

Supplemental digital content is available in the text.
Key Words: Inpatient Rehabilitation, COVID-19, Post-ICU Syndrome, Long COVID, Postacute Sequelae of SARS-CoV-2 Infection
Abstract
Objective
The aim of the study was to describe the characteristics and functional outcomes of patients undergoing acute inpatient rehabilitation after hospitalization for COVID-19.
Design
Using a retrospective chart review, patients were identified who were admitted to inpatient rehabilitation after COVID-19. Patient information collected included sociodemographic characteristics, comorbidities, length of stay, discharge disposition, self-care, mobility, and cognitive functioning. These patients were compared with patients (controls) without COVID-19 with similar impairment codes treated at the same facility before the COVID-19 pandemic.
Results
There were 43 patients who were admitted to the inpatient rehabilitation hospital after COVID-19 infection and 247 controls. Patients who had COVID-19 were significantly more likely to be African American and to have been admitted to a long-term acute care hospital. They also had a longer length of rehabilitation stay. The groups did not differ by age, sex, or insurance. Functionally, although presenting with significantly worse mobility, self-care, and motor scores, the patients previously infected with COVID-19 had similar functional outcomes at time of discharge to the control group.
Conclusions
Although patients with a history of COVID-19 had worse function at time of admission to acute rehabilitation, inpatient rehabilitation significantly improved their function to comparable levels as patients who did not have COVID-19.
To Claim CME Credits
Complete the self-assessment activity and evaluation online at http://www.physiatry.org/JournalCME
CME Objectives
Upon completion of this article, the reader should be able to: (1) Identify how characteristics of patients with COVID-19 admitted to acute rehabilitation differ from those with similar admission codes but without COVID-19; (2) Describe changes in functional measures at admission and discharge of COVID-19 patients compared with patients without COVID-19; and (3) Recognize how inpatient rehabilitation may help reduce inequities in outcomes after severe COVID-19 infection.
Level
Advanced
Accreditation
The Association of Academic Physiatrists is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
The Association of Academic Physiatrists designates this Journal-based CME activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
What Is Known
COVID-19 leads to significant short- and long-term morbidity and functional impairment.
What Is New
Although initially presenting with significantly worse mobility and self-care, by the time of discharge, patients in inpatient rehabilitation after COVID-19 had similar functional outcomes compared with rehabilitation patients who did not have COVID-19 (although similar impairment codes). Comprehensive rehabilitation may be an effective way to improve functional outcomes after severe COVID-19 infection.
The coronavirus disease 2019 (COVID-19) pandemic has led to more than 2 million hospitalizations in the United States,1 of whom 15%–25% required admission to the intensive care unit (ICU).2–4 Common complications of those hospitalized with COVID-19 include acute respiratory failure, acute respiratory distress syndrome, acute kidney failure, sepsis, shock, acute ischemic heart disease, neurologic disorders, and venous thromboembolism.4
One potential adverse outcome after hospitalization, particularly among those requiring ICU admission and mechanical ventilation, is post-ICU syndrome (PICS). Post–intensive care unit syndrome is a constellation of new or worsening cognitive, functional, and psychiatric functioning after critical illness.5 It has been estimated to occur in more than half of ICU survivors, and residual effects can last beyond 12 mos after hospital discharge.6 In the physical domain, PICS often manifests as generalized weakness, critical illness polyneuropathy, and critical illness myopathy.
Recent evidence suggests that individuals infected with COVID-19 may develop PICS at higher rates than other critically ill populations. A small observational cohort study of 111 individuals found that 9.9% of ICU patients infected with COVID-19 developed critical illness polyneuropathy/critical illness myopathy compared with 3.4% of a general ICU population.7 In addition to PICS, individuals previously infected COVID-19 report a wide variety of persistent symptoms, including cognitive dysfunction (also known as “brain fog”), anxiety, depression, dyspnea, fatigue, poor endurance, and insomnia.8–12 These symptoms can occur even in COVID-19 patients who were not hospitalized during their acute illness and are collectively known as postacute sequelae of SARS-CoV-2 infection.13 The extent to which patients who were critically ill from COVID-19 have a similar postacute course compared with patients who were critically ill for other reasons remains unknown.
Rehabilitation services provided in an inpatient setting is potentially well-suited to mitigate the debilitating sequelae of COVID-19 and related complications.14,15 Despite the potential benefit of postacute inpatient rehabilitation, only 4% of patients hospitalized with COVID-19 in the United States between March and August of 2020 were discharged to ongoing care (including long-term acute care and acute inpatient rehabilitation).16
The purposes of this study were to describe the characteristics and functional outcomes of a population of COVID-19 survivors receiving inpatient rehabilitation at an urban rehabilitation hospital and to compare them with a population who received inpatient rehabilitation for similar, although non–COVID-19–related impairments.
METHODS
Setting
The study was performed at the Penn Institute for Rehabilitation Medicine, an academic rehabilitation hospital located in Philadelphia, Pennsylvania. This work was done under the University of Pennsylvania Institutional Review Board through an approved research protocol. Institutional review board waived the requirement for written informed consent. This study conforms to all STROBE guidelines and reports the required information accordingly (see Supplementary Checklist, Supplemental Digital Content 1, http://links.lww.com/PHM/B393).
Study Design and Variable Definitions
This retrospective cohort study includes all consecutive, unique patients admitted to inpatient rehabilitation hospital from May 1 to November 15, 2020, after a hospitalization primarily for COVID-19 infection and related complications. Patients who tested positive for COVID-19 during their inpatient hospitalization were not included if their primary reason for admission was felt to be due to other causes by the study team. To maximize comparability, the comparator cohort of non–COVID-19–infected inpatient rehabilitation patients was restricted to those admitted with impairment codes of “debility,” “other pulmonary,” and “polyneuropathy,” which were the most common rehabilitation admission impairment codes for the COVID-19–infected population (accounting for 86% of impairment codes). Only patients who were admitted in 2019 were included in the comparison group to ensure a population completely free of individuals with COVID-19.
Information regarding these patients, as well as the comparative patient population, was obtained from the Uniform Data System for Medical Rehabilitation database, which is used to track outcomes from more than 80% of inpatient rehabilitation facilities in the United States. Data collected included demographics (e.g., age, sex, ethnicity, insurance status, and preadmission living arrangement), presence of comorbid conditions (as defined by International Classification of Diseases, 10th Revision, codes) and impairment codes at admission. In addition, data were collected on admission source, length of stay (LOS), and discharge disposition.
Assessment and Functional Measures
All patients underwent a customized inpatient rehabilitation protocol, which included therapies aimed at improving mobility, self-care, and independent functioning. All patients had at least 3 hrs of therapy per day, a minimum of 5 days per week, which included physical therapy and occupational therapy. If needed, speech therapy was included in the 3 hrs per day total.
All admitted patients underwent the same standardized assessments. Functional assessments conducted at the time of admission evaluated the patient’s motor and cognitive functioning.
Self-care and mobility were assessed at time of admission and time of discharge using the summed totals from items included in Section GG0130 (self-care) and GG1070 (mobility) of IRF-PAI Version 3.0. The IRF-PAI is required by the Centers for Medicare and Medicaid Services for all inpatient rehabilitation facilities and gathers data on the outcomes of inpatient rehabilitation. Section GG is composed of a standardized set of patient assessments outlined in the Postacute Care Transformation Act (IMPACT). Self-care measures include eating, oral hygiene, toilet hygiene, shower/bathing, upper body dressing, lower body dressing, and putting on/taking off footwear. Mobility measures include abilities to roll left and right in bed, to go from sitting to lying and vice versa while in bed, to go from sit to stand, to transfer (from toilet, chair, and car), to walk several distances and surfaces, and to take stairs. Each item is scored on an ordinal scale from 1 (dependent) to 6 (independent).17 These measures have undergone a rigorous analysis by the Centers for Medicare and Medicaid Services to demonstrate reliability and validity.18
Other required elements of the IRF-PAI include the quality indicator motor score and the Brief Interview for Mental Status. The quality indicator motor score is a weighted sum of functioning in dimensions of: eating, oral hygiene, toileting, showering/bathing, upper and lower body dressing, including footwear, sit to lying, lying to sitting on side of bed, sit to stand, transferring, and walking. It also includes assessments of bladder and bowel continence. Cognitive functioning was assessed using the Brief Interview for Mental Status,19 which is a short performance-based cognitive measure for inpatient rehabilitation and skilled nursing home patients.
Data Analysis
The cohort of COVID-19 inpatient rehabilitation patients at the study health system was compared with inpatient rehabilitation patients treated in 2019 (i.e., non–COVID-19–infected patients) at the same facility using standard t and Fisher’s exact statistical tests.
RESULTS
Table 1 presents summary statistics for the 43 COVID-19 inpatient rehabilitation patients included in the study cohort. Four patients had a history of a positive COVID test incidental to their main reason for admission and were excluded from analysis (one traumatic brain injury, one traumatic spinal cord injury, one nontraumatic spinal cord injury, and one amputation). Of those 43, 25 (58%) were African American, 12 (28%) White, 2 (5%) were Hispanic, and 4 (9) belonged to other ethnic groups or were unknown. The mean age of the group was 62.6 yrs (SD = 12.5 yrs) and 26 (60%) were male. Eight (19%) were covered by Medicaid insurance plans and 20 (47%) had a Medicare plan. Five (12%) lived alone at the time of their admission. The mean body mass index was 30.1 (SD = 7.9). The mean LOS in the rehabilitation hospital among COVID-19 patients was 20.5 days (SD = 11.8 days). Nearly three quarters, 31 (72%), were discharged from rehabilitation to home (with or without home health), 5 (12%) to a skilled nursing facility, and 5 (12%) were transferred back to an acute care hospital.
TABLE 1.
Sociodemographic characteristics
| COVID-19 Patients (n = 43) | Non-COVID Patientsa (n = 247) | P | |
|---|---|---|---|
| Age, mean (SD), yr | 62.6 (12.5) | 59.2 (14.8) | 0.16 |
| Male, n (%) | 26 (60) | 154 (62) | 0.82 |
| Ethnicity, n (%) | <0.0001 | ||
| African American/Black | 25 (58) | 48 (19) | |
| Hispanic | 2 (5) | 11 (4) | |
| White | 12 (28) | 171 (69) | |
| Other/unknown | 4 (9) | 17 (7) | |
| Body mass index, mean (SD) | 30.0 (7.9) | 29.8 (23.3) | 0.96 |
| Primary payer, n (%) | 0.39 | ||
| Medicare FFS | 13 (30) | 88 (36) | |
| Medicare advantage | 7 (16) | 37 (15) | |
| Medicaid | 8 (19) | 33 (13) | |
| HMO plan | 4 (9) | 49 (20) | |
| Private insurance | 11 (26) | 40 (16) | |
| Preadmit living arrangement, n (%) | 0.86 | ||
| Alone | 5 (12) | 34 (14) | |
| With family | 36 (84) | 194 (79) | |
| With others | 2 (5) | 19 (8) | |
| Admission source = LTACH, n (%) | 8 (19) | 12 (5) | 0.0011 |
| Length of stay, mean (SD), d | 20.5 (11.8) | 14.3 (7.7) | <0.0001 |
| Discharge destination, n (%) | 0.04 | ||
| Home without home health | 2 (5) | 41 (17) | |
| Services | 29 (67) | 141 (57) | |
| Home with home health Services | 5 (12) | 49 (20) | |
| Acute rehospitalization | 5 (12) | 14 (6) | |
| SNF | 2 (5) | 2 (1) | |
| Unknown |
a Non-COVID patients refer to the subset of patients admitted to the study facility during 2019 (prepandemic) with impairment groups 16, 10.9, and 3.3.
LTACH, long-term acute care hospital.
As shown in Table 1, inpatient rehabilitation patients admitted with a primary diagnosis of COVID-19 differed from the non–COVID-19 group in several dimensions. COVID-19 patients were nearly 3 times more likely to be African American/Black (58.0% vs. 19.4%, respectively, P < 0.001), were more likely to be admitted from a long-term acute care hospital (18.6% vs. 4.9%, P < 0.0001), and had a significantly longer LOS in rehabilitation (20.5 vs. 14.3 days, P = 0.033). Although there was no statistically significant difference in the likelihood of discharge home (with or without home health care), COVID-19 patients were less likely to be readmitted to an acute care hospital (11.6% vs. 19.8%, P = 0.04) but more likely to be discharge to a SNF (11.6% vs. 5.7%, P = 0.04) than non–COVID-19 patients.
In Table 2, we present and contrast the health and functioning characteristics at admission of COVID-19 and non–COVID-19 patients admitted to inpatient rehabilitation. COVID-19 patients had lower quality indicator motor scores at admission than their non–COVID-19 counterparts (48.2 vs. 57.8, respectively, P = 0.0001). Differences in cognitive functioning at admission were smaller in magnitude and not statistically significant at conventional levels (12.7 vs. 13.4, respectively, P = 0.14). In the lower panel of Table 2, we describe the top 20 comorbidities and complications by International Classification of Diseases, 10th Revision, codes of patients admitted to inpatient rehabilitation with COVID-19.
TABLE 2.
Health and functioning of COVID and non-COVID patients at admission
| COVID-19 Patients (n = 43) | Non-COVID Patientsa (n = 247) | P | |
|---|---|---|---|
| QI motor score at admission, mean (SD) | 48.2 (15.5) | 57.8 (14.3) | 0.0001 |
| BIMS summary score at admission, mean (SD) | 12.7 (4.0) | 13.4 (2.6) | 0.14 |
| Comorbidities at admissionb, n (%) | |||
| Essential (primary) hypertension | 20 (47) | 82 (33) | 0.092 |
| Severe protein-calorie malnutrition | 18 (42) | 90 (36) | 0.49 |
| Dysphagia | 17 (40) | 61 (25) | 0.043 |
| Type 2 diabetes | 15 (35) | 54 (22) | 0.06 |
| Anemia | 14 (33) | 55 (22) | 0.14 |
| Hyperlipidemia | 12 (28) | 56 (23) | 0.46 |
| Obesity | 11 (26) | 26 (11) | 0.006 |
| Obstructive sleep apnea | 10 (23) | 37 (15) | 0.17 |
| Long-term use of anticoagulants | 10 (23) | 45 (18) | 0.43 |
| Anxiety disorder | 8 (19) | 58 (24) | 0.48 |
| Gastroesophageal reflux disease | 8 (19) | 85 (34) | 0.041 |
| Insomnia | 8 (19) | 24 (10) | 0.085 |
| Tracheostomy present | 8 (19) | 21 (9) | 0.042 |
| Gastrostomy tube present | 8 (19) | 10 (4) | 0.0002 |
| Personal history of nicotine | 8 (19) | 44 (18) | 0.90 |
| Dependence on supplemental oxygen | 7 (16) | 6 (2) | <0.0001 |
| History of extracorporeal membrane | 6 (14) | 36 (15) | 0.92 |
| Oxygenation | |||
| Acute kidney failure | 6 (14.0) | 50 (20) | 0.34 |
| Major depressive disorder | 5 (12) | 40 (16) | 0.44 |
| Sacral pressure ulcer | 5 (12) | 13 (5) | 0.11 |
a Non-COVID patients refer to the subset of patients admitted to the study facility during 2019 (prepandemic) with impairment group codes of 16, 10.9, and 3.3.
b Subset of 20 most prevalent comorbidities or complications (International Classification of Diseases, 10th Revision, codes) documented at admission for the inpatient rehabilitation COVID population.
BIMS, Brief Interview for Mental Status; QI, quality indicator.
Figure 1 shows self-care and mobility functioning scores at admission and discharge for COVID-19 and non–COVID-19 inpatient rehabilitation patients. For both metrics, COVID-19 patients scored lower at admission than their non–COVID-19 counterparts. For self-care, COVID-19 patients scored 2.6 points lower than non–COVID-19 patients (21.5 vs. 24.1, P = 0.02). Differences were more pronounced with respect to mobility scores with COVID-19 patients scoring on average 8.8 points less than the non–COVID-19 group (28.6 vs. 37.4, P < 0.0001). There was no difference across groups in the discharge assessments for either metric, suggesting that inpatient rehabilitation improved functioning of COVID-19 patients to the level of non–COVID-19 individuals, despite their lower functioning at admission. On average, there was a 41% improvement in self-care scores among COVID-19 patients from 21.5 at admission to 30.3 at discharge (P = 0.01). Mobility scores improved by 93% from 28.6 to 55.1 (P < 0.001). Improvements in self-care and mobility functioning between admission and discharge, although evident, were less marked for non–COVID-19 patients (26% and 54% increase in scores, respectively).
FIGURE 1.
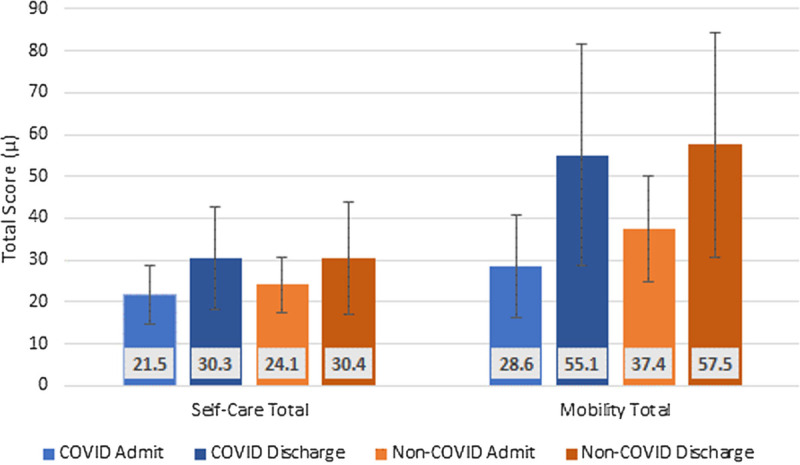
Admission and discharge scores for self-care and mobility for COVID and non-COVID patients.
DISCUSSION
COVID-19 is a disease characterized by damage to multiple organ systems and can lead to significant physical and cognitive impairment along with PICS in those who were critically ill. Despite this, few patients hospitalized with COVID-19 infection are discharged to acute rehabilitation and the characteristics and outcomes of these patients are unknown. Those persons admitted to inpatient rehabilitation likely represent patients with the most profound impairments after their acute infections.
The current study found that COVID-19 patients had significantly lower functional status at admission to inpatient rehabilitation relative to non–COVID-19 patients admitted with similar impairment codes. The current data also suggest that COVID-19 patients are more medically complex, as evidenced by their higher rate of admissions from long-term acute care hospitals and longer LOS. Perhaps most importantly, despite greater deficits at admission, COVID-19–infected patients eventually reach similar functional outcomes and were less likely to be readmitted to the acute care hospital than those admitted to inpatient rehabilitation with etiologies not due to COVID-19 infection.
Our study contributes to the emerging literature on the benefits of rehabilitation to patients admitted to inpatient rehabilitation after COVID-19 infection. Three European studies have demonstrated improvement after inpatient rehabilitation programs. Improvements were found in physical performance status, ability to perform ADLs, and pulmonary measures. These studies have limited comparability to the current study given significantly lower amount of time in rehabilitation, greater focus on pulmonary rehabilitation, and lack of a comparison group.20–22
There have also been a limited number of studies describing the characteristics and outcomes of patients undergoing inpatient rehabilitation after hospitalization with COVID-19 in the United States. Olezene et al.23 (2021) evaluated the effectiveness of inpatient rehabilitation for 29 patients presenting after COVID-19 infection, showing statistically significant improvements in mobility, cognition, speech, swallowing, and balance by time of discharge. Jain et al.24 (2021) examined the outcomes of 64 patients admitted to acute inpatient rehabilitation after COVID-19. They also compared 18 patients admitted to inpatient rehabilitation after an admission for COVID-19 to 18 patients with the same impairment code and similar ages. They found that individuals with COVID had similar functional outcomes, longer LOSs, and more cognitive symptoms compared with the comparison group.24
The US system of inpatient rehabilitation is highly formalized and regulated, guided by strict rules for admission and treatment, including the requirement of 15 hrs per week of rehabilitation, mandated by the Centers for Medicare and Medicaid Services, the agency responsible for the largest public health insurance programs in the country. In contrast to previous literature, our study leverages these mandatory standardized assessments by using uniform outcome metrics, thereby enabling us to make more direct, valid comparisons across COVID and non-COVID patients both at admission and discharge.
Our findings highlight the potential of inpatient rehabilitation in restoring functioning of even the sickest patients with COVID-19. Patients in the study experienced marked improvement in their motor and self-care scores during their stay. By providing intensive therapies targeted at improving respiratory function, exercise endurance, and self-care with basic and instrumental ADLs, inpatient rehabilitation offers a promising pathway to mitigate some of the well-documented long-term sequelae of COVID-19.25–28
Patients admitted to the study inpatient rehabilitation facility after COVID-19 infection were almost 3 times more likely to be African American/Black than the non–COVID-19 group. This finding is consistent with previous evidence suggesting that African Americans are more likely to test positive, to be hospitalized, and to experience more severe COVID-19–related outcomes.29,30 Taken together, the higher prevalence of African Americans receiving inpatient rehabilitation and the overall better outcomes of patients treated in this setting suggest that inpatient rehabilitation may be a means of reducing racial disparities in outcomes after COVID hospitalization. This is critically important as underserved and other marginalized patient populations may be unable to return to their pre-COVID independent living arrangement in the absence of these posthospitalization resources compared with more affluent patients.
It is worth reiterating that to qualify as inpatient rehabilitation facility in the United States, at least 60% of admissions must be patients having one of 13 specific qualifying conditions. Debility after COVID-19, PICS and post–COVID-19 syndrome would generally not qualify outside of documented critical illness polyneuropathy. Furthermore, insurance providers often attempt to stop admissions to acute rehabilitation or may limit admissions to certain qualifying conditions. This study suggests that patients who were admitted with COVID-19 sequelae may also benefit from inpatient rehabilitation and Centers for Medicare and Medicaid Services and insurance rules may need to be modified to accommodate this patient cohort.
There are several important limitations to this study. Given its retrospective nature, patients were only evaluated in a limited number of domains. There have been recommendations for a standardized set of comprehensive measures for the COVID patient population to more uniformly analyze treatment protocols and efficacy.31 In addition, patients admitted to acute rehabilitation are possibly a selected group more likely to benefit from such services. For this reason, our findings may not be generalizable to the larger population of SARS-CoV-2 infected–patients. Finally, although we attempted to homogenize the samples by selecting the comparison group to be comprised of inpatient rehabilitation patients likely to experiencing non-COVID–related PICS, there may be unmeasured differences given the broad range of diagnoses in the comparison cohort (in addition to the baseline differences discussed). For these reasons, although consistent with the small but growing literature on the subject, our findings must be interpreted with caution as the greater improvement in the COVID-19 cohort may also represent a regression to the mean effect.
Despite these limitations, the use of validated standardized outcome measures applied consistently to COVID patients and a comparison group of non-COVID inpatient rehabilitation subjects admitted with similar impairments is a unique strength of this study. Use of impairment group codes is relevant as it is the measure used by Medicare and other third-party payers to determine expected outcomes, cost, reimbursement, and LOS of acute inpatient rehabilitation. The comparison group was drawn from 2019, a period when the inpatient rehabilitation units were under the same regulatory requirements and the same set of data metrics were routinely collected as part of the regulatory requirements for inpatient rehabilitation centers. Similar types of care were given, and similar hours of care per week were provided across COVID-19 and the control group from a year earlier. This strengthens our findings and provides a benchmark for interpreting the functional outcomes of a smaller group of persons infected with COVID-19 undergoing acute inpatient rehabilitation.
CONCLUSIONS
Although COVID-19 patients had worse function at the time of their admission, early patient-centered rehabilitation therapies received at an inpatient setting resulted in discharge outcomes similar to those of non-COVID patients, suggesting that inpatient rehabilitation is an effective strategy to restore functioning to the large and growing number of COVID-19 survivors.
Footnotes
Supported in part by a research grant from the National Institute on Aging (NIA) to Drs Dillingham and Pezzin (5-R01-AG058718).
Financial disclosure statements have been obtained, and no conflicts of interest have been reported by the authors or by any individuals in control of the content of this article.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.ajpmr.com).
Contributor Information
Benjamin A. Abramoff, Email: ben.abramoff@gmail.com.
Timothy R. Dillingham, Email: Timothy.Dillingham@pennmedicine.upenn.edu.
Franklin E. Caldera, Email: Franklin.Caldera@pennmedicine.upenn.edu.
Marylyn D. Ritchie, Email: marylyn@pennmedicine.upenn.edu.
REFERENCES
- 1.Centers for Medicare and Medicaid Sevices : A weekly surveillance summary of U.S. COVID-19 activity. COVIDVIew. Available at: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html. Accessed December 20, 2020
- 2.Rodriguez-Morales AJ Cardona-Ospina JA Gutiérrez-Ocampo E, et al. : Clinical, laboratory and imaging features of COVID-19: a systematic review and meta-analysis. Travel Med Infect Dis 2020;34:101623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Anesi GL: Coronavirus disease 2019 (COVID-19): critical care and airway management issues. UpToDate 2020;2019(Cdc):1–40 [Google Scholar]
- 4.Rosenthal N Cao Z Gundrum J, et al. : Risk factors associated with in-hospital mortality in a US national sample of patients with COVID-19. JAMA Netw Open 2020;3:e2029058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mikkelsen ME Still M Anderson BJ, et al. : Society of Critical Care Medicine’s international consensus conference on prediction and identification of long-term impairments after critical illness. Crit Care Med 2020;48:1670–9 [DOI] [PubMed] [Google Scholar]
- 6.Marra A Pandharipande PP Girard TD, et al. : Co-occurrence of post–intensive care syndrome problems among 406 survivors of critical illness. Crit Care Med 2018;46:1393–401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Frithiof R Rostami E Kumlien E, et al. : Critical illness polyneuropathy and myopathy in COVID-19 patients: a prospective observational intensive care unit cross-sectional cohort study. Research Square 2020:1–31. doi: 10.21203/rs.3.rs-78038/v1 [DOI] [Google Scholar]
- 8.Wong AW Shah AS Johnston JC, et al. : Patient-reported outcome measures after COVID-19: a prospective cohort study. Eur Respir J 2020;56:2003276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Halpin SJ McIvor C Whyatt G, et al. : Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: a cross-sectional evaluation. J Med Virol 2021;93:1013–22 [DOI] [PubMed] [Google Scholar]
- 10.Carfì A, Bernabei R, Landi F: Persistent symptoms in patients after acute COVID-19. JAMA 2020;324:603–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Goërtz YMJ Van Herck M Delbressine JM, et al. : Persistent symptoms 3 months after a SARS-CoV-2 infection: the post-COVID-19 syndrome? ERJ Open Res 2020;6:00542–2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Xiong Q Xu M Li J, et al. : Clinical sequelae of COVID-19 survivors in Wuhan, China: a single-centre longitudinal study. Clin Microbiol Infect 2020;27:89–95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.National Institutes of Health : The NIH Director, NIH launches new initiative to study “Long COVID,” February 23, 2021. Available at: https://www.nih.gov/about-nih/who-we-are/nih-director/statements/nih-launches-new-initiative-study-long-covid. Accessed April 23, 2021
- 14.Simpson R, Robinson L: Rehabilitation after critical illness in people with COVID-19 infection. Am J Phys Med Rehabil 2020;99:470–4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Korupolu R Francisco G Levin H, et al. : Rehabilitation of critically ill COVID-19 survivors. J Int Soc Phys Rehabil Med 2020;3:45 [Google Scholar]
- 16.Lavery AM Preston LE Ko JY, et al. : Characteristics of hospitalized COVID-19 patients discharged and experiencing same-hospital readmission—United States, March–August 2020. MMWR Morb Mortal Wkly Rep 2020;69:1695–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Centers for Medicare and Medicaid Services : IRF-PAI Manual Version 3.0. Available at: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/IRFPAI. Accessed June 27, 2021
- 18.RTI International : Specifications for the function quality measures adopted in the inpatient rehabilitation facility quality reporting program. 2019. Available at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Post-Acu
- 19.Thomas KS Dosa D Wysocki A, et al. : The Minimum Data Set 3.0 Cognitive Function Scale. Med Care 2017;55:e68–72 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Piquet V Luczak C Seiler F, et al. : Do patients with COVID-19 benefit from rehabilitation? Functional outcomes of the first 100 patients in a COVID-19 rehabilitation unit. Arch Phys Med Rehabil 2021;102:1067–74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Puchner B Sahanic S Kirchmair R, et al. : Beneficial effects of multi-disciplinary rehabilitation in postacute COVID-19: an observational cohort study. Eur J Phys Rehabil Med 2021;57:189–98 [DOI] [PubMed] [Google Scholar]
- 22.Curci C Negrini F Ferrillo M, et al. : Functional outcome after inpatient rehabilitation in postintensive care unit COVID-19 patients: findings and clinical implications from a real-practice retrospective study. Eur J Phys Rehabil Med 2021;57:443–50 [DOI] [PubMed] [Google Scholar]
- 23.Olezene CS Hansen E Steere HK, et al. : Functional outcomes in the inpatient rehabilitation setting following severe COVID-19 infection. PLoS One 2021;16:e0248824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jain E, Harmon EY, Sonagere MB: Functional outcomes and post-discharge care sought by patients with COVID-19 compared to matched controls after completing inpatient acute rehabilitation. PM R 2021;13:618–25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Li J: Rehabilitation management of patients with COVID-19: lessons learned from the first experience in China. Eur J Phys Rehabil Med 2020;56:335–8 [DOI] [PubMed] [Google Scholar]
- 26.Lew HL Oh-Park M Cifu DX, et al. : The war on COVID-19 pandemic: role of rehabilitation professionals and hospitals. Am J Phys Med Rehabil 2020;99:571–2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sheehy LM: Considerations for postacute rehabilitation for survivors of COVID-19. JMIR Public Health Surveill 2020;6:e19462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Shan MX Tran YM Vu KT, et al. : Postacute inpatient rehabilitation for COVID-19. BMJ Case Rep 2020;13:e237406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yancy CW: COVID-19 and African Americans. JAMA 2020;323:1891–2 [DOI] [PubMed] [Google Scholar]
- 30.Muñoz-Price LS Nattinger AB Rivera F, et al. : Racial disparities in incidence and outcomes among patients with COVID-19. JAMA Netw Open 2020;3:e2021892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Carneiro I Costa AJ Lima A, et al. : Protocol proposal to the initial assessment of the post-intensive care syndrome in COVID-19 patients, in an inpatient rehabilitation setting. Rehabilitacion (Madr) 2020;55:82. [DOI] [PMC free article] [PubMed] [Google Scholar]