

Abstract
Cervical cancer rates in Mississippi are disproportionately high, particularly among Black individuals; yet, research in this population is lacking. We designed a statewide, racially diverse cohort of individuals undergoing cervical screening in Mississippi. Here, we report the baseline findings from this study.
We included individuals aged 21 years and older undergoing cervical screening with cytology or cytology-human papillomavirus (HPV) co-testing at the Mississippi State Health Department (MSDH) and the University of Mississippi Medical Center (UMMC) (December 2017-May 2020). We collected discarded cytology specimens for future biomarker testing. Demographics and clinical results were abstracted from electronic medical records and evaluated using descriptive statistics and chi-square tests.
A total of 24,796 individuals were included, with a median age of 34.8 years. The distribution of race in our cohort was 60.2% Black, 26.4% White, 7.5% other, and 5.9% missing. Approximately 15% had abnormal cytology and, among those who underwent co-testing at MSDH (n=6,377), HPV positivity was 17.4% and did not vary significantly by race. Among HPV positives, Black individuals were significantly less likely to be HPV16/18 positive and more likely to be positive for other high-risk 12 HPV types compared to White individuals (20.5% vs. 27.9%, and 79.5% and 72.1%, respectively, p=0.011).
Our statewide cohort represents one of the largest racially diverse studies of cervical screening in the U.S. We show a high burden of abnormal cytology and HPV positivity, with significant racial differences in HPV genotype prevalence. Future studies will evaluate cervical precancer risk, HPV genotyping, and novel biomarkers in this population.
Keywords: HPV, Cervical Cancer, Disparities, Race, Cervical Cancer Screening
Introduction
Notable racial and regional disparities exist for cervical cancer in the United States (U.S.).1,2 Mortality rates of cervical cancer are higher in Black and Hispanic individuals, and those living in non-metropolitan U.S. counties, whereas rates are lower in White individuals, among those living in metropolitan areas, and those with higher socioeconomic status.3 Mississippi (MS), a state with one of the highest burdens of cervical cancer, includes one of the largest proportions of Black individuals in the Southern U.S.1 Almost 80% of MS counties are rural with some of the lowest per capita income and poorest health outcomes within the U.S.3 Cervical cancer mortality rates in MS are 3.5 per 100,000 compared to 2.3 per 100,000 in the U.S. (2013–2017)4 and Black individuals in MS are nearly twice as likely to die from cervical cancer compared to their White counterparts (5.0 vs 2.8 per 100,000 respectively; 2013–2017).5 Whether these mortality differences can be explained by lack of screening, loss to follow-up, delayed or suboptimal treatment, or other reasons, is unclear.
As new technologies are being evaluated for cervical cancer screening and management, it is important that studies include diverse populations to ensure that recommendations and guidelines are applicable to all individuals undergoing cervical screening. For example, prior studies have revealed differences in the distribution of HPV genotypes by race. We previously showed a significantly lower prevalence of human papillomavirus (HPV) 16 among Black individuals with Atypical Squamous Cells of Undermined Significance (ASC-US) cytology results compared to White individuals in MS.6 Collectively these findings could have implications for HPV vaccination and HPV testing strategies using extended genotyping, and emphasize the need for studies that enrich for diverse populations when evaluating new technologies.
To date, very few cervical cancer screening studies have been conducted in diverse populations such as those in MS, despite the fact that it has one of the highest cervical cancer burdens in the U.S. To address this gap, we designed STRIDES - STudying Risk to Improve DisparitiES in cervical cancer in MS, a large statewide cohort study of individuals undergoing cervical cancer screening in MS. STRIDES is an interdisciplinary collaborative effort among the School of Nursing at the University of Mississippi Medical Center (UMMC), the Mississippi State Department of Health (MSDH), and the National Institutes of Health National Cancer Institute (NCI). STRIDES aims to evaluate the risk of cervical precancer and cancer and to assess the performance of HPV-related biomarkers in this high-risk, diverse population.
Materials and Methods
Study Population and Design
Our study population includes all individuals undergoing cervical cancer screening and management at UMMC or MSDH. UMMC is the sole academic medical center in the state, and all cervical pathology samples from both UMMC and MSDH clinics are sent to and interpreted by the Department of Pathology at UMMC. The statewide sample includes individuals from urban areas attending UMMC clinics in the metropolitan tri-county area and those attending the 88 MSDH clinics throughout the state, of which 79% are located in rural areas (Supplemental Figure 1). Cervical cancer screening services are covered by public funding at MSDH clinics. The sampling design for data collection includes all consecutive cumulative electronic health records (EHR) available from those receiving cytology, HPV testing, or both, as of December 23, 2017. We began collecting routinely discarded cytology specimens as of May 20, 2018 and gradually increased the coverage and as of November 2018 and onward, we achieved nearly complete specimen capture (96%) of all screened patients identified in the EHR data.
This study includes data from the baseline visit, defined as the first screening visit in the EHR as of December 23, 2017. A universal study ID and the key is secured in REDCap®7 with restricted study personnel access. Record linkage enables the ascertainment of repeat specimens and all follow-up data in the EHR from individuals included in the study. The Institutional Review Boards at UMMC and MSDH approved this protocol. A HIPAA waiver of authorization and HIPAA waiver of informed consent were granted.
Demographics and Co-variates
All information from the EHR is obtained at the time of the screening visit. The demographic patient variables include age, race, and ethnicity; these variables are reported in the EHR based on the intake information recorded from the patient. Race is based on the following categories reported in the EHR: White or Caucasian (“White”), Black or African American (“Black”), American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, Multiracial, Other Race, and includes Patient Refused or Unknown. Due to low sample size, American Indian or Alaska Native, Choctaw Indian, Asian, Native Hawaiian, or Other Pacific Islander, were combined into one category (“Other Race”). Ethnicity includes Not Hispanic or Latina, Hispanic or Latina, Unknown or Patient Refused. Co-variates include body mass index (BMI) and smoking. BMI was categorized according to clinical cutpoints as < 25 (underweight/normal) kg/m2, ≥ 25 and < 30 (overweight) kg/m2, ≥30 and < 35 (obese, class I) kg/m2, ≥ (obese, class II+) kg/m2. Smoking status includes never smokers, former, and current smokers.
Cytology Testing
All specimens are processed and interpreted in the UMMC Department of Pathology. Liquid-based cytology (Pap test) is performed on all cervical cytologic specimens using the ThinPrep Pap 2000 System (Hologic®). A cervical specimen is collected via spatula and Cytobrush (Pap Perfect Plastic Spatula and Cytobrush Plus GT Medscan; Trumbul, CT). Following specimen processing and prescreening with automated image analysis, the cytotechnologist continues with full screening prior to final cytologic interpretation by a pathologist. Cytologic interpretation occurs without prior knowledge of the HPV result. Cytology results are interpreted using the Bethesda 2014 terminology.8 All specimens were screened by 1–2 cytotechnologists followed by pathologist review per UMMC protocol. An average of 4 pathologists are responsible for the interpretations at UMMC. Results are classified as negative for intraepithelial lesion or malignancy (NILM, including NILM with atrophy, or reactive reparative). Additional cytologic categories include ASC-US, low-grade squamous intraepithelial lesions (LSIL), atypical squamous cells of undetermined significance high grade (ASC-H), or high-grade intraepithelial lesions (HSIL) or worse as HSIL+. Glandular lesions are categorized as “endometrial/glandular”.
HPV Testing
HPV testing was performed according to the 2012 ASCCP consensus management recommendations.9 Cervical cancer screening at MSDH changed from cytology with ASC-US triage with HPV testing (HPV ASC-US triage) to HPV and cytology co-testing on July 1, 2018, for those aged 30 years and older. UMMC clinics predominantly perform co-testing for individuals in this age group and HPV ASC-US triage for those under age 30; however, a portion of UMMC clinics/providers continue to perform screening using cytology with ASC-US triage. Therefore, we do not report overall HPV positivity here due to differences in screening practices and HPV testing between the two institutions. For this baseline analysis, we present HPV testing results for the MSDH cohort only which strictly adheres to co-testing recommendations as of July 1, 2018.
HPV testing is carried out using the Roche Diagnostics cobas4800® HPV genotyping test (Roche Molecular Systems, Pleasanton, CA) (Roche, 2018). The assay uses a total nucleic acid isolation sample preparation with real-time polymerase chain reaction and targets 14 HPV genotypes. The assay provides type-specific identification of types 16 and 18 and pools 12 „Other‟ high risk (HR 12) HPV genotypes: 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 (Roche, 2018).
Biospecimen Collection and Pathology Processing
We established a biospecimen bank at the UMMC School of Nursing (SON) biosafety level two laboratory. Specimens are collected after pathology processing following each screening visit within 2 weeks. The specimens are inventoried in the UMMC SON using a study-specific electronic data management system and the Biospecimen Inventory (BSI) and resource management system and stored at 4 degrees Celsius. A specimen inventory is maintained in BSI and REDCap®. Only de-identified data and specimens are shared outside UMMC and MSDH. Final storage of the biospecimens will be at the National Institutes of Health (NIH) biorepository.
Histologic Endpoints
Currently, we are reporting baseline HPV and cytology screening results. Ascertainment of histologic endpoints from the EHR is ongoing and will be reported in the future. Follow-up for screening and histology information in the EHR is planned for five years. We will evaluate risk of cervical precancer and cancer in subsequent studies when ascertainment of histologic outcomes is more complete.
Statistical Methodology
We used descriptive statistics and Pearson chi-square tests to evaluate study population characteristics overall, by institution, and by race. We evaluated the distribution of HPV genotypes using hierarchical categorization as follows: HPV 16, including single and multiple infection; then HPV 18, including single and multiple infections; then other HR 12 infections; then HPV negative. All reported p-values were two-sided, and a p-value <0.05 was considered significant. Statistical analyses were conducted using STATA/SE, version 16.0.
Results
Study Population
As of May 7, 2020, a total of 24,796 individuals who underwent cervical cancer screening and management at MSDH or UMMC were included. Our study sample includes individuals from every county in MS, with broad coverage across the state and in rural and urban areas (Supplemental Figure 1). So far, a total of 20,399 discarded cervical specimens have been collected from 18,873 individuals, of these 1,383 had at least one repeat sample.
A total of 16,631 individuals (67.1%) were screened at MSDH and 8,165 (32.9%) were screened at UMMC (Table 1). Among all individuals, the median age was 34.8 years (SD = ± 12.1 years; range = 16–89 years), and 14,079 (56.8%) were aged 30 years and older (Table 1). Individuals screened at MSDH tended to be younger compared to UMMC (52.9% vs. 23.5% under age 30 years, respectively). Black individuals comprised the largest racial group (n=14,933, 60.2%), followed by White individuals (n=6,545, 26.4%). Among those with ethnicity information, the majority (91.6%) were non-Hispanic. Overall, 48.1% of the study population was classified as obese, with a BMI ≥ 30 kg/m2. The prevalence of obesity was significantly higher among those screened at UMMC compared to MSDH (53.8% vs. 45.3%, respectively; p=0.0001). Two-thirds of the overall population reported never smoking; individuals screened at MSDH were significantly more likely to report current smoking compared to those at UMMC (26.3% vs. 13.0%, respectively; p=0.0001).
Table 1.
Population Characteristics of Individuals Undergoing Cervical Cancer Screening at MSDH and UMMC, December 23, 2017 – May 07, 2020
| UMMC (n, %) 8165 (32.9) |
MSDH (n, %) 16631 (67.1) |
Total N = 24796 |
|
|---|---|---|---|
| Age Group (years) | |||
| 20–24 | 862 (10.6) | 4675 (28.1) | 5537 (22.3) |
| 25–29 | 1057 (12.9) | 4123 (24.8) | 5180 (20.9) |
| 30–65 | 5837 (71.5) | 7831 (47.1) | 13668 (55.1) |
| >65 | 409 (5.0) | 2 (0.1) | 411 (1.7) |
| Race | |||
| White | 2404 (29.5) | 4141 (24.9) | 6545 (26.4) |
| African American or Black | 5351 (65.6) | 9582 (57.6) | 14933 (60.2) |
| Other | 302 (3.7) | 1552 (9.3) | 1854 (7.5) |
| Refused/Unknown/Missing | 108 (1.3) | 1356 (8.1) | 1464 (5.9) |
| Ethnicity | |||
| Not Hispanic or Latina | 7909 (96.9) | 12211 (73.4) | 20120 (81.3) |
| Hispanic or Latina | 128 (1.6) | 1720 (10.3) | 1848 (7.5) |
| Unknown/Refused/Missing | 128 (1.5) | 2700 (16.3) | 2828 (11.4) |
| Body Mass Index, kg/m2 | |||
| <25 | 1658 (20.3) | 3749 (22.5) | 5407 (21.8) |
| >= 25 and <30 | 1830 (22.4) | 3743 (22.5) | 5573 (22.5) |
| >=30 and <35 | 1629 (20.0) | 3132 (18.8) | 4761 (19.2) |
| >=35 | 2763 (33.8) | 4400 (26.5) | 7163 (28.9) |
| Missing | 285 (3.5) | 1607 (9.6) | 1892 (7.6) |
| Smoking Status | |||
| Never Smoker | 5718 (70.0) | 10814 (65.0) | 16532 (66.7) |
| Former | 1219 (14.9) | 1365 (8.2) | 2584 (10.4) |
| Current | 1058 (13.0) | 4369 (26.3) | 5427 (21.9) |
| Unknown/Missing | 170 (2.1) | 83 (0.5) | 253 (1.0) |
All comparisons were statistically significant at P<0.0001.
Abbreviations: UMMC, University of Mississippi Medical Center; MSDH, Mississippi State Department of Health; NA, not available
Baseline Characteristics by Race and Institution
As shown in Supplemental Table 1, within the two institutions age distributions were very similar. In both institutions, Black individuals were more likely to be classified as obese compared to White individuals, particularly among those screened at UMMC (63.1% obese Black and 37.2% obese White individuals). At both institutions, White individuals were more likely to be current smokers compared to Black individuals, with a particularly high proportion of White current smokers at MSDH (42.6%) (Supplemental Table 1).
Cytology and HPV Screening Overall and by Race
Cytology diagnoses were comparable across institutions (Table 2), with 15.5% of the population at UMMC and 15.3% at MSDH having cytology other than NILM (i.e., abnormal). Minimal differences in overall cytology diagnoses were noted between White and Black individuals. Individuals classified as “Other Race” had the highest proportion of NILM cytology at both institutions (86.8% at UMMC and 90.3% at MSDH).
Table 2.
Baseline cytology diagnosis by institution and race in the STRIDES cohort, Dec. 23, 2017 – May 7, 2020
| UMMC | ||||||
|---|---|---|---|---|---|---|
| n (%) | Caucasian or White 2404 (29.4) |
AA or Black 5351 (65.6) |
Other 302 (3.7) |
Missing 104 (1.3) |
Total 8165 (32.9) |
P-Value |
| NILM | 2061 (85.7) | 4476 (83.7) | 262 (86.8) | 100 (93.4) | 6899 (84.5) | 0.082 |
| ASC-US | 116 (4.8) | 323 (6.0) | 17 (5.6) | 1 (0.9) | 457 (5.6) | |
| LSIL | 102 (4.2) | 271 (5.1) | 8 (2.7) | 3 (2.9) | 384 (4.7) | |
| ASC-H | 6 (0.3) | 25 (0.5) | 2 (0.7) | 0 | 33 (0.4) | |
| HSIL | 30 (1.3) | 78 (1.5) | 5 (1.7) | 0 | 113 (1.4) | |
| Endometrial/Glandular | 5 (0.2) | 20 (0.4) | 0 | 1 (0.0) | 26 (0.3) | |
| Unsatisfactory | 84 (3.5) | 158 (3.0) | 8 (2.7) | 3 (2.8) | 253 (3.1) | |
| MSDH | ||||||
| n (%) | Caucasian or White 4141 (24.9) |
AA or Black 9582 (57.6) |
Other 1552 (9.3) |
Missing 1354 (8.2) |
Total 16631 (67.1) |
P-Value |
| NILM | 3480 (84.0) | 8041 (83.9) | 1402 (90.3) | 1155 (85.3) | 14078 (84.7) | <0.001 |
| ASC-US | 277 (6.7) | 669 (7.0) | 62 (3.9) | 83 (6.1) | 1091(6.6) | |
| LSIL | 245 (5.9) | 624 (6.5) | 60 (3.9) | 99 (7.3) | 1028 (6.1) | |
| ASC-H | 24 (0.6) | 46 (0.5) | 6 (0.4) | 3 (0.2) | 79 (0.5) | |
| HSIL | 73 (1.8) | 142 (1.5) | 6 (0.4) | 10 (0.7) | 231 (1.4) | |
| Endometrial/Glandular | 8 (0.2) | 5 (0.1) | 0 | 0 | 13 (0.1) | |
| Unsatisfactory | 34 (0.8) | 55 (0.6) | 16 (1.0) | 6 (0.4) | 111 (0.6) | |
Abbreviations: AA = African American, NILM = negative for intraepithelial lesion or malignancy, ASC-US = atypical squamous cells of undetermined significance, LSIL = low grade squamous intraepithelial lesion, ASC-H = atypical squamous cells of undetermined significance, high grade HSIL = high grade squamous intraepithelial lesion, Endometrial/Glandular = combined cytology categories with glandular lesions, Unsatisfactory = unsatisfactory for evaluation.
Screening practices differ by institution and over time. Based on provider preference, UMMC uses either HPV and cytology co-testing, or cytology alone with reflex HPV testing in those with ASC-US in approximately 30% of UMMC patients (data not shown). Beginning on July 1, 2018, MSDH fully transitioned from cytology with ASC-US HPV triage to co-testing for individuals aged 30 years and older (aged 30+), with those aged less than 30 years-old (aged <30) still undergoing cytology and ASC-US HPV triage. As stated earlier, due to these differences in screening practices involving selective HPV testing for a subgroup of individuals, we did not estimate the overall HPV positivity for the full population. Including the entire time frame of data, among those with ASC-US cytology, who are uniformly tested for HPV, HPV prevalence across institutions was 1,446 or 48.1% (data not shown).
Table 3 shows the distribution of cytology screening results before and after implementation of co-testing at MSDH, stratified by age. Among individuals aged 30+, the distribution of cytology results remained very similar across the two time periods, suggesting that cytology practice did not change with implementation of co-testing. After implementation of co-testing, the overall prevalence of HPV in the MSDH cohort was 17.4%, and increased with increasing severity of cytology (e.g., 13.6% in those with NILM and 93.6% in those with HSIL+). The prevalence of HPV among individuals with ASC-US increased slightly from 30.7% to 40.1% across the two periods (p=0.102). Among individuals aged <30 who underwent screening with cytology and ASC-US triage with HPV testing across both time periods at MSDH, the prevalence of HPV among those with ASC-US was similar (60.9% and 62.6%, respectively).
Table 3.
Age-stratified HPV results by cytology category for STRIDES individuals from the Mississippi State Department of Health (MSDH) before and after the institution changed to co-testing for women aged 30+
| n (%) = 16631 | ASC-US triage, Prior to July 1, 2018^ | Co-testing, After July 1, 2018^ | P-Value | ||
|---|---|---|---|---|---|
| HPV Results – Age 30+ | HPV Results – Age 30+ | ||||
| Cytology Category | Cytology (col %) | HPV + (row %) | Cytology (col %) | HPV + (row %) | |
| NILM | 1279 (87.8) | 5689 (89.2) | 775* (13.6) | ||
| ASC-US | 88 (6.0) | 27* (30.7) | 359 (5.6) | 144* (40.1) | 0.102 |
| LSIL | 43 (3.0) | 175 (2.7) | 100* (57.1) | ||
| ASC-H | 14 (1.0) | 21 (0.3) | 14* (66.7) | ||
| HSIL | 16 (1.1) | 78 (1.2) | 73 (93.6) | ||
| Endo/Glandular | 3 (0.2) | 9 (0.1) | 1* (11.1) | ||
| Inadequate | 13 (0.9) | 46 (0.7) | 4 (8.7) | ||
| Totals | 1456 | 27 (30.7) | 6377 | 1111 (17.4) | |
| HPV Results – Age <30 | HPV Results – Age <30 | ||||
| Cytology (col %) | HPV + (row %) | Cytology (col %) | HPV + (row %) | ||
| NILM | 1304 (78.9) | 5806 (81.3) | 4 (1.2) | ||
| ASC-US | 128 (7.7) | 78* (60.9%) | 516 (7.2) | 323* (62.6) | 0.806 |
| LSIL | 168 (10.2) | 642 (9.0) | 0 | ||
| ASC-H | 9 (0.5) | 35 (0.5) | 0 | ||
| HSIL | 29 (1.8) | 108 (1.5) | 0 | ||
| Endo/Glandular | 0 (0.0) | 1 (0.0) | 0 | ||
| Inadequate | 15 (0.9) | 37 (0.5) | 0 | ||
| Totals | 1653 | 78 (60.9%) | 7145 | 327 (63.8) | |
Abbreviations: NILM = negative for intraepithelial lesion or malignancy, ASC-US = atypical squamous cells of undetermined significance, LSIL = low grade squamous intraepithelial lesion, ASC-H = atypical squamous cells of undetermined significance, high grade HSIL = high grade squamous intraepithelial lesion, Endometrial/Glandular = combined cytology categories with glandular lesions, Unsatisfactory = unsatisfactory for evaluation.
Prior to July 1, 2018, screening practice at MSDH consisted of cytology with HPV triage of women with a diagnosis of ASC-US for women of all ages. MSDH switched to HPV and cytology co-testing for women aged 30+ as of July 1, 2018
Contains a missing HPV test., The HPV test was not available for evaluation. A total of 90 HPV tests are missing in all.
Partial HPV genotyping results for 5,515 Black and White individuals screened at MSDH with co-testing, stratified by age, are shown in Table 4. Overall, 23.1% were HPV positive; HPV positivity did not significantly differ by race within each age group. Of those that were HPV positive, 21.0% were positive for HPV16 and/or HPV18, whereas 79.0% were positive for other HR 12 HPV types. In those aged 30+, Black individuals were significantly less likely to be positive for HPV16/18 compared to White individuals (20.5% vs. 27.9%, respectively, p = 0.011), whereas there was no statistically significant difference in HPV16/18 prevalence among those aged <30. These differences persisted in multivariate models when adjusting for age, race, BMI, and smoking (data not shown).
Table 4.
Diagnosis of human papillomavirus (HPV) by age and race categories from the Mississippi State Department of Health (MSDH)., July 1, 2018 – May 7, 2020, N=5515
| n (%) |
*Age <
30 n = 469 (8.5) |
Age
30+ n = 5046 (91.5) |
Totals |
P-value Age <30 vs 30+ |
||
|---|---|---|---|---|---|---|
| HPV results by Race | White | AA or Black | White | AA or Black | n = 5515 | |
| HPV negative total | 57 (44.8) | 125 (36.4) | 1216 (80.5) | 2843 (80.4) | 4241 (76.9) | |
| HPV positive total | 69 (55.2) | 218 (63.6) | 294 (19.5) | 693 (19.6) | 1274 (23.1) | |
| Chi square tests | p = 0.083 | p = 0.916 | <0.001 | |||
| HPV positive type | White | AA or Black | White | AA or Black | n = 1274 | |
| HPV HR 12 Other, | 58 (84.1) | 185 (84.9) | 212 (72.1) | 551 (79.5) | 1006 (78.9) | |
| HPV HR 16/18 | 11 (15.9) | 33 (15.1) | 82 (27.9) | 142 (20.5) | 268 (21.0) | |
| Pearson chi square | p = 0.872 | p = 0.011 | <0.001 | |||
HPV HR 16/18 = HPV 16, 18. HPV HR 12 Other = HPV31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68.
HPV tests in those under age 30 are ASC-US triage only.
Discussion
In this large, racially diverse population, previously underrepresented in cervical cancer research, we present baseline characteristics and results for individuals undergoing cervical cancer screening and management in Mississippi. Overall, we observed a higher distribution of abnormal cytology results compared to other population-based studies of cervical cancer screening, e.g., 15.4% in MS vs. 7.2% in the New Mexico HPV Pap Registry and 6.1% in the Kaiser Permanente Northern California cohorts10 as well as higher overall HPV positivity among those aged 30+ (MSDH only) (e.g., 17.4% in MS vs. 7.5% in Northern California).11 Consistent with our statewide findings, a high HPV prevalence of 18% was previously reported in western Mississippi, a region commonly referred to as the Mississippi Delta.12 The factors underlying the high prevalence of abnormal screening results in our study cohort are not completely understood. Mississippi‟s Youth Risk Behavior Surveillance System (YRBSS) 2019 reports a higher percentage of the high school students who initiated sex prior to age 13 (5.4%) and those with more than 4 sexual partners (10.1%) in their lifetime compared with those living in the US on average (3.0% and 8.6%, respectively).13 However, we are not collecting information about sexual behaviors from our study population. Future follow-up will enable the assessment of screening and follow-up behaviors and how they relate to the burden of HPV and abnormal cytology in our cohort.
Notably, we found significant differences in HPV type distribution by race, with Black individuals aged 30+ more likely to be positive for other HR 12 HPV types and less likely to be positive for HPV16/18 compared to White individuals. These findings are in line with our previous study evaluating partial HPV genotyping in individuals from MSDH with ASC-US cytology.5 Previous studies have reported differences in HPV type variants and in HPV type distribution in different geographic regions around the world, and in different racial/ethnic groups, suggesting co-evalution and adaptation of HPV to host ancestry.14–16 For example, a lower prevalence of HPV16 has been reported in Blacks compared to Whites.17–21 Pinheiro, Gage, et al., (2020), confirmed that HPV35 is more common in Black individuals, but showed that risk of precancer and cancer is not elevated.22 Further investigation in our cohort using extended genotyping is underway23.
The 2019 ASCCP risk-based management consensus guidelines for cervical cancer were based on risk estimates of cervical precancer in large screening populations.24 However, the representation of Black individuals in large population-based studies with HPV genotyping in the U.S. is limited.10 With extended follow-up and repeat sample collection, our cohort study will allow assessment of natural history of specific HPV genotypes in a diverse and understudied population. Understanding racial differences in HPV genotype prevalence and HPV genotype-specific risk of precancer and cancer is important to inform cervical cancer prevention efforts. STRIDES will provide an opportunity to evaluate this important question. Moreover, we will be able to evaluate the performance of HPV-related biomarkers such as DNA methylation and p16/Ki-67 dual stain by race.25–28 Linkage to histologic outcomes and ascertainment of follow-up data are ongoing using informatics and clinician chart review; this will enable us to specifically address these questions in future studies. Further, our study allows us to address program-wide aspects of cervical cancer screening, particularly the important role of managing abnormal test results and treatment to assess the factors underlying the high cervical cancer incidence and mortality in MS.
Strengths and Limitations
A strength of our study is that our population includes a large proportion of African American or Black individuals and those living in rural areas who have been underrepresented with respect to cervical cancer research, in spite of experiencing a disproportionate burden of the disease and mortality. We used race information obtained from the EHR, which can be misclassified, as a proxy for genetic ancestry. Ancestry is typically not available in screening studies like ours. We have full ascertainment of the screening cohort at both MSDH and UMMC through the EHR with retrospective data and sample collection and centralized pathology review, limiting the potential for selection bias. While our study is fully representative of individuals undergoing cervical cancer screening at all MSDH clinics across the state and at UMMC, it may not be representative of all individuals eligible for cervical cancer screening in the state. For example, our study population is enriched for Black individuals compared to MS overall (60% vs. 38%). Given the fact that cervical cancer screening at MSDH is publicly funded, it is plausible that individuals included in our study are less likely to be insured and of lower socioeconomic status compared to those in MS overall; however, we are unable to directly assess this.
HPV vaccination status is not reported in our data. MS continues to rank lowest in the nation for HPV vaccine coverage (49.5% in MS versus 71.5% in the U.S. overall receiving at least one dose in 2019) and Black teens are more likely to receive at least one dose compared to White teens in MS (55.3% versus 40.7%, respectively in 2019). While it is possible that differential vaccine uptake could explain differences in the prevalence of HPV16/18 by race, our findings were largely restricted to those aged 30 years and older and only a small proportion of these individuals would have been vaccinated at catch-up ages.29 Finally, while we did not include cervical histology results in this baseline description, follow-up of the cohort‟s histological outcomes will enable calculation of cervical precancer and cancer risk estimates by HPV type.
Summary
With continued follow-up and additional specimen collection planned over several years, our cohort study will allow for the study of HPV natural history and risk of precancer and cancer in a racially-diverse state with a particularly high burden of cervical cancer incidence and mortality. Going forward, it will be important to evaluate the implications of our findings of differential prevalence of HPV genotypes by race with respect to cervical precancer and cancer risk. In addition, future analyses will evaluate testing results of new screening biomarkers such as extended HPV genotyping, DNA methylation assays, and p16/ki67 dual stain. Results from this work will be relevant for informing current cervical cancer screening and management guidelines and for the evaluation and development of new technologies.
Supplementary Material
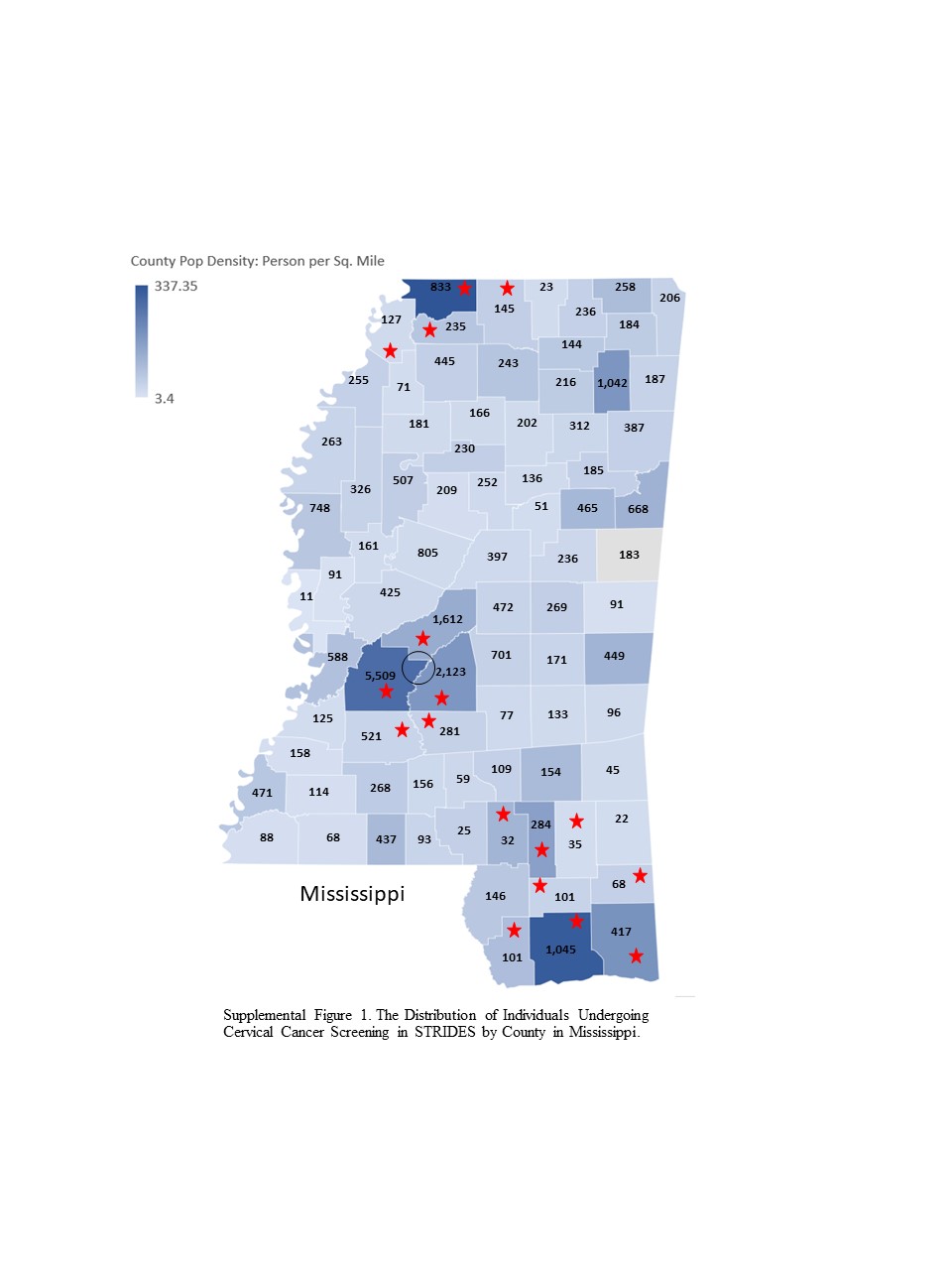
Supplemental Figure 1. The Distribution of Individuals Undergoing Cervical Cancer Screening in STRIDES by County in Mississippi. This figure depicts the number of individuals in STRIDES by county within MS. The map is color-coded according to population density including information from the 2010 U.S. Census on males and females of all ages living in the county. Lighter colors correspond to lower population density, whereas darker shading corresponds to higher population density. Counties with a red star are designated as Urban and counties without a red star are designated as rural, according to the USDA Office of Management and Budget https://www.ers.usda.gov/topics/rural-economypopulation/rural-classifications/. The hollow circle indicates the UMMC catchment area.
{kind=link}
Supplemental Table 1. Population characteristics stratified by race* of individuals undergoing cervical cancer screening at MSDH and UMMC, December 23, 2017 – May 07, 2020
Highlights.
Cervical screening cohort - underrepresented rural and racially diverse population
High prevalence of abnormal cytology and HPV positivity
Significant difference of HPV genotype distribution by race
Acknowledgments
The authors would like to thank Mildred Ridgway, MD, Bethany Sabins, NP, Laura Tucker, MSN, RN, and Thomas Dobbs, MD, for their collaborative clinical site guidance. Additionally, we are grateful for the contribution of Dr. Doug Hiser for his development of the novel methods used in our study-specific data and specimen management tool.
The opinions or assertations contained herein do not reflect the official policy of the Department of the Army, Department of Defense.3
Funding statement:
This work was supported by interagency funding at the U.S. National Cancer Institute, a grant from the Mississippi Nurses Foundation (MNF), the University of Mississippi Medical Center School of Nursing, and the Mississippi Center for Translational Research Center - National Institute of General Medical Sciences of the National Institutes of Health under Award Number 1U54GM115428.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of interest statement: The authors do not have any conflicts of interest to report.
Data statement - Data sharing is governed by the Institutional Review Board of the University of Mississippi Medical Center and restricted to investigators included on the study protocol. Summary data can be made available upon request.
References
- 1.Centers for Disease Control and Prevention and National Cancer Institute. State Cancer Profiles. Dynamic views of cancer statistics for prioritizing cancer control efforts across the nation. 2020. https://www.statecancerprofiles.cancer.gov/deathrates/index.php?stateFIPS=00&areatype=state&cancer=057&race=00&age=001&year=0&type=death&sortVariableName=rate&sortOrder=default#results. Last accessed, January 2, 2021.
- 2.Burger EA, Lee K, Saraiya M, et al. Racial and ethnic disparities in human papillomavirus-associated cancer burden with first-generation and second-generation human papillomavirus vaccines. Cancer. 2016; 122(13):2057–2066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mississippi State Department of Health Office of Rural Health and Primary Care Mississippi Primary Care Needs Assessment 2016. https://msdh.ms.gov/msdhsite/_static/resources/7357.pdf. Last accessed January 2, 2021.
- 4.Center for Disease Control and Prevention. United States Cancer Statistics: Data Visualizations. https://gis.cdc.gov/Cancer/USCS/DataViz.html. Last accessed April 27, 2021.
- 5.Mississippi Cancer Registry. https://www.umc.edu/cancerinstitute/Cancer-Research/Cancer-Registries/Mississippi%20Cancer%20Registry/HOME-PAGE-CONTENT.html. Last accessed, January 2, 2021.
- 6.Risley C, Clarke M, Geisinger K, Stewart M, Zhang L, DeMarco M, Schiffman M, Wentzensen N. Racial Differences in Human Papillomavirus Type 16 Prevalence in Women with Atypical Squamous Cells of Undetermined Significance of the Uterine Cervix. Cancer Cytopathology. Cancer Cytopathology, 2020; 128(8):528–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Harris PA, Taylor R Thielke J, Payne N, Gonzalez JG. Conde, Research electronic data capture (REDCap) – A metadata-driven methodology and workflow process for providing translational research informatics support, J Biomed Inform. 2009; April;42(2):377–81 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nayar R, Wilbur DC. The Pap test and Bethesda 2014. Cancer Cytopathol. 2015; 123(5):271–281. [DOI] [PubMed] [Google Scholar]
- 9.Massad LS, Einstein MH, Huh WK, et al. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. Obstet Gynecol. 2013; 121(4):829–846. [DOI] [PubMed] [Google Scholar]
- 10.Gage JC, Hunt WC, Schiffman M, et al. Similar Risk Patterns After Cervical Screening in Two Large U.S. Populations: Implications for Clinical Guidelines. Obstet Gynecol. 2016; 128(6):1248–1257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Demarco M, Lorey TS, Fetterman B, et al. Risks of CIN 2+, CIN 3+, and Cancer by Cytology and Human Papillomavirus Status: The Foundation of Risk-Based Cervical Screening Guidelines. Journal of lower genital tract disease. 2017; 21(4):261–267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Castle PE, Gage JC, Partridge EE, et al. : Human papillomavirus genotypes detected in clinician-collected and self-collected specimens from women living in the Mississippi Delta. BMC Infect Dis. 2013; 13(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Center for Disease Control and Prevention. High School YRBS. Mississippi 2019. https://nccd.cdc.gov/youthonline/App/Results.aspx?LID=MS. Last accessed, May 19, 2021.
- 14.Clifford GM, Tenet V, Georges D, et al. Human papillomavirus 16 sub-lineage dispersal and cervical cancer risk worldwide: Whole viral genome sequences from 7116 HPV16-positive women. Papillomavirus research (Amsterdam, Netherlands). 2019; 7:67–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Guan P, Howell-Jones R, Li N, et al. Human papillomavirus types in 115,789 HPV-positive women: a meta-analysis from cervical infection to cancer. International journal of cancer. 2012; 131(10):2349–2359. [DOI] [PubMed] [Google Scholar]
- 16.Bruni L, Albero G, Serrano B, Mena M, Gómez D, Muñoz J, Bosch FX, de Sanjosé S. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World. Summary Report 17 December 2020 ICO/IARC
- 17.Vidal AC, Smith JS, Valea F, et al. HPV genotypes and cervical intraepithelial neoplasia in a multiethnic cohort in the southeastern USA. Cancer causes & control : CCC. 2014; 25(8):1055–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Saraiya M, Unger ER, Thompson TD, et al. US Assessment of HPV Types in Cancers: Implications for Current and 9-Valent HPV Vaccines. JNCI: Journal of the National Cancer Institute. 2015; 107(6):1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Niccolai LM, Russ C, Julian PJ, et al. Individual and geographic disparities in human papillomavirus types 16/18 in high-grade cervical lesions: Associations with race, ethnicity, and poverty. Cancer. 2013; 119(16):3052–3058. [DOI] [PubMed] [Google Scholar]
- 20.Montealegre JR, Peckham-Gregory EC, Marquez-Do D, et al. Racial/ethnic differences in HPV 16/18 genotypes and integration status among women with a history of cytological abnormalities. Gynecologic oncology. 2018; 148(2):357–362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ramos Rivera G, Khader SN, Lajara S, et al. The ATHENA HPV study underrepresents “other” high-risk HPV genotypes when compared with a diverse New York City population. Cytopathlogy. 2017; 28: 413–418. 10.1111/cyt.12440. [DOI] [PubMed] [Google Scholar]
- 22.Pinheiro M, Gage JC, Clifford GM, et al. Association of HPV35 with cervical carcinogenesis among women of African ancestry: Evidence of viral-host interaction with implications for disease intervention. International journal of cancer. 2020; 2677–2686. [DOI] [PMC free article] [PubMed]
- 23.Wagner S, Roberson D, Boland J, et al. Development of the TypeSeq Assay for Detection of 51 Human Papillomavirus Genotypes by Next-Generation Sequencing. J Clin Microbiol. 2019; 57(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Egemen D, Cheung LC, Chen X, et al. Risk Estimates Supporting the 2019 ASCCP Risk-Based Management Consensus Guidelines. Journal of lower genital tract disease. 2020; 24(2):132–1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Clarke MA, Gradissimo A, Schiffman M, et al. Human Papillomavirus DNA Methylation as a Biomarker for Cervical Precancer: Consistency across 12 Genotypes and Potential Impact on Management of HPV-Positive Women. Clin Cancer Res. 2018; 24(9):2194–2202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wentzensen N, Lahrmann B, Clarke MA, et al. Accuracy and Efficiency of Deep-Learning-Based Automation of Dual Stain Cytology in Cervical Cancer Screening. Journal of the National Cancer Institute. 2020. Volume 113, Issue 1, January 2021, Pages 72–79, 10.1093/jnci/djaa066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wentzensen N, Clarke MA, Bremer R, et al. Clinical Evaluation of Human Papillomavirus Screening With p16/Ki-67 Dual Stain Triage in a Large Organized Cervical Cancer Screening Program. JAMA internal medicine. 2019; 179(7):881–888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Clarke MA, Cheung LC, Castle PE, et al. Five-Year Risk of Cervical Precancer Following p16/Ki-67 Dual-Stain Triage of HPV-Positive Women. JAMA oncology. 2019; 5(2):181–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Centers for Disease Control and Prevention. TeenVaxView. Adolescent Human Papillomavirus (HPV) Vaccination Coverage Dashboard 2019. https://www.cdc.gov/vaccines/imz-managers/coverage/teenvaxview/data-reports/hpv/dashboard/2019.html.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Figure 1. The Distribution of Individuals Undergoing Cervical Cancer Screening in STRIDES by County in Mississippi. This figure depicts the number of individuals in STRIDES by county within MS. The map is color-coded according to population density including information from the 2010 U.S. Census on males and females of all ages living in the county. Lighter colors correspond to lower population density, whereas darker shading corresponds to higher population density. Counties with a red star are designated as Urban and counties without a red star are designated as rural, according to the USDA Office of Management and Budget https://www.ers.usda.gov/topics/rural-economypopulation/rural-classifications/. The hollow circle indicates the UMMC catchment area.
Supplemental Table 1. Population characteristics stratified by race* of individuals undergoing cervical cancer screening at MSDH and UMMC, December 23, 2017 – May 07, 2020