

ABSTRACT
Background
Policy and social change have increased women’s participation in the labour market and their opportunity to combine paid work with family care. We analyse whether a specific combination of employment and domestic duties over the life course are associated with variations in English and French women’s health, focusing on two birth cohorts.
Methods
We used sequence analysis to group women in English Longitudinal Study of Ageing and Survey of Health, Ageing and Retirement in Europe, according to their work and family histories. Using ordered logistic regression, we tested for group differences in later self-reported health and depressive symptoms, while controlling for a range of adult socio-economic circumstances.
Results
The findings confirm important differences between birth cohorts and countries. French women report a higher risk of poor self-reported health and mental issues than English women. Full-time domestic duties were particularly deleterious for the health of the two younger cohorts, whereas a combination of employment and domestic duties across the life course had a positive association with later-life health.
Discussion
Further research is needed to explore the mechanisms linking work and care trajectories to poor health.
Keywords: life course, older people, women's health
Employment trajectories and health: cohort differences in English and French women
It is increasingly recognised that we require an understanding of risk factors across the life course in order to identify those at subsequent risk of ill-health in later life. Research has extensively indicated that the individual’s conditions in childhood are strongly associated with those in later life1 and that individual life courses have an important impact in framing physical and mental health of later lives.2–5 It has been documented convincingly that, in particular, labour market history affects our health over time.6–13
Earlier work10 highlighted the impact of work–life balance across countries for women. Despite the fact that social developments and policy change over the last decades have increased women’s participation in the labour market, female working lives are still constrained by family responsibilities. Therefore, compared with male life courses, women’s work trajectories are more fragmented, as women still combine economic employment with domestic duties. These experiences have the potential to shape their longer-term health, causing negative health conditions, as highlighted by the role conflict hypothesis14 or, on the contrary, leading to health advantages, as suggested by the role enhancement hypothesis.15
Previous work by Zella and Harper10 revealed that having paid work and combining it with domestic duties across the life course had a positive effect on late life health. In contrast, staying at home as care provider for the entire life was detrimental for health in old age. Therefore, the authors argued that work and family histories could be used to identify women at the risk of later life and allow proposing of concrete actions.
In this paper, we develop these ideas, analysing both mental- and self-rated health and suggesting that linking work history to later life health must also consider simultaneously generation effect and country effect. A central aspect of our paper is the identification of cohort differences. Cohort differences provide information about changes in health and quality of life over time, which will be useful for developing interventions. It might also suggest a rethinking of effective health policies, resource allocation models and intervention strategies to combat the societal costs associated with a health issue in later life. Furthermore, cohort improvements in health over time have the potential to reduce the costs associated with a more elderly population. Similarly, the comparative approach might clarify the need for labour market interventions and family-friendly policies.
French and English women have historically experienced very different employment patterns, as the interplay of different economic and demographic variables has shaped both job opportunities and family positions.16,17 In particular, it has been argued that the provision of good child support in France has enabled mothers to remain full-time within the labour market, whereas the lack of these created a part-time employment norm for mothers in England.18,19 Thus England has been characterised by limited and usually means-tested state support to families, with low public investment in childcare, and the dominance of market-based solution regarding welfare provision. The French state, instead, has long provided larger supports to families, with a medium provision of childcare services, and a medium level of replacement rates for leaves, but high child allowances, which has facilitated the combination of paid work and family responsibilities for women.17 As a consequence, French women have tended to combine full-time employment with parenting, whereas English women have either remained at home as full-time carers for their children or have combined child care with part-time employment. We thus examine these different work–care–life trajectories between the two countries and the impact these may have on late life (mental and physical) health.
We firstly summarise employment histories of English and French women using the annual information on the occupational situation from age 25–55 for two birth cohorts: pre-1940 and 1940–1954. Using ideal-type sequence analysis of work histories, we identified five patterns of combining work with family care across the life course.20 Second, we investigate whether there are differences in health between these two cohorts according to these trajectories, while taking into account country differences.
Methods
Data
Data from the Survey of Health, Ageing and Retirement in Europe (SHARE) for France and from the English Longitudinal Study of Ageing (ELSA) for England are employed. SHARE is a cross-national panel survey that provides comparable information on health, social conditions and employment of European individuals aged 50+.21 Similarly, ELSA is a longitudinal study of the English population aged 50 years and older. Both ELSA (in wave three, year 2006/07) and SHARE (in SHARELIFE, year 2009) provide retrospective information of each individual from childhood. They thus offer a complete history of changes in health and socio-economic characteristics over the entire life. The retrospective waves of ELSA and SHARE have been merged to, respectively, the first six waves of ELSA (from 2002 until 2013) and the first five waves of SHARE (from 2004 until 2013) in order to obtain a complete set of information on individuals’ health.
Some restrictions of the sample are necessary to avoid results, which are related to sample composition or to avoid findings, which are attributable to reverse causation. In particular, we have included individuals who had the entire working history between age 25 and 55 and excluded people who had difficulties in responding to the retrospective questionnaire and those who have declared to have had poor health during childhood. After the mentioned selections, our sample includes in total 3440 English women and 1113 French women.
Dependent variables
We used two variables to measure health in later life: self-reported health and depression. Self-reported health is measured both in ELSA and in SHARE by the following question: ‘How is your health in general?’ The possible responses are excellent, good, fair, bad and very bad, and they are coded 1, 2, 3, 4, and 5, respectively. Self-reported health has been found to be a reliable physical health measure in multiple studies.22,23
ELSA and SHARE define depressive symptoms based on two distinctive internationally established instruments: the Centre for Epidemiological Studies Depression scale24 and the EURO-D depression scale.25 A high degree of comparability of results from the two scales has been demonstrated,26–29 with a cut point ≥4 indicating clinically relevant depressive symptoms.27,28 However, the nature of these scales and the methodological discussion on the comparison between different outcomes lead us to read carefully the results.30
Independent variables
Both in SHARE and ELSA, the participants were asked to report each employment and unemployment episode since leaving full-time education. Several information on each job were collected: the year of job started and ended, whether a job was part-time or full-time and the duration of any gaps between jobs. As a part of family history, participants were asked to report the date of birth of each natural child. They were also asked whether and for how long they had stopped working when each child was born.
Using sequence analysis (‘SQ_Ados’ in Stata) and employing the principle of ‘sequencing’,31 a year-by-year labour market history was created for each woman in the French and English samples. In order to compare England and France, five identical categories have been created for these two countries:
Full-time employment: women who were employed full-time throughout their working life.
Combined full-time employment and part-time employment: women who exchange full-time and part-time employment throughout their working life.
Combined domestic duties and paid work: women who exchange domestic duties and paid work (full-time and part-time) throughout their working life.
Domestic duties: women who worked at home throughout their working life.
Other mixed-trajectories: includes all the other combinations (excluded in previous categories).
Covariates
Our analyses control for the main potential confounders of the relationship between work trajectory and health in later life, which are birth cohort, age, number of years of education, assets, presence of the partner and presence of children. All these variables have been harmonised in SHARE and ELSA. The cohort is organised in two categories: the first group includes women born before 1940, and the second category includes all the other women (born between 1940 and 1954). Age is kept as numerical variable. Education is a four-category variable (less than age 11, between age 11 and 13, between age 13 and 16, age 16 or more). Presence of the partner and the presence of children were measured in the same wave as self-reported health and depressive symptoms. Presence of the partner was distinguished as ‘living alone’ and ‘living with a partner’, whereas the presence of children was kept as a continuous variable (where ‘0’ means no children).
After a sample description and bivariate analyses (Table 1), linear and ordered logistic regression (OLR) models were used to study the association between the dependent variables and work trajectories in the two mentioned cohorts of English and French women (Tables 2 and 3). The OLR has four main assumptions: (i) the dependent variable is ordered, (ii) one or more of the independent variables are either continuous, categorical or ordinal, (iii) there is no multi-collinearity and (iv) the proportional odds. All these assumptions were tested at the beginning of our analyses. Finally, the predicted probabilities were estimated (Fig. 1).
Table 1.
A typology of job trajectory of English and French women in the two birth cohorts
| England | France | |||
|---|---|---|---|---|
| Birth cohort < 1940 | Birth cohort 1940–1954 | Birth cohort < 1940 | Birth cohort 1940–1954 | |
| Domestic work | 32.9 | 28.9 | 12.9 | 13.1 |
| Full-time employment | 24.0 | 27.7 | 35.8 | 48.1 |
| Combined full-time and part-time employment | 11.9 | 19.9 | 2.2 | 10.5 |
| Combined domestic work and paid work | 17.6 | 8.7 | 35.8 | 18.9 |
| Other mixed-trajectories | 13.6 | 14.8 | 13.3 | 9.4 |
| N | 1688 | 495 | 1752 | 618 |
Table 2.
Odds of having poor self-reported health (odds ratios and CI 95%) for the two birth cohorts
| Birth cohort < 1940 | Birth cohort 1940–1954 | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |
| Odds ratio | Odds ratio | Odds ratio | Odds ratio | |
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | |
| Domestic work* England | Ref. | Ref. | Ref. | Ref. |
| Full-time employment* England | 0.410 | 0.055 | 0.000 | 0.008 |
| (0.85, 1.49) | (0.99, 1.84) | (0.35, 0.71) | (0.33, 0.85) | |
| Combined full-time and part-time employment* England | 0.422 | 0.285 | 0.003 | 0.011 |
| (0.82, 1.60) | (0.85, 1.73) | (0.41, 0.84) | (0.33, 0.87) | |
| Combined domestic work and paid work* England | 0.361 | 0.081 | 0.000 | 0.001 |
| (0.86, 1.47) | (0.97, 1.69) | (0.36, 0.71) | (0.30, 0.73) | |
| Other mixed-trajectories* England | 0.388 | 0.143 | 0.324 | 0.987 |
| (0.83, 1.60) | (0.92, 1.81) | (0.83, 1.77) | (0.60, 1.64) | |
| Domestic work* France | 0.000 | 0.000 | 0.091 | 0.818 |
| (1.54, 3.06) | (2.13, 4.61) | (0.94, 2.30) | (0.57, 2.02) | |
| Full-time employment* France | 0.000 | 0.000 | 0.000 | 0.008 |
| (1.63, 3.21) | (2.41, 5.23) | (1.60, 3.33) | (1.23, 3.82) | |
| Combined full-time and part-time employment* France | 0.046 | 0.005 | 0.557 | 0.827 |
| (1.02, 9.65) | (1.64, 15.74) | (0.69, 1.98) | (0.43, 1.96) | |
| Combined domestic work and paid work* France | 0.000 | 0.000 | 0.023 | 0.560 |
| (1.52, 3.96) | (2.17, 6.01) | (1.08, 2.90) | (0.60, 2.46) | |
| Other mixed-trajectories* France | 0.000 | 0.000 | 0.007 | 0.018 |
| (1.82, 5.09) | (2.44, 7.20) | (1.24, 3.79) | (1.19, 6.16) | |
| Log likelihood | −2342.01 | −2196.82 | −2442.47 | −1391.41 |
| Pseudo R2 | 0.015 | 0.032 | 0.044 | 0.066 |
| N | 2181 | 2080 | 2363 | 1367 |
MODEL 2 adjusted for: age, number of years of education, assets, presence of the partner and presence of children.
CI, confidence interval.
Table 3.
Odds of having depressive symptoms (odds ratios and CI 95%) for the two birth cohorts
| Birth cohort < 1940 | Birth cohort 1940–1954 | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |
| Odds ratio | Odds ratio | Odds ratio | Odds ratio | |
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | |
| Domestic work* England | Ref. | Ref. | Ref. | Ref. |
| Full-time employment* England | 0.106 | 0.360 | 0.060 | 0.285 |
| (0.49, 1.07) | (0.54, 1.25) | (0.38, 1.02) | (0.35, 1.36) | |
| Combined full-time and part-time employment* England | 0.468 | 0.521 | 0.061 | 0.289 |
| (0.53, 1.33) | (0.53, 1.38) | (0.36, 1.02) | (0.35, 1.37) | |
| Combined domestic work and paid work* England | 0.241 | 0.493 | 0.085 | 0.178 |
| (0.56, 1.15) | (0.61, 1.27) | (0.40, 1.06) | (0.34, 1.22) | |
| Other mixed-trajectories* England | 0.631 | 0.430 | 0.146 | 0.348 |
| (0.73, 1.69) | (0.77, 1.84) | (0.88, 2.38) | (0.70, 2.70) | |
| Domestic work* France | 0.001 | 0.000 | 0.114 | 0.438 |
| (1.34, 3.09) | (1.76, 4.68) | (0.89, 2.85) | (0.60, 3.23) | |
| Full-time employment* France | 0.015 | 0.000 | 0.001 | 0.003 |
| (1.11, 2.60) | (1.50, 4.07) | (1.42, 3.67) | (1.49, 6.58) | |
| Combined full-time and part-time employment* France | 0.370 | 0.633 | 0.002 | 0.204 |
| (0.05, 3.08) | (0.07, 4.86) | (1.45, 5.28) | (0.71, 5.02) | |
| Combined domestic work and paid work* France | 0.035 | 0.002 | 0.004 | 0.029 |
| (1.04, 3.42) | (1.42, 5.10) | (1.34, 4.45) | (1.11, 6.50) | |
| Other mixed-trajectories* France | 0.001 | 0.000 | 0.015 | 0.093 |
| (1.52, 4.72) | (2.01, 6.86) | (1.18, 4.60) | (0.86, 6.61) | |
| Log likelihood | −1110.64 | −1061.83 | −1113.10 | −633.34 |
| Pseudo R2 | 0.026 | 0.038 | 0.051 | 0.075 |
| N | 2183 | 2080 | 2370 | 1367 |
Model 2 adjusted for: age, number of years of education, assets, presence of the partner and presence of children.
Fig. 1 .
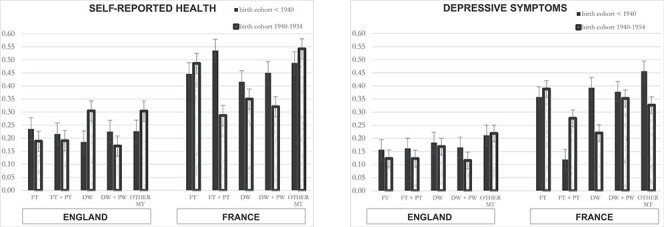
Probability of poor self-reported health and depressive symptoms by work history. FT, full-time employment; FT + PT, combined full-time employment and part-time employment; DW, domestic duties; DW + PW, combined domestic duties and paid work; OTHER MT, other mixed-trajectories.
Results
Differences between countries and cohorts
In general, a high proportion of all French women reported poorer subjective health and more depressive symptoms. Of the sample, one-fifth (22.6%) of English women compared with over one-third (38.4%) of French women reported only poor or fair health. Twice as many French women were at the higher risk of depression (33.2%) than English women (16.5%) (Supplementary Table S1). A higher proportion of English women in the older cohort had poor health post-retirement relative to the young cohort post-retirement, while this was reversed in the French sample, where the younger cohort of French women had poorer health in retirement than the older cohort. Bivariate analyses did not show differences in depression symptoms between cohorts in France, whereas in England women from the older cohorts were at higher risks of depression than those from the younger cohort.
There were notable differences in women’s employment experiences both between the two countries and between the two cohorts (Table 1). As we hypothesised, in both cohorts the largest group of French women undertook full-time employment, whereas in England this was care. In France, over one-third (35.8%) of women in the older cohort and nearly half of the women in the younger cohort (48.1%) had undertaken full-time employment throughout their entire life. In comparison, 32.9% of the older English women and 28.9% of the younger cohort had spent all their life in domestic duties, and a further near third had combined full-time child care with part-time work.
Ordered logistic models
Table 2 examines the odds of poor self-reported health, focusing on differences between countries and cohorts. Focusing on the older cohort, French women had a higher risk of poor health compared with English women and this happens regardless of their work trajectories.
The younger cohort presents instead a different picture. The combination of paid and unpaid work as well as working full-time for the entire life clearly decreased the risk of poor health for English women, in comparison with English women who stayed at home for their entire life. At the same time, French women who had worked full-time throughout their entire life in France were more likely to report worse health in later life than those who never participated in the labour market. The addition of covariates to the model had little effect on the estimates.
Table 3 shows the results of the association between work trajectories and depressive symptoms. The results of depression symptoms (Table 3) show that the odds of the older cohort do not highlight any statistical significance in depression symptoms among English women with different labour market trajectories. However, English women have lower risks of being depressed in later life than French women.
Predicted probabilities
Figure 1 describes the predicted probability of the two health measures by work history in the two cohorts.
In the older cohort, the greatest probability of poor self-reported health was observed for women who combined part-time and full-time work in France, followed by those who had mixed work trajectories. For the same cohort of English women, working full-time lead to poor self-reported health, whereas working domestic duties throughout their working life increased the chance of better health in later life.
Importantly, for the younger cohort of the English sample, the lowest risk of health problems was found among women who combined paid and unpaid work. The combination of part-time and full-time positions and the interchange of paid and unpaid work also protected the younger French women. However, for younger French women being involved in full-time employment or having unstable career lead to worse health outcomes.
In terms of mental well-being for the two older cohorts, unstable trajectories led to the highest probability of poor mental health for both English and French women. Interestingly, combining life styles (full-time employment and part-time employment as well as domestic duties and paid work) protected English women from mental issues in later life. However, working full-time led French women to better mental health in later life. This may be related to the norm in this country where older women’s peers will also have worked full-time. For the younger cohorts, however, having an occupation or interchanging employment with domestic duties reduced the risk of the mental health issue of English women. However, for younger France women, the best mental benefits arose through domestic duties or in the combination of full-time and part-time jobs.
Discussion and conclusion
Main finding of this study
The paper investigates the association between life course trajectories and health in later life of English and French women in two birth cohorts. The results highlight that differences between countries and cohorts are particularly interesting. Firstly, French women report poorer self-reported health and higher mental issues than English women regardless of their work history. In terms of ‘physical health,’ older cohorts in both France and England had better health if they had been full-time caregivers for their entire lives. Alternatively, for the younger cohorts in both countries, it was the combination of paid and unpaid work, which supported higher ‘physical health.’ In terms of ‘mental health,’ working full-time for the entire life was detrimental for women’s health for the older cohort of the English sample, whereas the combination of paid and unpaid work led to a better mental health for English women in both cohorts. The French evidence was less clear cut, working full-time for the entire life was detrimental for women’s mental health for the younger cohort of French sample, but less so for the older cohort. In common with other studies, these analyses reveal that women in this sample experience a mixture of health advantages and disadvantages in later life if they reported being unemployed and spending some time caring for family.
What is already known on this topic
Previous studies have highlighted that labour market history has an impact on individual’s health over time.6–9 Focusing on this association in 12 European countries, Zella and Harper (2018)10 showed that combining paid work with domestic duties across the life course had a positive effect on women’s late health, whereas staying at home as care provider for the entire life was detrimental for their health in old age. In addition, the context plays an important role in framing this association. Therefore, the authors argued that work and family histories could be used to identify women at the risk of poor health in later life and allow proposing of concrete actions.
What this study adds
Based on our knowledge, this is the first study that observes the differences in women’s work trajectories over 30 years, taking simultaneously into consideration differences between countries and birth cohorts. In particular, it further highlights the importance of policy in influencing women’s employment decisions and their subsequent well-being. Of interest is the main finding that enabling women to successfully combine child care with employment leads to better health outcomes. Furthermore, due to the richness of the ELSA and SHARE data, as well as their comparability, we are able to take into account two measures of health (physical and mental health) as well as important covariates.
Our results suggest avenues for public interventions, in particular for the new generations of old people. In this perspective, it is important that the mechanisms linking work and family care history to later life health are better understood, focusing on different contexts and birth cohort. Specifically, further research is needed to identify the timing when the health trajectories diverge, in order to identify the underlying causes of these health differences and suggesting interventions over individual’s life.
Limitations of this study
The present study represents an underexplored investigation of the association between work trajectories and health in later life in two births cohorts and in two countries. However, there are a few limitations that should be taken into consideration.
Firstly, this study does not reflect causal effect. Despite controlling for individuals characteristics, disentangling heterogeneity in attitudes, choices and preferences between individuals is complex and difficult to measure in social science research. Second, this study is based on the analysis of retrospective data and we acknowledge their limitations. Third, it is not possible to exclude that the relationship between work–family histories and health indicators differ according to other personal characteristics. If this is the case, then our study may be biased. However, adding other variables would have increased the number of work–family history categories and interactions (with corresponding reductions in cell sizes), which would make null findings more likely.
Supplementary Material
Acknowledgements
This paper uses data from ELSA and SHARE. ELSA was developed by a team of researcher based at the NatCen Social Reseach, University College London and the Institute for Fiscal Studies. The SHARE data collection has been primarily funded by the European Commission through the 5th Framework Programme (project QLK6-CT-2001-00360 in the thematic programme Quality of Life), through the 6th Framework Programme (projects SHARE-I3, RII-CT-2006-062193, COMPARE, CIT5-CT-2005-028857, and SHARELIFE, CIT4-CT-2006-028812) and through the 7th Framework Programme (SHARE-PREP, N. 211909, SHARE-LEAP, N. 227822 and SHARE M4, N. 261982). Additional funding from the US National Institute on Aging (U01 AG09740-13S2, P01 AG005842, P01 AG08291, P30 AG12815, R21 AG025169, Y1-AG4553- 01, IAG BSR06-11 and OGHA 04-064) and the German Ministry of Education and Research as well as from various national sources is gratefully acknowledged (see www.share-project.org for a full list of funding institutions).
References
- 1. Flores M, Kalwij A. The associations between early life circumstances and later life health and employment in Europe. Empir Econ 2014;4:1251–82. [Google Scholar]
- 2. Benshlomo Y, Kuh D. A life course approach to chronic disease epidemiology: conceptual models, empirical challenges and interdisciplinary perspectives. Int J Epidemiol 2002;3:285–93. [PubMed] [Google Scholar]
- 3. Elder GHJ, Johnson MK, Crosnoe R. The emergence and development of life course theory. In: Mortimer JT, Shanahan MJ (eds). Handbook of the Life Course. Hingham, MA: Kluwer Academic Publishers, 2003, 3–19. [Google Scholar]
- 4. Hayward M, Gorman B. The long arm of childhood: the influence of early-life social conditions on men’s mortality. Demography 2004;41:87–107. [DOI] [PubMed] [Google Scholar]
- 5. Platts LG, Netuveli G, Webb E et al. Physical occupational exposures during working life and quality of life after labour market exit: results from the GAZEL study. Aging Ment Health 2013;17:697–706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Avendano M, Berkman LF, Brugiavini A et al. The long-run effect of maternity leave benefits on mental health: evidence from European countries. Soc Sci Med 2015;132:45–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Benson R, Glaser K, Corna L et al. Do work and family care histories predict health in older women? Eur J Public Health 2017;6:1010–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Dragano N, Wahrendorf M. Consistent health inequalities in Europe: the importance of labour market disadvantage. J Epidemiol Community Health 2014;68:1–2. [DOI] [PubMed] [Google Scholar]
- 9. Lu W, Benson R, Glaser K et al. Relationship between employment histories and frailty trajectories in later life: evidence from the English longitudinal study of ageing. J Epidemiol Community Health 2017;71:439–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Zella S, Harper S. The impact of life course employment and domestic duties on the well-being of retired women and the social protection systems that frame this. J Aging Health 2020;32:285–295. [DOI] [PubMed] [Google Scholar]
- 11. Siegrist J, Marmot M. Health inequalities and the psychosocial environment – two scientific challenges. Soc Sci Med 2004;58:1463–73. [DOI] [PubMed] [Google Scholar]
- 12. Wahrendorf M, Blane D, Bartley M et al. Working conditions in mid-life and mental health in older ages. Adv Life Course Res 2013;18:16–25. [DOI] [PubMed] [Google Scholar]
- 13. Wahrendorf M. Previous employment histories and quality of life in older ages: sequence analyses using SHARELIFE. Ageing Soc 2015;35:1928–59. [Google Scholar]
- 14. Goode WJ. A theory of role strain. Am Sociol Rev 1960;25:483–96. [Google Scholar]
- 15. Nordenmark M. Multiple social roles and well-being a longitudinal test of the role stress theory and the role expansion theory. Acta Sociologica 2004;47:115–26. [Google Scholar]
- 16. Tilly L, Scott J. Women, Work and Family. Rutledge: New York, 1987. [Google Scholar]
- 17. O’Reilly J. Framing comparisons: gendering perspectives on cross-national comparative research on work and welfare. Work Empl Soc 2006;20:731–50. [Google Scholar]
- 18. Daune-Richard A-M. How does the “societal effect” shape the use of part-time work in France, the UK and Sweden? In: O’Reilly J, Fagan C (eds). Part-time Prospects. London: Routledge, 1998, 214–31. [Google Scholar]
- 19. Letablier M-T. Work and family balance: a new challenge for policies in France. In: Giele JZ, Holst E (eds). 2003. Changing Life Patterns in Western Industrial Societies (Advances in Life Course Research). Oxford: Elsevier, 2003, 189–210. [Google Scholar]
- 20. Abbott A. Sequence-analysis – new methods for old ideas. Annu Rev Sociol 1995;21:93–113. [Google Scholar]
- 21. Börsch-Supan A, Brandt M, Hunkler C et al. Data resource profile: the survey of health, ageing and retirement in Europe (SHARE). Int J Epidemiol 2013;42:992–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Idler E, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav 1997;38:21–37. [PubMed] [Google Scholar]
- 23. Jylhä M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med 2009;69:307–16. [DOI] [PubMed] [Google Scholar]
- 24. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Measur 1977;1:385–401. [Google Scholar]
- 25. Prince MJ, Reischies F, Beekman AT et al. Development of the EURO-D scale-a European, Union initiative to compare symptoms of depression in 14 European centres. Br J Psychiatry 1999;174:330–8. [DOI] [PubMed] [Google Scholar]
- 26. Castro-Costa E, Dewey M, Stewart R et al. Prevalence of depressive symptoms and syndromes in later life in ten European countries: the SHARE study. Br J Psychiatry 2007;191:393–401. [DOI] [PubMed] [Google Scholar]
- 27. Irwin M, Artin KH, Oxman MN. Screening for depression in the older adult: criterion validity of the 10-item Center for Epidemiological Studies Depression Scale (CES-D). Arch Intern Med 1999;159:1701–4. [DOI] [PubMed] [Google Scholar]
- 28. Larraga L, Saz P, Dewey ME et al. Validation of the Spanish version of the EURO-D scale: an instrument for detecting depression in older people. Int J Geriatr Psychiatry 2006;21:1199–205. [DOI] [PubMed] [Google Scholar]
- 29. Lunau T, Wahrendorf M, Dragano N et al. Work stress and depressive symptoms in older employees: impact of national labour and social policies. BMC Public Health 2013;13:1086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Courtin E, Knapp M, Grundy E et al. Are different measures of depressive symptoms in old age comparable? An analysis of the CES-D and Euro-D scales in 13 countries. Int J Methods Psychiatr Res 2015;24:287–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Billari FC, Fürnkranz J, Prskawetz A. Timing, sequencing, and quantum of life course events: a machine learning approach. Eur J Popul 2006;22:37–65. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.