

Abstract
Objective:
There is limited information regarding neurocognitive outcomes of right unilateral ultrabrief pulse width electroconvulsive therapy (RUL-UB ECT) combined with pharmacotherapy in older adults with major depressive disorder. We report longitudinal neurocognitive outcomes from Phase 2 of the Prolonging Remission in Depressed Elderly (PRIDE) study.
Method:
After achieving remission with RUL-UB ECT and venlafaxine, older adults (≥ 60 years old) were randomized to receive symptom-titrated, algorithm-based longitudinal ECT (STABLE) plus pharmacotherapy (venlafaxine and lithium) or pharmacotherapy-only. A comprehensive neuropsychological battery was administered at baseline and throughout the 6-month treatment period. Statistical significance was defined as a p-value of less than 0.05 (two-sided test).
Results:
With the exception of processing speed, there was statistically significant improvement across most neurocognitive measures from baseline to 6-month follow up. There were no significant differences between the two treatment groups at 6 months on measures of psychomotor processing speed, autobiographical memory consistency, short-term and long-term verbal memory, phonemic fluency, inhibition, and complex visual scanning and cognitive flexibility.
Conclusions:
To our knowledge, this is the first report of neurocognitive outcomes over a 6-month period of an acute course of RUL-UB ECT followed by one of 2 strategies to prolong remission in older adults with major depression. Neurocognitive outcome did not differ between STABLE plus pharmacotherapy versus pharmacotherapy alone over the 6-month continuation treatment phase. These findings support the safety of RUL-UB ECT in combination with pharmacotherapy in the prolonging of remission in late-life depression.
Keywords: Electroconvulsive Therapy, Major Depression, Neurocognitive adverse effects
BRIEF SUMMARY
There is limited longitudinal information regarding the neurocognitive outcomes of right unilateral ultrabrief pulse width electroconvulsive therapy (RUL-UB ECT) in combination with pharmacotherapy in older adults with major depressive disorder. Addressing this information gap, we report neurocognitive outcomes from Phase 2 of the Prolonging Remission in Depressed Elderly (PRIDE) study. Following remission from an acute course of ECT plus venlafaxine, older adults were randomized to receive one of two prolonging remission strategies: symptom-titrated, algorithm-based longitudinal ECT (STABLE) in combination with pharmacotherapy (venlafaxine and lithium) or only pharmacotherapy. Study participants completed neuropsychological assessments at baseline and throughout the 6-month continuation treatment period. There were no differences in neurocognitive outcome between STABLE plus pharmacotherapy versus pharmacotherapy alone over the 6-month continuation treatment phase.
INTRODUCTION
Electroconvulsive therapy (ECT) is a treatment of choice for older adults with major depressive disorder (MDD) that is chronic, treatment-resistant, and associated with elevated suicide risk (1–3). Consistent evidence supports the use of ECT in both the acute and continuation treatment phases based on its robust and rapid antidepressant effects (3). However, ECT can produce cognitive adverse effects that may complicate its use, particularly in older adults who are at increased risk for cognitive decline(4).
Adverse cognitive effects of ECT may be moderated by select ECT parameters including pulse-width and electrode configuration (5). Prior research found that cognitive adverse effects, particularly anterograde amnesia and inconsistent autobiographical recall, can persist for up to 6 months (particularly with sine wave ECT), but were of lesser magnitude with right unilateral (RUL) than bitemporal (BT) electrode placement and of lesser magnitude with ultrabrief (0.25-0.3 ms) pulse width than with brief-pulse width (>0.5 ms) (6). We previously reported that patients across the adult lifespan with MDD randomized to either continuation ECT (bitemporal, brief-pulse width) or pharmacotherapy (nortriptyline and lithium) had similar cognitive outcomes after 6-months of treatment (7). Newer ECT paradigms, including the use of RUL and ultrabrief pulse width (RUL-UB) may confer high efficacy while resulting in relatively benign cognitive adverse effects (8).
In Phase 1 of the Prolonging Remission in Depressed Elderly (PRIDE) study, we found that an acute course with RUL-UB ECT combined with venlafaxine was highly effective in treating depression and resulted in modest declines in performance across most neurocognitive measures(9). Specifically, patients showed acute decline in cognitive domains of processing speed, verbal learning and memory, verbal fluency, complex visual scanning/cognitive flexibility, and autobiographical memory consistency. This suggested that RUL-UB ECT combined with venlafaxine in the acute treatment phase may have better neurocognitive outcomes relative to other ECT modalities (e.g., bitemporal electrode placement) that can induce moderate to severe cognitive adverse effects(10, 11). While our and other studies had different designs that may limit direct comparisons, prior randomized controlled studies (12–14) and systematic reviews and meta-analytic studies (15–17) support the differential neurocognitive effects of ECT parameters.
To date, there is limited information regarding the long-term neurocognitive effects of an acute course of RUL-UB ECT combined with venlafaxine specifically in older adults. For instance, prior research in an adult cohort found that the addition of venlafaxine to RUL brief pulse ECT could have worsened the neurocognitive adverse effects (18). There is also limited information regarding whether continuing RUL-UB ECT on an as-needed basis (according to symptoms) compared with pharmacotherapy alone in the early phase of prolonging remission would confer any additional risks of cognitive side effects.
In Phase 2 of the PRIDE study, we found that remitted older patients randomized to receive symptom-titrated, algorithm-based longitudinal ECT (STABLE) plus pharmacotherapy (venlafaxine and lithium) as a prolonging remission strategy showed significantly lower depression symptom severity during a 6 month period relative to patients treated only with pharmacotherapy. Specifically, additional ECT was associated with continued sustained mood improvement and antidepressant benefit above and beyond medication alone. Moreover, there was no significant difference between groups with regard to changes in global cognitive function (19). Although the study used alternate forms of the Mini Mental State Examination (MMSE) (20) to measure global cognitive function, research has found that the MMSE is insensitive to the neurocognitive effects of ECT(10, 21, 22).
Here, we present the comprehensive neurocognitive outcomes of older adults with MDD who remitted with an acute course of RUL-UB ECT plus venlafaxine (VLF) and were then treated with STABLE plus pharmacotherapy or pharmacotherapy (VLF and Lithium (Li) alone in Phase 2 of the PRIDE study(19, 23).
METHODS
Study Design Overview
The PRIDE study methods have been described in detail (19, 23). In brief, this was a National Institute of Mental Health (NIMH) funded, multicenter, randomized trial of the individualized STABLE (24) paradigm combined with venlafaxine and lithium to improve overall maintenance phase outcomes of older adults with MDD. In Phase 1, patients received an acute course of RUL-UB ECT combined with venlafaxine. Those patients who remitted during Phase 1, entered into Phase 2 and were randomly assigned to receive pharmacotherapy (VLF and Li) alone or the combined modalities (STABLE plus pharmacotherapy) for six months.
The study sites included: Columbia University/New York State Psychiatric Institute, Duke University School of Medicine, Medical College of Georgia/Augusta University, Icahn School of Medicine at Mount Sinai (MSSM), Mayo Clinic, New York Presbyterian/Weill Cornell Medical Center, University of Texas Southwestern Medical Center, Wake Forest University Medical Center, Zucker Hillside Hospital/Northwell Health System. The Medical University of South Carolina served as the data management and statical coordinating center. The institutional review board at each study site approved the study protocol.
Study Sample
In Phase 1, inclusion criteria included in- or outpatients, age ≥ 60, DSM-IV-TR diagnosis of unipolar major depressive episode, and 24-item Hamilton Rating Scale for Depression (HRSD24)(25) total score ≥ 21. Exclusion criteria included bipolar disorder, schizoaffective disorder, dementia, substance abuse/dependence in last 6 months, active general medical or neurological conditions, contraindications to Li or VLF, or failure to respond to an adequate trial of lithium + venlafaxine, or ECT in the current depressed episode. For Phase 2, inclusion criteria included attainment of remission in Phase 1(19). All patients provided written informed consent before they entered each study Phase.
Electroconvulsive Therapy and Pharmacotherapy Treatment Procedures
STABLE plus medication procedure.
In the STABLE plus pharmacotherapy procedure condition, ECT was administered on a fixed, tapered schedule (four ECT sessions administered weekly over 1 month) followed by ECT administered via the STABLE algorithm(24), in combination with the same medication regimen (venlafaxine and lithium) as the pharmacotherapy only condition. For the STABLE algorithm, between 0 and 2 ECT sessions were prescribed based on the patient’s HRSD24 total score (see Kellner et al. for comprehensive information on the STABLE algorithm(19)).
In Phase 2, ECT was provided with the same parameters (e.g., right unilateral, ultrabrief pulse width, stimulus dose) as the last ECT session in Phase 1 with a Thymatron System IV (Somatics, LLC, Lake Bluff, IL) device with an ultrabrief pulse width of 0.25ms and current of 900 mA or a spECTrum (MECTA Corporation, Portland, OR) device with an ultrabrief pulse width of 0.3ms and current of 800 mA. Following the STABLE algorithm, an ECT session was postponed for 2 days if the patient had a MMSE(20) total raw score ≤ 21. Anesthesia included sedation with methohexital (~1 mg/kg), muscle relaxation with succinylcholine (~0.75 mg/kg), and ventilation with 100% oxygen. Both the ECT and anesthesia procedures complied with the American Psychiatric Association ECT recommendations(26).
Lithium was used in moderate doses (target blood level range: 0.4 – 0.6 mEq/L) as an adjunct to venlafaxine, and blood levels were obtained at weeks 2 – 6, 8, 12, 16, 20, and 24. Any changes to medications were made based on blood levels and side effects. Lithium was held a minimum of 24 hours before each ECT session, and additional time for lithium clearance was allotted for patients whose blood levels were above 0.8 mEq/L.
Pharmacotherapy-only procedure.
In the pharmacotherapy-only condition, venlafaxine and lithium procedures were identical to the STABLE plus pharmacotherapy condition. However, as there was no ECT, there was no withholding of lithium.
Clinical Assessment Procedures
Psychiatric diagnosis was established with the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I)(27) (study years 1 and 2) or the Mini-International Neuropsychiatric Interview (MINI)(28) (years 3 – 6). We assessed depressive symptom severity with the HRSD24 and suicidal ideation with the Beck Scale for Suicide Ideation (BSS)(29). Raters, masked to the randomized treatment condition, were trained to criteria via in-person and video interactive sessions. Ongoing rater consistency across sites was insured by having each rater rate a new set of videotapes annually for comparison with ratings of the “gold standard” rater at the Clinical Coordinating Center (MSSM).
Neurocognitive Assessment Procedures
Multiple standard instruments were included in the neurocognitive battery to assess several cognitive domains including attention and processing speed, verbal fluency, verbal learning and memory, autobiographical memory consistency, and executive functions. Specific instruments included: Autobiographical Memory Interview-Short Form (AMI-SF)(30), California Verbal Learning Test-II (CVLT-II)(31), Delis-Kaplan Executive Function System (DKEFS) Verbal Fluency (Condition 1: Letter Fluency) Test(32), Dementia Rating Scale-2nd Edition Initiation Perseveration Index (DRS-2 IP)(33), Stroop Color and Word Test(34), and Trail Making Test Parts A and B (TMT A and B).
Each neurocognitive instrument, with the exception of TMT A and AMI-SF, had at least one alternate form version in order to minimize possible practice effects. With the exception of the AMI-SF, all neurocognitive variable raw scores were converted into demographic- adjusted scores. We assessed global cognitive function with the MMSE (results were previously reported)(19) and premorbid intellectual ability was estimated with the Wechsler Test of Adult Reading (WTAR)(35). Patients completed a subset of neurocognitive instruments (AMI-SF, CVLT-II) each month, and all instruments at the mid- (12-weeks) and end- (24-weeks) points (see supplemental information for timing of the neurocognitive assessments).
Testers, masked to the randomized treatment condition, at all study sites were trained to criteria at all study sites via in-person and video interactive training sessions following the neurocognitive procedure manual. For longitudinal quality control, the electronic database was range validated to automatically detect errors and alert the study site to correct errors. Every four months, a random sample of data was examined for scoring accuracy.
Statistical Analysis
Descriptive statistics were used to characterize the demographic and clinical features of the study sample who began Phase 2. Means and standard deviations are presented for continuous variables, and frequency distributions are presented for discrete variables.
The intention-to-treat (ITT) sample was used for the neuropsychological (NP) outcome primary analyses. Patients were classified as premature exits (dropouts) if they withdrew consent or if they were discontinued by the study psychiatrist for safety reasons prior to the 24-week end-of-study time point. Protocol-defined safety reasons requiring patient discontinuation were two consecutive HRSD24 total scores ≥ 21, or psychiatric hospitalization, or if the patient became suicidal.
A mixed effects model (MEM) approach was used to compare the longitudinal profile of NP scores over the 6-month treatment period. MEM analyses allow for measurement of subjects at irregular time points, missing data, and time varying or invariant covariates, and can also account for the effect of clustering (e.g. within subjects and clinical sites). The NP variables were used separately as the dependent variable with treatment status (pharmacotherapy, STABLE plus pharmacotherapy), time, and time x treatment interaction as primary fixed independent variables. Additional covariates were added to the model to adjust for age, clinical center (site), psychosis, pre-morbid intellectual functioning (measured by the Wechsler Test of Adult Reading (WTAR)), and time-varying changes (over the 6-month period) in depression severity (HAM-D24 total score). Random subject effects were incorporated using random intercepts and slopes. A difference in neurocognitive variable trajectories (rate of change) over the full time period for STABLE plus pharmacotherapy vs pharmacotherapy was indicated by a significant time x treatment interaction term in the MEM. The presence of a curvilinear trend (rate of change in mean response depends on time) was evaluated by inclusion of a quadratic term (time centered) and interaction in the MEM with the significance of the p-values and the likelihood ratio test used to determine retention of the higher order terms in the model.
Because the STABLE algorithm directed rescue ECT at any time point in the flexible phase as indicated by increased depression symptom severity prior to that point, the final time point (6-months) represented the cumulative effect of treatment on cognitive function across all neurocognitive measures and was considered the primary analysis time point. Effect sizes for neurocognitive scores for STABLE plus pharmacotherapy vs pharmacotherapy, therefore, were determined from the MEM as differences in least squares means, with corresponding 95% confidence intervals, at study end (6-months) using either the linear or quadratic MEM model depending on optimal model fit. If significant differences were detected for a given neurocognitive outcome, both the Bonferroni-adjusted and unadjusted p-values were reported. If no significant differences were observed for a neurocognitive outcome, then there was no adjustment for multiple outcomes and the unadjusted p-values were reported (further adjustment does not modify non-significance).
The PRIDE Statistical and Data Management Center (Data Center) was responsible for data management and data analysis activities. Data were managed using a web-based clinical trials management system (WebDCU) tailored for the PRIDE study that incorporated secure direct data entry at the clinical site level, central randomization, extensive electronic range validation checks with immediate feedback to Study Coordinators, and real-time reporting capabilities. Statistical analyses were carried out using SAS Statistical Software Version 9.4 (Copyright © 2016 by SAS Institute Inc.,Cary NC, USA). All statistical tests were two-tailed using level of significance, alpha=0.05.
RESULTS
Sample Demographic and Clinical Characteristics
Of the 148 patients who remitted in Phase 1 and were eligible to be randomized for Phase 2, 120 patients consented to enter Phase 2 (see supplemental information for Consort Diagram). For the total sample, 62% of the participants were female, 95% were White, the mean age was 70.5 (SD=7.2), and the mean years of education was 14.5 (SD=3.3). With the exception of a not statistically significant trend for a higher percentage of patients in the pharmacotherapy-only condition to have psychotic features relative to those in the STABLE combined with pharmacotherapy condition, there were no statistically significant differences in demographic and clinical characteristics at Phase 2 baseline (Table 1). Only 34% of patients in the STABLE plus pharmacotherapy condition (21/61) received any additional ECT beyond the four fixed sessions in the first month. Of these, seven received only one additional ECT treatment.
Table 1.
Demographic and baseline patient characteristics for the intent-to-treat sample in a study of Symptom-Titrated Algorithm-Based Longitudinal ECT (STABLE) plus Medication versus Medication alone in geriatric depression
| Characteristic | Total Sample (n=120) | STABLE+PHARM (n=61) | PHARM (n=59) | test statistics | df | p-valuea | |||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| Mean | SD | Mean | SD | Mean | SD | ||||
|
| |||||||||
| Age (y) | 70.5 | 7.2 | 70.8 | 7.2 | 70.3 | 7.3 | −0.35 | 118 | 0.73 |
| Education (y) | 14.5 | 3.3 | 14.4 | 3.3 | 14.5 | 3.4 | 0.09 | 118 | 0.93 |
| HRSD24 baseline Phase 1 | 30.3 | 7.4 | 29.6 | 6.8 | 31.1 | 7.9 | 1.13 | 118 | 0.26 |
| HRSD24 baseline Phase 2 | 6.1 | 2.5 | 6.0 | 2.5 | 6.1 | 2.5 | 0.04 | 118 | 0.97 |
| MMSE baseline Phase 1 | 27.5 | 2.2 | 27.6 | 2.2 | 27.4 | 2.3 | −0.28 | 118 | 0.78 |
| MMSE baseline Phase 2 | 27.9 | 2.4 | 27.9 | 2.5 | 27.8 | 2.4 | −0.27 | 118 | 0.79 |
| CGI-S baseline Phase 1 | 5.2b | 0.9 | 5.1b | 0.8 | 5.3 | 0.9 | 1.1 | 117 | 0.28 |
| CGI-S baseline Phase 2 | 1.9 | 0.9 | 1.9 | 0.9 | 1.8 | 0.8 | −0.98 | 118 | 0.33 |
| Seizure threshold (mC) (baseline Phase1) | 29.8b | 12.8 | 29.4b | 12.7 | 30.1 | 13.0 | 0.28 | 117 | 0.78 |
| Prior antidepressants (baseline Phase1) | 2.3c | 1.5 | 2.3d | 1.6 | 2.4e | 1.5 | 0.13 | 1 | 0.72 |
| Wechsler Test of Adult Reading | 106.2f | 10.2 | 106.3e | 9.8 | 106.0g | 10.8 | −0.17 | 107 | 0.86 |
|
| |||||||||
| N | % | N | % | N | % | ||||
|
| |||||||||
| Age group (%) | |||||||||
| 60-69 | 57 | 47.5 | 29 | 47.5 | 28 | 47.5 | |||
| 70-79 | 49 | 40.8 | 24 | 39.3 | 25 | 42.4 | |||
| 80-89 | 14 | 11.7 | 8 | 13.1 | 6 | 10.2 | |||
| Female | 74 | 61.7 | 37 | 60.7 | 37 | 62.7 | 0.05 | 1 | 0.82 |
| White | 114 | 95 | 58 | 95.1 | 56 | 94.9 | 3 | 1 | 1.0 |
| Patients with psychosis (baseline) | 17 | 14.2 | 5 | 8.2 | 12 | 20.3 | 3.64 | 1 | 0.06 |
p-values for comparing STABLE+medication vs Medication are from pooled t-test for continuous variables and chi-square (or Fisher’s exact test or Kruskal-Wallis) for categorical variables.
missing data for 1 subject
missing data for 15 subjects
missing data for 10 subjects
missing data for 5 subjects
missing data for 11 subjects
missing data for 6 subjects
Phase 2 Baseline Neurocognitive Performance
For both groups at Phase 2 baseline, following an acute course of ECT and venlafaxine, the mean demographic adjusted scores for the neurocognitive variables (Table 2) ranged from low average to mildly and moderately impaired (impairment was defined based on the recommendations of Brooks and Iverson with 1.5 standard deviations representing mild to moderate impairment(36)).
Table 2. Model adjusted* difference in post-treatment neuropsychological assessment scores between STABLE+medication and Medication (ΔTx) with 95% confidence interval (CI) and p-values.
Table notation: Wk24= 24 weeks; SM= STABLE plus Medication; M= Medication only; ΔTx = difference in model adjusted post-treatment (Wk24) means for SM compared to M; p=p-value, df=degrees of freedom and t=test statistic from comparison of model adjusted (contrast) means
| Instrument | STABLE | PHARM | ΔTx Wk24 (P-S) | 95% CI ΔTx | PΔTx (DF, t-Statistic) | ||
|---|---|---|---|---|---|---|---|
| Baseline | End | Baseline | End | ||||
| Memory | |||||||
| AMI-SF - assesses retrograde amnesia for autobiographical information | |||||||
| AMI Total Score | 37.2 | 37.5 | 37.0 | 37.1 | −0.4 | (−4.0, 3.2) | 0.82 (140, −0.22) |
| CVLT-II - assesses anterograde verbal learning and memory | |||||||
| Trial 1-5 Free Recall Total Correct t-score | 42.2 | 57.1I | 44.6 | 54.4I | −2.7 | (−7.4, 2.0) | 0.25 (207, −1.14) |
| Short delay free recall correct standard score | −1.2 | 0.1I | −0.9 | 0.0I | −0.1 | (−0.5, 0.4) | 0.78 (198, −0.28) |
| Long delay free recall correct standard score | −1.3 | 0.1I | −1.1 | −0.1I | −0.2 | (−0.7, 0.3) | 0.37 (205, −0.90) |
| Delayed recognition: Total recognition discriminability (d’) standard score | −1.0 | 0.1I | −0.9 | 0.1I | 0.0 | (−0.5, 0.4) | 0.92 (211, −0.10) |
| Executive Function | |||||||
| D-KEFS –tests frontal lobe dysfunction | |||||||
| Letter fluency total correct scaled score | 8.3 | 10.8I | 8.3 | 10.3I | −0.6 | (−2.4, 1.2) | 0.54 (196, −0.61) |
| DRS-IP - tests verbal initiation & verbal, motor & graphomotor perseveration | |||||||
| Initiation/Perseveration AMSS score | 7.4 | 9.2I | 8.0 | 9.6I | 0.4 | (−0.9, 1.7) | 0.53 (231, 0.63) |
| Initiation/Perseveration Raw score | 32.2 | 34.8I | 32.7 | 35.4I | 0.6 | (−1.3, 2.6) | 0.52 (230, 0.65) |
| Item E-Complex Verbal Initiation/Perseveration | 15.9 | 18.3I | 16.5 | 18.8I | 0.5 | (−1.2, 2.2) | 0.57 (217, 0.56) |
| STROOP - is a measure of selective and divided attention and cognitive flexibility | |||||||
| Word T-Score | 31.8 | 35.3I | 32.3 | 38.3I | 2.9 | (−2.2, 8.1) | 0.26 (185, 1.13) |
| Color T-Score | 32.9 | 37.2I | 34.3 | 38.5I | 1.3 | (−3.4, 6.1) | 0.58 (191, 0.55) |
| Color-Word T-Score | 38.2 | 43.1I | 40.5 | 42.5 | −0.6 | (−5.2, 4.0) | 0.80 (163, −0.26) |
| Trail Making Test Part A - measures visual scanning/motor speed | |||||||
| Score | 7.2 | 8.1I | 7.6 | 8.2 | 0.1 | (−1.0, 1.2) | 0.87 (163, 0.17) |
| Trail Making Test Part B - measures cognitive flexibility | |||||||
| Score | 7.0 | 8.2I | 6.9 | 9.2I | 0.9 | (−0.5, 2.3) | 0.19 (184, 1.31) |
from mixed effects models with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading, and Ham-D (time varying). Adjusted (least squares) means corresponding to relevant model derived contrasts for ΔTx were compared and corresponding 95% confidence intervals were obtained (columns 7,8).
I=Significance of Change from baseline within each treatment group: pSM=p-value for significance of change within STABLE plus Medication group (df, t); pM =p-value for significance of change within Medication only group; pSMadj/pMadj=Bonferroni-adjusted p-value provided if significance changes; (df, t); df=degrees of freedom, t=t statistic from test of significance of model adjusted change from baseline within each group
AMI Total Score: pSM=0.7088 (447, 0.37), pM=0.9027 (448, 0.12)
CVLT: Item 12: pSM=<0.0001 (474, 9.67), pM=<0.0001 (479, 6.10)
Item16: pSM=<0.0001 (469, 8.55), pM=<0.0001 (475, 5.93)
Item20: pSM =<0.0001 (472, 9.31), pM=<0.0001 (’478, 5.97)
Item44: pSM=<0.0001 (473, 7.01), pM=<0.0001 (480, 6.00)
DKEFS_Tscaled: pSM=<0.0001 (169, 4.11), pM=0.0026 (174, 3.05)
DRS_IniPAMSS: pSM=0.0023 (182, 3.09), pM=0.0082 pMadj=0.1148 (194, 2.67)
DRS_IniPR: pSM=0.0042 pSMadj=0.0588 (181, 2.90), pM=0.0036 pMadj=0.0504 (193, 2.94)
DRS_ItemE: pSM=0.0031 (178, 3.00), pM=0.0055 pMadj=0.0770 (185, 2.81)
STROOP: WTScore: pSM=0.0361 pSMadj=0.5054 (162, 2.11), pM=0.0010 (165, 3.36)
CTScore: pSM=0.0076 pSMadj=0.1064 (164, 2.70), pM=0.0142 pMadj=0.1988 (167, 2.48)
CWTScore: pSM=0.0004 (151, 3.60), pM=0.1697 (153, 1.38)
TMTaS: pSM=0.0209 pSMadj=0.2926 (142, 2.34), pM=0.1283 (140, 1.53)
TMTbS: pSM=0.0242 pSMadj=0.3388 (142, 2.28), pM=0.0003 (150, 3.72)
Simple visual scanning/psychomotor processing speed (TMT-A) and cognitive processing speed (Stroop Word Reading) were low average and mildly to moderately impaired, respectively. Complex visual scanning/psychomotor processing speed and cognitive flexibility (TMT-B) and initiation/perseveration (DRS-2 Initiation/Perseveration) were low average, and inhibition (Stroop Color-Word) was mildly impaired. Phonemic fluency was average. On the CVLT-II, verbal learning was low average, and immediate and delayed free recall, and recognition of learned words were mildly impaired.
Change in Neurocognitive Performance Within Treatment Condition
Within each treatment condition, there was statistically significant improvement across most neurocognitive scores from Phase 2 baseline to the 24-week end time point (Table 2, Figures 1 and 2). Specifically, patients in both conditions showed statistically significant improved performance across time on measures of complex visual scanning, psychomotor processing speed, and cognitive flexibility, verbal learning, short-term and long-term free recall, and recognition of learned words, initiation and perseveration, and phonemic fluency (Table 2). After Bonferroni adjustment for multiple comparison, change in performance was no longer statistically significant for measures of complex visual scanning, psychomotor processing speed, and cognitive flexibility and initiation and perseveration.
Figure 1.
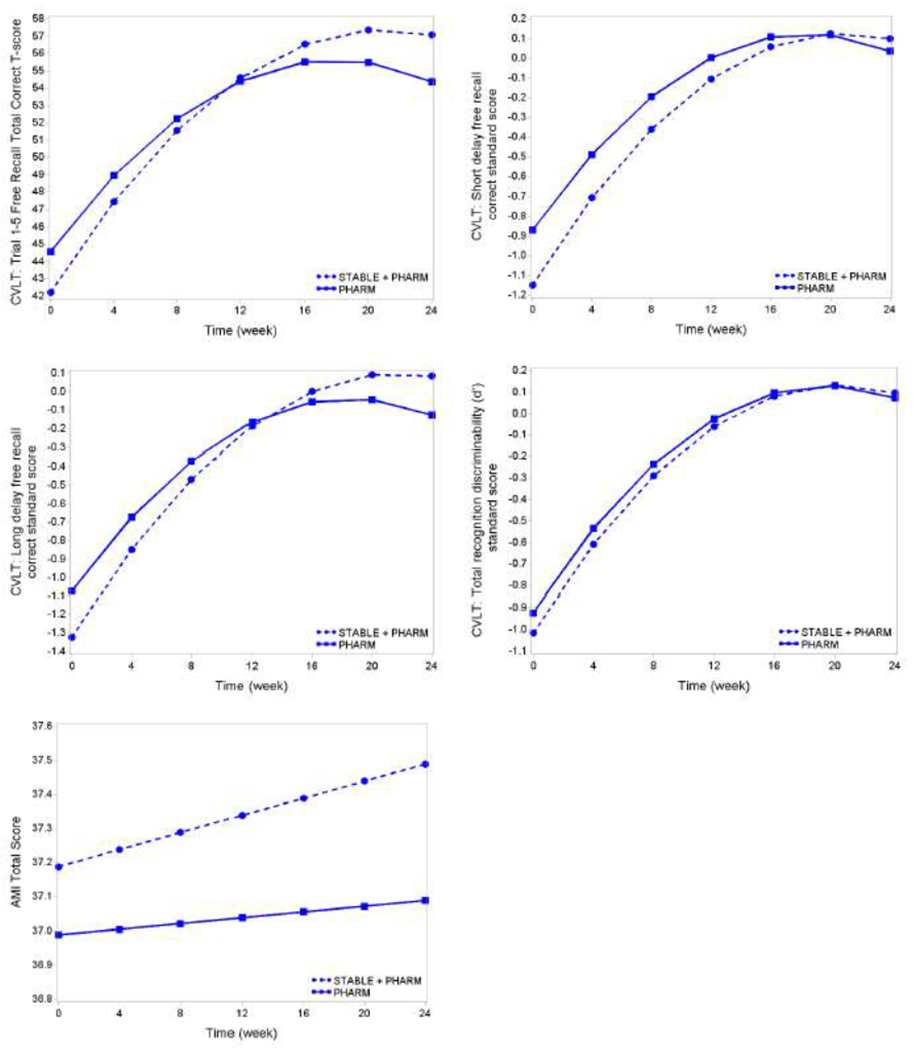
Trajectories of Memory Domain Neurocognitive Outcomes over the 6-month Study Period By Treatment Arm Using Model-Derived Adjusted Treatment Means
California Verbal Learning Test (CVLT) - anterograde verbal learning and memory:
These graphs show adjusted least squares means from quadratic mixed effects models with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading and Ham-D (time varying).The within group improvement from baseline was statistically significant at p≤0.05 for all CVLT items in both treatment groups (Item, p-value [DF, t-statistic]: Item12 Stable: <0.0001 [474, 9.67], Pharm: <0.0001 [479, 6.10]; Item16 Stable: <0.0001 [469, 8.55], Pharm: <0.0001 [475, 5.93]; Item20 Stable: <0.0001 [472, 9.31], Pharm: <0.0001 [478, 5.97]; Item44 Stable: <0.0001 [473, 7.01], Pharm: <0.0001 [480, 6.00]). There were no significant differences between the ECT plus Medication and Medication only treatment arms at the post-treatment (24 weeks) time point. For the comparison of trajectories of CVLT mean scores over time (time as continuous), there was a significant interaction for CVLT Trial 1–5 Free Recall Total Correct t-score (p [DF, t-statistic]: 0.02 [480, −2.27]) and CVLT Long delay free recall correct standard score (p [DF, t-statistic]: 0.04 [479, −2.11])
AMI-SF - retrograde amnesia for autobiographical information:
This graph shows adjusted least squares means from linear mixed effects model with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading and Ham-D (time varying). There was no significant differences between the ECT plus Medication and Medication only treatment arms at the post-treatment (24 weeks) time point. The within group improvement from baseline was not statistically significant in both treatment groups.
Figure 2.
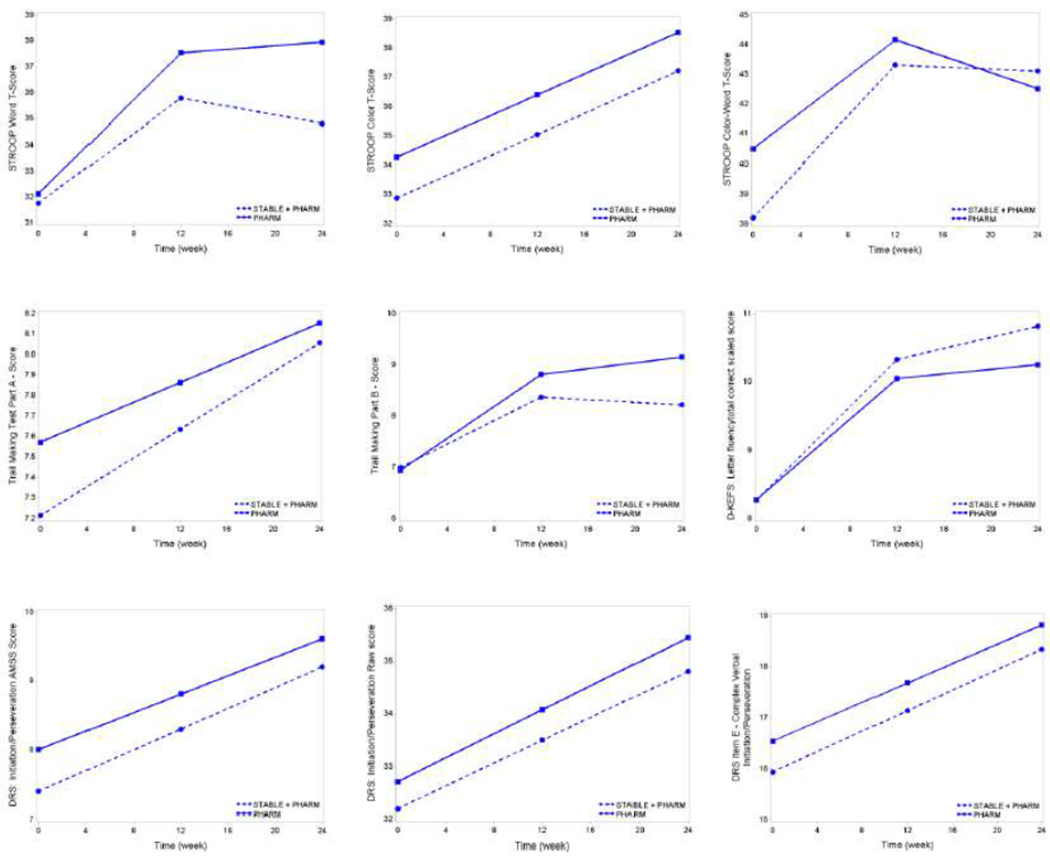
Trajectories of Executive Function Neurocognitive Outcomes over the 6- month Study Period By Treatment Arm Using Model-Derived Adjusted Treatment Means
Stroop - selective and divided attention and cognitive flexibility:
These graphs show adjusted least squares means from quadratic (STROOP Word T-score & STROOP Color-Word T-score) and linear (STROOP Color T-score) mixed effects models with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading and Ham-D (time varying). Except for Color-Word T-Score Medication only treatment group, the within group improvement from baseline was statistically significant at p≤0.05 (Measure, p-value [DF, t-statistic]: Word T-Score Stable: 0.0361 [162, 2.11], Pharm: 0.0010 [165, 3.36]; Color T-Score Stable: 0.0076 [164, 2.70], Pharm: 0.0142 [167, 2.48]; Color-Word T-Score Stable: 0.0004 [151, 3.60]).
Trail Making Test Parts A and B:
The graph of Trail Making Test Part A score shows adjusted least squares means from linear mixed effects model with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading and Ham-D (time varying). The within group improvement from baseline was not statistically significant in the Medication only treatment group.
The graph of Trail Making Test Part B score shows adjusted least squares means from quadratic mixed effects model with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading and Ham-D (time varying). The within group improvement from baseline was statistically significant at p≤0.05 in both treatment arms (Measure, p-value [DF, t-statisticj: TMT Score A Stable: 0.0209 [142, 2.34]; TMT Score B Stable: 0.0242 (142, 2.28), Pharm: 0.0003 [150, 3.72]).
Delis Kaplan Executive Function System (D-KEFS): Letter fluency total correct scaled score:
The graph shows adjusted least squares means from quadratic mixed effects model with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading and Ham-D (time varying). The within group improvement from baseline was statistically significant at p≤0.05 in both treatment arms (p [DF, t-statistic] Stable: <0.0001 [169, 4.11], Pharm: 0.0026 [174, 3.05]).
Dementia Rating Scale - IP (DRS-IP):
These graphs show adjusted least squares means from linear mixed effects model with random intercept using unstructured covariance adjusted for site, psychosis, age, Wechsler Test of Adult Reading and Ham-D (time varying). The within group improvement from baseline was statistically significant at p≤0.05 for all DRS items in both treatment groups.
There were no significant differences between the ECT plus Medication and Medication only treatment arms at the post-treatment (24 weeks) time point for all instrument items.
Only patients in the STABLE condition showed significantly improved performance on measures of simple visual scanning and psychomotor processing speed and inhibition. Patients in the pharmacotherapy-only condition showed significantly improved performance on a neurocognitive measure of cognitive processing speed. After Bonferroni adjustment only inhibition remained statistically significantly different. There was no significant change in autobiographical memory consistency. In terms of qualitative changes from baseline to end within each treatment condition, performance across most neurocognitive variables improved from low average and mildly/moderately impaired to average.
CONCLUSIONS
This is the first report of the long-term outcomes in older adults with depression of an acute course of RUL-UB ECT + VLF, followed by one of two prolonging remission strategies (STABLE+VLF+Li versus VLF+Li). Our key finding is that neurocognitive function improved over the 6-month follow up period. Regardless of which prolonging remission strategy was used, patients demonstrated recovery of the mild-to-moderate neurocognitive impairments they experienced after the acute course of RUL-UB ECT + VLF. For the group as a whole, performance on most neurocognitive measures returned to the average range. While processing speed remained mildly impaired, this could be related to either the ECT or pharmacotherapy treatment, or depression itself, but this did not differ between the prolonging remission strategies. This result supports the long-term safety of RUL-UB ECT + VLF in the acute treatment of depression in the older adult population, followed by VLF+Li, with or without STABLE in the prolonging of remission.
Importantly, the two prolonging remission strategies were relatively similar and showed no divergence at the 6-month time point in their neurocognitive outcomes. This is despite the fact that the STABLE+VLF+Li arm, relative to the VLF+Li arm, involved the continued provision of additional ECT sessions. Moreover, in combination with our previously reported data that the additional ECT sessions (STABLE) were associated with significant sustained mood improvement, these current data suggest that the STABLE remission strategy conferred antidepressant benefit without added cognitive adverse effects.
In contrast to prior studies on continuation ECT that used a fixed schedule for providing continued ECT treatments, we employed the STABLE algorithm which individualized the timing of additional ECT treatments based upon clinical need. The goals of the STABLE approach were to adequately treat patients who showed early signs of depression symptom re-emergence, without over-treating patients who were in a stable remission. This result is of high clinical importance because STABLE+VLF+Li was found to be more effective in prolonging remission following an acute course of ECT than VLF+Li alone (19). This means that patients can take advantage of the higher efficacy of STABLE+VLF+Li compared to pharmacotherapy alone, without appreciable additional adverse cognitive adverse effects. The fact that the two prolonging remission strategies were similar in safety suggested that the additional ECT treatments provided in the STABLE algorithm did not interfere with the expected recovery of neurocognitive function following an acute course of RUL-UB ECT. This finding is consistent with prior research that compared a fixed maintenance ECT schedule with pharmacotherapy (nortriptyline plus lithium) in an adult cohort and found that both prolonging remission strategies at the 6-month time point demonstrated similar neurocognitive outcomes (7).
Although the study used alternate forms of the neurocognitive measures, it remains possible that there were practice effects due to repeated testing (37). Also, as the group was highly educated, an indicator of cognitive reserve, that could have moderated the neurocognitive outcomes as prior research suggested that cognitive reserve (e.g., years of education, premorbid intellectual ability) could serve as a protective factor for ECT-induced cognitive effects(38, 39). Based on the neurocognitive trajectory, it appeared that stabilization of cognitive function after the Phase 1 acute RUL-UB ECT plus venlafaxine treatment course took longer than one-month, which is in contrast to prior research (10). Thus, this study provides new evidence that is consistent with recent findings(40) in older adults with depression that neurocognitive stabilization for some cognitive functions after an acute ECT course may require more than one-month. Additional research is warranted to track the long-term trajectory of neurocognitive stabilization and recovery after the acute ECT course for a period greater than six-months.
Older adult patients are in the demographic with the highest overall rates of completed suicide(41). ECT is highly effective in the acute and continuation treatment phases of depression, rapidly relieves suicidal ideation(19, 42), and improves quality-of-life(43). However, its use is often complicated by concerns over its cognitive side effects, especially in older adults. Without additional treatment, relapse after ECT can be high, highlighting the importance of identifying effective and safe prolonging remission strategies(44). Our results support both the long-term safety of an acute course of RUL-UB ECT plus venlafaxine as well as the safety of two specific prolonging remission strategies in the treatment of this clinically significant at risk demographic. Although some research has found differential neurocognitive trajectories at an individual level following ECT treatment(40), our findings are consistent with prior ECT research in older adults(21, 45–47). Indeed, following the end of the acute RUL-UB ECT plus venlafaxine treatment course, the group as a whole showed an improvement from mildly impaired to average performance at the 6-month follow up time point across most cognitive functions.
Limitations of this study include that the study cohort was primarily Caucasian, highly educated, had no current substance abuse or comorbid neurological illnesses, few had psychotic features, and few were age 80 or older. Also, patients knew whether they were in the STABLE+VLF+Li group or the VLF+Li group. This was the case because it was impossible to blind the fact that the patients in STABLE received additional ECT. Mitigating this limitation is the fact that the neuropsychometricians and clinical raters were blinded to group assignment. Another limitation is that the study had no third prolonging remission condition with a fixed scheduled maintenance ECT schedule that would have allowed us to determine whether STABLE+VLF+Li is better tolerated than fixed schedule continuation/maintenance ECT. On the other hand, the STABLE+VLF+Li did not significantly differ from the VLF+Li group, suggesting that the STABLE algorithm would be expected to be better tolerated than fixed schedule continuation/maintenance ECT. Another limitation is that we only examined long-term follow up for 6-months in patients who achieved remission in Phase 1, so our results cannot speak to long-term outcomes in patients who did not achieve remission with an acute course of RUL-UB ECT and venlafaxine. Counterbalancing this is the recent report that remission status did not affect most measures of cognitive function at four months post ECT(48), though that finding was in a small sample. Also, another recent report suggested in a naturalistic four-year longitudinal study that older adults with MDD treated with ECT showed a relatively stable cognitive trajectory from baseline to follow-up, though there was individual variability as some older adults showed decline and others showed improvement in cognitive functions (49). Thus, it is possible that some of the patients in the study could have cognitive difficulties following the 6-month time point. Future research is warranted to examine the longer term cognitive, and antidepressant, trajectory. Finally, we note that little additional ECT was needed to sustain remission in the STABLE arm, which may have reduced the chances of seeing cognitive differences between the groups. Nevertheless, demonstrating cognitive safety of even small amounts of additional ECT in combination with lithium+VLF in remitted geriatric patients is of clinical relevance when considering this group is vulnerable to cognitive side effects of pharmacotherapy and ECT.
Our results support the safety of both an acute course of RUL-UB ECT plus venlafaxine as well as two prolonging remission strategies in older patients with major depression. Given that STABLE+VLF+Li was more effective in sustaining antidepressant remission than VLF+Li alone without increasing the risk of neurocognitive side effects, these results support the use of STABLE+VLF+Li to prolong remission from depression after acute ECT. Future work will be needed to evaluate the translation and implementation of STABLE+VLF+Li into clinical practice as an optimized prolonging remission strategy for geriatric depression in a clinical setting so that this approach can be adopted into routine clinical care for older adult patients.
Supplementary Material
HIGHLIGHTS.
What is the primary question addressed by this study? What are the long-term neurocognitive effects of continuation treatment with ultra-brief pulse, six-times seizure threshold, right unilateral ECT in combination with venlafaxine and lithium relative to only venlafaxine and lithium in older adults with major depressive disorder?
What is the main finding of the study? At the 6-month final time point, there were no statistically significant differences across all neurocognitive outcomes between the two treatment groups. Equally important, within each treatment group, there was statistically significant and qualitative improvement across most neuropsychological measures.
What is the meaning of the finding? The combination of RUL-UB ECT with venlafaxine and lithium is a relatively tolerable and cognitively safe continuation treatment in late-life depression.
Acknowledgements
CORE/PRIDE Work Group: Icahn School of Medicine at Mount Sinai: Gabriella Ahle, Amy S. Aloysi, M.D., Ethan Bryson, M.D., Kate Farber, Matthew Majeske, M.D., Elizabeth Muller, Roya Nazarian, Rosa Pasculli; New York Presbyterian/Weill Cornell Medical Center: Ashly Cochran, M.S., Laura D. Evans, M.S., David Friedman, Nabil Kotbi, M.D., Bryony Lucas, Arielle Rogers; Augusta University: Brittany Gubosh, Chelsea Hodges, M.S., Laryssa McCloud, Ph.D., Mary Anne Riley, M.S.; Zucker Hillside Hospital/ Northwell Health System: Raphael Braga, M.D., Ingrid Fuentes, Ketan Hiranpara, M.D., Muhammad Khan, M.D., Carmel Powers, Susan Ray, Gail Reiter, Sohag Sanghani, M.D., Elina Shrestha, M.D.; Duke University School of Medicine: Julie L. Adams, M.D., M.P.H, Grace Falcone, N.P., D.N.P., Mehul V. Mankad, M.D., Charles P. McCormick, M.D., M.P.H., Scott D. Moore, M.D., Ph.D., Kristen G. Shirey, M.D., Chris Sikes-Keilp, David C. Steffens, M.D., M.H.S., Nagy Youssef, M.D.; University of Texas Southwestern Medical Center: Enisa Arslanagic, M.D., Matthieu Chansard, Melita Gonzalez, Katalin Martits, Michelle Nichols, M.D., Najeeb Ranginwale, M.D.; Medical University of South Carolina: Hiya Banergee, Catherine Dillon, Mary Dooley, Andre Thornhill, Wenle Zhao; Mayo Clinic: Allison Hanson, Simon Kung, M.D., Maria Lapid, M.D Lisa Seymour, Chris Sola, D.O., Cynthia Stoppel; Wake Forest University Medical Center: Niki Boggs, James Kimball, M.D.; NIMH: Galia Siegel, Ph.D., Elizabeth Zachariah, M.S. Also, we thank Judy Shaw for her guidance and recommendations regarding the neurocognitive procedures manual and test administration with study participants.
Research Support
Supported by National Institute of Mental Health (NIMH) grants U01 MH055495, U01 MH081362, U01 MH086127, U01 MH086127, U01 MH086130, U01 MH08612005, U01 MH084241, and U01 MH086122. Drs. Deng and Lisanby are supported by the NIMH Intramural Research Program.
Footnotes
Disclosures/Conflicts of Interest (listed in alphabetical order)
George Alexopoulos. Dr. Alexopoulos reports having served in the speakers bureau of Otsuka, Lundbeck, Takeda, Allergan, Sunovion, and Astra Zeneca.
Samuel H. Bailine. Dr. Bailine reports no conflicts of interest.
Elisabeth Bernhardt. Ms. Bernhardt reports no conflicts of interest.
Mimi C. Briggs. Dr. Briggs reports no conflicts of interest.
C. Munro Cullum. Dr. Cullum reports no conflicts of interest.
Zhi-De Deng. Dr. Deng reports no conflicts of interest.
Emma T. Geduldig. Ms. Geduldig reports no conflicts of interest.
Robert M. Greenberg. Dr. Greenberg reports no conflicts of interest.
Mustafa M. Husain. Dr. Husain reports research support from the National Institute of Mental Health, National Institute of Neurological Disorders and Stroke, Stanley Medical Research Foundation, Neuronetics, Inc., MagStim (equipment only), Brainsway, Inc., NeoSync and consulting income from Cerebain Inc. Speaker bureau for Acadia Pharmaceutical. Consultant to the Neurological Devices Panel of the Medical Devices Advisory Committee, Center for Devices and Radiological Health, Food and Drug Administration (FDA). Editorial Board Member of the Journal of ECT.
Styliani Kaliora. Dr. Kaliora reports no conflicts of interest.
Charles H. Kellner. Dr. Kellner receives honoraria from UpToDate, Psychiatric Times, and Northwell Health and royalties from Cambridge University Press
Rebecca G. Knapp. Dr. Knapp reports no conflicts of interest.
Vassilios Latoussakis. Dr. Latoussakis reports no conflicts of interest.
Lauren S. Liebman. Ms. Liebman reports no conflicts of interest.
Sarah H. Lisanby. Dr. Lisanby has received grant support from the Brain and Behavior Research Foundation, the Stanley Medical Research Foundation, Neosync, Nexstim, NIH, and Brainsway. This manuscript was prepared while Dr. Sarah H. Lisanby was employed at Duke University. The opinions expressed in this article are the author's own and do not reflect the views of the National Institutes of Health, the Department of Health and Human Services, or the United States government.
William V. McCall. Dr. McCall has served as a scientific adviser for Jazz, Sage, and Janssen pharmaceuticals, and he has received research support from the American Foundation for Suicide Prevention, NIMH, PCORI, MECTA Corp, Merck, Vistagen, and Otsuka. He has received royalties from Wolters Kluwer, and honoraria from Anthem, Inc., CME Outfitters, Global Medical Education, and Merck.
Shawn M. McClintock. Dr. McClintock reports research support from the National Institutes of Health. He is a consultant to Pearson Assessment.
Martina Mueller. Dr. Mueller reports no conflicts of interest.
Georgios Petrides. Dr. Petrides has received research support from Amgen, AstraZeneca, Corcept, Eli Lilly, Proteus, St. Jude Medical, and Sunovion, and he has served on an advisory panel for Corcept.
Joan Prudic. Dr. Prudic reports no conflicts of interest.
Peter B. Rosenquist. Dr. Rosenquist reports no conflicts of interest.
Matthew V. Rudorfer. Dr. Rudorfer reports no conflicts of interest.
Shirlene Sampson. Dr. Sampson reports no conflicts of interest.
Abeba Teklehaimanot. Ms. Teklehaimanot reports no conflicts of interest.
Kristen G. Tobias. Dr. Tobias reports no conflicts of interest.
Richard D. Weiner. Dr. Weiner reports no conflicts of interest.
Robert C. Young. Dr. Young has received research support from NIMH.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Previous Presentation
Parts of this manuscript have previously been presented at the 2017 American College of Neuropsychopharmacology (ACNP) Annual Meeting.
Clinicaltrials.gov identifier
REFERENCES
- 1.Spaans H-P, Sienaert P, Bouckaert F, et al. Speed of remission in elderly patients with depression: electroconvulsive therapy <em>v.</em> medication. The British Journal of Psychiatry 2015; 206:67–71 [DOI] [PubMed] [Google Scholar]
- 2.Meyer JP, Swetter SK,Kellner CH: Electroconvulsive therapy in geriatric psychiatry: A selective review. Clinics in Geriatric Medicine In Press; [DOI] [PubMed] [Google Scholar]
- 3.Socci C, Medda P, Toni C, et al. Electroconvulsive therapy and age: Age-related clinical features and effectiveness in treatment resistant major depressive episode. Journal of Affective Disorders 2018; 227:627–632 [DOI] [PubMed] [Google Scholar]
- 4.Kumar S, Mulsant BH, Liu AY, et al. Systematic review of cognitive effects of electroconvulsive therapy in late-life depression. American Journal of Geriatric Psychiatry 2016; 24:547–565 [DOI] [PubMed] [Google Scholar]
- 5.McClintock SM, Choi J, Deng Z-D, et al. Multifactorial Determinants of the Neurocognitive Effects of Electroconvulsive Therapy. The Journal of ECT 2014; 30:165–176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sackeim HA, Prudic J, Fuller R, et al. The Cognitive Effects of Electroconvulsive Therapy in Community Settings. Neuropsychopharmacology 2006; 32:244–254 [DOI] [PubMed] [Google Scholar]
- 7.Smith GE, Rasmussen KG, Cullum CM, et al. A randomized controlled trial comparing the memory effects of continuation electroconvulsive therapy versus continuation pharmacotherapy: Results from the Consortium for Research in ECT (CORE) Study. Journal of Clinical Psychiatry 2010; 71:185–193 [DOI] [PubMed] [Google Scholar]
- 8.Verwijk E, Comijs HC, Kok RM, et al. Short- and long-term neurocognitive functioning after electroconvulsive therapy in depressed elderly: A prospective naturalistic study. International Psychogeriatrics 2014; 26:315–324 [DOI] [PubMed] [Google Scholar]
- 9.Sh Lisanby, McClintock SM, Alexopoulos G, et al. Neurocognitive Effects of Combined Electroconvulsive Therapy (ECT) and Venlafaxine in Geriatric Depression: Phase 1 of the PRIDE Study. The American Journal of Geriatric Psychiatry 2020; 28:304–316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Semkovska M,McLoughlin DM: Objective Cognitive Performance Associated with Electroconvulsive Therapy for Depression: A Systematic Review and Meta-Analysis. Biological Psychiatry 2010; 68:568–577 [DOI] [PubMed] [Google Scholar]
- 11.Narchal S, Harris AWF,Allen B: A comparison between right unilateral ultrabrief electroconvulsive therapy and bilateral electroconvulsive therapy in the elderly: A pilot naturalistic observational study. Australasian Psychiatry 2018; 26:394–397 [DOI] [PubMed] [Google Scholar]
- 12.Loo CK, Sainsbury K, Sheehan P, et al. A comparison of RUL ultrabrief pulse (0.3 ms) ECT and standard RUL ECT. International Journal of Neuropsychopharmacology 2008; 11:883–890 [DOI] [PubMed] [Google Scholar]
- 13.Martin DM, Galvez V,Loo CK: Predicting retrograde autobiographical memory changes following electroconvulsive therapy: Relationships between individual, treatment, and early clinical factors. International Journal of Neuropsychopharmacology 2015; 18:1–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Semkovska M, Landau S, Dunne R, et al. Bitemporal versus high-dose unilateral twice-weekly electroconvulsive therapy for depression (EFFECT-Dep): A pragmatic, randomized, non-inferiority trial. American Journal of Psychiatry 2016; 173:408–417 [DOI] [PubMed] [Google Scholar]
- 15.Semkovska M, Keane D, Babalola O, et al. Unilateral brief-pulse electroconvulsive therapy and cognition: Effects of electrode placement, stimulus dosage and time. Journal of Psychiatric Research 2011; 45:770–780 [DOI] [PubMed] [Google Scholar]
- 16.Tor P-C, Bautovich A, Wang M-J, et al. A systematic review and meta-analysis of brief versus ultrabrief right unilateral electroconvulsive therapy for depression. The Journal of clinical psychiatry 2015; 76:1092–1098 [DOI] [PubMed] [Google Scholar]
- 17.Verwijk E, Comijs hC, Kok RM, et al. Neurocognitive effects after brief pulse and ultrabrief pulse unilateral electroconvulsive therapy for major depression: a review. Journal of affective disorders 2012; 140:233–243 [DOI] [PubMed] [Google Scholar]
- 18.Sackeim HA, Dillingham EM, Prudic J, et al. Effect of concomitant pharmacotherapy on electrocovulsive therapy outcomes: Short-term efficacy and adverse effects. Archives of Genral Psychiatry 2009; 66:729–737 [DOI] [PubMed] [Google Scholar]
- 19.Kellner CH, Husain MM, Knapp RG, et al. A novel strategy for continuation ECT in geriatric depression: Phase 2 of the PRIDE Study. American Journal of Psychiatry 2016; 173:1110–1118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Folstein MF, Folstein SE,McHugh PR: “Mini-Mental State”: A practical method for grading the cognitive state of patients for clinicians. Journal of Psychiatric Research 1975; 12:189–198. [DOI] [PubMed] [Google Scholar]
- 21.Obbels J, Vansteelandt K, Verwijk E, et al. MMSE changes during and after ECT in late-life depression: A prospective study. American Journal of Geriatric Psychiatry 2019; 27:934–944 [DOI] [PubMed] [Google Scholar]
- 22.Moirand R, Galvao F, Lecompte M, et al. Usefulness of the Montreal Cognitive Assessment (MoCA) to monitor cognitive impairments in depressed patients receiving electroconvulsive therapy. Psychiatry research 2018; 259:476–481 [DOI] [PubMed] [Google Scholar]
- 23.Kellner CH, Husain MM, Knapp RG, et al. Right unilateral ultrabrief pulse ECT in geriatric depression: Phase 1 of the PRIDE Study. American Journal of Psychiatry 2016; 173:1101–1109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lisanby SH, Sampson S, Husain MM, et al. Towards individualized post-ECT care: Piloting the symptom-titrated algorithm-based longitudinal ECT (STABLE) intervention. Journal of ECT 2008; 24:179–182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hamilton M: A rating scale for depression. Journal of Neruology Neurosurgery and Psychiatry 1960; 23:56–62 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.American Psychiatric Association Task Force: The Practice of Electroconvulsive Therapy: Recommendations for Treatment, Training, and Privileging Second. Washington, DC, American Psychiatric Association, 2001 [Google Scholar]
- 27.First MB, Gibbon M, Spitzer RL, et al. User’s Guide for the Structured Clinical Interview for the DSM-IV Axis I Disorders-Research Version (SCID-I, Version 2.0), 1996 [Google Scholar]
- 28.Lecrubier Y, Sheehan D, Weiller E, et al. The Mini International Neuropsychiatric Interview (MINI): A short diagnostic structured interview: Reliability and validity according to the CIDI. European Psychiatry 1997; 12:224–231 [Google Scholar]
- 29.Beck AT: Beck Scale for Suicide Ideation (BSS) Manual, San Antonio, TX, Pearson, 1991 [Google Scholar]
- 30.McElhiney MC, Moody BJ,Sackeim HA: The Autobiographical Memory Interview Short Form: Manual for Administration and Scoring, New York, Department of Psychiatry, New York State Psychiatric Institute, 2001 [Google Scholar]
- 31.Delis DC, Kramer JH, Kaplan E, et al. California Verbal Learning Test-Second Edition. Adult Version. Manual, San Antonio, TX, Psychological Corporation, 2000 [Google Scholar]
- 32.Delis DC, Kaplan E,J K: Delis Kaplan Executive Function System, San Antonio, TX, The Psychological Corporation, 2001 [Google Scholar]
- 33.Jurica PJ, Leitten CL,Mattis S: DRS-2: Dementia Rating Scale-2 Professional Manual, Lutz, FL, Psychological Assessment Resources, Inc., 2001 [Google Scholar]
- 34.Golden CJ,Freshwater SM: Stroop Color and Word Test: A manual for clincal and experimental use, Wood Dale, II, Stoelting Co., 2002 [Google Scholar]
- 35.Wechsler D: The Wechsler Test of Adult Reading (WTAR), San Antonio, TX, The Psychological Corporation, 2001 [Google Scholar]
- 36.Brooks BL, Iverson GL: Comparing actual to estimated base rates of “abnormal” scores on neuropsychological test batteries: Implications for interpretation. Archives of Clinical Neuropsychology 2010; 25:14–21 [DOI] [PubMed] [Google Scholar]
- 37.Beglinger LJ, Gaydos B, Tangphao-Daniels O, et al. Practice effects and the use of alternate forms in serial neuropsychological testing. Archives of Clinical Neuropsychology 2005; 20:517–529 [DOI] [PubMed] [Google Scholar]
- 38.McClintock SM, Choi J, Deng ZD, et al. Multifactorial determinants of the neurocognitive effecdts of electroconvulsive therapy. Journal of ECT 2014; 30:165–176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sackeim HA, Prudic J, Fuller R, et al. The cognitive effects of electroconvulsive therapy in community settings. Neuropsychopharmacology 2007; 32:244–254 [DOI] [PubMed] [Google Scholar]
- 40.Obbels J, Verwijk E, Vansteelandt K, et al. Long-term neurocognitive functioning after electroconvulsive therapy in patients with late-life depression. Acta Psychiatrica Scandinavica 2018; 138:223–231 [DOI] [PubMed] [Google Scholar]
- 41.Schmutte T,Wilkinson S: Suicide in older adults with and without known mental illness: Results from the national violent death reporting system, 2003–2016. American Journal of Preventive Medicine In Press; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kellner Charles H., Max Fink Rebecca Knapp, et al. Relief of Expressed Suicidal Intent by ECT: A Consortium for Research in ECT Study. American Journal of Psychiatry 2005; 162:977–982 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.McCall WV, Lisanby SH, Rosenquist PB, et al. Effects of continuation electroconvulsive therapy on quality of life in elderly depressed patients: A randomized clinical trial. Journal of Psychiatric Research 2018; 97:65–69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kellner CH, Knapp RG, Petrides G, et al. Continuation Electroconvulsive Therapy vs Pharmacotherapy for Relapse Prevention in Major Depression: A Multisite Study From the Consortium for Research in Electroconvulsive Therapy (CORE). Archives of General Psychiatry 2006; 63:1337–1344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Dybedal GS, Bjolseth TM, Benth JS, et al. Cognitive effects of bifrontal versus right unilateral electrconvulsive therapy in the treatment of major depression in elderly adults: A randomized, controlled trial. Journal of ECT 2016; 32:151–158 [DOI] [PubMed] [Google Scholar]
- 46.Kumar S, Mulsant BH, Liu A, et al. Systematic review of cognitive effects of electroconvulsive therapy in late-life depression. American Journal of Geriatric Psychiatry 2016; 24:547–565 [DOI] [PubMed] [Google Scholar]
- 47.Osler M, Rozing M, Christensen G, et al. Electroconvulsive therapy and risk of dementia in patients with affective disorders: A cohort Study. Lancet Psychiatry 2018; 5:348–356 [DOI] [PubMed] [Google Scholar]
- 48.Anderson I, McAllister-Williams R, Downey D, et al. Cognitive function after electroconvulsive therapy for depression: Relationship to clinical response. Psychological Medicine In Press; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Obbels J, Vansteelandt K, Bouckaert F, et al. Neurocognitive functioning after electroconvulsive therapy in late-life depression: a four-year prospective study. Acta Psychiatrica Scandinavica 2020; [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.