

This cross-sectional study performs deep phenotyping and identification of severity-associated factors in adolescent and adult patients with atopic dermatitis.
Key Points
Question
What are the main factors associated with the severity of atopic dermatitis (AD)?
Findings
In this analysis of cross-sectional data collected from 367 patients with active AD (age ≥12 years), the most important factors associated with increased probability of severe AD were age between 12 and 21 years or older than 52 years, age at AD onset older than 12 years, total serum immunoglobulin E level greater than 1708 IU/mL, eosinophil values greater than 6.8%, atopic stigmata (cheilitis, white dermographism), male sex, sports less than once per week, (former) smoking, and alopecia areata.
Meaning
The phenotypic characteristics and patient age frames found in this cross-sectional analysis might contribute to a deeper disease understanding, estimation of severity probability, closer monitoring of predisposed patients, and personalized prevention and therapy.
Abstract
Importance
Atopic dermatitis (AD) is the most common chronic inflammatory skin disease and is driven by a complex pathophysiology underlying highly heterogeneous phenotypes. Current advances in precision medicine emphasize the need for stratification.
Objective
To perform deep phenotyping and identification of severity-associated factors in adolescent and adult patients with AD.
Design, Setting, and Participants
Cross-sectional data from the baseline visit of a prospective longitudinal study investigating the phenotype among inpatients and outpatients with AD from the Department of Dermatology and Allergy of the University Hospital Bonn enrolled between November 2016 and February 2020.
Main Outcomes and Measures
Patients were stratified by severity groups using the Eczema Area and Severity Index (EASI). The associations of 130 factors with AD severity were analyzed applying a machine learning–gradient boosting approach with cross-validation–based tuning as well as multinomial logistic regression.
Results
A total of 367 patients (157 male [42.8%]; mean [SD] age, 39 [17] years; 94% adults) were analyzed. Among the participants, 177 (48.2%) had mild disease (EASI ≤7), 120 (32.7%) had moderate disease (EASI >7 and ≤ 21), and 70 (19.1%) had severe disease (EASI >21). Atopic stigmata (cheilitis: odds ratio [OR], 8.10; 95% CI, 3.35-10.59; white dermographism: OR, 4.42; 95% CI, 1.68-11.64; Hertoghe sign: OR, 2.75; 95% CI, 1.27-5.93; nipple eczema: OR, 4.97; 95% CI, 1.56-15.78) was associated with increased probability of severe AD, while female sex was associated with reduced probability (OR, 0.30; 95% CI, 0.13-0.66). The probability of severe AD was associated with total serum immunoglobulin E levels greater than 1708 IU/mL and eosinophil values greater than 6.8%. Patients aged 12 to 21 years or older than 52 years had an elevated probability of severe AD; patients aged 22 to 51 years had an elevated probability of mild AD. Age at AD onset older than 12 years was associated with increased probability of severe AD up to a peak at 30 years; age at onset older than 33 years was associated with moderate to severe AD; and childhood onset was associated with mild AD (peak, 7 years). Lifestyle factors associated with severe AD were physical activity less than once per week and (former) smoking. Alopecia areata was associated with moderate (OR, 5.23; 95% CI, 1.53-17.88) and severe (OR, 4.67; 95% CI, 1.01-21.56) AD. Predictive performance of machine learning–gradient boosting vs multinomial logistic regression differed only slightly (mean multiclass area under the curve value: 0.71 [95% CI, 0.69-0.72] vs 0.68 [0.66-0.70], respectively).
Conclusions and Relevance
The associations found in this cross-sectional study among patients with AD might contribute to a deeper disease understanding, closer monitoring of predisposed patients, and personalized prevention and therapy.
Introduction
Atopic dermatitis (AD) is the most common chronic inflammatory skin disease with a high impact on patients’ quality of life, productivity at work, and burden on the health system, with an increasing cumulative lifetime prevalence of 15% to 28% in industrial nations.1,2 The pathophysiology is complex and multifactorial. Main mechanistic factors are an altered skin barrier and a modified innate and adaptive immune system, both with a strong genetic background and influenced by gene–environment interactions as well as skin microbiome dysbiosis.1,3,4,5,6
There is a wide range in the clinical phenotype, with severity ranging from minimal to erythrodermic forms involving the whole body and many different disease courses.1,7,8,9,10,11,12,13,14 Apparently, the different genetic, immunologic, and environmental factors do not contribute in the same extent to every patient. This requires a more detailed definition of the heterogeneous (endo)phenotypes.
Owing to recent efforts of a precision medicine approach in AD, there has been a growing interest in deep phenotyping. Early phenotyping focused primarily on case/cohort ascertainment.15,16,17 Conversely, deep phenotyping shifted the focus from identification to characterization. It aims to deliver precise and comprehensive characterization of observable traits representing unique morphological, biochemical, physiological, or behavioral properties of the identified patient populations.16,17 This study aimed to evaluate the phenotype and potential risk factors in adolescent and adult patients with AD stratified by disease severity.
Methods
Study Design and Participants
In this study, cross-sectional data from the baseline visit of a prospective longitudinal study investigating the phenotype of patients with AD were analyzed. Inpatients and outpatients 12 years and older with active AD, fulfilling the Hanifin and Rajka criteria, were enrolled between November 2016 and February 2020 in the CK-CARE program18 at the University Hospital Bonn after providing oral and written informed consent. Exclusion criteria were systemic treatment and disease remission.
All participants completed a standardized questionnaire regarding personal and family history of atopy, disease course, comorbidities, lifestyle, environment, drug intake, and the Dermatology Life Quality Index (DLQI).19 They were examined regarding severity of eczema (Eczema Area and Severity Index [EASI]),20 SCORing Atopic Dermatitis (SCORAD),21,22 and atopic stigmata by an experienced dermatologist. Patients with an EASI of 7 or less were considered as having mild disease; EASI greater than 7 and less than or equal to 21 was moderate disease; and EASI greater than 21 was severe disease.20,21,22 All study methods followed the Declaration of Helsinki and have been approved by the local ethics committee.
Statistical Analysis
The associations of 130 factors with AD severity were analyzed using a machine learning–gradient boosting approach with cross-validation–based tuning (MLGB)23,24 and multinomial logistic regression with forward variable selection (MLR)25 (reference group: mild AD; eMethods in the Supplement). The contribution of variables to the MLGB prediction model was evaluated by permutation-based variable importance26 regarding differences in multinomial log-likelihood (eTable 1 in the Supplement). Each importance value represents the mean decrease in model fit if the values of the variable were permuted randomly. Higher numbers represent more important variables. To further illustrate the effects of each variable, we generated accumulated local effect (ALE) plots.27 These show the mean change of the predictions for a given value of the respective variable compared with an average prediction. Performance of the models was evaluated by computing the predictive multiclass area under the curve (AUC)28 with nested 10 × 10-fold stratified cross-validation. All P values are 2-sided and values less than .05 were considered statistically significant. Statistical analysis was conducted using R, version 3.5.3 (R Foundation)29 with packages xgboost,30 caret,31 pROC,32 coin33 and ALEPlot34 and SPSS Statistics for Windows, version 25.0 (IBM Corp).
Results
Patients and Disease Severity
A total of 367 patients were included: 210 (57%) female, 157 (43%) male; mean (SD) age, 39 (17) years (range, 12-89 years); 94% adults (Table; eTable 2 in the Supplement). The severity scores EASI, affected body surface area (BSA), and SCORAD highly correlated among each other (EASI vs BSA: rs = 0.82; 95% CI, 0.77-0.85; EASI vs SCORAD: rs = 0.78; 95% CI, 0.74-0.82; EASI vs objective SCORAD [oSCORAD]: rs = 0.80; 95% CI, 0.76-0.83; all P < .001).
Table. Multinomial Logistic Regression Analysis of Patients With Atopic Dermatitis (AD) Stratified by Disease Severity (EASI) Groupsa.
| Characteristic | No. (%) | Moderate AD | Severe AD | |||||
|---|---|---|---|---|---|---|---|---|
| All patients | Mild AD | No. (%) | OR (95% CI) | P value | No. (%) | OR (95% CI) | P value | |
| Female sex | 210/367 (57.2) | 118/177 (66.7) | 61/120 (50.8) | 0.46 (0.26-0.84) | .01 | 31/70 (44.3) | 0.30 (0.13-0.66) | .003 |
| Atopic stigmata | ||||||||
| Cheilitis sicca | 179/367 (48.8) | 71/177 (40.1) | 57/120 (47.5) | 1.65 (0.91-2.30) | .10 | 51/70 (72.9) | 8.10 (3.35-19.59) | <.001 |
| Nipple eczema | 42/367 (11.4) | 9/177 (5.1) | 16/120 (13.3) | 2.23 (0.83-6.02) | .11 | 17/70 (24.3) | 4.97 (1.56-15.78) | .007 |
| White dermographism | 244/367 (66.5) | 93/177 (52.5) | 90/120 (75.0) | 2.04 (1.10-3.80) | .03 | 61/70 (87.1) | 4.42 (1.68-11.64) | .003 |
| Dennie-Morgan fold | 187/367 (51.0) | 71/177 (40.1) | 74/120 (61.7) | 2.29 (1.27-4.13) | .006 | 42/70 (60.0) | 1.90 (0.85-4.25) | .12 |
| Hertoghe sign | 179/367 (48.8) | 70/177 (39.5) | 60/120 (50.0) | 0.90 (0.52-1.58) | .72 | 49/70 (70.0) | 2.75 (1.27-5.93) | .01 |
| Facial pallor/erythema | 199/367 (54.2) | 71/177 (40.1) | 80/120 (66.7) | 1.80 (1.01-3.19) | .046 | 48/70 (68.6) | 1.56 (0.71-3.46) | .27 |
| Xerosis cutis | 335/367 (91.3) | 150/177 (84.7) | 115/120 (95.8) | 2.19 (0.73-6.58) | .16 | 70/70 (100.0) | NAb | .99 |
| Ear rhagades | 134/367 (36.5) | 42/177 (23.7) | 50/120 (41.7) | 1.60 (0.86-2.97) | .14 | 42/70 (60.0) | 2.14 (0.95-4.80) | .07 |
| Parental atopy | 240/367 (65.4) | 109/177 (61.6) | 80/120 (66.7) | 0.77 (0.50-1.19) | .25 | 51/70 (72.9) | 1.72 (0.96-3.09) | .07 |
| Alopecia areata | 24/350 (6.9) | 5/171 (2.9) | 12/111 (10.8) | 5.23 (1.53-17.88) | .008 | 7/68 (10.3) | 4.67 (1.01-21.56) | .049 |
Abbreviations: EASI, Eczema Area and Severity Index (score <7: mild [n = 177, 48.2%]; score >7 and ≤ 21: moderate [n = 120, 32.7%]; score >21: severe [n = 70, 19.1%]); NA, not applicable; OR, odds ratio.
Individual effect sizes (ORs) and 95% CIs refer to the comparison of the moderate and severe AD group with the mild AD group as reference group for the outcome. Reference categories for covariates: male sex, absence of atopic stigmata, parental atopy, or alopecia areata, respectively.
Effect size was not estimable owing to 100% positivity in severity group leading to collinearity issues.
Using the EASI score, 48.2% had mild AD (n = 177), 32.7% had moderate AD (n = 120), and 19.1% had severe AD (n = 70). The DLQI correlated significantly with severity (EASI: rs = 0.49; 95% CI, 0.41-0.57; SCORAD: rs = 0.58; 95% CI, 0.51-0.65; oSCORAD: rs = 0.52; 95% CI, 0.44-0.59; BSA rs = 0.59; 95% CI, 0.52-0.65; all P < .001). One hundred forty-two (38.9%) of all patients and greater than 50% of patients with moderate to severe AD reported a highly reduced quality of life with a DLQI greater than 11 (mild, 16.9% [n = 30]; moderate, 57.1% [n = 68]; severe, 63.8% [n = 44]).
Model Performance
Primary predictive factors for AD severity groups in both models were total serum immunoglobulin E (tIgE) level, age at AD onset, atopic stigmata, and sex (Table; eTable 3 in the Supplement). Eosinophil values, age, sports, and (former) smoking were further key factors in the MLGB; alopecia areata was a key factor in the MLR.
The MLGB resulted in an average multiclass AUC value of 0.71 (95% CI, 0.69-0.72), MLR regression of 0.58 (95% CI, 0.66-0.71). The more complex MLGB had a better predictive performance, but the more “classic” MLR came close (95% CI of AUC differences: 0.003-0.056).
Association of tIgE Levels and Eosinophil Values With AD Severity
Total serum immunoglobulin E levels and eosinophil values were important factors for predicting severity, correlated with EASI (rs = 0.43; 95% CI, 0.34-0.51 for IgE; rs = 0.24; 95% CI, 0.14-0.35 for eosinophil values [%]) and among each other (rs = 0.33; 95% CI, 0.22-0.43; all P < .001). The probability of severe AD rose strongly with tIgE levels greater than 1708 IU/mL; the probability of mild AD rose with tIgE levels less than 467 IU/mL (55 IU/mL peak probability) (Figure 1). The MLR quantified flat tIgE effects with OR of 1.16 (95% CI, 1.05-1.30) for moderate AD (P = .004) and 1.31 (95% CI, 1.16-1.46) for severe AD (P < .001) for each step of 1000 IU/mL.
Figure 1. Total Serum IgE (tIgE) and Eosinophil Values as Predictive Parameters for Atopic Dermatitis (AD) Severity.

A, The tIgE level correlates with AD severity (Eczema Area and Severity Index [EASI]). Orange dots: patients with increased tIgE levels (75.1% of patients, n = 263; age-dependent cutoff points, in patients older than 15 y: 100 kU/L, patients 12 to 15 years: 200 kU/L). Blue dots: patients with normal tIgE levels (24.9% of patients, n = 87). rs = Spearman rank correlation coefficient. B, Higher tIgE levels in patients with severe AD (EASI >21, n = 68) compared with moderate AD (EASI >7 and ≤ 21, n = 114) or mild AD (EASI <7, n = 168). C-E, The estimated probability of severe AD increased from tIgE greater than 1708 IU/mL, while the probability of mild AD decreased from tIgE less than 467 IU/mL. F-H, Patients with less than 3.79% eosinophils had a high probability of mild AD. The probability of moderate AD rose from 3.7% on, while patients with greater than 6.8% eosinophils had a rising probability of severe AD (reference range eosinophils: 0.5%-5.5%). C-H, Accumulated local effect plots of the tIgE levels visualize the expected change in probability for the grouping into mild, moderate, or severe AD dependent on tIgE levels (C-E) and eosinophil values (D-H) compared with the average prediction in the complete data set.
A total of 263 patients (75.1%) exhibited increased tIgE levels, and 80 patients (23.0%) exhibited eosinophilia (eTable 2 in the Supplement). Patients with greater than 3.7% eosinophils had an increasing probability of moderate AD, with greater than 6.8% eosinophils associated with severe AD and with less than 3.8% (peak, 1.5%) associated with mild AD (Figure 1D).
Association of Age at Onset With Severity of AD
A total of 78 patients (21%) of the cohort had an adult onset of AD, 266 had childhood onset (73%), and 22 had adolescent onset (age ≥12 years and <18 years, 6%). Atopic dermatitis severity differed between different ages at AD onset without a linear association (Figure 2). Patients with childhood onset (peak, age 7 years) had an increased probability of mild AD. Conversely, the probability of severe AD rose strongly in cases of AD onset between age 12 and 30 years with a severity peak in mid-adulthood at age 30 years, then slightly decreased, but was still elevated beyond age 30 years with a second lower peak probability at age 60 years. Mid-adulthood and late adulthood beyond age 33 years was associated with increased probability for both moderate or severe AD. In the MLR, age at AD onset was associated with moderate (OR, 1.03; 95% CI, 1.01-1.04; P = .002) and severe AD (OR, 1.04; 95% CI, 1.02-1.06 per year; P < .001). However, the trend was very flat, and the boosting model appeared to enable better description of fluctuations than the LR model, especially with early age at onset and moderate AD.
Figure 2. Association of Atopic Dermatitis (AD) Severity With Age at AD Onset.

A, AD severity in patients stratified by age at AD onset. Boxplots visualize the Eczema Area and Severity Index (EASI) of patients with AD stratified by age at disease onset. Boxes display the 25th to 75th percentile (inner horizontal line: median) of the EASI scores; whiskers: minimum, maximum (excluding outliers). B, Childhood onset was associated with increased probability of mild AD; age at AD onset older than 12 years, with severe AD; and adulthood onset at older than 33 years, with moderate to severe AD. Accumulated local effect plots visualize the expected change in probability of grouping into mild, moderate, or severe AD dependent on age at onset of AD compared with the mean prediction in the complete data set.
Patients aged 22 to 51 years had the highest probability of mild AD (peak, age 26 years) (eFigure 1 in the Supplement). Younger patients (age ≥12 and <19 years) had a higher probability of moderate to severe AD. Age older than 52 years was associated with increased probability of severe AD (peak, 64 years); age older than 65 years was associated with moderate or severe AD.
Association of Atopic Stigmata With the Phenotype of Moderate to Severe AD
The so-called atopic stigmata are phenotypic traits that occur more frequently in patients with AD compared with the general population. Several atopic stigmata were associated with an increased probability for moderate to severe AD, and patients with stigmata had higher severity scores compared with patients without stigmata. In the MLR model, cheilitis sicca (OR, 8.10; 95% CI, 3.35-19.59), nipple eczema (OR, 4.97; 95% CI, 1.56-15,78), and thinning of the lateral eyebrow (Hertoghe sign) (OR, 2.75; 95% CI, 1.27-5.93) were associated with increased probability of severe AD; white dermographism was associated with moderate and severe AD (moderate: OR, 2.29; 95% CI, 1.27-4.13; severe: OR, 4.42; 95% CI, 1.68-11.64); and Dennie-Morgan fold (OR, 2.29; 95% CI, 1.27-4.13) and facial pallor/erythema (OR, 1.80; 95% CI, 1.01-3.19) were associated with moderate AD (Figure 3, Table; eFigure 2 and eTable 3 in the Supplement).
Figure 3. Association of Atopic Dermatitis (AD) Severity With Atopic Stigmata.

Higher severity scores and probability of moderate to severe AD in patients displaying atopic stigmata. Boxplots (leftmost graphs) visualize the Eczema Area and Severity Index (EASI) of patients with AD stratified by atopic stigmata. Boxes display the 25th to 75th percentile (inner horizontal line: median) of the respective EASI scores; whiskers: minimum, maximum (excluding outliers). Accumulated local effect plots (other graphs) visualize the expected change in probability of grouping into mild (EASI ≤7), moderate (EASI >7 and ≤21), or severe (EASI >21) AD dependent on respective atopic stigma compared with the mean prediction in the complete data set.
Association of Sex With AD Severity
Female sex was associated with reduced probability of moderate (OR, 0.47; 95% CI, 0.26-0.84) and severe AD (OR, 0.30; 95% CI, 0.13-0.66) (Table). Male patients showed higher severity scores and tIgE levels compared with female patients (Figure 4A-C). Reported quality of life was not found to differ between male and female patients.
Figure 4. Association of Atopic Dermatitis (AD) Severity With Sex and Sports Frequency.
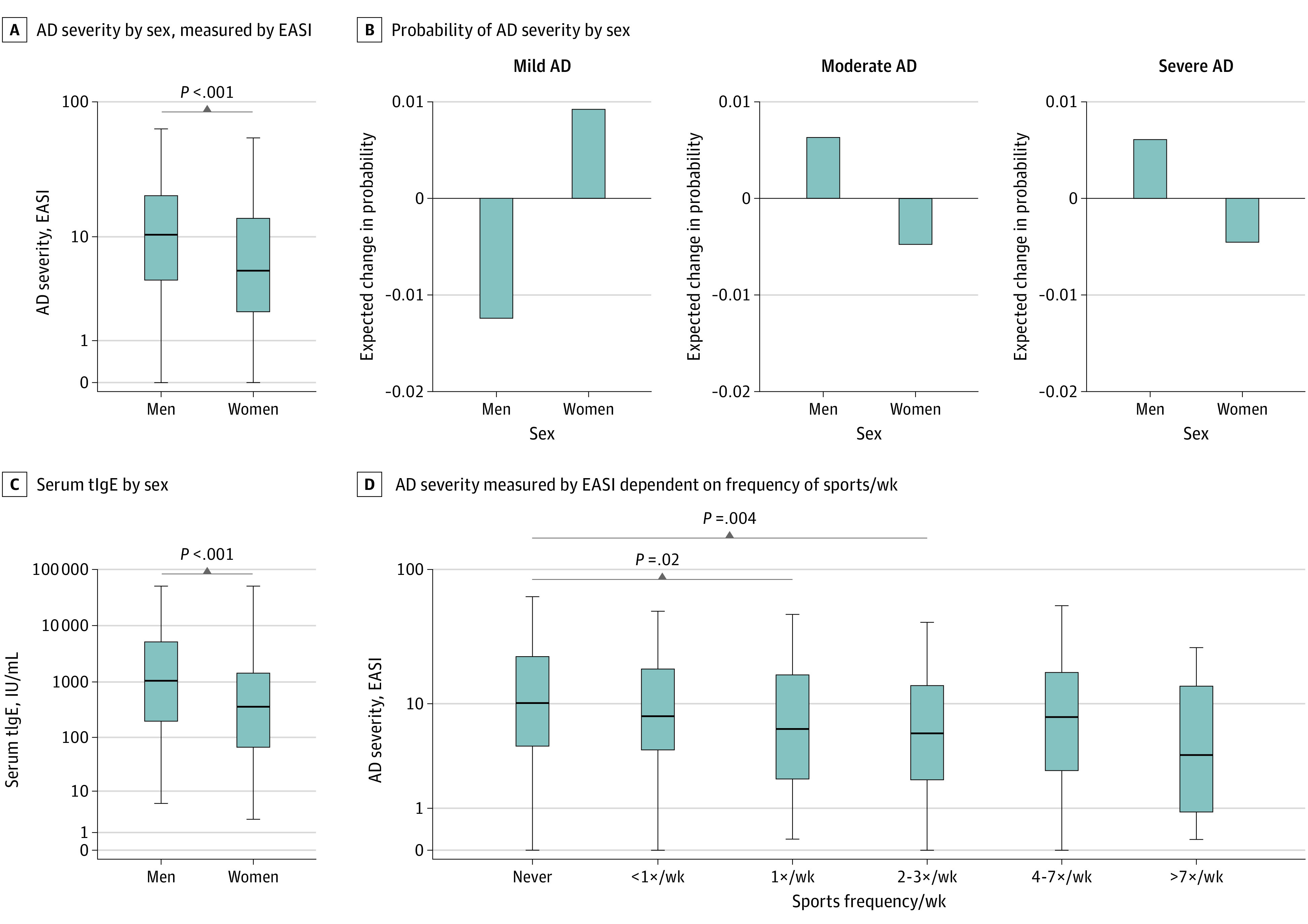
A, Male patients (n = 157 [42.8%]) had higher severity scores compared with female patients (n = 210 [57.2%]), measured by Eczema Area and Severity Index (EASI). B, Male patients had a lower estimated probability of mild AD (male, 37.6% vs female, 56.2%) and an increased probability of moderate AD (male, 37.6% vs female, 29.0%) or severe AD (male, 24.8% vs female, 14.8%). Accumulated local effect plots visualize the expected change in probability for the grouping into mild, moderate, or severe AD dependent on sex compared with the average prediction in the complete data set. C, Male patients had higher total serum immunoglobulin E (tIgE) levels compared with female patients. D, AD severity measured by EASI dependent on frequency of sports per week. Never sport: n = 68, less than once per week: n = 58, once per week: n = 68, 2 to 3 times per week: n = 107, 4 to 7 times per week: n = 60, more than 7 times per week: n = 4. EASI scores (A, D) and tIgE levels (C) are depicted in boxplots. Boxes display the 25th to 75th percentile (inner horizontal line: median) of EASI scores (A, D) and tIgE (C); whiskers: respective minimum, maximum (excluding outliers).
Lifestyle Factors and Comorbidities
Regarding lifestyle factors, smokers (daily and former) had a higher probability of moderate and severe AD. Never smokers had a higher probability of mild AD and exhibited lower EASI scores compared with daily smokers (median [IQR]: 6.7 [2.4-15.7] vs 11.7 [4.0-11.4]; P = .04). Note, however, that pack-years were not recorded in the study.
Doing sports less than once per week was associated with increased probability of severe AD, while sports 1 to 3 times per week was associated with slightly increased probability of mild AD. Yet effect sizes were modest (Figure 4D; eTables 2 and 3 in the Supplement). Body mass index (calculated as weight in kilograms divided by height in meters squared) correlated with age (rs = 0.24; 95% CI, 0.14-0.33), very weakly also with tIgE level (rs = 0.16; 95% CI, 0.06-0.26) and severity (EASI rs = 0.15; 95% CI, 0.06-0.25). However, most patients with AD had normal weight (eTable 2 in the Supplement). A subgroup of adult patients with AD with cardiovascular disease (CVD) (n = 56) exhibited significantly higher body mass index (mean [SD], 27.8 [6.7] vs 25.1 [6.2]; P = .001), EASI (mean [SD], 14.7 [14.3] vs 11.2 [11.4]; P = .03) and tIgE levels (mean [SD], 5136 [10 352] vs 2617 [5655] IU/mL; P = .03) compared with AD without CVD (n = 311), but they were also older (mean [SD] age, 58.9 [15.2] vs 37.3 [15.2] years; P < .001). Regarding other nonatopic comorbidities, alopecia areata was associated with moderate (OR, 5.23; 95% CI, 1.53-17.88) and severe (OR, 4.67; 95% CI, 1.01-21.56) AD.
Discussion
Atopic dermatitis is a multifactorial disease, and identification of individual risk factors still ongoing. Current advances in precision medicine emphasize the need for stratification of the highly heterogeneous phenotype. Through deep phenotyping with stratification by AD severity, we detected concrete ranges of age (and of age at AD onset), tIgE levels, eosinophil values, and atopic stigmata that might contribute to disease understanding, estimation of severity prognosis, and improved identification of suitable patients for personalized prevention and therapies at the right time point.
Male patients 12 years and older but younger than 21 years or older than 52 years, disease onset beyond 12 years, tIgE levels greater than 1708 IU/mL, eosinophil values greater than 6.8%, multiple atopic stigmata (cheilitis sicca, white dermographism, Hertoghe sign), history of (former) smoking and sports less than once per week represented the main risk candidates for severe AD in our cohort.
New key findings of our study include the detection of critical age frames. Age at AD onset older than 12 years was associated with increased probability of severe AD; onset in mid-adulthood and late adulthood beyond 33 years was associated with moderate or severe AD. Conversely, disease onset in childhood or age at time of inclusion older than 22 or younger than 51 years was associated with mild AD. This points toward different pathophysiological immunological mechanisms in childhood, adolescence, and mid-adulthood and late adulthood, potentially triggered by psychosocial factors and critical life events. However, 94% of our cohort were adults, limiting conclusions regarding adolescents.
While early birth-cohort studies have suggested a clearance of AD in more than 50% of affected children, there is growing evidence for AD as a lifelong disease with variable phenotypic expression, high rate of adult onset or relapsing AD after long asymptomatic intervals with different influencing factors depending on age (at onset), race and ethnicity, residence, and other criteria.1,9,10,11,12,13,35,36,37,38
Studies reporting clinical course together with age at AD onset in adolescents and adults are scarce.39 No significant differences in AD severity were found in a US cohort between age at AD onset younger than 18 years or 18 years and older.40 Interestingly, 42% of patients with moderate to severe AD in adulthood reported a worsening of AD by or after age 12 years in the time period from age 12 to 19 years.39 Our data suggest adolescence and mid-adulthood as critical time frames for the onset of AD with severe disease, while childhood onset was associated with a milder course.
In childhood, boys were reported to have a higher prevalence of allergic rhinitis and asthma41,42 than girls, but not of AD.41 In most studies, sex-balanced AD prevalence shifts to female predominance in adulthood.12,41 Pediatric studies have reported higher likelihood of girls for mild intermittent AD43; others have linked male sex to better AD control37 and to an early-onset, early-resolving course.9 There is evidence for suppression of type 2 response by testosterone and enhancement by estrogen and progesterone.44 Yet IgE levels generally remain higher or comparable in men compared with women after puberty.45,46,47 Higher severity scores and tIgE levels have been described in male patients with AD aged 12 to 89 years,7 according to our findings, indicating a more severe disease at least in adolescent and adult men with active AD. This might be a bystander phenomenon of the higher tIgE levels found in male individuals. Yet male individuals with mild disease might be less likely to participate in epidemiological studies compared with female individuals, causing a selection bias. Furthermore, the association of male sex with severity may not be generalized to children owing to an underrepresentation of the early-onset, early-resolving male course in our study collective with age 12 years and older and excluding patients in remission.
Levels of tIgE and eosinophil values are key mediators for allergic sensitization and inflammation with high evidence for severity correlation in AD.48,49,50 Thus, they were expected predictive factors for severity, but we detected new scalable ranges. High tIgE levels greater than 1708 IU/mL and eosinophil values greater than 6.8% were associated with exponential rising probability of severe AD; lower tIgE levels (peak probability, 55 IU/mL) and eosinophil values less than 3.7% (peak, 1.5%) were associated with mild AD.
Active smoking and passive smoke exposure have been associated with an increased prevalence of AD.51 Active smoking has also been associated with adult onset of AD2 and self-reported severe AD.52 We could confirm this association in physician-assessed AD severity. Potential causes are biological detrimental effects of smoke and reactive oxygen species on the immune system53 and skin barrier51,54,55 and/or worse health behavior owing to higher psychological burden6 in severe AD.
Atopic dermatitis has been associated with less physical activity in US56 but not in Swedish57 adults. We found an association of severe AD with sports less than once per week and mild AD with sports 1 to 3 times per week. Sport-avoidance in severe AD might be caused by increased pruritus6 or even exacerbations58 sweating from activity,6,59 localization of eczema,56 and indirect effects of comorbid fatigue, sleep disturbances, and depression.6,56 Interestingly, moderate-intensity aerobic exercise attenuated dermatitis and allergic inflammation in a mouse model for eczema.60
Other known risk factors for AD are a positive family history for atopic diseases (especially AD), living in an urban setting and in regions with low UV light exposure or dry climatic conditions, a “Westernized” diet (high in sugars and polyunsaturated fatty acids), and repeated exposure to antibiotics before age 5 years.1,4,6,11,14,61 Studies vary regarding the effects of cesarean delivery, breastfeeding, maternal tobacco exposure, childhood vaccinations, bacterial or viral infections, air pollutants, farm environment, pets, sex, family size, household education level, and association with atopic and nonatopic comorbidities such as CVD, obesity, metabolic diseases, inflammatory bowel disease, rheumatoid arthritis, and psychiatric diseases.1,4,9,11,35,36,37,61,62,63 The variation of reported effects dependent on the study design and readout stress the need for stratification of AD.1,2
Strengths and Limitations
Strengths of our study include a well-characterized cohort covering the whole spectrum of AD severity, based on dermatologist-assessed validated severity scores, assessment of multiple clinical and epidemiological characteristics, and a wide age range from early adolescence until late adulthood. Limitations include a recall bias in self-reported age at onset, particularly in older persons; only 6% adolescents in our cohort; and a potential selection bias in a specialized dermatologic setting, which may limit overall generalizability. Differentiation between pediatric and adult cohorts and stratification by AD severity, onset or persistence, and survey-based vs clinician-assessed is crucial for the interpretation of our data in the context of the literature. In contrast to other studies, such as birth-cohort studies investigating onset and persistence of AD compared with participants without AD, we did not include patients in remission (hereby also outgrown/early-resolving courses). Here, we aimed to evaluate the association of several variables with AD severity within the broad spectrum of already-existing and active AD in adolescent and adult patients to identify at-risk patients for further monitoring or therapy.
With this readout, our data further corroborate an association of maternal asthma, current and former smoking, and viral infections (herpes simplex virus, eczema herpeticum)1,2,64 with severe AD (eTable 2 in the Supplement), although these variables only had a modest effect size on our model compared with stronger effects of tIgE levels, eosinophil values, age (at onset), or atopic stigmata. We did not observe clear effects of family size, household education level, specific diet, cesarean delivery, contact with farm animals or pets, or urban vs rural living on AD severity in our study population. Although the number of residents showed a weak negative correlation with EASI, there was no clear (linear) effect on AD severity, suggesting a cluster effect.
Alopecia areata was associated with AD severity, confirming recent other reports.65,66,67 Regarding other nonatopic comorbidities, CVD was very weakly associated with AD severity, but not others, such as chronic inflammatory bowel disease, diabetes mellitus, rheumatoid arthritis, multiple sclerosis, or malignant neoplasms. Despite modest effect size, this is of interest because of the current discussion of AD as a systemic disease (CVD), effect of dupilumab treatment for alopecia areata,66,67 and of JAK inhibitors being in clinical trials not only for AD but also for alopecia areata as promising new indication with some shared pathophysiological mechanisms.1,67,68
A phenotype with several atopic stigmata was associated with an increased probability for moderate to severe AD, and patients with stigmata had significantly higher severity scores compared with patients without stigmata. These data complement other studies showing the association of selected atopic stigmata with AD persistence4 or childhood vs adult onset of AD.11
Conclusions
A better characterization of the phenotype might help to identify patients at risk for severe disease and facilitate early therapeutic intervention and prevention. Sports and avoidance of smoking are simple self-dependent preventive lifestyle factors. Moreover, we could identify concrete critical time frames regarding age and age at onset, cutoff points for tIgE levels and eosinophil values as predictive biomarkers, and several atopic stigmata associated with disease severity in this study. Limitations of sex and a single atopic stigma as isolated parameters are the low specificity and sensitivity. However, the overall phenotype with combination of several traits, especially with the ascertained ranges for age, age at disease onset, tIgE levels, and eosinophil values might facilitate estimation of severity prognosis. This is a highly relevant question for individual patients (and parents) and frequently asked in consultations. Thus, our findings might contribute to sensitization of physicians for predisposed patients and help shared decision-making regarding frequency of follow-up visits or initiation of further diagnostics or (systemic) therapies with simple and economic predictors.
Yet, while ranges of tIgE levels and age (at onset) were conclusive regarding their predictive value for mild or severe AD, probabilities of moderate AD showed more fluctuations and less clear cutoff points. These data suggest the wide range of moderate AD defined by EASI greater than 7 and less than 21 as a black box with multiple subgroups. A reevaluation of these threshold points might help to further elucidate this picture and allow better fine-tuning of subgroups. Further stratification of the heterogeneous phenotypes by several criteria is needed for better identification of critical life periods, biomarkers, and of the right patient for personalized therapeutic and preventive measures of (severe) AD.
eMethods. Statistical analysis
eTable 1. Variables included in the gradient boosting model for prediction of atopic dermatitis severity grades measured by Eczema Area and Severity Index
eTable 2. Importance and prevalence of clinical characteristics of patients with atopic dermatitis stratified by disease severity groups
eTable 3. Summary of major severity-associated factors in adolescent and adult patients with atopic dermatitis from the machine-learning gradient boosting model considering biological and epidemiolocal plausibility and clinical relevance for translation in daily practice
eFigure 1. Middle-aged patients have an increased probability of mild AD, younger and older patients of moderate-to-severe AD
eFigure 2. Atopic stigmata mark the phenotype of moderate-to-severe AD: ear rhagades, perleche, Dennie-Morgan-Fold, dirty neck
eReferences
References
- 1.Weidinger S, Beck LA, Bieber T, Kabashima K, Irvine AD. Atopic dermatitis. Nat Rev Dis Primers. 2018;4(1):1. doi: 10.1038/s41572-018-0001-z [DOI] [PubMed] [Google Scholar]
- 2.Abuabara K, Ye M, McCulloch CE, et al. Clinical onset of atopic eczema: results from 2 nationally representative British birth cohorts followed through midlife. J Allergy Clin Immunol. 2019;144(3):710-719. doi: 10.1016/j.jaci.2019.05.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Czarnowicki T, He H, Krueger JG, Guttman-Yassky E. Atopic dermatitis endotypes and implications for targeted therapeutics. J Allergy Clin Immunol. 2019;143(1):1-11. doi: 10.1016/j.jaci.2018.10.032 [DOI] [PubMed] [Google Scholar]
- 4.Thorsteinsdottir S, Stokholm J, Thyssen JP, et al. Genetic, clinical, and environmental factors associated with persistent atopic dermatitis in childhood. JAMA Dermatol. 2019;155(1):50-57. doi: 10.1001/jamadermatol.2018.4061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Reiger M, Traidl-Hoffmann C, Neumann AU. The skin microbiome as a clinical biomarker in atopic eczema: promises, navigation, and pitfalls. J Allergy Clin Immunol. 2020;145(1):93-96. doi: 10.1016/j.jaci.2019.11.004 [DOI] [PubMed] [Google Scholar]
- 6.Ständer S. Atopic dermatitis. N Engl J Med. 2021;384(12):1136-1143. doi: 10.1056/NEJMra2023911 [DOI] [PubMed] [Google Scholar]
- 7.Garmhausen D, Hagemann T, Bieber T, et al. Characterization of different courses of atopic dermatitis in adolescent and adult patients. Allergy. 2013;68(4):498-506. doi: 10.1111/all.12112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Roduit C, Frei R, Depner M, et al. ; the PASTURE study group . Phenotypes of atopic dermatitis depending on the timing of onset and progression in childhood. JAMA Pediatr. 2017;171(7):655-662. doi: 10.1001/jamapediatrics.2017.0556 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Paternoster L, Savenije OEM, Heron J, et al. Identification of atopic dermatitis subgroups in children from 2 longitudinal birth cohorts. J Allergy Clin Immunol. 2018;141(3):964-971. doi: 10.1016/j.jaci.2017.09.044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Silverberg JI. Adult-onset atopic dermatitis. J Allergy Clin Immunol Pract. 2019;7(1):28-33. doi: 10.1016/j.jaip.2018.09.029 [DOI] [PubMed] [Google Scholar]
- 11.Lee HH, Patel KR, Singam V, Rastogi S, Silverberg JI. A systematic review and meta-analysis of the prevalence and phenotype of adult-onset atopic dermatitis. J Am Acad Dermatol. 2019;80(6):1526-1532.e7. doi: 10.1016/j.jaad.2018.05.1241 [DOI] [PubMed] [Google Scholar]
- 12.Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284-1293. doi: 10.1111/all.13401 [DOI] [PubMed] [Google Scholar]
- 13.Kim JP, Chao LX, Simpson EL, Silverberg JI. Persistence of atopic dermatitis (AD): a systematic review and meta-analysis. J Am Acad Dermatol. 2016;75(4):681-687.e11. doi: 10.1016/j.jaad.2016.05.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Abuabara K, Yu AM, Okhovat J-P, Allen IE, Langan SM. The prevalence of atopic dermatitis beyond childhood: a systematic review and meta-analysis of longitudinal studies. Allergy. 2018;73(3):696-704. doi: 10.1111/all.13320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pathak J, Kho AN, Denny JC. Electronic health records-driven phenotyping: challenges, recent advances, and perspectives. J Am Med Inform Assoc. 2013;20(e2):e206-e211. doi: 10.1136/amiajnl-2013-002428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Weng C, Shah NH, Hripcsak G. Deep phenotyping: embracing complexity and temporality—towards scalability, portability, and interoperability. J Biomed Inform. 2020;105:103433. doi: 10.1016/j.jbi.2020.103433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Robinson PN. Deep phenotyping for precision medicine. Hum Mutat. 2012;33(5):777-780. doi: 10.1002/humu.22080 [DOI] [PubMed] [Google Scholar]
- 18.Bieber T, Traidl-Hoffmann C, Schäppi G, Lauener R, Akdis C, Schmid-Grendlmeier P. Unraveling the Complexity of Atopic Dermatitis: The CK-CARE Approach Toward Precision Medicine. Wiley; 2020. [DOI] [PubMed] [Google Scholar]
- 19.Silverberg JI, Gelfand JM, Margolis DJ, et al. Severity strata for POEM, PO-SCORAD, and DLQI in US adults with atopic dermatitis. Ann Allergy Asthma Immunol. 2018;121(4):464-468.e3. doi: 10.1016/j.anai.2018.07.004 [DOI] [PubMed] [Google Scholar]
- 20.Leshem YA, Hajar T, Hanifin JM, Simpson EL. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol. 2015;172(5):1353-1357. doi: 10.1111/bjd.13662 [DOI] [PubMed] [Google Scholar]
- 21.Kunz B, Oranje AP, Labrèze L, Stalder JF, Ring J, Taïeb A. Clinical validation and guidelines for the SCORAD index: consensus report of the European Task Force on Atopic Dermatitis. Dermatology. 1997;195(1):10-19. doi: 10.1159/000245677 [DOI] [PubMed] [Google Scholar]
- 22.Wollenberg A, Oranje A, Deleuran M, et al. ; European Task Force on Atopic Dermatitis/EADV Eczema Task Force . ETFAD/EADV eczema task force 2015 position paper on diagnosis and treatment of atopic dermatitis in adult and paediatric patients. J Eur Acad Dermatol Venereol. 2016;30(5):729-747. doi: 10.1111/jdv.13599 [DOI] [PubMed] [Google Scholar]
- 23.Kuhn M, Johnson K. Applied Predictive Modelling. Springer Science+Business Media; 2013. doi: 10.1007/978-1-4614-6849-3 [DOI] [Google Scholar]
- 24.Friedman JH. Greedy function approximation: a gradient boosting machine. Ann Stat. 2001;29(5):1189-1232. doi: 10.1214/aos/1013203451 [DOI] [Google Scholar]
- 25.Hurvich CM, Tsai CL. Model selection for extended quasi-likelihood models in small samples. Biometrics. 1995;51(3):1077-1084. doi: 10.2307/2533006 [DOI] [PubMed] [Google Scholar]
- 26.Fisher A, Rudin C, Dominici F. All models are wrong, but many are useful: learning a variable’s importance by studying an entire class of prediction models simultaneously. J Mach Learn Res. 2019;20(20):1-81. [PMC free article] [PubMed] [Google Scholar]
- 27.Apley DW, Zhu J. Visualizing the effects of predictor variables in black box supervised learning models. Cornell University Library. August 19, 2019. Accessed October 4, 2021. https://arxiv.org/abs/1612.08468 doi: 10.1111/rssb.12377 [DOI]
- 28.Hand DJ, Robert JT. A simple generalisation of the area under the ROC curve for multiple class classification problems. Mach Learn. 2001;45(2):171-186. doi: 10.1023/A:1010920819831 [DOI] [Google Scholar]
- 29.R Core Team . R: A language and environment for statistical computing. Accessed October 4, 2021. https://www.R-project.org/
- 30.Chen T, He T, Benesty M, et al. xgboost: extreme gradient boosting. R package version 0.90.0.2. Accessed October 4, 2021. https://cran.r-project.org/web/packages/xgboost/index.html
- 31.Kuhn M. Classification and regression training. R package version 6.0-86. Accessed October 4, 2021. https://cran.r-project.org/web/packages/caret/index.html
- 32.Robin X, Turck N, Hainard A, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinformatics. 2011;12:77. doi: 10.1186/1471-2105-12-77 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hothorn T, Hornik K, van de Wiel MA, Zeileis A. A Lego system for conditional inference. Am Stat. 2006;60(3):257-263. doi: 10.1198/000313006X118430 [DOI] [Google Scholar]
- 34.Apley D. ALEPlot: accumulated local effects (ALE) plots and partial dependence (PD) plots. R package version 1.1. Accessed October 4, 2021. https://cran.r-project.org/web/packages/ALEPlot/index.html
- 35.Kantor R, Silverberg JI. Environmental risk factors and their role in the management of atopic dermatitis. Expert Rev Clin Immunol. 2017;13(1):15-26. doi: 10.1080/1744666X.2016.1212660 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Paller A, Jaworski JC, Simpson EL, et al. Major comorbidities of atopic dermatitis: beyond allergic disorders. Am J Clin Dermatol. 2018;19(6):821-838. doi: 10.1007/s40257-018-0383-4 [DOI] [PubMed] [Google Scholar]
- 37.Wan J, Mitra N, Hoffstad OJ, Yan AC, Margolis DJ. Longitudinal atopic dermatitis control and persistence vary with timing of disease onset in children: a cohort study. J Am Acad Dermatol. 2019;81(6):1292-1299. doi: 10.1016/j.jaad.2019.05.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nettis E, Ortoncelli M, Pellacani G, et al. A multicenter study on the prevalence of clinical patterns and clinical phenotypes in adult atopic dermatitis. J Investig Allergol Clin Immunol. 2020;30(6):448-450. doi: 10.18176/jiaci.0519 [DOI] [PubMed] [Google Scholar]
- 39.Tanaka A, Morioke S, Ohya Y, et al. Time course of disease severity from birth to 19 years old in patients with moderate to severe atopic dermatitis in adulthood. J Dermatol. 2021;48(5):e205-e206. doi: 10.1111/1346-8138.15790 [DOI] [PubMed] [Google Scholar]
- 40.Silverberg JI, Vakharia PP, Chopra R, et al. Phenotypical differences of childhood- and adult-onset atopic dermatitis. J Allergy Clin Immunol Pract. 2018;6(4):1306-1312. doi: 10.1016/j.jaip.2017.10.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lau S, Matricardi PM, Wahn U, Lee YA, Keil T. Allergy and atopy from infancy to adulthood: messages from the German birth cohort MAS. Ann Allergy Asthma Immunol. 2019;122(1):25-32. doi: 10.1016/j.anai.2018.05.012 [DOI] [PubMed] [Google Scholar]
- 42.Fröhlich M, Pinart M, Keller T, et al. Is there a sex-shift in prevalence of allergic rhinitis and comorbid asthma from childhood to adulthood? a meta-analysis. Clin Transl Allergy. 2017;7(1):44. doi: 10.1186/s13601-017-0176-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Mulick AR, Mansfield KE, Silverwood RJ, et al. Four childhood atopic dermatitis subtypes identified from trajectory and severity of disease and internally validated in a large UK birth cohort. Br J Dermatol. 2021. doi: 10.1111/bjd.19885 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Roved J, Westerdahl H, Hasselquist D. Sex differences in immune responses: hormonal effects, antagonistic selection, and evolutionary consequences. Horm Behav. 2017;88:95-105. doi: 10.1016/j.yhbeh.2016.11.017 [DOI] [PubMed] [Google Scholar]
- 45.Leffler J, Stumbles PA, Strickland DH. Immunological processes driving IgE sensitisation and disease development in males and females. Int J Mol Sci. 2018;19(6):E1554. doi: 10.3390/ijms19061554 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Rosário CS, Cardozo CA, Neto HJC, Filho NAR. Do gender and puberty influence allergic diseases? Allergol Immunopathol (Madr). 2021;49(2):122-125. doi: 10.15586/aei.v49i2.49 [DOI] [PubMed] [Google Scholar]
- 47.Vinnik T, Kreinin A, Abildinova G, Batpenova G, Kirby M, Pinhasov A. Biological sex and IgE sensitization influence severity of depression and cortisol levels in atopic dermatitis. Dermatology. 2020;236(4):336-344. doi: 10.1159/000504388 [DOI] [PubMed] [Google Scholar]
- 48.Renert-Yuval Y, Thyssen JP, Bissonnette R, et al. Biomarkers in atopic dermatitis—a review on behalf of the International Eczema Council. J Allergy Clin Immunol. 2021;147(4):1174-1190.e1. doi: 10.1016/j.jaci.2021.01.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hu Y, Liu S, Liu P, Mu Z, Zhang J. Clinical relevance of eosinophils, basophils, serum total IgE level, allergen-specific IgE, and clinical features in atopic dermatitis. J Clin Lab Anal. 2020;34(6):e23214. doi: 10.1002/jcla.23214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Mittermann I, Wikberg G, Johansson C, et al. IgE sensitization profiles differ between adult patients with severe and moderate atopic dermatitis. PLoS One. 2016;11(5):e0156077. doi: 10.1371/journal.pone.0156077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kantor R, Kim A, Thyssen JP, Silverberg JI. Association of atopic dermatitis with smoking: a systematic review and meta-analysis. J Am Acad Dermatol. 2016;75(6):1119-1125.e1. doi: 10.1016/j.jaad.2016.07.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Smirnova J, Montgomery S, Lindberg M, Svensson Å, von Kobyletzki L. Associations of self-reported atopic dermatitis with comorbid conditions in adults: a population-based cross-sectional study. BMC Dermatol. 2020;20(1):23. doi: 10.1186/s12895-020-00117-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Sopori M. Effects of cigarette smoke on the immune system. Nat Rev Immunol. 2002;2(5):372-377. doi: 10.1038/nri803 [DOI] [PubMed] [Google Scholar]
- 54.Sticozzi C, Belmonte G, Pecorelli A, et al. Correction: cigarette smoke affects keratinocytes SRB1 expression and localization via H2O2 production and HNE protein adducts formation. PLoS One. 2020;15(1):e0228663. doi: 10.1371/journal.pone.0228663 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Sticozzi C, Belmonte G, Pecorelli A, et al. Cigarette smoke affects keratinocytes SRB1 expression and localization via H2O2 production and HNE protein adducts formation. PLoS One. 2012;7(3):e33592. doi: 10.1371/journal.pone.0033592 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Silverberg JI, Song J, Pinto D, et al. Atopic dermatitis is associated with less physical activity in US adults. J Invest Dermatol. 2016;136(8):1714-1716. doi: 10.1016/j.jid.2016.04.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Lonne-Rahm S-B, Sundström I, Nordlind K, Engström L-M. Adult atopic dermatitis patients and physical exercise: a Swedish questionnaire study. Acta Derm Venereol. 2014;94(2):185-187. doi: 10.2340/00015555-1556 [DOI] [PubMed] [Google Scholar]
- 58.Williams JR, Burr ML, Williams HC. Factors influencing atopic dermatitis—a questionnaire survey of schoolchildren’s perceptions. Br J Dermatol. 2004;150(6):1154-1161. doi: 10.1111/j.1365-2133.2004.05869.x [DOI] [PubMed] [Google Scholar]
- 59.Huet F, Faffa M-S, Poizeau F, Merhand S, Misery L, Brenaut E. Characteristics of pruritus in relation to self-assessed severity of atopic dermatitis. Acta Derm Venereol. 2019;99(3):279-283. doi: 10.2340/00015555-3053 [DOI] [PubMed] [Google Scholar]
- 60.Son WK, Yoon W, Kim S, et al. Can moderate-intensity aerobic exercise ameliorate atopic dermatitis? Exp Dermatol. 2020;29(8):699-702. doi: 10.1111/exd.14138 [DOI] [PubMed] [Google Scholar]
- 61.Flohr C, Mann J. New insights into the epidemiology of childhood atopic dermatitis. Allergy. 2014;69(1):3-16. doi: 10.1111/all.12270 [DOI] [PubMed] [Google Scholar]
- 62.Papathoma E, Triga M, Fouzas S, Dimitriou G. Cesarean section delivery and development of food allergy and atopic dermatitis in early childhood. Pediatr Allergy Immunol. 2016;27(4):419-424. doi: 10.1111/pai.12552 [DOI] [PubMed] [Google Scholar]
- 63.Ascott A, Mulick A, Yu AM, et al. Atopic eczema and major cardiovascular outcomes: a systematic review and meta-analysis of population-based studies. J Allergy Clin Immunol. 2019;143(5):1821-1829. doi: 10.1016/j.jaci.2018.11.030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Ascott A, Yu AM, Schmidt M, Abuabara K, Smeeth L, Langan SM. Association between eczema and major cardiovascular outcomes in population-based studies: a systematic review protocol. BMJ Open. 2017;7(9):e017979. doi: 10.1136/bmjopen-2017-017979 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Egeberg A, Anderson S, Edson-Heredia E, Burge R. Comorbidities of alopecia areata: a population-based cohort study. Clin Exp Dermatol. 2021;46(4):651-656. doi: 10.1111/ced.14507 [DOI] [PubMed] [Google Scholar]
- 66.Alniemi DT, McGevna L. Dupilumab treatment for atopic dermatitis leading to unexpected treatment for alopecia universalis. JAAD Case Rep. 2019;5(2):111-112. doi: 10.1016/j.jdcr.2018.11.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Kageyama R, Ito T, Hanai S, et al. Immunological properties of atopic dermatitis-associated alopecia areata. Int J Mol Sci. 2021;22(5):2618. doi: 10.3390/ijms22052618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Malik K, Guttman-Yassky E. Cytokine targeted therapeutics for alopecia areata: lessons from atopic dermatitis and other inflammatory skin diseases. J Investig Dermatol Symp Proc. 2018;19(1):S62-S64. doi: 10.1016/j.jisp.2017.10.005 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods. Statistical analysis
eTable 1. Variables included in the gradient boosting model for prediction of atopic dermatitis severity grades measured by Eczema Area and Severity Index
eTable 2. Importance and prevalence of clinical characteristics of patients with atopic dermatitis stratified by disease severity groups
eTable 3. Summary of major severity-associated factors in adolescent and adult patients with atopic dermatitis from the machine-learning gradient boosting model considering biological and epidemiolocal plausibility and clinical relevance for translation in daily practice
eFigure 1. Middle-aged patients have an increased probability of mild AD, younger and older patients of moderate-to-severe AD
eFigure 2. Atopic stigmata mark the phenotype of moderate-to-severe AD: ear rhagades, perleche, Dennie-Morgan-Fold, dirty neck
eReferences