

Abstract
Background:
Depression symptoms are associated with the initiation of cigarette smoking and progression to regular use. Whether similar relationships exist between depression symptoms and adolescent e-cigarette progression has not been firmly established.
Methods:
This prospective longitudinal survey study measured the relationship between depression symptoms and e-cigarette use among 1822 adolescents from four public high schools outside of Philadelphia, PA. Adolescents completed in-classroom surveys at wave 1 (fall 2016, 9th grade) and 6-month intervals for the following 36 months (fall 2019, 12th grade). E-cigarette use, depression symptoms, and potential covariates were measured at each wave. A latent growth curve model was used to assess the longitudinal relationship between e-cigarette use and depression symptoms.
Results:
Baseline depressive symptoms had a significant effect on e-cigarette use trend (b=0.01, z=4.29, p < 0.0001) while holding other variables constant. A standard deviation increase in depressive symptoms at baseline was associated with a 0.25 standard deviation increase in the rate of e-cigarette progression across the following 36 months. By contrast, the path from baseline e-cigarette use to depressive symptoms trend was not significant (p = 0.74).
Conclusions:
The present study provides new evidence for the effects of depression symptoms on adolescent e-cigarette progression. Greater depressive symptoms at age 14 years old were associated with a faster rate of e-cigarette escalation. However, e-cigarette use was not related to the development of depression symptoms over time. It will be important to examine whether adolescents with elevated depression symptoms respond similarly to e-cigarette prevention campaigns as adolescents in general.
Keywords: adolescent, e-cigarette, depression, longitudinal studies
1. INTRODUCTION
Over the past decade, the percentage of adolescents reporting current (past 30-day) e-cigarette use increased from less than two percent to about 20%, making e-cigarettes the most commonly used tobacco product among adolescents (Gentzke et al., 2020; Substance Abuse and Mental Health Services Administration, 2020). E-cigarettes expose adolescents to nicotine, negatively impacting cognitive functions and increasing the likelihood of becoming nicotine dependent (DeBry & Tiffany, 2008; Demissie et al., 2017; Dwyer et al., 2009; Jacobsen et al., 2005; Musso et al., 2007; Vogel et al., 2020).
Depression among youth also poses a public health concern. The overwhelming majority (82%) of youth who received mental health care in 2018 and 2019 were treated for depressive symptoms (Merikangas et al., 2010; Mojtabai & Olfson, 2020). Rates of major depression doubled from 8% to 16% over the past decade, and almost one-third of high school students report depression symptoms (Centers for Disease Control and Prevention, 2020). Only 43% of youth with depression receive treatment for their symptoms (Substance Abuse and Mental Health Services Administration, 2020).
Depression often co-occurs with adolescent tobacco use. While the nature of the causal relationship remains inconclusive, studies have documented associations between adolescent depression, smoking initiation, and progression to regular use (Fluharty et al., 2017; Fuemmeler et al., 2013; Mathew et al., 2017; Shahwan et al., 2019). It is thought that nicotine may normalize mood by increasing positive affect while decreasing negative affect, especially in individuals already prone to depression (Audrain-McGovern et al., 2014). Whether similar relationships exist between depression symptoms and adolescent e-cigarette progression has not been firmly established. Most studies to date have been cross-sectional and or measured lifetime but not current e-cigarette use (Chadi et al., 2019; Lee & Lee, 2019; Leventhal et al., 2016).
A recent review of adolescent mental health and e-cigarette use included six studies involving adolescent depression symptoms. The findings regarding the association between e-cigarette use and depression were mixed (Becker et al., 2021). Four of the cross-sectional studies found that adolescents who reported either lifetime or past 30-day exclusive e-cigarette use reported higher rates of depressive symptoms than those who never used e-cigarettes (Chadi et al., 2019; Jee, 2016; Lee & Lee, 2019; Leventhal et al., 2016). In contrast, one cross-sectional study found that exclusive lifetime conventional cigarette use was significantly associated with depressive symptoms, but exclusive lifetime e-cigarette use was not (Chen et al., 2019). Of the six included studies, only one had a longitudinal design and revealed a bi-directional relationship between depression symptoms and e-cigarette use (Lechner et al., 2017). That is, higher depressive symptoms predicted an increased likelihood of e-cigarette initiation (ever use) 12 months later. Sustained e-cigarette use, defined as past 30-day use at both 6-month and 12-month follow-ups, was associated with a more rapid increase in depressive symptoms over the 12 months (Lechner et al., 2017). A more recent longitudinal study of adolescents found that higher depression symptoms were associated with a more rapid escalation in the number of days of e-cigarette use over 30 months, but not the onset of e-cigarette use (Audrain-McGovern et al., 2020). These studies collectively highlight the importance of longitudinal designs with longer follow-up periods and the value of investigating how changes in depression and e-cigarette use affect each other across time.
This prospective cohort survey study examined the longitudinal relationship between adolescent depression symptoms and e-cigarette use across three years and seven different time points. We hypothesized that depression symptoms would be associated with adolescent e-cigarette progression and that e-cigarette use would be related to changes in depression symptoms. The findings have the potential to identify youth at greater risk for e-cigarette progression and inform the content of e-cigarette prevention and intervention campaigns.
2. METHODS
2.1. Participants and Procedures
Participants were adolescents in the 9th grade taking part in a longitudinal cohort study of the relationship among combustible cigarette smoking, e-cigarette use, and other tobacco use. Participants were enrolled in four public high schools within a 65-mile radius outside of Philadelphia, PA. The schools were selected from four different districts and cities (three suburban and one rural) that varied in demographic features (race, ethnicity, annual household income). The selection yielded a sample that was demographically representative of adolescents nationwide. The cohort participants were drawn from 2198 students identified through class rosters at the start of 9th grade. Adolescents were ineligible to participate if they had a severe learning disability or did not speak fluent English. Based on the selection criteria, 2017 of 2198 (92%) students were eligible to participate.
Parents were mailed a study information letter (active information) with a telephone number to call to answer any questions and decline consent for their adolescent participation (passive consent). Of the 2017 eligible adolescents, 17 (1%) had a parent who actively declined their adolescent’s participation. Adolescents with parental consent were approached to provide their written assent for study participation. Adolescents who were absent on the assent/baseline survey days (n = 124, 6%) and adolescents who did not provide assent (n = 41, 2%) due to lack of interest were not enrolled in the cohort. Thus, 1835 of the 2000 adolescents with consent (92%) provided their assent to participate and completed a 40-minute paper and pencil survey. This baseline, or wave 1, survey was completed on-site during compulsory classes in the fall of 2016.
Adolescents completed six paper and pencil follow-up surveys at 6-month intervals with 92% completing a survey at wave 2 (N = 1687, spring 2017), 90% completing a survey at wave 3 (N = 1658, fall 2017), 89% completing a survey at wave 4 (N = 1643, spring 2018), 87% completing a survey at wave 5 (N = 1601, fall 2018), 84% completing a survey at wave 6 (N = 1538, spring 2019), and 83% completing a survey at wave 7 (N = 1530, fall 2019). Adolescents were assigned a unique ID at the baseline survey. A cover page with the adolescent’s name connected to their ID on the follow-up survey was removed at the time of survey receipt. The participants included in this study are adolescents who had complete data on the study variables at baseline (N = 1822). The Institutional Review Board of the University of Pennsylvania and the administration of each of the four high schools approved the study. Data analyses were conducted in April of 2021.
2.2. Measures
2.2.1. E-cigarette Use.
The survey included an introduction explaining e-cigarettes and the types of products or devices labeled as e-cigarettes. Images of different e-cigarette devices were provided to facilitate clarity (Audrain-McGovern et al., 2019; Conway et al., 2018). From baseline (wave 1) to wave 3, these images included e-cigarettes, e-hookah, vape pens, and mods. Images of USB-style pod vaporizers were added at wave 4 (early 2018). Excluding using an e-cigarette device for vaping marijuana, adolescents were asked: “Have you ever used an e-cigarette like the ones pictured above, even 1 or 2 times?” Adolescents who reported ever use of an e-cigarette were prompted to answer subsequent questions assessing lifetime frequency of e-cigarette use and time since last e-cigarette use. The following ordered categorical variable was created to define progression in e-cigarette use: 0 = never used; 1 = used, but not in the past 6 months; 2 = used in the past 6 months, but not in the past 30 days; and 3 = used in the past 30 days. Progression was captured by modeling the within-subject rate of movement across the ordered categories at subsequent timepoints. As is standard, current use was defined as using an e-cigarette on at least one day in the past 30 days (Audrain-McGovern et al., 2018; Wang et al., 2019). E-cigarette use was measured in all seven waves.
2.2.2. Depression Symptoms.
The Centers for Epidemiology Studies of Depression (CES-D) assessed depression symptoms over the past week (Radloff, 1991). The 20-item Likert style scale (0 = rarely or none of the time to 3 = most of the time) is frequently used to assess depressive symptoms among adolescents in epidemiological studies (Audrain-McGovern et al., 2009; Lechner et al., 2017). The responses were summated after reverse coding four items. The scores could range from 0-60. Cronbach’s coefficient alpha for this scale was .84. Depression was measured in all seven waves.
2.2.3. Covariates.
Demographic characteristics such as sex, race, and ethnicity were assessed at baseline using self-report items. These demographic variables were included in the model to characterize the sample. All covariates were measured at baseline.
2.2.4. Peer and household e-cigarette use.
Peer e-cigarette use was measured by asking adolescents whether their best friend, four other best male friends, and four other best female friends use e-cigarettes (Coleman et al., 2006; Etim et al., 2020). If an adolescent responded “yes” to either of these questions, they were prompted to answer how many. Peer e-cigarette use was summarized as no peers versus at least one peer used e-cigarettes. Household e-cigarette use was measured with the question, “Does anyone in your house use e-cigarettes?” (Etim et al., 2020). Household e-cigarette use was summarized as no household e-cigarette use versus at least one household member.
2.2.5. Perceived Benefits.
The perceived benefits of using e-cigarettes were measured with 12 items using a Likert scale (0 = strongly disagree to 3 = strongly agree). Items assessed available flavors, smell, affordability, impact on non-tobacco users, substitution in smoke-free situations, and similarity to smoking (Bernat et al., 2018; Gibson et al., 2018; Moustafa et al., 2021; Vogel et al., 2019). Scores could range from 0 to 36, with higher scores indicating greater perceived benefits. Cronbach’s coefficient alpha for this scale was .89.
2.2.6. Positive Expectations.
Positive expectations of e-cigarette use were measured with a 9-item Likert-style scale (Gibson et al., 2018; Harrell et al., 2015; Moustafa et al., 2021; Wills et al., 2015). The items included, “I think vaping e-cigarettes would…give me something to do when I’m bored, …help me deal with problems or stress, …feel more comfortable at parties.” Response options ranged from 0 = strongly disagree to 3 = strongly agree. Scores could range from 0 to 27, with higher scores indicating more positive expectations. Cronbach’s coefficient alpha for this scale was .83.
2.2.7. Combustible Cigarette Smoking.
Combustible cigarette smoking at baseline was measured by asking adolescents, “Have you ever tried smoking a cigarette, even a few puffs?” Adolescents who reported ever smoking a cigarette were prompted to answer subsequent questions assessing lifetime frequency of cigarette smoking and time since last cigarette. The following ordered categorical variable was created to define cigarette smoking: 0=never smoked; 1 = smoked, but not in the past 6 months; 2 = smoked in the past 6 months; and 3 = smoked a cigarette in the past 30 days.
2.2.8. Alcohol and Marijuana Use.
Marijuana use and alcohol use were assessed by asking adolescents if they had used these substances in the past six months (Audrain-McGovern et al., 2018).
2.3. Statistical Analysis
Data were analyzed using latent growth curve modeling (LGCM) to assess the longitudinal relation between e-cigarette use and depressive symptoms across seven waves of data, each six months apart. LGCM is a multivariate structural equation modeling method that models repeated measures of a variable on latent variables (factors) representing baseline (level or intercept) and rate of change (trend or slope) (Duncan et al., 2013; Loehlin & Beaujean, 2016). The product is an average trajectory across all participants on the variable of interest. The present study conducted an associated-processes LGCM to model depressive symptoms and e-cigarette use trajectories and how each affects the other. Thus, there are two LGCMs, one each for repeated measures of depressive symptoms and e-cigarette use.
The LGCM was conducted in two phases. First, a measurement model was examined. This model involved assessing the relationship between the two associated processes without any predictor variables, and all paths among the factors were allowed to correlate freely. Second, predictor variables and covariates were added (adjusted model). The covariates included sex, race (two dummy variables comparing Black race and other race to White race), ethnicity (Hispanic versus not-Hispanic ethnicity), household e-cigarette use, peer e-cigarette use, past six-month alcohol and marijuana use (two binary variables, yes/no), cigarette smoking, positive expectations of e-cigarette use, and the perceived benefits of e-cigarette use.
Model fit in both the crude and adjusted models was evaluated via chi-square, Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), and Weighted Root Mean Residual (WRMR). Heuristics for ideal fit include a non-significant chi-square statistic, CFI ≥ 0.95, RMSEA < 0.08, and WRMR < 0.90 (DiStefano et al., 2018; Schreiber et al., 2006; Sivo et al., 2006). Mplus 8.3 software was used to complete the LGCM and test for mediation (Muthén & Muthén, 2017).
3. RESULTS
Descriptive statistics appear in Table 1. Half of the sample was female, 27% minority, and 20.8% Hispanic ethnicity. The proportion of participants ever using e-cigarettes increased from 16% to 21% from wave 1 to wave 7. Past 30-day e-cigarette use increased from 5.8% at baseline to 11.3% at wave 7. Depressive symptoms remained relatively constant between wave 1 (Mean = 18.30, SD = 9.42) and wave 7 (Mean = 18.39, SD = 10.49).
Table 1.
Descriptive statistics for the sample at baseline (n = 1822).
| Categorical Variables Level N % | |||
|---|---|---|---|
| Sex | Male | 908 | 49.8 |
| Female | 914 | 50.2 | |
| Race | Black | 260 | 14.3 |
| White | 232 | 12.7 | |
| Other | 1330 | 73 | |
| Ethnicity | Hispanic | 379 | 20.8 |
| Non-Hispanic | 1443 | 79.2 | |
| Household e-cigarette use | No one | 1591 | 87.3 |
| At least one person | 231 | 12.7 | |
| Marijuana use | Did not use in the past six months | 202 | 11.1 |
| Used in the past six months | 1620 | 88.9 | |
| Alcohol use | Did not use in the past six months | 1518 | 83.3 |
| Used in the past six months | 304 | 16.7 | |
| Peer e-cigarette use | No peers | 1468 | 80.6 |
| One or more | 354 | 9.4 | |
| Cigarette smoking | Never smoked | 1698 | 93.2 |
| Smoked, but not in the past six months | 32 | 1.8 | |
| Smoked in the past six months | 52 | 2.9 | |
| Smoked in the past 30 days | 40 | 2.2 | |
| E-cigarette use | Never | 1530 | 83.9 |
| Used but not in the past six months | 114 | 6.3 | |
| Used but not within the past 30 days | 75 | 4.1 | |
| Used within the past 30 days | 103 | 5.7 | |
| Mean SD | |||
| Perceived benefits of e-cigarette use | 12.80 | 5.83 | |
| Positive expectations of e-cigarette use | 6.57 | 4.40 | |
| Depressive symptoms | 18.30 | 9.42 | |
3.1. Multivariate model
The measurement model with the two associated processes and free correlations among the latent variables fit the data well, x297 = 390.64, p < 0.0001; CFI = 0.98; RMSEA = 0.04, 90% CI = 0.04, 0.05; SRMR = 0.04. The adjusted model with non-standardized path coefficients, standard errors, and z-statistics are presented for all model paths in Table 2. A graphic presentation of the results is presented in Figure 1, with standardized path coefficients for all effects. Adding the predictor variables to the model and paths from the baseline level of each process to the linear trend of the other process, the model fit the data well, x2210 = 640.31, p < 0.0001; CFI = 0.96; RMSEA = 0.03, 90% CI = 0.03, 0.04; SRMR = 0.04. The correlation between the two trend factors was significant (r = 0.08, z = 2.92, p = 0.003).
Table 2.
Non-standardized results of the associated processes LGCM of depression symptoms and e-cigarette use.
| Depressive symptoms | ||||||||
|---|---|---|---|---|---|---|---|---|
| Baseline level | Linear trend | |||||||
| b | SE | z-value | p-value | b | SE | z-value | p-value | |
| Baseline e-cigarette use | −0.03 | 0.10 | −0.35 | 0.73 | ||||
| Sex | 5.35 | 0.39 | 13.85 | <0.0001 | 0.05 | 0.09 | 0.51 | 0.61 |
| Black race | −0.03 | 0.51 | −0.05 | 0.96 | −0.21 | 0.11 | −1.77 | 0.08 |
| Other race | −0.68 | 0.62 | −1.10 | 0.27 | 0.10 | 0.14 | 0.67 | 0.51 |
| Ethnicity | −0.40 | 0.46 | −0.81 | 0.42 | −0.07 | 0.11 | −0.71 | 0.48 |
| Peers e-cigarette use | 0.19 | 0.10 | 1.84 | 0.07 | −0.03 | 0.03 | −0.85 | 0.40 |
| Household e-cigarette use | 1.23 | 0.55 | 2.24 | 0.03 | −0.01 | 0.14 | −0.02 | 0.98 |
| Marijuana use | −0.63 | 0.64 | −0.98 | 0.33 | 0.22 | 0.18 | 1.22 | 0.22 |
| Alcohol use | 0.80 | 0.56 | 1.41 | 0.16 | 0.24 | 0.15 | 1.62 | 0.11 |
| Positive expectations | −0.01 | 0.05 | −0.71 | 0.86 | −0.03 | 0.02 | −1.54 | 0.12 |
| Cigarette smoking | 1.68 | 0.29 | 5.92 | <0.0001 | −0.24 | 0.08 | −2.97 | 0.003 |
| Perceived benefits | 0.14 | 0.04 | 4.01 | <0.0001 | −0.03 | 0.01 | −2.86 | 0.004 |
| E-cigarette use | ||||||||
| Baseline level | Linear trend | |||||||
| b | SE | z-value | p-value | b | SE | z-value | p-value | |
| Baseline depression | 0.01 | 0.00 | 4.26 | <0.0001 | ||||
| Sex | −0.04 | 0.08 | −0.56 | 0.57 | 0.00 | 0.03 | 0.04 | 0.97 |
| Black race | −0.05 | 0.11 | −0.45 | 0.66 | −0.14 | 0.05 | −2.87 | 0.004 |
| Other race | −0.05 | 0.13 | −0.36 | 0.72 | −0.09 | 0.05 | −1.76 | 0.08 |
| Ethnicity | −0.24 | 0.09 | −2.58 | 0.01 | 0.08 | 0.04 | 2.28 | 0.02 |
| Peer e-cigarette use | 0.17 | 0.02 | 9.09 | <0.0001 | −0.02 | 0.01 | −2.49 | 0.01 |
| Household e-cigarette use | 0.19 | 0.10 | 1.90 | 0.06 | −0.07 | 0.04 | −1.69 | 0.09 |
| Marijuana use | 0.54 | 0.10 | 5.30 | <0.0001 | 0.05 | 0.05 | 0.97 | 0.33 |
| Alcohol use | 0.23 | 0.09 | 2.46 | 0.02 | 0.13 | 0.04 | 2.89 | 0.004 |
| Positive expectations | 0.12 | 0.01 | 9.78 | <0.0001 | 0.01 | 0.01 | −1.89 | 0.06 |
| Cigarette smoking | 0.31 | 0.05 | 5.77 | <0.0001 | −0.07 | 0.02 | −2.78 | 0.005 |
| Perceived benefits | 0.10 | 0.01 | 1.14 | 0.25 | 0.01 | 0.01 | 0.45 | 0.66 |
Figure 1.
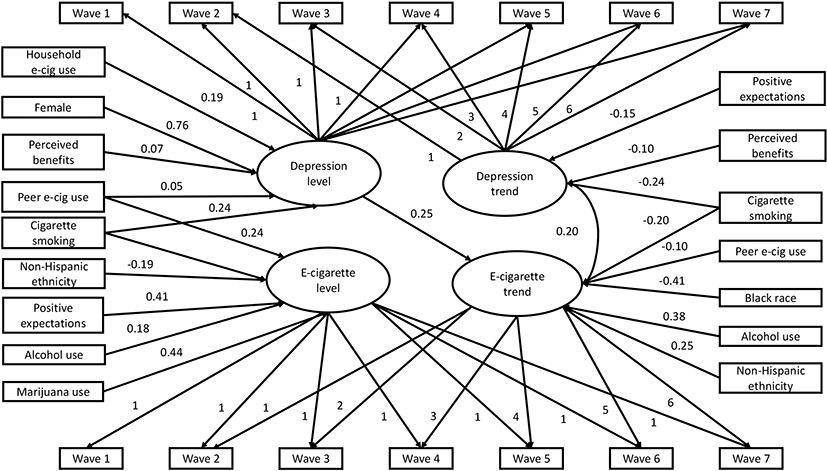
Associated processes LGCM with standardized path coefficients.
Baseline depressive symptoms had a significant effect on e-cigarette use trend (b=0.01, z=4.29, p < 0.0001). A standard deviation increase in depressive symptoms at baseline was associated with a 0.25 standard deviation increase in the rate of e-cigarette progression from baseline, holding all other variables constant. In contrast, the path from baseline e-cigarette use to depressive symptoms trend was not significant (p = 0.74).
Several covariates variables were related to e-cigarette use. Non-Hispanic ethnicity was negatively related to baseline e-cigarette use (b = −0.24, z = −2.67, p = 0.01). Peer e-cigarette use (b = 0.17, z = 9.19, p < 0.0001), past six-month alcohol use (b = 0.22, z = 2.39, p = 0.02) past six- month marijuana use (b = 0.55, z = 5.40, p < 0.0001), positive e-cigarette expectations (b = 0.12, z = 10.16, p < 0.0001), and combustible cigarette smoking (b = 0.31, z = 5.82, p<0.0001) were all associated with greater e-cigarette use at baseline. Black race (versus White race) (b = −0.14, z = −2.89, p = 0.004), peer e-cigarette use (b = −0.02, z = −2.45, p = 0.01), and combustible cigarette smoking (b = −0.07, z = −2.81, p = 0.005) were all associated with a decreased rate of e-cigarette progression across the following 36 months. By contrast, non-Hispanic ethnicity (b = 0.09, z = 2.30, p = 0.02) and past six-month alcohol use (b = 0.13, z = 2.93, p = 0.003) were associated with an increased rate of e-cigarette progression across follow-up.
Several covariates were related to depressive symptoms at baseline and predicted the rate of change in depressive symptoms across time. Female gender (b = 5.37, z = 13.89, p < 0.0001), peer e-cigarette use (b = 0.22, z = 2.09, p = 0.04), household e-cigarette use (b = 1.33, z = 2.41, p = 0.02), and combustible cigarette smoking (b = 1.68, z = 5.89, p < 0.0001) were associated with greater depressive symptoms at baseline. Positive e-cigarette expectations (b = −0.03, z = −2.00, p < 0.05), combustible cigarette smoking (b = −0.24, z = −2.97, p = 0.003), and perceived benefits of e-cigarette use (b = −0.13, z = −2.13, p = 0.03) were associated with decreased rate of change in depressive symptoms across time.
4. DISCUSSION
The present study provides new evidence for the effects of depression symptoms on e-cigarette progression among adolescents. Greater depressive symptoms at age 14 were associated with a faster rate of e-cigarette progression across the following 36 months. E-cigarette use was not related to the development of depression symptoms over time. These findings suggest that elevated depression symptoms enhance adolescent vulnerability to e-cigarette use. Screening for depression will aid in the identification of adolescents at risk for e-cigarette progression.
The finding that depression symptoms foster rapid progression raises concerns, as faster progression has been associated with sustained e-cigarette use and greater nicotine dependence among adolescents (Vogel et al., 2019, 2020). Adolescents with elevated depression symptoms may find the nicotine in e-cigarettes more rewarding than adolescents with fewer symptoms. These relationships have been identified in epidemiological studies of adolescent and young adult cigarette smoking and depression (Audrain- McGovern et al., 2009, 2011) and human laboratory studies of depressed and nondepressed adult smokers (Audrain-McGovern et al., 2014). Flavoring in e-cigarettes has been shown to enhance nicotine's rewarding and reinforcing effects (Audrain-McGovern et al., 2016). Although speculative, nicotine and flavoring may work together to promote swift progression among youth with higher depression symptoms. Adult smokers with mental health conditions, including depression, tend to value e-cigarette flavors more than those with no mental health conditions (Spears et al., 2018).
Research suggests that adolescents who use e-cigarettes have a lower risk profile than adolescents who smoke combustible cigarettes or adolescents who use both (Wills et al., 2015). While this appears to be the case, even for depression symptoms (Lee & Lee, 2019; Leventhal et al., 2016), depression remains a risk factor for progression in e-cigarette use. Adolescents with elevated depression at baseline tended to be female, have peers who use e-cigarettes, have a household member who uses e-cigarettes, and smoke combustible cigarettes. These relationships highlight potential variables to target to prevent depression as well as e-cigarette use.
In contrast to a previous longitudinal study of depression and e-cigarette use, we did not find evidence for a bi-directional effect (Lechner et al., 2017). That is, e-cigarette use was not associated with an escalation in depression symptoms. This finding may be due to differences in the length of follow-up, with a potential bidirectional relationship becoming less significant over a longer follow-up period. It is also possible that e-cigarette use maintains or stabilizes depression symptoms over time rather than exacerbating symptoms. As novel e-cigarettes continue to emerge with various characteristics (e.g., types and levels of nicotine, flavoring), these relationships warrant further study.
This study has several strengths as the first multi-year study to assess the longitudinal relationship between adolescent depression and e-cigarette progression. The sample was measured every six months across 36 months. Depression and e-cigarette use were both measured seven times to examine relationships across time. The sample was large, relatively diverse, and participation and retention rates were excellent. Also, we controlled for several variables that could confound the investigation of the relationship between depression symptoms and e-cigarette progression, including peer e-cigarette use, combustible cigarette use, and household e-cigarette use.
One potential limitation of the study is that all participants were recruited from one geographic area. Although the findings may not generalize across the country, the sample demographics and the prevalence of nicotine vaping are consistent with national surveys. At baseline, the prevalence of lifetime (ever) e-cigarette use (16%) and 30-day e-cigarette use (6%) were comparable to the 2016 prevalence rates reported by Monitoring the Future (average for 8th and 10th-grade prevalence rates: ever use 23% and 30-day use 8.5%) (R. A. Miech et al., 2017). In 2019, our prevalence rates for ever use (21%) and 30-day use (11.3%) were lower than those reported by Monitoring the Future (41% and 22%, respectively) (R. Miech et al., 2021), but comparable to YRBS regional/local prevalence rates as well as the Truth Longitudinal Cohort Study (23% to 41% and 11%) (Centers for Disease Control and Prevention (CDC, 2019; Vallone et al., 2020).
Another potential limitation is that adolescents reported on psychological and behavioral variables that spanned various periods (e.g., today, past week, past 30 days, past six months), and the impact of recall biases is uncertain. In addition, as is typical of using the CES-D in epidemiological studies, depression symptoms were assessed for the week prior to the survey, which may not be representative of the past six months. This study did not evaluate the type of e-cigarette device used, the associated nicotine type, and the intensity of e-cigarette use. These variables may offer a refined understanding of the association between depression and e-cigarette use and should be examined in future research.
While depression symptoms were measured, a diagnosis of major depression was not determined through a structured clinical interview. However, these findings suggest that depression symptoms may be sufficient to increase vulnerability to e-cigarette uptake and that these symptoms can be identified via a short self-report instrument. Additionally, parent depression may be significant to the relationship between e-cigarette use and depressive symptoms, but it was not measured. Previous research found that depression symptoms were positively associated with current e-cigarette use only among adolescents of a parent who suffered from depression and not among adolescents whose parents did not have depression (Cho, 2019). It is important to note that the depression symptoms remained stable over time. However, there may be distinct subgroups of adolescents who have different longitudinal patterns of depression (e.g., increasing, decreasing, stable chronic) across time. These subgroups may vary in their likelihood of e-cigarette use. Future research should evaluate these relationships in addition to potential mechanisms that may explain the relationship between depression symptoms and e-cigarette uptake.
5. CONCLUSIONS
This prospective cohort study demonstrates that adolescents with elevated depression symptoms at age 14 have a faster rate of e-cigarette progression. Further research is needed to identify mechanisms that account for this relationship, further informing public health campaigns and e-cigarette regulatory actions. It will be important to examine whether adolescents with elevated depression symptoms respond similarly to e-cigarette prevention campaigns as adolescents in general. If not, the next step may be to target adolescents with elevated depression symptoms in e-cigarette prevention campaigns, perhaps similar to the campaigns that targeted novelty-seeking to prevent adolescent tobacco use (Crosby et al., 2019). Such efforts may be informed by smoking cessation interventions that have targeted depression symptoms (Hoeppner et al., 2019; Kahler et al., 2015; MacPherson et al., 2010).
Highlights:
Depression symptoms predicted more rapid e-cigarette progression in adolescents.
E-cigarette use was not associated with an escalation in depression symptoms.
Depression screening may aid in identifying those at risk of e-cigarette progression.
These findings from adolescents in PA should be replicated in a national sample.
Acknowledgements
Funding: This study was supported by National Cancer Institute RO1 CA202262 (JAM).
Role of Funding Source:
The funding agency had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Abbreviations:
- LGCM
latent growth curve modeling
- CFI
Comparative Fit Index
- RMSEA
Root Mean Square Error of Approximation
- WRMR
Weighted Root Mean Residual
- SD
Standard Deviation
Footnotes
Conflicts of Interest: The authors report no potential conflicts of interest.
Access to Data and Data Analysis: The corresponding author (JAM) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- Audrain-McGovern J, Rodriguez D, & Kassel JD (2009). Adolescent smoking and depression: evidence for self-medication and peer smoking mediation. Addiction, 104(10), 1743–1756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audrain-McGovern J, Rodriguez D, Pianin S, & Alexander E (2019). Initial e-cigarette flavoring and nicotine exposure and e-cigarette uptake among adolescents. Drug and Alcohol Dependence, 202, 149–155. 10.1016/j.drugalcdep.2019.04.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audrain-McGovern J, Rodriguez D, Rodgers K, & Cuevas J (2011). Declining alternative reinforcers link depression to young adult smoking. Addiction, 106(1), 178–187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audrain-McGovern J, Rodriguez D, Testa S, Alexander E, & Pianin S (2020). Adolescent e-cigarette onset and escalation: associations with internalizing and externalizing symptoms. Journal of Adolescent Health. 10.1016/j.jadohealth.2020.09.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audrain-McGovern J, Stone MD, Barrington-Trimis J, Unger JB, & Leventhal AM (2018). Adolescent e-cigarette, hookah, and conventional cigarette use and subsequent marijuana use. Pediatrics, 142(3), e20173616. 10.1542/peds.2017-3616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audrain-McGovern J, Strasser AA, & Wileyto EP (2016). The impact of flavoring on the rewarding and reinforcing value of e-cigarettes with nicotine among young adult smokers. Drug and Alcohol Dependence, 166, 263–267. PubMed. 10.1016/j.drugalcdep.2016.06.030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audrain-McGovern J, Wileyto EP, Ashare R, Cuevas J, & Strasser AA (2014). Reward and affective regulation in depression-prone smokers. Biological Psychiatry, 76(9), 689–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Becker TD, Arnold MK, Ro V, Martin L, & Rice TR (2021). Systematic review of electronic cigarette use (vaping) and mental health comorbidity among adolescents and young adults. Nicotine & Tobacco Research, 23(3), 415–425. 10.1093/ntr/ntaa171 [DOI] [PubMed] [Google Scholar]
- Bernat D, Gasquet N, Wilson KO, Porter L, & Choi K (2018). Electronic cigarette harm and benefit perceptions and use among youth. American Journal of Preventive Medicine, 55(3), 361–367. 10.1016/j.amepre.2018.04.043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2020). Youth risk behavior survey data summary & trends report 2007–2017.
- Centers for Disease Control and Prevention (CDC. (2019). Youth risk behavior survey (YRBS).
- Chadi N, Li G, Cerda N, & Weitzman ER (2019). Depressive symptoms and suicidality in adolescents using e-cigarettes and marijuana: a secondary data analysis from the Youth Risk Behavior Survey. Journal of Addiction Medicine, 13(5). [DOI] [PubMed] [Google Scholar]
- Chen Y-L, Wu S-C, Chen Y-T, Hsiao P-C, Yu Y-H, Ting T-T, Chen C-Y, Tu Y-K, Huang J-H, Yang H-J, Li C-Y, Strong C, Yen C-F, Yen C-F, & Chen WJ (2019). E-cigarette use in a country with prevalent tobacco smoking: a population-based study in Taiwan. Journal of Epidemiology, 29(4), 155–163. PubMed. 10.2188/jea.JE20170300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cho B-Y (2019). Parent’s depression as a moderator of the association between offspring’s depressive symptoms and use of combustible cigarettes and electronic vapor products. The Journal of Behavioral Health Services & Research, 46(4), 648–655. PubMed. 10.1007/s11414-019-09655-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coleman M, Donaldson CD, Crano WD, Pike JR, & Stacy AW (2006). Associations between family and peer e-cigarette use with adolescent tobacco and marijuana usage: a longitudinal path analytic approach. Nicotine & Tobacco Research. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conway KP, Green VR, Kasza KA, Silveira ML, Borek N, Kimmel HL, Sargent JD, Stanton CA, Lambert E, Hilmi N, Reissig CJ, Jackson KJ, Tanski SE, Maklan D, Hyland AJ, & Compton WM (2018). Co-occurrence of tobacco product use, substance use, and mental health problems among youth: Findings from wave 1 (2013–2014) of the population assessment of tobacco and health (PATH) study. Addictive Behaviors, 76, 208–217. 10.1016/j.addbeh.2017.08.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crosby K, Santiago S, Talbert EC, Roditis ML, & Resch G (2019). Bringing “the real cost” to life through breakthrough, evidence-based advertising. American Journal of Preventive Medicine, 56(2), S16–S23. [DOI] [PubMed] [Google Scholar]
- DeBry SC, & Tiffany ST (2008). Tobacco-induced neurotoxicity of adolescent cognitive development (TINACD): A proposed model for the development of impulsivity in nicotine dependence. Nicotines & Tobacco Research, 10(1), 11–25. [DOI] [PubMed] [Google Scholar]
- Demissie Z, Jones SE, Clayton HB, & King BA (2017). Adolescent risk behaviors and use of electronic vapor products and cigarettes. Pediatrics, 139(2). [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiStefano C, Liu J, Jiang N, & Shi D (2018). Examination of the weighted root mean square residual: Evidence for trustworthiness? Structural Equation Modeling: A Multidisciplinary Journal, 25(3), 453–466. [Google Scholar]
- Duncan TE, Duncan SC, & Strycker LA (2013). An introduction to latent variable growth curve modeling: Concepts, issues, and application. Routledge. [Google Scholar]
- Dwyer JB, McQuown SC, & Leslie FM (2009). The dynamic effects of nicotine on the developing brain. Pharmacology & Therapeutics, 122(2), 125–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Etim N, Pike J, & Xie B (2020). Age-varying associations between e-cigarette use and peer use, household use, and exposure to e-cigarette commercials among alternative high school students in Southern California. Tobacco Induced Diseases, 18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fluharty M, Taylor AE, Grabski M, & Munafò MR (2017). The association of cigarette smoking with depression and anxiety: A Systematic Review. Nicotine & Tobacco Research : Official Journal of the Society for Research on Nicotine and Tobacco, 19(1), 3–13. PubMed. 10.1093/ntr/ntw140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuemmeler B, Lee C-T, Ranby KW, Clark T, McClernon FJ, Yang C, & Kollins SH (2013). Individual- and community-level correlates of cigarette-smoking trajectories from age 13 to 32 in a U.S. population-based sample. Drug and Alcohol Dependence, 132(1–2), 301–308. PubMed. 10.1016/j.drugalcdep.2013.02.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gentzke AS, Wang TW, Jamal A, Park-Lee E, Ren C, Cullen KA, & Neff L (2020). Tobacco product use among middle and high school students—United States, 2020. MMWR. Morbidity and Mortality Weekly Report, 69(50), 1881–1888. PubMed. 10.15585/mmwr.mm6950a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson LA, Creamer MR, Breland AB, Giachello AL, Kaufman A, Kong G, Pechacek TF, Pepper JK, Soule EK, & Halpern-Felsher B (2018). Measuring perceptions related to e-cigarettes: Important principles and next steps to enhance study validity. Addictive Behaviors, 79, 219–225. 10.1016/j.addbeh.2017.11.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrell PT, Marquinez NS, Correa JB, Meltzer LR, Unrod M, Sutton SK, Simmons VN, & Brandon TH (2015). Expectancies for cigarettes, e-cigarettes, and nicotine replacement therapies among e-cigarette users (aka vapers). Nicotine & Tobacco Research, 17(2), 193–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoeppner BB, Hoeppner SS, Carlon HA, Perez GK, Helmuth E, Kahler CW, & Kelly JF (2019). Leveraging positive psychology to support smoking cessation in nondaily smokers using a smartphone app: feasibility and acceptability study. JMIR MHealth and UHealth, 7(7), e13436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobsen LK, Krystal JH, Mencl WE, Westerveld M, Frost SJ, & Pugh KR (2005). Effects of smoking and smoking abstinence on cognition in adolescent tobacco smokers. Biological Psychiatry, 57(1), 56–66. [DOI] [PubMed] [Google Scholar]
- Jee Y-J (2016). Comparison of emotional and psychological indicators according to the presence or absence of the use of electronic cigarettes among Korea youth smokers. International Information Institute (Tokyo). Information, 19(10A), 4525. [Google Scholar]
- Kahler CW, Spillane NS, Day AM, Cioe PA, Parks A, Leventhal AM, & Brown RA (2015). Positive psychotherapy for smoking cessation: A pilot randomized controlled trial. Nicotine & Tobacco Research, 17(11), 1385–1392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lechner WV, Janssen T, Kahler CW, Audrain-McGovern J, & Leventhal AM (2017). Bi-directional associations of electronic and combustible cigarette use onset patterns with depressive symptoms in adolescents. Preventive Medicine, 96, 73–78. PubMed. 10.1016/j.ypmed.2016.12.034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee Y, & Lee K-S (2019). Association of depression and suicidality with electronic and conventional cigarette use in South Korean adolescents. Substance Use & Misuse, 54(6), 934–943. 10.1080/10826084.2018.1552301 [DOI] [PubMed] [Google Scholar]
- Leventhal AM, Strong DR, Sussman S, Kirkpatrick MG, Unger JB, Barrington-Trimis JL, & Audrain-McGovern J (2016). Psychiatric comorbidity in adolescent electronic and conventional cigarette use. Journal of Psychiatric Research, 73, 71–78. PubMed. 10.1016/j.jpsychires.2015.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loehlin JC, & Beaujean AA (2016). Latent variable models: An introduction to factor, path, and structural equation analysis. Taylor & Francis. [Google Scholar]
- MacPherson L, Tull MT, Matusiewicz AK, Rodman S, Strong DR, Kahler CW, Hopko DR, Zvolensky MJ, Brown RA, & Lejuez CW (2010). Randomized controlled trial of behavioral activation smoking cessation treatment for smokers with elevated depressive symptoms. Journal of Consulting and Clinical Psychology, 78(1), 55–61. PubMed. 10.1037/a0017939 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mathew AR, Hogarth L, Leventhal AM, Cook JW, & Hitsman B (2017). Cigarette smoking and depression comorbidity: systematic review and proposed theoretical model. Addiction (Abingdon, England), 112(3), 401–412. PubMed. 10.1111/add.13604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, & Patrick ME (2017). Monitoring the Future national survey results on drug use, 1975–2016: Volume I, secondary school students. [Google Scholar]
- Miech R, Leventhal A, Johnston L, O’Malley PM, Patrick ME, & Barrington-Trimis J (2021). Trends in use and perceptions of nicotine vaping among US youth from 2017 to 2020. JAMA Pediatrics, 175(2), 185–190. 10.1001/jamapediatrics.2020.5667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mojtabai R, & Olfson M (2020). National trends in mental health care for US adolescents. JAMA Psychiatry, 77(7), 703–714. 10.1001/jamapsychiatry.2020.0279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moustafa AF, Rodriguez D, Mazur A, & Audrain-McGovern J (2021). Adolescent perceptions of e-cigarette use and vaping behavior before and after the EVALI outbreak. Preventive Medicine, 145, 106419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Musso F, Bettermann F, Vucurevic G, Stoeter P, Konrad A, & Winterer G (2007). Smoking impacts on prefrontal attentional network function in young adult brains. Psychopharmacology, 191(1), 159–169. [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén B (2017). Mplus user’s guide: Statistical analysis with latent variables, user’s guide. Muthén & Muthén. [Google Scholar]
- Radloff LS (1991). The use of the Center for Epidemiologic Studies Depression Scale in adolescents and young adults. Journal of Youth and Adolescence, 20(2), 149–166. [DOI] [PubMed] [Google Scholar]
- Schreiber JB, Nora A, Stage FK, Barlow EA, & King J (2006). Reporting structural equation modeling and confirmatory factor analysis results: A review. The Journal of Educational Research, 99(6), 323–338. [Google Scholar]
- Shahwan S, Abdin E, Shafie S, Chang S, Sambasivam R, Zhang Y, Vaingankar JA, Teo YY, Heng D, Chong SA, & Subramaniam M (2019). Prevalence and correlates of smoking and nicotine dependence: Results of a nationwide cross-sectional survey among Singapore residents. BMJ Open, 9(10), e032198–e032198. PubMed. 10.1136/bmjopen-2019-032198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sivo SA, Fan X, Witta EL, & Willse JT (2006). The search for" optimal" cutoff properties: Fit index criteria in structural equation modeling. The Journal of Experimental Education, 74(3), 267–288. [Google Scholar]
- Spears CA, Jones DM, Weaver SR, Pechacek TF, & Eriksen MP (2018). Motives and perceptions regarding electronic nicotine delivery systems (ENDS) use among adults with mental health conditions. Addictive Behaviors, 80, 102–109. PubMed. 10.1016/j.addbeh.2018.01.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration. (2020). Key substance use and mental health indicators in the United States: Results from the 2019 National Survey on Drug Use and Health (HHS Publication No. PEP20-07-01-001, NSDUH Series H-55).
- Vallone DM, Cuccia AF, Briggs J, Xiao H, Schillo BA, & Hair EC (2020). Electronic cigarette and JUUL use among adolescents and young adults. JAMA Pediatrics, 174(3), 277–286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vogel EA, Cho J, McConnell RS, Barrington-Trimis JL, & Leventhal AM (2020). Prevalence of electronic cigarette dependence among youth and its association with future use. JAMA Network Open, 3(2), e1921513–e1921513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vogel EA, Prochaska JJ, Ramo DE, Andres J, & Rubinstein ML (2019). Adolescents’ e-cigarette use: Increases in frequency, dependence, and nicotine exposure over 12 months. Journal of Adolescent Health, 64(6), 770–775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang TW, Gentzke AS, Creamer MR, Cullen KA, Holder-Hayes E, Sawdey MD, Anic GM, Portnoy DB, Hu S, Homa DM, Jamal A, & Neff LJ (2019). Tobacco product use and associated factors among middle and high school students—United States, 2019. Morbidity and Mortality Weekly Report. Surveillance Summaries (Washington, D.C. : 2002), 68(12), 1–22. 10.15585/mmwr.ss6812a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wills TA, Knight R, Williams RJ, Pagano I, & Sargent JD (2015). Risk factors for exclusive e-cigarette use and dual e-cigarette use and tobacco use in adolescents. Pediatrics, 135(1), e43–e51. 10.1542/peds.2014-0760 [DOI] [PMC free article] [PubMed] [Google Scholar]