

Abstract
Background:
Bertolotti’s syndrome (i.e., varying extent of fusion between the last lumbar vertebra and the first sacral segment) or lumbosacral transitional vertebrae is a rare cause of back pain. Notably, this syndrome is one of the differential diagnoses for patients with refractory back pain/sciatica.
Case Description:
A 71-year-old male presented with low back pain of 3 years duration that radiated into the right lower extremity resulting in numbness in the L5 distribution. He then underwent a minimally invasive approach to resect the L5 “wide” transverse process following the CT diagnosis of Bertolotti’s syndrome. Prior to surgery, patient reported pain that was exacerbated by ambulation that resolved post-operative.
Conclusion:
Bertolotti’s syndrome is one of the rare causes of sciatica that often goes undiagnosed. Nevertheless, it should be ruled out for patients with back pain without disc herniations or other focal pathology diagnosed on lumbar MR scans.
Keywords: Anatomical variation, Back pain, Bertolotti’s syndrome, Spinal anomaly, Transitional vertebrae

INTRODUCTION
Bertolotti’s syndrome also called lumbosacral transitional vertebrae rarely cause low back pain. The syndrome is defined by fusion between the last lumbar vertebra and the first sacral segment to varying degrees.
Here, we present a 71-year-old male with refractory back pain due to Bertolotti’s syndrome who did well following a minimally invasive resection of L5 (i.e., wide transverse process resection).
CASE PRESENTATION
A 71-year-old male presented with 3 years of low back and right lower extremity pain with accompanying numbness. Bertolotti’s syndrome was diagnosed on a preoperative CT scan. that showed a transitional vertebra at the lumbosacral spine junction (i.e., labeled as a partially lumbarized S1 with pseudoarthrosis on the right side [Figures 1a, b and 2].
Figure 1:
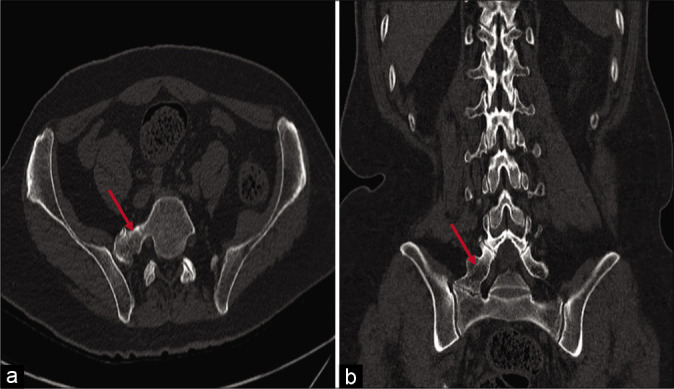
(a and b) Axial and coronal CT lumbosacral spine showing the l5 wide transverse process with a bony ridge connecting the l5 to the sacrum. (Red arrow).
Figure 2:
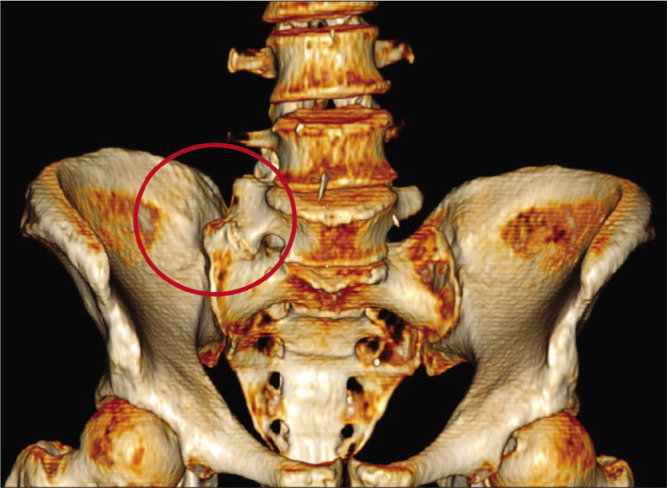
3D reconstruction of the lumbosacral spine showing the l5 wide transverse process with a bony ridge connecting the l5 to the sacrum. (Red circle).
He underwent a minimally invasive “wide” L5 transverse process resection for decompression of the right L5 nerve root (i.e., a bony ridge was found below the muscle extending from the transverse process of L5 to sacral ala). Using a drill and Kerrison rongeurs, the excess bone was removed from the transverse process superiorly to sacral ala inferiorly, and from the L5 pedicle medially all the way laterally. Postoperatively, the patient reported full resolution of his pain and radiculopathy.
DISCUSSION
Bertolotti’s syndrome (i.e., lumbosacral transitional vertebrae), is a morphological variation or a congenital spinal anomaly. It typically occurs when an elongated transverse process of the last lumbar vertebra fuses to the first sacral segment (i.e, to varying degrees).[2] It ranges from partial to complete L5 sacralization, and partial to complete S1 lumbarization.[2]
The diagnosis is often missed on X-rays alone, and may even not be recognized on either MRI or CT scans.[3] Bertolotti’s syndrome showed to encounter longer work up and received more epidural steroid injections whereby they were found out to have worse physical and mental health scores.[1] Notably, recognizing this anatomic variant becomes particularly important in patients complaining of sciatica without disc herniations or other clear pathology on MRI/CT studies.
CONCLUSION
Bertolotti’s syndrome, defined as typically involving an elongated transverse process of the last lumbar vertebra fused to differing degrees to the first sacral segment, is a rare cause of back pain/sciatica. Notably, it should be more readily diagnosed utilizing MR, and/or CT studies as it may be readily remediated with surgery.
Footnotes
How to cite this article: Kawtharani S, Bsat SA, El Housheimy M, Moussalem C, Halaoui A, Sunna T. A case of Bertolotti’s syndrome as a cause of sciatica. Surg Neurol Int 2021;12:516.
Contributor Information
Sarah Kawtharani, Email: sk194@aub.edu.lb.
Shadi Abdelatif Bsat, Email: sb86@aub.edu.lb.
Mohamad El Housheimy, Email: me179@aub.edu.lb.
Charbel Moussalem, Email: cm48@aub.edu.lb.
Adham Halaoui, Email: ah289@aub.edu.lb.
Tarek Sunna, Email: ts18@aub.edu.lb.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Publication of this article was made possible by the James I. and Carolyn R. Ausman Educational Foundation.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Golubovsky JL, Momin A, Thompson NR, Steinmetz MP. Understanding quality of life and treatment history of patients with Bertolotti syndrome compared with lumbosacral radiculopathy. J Neurosurg Spine. 2019;1:1–7. doi: 10.3171/2019.2.SPINE1953. [DOI] [PubMed] [Google Scholar]
- 2.Jancuska JM, Spivak JM, Bendo JA. A review of symptomatic lumbosacral transitional vertebrae: Bertolotti’s syndrome. Int J Spine Surg. 2015;9:42. doi: 10.14444/2042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.McGrath K, Schmidt E, Rabah N, Abubakr M, Steinmetz M. Clinical assessment and management of Bertolotti syndrome: A review of the literature. Spine J. 2021;21:1286–96. doi: 10.1016/j.spinee.2021.02.023. [DOI] [PubMed] [Google Scholar]