

Abstract
A 50-year-old woman with stage IV sigmoid adenocarcinoma presented for restaging FDG PET/CT status post neoadjuvant chemotherapy/immunotherapy and diverting sigmoid colostomy. FDG PET/CT demonstrated FDG uptake in the known sigmoid mass and in abdominopelvic lymph node metastases. Bilateral, asymmetric, hypermetabolic axillary lymphadenopathy was also observed, an atypical pattern of spread for colon cancer. Further investigation revealed the patient had received both doses of COVID-19 vaccine in the 2 months prior to presentation. The authors discuss immunogenic nodal hypermetabolism following vaccination against COVID-19 and incorporating vaccination history to aid in PET/CT interpretation, especially in malignancies involving the axillae.
Key Words: bilateral lymphadenopathy, COVID-19, FDG PET/CT, vaccination
FIGURE 1.
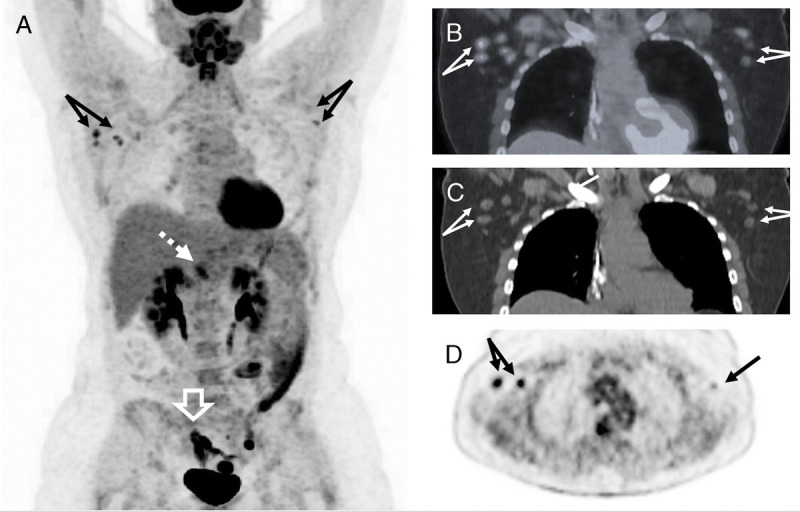
A 50-year-old woman with biopsy-proven stage IV invasive adenocarcinoma of the sigmoid colon with known nodal and peritoneal metastases presented for restaging FDG PET/CT status post neoadjuvant chemotherapy/immunotherapy and diverting sigmoid colostomy without resection. No prior FDG PET/CT was available for comparison. FDG PET/CT demonstrated FDG uptake within the known sigmoid mass and several hypermetabolic abdominopelvic lymph node metastases. Unexpected bilateral, asymmetric, FDG-avid lymphadenopathy was also observed. Maximum intensity projection coronal PET (A), coronal fused (B), CT (C), and axial PET (D) images demonstrate FDG-avid bilateral axillary lymph nodes with right-sided SUVmax of 5.2 (double arrow in D) and left-sided SUVmax of 3.5 (single arrow in D). Axillary uptake was less than that of the primary sigmoid tumor (white outlined arrow in A with SUVmax of 22.5) and a portocaval lymph node metastasis (white dashed arrow in A with SUVmax of 5.8). Additional clinical history revealed the patient received the first dose of the Moderna COVID-19 vaccine in the left deltoid muscle 2 months prior to imaging and the second dose in the right deltoid muscle 1 month prior to imaging. The higher SUVmax on the right in comparison to the left likely reflects the longer time interval between the left-sided vaccination and imaging and corresponding decreasing hypermetabolism. There have been reports of lymphadenopathy following vaccination in the literature since at least 1984, including after the bacillus Calmette-Guérin vaccine and following vaccination against human papillomavirus.1–3 FDG uptake in axillary lymph nodes has been observed following vaccination against influenza,4,5 H1N1 influenza,6 and most recently the Pfizer and Moderna mRNA COVID-19 vaccines.7,8 The initial Moderna vaccine trial reported adenopathy in 1.1% of patients and axillary swelling or tenderness in 16% of patients 18 to 64 years old and 8.4% in patients older than 65 years.9 Although clinical reports describing imaging evidence of lymphadenopathy following COVID-19 vaccination10–12 are increasing in the literature, the incidence of these imaging findings is not yet known. As mass-vaccination efforts against COVID-19 continue, radiology has responded with a special report by a multidisciplinary panel of experts.13 Their recommendations include imaging prior to vaccination whenever possible, never delaying vaccination, and waiting at least 6 weeks for routine surveillance imaging following vaccination. Imaging that is urgent or time-sensitive, including for assessment of treatment response, should not be delayed. These images show the evolution of dose 1– and dose 2–induced FDG-avid lymphadenopathy in a single patient following COVID-19 vaccination. The residual FDG uptake in the left arm 8 weeks following dose 1 of the vaccination is significantly longer than the previously reported 5 weeks8 and after the 6-week waiting period recommended before surveillance imaging recommences.13 In this case, the rarity of axillary lymph node metastases in colon cancer14 prompted investigation, which revealed recent vaccination. As vaccination efforts increase, the interpreting physician must be cognizant of the sequelae of vaccination and its time course, especially in patients with active malignancy.
Footnotes
Conflicts of interest and sources of funding: none declared.
Contributor Information
Sophia R. O’Brien, Email: sophiarobrien@gmail.com.
Karen C. Rosenspire, Email: karen.rosenspire@pennmedicine.upenn.edu.
Jacob G. Dubroff, Email: jacob.dubroff@pennmedicine.upenn.edu.
Austin R. Pantel, Email: austin.pantel@pennmedicine.upenn.edu.
REFERENCES
- 1.Katzir Z Okon E Ludmirski A, et al. Generalized lymphadenitis following B.C.G. vaccination in an immunocompetent 12-year-old boy. Eur J Pediatr. 1984;141:165–167. [DOI] [PubMed] [Google Scholar]
- 2.Studdiford J Lamb K Horvath K, et al. Development of unilateral cervical and supraclavicular lymphadenopathy after human papilloma virus vaccination. Pharmacotherapy. 2008;28:1194–1197. [DOI] [PubMed] [Google Scholar]
- 3.Pereira MP, Flores P, Neto AS. Neck and supraclavicular lymphadenopathy secondary to 9-valent human papillomavirus vaccination. BMJ Case Rep. 2019;12:e231582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Williams G, Joyce RM, Parker JA. False-positive axillary lymph node on FDG-PET/CT scan resulting from immunization. Clin Nucl Med. 2006;31:731–732. [DOI] [PubMed] [Google Scholar]
- 5.Ayati N Jesudason S Berlangieri SU, et al. Generalized lymph node activation after influenza vaccination on 18F FDG-PET/CT imaging, an important pitfall in PET interpretation. Asia Ocean J Nucl Med Biol. 2017;5:148–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Burger IA Husmann L Hany TF, et al. Incidence and intensity of F-18 FDG uptake after vaccination with H1N1 vaccine. Clin Nucl Med. 2011;36:848–853. [DOI] [PubMed] [Google Scholar]
- 7.Eifer M, Eshet Y. Imaging of COVID-19 vaccination at FDG PET/CT. Radiology. 2021;210030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hanneman K, Iwanochko RM, Thavendiranathan P. Evolution of lymphadenopathy at PET/MRI after COVID-19 vaccination. Radiology. 2021;210386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Local reactions, systemic reactions, adverse events, and serious adverse events: Moderna COVID-19 vaccine | CDC. Available at: https://www.cdc.gov/vaccines/covid-19/info-by-product/moderna/reactogenicity.html. Accessed February 2, 2021.
- 10.Özütemiz C Krystosek LA Church AL, et al. Lymphadenopathy in COVID-19 vaccine recipients: diagnostic dilemma in oncology patients. Radiology. 2021;210275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Edmonds CE, Zuckerman SP, Conant EF. Management of unilateral axillary lymphadenopathy detected on breast MRI in the era of coronavirus disease (COVID-19) vaccination. AJR Am J Roentgenol. 2021. [DOI] [PubMed] [Google Scholar]
- 12.Cellina M, Irmici G, Carrafiello G. Unilateral axillary lymphadenopathy after coronavirus disease (COVID-19) vaccination. AJR Am J Roentgenol. 2021;W1. [DOI] [PubMed] [Google Scholar]
- 13.Becker AS Perez-Johnston R Chikarmane SA, et al. Multidisciplinary recommendations regarding post-vaccine adenopathy and radiologic imaging: Radiology Scientific Expert Panel. Radiology. 2021;210436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lipsyc MD Yaeger R Dengel LT, et al. Axillary lymph node involvement, a unique pattern of metastasis in BRAF-mutant colorectal cancer. JAMA Oncol. 2015;1:686–687. [DOI] [PMC free article] [PubMed] [Google Scholar]