

Abstract
Objective
To assess the use of Medicaid programs, including waivers, to address the needs of aging autistic individuals.
Data sources
We gathered data on Medicaid programs in place between 2004 and 2015 for 50 states and the District of Columbia from the Centers for Medicare and Medicaid Services website, by contacting state Medicaid administrators and advocacy groups, and by reviewing the Medicaid Analytic eXtract Waiver Crosswalk.
Study design
This retrospective analysis classified each Medicaid program and documented state changes over time in eligibility criteria: those serving autism spectrum disorder only, autism spectrum disorder or intellectual disability, and intellectual disability only.
Data collection/extraction methods
We captured age and diagnosis eligibility criteria for Medicaid programs serving any of the three target groups.
Principal findings
A total of 269 Medicaid programs met our criteria and most programs (51%) were 1915(c) waivers. The number of autism‐specific 1915(c) waivers grew more than fivefold during the study period, outpacing increases in waivers serving individuals with intellectual disability.
Conclusions
States varied in their use of Medicaid to address the needs of the aging autism population. Further study of characteristics of states that changed their Medicaid programs, and of the health care use and outcomes associated with these changes, are needed to identify opportunities to replicate effective approaches to meeting the needs of this population.
Keywords: disability, health care financing, health policy, Medicaid, program evaluation
What is already known on this topic
The number of individuals diagnosed with autism spectrum disorder (ASD) is increasing. Most will need services and supports throughout their lives.
Medicaid 1915(c) waivers are a policy mechanism that states frequently use to provide health care insurance to specific populations for targeted services.
What this study adds
States use a variety of Medicaid programs to enroll and serve individuals with ASD; the most common mechanism being the 1915(c) waiver authority.
Twenty‐six states changed their 1915(c) waiver programs to increase options for individuals with ASD.
Identifying state policy changes is the first step in comparing outcomes associated with varying approaches.
1. INTRODUCTION
Increasing access to health care improves health outcomes. 1 , 2 An effective health insurance program adjusts coverage to respond to emerging needs of the people it serves. Medicaid is the largest insurer in the United States, 3 and states have considerable flexibility in structuring their Medicaid programs. 4 For example, during the COVID‐19 pandemic, states have modified Medicaid copayment requirements 5 and amended waivers to increase access to care. 6
Medicaid home‐ and community‐based services (HCBS) are an important tool for serving individuals with disabilities in community settings. HCBS options include 1915(c) fee‐for‐service waivers, 1915(a) and 1915(b) managed care programs, 1915i and 1915k state plan amendments, and section 1115 demonstration initiatives. Average per enrollee spending in these programs is $30 000 per year, substantially more than expenditures in other health care programs. 7 In 2018, federal and state Medicaid spending on home and community‐based services totaled $92 billion, about 15.4% of the total Medicaid budget. 7
Most states have used 1915(c) waivers to customize and expand coverage for services for individuals with disabilities and the elderly. 8 , 9 , 10 , 11 , 12 In 2018, states averaged five active 1915(c) waivers 13 that provided community‐based services. Most have been used for decades to provide community‐based support to people with intellectual and developmental disabilities (ID/DD). 7 , 8 , 14 , 15 This coverage is typically not available through private insurance or Medicare. 13
Over the last two decades, many states have changed their Medicaid programs 11 in response to the 30‐fold increase in the reported prevalence 16 , 17 , 18 , 19 , 20 in addition to reported needs across the lifespan 21 , 22 of autistic individuals, often by using waivers. Studies have found that waivers ameliorate health disparities among autistic children from underserved and underrepresented groups, 23 reduce parent workforce engagement barriers, 11 and improve children's quality of life and clinical trajectory. 24
Research to date has not specifically described these programs, has been cross‐sectional, and has not included adults. 8 , 10 , 14 We addressed this gap by documenting the frequency of Medicaid programs and specifically ASD‐related 1915(c) waivers that target different age groups and to assess patterns of change over time.
2. METHODS
2.1. Study sample and data sources
We identified Medicaid programs in all 50 states and the District of Columbia from 2004 to 2015 using information from state websites and the Centers for Medicare and Medicaid Services. These programs included 1915(a), (b), and (c) waivers/programs, 1915i and 1915k state plan amendments, and Section 1115 demonstration programs. Because 1915(c) waivers are the most commonly occurring and can serve individuals with ASD as a separate group or jointly with individuals with ID, we identified waivers specified for an ASD diagnosis only, ASD or ID diagnoses, or an ID diagnosis only, with the ID only waivers serving as a comparison group. We gathered data on state Medicaid 1915(c) waiver applications for 2004 to 2015 from the Centers for Medicare and Medicaid Services website, by contacting state Medicaid administrators and advocacy groups directly, and by reviewing the Medicaid Analytic eXtract (MAX) Waiver Crosswalk, which began in 2005 and lists all Medicaid waivers by state. This approach ensured that we captured all active waivers from the study period.
2.2. Procedures
The prevalence of individuals with ASD or ID for each state was calculated using the state population from the 2010 U.S. Census and the most recent ASD and ID prevalence rates produced by the Centers for Disease Control and Prevention (CDC). 25 The number of individuals with ASD or ID that could be served for 1915(b) and 1915(c) Medicaid programs was totaled using Appendix B. Participant Access and Eligibility, B‐3. Number of individuals served from Medicaid waiver applications. Medicaid 1915(a), 1915i, and 1915k are state plan amendments allowing eligible residents to qualify, instead of limiting to a predefined program capacity.
Research staff reviewed diagnostic eligibility criteria listed in each 1915(c) waiver application and classified the waiver into one of three categories: (a) requires an ASD diagnosis (ASD only), (b) requires an ASD or ID diagnosis (ASD/ID), or (c) requires an ID diagnosis (ID only). We also recorded age eligibility requirements. Next, we contacted Medicaid waiver administrators and Protection and Advocacy Systems (P&A) from each state to verify the waiver classifications. P&As are non‐federal entities that help to protect the rights of individuals with disabilities and have expertise in and historical knowledge of relevant state and federal supports for individuals with disabilities. 26
We assigned states to one of four baseline categories, based on 2004 1915(c) waiver status: (a) had an ASD‐specific Medicaid 1915(c) waiver, (b) had an ASD/ID Medicaid 1915(c) waiver, (c) had an ID‐specific Medicaid 1915(c) waiver, and (d) had no Medicaid 1915(c) waiver serving ASD or ID. Because states could have more than one waiver, and a single waiver could fit multiple categories, we assigned state status with priority to the ASD‐specific program. Next, we categorized states based on changes to waiver programs during the study period, using the same hierarchy of rankings based on the most ASD‐specific program available. Each waiver was grouped based on its eligible age groups: children (age 10 and under), children and adolescents (ages 0‐21), adolescents and adults (age 12 and older), adults only (age 18 and older), or no age limits.
2.3. Analysis
We calculated the proportion of the state ASD/ID population that Medicaid 1915(b) or (c) waivers could serve based on program capacity and state population. We constructed Sankey diagrams using the ggplot2‐ggalluvial package in R to visualize changes over time, where the flow between nodes summarized changes in Medicaid 1915(c) waiver composition within each state or changes in eligibility criteria by waiver (Figure S1). Using Tableau, we constructed a hex map of state status in 2015 to visualize how waiver changes were distributed. A table displaying changes in the proportion of waivers by age group served in 2004 compared to 2015 is provided in Figure S2. The Institutional Review Board of Drexel University approved this study.
3. RESULTS
The most common type of Medicaid program (51%) was Medicaid 1915(c) waivers, followed by 1115 demonstration projects (21%), and 1915(b) managed care waivers (17%). Medicaid 1915(a) and 1915i programs comprised the smallest proportion (6% and 5% respectively). On average, states could serve 4% of the ASD/ID population through Medicaid 1915(b) or 1915(c) waivers (Figure 1). Wisconsin could serve one in five individuals with ASD/ID, followed by Minnesota (14%). All other states could serve <10% of the ASD/ID population through their 1915(b) or 1915(c) waivers.
FIGURE 1.
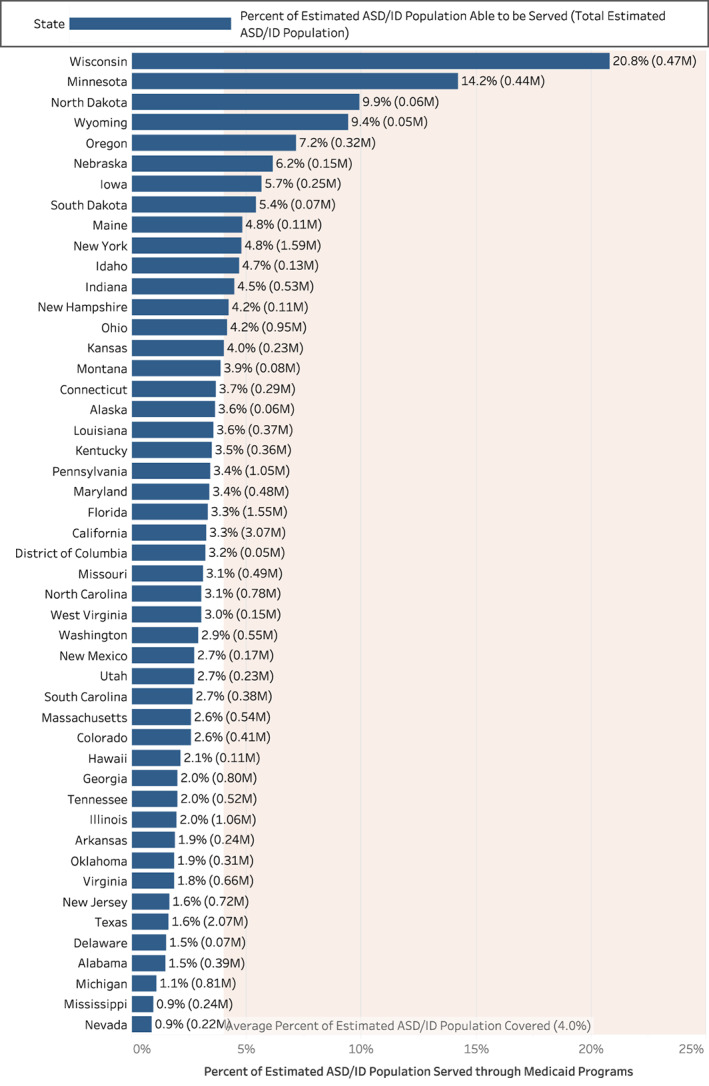
Proportion of the state ASD/ID population that Medicaid 1915(a) or (c) within capacity, 2010. ASD, autism spectrum disorder; ID, intellectual disability; Arizona, Vermont, and Rhode Island did not have any waivers during the study period [Color figure can be viewed at wileyonlinelibrary.com]
Among 1915(c) waivers, 135 were active during the study period. Three states (Arizona, Rhode Island, and Vermont) operated no Medicaid 1915(c) waivers during this time but all three had 1115 demonstration projects that served individuals with ASD or ID. In 2004, three states had ASD‐specific waivers, and 30 states had ASD/ID waivers. Eleven had ID‐specific waivers.
During the study period, 21 states made no changes. Nine added ASD‐specific waivers; by 2015, 12 states had ASD‐specific Medicaid 1915(c) waivers (Figure 2). Most ASD‐specific waivers were generated by states that already had an ASD/ID waiver; about one in three states with an ASD/ID waiver added an ASD/ID waiver. No states with an ASD‐specific waiver added another. Few states with an ID‐specific waiver added an ASD‐specific waiver or an ASD/ID waiver. Of the seven states with no waiver at the start of the study period, three made no change and four either added an ASD‐specific waiver (two states) or an ASD/ID waiver (two states).
FIGURE 2.
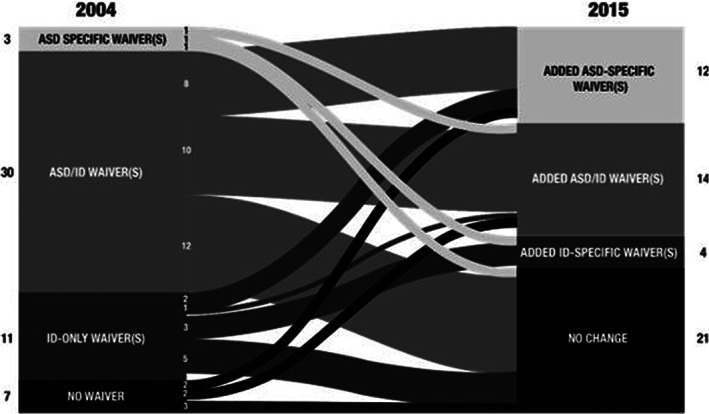
States that made Medicaid 1915(c) waiver changes from 2004 to 2015, by waiver eligibility type. Numbers at the left indicate the number of states in each designated category at baseline in 2004; numbers to the right indicate the number of states in each category in 2015. ASD, autism spectrum disorder; ID, intellectual disability
States that implemented new ASD‐specific waivers (Figure 3) were spread across the country, with a cluster in central and southwest United States. Among the 10 states with the largest populations, only Pennsylvania added an ASD‐specific waiver; New York and Illinois added an ASD/ID waiver; and three (California, Florida, and Texas) made no change to their ASD‐specific, ASD/ID, or ID‐specific waivers.
FIGURE 3.
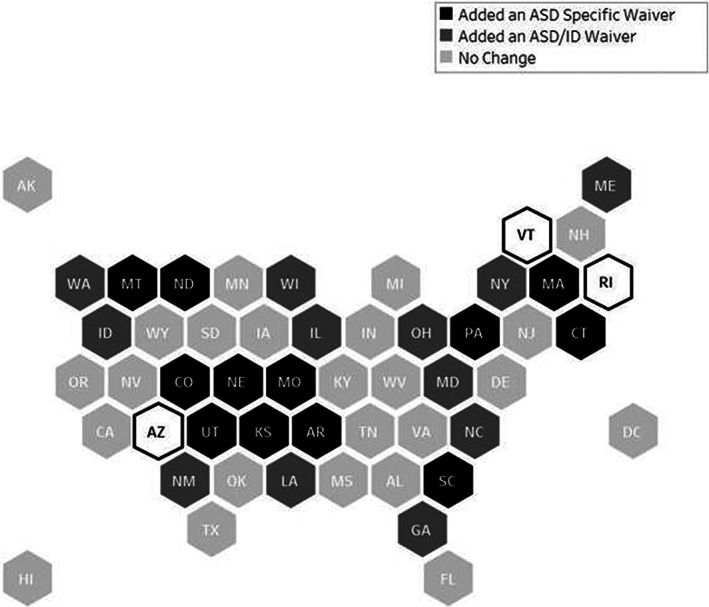
Changes in ASD‐related 1915(c) waivers by state, 2004 to 2015. ASD, autism spectrum disorder; ID, intellectual disability; Arizona, Vermont, and Rhode Island did not have any waivers during the study period
The proportion of the 1351915(c) waivers that served people with ASD/ID remained stable across all age groups from 2004 to 2015. The number of ASD‐specific waivers serving only children increased from zero in 2004 to nine in 2015. The number of ASD‐specific waivers serving children and adolescents increased from one to three. The number of waivers that were ASD‐specific did not change during the study period but represented a decreasing proportion of total waivers (67% in 2004 to 13% in 2015). At the start of the study, there were no ASD‐specific waivers serving adults only; one was created during the study period. The proportion of ID‐specific waivers serving children, adolescents, and adults, and adults only did not change. There were small decreases in the number of ID‐specific waivers serving children and adolescents only (four to two) and an increase from 14 to 19 ID‐specific waivers serving the lifespan.
4. DISCUSSION
This analysis shows how different states have used Medicaid programs, and specifically 1915(c) waivers to respond to the emerging needs of autistic individuals. We found that Medicaid 1915(c) waivers were the most common waiver type used to deliver services to individuals with ASD or ID. Although the use of these waivers increased nationally, most individual states implemented no waiver changes between 2004 and 2015 despite the increase in individuals needing services. Although two‐thirds of states had a waiver serving individuals with ASD in 2004, only three had ASD‐specific waivers. Both ASD‐specific waivers and waivers that added ASD eligibility on to other programs increased over the study period, which demonstrates movement towards increased pathways to access to services for autistic individuals through Medicaid. Most new ASD‐specific waivers were for children only, however, suggesting that states are crafting policy responses that align with public health and advocacy messaging around early detection but may be less focused on adults.
ASD/ID waivers may be well poised to serve individuals with either ASD, ID or both diagnosis, although further research is needed to understand program differences. It is also critical to consider that ASD/ID waivers use functional eligibility requirements or IQ requirements that may affect the eligibility of individuals on the spectrum who do not have a co‐occurring ID diagnosis. The population of adolescents with ASD will continue to present with service needs, 21 , 22 and it is unclear if the uptick in ASD/ID waivers will result in the lifelong supports individuals with ASD need, or if there will be a change in outcomes as they shift from ASD‐specific to ASD/ID programs over time. Studies have found that adults on the spectrum often lack access to needed services and supports after education entitlements end, 15 , 27 and Medicaid 1915(c) waivers may represent a critical yet underused opportunity to create programming that includes autistic individuals as they age, though this would depend on the functional level of care requirements of the 1915(c) waivers. It is possible that state Medicaid program changes through other mechanisms may have included autistic individuals or their families, such as increasing access to Medicaid via Medicaid expansion or through enrollment in ID‐specific programs because of a co‐occurring ID diagnosis. However, Medicaid expansion would only allow access to services available through the state plan and would likely not include the robust array of home and community‐based services and supports available through Medicaid 1915(c) waivers.
Further research is needed to compare access, service use, and outcomes among autistic individuals in states that modified their 1915(c) waivers and those that did not. For example, if individuals in states without increased access were less likely to receive services and supports that may prevent crises, those states might have seen increased use of emergency care. Autistic adults have an increased risk for emergency department use and hospitalization, 28 and these services are a tremendous driver of health care costs. 29 At the same time, states with more generous home and community‐based service (HCBS) eligibility (the proportion of HCBS receipt among users of long term services and supports, or LTSS) have lower hospitalization rates and lower rates of potentially avoidable hospitalizations among other populations. 30 Future research should examine how changes in eligibility criteria and Medicaid programs have impact autistic individuals specifically, as well as to compare them to other populations to identify if changes are keeping pace with need.
It is noteworthy that one in four states that implemented new ASD‐specific waivers are home to CDC‐funded Autism and Developmental Disability Monitoring (ADDM) network sites, which surveil ASD prevalence. The additional data and political capital that come from these initiatives may propel increases in ASD‐specific programming. Research on waiver implementation within states has demonstrated that framing the purpose of waivers is essential in their passage and implementation. 31 A better understanding of state or local factors that have contributed to ASD or other disease/diagnosis‐specific program passage and implementation may explain the variability we observed.
Interactions between state education and Medicaid systems may further explain how and why Medicaid programs have changed to support children with ASD. In 2014, the Centers for Medicare & Medicaid Service (CMS) issued guidance that states should cover autism services through Early and Periodic Screening, Detection, and Treatment (EPSDT). 32 This directive defined the types of autism services Medicaid programs could provide, including respite and home/vehicle adaptations that are not EPSDT mandated. 32 The CMS directive redefined the interaction between EPSDT and Medicaid programs such as 1915(c) waivers by broadening the entitlement to services for children on the autism spectrum under ESPDT. 32 This shift limits if and how states maintain or create new ASD‐specific waivers or add ASD to ID‐specific waivers after 2014 that serve children and adolescents by presuming the responsibility for many services should covered by EPSDT. 32 Continued research to more fully quantify the impact of this directive on state program formation is needed given the critical interplay between these systems, since children spend a substantial portion of their time in schools and given the mandate that Medicaid is the payer of last resort.
Our analysis is limited by the ways that Medicaid programs and waivers are structured and implemented. First, eligibility criteria vary considerably by state, especially functional eligibility requirements. 13 Second, there is a difference between availability of waivers and access. 13 In 2013, all states used some form of a cost control measure across functional limitation requirements, enrollment caps, or waiting lists. 33 In 2018, three‐quarters of states with ASD/ID waivers had waiting lists, representing nearly 820 000 people. We present Medicaid programs organized by diagnostic criteria for eligibility, and comparing ASD to ID is useful since they share a lifespan trajectory and are primarily supported through behavioral interventions. However, research has indicated that an unclear proportion of the ASD population increase may be countered by decreases in the prevalence of other diagnoses, including ID. 34 The most recent research from the CDC ADDM Network indicates that one in three children with ASD also have ID. 35 The co‐occurrence of these conditions, especially among adults, warrants further study and would aid in policy recommendations for eligibility criteria for the development of Medicaid programs. Finally, we did not examine waiver quality, as it is not measured consistently and there is no standardized requirement for doing so. 13
Identifying factors that generated new access options for autistic individuals may help other states develop policy that addresses the needs of autistic individuals. Because autism is a spectrum disorder, presenting with wide array of needs that that may or may not present in an individual having a co‐occurring ID, we believe that programming, through any multitude of Medicaid financing mechanisms, designed specifically for the ASD population with provider training requirements and services packages anchored in an evidence base is an optimal direction to serve this population. One also could use this process to explore the use of 1915(c) and other waiver authorities, like 1115 demonstration projects, for other public health issues including substance use disorders, traumatic brain injury, as well as emerging needs such as the COVID‐19 pandemic. 36 As the Medicaid system continues to innovate and consider novel mechanisms such as work requirements and health savings accounts, 37 establishing a baseline for comparison regarding how Medicaid is used to provide coverage will be critical for identifying new policies and practices and testing their impact.
Supporting information
Supplemental Figure S1 Total number of 1915(c) Waivers Meeting Specific Eligibility Criteria, 2004 to 2015
Where the flow between nodes summarized changes in Medicaid 1915(c) waiver composition within each state or changes in eligibility criteria by waiver (Supplemental Figure S1).
{kind=link}
Supplemental Figure S2 Trends in state 1915(c) waiver changes by eligibility age range from 2004
A table displaying changes in the proportion of waivers by age group served in 2004 compared to 2015 is provided in Supplemental Figure S2.
{kind=link}
Shea LL, Koffer Miller KH, Verstreate K, Tao S, Mandell D. States' use of Medicaid to meet the needs of autistic individuals. Health Serv Res. 2021;56(6):1207–1214. 10.1111/1475-6773.13671
[Correction added on 16 July 2021, after first online publication: The title has been updated in this version.]
Funding information National Institute of Mental Health, Grant/Award Number: 5R01MH117653
REFERENCES
- 1. Freeman JD, Kadiyala S, Bell JF, Martin DP. The causal effect of health insurance on utilization and outcomes in adults: a systematic review of US studies. Med Care. 2008;46(10):1023‐1032. 10.1097/MLR.0b013e318185c913. [DOI] [PubMed] [Google Scholar]
- 2. Gaudette É, Pauley GC, Zissimopoulos JM. Lifetime consequences of early‐life and midlife access to health insurance: a review. Med Care Res Rev. 2018;75(6):655‐720. 10.1177/1077558717740444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. The Commonwealth Fund . What is Medicaid's value? https://onlinelibrary.wiley.com/journal/14756773. Accessed November 6, 2020.
- 4. Center on Budget and Policy Priorities . Policy basics: Introduction to Medicaid. https://www.cbpp.org/research/health/policy‐basics‐introduction‐to‐medicaid. Accessed November 6, 2020.
- 5. The National Academy for State Health Policy (NASHP) . State Medicaid and CHIP strategies to protect coverage during COVID‐19. https://www.nashp.org/state-medicaid-and-chip-strategies-to-protect-coverage-during-covid-19/. Accessed November 6, 2020.
- 6. The National Academy for State Health Policy (NASHP) . States use appendix K and emergency waivers to support home‐ and community‐based services in response to COVID‐19. https://www.nashp.org/states‐use‐appendix‐k‐waivers‐to‐support‐home‐and‐community‐based‐services‐in‐response‐to‐covid‐19/. Accessed November 6, 2020.
- 7. Watts M, Musumeci M, Chidambaram P. Medicaid Home and Community‐Based Services Enrollment and Spending. Kaiser Family Foundation; 2020.
- 8. Rizzolo MC, Friedman C, Lulinski‐Norris A, Braddock D. Home and community based services (HCBS) waivers: a nationwide study of the states. Intellect Dev Disabil. 2013;51(1):1‐21. 10.1352/1934-9556-51.01.001. [DOI] [PubMed] [Google Scholar]
- 9. O'Keeffe J, Saucier P, Jackson B, et al. Understanding Medicaid home and community services: A primer; 2010. https://aspe.hhs.gov/report/understanding-medicaid-home-and-community-services-primer-2010-edition
- 10. Velott DL, Agbese E, Mandell D, et al. Medicaid 1915(c) home‐ and community‐based services waivers for children with autism spectrum disorder. Autism. 2016;20(4):473‐482. 10.1177/1362361315590806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Leslie DL, Iskandarani K, Velott DL, et al. Medicaid waivers targeting children with autism spectrum disorder reduce the need for parents to stop working. Health Aff (Millwood). 2017;36(2):282‐288. 10.1377/hlthaff.2016.1136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Leslie DL, Iskandarani K, Dick AW, et al. The effects of Medicaid home and community‐based services waivers on unmet needs among children with autism spectrum disorder. Med Care. 2017;55(1):57‐63. 10.1097/MLR.0000000000000621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Musumeci M, O'Malley Watts M, Chidambaram P. Key State Policy Choices about Medicaid Home and Community‐Based Services. Kaiser Family Foundation; 2020.
- 14. Hall‐Lande J, Hewitt A, Mosely CR. Policy research brief: A National Review of Home and Community Based Services (HCBS) for individuals with autism spectrum disorders. Vol. 21; 2011.
- 15. Turcotte P, Mathew M, Shea LL, Brusilovskiy E, Nonnemacher SL. Service needs across the lifespan for individuals with autism. J Autism Dev Disord. 2016;46(7):2480‐2489. 10.1007/s10803-016-2787-4. [DOI] [PubMed] [Google Scholar]
- 16. Baio J, Wiggins L, Christensen DL, et al. Prevalence of autism spectrum disorder among children aged 8 years — Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. Morb Mortal Wkly Rep. (MMWR). 2018;67(No. SS‐6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Rutter M. Aetiology of autism: findings and questions. J Intellect Disabil Res. 2005;49(Pt 4):231‐238. 10.1111/j.1365-2788.2005.00676.x. [DOI] [PubMed] [Google Scholar]
- 18. Billstedt E, Gillberg IC, Gillberg C. Autism after adolescence: population‐based 13‐ to 22‐year follow‐up study of 120 individuals with autism diagnosed in childhood. J Autism Dev Disord. 2005;35(3):351‐360. [DOI] [PubMed] [Google Scholar]
- 19. Christensen DL, Baio J, Van Naarden Braun K, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 Years–Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2012. MMWR Surveill Summ. Apr 2016;65(3):1‐23. 10.15585/mmwr.ss6503a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators, Centers for Disease Control and Prevention (CDC) . Prevalence of autism spectrum disorder among children aged 8 years ‐ Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. MMWR Surveill Summ. Mar. 2014;63(2):1‐21. [PubMed] [Google Scholar]
- 21. Dudley KM, Klinger MR, Meyer A, Powell P, Klinger LG. Understanding service usage and needs for adults with ASD: the importance of living situation. J Autism Dev Disord. 2019;49(2):556‐568. 10.1007/s10803-018-3729-0. [DOI] [PubMed] [Google Scholar]
- 22. Simonoff E, Kent R, Stringer D, et al. Trajectories in symptoms of autism and cognitive ability in autism from childhood to adult life: findings from a longitudinal epidemiological cohort. J Am Acad Child Adolesc Psychiatry. 2020;59(12):1342‐1352. 10.1016/j.jaac.2019.11.020. [DOI] [PubMed] [Google Scholar]
- 23. LaClair M, Mandell DS, Dick AW, Iskandarani K, Stein BD, Leslie DL. The effect of Medicaid waivers on ameliorating racial/ethnic disparities among children with autism. Health Serv Res. 2019;54(4):912‐919. 10.1111/1475-6773.13176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Eskow KG, Chasson GS, Summers JA. The role of choice and control in the impact of autism waiver services on family quality of life and child progress. J Autism Dev Disord. 2019;49(5):2035‐2048. 10.1007/s10803-019-03886-5. [DOI] [PubMed] [Google Scholar]
- 25. Centers for Disease Control and Prevention (CDC) . Research on developmental disabilities. https://www.cdc.gov/ncbddd/developmentaldisabilities/research.html. Accessed November 6, 2020.
- 26. Administration for Community Living (ACL) . State protection & advocacy systems. https://acl.gov/programs/aging‐and‐disability‐networks/state‐protection‐advocacy‐systems. Accessed 19 February, 2020.
- 27. Shattuck PT, Roux AM, Hudson LE, Taylor JL, Maenner MJ, Trani JF. Services for adults with an autism spectrum disorder. Can J Psychiatry. 2012;57(5):284‐291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Vohra R, Madhavan S, Sambamoorthi U. Comorbidity prevalence, healthcare utilization, and expenditures of Medicaid enrolled adults with autism spectrum disorders. Autism. 2017;21(8):995‐1009. 10.1177/1362361316665222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Lokhandwala T, Khanna R, West‐Strum D. Hospitalization burden among individuals with autism. J Autism Dev Disord. 2012;42(1):95‐104. 10.1007/s10803-011-1217-x. [DOI] [PubMed] [Google Scholar]
- 30. Segelman M, Intrator O, Li Y, Mukamel D, Temkin‐Greener H. Variations in HCBS spending, use, and hospitalizations among Medicaid 1915(c) waiver enrollees. World Med Health Policy. 2019;11(3):213‐247. [Google Scholar]
- 31. Grogan CM, Singer PM, Jones DK. Rhetoric and reform in waiver states. J Health Polit Policy Law. 2017;42(2):247‐284. 10.1215/03616878-3766719. [DOI] [PubMed] [Google Scholar]
- 32. Mann C. Clarification of Medicaid coverage of services to children with autism. Centers for Medicare & Medicaid Services (CMS). https://www.medicaid.gov/federal‐policy‐guidance/downloads/cib‐07‐07‐14.pdf. Accessed 8 February 2021.
- 33. Ng T, Stone J, Harrington C. Medicaid home and community‐based services: how consumer access is restricted by state policies. J Aging Soc Policy. 2015;27(1):21‐46. 10.1080/08959420.2015.969078. [DOI] [PubMed] [Google Scholar]
- 34. Shattuck PT. The contribution of diagnostic substitution to the growing administrative prevalence of autism in US special education. Pediatrics. 2006;117(4):1028‐1037. 10.1542/peds.2005-1516. [DOI] [PubMed] [Google Scholar]
- 35. Maenner M. Prevalence of autism Spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2016. MMWR Surveill Summ. 2020;69(4):1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Kaiser Family Foundation . Medicaid emergency authority tracker: Approved state actions to address COVID‐19. https://www.kff.org/coronavirus‐covid‐19/issue‐brief/medicaid‐emergency‐authority‐tracker‐approved‐state‐actions‐to‐address‐covid‐19/. Accessed May 21, 2020.
- 37. Sommers BD, Fry CE, Blendon RJ, Epstein AM. New approaches in Medicaid: work requirements, health savings accounts, and health care access. Health Aff (Millwood). 2018;37(7):1099‐1108. 10.1377/hlthaff.2018.0331. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Figure S1 Total number of 1915(c) Waivers Meeting Specific Eligibility Criteria, 2004 to 2015
Where the flow between nodes summarized changes in Medicaid 1915(c) waiver composition within each state or changes in eligibility criteria by waiver (Supplemental Figure S1).
Supplemental Figure S2 Trends in state 1915(c) waiver changes by eligibility age range from 2004
A table displaying changes in the proportion of waivers by age group served in 2004 compared to 2015 is provided in Supplemental Figure S2.