

Abstract
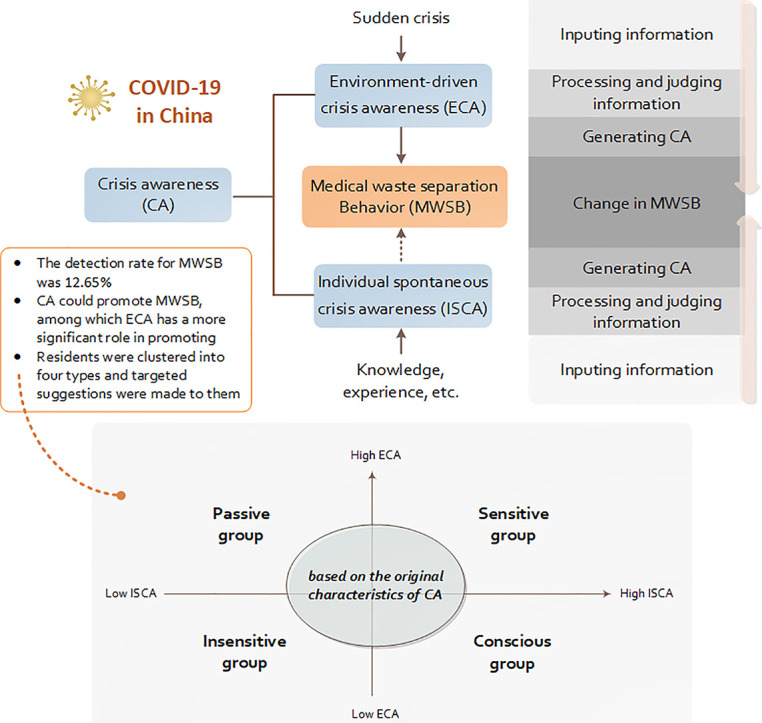
Specific awareness is an important factor that affects individual behavioral decisions. This study explored the relationship between crisis awareness and medical waste separation behavior shown by urban residents during the COVID-19 epidemic in China. The results of a questionnaire survey data (N = 668) were subjected to statistical analyses, regression analyses, and cross-analyses. In terms of medical waste separation, the detection rate was 12.65%, among which, the waste separation behavior by citizens was the highest (24.56%). In terms of the relationship between crisis awareness and medical waste separation behavior, the crisis awareness generated by the environmental situation is significantly related to individuals' participation in the separation of medical waste. In particular, individual spontaneous crisis awareness only had a significant positive correlation with the waste separation behavior for the decision factor. The residents were clustered into “sensitive“, “conscious”, “passive”, and “insensitive” types based on the original crisis awareness characteristics. The “sensitive” group was more actively involved in the separation of medical waste, while the “insensitive” group showed the worst performance for the separation of medical waste. A comparison of the separation behaviors shown by the “conscious” group and the “passive” group confirmed that environment-driven crisis awareness has a higher correlation with the separation of medical waste by residents.
Keywords: Crisis awareness, Medical waste separation behavior, Correlation
Graphical abstract
1. Introduction
According to the National Annual Report on the Prevention and Control of Environmental Pollution by Solid Waste in Large and Medium-sized Cities in 2019 (MEERPC, 2019) issued by the Ministry of Ecology and Environment of China, the amount of urban medical waste increased between 2014 and 2018 by 67.1% per year. Furthermore, the COVID-19 epidemic is expected to substantially increase the output of medical waste in 2020 (Chang et al., 2020). Improper or incomplete treatment of medical waste will not only cause harm to the environment and human health but may even become a source of the epidemic (Dzekashu et al., 2017). Therefore, the disposal of medical waste has attracted the attention of a large number of researchers (Muduli and Barve, 2012; Barnett-Itzhaki et al., 2016; Nie, 2018). The effectiveness of source classification determines the difficulty associated with medical waste collection, transportation, and treatment, and is of great significance when attempting to strengthen the safe and harmless treatment of medical waste (Geller et al., 1982). How to guide separation behavior by residents and strengthen the management of medical waste separation have become an important and urgent issue for government and society.
It is thought that awareness has an important influence on individual behavior and decision making (Bargh, 2002, Casali et al., 2013), and this is also true in the field of environmental behavior (Krause, 1993). Kautish et al. (2019) conducted empirical research on Indian consumers and the results showed that individual environmental awareness significantly affected their environmental behavior. Shimoda et al. (2020) suggested that health awareness was a predictor of environmental and health behavior. Low carbon mental awareness is thought to be the main psychological attribution that promotes low-carbon consumption behavior and that internal and external contextual factors play a moderating role in the relationship between the two (Wang and Wang, 2011). Investigations about different kinds of waste separation and recycling have been conducted (e.g. Evison and Read, 2001; Chalak et al., 2016; Vassanadumrongdee and Kittipongvises, 2018; Chen et al., 2019; Papaoikonomou et al., 2020). According to these studies, awareness on a direct or indirect way, is an important factor in enhancing waste management.
In the field of modern psychology, awareness is defined as the “individual's consciousness of external stimuli and their own feelings, experiences, and thoughts” (Block, 2007). The perception of external stimuli by an individual and their awareness of original memory and thinking are different forms of awareness. Crisis awareness is a specific type of awareness and it may be manifested as awareness during emergencies. It involves risk perception, and is partly based on individual memory and knowledge experience. Crisis awareness has a significant influence on individual behavior and decision making, especially environmental protection behaviors (Keshavarz and Karami, 2016; Maleksaeidi and Keshavarz, 2019). For example, Kim et al. (2013) suggested that individual participation in environmental protection behavior is significantly affected by risk perception, including the perception of the severity of climate change-related consequences and the response effect of perception. Also, the crisis awareness generated by individual factors, such as information memory, knowledge, and experience, has been shown to have a direct impact on individual energy-saving behavior (Abrahamse et al., 2007) and green purchase behavior (Geppert and Stamminger, 2010). Previous studies on the relationship between crisis awareness and behavior have shown that individual implementation costs, social reference norms, and other contextual factors affect the transmission path for crisis awareness behavioral decisions (Cialdini et al., 1990).
In summary, crisis awareness arises from the perception of risk by an individual and their awareness of memory, knowledge, and experience. It has been shown to have an important influence on the implementation of individual behavior (Fig. 1 ). The COVID-19 epidemic provides an important context for studying the relationship between crisis awareness by residents and medical waste separation behavior. Therefore, this study investigated the correlation of the crisis awareness mechanism on medical waste separation behavior shown by urban residents during the COVID-19 epidemic.
Fig. 1.

Analysis of the relationship between crisis awareness and medical waste separation behavior.
2. Materials and methods
2.1. Literature review
2.1.1. Crisis awareness
Crisis awareness was defined in this study as “the combination of an individual's perception of risk and awareness of their own feelings, experiences and thoughts”. Crisis awareness based on personal feelings, experiences, and thoughts is not necessarily related to the occurrence of risks. That is to say, it is the awareness that an individual has without external stimulation. Risk perception is formed through comprehensive judgments of various types of information (Schwing and Albers, 1982) and is concentrated in the cognitive and psychological responses to threatening situations (Setbon et al., 2005). Kasperson et al. (2003) put forward the theory of risk amplification and suggested that risk perception arose from the interaction between disaster events, and psychology, society, institutions, and culture. Based on the above research, risk perception is summarized in this study as the “psychological feelings and cognitive behaviors toward emergencies shown by people”.
Research on crisis awareness is typically concentrated on public administration and corporate management. Risk perception arises in two main ways. One is that public acceptance and understanding of disasters play a major role in risk perception (Covello and Merkhofer, 1993; Huang et al., 2013). Also, media reports change personal perceptions of crises. For example, the number of media reports usually determines the perception of crises by a person (Wei et al., 2012). The development of the internet has magnified the level of public risk perception and behavior (Skarlatidou et al., 2012). Related theories, such as resource dependence (Blau, 1964; Emerson, 1962), are used in the organization and management process. Previous studies have suggested that awareness of a crisis shown by company senior management depends on whether the key resources needed by the company are in the hands of other companies (Pfeffer and Salancik, 1978). On this basis, Wu et al. (2012) found that the crisis awareness shown by enterprise managers is mainly affected by the redundant resources of the enterprise.
Existing research conclusions suggested that crisis awareness mainly referred to individual perception of risk and the feelings, memory, and thinking shown by people. It could be affected by the public acceptance and understanding of disasters, the number of media reports, the development of the internet, and the key resource owners, redundant enterprise resources, and other factors available within an enterprise.
2.1.2. Medical waste separation
In general, waste is any substance that has no direct use and is permanently discarded (Shareefdeen, 2012). According to the Regulations on the Management of Medical Waste, issued by the State Council of the People's Republic of China (SCRPC, 2003), medical waste refers to toxic or indirectly toxic, infectious, and other hazardous waste generated by medical and health institutions due to medical treatments, health care, prevention, and related medical activities. Medical waste is one of the types of waste that needs special treatment because it poses potentially high risks to human health and the environment. Some lower-middle-income countries, such as Bangladesh, suffer from poor medical waste management practices, which have now been put under further strain by the sudden increase in medical waste due to COVID-19 (Rahman et al., 2020). How to strengthen the separation and management of medical waste has become an important issue that government and society urgently need to solve.
At present, urban medical waste in China is mainly recycled and processed in a centralized manner, that is, medical waste from various medical units is collected and transported to a professional recycling center for centralized processing (Pu and Xia, 2018). During the COVID-19 epidemic, the daily production of medical waste in China significantly increased, which severely tested the national medical waste disposal system. To cope with the added pressure on medical waste treatment brought about by COVID-19, China has improved the medical waste disposal capacity in various places by building new, centralized disposal centers, adding mobile disposal facilities, and by transforming hazardous waste disposal facilities. As of March 21, 2020, the national medical waste disposal capacity was 6066.8 tons per day, an increase of 1164.0 tons per day from the 4902.8 tons per day before the epidemic (MEEPRC, 2019).
Compared to the medical waste generated by medical units, household medical waste has a small output and scattered production areas, so it is easily ignored. With the outbreak of the epidemic, the amount of medical waste generated by households using face masks, gloves, pills, vials, and medicinal liquids etc. has increased sharply and how to dispose of this kind of waste has attracted widespread attention (Chang et al., 2020). At present, China is guiding residents to participate in medical waste separation activities by setting up garbage bins in communities and public streets that are dedicated to household medical waste recycling. After recycling, this type of waste is sent to a centralized disposal center for processing. However, some residents arbitrarily discard domestic medical waste, which increases the pressure on medical waste disposal during the epidemic. Therefore, this study focuses on the medical waste generated by the family, such as face masks, gloves, pills, vials, and medicinal liquids, etc.
Gradually, it has been realized that relying on back-end waste disposal alone is not the best choice. The effectiveness of source separation determines the difficulty associated with medical waste treatment (Loan et al., 2017). A new approach based on separation at the front-end has been implemented in China (Hou et al., 2020). However, in general, the current situation regarding medical waste separation in China is not ideal, and effective guidance measures are needed.
2.1.3. The impact of crisis awareness on waste separation behavior
Behavioral psychology research regards awareness as a factor that determines behavior motivation and that behavioral ability further promotes behavior (Sharma and Bansal, 2013; Yue et al., 2013). Awareness internally affects individual information processing methods (Dijksterhuis et al., 2005) and emotions (Meneses, 2010), etc., which leads to explicit behavior differences. This recognition has led to a call for further research on the link between awareness and pro-environmental outcomes (Corsini et al., 2018). Chen et al. (2014) suggested that awareness reactions outweigh cognition in determining recycling behavior by residents.
Crisis awareness also has an impact on individual behavior. If conscious urban residents retain their thoughts on a crisis, they are more likely to change their behaviors (Walle et al., 2016). In crisis situations (such as in epidemics), improving the certainty of environmental perception and forming a set of self-consistent, subjective perceptions of epidemics can guide individual behavior and decision-making (Leppin and Aro, 2009). However, reports on public emergencies can also easily lead to public psychosocial crises, which can trigger rumors and increase panic (Verbeek, 2006). Also, the perception of crisis and risk is also considered to have a significant influence on environmental behavior. Some studies have suggested that a preventive focus has a significant predictive effect on the undesired environmental behavior of individuals. This conclusion is based on the adjustment focus theory (Higgins, 1997; Meyer et al., 2004).
The selection of individual behavior and the refinement of behavioral manifestations are conducive to systematic and professional research. This study drew on research by Chen et al., 2017a, Chen et al., 2017b, Chen et al., 2017c and classified medical waste separation behaviors into four categories based on behavior motivation: These were (1) waste separation behavior by habit (HWSB), which is separation behavior based on their own living habits; (2) waste separation behavior by decision (DWSB), which is the separation behavior shown by urban residents after weighing up the interests of economy and health; (3) waste separation behavior by relationship (RWSB), which is the selection behavior shown by urban residents after they are affected by the behavior and attitude shown by other people toward garbage separation; and (4) waste separation behavior by the citizen (CWSB), which is the separation behavior shown by urban residents that is based on social responsibility and citizen awareness.
In summary, awareness is an important factor that affects individual behavior motivation and decision making. The peculiar psychological presentation of crisis awareness also has an effect on related behaviors. A large number of studies have investigated the relationship between risk perception and environmental behavior. However, few studies have performed an in-depth analysis of the relationship between crisis awareness and waste separation behavior, especially the effects of diverse crisis awareness sources on different forms of medical waste separation behavior. Therefore, this study explored how the crisis awareness is related to the separation behavior shown by residents during the COVID-19 epidemic.
2.2. Qualitative analysis
2.2.1. Sampling and data collection
Stratified sampling was used to determine the sample structure. To ensure the rationality of the sample, six cities (Jiaxing, Hangzhou, Xuzhou, Suzhou, Taiyuan, and Yinchuan) in four provinces distributed across eastern, western, and central China were selected for investigation. Eight samples were selected from each province. The age range of the samples was 21–55 years old and the samples had a normal distribution.
The interviews were based on structured questionnaires, and the main channels used to conduct the interviews were phone and social software (Wechat, Tencent QQ). The interview time for each resident was 25–40 min. During the interview, we adjusted and added questions based on the actual situation to ensure that the interview could be further extended. This study used the theoretical saturation test to determine whether the sampling for a certain structural category was saturated, which means that no additional information can be found. About 2/3 of the sample interviews were randomly selected for open coding, spindle coding, and selective coding analysis. The remaining 1/3 of the sample interviews were reserved for theoretical saturation testing.
2.2.2. Open coding
Open coding is a process of decomposing, testing, comparing, conceptualizing, and generalizing the collected data. The original interview records were conceptualized and categorized (see Appendix 1) and the structural elements related to crisis awareness were obtained. Space limitations meant that only representative original record sentences and initial concepts for each category are listed.
2.2.3. Spindle coding
The main task of spindle coding is to discover the potential logical connections between categories. During spindle coding, researchers only conduct an in-depth analysis of one category at a time and then further explore the correlations around this category. The various connections between the categories become more specific as the analysis deepens. Spindle coding identified the main category for crisis awareness (CA), which included individual spontaneous crisis awareness (ISCA) and environment-driven crisis awareness (ECA). Individual spontaneous crisis awareness refers to the crisis awareness that is not affected by the environment and takes into account civic responsibility, health, and habit consciousness. In contrast, ECA refers to the crisis awareness that is affected by the family environment, professional environment, and social environment. The specific coding process is shown in Appendix 2.
2.2.4. Selective coding
Selective coding identifies the core category from the main category and analyzes the connection relationship between the core category, and the main and other categories. It can then depict the phenomenon and context structure in the form of a “story line”. This study focused on the “story line”: “relationship between crisis awareness (CA) and medical waste separation behavior (MWSB) of urban residents”. A conceptual model was then constructed based on this “story line” that included CA and MWSB (Fig. 2 ).
Fig. 2.

Conceptual model.
Note: CA- Crisis awareness; MWSB- medical waste separation behavior; CR- Civic responsibility; LH- Life and health; HC- Habitual consciousness; SE- Social environment; FE- Family environment; PE- Professional environment.
2.2.5. Saturation testing and theory construction
Theoretical saturation is used to determine whether the sampling for a certain structural category is saturated. Saturation means that no additional information can be found. Therefore, researchers can develop characteristics for the category based on the available information. The results showed that the category dimensions and categories in the model shown in Fig. 2 have been sufficiently developed. No new categories and relationships were detected for the two crisis awareness subcategories and no new constituent factors were discovered. The results suggested that the structural dimension of crisis awareness was theoretically saturated. Therefore, the hypotheses used in this study were as follows:
H1. ISCA has a positive relationship with the MWSB shown by urban residents.
H2. ECA has a positive relationship with the MWSB shown by urban residents.
2.3. Variables measurement and implementation
2.3.1. Variables measurement
The initial scale was obtained by revising and developing relevant items based on an existing maturity scale for waste separation behavior shown by urban residents (Chen et al., 2017a, Chen et al., 2017b, Chen et al., 2017c) and previous qualitative analyses. In order to test the feasibility of the scale, an online pre-survey was conducted from April 6 to 16, 2020. A total of 231 questionnaires were collected, and the final valid questionnaire count was 196. After pre-testing, we improved the description of two ambiguous items, based on feedback from interviewees during data collection, to ensure that each item of the questionnaire was accurate and easy to understand.
A formal survey questionnaire was obtained and the initial items were adjusted and modified based on the analysis results for reliability and validity. The questionnaire was divided into three parts. The first part was the basic information survey, which included gender, age, education, and monthly income level of the person, etc. In the second part, 22 items are used to measure CA (10 items for ISCA and 12 items for ECA) and 11 items are used to measure MWSB (3 items for HWSB, 2 items for DWSB, 3 items for RWSB, and 3 items for CWSB). A higher score indicated a stronger psychological tendency to engage in MWSB. The scales for CA and MWSB are shown in Appendix 3.
2.3.2. Research sample
Stratified sampling was used when conducting the formal survey. The sample objects of the survey were roughly determined for items such as sex, age and occupational fields. The study will try to ensure that there are as many females as males. In addition, about 40% of the samples between the ages of 18 and 30 will be investigated, and about 40% of the samples between the ages of 30 and 60 will be investigated. In terms of occupational fields, the study will also try to ensure that the proportion of respondent s in the non-industrial field is 50% - 60%. The official questionnaire was mainly distributed around cities in China that produced large amounts of medical waste during the epidemic, such as Wuhan, Shanghai, Suzhou, Tianjin, Jiaxing, Taiyuan, Yinchuan, Xuzhou, Beijing, and Guangzhou. The conditions caused by the epidemic meant that the questionnaires were mainly distributed in the form of online surveys (questionnaire links), but they were supplemented by on-site surveys, that is, the questionnaires were distributed in densely populated areas, such as residential and commercial areas. The sample distribution is shown in Appendix 4. The sample consisted of 53.6% female respondents. The average age was about 32 years old and 44.9% of respondents was younger than 30. The overall education level of the sample was relatively high, 57.9% of the sample received undergraduate education and above. 64.1% of the sample was married. The average monthly income of the sample was mostly below 10,000 yuan, 21.7% of the sample's monthly income was not higher than 2000 yuan, 32.2% of the samples' monthly income was 2001–6000 yuan, 35.6% of the samples' monthly income was 6001–10,000 yuan. And 40.6% of respondents worked in the industrial field. We used SPSS 22.0 (IBM Corp., Armonk, NY, USA) to analyze the 668 valid samples.
2.3.3. Reliability and validity testing, and factor analysis
The internal consistency test results for each dimension of the formal questionnaire are shown in Appendix 5 (Cronbach's α > 0.66). The data showed that the scale was reliable.
Also, a confirmatory factor analysis was conducted on the formal scale (Appendix 6). The statistical results showed that the structural fitting indicators of the two-factor model for CA and the four-factor model for MWSB reached an acceptable level, and the structural validity of the CA and MWSB were verified. Furthermore, the average extraction value of variance (AVE) for each factor was >0.5, which indicated that the scale had good convergence validity.
3. Results
3.1. Descriptive statistical analysis
The Likert 5-point scale measurement in The Medical Waste Separation Behavior Measurement Scale was used in this study. Participants rated their agreement with each item on a scale from 1 (disagree strongly) to 5 (strongly agree). When the score was lower than 3, then an individual rarely showed any MWSB. Therefore, a MWSB score with a mean value of <3 points was defined as the inferior value (Chen et al., 2017a, Chen et al., 2017b, Chen et al., 2017c). According to Table 1 , the overall average value for MWSB was 3.7 and the detection rate for inferiority was 12.65%. Also, the inferiority detection rates for HWSB and CWSB were relatively high at 19.04% and 24.56%, respectively.
Table 1.
Descriptive statistical analysis results for urban residents.
| Variables | Mean | Standard deviation | Inferiority value(mean < 3) |
|
|---|---|---|---|---|
| Frequency | The detection rate(%) | |||
| MWSB | 3.70 | 0.681 | 87 | 12.65% |
| HWSB | 3.73 | 0.890 | 131 | 19.04% |
| DWSB | 3.90 | 0.916 | 78 | 11.34% |
| RWSB | 3.76 | 0.898 | 94 | 13.66% |
| CWSB | 3.48 | 0.942 | 169 | 24.56% |
3.2. Regression analysis
Each variable was first centralized (except demographic variables) and then a Pearson's correlation analysis of each variable was conducted (Appendix 7). The analysis results showed that at a significance level of 0.05, the CA (ISCA and ECA) and the MWSB (HWSB, DWSB, RWSB, and CWSB) were significantly positively correlated. The VIF value for each item was between 1.861 and 1.903, and the D—W statistic was close to 2, which indicated that the data did not have any collinearity and autocorrelation issues.
Table 2 shows the regression analyses results for CA and MWSB. The addition of control variables (demographic variables, Appendix 8 shows how the variables were assigned) increased the goodness of fit of the model (R22 = 0.357 > R12 = 0.314). Based on model 6, ISCA was positively related to DWSB (p < 0.05), and models 2, 6, 8, and 10 indicated that ECA was positively related to DWSB, RWSB, and CWSB (p < 0.01). The results provided support for hypotheses H1 and H2. In terms of relationship between socio-demographics and medical waste separation behavior, residents aged 31–60 years old, marital status, and total monthly income of 2001–6000 RMB and > 10,000 RMB passed the significance test.
Table 2.
Regression analysis of CA on MWSB.
| Variables | MWSB |
HWSB |
DWSB |
RWSB |
CWSB |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 | Model 9 | Model 10 | ||
| Constant | 1.753 | 1.599 | 3.153 | 3.125 | 1.604 | 1.478 | 1.407 | 1.192 | 0.797 | 0.560 | |
| ISCA | 0.041 | 0.064 | 0.065 | 0.053 | 0.072 | 0.098⁎ | 0.007 | 0.039 | −0.006 | 0.020 | |
| ECA | 0.531⁎⁎⁎ | 0.496⁎⁎⁎ | 0.051 | 0.070 | 0.421⁎⁎⁎ | 0.380⁎⁎⁎ | 0.538⁎⁎⁎ | 0.491⁎⁎⁎ | 0.587⁎⁎⁎ | 0.546⁎⁎⁎ | |
| Gender | −0.023 | −0.029 | −0.025 | −0.021 | 0.002 | ||||||
| Age (Reference: 18–30 years old) |
31–60 years old | 0.135⁎⁎⁎ | 0.131⁎⁎ | 0.093⁎ | 0.087⁎ | 0.092 | |||||
| >60 years old | 0.060 | 0.048 | 0.006 | 0.063⁎ | 0.051⁎ | ||||||
| Marital status | 0.208⁎⁎⁎ | 0.049 | 0.180⁎⁎⁎ | 0.222⁎⁎⁎ | 0.181⁎⁎⁎ | ||||||
| City | −0.047 | −0.092⁎⁎ | −0.025 | −0.013 | −0.009 | ||||||
| Education | 0.045 | 0.064 | −0.007 | 0.024 | 0.042 | ||||||
| Total monthly income (Reference: ≤2000 RMB) |
2001–6000 RMB | 0.098⁎ | −0.077 | 0.125⁎⁎ | 0.145⁎⁎ | 0.118⁎⁎ | |||||
| 6001–10,000 RMB | 0.088 | −0.116⁎ | 0.111⁎ | 0.157⁎⁎ | 0.125⁎⁎ | ||||||
| >10,000 RMB | 0.081⁎ | −0.067 | 0.071 | 0.132⁎⁎ | 0.109⁎⁎ | ||||||
| Career field | −0.060 | −0.124⁎⁎ | −0.043 | −0.028 | 0.014 | ||||||
| R2 | 0.314 | 0.357 | 0.011 | 0.046 | 0.223 | 0.255 | 0.295 | 0.340 | 0.339 | 0.371 | |
| Adj-R2 | 0.311 | 0.350 | 0.008 | 0.036 | 0.221 | 0.247 | 0.293 | 0.333 | 0.337 | 0.364 | |
| ∆R2 | 0.314 | 0.044 | 0.011 | 0.034 | 0.223 | 0.032 | 0.295 | 0.045 | 0.339 | 0.032 | |
| F | 151.866 | 52.400 | 3.855 | 4.524 | 95.500 | 32.255 | 138.990 | 48.525 | 170.684 | 55.561 | |
p < 0.05.
p < 0.01.
p < 0.001.
3.3. Cross analysis
The residents were clustered into four groups based on the source characteristics for CA so that the relationship between CA and MWSB could be explored in depth. The performance characteristics of the different MWSB sample types were (1) individuals with high scores for ISCA (>3) and high scores for ECA (>3) were in the “sensitive” group; (2) individuals with low scores for ISCA (<3) and low scores for ECA (<3) were in the “insensitive” group; (3) individuals with high scores for ISCA (>3) and low scores for ECA (<3) were in the “conscious” group; and (4) individuals with low scores for ISCA (<3) and high scores for ECA (>3) were in the “passive” group.
The average values for MWSB in the “sensitive”, “insensitive”, “conscious”, and “passive” groups were then analyzed (Fig. 3 ). The “sensitive” group had the highest average score for MWSB (3.88) and their scores for all the dimensions were higher than for the other groups. In other words, they participated in medical waste separation activities most frequently. In contrast, the “insensitive” group had the lowest average MWSB score (3.17), which meant they were least involved in medical waste sorting. The results indicated that individuals who showed a high level of crisis awareness due to spontaneous or environmental drive were most likely to take part in medical waste separation and classification. The remaining individuals did not exhibit high levels of MWSB, but they may undertake some medical waste classification. In particular, although ISCA only had positive correlation on HWSB, individuals with a high ISCA tended to undertake more MWSB.
Fig. 3.

Mean MWSB values for the classified samples.
The “insensitive” group was used as a reference to analyze the differences in the MWSB between the “passive” and “conscious” groups (see Table 3 ). The results showed that the “conscious” and “insensitive” groups did not demonstrate significant MWSB differences. However, the “passive” and “insensitive” groups had significantly different MWSB, DWSB, and RWSB values. This further showed that ECA had a higher correlation with on MWSB than ISCA.
Table 3.
t-Test results for the “conscious”, “passive”, and “insensitive” groups.
| ISCA | Levene test of variance equation |
t-Test of variance equation |
ECA | Levene test of variance equation |
t-Test of variance equation |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Sig | t | Sig | F | Sig | t | Sig | ||||
| MWSB | Assuming equal variances | 0.913 | 0.341 | −0.888 | 0.376 | MWSB | Assuming equal variances | 1.13 | 0.29 | −2.119 | 0.036 |
| Assuming that the variances are not equal | −0.886 | 0.377 | Assuming that the variances are not equal | −2.200 | 0.030 | ||||||
| HWSB | Assuming equal variances | 0.068 | 0.795 | −0.756 | 0.451 | HWSB | Assuming equal variances | 0.003 | 0.957 | −0.016 | 0.987 |
| Assuming that the variances are not equal | −0.756 | 0.451 | Assuming that the variances are not equal | −0.016 | 0.987 | ||||||
| DWSB | Assuming equal variances | 2.879 | 0.092 | −1.198 | 0.233 | DWSB | Assuming equal variances | 0.027 | 0.869 | −2.184 | 0.031 |
| Assuming that the variances are not equal | −1.194 | 0.234 | Assuming that the variances are not equal | −2.186 | 0.031 | ||||||
| RWSB | Assuming equal variances | 1.937 | 0.166 | −0.76 | 0.448 | RWSB | Assuming equal variances | 0.918 | 0.34 | −2.345 | 0.021 |
| Assuming that the variances are not equal | −0.757 | 0.45 | Assuming that the variances are not equal | −2.407 | 0.018 | ||||||
| CWSB | Assuming equal variances | 1.673 | 0.198 | −0.158 | 0.875 | CWSB | Assuming equal variances | 0.918 | 0.340 | −2.345 | 0.0210 |
| Assuming that the variances are not equal | −0.157 | 0.875 | Assuming that the variances are not equal | −2.407 | 0.0180 | ||||||
4. Discussion
The descriptive analysis results showed that the detection rate for the inferiority value of medical waste separation behavior during the COVID-19 epidemic was low (12.65%). It is worth noting that the detection rate for waste separation behavior by citizens was the highest (24.56%), which shows that the level of citizenship among Chinese urban residents is relatively low when it comes to handling waste separation. In general, residents showed better medical waste separation behavior compared to their general waste separation behavior (Chen et al., 2017a, Chen et al., 2017b, Chen et al., 2017c). They also showed certain risk perceptions, and moderate fear and anxiety due to the epidemic (Wang and Ying, 2020), which may stimulate or increase their crisis awareness and promote their participation in medical waste classification activities. Furthermore, previous studies have shown that psychological distance has an effect on individual perception and judgment, thereby affecting their acceptance attitude and ability (Soderberg et al., 2015). Furthermore, public safety events that directly affect the life and health of individuals will shorten the psychological distance of an individual (Burns and Slovic, 2007; Rahmi et al., 2019). Also, the widespread application of mobile social media has greatly increased the amount of information and the number of information sources. These changes also reduce the psychological distance of individuals (Zhang and Gan, 2020). During the epidemic, the relevance and transparency of information may have had a certain effect on the psychological distance of residents, which meant that they better understood the importance and necessity of medical waste classification. This may be the reason why the residents showed an improved response attitude toward the medical waste separation policy.
The results of the relationship between crisis awareness and medical waste separation behavior showed that the different forms of crisis awareness had no correlation with the waste separation behavior for habit factor. The idea behind habitual behavior is that some people realize that they sometimes follow the same mindset (Marchetti and Rosenberg, 2017). For example, previous research has suggested that habitual behavior was a completely unconscious automated action process (Garndner, 2009), which took a long time to shape (Dewsbury and Bissell, 2015). However, the crisis awareness triggered by the COVID-19 epidemic was mostly an emergency response to a sudden situation. It is difficult to affect the way of thinking by residents over a short period of time, which means that residents do not form stable habits.
The cross-analysis results showed that environmentally-driven crisis awareness had a higher correlation with the separation of medical waste than spontaneous crisis awareness. This study confirmed the relationship between environmental stimuli and individual behavior reported in previous studies. According to the “stimulus-body-response” model, external stimuli drive individual emotional responses (consciousness), and their emotional responses (awareness) lead to individual behavior (Mehrabian and Russell, 1974). In the context of this research, the COVID-19 epidemic may stimulate individual emotional responses (environment-driven crisis awareness), and this emotional response (environment-driven crisis awareness) could improve their participation in medical waste separation. Also, Tversky and Kahneman (1974) suggested that individuals often adopt the principle of anchoring and adjustment when recognizing and judging new things, that is, they formed an “anchor” based on original knowledge and experience, and then adjusted the “anchor” by obtaining external information. This new information then determined related behavior and decision making by individuals. Spontaneously generated crisis awareness is the “anchor” and is based on long-term life judgments by residents. Related media news, national policies, and other information about the epidemic will prompt residents to adjust their corresponding awareness and stimulate their environment-driven crisis awareness, which makes it more relevant to separation behavior by residents.
Previous studies have shown that individual implementation costs (Mee et al., 2004), social reference norms (Saphores et al., 2012), relevant promotional measures (Stoeva and Alriksson, 2017), and other contextual factors affect individual waste separation behavior. Future research should extend the model outlined in this study and consider the impact mechanisms underlying other contextual factors that affect medical waste separation behavior. Although this study tried to ensure the representativeness of the sample as much as possible during sample selection, randomness could not be fully guaranteed in a sample and it was difficult to create a sample distribution that matched the actual distribution. The sample in this study was biased toward younger people with a higher education. Other data collection methods will be tried in future research.
5. Conclusions
Under the background of the COVID-19 epidemic, this study introduced the concept of crisis awareness combined with the results of a qualitative analysis, and has constructed a correlation model that includes crisis awareness and medical waste separation behavior. The data from 668 urban residents showed that the detection rate for individual medical waste separation behavior was 12.65%, among which, the detection rate for waste separation behavior by citizen was the highest (24.56%). The regression analysis results showed that environment-driven crisis awareness had a significant correlation with the medical waste separation behavior for citizen's factors and its related dimensions, while individual spontaneous crisis awareness only had a positive correlation with the waste separation behavior for decision factor. Therefore, strengthening resident crisis awareness maybe conducive to promoting their participation in medical waste separation. Based on the original characteristics of crisis awareness, residents can be clustered into “sensitive”, “conscious”, “passive”, and “insensitive” types. The “sensitive” group was more actively involved in the separation of medical waste. In contrast, the “insensitive” group showed the worst medical waste separation behavior according to the medical waste separation behavior results and the characteristics of its dimensions. Also, environmental-driven crisis awareness has a higher correlation with medical waste separation behavior by residents according to the comparison between the “conscious” groups and “passive” groups. We believe that the reinforcement of public awareness about environmental issues can increase resident participation in medical waste separation activities. The results provided important theoretical and practical support for medical waste separation.
CRediT authorship contribution statement
Feiyu Chen: Conceptualization, Methodology, Investigation, Writing – original draft, Project administration, Funding acquisition. Jingxuan Lou: Writing – review & editing, Software, Formal analysis. Jiangxin Hu: Software, Formal analysis. Hong Chen: Conceptualization, Validation, Resources, Writing – review & editing, Supervision. Ruyin Long: Supervision, Validation, Resources. Wenbo Li: Formal analysis.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
This work was financially supported by the National Natural Science Foundation of China (71904187, 71904183), the Major Projects Supported by the National Social Science Foundation (19ZDA107), the Key Projects Supported by the National Social Science Foundation (18AZD014), the Social Science Fund of Jiangsu Province (18GLB015), the Project funded by China Postdoctoral Science Foundation (2019T120483, 2018M640539), and the Teaching Research Project of China University of Mining and Technology (2020YB36). The authors would like to extend special thanks to the editor and anonymous reviewers for their constructive comments and suggestions for improving the quality of this study.
Editor: Damia Barcelo
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.scitotenv.2021.147522.
Appendix A. Supplementary data
Partial data analysis results
References
- Abrahamse W., Steg L., Vlek C. The effect of tailored information, goal setting, and tailored feedback on household energy use, energy-related behaviors, and behavioral antecedents. J. Environ. Psychol. 2007;27(4):265–276. [Google Scholar]
- Bargh J.A. Losing consciousness: automatic influences on consumer judgment, behavior, and motivation. J. Consum. Res. 2002;29(2):280–285. [Google Scholar]
- Barnett-Itzhaki Z., Berman T., Grotto I., Schwartzberg E. Household medical waste disposal policy in Israel. Isr. J. Health Policy Res. 2016;5(1):48. doi: 10.1186/s13584-016-0108-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blau P.M. John Wiley and Sons; NewYork: 1964. Exchange and Power in Social Life. [Google Scholar]
- Block N. Consciousness, accessibility, and the mesh between psychology and neuroscience. Behav. Brain Sci. 2007;30(5–6):481–499. doi: 10.1017/S0140525X07002786. [DOI] [PubMed] [Google Scholar]
- Burns W.J., Slovic P. The diffusion of fear: modeling community response to a terrorist strike. J. Def. Model. Simul. Appl. Methodol. Technol. 2007;4(4):298–317. [Google Scholar]
- Casali A.G., Gosseries O., Rosanova M., Boly M., Sarasso S., Casali K.R., Casarotto S., Bruno M., Laureys S., Tononi G., Massimini M. A theoretically based index of consciousness independent of sensory processing and behavior. Sci. Transl. Med. 2013;5(198) doi: 10.1126/scitranslmed.3006294. [DOI] [PubMed] [Google Scholar]
- Chalak A., Abou-Daher C., Chaaban J., et al. The global economic and regulatory determinants of household food waste generation: a cross-country analysis. Waste Manag. 2016;48:418–422. doi: 10.1016/j.wasman.2015.11.040. [DOI] [PubMed] [Google Scholar]
- Chang M., Tang Y.D., Yang L. Analysis and reference of international medical waste wanagement, treatment and disposal system. Environ. Prot. 2020;48(8):63–69. [Google Scholar]
- Chen H., Long R., Niu W., et al. How does individual low-carbon consumption behavior occur? — an analysis based on attitude process. Appl. Energy. 2014:376–386. [Google Scholar]
- Chen F., Chen H., Guo D., et al. Analysis of undesired environmental behavior among Chinese undergraduates. J. Clean. Prod. 2017;162:1239–1251. [Google Scholar]
- Chen F., Chen H., Huang X., et al. Public response to the regulation policy of urban household waste: evidence from a survey of Jiangsu province in China. Sustainability. 2017;9(6):1034. [Google Scholar]
- Chen F.Y., Chen H., Long R.Y. Undesired environmental behavior and its presentation - the impact to regulatory focus. Journal of Beijing Institute of Technology (Social Sciences Edition) 2017;19(5):28–36. [Google Scholar]
- Chen F., Chen H., Wu M., et al. Research on the driving mechanism of waste separation behavior: based on qualitative analysis of Chinese urban residents. Int. J. Environ. Res. Public Health. 2019;16(10):1859. doi: 10.3390/ijerph16101859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cialdini R.B., Reno R.R., Kallgren C.A. A focus theory of normative conduct: recycling the concept of norms to reduce littering in public places. J. Pers. Soc. Psychol. 1990;58(6):1015–1026. [Google Scholar]
- Corsini F., Gusmerotti N.M., Testa F., Iraldo F. Exploring waste prevention behaviour through empirical research. Waste Manag. 2018:132–141. doi: 10.1016/j.wasman.2018.07.037. [DOI] [PubMed] [Google Scholar]
- Covello V.T., Merkhofer M.W. Springer; US: 1993. Risk Assessment Methods. [Google Scholar]
- Dewsbury J.C., Bissell D. Habit geographies: the perilous zones in the life of the individual. Cult. Geogr. 2015;22(1):21–28. [Google Scholar]
- Dijksterhuis A., Smith P.K., Van Baaren R.B., Wigboldus D.H. The unconscious consumer: effects of environment on consumer behavior. J. Consum. Psychol. 2005;15(3):193–202. [Google Scholar]
- Dzekashu L.G., Akoachere J.F., Mbacham W.F. Medical waste management and disposal practices of health facilities in Kumbo East and Kumbo West health districts. Int. J. Med. Med. Sci. 2017;9(1):1–11. [Google Scholar]
- Emerson R.M. Power-dependence relations. Am. Sociol. Rev. 1962;27(1):31–41. [Google Scholar]
- Evison T., Read A.D. Local authority recycling and waste - awareness publicity/promotion. Resour. Conserv. Recycl. 2001;32:275–291. [Google Scholar]
- Garndner B. Modeling motivation and habit in stable travel mode contexts. Transport. Res. F: Traffic Psychol. Behav. 2009;12(1):68–76. [Google Scholar]
- Geller E.S., Richard A.W., Peter B.E. Preserving the environment: new strategies for behavior change. J. Leis. Res. 1982;14(4):365–366. [Google Scholar]
- Geppert J., Stamminger R. Do consumers act in a sustainable way using their refrigerator? The influence of consumer real life behaviour on the energy consumption of cooling appliances. Int. J. Consum. Stud. 2010;34(2):219–227. [Google Scholar]
- Higgins E.T. Beyond pleasure and pain. Am. Psychol. 1997;52(12):1280–1300. doi: 10.1037//0003-066x.52.12.1280. [DOI] [PubMed] [Google Scholar]
- Hou J., Wang F., Chen F. Should waste separation be mandatory? A study on public’s response to the policies in China. Int. J. Environ. Res. Public Health. 2020;17(12):4539. doi: 10.3390/ijerph17124539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang L., Zhou Y., Han Y., Hammitt J.K., Bi J., Liu Y. Effect of the Fukushima nuclear accident on the risk perception of residents near a nuclear power plant in China. Proc. Natl. Acad. Sci. U. S. A. 2013;110(49):19742–19747. doi: 10.1073/pnas.1313825110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasperson J.X., Kasperson R.E., Pidgeon N., Slovic P. The Social Amplification of Risk. Vol. 1. 2003. The social amplification of risk: assessing fifteen years of research and theory; pp. 13–46. [Google Scholar]
- Kautish P., Paul J., Sharma R. The moderating influence of environmental consciousness and recycling intentions on green purchase behavior. J. Clean. Prod. 2019;228:1425–1436. [Google Scholar]
- Keshavarz M., Karami E. Farmers’ pro-environmental behavior under drought: application of protectionmotivation theory. J. Arid Environ. 2016;127:128–136. [Google Scholar]
- Kim S., Jeong S.H., Hwang Y. Predictors of pro-environmental behaviors of American and Korean students: the application of the theory of reasoned action and protection motivation theory. Sci. Commun. 2013;35(2):168–188. [Google Scholar]
- Krause D.R. Environmental consciousness: an empirical study. Environ. Behav. 1993;25(1):126–142. [Google Scholar]
- Leppin A., Aro A.R. Risk perceptions related to SARS and avian influenza: theoretical foundations of current empirical research. Int. J. Behav. Med. 2009;16(1):7–29. doi: 10.1007/s12529-008-9002-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loan L.T.T., Nomura H., Takahashi Y., et al. Psychological driving forces behind households’ behaviors toward municipal organic waste separation at source in Vietnam: a structural equation modeling approach. J. Mater. Cycles Waste Manage. 2017;19(3):1052–1060. [Google Scholar]
- Maleksaeidi H., Keshavarz M. Global Ecology and Conservation. Vol. 20. 2019. What influences farmers' intentions to conserve on-farm biodiversity? An application of the theory of planned behavior in Fars province, Iran; pp. 28–34. [Google Scholar]
- Marchetti S., Rosenberg A. A history of habit: from Aristotle to Bourdieu ed. by Tom Sparrow, Adam Hutchinson (review) Trans. Charles S. Peirce Soc. 2017;53(4):635–640. [Google Scholar]
- Mee N., Clewes D., Phillips P.S., Read A.D. Effective implementation of a marketing communications strategy for kereside recycling: a case study from Rushcliffe. UK. Resour. Conserv. Recycl. 2004;42(1):1–26. [Google Scholar]
- Mehrabian A., Russell J.A. 1974. An Approach to Environmental Psychology. [Google Scholar]
- Meneses G.D. Refuting fear in heuristics and in recycling promotion. J. Bus. Res. 2010;63(2):104–110. [Google Scholar]
- Meyer J.P., Becker T., Vandenberghe C. Employee commitment and motivation: a conceptual analysis and integrative model. J. Appl. Psychol. 2004;89(6):991–1007. doi: 10.1037/0021-9010.89.6.991. [DOI] [PubMed] [Google Scholar]
- Ministry of ecology and environment of the people's Republic of China (MEEPRC) 2019. The National Annual Report on the Prevention and Control of Environmental Pollution by Solid Waste in Large and Medium-sized Cities in 2019. [Google Scholar]
- Muduli K., Barve A. Barriers to green practices in health care waste sector: an Indian perspective. Int. j. Environ. Sci. Dev. 2012;3(4):393–399. [Google Scholar]
- Nie L. Multi-objective incremental coverage model and solution for the temporary location of medical waste China population. Resour. Environ. 2018;28(S1):105–107. [Google Scholar]
- Papaoikonomou K., Latinopoulos D., Emmanouil C., et al. A survey on factors influencing recycling behavior for waste of electrical and electronic equipment in the Municipality of Volos, Greece. Environ. Process. 2020;7:321–339. [Google Scholar]
- Pfeffer J., Salancik G.R. Harper and Row; New York: 1978. The External Control of Organization: A Resource Dependence Perspective. [Google Scholar]
- Pu S., Xia C. Robust optimization model for the recycling path of urban medical waste. Syst. Eng. 2018;36(6):117–123. [Google Scholar]
- Rahman M.M., Bodrud-Doza M., Griffiths M.D., Mamun M.A. Biomedical waste amid COVID-19: perspectives from Bangladesh. Lancet Glob. Health. 2020;8(10) doi: 10.1016/S2214-109X(20)30349-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rahmi R., Joho H., Shirai T. An analysis of natural disaster-related information-seeking behavior using temporal stages. J. Assoc. Inf. Sci. Technol. 2019;70(7):715–728. [Google Scholar]
- Saphores J., Ogunseitan O.A., Shapiro A.A. Willingness to engage in a pro-environmental behavior: an analysis of e-waste recycling based on a national survey of U.S. households. Resour. Conserv. Recycl. 2012;60:49–63. [Google Scholar]
- Schwing R.C., Albers W.A. Societal risk assessment: how safe is safe enough? Med. Phys. 1982;9(3):442–443. [Google Scholar]
- Setbon M., Raude J., Fischler C., Flahault A. Risk perception of the “mad cowdisease” in France: determinants and consequences. Risk Anal. 2005;25(4):813–826. doi: 10.1111/j.1539-6924.2005.00634.x. [DOI] [PubMed] [Google Scholar]
- Shareefdeen Z.M. Medical waste management and control. J. Environ. Prot. 2012;3(12):1625–1628. [Google Scholar]
- Sharma K., Bansal M. Environmental consciousness, its antecedents and behavioural outcomes. J. Indian Bus. Res. 2013;5(3):198–214. [Google Scholar]
- Shimoda A., Hayashi H., Sussman D., Nansai K., Fukuba I., Kawachi I., Kondo N. Our health, our planet: a cross-sectional analysis on the association between health consciousness and pro-environmental behavior among health professionals. Int. J. Environ. Health Res. 2020;30(1):63–74. doi: 10.1080/09603123.2019.1572871. [DOI] [PubMed] [Google Scholar]
- Skarlatidou A., Cheng T., Haklay M. What do lay people want to know about the disposal of nuclear waste? A mental model approach to the design and development of an online risk communication. Risk Anal. 2012;32(9):1496–1511. doi: 10.1111/j.1539-6924.2011.01773.x. [DOI] [PubMed] [Google Scholar]
- Soderberg C.K., Callahan S.P., Kochersberger A.O., Amit E., Ledgerwood A. The effects of psychological distance on abstraction: two meta-analyses. Psychol. Bull. 2015;141(3):525–548. doi: 10.1037/bul0000005. [DOI] [PubMed] [Google Scholar]
- State Council of the People's Republic of China (SCRPC) Regulations on the Management of Medical Waste. 2003. http://www.gov.cn/banshi/2005-08/02/content_19238.htm Central Government Portal.
- Stoeva K., Alriksson S. Influence of recycling programmes on waste separation behaviour. Waste Manag. 2017;68:732–741. doi: 10.1016/j.wasman.2017.06.005. [DOI] [PubMed] [Google Scholar]
- Tversky A., Kahneman D. Judgement under uncertainty: heuristics and biases. Science. 1974;185:1124–1131. doi: 10.1126/science.185.4157.1124. [DOI] [PubMed] [Google Scholar]
- Vassanadumrongdee S., Kittipongvises S. Factors influencing source separation intention and willingness to pay for improving waste management in Bangkok, Thailand. Sustain. Environ. Res. 2018;28:90–99. [Google Scholar]
- Verbeek B. The politics of crisis management: public leadership under pressure. Acta Politica. 2006;41(4):457–460. [Google Scholar]
- Walle B.V.D., Brugghemans B., Comes T. Improving situation awareness in crisis response teams. Int. J. Hum. Comput. Stud. 2016;95:66–79. [Google Scholar]
- Wang J.M., Wang J.H. The model of influencing factors of public low-carbon consumption patterns and government control policies—an exploratory study based on grounded theory. Manage. World. 2011;4:58–68. [Google Scholar]
- Wang J.X., Ying X.P. Exploration and Free Views. 232–243. 2020. Cognition, emotion and action: social mentality in the emergency response; pp. 291–292. + [Google Scholar]
- Wei J., Wang F., Zhao D. A risk perception model: simulating public response to news reports in China. Inf. Res. 2012;17(2):411–436. [Google Scholar]
- Wu J.F., Xu W.H., Xu H.J. On the determinants of top managers' crisis awareness under the financial turmoil—an empirical study based on resource dependence and behavior theories. Journal of Northeastern University (Social Science) 2012;14(1):17–22. [Google Scholar]
- Yue T., Long R.Y., Ge S.W. Research on affecting factors model of urban residents’ energy saving behavior of Jiangsu province—based on grounded theory. Journal of Beijing Institute of Technology (Social Sciences Edition) 2013;15(1):34–39. [Google Scholar]
- Zhang F., Gan H.C. On the influence of temporal and spatial distance from epidemic on public sentiment: a computational analysis based on panel data of weibo text about COVID-19. J. Mass Commun. Mon. 2020;6:39–49. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Partial data analysis results