

Abstract
Pressure-mediated reflection spectroscopy (RS) measures skin carotenoid content (SCC). Continued validation of this method is pertinent to validate its use as an objective measure of fruit and vegetable intake. This study aimed to assess relationships between SCC scores and self-reported dietary carotenoid intake from 3-day food records in community dwelling older adults. This was a cross-sectional analysis of baseline data among cognitively normal older adults (n=95) participating in the Nutrition Interventions for Cognitive Enhancement (NICE) study. Food-derived vitamin A (R=0.24, p<0.05) and food plus supplemental vitamin A (R=0.29, p<0.01) were correlated with SCC. All food-derived carotenoids (R: 0.20-0.39, p<0.05) except beta-cryptoxanthin and lycopene were correlated with SCC. Lutein + zeaxanthin from food more strongly correlated with SCC (R=0.38, p<0.001) than combined food plus supplemental intake (R=0.31, p=0.002). Correlations for total fruit and SCC (R=0.23, p=0.02), total vegetable and SCC (R= 0.31, p=0.002), and combined total fruit and vegetable and SCC (R=0.35, p<0.001) were significant; no sub-categories of fruit or vegetables except dark green vegetables (Rho=0.4, p<0.001) had significant correlations with SCC. The current study demonstrates RS-derived SCC scores correlate with 3-day self-reported intakes of F/V and certain carotenoids in community dwelling older adults.
Keywords: skin carotenoid content, fruit and vegetable intake, older adults, pressure-mediated reflection spectroscopy, self-reported dietary intake
1. Introduction
Carotenoids are a class of bioactive terpenoids that exist in photosynthetic plants, bacteria and fungi and are absorbed by humans through dietary intake (von Lintig and Quadro, 2020). Carotenoids are pigments in plants and are responsible for the dark green, red, yellow, and orange appearance of many fruits and vegetables. Of the hundreds of these carotenoids that exist, only a small number are sufficient in the human diet to be detected through various measurement methods. Carotenoids found in the greatest abundance in human samples are lycopene, beta-carotene, alpha-carotene, beta-cryptoxanthin, zeaxanthin, and lutein (Eggersdorfer and Wyss, 2018; Moran et al., 2018). Fruit and vegetable (F/V) intake has long been positively correlated with a variety of beneficial health outcomes and much of their benefit is derived from the antioxidant action of carotenoids. Carotenoid intake has been associated with reduced cancer risk (Rowles and Erdman, 2020; Slattery et al., 2000; Wu et al., 2020), eye health (Schalch et al., 2007), immune system function (Sommer et al., 1986; Sommer et al., 2008), reduced risk of cardiovascular disease (CVD) and reduced all-cause mortality (Aune et al., 2018). Although there are controversial data surrounding risks and/or benefits of carotenoid supplementation in various groups, it is common, especially in the aging population. In general, dietary carotenoids are thought to reduce chronic disease risk and therefore should be emphasized as part of a healthy eating pattern across the lifespan.
Skin carotenoid content (SCC) measured by pressure-mediated spectroscopy has been validated to correlate with plasma carotenoid concentration in a number of populations (Beccarelli et al. 2017; Jilcott Pitts et al., 2018; May et al., 2020; Nagao-Sato, 2021; Nguyen et al., 2015; Rush et al., 2020). The measurement of SCC offers potential as an objective biomarker for F/V intake in large cohort studies, community initiatives, and clinical interventions (May et al., 2020). The non-invasive measurement of SCC expands the opportunity to study the potential benefits of carotenoids and the accompanying measurement of objective markers for F/V intake with dietary intake data may help overcome inherent limitations to self-reported dietary intake. Although relationships between skin and plasma carotenoids have been analyzed in non-community-dwelling older adults (Hill et al., 2021), to our knowledge, SCC has not been studied in cognitively normal, generally healthy older adults who are community-dwelling in the US. Our aim in this study was to assess the relationship between SCC and self-reported dietary and supplement intake from three-day food records (3DFR) in this study population.
2. Materials and Methods
This was a cross-sectional analysis using baseline data collected among cognitively normal older adults in the Greater Kansas City metropolitan area participating in the Nutrition Interventions for Cognitive Enhancement (NICE) study (NCT03841539). This study was approved by the University of Kansas Medical Center Institutional Review Board. Informed consent was obtained for all participants.
2.1. Setting and participants
The NICE study is a randomized dietary intervention to evaluate the effects of a Mediterranean diet versus a low-fat diet on cognitive function in cognitively normal older adults (≥ 65 years, MMSE ≥ 25). The study will randomize and enroll 200 participants to follow either the Mediterranean or low-fat diet intervention for 12 months. For this cross-sectional study, baseline (prior to randomization) self-reported dietary intake data and SCC scores were available for n=98 participants and were collected between April 2019 and September 2020. Major inclusion criteria included normal cognition (Mini-Mental State Examination score ≥ 25; AD8 dementia screening interview score of 2 or less; no prior diagnosis of mild cognitive impairment (MCI), Alzheimer’s Disease, or dementia; and not medically treated for cognitive impairment or dementia) and individuals who were not currently following either a Mediterranean or low fat eating pattern. Exclusion criteria included serious medical risk (type I diabetes mellitus, cancer requiring chemotherapy or radiation therapy within 6 months, cardiac event within 6 months), BMI lower than 20kg/m2 or higher than 40kg/m2, inability to control dietary intake, current use of the drug Warfarin, and inability to read or speak English.
2.2. Skin carotenoid content
SCC was measured at the initial study visit using the portable Veggie Meter® (Longevity Link Corporation, Holladay, UT) device which uses pressure-mediated reflection spectroscopy. The Veggie Meter® has been validated in groups such as racially diverse adolescents and adults (Jilcott et al., 2018; Nagao-Sato et al., 2021), school-aged children (Beccarelli et al., 2017; May et al., 2020; Nguyen et al., 2015), and adults of varying body size (Rush et al., 2020). Participants were instructed to wash and dry their hands prior to measurement. Participants placed their right index finger into the Veggie Meter® device, a small mechanical arm was lowered onto the finger to apply pressure, and broadband white light was reflected onto the index finger to measure carotenoid content. Three measurements were taken and averaged for a final SCC score between 0 and 800.
2.3. Self-reported dietary and supplement intake
Participants were provided blank 3-day food records (3DFRs) and a Food Amounts Booklet (Valencia and Stevens, 2007; Van Horn et al., 1993) at the initial visit. Study dietitians explained how to fill out the 3DFRs and how to use the Food Amounts Booklet for estimated serving sizes. The 3DFRs included dietary intake information for two weekdays and one weekend day within 7-10 days of instruction and SCC measurement. Participants were instructed to follow their normal eating habits during the recorded period. The records also included daily supplement intake information including brand, dosage, and frequency of intake. A dietitian reviewed 3DFRs with participants to obtain any necessary clarification at the baseline visit.
Study dietitians entered food and supplement data from the 3DFRs into the Nutrition Data System for Research (NDSR, version 2019) to quantify energy, food, and nutrient intake. We used NDSR output variables for vitamin A, individual carotenoids, and fruit and vegetables. Although the NDSR database provides output data for individual carotenoids, certain dietary supplement brand data is unavailable due to insufficient product information. In these instances, NDSR reports individual carotenoid intake from dietary supplements as zero. Because the NDSR database did not provide data for beta-carotene, alpha-carotene, nor beta-cryptoxanthin from the specific supplements that were consumed by participants in this study, we could not calculate total intake of these carotenoids derived from both food and supplements.
2.4. Anthropometrics
Body weight and height were measured at baseline. Weight was obtained using a digital scale (± 0.1 kg; Befour Inc model #PS6600, Saukville, WI) and height was measured using a stadiometer (Model PE-WM-60-84, Perspective Enterprises, Portage, MI). Body mass index (kg/m2) was calculated using these measurements.
3. Statistical analysis
The primary aim of this study was to investigate the correlation of SCC with the 3-day average intake of individual food-derived carotenoids, individual food- and supplement-derived (F+S-derived) carotenoids, and fruits and vegetables. Three participants were determined to have implausible 3-day average energy intake (n=2 consuming <700 kcals and n=1 consuming >5500 kcals) and were removed from the analysis. Continuous values were expressed as mean ± SDs. We used correlation analyses to assess relationships between our intake variables and SCC. Because correlation analyses are reflective of linear relationships, we assessed all models for linear model assumptions using residual analyses, including residual histograms, QQplots, and scale-location plots. We used Pearson’s correlations for all models that satisfied model assumptions. Several dietary variables were zero-inflated, thus we used Spearman correlations to determine rank correlation with SCC. We also constructed separate ordinary least squares regression models using SCC as the dependent variable and total vegetables, total fruit, and fruit and vegetables as independent variables to calculate regression coefficients for these specific relationships. Statistical analyses were performed using R (v. 3.6.1; R Foundation, Vienna, Austria). Statistical significance was two-tailed and set at p < 0.05.
4. Results
Baseline data from 95 NICE Study participants aged 65 to 86 years (72.0 ± 5.1) with plausible energy intake were included in this analysis. Participant demographic and dietary intake data are presented in Table 1. Briefly, participants were predominantly white (89.4%), female (80.0%), and had a BMI of 28.6 ± 4.7 kg/m2.
Table 1.
Participant characteristics and dietary intake.
| N=95 | |
|---|---|
| Participant Characteristics | |
| Age (years) | 72.0 ± 5.0 |
| Sex | |
| Female | 76 (80%) |
| Male | 19 (20%) |
| Ethnicity | |
| Hispanic/Latino | 2 (2.1%) |
| Not Hipanic/Latino | 89 (93.7%) |
| Unknown | 4 (4.2%) |
| Race | |
| White | 85 (89.4%) |
| Black or African American | 7 (7.4%) |
| Other | 1 (1.1%) |
| Unknown | 2 (2.1%) |
| BMI (kg/m2) | 28.6 ± 4.7 |
| Skin Carotenoid Content | 272 ± 78.6 |
| Dietary Intake | |
| Energy (kcal) | 1700 ± 510 |
| Total Fat (g) | 75 ± 27 |
| Total Carbohydrate (g) | 183 ± 63 |
| Total Protein (g) | 69 ± 23 |
| Food-Derived Carotenoids | |
| Total Vitamin A (IU) | 8500 ± 6070 |
| Beta-Carotene (mcg) | 3950 ± 3260 |
| Alpha-Carotene (mcg) | 710 ± 950 |
| Beta-Cryptoxantdin (mcg) | 120 ± 280 |
| Lutein + Zeaxantdin (mcg) | 2170 ± 2480 |
| Lycopene (mcg) | 4750 ± 5500 |
| F+S-Derived Carotenoids | |
| Total Vitamin A (IU) | 9690 ± 6320 |
| Beta-Carotene (mcg) | 3950 ± 3260 |
| Alpha-Carotene (mcg) | 710 ± 950 |
| Beta-Cryptoxantdin (mcg) | 120 ± 280 |
| Lutein + Zeaxantdin (mcg) | 3580 ± 6010 |
| Lycopene (mcg) | 4800 ± 5500 |
| Fruit (servings*) | |
| Citrus Fruit | 0.1 ± 0.3 |
| Other Fruit | 1.6 ± 1.2 |
| Total Fruit | 2.0 ± 1.4 |
| Vegetables (servings*) | |
| Dark Green Vegetables | 0.6 ± 0.9 |
| Deep Yellow Vegetables | 0.3 ± 0.4 |
| Tomato | 0.5 ± 0.5 |
| Other Starchy Vegetables | 0.1 ± 0.2 |
| Other Vegetables | 1.2 ± 0.9 |
| Vegetable Juice | 0.1 ± 0.4 |
| Total Vegetables | 2.8 ± 1.8 |
| Fruit + Vegetables | 4.8 ± 2.5 |
One serving is defined by the USDA’s 2000 Dietary Guidelines for Americans as 1 medium piece of fruit, 1 cup of raw leafy vegetables, ½ cup raw or cooked fruit and vegetables, or ¼ cup dried fruit.
We first tested the correlation relationships of 3-day average food-derived carotenoids, F+S-derived carotenoids, and fruit and vegetable intake with SCC. Results from all correlation analyses are presented in Table 2. Food-derived vitamin A was correlated with SCC (R=0.24, p<0.05) and was more strongly correlated with SCC when accounting for supplement intake (R=0.29, p<0.01). All food-derived carotenoids (R: 0.20 – 0.39, all p-values <0.05) except for beta-cryptoxanthin and lycopene were correlated with SCC. Lutein and zeaxanthin (L+Z) from food was more strongly correlated with SCC (R=0.38, p<0.001) than combined intake from food and supplements (R=0.31, p=0.002). No individual fruit categories were correlated with SCC; yet, total fruit intake and SCC were correlated (R=0.23, p=0.02). Dark green vegetables and SCC were strongly correlated (Rho=0.4, p<0.001) as was intake of total vegetables (R=0.31, p=0.002). Combined fruit and vegetable intake was also strongly correlated with SCC (R=0.35, p<0.001). The most commonly consumed carotenoid-containing foods by food group category were oranges and tangerines (citrus fruit); bananas, blueberries, and grapes (other fruit); romaine lettuce, spinach, and broccoli (dark green vegetables); carrots and sweet potatoes (deep yellow vegetables); green beans, asparagus, and bell peppers (other vegetables); peas and corn (other starchy vegetables); raw tomatoes and salsa (tomato); and tomato juice (vegetable juice).
Table 2.
Correlation coefficients for the relation of skin carotenoid content with participant characteristics and dietary intake variables.
| Correlation Coefficient | |
|---|---|
| Age | −0.12 |
| BMI | −0.27** |
| Food-Derived Carotenoids | |
| Total Vitamin A (IU) | 0.24* |
| Beta-Carotene (mcg) | 0.25* |
| Alpha-Carotene (mcg) a | 0.20* |
| Beta-Cryptoxanthin (mcg) a | 0.16 |
| Lutein + Zeaxanthin (mcg) | 0.39*** |
| Lycopene (mcg) | 0.10 |
| Total Food Carotenoids (mcg) | 0.29** |
| Food- and Supplement-Derived Carotenoids | |
| Total Vitamin A (IU) | 0.29** |
| Lutein + Zeaxanthin (mcg) | 0.32** |
| Lycopene (mcg) | 0.10 |
| Total Carotenoids (mcg) | 0.33** |
| Fruit | |
| Citrus Juice a | 0.04 |
| Other Fruit Juice a | −0.12 |
| Citrus Fruit a | 0.12 |
| Other Fruit a | 0.14 |
| Total Fruit | 0.23* |
| Vegetables | |
| Dark Green Vegetables a | 0.41*** |
| Deep Yellow Vegetables a | 0.01 |
| Tomato a | −0.04 |
| Other Starchy Vegetables a | 0.10 |
| Other Vegetables a | 0.12 |
| Vegetable Juice a | 0.03 |
| Total Vegetables | 0.31** |
| Fruit + Vegetables | 0.35*** |
Indicates Spearman’s rho
Indicates p<0.05
Indicates p<0.01
lndicates p<0.001
We used OLS regression models of SCC with fruit, vegetable, and fruit + vegetable intake in order to interpret the regression coefficient of these relationships. SCC scores were 28.2 points higher for every cup of vegetables consumed, 27.5 points higher for every cup of fruit consumed, and 22.7 points higher for every cup of combined fruits and vegetables consumed. These relationships are illustrated in Figure 1.
Figure 1.
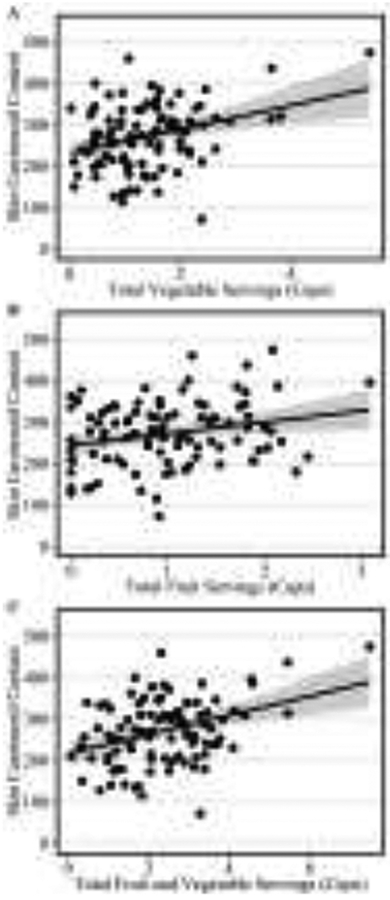
Regression relationships between skin carotenoid content and 3-day average fruit and vegetable intake. A) Illustrates the relationship between vegetable intake and SCC. B) Illustrates the relationship between fruit intake and SCC. C) Illustrates the relationship between combined fruit and vegetable intake and SCC.
5. Discussion
The current study indicates that self-reported dietary intake of vitamin A, carotenoids, and F/V from 3DFRs correlates with SCC scores in cognitively normal older adults. This suggests that short-term, self-reported dietary data aligns with this objective biomarker. Intake of dark green vegetables was most strongly correlated with SCC scores followed by food-derived intake of L+Z. Similar correlation of these two variables with SCC is unsurprising as many dark green vegetables have high L+Z content. These data suggest that these components may be the strongest contributors to carotenoid deposition in the skin and could inform the dietary composition of dietary interventions that aim to raise carotenoid status in older adults.
Total fruit, total vegetable, and combined F/V intake was strongly correlated with SCC scores, though no individual categories of these foods except dark green vegetables had significant relationships with SCC. This is likely due, in part, to limited intake of these specific foods and several foods falling into ‘other fruits’, ‘other vegetables’, or ‘other starchy vegetables’ categories. Our study demonstrates that SCC is a better objective measure of overall fruit, overall vegetable, or combined total F/V intake than individual types of F/V. Additionally, by interpreting our correlation coefficients between total fruit, total vegetable, and combined total F/V and SCC scores, we were able to determine a per-serving estimate of increased SCC for this population. This information can be useful in both intervention studies and clinical settings as researchers and health practitioners who engage older adults in improved F/V intake can more effectively use SCC to establish baseline F/V intake and track diet adherence. Future studies in this population should compare per-serving point estimates to ours in an effort to translate SCC scores to tangible intakes for investigators, practitioners, and the individual.
Unsurprisingly, F+S-derived vitamin A was more strongly correlated with SCC scores than food-derived vitamin A. Supplemental provitamin A is well researched and widely distributed to both prevent and treat a variety of disease states. It is therefore predictable that our results showed an increase in the strength of relationship. Interestingly, our results showed that adding supplemental L+Z to dietary L+Z intake weakened the relationship between L+Z and SCC. Although our sample is relatively small and homogenous, this may suggest that food-derived L+Z contribute more to skin deposition of carotenoids than supplemental sources. There are several potential mechanisms that may contribute to this phenomenon, including the possibility that certain food-derived L+Z is more bioavailable than supplemental L+Z (Eisenhauer et al., 2017) and/or that supplemental formulation (i.e. free versus solubilized carotenoids) impacts absorption and subsequent deposition in skin (Green-Gomez et al., 2020). Green-Gomez et al. recently reported that micellarisation of supplemental zeaxanthin and mesozeaxanthin increased both serum zeaxanthin/mesozeaxanthin and overall SCC scores compared to free formulations. This type of formulation is unlikely to be used by our study population due to its more recent development. Another recent finding by Mansour et al. reported increased absorption of supplemental lutein when ingested alongside bile salts in an animal model (Mansour et al., 2020), thus supporting the hypothesis that solubility of these carotenoids in supplemental formulations impacts bioavailability and therefore deposition in skin. This may account for the weaker relationship between combined dietary and supplemental L+Z and SCC scores in our population. Future studies investigating the relationship between intake of individual carotenoids with SCC and mechanisms of their deposition would be beneficial to aid in understanding the function of food-derived and supplemental carotenoid intake.
Our study was the first to assess the relationship between self-reported dietary intake and SCC in community-dwelling healthy older adults, though other studies have investigated the relationship between SCC and various methods of self-reported F/V intake with mixed results in different populations. Jahns et al. completed a validity trial in 2019 (Jahns et al., 2019) that found pressure-mediated reflection spectroscopy was moderately or strongly correlated with the Automated Self-Administered 24-Hour Dietary Assessment Tool (ASA24) and plasma carotenoid levels in 40-60-year-old women (n=52). This method was more strongly correlated with self-reported F/V intake cross-sectionally than longitudinally, though correlations over time remained significant. Nagao-Sato et al. more recently found significant correlations between 24-hour intake of F/V and pressure-mediated reflection spectroscopy scores in Latino adolescents (Nagao-Sato et al., 2021). Jilcott Pitts et al. (Jilcott Pitts et al., 2018) completed two small pilot studies. In their first study, the authors found no relationship between SCC and F/V intake over the past month using the National Cancer Institute’s (NCI) Fruit and Vegetable Screener in shoppers at a major grocery store chain. Null findings in this study were likely attributed to the brief assessment of total F/V consumption using the NCI screener and that most of the daily vegetables consumed by their study population were fried potatoes and chips, which are a poor source of carotenoids. In their second study, F/V and carotenoid intake measured by the Fred Hutchinson Cancer Research Center food frequency questionnaire was correlated with SCC in African American and non-Hispanic white participants (Jilcott Pitts et al., 2018). May et al. assessed the relationship between self-reported F/V intake using a pictorial liking tool correlated with SCC scores in school-aged children ranging from preschool to high school (May et al., 2020). Fruit intake was positively correlated with SCC scores in high schoolers and soda intake was negatively correlated with SCC scores in all age groups with the authors noting that soda may replace other healthful food items in the diet.
We chose to use 3DFRs as they have been shown to correlate with usual dietary intake (Yang et al., 2010) and are less burdensome for participants compared to 7-day food records. Due to this, we are unsure whether these findings reflect the correlation strength of short-term dietary intake or whether these data reflect a relationship between SCC and more long-term dietary intake. We are also unsure how quickly SCC scores may be affected by abrupt changes in dietary intake and it is possible that results may be confounded by altered dietary habits during the three-day dietary collection period. It is reasonable to hypothesize that dietary intake data from 7-day food records may result in stronger correlation with SCC as they would collect dietary intake over a longer interval, allowing for biological deposition of consumed carotenoids. Future trials should aim to confirm our results and compare the use of different dietary collection methods.
Our study was not without limitations. Our sample size was small and we observed a high report of zero-intake for certain fruit and vegetable sub-categories, thus impacting our distributions. For instance, we were unable to assess the relationship between intake of avocados, a carotenoid-rich fruit, and SCC since >75% of participants reported no avocado intake. Future studies in this population should aim to enroll participants with a range of intake and less zero-inflation. We measured SCC prior to capturing the 3-day dietary intake data and therefore are unsure if the food records reflect similar intake to that which contributed to the SCC score. All participants were told to follow their regular eating pattern, though we cannot say for certain that dietary intake remained consistent. We were unable to adequately assess the impact of supplemental carotenoid intake for three individual carotenoids, which is a major limitation to this study. Food and nutrient databases, such as NDSR, provide excellent support for nutrition researchers, but are not immune to certain limitations. In this instance, we discovered that the supplements consumed by our participants containing beta-carotene, alpha-carotene, and beta-cryptoxanthin were not included in the output for supplemental intake of these specific carotenoids. Thus, each participant had F+S-derived values that were identical to their food-derived values for these carotenoids. For the purpose of this study, manual calculation of these values among hundreds of vitamin A containing supplements would have required a large-scale effort from many study personnel. Including these values in nutrient databases would be beneficial for future carotenoid research, however, we recognize that developing this resource will be a tedious task.
Our study did, however, have its strengths. We assessed the contribution of F/V and F+S-derived carotenoids to SCC in community dwelling, healthy older adults. We were also able to establish estimates of per-serving influence of total fruit, total vegetable, and total combined F/V intake on SCC scores in our population. This is the first study, to our knowledge, investigating SCC and dietary intake in this population and our results are perhaps indicative of real life.
6. Conclusions
The current study demonstrates that pressure-mediated reflection spectroscopy-derived SCC scores correlate with 3-day self-reported intake of F/V and certain carotenoids in community dwelling older adults. This finding further contributes to literature surrounding validation of this technique as an objective measure of carotenoid-containing F/V intake and provides evidence that SCC scores may be influenced in a carotenoid-specific manner.
Highlights.
Pressure-mediated reflection spectroscopy correlates with 3-day intake of fruit and vegetables
This method correlates with carotenoids in free living, healthy older adults
Skin carotenoid content may be influenced in a carotenoid-specific manner
Dark green vegetables are strongly associated with higher skin carotenoid scores
Revision to dietary supplement data in databases is required for analysis
Acknowledgements
This study was supported by the University of Kansas Alzheimer's Disease Center (P30AG035982), the University of Kansas Heartland Clinical Translational Science Award Center (UL1TR002366), the University of Kansas Cancer Center Nutrition Shared Resource (P30CA168524) and the University of Kansas Department of Dietetics and Nutrition.
Funding/Support
This project was supported by the National Institute of Health’s National Institute on Aging (grant no.: AG060157).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Statement of Potential Conflict of Interest
No potential conflict of interest reported by the authors.
References
- 1.Aune D (2019). Plant Foods, Antioxidant Biomarkers, and the Risk of Cardiovascular Disease, Cancer, and Mortality: A Review of the Evidence. Advances in nutrition (Bethesda, Md.), 10(Suppl_4), S404–S421. 10.1093/advances/nmz042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Beccarelli LM, Scherr RE, Dharmar M, Ermakov IV, Gellermann W, Jahns L, Linnell JD, Keen CL, Steinberg FM, Young HM, & Zidenberg-Cherr S (2017). Using Skin Carotenoids to Assess Dietary Changes in Students After 1 Academic Year of Participating in the Shaping Healthy Choices Program. Journal of nutrition education and behavior, 49(1), 73–78.e1. 10.1016/j.jneb.2016.09.007 [DOI] [PubMed] [Google Scholar]
- 3.Dietaryguidelines.gov. 2000. Dietary Guidelines for Americans 2000. [online] Available at: <https://www.dietaryguidelines.gov/sites/default/files/2019-05/2000%20Dietary%20Guidelines%20for%20Americans.pdf> [Accessed 19 October 2021].
- 4.Eggersdorfer M, & Wyss A (2018). Carotenoids in human nutrition and health. Archives of biochemistry and biophysics, 652, 18–26. 10.1016/j.abb.2018.06.001 [DOI] [PubMed] [Google Scholar]
- 5.Eisenhauer B, Natoli S, Liew G, & Flood VM (2017). Lutein and Zeaxanthin-Food Sources, Bioavailability and Dietary Variety in Age-Related Macular Degeneration Protection. Nutrients, 9(2), 120. 10.3390/nu9020120 [DOI] [Google Scholar]
- 6.Green-Gomez M, Prado-Cabrero A, Moran R, Power T, Gómez-Mascaraque LG, Stack J, & Nolan JM (2020). The Impact of Formulation on Lutein, Zeaxanthin, and meso-Zeaxanthin Bioavailability: A Randomised Double-Blind Placebo-Controlled Study. Antioxidants (Basel, Switzerland), 9(8), 767. 10.3390/antiox9080767 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hill CM, Paschall MJ, O'Brien DM, & Bersamin A (2021). Characterizing Vegetable and Fruit Intake in a Remote Alaska Native Community Using Reflection Spectroscopy and 24-Hour Recalls. Journal of nutrition education and behavior, S1499-4046(21)00045-2. Advance online publication. 10.1016/j.jneb.2021.02.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jahns L, Johnson LK, Conrad Z, Bukowski M, Raatz SK, Jilcott Pitts S, Wang Y, Ermakov IV, & Gellermann W (2019). Concurrent validity of skin carotenoid status as a concentration biomarker of vegetable and fruit intake compared to multiple 24-h recalls and plasma carotenoid concentrations across one year: a cohort study. Nutrition journal, 18(1), 78. 10.1186/s12937-019-0500-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jilcott Pitts SB, Jahns L, Wu Q, Moran NE, Bell RA, Truesdale KP, & Laska MN (2018). A non-invasive assessment of skin carotenoid status through reflection spectroscopy is a feasible, reliable and potentially valid measure of fruit and vegetable consumption in a diverse community sample. Public health nutrition, 21(9), 1664–1670. 10.1017/S136898001700430X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mansour AT, El-Feky M, El-Beltagi HS, & Sallam AE (2020). Synergism of Dietary Co-Supplementation with Lutein and Bile Salts Improved the Growth Performance, Carotenoid Content, Antioxidant Capacity, Lipid Metabolism, and Lipase Activity of the Marbled Spinefoot Rabbitfish, Siganus rivulatus. Animals : an open access journal from MDPI, 10(9), 1643. 10.3390/ani10091643 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.May K, Jilcott Pitts S, Stage VC, Kelley CJ, Burkholder S, Fang X, … Lazorick S (2020). Use of the Veggie Meter® as a tool to objectively approximate fruit and vegetable intake among youth for evaluation of preschool and school-based interventions. Journal of Human Nutrition and Dietetics, 33(6), 869–875. doi: 10.1111/jhn.12755 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Moran NE, Mohn ES, Hason N, Erdman JW Jr, & Johnson EJ (2018). Intrinsic and Extrinsic Factors Impacting Absorption, Metabolism, and Health Effects of Dietary Carotenoids. Advances in nutrition (Bethesda, Md.), 9(4), 465–492. 10.1093/advances/nmy025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nagao-Sato S, Baltaci A, Peralta Reyes AO, Zhang Y, Hurtado Choque GA, & Reicks M (2021). Skin Carotenoid Scores Assessed with Reflection Spectroscopy Are Associated with Self-Reported Fruit and Vegetable Intake Among Latino Early Adolescents. Journal of the Academy of Nutrition and Dietetics, S2212-2672(21)00140-4. Advance online publication. 10.1016/j.jand.2021.02.019 [DOI] [PubMed] [Google Scholar]
- 14.Nguyen LM, Scherr RE, Linnell JD, Ermakov IV, Gellermann W, Jahns L, Keen CL, Miyamoto S, Steinberg FM, Young HM, & Zidenberg-Cherr S (2015). Evaluating the relationship between plasma and skin carotenoids and reported dietary intake in elementary school children to assess fruit and vegetable intake. Archives of biochemistry and biophysics, 572, 73–80. 10.1016/j.abb.2015.02.015 [DOI] [PubMed] [Google Scholar]
- 15.Rowles JL 3rd, & Erdman JW Jr (2020). Carotenoids and their role in cancer prevention. Biochimica et biophysica acta. Molecular and cell biology of lipids, 1865(11), 158613. 10.1016/j.bbalip.2020.158613 [DOI] [PubMed] [Google Scholar]
- 16.Rush E, Amoah I, Diep T, & Jalili-Moghaddam S (2020). Determinants and Suitability of Carotenoid Reflection Score as a Measure of Carotenoid Status. Nutrients, 12(1), 113. 10.3390/nu12010113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schalch W, Cohn W, Barker FM, Köpcke W, Mellerio J, Bird AC, Robson AG, Fitzke FF, & van Kuijk FJ (2007). Xanthophyll accumulation in the human retina during supplementation with lutein or zeaxanthin - the LUXEA (LUtein Xanthophyll Eye Accumulation) study. Archives of biochemistry and biophysics, 458(2), 128–135. 10.1016/j.abb.2006.09.032 [DOI] [PubMed] [Google Scholar]
- 18.Slattery ML, Benson J, Curtin K, Ma KN, Schaeffer D, & Potter JD (2000). Carotenoids and colon cancer. The American journal of clinical nutrition, 71(2), 575–582. 10.1093/ajcn/71.2.575 [DOI] [PubMed] [Google Scholar]
- 19.Sommer A, Tarwotjo I, Djunaedi E, West KP Jr, Loeden AA, Tilden R, & Mele L (1986). Impact of vitamin A supplementation on childhood mortality. A randomised controlled community trial. Lancet (London, England), 1(8491), 1169–1173. 10.1016/s0140-6736(86)91157-8 [DOI] [PubMed] [Google Scholar]
- 20.Sommer A (2008). Vitamin a deficiency and clinical disease: an historical overview. The Journal of nutrition, 138(10), 1835–1839. 10.1093/jn/138.10.1835 [DOI] [PubMed] [Google Scholar]
- 21.Valencia A, Stevens M (2007). Nutrition Coordinating Center, University of Minnesota for the Hispanic Community Healthy Study, Study of Latinos. [Google Scholar]
- 22.Van Horn LV, Stumbo P, Moag-Stahlberg A, Obarzanek E. Hartmuller VW, Farris RP, Kimm SY, Frederick M Snetselaar L Liu K (1993). The Dietary Intervention Study in Children (DISC): dietary assessment methods for 8- to 10-year-olds. Journal of the American Dietetic Association, 93(12), 1396–403. [DOI] [PubMed] [Google Scholar]
- 23.von Lintig J, & Quadro L (2020). Biology of carotenoids in mammals. Biochimica et biophysica acta. Molecular and cell biology of lipids, 1865(11), 158754. 10.1016/j.bbalip.2020.158754 [DOI] [PubMed] [Google Scholar]
- 24.Wu S, Liu Y, Michalek JE, Mesa RA, Parma DL, Rodriguez R, Mansour AM, Svatek R, Tucker TC, & Ramirez AG (2020). Carotenoid Intake and Circulating Carotenoids Are Inversely Associated with the Risk of Bladder Cancer: A Dose-Response Meta-analysis. Advances in nutrition (Bethesda, Md.), 11(3), 630–643. 10.1093/advances/nmz120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yang YJ, Kim MK, Hwang SH, Ahn Y, Shim JE, & Kim DH (2010). Relative validities of 3-day food records and the food frequency questionnaire. Nutrition research and practice, 4(2), 142–148. doi: 10.4162/nrp.2010.4.2.142 [DOI] [PMC free article] [PubMed] [Google Scholar]