

Key Points
Question
How common are new and co-occurring medical, cognitive, or psychological diagnoses, new nursing care dependency, and postacute mortality among individuals who survive sepsis?
Findings
In this cohort study of 116 507 survivors of hospital-treated sepsis in Germany, nearly three-quarters had new medical, cognitive, or psychological diagnoses; nearly one-third were newly dependent on nursing care; and more than of 3 in 10 died in first year post sepsis. New diagnoses co-occurred in one-quarter of participants and affected sepsis survivors irrespective of preexisting diagnoses, sepsis severity, and intensive care unit treatment.
Meaning
These findings suggest that postsepsis morbidity may be more common and severe than previously believed, calling for increased efforts to prevent and treat the sequelae of severe infections.
This cohort study evaluates the frequency and co-occurrence of new diagnoses consistent with postsepsis morbidity and mortality as well as new nursing care dependency and total health care costs after sepsis.
Abstract
Importance
Sepsis survivorship is associated with postsepsis morbidity, but epidemiological data from population-based cohorts are lacking.
Objective
To quantify the frequency and co-occurrence of new diagnoses consistent with postsepsis morbidity and mortality as well as new nursing care dependency and total health care costs after sepsis.
Design, Setting, and Participants
This retrospective cohort study based on nationwide health claims data included a population-based cohort of 23.0 million beneficiaries of a large German health insurance provider. Patients aged 15 years and older with incident hospital-treated sepsis in 2013 to 2014 were included. Data were analyzed from January 2009 to December 2017.
Exposures
Sepsis, identified by International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) hospital discharge codes.
Main Outcomes and Measures
New medical, psychological, and cognitive diagnoses; long-term mortality; dependency on nursing care; and overall health care costs in survivors at 1 to 12, 13 to 24, and 25 to 36 months after hospital discharge.
Results
Among 23.0 million eligible individuals, we identified 159 684 patients hospitalized with sepsis in 2013 to 2014. The mean (SD) age was 73.8 (12.8) years, and 75 809 (47.5%; 95% CI, 47.2%-47.7%) were female patients. In-hospital mortality was 27.0% (43 177 patients; 95% CI, 26.8%-27.3%). Among 116 507 hospital survivors, 86 578 (74.3%; 95% CI, 74.1%-74.6%) had a new diagnosis in the first year post sepsis; 28 405 (24.4%; 95% CI, 24.1%-24.6%) had diagnoses co-occurring in medical, psychological, or cognitive domains; and 23 572 of 74 878 survivors (31.5%; 95% CI, 31.1%-31.8%) without prior nursing care dependency were newly dependent on nursing care. In total, 35 765 survivors (30.7%; 95% CI, 30.4%-31.0%) died within the first year. In the second and third year, 53 089 (65.8%; 95% CI, 65.4%-66.1%) and 40 959 (59.4%; 95% CI, 59.0%-59.8%) had new diagnoses, respectively. Health care costs for sepsis hospital survivors for 3 years post sepsis totaled a mean of €29 088/patient ($32 868/patient) (SD, €44 195 [$49 938]). New postsepsis morbidity (>1 new diagnosis) was more common in survivors of severe sepsis (75.6% [95% CI, 75.1%-76.0%]) than nonsevere sepsis (73.7% [95% CI, 73.4%-74.0%]; P < .001) and more common in survivors treated in the intensive care unit (78.3% [95% CI, 77.8%-78.7%]) than in those not treated in the intensive care unit (72.8% [95% CI, 72.5%-73.1%]; P < .001). Postsepsis morbidity was 68.5% (95% CI, 67.5%-69.5%) among survivors without prior morbidity and 56.1% (95% CI, 54.2%-57.9%) in survivors younger than 40 years.
Conclusions and Relevance
In this study, new medical, psychological, and cognitive diagnoses consistent with postsepsis morbidity were common after sepsis, including among patients with less severe sepsis, no prior diagnoses, and younger age. This calls for more efforts to elucidate the underlying mechanisms, define optimal screening for common new diagnoses, and test interventions to prevent and treat postsepsis morbidity.
Introduction
Sepsis is a disability-inducing event, resulting in considerable financial burden for health care systems.1,2,3 An estimated 38 million patients survive sepsis each year,4 many of whom experience persisting health problems,1,5 including new or worsened physical,6 psychological,7,8 and cognitive6 impairments. Because of these sequelae, sepsis survivors often need ongoing nursing care and experience increased risk of death.9
While the long-term consequences of sepsis are increasingly recognized, there are limited epidemiologic data on the co-occurrence of sepsis sequelae and the rate of sequelae in younger patients or those with less severe sepsis. In a nationwide US cohort of older sepsis survivors, one-sixth experienced persistent physical disability or cognitive impairment, and one-third died during the following year.6,10 In survivors treated in the intensive care unit (ICU), there seems to be a considerable overlap with post–intensive care syndrome.11 However, 50% of severe sepsis patients in the United States12 and two-thirds of patients hospitalized with sepsis in Germany13 are not treated in an ICU. Data on sepsis sequelae in this patient group are lacking. This study aimed to (1) quantify the frequency and co-occurrence of new medical, psychological, and cognitive diagnoses consistent with postsepsis morbidity; (2) compare the rates of mortality and new diagnoses by age group, sepsis severity, ICU treatment, and preexisting diseases; and (3) measure the cumulative costs of care.
Methods
The study was preregistered (DRKS00016340) and approved by the Jena University Hospital institutional review board. The requirement for informed consent was waived because all data were deidentified. This study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Data Source
We performed a longitudinal population-based cohort study using deidentified health claims data from the health insurer Allgemeine Ortskrankenkasse (AOK) from 2009 to 2017. Health insurance is mandatory in Germany; residents select any insurer and enroll without restriction. AOK is the largest nationwide health insurer, covering approximately 30% of the German population.14
Identification of Patients With Sepsis
Patients aged 15 years and older with an inpatient hospitalization for sepsis (discharged January 1, 2013, to December 31, 2014) were identified by explicit International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, German Modification (ICD-10-GM) codes for sepsis coded as primary or secondary discharge diagnoses (eAppendix in the Supplement). We defined and stratified sepsis severity according to the sepsis 1 and sepsis 2 definitions15,16 as sepsis, indicating all forms; severe sepsis or septic shock; and nonsevere sepsis. Coding of sepsis in Germany is rigorously controlled by the Medical Service of the Health Funds; coding of nonsevere sepsis was restricted to cases with positive blood culture and at least 2 Systemic Inflammatory Response Syndrome (SIRS) criteria or to cases with 4 SIRS criteria in case of negative blood cultures, according to German coding regulations during the complete observation period.13,17 The first hospitalization with sepsis was defined as the index hospitalization. We excluded patients with a diagnosis of sepsis in the 2 years preceding hospitalization. Preexisting diagnoses and comorbidities were assessed in a period for as long as 12 months (or 5 years for asplenia) prior to hospitalization. Therefore, patients who were not continuously insured from January 1, 2009, through the 3-year follow-up period after the index hospitalization (or until death) were excluded.
Characteristics of Patients With Sepsis
Patient demographics and clinical characteristics were assessed based on hospital discharge data as well as a 12-month look-back in inpatient and outpatient claims. Study definitions are presented in the eAppendix in the Supplement. Prior nursing home residency and dependency on nursing care were determined based on graded care needs (entitling patients to long-term care insurance benefits, which include care provided by informal or formal caregivers or nursing home placement).18
Determining New Diagnoses and Costs
Based on a comprehensive literature review on postsepsis morbidity, we identified relevant diagnoses consistent with postsepsis morbidity. To translate diagnoses to ICD-10-GM codes, we adapted established definitions19,20,21 and complemented them by own searches (eAppendix in the Supplement). Experts from intensive care, internal medicine, neurology, psychiatry, family medicine, and rehabilitation medicine reviewed and approved the list of diagnoses consistent with postsepsis morbidity. Diagnoses were grouped into 3 domains (ie, medical, psychological, and cognitive) denoting 3 categories of clinical sequelae.9 The medical domain included respiratory, cardiovascular, cerebrovascular, kidney, hepatic, metabolic, urogenital, and neuromuscular/musculoskeletal diagnoses, sensory disorders, anemia, fatigue, decubitus ulcer, pain, multidrug-resistant infections, complications of the tracheostomy, and impairments of nutrition. The psychological domain included depression, anxiety, posttraumatic stress disorder (PTSD), sleeping disorders, and substance use disorders. The cognitive domain included mild to severe cognitive impairment as a single diagnosis. We also assessed nursing care dependency and postdischarge mortality. Finally, we used ICD-10-GM and Operationen- und Prozedurenschlüssel (OPS) codes to assess long-term mechanical ventilation and dialysis (eAppendix in the Supplement).
We determined the prevalence of each diagnosis after sepsis during the 1 to 12, 13 to 24, and 25 to 36 months after index hospital discharge among hospital survivors, 12-month survivors, and 24-month survivors, respectively. Diagnoses were considered present if at least 1 of the ICD-10-GM codes for the diagnosis was reported during a hospitalization or outpatient visit after the index hospital discharge. Diagnoses were considered new if there was no related ICD-10-GM code during the preceding observation period (12-month look-back: first year diagnoses; first year: second year diagnoses; second year: third year diagnoses) in inpatient and outpatient claims data. Survivors who did not have the particular diagnosis during the preceding time period were considered at-risk for incident diagnoses. Thus, incidence of each diagnosis in the first year post sepsis was measured only in patients at risk (ie, did not have the diagnosis in the year before sepsis diagnosis). Likewise, incident diagnoses in the second- and third-year survivors were measured among patients without the diagnosis through the first and second years, respectively. Total health care costs were measured from a health insurance perspective and calculated per patient as sum of costs of hospitalizations, outpatient consultations, medication prescriptions, treatment prescriptions (eg, physical therapy) and rehabilitation.
Statistical Analysis
We reported continuous variables with means and SDs and medians and IQRs and categorical variables by proportions and 95% CIs. We used χ2 test and Welch-Satterthwaite t test for comparisons between subgroups. All reported P values refer to 2-sided tests with a statistical significance level of α = .05. For all descriptive and inferential statistical analyses, SAS Enterprise Guide version 7.1 (SAS Institute) was used. Kaplan-Meier estimates of the survivor functions were used for survival analyses. Differences in the survivor functions between subpopulations were tested with the log-rank test. To facilitate the interpretation of survivor functions, nonparametric estimates of hazard functions based on B-splines with 95% confidence bands are provided.22 The software R version 4.1.0 was used for all survival analyses by means of the R packages survival23,24 and bshazard25 (R Project for Statistical Computing).
Results
Index Population
Among 23.0 million eligible individuals, there were 159 684 index sepsis hospitalizations from 2013 to 2014 (353 per 100 000 person-years) (Figure 1A). Patients with sepsis had a mean (SD) age of 73.8 (12.8) years, 75 809 (47.5%; 95% CI, 47.2%-47.7%) were female patients, and had modest comorbidity burden (mean [SD] unweighted Charlson Comorbidity Index, 2.1 [1.5]). In the 12 months prior to sepsis, 61 167 (38.3%; 95% CI, 38.1%-38.5%) were dependent on nursing care, and 18 636 (11.7%; 95% CI, 11.5%-11.8%) resided in nursing homes. Only 10 666 (6.7%; 95% CI, 6.6%-6.8%) had no preexisting medical, psychological, or cognitive diagnoses in the 12 months before sepsis. Overall, 20 144 (12.6%; 95% CI, 12.5%-12.8%) were employed prior to hospitalization.
Figure 1. Study Flowchart and Postsepsis Morbidity by Domains and Co-occurrence.
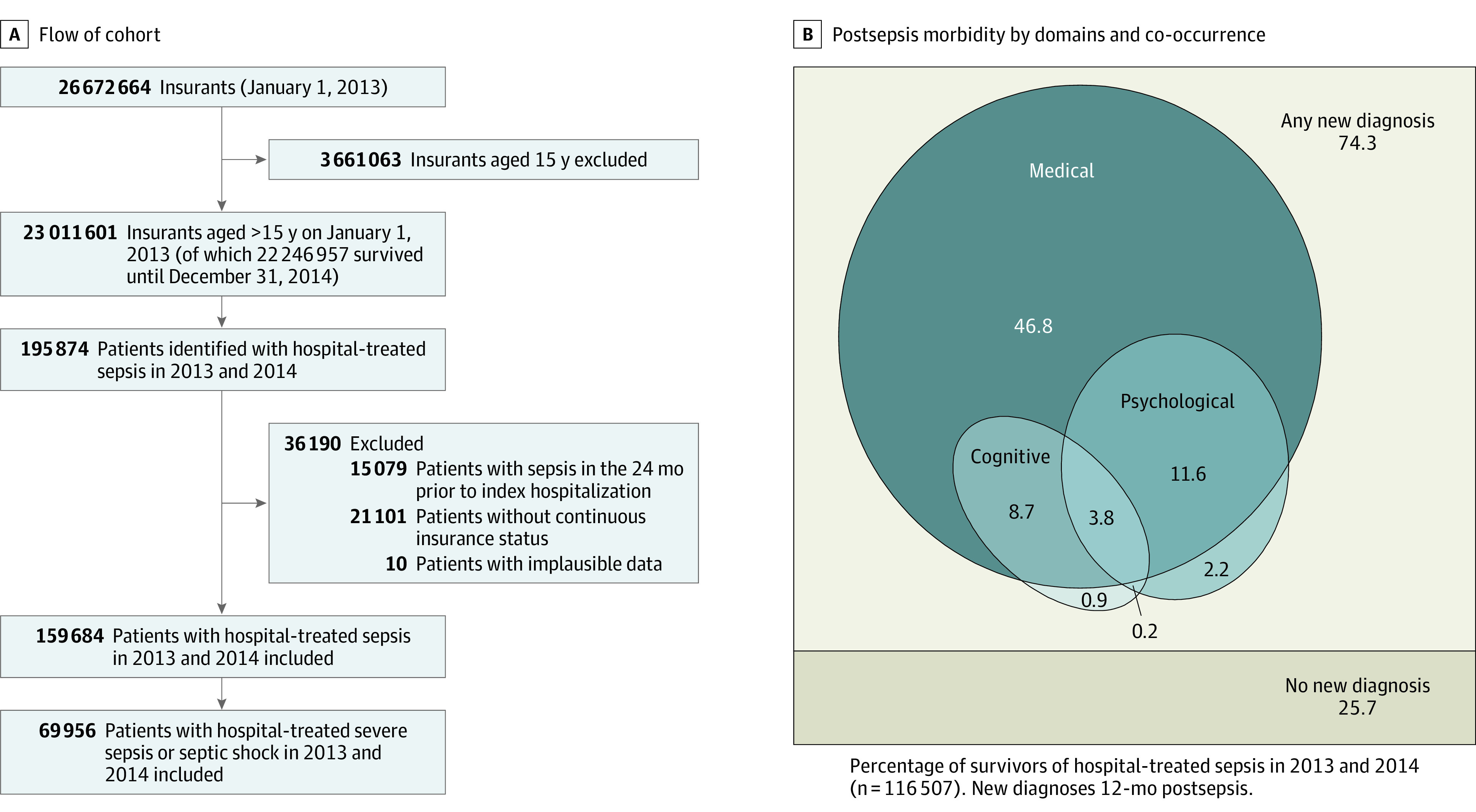
B, This Euler diagram shows the proportion of survivors with new medical, cognitive, or psychological diagnoses in the first year.
Of 159 684 sepsis hospitalizations, 54 317 (34.0%) received intensive care; 69 956 (43.8%) had severe sepsis, including 20 589 (29.4%) with septic shock. Patients with sepsis were hospitalized for a mean (SD) 20.6 (20.8) days, and in-hospital mortality was 27.0% (43 177 patients; 95% CI, 26.8%-27.3%) (eTable 1 in the Supplement). In-hospital mortality was higher in patients treated in the ICU vs those who were not (22 079 [40.6%; 95% CI, 40.2%-41.1%] vs 21 098 [20.0%; 95% CI, 19.8%-20.3%]; P < .001), was higher for those with severe vs nonsevere sepsis (32 116 [45.9%; 95% CI, 45.5%-46.3%] vs 11 061 [12.3%; 12.1%-12.5%]; P < .001), and highest in those with septic shock (12 701 [61.7%; 95% CI, 61.0%-62.4%) (eTable 2 in the Supplement). Patients with no preexisting medical, psychological, or cognitive diagnoses had an in-hospital mortality of 19.2% (2044 patients; 95% CI, 18.4%-19.9%). Overall, 6397 hospital survivors (5.5%; 95% CI, 5.4%-5.6%) were discharged to postacute inpatient rehabilitation. Demographic and clinical features of subgroups are reported in eTable 2 in the Supplement.
New Diagnoses and Care Dependency in Sepsis Survivors
Of the 116 507 patients who survived index hospitalization, 86 578 (74.3%; 95% CI, 74.1%-74.6%) had a new medical, psychological, or cognitive diagnosis consistent with postsepsis morbidity during their first year post discharge. Specifically, 82 629 (70.9%; 95% CI, 70.7%-71.2%) had a new medical diagnosis, 20 840 (17.9%; 95% CI, 17.7%-18.1%) had a new psychological diagnosis, and 15 955 of 86 350 at-risk survivors (18.5%; 95% CI, 18.2%-18.7%) had a new cognitive diagnosis (Table 1).26 Among 74 878 hospital survivors without prior nursing care dependency, 23 572 (31.5%; 95% CI, 31.1%-31.8%) had new nursing care dependency during the first year post sepsis, 1890 of 115 025 at-risk survivors (1.6%; 95% CI, 1.6%-1.7%) required new long-term mechanical ventilation, and 3144 of 111 993 at-risk survivors (2.8%; 95% CI, 2.7%-2.9%) required new dialysis.
Table 1. Postsepsis Diagnoses, Mortality, and Costs Over 3 Yearsa.
| Outcomes among all survivors at start of the time period | Survivors, by follow-up from index hospital discharge | |||||
|---|---|---|---|---|---|---|
| 1-12 mos | 13-24 mos | 25-36 mos | ||||
| No. (n = 116 507) | % (95% CI) | No. (n = 80 742) | % (95% CI) | No. (n = 68 940) | % (95% CI) | |
| Any new diagnosisb | 86 578 | 74.3 (74.1-74.6) | 53 089 | 65.8 (65.4-66.1) | 40 959 | 59.4 (59.0-59.8) |
| New medical diagnosis | 82 629 | 70.9 (70.7-71.2) | 49 486 | 61.3 (61.0-61.6) | 37885 | 55.0 (54.6-55.3) |
| New medical diagnoses, No. | ||||||
| Mean (SD) | 1.9 (1.9) | NA | 1.4 (1.6) | NA | 1.4 (1.6) | NA |
| Median (IQR) | 1 (0-3) | NA | 1 (0-2) | NA | 1 (0-2) | NA |
| New psychological diagnosis | 20 840 | 17.9 (17.7-18.1) | 10 296 | 12.8 (12.5 – 13.0) | 8429 | 12.2 (12.0-12.5) |
| New psychological diagnoses, No. | ||||||
| Mean (SD) | 1.2 (0.5) | NA | 1.2 (0.4); | NA | 1.1 (0.4) | NA |
| Median (IQR) | 1 (1-1) | NA | 1 (1-1) | NA | 1 (1-1) | NA |
| New cognitive diseases, No./No. at risk | 15 955/86 350 | 18.5 (18.2-18.7) | 5383/55 144 | 9.8 (9.5 – 10.) | 4807/48 909 | 9.8 (9.6-10.1) |
| New mechanical ventilation, No./No. at risk | 1890/115 025 | 1.6 (1.6-1.7) | 906/78 999 | 1.1 (1.1-1.2) | 751/67 531 | 1.1 (1.0-1.2) |
| New dialysis, No./No. at risk | 3144/111 993 | 2.8 (2.7-2.9) | 1040/76 863 | 1.4 (1.3-1.4) | 789/65 925 | 1.2 (1.1-1.3) |
| New nursing home residence, No./No. at risk | 12 485/103 912 | 12.0 (11.8-12.2) | 2223/66 502 | 3.3 (3.2-3.5) | 1950/57 409 | 3.4 (3.3-3.5) |
| New dependency on nursing care, No./No. at riskc | 23 572/74 878 | 31.5 (31.1-31.8) | 3784/40 925 | 9.2 (9.0-9.5) | 4272/36 166 | 11.8 (11.5-12.1) |
| Mortality | 35 765 | 30.7 (30.4-31.0) | 11 802 | 14.6 (14.4-14.9) | 9082 | 13.2 (12.9-13.4) |
| Total health care costs, €d | ||||||
| Mean (SD) | 14 891 (24 737) | NA | 11 503 (20 788) | NA | 10 521 (19 146) | NA |
| Median (IQR) | 7055 (2422-17 379) | NA | 5040 (1909-12 813) | NA | 4607 (1771-11 573) | NA |
Abbreviation: NA, not applicable.
All International Classification of Disease–based definitions for the baseline and index hospitalization characteristics can be found in the eAppendix in the Supplement.
At least 1 new cognitive, psychological, or medical diagnosis in the respective time frame.
Eligibility for long-term care benefits in line with the German Social Code, ranging from grade 1 (ie, “Little impairment of independence”) to grade 5 (“Hardship cases”).
Total health care costs include cost for hospitalizations, outpatient consultations, medication, treatments (eg, physical or occupational therapy), and rehabilitation. To convert to US dollars, apply the 2017 mean exchange rate of 0.885 €/US $.26
The most common new diagnoses were neuromuscular/musculoskeletal, cardiovascular, respiratory, kidney, and urogenital diseases, occurring in between 21% and 27% of at-risk survivors (Figure 2A; eTable 3 in the Supplement). For example, 12 893 survivors (26.5%; 95% CI, 26.1%-26.9%) were diagnosed with cardiovascular diseases. New diagnoses of decubitus ulcers, chronic pain, and nutritional impairment occurred in 13% to 14% of at-risk survivors. For example, 12 416 survivors (12.9%; 95% CI, 12.7%-13.1%) had a new chronic pain diagnosis. New fatigue occurred in 8925 (8.2%; 95% CI, 8.1%-8.4%), dysphagia in 7572 (6.9%; 95% CI, 6.7%-7.0%), depression in 9878 (11.7%; 95% CI, 11.5%-11.9%), anxiety in 3550 (3.3%; 95% CI, 3.2%-3.4%), and PTSD in 211 (0.2%; 95% CI, 0.2%-0.2%) of at-risk survivors. New diagnoses in 2 and 3 domains affected 23 964 (20.6%; 95% CI, 20.3%-20.8%) and 4441 (3.8%; 95% CI, 3.7%-3.9%), respectively (Figure 1B). In the second and third year post sepsis, new diagnoses occurred in 53 089 (65.8%; 95% CI, 65.4%-66.1%) and 40 959 (59.4%; 95% CI, 59.0%-59.8%) of 1- and 2-year survivors, respectively (Figure 3 and eTable 4 in the Supplement).
Figure 2. New Postsepsis Diagnoses in the 1 to 12 Months After Hospital Discharge Among Survivors of Nonsevere vs Severe Sepsis and by Age Group.
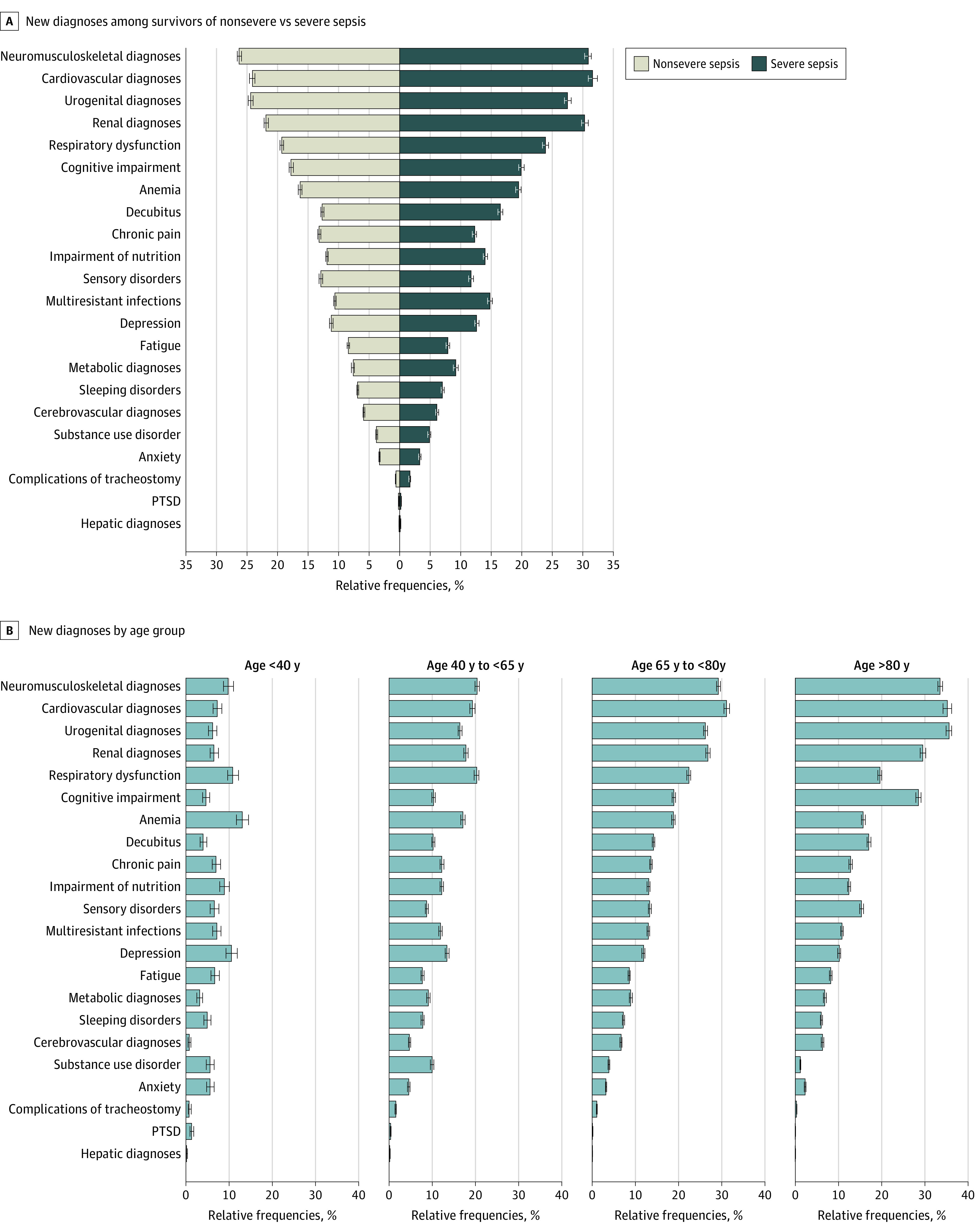
PTSD indicates posttraumatic stress disorder.
Figure 3. Postsepsis Morbidity and Mortality 1 to 12, 13 to 24, and 25 to 36 Months After Sepsis.

This figure shows the percentage of afflicted survivors among all sepsis survivors in the first, second, and third year after sepsis. Of note, the proportion of patients with new nursing need is for all sepsis survivors, not just those at risk.
New Diagnoses and Care Dependency by Subgroup
Approximately three-quarters of survivors were older than 65 years. Patients younger than 40 years were less commonly affected by any new diagnosis (56.1%; 95% CI, 54.2%-57.9%) than patients between 40 and 65 years (72.1%; 95% CI, 71.6%-72.7%), those between 65 and 80 years (76.0%; 95% CI, 75.7%-76.4%) or older than 80 years (74.7%; 95% CI, 74.3%-75.2%) (Table 2). Younger patients at risk were also less frequently affected by new dependency on nursing care (6.9%; 95% CI, 5.9%-8.0%) than older patients (between 19.9% and 47.7%). Patients younger than 40 years had fewer medical diagnoses than older patients (48.5% [95% CI, 46.6%-50.4%] of those aged <40 years vs 72.1% [95% CI, 71.6%-72.5%] of those aged >80 years) but comparatively similar rates of depression and anxiety compared with older patients (depression: between 13.4% [95% CI, 13.0%-13.9%] of those aged <40 years and 10.2% [95% CI, 9.8%-10.5%) of those aged >80 years; anxiety: from 5.8% [95% CI, 5.0%-6.8%] of those aged <40 years and 2.3% [95% CI, 2.1%-2.5%] of those aged >80 years) (Figure 2B).
Table 2. Postsepsis Morbidity and Mortality at 12 Months, by Age Group and Severitya.
| Outcome | Survivors, % (95% CI) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| <40 y (n = 2649) | 40-65 y (n = 25 860) | 66-80 y (n = 51 787) | >80 y (n = 36 211) | Nonsevere sepsis (n = 78 667)b | Severe sepsis or septic shock (n = 37 840)b | Not treated in ICU (n = 84 269)b | Treated in ICU (n = 32 238)b | No preexisting diagnosis (n = 8622) | |
| Any new diagnosisc | 56.1 (54.2-57.9) | 72.1 (71.6-72.7) | 76.0 (75.7-76.4) | 74.7 (74.3-75.2) | 73.7 (73.4-74.0) | 75.6 (75.1-76.0) | 72.8 (72.5-73.1) | 78.3 (77.8-78.7) | 68.5 (67.5-69.5) |
| New medical diagnosis | 48.5 (46.6-50.4) | 67.2 (66.6-67.8) | 73.1 (72.7-73.5) | 72.1 (71.6-72.5) | 70.0 (69.7-70.4) | 72.8 (72.3-73.2) | 69.3 (69.0-69.6) | 75.3 (74.8-75.7) | 63.5 (62.4-64.5) |
| New psychological diagnosis | 19.5 (18.1-21.1) | 23.0 (22.5-23.5) | 18.1 (17.8-18.4) | 13.8 (13.5-14.2) | 17.4 (17.1-17.6) | 19.0 (18.6-19.4) | 16.5 (16.3-16.8) | 21.4 (21.0-21.9) | 25.0 (24.1-25.9) |
| New cognitive diagnosisd | 4.8 (4-5.7) | 10.3 (9.9-10.7) | 18.9 (18.5-19.3) | 28.5 (27.9-29.1) | 17.8 (17.4-18.1) | 19.9 (19.5-20.4) | 17.8 (17.4-18.1) | 20.2 (19.7-20.7) | 12.8 (12.1-13.6) |
| New diagnoses in 2 domains | 14.0 (12.7-15.4) | 20.7 (20.2-21.2) | 21.2 (20.8-21.5) | 20.1 (19.7-20.5) | 19.9 (19.6-20.2) | 22.0 (21.6-22.4) | 19.2 (18.9-19.4) | 24.2 (23.7-24.7) | 22.1 (21.2-23.0) |
| New diagnoses in 3 domains | 1.2 (0.9-1.7) | 3.3 (3.1-3.6) | 4.2 (4-4.4) | 3.8 (3.6-4) | 3.4 (3.3-3.6) | 4.6 (4.4-4.8) | 3.3 (3.2-3.4) | 5.2 (5.0-5.5) | 5.4 (4.9-5.9) |
| New nursing home residenced | 1.4 (1-2) | 6.7 (6.4-7.1) | 10.6 (10.4-10.9) | 19.6 (19.2-20.1) | 11.5 (11.3-11.7) | 13.1 (12.7-13.4) | 11.5 (11.3-11.8) | 13.2 (12.8-13.5) | 7.2 (6.7-7.8) |
| New nursing cared,e | 6.9 (5.9-8) | 19.9 (19.4-20.5) | 32.6 (32.1-33.1) | 47.7 (46.9-48.5) | 29.9 (29.5-30.3) | 34.8 (34.2-35.3) | 29.1 (28.7-29.5) | 36.8 (36.2-37.5) | 19.3 (18.5-20.2) |
| Mortality | 7.9 (6.9-8.9) | 21.9 (21.4-22.4) | 30.2 (29.8-30.6) | 39.4 (38.9-39.9) | 29.2 (28.9-29.5) | 33.9 (33.4-34.4) | 30.3 (30.0-30.6) | 31.8 (31.3-32.3) | 15.2 (14.4-15.9) |
| Total health care costs, €f | |||||||||
| Mean (SD) | 21 847 (49 351) | 20 586 (33 973) | 15 686 (22 778) | 9178 (12 817) | 14 372 (24 289) | 15 969 (25 610) | 13 682 (23 214) | 18 051 (28 090) | 12 583 (25 932) |
| Median (IQR) | 5391 (803 to 23 102) | 9281 (2772 to 24 840) | 8049 (2961 to 19 330) | 5107 (1797 to 11 565) | 6763 (2368 to 16 625) | 7736 (2536 to 18 933) | 6414 (2223 to 15 814) | 9146 (3100 to 21 813) | 3716 (812 to 12 696) |
Abbreviation: ICU, intensive care unit.
All International Classification of Disease–based definitions for the baseline and index hospitalization characteristics can be found in the eAppendix in the Supplement.
Differences between groups (nonsevere vs severe sepsis; non-ICU vs ICU) were statistically significant (each P < .001).
At least 1 new cognitive, psychological, or medical diagnosis in the 12 months after index hospitalization discharge.
New cognitive diagnosis, new nursing home residence, and new nursing care were determined among survivors without these in the 12 months prior to index hospitalization.
New care level according to German care level system or new nursing home residence, ranging from grade 1 (“Little impairment of independence”) to grade 5 (“Hardship cases”).
Total health care costs include cost for hospitalizations, outpatient consultations, medication, treatments (eg, physical or occupational therapy), and rehabilitation. To convert to US dollars, apply the 2017 mean exchange rate of 0.885 €/US $.26
New-onset diagnoses were more common among survivors of severe vs nonsevere sepsis (any new diagnosis: 75.6% [95% CI, 75.1%-76.0%] vs 73.7% [73.4%-74.0%]; P < .001) (Table 2; eTable 5 in the Supplement) and among those treated in the ICU vs those not treated in the ICU (78.3% [95% CI, 77.8%-78.7%] vs 72.8% [72.5%-73.1%]; P < .001) (Table 2; eTable 6 in the Supplement). Among survivors with no prior diagnoses, 63.5% (95% CI, 62.4%-64.5%) had a new medical diagnosis, 25.0% (95% CI, 24.1%-25.9%) had a new psychological diagnosis, and 12.8% (95% CI, 12.1%-13.6%) had a new cognitive diagnosis (Table 2; eTable 7 and eFigure 1 in the Supplement).
New nursing care was more common in at-risk survivors of severe vs nonsevere sepsis (34.8% [95% CI, 34.2%-35.3%] vs 29.9% [29.5%-30.3%]; P < .001) and in those treated in the ICU vs those not treated in the ICU (36.8% [95% CI, 36.2%-37.5%] vs 29.1% [95% CI, 28.7%-29.5%]; P < .001). Overall, 19.3% (95% CI, 18.5%-20.2%) of at-risk survivors without preexisting diseases required new nursing care.
Long-term Mortality in Sepsis Survivors
One-year postdischarge mortality was 30.7% (35 765 patients; 95% CI, 30.4%-31.0%, and most post–hospital deaths occurred within 100 days of hospital discharge (20 432 deaths [17.6%; 95% CI, 17.4%-17.8%]) (eFigure 2 in the Supplement). One-year post-discharge mortality was higher in patients with severe vs nonsevere sepsis, in those treated in the ICU vs those not treated in the ICU, in patients with vs without preexisting diagnoses, and in older vs younger patients. After approximately 100 to 150 days post discharge, risk of subsequent mortality was similar between patients with severe vs nonsevere sepsis and between those treated in the ICU vs not treated in the ICU. However, mortality remained higher in older patients and patients with preexisting diseases for the full 3 years post sepsis (eFigures 3A, 3B, 3C, 3D, and 3E in the Supplement).
Total Health Care Costs
Among all sepsis survivors, mean health care costs were €14 891 (US $16 826) per patient (SD, €24 737 [US $27 951]; median, €7055 [US $7972]; IQR, €2422-€17 379 [US $2737-$19 637) in the first year and decreased to a mean of €11 503 (US $12 998) per patient (SD, €20 788 [US $23 489]; median , €5040 [US $5695]; IQR, €1909-€12 813 [US $2157-$14 478]) and a mean of €10 521 (US $11 888) per patient (SD, €19 146 [US $21 634]; median, €4607 [US $5206]; IQR, €1771-€11 573 [US $2001-$13 077]) in the second and third year, respectively (Table 1). Mean total costs were higher for younger patients (€21 847 [US $24 686]; SD, €49 351 [US $55 764]; median, €5391 [US $6092]; IQR, €803-€23 102 [US $907-$26 104]), declined by age group, and were lowest for patients older than 80 years (€9178 [US $10 371]; SD, €12 817 [US $14 482]; median, €5107 [US $5771]; IQR, €1797-€11 565 [US $2031-$13 068) (Table 2). For survivors of severe sepsis compared with survivors of nonsevere sepsis, mean total health care costs were approximately €1600 Euro higher in the first year (Table 2). Similar differences were found in the following years (eTable 5 in the Supplement). Mean costs for patients treated in the ICU were approximately €4400 higher than for those not treated in the ICU in the first year after sepsis (Table 2). This difference was also evident in the second and third year (eTable 6 in the Supplement). Total health care costs for sepsis hospital survivors for 3 years post sepsis were a mean of €29 088 per patient (SD, €44 195; median, €15 903; IQR, €6004-€34 568) or US $32 868 per patient (SD, $49 938; median, $17 968; IQR, $6784-$39 060) when applying a 2017 mean exchange rate of 0.885 €/US $26 (eTable 8 in the Supplement).
Discussion
In this population-based cohort of more than 100 000 survivors of hospital-treated sepsis with longitudinal follow-up to 3 years post discharge, there were high rates of new diagnoses consistent with postsepsis morbidity, new nursing care dependency, and death. Specifically, three-fourths of survivors were diagnosed with a new medical, psychological, or cognitive condition, and one-third died in the first year. Co-occurrence of new diagnoses in more than 1 domain affected one-quarter of survivors. Importantly, and in contrast to many prior studies, this study captured a broad range of sepsis survivors and showed that postsepsis morbidity is not limited to the oldest survivors or those with the most severe illness—but also affects younger survivors and those without preexisting diagnoses.
The rate of new diagnoses consistent with postsepsis morbidity in our cohort may be higher than prior estimates. In a longitudinal cohort of older US residents, sepsis survivors acquired a median of 1 to 2 new functional limitations, and 10.6% developed new moderate to severe cognitive impairment following sepsis.6 This prior study suggested—based on the incidence of new functional and cognitive impairment—that sepsis was likely associated with substantial need for new nursing home placement and informal caregiving by family members but was unable to measure these downstream impacts directly. By contrast, our study directly measured the incidence of new nursing care dependency and found that one-third of at-risk sepsis survivors were newly dependent on nursing care, one-fifth had new cognitive diagnoses, and one-eighth of at-risk survivors had a new diagnosis of depression.
With approximately 320 000 patients with sepsis annually in Germany13 and an in-hospital mortality rate of 27.0%, the total direct costs for 3-year follow-up health care can be estimated at €6.8 billion (US $7.7 billion) per year. The full economic impact of sepsis would be even higher if one considers the reduced economic productivity of survivors, the need for informal nursing care, and the life-changing effects on caregivers,27,28 on whom many survivors depend for physical and financial support. These results highlight the considerable burden of sepsis and its long-lasting and multifaceted sequelae for patients, families, and the health care system.
Although most survivors had new diagnoses consistent with postsepsis morbidity, only 5.5% were discharged to rehabilitation facilities. Cardiovascular diseases were among the most common new diagnoses, likely an important mediator of long-term mortality in sepsis survivors.29 The incidence of new pain diagnosis (12.9%) in our cohort is similar to a previous case-control study, which found that 16% of patients treated in the ICU with and without sepsis experienced chronic pain at 6 months, but could detect no difference between the 2 groups.30 Fatigue is a severely disabling symptom and an important determinant of quality of life for sepsis survivors.28 Fatigue incidence in our study (8.2%) was in a similar range as reported by survivors of hospital-treated COVID-19.31 This underscores that fatigue may also be associated with activation of the immune system.32 Long-term ventilation is comparatively rare (1.6%) but nonetheless affects several thousand survivors yearly at enormous costs.33 The incidence of anxiety (3.3%) or PTSD (0.2%) in our study was much lower than assessed among convenience samples of survivors from a sepsis self-help group (anxiety, 60%; PTSD, 69%).34 The difference can be explained because we assessed incident diseases in a population-based cohort. On the other hand, psychological diagnoses may be undercaptured in our cohort if physicians fail to provide a diagnosis for survivor symptoms.5
Our study provides new insight into postsepsis morbidity that may also have relevance for survivors of COVID-19. Sepsis is a frequent complication in patients with COVID-19 treated in the ICU and not treated in the ICU.35 In a cohort of patients discharged from the hospital, 76% had 1 or more residual symptom at 6 months, including fatigue/muscle weakness (63%), sleep problems (23%), and anxiety or depression (23%).36 Furthermore, our findings demonstrate that new medical, psychological, and cognitive diagnoses consistent with postsepsis morbidity are also common among patients who fulfil the criteria of nonsevere sepsis according to the old sepsis 1 and sepsis 2 criteria.15,16
These findings raise questions about the sensitivity of the new sepsis 3 definition in terms of the differentiation between patients with uncomplicated infections, which are less likely to cause major long-term morbidity, and patients with severe infections, formerly categorized as sepsis without organ dysfunction. SIRS criteria are no longer part of the current sepsis definition,37,38 but the presence of at least 2 SIRS criteria in patients with proven or clinical suspected infection seems to identify an increased risk of major postinfection morbidity and hospital mortality. Overall, our findings highlight the burden of postsepsis morbidity and the need to develop and implement better systems to support survivors.39
Strengths and Limitations
Our study has several strengths. To our knowledge, it is the first study to comprehensively investigate the epidemiology of postsepsis morbidity across a population-based cohort of adult patients of all ages and with different severities of sepsis. The study used nationwide data of the largest health care insurance provider in Germany and covers approximately one-third of all German patients. Our study had a rigorous process to identify the specific diagnoses and diagnostic codes consistent with postsepsis morbidity, based on a multiprofessional panel of experts who care for patients after sepsis.
Several limitations need to be acknowledged. First, the identification of patients with sepsis and their subsequent diagnoses depends on the quality of coding. The explicit sepsis codes we used for case identification may have missed some patients who met clinical criteria for sepsis.12,40 Second, measuring postsepsis morbidity based on diagnostic codes may result in misclassification. However, systematic screening of survivors for new medical, psychological, and cognitive diagnoses would not be feasible for such a large, population-based cohort. In Germany, the plausibility of inpatient and outpatient coding is audited by the Medical Services of the Health Care Funds and the Association of Statutory Health Insurance Physicians, which helps ensure the accuracy of coded diagnoses and mitigate the risk of misclassification in this study. Nevertheless, poor awareness of sepsis sequelae among patients and physicians may result in underdiagnosis. Third, our study is observational and cannot establish causality of postsepsis morbidity. However, prior matched studies suggest that sepsis is associated with subsequent morbidity,9 particularly functional limitations, cognitive impairment, and select medical conditions. Fourth, our approach only allowed us to identify new-onset diagnoses but not accelerated progression of preexisting diagnoses. Fifth, our data lacked costs of emergency service utilization, transport, therapeutic aid prescriptions, dental care, home care prescription, nursing care, and indirect costs due to productivity loss, so it underestimates the total financial toll of sepsis. Sixth, we also cannot rule out that differences may exist in comparison with the general German patient population, but prior studies have suggested only small differences between AOK and non-AOK beneficiaries in Germany.41
Conclusions
In this study, postsepsis morbidity was common across all age groups and severities of sepsis, and the financial toll of sepsis was substantial. Future research is needed to prevent, screen for, and treat postsepsis morbidity. The development of comprehensive rehabilitation infrastructure also requires a better understanding of the mechanisms of long-term morbidity.
eAppendix. Supplementary Methods and Definitions and Codes for Case Identification
eTable 1. Patient and Hospitalization Characteristics and Outcomes for 159 684 Index Sepsis Hospitalizations
eTable 2. Baseline Characteristics of Different Patient Groups
eTable 3. Underlying Diseases in the Psychological and Medical Domain
eTable 4. Prevalent and Incident Impairments in Hospital Survivors, 1 to 12, 13 to 24, and 25 to 36 Months After Sepsis
eTable 5. Comparison of Outcomes and Costs 1 to 12, 13 to 24, and 25 to 36 Months Among Survivors With Nonsevere and Severe Sepsis
eTable 6. Comparison of Outcomes and Costs 1 to 12, 13 to 24, and 25 to 36 Months Among Patients Treated in the ICU and Those Not Treated in the ICU
eTable 7. Outcomes and Costs 1 to 12, 13 to 24, and 25 to 36 Months Among Patients Without Preexisting Impairments
eTable 8. Total Health Care Costs Among Hospital Survivors, 1 to 12, 13 to 24, and 25 to 36 Months After Sepsis
eFigure 1. Co-occurrence and Mortality in Patients 1 to 12 Months After Discharge From the Index Hospitalization According to Preexisting Impairments
eFigure 2. Kaplan Meier Survival Curve Until 36 Months After Discharge
eFigure 3. Hazard Functions for Death for All Patients With Sepsis, Patients With Severe and Nonsevere Sepsis, Patients Treated in the ICU and Not Treated in the ICU, Patients with Sepsis According to Preexisting Impairments and by Age Groups
References
- 1.Prescott HC, Iwashyna TJ, Blackwood B, et al. Understanding and enhancing sepsis survivorship: priorities for research and practice. Am J Respir Crit Care Med. 2019;200(8):972-981. doi: 10.1164/rccm.201812-2383CP [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Torio CM, Moore BJ. National inpatient hospital costs: the most expensive conditions by payer, 2013. Statistical Brief #204. Healthcare Cost and Utilization Project (HCUP). May 2016. Accessed October 12, 2021. https://www.hcup-us.ahrq.gov/reports/statbriefs/sb204-Most-Expensive-Hospital-Conditions.jsp
- 3.Buchman TG, Simpson SQ, Sciarretta KL, et al. Sepsis among Medicare beneficiaries: 1. the burdens of sepsis, 2012-2018. Crit Care Med. 2020;48(3):276-288. doi: 10.1097/CCM.0000000000004224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200-211. doi: 10.1016/S0140-6736(19)32989-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Huang CY, Daniels R, Lembo A, et al. ; Sepsis Survivors Engagement Project (SSEP) . Life after sepsis: an international survey of survivors to understand the post-sepsis syndrome. Int J Qual Health Care. 2019;31(3):191-198. doi: 10.1093/intqhc/mzy137 [DOI] [PubMed] [Google Scholar]
- 6.Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794. doi: 10.1001/jama.2010.1553 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rabiee A, Nikayin S, Hashem MD, et al. Depressive symptoms after critical illness: a systematic review and meta-analysis. Crit Care Med. 2016;44(9):1744-1753. doi: 10.1097/CCM.0000000000001811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nikayin S, Rabiee A, Hashem MD, et al. Anxiety symptoms in survivors of critical illness: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2016;43:23-29. doi: 10.1016/j.genhosppsych.2016.08.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Prescott HC, Angus DC. Enhancing recovery from sepsis: a review. JAMA. 2018;319(1):62-75. doi: 10.1001/jama.2017.17687 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Prescott HC, Langa KM, Liu V, Escobar GJ, Iwashyna TJ. Increased 1-year healthcare use in survivors of severe sepsis. Am J Respir Crit Care Med. 2014;190(1):62-69. doi: 10.1164/rccm.201403-0471OC [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012;40(2):502-509. doi: 10.1097/CCM.0b013e318232da75 [DOI] [PubMed] [Google Scholar]
- 12.Rhee C, Dantes R, Epstein L, et al. ; CDC Prevention Epicenter Program . Incidence and trends of sepsis in US hospitals using clinical vs claims data, 2009-2014. JAMA. 2017;318(13):1241-1249. doi: 10.1001/jama.2017.13836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fleischmann-Struzek C, Mikolajetz A, Schwarzkopf D, et al. Challenges in assessing the burden of sepsis and understanding the inequalities of sepsis outcomes between National Health Systems: secular trends in sepsis and infection incidence and mortality in Germany. Intensive Care Med. 2018;44(11):1826-1835. doi: 10.1007/s00134-018-5377-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bundesministerium für Gesundheit. Gesetzliche Krankenversicherung Mitglieder, mitversicherte Angehörige und Krankenstand 2014. Accessed April 2, 2021. https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/Statistiken/GKV/Mitglieder_Versicherte/KM1_JD_2014.pdf
- 15.Bone RC, Balk RA, Cerra FB, et al. ; The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine . Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101(6):1644-1655. doi: 10.1378/chest.101.6.1644 [DOI] [PubMed] [Google Scholar]
- 16.Levy MM, Fink MP, Marshall JC, et al. ; SCCM/ESICM/ACCP/ATS/SIS . 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250-1256. doi: 10.1097/01.CCM.0000050454.01978.3B [DOI] [PubMed] [Google Scholar]
- 17.DIMDI . Was versteht man unter SIRS (Systemisches inflammatorisches Response-Syndrom)? Accessed October 12, 2021. https://www.dimdi.de/static/.downloads/deutsch/maticd-sirs-def-2007-1007.pdf
- 18.Büscher A, Wingenfeld K, Schaeffer D. Determining eligibility for long-term care-lessons from Germany. Int J Integr Care. 2011;11:e019. doi: 10.5334/ijic.584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.van den Bussche H, Koller D, Kolonko T, et al. Which chronic diseases and disease combinations are specific to multimorbidity in the elderly? results of a claims data based cross-sectional study in Germany. BMC Public Health. 2011;11:101. doi: 10.1186/1471-2458-11-101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Allers K, Hoffmann F. Mortality and hospitalization at the end of life in newly admitted nursing home residents with and without dementia. Soc Psychiatry Psychiatr Epidemiol. 2018;53(8):833-839. doi: 10.1007/s00127-018-1523-0 [DOI] [PubMed] [Google Scholar]
- 21.Wittchen HU, Jacobi F, Klose M, Ryl L. Depressive Erkrankungen. Robert Koch Institute. 2010. Accessed October 12, 2021. https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsT/depression.pdf?__blob=publicationFile
- 22.Rebora P, Salim A, Reilly M. bshazard: A flexible tool for nonparametric smoothing of the hazard function. The R Journal 2014;6(2): 114-122. doi: 10.32614/RJ-2014-028 [DOI] [Google Scholar]
- 23.Therneau TM. A package for survival analysis in R. R package version 3.1-12. Accessed October 12, 2021. https://CRAN.R-project.org/package=survival
- 24.Therneau TM, Grambsch PM. Modeling Survival Data: Extending the Cox Model. Springer-Verlag; 2020. [Google Scholar]
- 25.Rebora P, Salim A, Reilly M. bshazard: Nonparametric smoothing of the hazard function. 2018; R package version 1.1. Accessed October 12, 2021. https://CRAN.R-project.org/package=bshazard
- 26.OECD . Exchange rates. Accessed October 12, 2021. https://www.oecdilibrary.org/finance-and-investment/exchange-rates/indicator/english_037ed317-en
- 27.Cameron JI, Chu LM, Matte A, et al. ; RECOVER Program Investigators (Phase 1: towards RECOVER); Canadian Critical Care Trials Group . One-year outcomes in caregivers of critically ill patients. N Engl J Med. 2016;374(19):1831-1841. doi: 10.1056/NEJMoa1511160 [DOI] [PubMed] [Google Scholar]
- 28.König C, Matt B, Kortgen A, Turnbull AE, Hartog CS. What matters most to sepsis survivors: a qualitative analysis to identify specific health-related quality of life domains. Qual Life Res. 2019;28(3):637-647. doi: 10.1007/s11136-018-2028-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ou SM, Chu H, Chao PW, et al. Long-term mortality and major adverse cardiovascular events in sepsis survivors. a nationwide population-based study. Am J Respir Crit Care Med. 2016;194(2):209-217. doi: 10.1164/rccm.201510-2023OC [DOI] [PubMed] [Google Scholar]
- 30.Baumbach P, Götz T, Günther A, Weiss T, Meissner W. Prevalence and characteristics of chronic intensive care-related pain: the role of severe sepsis and septic shock. Crit Care Med. 2016;44(6):1129-1137. doi: 10.1097/CCM.0000000000001635 [DOI] [PubMed] [Google Scholar]
- 31.Carfì A, Bernabei R, Landi F; Gemelli Against COVID-19 Post-Acute Care Study Group . Persistent symptoms in patients after acute COVID-19. JAMA. 2020;324(6):603-605. doi: 10.1001/jama.2020.12603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lee C-H, Giuliani F. The role of inflammation in depression and fatigue. Front Immunol. 2019;10:1696-1696. doi: 10.3389/fimmu.2019.01696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Karagiannidis C, Strassmann S, Callegari J, Kochanek M, Janssens U, Windisch W. Evolving epidemiology of home mechanical ventilation: a rapidly growing challenge for patient care. Article in German. Dtsch Med Wochenschr. 2019;144(9):e58-e63. [DOI] [PubMed] [Google Scholar]
- 34.Rosendahl J, Brunkhorst FM, Jaenichen D, Strauss B. Physical and mental health in patients and spouses after intensive care of severe sepsis: a dyadic perspective on long-term sequelae testing the Actor-Partner Interdependence Model. Crit Care Med. 2013;41(1):69-75. doi: 10.1097/CCM.0b013e31826766b0 [DOI] [PubMed] [Google Scholar]
- 35.Karakike E, Giamarellos-Bourboulis EJ, Kyprianou M, et al. COVID-19 as cause of viral sepsis: a systematic review and meta-analysis. medRxiv. Preprint published October 4, 2020. doi: 10.1101/2020.12.02.20242354 [DOI]
- 36.Huang C, Huang L, Wang Y, et al. 6-Month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220-232. doi: 10.1016/S0140-6736(20)32656-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med. 2015;372(17):1629-1638. doi: 10.1056/NEJMoa1415236 [DOI] [PubMed] [Google Scholar]
- 38.Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801-810. doi: 10.1001/jama.2016.0287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Mostel Z, Perl A, Marck M, et al. Post-sepsis syndrome—an evolving entity that afflicts survivors of sepsis. Mol Med. 2019;26(1):6. doi: 10.1186/s10020-019-0132-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Fleischmann-Struzek C, Thomas-Rüddel DO, Schettler A, et al. Comparing the validity of different ICD coding abstraction strategies for sepsis case identification in German claims data. PLoS One. 2018;13(7):e0198847. doi: 10.1371/journal.pone.0198847 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Jeschke E, Gehrke T, Günster C, et al. Low hospital volume increases revision rate and mortality following revision total hip arthroplasty: an analysis of 17,773 cases. J Arthroplasty. 2019;34(9):2045-2050. doi: 10.1016/j.arth.2019.05.005 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix. Supplementary Methods and Definitions and Codes for Case Identification
eTable 1. Patient and Hospitalization Characteristics and Outcomes for 159 684 Index Sepsis Hospitalizations
eTable 2. Baseline Characteristics of Different Patient Groups
eTable 3. Underlying Diseases in the Psychological and Medical Domain
eTable 4. Prevalent and Incident Impairments in Hospital Survivors, 1 to 12, 13 to 24, and 25 to 36 Months After Sepsis
eTable 5. Comparison of Outcomes and Costs 1 to 12, 13 to 24, and 25 to 36 Months Among Survivors With Nonsevere and Severe Sepsis
eTable 6. Comparison of Outcomes and Costs 1 to 12, 13 to 24, and 25 to 36 Months Among Patients Treated in the ICU and Those Not Treated in the ICU
eTable 7. Outcomes and Costs 1 to 12, 13 to 24, and 25 to 36 Months Among Patients Without Preexisting Impairments
eTable 8. Total Health Care Costs Among Hospital Survivors, 1 to 12, 13 to 24, and 25 to 36 Months After Sepsis
eFigure 1. Co-occurrence and Mortality in Patients 1 to 12 Months After Discharge From the Index Hospitalization According to Preexisting Impairments
eFigure 2. Kaplan Meier Survival Curve Until 36 Months After Discharge
eFigure 3. Hazard Functions for Death for All Patients With Sepsis, Patients With Severe and Nonsevere Sepsis, Patients Treated in the ICU and Not Treated in the ICU, Patients with Sepsis According to Preexisting Impairments and by Age Groups