

Abstract
Background:
Multiple drug use involves particular pleasures and risks, and is disproportionately practiced by some minority and socially marginalized groups. The unique patterns, intentions, and social contexts of multiple drug use for these groups are poorly understood.
Methods:
Our mixed method integrates geo-enabled smartphone survey data collection with a qualitative mapping interview method. This brief report presents data from one study participant to demonstrate this method’s potential contributions to multiple drug use research for priority groups in different settings.
Results:
‘Jason’s’ data revealed the interrelated dynamics within his drug use repertoire and links between his substance use to rural life as a transgender person with autism spectrum disorder (ASD). Cigarettes played a role in coping with acute stress from repeatedly being misgendered. Cannabis intoxication helped manage social interactions as a person with ASD, while ‘chasing’ with cigarettes calibrated cannabis intoxication. Methamphetamine use related to managing body dysmorphia in a rural context with poor access to transgender health services.
Conclusion:
This mixed method can integrate reliable and ecologically valid assessments of multiple drug use repertoires and combination patterns with the place-embedded experiences, intersecting identities, structural barriers, and intentions related to multiple drug use for different priority groups.
Keywords: polydrug use, substance use, social determinants of health, sexual and gender minorites, ecological momentary assessment, qualitative research, Geographic Information Systems
Introduction
Social science contributions to understanding multiple drug use have lagged behind those from the natural sciences (Kataja, Tigerstedt, & Hakkarainen, 2018). The regular and combined use of multiple substances is disproportionately practiced by some minority and socially marginalized groups, such as gender minority individuals (Benotsch et al., 2013). The particular risks (e.g., overdose) and benefits (e.g., enhanced capacities) associated with multiple drug use demand a better understanding of its unique characteristics, including its specific patterns, combinations, intentions, and contexts (Kataja et al., 2018). We use the term multiple drug use to encompass both ‘drug use repertoires’ and ‘drug use combinations’. Drug use repertoires refer to the variety of substances a person ingests during a particular timeframe (Boys et al., 1999). ‘Drug use combinations’ refer to the ingestion of two or more substances at the same time or in close temporal proximity so that overlapping psychoactive effects are produced (Hakkarainen, O’Gorman, Lamy, & Kataja, 2019).
Prominent methods for researching multiple drug use include retrospective surveys that inventory participants’ drug use repertoires over the past month or year, and in-depth interviews and ethnographic field work that examine practices and experiences of drug use combinations. Increasingly, mobile and geo-enabled technologies (e.g., smartphones, geographic information systems) are being integrated with qualitative research methods (e.g., in-depth interviews) to ground drug use practices and experiences in their social and physical environments (Mennis, Mason, & Cao, 2013; Valdez & Sifaneck, 2010). In the spirit of creative research methods like these (Kara, 2015), we integrated geo-enabled smartphone survey data collection with a qualitative mapping interview method and piloted it to explain tobacco use disparities among bisexual young adults. The pilot study revealed smoking patterns and situations that reflect young adult smokers, generally, but also the unique roles that smoking plays for bisexual young adults as they navigate differently sexualized spaces in everyday life (McQuoid, Thrul, & Ling, 2018; McQuoid, Thrul, Ozer, Ramo, & Ling, 2019). This brief report draws from preliminary data to demonstrate how the method may also provide integrated insights into the unique patterns, intentions, and socio-structural contexts of multiple drug use for different groups of people.
Integrating mobile health and qualitative mapping methods
Smartphone apps that repeatedly administer surveys to participants and record their locations over time are often used to research recurring and episodic behaviours. These approaches can ‘reach into’ the fabric of everyday life to collect data within participants’ natural environments and routines (Kirchner & Shiffman, 2016). Smartphone ownership is increasingly ubiquitous even among low income and rural groups, making this approach feasible with diverse populations. Mobile health (mHealth) research methods, such as these, minimize the retrospective recall bias that occurs when participants are asked to characterize their behaviours or experiences, and can be integrated into spatial frameworks and analyses when geolocation data is also collected (Kirchner & Shiffman, 2016).
The value of mHealth methods for researching tobacco use is established (Ferguson & Shiffman, 2011). mHealth methods are now used to research patterns and situational predictors of use of other substances, including cannabis, opioids, cocaine, MDMA, and alcohol (e.g., Roth et al., 2017; Santa Maria et al., 2017). Because mHealth surveys must be kept short to reduce participant burden and encourage data collection compliance, they cannot capture the richness of individuals’ experiences of use contexts and practices, nor how individuals make sense of their drug use within the context of their broader life narratives. Integrating qualitative mapping methods with mHealth momentary assessements can provide reliable and ecologically valid measures of substance use behaviours while also revealing the richness of experiences and contexts of use. Qualitative mapping, also known as qualitative Geographic Information System (GIS), integrates mapping techniques with qualitative methods to explain the processes that produce spatial patterns, relationships, and behaviours (Elwood & Cope, 2009). It has been used in research on substance use, including to understand place-based practices and norms of tobacco use (McQuoid et al., 2019; Pearson et al., 2016), the impact of area restrictions on people who use drugs (McNeil, Cooper, Small, & Kerr, 2015), and characteristics of drug overdose contexts (Curtis, Felix, Mitchell, Ajayakumar & Kerndt, 2018).
Our mixed method approach leverages the “productive complementarity” of multiple methods, acknowledging that different ways of knowing about social phenomena, like drug use, are all inherently partial and are shaped by the conditions and actors involved in the creation of knowledge (Elwood, 2010, pp. 96–97). We integrate real-time, smartphone-collected surveys, location tracking, and subsequent in-depth interviews that are guided by viewing maps of participants’ own mHealth data in an explanatory sequential mixed methods approach (see McQuoid, Thrul, et al., 2018 for a detailed description of the method). Participants use a smartphone app for a period of time (e.g., 30 days) to report on the substances they used and the situations they used them in via participant-initiated real-time reports of use, prompted momentary surveys about use and non-use situations, and prompted daily diary surveys. The real-time reports and prompted surveys collected multiple choice responses with write-in options. Subsequently, real-time reports of use and location tracking data are visualized in mapping software and brought into in-depth interviews to guide and ground discussion of drug use experiences within everyday contexts and situations of use. The interviewer and/or participant toggle between map layers and zoomed in and out of places in Google Earth. Together, they identify apparent spatial clusters of use of different substances and discuss what those places are, what they usually do and experience there, who they interact with, and how it is that use of particular substances fold into those experiences. This is similar to the use of travel and activity diaries to guide interviews, but further ‘grounds’ interview discussion by interacting with spatially-visualized representations of participant data. Quantitative and qualitative data are analysed separately and then integrated in a table. Visually organizing and juxtaposing the quantitative and qualitative data sets helps to identify threads of interest to explore across the data sets and to observe the convergence, complementarity, and/or dissonance (O’Cathain, Murphy, & Nicholl, 2010) between their depictions of participant’s everyday use of and experiences with substance use.
We collected data in 2019–2020 with 32 young adults in California who regularly used both tobacco and cannabis with the mixed method (University of California, San Francisco Institutional Review Board #13-11907) (McQuoid, Thrul, Lopez, & Ling, 2020). We draw from that study on tobacco and cannabis use to explore one participant’s data, which provided particularly informative insights into the complex patterns, intentions, and socio-structural contexts of multiple drug use repertoires and combinations. IRB approval included consent to publish the data as a case study. The participant did not respond to our request for feedback on the manuscript. To protect the participant’s identity, we use a pseudonym and have added fictional details about the participant that are not relevant to interpreting the data presented below. mHealth data were descriptively analysed using STATA statistical analysis software. Transcript analysis followed an inductive-deductive thematic approach (Bradley, Curry, & Devers, 2007). Transcripts were coded with NVIVO qualitative data analysis software. The initial transcript coding scheme was informed by our previous studies and the literature (e.g., Hakkarainen et al., 2019; McQuoid, Keamy-Minor, & Ling, 2018; McQuoid et al., 2019) and was used to sort content by substance type, location, social identity, and roles/intensions of use. Emergent themes regarding roles and intensions of use were identified in a series of group readings of transcript excerpts, as we have done in the past (McQuoid, Keamy-Minor, et al., 2018).
Findings: Patterns, intentions, and contexts of multiple drug use
‘Jason’ (T044) was a transgender man in his mid-twenties who lived in a rural community, had a history of homelessness, and reported having autism spectrum disorder (ASD). He worked part-time in constrution and lived with his partner in a small house. Jason completed 70% of all prompted surveys during his 30 days of data collection. Jason’s mHealth survey data indicated that he smoked a daily average of 6.5 cigarettes. He most often smoked alone, and frequently smoked at home, in a vehicle, or at someone else’s home. On the minority of occasions that he smoked cigarettes with others, it was usually with friends or his partner.
Jason’s mHealth survey data indicated that he used cannabis almost every day (28/30 days); 4.9 times per day, on average. He frequently used cannabis in his garage or backyard, someone else’s home, or in a vehicle. He was with friends or his partner during most of these sessions (58%), and was alone for the rest. On most days of the study (25/30 days) he reported using cannabis and cigarettes together some or most of the time. He used alcohol on only 15 days and most of those reports were for one drink. On only 5 days did he report using alcohol and cigarettes together some or most of the time. In short, Jason’s mobile data indicated that he used cigarettes and cannabis daily or almost daily, less regularly used alcohol, and that he often used cigarettes and cannabis at the same time.
The qualitative mapping interview elicited rich descriptions of the experiences, contexts, and intentions linked to these and other substances in Jason’s everyday life. Jason’s account of his drug use repertoire and combinations converged with the quantitative sketch made by his mHealth survey data, and complemented it by providing insight into the place-based experiences and intentions behind his use of these substances. The map provides a zoomed in view of Jason’s use around his home and nearby friend’s house (Map 1). He described his alcohol use as mostly related to accompanying a friend at their house while they drank. In contrast, his cannabis dab pen went everywhere with him beyond this home area to help navigate social interactions as a person with ASD. He described cannabis as helping him “get on the same mental level” as others so that he could better interpret their meaning:
Map 1:
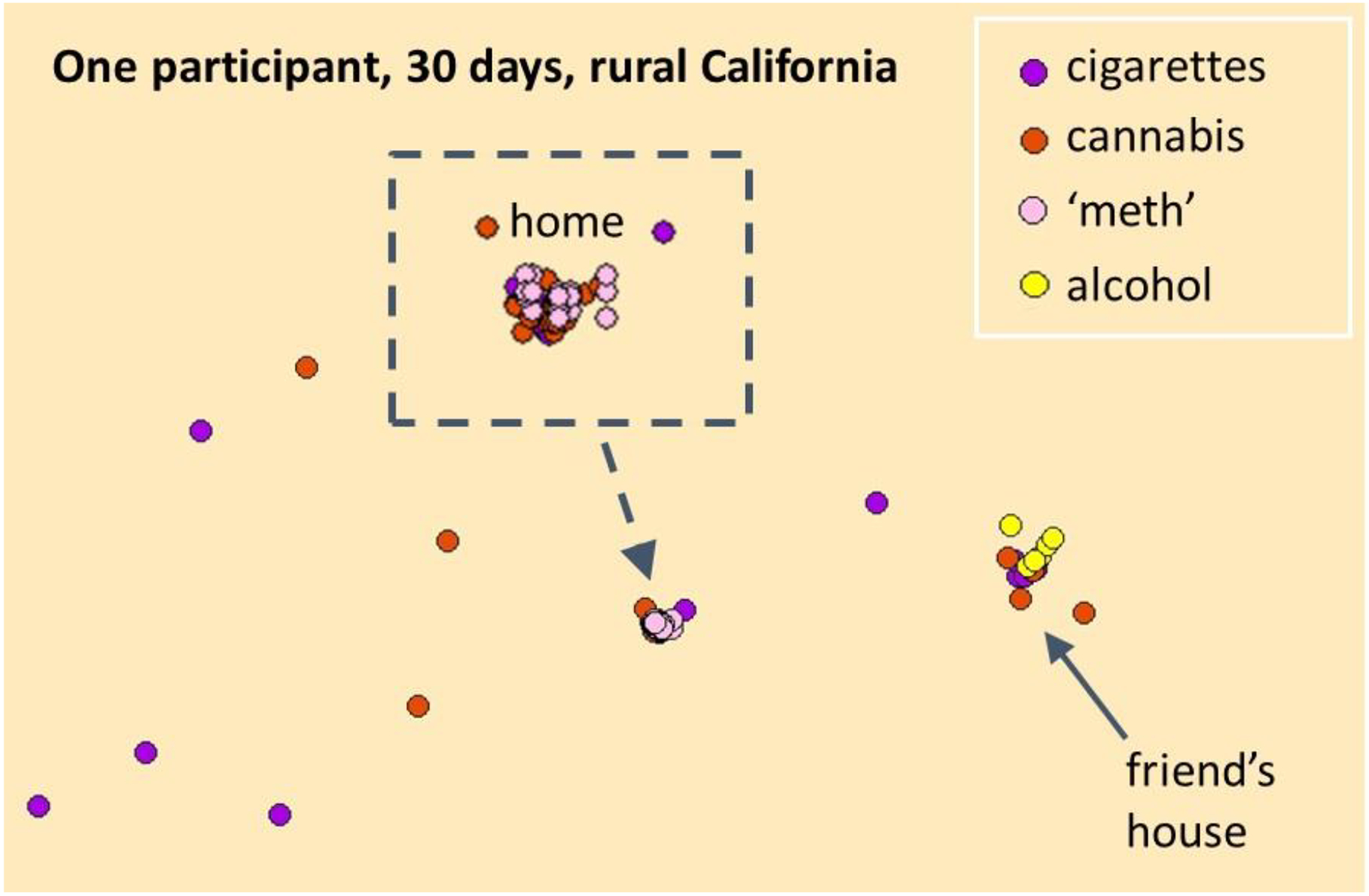
This anonymized map visualizes a zoomed in view on 30 days of Jason’s multiple drug use reports. The interview revealed complementary roles of different substances in navigating life as a transgender person with autism in a rural community.
[I’m] on the other side of a big thick piece of Plexiglas. Like I can see them, I can wave at them. I’m like hey what’s up, but I can’t hear a thing. […] Marijuana kind of makes that Plexiglas kind of go into like more like a fog.
While viewing and interpreting his data maps with the first author, Jason explained that his cigarette and cannabis use reports were highly co-located because he ‘chased’ cannabis with cigarettes to moderate intoxication and produce a pleasurable flavour combination: “It’s a nice little end cap, especially if I smoke a little too much weed.” The co-location of cannabis and tobacco is not apparent in the zoomed in view provided in Map 1. He also described cigarette smoking as related to coping with the acute stress of being repeatedly misgendered by the same people in his life:
It almost feels like someone’s squeezing the centre of my chest and just like crushing my spirit […] I get all like anxious and I just get this anxiety that just builds and I’m like I need a fucking cigarette.
When Jason shared that he also regularly injected methamphetamine, the first author asked him to describe where and how frequently he did, and to imagine a ‘methamphetamine map’ with her. Map 1 shows Jason’s real-time cannabis and cigarette reports around his home and visualizes his methamphetamine and alcohol use as if they were real-time reports. Jason first tried methamphetamine at age 18 when he was homeless, but continued using it because it helped manage his relationship to his body, which he feels would be improved with hormone therapy:
For me [methamphetamine] definitely helps with more the body dysmorphia. […] It helps me definitely feel more like I’m in control of my body.
Jason has found it difficult to access hormone therapy as a transgender person. He met with four different doctors, but none would help:
I finally just gave up. Trying to get services like that up north [in rural areas] is even harder.
Jason almost exclusively uses methamphetamine at the end of his morning routine at home as he gets ready for his work day. This consists of drinking coffee, then using cannabis, and then capping with a cigarette. Jason’s data offered glimpses into the dynamics between different substances within his drug use repertoire. Rather than occurring in isolation, his cigarette use was motivated by its role in calibrating the intoxicating effects of cannabis, which he finds crucial for managing social interactions as a person with ASD, and helped cope with the acute stress of being misgendered. Moreover, Jason’s use of methamphetamine cannot be solely attributed to addiction, but also to his efforts to manage his experience of body dysmorphia as a transgender person living in a rural area with low access to transgender health services.
Discussion and conclusions
This one individual’s mHealth and map-led interview data offered an integrated understanding of the complex use patterns, combinations, and intentions within his drug use repertoire (Hakkarainen et al., 2019; Kataja et al., 2018), and linked these to his intersecting identities and the particular social and structural characteristics of his environment. Specifically, it revealed relationships between how and why he uses multiple drugs and his day-to-day experiences as a transgender person with ASD living in a rural community. A key strength of this mixed method appears to be its capacity to go beyond examination of individual substances and individual drug use ‘risk factors’, to link use patterns and intentions of multiple drugs to the intersecting characteristics and place-based experiences of different people. The perspective offered by integrating mHealth and qualitative mapping methods may help identify particular drug use patterns and combinations (e.g., Santa Maria et al., 2017) that increase risk of drug-related harm for priority groups, like gender minority individuals, as well as provide insight into the place-embedded experiences that give rise to motives for those ‘risky’ drug use practices (e.g., Curtis et al., 2018).
Our findings suggest that participant narratives of multiple drug use patterns, intentions, and experiences can be enhanced and further grounded in context by viewing and discussing maps of participants’ own data during interviews. Maps that show where and how frequently participants use different drugs provide an avenue for the participant and interviewer to organize their discussion around the complexities and diverse factors related to multiple drug use. Moreover, similar to other creative methods that integrate images or other objects into interviews (Kara, 2015, p. 84), the visual representation of drug use practices in map form may help depersonalize highly stigmatized use practices, like methamphetamine use, and reinforce the participant’s role as expert while cultivating an experience of discovery, reflection, and ownership over the interpreted ‘story’ of their data. This mixed method is limited, however, by being time-consuming and resource-intensive, especially with regards to participant and investigator time effort, as well as obtaining the smartphone data collection software and mapping software. Participant burden must be considered when designing the frequency and length of smartphone-collected surveys, the duration of data collection (i.e., number of days), and participant incentives. Moreover, great care must be taken to protect participant confidentiality when using any geo-enabled data collection method. This method could be used with a larger sample size by grouping participants for comparison (e.g., by demographic characteristics or drug use repertoires) rather than at the individual case level, and triangulating between the quantitative and qualitative data for each group.
Future studies can build on research that has identified individual ‘risk factors’ related to multiple drug use (e.g., gender minority status; mental health), by gaining integrated and geographically-grounded insights into how these diverse and place-embedded factors intersect and interact with one another to shape drug use repertoires and combinations. In-depth knowledge like this can inform the resources and services directed toward and tailored to the needs of diverse groups of people who experience the unique pleasures, roles, and risks of multiple drug use.
Highlights.
The patterns, intentions, and contexts of multiple drug use are poorly understood
We integrated mobile health research methods with qualitative mapping interviews
Findings revealed intersecting, place-embedded factors shaping multiple drug use
This method can examine multiple drug use for priority groups in different settings
Acknowledgements
We are grateful to the participant whose data we presented in this brief report for his time and generosity in sharing his experiences, and to the anonymous reviewers for their helpful input. This work was funded by the California Tobacco-Related Disease Research Program (27IR-0042; T29FT0436), Oklahoma Tobacco Settlement Endowment Trust (TSET) Grant R21-02, and NCI Cancer Center Support Grant P30CA225520 awarded to the Stephenson Cancer Center.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosure of Interest: The authors report no conflict of interest.
Contributor Information
Julia McQuoid, TSET Health Promotion Research Center, Department of Preventive and Family Medicine, University of Oklahoma Health Sciences Center; Center for Tobacco Control Research and Education, University of California, San Francisco.
Johannes Thrul, Department of Mental Health Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA;; Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University, Baltimore, Maryland, USA; Centre for Alcohol Policy Research, La Trobe University, Melbourne, Australia
Kekoa Lopez-Paguyo, Center for Tobacco Control Research and Education, Department of Medicine, University of California, San Francisco and School of Public Health, University of California, Berkeley.
Pamela M. Ling, Center for Tobacco Control Research and Education and Division of General Internal Medicine, Department of Medicine, University of California, San Francisco
References
- Benotsch EG, Zimmerman R, Cathers L, McNulty S, Pierce J, Heck T, … Snipes D (2013). Non-medical use of prescription drugs, polysubstance use, and mental health in transgender adults. Drug and Alcohol Dependence, 132(1), 391–394. doi: 10.1016/j.drugalcdep.2013.02.027 [DOI] [PubMed] [Google Scholar]
- Boys A, Marsden J, Fountain J, Griffiths P, Stillwell G, & Strang J (1999). What Influences Young People’s Use of Drugs? A qualitative study of decision-making. Drugs: Education, Prevention and Policy, 6(3), 373–387. doi: 10.1080/09687639997052 [DOI] [Google Scholar]
- Bradley EH, Curry LA, & Devers KJ (2007). Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Services Research, 42(4), 1758–1772. doi: 10.1111/j.1475-6773.2006.00684.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis A, Felix C, Mitchell S, Ajayakumar J, & Kerndt PR (2018). Contextualizing Overdoses in Los Angeles’s Skid Row between 2014 and 2016 by Leveraging the Spatial Knowledge of the Marginalized as a Resource. Annals of the American Association of Geographers, 108(6), 1521–1536. doi: 10.1080/24694452.2018.1471386 [DOI] [Google Scholar]
- Elwood S (2010). Mixed methods: Thinking, doing, and asking in multiple ways (Vol. 1): Sage; Thousand Oaks, CA. [Google Scholar]
- Elwood S, & Cope M (2009). Introduction: Qualitative GIS: Forging mixed methods through representations, analytical innovations, and conceptual engagements. In Cope M & Elwood S (Eds.), Qualitative GIS: A Mixed Methods Approach (pp. 1–12). London: SAGE Publications Ltd. [Google Scholar]
- Ferguson SG, & Shiffman S (2011). Using the methods of ecological momentary assessment in substance dependence research—Smoking cessation as a case study. Substance Use & Misuse, 46(1), 87–95. doi: 10.3109/10826084.2011.521399 [DOI] [PubMed] [Google Scholar]
- Hakkarainen P, O’Gorman A, Lamy F, & Kataja K (2019). (Re)conceptualizing “polydrug use”: Capturing the complexity of combining substances. Contemporary Drug Problems, 46(4), 400–417. doi: 10.1177/0091450919884739 [DOI] [Google Scholar]
- Kara H (2015). Creative research methods in the social sciences: A practical guide. Bristol: Policy Press. [Google Scholar]
- Kataja K, Tigerstedt C, & Hakkarainen P (2018). More social research into polydrug use. Nordic Studies on Alcohol and Drugs, 35(6), 399–403. doi: 10.1177/1455072518807055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirchner TR, & Shiffman S (2016). Spatio-temporal determinants of mental health and well-being: Advances in geographically-explicit ecological momentary assessment (GEMA). Social Psychiatry and Psychiatric Epidemiology, 51(9), 1211–1223. doi: 10.1007/s00127-016-1277-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McNeil R, Cooper H, Small W, & Kerr T (2015). Area restrictions, risk, harm, and health care access among people who use drugs in Vancouver, Canada: A spatially oriented qualitative study. Health & Place, 35, 70–78. doi: 10.1016/j.healthplace.2015.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McQuoid J, Keamy-Minor E, & Ling PM (2018). A practice theory approach to understanding polytobacco use in the United States. Critical Public Health, 1–16. doi: 10.1080/09581596.2018.1541226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McQuoid J, Thrul J, & Ling P (2018). A geographically explicit ecological momentary assessment (GEMA) mixed method for understanding substance use. Social Science & Medicine, 202, 89–98. doi: 10.1016/j.socscimed.2018.02.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McQuoid J, Thrul J, Lopez K, & Ling PM (2020). Locating tobacco within poly-substance use landscapes: An mHealth, mapping-interview method for research with ‘high risk’ groups. Paper presented at the American Public Health Association Annual Meeting, San Francisco. Poster retrieved from [Google Scholar]
- McQuoid J, Thrul J, Ozer E, Ramo D, & Ling PM (2019). Tobacco use in the sexual borderlands: The smoking contexts and practices of bisexual young adults. Health & Place. doi: 10.1016/j.healthplace.2018.12.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mennis J, Mason MJ, & Cao Y (2013). Qualitative GIS and the visualization of narrative activity space data. Int J Geogr Inf Sci, 27. doi: 10.1080/13658816.2012.678362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Cathain A, Murphy E, & Nicholl J (2010). Three techniques for integrating data in mixed methods studies. BMJ, 341, c4587 doi: 10.1136/bmj.c4587 [DOI] [PubMed] [Google Scholar]
- Pearson JL, Smiley SL, Rubin LF, Anesetti-Rothermel A, Elmasry H, Davis M, … Abrams DB (2016). The Moment Study: Protocol for a mixed method observational cohort study of the Alternative Nicotine Delivery Systems (ANDS) initiation process among adult cigarette smokers. Bmj Open, 6(4), e011717. doi: 10.1136/bmjopen-2016-011717 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roth AM, Felsher M, Reed M, Goldshear JL, Truong Q, Garfein RS, & Simmons J (2017). Potential benefits of using ecological momentary assessment to study high-risk polydrug use. mHealth, 3, 46–46. doi: 10.21037/mhealth.2017.10.01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Santa Maria D, Padhye N, Yang Y, Gallardo K, Santos G-M, Jung J, & Businelle M (2017). Drug use patterns and predictors among homeless youth: results of an ecological momentary assessment. The American Journal of Drug and Alcohol Abuse, 1–10. doi: 10.1080/00952990.2017.1407328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valdez A, & Sifaneck SJ (2010). Qualitative methodological issues in drug user research. Substance Use & Misuse, 45(5), 645–647. doi: 10.3109/10826081003594708 [DOI] [PubMed] [Google Scholar]