

Abstract
Coronavirus disease 2019 (COVID-19) disease leads to a hypercoagulable state and associated with thrombotic events that can cause mortality and morbidity. Thrombotic events include both venous and arterial thrombosis. In this case report, we present a 68-year-old COVID-19 patient with multisystemic infarction who was admitted to the hospital by splenic infarction and later pulmonary embolism diagnosed during the stay in hospital despite anticoagulant use. It is important for emergency physicians to know that patients who had COVID-19 infection but not confirmed or not tested can visit the emergency department due to complications of COVID-19 infection such as thromboembolic events primarily.
Keywords: Coronavirus disease 2019, emergency department, pulmonary embolism, splenic infarction
Introduction
Thrombotic complications are common in coronavirus disease 2019 (COVID-19) and strongly related with mortality and morbidity.[1] The interaction between coagulation and inflammation was shown previously in many diseases and has been termed as thromboinflammation by some authors.[2] COVID-19 disease also leads to a hypercoagulable state and is associated with thromboinflammation.[3] Thrombotic events encompass both arterial and venous thrombosis. Arterial thromboembolism encompasses a broad range of conditions including myocardial infarction, stroke, splenic, and renal infarcts. Venous thromboembolism consists of pulmonary embolism (PE) and deep vein thrombosis. Thrombotic events have been reported in COVID-19 patients who were not hospitalized, but data on the incidence are limited. Below, we discuss a COVID-19 case with both splenic infarction and PE.
Case Report
A 68-year-old male patient was admitted to the emergency department with shortness of breath and epigastric pain radiating to the left upper quadrant that last 3 days. The patient had a previous history of cerebrovascular events, hypertension, and coronary bypass surgery. The patient had a history of suspicious contact with a confirmed COVID-19 patient. He was taking pantoprazole, metoprolol succinate, clopidogrel, perindopril/amlodipine, and atorvastatin. His vital signs included a temperature of 36.1°C, oxygen saturation of 90% on room air, a respiratory rate of 18/min, a blood pressure of 109/76 mmHg, and a pulse of 78 beats per minute. His physical examination identified marked tenderness in the left upper quadrant, without guarding in the same area. The rest of his physical examination was normal. His electrocardiography showed no abnormal findings. Laboratory studies showed abnormal white blood cell count 12.62 × 103/mm3 (3.6–11 × 103/mm3), C-reactive protein 97.5 mg/L (0–8 mg/L), lactate dehydrogenase 576 U/L (200–450 U/L), and D-dimer 1.72 mcg/mL (0–0.5 mcg/mL). The patient's lymphocyte, hemoglobin, creatinine, lactic acid values, liver function tests, and coagulation parameters were normal. An abdomen and pelvis computed tomography (CT) with intravenous (IV) contrast demonstrated splenic infarction [Figure 1]. Lung lesions in chest CT reported “in both lung parenchyma, peripheral-weighted infiltration areas, which have started to gain a largely consolidated character are noticeable. In addition, curvilinear band formations are observed in subpleural areas. Findings were considered to be significant in favor of mid-to-late COVID-19 pneumonia.” by the radiologist [Figure 2]. Close monitoring of vital signs and laboratory values along with supportive care with hydration and pain control was initiated. The patient consulted with a general surgeon and an infectious diseases specialist. Hospitalization for close follow-up, and treatment was recommended. Favipiravir (1st day 1600 mg, other 4 days 600 mg PO BID), enoxaparin 60 mg SC BID, famotidine 40 mg PO BID, and ceftriaxone 2 g QD IV treatment was given to the patient during his stay in hospital. He tested negative three times for SARS-Cov-2 through reverse transcriptase-polymerase chain reaction. He presented hypoxia and tachypnea on his 4th day of hospitalization. A CT pulmonary angiography revealed PE in the distal part of the right main pulmonary artery extending into the right upper and lower lobe in the patient. In addition, filling defect consistent with PE was observed in the segmental artery of the lower lobe of the left lung [Figure 3]. The patient was discharged, 6 days later with improving laboratory studies and clinical condition. For publication of this case report, written informed consent was obtained from the patient.
Figure 1.
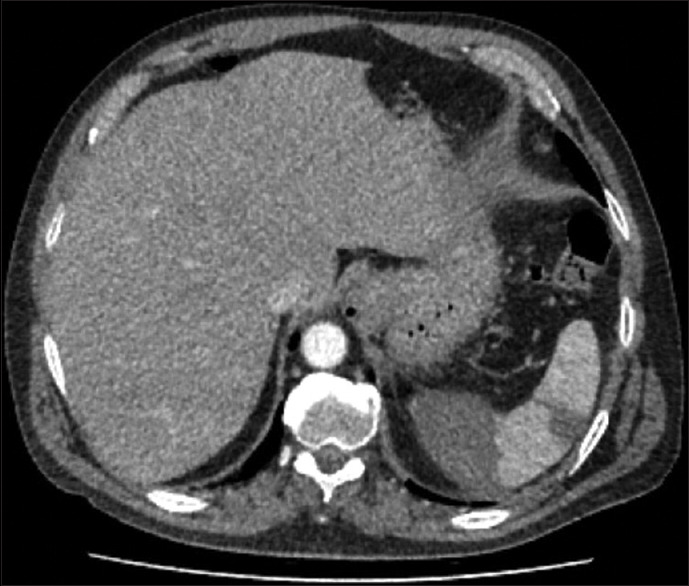
Abdomen/pelvis computed tomography with intravenous contrast demonstrating infarction in the spleen
Figure 2.
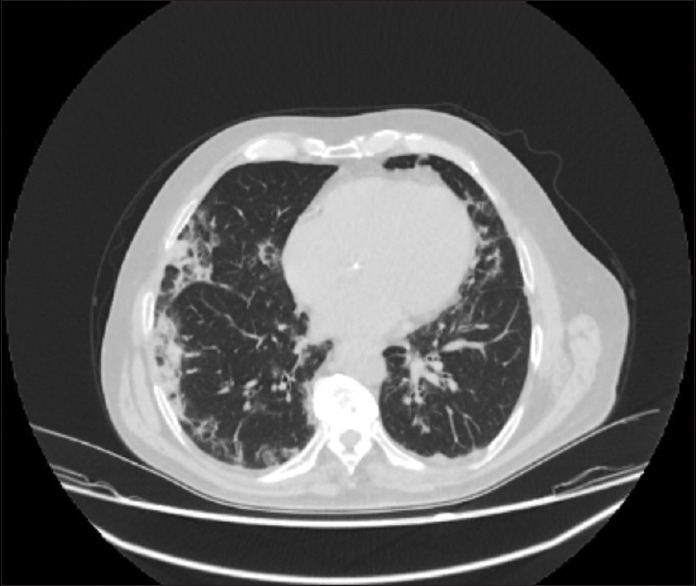
Chest computed tomography contains findings that are considered to be significant in favor of mid-to-late COVID-19 pneumonia
Figure 3.
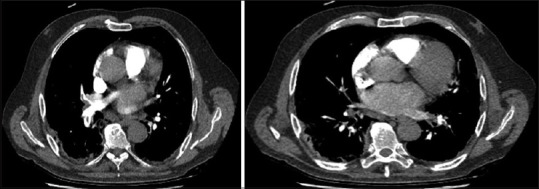
Computed tomography pulmonary angiography revealing pulmonary embolism in the distal part of the right main pulmonary artery (left) and in the segmental artery of the lower lobe of the left lung (right)
Discussion
On February 21, 2021, we searched the literature through PubMed, Google Scholar, Scopus, and Web of Science for the relevant terms, which included “COVID and PE,” “COVID and splenic infarction.” In the literature search, we found a COVID-19 case with splenic infarction, PE, and acute ischemic stroke at the time of diagnosis.[4] That case was admitted to the hospital for the symptoms related to acute ischemic stroke. No additional information that leads to the diagnosis of PE and splenic infarct for that patient are included in that report. Our case is the first COVID-19 case with both splenic infarction and PE at the same time in the literature.
A broad spectrum of thromboembolic manifestations and an increased risk for both venous and arterial thromboembolism may be seen in the patients with COVID-19 infection.[5] In a large study that examines hospitalized COVID-19 patients whose prophylactic dose anticoagulation was given in most found that any thrombotic event occurred in 16% of the patients. All-cause mortality was higher in the patients with thrombotic events.[6]
Among the patients with COVID-19 infection, splenic thrombosis is infrequent and should be considered in patients who presented with left-sided abdominal pain.[7]
Venous thromboembolism prophylaxis is appropriate according to the current society guidelines in all hospitalized patients with COVID-19 and a treatment of full-dose (therapeutic) anticoagulation is appropriate in patients with documented or strongly suspected thromboembolism in the absence of a contraindication.[8] Our patient received therapeutic anticoagulation after a CT scan confirmed splenic infarcts during his stay in the hospital, but on his 4 days of stay, he was diagnosed with PE.
Conclusion
Emergency physicians should be aware of the fact that patients who had COVID-19 infection but not confirmed or not tested can visit the hospital or emergency department due to complications of COVID-19 infection primarily. COVID-19 disease can be associated with splenic infarction and thrombosis in unusual sites.[7] It is important for emergency physicians to know that the complications of COVID-19 such as thromboembolic events can be the primary complaint of patients who have unconfirmed COVID-19 infections.
Acknowledgment
We verify and confirm that everyone who contributed to this manuscript is either listed as an author.
Footnotes
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
None.
Conflicts of interest
None Declared.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report. A copy of the written consent is available.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
References
- 1.Connors JM, Levy JH. COVID-19 and its implications for thrombosis and anticoagulation. Blood. 2020;135:2033–40. doi: 10.1182/blood.2020006000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jackson SP, Darbousset R, Schoenwaelder SM. Thromboinflammation: Challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood. 2019;133:906–18. doi: 10.1182/blood-2018-11-882993. [DOI] [PubMed] [Google Scholar]
- 3.Connors JM, Levy JH. Thromboinflammation and the hypercoagulability of COVID-19. J Thromb Haemost. 2020;18:1559–61. doi: 10.1111/jth.14849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Santos Leite Pessoa M, Franco Costa Lima C, Farias Pimentel AC, Godeiro Costa JC, Bezerra Holanda JL. Multisystemic infarctions in COVID-19: Focus on the spleen. Eur J Case Rep Intern Med. 2020;7:001747. doi: 10.12890/2020_001747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Klok FA, Kruip MJ, van der Meer NJ, Arbous MS, Gommers DA, Kant KM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;191:145–7. doi: 10.1016/j.thromres.2020.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bilaloglu S, Aphinyanaphongs Y, Jones S, Iturrate E, Hochman J, Berger JS. Thrombosis in hospitalized patients with COVID-19 in a New York City health system. JAMA. 2020;324:799–801. doi: 10.1001/jama.2020.13372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ramanathan M, Chueng T, Fernandez E, Gonzales-Zamora J. Concomitant renal and splenic infarction as a complication of COVID-19: A case report and literature review. Infez Med. 2020;28:611–5. [PubMed] [Google Scholar]
- 8.COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. [Last accessed on 2020 Dec 18]. Available from: https://www.covid19treatmentguidelines .nih.gov/ [PubMed]