

Abstract
Background/Aims
Crohn’s disease is a chronic disorder; therefore, it is essential to investigate long-term safety and efficacy of treatments. This study assessed the safety and effectiveness of adalimumab for up to 3 years in Japanese patients with Crohn’s disease in real-world settings.
Methods
This was a multicenter, single-cohort, observational study of patients with Crohn’s disease. Safety assessments included incidence of adverse drug reactions. Effectiveness assessments included clinical remission, mucosal healing, and Work Productivity and Activity Impairment (WPAI).
Results
The safety and effectiveness analysis populations comprised 389 and 310 patients, respectively. Mean (standard deviation) exposure to adalimumab in the safety analysis population was 793.4 (402.8) days, with a 58.1% retention rate. A total of 105 patients (27.0%) and 43 patients (11.1%) experienced adverse drug reactions and serious adverse drug reactions, respectively, with no patient reporting tuberculosis or hepatitis B. Infections and serious infections were reported in 37 patients (9.5%) and 17 patients (4.4%), respectively. Malignancy was reported as an adverse drug reaction in 2 patients (0.5%). Remission rate increased from 37.8% (98/259) at baseline to 73.9% (167/226) at week 4 and remained > 70% over 3 years. Proportion of patients without mucosal ulcerations increased from 2.7% (2/73) at baseline to 42.3% (11/26) between years > 2 to ≤ 3. WPAI improvement started at 4 weeks, with the overall work impairment score improving from 42.7 (n = 102) at baseline to 26.9 (n = 84) at 4 weeks.
Conclusions
Results from this study confirm the long-term safety and effectiveness of adalimumab treatment in Japanese patients with Crohn’s disease in the real-world setting.
Keywords: Adalimumab, Crohn disease, Inflammatory bowel diseases, Japanese, Postmarketing surveillance
INTRODUCTION
Crohn’s disease (CD) is an inflammatory bowel disease characterized by persistent and chronic transmural intestinal inflammation and ulceration that may affect any part of the gastrointestinal tract, but most commonly involves the colon and/or the ileum [1]. Clinical symptoms include abdominal pain, diarrhea, fever, and weight loss [2]. In addition, up to 40% of patients with CD report extraintestinal manifestations (EIMs) [3,4]. Patients who experience debilitating gastrointestinal symptoms report a negative impact on their day-to-day activities, ability to work, and work productivity and an overall impaired quality of life [5-7].
CD has long been considered a disease of the Western world, where its incidence is the highest [8]. However, over recent decades, epidemiologic studies have reported a rapid increase in the incidence of CD in Asian countries, including Japan, Korea, China, Hong Kong, and India [8,9]. Indeed, from 1991 to 2014, the annual prevalence rate of CD in Japan increased from 5.9 to 55.6 per 100,000 persons [10,11].
Adalimumab, a fully human anti-tumor necrosis factor-α (TNF-α) monoclonal antibody, is efficacious and well tolerated in both Western and Japanese populations with moderate to severe CD. In clinical studies in Western populations, adalimumab induced and maintained clinical remission [12-14], with prolonged adalimumab therapy maintaining clinical remission for up to 4 years [15]. Moreover, adalimumab was well tolerated in the long term, with no new safety concerns observed over 6 years of follow-up [16-18]. In Japan, a randomized, double-blind, placebo-controlled clinical trial and its open-label extension study showed that adalimumab is an effective and well-tolerated treatment option for inducing and maintaining clinical remission up to 3 years in patients with moderate to severe CD [19,20]. Notably, results from a 24-week real-world study in 1,693 Japanese patients with CD showed that adalimumab treatment significantly reduced disease activity without any unexpected adverse drug reactions (ADRs) [21].
However, given the chronic nature of CD, long-term real-world evidence studies are essential to evaluate the incidence of known safety events, provide insights into long-term safety and rare adverse events (AEs), and confirm the sustained efficacy of treatments in clinical practice. Therefore, the objective of this prospective, observational study was to evaluate the long-term (up to 3 years) safety and effectiveness of adalimumab in Japanese patients with CD in clinical practice.
METHODS
1. Study Design
This multicenter, single-cohort, noninterventional, postmarketing surveillance study was conducted to evaluate the safety and effectiveness of adalimumab over 3 years in patients with active CD (ClinicalTrials.gov, NCT01464333). The surveillance period was from November 2011 to March 2017. Patients were registered in the study from November 2011 to October 2013. The study protocol was reviewed and approved by the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) before the study began. The study was conducted at medical institutions in Japan in compliance with Good Postmarketing Study Practice; therefore, institutional review board approval and written informed patient consent were not required.
2. Patients
In accordance with the package insert for adalimumab in Japan, patients with moderate to severe CD who were refractory to conventional therapies were considered suitable for adalimumab treatment and therefore eligible for participation in the study. Patients who presented with malignancy at baseline or who had a history of malignancy were excluded.
3. Adalimumab Dosing Regimen
Patients received subcutaneous injections of adalimumab at a starting dose of 160 mg, followed by 80 mg at week 2, and 40 mg every other week (eow) thereafter for 3 years. Starting in June 2016 in Japan, escalation of the maintenance dose of adalimumab to 80 mg eow was permitted in patients who no longer responded to adalimumab 40 mg eow, per PMDA approval [22].
4. Assessments
A paper-based case report form (CRF) was used to collect data for analysis. Safety assessments included the incidence of ADRs, serious ADRs, malignancy, infections, and serious infections. AEs were coded using preferred terms (PT) from the bilingual (English-Japanese) version of the Medical Dictionary for Regulatory Activities (MedDRA/J, version 20.1). AEs for which causality with adalimumab could not be excluded were defined as ADRs.
Effectiveness assessments, including Crohn’s Disease Activity Index (CDAI) score, EIMs, C-reactive protein (CRP) levels, and Work Productivity and Activity Impairment (WPAI) score, were performed among the observed cases at baseline; week 4; months 3 and 6; years 1, 1.5, 2, 2.5, and 3; and at study discontinuation. Clinical remission was defined as a CDAI score < 150. Assessment of EIMs in the effectiveness analysis population was based on question 4 of the CDAI, which evaluated the following EIM categories: arthritis or arthralgia, ocular complications (iritis or uveitis), and cutaneous complications (erythema nodosum, pyoderma gangrenosum, or aphthous stomatitis). Based on patient responses to the WPAI questionnaire, the following categories were assessed: absenteeism, presenteeism, overall work impairment, and activity impairment. Endoscopic examinations were performed at the following aggregated time points: baseline, ≤ 6 months, > 6 months to ≤ 1 year, > 1 to ≤ 2 years, and > 2 to ≤ 3 years.
Subgroup analyses were conducted to examine a potential association between the incidence of ADRs and baseline factors, such as sex, prior use of anti-TNF-α therapy, and concomitant corticosteroid and immunomodulator use.
5. Statistical Analysis
The safety analysis population included all registered patients who had a completed CRF and initiated adalimumab after registration. Patients with any protocol violation were excluded from the safety analysis population. The effectiveness analysis population included all patients in the safety analysis population except those for whom CDAI could not be assessed after adalimumab initiation. Effectiveness analysis was conducted for those patients in the effectiveness analysis population who were assessed at baseline and ≥ 1 time point thereafter. Categorical data were summarized as the number and proportion of cases, and quantitative data were summarized using descriptive statistics (number, proportion, mean, standard deviation [SD], median, and interquartile range). A univariate logistic regression analysis was conducted to examine the potential association between the incidence of ADRs and baseline factors; P values were calculated using Fisher exact test. All tests were performed using a two-sided significance level of 5%. Statistical analysis was performed using SAS version 9.3 (SAS Institute, Cary, NC, USA).
RESULTS
1. Patient Disposition
A total of 511 patients were enrolled in the study; of these, 504 had assessable data in their CRFs. Of the 115 patients excluded from the study, 111 were excluded because they were registered after the period of registration defined in the protocol, that is, the registration form was postmarked on or after 15 days following adalimumab initiation, and 3 because of a history or presence of malignancy, which was defined as an exclusion criterion. After exclusion of 115 patients, the safety analysis population comprised 389 patients. CDAI data were unavailable for 79 of these patients; therefore, the effectiveness analysis population comprised 310 patients (Fig. 1A). The mean ± SD exposure to adalimumab in the safety analysis set was 793.4 ± 402.8 days (median, 1,093 days). Overall, 226 patients (58.1%) continued adalimumab treatment for 3 years (Fig. 1B) and 163 discontinued owing to insufficient efficacy (72/163, 44.2%), loss to follow-up (42/163, 25.8%), AEs (34/163, 20.9%), patient request (11/163, 6.7%), and other reasons (4/163, 2.5%).
Fig. 1.

(A) Patient disposition. (B) Kaplan-Meier curve for drug survival (safety analysis population). aThere could be more than 1 reason for exclusion of patients. CRF, case report form.
2. Patient Demographics and Baseline Characteristics
In the safety analysis population, 283 patients (72.8%) were male and the mean age was 34 years. The mean duration of CD was 9 years, and 36.5% of patients had had CD for ≥ 10 years (Table 1). Overall, 32.1% of patients were receiving concomitant immunomodulators, 42.9% of patients had CD-related intestinal complications, and 29.0% of patients had CD-related EIMs. The majority of patients (56.6%) had ileocolonic disease. The mean baseline CDAI score was 193.9. Overall, 140 patients (36.0%) had previously received anti-TNF-α therapy, of whom 53.6% had discontinued owing to lack of efficacy, 28.6% owing to AEs, and 19.3% for other reasons.
Table 1.
Patient Demographics and Baseline Disease Characteristics
| Characteristic | Safety analysis population (n = 389) |
|---|---|
| Age (yr) | 34.0 ± 11.8 |
| Male sex | 283 (72.8) |
| Weight (kg) | 55.1 ± 10.4 |
| Duration of CD (yr) | 9.0 ± 9.4 |
| < 2 | 115 (29.6) |
| 2 to < 5 | 48 (12.3) |
| 5 to < 10 | 55 (14.1) |
| ≥ 10 | 142 (36.5) |
| Unknown | 29 (7.5) |
| History of smoking, never smoked | 243 (62.5) |
| Comorbidities | |
| Liver disorders | 17 (4.4) |
| Renal disorders | 5 (1.3) |
| Blood disorders | 44 (11.3) |
| Respiratory disorders | 11 (2.8) |
| Others | 71 (18.3) |
| CD-related pretreatment drugs | |
| Anti-TNF-α agent | 140 (36.0) |
| Aminosalicylates | 351 (90.2) |
| Corticosteroids | 62 (15.9) |
| Immunomodulators | 80 (20.6) |
| Antibiotics | 46 (11.8) |
| CD-related concomitant drugs | |
| Aminosalicylates | 336 (86.4) |
| Corticosteroids | 59 (15.2) |
| Immunomodulators | 125 (32.1) |
| Antibiotics | 49 (12.6) |
| Others | 286 (73.5) |
| Disease locationa | |
| Ileal | 104 (26.7) |
| Colonic | 57 (14.7) |
| Ileocolonic | 220 (56.6) |
| Isolated upper disease | 53 (13.6) |
| CD-related intestinal complications | 167 (42.9) |
| CD-related extraintestinal manifestations | 113 (29.0) |
| Self-administration of adalimumab | 342 (87.9) |
| Work status | |
| Employed ≥ 35 hr/wk | 192 (49.4) |
| Employed < 35 hr/wk | 32 (8.2) |
| Unemployed, but can perform normal daily activitiesa | 113 (29.0) |
| No normal daily activities (due to hospitalization, etc.) | 49 (12.6) |
| Unknown | 3 (0.8) |
| CDAI scorec | 193.9 ± 102.2 |
| < 150 | 101 (26.0) |
| 150 to < 220 | 65 (16.7) |
| 220 to < 450 | 98 (25.2) |
| ≥ 450 | 5 (1.3) |
| Unknown | 120 (30.8) |
| CRP levels (mg/dL)d | 0.72 (0.19-2.14) |
Values are presented as mean±standard deviation, number (%), or median (interquartile range).
According to Montreal classification.
Daily activity includes working around the house, shopping, childcare, exercising, and studying.
(n=269).
(n=364).
CD, Crohn’s disease; TNF-α, tumor necrosis factor alpha; CDAI, Crohn’s Disease Activity Index; CRP, C-reactive protein.
3. Safety
Overall, the incidence of ADRs was 27.0% (n = 105) and that of serious ADRs was 11.1% (n = 43) (Table 2). Per 100 patient-years (PY), 18.6 ADRs and 6.2 serious ADRs were reported. By MedDRA system organ class (SOC), the most frequent (> 5%) ADRs were infections and infestations (n = 37, 9.5%), followed by gastrointestinal disorders (n = 27, 6.9%). In addition, 14 patients (3.6%) reported ADRs in the skin and subcutaneous tissue disorders SOC; of these, 1 patient had psoriasis (by PT). The most frequent ( > 1%) serious ADRs by SOC were gastrointestinal disorders (n = 19, 4.9%) and infections and infestations (n = 17, 4.4%) (Table 2). Results from the univariate analysis identified female sex as being associated with a significantly higher incidence of ADRs (female vs. male, 34.9% vs. 24.0%; P=0.040). However, prior use of anti-TNF-α therapy (use vs. no use, 27.1% vs. 26.9%; P=1.000), concomitant corticosteroids (use vs. no use, 32.2% vs. 26.1%; P=0.341), and immunomodulators (use vs. no use, 21.6% vs. 29.5%; P=0.112) was not associated with a significantly higher incidence of ADRs. On further stratified analysis, no difference in the incidence of ADRs by MedDRA SOC was found between female and male patients. The ADRs that were more frequently (difference in incidence > 1.0%) reported in female versus male patients included pyrexia (3.8% [4/106] vs. 0.7% [2/283]), CD (3.8% [4/106] vs. 2.1% [6/283]), pruritus (1.9% [2/106] vs. 0% [0/283]), injection site pruritus (1.9% [2/106] vs. 0% [0/283]), small intestine stenosis (1.9% [2/106] vs. 0.4% [1/283]), arthralgia (1.9% [2/106] vs. 0.4% [1/283]), injection site swelling (1.9% [2/106] vs. 0.4% [1/283]), and rash (1.9% [2/106] vs. 0.7% [2/283]).
Table 2.
Incidence of ADRs and Serious ADRs (n=389)
| Type of ADR | All ADRs | Serious ADRs |
|---|---|---|
| All ADRs | 105 (27.0) | 43 (11.1) |
| ADRs by SOC | ||
| Infections and infestations | 37 (9.5) | 17 (4.4) |
| Neoplasms benign, malignant and unspecified (including cysts and polyps) | 2 (0.5) | 2 (0.5) |
| Blood and lymphatic system disorders | 4 (1.0) | 0 |
| Immune system disorders | 2 (0.5) | 1 (0.3) |
| Endocrine disorders | 1 (0.3) | 0 |
| Metabolism and nutrition disorders | 2 (0.5) | 0 |
| Psychiatric disorders | 2 (0.5) | 1 (0.3) |
| Nervous system disorders | 4 (1.0) | 0 |
| Cardiac disorders | 1 (0.3) | 0 |
| Vascular disorders | 1 (0.3) | 0 |
| Respiratory, thoracic and mediastinal disorders | 6 (1.5) | 0 |
| Gastrointestinal disorders | 27 (6.9) | 19 (4.9) |
| Hepatobiliary disorders | 3 (0.8) | 1 (0.3) |
| Skin and subcutaneous tissue disorders | 14 (3.6) | 0 |
| Musculoskeletal and connective tissue disorders | 6 (1.5) | 2 (0.5) |
| Reproductive system and breast disorders | 1 (0.3) | 0 |
| General disorders and administration-site conditions | 15 (3.9) | 2 (0.5) |
| Investigations | 14 (3.6) | 3 (0.8) |
| Injury, poisoning and procedural complications | 1 (0.3) | 1 (0.3) |
| ADRs of special interest | ||
| Infection | 37 (9.5) | 17 (4.4) |
| Malignancy | 2 (0.5) | 2 (0.5) |
Value are presented as number (%).
ADR, adverse drug reaction; SOC, system organ class.
The incidence of infections was 9.5% (n = 37; 4.7 events/100 PY) and that of serious infections was 4.4% (n = 17; 2.1 events/100 PY). All serious infections were reported in 1 patient each, except for an anal abscess and an abdominal abscess, which were reported in 2 patients each. No patient reported de novo tuberculosis or reactivation of tuberculosis. In addition, reactivation of hepatitis B was not reported. Malignancy was reported in 3 patients as an AE (0.8%). Causality with adalimumab could not be excluded in 2 patients (0.5%, 3 events; 0.34 events/100 PY): a man who developed anal cancer 406 days after adalimumab initiation, which subsequently resolved, and a man who developed metastases to the bone at 1,030 days after adalimumab initiation and was diagnosed with metastatic renal cell carcinoma at 1,034 days, which resulted in death. Of the 3 patients with malignancy, 1 woman, who was diagnosed with squamous cell carcinoma of the skin 63 days after adalimumab initiation, received concomitant immunomodulators with adalimumab for 3 years. Causality with adalimumab could not be established in this case, and the patient recovered subsequently. The incidence of ADRs at the “injection site,” “administration site,” “indication site” or “infusion site” in the MedDRA SOC general disorders and administration site conditions by PT was as follows: injection site swelling (n = 3, 0.77%), injection site pruritus (n = 2, 0.51%), injection site reaction (n = 1, 0.26%), and injection site erythema (n = 1, 0.26%).
4. Effectiveness
Of patients who had a CDAI score at baseline and ≥ 1 time point thereafter in the effectiveness analysis population, the proportion of patients with clinical remission at baseline (37.8%, 98/259) increased to 73.9% (167/226) at 4 weeks and was maintained over 70% thereafter throughout the 3-year observation period in the observed cases (Fig. 2A). Remission rate at last evaluation in this population was 68.3% (177/259). Of patients with a CDAI score ≥ 150 at baseline who achieved remission at 4 weeks, 65.9% (54/82) remained in remission at the last evaluation.
Fig. 2.

(A) Clinical remission (Crohn’s Disease Activity Index <150). (B) Proportion of patients with extraintestinal manifestation (EIM). (C) Proportion of patients with mucosal healing on endoscopic evaluation. aNot limited to patients who underwent balloon endoscopic assessment; bOnly patients with data available on the same day for both the large and small intestines were included.
The course of EIMs was assessed in 37 patients who reported EIMs at baseline and underwent postbaseline assessments, based on question 4 of the CDAI, during the adalimumab treatment period; of these patients, 21 had arthritis or arthralgia and 25 had cutaneous complications, such as erythema nodosum, pyoderma gangrenosum, or aphthous stomatitis, at baseline. No patients presented with ocular complications. Following 4 weeks of adalimumab therapy, EIMs were observed in 29.4% (10/34) of patients. After 3 years of adalimumab therapy, there were no documented cases of EIMs (0/14) among the observed cases (Fig. 2B).
At baseline, the majority of patients had mucosal ulceration in the large intestine (84.5%, 109/129) and small intestine (92.8%, 90/97). Of patients with data available on the same day for both the large and small intestines, 97.3% of patients (71/73) had mucosal ulceration in both at baseline. Following adalimumab therapy, the proportion of patients without mucosal ulceration in the large intestine, small intestine, or both increased to 64.3% (36/56), 46.3% (19/41), and 42.3% (11/26), respectively, between years > 2 and ≤ 3 (Fig. 2C). Mean ± SD CRP levels decreased from 1.53 ± 2.00 mg/dL (n = 293) at baseline to 0.66 ± 2.90 mg/dL (n = 145) at 3 years (Fig. 3).
Fig. 3.
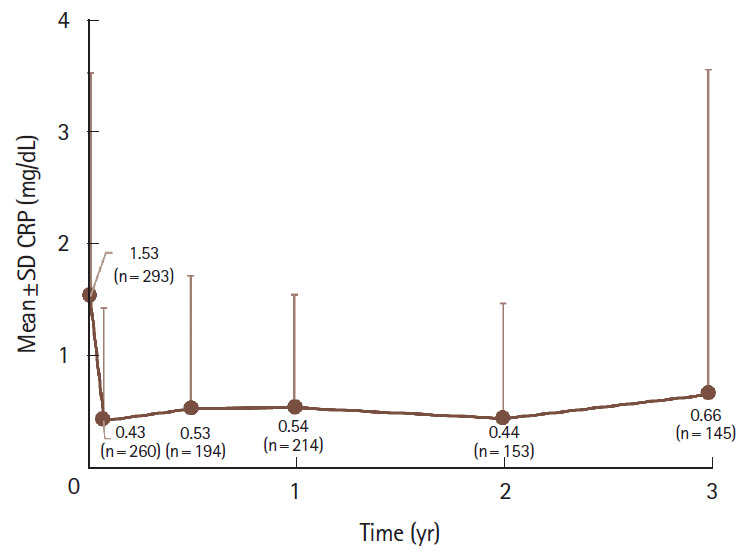
Change in C-reactive protein (CRP) levels. SD, standard deviation.
5. Work Productivity and Activity Impairment Scores
At baseline, mean scores on the WPAI questionnaire for patients who were employed indicated impairment in both work productivity and daily activities. Treatment with adalimumab improved WPAI domain scores as early as week 4, with an overall work impairment score of 42.7 (n = 102) at baseline and 26.9 (n = 84) at week 4, which was sustained throughout the 3-year observation period (Fig. 4).
Fig. 4.

Work Productivity and Activity Impairment scores. aIncluded only patients who were employed.
DISCUSSION
In this long-term, real-world study of adalimumab in Japanese patients with CD, the safety profile of adalimumab was similar to that reported in previous studies [15,18-20], and no new safety concerns were observed. The most frequent serious ADR by MedDRA SOC was infections and infestations. Nevertheless, the incidence of serious infections (2.1 events/100 PY) was lower than that reported in a 3-year follow-up of a cohort of Japanese patients with moderate to severe CD receiving adalimumab (7.1 events/100 PY) [20], and lower than that reported over a 6-year follow-up in an international postmarketing registry (PYRAMID) that included patients with moderate to severe CD receiving adalimumab (5.0 events/100 PY) [23].
The absolute risk of tuberculosis is higher in Asian than in Western countries, leading to a greater risk of tuberculosis in Asian patients receiving anti-TNF-α therapy [24]. However, the projected incremental risk is lower in Japan compared with other Asian countries owing to a relatively low incidence of tuberculosis. This is consistent with no cases of de novo tuberculosis or reactivation of tuberculosis reported with adalimumab therapy in our study in Japanese patients. The incidence of malignancy in the current study (0.3 events/100 PY) was consistent with that observed in the PYRAMID registry (0.7 events/ 100 PY) [23]. There was 1 case of anal cancer in a patient who did not have anal-perianal lesions associated with CD at baseline, a case of renal cell carcinoma with bone metastasis, and a case of squamous cell carcinoma of the skin.
In ADJUST, a large (n = 1,189), multicenter, retrospective cohort study, female sex, previous infliximab use, and concomitant treatment with prednisolone at baseline were associated with discontinuation of adalimumab due to AEs in patients with CD [25]. In the present study, regression analysis demonstrated that the incidence of ADRs was significantly higher in female patients but not in patients with prior use of anti-TNF-α therapy or concomitant corticosteroid use. Similarly, no significant difference in the incidence of ADRs between patients with and without concomitant immunomodulator use was demonstrated. This was consistent with observations in an open-label prospective study, DIAMOND, in which the incidence of AEs was similar between patients with active CD receiving adalimumab monotherapy and those receiving adalimumab with azathioprine [26], although a higher proportion of patients receiving combination therapy discontinued treatment owing to side effects [26,27]. It is noteworthy that in this study, patients receiving concomitant medications were not limited to those who received it at the time of an ADR, but also included those who received it at any time during the study.
Since this was a postmarketing surveillance, inclusion criterion of moderate to severe CD was determined in accordance with the indication described in the package insert, and a concrete definition of disease activity was not provided in the study protocol. Results revealed that a considerable proportion of patients with a baseline CDAI score less than 220 (> 40%) and those with a missing CDAI score ( > 30%) were included in the study. Considering the observational nature of the study and the variable course of CD, which includes spontaneous flare-ups and remissions, patients were not excluded based on the baseline CDAI score at physicians’ decision. These data present a real-world scenario of adalimumab utilization in patients with CD in routine practice. Among patients whose CDAI scores were assessed at baseline and ≥ 1 time point thereafter, remission rate increased at 4 weeks (73.9%) from baseline (37.8%) and remained over 70% thereafter in the observed cases. The sustained effectiveness of adalimumab observed in this study is consistent with that observed in other observational studies in patients with CD [23].
The present study is the first to show the effectiveness of adalimumab in resolving EIMs in Japanese patients with CD. Although the number of patients with EIM who were assessed was low, resolution of EIMs with adalimumab treatment started as early as week 4 in this study. Results from data pooled from previous studies on CD (i.e., 11 induction, maintenance, and open-label extension studies of adalimumab) have also concluded that the resolution of EIMs is rapid and durable with adalimumab therapy versus placebo [28].
Previous studies have emphasized the importance of including objective measures of inflammation, such as endoscopic lesions and CRP levels, in CD trials [1,29,30]. The first endoscopic study of adalimumab treatment, EXTEND, demonstrated mucosal healing at 52 weeks in 24% of patients who continued adalimumab treatment [1]. Similarly, in our study, the rate of mucosal healing in both the small and large intestines was relatively high (39%) between 6 months and 1 year, and increased by the last evaluation time point. Although the proportion of patients without mucosal lesions in the large intestine increased over time, no clear trend over time was observed for those with lesions in the small intestine. The difference in results could be due to variations in the endoscopic procedures (single balloon/double balloon) [31] for visualizing the small intestine because they were not specified in the protocol. Additionally, because there was no specified time point for conducting endoscopic assessments in this study, the assessment time points may have varied among patients, leading to this difference. Decrease in CRP levels from baseline was observed at all evaluated time points (mean ± SD, 1.53 ± 2.00 mg/dL at baseline vs. 0.66 ± 2.90 mg/dL at 3 years).
In addition to improvements in rates of clinical and endoscopic remission, improvements in WPAI scores—an important treatment goal in CD—were observed over 3 years with adalimumab treatment. This is the first study to show improvement in the WPAI in the Japanese population. Significant improvements in all components of the WPAI were also observed after 20 weeks of treatment with adalimumab in an open-label, phase 3b study involving 945 patients with CD, outside of Japan [5]. Similarly, long-term improvement in the WPAI for up to 6 years was observed with adalimumab in the PYRAMID registry [23].
Because this study was performed in the real-world clinical setting, there was no control group for comparison and the patient criteria relating to previous and concomitant medications were less stringent. Further, since this study was a postmarketing surveillance and its focus was on assessment of drug safety in routine clinical practice, effectiveness data were missing for several patients. In addition, in accordance with the study protocol, a substantial number of patients were excluded from the analyses. As a result, effectiveness analyses were conducted only in 310 of 511 patients who had registered in the study, which could be a limitation of this study. Moreover, very few patients were assessed for certain outcomes, such as EIMs, which may have introduced bias and limited the interpretation of results. Furthermore, we cannot exclude the possibility that observed case analysis may have caused overestimation of the remission rate since patients with favorable responses are more likely to continue treatment. Nevertheless, our study provides results of long-term adalimumab use in routine clinical practice in Japanese patients with CD and therefore offers useful additional insights into the safety and effectiveness of adalimumab.
The long-term safety profile of adalimumab in Japanese patients with CD in real-world settings was consistent with the existing profile, and no new safety concerns were identified. Further, the long-term effectiveness of adalimumab treatment was confirmed in Japanese patients with CD.
Footnotes
Funding Source
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
Hisamatsu T has received grants and personal fees from Mitsubishi Tanabe Pharma Corporation, EA Pharma Co. Ltd., AbbVie GK, JIMRO Co. Ltd., Zeria Pharmaceutical Co. Ltd., Kyorin Pharmaceutical Co. Ltd., Takeda Pharmaceutical Co. Ltd., Pfizer Japan Inc., and Mochida Pharmaceutical Co. Ltd.; grants from Asahi Kasei Kuraray Medical Co. Ltd., Daiichi Sankyo Co. Ltd., Nippon Kayaku Co. Ltd., and Astellas Pharma Inc.; and personal fees from Celgene, Janssen Pharmaceutical K.K., and Nichi-Iko Pharmaceutical Co. Ltd.
Suzuki Y has received honoraria from Takeda Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, AbbVie GK, EA Pharma Co. Ltd., Zeria Pharmaceutical Co. Ltd., Mochida Pharmaceutical Co. Ltd., and Kyorin Pharmaceutical Co. Ltd. and scholarship grants from Mitsubishi Tanabe Pharma Corporation, AbbVie GK, EA Pharma Co. Ltd., JIMRO Co. Ltd., Mochida Pharmaceutical Co. Ltd., Nippon Kayaku Co. Ltd., and Kissei Pharmaceutical Co. Ltd.
Kobayashi M, Hagiwara T, and Kawaberi T are employees of AbbVie GK.
Ogata H has received honoraria from Takeda Pharmaceutical Co. Ltd. and scholarship grants from Mitsubishi Tanabe Pharma Corporation, Mochida Pharmaceutical Co. Ltd., and Pfizer Japan Inc.
Matsui T has received honoraria from EA Pharma Co. Ltd., Ajinomoto Seiyaku, AbbVie GK, Eisai Co. Ltd., Kyorin Pharmaceutical Co. Ltd., Zeria Pharmaceutical Co. Ltd., Takeda Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, Mochida Pharmaceutical Co. Ltd., and Janssen Pharmaceutical K.K.; research grants from Takeda Pharmaceutical Co. Ltd., Miyarisan Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, and Otsuka Pharmaceutical Co. Ltd.; scholarship grants from AbbVie GK, Asahi Kasei Medical Co. Ltd., Astellas Pharma Inc., AstraZeneca K.K., EA Pharma Co. Ltd., Eisai Co. Ltd., MSD K.K., Otsuka Pharmaceutical Co. Ltd., JIMRO Co. Ltd., Zeria Pharmaceutical Co. Ltd., Taiho Pharmaceutical Co. Ltd., Daiichi Sankyo Co. Ltd., Takeda Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, Nippon Kayaku Co. Ltd., and Mochida Pharmaceutical Co. Ltd.; and was a recipient of endowed chairs funded by AbbVie GK, Asahi Kasei Medical Co. Ltd., Ajinomoto Seiyaku, Inflammatory Bowel Disease Advanced Clinical Treatment, Regional/Emergency Medical Management (Fukuoka), Eisai Co. Ltd., Otsuka Pharmaceutical Co. Ltd., Kyowa Hakko Kirin Co. Ltd., Kyorin Pharmaceutical Co. Ltd., JIMRO Co. Ltd., Zeria Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, UCB Japan Co. Ltd., EA Pharma Co. Ltd., Mochida Pharmaceutical Co. Ltd., and Chugai Pharmaceutical Co. Ltd.
Watanabe M has received honoraria from Mitsubishi Tanabe Pharma Corporation, Takeda Pharmaceutical Co. Ltd., EA Pharma Co. Ltd., Zeria Pharmaceutical Co. Ltd., Ajinomoto Seiyaku, and Eisai Co. Ltd.; research grants from Kaken Pharmaceutical Co. Ltd., Alfresa Pharma Corporation, and Eisai Co. Ltd.; scholarship grants from EA Pharma Co. Ltd., Zeria Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, Astellas Pharma Inc., MSD K.K., Daiichi Sankyo Co. Ltd., Taiho Pharmaceutical Co. Ltd., Takeda Pharmaceutical Co. Ltd., Nippon Kayaku Co. Ltd., Mochida Pharmaceutical Co. Ltd., Ayumi Pharmaceutical Corporation, Kissei Pharmaceutical Co. Ltd., and Miyarisan Pharmaceutical Co. Ltd.; and was a recipient of endowed chairs funded by Asahi Kasei Medical Co. Ltd., EA Pharma Co. Ltd., JIMRO Co. Ltd., Zeria Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, Kyorin Pharmaceutical Co. Ltd., AbbVie GK, Kyowa Hakko Kirin Co. Ltd., MSD K.K., Toray Industries, Inc., Chugai Pharmaceutical Co. Ltd., Gilead Sciences, Inc., and Fujirebio Inc.
Hibi T has received lecture fees from Aspen Japan K.K, AbbVie GK, Ferring Pharmaceuticals Co. Ltd., Gilead Sciences, Inc., Janssen Pharmaceutical K.K., JIMRO Co. Ltd., Kissei Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, Mochida Pharmaceutical Co. Ltd., Nippon Kayaku Co. Ltd., Pfizer Japan Inc., Takeda Pharmaceutical Co. Ltd., and Zeria Pharmaceutical Co. Ltd.; advisory/consultancy fees from AbbVie GK, Bristol-Myers Squibb Company, Celltrion, EA Pharma Co. Ltd., Eli Lilly Japan K.K., Gilead Sciences, Inc., Janssen Pharmaceutical K.K., Kyorin Pharmaceutical Co. Ltd., Mitsubishi Tanabe Pharma Corporation, Nichi-Iko Pharmaceutical Co. Ltd., Pfizer Japan Inc., Takeda Pharmaceutical Co. Ltd., and Zeria Pharmaceutical Co. Ltd.; research grants from AbbVie GK, EA Pharma Co. Ltd., JIMRO Co. Ltd., Otsuka Holdings Co. Ltd., and Zeria Pharmaceutical Co. Ltd.
Watanabe M and Hibi T are editorial board members of the journal but were not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Author Contribution
Conceptualization: Hisamatsu T, Kobayashi M, Hagiwara T. Methodology: Kobayashi M, Hagiwara T, Kawaberi T. Formal analysis: Kobayashi M, Hagiwara T, Kawaberi T. Supervision: Hisamatsu T, Hibi T. Writing - original draft: Kobayashi M. Writing - review and editing: Hisamatsu T, Suzuki Y, Kobayashi M, Hagiwara T, Kawaberi T, Ogata H, Matsui T, Watanabe M, Hibi T. Approval of final manuscript: all authors.
Others
The standard operation procedure manual for data management and transformation was developed by A2 Healthcare Corporation (Tokyo, Japan) and approved by the Postmarketing Surveillance group at AbbVie GK (Tokyo, Japan). This support was funded by the sponsors (AbbVie GK and Eisai Co., Ltd.). AbbVie GK participated in the study design; data collection; analysis and interpretation of data; and writing, reviewing, and approval of the publication. Medical writing support was provided by Avinash Thakur (Mumbai, India) and Nicola West (London, UK) of Cactus Life Sciences (a part of Cactus Communications) and funded by the sponsors.
The authors would like to thank Kazuo Morita and Kaori Hozumi, employees of AbbVie, for assistance.
REFERENCES
- 1.Rutgeerts P, Van Assche G, Sandborn WJ, et al. Adalimumab induces and maintains mucosal healing in patients with Crohn’s disease: data from the EXTEND trial. Gastroenterology. 2012;142:1102–1111. doi: 10.1053/j.gastro.2012.01.035. [DOI] [PubMed] [Google Scholar]
- 2.Lichtenstein GR, Loftus EV, Isaacs KL, Regueiro MD, Gerson LB, Sands BE. ACG clinical guideline: management of Crohn’s disease in adults. Am J Gastroenterol. 2018;113:481–517. doi: 10.1038/ajg.2018.27. [DOI] [PubMed] [Google Scholar]
- 3.Williams H, Walker D, Orchard TR. Extraintestinal manifestations of inflammatory bowel disease. Curr Gastroenterol Rep. 2008;10:597–605. doi: 10.1007/s11894-008-0108-6. [DOI] [PubMed] [Google Scholar]
- 4.Zippi M, Corrado C, Pica R, et al. Extraintestinal manifestations in a large series of Italian inflammatory bowel disease patients. World J Gastroenterol. 2014;20:17463–17467. doi: 10.3748/wjg.v20.i46.17463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Louis E, Löfberg R, Reinisch W, et al. Adalimumab improves patient-reported outcomes and reduces indirect costs in patients with moderate to severe Crohn’s disease: results from the CARE trial. J Crohns Colitis. 2013;7:34–43. doi: 10.1016/j.crohns.2012.02.017. [DOI] [PubMed] [Google Scholar]
- 6.Zeitz J, Ak M, Müller-Mottet S, et al. Pain in IBD patients: very frequent and frequently insufficiently taken into account. PLoS One. 2016;11:e0156666. doi: 10.1371/journal.pone.0156666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Feagan BG, Bala M, Yan S, Olson A, Hanauer S. Unemployment and disability in patients with moderately to severely active Crohn’s disease. J Clin Gastroenterol. 2005;39:390–395. doi: 10.1097/01.mcg.0000159220.70290.41. [DOI] [PubMed] [Google Scholar]
- 8.Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2018;390:2769–2778. doi: 10.1016/S0140-6736(17)32448-0. [DOI] [PubMed] [Google Scholar]
- 9.Ng WK, Wong SH, Ng SC. Changing epidemiological trends of inflammatory bowel disease in Asia. Intest Res. 2016;14:111–119. doi: 10.5217/ir.2016.14.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Japan Intractable Diseases Information Center Crohn’s disease [Internet]. [cited 2019 Jul 4]. http://www.nanbyou.or.jp/entry/81.
- 11.Murakami Y, Nishiwaki Y, Oba MS, et al. Estimated prevalence of ulcerative colitis and Crohn’s disease in Japan in 2014: an analysis of a nationwide survey. J Gastroenterol. 2019;54:1070–1077. doi: 10.1007/s00535-019-01603-8. [DOI] [PubMed] [Google Scholar]
- 12.Colombel JF, Sandborn WJ, Rutgeerts P, et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: the CHARM trial. Gastroenterology. 2007;132:52–65. doi: 10.1053/j.gastro.2006.11.041. [DOI] [PubMed] [Google Scholar]
- 13.Sandborn WJ, Hanauer SB, Rutgeerts P, et al. Adalimumab for maintenance treatment of Crohn’s disease: results of the CLASSIC II trial. Gut. 2007;56:1232–1239. doi: 10.1136/gut.2006.106781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sandborn WJ, Rutgeerts P, Enns R, et al. Adalimumab induction therapy for Crohn disease previously treated with infliximab: a randomized trial. Ann Intern Med. 2007;146:829–838. doi: 10.7326/0003-4819-146-12-200706190-00159. [DOI] [PubMed] [Google Scholar]
- 15.Panaccione R, Colombel JF, Sandborn WJ, et al. Adalimumab maintains remission of Crohn’s disease after up to 4 years of treatment: data from CHARM and ADHERE. Aliment Pharmacol Ther. 2013;38:1236–1247. doi: 10.1111/apt.12499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Colombel JF, Sandborn WJ, Reinisch W, et al. Long-term safety of adalimumab in clinical trials in adult patients with Crohn’s disease or ulcerative colitis. Aliment Pharmacol Ther. 2018;47:219–228. doi: 10.1111/apt.14420. [DOI] [PubMed] [Google Scholar]
- 17.Burmester GR, Panaccione R, Gordon KB, McIlraith MJ, Lacerda AP. Adalimumab: long-term safety in 23 458 patients from global clinical trials in rheumatoid arthritis, juvenile idiopathic arthritis, ankylosing spondylitis, psoriatic arthritis, psoriasis and Crohn’s disease. Ann Rheum Dis. 2013;72:517–524. doi: 10.1136/annrheumdis-2011-201244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.D’Haens G, Reinisch W, Panaccione R, et al. Lymphoma risk and overall safety profile of adalimumab in patients with Crohn’s disease with up to 6 years of follow-up in the PYRAMID registry. Am J Gastroenterol. 2018;113:872–882. doi: 10.1038/s41395-018-0098-4. [DOI] [PubMed] [Google Scholar]
- 19.Watanabe M, Hibi T, Lomax KG, et al. Adalimumab for the induction and maintenance of clinical remission in Japanese patients with Crohn’s disease. J Crohns Colitis. 2012;6:160–173. doi: 10.1016/j.crohns.2011.07.013. [DOI] [PubMed] [Google Scholar]
- 20.Watanabe M, Hibi T, Mostafa NM, et al. Long-term safety and efficacy of adalimumab in Japanese patients with moderate to severe Crohn’s disease. J Crohns Colitis. 2014;8:1407–1416. doi: 10.1016/j.crohns.2014.04.012. [DOI] [PubMed] [Google Scholar]
- 21.Ogata H, Watanabe M, Matsui T, et al. Safety of adalimumab and predictors of adverse events in 1693 Japanese patients with Crohn’s disease. J Crohns Colitis. 2016;10:1033–1041. doi: 10.1093/ecco-jcc/jjw060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pharmaceuticals and Medical Devices Agency New drugs approved in FY 2016 [Internet]. c2017 [cited 2020 Oct 16]. https://www.pmda.go.jp/english/review-services/reviews/approved-information/drugs/0002.html.
- 23.Loftus EV, Reinisch W, Panaccione R, et al. Adalimumab effectiveness up to six years in adalimumab-naïve patients with Crohn’s disease: results of the PYRAMID Registry. Inflamm Bowel Dis. 2019;25:1522–1531. doi: 10.1093/ibd/izz008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Navarra SV, Tang B, Lu L, et al. Risk of tuberculosis with antitumor necrosis factor-α therapy: substantially higher number of patients at risk in Asia. Int J Rheum Dis. 2014;17:291–298. doi: 10.1111/1756-185X.12188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tanaka H, Kamata N, Yamada A, et al. Long-term retention of adalimumab treatment and associated prognostic factors for 1189 patients with Crohn’s disease. J Gastroenterol Hepatol. 2018;33:1031–1038. doi: 10.1111/jgh.14034. [DOI] [PubMed] [Google Scholar]
- 26.Matsumoto T, Motoya S, Watanabe K, et al. Adalimumab monotherapy and a combination with azathioprine for Crohn’s disease: a prospective, randomized trial. J Crohns Colitis. 2016;10:1259–1266. doi: 10.1093/ecco-jcc/jjw152. [DOI] [PubMed] [Google Scholar]
- 27.Hisamatsu T, Matsumoto T, Watanabe K, et al. Concerns and side effects of azathioprine during adalimumab induction and maintenance therapy for Japanese patients with Crohn’s Disease: a subanalysis of a prospective randomised clinical trial [DIAMOND Study] J Crohns Colitis. 2019;13:1097–1104. doi: 10.1093/ecco-jcc/jjz030. [DOI] [PubMed] [Google Scholar]
- 28.Louis EJ, Reinisch W, Schwartz DA, et al. Adalimumab reduces extraintestinal manifestations in patients with Crohn’s disease: a pooled analysis of 11 clinical studies. Adv Ther. 2018;35:563–576. doi: 10.1007/s12325-018-0678-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Peyrin-Biroulet L, Reinisch W, Colombel JF, et al. Clinical disease activity, C-reactive protein normalisation and mucosal healing in Crohn’s disease in the SONIC trial. Gut. 2014;63:88–95. doi: 10.1136/gutjnl-2013-304984. [DOI] [PubMed] [Google Scholar]
- 30.Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting therapeutic targets in inflammatory bowel disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol. 2015;110:1324–1338. doi: 10.1038/ajg.2015.233. [DOI] [PubMed] [Google Scholar]
- 31.MacKalski BA, Bernstein CN. New diagnostic imaging tools for inflammatory bowel disease. Gut. 2006;55:733–741. doi: 10.1136/gut.2005.076612. [DOI] [PMC free article] [PubMed] [Google Scholar]