placental detachment. Each inflation time did not exceed 15 min. If necessary, the balloon was completely released for 1 min. The balloon was re-inflated, and the total inflation time did not exceed 45 min. If a placental accretion of the cervix was found during the surgery, gauze pads were utilized to temporarily compress and stop the bleeding, and an emergency sequential uterine artery embolism was performed after suturing the uterus. At the end of the placental peeling, the placenta and myometrium were sutured. If after the suturing the uterine incision, active bleeding was still observed on pressing the floor of uterus, then the balloon was withdrawn, and bilateral uterine arteriography was performed by a 5-Fr Cobra catheter through the sheath. Gelatin sponge particles (350~560 μm) were used to plug the bilateral uterine arteries, and if necessary, an internal iliac artery and / or ovarian artery embolism was performed to control the bleeding. If the above methods could not effectively control the active bleeding, hysterectomy was performed. After the obstetrician sutured the skin incision, the vaginal packing was removed, arterial sheath was pulled out, and puncture point was bandaged using a pressure of the pressure device.
Indicators and follow-up
The main outcome measures were: placental implantations, total intra-operative bleeding, transfusions, fetal acceptance of radiation, appearance, pulse, grimace, activity, and respiration (Apgar) scores, and intra- and post-operative complications. The volume method and weighing method were used to calculate the total amount of bleed loss. The time and dose of X-ray radiation received by the fetus were estimated according to the digital subtraction angiography (DSA) procedure recommendations for exposure time and location during balloon implantation. Four hours after the surgery, the pressure bandage was removed and bedside color Doppler ultrasound examinations of the lower extremities showed that there were no arterial or venous thromboses, arteriovenous fistulas, pseudoaneurysms, or other related complications. Within 7 days after the surgery, the movements of the lower extremities, sensation in and pulsatility of the dorsalis pedis artery, fever, abnormal pain and other symptoms were recorded.
Statistical analysis
The statistical analyses were processed using SPSS19.0 statistical software. The measurement data of normal distribution were represented by ‾x ± s, and the counting data were represented by frequencies and rate.
Results
In 623 cesarean section cases, the abdominal aortic balloon catheter was temporarily blocked and the fetus was delivered uneventfully. Among them, 545 patients had no massive bleeding during or after the surgery, and no uterine artery embolisms were performed. Seventy-eight patients underwent emergency sequential uterine artery embolism due to intraoperative or postoperative bleeding. Of these 78 patients, 13 were found to have placental accretions of their cervixes during surgery, and it was not possible to suture, or to prevent their bleeding by temporarily applying pressure to the gauze packing. The other 65 patients were treated with bilateral uterine artery embolisms after suturing the uterus and compressing the uterine floor to assess for further bleeding. Bilateral uterine artery embolisms were performed because of active bleeding, and typical cases are shown in (Fig. 3, Fig. 4).
Fig. 3.
The distal branch of the uterine artery is tortuous and has obvious abnormal staining.
Fig. 4.
Abnormal staining was significantly reduced after embolization was performed using 350~560 μm gelatin sponge particles.
The intra-operative bleeding volume for the 78 patients was less than 1,000 ml for 27 patients, 1,000–3,000 ml for 32 patients, and more than 3,000 ml for 19 patients. The average bleeding volume was 1,650 ml. The volume of bleed transfused each time was 960 ml. The time for fetal fluoroscopy was 3–8 s, with an average of 5 s, and the amount of radiation received was (4.2 ± 2.9) mGy. Seventy-eight infants were successfully delivered with normal Apgar scores.
During the follow-up period, 78 patients had no complications such as renal insufficiency and/or ectopic embolism. Five cases had thromboses of the artery of right thigh, which may have been related to the state of hypercoagulability during pregnancy, balloon injuries of the intima and other factors. With treatment, blood-flow was re-established. Within 3 days after the surgery, 67 cases of post-embolism syndrome, mainly manifested as lower abdominal distension, pain and fever, were noted, which were all resolved with one week by using analgesics, antipyretics and other symptomatic treatment.
Discussion
With the increase of cesarean section rates, the incidence of placental accreta has increased significantly.6 Studies have shown that color Doppler ultrasound7 is the first choice for the diagnosis of this disease, and an MRI can improve the accuracy of the diagnosis.8,9 With the wide application of color Doppler ultrasound and MRI, it is not difficult to diagnose dangerous placental implantation accreta before delivery. According to the study, about 90% of pregnant women with pernicious placenta previa complicated with placenta accreta bleed more than 3,000 ml, and 10% bleed more than 10,000 ml, during cesarean sections, which often lead to hemorrhagic shock, disseminated intravascular coagulation and other serious complications, possibly endangering the life of the mother and infant, with a resulting hysterectomy rate of more than 50%.3,10
In recent years, abdominal aortic balloons to control bleeding have been widely used in a variety of surgeries.11 It was reported that temporary aortic balloon closures before caesarean sections can effectively reduce the amount of intra-operative blood loss and transfusions, clear the surgical field and reduce the rate of hysterectomies in patients with pernicious placenta previa complicated with placenta accreta.12, 13, 14, 15 The main surgical methods were uterine artery occlusion,16 internal ilium artery occlusions,13 and abdominal aortic occlusions.17 Compared with other surgical methods, abdominal aortic balloon occlusions have the advantages of being simple surgical procedures, have low radiation dosagese for pregnant women and fetuses, have unilateral arterial approaches and result in reduced intra-operative bleeding,4,18 making them the most commonly used surgical method at present.
However, active bleeding can still occur in some patients, even when abdominal aortic balloon closure is performed. The reasons are as follows: (1) the balloon used at present is non-compliant, and the effect of the balloon attachment is not ideal; (2) there are no clear guidelines regarding balloon diameters and the length of time for balloon closure, which may have deleterious hemostatic effects; (3) pernicious placenta accreta often necessitates that the placenta is peeled off manually, with all suspected bleeding points, sewn and ligated, and yet the wound may continue to bleed. (4) There are often many collateral areas of circulation in the uteri of patients with pernicious placenta accreta, such as ovarian arteries and−/−or inferior ventral arteries of the external ilium artery participating in the establishment of lateral branches of blood supplies,19, 20, 21 and the hemostatic effect of simply ligating the uterine artery is not ideal; or (5) uterine atony.22 Jijun et al.17 reported that some patients with pernicious placenta previa still underwent hysterectomy due to active bleeding after cesarean section combined with abdominal aortic balloon closure. Zhou et al.,23 claimed that uterine arterial embolization can be used for effectively preventing and treating obstetric hemorrhage and for improving the retention of the uterus. In this study, the placenta of 13 out of 623 patients who experienced pernicious placenta previa complicated with placenta accreta and received cesarean section combined with balloon occlusion, were found in the cervical orifice. Active bleeding was noted in 65 patients after abdominal aortic balloon occlusion, who were treated with emergency sequential uterine artery embolism and no hysterectomy. Thus, abdominal aortic balloon occlusion followed by uterine artery embolization for the treatment of pernicious placenta previa complicated with placenta accreta can effectively reduce fatal massive bleeding and lower the risk of hysterectomy.
In 2004, the American College of Obstetrics and Gynecologists guidelines stated that short-term exposure to X-ray less than 50 mGy does not increase the long-term complications for newborn children. In this study, the average fluoroscopy time for 78 fetuses was 5 s, and the radiation dose was (4.2 ± 2.9) mGy, which was significantly lower than the current recommendation. Uterine artery occlusions were performed after deliveries and did not increase the amount of radiation received by the fetus compared to balloon occlusions alone. During the follow-up periods for the 78 patients, no complications such as renal insufficiency, or renal and intestinal ischemia-reperfusion injuries were notes. In this study, gelatin sponge particles were used as an embolic agent. The results showed that the gelatin sponges were absorbed after an average of 3 weeks, and would not affect the fertility of the patients.24
In summary, active bleeding was still observed in patients with pernicious placenta previa complicated with placenta accrete who undergo partial simple cesarean section only combined with abdominal aortic balloon occlusion, if the placenta was present in the cervix, or the floor of the uterus was pressed. Emergency sequential bilateral uterine artery embolism was then performed. Abdominal aortic balloon occlusion followed by uterine artery embolization for the treatment of pernicious placenta previa complicated with placenta accreta during cesarean section can effectively reduce the amount of intra-operative bleeding, number of blood transfusions, and risk of hysterectomy, with no serious adverse effects on pregnant women or fetuses.
Contributor Information
Yanli Wang, Email: jiangtianyishui@163.com.
Xinwei Han, Email: hanxinwei2006@163.com.
References
- 1.Kollmann M., Gaulhofer J., Lang U. Placenta praevia: incidence, risk factors and outcome. J Matern Fetal Neonatal Med. 2013;29:1395–1398. doi: 10.3109/14767058.2015.1049152. [DOI] [PubMed] [Google Scholar]
- 2.Baba Y., Matsubara S., Ohkuchi A. Anterior placentation as a risk factor for massive hemorrhage during cesarean section in patients with placenta previa. J Obstet Gynaecol Res. 2014;40:1243–1248. doi: 10.1111/jog.12340. [DOI] [PubMed] [Google Scholar]
- 3.Bowman Z.S., Manuck T.A., Eller A.G. Risk factors for unscheduled delivery in patients with placenta accreta. Am J Obstet Gynecol. 2014;210 doi: 10.1016/j.ajog.2013.09.044. 241.e1-6. [DOI] [PubMed] [Google Scholar]
- 4.Wang Y.L., Duan X.H., Han X.W. Comparison of temporary abdominal aortic occlusion with internal iliac artery occlusion for patients with placenta accreta - a non-randomised prospective study. VASA. 2017;46:53–57. doi: 10.1024/0301-1526/a000577. [DOI] [PubMed] [Google Scholar]
- 5.Chu Q., Shen D., He L. Anesthetic management of cesarean section in cases of placenta accreta, with versus without abdominal aortic balloon occlusion: study protocol for a randomized controlled trial. Trials. 2017;18:240. doi: 10.1186/s13063-017-1977-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.O’Connor D., Berndl A. Placenta percreta. CMAJ (Can Med Assoc J) 2018;190:E168. doi: 10.1503/cmaj.171411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Riteau A.S., Tassin M., Chambon G. Accuracy of ultrasonography and magnetic resonance imaging in the diagnosis of placenta accreta. PLoS One. 2014;9 doi: 10.1371/journal.pone.0094866. e94866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang Y.L., Duan X.H., Han X.W. Abnormal placentation: the role of MRI in diagnosis and therapeutic planning. Clin Radiol. 2017;72 doi: 10.1016/j.crad.2016.09.015. 176.e9-176.e14. [DOI] [PubMed] [Google Scholar]
- 9.Leyendecker J.R., Dubose M., Hosseinzadeh K. MRI of pregnancy-related issues: abnormal placentation. AJR Am J Roentgenol. 2012;198:311–320. doi: 10.2214/AJR.11.7957. [DOI] [PubMed] [Google Scholar]
- 10.Minas V., Gul N., Shaw E. Prophylactic balloon occlusion of the common iliac arteries for the management of suspected placenta accreta/percreta: conclusions from a short case series. Arch Gynecol Obstet. 2015;291:461–465. doi: 10.1007/s00404-014-3436-9. [DOI] [PubMed] [Google Scholar]
- 11.Gong H.S., Liu G.J., Huang Q.S. Surgical management of sacrococcygeal region giant tumors by use of balloon occlusion abdominal aorta. Turk Neurosurg. 2016;26:904–911. doi: 10.5137/1019-5149.JTN.13606-14.1. [DOI] [PubMed] [Google Scholar]
- 12.Cui S.H., Zhi Y.X., Zhang K. Application of temporary balloon occlusion of the abdominal aorta in the treatment of complete placenta previa complicated with placenta accreta. Zhonghua Fu Chan Ke Za Zhi. 2016;51:672–677. doi: 10.3760/cma.j.issn.0529-567X.2016.09.007. [DOI] [PubMed] [Google Scholar]
- 13.Zhao X.L., Liu Z., Wang Y.L. Value of temporary balloon occlusion of abdominal aorta in prevention of bleeding during cesarean section in women with pernicious placenta previa and placenta accreta. Chin J Prev Med. 2015;7:507–511. [Google Scholar]
- 14.Wu Q., Liu Z., Zhao X. Outcome of pregnancies after balloon occlusion of the infrarenal abdominal aorta during caesarean in 230 patients with placenta praevia accreta. Cardiovasc Interv Radiol. 2016;39:1573–1579. doi: 10.1007/s00270-016-1418-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tian J., Wang Y.L., Han X.W. The clinical application of abdominal aortic balloon occlusion followed by uterine artery embolization in the treatment of pernicious placenta previa complicated with placenta accreta during cesarean section. Chin J Infrared Res. 2017;5:149–152. doi: 10.1016/j.jimed.2019.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Luo F., Xie L., Xie P. Intraoperative aortic balloon occlusion in patients with placenta previa and/or placenta accreta: a retrospective study. Taiwan J Obstet Gynecol. 2017;56:147–152. doi: 10.1016/j.tjog.2016.11.004. [DOI] [PubMed] [Google Scholar]
- 17.Jijun L.I., Changting Z., Xietong W. Application of abdominal aorta balloon occlusion in cesarean section for patients with pernicious placenta previa complicated by placenta accreta. J Shandong Univ (Nat Sci) 2016;54:22–25. [Google Scholar]
- 18.Wang Y.L., Duan X.H., Han X.W. Temporary aortic balloon occlusion in management of cesarean section for pernicious placenta previa/accreta. Pract Radiol. 2015;7 1186-1188,1197. [Google Scholar]
- 19.Soyer P., Morel O., Fargeaudou Y. Value of pelvic embolization in the management of severe postpartum hemorrhage due to placenta accreta, increta or percreta. Eur J Radiol. 2011;80:729–735. doi: 10.1016/j.ejrad.2010.07.018. [DOI] [PubMed] [Google Scholar]
- 20.Palacios Jaraquemada J.M., García Mónaco R., Barbosa N.E. Lower uterine blood supply: extrauterine anastomotic system and its application in surgical devascularization techniques. Acta Obstet Gynecol Scand. 2007;86:228–234. doi: 10.1080/00016340601089875. [DOI] [PubMed] [Google Scholar]
- 21.Ramoni A., Strobl E.M., Tiechl J. Conservative management of abnormally invasive placenta: four case reports. Acta Obstet Gynecol Scand. 2013;92:468–471. doi: 10.1111/aogs.12079. [DOI] [PubMed] [Google Scholar]
- 22.Muir H.A. Pharmacologic intervention for managing uterine atony and related maternal hemorrhage: what is the most effective drug dose? Can J Anaesth. 2013;60:1047–1053. doi: 10.1007/s12630-013-0030-8. [DOI] [PubMed] [Google Scholar]
- 23.Zhou Y.M., Zhai R.Y., Jiang L. Super sclective transcatheter angiographic embolization:an effective and prophylactic treatment for massive obstetric haemorrhage. J Interv Radiol. 2008;17:211–214. [Google Scholar]
- 24.Chrisman H.B., Saker M.B., Ryu R.K. The impact of uterine fibroid embolization on resumption of menses and ovarian function. J Vasc Interv Radiol. 2000;11:699–703. doi: 10.1016/s1051-0443(07)61627-3. [DOI] [PubMed] [Google Scholar]