

ABSTRACT
Background
Socioeconomic inequities in diet quality are stable or widening in the United States; however, these trends have not been well characterized in other nations. Moreover, purpose-developed indices of inequities that can provide a more comprehensive and precise perspective of trends in absolute and relative dietary gaps and gradients using multiple indicators of socioeconomic position (SEP) have not yet been used, and can inform strategies to narrow dietary inequities.
Objectives
We quantified nationally representative trends in absolute and relative gaps and gradients in diet quality between 2004 and 2015 according to 3 indicators of SEP among adults in Canada.
Methods
Adults (≥18 y old) who participated in the nationally representative, cross-sectional Canadian Community Health Survey—Nutrition in 2004 (n = 20,880) or 2015 (n = 13,970) were included. SEP was classified using household income (quintiles), education (5 categories), and neighborhood deprivation (quintiles). Dietary intake data from 24-h recalls were used to derive Healthy Eating Index-2015 (HEI-2015) scores. Dietary inequities were quantified using absolute and relative gaps (between the most and least disadvantaged) and absolute [Slope Index of Inequality (SII)] and relative gradients (Relative Index of Inequality). Overall and sex-stratified multivariable linear regression and generalized linear models examined trends in HEI-2015 scores between 2004 and 2015.
Results
Mean HEI-2015 scores improved from 55.3 to 59.0 (maximum: 100); however, these trends were not consistently equitable. Whereas inequities in HEI-2015 scores were stable in the total population and in females, the absolute gap [from 1.60 (95% CI: 0.09, 3.10) to 4.27 (95% CI: 2.20, 6.34)] and gradient [from SII = 2.09 (95% CI: 0.45, 3.73) to SII = 4.84 (95% CI: 2.49, 7.20)] in HEI-2015 scores for household income, and the absolute gradient for education [from SII = 8.06 (95% CI: 6.41, 9.71) to SII = 10.52 (95% CI: 8.73, 12.31)], increased in males.
Conclusions
Absolute and relative gaps and gradients in overall diet quality remained stable or widened between 2004 and 2015 among adults in Canada.
Keywords: diet quality, dietary inequities, Healthy Eating Index, relative inequities, absolute inequities, adults
Introduction
Individuals’ position in the social hierarchy, termed socioeconomic position (SEP), shapes their access to health-promoting resources, along with their exposure and vulnerability to adverse environmental conditions (1–3). These inequities in the conditions of daily life have significant dietary consequences, as individuals with a lower SEP have poorer diet quality than their more advantaged counterparts (4–6). Dietary inequities contribute substantially to health inequities (7), and therefore understanding trends in dietary inequities is a priority to inform early action to address widening inequities. In the United States, absolute inequities in the diet quality of lower-SEP groups have persisted or widened over the past several decades (6, 8–13). However, these trends have not been well characterized in other nations, including in Canada.
Trends in inequities in diet quality can be assessed using different indicators of SEP and indices of inequities, the selection of which can lead to different conclusions regarding the presence, strength, direction, and/or rate of change of inequities (14). In the current study, we examined trends according to 3 commonly used indicators of SEP, including household income, educational attainment, and neighborhood deprivation. These indicators reflect both similar and distinct mechanisms that generate and perpetuate inequities. Household income most strongly reflects access to material resources, whereas educational attainment also captures access to material resources through its association with occupation and income, while additionally reflecting cultural and knowledge-related assets and prestige (15–17). Indicators of neighborhood deprivation typically reflect both compositional and contextual features of “place” that shape social advantage/disadvantage (18). Comparing trends in diet quality among these indicators may provide insight into important axes of dietary stratification (19, 20). Subgroup analyses that acknowledge the heterogeneity of statuses that exist within SEP groups, such as differences according to sex/gender, are also important because different subgroups may experience their SEP differently owing to the other social positions they occupy (19).
Prior US studies have examined directional trends in dietary inequities on an absolute basis (6, 8–13). Although helpful, such analyses provide a limited perspective of dietary inequities. The WHO (21) and others (22–24) have outlined indices of inequities that can be used to more comprehensively and precisely quantify the magnitude and direction of trends in absolute and relative dietary gaps and gradients, and thereby help to identify the types of inequities and populations to prioritize for intervention. Indices that quantify gaps reflect differences in diet quality between those situated at the extreme ends of the socioeconomic spectrum (25). Indices that quantify gradients also reflect differences in diet quality between the highest and lowest SEP groups, but they do so in a manner that accounts for the slope of the entire distribution, along with the rank and size of the various SEP groups (25). These dietary gaps and gradients can be quantified on an absolute or a relative basis. Absolute measures reflect a materialist perspective that attaches greater importance to ensuring that diet quality remains high at a population level rather than to its distribution (14, 26). Relative measures endorse a stricter egalitarian psychosocial perspective that diet quality should be equal in all groups, regardless of its absolute level or how greater equity is achieved (14, 26). To our knowledge, these indices have not yet been used to quantify absolute and relative gaps and gradients in diet quality. The purpose of this study was to quantify nationally representative trends in absolute and relative gaps and gradients in diet quality between 2004 and 2015 according to 3 indicators of SEP among females and males in Canada.
Methods
Study design and participants
The 2004 and 2015 Canadian Community Health Survey (CCHS)—Nutrition cycles were cross-sectional, nationally and provincially representative surveys of Canadians’ dietary intake. Details of both surveys have been described in full elsewhere (27–30). The surveys were designed to be comparable, and thus, except where indicated, consistent methods were used in both years (28).
The surveys used multistage, stratified, clustered, probabilistic sampling procedures to sample private dwellings in rural and urban locations in all 10 Canadian provinces. The surveys covered 98% of the Canadian population, excluding residents living in the 3 territories, institutions, on Indigenous reserves, and all members of the Canadian Armed Forces. Response rates were 77% and 62% in 2004 and 2015, respectively. This study used data from adults (≥18 y old) who completed the CCHS in 2004 or 2015 (Figure 1). Individuals whose food intake was null or deemed unreliable by Statistics Canada, or who were pregnant or breastfeeding, were excluded. The final analytic sample was 34,850 adults, including n = 20,880 in 2004 and n = 13,970 in 2015.
FIGURE 1.
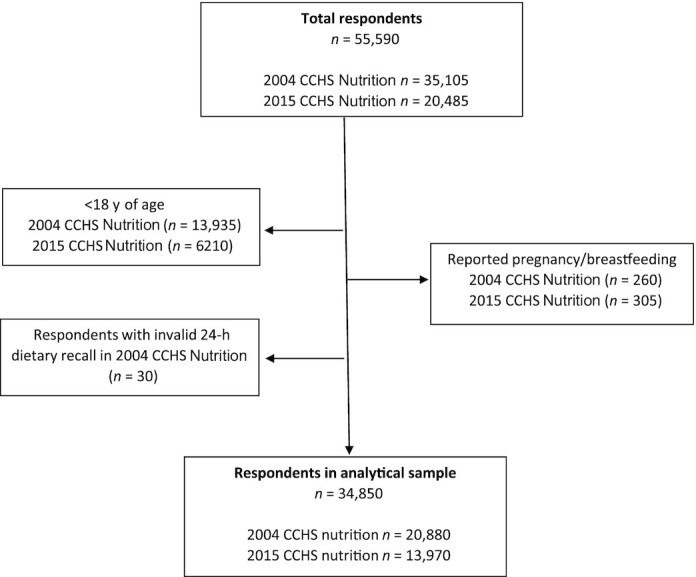
Participant flowchart for the 2004 and 2015 CCHS—Nutrition cycles (unweighted data). CCHS, Canadian Community Health Survey.
The procedures followed were in accordance with the ethical standards of the Helsinki Declaration of 1975 as revised in 1983. The Conjoint Health Research Ethics Board at the University of Calgary deemed this study exempt from ethical approval because it involved secondary data analysis of a survey conducted by Statistics Canada.
Variables
All analyses were preplanned. The primary outcomes were trends in Healthy Eating Index (HEI)-2015 total scores according to 3 SEP indicators and 4 indices of inequities, both overall and stratified by sex (gender was not available in our data sources). Secondary outcomes examined these trends for HEI-2015 component scores.
Indicators of SEP
Participants reported total household income before taxes in the previous 12 months. Statistics Canada imputed total household income for 24.1% of adult respondents in 2015 (27, 31), and we used Statistics Canada procedures (32) to impute income for 11.4% of adults in 2004. Statistics Canada uses a nearest neighbor donor approach to impute income based on family structure, residence (e.g., dwelling owned or rented, median tax value by postal code and household size), sociodemographic (e.g., education, main source of income, immigrant status), and health variables (e.g., general health) (32, 33). In addition, partial or full information on range of income was available for 18.9% of our respondents in 2015, and was included in the imputations (31). In a simulation study, Statistics Canada confirmed that the imputation process preserved 89%–94% of all income quintiles (i.e., imputed values fell within the same quintile as what would have been reported) and likely reduced nonresponse biases (32). Respondents’ household income was classified into quintiles based on the adjusted ratio of their total household income to the low-income cutoff corresponding to their household and community size in the year before each survey (34, 35).
Respondents indicated their own educational attainment and the highest educational attainment at a household level. Responses were classified into 5 categories of less than high school, high school, some postsecondary or trade/diploma/certificate, undergraduate degree, and graduate degree or higher. Our main analysis assessed trends in diet quality according to the respondents’ own educational attainment, because education can enhance individuals’ skills, knowledge, prestige, finances, and general capabilities, along with access to societal resources (15, 17, 36). We also conducted a sensitivity analysis using highest educational attainment at a household level to acknowledge that the benefits that accrue to 1 member may also be experienced by other household members.
Neighborhood deprivation was assessed using a Canadian area-based deprivation index that has demonstrated acceptable content, convergent and predictive validity, reliability (i.e., internal coherence), and responsiveness (i.e., sensitivity to differences and changes) (18, 37). The index is based on 6 indicators of material and social deprivation among individuals ≥15 y of age, standardized by age and sex. Values are calculated for the smallest area for which census data are available (i.e., the dissemination area), and on average comprise 400–700 persons. We used methods described by Gamache et al. (38) to assign neighborhoods into quintiles of disadvantage; however, we reverse-scored the items so that quintiles 1 and 5 corresponded to the most and least deprived neighborhoods, respectively.
Diet quality
Participants completed an in-person, computer-assisted 24-h dietary recall to report all foods and beverages consumed the day before the survey. The method for collection of dietary intake data was based on the 5-stage Automated Multiple Pass Method which was developed to improve accuracy of recall (39, 40). A food model booklet was provided in both years to aid in portion size estimation. The majority of dietary intake data were auto-coded (55% in 2004; 75% in 2015; the remainder were manually coded) using the Canadian Nutrient File (2004: 2001b version; 2015: 2015 version) by Statistics Canada. Nutrient intakes were derived from the Canadian Nutrient File, and Canadian Nutrient File codes were subsequently linked to codes from the Food and Nutrient Database for Dietary Studies (41) and the USDA's Food Patterns Equivalents Database (42) to estimate intakes of food groups and other dietary components required to calculate HEI-2015 scores (43).
Adherence to a healthful dietary pattern was evaluated using the HEI-2015, with higher scores indicating greater adherence to recommendations for consumption of adequacy (total fruits, whole fruits, total vegetables, greens and beans, whole grains, dairy, total protein foods, seafood and plant proteins, fatty acids) and moderation components (refined grains, sodium, added sugars, saturated fats) in the 2015–2020 Dietary Guidelines for Americans (range: 0–100) (44, 45). The HEI-2015 is among the most robust diet quality scores (46) because it has shown predictive validity (47), is updated to reflect evolving dietary guidance, and is density-based and therefore not confounded by energy intake (48). HEI scores have been associated with indicators of SEP (49) and chronic disease in numerous studies (47, 50–55) and are recommended for international use (48).
Data analysis
Indices of inequities
Four indices were used to quantify trends in inequities in diet quality using procedures described by the WHO (21). First, absolute dietary gaps were calculated by subtracting the mean HEI-2015 score of the lowest from the highest SEP group (21). Second, absolute dietary gradients were assessed using the Slope Index of Inequality (SII). The SII is a weighted indicator of the difference in HEI-2015 scores between the highest and lowest SEP groups that takes into account the association between SEP and HEI-2015 scores across the entire distribution (i.e., the slope) (21, 23, 24, 56, 57). To calculate the SII, SEP categories were ordered from lowest to highest and weighted by the proportional distribution of the population in each SEP group (21, 58). The cumulative percentage of each group in the distribution was subsequently calculated, and the midpoint of this range was assigned to the group. The SII was obtained by regressing HEI-2015 scores against this ranking variable using a generalized linear model (log-binomial regression) with an identity link function. When the absolute gap or gradient is 0 there is no inequality. Positive values indicate that HEI-2015 scores are higher among the advantaged and negative values indicate that HEI-2015 scores are higher among the disadvantaged. An increase in values therefore indicates a widening of absolute dietary gaps or gradients.
Third, relative dietary gaps were calculated as the ratio of HEI-2015 scores in the highest to the lowest SEP group (21). Fourth, relative dietary gradients were assessed using the Relative Index of Inequality (RII), which is a weighted indicator of the ratio of HEI-2015 scores in the highest to the lowest SEP group that accounts for the ratios of all other SEP groups (21). It was calculated similarly to the SII; however, in this case HEI-2015 scores were regressed against the ranking variable using a generalized linear model with a logarithmic link function (58). Relative gaps and gradients are always positive and take the value of 1 if there is no inequality. Values > 1 indicate that HEI-2015 scores are higher in the advantaged and values < 1 indicate that HEI-2015 scores are higher in the disadvantaged. An increase in values therefore indicates a widening of relative dietary gaps or gradients.
Statistical analyses
Descriptive statistics (e.g., means and frequencies) were used to characterize the samples in 2004 and 2015. HEI-2015 total and component scores were calculated using the National Cancer Institute simple HEI scoring algorithm using the first dietary recall for each participant, which is a recommended approach for describing mean scores at a population level (59). Trends in HEI-2015 total scores by SEP were assessed by treating survey year as a continuous variable in a survey-weighted linear regression model. Multivariable linear regression models examined trends in gaps, whereas generalized linear models (log-binomial regression) examined trends in gradients (SII: identity link function; RII: logarithmic link function), in HEI-2015 total and component scores between 2004 and 2015 in the total population and stratified by sex. Separate models were constructed for each of the 3 indicators of SEP including an interaction term for SEP × survey year to examine trends over time. Analyses in the total population were adjusted for sex, age, and dietary recall day (weekend, weekday including Fridays), whereas sex-stratified analyses were adjusted for age and dietary recall day. We also examined whether trends in the SII and RII differed for younger (18–39 y old), middle-aged (40–64 y old), and older adults (≥65 y old). Because only 1 significant difference was found, these results are not presented.
Missing data were minimal (<1% for all variables except neighborhood deprivation, which had 5.2% missing data) and therefore list-wise deletion was used. Person-specific and bootstrap weights supplied by Statistics Canada were used to account for the complex sampling and to adjust for nonresponse, as well as to ensure accurate estimation of variance components. Analyses were conducted using Stata version 15.0 (Stata Corp.) and SAS version 9.4 (SAS Institute) with P < 0.05 considered statistically significant. Consistent with prior analyses, no adjustments were made for multiple comparisons (6, 8–10).
Sensitivity analysis
In sensitivity analyses we also adjusted for self-reported race/ethnicity (white compared with nonwhite) to examine whether changes in the racial/ethnic composition of the population were driving any differential trends. Given that younger adults may not have fully completed their education at the time of the survey, we also considered the impact on findings of using highest educational attainment at a household rather than an individual level. We considered adjusting for an indicator of misreporting, the ratio of total energy intake to total energy expenditure (TEI:TEE). However, in a logistic regression, we found that the odds of misreporting [TEI < 70% or >142% of TEE (60)] by SEP did not differ between the 2 surveys. This indicates that misreporting is unlikely to have biased our estimates of dietary trends and therefore TEI:TEE was not included in our models.
Results
Descriptive results
Table 1 presents survey-weighted participant characteristics. Mean HEI-2015 total scores were higher in 2015 (59.04 ± 0.23) than in 2004 (55.29 ± 0.16; P < 0.001) (Table 1) both overall, and for all SEP groups, with the exception of individuals with less than a high school education (Table 2). HEI-2015 total scores exhibited a marked socioeconomic patterning in both years (Table 2, Figure 2).
TABLE 1.
Characteristics of adults who participated in the Canadian Community Health Survey—Nutrition in 2004 or 20151
| Variables | 2004 | 2015 |
|---|---|---|
| Age, y | 46.0 ± 17.3 | 48.9 ± 17.5 |
| Sex | ||
| Male | 11,846,000 (50.0) | 13,788,000 (50.0) |
| Female | 11,836,000 (49.9) | 13,778,000 (49.9) |
| Individual educational attainment | ||
| Less than high school | 4,645,000 (19.8) | 3,254,000 (11.8) |
| High school | 4,256,000 (18.1) | 7,337,000 (26.7) |
| Some postsecondary | 10,008,000 (42.6) | 9,259,000 (33.8) |
| Bachelor's degree | 3,139,000 (13.3) | 5,071,000 (18.5) |
| Higher than bachelor's degree | 1,402,000 (5.9) | 2,468,000 (9.0) |
| Household educational attainment | ||
| Less than high school | 2,431,000 (10.4) | 1,920,000 (6.9) |
| High school | 2,603,000 (11.2) | 4,701,000 (17.0) |
| Some postsecondary | 11,126,000 (48.0) | 10,274,000 (37.3) |
| Bachelor's degree | 4,462,000 (19.2) | 6,863,000 (24.9) |
| Higher than bachelor's degree | 2,552,000 (11.0) | 3,748,000 (13.6) |
| Household income (quintile) | ||
| 1 (lowest income) | 4,516,000 (19.1) | 5,431,000 (19.7) |
| 2 | 4,678,000 (19.7) | 5,568,000 (20.1) |
| 3 | 4,615,000 (19.5) | 5,355,000 (19.4) |
| 4 | 4,878,000 (20.6) | 5,386,000 (19.5) |
| 5 (highest income) | 4,941,000 (20.9) | 5,825,000 (21.1) |
| Neighborhood deprivation (quintile) | ||
| 1 (most deprived) | 6,401,000 (28.2) | 6,546,000 (24.9) |
| 2 | 3,502,000 (15.4) | 3,608,000 (13.7) |
| 3 | 4,792,000 (21.1) | 5,818,000 (21.4) |
| 4 | 3,190,000 (14.0) | 4,662,000 (18.4) |
| 5 (least deprived) | 4,742,000 (20.9) | 5,843,000 (21.5) |
| Day of dietary recall | ||
| Weekend | 6,914,000 (29.1) | 7,704,000 (27.9) |
| Weekday | 16,769,000 (70.8) | 19,862,000 (72.0) |
| Race/ethnicity | ||
| White | 19,984,000 (84.5) | 20,569,000 (74.7) |
| Nonwhite | 3,659,000 (15.4) | 6,961,000 (25.2) |
| HEI-2015 total score | 55.29 ± 0.16 | 59.04 ± 0.23 |
2004 weighted n = 23,682,000; 2015 weighted n = 27,566,000. Values are mean ± SD or n (%). Data are weighted to be nationally representative and are rounded in accordance with Statistics Canada's confidentiality policies. HEI, Healthy Eating Index.
TABLE 2.
Trends in HEI-2015 total scores by socioeconomic position among adults who participated in the Canadian Community Health Survey—Nutrition in 2004 or 20151
| HEI-2015 total scores (range: 0–100) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total population | P value for time trend | Males | P value for time trend | Females | P value for time trend | ||||
| 2004 | 2015 | 2004 | 2015 | 2004 | 2015 | ||||
| Household income (quintile) | |||||||||
| 1 (lowest income) | 54.3 (53.5, 55.0) | 57.8 (56.8, 58.6) | <0.001 | 53.2 (52.1, 54.4) | 56.1 (54.7, 57.6) | 0.005 | 55.0 (53.9, 56.0) | 59.1 (57.9, 60.1) | <0.001 |
| 2 | 55.2 (54.4, 56.0) | 58.0 (56.9, 59.0) | <0.001 | 53.5 (52.4, 54.7) | 57.2 (55.7, 58.6) | <0.001 | 56.6 (55.5, 57.7) | 58.7 (57.3, 59.9) | 0.057 |
| 3 | 55.3 (54.5, 56.0) | 59.1 (58.1, 60.0) | <0.001 | 53.6 (52.5, 54.7) | 58.0 (56.8, 59.3) | <0.001 | 57.2 (56.0, 58.2) | 60.0 (58.6, 61.4) | 0.012 |
| 4 | 54.8 (54.1, 55.5) | 59.3 (58.2, 60.4) | <0.001 | 53.9 (52.9, 54.9) | 57.3 (55.7, 58.8) | 0.039 | 55.9 (54.8, 57.0) | 61.4 (59.8, 63.1) | <0.001 |
| 5 (highest income) | 56.8 (56.1, 57.4) | 60.9 (59.9, 61.9) | <0.001 | 54.8 (54.0, 55.7) | 60.4 (58.9, 61.9) | <0.001 | 58.9 (57.9, 59.9) | 61.5 (60.1, 62.9) | 0.007 |
| P value for within-year differences | <0.001 | <0.001 | 0.0014 | <0.001 | <0.001 | <0.001 | |||
| Educational attainment | |||||||||
| Less than high school | 53.7 (53.0, 54.4) | 54.5 (53.3, 55.5) | 0.805 | 52.0 (50.9, 53.1) | 52.9 (51.5, 54.3) | 0.770 | 55.3 (54.4, 56.1) | 56.2 (54.5, 57.9) | 0.959 |
| High school | 53.8 (53.0, 54.6) | 57.6 (56.7, 58.4) | <0.001 | 52.4 (51.2, 53.6) | 55.7 (54.6, 56.8) | <0.001 | 55.0 (53.8, 56.2) | 59.3 (58.0, 60.5) | <0.001 |
| Some postsecondary | 54.8 (54.3, 55.2) | 59.0 (58.2, 59.7) | <0.001 | 53.3 (52.7, 54.0) | 58.6 (57.4, 59.8) | <0.001 | 56.3 (55.6, 57.0) | 59.4 (58.4, 60.4) | <0.001 |
| Bachelor's degree | 59.0 (58.0, 59.9) | 61.9 (60.9, 62.9) | <0.001 | 57.7 (56.4, 59.1) | 61.5 (60.2, 62.9) | 0.001 | 60.2 (58.8, 61.4) | 62.25 (60.7, 63.7) | 0.098 |
| Higher than bachelor's degree | 60.4 (58.8, 61.8) | 63.4 (62.1, 64.7) | 0.008 | 58.8 (57.1, 60.5) | 61.6 (60.0, 63.3) | 0.024 | 62.4 (60.0, 64.8) | 65.25 (63.3, 67.1) | 0.090 |
| P value for within-year differences | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
| Neighborhood deprivation (quintile) | |||||||||
| 1 (most deprived) | 54.1 (53.4, 54.7) | 57.0 (56.1, 57.9) | <0.001 | 52.4 (51.4, 53.4) | 55.7 (54.4, 57.0) | <0.001 | 55.8 (54.9, 56.6) | 58.3 (56.9, 59.6) | 0.010 |
| 2 | 54.5 (53.6, 55.2) | 58.5 (57.2, 59.7) | <0.001 | 53.2 (52.0, 54.3) | 58.2 (56.5, 60.0) | <0.001 | 55.7 (54.4, 56.9) | 58.7 (56.9, 60.4) | 0.021 |
| 3 | 55.5 (54.7, 56.2) | 60.0 (59.0, 60.8) | <0.001 | 53.7 (52.7, 54.7) | 58.6 (57.4, 59.8) | <0.001 | 57.35 (56.3, 58.3) | 61.15 (59.8, 62.4) | <0.001 |
| 4 | 56.0 (55.1, 56.8) | 59.2 (57.9, 60.4) | <0.001 | 55.4 (54.1, 56.7) | 57.4 (55.7, 59.1) | <0.001 | 56.65 (55.3, 57.9) | 60.9 (59.2, 62.5) | <0.001 |
| 5 (least deprived) | 56.9 (56.0, 57.6) | 60.6 (59.6, 61.5) | <0.001 | 55.6 (54.6, 56.6) | 60.4 (59.0, 61.7) | 0.039 | 58.2 (57.0, 59.3) | 60.8 (59.4, 62.1) | 0.010 |
| P value for within-year differences | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
2004 weighted n = 23,682,000; 2015 weighted n = 27,566,000. Values are means (95% CIs) unless otherwise indicated. Analyses were conducted using multivariable linear regression. Data are weighted to be nationally representative and are adjusted for age, sex (except in sex-stratified analyses), and dietary recall day. Weighted sample sizes are rounded in accordance with Statistics Canada's confidentiality policies. HEI, Healthy Eating Index.
FIGURE 2.
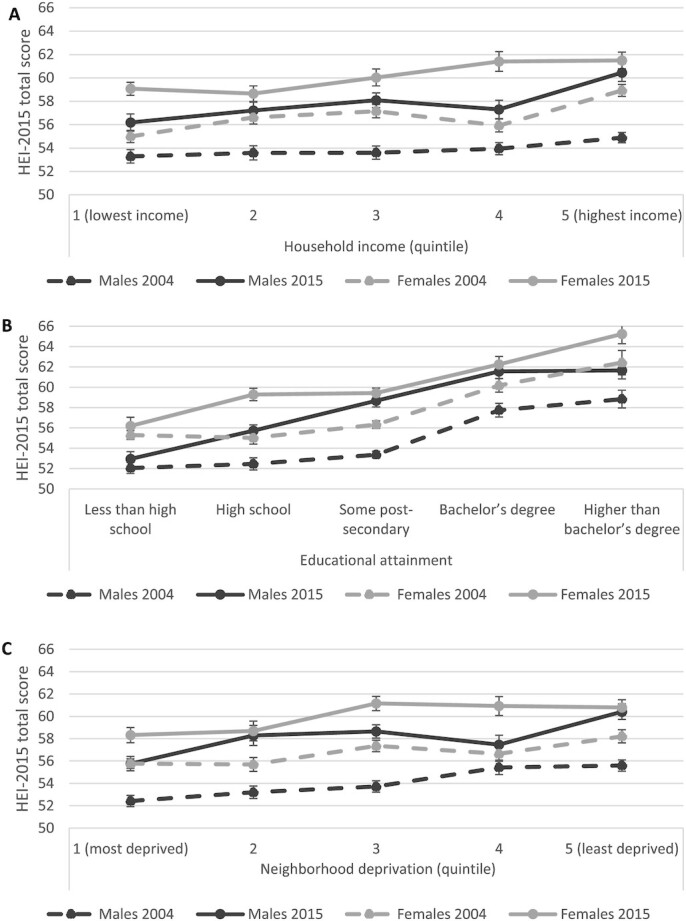
Trends in HEI-2015 total scores by household income (A), educational attainment (B), and neighborhood deprivation (C) among adults who participated in the Canadian Community Health Survey—Nutrition in 2004 (weighted n = 23,682,000) or 2015 (weighted n = 27,566,000). Analyses were conducted using multivariable linear regression. Data are weighted to be nationally representative and are adjusted for age and dietary recall day. HEI, Healthy Eating Index.
Trends in inequities in diet quality between 2004 and 2015
Figure 3 provides a visual summary of trends in HEI-2015 total scores.
FIGURE 3.

Summary of trends in HEI-2015 total scores between 2004 and 2015 by socioeconomic position among adults who participated in the Canadian Community Health Survey—Nutrition in 2004 or 2015. Multivariable linear regression models examined trends in gaps, whereas generalized linear models examined trends in gradients, in HEI-2015 total scores between 2004 and 2015, adjusted for age and dietary recall day. ↔, stable trends; ↑, widening inequities. HEI, Healthy Eating Index.
Absolute gaps in diet quality
There were significant positive absolute gaps in HEI-2015 total scores according to all 3 SEP indicators in 2004 and 2015 (Tables 3 and 4). The positive values indicate that HEI-2015 scores were highest in the advantaged groups. In the total population, absolute gaps in HEI-2015 total and component scores remained stable (i.e., did not change significantly) for all SEP indicators between 2004 and 2015, with the exception of an increase in the absolute gap in scores for whole fruits according to educational attainment. Among males, the absolute gap in HEI-2015 total scores according to household income increased from 1.60 (95% CI: 0.09, 3.10) to 4.27 (95% CI: 2.20, 6.34), with no trends according to educational attainment or neighborhood deprivation. With respect to HEI-2015 components, the absolute gap in scores for fatty acids according to household income, and in scores for whole fruits and whole grains according to educational attainment, increased between 2004 and 2015. Among females, the absolute gap in HEI-2015 total scores remained stable for all SEP indicators. For HEI-2015 components, the absolute gap in scores for whole fruits and for total vegetables according to educational attainment increased, and the absolute gap in scores for total dairy according to neighborhood deprivation declined, between 2004 and 2015.
TABLE 3.
Trends in gaps and gradients in HEI-2015 total and component scores by socioeconomic position among adults who participated in the Canadian Community Health Survey—Nutrition in 2004 or 20151
| Household income | Educational attainment | Neighborhood deprivation | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HEI-2015 scores | 2004 | 2015 | P value for time trend | 2004 | 2015 | P value for time trend | 2004 | 2015 | P value for time trend |
| Absolute gaps (95% CIs) | |||||||||
| Total | 2.50 (1.43, 3.53)** | 3.15 (1.75, 4.55)** | 0.450 | 6.62 (4.99, 8.24)** | 8.93 (7.17, 10.7)** | 0.057 | 2.76 (1.74, 3.76)** | 3.58 (2.22, 4.93)** | 0.270 |
| Total fruits | 0.04 (−0.12, 0.20) | −0.05 (−0.27, 0.17) | 0.528 | 0.54 (0.30, 0.77)** | 0.72 (0.43, 1.01)** | 0.336 | 0.08 (−0.08, 0.25) | 0.23 (0.01, 0.44)* | 0.281 |
| Whole fruits | 0.03 (−0.14, 0.21) | 0.19 (−0.06, 0.43) | 0.352 | 0.40 (0.12, 0.68)* | 1.14 (0.84, 1.44)** | 0.001 | 0.10 (−0.09, 0.27) | 0.39 (0.14, 0.62)* | 0.050 |
| Total vegetables | 0.21 (0.07, 0.35)* | 0.23 (0.03, 0.43)* | 0.846 | 0.26 (0.07, 0.44)* | 0.54 (0.27, 0.80)** | 0.100 | 0.17 (0.03, 0.30)* | 0.36 (0.17, 0.52)** | 0.117 |
| Greens and beans | 0.18 (−0.001, 0.36) | 0.36 (0.12, 0.60)* | 0.244 | 0.77 (0.48, 1.06)** | 1.17 (0.84, 1.50)** | 0.069 | 0.29 (0.10, 0.46)* | 0.42 (0.19, 0.63)** | 0.335 |
| Whole grains | 0.27 (−0.03, 0.56) | 0.12 (−0.29, 0.52) | 0.552 | 0.42 (−0.05, 0.90) | 0.73 (0.22, 1.23)* | 0.395 | 0.38 (0.06, 0.67)* | 0.61 (0.22, 1.00)* | 0.336 |
| Dairy | 0.41 (0.12, 0.69)* | 0.50 (0.15, 0.83)* | 0.727 | 0.57 (0.14, 0.99)* | 0.56 (0.06, 1.05)* | 0.975 | 0.31 (0.02, 0.60)* | 0.07 (−0.26, 0.42) | 0.310 |
| Total protein foods | 0.31 (0.15, 0.46)** | 0.27 (0.12, 0.41)** | 0.716 | 0.45 (0.18, 0.71)* | 0.42 (0.25, 0.58)** | 0.834 | 0.19 (0.03, 0.34)* | 0.16 (0.02, 0.28)* | 0.784 |
| Seafood and plantproteins | 0.28 (0.09, 0.46)* | 0.32 (0.08, 0.56)* | 0.772 | 0.80 (0.48, 1.11)** | 1.16 (0.83, 1.48)** | 0.127 | 0.19 (0.01, 0.34)* | 0.19 (−0.04, 0.42) | 0.945 |
| Fatty acids | −0.22 (−0.56, 0.12) | 0.22 (−0.20, 0.64) | 0.107 | −0.02 (−0.51, 0.48) | 0.33 (−0.19, 0.84) | 0.354 | 0.15 (−0.17, 0.47) | 0.21 (−0.16, 0.58) | 0.804 |
| Refined grains | 0.87 (0.62, 1.11)** | 0.84 (0.50, 1.17)** | 0.880 | 0.55 (0.23, 0.86)* | 0.47 (0.02, 0.92)* | 0.799 | 0.37 (0.13, 0.60)* | 0.44 (0.15, 0.71)* | 0.729 |
| Sodium | −0.05 (−0.33, 0.24) | 0.16 (−0.26, 0.57) | 0.458 | 0.47 (0.10, 0.93)* | 0.84 (0.30, 1.37)* | 0.325 | 0.18 (−0.12, 0.48) | 0.17 (−0.19, 0.54) | 0.985 |
| Added sugars | 0.44 (0.23, 0.65)** | 0.37 (0.12, 0.61)* | 0.627 | 0.91 (0.64, 1.17)** | 0.78 (0.46, 1.10)** | 0.547 | 0.32 (0.12, 0.52)* | 0.29 (0.01, 0.56)* | 0.836 |
| Saturated fats | −0.31 (−0.60, −0.01)* | −0.36 (−0.68, −0.02)* | 0.836 | 0.49 (0.04, 0.93)* | 0.07 (−0.42, 0.55) | 0.186 | 0.05 (−0.23, 0.34) | 0.04 (−0.29, 0.36) | 0.958 |
| Relative gaps (95% CIs) | |||||||||
| Total | 1.04 (1.02, 1.06)** | 1.07 (1.02, 1.08)** | 0.584 | 1.12 (1.09, 1.15)** | 1.16 (1.12, 1.19)** | 0.084 | 1.05 (1.03, 1.06)** | 1.06 (1.03, 1.08)** | 0.351 |
| Total fruits | 1.01 (0.95, 1.07)** | 0.98 (0.90, 1.05)** | 0.531 | 1.19 (1.10, 1.27)** | 1.28 (1.16, 1.41)** | 0.220 | 1.02 (0.97, 1.08)** | 1.08 (1.00, 1.16)** | 0.269 |
| Whole fruits | 1.01 (0.94, 1.07)** | 1.06 (0.97, 1.16)** | 0.364 | 1.15 (1.04, 1.26)** | 1.46 (1.32, 1.61)** | 0.001 | 1.03 (0.96, 1.10)** | 1.14 (1.04, 1.24)** | 0.062 |
| Total vegetables | 1.06 (1.02, 1.11)** | 1.08 (1.01, 1.15)** | 0.743 | 1.08 (1.02, 1.14)** | 1.18 (1.08, 1.28)** | 0.068 | 1.05 (1.01, 1.09)** | 1.12 (1.05, 1.18)** | 0.098 |
| Greens and beans | 1.14 (0.98, 1.30)** | 1.26 (1.06, 1.45)** | 0.371 | 1.74 (1.43, 2.05)** | 2.13 (1.70, 2.57)** | 0.130 | 1.24 (1.07, 1.40)** | 1.31 (1.17, 1.43)** | 0.568 |
| Whole grains | 1.12 (0.97, 1.26)** | 1.03 (0.91, 1.15)** | 0.352 | 1.17 (0.97, 1.38)** | 1.23 (1.05, 1.40)** | 0.707 | 1.17 (1.02, 1.32)** | 1.18 (1.05, 1.32)** | 0.867 |
| Dairy | 1.09 (1.02, 1.17)** | 1.10 (1.02, 1.17)** | 0.727 | 1.14 (1.03, 1.25)** | 1.11 (1.01, 1.22)** | 0.775 | 1.07 (1.00, 1.14)** | 1.01 (0.94, 1.08)** | 0.254 |
| Total protein foods | 1.11 (1.05, 1.17)** | 1.06 (1.03, 1.10)** | 0.202 | 1.16 (1.06, 1.27)** | 1.10 (1.06, 1.15)** | 0.278 | 1.06 (1.01, 1.12)** | 1.04 (1.00, 1.07)** | 0.419 |
| Seafood and plantproteins | 1.17 (1.04, 1.31)** | 1.14 (1.02, 1.26)** | 0.717 | 1.54 (1.31, 1.77)** | 1.63 (1.40, 1.86)** | 0.586 | 1.11 (1.00, 1.22)** | 1.08 (0.97, 1.19)** | 0.742 |
| Fatty acids | 0.95 (0.89, 1.02)** | 1.04 (0.95, 1.12)** | 0.103 | 0.99 (0.89, 1.09)** | 1.06 (0.95, 1.17)** | 0.344 | 1.03 (0.96, 1.09)** | 1.04 (0.96, 1.12)** | 0.808 |
| Refined grains | 1.10 (1.07, 1.14)** | 1.11 (1.06, 1.15)** | 0.966 | 1.06 (1.02, 1.10)** | 1.06 (1.00, 1.12)** | 0.924 | 1.04 (1.01, 1.07)** | 1.05 (1.01, 1.09)** | 0.674 |
| Sodium | 0.99 (0.94, 1.04)** | 1.02 (0.95, 1.09)** | 0.459 | 1.08 (1.00, 1.17)** | 1.15 (1.05, 1.26)** | 0.310 | 1.03 (0.97, 1.08)** | 1.02 (0.96, 1.09)** | 0.974 |
| Added sugars | 1.05 (1.02, 1.08)** | 1.04 (1.01, 1.07)** | 0.632 | 1.11 (1.07, 1.14)** | 1.09 (1.05, 1.14)** | 0.586 | 1.03 (1.01, 1.06)** | 1.03 (1.00, 1.07)** | 0.876 |
| Saturated fats | 0.95 (0.91, 0.99)** | 0.94 (0.89, 0.99)** | 0.817 | 1.07 (1.00, 1.14)** | 1.01 (0.93, 1.08)** | 0.200 | 1.00 (0.96, 1.05)** | 1.00 (0.95, 1.05)** | 0.963 |
| Absolute gradients: Slope Index of Inequality (95% CIs) | |||||||||
| Total | 3.37 (2.27, 4.47)** | 4.69 (3.09, 6.28)** | 0.072 | 8.76 (7.56, 9.96)** | 9.57 (8.17, 10.98)** | 0.096 | 3.61 (2.30, 4.93)** | 4.64 (2.91, 6.37)** | 0.378 |
| Total fruits | 0.14 (−0.04, 0.33) | 0.03 (−0.22, 0.30) | 0.787 | 0.86 (0.66, 1.06)** | 0.83 (0.59, 1.08)** | 0.702 | 0.15 (−0.06, 0.36) | 0.31 (0.03, 0.58)* | 0.375 |
| Whole fruits | 0.11 (−0.08, 0.31) | 0.31 (0.03, 0.59)* | 0.095 | 0.84 (0.63, 1.06)** | 1.29 (1.03, 1.55)** | 0.001 | 0.18 (−0.05, 0.41) | 0.49 (0.18, 0.80)* | 0.123 |
| Total vegetables | 0.31 (0.16, 0.47)** | 0.36 (0.14, 0.58)* | 0.639 | 0.35 (0.19, 0.51)** | 0.66 (0.45, 0.86)** | 0.005 | 0.21 (0.04, 0.38)* | 0.42 (0.19, 0.66)** | 0.170 |
| Greens and beans | 0.24 (0.04, 0.44)* | 0.45 (0.17, 0.72)* | 0.163 | 0.82 (0.61, 1.03)** | 1.12 (0.87, 1.37)** | 0.021 | 0.41 (0.18, 0.63)** | 0.57 (0.29, 0.86)** | 0.373 |
| Whole grains | 0.29 (−0.04, 0.62) | 0.34 (−0.11, 0.80) | 0.722 | 0.74 (0.39, 1.09)** | 0.87 (0.44, 1.29)** | 0.436 | 0.40 (0.02, 0.77)* | 0.78 (0.28, 1.28)* | 0.260 |
| Dairy | 0.49 (0.15, 0.83)* | 0.57 (0.17, 0.98)* | 0.566 | 0.72 (0.36, 1.07)** | 0.29 (−0.10, 0.68) | 0.179 | 0.48 (0.11, 0.84)* | 0.16 (−0.27, 0.60) | 0.260 |
| Total protein foods | 0.30 (0.13, 0.48)* | 0.29 (0.12, 0.46)* | 0.518 | 0.67 (0.48, 0.87)** | 0.24 (0.08, 0.40)* | 0.010 | 0.21 (0.02, 0.41)* | 0.26 (0.09, 0.43)* | 0.755 |
| Seafood and plantproteins | 0.24 (0.03, 0.46)* | 0.43 (0.15, 0.71)** | 0.235 | 1.06 (0.85, 1.27)** | 1.13 (0.87, 1.40)** | 0.472 | 0.22 (0.01, 0.43)* | 0.37 (0.08, 0.66)* | 0.443 |
| Fatty acids | −0.13 (−0.53, 0.26) | 0.33 (−0.15, 0.82) | 0.095 | 0.07 (−0.31, 0.46) | 0.39 (−0.03, 0.83) | 0.163 | 0.19 (−0.23, 0.61) | 0.27 (−0.20, 0.76) | 0.799 |
| Refined grains | 1.09 (0.82, 1.36)** | 1.31 (0.93, 1.70)** | 0.333 | 0.43 (0.15, 0.72)* | 0.78 (0.41, 1.14)** | 0.142 | 0.40 (0.10, 0.71)* | 0.30 (−0.07, 0.67) | 0.655 |
| Sodium | −0.04 (−0.37, 0.28) | 0.14 (−0.32, 0.61) | 0.749 | 0.54 (0.17, 0.91)* | 0.79 (0.38, 1.21)** | 0.705 | 0.16 (−0.23, 0.56) | 0.15 (−0.31, 0.62) | 0.992 |
| Added sugars | 0.57 (0.34, 0.80)** | 0.46 (0.15, 0.77)* | 0.768 | 1.11 (0.86, 1.36)** | 0.99 (0.68, 1.30)** | 0.949 | 0.50 (0.24, 0.76)** | 0.45 (0.11, 0.80)* | 0.795 |
| Saturated fats | −0.27 (−0.60, 0.05) | −0.38 (−0.77, 0.005) | 0.657 | 0.47 (0.09, 0.84)* | 0.13 (−0.24, 0.51) | 0.179 | 0.06 (−0.32, 0.44) | 0.05 (−0.37, 0.48) | 0.984 |
| Relative gradients: Relative Index of Inequality (95% CIs) | |||||||||
| Total | 1.06 (1.04, 1.08)** | 1.08 (1.05, 1.11)** | 0.104 | 1.17 (1.14, 1.19)** | 1.17 (1.14, 1.20)** | 0.290 | 1.06 (1.04, 1.09)** | 1.08 (1.05, 1.11)** | 0.527 |
| Total fruits | 1.06 (1.00, 1.13) | 1.01 (0.92, 1.11) | 0.732 | 1.35 (1.26, 1.44)** | 1.33 (1.22, 1.45)** | 0.728 | 1.05 (0.98, 1.13) | 1.11 (1.01, 1.22)* | 0.361 |
| Whole fruits | 1.06 (0.99, 1.14) | 1.11 (1.01, 1.22)* | 0.095 | 1.36 (1.20, 1.46)** | 1.53 (1.40, 1.67)** | 0.004 | 1.08 (0.99, 1.17) | 1.18 (1.07, 1.32)* | 0.131 |
| Total vegetables | 1.11 (1.06, 1.16) | 1.13 (1.05, 1.21) | 0.538 | 1.11 (1.06, 1.17) | 1.24 (1.16, 1.32) | 0.003 | 1.07 (1.01, 1.12) | 1.14 (1.06, 1.23) | 0.149 |
| Greens and beans | 1.24 (1.05, 1.46)* | 1.36 (1.13, 1.64)* | 0.264 | 1.91 (1.62, 2.24)** | 2.12 (1.78, 2.53)** | 0.229 | 1.39 (1.16, 1.66)** | 1.44 (1.20, 1.74)** | 0.751 |
| Whole grains | 1.16 (1.01, 1.33)* | 1.09 (0.97, 1.23) | 0.945 | 1.39 (1.21, 1.60)** | 1.28 (1.14, 1.43)** | 0.880 | 1.16 (1.00, 1.36)* | 1.21 (1.06, 1.38)* | 0.772 |
| Dairy | 1.12 (1.03, 1.20)* | 1.12 (1.03, 1.22)* | 0.746 | 1.18 (1.08, 1.28)** | 1.06 (0.98, 1.01) | 0.118 | 1.12 (1.03, 1.22)* | 1.03 (0.94, 1.13) | 0.158 |
| Total protein foods | 1.11 (1.05, 1.18)** | 1.07 (1.03, 1.12)* | 0.828 | 1.26 (1.18, 1.35)** | 1.06 (1.02, 1.10)* | 0.001 | 1.08 (1.01, 1.15)* | 1.06 (1.02, 1.11)* | 0.734 |
| Seafood and plantproteins | 1.16 (1.03, 1.32)* | 1.21 (1.07, 1.37)* | 0.477 | 1.86 (1.63, 2.11)** | 1.62 (1.45, 1.82)** | 0.272 | 1.14 (1.01, 1.29)* | 1.17 (1.03, 1.32)* | 0.784 |
| Fatty acids | 0.97 (0.89, 1.05) | 1.06 (0.96, 1.17) | 0.092 | 1.01 (0.93, 1.09) | 1.07 (0.99, 1.17) | 0.172 | 1.03 (0.95, 1.13) | 1.05 (0.96, 1.15) | 0.812 |
| Refined grains | 1.13 (1.10, 1.17)** | 1.17 (1.12, 1.23)** | 0.254 | 1.05 (1.01, 1.09)* | 1.10 (1.05, 1.15)** | 0.125 | 1.04 (1.01, 1.08)* | 1.03 (0.99, 1.08) | 0.711 |
| Sodium | 0.99 (0.93, 1.05) | 1.02 (0.94, 1.11) | 0.763 | 1.10 (1.03, 1.17)* | 1.14 (1.06, 1.22)** | 0.819 | 1.02 (0.95, 1.10) | 1.02 (0.94, 1.10) | 0.972 |
| Added sugars | 1.07 (1.04, 1.10)** | 1.05 (1.01, 1.10)* | 0.800 | 1.14 (1.10, 1.17)** | 1.12 (1.08, 1.17)** | 0.958 | 1.06 (1.03, 1.09)** | 1.05 (1.01, 1.10)* | 0.806 |
| Saturated fats | 0.95 (0.91, 1.00) | 0.94 (0.88, 1.00) | 0.700 | 1.07 (1.01, 1.13)* | 1.02 (0.96, 1.08) | 0.185 | 1.00 (0.95, 1.06) | 1.00 (0.94, 1.07) | 0.979 |
2004 weighted n = 23,682,000; 2015 weighted n = 27,566,000. Multivariable linear regression models examined trends in gaps, whereas generalized linear models examined trends in gradients, in HEI-2015 total and component scores between 2004 and 2015. Data are weighted to be nationally representative and are adjusted for age, sex, and dietary recall day. Weighted sample sizes are rounded in accordance with Statistics Canada's confidentiality policies. HEI, Healthy Eating Index.
*P < 0.05 for within-year inequities, **P < 0.001 for within-year inequities.
TABLE 4.
Trends in gaps and gradients in HEI-2015 total and component scores by socioeconomic position among males and females who participated in the Canadian Community Health Survey—Nutrition in 2004 or 20151
| Males | Females | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Household income | Educational attainment | Neighborhood deprivation | Household income | Educational attainment | Neighborhood deprivation | |||||||||||||
| HEI-2015 scores | 2004 | 2015 | P value for time trend | 2004 | 2015 | P value for time trend | 2004 | 2015 | P value for time trend | 2004 | 2015 | P value for time trend | 2004 | 2015 | P value for time trend | 2004 | 2015 | P value for time trend |
| Absolute gaps (95% CIs) | ||||||||||||||||||
| Total | 1.60 (0.09, 3.10)* | 4.27 (2.20, 6.34)** | 0.043 | 6.73 (4.74, 8.79)** | 8.70 (6.53, 10.91)** | 0.202 | 3.20 (1.75, 4.59)** | 4.70 (2.75, 6.54)** | 0.216 | 3.90 (2.44, 5.42)** | 2.47 (0.59, 4.34)* | 0.221 | 7.10 (4.58, 9.66)** | 9.00 (6.45, 11.65)** | 0.287 | 2.50 (0.98, 3.87)* | 2.40 (0.56, 4.37)* | 0.974 |
| Total fruits | −0.01 (−0.28, 0.26) | 0.01 (−0.36, 0.37) | 0.942 | 0.66 (0.31, 1.01)** | 0.91 (0.52, 1.29)** | 0.359 | 0.06 (−0.18, 0.30) | 0.35 (0.05, 0.65)* | 0.132 | 0.20 (−0.01, 0.40) | −0.06 (−0.37, 0.24) | 0.153 | 0.51 (0.19, 0.83)* | 0.52 (0.09, 0.93)* | 0.991 | 0.13 (−0.09, 0.34) | 0.10 (−0.18, 0.39) | 0.905 |
| Whole fruits | 0.05 (−0.24, 0.34) | 0.27 (−0.13, 0.67) | 0.400 | 0.47 (0.07, 0.87)* | 1.21 (0.79, 1.61)** | 0.013 | 0.09 (−0.18, 0.35) | 0.51 (0.18, 0.82)* | 0.051 | 0.16 (−0.09, 0.40) | 0.15 (−0.16, 0.46) | 0.998 | 0.46 (0.05, 0.63)* | 1.07 (0.63, 1.49)** | 0.045 | 0.12 (−0.10, 0.34) | 0.26 (−0.05, 0.57) | 0.477 |
| Total vegetables | 0.10 (−0.12, 0.32) | 0.11 (−0.14, 0.37) | 0.959 | 0.26 (0.01, 0.50)* | 0.24 (−0.15, 0.63) | 0.967 | 0.20 (0.01, 0.39)* | 0.35 (0.09, 0.58)* | 0.401 | 0.40 (0.22, 0.56)** | 0.48 (0.21, 0.75)** | 0.553 | 0.33 (0.04, 0.63)* | 0.84 (0.54, 1.13)** | 0.019 | 0.16 (−0.02, 0.33)* | 0.37 (0.14, 0.59)* | 0.136 |
| Greens and beans | 0.09 (−0.18, 0.34) | 0.29 (−0.04, 0.61) | 0.358 | 0.70 (0.35, 1.06)** | 1.02 (0.58, 1.47)** | 0.263 | 0.26 (0.01, 0.53)* | 0.49 (0.19, 0.78)* | 0.277 | 0.33 (0.09, 0.57)* | 0.51 (0.15, 0.85)* | 0.418 | 0.89 (0.43, 1.34)** | 1.32 (0.87, 1.76)** | 0.186 | 0.31 (0.07, 0.54)* | 0.34 (0.03, 0.65)* | 0.852 |
| Whole grains | 0.15 (−0.23, 0.53) | 0.49 (−0.07, 1.04) | 0.333 | 0.41 (−0.12, 0.95) | 1.33 (0.68, 1.99)** | 0.034 | 0.71 (0.28, 1.13)* | 1.05 (0.52, 1.58)** | 0.335 | 0.45 (0.01, 0.89)* | −0.14 (−0.71, 0.44) | 0.101 | 0.50 (−0.26, 1.27) | 0.04 (−0.75, 1.27) | 0.414 | 0.04 (−0.36, 0.44) | 0.16 (−0.37, 0.68) | 0.721 |
| Total dairy | 0.42 (−0.01, 0.84) | 0.60 (0.12, 1.07)* | 0.576 | 0.90 (0.34, 1.46)* | 0.31 (−0.29, 0.91) | 0.166 | 0.05 (−0.33, 0.45) | 0.47 (−0.01, 0.96) | 0.192 | 0.55 (0.16, 0.93)** | 0.49 (0.01, 0.98)* | 0.867 | 0.27 (−0.40, 0.96) | 0.81 (0.07, 1.53)* | 0.293 | 0.59 (0.19, 0.98)* | −0.34 (−0.82, 0.14) | 0.004 |
| Total protein foods | 0.18 (−0.05, 0.39) | 0.30 (0.09, 0.49)* | 0.430 | 0.51 (0.19, 0.83)* | 0.31 (0.05, 0.56)* | 0.325 | 0.32 (0.08, 0.53)* | 0.19 (0.02, 0.36)* | 0.408 | 0.43 (0.21, 0.65)** | 0.18 (−0.04, 0.40) | 0.114 | 0.36 (−0.04, 0.76) | 0.54 (0.31, 0.77)** | 0.445 | 0.06 (−0.14, 0.27) | 0.12 (−0.07, 0.31) | 0.698 |
| Seafood and plantproteins | 0.24 (−0.03, 0.51) | 0.22 (−0.15, 0.58) | 0.909 | 0.77 (0.37, 1.16)** | 1.08 (0.64, 1.52)** | 0.311 | 0.25 (0.01, 0.49)* | 0.19 (−0.14, 0.53) | 0.774 | 0.34 (0.08, 0.59)* | 0.45 (0.13, 0.76)* | 0.600 | 0.82 (0.34, 1.28)* | 1.23 (0.78, 1.68)** | 0.232 | 0.11 (−0.12, 0.35) | 0.19 (−0.11, 0.49) | 0.690 |
| Fatty acids | −0.34 (−0.86, 0.16) | 0.45 (−0.14, 1.04) | 0.040 | −0.20 (−0.88, 0.47) | 0.04 (−0.58, 0.66) | 0.608 | 0.16 (−0.31, 0.64) | 0.05 (−0.48, 0.60) | 0.774 | −0.10 (−0.55, 0.34) | −0.04 (−0.64, 0.56) | 0.865 | 0.26 (−0.52, 1.03) | 0.64 (−0.16, 1.44) | 0.500 | 0.14 (−0.30, 0.57) | 0.37 (−0.13, 0.87) | 0.690 |
| Refined grains | 1.08 (0.69, 1.45)** | 1.22 (0.47, 1.68)** | 0.651 | 0.34 (−0.10, 0.78) | 0.19 (−0.46, 0.84) | 0.722 | 0.37 (0.01, 0.70)* | 0.39 (−0.04, 0.81) | 0.598 | 0.72 (0.39, 1.04)** | 0.48 (0.04, 0.92)* | 0.381 | 0.80 (0.38, 1.20)** | 0.78 (0.20, 1.34)* | 0.951 | 0.38 (0.09, 0.67)* | 0.50 (0.11, 0.87)* | 0.582 |
| Sodium | −0.10 (−0.56, 0.37) | 0.35 (−0.27, 0.98) | 0.279 | 0.26 (−0.34, 0.88) | 0.98 (0.26, 1.70)* | 0.147 | 0.24 (−0.21, 0.69) | 0.07 (−0.43, 0.55) | 0.766 | −0.03 (−0.41, 0.36) | −0.01 (−0.57, 0.55) | 0.965 | 0.75 (0.10, 1.39)* | 0.70 (−0.10, 1.48) | 0.912 | 0.10 (−0.28, 0.49) | 0.29 (−0.22, 0.80) | 0.491 |
| Added sugars | 0.33 (0.01, 0.64)* | 0.18 (−0.19, 0.57) | 0.562 | 0.95 (0.60, 1.29)** | 0.63 (0.15, 1.11)* | 0.282 | 0.38 (0.08, 0.67)* | 0.45 (0.09, 0.79)* | 0.765 | 0.58 (0.26, 0.88)** | 0.51 (0.15, 0.85)* | 0.746 | 0.88 (0.46, 1.30)** | 0.94 (0.52, 1.34)** | 0.855 | 0.27 (−0.04, 0.58) | 0.12 (−0.27, 0.51) | 0.546 |
| Saturated fats | −0.57 (−1.00, −0.13)* | −0.21 (−0.67, 0.26) | 0.248 | 0.71 (0.06, 1.35)* | 0.45 (−0.14, 1.04) | 0.543 | 0.08 (−0.31, 0.48) | 0.09 (−0.38, 0.56) | 0.983 | −0.08 (−0.49, 0.32) | −0.53 (−1.04, −0.01)* | 0.192 | 0.29 (−0.30, 0.88) | −0.35 (−1.04, 0.33) | 0.156 | 0.02 (−0.36, 0.40) | −0.01 (−0.45, 0.43) | 0.907 |
| Relative gaps(95% CIs) | ||||||||||||||||||
| Total | 1.03 (1.00, 1.05)** | 1.07 (1.03, 1.11)** | 0.060 | 1.12 (1.08, 1.17)** | 1.16 (1.12, 1.20)** | 0.259 | 1.06 (1.03, 1.08)** | 1.08 (1.04, 1.11)** | 0.312 | 1.07 (1.04, 1.09)** | 1.04 (1.00, 1.07)** | 0.166 | 1.12 (1.08, 1.17)** | 1.16 (1.11, 1.21)** | 0.343 | 1.04 (1.01, 1.06)** | 1.04 (1.00, 1.07)** | 0.955 |
| Total fruits | 0.99 (0.89, 1.10)** | 1.00 (0.86, 1.13)** | 0.942 | 1.26 (1.11, 1.42) | 1.40 (1.20, 1.60)** | 0.297 | 1.02 (0.92, 1.11)** | 1.14 (1.00, 1.27)** | 0.132 | 1.06 (0.99, 1.13)** | 0.98 (0.87, 1.08)** | 0.177 | 1.16 (1.05, 1.27)** | 1.18 (1.02, 1.34)** | 0.832 | 1.04 (0.96, 1.11)** | 1.03 (0.93, 1.13)** | 0.927 |
| Whole fruits | 1.02 (0.89, 1.14)** | 1.10 (0.93, 1.27)** | 0.438 | 1.20 (1.02, 1.38)** | 1.55 (1.31, 1.78)** | 0.026 | 1.03 (0.91, 1.15)** | 1.20 (1.05, 1.34)** | 0.081 | 1.05 (0.96, 1.13)** | 1.05 (0.94, 1.16)** | 0.991 | 1.15 (1.01, 1.29)** | 1.39 (1.21, 1.57)** | 0.038 | 1.04 (0.96, 1.11)** | 1.09 (0.97, 1.20)** | 0.475 |
| Total vegetables | 1.03 (0.95, 1.11)** | 1.04 (0.94, 1.13)** | 0.915 | 1.08 (0.99, 1.16)** | 1.08 (0.94, 1.23)** | 0.940 | 1.06 (1.00, 1.13)** | 1.12 (1.02, 1.21)** | 0.370 | 1.12 (1.06, 1.18)** | 1.16 (1.06, 1.26)** | 0.470 | 1.11 (1.01, 1.18)** | 1.27 (1.16, 1.37)** | 0.016 | 1.04 (0.99, 1.10)** | 1.12 (1.04, 1.19)** | 0.118 |
| Greens and beans | 1.08 (0.82, 1.31)** | 1.22 (0.93, 1.50)** | 0.450 | 1.74 (1.31, 2.14)** | 2.13 (1.48, 2.76)** | 0.278 | 1.24 (0.97, 1.53)** | 1.40 (1.10, 1.70)** | 0.487 | 1.25 (1.04, 1.46)** | 1.35 (1.07, 1.61)** | 0.586 | 1.81 (1.34, 2.26)** | 2.13 (1.59, 2.66)** | 0.368 | 1.23 (1.04, 1.42)** | 1.22 (1.00, 1.45)** | 0.982 |
| Whole grains | 1.07 (0.87, 1.26)** | 1.16 (0.95, 1.37)** | 0.517 | 1.18 (0.93, 1.43)** | 1.53 (1.21, 1.86)** | 0.092 | 1.39 (1.11, 1.66)** | 1.36 (1.14, 1.58)** | 0.885 | 1.19 (0.98, 1.41)** | 0.96 (0.81, 1.11)** | 0.061 | 1.19 (0.88, 1.51)** | 1.01 (0.80, 1.21)** | 0.302 | 1.01 (0.85, 1.18)** | 1.04 (0.89, 1.19)** | 0.799 |
| Total dairy | 1.11 (0.99, 1.23)** | 1.13 (1.02, 1.24)** | 0.784 | 1.24 (1.06, 1.37)** | 1.06 (0.91, 1.14)** | 0.108 | 1.01 (0.91, 1.11)** | 1.10 (0.99, 1.21)** | 0.241 | 1.12 (1.03, 1.21)** | 1.09 (0.99, 1.20)** | 0.712 | 1.06 (1.01, 1.11)** | 1.16 (0.98, 1.40)** | 0.371 | 1.13 (1.04, 1.22)** | 0.93 (0.84, 1.02)** | 0.003 |
| Total protein foods | 1.06 (0.97, 1.14)** | 1.07 (1.02, 1.12)** | 0.836 | 1.18 (1.04, 1.50)** | 1.07 (1.03, 1.14)** | 0.100 | 1.11 (1.02, 1.20)** | 1.04 (1.00, 1.08)** | 0.840 | 1.16 (1.07, 1.25)** | 1.04 (0.98, 1.10)** | 0.029 | 1.13 (1.04, 1.19)** | 1.14 (1.05, 1.21)** | 0.886 | 1.02 (0.94, 1.09)** | 1.03 (0.97, 1.08)** | 0.840 |
| Seafood and plantproteins | 1.15 (0.95, 1.35)** | 1.09 (0.92, 1.26)** | 0.646 | 1.50 (0.72, 1.26)** | 1.61 (0.95, 1.94)** | 0.602 | 1.16 (1.00, 1.34)** | 1.08 (0.92, 1.24)** | 0.505 | 1.21 (1.03, 1.38)** | 1.20 (1.04, 1.36)** | 0.963 | 1.58 (1.21, 1.87)** | 1.64 (1.27, 1.72)** | 0.775 | 1.06 (0.92, 1.20)** | 1.08 (0.94, 1.22)** | 0.845 |
| Fatty acids | 0.93 (0.83, 1.02)** | 1.08 (0.96, 1.21)** | 0.039 | 0.96 (0.84, 1.07)** | 1.00 (0.90, 1.17)** | 0.610 | 1.02 (0.93, 1.13)** | 1.01 (0.90, 1.11)** | 0.505 | 0.98 (0.89, 1.06)** | 0.99 (0.87, 1.10)** | 0.858 | 1.05 (0.96, 1.09)** | 1.14 (1.07, 1.21)** | 0.444 | 1.02 (0.93, 1.11)** | 1.07 (0.96, 1.19)** | 0.845 |
| Refined grains | 1.13 (1.08, 1.19)** | 1.16 (1.09, 1.23)** | 0.538 | 1.04 (0.99, 1.09)** | 1.02 (0.93, 1.06)** | 0.776 | 1.04 (1.00, 1.08)** | 1.05 (0.99, 1.10)** | 0.600 | 1.08 (1.04, 1.13)** | 1.06 (1.00, 1.11)** | 0.446 | 1.09 (1.01, 1.18)** | 1.10 (1.02, 1.20)** | 0.917 | 1.04 (1.01, 1.08)** | 1.06 (1.01, 1.10)** | 0.598 |
| Sodium | 0.98 (0.90, 1.06)** | 1.06 (0.94, 1.17)** | 0.279 | 1.05 (1.00, 1.11)** | 1.17 (1.08, 1.20)** | 0.147 | 1.04 (0.96, 1.12)** | 1.01 (0.92, 1.09)** | 0.758 | 0.99 (0.92, 1.06)** | 0.99 (0.90, 1.09)** | 0.961 | 1.13 (1.05, 1.19)** | 1.13 (1.04, 1.18)** | 0.951 | 1.01 (0.94, 1.08)** | 1.05 (0.95, 1.13)** | 0.479 |
| Added sugars | 1.04 (1.00, 1.08)** | 1.02 (0.97, 1.06)** | 0.550 | 1.12 (1.02, 1.25)** | 1.08 (0.99, 1.20)** | 0.311 | 1.04 (1.00, 1.08)** | 1.05 (1.01, 1.10)** | 0.741 | 1.07 (1.03, 1.11)** | 1.06 (1.01, 1.10)** | 0.787 | 1.10 (1.01, 1.19)** | 1.11 (1.02, 1.21)** | 0.839 | 1.03 (0.99, 1.07)** | 1.01 (0.96, 1.06)** | 0.567 |
| Saturated fats | 0.91 (0.86, 0.97)** | 0.96 (0.90, 1.03)** | 0.256 | 1.11 (1.03, 1.21)** | 1.07 (1.00, 1.14)** | 0.552 | 1.01 (0.95, 1.07)** | 1.01 (0.93, 1.08)** | 0.978 | 0.98 (0.92, 1.04)** | 0.92 (0.84, 0.99)** | 0.194 | 1.04 (0.97, 1.11)** | 0.94 (0.88, 1.02)** | 0.165 | 1.00 (0.94, 1.06)** | 0.99 (0.92, 1.06)** | 0.908 |
| Absolute gradients: Slope Index of Inequality (95% CIs) | ||||||||||||||||||
| Total | 2.09 (0.45, 3.73)* | 4.84 (2.49, 7.20)** | 0.049 | 8.06 (6.41, 9.71)** | 10.52 (8.73, 12.31)** | 0.024 | 4.05 (2.24, 5.85)** | 5.16 (2.72, 7.60)** | 0.520 | 4.59 (2.99, 6.20)** | 4.48 (2.28, 6.68)** | 0.748 | 9.59 (7.88, 11.30)** | 8.58 (6.43, 10.74)** | 0.837 | 3.19 (1.36, 5.02)* | 4.03 (1.56, 6.50)* | 0.578 |
| Total fruits | −0.01 (−0.30, 0.28) | 0.13 (−0.28, 0.54) | 0.578 | 0.89 (0.57, 1.20)** | 1.10 (0.75, 1.44)** | 0.304 | 0.15 (−0.16, 0.47) | 0.29 (−0.09, 0.68) | 0.600 | 0.28 (0.04, 0.51)* | −0.07 (−0.43, 0.27) | 0.194 | 0.84 (0.55, 1.13)** | 0.54 (0.18, 0.90)* | 0.571 | 0.13 (−0.14, 0.42) | 0.30 (−0.06, 0.67) | 0.474 |
| Whole fruits | −0.002 (−0.31, 0.31) | 0.41 (−0.02, 0.85) | 0.117 | 0.71 (0.38, 1.04)** | 1.51 (1.14, 1.88)** | 0.001 | 0.17 (−0.17, 0.51) | 0.45 (0.03, 0.86)* | 0.365 | 0.21 (−0.05, 0.48) | 0.18 (−0.17, 0.54) | 0.710 | 0.98 (0.67, 1.29)** | 1.03 (0.65, 1.41)** | 0.285 | 0.19 (−0.10, 0.48) | 0.52 (0.11, 0.93)* | 0.184 |
| Total vegetables | 0.09 (−0.14, 0.32) | 0.04 (−0.25, 0.34) | 0.832 | 0.24 (0.01, 0.48)* | 0.49 (0.17, 0.81)* | 0.174 | 0.22 (−0.20, 0.47) | 0.31 (−0.01, 0.63) | 0.718 | 0.53 (0.33, 0.73)** | 0.68 (0.37, 0.99)** | 0.202 | 0.47 (0.25, 0.69)** | 0.80 (0.55, 1.06)** | 0.006 | 0.20 (−0.02, 0.43) | 0.53 (0.23, 0.82)** | 0.071 |
| Greens and beans | 0.08 (−0.20, 0.36) | 0.20 (−0.16, 0.57) | 0.602 | 0.79 (0.50, 1.08)** | 1.13 (0.79, 1.46)** | 0.079 | 0.37 (0.04, 0.70)* | 0.55 (0.17, 0.92)* | 0.527 | 0.38 (0.11, 0.66)* | 0.68 (0.29, 1.07)* | 0.110 | 0.83 (0.53, 1.13)** | 1.08 (0.69, 1.47)** | 0.140 | 0.43 (0.13, 0.74)* | 0.58 (0.17, 0.99)* | 0.530 |
| Whole grains | 0.15 (−0.28, 0.58) | 0.44 (−0.18, 1.08) | 0.370 | 0.50 (0.02, 0.97)* | 1.53 (0.92, 2.14)** | 0.005 | 0.72 (0.18, 1.27)* | 1.33 (0.63, 2.03)** | 0.248 | 0.40 (−0.08, 0.89) | 0.27 (−0.38, 0.93) | 0.702 | 0.99 (0.51, 1.48)** | 0.25 (−0.35, 0.87) | 0.091 | 0.03 (−0.48, 0.56) | 0.23 (−0.42, 0.89) | 0.692 |
| Total dairy | 0.44 (−0.05, 0.93) | 0.81 (0.24, 1.37)* | 0.302 | 0.70 (0.22, 1.18)* | 0.14 (−0.41, 0.71) | 0.157 | 0.05 (−0.44, 0.56) | 0.85 (0.20, 1.49)* | 0.062 | 0.55 (0.12, 0.98)* | 0.34 (−0.22, 0.92) | 0.658 | 0.77 (0.27, 1.28)* | 0.46 (−0.12, 1.04) | 0.659 | 0.90 (0.41, 1.40)** | −0.55 (−1.15, 0.05) | <0.001 |
| Total protein foods | 0.21 (−0.02, 0.46) | 0.29 (0.07, 0.52)* | 0.501 | 0.62 (0.36, 0.89)** | 0.30 (0.07, 0.53)* | 0.134 | 0.33 (0.05, 0.61)* | 0.25 (0.03, 0.47)* | 0.618 | 0.40 (0.15, 0.66)* | 0.29 (0.03, 0.56)* | 0.834 | 0.73 (0.44, 1.02)** | 0.19 (−0.03, 0.42) | 0.039 | 0.11 (−0.14, 0.37) | 0.27 (0.025, 0.52)* | 0.373 |
| Seafood and plantproteins | 0.21 (−0.09, 0.52) | 0.18 (−0.21, 0.58) | 0.968 | 0.98 (0.68, 1.28)** | 1.16 (0.78, 1.54)** | 0.372 | 0.34 (0.04, 0.64)* | 0.28 (−0.13, 0.70) | 0.807 | 0.27 (−0.01, 0.56) | 0.68 (0.31, 1.05)** | 0.062 | 1.12 (0.80, 1.45)** | 1.11 (0.72, 1.49)** | 0.916 | 0.10 (−0.19, 0.41) | 0.45 (0.06, 0.83)* | 0.150 |
| Fatty acids | −0.28 (−0.85, 0.28) | 0.51 (−0.16, 1.19) | 0.060 | 0.13 (−0.40, 0.68) | 0.28 (−0.28, 0.84) | 0.670 | 0.26 (−0.34, 0.87) | −0.01 (−0.72, 0.68) | 0.500 | 0.002 (−0.50, 0.51) | 0.12 (−0.56, 0.81) | 0.616 | 0.01 (−0.56, 0.59) | 0.48 (−0.14, 1.12) | 0.139 | 0.11 (−0.45, 0.68) | 0.58 (−0.06, 1.24) | 0.251 |
| Refined grains | 1.39 (0.99, 1.78)** | 1.30 (0.77, 1.83)** | 0.849 | 0.10 (−0.32, 0.53) | 0.58 (0.06, 1.11)* | 0.166 | 0.41 (−0.03, 0.86) | 0.11 (−0.44, 0.68) | 0.459 | 0.84 (0.48, 1.20)** | 1.34 (0.82, 1.86)** | 0.109 | 0.82 (0.44, 1.21)** | 1.00 (0.50, 1.50)** | 0.551 | 0.43 (0.06, 0.80)* | 0.49 (−0.01, 0.99) | 0.862 |
| Sodium | 0.03 (−0.49, 0.55) | 0.23 (−0.45, 0.93) | 0.696 | 0.56 (0.02, 1.09)* | 0.97 (0.39, 1.56)* | 0.405 | 0.23 (−0.33, 0.80) | 0.13 (−0.49, 0.77) | 0.934 | −0.09 (−0.53, 0.33) | 0.50 (−0.54, 0.66) | 0.912 | 0.56 (0.06, 1.06)* | 0.64 (0.06, 1.23)* | 0.773 | 0.12 (−0.37, 0.63) | 0.17 (−0.47, 0.81) | 0.935 |
| Added sugars | 0.37 (0.02, 0.72)* | 0.39 (−0.08, 0.86) | 0.891 | 1.05 (0.70, 1.39)** | 1.09 (0.65, 1.53)** | 0.726 | 0.54 (0.17, 0.91)* | 0.61 (0.15, 1.06)* | 0.862 | 0.75 (0.40, 1.10)** | 0.52 (0.10, 0.94)* | 0.605 | 1.17 (0.78, 1.56)** | 0.87 (0.45, 1.29)** | 0.643 | 0.45 (0.07, 0.84)* | 0.28 (−0.19, 0.76) | 0.585 |
| Saturated fats | −0.60 (−1.05, −0.15)* | −0.13 (−0.68, 0.40) | 0.225 | 0.74 (0.19, 1.30)* | 0.18 (−0.31, 0.69) | 0.094 | 0.19 (−0.32, 0.71) | −0.02 (−0.62, 0.58) | 0.605 | 0.03 (−0.45, 0.50) | −0.65 (−1.25, −0.04)* | 0.094 | 0.23 (−0.24, 0.70) | 0.07 (−0.47, 0.62) | 0.884 | −0.08 (−0.60, 0.43) | 0.14 (−0.45, 0.74) | 0.562 |
| Relative gradients: Relative Index of Inequality (95% CIs) | ||||||||||||||||||
| Total | 1.04 (1.01, 1.07)* | 1.08 (1.05, 1.11)** | 0.060 | 1.16 (1.12, 1.19)** | 1.19 (1.16, 1.23)** | 0.093 | 1.07 (1.04, 1.11)** | 1.09 (1.04, 1.14)** | 0.661 | 1.08 (1.05, 1.11)** | 1.07 (1.03, 1.11)** | 0.857 | 1.18 (1.14, 1.22)** | 1.15 (1.11, 1.19)** | 0.932 | 1.05 (1.02, 1.09)* | 1.06 (1.02, 1.11)* | 0.688 |
| Total fruits | 1.01 (0.90, 1.12) | 1.05 (0.90, 1.22) | 0.584 | 1.39 (1.24, 1.56)** | 1.48 (1.31, 1.68)** | 0.403 | 1.06 (0.95, 1.20) | 1.12 (0.97, 1.30) | 0.599 | 1.09 (1.02, 1.17)* | 0.98 (0.87, 1.10) | 0.209 | 1.31 (1.19, 1.43)** | 1.20 (1.07, 1.35)* | 0.662 | 1.04 (0.95, 1.14) | 1.10 (0.97, 1.24) | 0.471 |
| Whole fruits | 1.03 (0.91, 1.17) | 1.16 (0.99, 1.36) | 0.149 | 1.32 (1.17, 1.50)** | 1.68 (1.48, 1.92)** | 0.006 | 1.08 (0.94, 1.24) | 1.18 (1.02, 1.37)* | 0.440 | 1.08 (0.99, 1.17) | 1.07 (0.96, 1.20) | 0.629 | 1.36 (1.24, 1.50)** | 1.40 (1.24, 1.58)** | 0.231 | 1.07 (0.97, 1.17) | 1.18 (1.04, 1.34)* | 0.189 |
| Total vegetables | 1.03 (0.96, 1.11) | 1.02 (0.92, 1.13) | 0.889 | 1.08 (1.00, 1.16) | 1.18 (1.05, 1.31)* | 0.166 | 1.08 (0.99, 1.17) | 1.11 (0.99, 1.24) | 0.699 | 1.17 (1.10, 1.24)* | 1.23 (1.12, 1.34)* | 0.191 | 1.14 (1.07, 1.22) | 1.29 (1.19, 1.39)* | 0.003 | 1.06 (0.99, 1.13) | 1.16 (1.07, 1.27)* | 0.073 |
| Greens and beans | 1.09 (0.84, 1.42) | 1.16 (0.88, 1.53) | 0.690 | 2.03 (1.55, 2.67)** | 2.22 (1.74, 2.84)** | 0.609 | 1.43 (1.07, 1.91)* | 1.49 (1.13, 1.97)* | 0.824 | 1.32 (1.08, 1.62)* | 1.51 (1.21, 1.89)** | 0.242 | 1.78 (1.45, 2.20)** | 2.00 (1.55, 2.57)** | 0.301 | 1.36 (1.09, 1.69)* | 1.40 (1.10, 1.78)* | 0.830 |
| Whole grains | 1.07 (0.88, 1.31) | 1.14 (0.96, 1.36) | 0.404 | 1.27 (1.04, 1.55)* | 1.54 (1.30, 1.82)** | 0.057 | 1.39 (1.09, 1.78)* | 1.46 (1.20, 1.78)** | 0.826 | 1.21 (1.00, 1.46)* | 1.06 (0.90, 1.25) | 0.476 | 1.49 (1.25, 1.79)** | 1.10 (0.94, 1.29) | 0.102 | 1.00 (0.83, 1.22) | 1.02 (0.87, 1.21) | 0.925 |
| Total dairy | 1.11 (0.98, 1.26) | 1.18 (1.05, 1.33)* | 0.454 | 1.19 (1.05, 1.34)* | 1.03 (0.91, 1.16) | 0.094 | 1.01 (0.89, 1.14) | 1.20 (1.05, 1.39)* | 0.076 | 1.12 (1.02, 1.23)* | 1.07 (0.95, 1.20) | 0.596 | 1.17 (1.05, 1.31)* | 1.09 (0.97, 1.23) | 0.591 | 1.21 (1.09, 1.35)** | 0.89 (0.79, 1.01) | <0.001 |
| Total protein foods | 1.08 (0.99, 1.18) | 1.07 (1.01, 1.13)* | 0.920 | 1.24 (1.13, 1.37)** | 1.07 (1.01, 1.13)* | 0.019 | 1.12 (1.02, 1.24)* | 1.06 (1.00, 1.12)* | 0.289 | 1.15 (1.05, 1.26)* | 1.08 (1.00, 1.15)* | 0.456 | 1.28 (1.16, 1.41)** | 1.05 (0.99, 1.11) | 0.013 | 1.04 (0.95, 1.14) | 1.07 (1.00, 1.14)* | 0.582 |
| Seafood and plantproteins | 1.16 (0.96, 1.40) | 1.08 (0.90, 1.30) | 0.779 | 1.82 (1.52, 2.18)** | 1.66 (1.40, 1.96)** | 0.574 | 1.24 (1.04, 1.48)* | 1.13 (0.94, 1.36) | 0.500 | 1.17 (0.99, 1.37) | 1.33 (1.14, 1.55)** | 0.191 | 1.85 (1.55, 2.22)** | 1.58 (1.35, 1.86)** | 0.341 | 1.06 (0.89, 1.25) | 1.19 (1.01, 1.40)* | 0.266 |
| Fatty acids | 0.94 (0.84, 1.05) | 1.11 (0.96, 1.27) | 0.059 | 1.02 (0.91, 1.14) | 1.05 (0.94, 1.17) | 0.680 | 1.05 (0.93, 1.19) | 0.99 (0.87, 1.14) | 0.506 | 0.99 (0.90, 1.10) | 1.02 (0.89, 1.17) | 0.608 | 1.00 (0.88, 1.12) | 1.10 (0.97, 1.24) | 0.147 | 1.02 (0.91, 1.14) | 1.11 (0.98, 1.26) | 0.269 |
| Refined grains | 1.18 (1.12, 1.23)** | 1.17 (1.10, 1.25)** | 0.940 | 1.01 (0.96, 1.06) | 1.07 (1.00, 1.14)* | 0.161 | 1.05 (0.99, 1.10) | 1.01 (0.94, 1.08) | 0.487 | 1.10 (1.05, 1.15)** | 1.17 (1.10, 1.25)** | 0.085 | 1.10 (1.05, 1.15)** | 1.13 (1.06, 1.20)** | 0.490 | 1.05 (1.00, 1.10)* | 1.06 (1.00, 1.13)* | 0.808 |
| Sodium | 1.00 (0.91, 1.10) | 1.03 (0.92, 1.17) | 0.726 | 1.10 (1.00, 1.21)* | 1.17 (1.06, 1.29)* | 0.448 | 1.04 (0.94, 1.15) | 1.02 (0.91, 1.13) | 0.924 | 0.98 (0.90, 1.06) | 1.01 (0.91, 1.12) | 0.898 | 1.10 (1.01, 1.21)* | 1.11 (1.01, 1.22)* | 0.678 | 1.02 (0.93, 1.11) | 1.02 (0.92, 1.14) | 0.955 |
| Added sugars | 1.04 (1.00, 1.09)* | 1.05 (0.99, 1.11) | 0.860 | 1.13 (1.08, 1.18)** | 1.14 (1.08, 1.20)** | 0.682 | 1.06 (1.02, 1.11)* | 1.07 (1.01, 1.13)* | 0.861 | 1.09 (1.05, 1.14)** | 1.06 (1.01, 1.12)* | 0.609 | 1.14 (1.09, 1.20)** | 1.11 (1.05, 1.16)** | 0.724 | 1.05 (1.01, 1.10)* | 1.03 (0.97, 1.09) | 0.603 |
| Saturated fats | 0.90 (0.84, 0.97)* | 0.98 (0.90, 1.06) | 0.202 | 1.11 (1.02, 1.21)* | 1.03 (0.95, 1.11) | 0.852 | 1.02 (0.95, 1.10) | 0.99 (0.91, 1.09) | 0.628 | 1.00 (0.93, 1.07) | 0.90 (0.82, 0.99)* | 0.097 | 1.03 (0.96, 1.11) | 1.01 (0.92, 1.10) | 0.111 | 0.98 (0.91, 1.06) | 1.02 (0.93, 1.11) | 0.574 |
2004 males weighted n = 11,846,000, females weighted n = 11,836,000; 2015 males weighted n = 13,788,000, females weighted n = 13,778,000. Multivariable linear regression models examined trends in gaps, whereas generalized linear models examined trends in gradients, in HEI-2015 total and component scores between 2004 and 2015. Data are weighted to be nationally representative and are adjusted for age and dietary recall day. Weighted sample sizes are rounded in accordance with Statistics Canada's confidentiality policies. HEI, Healthy Eating Index.
*P < 0.05 for within-year inequities, **P < 0.001 for within-year inequities.
Relative gaps in diet quality
There were significant positive relative gaps in HEI-2015 total scores according to all 3 SEP indicators in 2004 and 2015 (Tables 3 and 4). In the total population, relative gaps in HEI-2015 total and component scores remained stable for all SEP indicators between 2004 and 2015, with the exception of an increase in the relative gap in scores for whole fruits according to educational attainment. There were no significant trends in relative gaps in HEI-2015 total scores among males or females for any of the SEP indicators. In terms of HEI-2015 component scores, among males, the relative gap in scores for fatty acids according to household income increased, as did the gap in scores for whole fruits according to educational attainment between 2004 and 2015. Among females, the relative gap in scores for whole fruits and total vegetables according to educational attainment increased, whereas the relative gap in scores for total protein foods according to household income and for total dairy according to neighborhood deprivation declined, between 2004 and 2015.
Absolute gradients in diet quality
There were significant positive absolute gradients in HEI-2015 total scores according to all 3 SEP indicators in 2004 and 2015 (Tables 3 and 4). In the total population, absolute gradients in HEI-2015 total and component scores remained stable for all SEP indicators between 2004 and 2015, with the exception of increases in the absolute gradient in scores for whole fruits, total vegetables, and greens and beans, and a decline in the gradient in scores for total protein foods, all according to educational attainment. Among males, the absolute gradient in HEI-2015 total scores increased according to household income [from SII = 2.09 (0.45, 3.73) to SII = 4.84 (2.49, 7.20)] and educational attainment [from SII = 8.06 (6.41, 9.71) to SII = 10.52 (8.73, 12.31)], with no change for neighborhood deprivation. The absolute gradient in scores for whole fruits and whole grains according to educational attainment increased among males between 2004 and 2015. Among females, the absolute gradient in HEI-2015 total scores remained stable for all SEP indicators. For HEI-2015 components, the absolute gradient in scores for total vegetables according to educational attainment increased, whereas the absolute gradient in scores for total protein foods according to educational attainment and in scores for total dairy according to neighborhood deprivation declined, between 2004 and 2015.
Relative gradients in diet quality
There were significant positive relative gradients in HEI-2015 total scores according to all 3 SEP indicators in 2004 and 2015 (Tables 3 and 4). In the total population, relative gradients in HEI-2015 total and component scores remained stable for all SEP indicators between 2004 and 2015, with the exception of an increase in the relative gradient in scores for whole fruits and total vegetables, and a decline in the gradient in scores for total protein foods, all according to educational attainment. Relative gradients in HEI-2015 total scores remained stable among males and females for all of the SEP indicators. Among males, the relative gradient in scores for whole fruits according to educational attainment increased, whereas the relative gradient in scores for total protein foods according to educational attainment declined, between 2004 and 2015. Among females, the relative gradient in scores for total vegetables according to educational attainment increased, whereas the relative gradient in scores for total protein foods according to educational attainment and in scores for total dairy according to neighborhood deprivation both declined, between 2004 and 2015.
Sensitivity analysis
Findings were unchanged when models were adjusted for race/ethnicity. There was more evidence of widening gaps and gradients when educational attainment at a household level was used as the indicator of SEP (Supplemental Tables 1–3). In the total population, both absolute and relative gaps in HEI-2015 total scores widened between 2004 and 2015. Among males, the absolute gap and gradient and the relative gradient in HEI-2015 total scores widened. Among females, the absolute gap in HEI-2015 total scores widened.
Discussion
We conducted a comprehensive analysis of trends in socioeconomic inequities in diet quality among adults living in Canada. Between 2004 and 2015, mean overall diet quality improved significantly at a population level; however, these trends were not consistently equitable. Among males, the absolute gap and gradient in overall diet quality according to household income widened, as did the absolute gradient according to educational attainment. Trends in overall diet quality in the total population and among females remained stable for all SEP indicators. Despite the relative stability of dietary inequities over time, diet quality was clearly socioeconomically patterned on both an absolute and a relative basis in both years according to all 3 SEP indicators, indicating a need for intervention. Findings suggest that action is particularly needed to improve diet quality at an absolute level among males across the spectrum of income and educational attainment. Because diet quality mediates associations between SEP and chronic disease (7), reducing these dietary inequities may reduce health inequities.
Between 2004 and 2015, inequities in overall diet quality remained stable in the total population and in females, whereas the absolute gap and gradient according to household income and the absolute gradient according to educational attainment widened among males. Although statistically significant and potentially indicative of unfavorable trends, we cannot rule out the possibility that these trends were stable given that CIs were overlapping. In addition, the degree of widening observed (∼2.5 points) may not be clinically meaningful and could also reflect measurement error (61). US studies have also observed evidence both of stability and of widening absolute inequities according to these indicators in the total population, although sex-stratified analyses were not conducted (6, 8–13). It was notable that there was only evidence of widening inequities among males in Canada. Females also maintained consistently higher diet quality than males, and in some cases the diet quality of females with the lowest SEP was comparable to that of males with the highest SEP. Although we were limited to analyzing biological sex, it is likely that these findings reflect gender roles and identities. Women may place a higher priority on healthy eating than men because they face greater social pressures to maintain an ideal body weight (62) and/or because as caregivers and nurturers, women may be expected to model optimal dietary patterns to those under their care. Women may therefore be more inclined to channel their available resources to support a higher diet quality over time regardless of their SEP, whereas men with a lower SEP may be less inclined or able to do so.
Some of the negative trends in HEI-2015 total scores among males appear to have been driven by widening inequities in intakes of whole fruits, whole grains, and/or fatty acids, although inequities in intake of total protein foods also narrowed in 1 instance. Among females, there was also evidence of both widening (whole fruits, total vegetables) and narrowing (total protein foods, total dairy) inequities in intakes of HEI-2015 components. The only common trends between males and females were a widening of absolute and relative gaps in scores for whole fruits, and a narrowing of relative gradients in scores for total protein foods, all according to educational attainment.
The decision to quantify absolute or relative trends in dietary gaps or gradients and the selection of socioeconomic indicators can lead to different conclusions regarding the presence, strength, direction, and/or rate of change of inequities (14). Given that relative gaps and gradients were consistently stable, whereas absolute gaps and gradients exhibited some evidence of widening, our findings point to the importance of improving absolute diet quality across the socioeconomic spectrum in Canada. Inequities were also consistently high according to educational attainment, with clinically meaningful gaps and gradients ranging from 7 to 11 points (61), and inequities according to individual educational attainment and household income widened among males. Sensitivity analyses showed that these trends toward widening inequities were even stronger when household educational attainment was used to indicate SEP among both females and males. Although associations between diet quality and SEP are often attributed to the higher costs of healthy foods (63), the importance of educational attainment in structuring diet quality suggests that mechanisms linking SEP to diet quality are not limited to the material disadvantages imposed by poverty, but also encompass differentials in knowledge, status, influence, and power, among others, that may be better captured by educational attainment (16, 17). These findings may have implications for health inequities, as diet quality mediates associations between individual educational attainment and chronic disease (7), although the health implications of widening inequities according to household-level educational attainment require further study. Notably, educational inequities (according to individual educational attainment) in mortality also widened in Canada during the period of study (64).
It is possible that educational expansion (i.e., more individuals attaining higher education than in previous generations) may have resulted in selection effects, whereby those in the least educated group in 2015 represented a more negatively selected group of individuals (e.g., with more chronic disease and disability) who were subject to more profound experiences of disadvantage that negatively affected their diet quality, thereby widening inequities (17, 65, 66). The high and continually escalating costs of many healthful foods (67, 68) may be partly responsible for widening inequities according to household income, along with increases in the costs of other essential resources such as housing and transportation which can reduce the income available to purchase food, while also limiting food access in other ways (e.g., travel to supermarkets). Although we did not find evidence of widening inequities according to neighborhood deprivation, it was still an important determinant of dietary inequities.
The current study represents the most comprehensive analysis of nationally representative trends in socioeconomic inequities in diet quality among adults internationally. The value of our approach can be seen in our nuanced findings. Had we conducted more limited analyses using more traditional descriptive approaches we would have missed the opportunity to precisely quantify sex-specific trends in dietary inequities on an absolute and relative basis, both across the socioeconomic spectrum and at its extreme ends, and along multiple axes of social stratification. By using the SII and the RII to assess dietary gradients we were in addition able to take into account the rank and the size of the SEP groups that were being compared, which is highly relevant to policy development (23).
Study limitations must also be considered. First, although 24-h dietary recalls have less systematic error than other dietary assessment tools, misreporting can inflate HEI-2015 scores (61, 69, 70). Underreporting was higher in 2015 than in 2004 (60), and therefore caution is advised in interpreting the increase in HEI-2015 scores at a population level and within socioeconomic strata. However, the fact that the odds of misreporting by SEP did not change over time provides confidence in our estimates of trends. Furthermore, although a single recall is recommended to describe mean intake at a population level (59), 1 recall cannot fully capture usual intake, particularly of episodically consumed foods. Although the 2004 and 2015 CCHS cycles were designed to be comparable, some differences between survey cycles were inevitable (28). Updates to the food database and to food model booklets may have contributed to lower energy intakes of ≤20 kcal/d and ≤35 kcal/d in 2015, respectively (71). However, these limitations would only affect our analyses if they differed by SEP, which we do not have reason to expect. Although household income was imputed for nearly one-quarter of participants in 2015, the quality of these imputations has been confirmed (32). Finally, although the CCHS captures 98% of the Canadian population, it does not capture individuals living on Indigenous reserves or in Canada's 3 territories which have very high rates of food insecurity and may therefore show differential dietary trends.
The diet quality of adults in Canada improved between 2004 and 2015; however, these improvements were not consistently equitable. Whereas absolute and relative gaps and gradients in overall diet quality remained stable in the total population and in females for all 3 SEP indicators, the absolute gap and gradient in overall diet quality according to household income widened among males, as did the absolute gradient according to educational attainment. The fact that higher-SEP groups consistently maintained or improved their diet quality relative to lower-SEP groups suggests that a higher-quality diet is attainable through improving socioeconomic conditions. As such, policies that address the root socioeconomic causes of poor diet quality such as by improving educational attainment (e.g., subsidizing postsecondary education) and ensuring sufficient household income (e.g., increasing social assistance rates), among others, should be prioritized to reduce inequities in diet quality.
Supplementary Material
Acknowledgments
The authors’ responsibilities were as follows—SN and CV: analyzed the data; DLO: wrote the paper and had primary responsibility for the final content; and all authors: designed the research and read and approved the final manuscript. DLO has received funding from a Petro-Canada Young Innovator Award in Community Health. All other authors report no conflicts of interest.
Notes
Supported by the O'Brien Institute for Public Health (to DLO). SN was supported by a Libin Cardiovascular Institute/Cumming School of Medicine Postdoctoral Award. LM was supported by an Applied Public Health Chair award funded by the Canadian Institutes of Health Research (Institute of Population and Public Health and Institute of Musculoskeletal Health and Arthritis), the Public Health Agency of Canada, and Alberta Innovates—Health Solutions.
Supplemental Tables 1–3 are available from the “Supplementary data” link in the online posting of the article and from the same link in the online table of contents at https://academic.oup.com/ajcn/.
Abbreviations used: CCHS, Canadian Community Health Survey; HEI, Healthy Eating Index; RII, Relative Index of Inequality; SEP, socioeconomic position; SII, Slope Index of Inequality; TEE, total energy expenditure; TEI, total energy intake.
Contributor Information
Dana Lee Olstad, Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Sara Nejatinamini, Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Charlie Victorino, Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Sharon I Kirkpatrick, School of Public Health and Health Systems, University of Waterloo, Waterloo, Ontario, Canada.
Leia M Minaker, School of Planning, University of Waterloo, Waterloo, Ontario, Canada.
Lindsay McLaren, Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Data Availability
Data described in the article, code book, and analytic code will not be made available because the data are held by Statistics Canada. Statistics Canada permits approved researchers to access its data sets within its Research Data Centres (https://www.statcan.gc.ca/eng/microdata/data-centres).
References
- 1. World Health Organization. A conceptual framework for action on the social determinants of health. [Internet]. Geneva, Switzerland: WHO; 2017; [cited 2 November, 2017]. Available from: http://www.who.int/sdhconference/resources/ConceptualframeworkforactiononSDH_eng.pdf. [Google Scholar]
- 2. Marmot M, Friel S, Bell R, Houweling TA, Taylor S, Commission on Social Determinants of Health . Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372(9650):1661–9. [DOI] [PubMed] [Google Scholar]
- 3. Graham H. Social determinants and their unequal distribution: clarifying policy understandings. Milbank Q. 2004;82(1):101–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Livingstone KM, Olstad DL, Leech RM, Ball K, Meertens B, Potter J, Cleanthous X, Reynolds R, McNaughton SA. Socioeconomic inequities in diet quality and nutrient intakes among Australian adults: findings from a nationally representative cross-sectional study. Nutrients. 2017;9(10):1092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Garriguet D. Diet quality in Canada. Health Rep. 2009;20(3):41–52. [PubMed] [Google Scholar]
- 6. Rehm CD, Peñalvo JL, Afshin A, Mozaffarian D. Dietary intake among US adults, 1999-2012. JAMA. 2016;315(23):2542–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Petrovic D, de Mestral C, Bochud M, Bartley M, Kivimaki M, Vineis P, Mackenbach J, Stringhini S. The contribution of health behaviors to socioeconomic inequalities in health: a systematic review. Prev Med. 2018;113:15–31. [DOI] [PubMed] [Google Scholar]
- 8. Wang DD, Leung CW, Li Y, Ding EL, Chiuve SE, Hu FB, Willett WC. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern Med. 2014;174(10):1587–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wang DD, Li Y, Chiuve SE, Hu FB, Willett WC. Improvements in US diet helped reduce disease burden and lower premature deaths, 1999–2012. Health Aff. 2015;34(11):1916–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Zhang FF, Liu J, Rehm CD, Wilde P, Mande JR, Mozaffarian D. Trends and disparities in diet quality among US adults by Supplemental Nutrition Assistance Program participation. JAMA Network Open. 2018;1(2):e180237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Orr CJ, Keyserling TC, Ammerman AS, Berkowitz SA. Diet quality trends among adults with diabetes by socioeconomic status in the U.S.: 1999–2014. BMC Endocr Disord. 2019;19(1):54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Shan Z, Rehm CD, Rogers G, Ruan M, Wang DD, Hu FB, Mozaffarian D, Zhang FF, Bhupathiraju SN. Trends in dietary carbohydrate, protein, and fat intake and diet quality among US adults, 1999-2016. JAMA. 2019;322(12):1178–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Patetta MA, Pedraza LS, Popkin BM. Improvements in the nutritional quality of US young adults based on food sources and socioeconomic status between 1989–1991 and 2011–2014. Nutr J. 2019;18(1):32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Harper S, King NB, Meersman SC, Reichman ME, Breen N, Lynch J. Implicit value judgments in the measurement of health inequalities. Milbank Q. 2010;88(1):4–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Liu SY, Walter S, Marden J, Rehkopf DH, Kubzansky LD, Nguyen T, Glymour MM. Genetic vulnerability to diabetes and obesity: does education offset the risk?. Soc Sci Med. 2015;127:150–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey Smith G. Indicators of socioeconomic position (part 1). J Epidemiol Community Health. 2006;60(1):7–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Hayward MD, Hummer RA, Sasson I. Trends and group differences in the association between educational attainment and U.S. adult mortality: implications for understanding education's causal influence. Soc Sci Med. 2015;127:8–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Pampalon R, Hamel D, Gamache P, Philibert MD, Raymond G, Simpson A. An area-based material and social deprivation index for public health in Quebec and Canada. Can J Public Health. 2012;103(S2):S17–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Olstad DL, McIntyre L. Reconceptualising precision public health. BMJ Open. 2019;9(9):e030279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M, Posner S. Socioeconomic status in health research: one size does not fit all. JAMA. 2005;294(22):2879–88. [DOI] [PubMed] [Google Scholar]
- 21. World Health Organization. HEAT, built-in database edition. [Internet]. Geneva, Switzerland: WHO; 2020; [cited 20 September, 2020]. Available from: https://www.who.int/data/gho/health-equity/heat-built-in-database-edition. [Google Scholar]
- 22. Wagstaff A, Paci P, van Doorslaer E. On the measurement of inequalities in health. Soc Sci Med. 1991;33(5):545–57. [DOI] [PubMed] [Google Scholar]
- 23. Mackenbach JP, Kunst AE. Measuring the magnitude of socio-economic inequalities in health: an overview of available measures illustrated with two examples from Europe. Soc Sci Med. 1997;44(6):757–71. [DOI] [PubMed] [Google Scholar]
- 24. Keppel K, Pamuk E, Lynch J, Carter-Pokras O, Kim I, Mays V, Pearcy J, Schoenbach V, Weissman JS. Methodological issues in measuring health disparities. Vital Health Stat 2. 2005;(141):1–16. [PMC free article] [PubMed] [Google Scholar]
- 25. Graham H. Tackling inequalities in health in England: remedying health disadvantages, narrowing health gaps or reducing health gradients?. J Soc Policy. 2004;33(1):115–31. [Google Scholar]
- 26. Alonge O, Peters DH. Utility and limitations of measures of health inequities: a theoretical perspective. Glob Health Action. 2015;8(1):27591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Statistics Canada. Canadian Community Health Survey - Nutrition (CCHS). [Internet]. Ottawa, Ontario: Statistics Canada; 2017; [cited 16 September, 2020]. Available from: http://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=5049. [Google Scholar]
- 28. Statistics Canada. Reference guide to understanding and using the data: 2015 Canadian Community Health Survey - Nutrition. [Internet]. Ottawa, Ontario: Health Canada; 2017; [cited 1 January, 2021]. Available from: https://www.canada.ca/en/health-canada/services/food-nutrition/food-nutrition-surveillance/health-nutrition-surveys/canadian-community-health-survey-cchs/reference-guide-understanding-using-data-2015.html. [Google Scholar]
- 29. Statistics Canada. Canadian Community Health Survey (CCHS): Nutrition - 2015 (First Interview): Survey Introduction (INT). [Internet]. Ottawa, Ontario: Statistics Canada; 2017; [cited 20 October, 2020]. Available from: http://www23.statcan.gc.ca/imdb/p3Instr.pl?Function=assembleInstr&Item_Id=202664#qb210812. [Google Scholar]
- 30. Health Canada. Canadian Community Health Survey Cycle 2.2, Nutrition (2004): a guide to accessing and interpreting the data. [Internet]. Ottawa, Ontario: Health Canada; 2006; [cited 20 October, 2020]. Available from: http://www.hc-sc.gc.ca/fn-an/alt_formats/hpfb-dgpsa/pdf/surveill/cchs-guide-escc-eng.pdf. [Google Scholar]
- 31. Statistics Canada. Canadian Community Health Survey (CCHS) - Nutrition, 2015. General health and summary data for 24-hour dietary recall and nutritional supplements. Master file version (Rounded frequencies), June 2018. Ottawa, Ontario: Statistics Canada; 2018. [Google Scholar]
- 32. Yeung CW, Thomas S. Income imputation for the Canadian Community Health Survey. Ottawa, Ontario: Household Survey Method Division, Statistics Canada; 2013. [Google Scholar]
- 33. Durrant GB, Skinner C. Survey methodology. [Internet]. Ottawa, Ontario: Statistics Canada; 2006; [cited 7 June, 2021]. Available from: https://www150.statcan.gc.ca/n1/en/pub/12-001-x/2006001/article/9260-eng.pdf?st=MjoLeNIo. [Google Scholar]
- 34. Statistics Canada. Canadian Community Health Survey (CCHS) Annual Component - Public Use Microdata File, 2015–2016. Derived Variable (DV) specifications. Ottawa, Ontario: Statistics Canada; 2016. [Google Scholar]
- 35. Statistics Canada. Low income cut-offs (LICOs) before and after tax by community size and family size, in current dollars. [Internet]. Ottawa, Ontario: Statistics Canada; 2016; [cited 10 January, 2021]. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1110024101&pickMembers%5B0%5D=2.1&cubeTimeFrame.startYear=2014&cubeTimeFrame.endYear=2014&referencePeriods=20140101%2C20140101. [Google Scholar]
- 36. Becker GS. Human capital: a theoretical and empirical analysis with special reference to education. 3rd ed. Chicago, IL: The University of Chicago Press; 1994. [Google Scholar]
- 37. Pampalon R, Hamel D, Gamache P, Simpson A, Philibert MD. Validation of a deprivation index for public health: a complex exercise illustrated by the Quebec index. Chronic Dis Inj Can. 2014;34(1):12–22. [PubMed] [Google Scholar]
- 38. Gamache P, Hamel D, Blaser C. Material and social deprivation index: a summary. [Internet]. Québec City: Institut National de Santé Publique du Québec; 2019; [cited 20 December, 2020]. Available from: https://www.inspq.qc.ca/sites/default/files/publications/2639_material_social_deprivation_index.pdf. [Google Scholar]
- 39. Conway JM, Ingwersen LA, Vinyard BT, Moshfegh AJ. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am J Clin Nutr. 2003;77(5):1171–8. [DOI] [PubMed] [Google Scholar]
- 40. Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rumpler WV, Paul DR, Sebastian RS, Kuczynski KJ, Ingwersen LAet al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88(2):324–32. [DOI] [PubMed] [Google Scholar]
- 41. USDA. FNDDS overview. [Internet]. Beltsville, MD: USDA Agricultural Research Service; 2020; [cited 19 October, 2020]. Available from: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds. [Google Scholar]
- 42. USDA. Overview of Food Patterns Equivalents Database. [Internet]. Beltsville, MD: USDA Agricultural Research Service; 2020; [cited 19 October, 2020]. Available from: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fped-overview/. [Google Scholar]
- 43. National Cancer Institute (NCI). Comparing the HEI-2015, HEI–2010 & HEI–2005. [Internet]. Bethesda, MD: NCI Epidemiology and Genomics Research Program; 2017; [cited 3 May, 2017]. Available from: https://epi.grants.cancer.gov/hei/comparing.html. [Google Scholar]
- 44. Krebs-Smith SM, Pannucci TE, Subar AF, Kirkpatrick SI, Lerman JL, Tooze JA, Wilson MM, Reedy J. Update of the Healthy Eating Index: HEI-2015. J Acad Nutr Diet. 2018;118(9):1591–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. US Department of Health and Human Services (DHHS) and USDA. 2015–2020 Dietary Guidelines for Americans. [Internet]. 8th ed. Washington (DC): US DHHS and USDA; 2015; [cited 20 June, 2021]. Available from: https://health.gov/dietaryguidelines/2015/guidelines/. [Google Scholar]
- 46. Miller V, Webb P, Micha R, Mozaffarian D, Global Dietary Database . Defining diet quality: a synthesis of dietary quality metrics and their validity for the double burden of malnutrition. Lancet Planet Health. 2020;4(8):e352–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Reedy J, Lerman JL, Krebs-Smith SM, Kirkpatrick SI, Pannucci TE, Wilson MM, Subar AF, Kahle LL, Tooze JA. Evaluation of the Healthy Eating Index-2015. J Acad Nutr Diet. 2018;118(9):1622–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Burggraf C, Teuber R, Brosig S, Meier T. Review of a priori dietary quality indices in relation to their construction criteria. Nutr Rev. 2018;76(10):747–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Mullie P, Clarys P, Hulens M, Vansant G. Dietary patterns and socioeconomic position. Eur J Clin Nutr. 2010;64(3):231–8. [DOI] [PubMed] [Google Scholar]
- 50. Schwingshackl L, Hoffmann G. Diet quality as assessed by the Healthy Eating Index, the Alternate Healthy Eating Index, the Dietary Approaches to Stop Hypertension score, and health outcomes: a systematic review and meta-analysis of cohort studies. J Acad Nutr Diet. 2015;115(5):780–800.e5. [DOI] [PubMed] [Google Scholar]
- 51. Schwingshackl L, Bogensberger B, Hoffmann G. Diet quality as assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and health outcomes: an updated systematic review and meta-analysis of cohort studies. J Acad Nutr Diet. 2018;118(1):74–100.e11. [DOI] [PubMed] [Google Scholar]
- 52. Potter J, Brown L, Williams RL, Byles J, Collins CE. Diet quality and cancer outcomes in adults: a systematic review of epidemiological studies. Int J Mol Sci. 2016;17(7):1052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Schwingshackl L, Hoffmann G. Does a Mediterranean-type diet reduce cancer risk?. Curr Nutr Rep. 2016;5(1):9–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Schwingshackl L, Schwedhelm C, Galbete C, Hoffmann G. Adherence to Mediterranean diet and risk of cancer: an updated systematic review and meta-analysis. Nutrients. 2017;9(10):1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Morze J, Danielewicz A, Hoffmann G, Schwingshackl L. Diet quality as assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and health outcomes: a second update of a systematic review and meta-analysis of cohort studies. J Acad Nutr Diet. 2020;120(12):1998–2031.e15. [DOI] [PubMed] [Google Scholar]
- 56. da Silva ICM, França GV, Barros AJD, Amouzou A, Krasevec J, Victora CG. Socioeconomic inequalities persist despite declining stunting prevalence in low- and middle-income countries. J Nutr. 2018;148(2):254–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Seiluri T, Lahelma E, Rahkonen O, Lallukka T. Changes in socio-economic differences in food habits over time. Public Health Nutr. 2011;14(11):1919–26. [DOI] [PubMed] [Google Scholar]
- 58. Ernstsen L, Strand BH, Nilsen SM, Espnes GA, Krokstad S. Trends in absolute and relative educational inequalities in four modifiable ischaemic heart disease risk factors: repeated cross-sectional surveys from the Nord-Trondelag Health Study (HUNT) 1984–2008. BMC Public Health. 2012;12(1):266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. National Cancer Institute (NCI). Summary tables: recommendations on potential approaches to dietary assessment for different research objectives requiring group-level estimates. [Internet]. Bethesda, MD: NCI; 2020; [cited 19 April, 2020]. Available from: https://dietassessmentprimer.cancer.gov/approach/table.html. [Google Scholar]
- 60. Garriguet D. Accounting for misreporting when comparing energy intake across time in Canada. Health Rep. 2018;29(5):3–12. [PubMed] [Google Scholar]
- 61. Kirkpatrick SI, Reedy J, Krebs-Smith SM, Pannucci TE, Subar AF, Wilson MM, Lerman JL, Tooze JA. Applications of the Healthy Eating Index for surveillance, epidemiology, and intervention research: considerations and caveats. J Acad Nutr Diet. 2018;118(9):1603–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. McLaren L. Socioeconomic status and obesity. Epidemiol Rev. 2007;29(1):29–48. [DOI] [PubMed] [Google Scholar]
- 63. Aggarwal A, Monsivais P, Cook AJ, Drewnowski A. Does diet cost mediate the relation between socioeconomic position and diet quality?. Eur J Clin Nutr. 2011;65(9):1059–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Shahidi FV, Parnia A, Siddiqi A. Trends in socioeconomic inequalities in premature and avoidable mortality in Canada, 1991–2016. Can Med Assoc J. 2020;192(39):E1114–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Hendi AS, Elo IT, Martikainen P. The implications of changing education distributions for life expectancy gradients. Soc Sci Med. 2021;272:113712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Montez JK, Zajacova A. Why is life expectancy declining among low-educated women in the United States?. Am J Public Health. 2014;104(10):e5–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Rao M, Afshin A, Singh G, Mozaffarian D. Do healthier foods and diet patterns cost more than less healthy options? A systematic review and meta-analysis. BMJ Open. 2013;3(12):e004277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Dalhousie University, University of Guelph. Canada's Food Price Report. [Internet]. 10th ed. Halifax, Nova Scotia and Guelph, Ontario: Dalhousie University and University of Guelph; 2020; [cited 7 January, 2020]. Available from: https://cdn.dal.ca/content/dam/dalhousie/pdf/sites/agri-food/Canada%20Food%20Price%20Report%20Eng%202020.pdf. [Google Scholar]
- 69. Freedman LS, Commins JM, Moler JE, Arab L, Baer DJ, Kipnis V, Midthune D, Moshfegh AJ, Neuhouser ML, Prentice RLet al. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for energy and protein intake. Am J Epidemiol. 2014;180(2):172–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Freedman LS, Commins JM, Moler JE, Willett W, Tinker LF, Subar AF, Spiegelman D, Rhodes D, Potischman N, Neuhouser MLet al. Pooled results from 5 validation studies of dietary self-report instruments using recovery biomarkers for potassium and sodium intake. Am J Epidemiol. 2015;181(7):473–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Statistics Canada. Comparison of results from the Canadian Community Health Surveys-Nutrition 2004 vs 2015, presented via webinar. Ottawa, Ontario: Statistics Canada; 2018. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data described in the article, code book, and analytic code will not be made available because the data are held by Statistics Canada. Statistics Canada permits approved researchers to access its data sets within its Research Data Centres (https://www.statcan.gc.ca/eng/microdata/data-centres).