

Abstract
Although drug use is considered a risk factor for child maltreatment, very little work has examined how the drug environment may affect physical abuse and neglect by parents. Utilizing information from a telephone survey with 2,597 respondents from 43 cities with valid police data on narcotics incidents, we analyzed the relationship between drug use, drug availability and child maltreatment using multilevel models. City-level rates of drug abuse and dependence were related to more frequent physical abuse. Parents who use drugs in areas with greater availability of drugs reported more physical abuse and physical neglect. Emotional support was protective of all types of maltreatment. While most child welfare interventions focus on reducing parental drug use in order to reduce child abuse, these findings suggest environmental prevention or neighborhood strengthening approaches designed to reduce the supply of illicit drugs may also reduce child abuse through multiple mechanisms.
Drug use, particularly if it rises to the level of drug abuse or dependence, can interfere with positive parenting (Kepple, 2017). However, the timeline for intervention and treatment approaches designed to reduce drug misuse are often at odds with those timelines required for parents involved with the child welfare system (Testa & Smith, 2009). Interventions that seek to reduce the supply of drugs may not only reduce drug use, but also reduce abusive and neglectful parenting (Freisthler, Needell & Gruenewald, 2005). This premise assumes that drug market forces exert significant and measurable impacts on parenting.
Theoretical support for this can be found in the work of Eck (1995). Eck (1995) hypothesized that drug markets operate through two primary structures: social networks and routine activities. A social network drug market is one that is primarily invisible and where contacts for drug sales are made through friends and friends of friends. This helps to ensure that the drug seller maximizes control of the market and minimizes detection by law enforcement. A routine activity drug market is one that is positioned in places where individuals who want drugs are likely to look in order to make a purchase. These markets are likely known by individuals who live in these areas because they have seen indicators of drug activity (e.g., sales) and view them as a problem. Violence may be used in those drug markets to enforce illegal drug transactions (Banerjee, Gruenewald, Freisthler, Treno & Remer, 2008; Goldstein, 1998).
The distinction between social network and routine activity drug markets serves as the basis for examining social mechanisms as they are related to abusive and neglectful parenting practices. Figure 1 provides a model (adapted by Gruenewald et al., 2013) that examines potential mechanisms relating aspects of drug use and drug availability with child abuse and neglect. Using language from alcohol and drug environmental interventions, we focus on aspects of drug demand and drug supply as described below (Treno & Lee, 2002; Gruenewald et al., 2013). Drug demand refers to the use of illicit drugs. Places with fewer drug users will have lower rates of demand for drugs. In our study, we represent drug demand using measures of individual drug use and rates of drug abuse and dependence at the city-level (Gruenewald et al., 2013). Drug supply refers to those to the production, distribution, and sale of illicit drugs (Gruenewald et al., 2013). Together these drug market forces may independently affect use of child physical abuse and neglect as described below.
Figure 1.
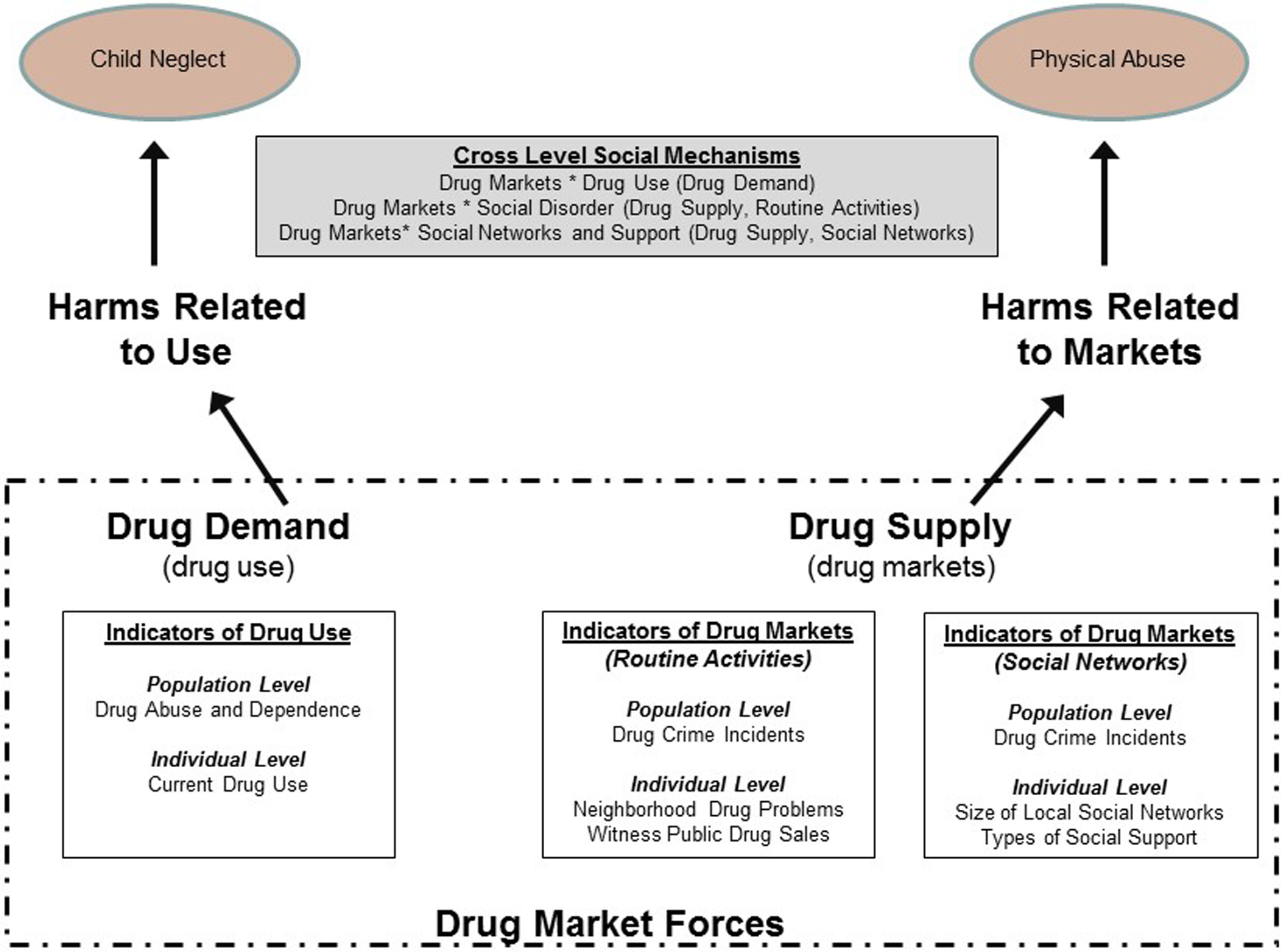
Conceptual model relating drug demand and drug supply to child maltreatment.
Drug Availability, Drug Use, and Child Maltreatment
Although drug use has been related to both physical abuse and neglect, a higher percentage of neglect cases involve drug use in the general population (Sedlak et al., 2010), with several studies finding no relationship between drug use and child physical abuse (Berger, 2005; DiLauro, 2004; Yampolskaya & Banks, 2006). Thus our model proposes that forces related to drug demand (e.g., use of drugs) will be most likely related to child neglect. The physiological effects of drug use might also support neglectful, more than physically abusive, parenting behavior. Neglect may be more likely to arise when psychoactive drug use “hijacks” reward centers of the brain important for parents to feel motivated to engage with and nurture their children (Rutherford, Williams, Moy, Mayes & Johns, 2011). Recent ecological evidence suggests that prescription drug overdoses are associated with child hospitalizations for unintentional injury (Price Wolf, Ponicki, Kepple, & Gaidus, 2016), indicating that greater drug demand in neighborhoods could be increasing neglectful parenting and thus raising risk of unintentional injury.
Greater availability of drugs, whether through social networks or more public, routine activities, drug markets, means that more parents may be using drugs. Thus if drugs are more difficult for potential users to obtain, they may forego using drugs for some other activity. Individual-level studies of illicit drug use find that children of parents who use drugs are at increased risk of maltreatment, especially neglect (DiLauro, 2004; Yampolskaya & Banks, 2006). In addition, ecological studies of the physical availability of drugs find that higher levels of drug availability (measured as police drug incidents, Freisthler et al., 2005; Freisthler, Kepple & Holmes, 2012; and as rates of drug treatment, Albert & Barth, 1996; Freisthler & Weiss, 2008) were related to higher rates of child maltreatment. Drug use may contribute to and/or exacerbate impairments in cognitive functioning, making it more difficult for parents to supervise their children adequately or to provide for their basic needs (Crittenden, 1993; De Paul & Guibert, 2008; Kepple, 2016). Along these lines, locations where one get drugs more readily may be more likely to trigger drug seeking and/or use behaviors among parents with uncontrolled drug use, resulting in drug behaviors being prioritized over addressing children’s basic needs.
Routine Activity Drug Markets and Social Disorder
As the routine activities approach to drug sales relies more on detailing the type of places that are attractive to drug dealers, individuals living within these areas may be at greater risk for being targeted by drug dealers to participate in some aspect of the markets—either as drug users or low-level sellers. Further, the drug dealer is at greater risk for being detected as he or she is less likely to know anything or to have built trust with his or her customers. Neighborhood areas that may be attractive as public drug markets include those with low levels of informal social control (i.e., the transmission norms and standards of acceptable behaviors). A neighborhood with high informal social control may be more likely to keep public drug sales from occurring in these areas. Drug markets might erode social control as people become afraid, stay indoors more, and worry about possible violent retribution if they speak out against problems in their neighborhood. Community members may then also become less likely to intervene against physical abuse or provide positive examples of parenting. People living within neighborhood areas with lower levels of social control may be more likely to witness drug sales or view these sales as a problem for the neighborhood.
Private Drug Markets, Social Networks, and Child Maltreatment
Within Figure 1, drugs sold through a social network approach are more likely to affect parents whose social network includes many individuals who use drugs. The more members of one’s social network who use drugs increase the opportunities that a person will either be introduced to the drug seller or increase the chances that they can purchase drugs in this manner. Here the characteristics of social network members and the type of social support received by those members are important mechanisms for determining the risk of maltreatment for children. For example, social networks that offer social companionship support may include social activities where drug use may be more likely, particularly in an area where drugs are more readily available. These social network markets, particularly through social companionship support, may be related to more frequent physical abuse (Freisthler, Holmes, & Price Wolf, 2014).
The current study assesses the relationship between indicators of drug demand and drug supply on physical abuse, physical neglect, and supervisory neglect in a general population sample. Drug demand is measured by individual-level drug use and city-level rates of drug abuse and dependence. Drug supply is measured using police incidents of drug sales and drug possessions at the city-level. We hypothesize that (1) individual drug use and city-level rates of drug abuse and dependence will be related to use of more physical and supervisory neglect; (2) size of neighborhood social networks and social companionship support will be related to more frequent physical abuse; and (3) perceptions of neighborhood drug problems, witnessing drug sales, and city-level density of drug crime incidents will be related to more frequent use of child physical abuse. We also hypothesize that city-level drug crime incidents will moderate the relationship between (1) drug use and supervisory and physical neglect; (2) social control and child physical abuse; and (3) size of local neighborhood social networks and type of social support and child physical abuse.
Methods
Data were collected using a telephone survey from parents of children aged 12 or younger in 50 cities in California in 2009. These cities were chosen from 138 cities in California with a population size of 50,000 to 500,000 in the 2000 Census. The list of cities was randomized and the first city on that list was considered the “seed city.” The next city on the list was chosen if the boundaries of the city were at least one mile and two cities away from any other city in the sample. This procedure continued until 50 cities were chosen. This was done to maximize the geographic validity of the overall sample.
The original survey contained 3,023 respondents. This study utilizes data on 2,597 respondents from 43 cities where we also had valid police data on narcotics incidents. Respondents were sampled using list-assisted samples of landlines in each of the 50 cities in order to target telephone numbers in those specific areas. Letters announcing the study’s purpose and providing a 1–800 “opt out” number were sent before the study began. These types of pre-announcement letters were used to increase the study response rate. Potential respondents were contacted ten times, unless deemed ineligible, or until the respondent agreed or declined to participate. If a potential respondent was interested in participating but was not available at the time of the call, the interviewer re-scheduled for a better time. A potential respondent was deemed eligible if he or she was a parent or guardian to at least one child 12 years old or younger, that child lived in the respondent’s home at least 50% of the time, spoke and understand English or Spanish, lived within the city limits of one of the 50 cities, and did not live in an institutional setting.
The total sample consisted of 21114 households. Of those, 2600 respondents completed the survey (2594 completed the full survey, 6 partially completed the survey). The number of eligible households refused that refused was 485. Less than 9000 (n = 8798) households were deemed ineligible. Of the remaining 9231 households, 4228 were contacted but eligibility could not be determined and 5003 were not contacted. The fraction of households likely to be eligible is .288. Using the American Association of Public Opinion Research (AAPOR) calculation, the number of completed divided by the sum of the completed, eligible households that refused and the fraction of likely eligible unknowns. The final response rate for this subsample 45.3%.
The survey was completed using a combination of a live interviewer on computer-assisted telephone interviewing software and interactivity voice recording (IVR) technology. The majority of the interview was conducted with a live interview. However, in order to increase a respondent’s willingness to answer honestly about sensitive parenting behaviors (e.g., use of physical force), parenting questions that may be indicative of child neglect or physical abuse were asked using IVR. Essentially, IVR uses a voice recording that asks the questions and includes prompts for response categories (e.g. press “1” for never, press “2” for sometimes). This approach provided security to the respondent to answer questions honestly without fear of being reported to Child Protective Services. The interview took approximately 30 minutes (25 minutes with the live interview, 5 minutes for the IVR) and an incentive of $30 was given to respondents. Survey weights adjusting for gender, race/ethnicity, and family type were created post hoc to adjust for potential sampling bias.
Outcome measures.
This study had three outcome measures: (1) frequency of physical abuse, (2) average of physical neglect behaviors; and (3) average of a variety of supervisory neglect behaviors. For all measures, the respondent answered the questions for one child 12 years or younger living the household (called the focal child). If more than one child met the inclusion criteria, the respondent was asked to choose the child who had the most recent birthday.
Child physical abuse was measured using the Conflict Tactics Scale, Parent Child version (Straus et al., 1998) which contains four measures of severe child assaults (five for children under 2 years of age). The physical abuse items asked how often the respondent had used the behaviors such as slapping a child on the face, head or ears or hitting the child on the bottom with a belt, stick or other hard object in the past year. Response categories included “never,” “1 to 5 times,” “6 to 10 times,” and “more than 10 times.” The midpoint for each response category was summed to create a count of the number of times the parent reported using child physical abuse in the past year. “More than 10 times” was recoded to 15. The average number of times physical abuse was used was 0.34 with a range of 0 to 50.
Both child physical neglect and child supervisory neglect were measured using the Multidimensional Neglectful Behavior Scale (Kantor, Holt, & Straus, 2003). The short form of the physical neglect scale was three items: (1) taking a child to a doctor when he or she was really sick; (2) having enough food in the house; and (3) keeping the house warm enough when it was cold outside. The supervisory neglect scale contained developmentally appropriate items for children 0 to 4 (6 items), 5 to 9 (10 items) and 10 to 12 (10 items). These included items like leaving a child home alone when an adult should be present or not watching a child closely enough. For all neglect measures, the response categories were “never,” “sometimes,” “often,” and “always.” When necessary items were reverse coded so that the higher number referred to the less desirable parenting behavior (e.g. never knew where my child was after school). The final score was an average for all items with a valid response. The physical neglect scale had an average of 1.02 and a range of 1 to 2.5. The supervisory neglect scale had a mean of 1.26 and a rage of 1 to 3.75.
Individual-level drug use and availability measures.
Three items assessed past year drug use among respondents for (1) marijuana or hashish, (2) methamphetamines, and (3) other illegal drugs such as cocaine, crack, heroin, hallucinogens, uppers, or downers. A positive response to any of the items was recoded to represent past year drug use (1) or no past year drug use (0). Two measures represented individual-level drug availability for study respondents. Respondents were asked whether or not they had seen public drug sales take place in their neighborhoods and whether drugs and drug sales were a “big problem,” “somewhat of a problem,” or “not a problem” in their neighborhood. The latter was recoded to a dichotomous variable where “big problem” and “somewhat of a problem” were combined.
Social control.
A modified version of the informal social control scale developed by the Project on Human Development in Chicago Neighborhoods (PHDCN) community survey was used to assess in this study (Sampson et al., 1999; Sampson et al., 1997). Informal child-centered social control was measured using four questions. Reliability, measured with Cronbach’s alpha, of the scale in this sample was .70. These questions asked the likelihood that a neighbor would do something about neighborhood children skipping school and hanging out on a street corner, spray-painting graffiti on a local building, beating up or threatening to beat up someone, and showing disrespect to an adult. Parent responses included “very likely,” “likely,” “neither likely nor unlikely,” “unlikely,” and “very unlikely.” Responses were summed, where higher responses indicate higher levels of informal social control in the neighborhood.
Social Support and Social Network.
Social support was assessed using the Interpersonal Support Evaluation List – Short Form (Cohen, Mermelstein, Kamarck, & Hoberman, 1985) which consisted of 12 items. Four items assessed social companionship or belongingness support (e.g., If I wanted to go on a trip for the day, I would have a hard time finding someone.), emotional support (e.g., I feel that there is no one I can share my most private worries and fears with.), and tangible support (e.g., If I were sick, I could easily find someone to help me with my daily chores.) Parents were asked if these statements were “definitely false,” “probably false,” “probably true,” or “definitely true.” Responses were summed for each type of social support where higher values indicated a higher presence of that type of social support.
The size of a respondent’s neighborhood social network was assessed with three questions - How many family and friends who live in your neighborhood can you (1) talk through problems with, share concerns, or ask for advice; (2) do recreational activities with such as going to lunch, to the movies, or out to bars; and (3) ask to help provide material things for your children if you need it. Because the respondent could conceivably be thinking of the same people who could provide all types of support, the responses were averaged across all three questions creating a size of the neighborhood social network available to provide support to respondents. Given that we do not have direct measures of drug use of the social networks of our respondents and support for using drugs, we assess the moderating effect of city-level drug crime incidents on our measures of neighborhood network size, companionship support, tangible support, and emotional support
City-level police incidents of drug sales and possessions.
Police-reported drug availability was measured using police incident data from 43 of the original 50 cities in the study. These data were collected for 2009 from each city’s Police Department. These data contained the street address (e.g., 123 Main St.) or street block (e.g. 100 block of Main St.) level and were geocoded. Narcotics incidents included police incidents that fall into Uniform Crime Reporting categories for drug abuse violations and other violations including (a) narcotic possessions, (b) narcotic drug sales, and (c) narcotic transportation and manufacturing and other violations related to (a) possession of drug paraphernalia and (b) unlawfully bringing drugs into prisons, hospitals, airports, businesses, schools, etc. The geocoding rate, or the number of locations where we could provide x, y coordinates for the location of the event, was 93.12% and ranged from 36% to 100% per city. These data were aggregated to the city-level and divided by the number of roadway miles to create a measure of the physical availability of drugs in each city.
City-level drug abuse and dependence.
Data from the California Office of Statewide Health Planning and Development were used to examine the percentage of hospital discharges related to drug abuse and dependence for the 43 cities in 2009. These discharges represent incidents that included at least one overnight stay. Up to five eternal causes of injuries and poisonings (e-codes) from the International Classification of Diseases, Ninth Revision (ICD-9) codes that describe the cause of the hospitalization as well as the residential address of the patient are recorded. These classifications were assessed to identify if any one of those classifications included that drug abuse or dependence.
Control variables.
A variety of control variables were included in all of the multivariate models. Demographic variables included child age, child gender, parent age (coded as < 30 years, 31 – 45 years, and 46 years and older), parent gender, marital status (married or in a marriage-like relationship vs. single/divorced/widowed), race/ethnicity (Black, White, Hispanic, Asian, Other, including multi-racial), and income (< $60,000, $60,001 - $100,000, > $100,000). Parenting stress was measured using two items from the Dimensions of Discipline Inventory (Straus & Fauchier, 2011). These items assessed whether or not a parent got angry when the child misbehaved or felt stressed out when a child missed behaved. Responses to these items (“Never,” “Sometimes.” “Often,” and “Always”) were averaged. Impulsivity was measured using seven items from Dickson’s Dysfunctional impulsivity scale. Yes/no responses were summed to create an index. Drinking behaviors were assessed with a variety of questions that asked how often a person drank and how much alcohol they consumed when they did drink. These measures were recoded into abstainers (never drank in their lifetime or did not have a drink in the past year), light drinkers (only drank 1 to 2 drinks at a time, never drank 3 or more drinks in one setting in the past year), moderate drinkers (drank three to four drinks per occasion, but never more than five drinks), and heavy drinkers (drank five or more drinks at least one in the past year) (Kantor & Straus, 1987; Paschall, Freisthler, & Lipton 2005). At the city-level, variables representing the density (per roadway miles) of off-premise alcohol outlets (e.g. grocery and liquor stores), on-premise alcohol outlets (e.g., bars and restaurants) and the proportion of on-premise alcohol outlets that are bars. We also included the percentage of households with less than $25,000 income as a measure of socio-economic disadvantage.
Data analysis procedures.
Negative binomial models with random effects (to address issues of clustering within cities) were used to analyze the relationship of the drug environment to child physical abuse. The study controlled for a variety of individual demographic and psychosocial characteristics of parents and families. Multilevel linear (regression) models were used to analyze the relationship of the drug models with the neglect outcomes (physical and supervisory) neglect. To test the moderating effect of the individual-level and city-level variables we created cross-level interactions within the statistical software.
Results
Descriptive statistics can be found in Table 1. Tables 2 through 4 present the findings for each of the outcomes: physical abuse (Table 2), physical neglect (Table 3) and supervisory neglect (Table 4). In each table, the presentation of the findings includes a base model (Model 1 with no interactions), Model 2 showing drug use variables as a proxy for drug demand and interactions between drug use and density of drug incidents and drug use and rates of drug abuse and dependence, Model 3 examining the routine activities theory of drug supply (including interactions for witness drug problems by density of drug incidents, drug problems in the neighborhood by density of drug incidents, and informal social control by density of drug incidents), and a model for the social network theory for drug supply (including the interaction of density of drug incidents with average size of social network members living within the neighborhood, companionship support, emotional support, and tangible support). All models control for child age, child gender, parent age, parent gender, marital status, race/ethnicity, income, parenting stress, impulsivity, and drinking behaviors at the individual level and alcohol outlet density at the city-level.
Table 1:
Descriptive Statistics for Dependent, Primary Independent and Control Variables
| % or (sd) | n | |
|---|---|---|
| Dependent Variables | ||
| Supervisory Neglect | 1.26 (0.33) | 2461 |
| Physical Neglect | 1.02 (0.10) | 2465 |
| Physical Abuse | 0.34 (2.04) | 2375 |
| Primary Independent Variables | ||
| Drug Crime Incidents per area (city-level) | 24.68 (23.54) | 43 |
| Drug Abuse and Dependence per population (city-level) | 4.01 (1.68) | 43 |
| Past Year Drug Use | ||
| Yes | 9.4 | 241 |
| No | 90.6 | 2335 |
| Drug and Drug Sales are a Problem | ||
| Yes | 21.2 | 531 |
| No | 78.8 | 1970 |
| Informal Social Control | 16.34 (3.01) | 2364 |
| Local Social Network Size (within neighborhood) | 3.52 (5.17) | 2406 |
| Types of Social Support | ||
| Companionship Support | 14.12 (2.12) | 2572 |
| Emotional Support | 14.87 (1.89) | 2572 |
| Tangible Support | 14.48 (2.03) | 2572 |
| Demographic Control Variables | ||
| Child age (in years) | 6.71 (3.62) | 2500 |
| Child Gender | ||
| Male | 51.0 | 1273 |
| Female | 49.0 | 1224 |
| Parent age (in years) | ||
| ≤ 30 | 13.1 | 341 |
| 31 – 45 | 67.2 | 1745 |
| 46 and older | 19.7 | 511 |
| Parent Gender | ||
| Male | 35.0 | 910 |
| Female | 65.0 | 1687 |
| Marital Status | ||
| Married or Living in a Marriage-like Relationship | 88.7 | 2304 |
| Single/Widowed/Divorced | 11.3 | 293 |
| Parent Race/Ethnicity | ||
| White, non-Hispanic | 57.3 | 1482 |
| Black, non Hispanic | 3.9 | 100 |
| Asian | 8.5 | 221 |
| Hispanic | 24.7 | 638 |
| Multi-race/Other | 5.6 | 145 |
| Income | ||
| Less than $60,000 | 29.1 | 727 |
| $60,000 to $100,000 | 37.2 | 928 |
| $100,001 and higher | 10.1 | 262 |
| Parenting Stress | 3.97 (1.31) | 2564 |
| Impulsivity | 0.74 (1.30) | 2554 |
| Drinking Behaviors | ||
| Abstainer/Ex-Drinker | 28.7 | 743 |
| Light Drinker | 45.4 | 1173 |
| Moderate Drinker | 16.8 | 435 |
| Heavy Drinker | 9.1 | 234 |
| Percent of Households with Income < $25,000 (city-level) | 43 | |
| Density (per area) of Off-Premise Alcohol Outlets (city-level) | 3.95 (3.05) | 43 |
| Density (per area) of On-Premise Alcohol Outlets (city-level) | 6.40 (4.70) | 43 |
| Proportion of On-Premise Outlets that are Bars (city-level) | 0.12 (0.05) | 43 |
Table 2:
Relationship of Drug Supply and Drug Demand on Physical Abuse by Parents (n = 1831)
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Base Model | Drug Demand | Drug Supply | Drug Supply | |||||||||
| Routine Activities | Social Networks | |||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | |
| City-Level | ||||||||||||
| Drug Availability | 0.015 | 0.014 | 0.008 | 0.014 | −0.048 | 0.045 | 0.072 | 0.098 | ||||
| Drug Abuse and Dependence | 0.240 | 0.095 | * | 0.161 | 0.100 | 0.207 | 0.097 | * | 0.203 | 0.096 | * | |
| Drug Demand | ||||||||||||
| Past Year Drug Use | 0.860 | 0.426 | * | 0.340 | 0.563 | 0.905 | 0.431 | * | 0.811 | 0.432 | ||
| Current Drug Use * Availability | 0.051 | 0.023 | * | |||||||||
| Current Drug Use * Abuse/Dependence | 0.311 | 0.222 | ||||||||||
| Drug Supply (Routine Activity Markets) | ||||||||||||
| Witness Drug Sale | 1.039 | 0.340 | ** | 1.088 | 0.332 | *** | 0.893 | 0.365 | * | 1.071 | 0.340 | ** |
| Witness Drug Sales * Availability | 0.031 | 0.022 | ||||||||||
| Drug and Drug Sales Problem | 0.167 | 0.337 | 0.152 | 0.327 | 0.047 | 0.350 | 0.130 | 0.334 | ||||
| Drugs as Problem * Availability | 0.029 | 0.022 | ||||||||||
| Informal Social Control | −0.091 | 0.041 | * | −0.095 | 0.039 | * | −0.101 | 0.040 | * | −0.097 | 0.041 | * |
| Social Control * Availability | 0.002 | 0.002 | ||||||||||
| Drug Supply (Social Network Markets) | ||||||||||||
| Neighborhood Network Size | 0.025 | 0.019 | 0.015 | 0.024 | 0.017 | 0.025 | 0.009 | 0.030 | ||||
| Network Size * Availability | 0.002 | 0.001 | ||||||||||
| Companionships Support | 0.146 | 0.079 | 0.167 | 0.078 | * | 0.151 | 0.077 | * | 0.163 | 0.079 | * | |
| Companionship * Availability | −0.001 | 0.007 | ||||||||||
| Emotional Support | −0.183 | 0.078 | * | −0.196 | 0.076 | ** | −0.165 | 0.075 | * | −0.191 | 0.079 | * |
| Emotional * Availability | −0.004 | 0.006 | ||||||||||
| Tangible Support | −0.132 | 0.073 | −0.129 | 0.071 | −0.140 | 0.072 | −0.136 | 0.072 | ||||
| Tangible * Availability | −0.003 | 0.004 | ||||||||||
p < .05,
p < .01,
p < .001
Model controls for child age, child gender, parent age, parent gender, marital status, race/ethnicity, income, parenting stress, impulsivity, and drinking behaviors at the individual level and alcohol outlet density and percent of households with income less than $25,000 at the city-level
Table 4:
Relationship of Drug Supply and Drug Demand on Supervisory Neglect by Parents (n = 1900)
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Base Model | Drug Demand | Drug Supply | Drug Supply | |||||||||
| (Routine Activities) | (Social Networks) | |||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | |
| City-Level | ||||||||||||
| Drug Availability | 0.001 | 0.001 | 0.001 | 0.001 | 0.003 | 0.003 | 0.013 | 0.007 | ||||
| Drug Abuse and Dependence | 0.002 | 0.008 | <−0.001 | 0.008 | 0.002 | 0.007 | 0.003 | 0.008 | ||||
| Drug Demand | ||||||||||||
| Past Year Drug Use | 0.045 | 0.042 | 0.041 | 0.042 | 0.044 | 0.042 | 0.048 | 0.042 | ||||
| Current Drug Use * Availability | −0.001 | 0.003 | ||||||||||
| Current Drug Use * Abuse/Dependence | 0.033 | 0.026 | ||||||||||
| Drug Supply (Routine Activity Markets) | ||||||||||||
| Witness Drug Sale | 0.040 | 0.033 | 0.037 | 0.033 | 0.046 | 0.033 | 0.043 | 0.033 | ||||
| Witness Drug Sales * Availability | −0.002 | 0.002 | ||||||||||
| Drug and Drug Sales Problem | −0.029 | 0.024 | −0.029 | 0.024 | −0.026 | 0.024 | −0.029 | 0.024 | ||||
| Drugs as Problem * Availability | −0.001 | 0.001 | ||||||||||
| Informal Social Control | <0.001 | 0.003 | <0.001 | 0.003 | 0.001 | 0.003 | <0.001 | 0.003 | ||||
| Social Control * Availability | <−0.001 | <0.001 | ||||||||||
| Drug Supply (Social Network Markets) | ||||||||||||
| Neighborhood Network Size | −0.003 | 0.002 | −0.003 | 0.002 | −0.003 | 0.002 | −0.003 | 0.002 | ||||
| Network Size * Availability | <0.001 | <0.001 | ||||||||||
| Companionships Support | −0.012 | 0.006 | −0.011 | 0.006 | −0.012 | 0.006 | * | −0.011 | 0.006 | |||
| Companionship * Availability | <0.001 | <0.001 | ||||||||||
| Emotional Support | −0.016 | 0.007 | * | −0.016 | 0.007 | * | −0.015 | 0.007 | * | −0.015 | 0.007 | * |
| Emotional * Availability | −0.001 | <0.001 | ** | |||||||||
| Tangible Support | −0.004 | 0.007 | −0.004 | 0.007 | −0.004 | 0.007 | −0.004 | 0.007 | ||||
| Tangible * Availability | <0.001 | <0.001 | ||||||||||
p < .05,
p < .01,
p < .001
Model controls for child age, child gender, parent age, parent gender, marital status, race/ethnicity, income, parenting stress, impulsivity, and drinking behaviors at the individual level and alcohol outlet density and percent of households with income less than $25,000 at the city-level
Table 3:
Relationship of Drug Supply and Drug Demand on Physical Neglect by Parents (n = 1896)
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Base Model | Drug Demand | Drug Supply | Drug Supply | |||||||||
| (Routine Activities) | (Social Networks) | |||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | |
| City-Level | ||||||||||||
| Drug Availability | <0.001 | <0.001 | <0.001 | <0.001 | −0.001 | 0.001 | 0.001 | 0.002 | ||||
| Drug Abuse and Dependence | 0.004 | 0.003 | 0.001 | 0.003 | 0.004 | 0.003 | 0.004 | 0.003 | ||||
| Drug Demand | ||||||||||||
| Past Year Drug Use | 0.036 | 0.014 | * | 0.039 | 0.014 | ** | 0.037 | 0.014 | ** | 0.035 | 0.014 | * |
| Current Drug Use * Availability | 0.003 | 0.001 | *** | |||||||||
| Current Drug Use * Abuse/Dependence | 0.036 | 0.009 | *** | |||||||||
| Drug Supply (Routine Activity Markets) | ||||||||||||
| Witness Drug Sale | 0.044 | 0.012 | *** | 0.041 | 0.012 | *** | 0.039 | 0.012 | *** | 0.041 | 0.012 | *** |
| Witness Drug Sales * Availability | 0.002 | 0.001 | * | |||||||||
| Drug and Drug Sales Problem | 0.005 | 0.008 | 0.003 | 0.008 | 0.004 | 0.008 | 0.004 | 0.008 | ||||
| Drugs as Problem * Availability | <0.001 | <0.001 | ||||||||||
| Informal Social Control | −0.001 | 0.001 | −0.001 | 0.001 | −0.001 | 0.001 | −0.001 | 0.001 | ||||
| Social Control * Availability | <0.001 | <0.001 | ||||||||||
| Drug Supply (Social Network Markets) | ||||||||||||
| Neighborhood Network Size | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | ||||
| Network Size * Availability | <0.001 | <0.001 | * | |||||||||
| Companionships Support | 0.002 | 0.002 | 0.003 | 0.002 | 0.002 | 0.002 | 0.002 | 0.002 | ||||
| Companionship * Availability | <−0.001 | <0.001 | ||||||||||
| Emotional Support | −0.007 | 0.002 | ** | −0.008 | 0.002 | *** | −0.007 | 0.002 | ** | −0.007 | 0.002 | ** |
| Emotional * Availability | <0.001 | <0.001 | ||||||||||
| Tangible Support | −0.003 | 0.002 | −0.003 | 0.002 | −0.003 | 0.002 | −0.003 | 0.002 | ||||
| Tangible * Availability | <−0.001 | <0.001 | ||||||||||
p < .05,
p < .01,
p < .001
Model controls for child age, child gender, parent age, parent gender, marital status, race/ethnicity, income, parenting stress, impulsivity, and drinking behaviors at the individual level and alcohol outlet density and percent of households with income less than $25,000 at the city-level
Physical Abuse.
In Model 1, city-level rates of drug abuse and dependence and individual-level drug use were positively related to physical abuse (see Table 2). Respondents who witnessed drug sales in their neighborhood also reported more frequent physical abuse. Higher levels of informal child-centered social control and higher levels of emotional support were related to less frequent use of child physical abuse. In Model 2, the results are fairly similar. However, drug use by itself was no longer statistically significant, rather the interaction between density of drug crime incidents and drug use exhibits a positive relationship with child physical abuse. Parents who live in neighborhoods with more drug crime incidents and use drugs are more likely to use physical abuse than parents who live in neighborhoods with more drug crime incidents but do not use drugs. Higher levels of social companionship were related to more frequent use of child physical abuse. In the Model 3, none of the interaction variables were statistically significant; however, city-level drug abuse and dependence, individual-level drug use, witnessing drug sales and social companionship had a positive statistically significant relationship with child physical abuse. Informal social control and emotional support were negatively related to child physical abuse. For the Model 4, none of the interaction variables were significant and the findings remained relatively stable when compared to previous models.
Physical Neglect.
In Table 3, having more emotional support was consistently negatively related to physical neglect across all four models. Individual-level drug use and witnessing neighborhood drug sales were positively related to physical neglect across all four models. In Model 2, the interaction between city-level drug incidents and individual drug use and the interaction between individual-level drug use and city-level rates of drug abuse and dependence were related to higher levels of reported physical neglect. Thus, parents who lived in neighborhoods with more drug crime incidents and used drugs had higher levels of physical neglect than parents who lived in neighborhoods with fewer drug crime incidents. In Model 4, the interaction between neighborhood network size and density of drug crime incidents was positively related to child physical neglect. In other words, respondents who had larger neighborhood networks and lived in cities with higher densities of drug crimes reported significantly higher levels of physical neglect.
Supervisory Neglect.
Emotional support was consistently negatively related to use of supervisory neglect by parents across all four models (Table 4). In Model 4 the interaction between emotional support and density of police drug crime incidents was negatively related to supervisory neglect.
Discussion
Our study sought to examine how the drug environment may affect abusive and neglectful parenting behaviors. In particular, we hypothesized that the drug environment might interact with drug use, neighborhood drug exposure, or through social networks and types of social support. We found mixed support for our hypotheses. Elements of drug use were related to more frequent physical abuse and physical but not supervisory neglect. City-level density of police drug incidents moderated the relationship between drug use and child physical abuse and physical neglect such that parents who use drugs in areas with greater availability of drugs reported higher levels of physical abuse and physical neglect.
Parents who report witnessing drug sales also reported higher levels of physical neglect. Although we hypothesized no relationship between witnessing drug sales and either forms of child neglect, higher levels of drug local drug sales in cities may reflect a general lack of resources for families within their local neighborhood (Freisthler, LaScala, Gruenewald, & Treno, 2005; Maguire-Jack & Klein, 2015; Saxe et al., 2001). This lack of resources could impede a parent’s ability to take their child to the doctor or make sure that the house is warm enough. Further, parents who report witnessing drug sales in their neighborhood and live in cities with greater densities of police drug crime incidents report even higher levels of child physical neglect. Thus, this disadvantage appears to be even greater where both local and city-wide drug availability is higher.
Concerning the routine activities drug supply models, parents who witness drug sales in their neighborhood reported more physical abuse and physical neglect. Informal social control was negatively related to physical abuse. Neither of these relationships were moderated by drug availability. Parents who witness drug sales may feel the need to use physical force when disciplining their children in order to convey the seriousness of misbehavior in neighborhoods with lots of visible drug activity. Alternatively, drug markets are also known to use violence to enforce drug transactions, which may lead to a culture of violence in those neighborhood areas. This may be particularly true for routine activity drug markets, which require finding public areas in which to “set up shop” may be characterized by violent interactions in order to ensure market transactions are enforced (Banerjee et al., 2008). This violence may indicate areas where norms against violent behaviors have weakened, resulting in child physical abuse. More active drug environments (as measured by drug availability) may also make it easier for parents to obtain illicit drugs for their own use. The combination of this environment and parental drug use may place children at greater risk for being physically abused.
Finally, social mechanisms detailing aspects of social network drug supply markets were primarily related to physical and supervisory neglect. Parents living in areas with high densities of city-level drug availability and had more people in their neighborhood social networks reported higher levels of physical neglect. These social network members may be also be drug users making it easier for parents to neglect the physical needs of their children. Emotional support buffered the relationship between city-level drug crimes for physical neglect and emotional support buffered the relationship of city-level drug availability for both supervisory neglect. In fact, emotional support was negatively related to physical abuse, physical neglect, and supervisory neglect in all four models. Thus, developing interventions that seek to bolster positive emotional connections among parents would appear to prevent a broad range of negative parenting behaviors.
Although previous literature found rates of child maltreatment were higher in areas with greater drug availability (Freisthler et al., 2005; Freisthler et al., 2008), we find that the mechanisms relating this to specific types of child maltreatment are more nuanced than those studies suggest. The testing of these mechanisms allows us to assess how the drug environment may place children at risk for abuse or neglect. For example, while most child welfare interventions focus on reducing parental drug use in order to reduce child abuse, these findings suggest environmental prevention or neighborhood strengthening approaches that reduce the supply of illicit drugs may also reduce child abuse through multiple mechanisms.
Results should be interpreted cautiously as they are based on a cross-sectional study and some variables not controlled for in the study could be influencing the results. An alternate explanation to the findings presented here is that cities with high levels of police-identified drug activity may also have high levels of violence. Thus, it may be the violence that is a driving physical abuse and neglect, not drug markets. Causation cannot be inferred by the current study. Although this study is a general population survey, households with only cell phones are not represented, which may mean low income and younger parents might be underrepresented. The study is also limited in that the lower response rate may mean that biases may exist who participated. We did create post hoc weights in an attempt to minimize this source of bias. By dichotomizing our drug use measures, we lose specificity on differences between infrequent and frequent users. In general, however, the respondents in this study were infrequent drug users. Police incidents related to drug crimes may underestimate drug availability, as they may be more likely to reflect patrol patterns by police or concerns about where drug markets may located as opposed to true availability of drugs. This might be true particularly for social network drug markets, which might be more difficult for police to identify and infiltrate (Eck, 1995). City-level measures of police drug incidents do not allow us to assess how very local effects related to how drug availability may affect parenting behavior. Future work should assess these relationships with smaller spatial units (e.g., Census tracts or block groups.) Finally, disentangling physical neglect from poverty is difficult. We control for family income and neighborhood income as a way to try and assess effects related to poverty and neglectful parenting separately.
This study represents a first step in understanding the social mechanisms relating drug environment to different types of child maltreatment. Future work might assess how the context of drug use (i.e., where, when, how much, and with whom) might relate to abusive or neglectful parenting. This may be especially important in identifying intervention points for social network drug markets as those may not easily be addressed through place management techniques. Finally, risks from the drug environment might be directly related to how people use those local areas. Parents who regularly go through areas where routine activity drug markets are located may be more attuned to the problems associated with those places. Parents who regularly interact with drug-using social networks may be more prone to problems associated with social network drug markets. Future work should focus on the social networks of parents to assess how their individual drug use and the drug use of their network members affect both the availability of drugs and parenting behaviors as this might provide key insights into avenues for prevention. These findings may hold implications for the current debates around legalization of marijuana as legalizing marijuana for either recreational or medical purposes will increase the availability of marijuana through outlets such as dispensaries or retail stores (Freisthler, Gruenewald, & Price Wolf, 2015).
Funding acknowledgement:
This project was supported by grant number P60-AA-006282 from the National Institute on Alcohol Abuse and Alcoholism. The content is solely the responsibility of the authors and does not necessarily represent the National Institute on Alcohol Abuse and Alcoholism or the National Institutes of Health.
Contributor Information
Bridget Freisthler, Ohio State University, College of Social Work, 1947 College Road, Columbus, Ohio 43210
Jennifer Price Wolf, Division of Social Work, California State University, Sacramento, 6000 J Street, Sacramento, CA 95819
Wendy Wiegmann, California Child Welfare Indicators Project, School of Social Welfare, University of California, Berkeley, 120 Haviland Hall #7400, Berkeley, CA 94720-7400.
Nancy J. Kepple, School of Social Welfare, University of Kansas, 1545 Lilac Ln., Lawrence, KS 66045
References
- Albert VN, & Barth RP (1996). Predicting growth in child abuse and neglect reports in urban, suburban, and rural counties. Social Service Review, 70, 58–82. [Google Scholar]
- Banerjee A, LaScala E, Gruenewald PJ, Freisthler B, Treno A, & Remer LG (2008). Social disorganization, alcohol and other drug markets and violence: A space-time model of community structure. In Thomas YF, Richardson D and Cheung I (eds.) Geography and Drug Addiction, pp. 117–130. New York, NY: Springer. [Google Scholar]
- Berger LM (2005). Income, family characteristics, and physical violence toward children. Child Abuse and Neglect, 29(2), 107–133. [DOI] [PubMed] [Google Scholar]
- Cohen S, Mermelstein R, Kamarack T, & Hoberman H (1985). Measuring the functional components of social support. In Sarason IG & Sarason BR (Eds.), Social support: Theory, research, and application (pp. 73–94). Dordrecht, Netherlands: Martinus Nijhoff. [Google Scholar]
- Crittenden PM (1993). An information-processing perspective on the behavior of neglectful parents. Criminal Justice and Behavior, 20(1), 27–48. [Google Scholar]
- DePaul J, & Guibert M (2008). Empathy and child neglect: A theoretical model. Child Abuse & Neglect, 32(11), 1063–1071. [DOI] [PubMed] [Google Scholar]
- DiLauro M (2004). Psychosocial factors associated with types of child maltreatment. Child Welfare, 83(1), 69–99. [PubMed] [Google Scholar]
- Eck JE (1995). A general model of the geography of illicit retail market places. In Eck JE & Weisburd D (Eds.), Crime and place: Crime prevention studies (Vol. 4, pp. 67–94). Monsey: Criminal Justice Press. [Google Scholar]
- Freisthler B & Weiss RE (2008). Using Bayesian space-time models to understand the substance use environment and risk for being referred to Child Protective Services. Substance Use & Misuse Special Issue, 43(2), 239–251. [DOI] [PubMed] [Google Scholar]
- Freisthler B, Kepple NJ, & Holmes MR (2012). The geography of drug market activities and child maltreatment. Child Maltreatment, 17(2), 144–152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freisthler B, Holmes MR, & Price Wolf J (2014). The dark side of social support: Understanding the role of social support, drinking behaviors and alcohol outlets for child physical abuse. Child Abuse and Neglect, 38, 1106–1119. doi: 10.1016/j.chiabu.2014.03.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freisthler B, Gruenewald PJ, & Price Wolf J (2015). Examining the relationship between marijuana use, medical marijuana dispensaries, and abusive and neglectful parenting. Child Abuse and Neglect, 49, 170–178. doi: 10.1016/j.chiabu.2015.07.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freisthler B, Needell B, & Gruenewald PJ (2005). Is the physical availability of alcohol and illicit drugs related to neighborhood rates of child maltreatment? Child Abuse and Neglect, 29(9), 1049–1060. [DOI] [PubMed] [Google Scholar]
- Freisthler B, LaScala EA, Gruenewald PJ & Treno AJ (2005). An examination of drug activity: Effects of neighborhood social organization on the development of drug distribution systems. Substance Use and Misuse 40(5), 671–686. [DOI] [PubMed] [Google Scholar]
- Goldstein PJ (1998). Drugs, violence, and federal funding: a research odyssey. Substance Use and Misuse, 33, 1915–1936. [DOI] [PubMed] [Google Scholar]
- Gruenewald PJ; Ponicki WR; Remer LG; Johnson FW; Waller LA, Gorman DM; and Zhu L (2013). Spatial models of the growth and spread of methamphetamine abuse in California. In Sanders B, Thomas YF, and Deeds BG (eds.) Crime, HIV and Health: Intersections of Criminal Justice and Public Health Concerns, pp. 167–186. New York: Springer. [Google Scholar]
- Kantor GK, Holt M, & Straus MA (2003). The Parent-Report Multidimensional Neglectful Behavior Scale. Durham, NH: Family Research Laboratory. [Google Scholar]
- Kantor GK & Straus M (1987). The “drunken bum” theory of wife beating. Social Problems, 34, 214–231. [Google Scholar]
- Kepple NJ (2017). The complex nature of parental substance use: Examining past year and prior use patterns as correlates of child maltreatment frequency. Substance Use & Misuse. Available online early 10.1080/10826084.2016.1253747 [DOI] [PubMed] [Google Scholar]
- Kepple NJ (2016, January). Does Parental Substance Use Always Engender Risk for Children? Decomposing Substance Use by Behavior Patterns. 20th Annual Conference Anniversary Celebration of the Society for Social Work and Research, Washington, D.C. [Google Scholar]
- Maguire-Jack K & Klein S (2015). Parenting and Proximity to Social Services: Lessons from Los Angeles County in the Community Context of Child Neglect. Child Abuse & Neglect, 45, 35–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozanne-Smith J, Day L, Parsons B, Tibballs J, Dobbin M (2001). Childhood poisoning: Access and prevention. Journal of Paediatrics and Child Health, 37(3), 262–265. [DOI] [PubMed] [Google Scholar]
- Paschall MJ, Freisthler B, & Lipton RI (2005). Moderate alcohol use and depression in young adulthood: Findings from a National Longitudinal Study. American Journal of Public Health, 95, 453–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price Wolf J, Ponicki W, Kepple N, Gaidus A (2016). Are community level prescription opioid overdoses associated with child harm? A spatial analysis of California zip codes, 2001–2011. Drug and Alcohol Dependence, 166, 202–208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutherford HJV, Williams SK, Moy S, Mayes LC, & Johns JM (2011). Disruption of maternal parenting circuitry by addictive process: rewiring of reward and stress systems. Frontiers of Psychiatry, 2(37). doi: 10.3389/fpsyt.2011.00037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sampson RJ, Morenoff JD, & Earls F (1999). Beyond social capital: Spatial dynamics of collective efficacy for children. American Sociological Review, 64, 633.-. [Google Scholar]
- Sampson RJ, Raudenbush SW, & Earls F (1997). Neighborhoods and violent crime: A multilevel study of collective efficacy. Science, 277, 918–924. [DOI] [PubMed] [Google Scholar]
- Saxe L, Kadushin C, Beveridge A, Livert D, Tighe E, Rindskopf D, Ford J, & Brodsky A (2001). The visibility of illicit drugs: implications for community-based drug control strategies. American Journal of Public Health, 91, 1987–1994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sedlak AJ, Mettenburg J, Basena M, Petta I, McPherson K, Greene A, & Li S (2010). Fourth National Incidence Study of Child Abuse and Neglect (NIS–4): Report to Congress. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families. [Google Scholar]
- Straus MA, Hamby SL, Finkelhor D, Moore DW, & Runyan D (1998). Identification of child maltreatment with the parent-child conflict tactics scales: Development and psychometric data for a national sample of American parents. Child Abuse & Neglect, 22(4), 249–270. [DOI] [PubMed] [Google Scholar]
- Straus MA and Fauchier A. (2011). “Manual for the Dimensions of Discipline Inventory (DDI).” Durham, NH: Family Research Laboratory, University of New Hampshire. http://pubpages.unh.edu/~mas2/ [Google Scholar]
- Testa MF & Smith B (2009). Prevention and drug treatment. The Future of Children, 19, 147–168. [DOI] [PubMed] [Google Scholar]
- Treno AJ & Lee JP (2002). Approaching alcohol problems through local environmental interventions. Alcohol Research & Health, 26(1), 35–40. [PMC free article] [PubMed] [Google Scholar]
- Yampolskaya S, & Banks SM (2006). An assessment of the extent of child maltreatment using administrative databases. Assessment, 13(3), 342–355. [DOI] [PubMed] [Google Scholar]