

Abstract
Objectives:
The Galápagos provides an important setting to investigate the health impacts of a new drinking water treatment plant (DWTP) in a limited resource environment. We examine how household perceptions and practices affect the relationship between water quality and infections before and after DWTP.
Methods:
Ethnographic data and self-reported infections were collected from 121 mothers and 168 children ages 2-10 from Isla San Cristóbal. Household tap water samples were tested for levels of fecal contamination. Community level infection rates were estimated using discharge records from the Ministry of Public Health. The effects of the new DWTP and fecal contamination levels on infections were tested using logistic and Poisson models.
Results:
Perceptions of water quality and household practices influenced exposures to contaminated tap water. We found minimal change in drinking water sources with 85% of mothers sampled before the DWTP and 83% sampled after using bottled water, while >85% from the pooled sample used tap water for cooking and hygiene practices. The DWTP opening was associated with lower odds of fecal contamination in tap water, reported urinary infections, and community level rates of urinary and gastrointestinal infections. The household practice of recently washing the cistern contributed to higher contamination levels after the DWTP opened.
Conclusions:
To ensure access to clean water, public health works need to consider how household perceptions and practices influence tap water use and quality, in addition to infrastructure improvements. Exposures to contaminated tap water contribute to the burden of infectious disease in environments with inadequate water infrastructure.
Keywords: WaSH, safely managed water, fecal contamination, water quality, water-borne infections
INTRODUCTION
The United Nations “recognizes the right to safe and clean drinking water and sanitation as a human right that is essential for the full enjoyment of life and all human rights” (UN, 2010:2). The World Health Organization (WHO) estimated that inadequate water, sanitation and hygiene (WASH) caused 829,000 deaths in 2016 and that improved infrastructure and access to WASH could lessen the global burden of disease by 10% (WHO, 2016). The Joint Monitoring Programme (JMP) between WHO and UNICEF introduced new indicators of safely managed drinking water and sanitation towards the achievement of the 2030 Agenda for Sustainable Development Goal (SDG) 6 on “access to safe and affordable drinking water” (UN, 2018:11; WHO and UNICEF, 2017). The new standard for safely managed drinking water is free of fecal contamination, available when needed, and accessible at home. However, the SDG-6 Synthesis Report 2018 on Water and Sanitation stated that countries are not on track to meet these targets, citing renewed challenges to ensure water safety and improve water quality among basic services, with 2.1 billion people lacking access to safely managed water (UN, 2018). The report called for national governments to adapt targets for local conditions and provide improved monitoring, yet it is not clear how are these targets will be implemented in limited resources environments.
In Ecuador between 2000 and 2015, access to basic water services grew from 83% to 93%, and safely managed drinking water rose from 66% to 74%, according to the JMP report (WHO and UNICEF, 2017). Ecuadorians with basic sanitation services increased from 71% to 86%, yet safely managed sanitation services remained constant at 42%. The Galapágos Archipelago is an important research setting to investigate the health effects of improved water since access to clean water is a major public health concern (Page, Bentley, & Waldrop, 2013; Walsh et al., 2010). With only two fresh water sources in the highlands of Isla San Cristóbal, the availability of water has historically been a pressing issue for the four populated islands (Liu & d’Ozouville, 2013). Located more than 700 miles from the Ecuadorian coast, providing and maintaining adequate water and sanitation infrastructures to the 25,000 residents and over 200,000 yearly tourists can be challenging (INEC, 2015; Schep, Ruesen, Lujan Gallegos, Van Beukering, & Botzen, 2014). In 2010, 90% of households on Isla San Cristóbal received piped water from the municipality (CGREG & INEC, 2010), yet the water treatment facility was not operational. Residents viewed the piped water as unsafe and contaminated, relying on bottled water for drinking and using the contaminated municipal water for household purposes (Guyot-Tephany, Grenier, & Orellana, 2013). In 2010, 75% of households on the island had toilets connected to the municipal sewer system and an additional 23% connected to septic tanks (CGREG & INEC, 2010), yet the waste water treatment facility was also not operational and untreated sewage water was drained into the ocean (Gerhard, Choi, Houck, & Stewart, 2016). During this time, the island’s public hospital reported high rates of water-borne illnesses and other gastrointestinal (GI) infections consistent with fecal bacteria exposure (CGREG, 2010).
In August to September of 2013, the municipality on Isla San Cristóbal opened a new, modern drinking water treat plant (DWTP) to replace the previous ineffective system. With a safely managed, properly functioning DWTP, fecal contamination should not be detectable, water should be clean and the health risk of water-borne illnesses at should be low (WHO, 2011). Recent work examining levels of fecal contamination in the municipal distribution network before and after the new DWTP demonstrated marked improvements, but sporadic contamination persisted at the household level (Gerhard, Choi, Houck, & Stewart, 2016).
The interaction between behavior and environment is a main component of the WHO framework for WASH interventions (WHO, 2018). Disease transmission is determined by the interaction between lifestyles or practices and environment, and interventions must incorporate an understanding of local behaviors (Fink, Günther, & Hill, 2011; Fisher, Kabir, Lahiff, & MacLachlan, 2011). In keeping with the UN’s recommendation of implementing and monitoring water improvements at the local level, we aimed to evaluate the health impacts associated with improvements in water quality on Isla San Cristóbal brought by the new DWTP. Our study focused on points of water exposures within the household, and incorporated community level data collected from public health centers.
Using a biocultural perspective, we investigated household perceptions and practices concerning water quality and use in order to contextualize the link between contaminated water, exposures and infections. This paper 1) describes how households use the municipal tap water and their perceptions of water quality before and after the DWTP, 2) analyzes levels of fecal contamination in household tap water before and after the DWTP, and determines what additional household factors influenced tap and drinking water quality, 3) tests the relationships between self-reported urinary and GI infections before and after the DWTP and levels of fecal contamination in tap and drinking water, and 4) examines changes in community level urinary and GI infections before and after the new DWTP.
SAMPLE AND METHODS
Cross-sectional household data were collected over two field seasons that fell before and after the new DWTP began operation in August-September 2013. We used a convenience sample of children 2-10 years old and their mothers in 12 neighborhoods in Puerto Baquerizo Moreno, which constitutes the urban populated area of the island of San Cristóbal. Sixty-one mothers and their 82 children were interviewed during the first field season between June and July 2013, and an additional 60 mothers and their 86 children were interviewed during second field season between February and March 2014. A small subsample of 29 mothers from the first field season were revisited during April 2014 to examine longitudinal tap water quality. This study received approval for human subject research by the University of North Carolina, Chapel Hill (UNC-Chapel Hill) and the local review board at the Universidad San Francisco de Quito.
Data collection methods and analyses are described elsewhere (Houck, 2017). Briefly, levels of fecal contamination in household water were tested for the presence and most probable number (MPN) of Escherichia coli using the culture-based IDEXX Colilert test (IDEXX Laboratories, Inc. Westbrook, Maine). One sample of tap water was analyzed from each household surveyed during both field seasons to determine water quality before and after the DWTP. Tap water samples from a subset of households from the first field season were collected and tested after the DWTP opened to examine longitudinal tap water quality. Samples of drinking water were collected from the source (bottled, boiled tap or filtered tap) during the first field season only and analyzed for fecal contamination. Household tap and drinking water quality was defined according to the WHO, levels <1 E. coli MPN/100mL water are at low health risk for the community, 1-10 E. coli MPN/100mL are intermediate risk, >10 E. coli MPN/100mL are high risk (WHO, 2011).
Using data from mothers’ interviews, household water use measures were created, including the source of water used for drinking, cooking, washing dishes, laundry, hand washing and bathing. Questions regarding the source of water for cleaning produce and brushing teeth were added during the second field season. We noted the presence of a toilet and its location inside or outside of the home to assess sanitation and classified the facilities as improved or unimproved. We asked mothers how often their children washed their hands with soap and water after using the bathroom, and whether children bathed inside or outside of the house. Mothers were asked about the municipal tap water quality, how they received and stored municipal water, and treatment practices. After the first field seasons had begun, questions were added concerning cistern cleaning practices, such as physically cleaning (emptying and washing) the cistern and adding chlorine. During the second field season, we asked whether the household was notified that the municipal tap water was potable. Lastly, mothers were asked if they or their children experienced symptoms of urinary infection, such as painful urination or increased frequency, or diarrhea or vomiting indicating GI infection within the past two weeks.
Community level infection data for Galápagos came from the study of Egresos hospitalarios y perfil de morbilidad hospitalaria del Sistema Nacional de Salud, which contains all in-/out-patient admission records and diagnoses from every public hospital, clinic and health post, compiled by the Ministerio de Salud Pública (MSP) or Ecuadorian Ministry of Public Health. Since treatment at public hospitals and clinics is free of charge and because there were few private doctors on the island, the majority of residents who sought medical care would have been captured in this database. Special permission to access these data was given by the Galápagos MSP and the analyses received human subject research approval by the Institutional Review Board at UNC-Chapel Hill.
Cases of urinary and GI infections were summarized using relevant diagnoses from the MSP data for 2013 to 2014 from Isla San Cristóbal, as the main focus of the study, and from Isla Santa Cruz as a comparison. Cases of diarrhea, gastroenteritis, and intestinal infections caused by protozoa, helminths, bacteria or viruses were recorded as GI infections. Urinary tract infection diagnoses were recorded as urinary infections. Individuals who were repeatedly seen for the same type of infection within a two-month period were only counted as one case. Rates of urinary and GI infections were calculated using population estimates from the special 2015 population and household census for Galápagos (INEC, 2015).
Statistical analysis
Household survey data:
Non-parametric tests of association were used to evaluate variables influencing tap and drinking water quality, and reported infection. We used logistic regression to estimate the odds ratios of households sampled during the second field season (referent: first season) on experiencing high levels of fecal contaminated water (>10 E. coli MPN/100mL of water) and self-reported GI and urinary infections separately, adjusted for sanitation type. Logistic models were also used to calculate the odds ratios of high levels of fecal contaminated water (>10 E. coli MPN/100mL of water) on risk of GI and urinary infections. All infection models were stratified by mothers and children and adjusted for sanitation type and age, along with sex and clustering at the household level for children.
Community infection rates:
Poisson regression models were used to estimate the independent effects of the DWTP opening (after DWTP October 2013-December 2014; referent: before DWTP January-September 2013) on monthly urinary and GI infections by island, adjusted for the rainy season (January to April).
RESULTS
Water usage from household survey:
All households in our study received municipal water by pipe or sometimes water truck, which was typically stored in above-ground plastic or concrete cisterns and distributed into the home for use by faucets. Mothers used the municipal tap water for household cleaning such as washing dishes and laundry, and a few used collected rainwater when available. However, 11% used bottled or filtered water for cooking purposes and 15% of mothers (from the second field season) used treated tap water (either boiled, filtered or disinfected) for cleaning fruits and vegetables (Table 1).
Table 1.
Sample characteristics of the household survey
| Mothers n=121 |
Children n=168 |
|
|---|---|---|
| Demographics | ||
| Sample, % before H2O treatment (n) | 50.4 (61) | 48.8 (82) |
| % after H2O treatment (n) | 49.6 (60) | 51.2 (86) |
| Mean age, years (SD) | 30 (8) | 6 (3) |
| Sex, % female (n) | 100 (121) | 48.2 (81) |
| Water sources for household usage | ||
| Cooking water source, % tap (n) | 89.3 (108) | |
| % bottled or filtered (n) | 10.7 (13) | |
| Cleaning produce water sourcea, % tap (n) | 85.2 (52) | |
| % boiled tap (n) | 4.9 (3) | |
| % filtered tap (n) | 8.2 (5) | |
| % disinfectant (n) | 1.6 (1) | |
| Sanitation | ||
| Sanitation, % improved inside home (n) | 82.6 (100) | |
| % improved outside home (n) | 17.4 (21) | |
| Hygiene behaviors | ||
| Hand washing, % always (n) | 63.7 (107) | |
| % frequently (n) | 14.9 (25) | |
| % sometimes or rarely (n) | 21.4 (36) | |
| Bathing location, % inside (n) | 85.7 (144) | |
| % outside (n) | 14.3 (24) | |
| Brushing teeth water sourcea, % tap (n) | 87.4 (76) | |
| % filtered or bottled (n) | 12.6 (11) |
Only for the 2nd field season
Most mothers reported that they used tap water for family hygiene behaviors of hand washing and bathing. When asked about the frequency of hand washing of their children, mothers reported that 64% always wash, 15% frequently wash and 21% sometimes or rarely wash with soap after using the toilet. Approximately 14% of children bathed outside of the house, often in separate containers or tubs using the tap water. Only one mother said she used filtered water for bathing her children. Among children from the second field season, 87% used household tap water for brushing teeth, while 13% used filtered or bottled water.
Household sanitation facilities:
All households in our study had improved sanitation facilities, 83% inside the home and 17% outside (Table 1). Since the sewage waste facility was not operational during the time of study, they would not be considered safely managed according to JMP classification (WHO and UNICEF, 2017).
Perceptions and practices concerning household tap water quality:
When asked about the quality of the municipal water households received, all mothers from the first field season reported that the water was contaminated and not suitable for drinking (Table 2). Among mothers from households sampled after the DWTP opened, 50% said it was potable, 27% heard it was potable, 17% did not know and 7% responded that it was unsafe for drinking. Of the 30 mothers who said it was potable, 25 of them reported that they were notified of this by the municipality. Approximately 91% of mothers from the first field season reported that they added chlorine to their cisterns compared to 70% during the second field season. Among households from the first field season, 57% reported that they had physically emptied and washed their cistern within the last month compared to 41% from the second field season.
Table 2.
Perceptions and practices on Isla San Cristóbal concerning household water quality
| Before H2O treatment n=61 |
After H2O treatment n=60 |
|
|---|---|---|
| Municipal water potablea, % no (n) | 100 (60) | 6.7 (4) |
| % yes (n) | 0 | 50 (30) |
| % heard it was (n) | 0 | 26.7 (16) |
| % do not know (n) | 0 | 16.7 (10) |
| Notified by municipality b, % yes (n) | - | 48.1 (25) |
| % no (n) | - | 51.9 (27) |
| Chlorine treatment in cistern c, % yes (n) | 91.3 (21) | 69.5 (41) |
| % no (n) | 8.7 (2) | 30.5 (18) |
| Physical washing cistern c, % <month (n) | 57.1 (12) | 41.4 (24) |
| % month-year (n) | 42.9 (9) | 41.4 (24) |
| % >year or never (n) | 0 | 17.2 (10) |
| Drinking water source, % bottled (n) | 85.2 (52) | 83.3 (50) |
| % boiled tap (n) | 4.9 (3) | 6.7 (4) |
| % filtered tap (n) | 6.6 (4) | 6.7 (4) |
| % untreated tap (n) | 3.3 (2) | 3.3 (2) |
Mother’s perception of municipal water quality
From 2nd field season only
Question was not asked of entire sample from the 1st field season
Drinking water source and quality:
There were few differences in drinking water sources between the two field seasons with 85% of households using bottled water prior to the DWTP and 83% after (Table 2). Approximately 12% before and 13% after used boiled or filtered tap water, and only 3% of households relied on untreated tap water during both field seasons. During the first field season, 77% of households had low fecal contamination levels in drinking water, 10% had intermediate levels and 13% had high levels (Figure S1). We found no significant differences in fecal contamination levels based on drinking water source (p>.05). There were also no significant relationships between drinking water contamination levels and reported infections (p>.05).
Household tap water quality before and after water treatment facility:
Based on the longitudinal water quality data from the 29 households that were visited before and after the DWTP opened, 83% went from high to low fecal contamination, 10% remained at intermediate levels and 7% remained at high levels (p<.001) (Figure S2).
Based on the cross-sectional data, 79% of households sampled prior to the DWTP had high fecal contamination levels in tap water, which was significantly reduced to 7% after the DWTP opened (p<.001) (Figure 1). Yet, the proportion of household tap water samples with intermediate levels rose slightly from 15% to 17%, signifying that contamination was still occurring. Based on the WHO standards, 77% of households had safe levels following the opening, compared to only 7% prior. Logistic regression demonstrates that households sampled after the DWTP opened had significantly lower odds of highly contaminated water >10 E. coli MPN/100mL (OR 0.02, 95%CI 0.01-0.06) than households sampled before (Table 3).
Figure 1:
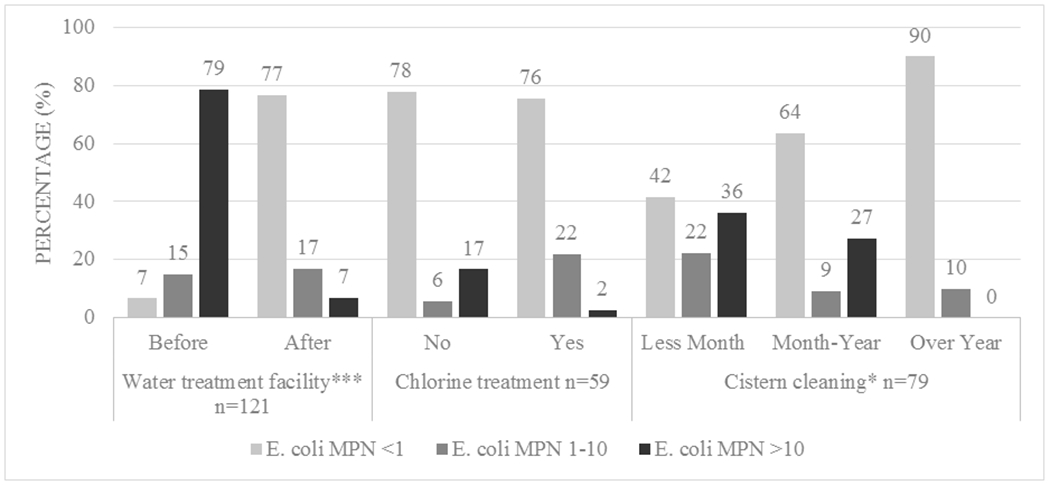
Water treatment and handling factors influencing household tap water quality on Isla San Cristóbal. Note: * p < .05 ***; p < .001
Table 3.
Adjusted odds of high fecal contamination in tap water and reported infection by household water quality factors
| Householdsa |
Mothersb |
Childrenc |
|||
|---|---|---|---|---|---|
| High fecal levelsc | Urinary infection | GI infection | Urinary infection | GI infection | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Model set A | |||||
| After water treatmentd | 0.02 (0.01, 0.06)*** | 0.22 (0.09, 0.57)** | 3.15 (0.90, 11.07) | 0.08 (0.02, 0.39)** | 0.79 (0.36, 1.72) |
| Model set B | |||||
| High fecal levelse | - | 3.84 (1.62-9.11)** | 0.66 (0.20, 2.25) | 4.95 (1.50-16.41)** | 1.95 (0.92, 4.15) |
Model adjusted for sanitation
Models adjusted for sanitation and age
Models adjusted for sanitation, age, sex and clustering at the household level
Modeling the effects of households sampled during the 2nd field season
Modeling the effects of households with high levels of fecal contamination (>10 E. coli MPN per 100mL) on the pooled sample
p < .01
p < .001
After the DWTP opened, 2% of the households that used chlorine treatment (n=41) had high contamination levels, compared to 17% who did not add chlorine to their cisterns (n=18) (p=.062) (Figure 1). Among the households that physically washed their cistern within the last month of the study (n=36) 36% had high levels of fecal contamination, compared to 27% that washed the tank between 1-12 months ago (n=33). Among those that had never cleaned their tank or had cleaned it more than a year ago (n=10), 90% had low contamination levels and no households had high fecal contamination levels (p=.041).
Self-reported infections before and after water treatment:
Based on the cross-sectional data before the DWTP, 41% of mothers sampled reported urinary infections, which was significantly reduced to 15% following the opening (p=.002) (Figure 2A). Among children, reports of urinary infections also dropped from 15% to 2% following the DWTP opening (p=.004). Logistic models demonstrate that households sampled after the DWTP opened had significantly lower odds of reported urinary infection among mothers (OR 0.22, 95%CI 0.09-0.57) and children (OR 0.08, 95%CI 0.02-0.39) (Table 3).
Figure 2:
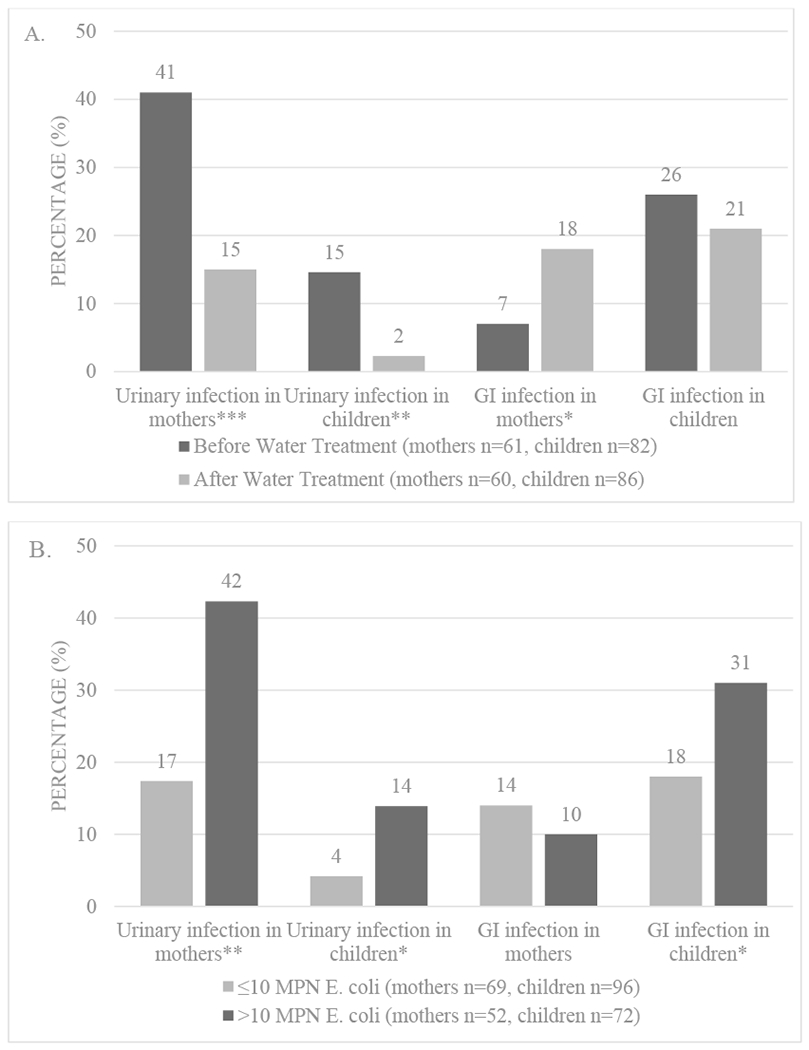
Self-reported infections among mothers and children on Isla San Cristóbal including (A) infections before and after installation of a new drinking water treatment plant, and (B) infections in households with fecal contamination detected in household tap water. Note: * p <.05; ** p <.01; *** p <.001
Self-reported GI infection among mothers significantly increased from 7% before to 18% after the DWTP opened (p=.044), while rates of GI infections among children decreased from 26% to 21%, yet not significantly (Figure 2A). Logistic regression found no association between GI infections before and after the opening of the DWTP among mothers or children (Table 3).
Self-reported infections and fecal bacterial contamination in household tap water:
In the pooled cross-sectional sample, mothers from households with high fecal contamination levels in tap water reported significantly higher rates of urinary infection at 42%, compared to 17% from households with lower fecal contamination (≤10 E. coli MPN per 100mL) (p=.002) (Figure 2B). Similarly, 14% of children from households with high contamination levels reported urinary infections, whereas only 4% of households with lower levels reported urinary infections (p=.024). Belonging to a household with high fecal contamination in tap water increased odds of reporting urinary infections among mothers (OR 3.84, 95%CI 1.62-9.11) and children (OR 4.95, 95%CI 1.50-16.41) (Table 3).
Among mothers from households with high fecal contamination levels in tap water, 10% reported GI infections compared to 14% among households with lower levels, yet these differences were not significant (Figure 2B). However, 31% of children from households with high contamination levels reported GI infections compared to 18% from households with lower levels (p=.039). High contamination levels in household tap water were not significantly associated with GI infections among mothers and were marginally associated with higher odds in children (OR 1.95, 95%CI 0.92-4.15) (Table 3).
Community level infections treated by the MSP health centers:
There was considerable monthly variability over time in GI infections on both islands, and urinary infections on Santa Cruz, resulting in overall declines in urinary and GI cases (Figure 3). Following the DWTP opening in August-September 2013, the mean monthly rate of urinary infections declined from 0.04 to 0.02 per 1,000 people on San Cristóbal and 0.09 to 0.07 on Santa Cruz (Figure S3). Monthly rates of GI infections also fell from 0.20 to 0.12 per 1,000 people on San Cristóbal and 0.18 to 0.15 on Santa Cruz after the DWTP. Poisson models indicate significant declines following the opening of the DWTP on both islands, independent of seasonal effects (Table 4). The negative effects of the DWTP opening on monthly urinary (β −0.67, SE 0.07 p<.001) and GI (β −0.69, SE 0.04 p<.001) cases were greater on Isla San Cristóbal, compared to Isla Santa Cruz (β −0.45, SE 0.04 p<.001 and β −0.37, SE 0.03 p<.001, respectively).
Figure 3:
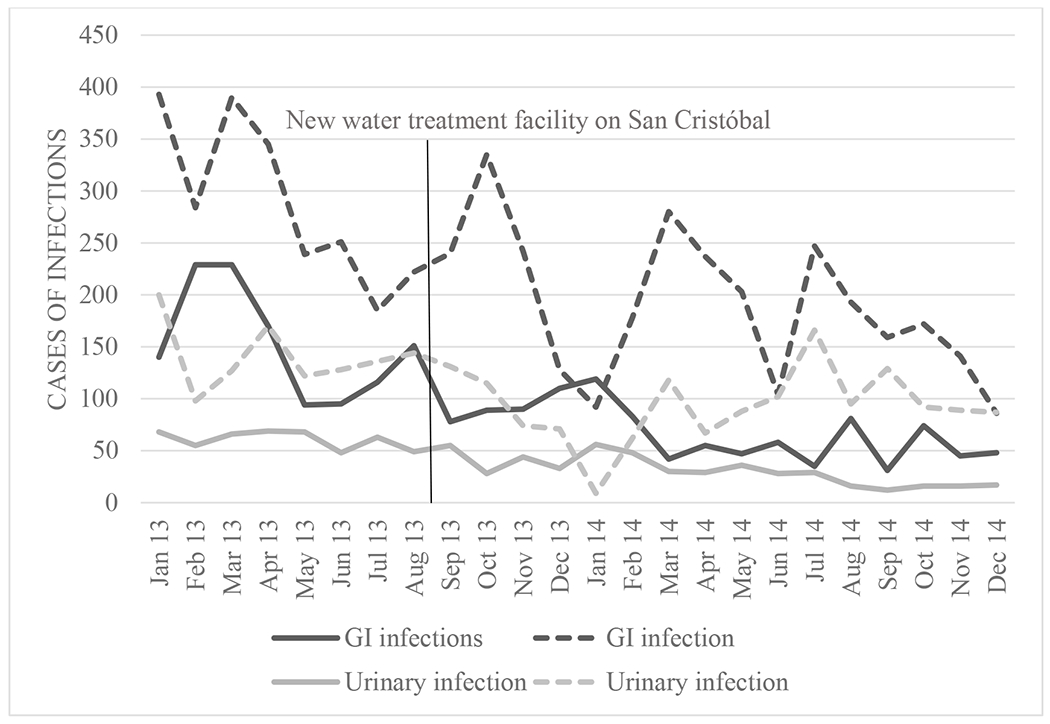
Monthly infection cases on Isla San Cristóbal and Isla Santa Cruz
Table 4.
Results for Poisson models after the DWTP on MSP cases of community infections
| Urinary infection models | GI infection models | |||||
|---|---|---|---|---|---|---|
| Coefficient | SEa | P value | Coefficient | SEa | P value | |
|
|
|
|||||
| San Cristóbal | ||||||
| After DWTPb | −0.67 | 0.07 | 0.000 | −0.69 | 0.04 | 0.000 |
| Rainy seasonc | 0.28 | 0.07 | 0.000 | 0.41 | 0.04 | 0.000 |
| Santa Cruz | ||||||
| After DWTPb | −0.45 | 0.04 | 0.000 | −0.37 | 0.03 | 0.000 |
| Rainy seasonc | −0.13 | 0.04 | 0.003 | 0.26 | 0.03 | 0.000 |
Standard error
Drinking water treatment plant
January to April
DISCUSSION
The greatest health impact associated with the opening of the DWTP was significantly reduced odds of self-reported urinary infections in mothers and children. At the community level on Isla San Cristóbal, the DWTP opening was associated with significantly lower cases of urinary infections treated at public health centers, with a smaller effect size observed on Isla Santa Cruz. Supporting these findings, mothers and children from households with high fecal contamination levels had higher odds of urinary infection. Bathing or showering in contaminated water may allow for fecal bacteria to enter the urinary tract. There are limited studies examining bathing or swimming in fecal contaminated water and community-acquired urinary infections, yet exposure to Pseudomonas aeruginosa in contaminated hot tubs have been reported to cause urinary infections (Mena & Gerba, 2009; Salmen et al., 1983).
Additional ecological factors can increase risk of urinary infection when exposed to fecal bacteria, which may contribute to the higher overall rates in Galápagos. Studies have suggested that populations with unsafe drinking water have higher consumption of sweetened beverages such as bottled juice and sodas (Barquera et al., 2010; Piernas, Barquera, & Popkin, 2013), which can worsen dehydration and increase the risk of urinary infections (Beetz, 2003; García-Arroyo et al., 2016). Mothers in our sample reported higher rates of infection than children, which may be due to sexual activity or recurrent infections (Tandogdu & Wagenlehner, 2016). Ecuador and other Latin American countries have high rates of multidrug-resistant urinary tract E. coli isolates, which could be contributing to the elevated levels of infection (Salles et al., 2013).
We speculate that urinary infections such as asymptomatic bacteriuria in children may go unreported, as symptoms are less obvious, especially among infants and younger children (Nicolle et al., 2005). As a consequence of inadequate water and sanitation infrastructure in resource poor environments, diarrheal disease, parasitic infection and environmental enteric dysfunction are the main research foci in improving childhood health and development. We suggest a complementary focus on investigating the causes and consequences of urinary infections as they contribute to the burden of disease and immune activation in these environments.
The strength of this study was the biocultural context provided by the household survey, without it the community-level analyses of water quality and infections offer a limited understanding of the health impacts of the DWTP on the island. Based on data from the MSP, we found evidence of a decline in cases of urinary and GI infections after the DWTP, yet attributing these reduced rates to the DWTP opening is problematic. Santa Cruz also experienced significant improvements in rates of infection without a functioning DWTP during the same time period. Water-borne infections, especially childhood diarrhea can be driven by climatic conditions such as rainfall through the contamination of drinking water sources (Carlton et al., 2014; Levy, Woster, Goldstein, & Carlton, 2016). Some studies indicate that urinary tract infections also show seasonal variability (Anderson, 1983; Simmering, Tang, Cavanaugh, Polgreen, & Polgreen, 2017). We found that seasonal effects partially explain the patterning of rates due to the rainy season. More research is necessary to determine how environmental factors such as flooding, temperature and humidity interact with water quality and availability, and influence community level infections in Galápagos.
Previous work documented considerable improvements of water quality in the finished water (output) from the DWTP on Isla San Cristóbal; yet, fecal contamination persisted at the household level (Gerhard et al., 2016). A global review of fecal contamination in improved (piped) versus unimproved sources found significantly lower odds of fecal contamination, yet 38% of the almost 200 sites with improved sources were contaminated (Bain et al., 2014). Municipal tap water quality data from our study demonstrated significant improvements associated with the opening of the DWTP on Isla San Cristóbal, yet infrastructure and household factors also influenced persistent levels of contamination. In over 20 years in the United States, problems with the public water distribution system have caused 21 thousand cases of infections (Craun & Calderon, 2001). In global areas with limited urban planning, the construction of sewerage and water line networks are sometimes laid together, allowing for cross contamination if pipes break or for back-siphoning related to low pressure (Lee, Lee, Schwab, & Schwab, 2005; Moe & Rheingans, 2006). With the completion of the new DWTP on Isla San Cristóbal, the municipality began replacing the water distribution network, although at the time of this study the basic sewage waste water remained untreated (Gerhard et al., 2016).
Our investigation of household level factors concerning perceptions and practices of water quality and water use provided the background to explain the persistent levels of contamination and their link to health outcomes at the community level. The household practice of regularly adding chlorine to the cistern provided an additional protective effect in decreasing high fecal contamination levels after the DWTP. In limited resource settings, home chlorination interventions have been associated with dramatically reduced rates of self-reported diarrhea (Fagerli et al., 2017; Mengistie, Berhane, & Worku, 2013). In contrast, households that reported that they washed their cistern within the last month, or even less than a year ago had high levels of fecal contamination, which were not present in households that washed their cistern over a year ago or had never washed it. This pathway of contamination may be caused by transferring fecal bacteria by hand. Numerous studies have demonstrated the relationship between poor hand hygiene, water contamination and childhood diarrhea (Ercumen et al., 2017; Ngure et al., 2013; Pickering et al., 2010). Intervention and education programs on water quality need to address infrastructure improvements along with household practices to ensure access to clean water (Fisher et al., 2011).
We also found a mismatch between perceptions of municipal water quality after the DWTP opened and drinking water practices. After the opening, the majority of mothers reported that the tap water was potable or that they heard it was, with close to half being notified by the municipality. Despite this, there was little to no change in reported drinking water sources between the two field seasons. A water study in Galápagos from 2011 suggested that water use is based on the community’s perception of worth, where drinking water has high economic value and high quality, compared to piped water with little value and poor quality (Guyot-Tephany et al., 2013). This may explain why even though mothers were told by the municipality or others that the tap water was safe to drink the community had not changed its perception of water quality. Public perceptions of water quality seems to be a stable concept over time that greatly influences drinking water behaviors globally (Doria, Pidgeon, & Hunter, 2009).
In addition to poor drinking water quality, habitual exposure to fecal contamination in household tap water through daily activities may also contribute to the burden of infection in low resource environments. Improvements in water quality used for household cleaning and hygiene greatly reduced rates of diarrhea by 26% and ascariasis infection by 29% in a review of 144 studies (Esrey, Potash, Roberts, & Shiff, 1991). Mothers in our study relied on the municipal tap water for daily household cleaning practices and family hygiene behaviors that could result in exposure, since 24% of households had unsafe fecal contamination levels after the DWTP opened. Likewise, showering, bathing or brushing teeth with tap water can result in small amounts being swallowed, in addition to being inhaled (McKone & Daniels, 1991; Weisel & Jo, 1996).
Children from the household survey had higher rates of GI infections compared to mothers, which is similar to other studies that have suggested that children are more vulnerable to unhealthy environmental conditions (Sly & Flack, 2008; Wild & Kleinjans, 2003). This may be due to the development of the immature immune system and gut microbiota (Koenig et al., 2011; Thompson, 2012), and behavioral conditions such as poor hygiene and putting fingers in their mouths (Ngure et al., 2013; Xue et al., 2007). Exposures to fecal contamination causing GI infections can also occur at schools (Jasper, Le, & Bartram, 2012). Bacterial and parasitic intestinal infections have critical growth and development implications for Ecuadorian children, who by the age of 2, exhibited a 90% prevalence of enterotoxigenic E. coli antibody titers (Brüssow et al., 1990).
The application of a mixed methods approach improved our understanding of the link between water quality and reduced infection rates associated with the new DWTP on the island of San Cristóbal. However, several limitations of this work must be considered. This observational study was not prospective in design around the DWTP and cannot draw causal links between water quality and health outcomes. The small sample size for each field season and the limited longitudinal data before and after the DWTP opened constrain statistical inference about the effects of improved water quality. Yet, we were able to establish a significant association between higher levels of fecal contamination in household tap water and self-reported urinary tract infections. Linking these self-reported infections to biomarkers of immune function and urinalysis will be an interesting next step in this research.
Community level infection rates were calculated from the MSP monthly diagnostic cases, and the Ecuadorian census for Galápagos does not provide person-month estimates for the islands, which can fluctuate given migration and employment conditions (Epler, 2007; Taylor, Hardner, & Stewart, 2009). Having only eight months of MSP data before the DWTP opening limits our understanding of the exogenous negative trends in cases of infection on both island prior to the DWTP. We speculate measurement error may account for a proportion of the declines as the MSP began using a computer-based patient record system in January 2013 and diligence of data entry may have decreased over time. In addition, changes in treatment seeking behavior may have changed and these data only captured cases treated in the public health system on the islands, excluding cases treated at home, on the mainland or untreated.
CONCLUSION
Access to clean water is a human right, yet solely providing improved water sources such as piped water does not alone ensure healthy conditions. The case on Isla San Cristóbal is a crucial example of this paradox as the previous water treatment facility was not functioning and the new DWTP produced safe water but still did not ensure universal access to safe drinking water at the point of use. At first glance, municipal improvements in drinking water quality seemed to underlie the significant community level declines in GI and urinary infections. Anthropological investigation of household perceptions and practices provided vital insight into water quality and exposures to contaminated household tap water, showing that the majority of the population relied on purchasing clean bottled water for drinking. Habitual exposures to contaminated household tap water through household cleaning and hygiene behaviors were linked to risk of urinary infections in mothers and children. The implications of this work is two-fold. First, in understanding and ensuring access to clean water, public health works need to consider how household level perceptions and practices influence water quality and water use, in addition to infrastructure improvements. Second, we propose that daily exposures to contaminated non-drinking tap water and their link to urinary tract infections are crucial factors missing in research on the burden of infectious disease in poor resource environments with inadequate water and sanitation infrastructure.
Supplementary Material
ACKNOWLEDGEMENTS
We would like to thank the participants of the household survey and the Galápagos Science Center for their support. We also thank the anonymous reviewers for critically reading the manuscript and suggesting substantial improvements.
Funding information:
National Science Foundations; Wenner-Gren; NIH Eunice Kennedy Shriver National Institute of Child Health and Human Development 5T32HD007168; Carolina Population Center; University of North Carolina’s Institute for Global Health and Infectious Disease; University of North Carolina’s Royster Society of Fellows; Triangle Center for Evolutionary Medicine.
Footnotes
CONFLICT OF INTEREST
We have none to declare.
REFERENCES
- Anderson JE (1983). Seasonality of symptomatic bacterial urinary infections in women. Journal of Epidemiology and Community Health, 37(4), 286–290. doi: 10.1136/jech.37.4.286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bain R, Cronk R, Wright J, Yang H, Slaymaker T, & Bartram J (2014). Fecal Contamination of Drinking-Water in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLOS MEDICINE, 11(5), e1001644. doi: 10.1371/journal.pmed.1001644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barquera S, Campirano F, Bonvecchio A, Hernndez-Barrera L, Rivera JA, & Popkin BM (2010). Caloric beverage consumption patterns in Mexican children. Nutrition Journal, 9(1), 47–47. doi: 10.1186/1475-2891-9-47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beetz R (2003). Mild dehydration: a risk factor of urinary tract infection? European journal of clinical nutrition, 57(S2), S52–S58. doi: 10.1038/sj.ejcn.1601902 [DOI] [PubMed] [Google Scholar]
- Brussow H, Sidoti J, Dirren H, & Freire WB (1995). Effect of malnutrition in Ecuadorian children on titers of serum antibodies to various microbial antigens. Clinical and Vaccine Immunology, 2(1), 62–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brüssow H, Sidoti J, Link H, Hoang YK, Barclay D, Dirren H, & Freire WB (1990). Age-specific prevalence of antibody to enterotoxigenic Escherichia coli in Ecuadorian and German children. Journal of Infectious Diseases, 162(4), 974. [DOI] [PubMed] [Google Scholar]
- Carlton EJ, Eisenberg JNS, Goldstick J, Cevallos W, Trostle J, & Levy K (2014). Heavy rainfall events and diarrhea incidence: The role of social and environmental factors. American Journal of Epidemiology, 179(3), 344–352. doi: 10.1093/aje/kwt279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- CGREG. (2010). Sistema Integrado de indicadores de Galapagos. Puerto Baquerizo Moreno, Galapagos: Consejo de Gobierno de Regimen Especial de Galapagos. [Google Scholar]
- CGREG, & INEC. (2010). Encuesta de condiciones de vida Galapagos 2009-2010. Quito, Ecuador: Consejo de Gobierno de Regimen Especial de Galapagos and Instituto Nacional de Estadistica y Censos. [Google Scholar]
- Craun GE, & Calderon RL (2001). Waterborne disease outbreaks caused by distribution system deficiencies. Journal American Water Works Association, 93(9), 64–75. [Google Scholar]
- Doria M. d. F., Pidgeon N, & Hunter PR (2009). Perceptions of drinking water quality and risk and its effect on behaviour: A cross-national study. Science of the Total Environment, 407(21), 5455–5464. doi: 10.1016/j.scitotenv.2009.06.031 [DOI] [PubMed] [Google Scholar]
- Epler B (2007). Tourism, the economy, population growth, and conservation in Galapagos. Puerto Ayora, Galapagos, Ecuador: Charles Darwin Foundation. [Google Scholar]
- Ercumen A, Pickering AJ, Kwong LH, Arnold BF, Parvez SM, Alam M, … Colford JM (2017). Animal Feces Contribute to Domestic Fecal Contamination: Evidence from E. coli Measured in Water, Hands, Food, Flies, and Soil in Bangladesh. Environmental Science and Technology, 51(15), 8725–8734. doi: 10.1021/acs.est.7b01710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Esrey SA, Potash JB, Roberts L, & Shiff C (1991). Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bulletin of the World Health Organization, 69(5), 609. [PMC free article] [PubMed] [Google Scholar]
- Fink G, Günther I, & Hill K (2011). The effect of water and sanitation on child health: evidence from the demographic and health surveys 1986-2007. International Journal of Epidemiology, 40(5), 1196–1204. doi: 10.1093/ije/dyr102 [DOI] [PubMed] [Google Scholar]
- Fisher S, Kabir B, Lahiff E, & MacLachlan M (2011). Knowledge, attitudes, practices and implications of safe water management and good hygiene in rural Bangladesh: Assessing the impact and scope of the BRAC WASH programme. Journal of Water and Health, 9(1), 80–93. doi: 10.2166/wh.2010.023 [DOI] [PubMed] [Google Scholar]
- García-Arroyo FE, Cristóbal M, Arellano-Buendía AS, Osorio H, Tapia E, Soto V, … Sánchez-Lozada L-G (2016). Rehydration with soft drink-like beverages exacerbates dehydration and worsens dehydration-associated renal injury. American Journal of Physiology-Regulatory Integrative and Comparative Physiology, 311(1), R57–R65. doi: 10.1152/ajpregu.00354.2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerhard WA, Choi WS, Houck KM, & Stewart JR (2016). Water quality at points-of-use in the Galapagos Islands. International Journal of Hygiene and Environmental Health, 220(2), 485–493. doi: 10.1016/j.ijheh.2017.01.010 [DOI] [PubMed] [Google Scholar]
- Guyot-Tephany J, Grenier C, & Orellana D (2013). Usos, percepciones y manejo del agua en Galapagos Informe Galapagos 2011-2012 (pp. 67–75). Puerto Ayora, Galapagos, Ecuador: Dirección del Parque Nacional Galápagos, Consejo de Gobierno del Régimen Especial de Galápagos, Fundación Charles Darwin, Galapagos Conservancy. [Google Scholar]
- Houck KM (2017). Early life effects of a dual burden environment: Childhood intestinal health and immune function in Galápagos, Ecuador (Doctoral Dissertation). University of North Carolina, Chapel Hill, NC. (10681674) [Google Scholar]
- INEC. (2015). Censo de Poblacion y Vivienda-Galapagos. Quito, Ecuador: Instituto nactional de estadistica y censos. [Google Scholar]
- Jasper C, Le T-T, & Bartram J (2012). Water and sanitation in schools: A systematic review of the health and educational outcomes. International Journal of Environmental Research and Public Health, 9(8), 2772–2787. doi: 10.3390/ijerph9082772 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenig JE, Spor A, Scalfone N, Fricker AD, Stombaugh J, Knight R, … Ley RE (2011). Succession of microbial consortia in the developing infant gut microbiome. Proceedings of the National Academy of Sciences, 108(Supplement 1), 4578–4585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee EJ, Lee EJ, Schwab KJ, & Schwab KJ (2005). Deficiencies in drinking water distribution systems in developing countries. Journal of Water and Health, 3(2), 109–127. doi: 10.2166/wh.2005.0012 [DOI] [PubMed] [Google Scholar]
- Levy K, Woster AP, Goldstein RS, & Carlton EJ (2016). Untangling the Impacts of Climate Change on Waterborne Diseases: A Systematic Review of Relationships between Diarrheal Diseases and Temperature, Rainfall, Flooding, and Drought. Environmental Science and Technology, 50(10), 4905–4922. doi: 10.1021/acs.est.5b06186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu J, & d’Ozouville N (2013). Contaminación del agua en Puerto Ayora: investigación interdisciplinaria aplicada utilizando Escherichia coli como una bacteria indicador Informe Galápagos 2011-2012. Puerto Ayora, Galapagos: Dirección del Parque Nacional Galápagos, Consejo de Gobierno del Régimen Especial de Galápagos, Charles Darwin Foundation and Galapagos Conservancy. [Google Scholar]
- McKone TE, & Daniels JI (1991). Estimating human exposure through multiple pathways from air, water, and soil. Regulatory Toxicology and Pharmacology, 13(1), 36–61. doi: 10.1016/0273-2300(91)90040-3 [DOI] [PubMed] [Google Scholar]
- Moe CL, & Rheingans RD (2006). Global challenges in water, sanitation and health. Journal of Water and Health, 4(1), 41–58. doi: 10.2166/wh.2005.039 [DOI] [PubMed] [Google Scholar]
- Ngure FM, Humphrey JM, Mbuya MNN, Majo F, Mutasa K, Govha M, … Stoltzfus RJ (2013). Formative Research on Hygiene Behaviors and Geophagy among Infants and Young Children and Implications of Exposure to Fecal Bacteria. American Journal of Tropical Medicine and Hygiene, 89(4), 709–716. doi: 10.4269/ajtmh.12-0568 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicolle LE, Bradley S, Colgan R, Rice JC, Schaeffer A, Hooton TM, … American Society of, N. (2005). Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asymptomatic Bacteriuria in Adults. Clinical Infectious Diseases, 40(5), 643–654. doi: 10.1086/427507 [DOI] [PubMed] [Google Scholar]
- Page R, Bentley M, & Waldrop J (2013). People Live Here: Maternal and Child Health on Isla Isabela, Galapagos. In Walsh SJ & Mena CF (Eds.), Science and Conservation in the Galapagos Islands (pp. 141–153). New York, NY: Springer-Verlag. [Google Scholar]
- Pickering AJ, Davis J, Walters SP, Horak HM, Keymer DP, Mushi D, … Boehm AB (2010). Hands, water, and health: Fecal contamination in Tanzanian communities with improved, non-networked water supplies. Environmental Science and Technology, 44(9), 3267–3272. doi: 10.1021/es903524m [DOI] [PubMed] [Google Scholar]
- Piernas C, Barquera S, & Popkin BM (2013). Current patterns of water and beverage consumption among Mexican children and adolescents aged 1-18 years: Analysis of the Mexican National Health and Nutrition Survey 2012. Public Health Nutrition, 17(10), 2166–2175. doi: 10.1017/S1368980014000998 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salles MJC, Zurita J, Mejía C, Villegas MV, Alvarez C, Bavestrello L, … Latin America Working Group on Bacterial, R. (2013). Resistant Gram-negative infections in the outpatient setting in Latin America. Epidemiology and Infection, 141(12), 2459–2472. doi: 10.1017/S095026881300191X [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schep S, Ruesen M, Lujan Gallegos V, Van Beukering P, & Botzen W (2014). Does tourism growth on the Galapagos Islands contribute to sustainable economic development? Ecuador: Wolfs Company, Bonaire, Instituto de Estudios Ambientales (IVM) de la Universidad VU de Amsterdam, Países Bajos. [Google Scholar]
- Simmering JE, Tang F, Cavanaugh JE, Polgreen LA, & Polgreen PM (2017). The Increase in Hospitalizations for Urinary Tract Infections and the Associated Costs in the United States, 1998-2011. Open Forum Infectious Diseases, 4(1), ofw281. doi: 10.1093/ofid/ofw281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sly PD, & Flack F (2008). Susceptibility of Children to Environmental Pollutants. Annals of the New York Academy of Sciences, 1140(1), 163–183. doi: 10.1196/annals.1454.017 [DOI] [PubMed] [Google Scholar]
- Tandogdu Z, & Wagenlehner FME (2016). Global epidemiology of urinary tract infections. Current Opinion in Infectious Diseases, 29(1), 73–79. doi: 10.1097/QCO.0000000000000228 [DOI] [PubMed] [Google Scholar]
- Taylor JE, Hardner J, & Stewart M (2009). Ecotourism and economic growth in the Galapagos: an island economy-wide analysis. Environment and Development Economics, 14(2), 139–162. doi: 10.1017/s1355770x08004646 [DOI] [Google Scholar]
- Thompson AL (2012). Developmental origins of obesity: Early feeding environments, infant growth, and the intestinal microbiome. American Journal of Human Biology, 24(3), 350–360. doi: 10.1002/ajhb.22254 [DOI] [PubMed] [Google Scholar]
- UN. (2010). Resolution 64/292. The human right to water and sanitation. Geneva, Switzerland: United Nations. [Google Scholar]
- UN. (2018). Sustainable development goal 6 synthesis report 2018 on water and sanitation. New York: United Nations. [Google Scholar]
- Walsh SJ, McCleary AL, Heumann BW, Brewington L, Raczkowski EJ, & Mena CF (2010). Community Expansion and Infrastructure Development: Implications for Human Health and Environmental Quality in the Galápagos Islands of Ecuador. Journal of Latin American Geography, 9(3), 137–159. [Google Scholar]
- Weisel CP, & Jo W-K (1996). Ingestion, Inhalation, and Dermal Exposures to Chloroform and Trichloroethene from Tap Water. Environmental health perspectives, 104(1), 48–51. doi: 10.1289/ehp.9610448 [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO. (2011). WHO Guidelines for Drinking-water Quality, 4th ed. Geneva: World Health Organization. [Google Scholar]
- WHO. (2016). Mortality and burden of disease from water and sanitation. Geneva: World Health Organization. [Google Scholar]
- WHO. (2018). WASH and health working together. A how-to’ guide for neglected tropical disease programmes. Geneva: World Health Organization. [Google Scholar]
- WHO & UNICEF. (2017). Progress on drinking water, sanitation and hygiene: 2017 update and SDG baselines. Geneva: : World Health Organization and United Nation’s Children Fund. [Google Scholar]
- Wild C, & Kleinjans JCS (2003). Children and increased susceptibility to environmental carcinogens: evidence or empathy? Cancer Epidemiology Biomarkers & Prevention, 12(12), 1389–1394. [PubMed] [Google Scholar]
- Xue J, Zartarian V, Moya J, Freeman N, Beamer P, Black K, … Shalat S (2007). A Meta-Analysis of Children’s Hand-to-Mouth Frequency Data for Estimating Nondietary Ingestion Exposure. Risk Analysis, 27(2), 411–420. doi: 10.1111/j.1539-6924.2007.00893.x [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.