

Abstract
Objectives
This study evaluated and compared the effect of silver diamine fluoride (SDF) and silver-modified atraumatic restorative treatment (SMART) sealants for the treatment of initial carious lesions of permanent molars affected by molar incisor hypomineralization (MIH).
Methods
One hundred and twelve hypomineralized permanent molars with ICDAS 1 or 2 lesions were selected in 48 children. The teeth were randomized into SDF and SMART sealant groups (n = 56 teeth/group) in a split-mouth fashion. Hypersensitivity, formation of caries, and enamel breakdown were evaluated in both groups. Hypersensitivity was assessed by Schiff Cold Air Sensitivity Scale (SCASS), and clinical assessments of SMART sealants were performed according to modified USPHS criteria at 1, 6, and 12 months. The data were analyzed statistically using Fisher’s exact test, Kaplan–Meier analysis, Mann–Whitney U test, and Friedman test.
Results
Twenty-six hypomineralized molars with marked baseline hypersensitivity showed significantly lower SCASS scores at all evaluation periods (p < 0.001). There was no significant difference in hypersensitivity scores between the groups at the repeated applications of SDF at 1, 6, and 12 months. The cumulative survival rates of SMART sealants on occlusal and palatal surfaces were 88.7% and 58.8%, respectively.
Conclusions
In hypomineralized molars, both SDF and SMART sealants showed favorable short-term prevention against dental caries while providing effective desensitization. Marginal discoloration was the most common side effect of the SMART sealants as a result of SDF application.
Clinical Significance
Both SDF and SMART sealants showed similar short-term effectiveness as non-aerosol procedures in arresting enamel caries and reducing hypersensitivity in hypomineralized molars.
Trial registration
Clinical Trials Registration Number: NCT03862014.
Keywords: Clinical trials, Dental caries, Molar incisor hypomineralization, Prevention, Silver diamine fluoride
Introduction
Molar incisor hypomineralization (MIH) is defined as a developmental defect of the enamel with a clinical view of enamel hypomineralization affecting one or more first permanent molars that are associated frequently with affected incisors [1]. Its prevalence varies from 20 to 40%, depending on the population studied and diagnostic criteria used [2, 3]. Clinically, MIH is characterized by well-demarcated opacities ranging from white/creamy to yellow/brown, occasionally in combination with (post-eruptive) enamel breakdown on affected teeth [4]. Histologically, these opacities are more porous and are mostly located in the inner part of the enamel [5].
Children with MIH present several clinical problems, including rapid tooth wear and enamel loss, increased caries risk and consequent treatment need, loss of fillings, and eventually tooth loss [6]. The porous sub-surface enamel and the dentine in affected teeth could be exposed by post-eruptive breakdown, resulting the teeth being sensitive to cold air, water, and even tooth brushing [1]. Affected molars are nearly 10 times more prone to caries than normal teeth and can be difficult to anesthetize and to restore [7].
Several non-invasive and minimally invasive procedures have been proposed as preventive measures against caries in hypomineralized molars [8]. Silver diamine fluoride (SDF) is an effective agent for stabilizing active caries lesions by virtue of the remineralizing effect of fluoride and the antibacterial properties of silver. SDF is non-invasive and preserves tooth structure when used as a single chemotherapeutic option or in combination with glass ionomer cements for caries management [9, 10]. SDF also provides profound, long-lasting relief of hypersensitivity, since it can block dentinal tubules by producing fluorohydroxyapatite and increasing mineral density and hardness [11]. Indeed, the product was cleared by the US Food and Drug Administration (FDA) in 2014 for the treatment of dentinal hypersensitivity. Several SDF products have been introduced due to its increased popularity over the time. A commercial product (Riva Star, SDI, Bayswater, Australia), consisting of 30–35% SDF and a saturated solution of potassium iodide (KI), has been introduced for the treatment of hypersensitive dentine [12]. Knight et al. [13] reported that KI could further reduce dentin permeability when it was applied after silver diamine fluoride.
SMART (silver-modified atraumatic restorative treatment) is a technique in which a carious lesion is treated first with SDF and then sealed/restored with a conventional or high viscosity glass ionomer cement (HVGIC) [14–17]. HVGICs bond to dental hard tissues via chemical and micromechanical adhesion and release fluoride which might help reduce biofilm formation and recurrent caries. Grossi et al. [8] reported a survival rate of 98% for HVGIC restorations on first permanent molars affected by MIH placed with atraumatic restorative technique (ART).
There is no consensus regarding the best restorative option for MIH in the dental literature. SMART is an ultraconservative treatment option for MIH, and currently only one case study [11] has reported the use this technique on MIH-affected molars. The SMART technique utilizes SDF to inhibit the cariogenic biofilm formation [18] and reduce hypersensitivity [19], while sealing over with glass ionomer can enhance tissue remineralization, inhibit the biofilm formation, and provide a cleansable surface. As an additional benefit, the glass ionomer can also mask the black stain caused by the SDF.
The present study was conducted to evaluate and compare the clinical effect of SDF and SDF + atraumatic restorative technique (SMART) in MIH-affected molars. This study tested the null hypothesis that there is no difference in the preventive and desensitizing performance of SDF and SMART restorations placed in hypomineralized permanent molars.
Materials and methods
This randomized, prospective study was approved by the Local Ethics Committee (Reg. no: KA-190033) and was conducted in strict adherence to the 2010 CONSORT statement [20]. The study protocol was registered on ClinicalTrials (NCT03862014). All parents/guardians were asked to sign an informed consent after thorough explanation of the procedures and possible outcomes of treatment. Children were excluded from the study when their parents declined to sign the form.
Selection of participants
The participants were recruited from patients attending to the Pediatric Dentistry Clinic at the Hacettepe University School of Dentistry in Ankara.
The inclusion criteria of the study were as follows:
6–13-year-old healthy children with at least two fully erupted permanent first molars diagnosed with MIH according to the European Academy of Paediatric Dentistry (EAPD) criteria [21]
Hypomineralized first molars with enamel defects (codes; the International Caries Detection and Assessment System (ICDAS) 1, 2) according to ICDAS II
The exclusion criteria were as follows:
Ongoing orthodontic treatment
Lack of cooperation for dental procedures
Teeth with ICDAS 3, 4, 5, 6 lesions, existing restorations, fluorosis, or enamel malformation due to specific syndromes.
The presence of pulpal symptoms
Sample size could not be determined since there is no previous study that evaluated the retention rates of GIC sealants placed after SDF application, secondary caries rates along SMART margins, and tooth sensitivity after SDF and SMART application.
Study design
This was a prospective randomized, controlled study, carried out in a split-mouth design. Operator and patient blinding were not possible due to the application procedures of study groups. All treatments were made by two experienced, calibrated pediatric dentists. Randomization was obtained with a contingency number table on www.random.org and preserved in sequentially numbered, sealed envelopes.
Baseline assessments
Tooth surfaces were professionally cleaned with a slow-speed rotary brush and air-dried before assessments using the ICDAS II index [22]. Only early enamel caries lesions (ICDAS 1, 2) were assessed by visual/tactile examination, and without radiographs.
The DMFT/dmft values (decayed, missed, filled teeth) of the patients were assessed according to the World Health Organization (WHO) evaluation criteria. The diagnosis of MIH was established in the presence of demarcated opacities/post-eruptive enamel breakdown in at least one first permanent molar as per the EAPD criteria. Demarcated opacities with a diameter < 2 mm was not included in the study [23].
Schiff Cold Air Sensitivity Scale (SCASS) [24] was used to assess the presence of hypersensitivity in affected teeth by applying an air blast perpendicularly on the occlusal surface of the tooth for 1 s at a distance of 1 cm. The patient’s response was recorded according to the following scores: 0 = subject does not respond to the stimulus; 1 = subject does not respond to the stimulus but considers stimulus to be painful; 2 = subject responds to air stimulus and moves from the stimulus, and 3 = subject responds to air stimulus, moves from the stimulus, and requests immediate cease of the stimulus.
Clinical procedures
Following rubber dam isolation, the crowns were cleaned with a slow-speed rotary bristle brush, rinsed with water spray, and dried with air spray. The teeth were randomly assigned to one of the following groups (n = 56/group): group 1, SDF application only (Riva Star), and group 2, SDF (Riva Star) + ART (SMART) with HVGIC (Equia Forte®, GC Europe, Leuven, Belgium). In both groups, Riva Star was applied as follows: the SDF (gray) vial was perforated with the blunt end of a micro-brush applicator, and SDF was applied on the entire tooth surface using the brush. Then, the KI (green) vial was applied over the tooth surfaces as with the SDF vial. The white precipitate occurring after KI application was rinsed off with copious water spray. In the SMART group, the tooth was blot-dried with cotton pellets, after rinsing off of the KI with water. Finally, the HVGIC capsule was mixed according to the manufacturer’s instructions and then injected over the pits and fissures using the applicator tip. ART sealants were gently adapted under finger pressure [25]. The excess material was quickly removed, and the occlusion was checked and adjusted (if necessary) after removing the rubber dam. The HVGIC was sealed with the resin surface sealant (Equia Coat®, GC, Leuven, Belgium) and light-cured for 20 s.
The United States Public Health Service (USPHS) clinical rating system [26] was used for clinical evaluation of the SMART sealants at baseline and at 1, 6, and 12 months. Digital photographs of teeth were obtained directly after treatment (baseline) and at control appointments, using an EOS 600D camera, ring flash, and 100-mm macro lens (all Canon, Tokyo, Japan) at a standardized 1:1.2 magnification and manual parameters (ISO 200, T:1/200, F:22). The photographs were used to evaluate discoloration and seconder caries under magnification (Fig. 1). At each recall period, the retention of SMART sealants was evaluated clinically by using a calibrated right-angled dental explorer with a tip thickness of 250 μm after removing the plaque and debris with a gauze and air-drying. When one or more Charlie score was present, the sealant was recorded as failure, and the tooth was excluded from the study. When those teeth had no visible sign of caries under the lost sealant, they were scheduled for regular controls and SDF&KI application. If a new caries lesion was identified, the tooth was restored.
Fig. 1.

Clinical intra-oral photos of the teeth in SDF and SMART groups at all time points. Intra-oral photos of the teeth: a at baseline with/without rubber dam, b after SDF application, c after SMART restoration, d at 1 month, e at 6 months, f at 12 months
At 6 and 12 months, all teeth in group 1 (SDF only) received SDF&KI application under rubber dam isolation. In all control visits, the air blast stimuli was reapplied before SDF applications in both groups, and the SCASS score was recorded.
Statistical analysis
The results were analyzed by using SPSS 23.0 software (SPSS Inc., Chicago, IL, USA). The difference between the measurements of two independent groups (SDF and SMART) at different times was examined using the Mann–Whitney U Test, and the difference between the dependent groups (comparing different time points with each other) was examined by Friedman Test. Kaplan–Meier analysis was used to evaluate the cumulative survival rates of SMART sealants.
Intra- and inter-examiner reliability was calculated using Cohen’s kappa test. The intra-examiner reliability for determining the presence of MIH was 0.87 and 0.89, respectively, and inter-examiner reliability was 0.87. In case of disagreement, a consensus scoring was made. The intra-examiner reliability for USPHS-modified criteria was 0.90. For all statistical tests, p < 0.05 was considered statistically significant.
Results
A total of 56 patients (62% girls and 38% boys) with a mean age of 8.8 ± 1.58 years were included in the SDF group (n = 56) and SMART group (n = 56). Three patients (6 teeth) were lost to follow-up, and 53 patients with 106 teeth (91 first molars and 15 s molars) were available for evaluations through the 12-month follow-up. The recruitment and flow diagram of patients are presented in Fig. 2. The mean dmft of all patients was 4.1 ± 3.39.
Fig. 2.

Flow diagram of participants up to 1 year
Over the 12-month follow-up period, none of the teeth presented as failure in regard to secondary caries, marginal discoloration, or marginal adaptation. Therefore, those three parameters were not included in the statistical analyses. Table 1 shows a summary of clinical evaluations using the modified USPHS criteria and retention rates for occlusal and palatal surfaces. The cumulative survival rates at 12 months were 88.7% for occlusal surfaces and 58.8% for the palatal surfaces.
Table 1.
Clinical performance of SMART sealants according to the modified USPHS criteria for occlusal and palatal surfaces. A = Alpha, B = Bravo, C = Charlie
| Criteria | Score | Baseline | Follow-up | ||
|---|---|---|---|---|---|
| 1 month n (%) |
6 months n (%) |
12 months n (%) |
|||
| Marginal adaptation | |||||
| A | 53 | 40 (75.5) | 15 (28.3) | 10 (18.9) | |
| B | - | 13 (24.5) | 34 (64.2) | 37 (69.8) | |
| C | - | - | - | - | |
| Marginal discoloration | |||||
| A | 53 | 31 (58.5) | 16 (32.7) | 6 (12.7) | |
| B | - | 22 (41.5) | 33 (67.3) | 41 (87.2) | |
| C | - | - | - | - | |
| Anatomic form (occlusal) | |||||
| A | 53 | 47 | 31 (58.5) | 19 (38.8) | |
| B | - | 6 (11.3) | 18 (33.9) | 28 (57.1) | |
| C | - | - | 4 (7.5) | 2 (4.1) | |
| Total | 53 (100) | 49 (92.5) | 47 (88.7) | ||
| Anatomic form (palatal) | |||||
| A | 34 | 30 (88.2) | 20 (58.8) | 17 (50) | |
| B | - | 1 (2.9) | 2 (5.8) | 2 (5.8) | |
| C | - | 3 (8.8) | 9 (26.5) | 2 (5.8) | |
| Total | 31 (91.1) | 22 (64.7) | 20 (58.8) | ||
Intra-examiner agreement was not determined for the air-blast test. The test scores (Schiff score) of the SDF and SMART groups are presented in Table 2. Twenty-six molars (13 patients), which presented with hypersensitivity, were included for statistical analysis. There was no significant difference between the hypersensitivity levels of SDF and SMART groups at any recall period (Mann–Whitney U test, p = 1.000, p = 0.801, p = 0.762, p = 0.762, respectively). The hypersensitivity scores were significantly higher at baseline compared to other time points (Fig. 3, Friedman test, p < 0.001). The hypersensitivity scores at 1-, 6-, and 12-month recalls were similar (p > 0.05).
Table 2.
The distributions of the air blast test scores (Schiff score) for SDF and SMART groups at baseline and controls
| Time | SDF (13 patients, 13 teeth) | SMART (13 patients, 13 teeth) | Z | p* | ||||
|---|---|---|---|---|---|---|---|---|
| Median (IQR) | Mean ± SD | Min–max | Median (IQR) | Mean ± SD | Min–max | |||
| Baseline | 2.00–1.00 | 1.77 ± 0.83 | 1.00–3.00 | 2.00–1.00 | 1.77 ± 0.83 | 1.00–3.00 | 0.000 | 1.000 |
| 1th month | 0.00–0.00 | 0.38 ± 0.77 | 0.00–2.00 | 0.00–1.00 | 0.46 ± 0.78 | 0.00–2.00 | − 0.362 | 0.801 |
| 6th month | 0.00–0.00 | 0.15 ± 0.38 | 0.00–1.00 | 0.00–0.00 | 0.08 ± 0.28 | 0.00–1.00 | − 0.602 | 0.762 |
| 12th month | 0.00–0.00 | 0.15 ± 0.38 | 0.00–1.00 | 0.00–0.00 | 0.08 ± 0.28 | 0.00–1.00 | − 0.602 | 0.762 |
*Mann–Whitney U test
Fig. 3.
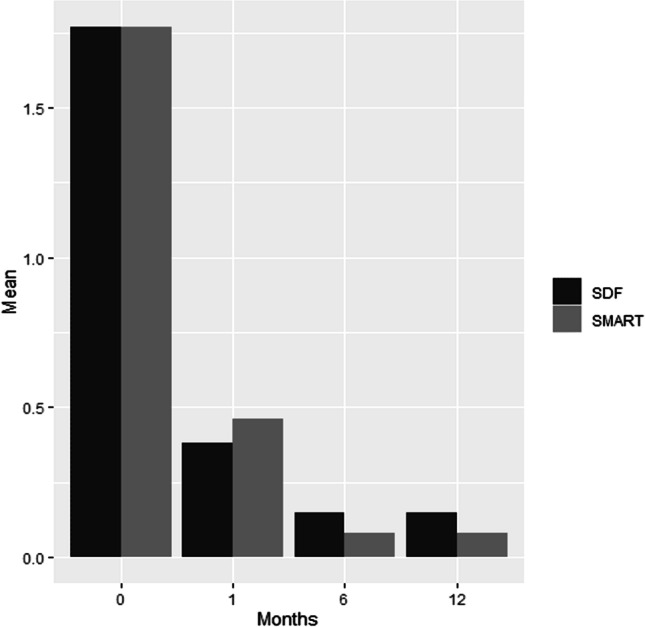
Air blast test scores (Schiff score) of the hypersensitive molars (n = 26) during the study period
Discussion
Both SDF and SDF + glass ionomer cement have the potential to prevent dental caries and treat hypersensitivity in hypomineralized young permanent teeth. To the best of our knowledge, this is the first clinical study that evaluated and compared the clinical effectiveness of SDF and SMART sealant techniques on MIH-affected molars with initial enamel lesions. The use of SDF for hypomineralized teeth has been proposed in a few articles [11, 27], but no clinical trial has been published so far.
In hypomineralized enamel, porosity is known to be more severe in yellow/brown defects [5]. These pores are sufficiently large to enable bacterial adhesion and invasion, even on apparently intact surfaces [28], and thus require special attention to avoid further pulpal complications [29]. Mild carious lesions may also present with tissue breakdown over the time due to invasion of cariogenic bacteria into the defective enamel and dentin [28]. In the present study, two teeth with brown discoloration from each group showed such breakdown at the 12-month recall. As no dental caries was present, the defects were re-treated with SDF and restored with glass hybrid restorative system, regardless of the study group.
Restoration of hypomineralized teeth is challenging, and adhesive resin restorations have shown poor retention rates on MIH-affected molars, irrespective of the bonding strategy [30–33]. Glass hybrid restorations seem more promising in adhesion to MIH-affected molars, with reported high short-term retention rates [8, 34]. Unlike direct restorations, the retention of ART sealants should be evaluated exclusively, since the cavity design plays a crucial role for retention. Owing to the lack of studies on ART sealants in MIH-affected molars, a comparison can only be made with the studies that investigated ART sealants on healthy molars. Hilgert et al. [34] applied composite resin (CR) sealants and ART sealants with high viscosity glass-ionomer cement to the occlusal surface of first permanent molars in school children and reported 1-year cumulative survival rates of 91.6% and 82.2% for CR and ART sealants, respectively. A recent meta-analysis [35] reported a 78.7% 1-year survival of retained ART sealants in permanent molars. Although it is logical to anticipate lower retention of ART sealants here due to the presence of hypomineralized enamel, the higher retention rates (88.7%) compared to the latter study may be attributed to strict isolation measures using the rubber dam. It should also be emphasized that the evaluation criteria (USPHS vs ART criteria) has no significant impact on survival outcomes [36, 37]. In fact, the failure criteria are more stringent in the ART criteria compared to that of the USPHS.
The major drawback of SDF is the irreversible dark staining of demineralized tooth surfaces, cavitated lesions, and restoration margins. While application of KI immediately after SDF may reduce the staining to a large extent, restoration margins may still remain stained [38]. The intensity of the discoloration has been reported to be less in SDF&KI compared to SDF alone [39]. In present study, only 6 SMART sealants had no marginal discoloration after 12 months. Marginal discoloration of restorations can result from poor marginal adaptation or adhesive degradation and may be indicative of microleakage and secondary caries [40]. In the present study, however, the marginal discoloration was an expected outcome of prior SDF application, rather than being an indicator of failure. Moreover, exposure of SDF to curing light source affects discoloration significantly [41]. Equia requires immediate isolation with its light-cured resin coating, which increases the staining effect of SDF and in turn marginal discoloration.
In the present study, 26 of 106 hypomineralized molars showed hypersensitivity as verified by the air blast test. Products containing arginine and calcium carbonate or casein phosphopeptide amorphous calcium phosphate (CPP-ACP) have been evaluated for the management of hypersensitivity in MIH-affected teeth and have shown successful outcomes [42, 43].
SDF reacts with calcium and phosphate ions within tooth structure to produce fluorohydroxyapatite [44], which precipitates over the tooth and ensures reduced solubility. The alkalinity of SDF also favors production of fluorohydroxyapatite, which may further promote the precipitation process. SDF has been tested clinically as a tooth desensitizer with reported short-term effects [45], but its use in management of hypersensitivity in hypomineralized molars has not been studied previously. The frequency of application and the longevity of the effect may be important for determining whether a single application or repeated applications are needed to manage hypersensitivity in MIH-affected molars. Although the optimal frequency of application SDF is not known, it is commonly applied once a year or every 6 months for caries arrest [46]. It was reported that increasing the frequency of application from annually to semiannually can increase the rate of caries arrest in children with poor oral hygiene [47]. In the present study, both groups showed a significant relief 1 month after the SDF application. As for the repeated applications at 6 and 12 months, there was no significant difference in sensitivity scores compared to the first month, indicating that a single application of SDF can provide sufficient initial relief in most teeth with hypersensitivity and that repeated applications of SDF to maintain caries prevention may also prolong the desensitizing effect.
In the present study, the regular follow-up visits and repeated SDF applications were conducted during the COVID-19 pandemic. Both the nature of treatments and repeated applications of SDF provided an effective, non-aerosol treatment approach during the ongoing pandemic conditions. Our favorable short-term results encourage these minimally invasive, non-aerosol procedures for preventing development of caries in MIH-affected molars for school children under field conditions, for patients with dental phobia, and for patients with hypersensitive MIH-affected molars that are unresponsive to achieving profound local anesthesia.
The results of the present study should be assessed along with its limitations. Here, the color, size, and location of hypomineralized lesions showed variations. Future clinical trials should evaluate the effect of SDF and the survival of SMART sealants over standardized lesions. The survival of SMART sealants to healthy but at high caries risk molars should also be assessed along with an SDF-only group. Nevertheless, the present results are encouraging and provide a favorable short-term outcome of SDF and SMART approaches in MIH-affected, hypersensitive young permanent molars.
Conclusions
Hybrid glass ionomer sealants placed immediately after SDF application showed a reasonable retention rate of 88.7% in hypomineralized molars with incipient lesions. Both SDF application alone and SMART sealants showed similar 1-year clinical effectiveness, necessitating acceptance of the null hypothesis. Marginal discoloration associated with prior SDF application at the same visit was the most common drawback of SMART sealants. SDF application continued by repeated applications, and SMART sealants provided a significant level of desensitization.
Funding
This study was funded by the Hacettepe University Scientific Research Projects Coordination Unit (Grant No: THD-2019–18001).
Declarations
Conflict of interest
The authors declare no competing interests.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Weerheijm KL. Molar incisor hypomineralisation (MIH) Eur J Paediatr Dent. 2003;4:115–120. [PubMed] [Google Scholar]
- 2.Weerheijm KL, Duggal M, Mejare I, Papagiannoulis L, Koch G, Martens LC, Hallonsten AL. Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: a summary of the European meeting on MIH held in Athens, 2003. Eur J Paediatr Dent. 2003;4:110–113. [PubMed] [Google Scholar]
- 3.Cabral RN, Nyvad B, Soviero VLVM, Freitas E, Leal SC. Reliability and validity of a new classification of MIH based on severity. Clin Oral Investig. 2019;24:727–734. doi: 10.1007/s00784-019-02955-4. [DOI] [PubMed] [Google Scholar]
- 4.Da Costa-Silva CM, Ambrosano GM, Jeremias F, De Souza JF, Mialhe FL. Increase in severity of molar–incisor hypomineralization and its relationship with the colour of enamel opacity: a prospective cohort study. Int J Paediatr Dent. 2011;21:333–341. doi: 10.1111/j.1365-263X.2011.01128.x. [DOI] [PubMed] [Google Scholar]
- 5.Jälevik B, Norén JG. Enamel hypomineralization of permanent first molars: a morphological study and survey of possible aetiological factors. Int J Paediatr Dent. 2000;10:278–289. doi: 10.1046/j.1365-263x.2000.00210.x. [DOI] [PubMed] [Google Scholar]
- 6.Pitiphat W, Savisit R, Chansamak N, Subarnbhesaj A. Molar incisor hypomineralization and dental caries in six-to seven-year-old Thai children. Pediatr Dent. 2014;36:478–482. [PubMed] [Google Scholar]
- 7.Jalevik B, Klingberg GA. Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent first molars. Int J Paediatr Dent. 2002;12:24–32. doi: 10.1046/j.0960-7439.2001.00318.x. [DOI] [PubMed] [Google Scholar]
- 8.de Aguiar Grossi J, Cabral RN, Ribeiro APD, Leal SC. Glass hybrid restorations as an alternative for restoring hypomineralized molars in the ART model. BMC Oral Health. 2018;18:65. doi: 10.1186/s12903-018-0528-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhao IS, Gao SS, Hiraishi N, Burrow MF, Duangthip D, Mei ML, Lo ECM, Chu CH. Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int Dent J. 2018;68:67–76. doi: 10.1111/idj.12320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Horst JA, Ellenikiotis H, Milgrom PM, Committee USCA. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications, and consent. J Calif Dent Assoc. 2016;44:16. [PMC free article] [PubMed] [Google Scholar]
- 11.MacLean J. Minimally invasive treatment for molar incisor hypomineralization. J Multidiscip Care Decis Dent. 2018;4:18–23. [Google Scholar]
- 12.Hamama H, Yiu C, Burrow M. Effect of silver diamine fluoride and potassium iodide on residual bacteria in dentinal tubules. Aust Dent J. 2015;60:80–87. doi: 10.1111/adj.12276. [DOI] [PubMed] [Google Scholar]
- 13.Knight G, McIntyre J, Craig G, Zilm P, Gully N. An in vitro model to measure the effect of a silver fluoride and potassium iodide treatment on the permeability of demineralized dentine to Streptococcus mutans. Aust Dent J. 2005;50:242–245. doi: 10.1111/j.1834-7819.2005.tb00367.x. [DOI] [PubMed] [Google Scholar]
- 14.Hu S, Meyer B, Duggal M. A silver renaissance in dentistry. Eur Arch Paediatr Dent. 2018;19:221–227. doi: 10.1007/s40368-018-0363-7. [DOI] [PubMed] [Google Scholar]
- 15.Alvear Fa B, Jew J, Wong A, Young D. Silver Modified Atraumatic Restorative Technique (SMART): an alternative caries prevention tool. Stoma Edu J. 2016;3:18–24. [Google Scholar]
- 16.Modasia R, Modasia D. Application of silver diamine fluoride as part of the Atraumatic Restorative Technique. BDJ Student. 2021;28:42–43. doi: 10.1038/s41406-021-0199-1. [DOI] [Google Scholar]
- 17.Bridge G, Martel A-S, Lomazzi M. Silver diamine fluoride: transforming community dental caries program. Int Dent J. 2021 doi: 10.1016/j.identj.2020.12.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mei ML, Li Q-L, Chu C-H, Lo E-M, Samaranayake LP. Antibacterial effects of silver diamine fluoride on multi-species cariogenic biofilm on caries. Ann Clin Microbiol Antimicrob. 2013;12:4. doi: 10.1186/1476-0711-12-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Craig G, Knight G, McIntyre J. Clinical evaluation of diamine silver fluoride/potassium iodide as a dentine desensitizing agent. A pilot study. Aust Dent J. 2012;57:308–311. doi: 10.1111/j.1834-7819.2012.01700.x. [DOI] [PubMed] [Google Scholar]
- 20.Schulz KF, Altman DG, Moher D, C. Group CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Trials. 2010;11:1–8. doi: 10.1186/1745-6215-11-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lygidakis N, Wong F, Jälevik B, Vierrou A, Alaluusua S, Espelid I. Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH) Eur Arch Paediatr Dent. 2010;11:75–81. doi: 10.1007/BF03262716. [DOI] [PubMed] [Google Scholar]
- 22.Ismail AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H, Pitts NB. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35:170–178. doi: 10.1111/j.1600-0528.2007.00347.x. [DOI] [PubMed] [Google Scholar]
- 23.Jeremias F, Souza JFd, Costa Silva CMd, Cordeiro RdCL, Zuanon ÂCC, Santos-Pinto L. Dental caries experience and molar-incisor hypomineralization. Acta Odontol Scand. 2013;71:870–876. doi: 10.3109/00016357.2012.734412. [DOI] [PubMed] [Google Scholar]
- 24.Schiff T, Delgado E, Zhang Y, Cummins D, DeVizio W, Mateo L. Clinical evaluation of the efficacy of an in-office desensitizing paste containing 8% arginine and calcium carbonate in providing instant and lasting relief of dentin hypersensitivity. Am J Dent. 2009;22:8A–15A. [PubMed] [Google Scholar]
- 25.Frencken J. Atraumatic restorative treatment and minimal intervention dentistry. Br Dent J. 2017;223:183–189. doi: 10.1038/sj.bdj.2017.664. [DOI] [PubMed] [Google Scholar]
- 26.Schmalz G, Ryge G. Reprint of Criteria for the clinical evaluation of dental restorative materials. Clin Oral Investig. 2005;9:215–232. doi: 10.1007/s00784-005-0018-z. [DOI] [PubMed] [Google Scholar]
- 27.Seifo N, Robertson M, MacLean J, Blain K, Grosse S, Milne R, Seeballuck C, Innes N. The use of silver diamine fluoride (SDF) in dental practice. Br Dent J. 2020;228:75–81. doi: 10.1038/s41415-020-1203-9. [DOI] [PubMed] [Google Scholar]
- 28.Leppaniemi A, Lukinmaa P-L, Alaluusua S. Nonfluoride hypomineralizations in the permanent first molars and their impact on the treatment need. Caries Res. 2001;35:36–40. doi: 10.1159/000047428. [DOI] [PubMed] [Google Scholar]
- 29.Fagrell TG, Lingström P, Olsson S, Steiniger F, Norén JG. Bacterial invasion of dentinal tubules beneath apparently intact but hypomineralized enamel in molar teeth with molar incisor hypomineralization. Int J Paediatr Dent. 2008;18:333–340. doi: 10.1111/j.1365-263X.2007.00908.x. [DOI] [PubMed] [Google Scholar]
- 30.Krämer N, Khac N-HNB, Lücker S, Stachniss V, Frankenberger R. Bonding strategies for MIH-affected enamel and dentin. Dent Mater. 2018;34:331–340. doi: 10.1016/j.dental.2017.11.015. [DOI] [PubMed] [Google Scholar]
- 31.Lygidakis N, Chaliasou A, Siounas G. Evaluation of composite restorations in hypomineralized permanent molars: a four year clinical study. Eur J Paediatr Dent. 2003;4:143–148. [PubMed] [Google Scholar]
- 32.Rolim TZC, da Costa TRF, Wambier LM, Chibinski AC, Wambier DS, da Silva Assunção LR, de Menezes JVBN, Feltrin-Souza J. Adhesive restoration of molars affected by molar incisor hypomineralization: a randomized clinical trial. Clin Oral Investig. 2020;25:1513–1524. doi: 10.1007/s00784-020-03459-2. [DOI] [PubMed] [Google Scholar]
- 33.de Souza JF, Fragelli CB, Jeremias F, Paschoal MAB, Santos-Pinto L, R.d.C.L. Cordeiro, Eighteen-month clinical performance of composite resin restorations with two different adhesive systems for molars affected by molar incisor hypomineralization. Clin Oral Investig. 2017;21:1725–1733. doi: 10.1007/s00784-016-1968. [DOI] [PubMed] [Google Scholar]
- 34.Hilgert LA, Leal SC, Freire GML, Mulder J, Frencken JE. 3-year survival rates of retained composite resin and ART sealants using two assessment criteria. Braz Oral Res. 2017;31:1–13. doi: 10.1590/1807-3107BOR-2017. [DOI] [PubMed] [Google Scholar]
- 35.De Amorim R, Frencken J, Raggio D, Chen X, Hu X, Leal S. Survival percentages of atraumatic restorative treatment (ART) restorations and sealants in posterior teeth: an updated systematic review and meta-analysis. Clin Oral Investig. 2018;22:2703–2725. doi: 10.1007/s00784-018-2625-5. [DOI] [PubMed] [Google Scholar]
- 36.Holmgren CJ, Lo EC, Hu D, Wan H. ART restorations and sealants placed in Chinese school children–results after three years. Community Dent Oral Epidemiol. 2000;28:314–320. doi: 10.1034/j.1600-0528.2000.280410.x. [DOI] [PubMed] [Google Scholar]
- 37.Zanata RL, Fagundes TC, de Almendra Freitas MCC, Lauris JRP, de Lima Navarro MF. Ten-year survival of ART restorations in permanent posterior teeth. Clin Oral Investig. 2011;15:265–271. doi: 10.1007/s00784-009-0378-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Garg S, Sadr A, Chan D. Potassium iodide reversal of silver diamine fluoride staining: a case report. Oper Dent. 2019;44:221–226. doi: 10.2341/17-266-S. [DOI] [PubMed] [Google Scholar]
- 39.Zhao IS, Mei ML, Burrow MF, Lo EC-M, Chu C-H. Effect of silver diamine fluoride and potassium iodide treatment on secondary caries prevention and tooth discolouration in cervical glass ionomer cement restoration. Int J Mol Sci. 2017;18:1–12. doi: 10.3390/ijms18020340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mjör IA, Toffentti F. Secondary caries: a literature review with case reports. Quintessence Int. 2000;31:165–179. [PubMed] [Google Scholar]
- 41.Sayed M, Matsui N, Hiraishi N, Inoue G, Nikaido T, Burrow MF, Tagami J. Evaluation of discoloration of sound/demineralized root dentin with silver diamine fluoride: in-vitro study. Dent Mater J. 2018;38:143–149. doi: 10.4012/dmj.2018-008. [DOI] [PubMed] [Google Scholar]
- 42.Bekes K, Heinzelmann K, Lettner S, Schaller H-G. Efficacy of desensitizing products containing 8% arginine and calcium carbonate for hypersensitivity relief in MIH-affected molars: an 8-week clinical study. Clin Oral Investig. 2017;21:2311–2317. doi: 10.1007/s00784-016-2024-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ozgül BM, Saat S, Sönmez H, Oz FT. Clinical evaluation of desensitizing treatment for incisor teeth affected by molar-incisor hypomineralization. J Clin Pediatr Dent. 2013;38:101–5. doi: 10.17796/jcpd.38.2.92mx26l6n482j682. [DOI] [PubMed] [Google Scholar]
- 44.Mei M, Nudelman F, Marzec B, Walker J, Lo E, Walls A, Chu C. Formation of fluorohydroxyapatite with silver diamine fluoride. J Dent Res. 2017;96:1122–1128. doi: 10.1177/0022034517709738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Castillo J, Rivera S, Aparicio T, Lazo R, Aw T-C, Mancl L, Milgrom P. The short-term effects of diammine silver fluoride on tooth sensitivity: a randomized controlled trial. J Dent Res. 2011;90:203–208. doi: 10.1177/0022034510388516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Duangthip D, Chu C, Lo E. A randomized clinical trial on arresting dentine caries in preschool children by topical fluorides—18 month results. J Dent. 2016;44:57–63. doi: 10.1016/j.jdent.2015.05.006. [DOI] [PubMed] [Google Scholar]
- 47.Horst J. Silver fluoride as a treatment for dental caries. Adv Dent Res. 2018;29:135–140. doi: 10.1177/0022034517743750. [DOI] [PMC free article] [PubMed] [Google Scholar]