

Abstract
Issue addressed
The Anthropocene is a new era in which human activity has been the dominant influence on climate and the environment. The negative impact humans have on the earth's systems pose significant threats to human health. Health promotion is a discipline well placed to respond to planetary health challenges of the Anthropocene. The overarching aim of this paper is to describe the elements of 21st century socio‐ecological health and apply them in a revised socio‐ecological framework for health promotion.
Methods
A qualitative description study design was employed to explore the significance of ecological and cultural determinants of health and review models in contemporary health promotion to inform the development of a revised Mandala of Health. Purposeful sampling was used to recruit ten experts from across Australia including academics and practitioners working at the nexus of health promotion, environmental management and sustainability. Data were analysed thematically, using deductive and inductive methods.
Results
A revised Mandala of Health could address existing gaps in health promotion theory and practice. Ecological and cultural determinants of health were considered essential components of health promotion that is often lacking in socio‐ecological frameworks. Indigenous Knowledge Systems were considered immensely important when addressing ecological and cultural determinants of health.
Conclusions
A revised Mandala of Health could encourage development of contemporary health models, assisting health promotion to evolve with the health and environmental issues of the Anthropocene. This study highlights the need for more theoretical development and empirical research regarding ecological and cultural determinants of health in a health promotion context.
So what?
In the context of the Anthropocene, this study highlights the potential gaps in health promotion theory and practice in terms of the natural environment and health and emphasises the need of a paradigm shift to embed ecological and cultural determinants with other determinants of health.
Keywords: Anthropocene, cultural determinants, ecological determinants, health promotion, Mandala of Health, planetary health
1. INTRODUCTION
During the past half century, the physical and natural environment has been dramatically altered at such a magnitude and speed that critical ecological boundaries have been exceeded. 1 , 2 , 3 This pattern has created a new epoch called the ‘Anthropocene’. 1 The Anthropocene is a geological phenomenon recognising the dramatic impact humans have made on the earth's systems. 1 , 4 These systems are ecological determinants of health (EDoH), which include oxygen, water, food, materials and other protective mechanisms of the ecosystem. 5 These have been relatively stable for the past 11 000 years. 1 However anthropocentric activities are disrupting these systems through population growth and rapid urbanisation, economic growth and industrialisation. 1 , 5 The human subsystem is expanding at a rate which is disproportionate to other supporting ecosystems which have fixed boundaries. 6 These boundaries (or thresholds) include climate change, biodiversity, ecotoxicity, ocean acidification and resource depletion. 1 As a result, ecosystem services that provide fundamental pre‐requisites for human health become disrupted, fragmented and scarce, consequently declining human health ensues. 4 , 7 , 8 Ecosystem services are the benefits people obtain from ecosystems. These include:
-
●
provisioning services (for example food, fresh water, fuel);
-
●
regulating services (including climate and disease regulation and water purification);
-
●
cultural services (including spiritual, educational and recreational), and;
-
●
supporting services (for example soil formation and photosynthesis). 9
This is a geological phenomenon recognising the dramatic impact humans have made on the earth's systems. 1 , 4 It is due to both the scale and the rapidity of these changes that this era is arguably the greatest public health threat in the 21st century. 10
Human health and wellbeing are inextricably linked to these environmental changes of the Anthropocene. 4 , 6 , 10 The Lancet recognises the improved quality of health that comes with respecting the integrity of natural systems and calls for improved understanding on planetary health. 10 Planetary health seeks to understand and promote the safe planetary limits in which human civilisation can flourish. 10 Numerous studies demonstrate that the natural environment can promote or harm health. 11 , 12 , 13 There has been a growing number of reviews about the associated positive physical, social and mental health benefits from engagement with nature. 14 , 15 Conversely, environmental damage (such as air, water and noise pollution) can threaten human health and wellbeing. 16
It is thought health promotion is well‐suited to address the complex planetary health issues. 4 , 17 , 18 Planetary health encompasses a range of disciplines as it recognises the interdependencies between human health and the planet's life‐sustaining systems. 10 Planetary health builds on the existing mandates that guide the field of health promotion and represents a new chapter in its constant redefinition within public health. The transferable competencies and intersectoral nature that is embedded in health promotion, is a well‐suited foundation to addressing complex health issues such as planetary health. Additionally, the Health Promotion Journal of Australia has now clarified their intent to include EDoH which further emphasises the role of health promotion in the era of planetary health. 19
The constant re‐definition of health promotion has been expanded to include planetary health which was reflected in April of 2019 at the 23rd IUHPE World Conference on Health Promotion in Rotorua (New Zealand). This fostered the space for health promoters around the world to come together and discuss its theme: “Waiora: Promoting planetary health and sustainable development for all”. 20 Furthermore, “stable ecosystems” and “sustainable resources” are outlined in the Ottawa Charter for Health Promotion as prerequisites for human health. 21 These mandates demonstrate the reciprocal relationship between the natural environment and human health and highlight the role health promotion has in addressing EDoH. There is an opportunity to improve the conceptual modelling of our relationship with the natural environment to better our progress in addressing the health threats of the Anthropocene.
A socio‐ecological approach to health is required which recognises both the dynamic interplay between individual and environmental factors at different scales and the interaction between the social and EDoH. 1 . However, it has been argued that health promotion has been “ecologically blind”. 1 The primary focus of health promotion has been on the social aspect of health which was encapsulated by the World Health Organisation (WHO) Commission of the Social Determinants of Health in 2008. 22 Research and experts proclaim that the health impacts of EDoH (ie key elements of the natural environment) are as significant and comparable to those of social determinants of health (SDoH). 4 , 5 , 6 , 10 Thus, the goals of 21st century health promotion should predicate ecological equity and stable ecosystems, creating a pathway for transition from public to planetary health. 3 , 10 This requires an ecological analysis of health promotion models focusing on the interdependence of social and EDoH.
Health promotion has also been criticised for being western centric, particularly for lacking emphasis on cultural determinants of health (CDoH). 4 , 23 For example, CDoH from an Aboriginal and Torres Strait Islander perspective acknowledges that strong connection to culture and land generates a stronger sense of self‐identity, self‐esteem and resilience. 24 A core principle of health promotion is equity, however, it is usually within a dominant western paradigm where Indigenous Knowledge Systems (IKS) are often omitted from conventional public health approaches. 4 , 23 Therefore cultural determinants will be considered in the study as research shows that these determinants can provide invaluable insights into fostering the health of ecosystems and ensuring ecological sustainability. 4 , 23 , 25 , 26 , 27 , 28
The exploration of the intersection between health promotion and protecting the natural environment is a relatively emerging field of practice and research. For example, in 2011 a special edition in Health Promotion Journal of Australia opened discussion about the role of health promotion in addressing climate change. In 2015, The Lancet recognised that integrated approaches necessitate engagement with a number of stakeholders, specifically including ‘Indigenous peoples and local communities’ who can generate new insights and knowledge in the field of planetary health. 10 At the same time, the Intergovernmental science‐policy Platform for Biodiversity and Ecosystem Services (IPBES) attempted to construct a framework that embeds the western‐different knowledge systems (including IKS). 29 Other studies over a similar timeframe have explored the correlation between Aboriginal connection to country and wellbeing, and researchers have emphasised the need for health promotion to embrace IKS. 5 , 25 , 30 However, there lacks investigation in an Australian health promotion context about how to practically merge CDoH into socio‐ecological models that dominate contemporary health promotion theory and practice.
Following a comparative review of health‐related key socio‐ecological models that have been developed across time (n = 12) (Table 1), the Mandala of Health 31 was chosen to guide the study (Figure 1). This model is a longstanding and frequently used conceptual model published in 1986 in the field of public health and health promotion and popularised the focus on an ecological approach to wellbeing. 31 It displays a holistic system level understanding of the interrelationships between the individual and its surrounding environments. Some authors have already critiqued this model, suggesting that having the human at the centre of the model does not truly comprehend the true cycle of life. 27 , 32 Instead the model needs to be refined to incorporate more layers to demonstrate the different perspective of nature. However, this critique has only done theoretically and not through research, so this study aims to address this gap in literature.
TABLE 1.
Socio‐ecological frameworks
| Model | Description | Strengths/limitations |
|---|---|---|
| Ecological model 33 | Displays a dynamic equilibrium between host, environment and agent. |
|
| The Wellness Model 34 | Portrays health along a continuum with no end‐state. Although not explicitly in the model, other influencing factors to health are identified such as stress management, nutrition and physical activity. |
|
| Community Ecosystem Model 35 | A community‐orientated model that integrates community health and sustainable development. |
|
| Biopsychosocial Model of Health 36 | Emphasises the interdependence between psychological dispositions, biological processes and social behaviour in the context of health and illness. |
|
| Bronfenbrenner – Ecology of Human Development 37 | Interactions are displayed between the individual (centre) and environments at different levels; micro‐, meso‐, exo and macrosystem. |
|
| Ecological Model for Health Promotion 38 | Patterned behaviour is the outcome of interest with five levels of influence. |
|
| Ottawa Charter 21 | Identifies prerequisites for health including “stable ecosystems” and importance of advocate, enable and mediate as action areas. |
|
| The Health Map 55 | Depicts overarching influence of the global ecosystem on human health or ‘habitat’. Different facets of human life are reflected in spheres that move through social, economic and environmental categories. |
|
| The Butterfly Model of Health 39 | Capacity of achieving health is dependent on the balance between socioeconomic and biophysical environmental pressures. These are influenced by each other through the actions of individuals. |
|
| Transformation via Balanced Exchanges Model (T‐BE) 40 | Presents the exchanges between human and natural systems within the built and natural environment. Outcome of these exchanges is human health. |
|
| “Our Wellbeing” A holistic model of Indigenous Wellbeing 30 | Focuses on the interrelated nature of wellbeing and the environment. |
|
| Exploratory Framework for Aboriginal Victorian People's Wellbeing 30 | Provides visual understanding of Aboriginal peoples’ connection to/interaction with Country. Includes both Western and Aboriginal determinants that impact on wellbeing. |
|
FIGURE 1.
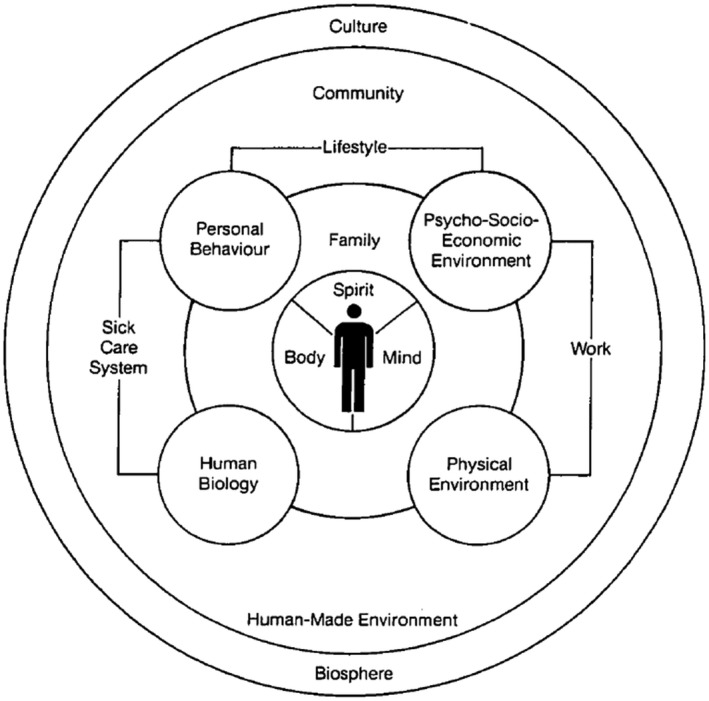
Mandala of Health 24
The conceptual model has been widely used in academia and practice, thus has high levels of utility to guide research and action in the field of health. However, to date no studies have been found that assesses the applicability of the Mandala of Health in the context of 21st century health promotion and how it resonates with contemporary health issues. This paper has two aims;
To explore the perceptions of health promotion and sustainability experts about the significance of key determinants of health, in particular EDoH and CDoH, in 21st century Australian health promotion.
To develop a revised Mandala of Health model which will provide an updated visual representation of the role of Australian health promotion in addressing contemporary health issues in the Anthropocene.
Little has been done in Australia to gain insights from health promotion and EDoH experts and academics working in the field, so this will play a vital role in creating such a framework. Using key informant interviews, health and sustainability experts discussed how they use and adapt models, such as the Mandala of Health, to address challenges of the Anthropocene. They were also asked for their critique and input in relation to the Mandala of Health which informed the creation of a revised framework.
2. METHODOLOGY
2.1. Design and sample
Qualitative description guided the study design. 41 This design was chosen as it provides a rich description of the data from the viewpoint of the participants which is suitable for the study aim. 42 The study was conducted with approval from Deakin University, Faculty of Health, Human research ethics committee (Project Number: HEAG‐H 46_2019).
The lead author conducted a comprehensive review, comparison and critique of available socio‐ecological models prior to starting data collection (Figure 2).
FIGURE 2.
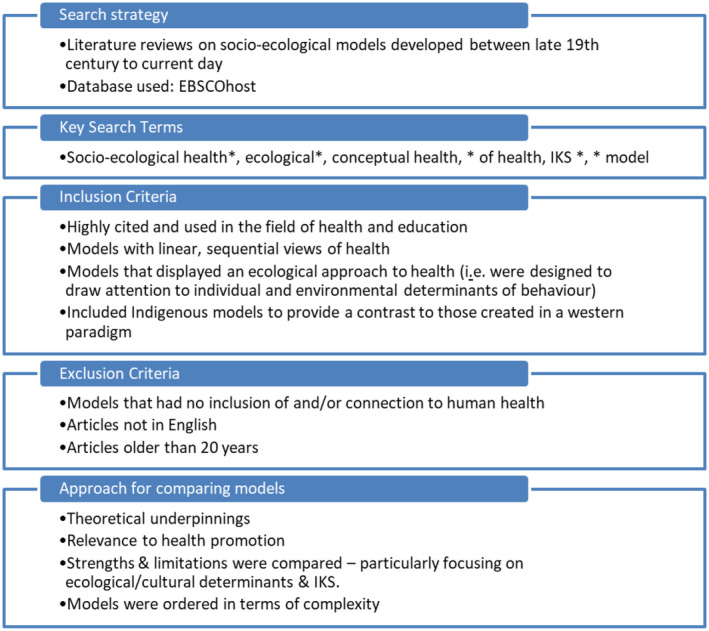
Literature review strategy
The relevance of the identified models to health promotion, the model's strengths and limitations in relation to planetary health and more specifically ecological and cultural determinants were compared (outlined in Table 1). Furthermore, the research team consulted with a lead author of the Mandala of Health as part of the decision‐making process. After much deliberation, the Mandala of Health was chosen to guide the study. It is holistic in nature with clear boundaries making it easy to identify the interactions between determinants. 43
The study employed a purposeful sampling strategy, in particular convenience sampling. 44 This sampling technique is valuable for capturing and describing a diverse range of perspectives that have emerged from adapting to different conditions. 44 Convenience sampling was deemed most appropriate due to time restraints where access and easy collection was necessary. 45 Eligibility criteria for participation were applied to enhance credibility. 45 The criteria for inclusion limited participants to: people with experience or qualifications with working at the nexus of health promotion and environmental management/sustainability; are currently employed as an academic or practitioner in Australia; are working from culturally and geographically diverse parts of Australia; and were suitable for inclusion in a low‐risk human research ethics approved project. This was established by their publicly available profiles.
Ten health experts (n = 5 Female; n = 5 Male) were recruited in the study including seven academics and three practitioners. Gender equity is a guiding principle of the authors research field, thus guided the approach to sampling. 46 The sample was limited to 10 participants as this study was intended for rich data and a deeper investigation which provides a snapshot for further research. These participants were identified from the chief investigators existing list of extensive national and international networks working in the nexus of health promotion and/or planetary health. Invitations took place via email and once individuals responded, they were sent a Plain Language Statement (PLS) and a Consent Form.
The lead author undertook all interviews. This had the benefit of minimising the risk of perceived bias from pre‐existing relationships (as the lead author did not have the existing relationships, the senior authors did). Furthermore, the PLS clearly states participants’ withdrawal rights as well as a statement outlining that the decision to participate will not affect any relationship the participant may have with the research team. A future research direction can build from this initial convenience sample and instead identify experts in socio‐ecological health and health promotion to gather further and broader input.
2.2. Data collection and analysis
Individual semi‐structured interviews were conducted either face‐to‐face at the participants’ workplace (n = 3) and via video (n = 5) or phone call (n = 2). Interviews are the most common form of data collection in a qualitative description study. 45 Semi‐structured interviews were used as they offer participants the opportunity to explore the issues they feel are important, creating a diverse range of data. 47 One interview per participant was audio‐recorded, with an average duration of 30‐60 minutes. After questions about demographics, a predetermined semi‐structured set of questions was followed which included investigating the value participants placed on CDoH and EDoH in research and practice, and what future strategies or priorities they believed were essential for health promotion to adapt to future health issues.
The audio recorded interviews were transcribed verbatim by the lead author. During transcription of the data all original names were replaced by pseudonyms and information was coded. Data were therefore re‐identifiable. A copy of the interview transcript was sent to participants to ensure accuracy and transparency prior to data analysis. 42 Participants were provided an opportunity to clarify or add further data they may deem important or valuable.
Transcriptions were coded thematically using NVivo (version 12); data analysis software. In keeping with qualitative description approach, thematic analysis techniques were used to stay close to the data. 41 Thematic analysis provides a rich, detailed and complex account of data that are qualitative in nature. 48
Analysis followed an iterative, inductive and deductive process. Initially, codes were inductively derived from the data then categorised into themes prior to any interpretation. 49 Once complete, the transcript was re‐read alongside the final list of themes to make sure codes were not taken out of context and analysis stayed close to the data. 50 Low inference was then used to analyse these themes and consider them in relation to the literature. 51
Finally, a deductive process was used to develop a revised model of the Mandala of Health. 50 Themes that referred to participants’ perspectives about ecological models, including the Mandala of Health, were collated. Using a deductive process, necessary changes to the original Mandala of Health were made that reflected these categorised themes and summarised participants’ perspectives.
To ensure rigour, the researchers implemented several strategies including; investigator triangulation during data analysis to obtain descriptive validity and ensuring accuracy and credibility 52 ; and reflexivity where authors actively engaged in critical self‐reflection when analysing and discussing findings. This ensured findings represented the views and perspectives of the participant and were not be affected by researcher bias. 53
Second, interpretative validity was achieved through participant member checking of the interview transcripts, key findings from the analysis and revised conceptual Mandala of Health model. 49 , 51 Interview transcripts were emailed to participants as well as an opportunity to provide any feedback on the revised Mandala of Health model (five participants provided further feedback).
3. RESULTS
The central finding was that CDoH and EDoH are fundamental determinants of health and essential components of health promotion theory and practice, however they both lack attention. This section unpacks these key findings in relation to four themes:
-
●
CDoH: the cultural context of communities and gaining further understanding of Indigenous cultures are crucial elements of health promotion.
-
●
EDoH: these determinants require more attention in the field of health promotion, there is a lack of understanding about the link between environment and health.
-
●
Conceptual models/ theoretical perspectives: participants gave examples of what they believed were useful and relevant socio‐ecological conceptual models other than the Mandala of Health.
-
●
The Mandala of Health: includes participants’ feedback when discussing the applicability and relevance of this model in today's society. A revised model was created in response to this feedback (Figure 2).
3.1. Cultural determinants of health
CDoH were described as a major influencing factor on how humans perceive the environment and the connection they have to nature. This was emphasised by one participant stating:
“If you look at what it is that’s driving ecological change, it fundamentally has to do with our cultural values.” (P10)
Participants believed culture is very context specific, so community consultation is essential to identify the cultural determinants of health of a particular population group for it then to be integrated into health promotion. When discussing CDoH, participants discussed the tendency of a western culture to view nature as separate, subserving and inferior to the human world. Participants labelled western society having “topophylic, not biophilic” (P5) connections to places. The perceived lack of understanding that western cultures have about the interdependent relationship between the natural and human world was contrasted to IKS. This was highlighted by one participant acknowledging:
“They [Indigenous cultures] have a kind of understanding that you don’t take more than what you need from their environment. We just do not have that.” (P5)
Participants mentioned that health promotion in both theory and practice need to engage with other cultures, learning from Traditional Owners of the land and incorporate IKS into contemporary way of living. Language was listed as an inhibiting factor in understanding other cultures and to having a connection to nature. Language through speech, stories and dance is just as valuable as empirical evidence which “we're only just now coming to grips with.” (P1).
3.2. Ecological determinants of health
It was suggested by participants that EDoH has been a neglected part of health promotion due to a lack of understanding among health professionals about EDoH compared to other determinants of health. The term “ecologically blind” was used by several participants, suggesting that health promotion's explicit focus on SDoH as hindered the role of EDoH. One participant articulated that:
“Since the 1980s we’ve been pushing a social determinants agenda and that to the detriment of ecological determinants. Now it’s time to stop being ecologically blind and bring it back into the picture.” (P5)
Participants thought EDoH need explaining and portrayed in a way that is easily understood and that is related to human health. Furthermore, it is essential to have SDoH and EDoH connected and not separate to aid the lack of understanding among health experts and the public. As explained by one participant:
“I think that is a more contemporary way to look at it ‐ meshing the social determinants with the ecological determinants. So that people can kind of get it a bit better.” (P5)
Participants’ responses questioned the principles of health promotion through their varying levels of frustration about the lack of leadership, urgency and action around EDoH. Participants felt that there was a lack of understanding of the non‐linear relationships between the environment and health in health promotion. Climate change was used as an example to demonstrate this. One participant's remark was that:
“Australia lags behind comparable countries when it comes to tackling the health impacts of climate change.” (P2)
This discussion linked back to CDoH as it was explained how ill‐health can be prescribed to the way that humans are impacting the natural environment. This refers to the lack of respect and connection to nature can cause repercussions for human health. For example, participants believed literature on climate change and EDoH is climate‐science focused with little attention to human health and wellbeing, which further distances people from the environment. As a strategy to overcome this, it was suggested to focus on the effects that the characteristics of the Anthropocene has upon human health. Participants suggested focusing on the effects of human health rather than the health of ecosystems as this is more easily understood by many people. If human health is perceived to be under threat, it creates a sense of urgency and action towards mitigating these environmental problems.
3.3. Conceptual models/theoretical perspectives
Overall, there was consensus among participants that conceptual models are a useful tool for communication and encouraging interdisciplinary work. However, due to the complexity of health promotion, participants found it difficult for one model to demonstrate the many nested systems of ecosystems, thus conceptual health models are more useful as a guide.
Models that were used by participants included the Donut Model by Raworth 6 which integrates both social and ecological determinants, emphasising ecological boundaries. It was described as a “modern comparator” (P10) to the Mandala of Health. In addition, The Health Map by Barton and Grant 54 was believed to be a good example of clearly demonstrating the interface of the natural and build environment, including EDoH, within a global ecological system. In summary, it appears that there are other helpful models of health beyond the Mandala of Health (for example Sallis’ Ecological Model of Active Living 55 ). However, this model was not included as it is purely a behavioural model with a focus on physical activity. The other models are encapsulating the relationships between humans and environment through a variety of mechanisms. Thus, this paper has a focus on relationships of human environments as opposed to the behaviours of humans to environments.
3.4. The mandala of health
Apart from one participant, all other participants were familiar with the Mandala of Health and all were able to provide critical and constructive feedback on its design, applicability and development. The “body, mind and spirit” was the most praised aspect of the model as well as the “onion ring” format which demonstrates the non‐linear relationships among the determinants of health. However, they found it so fully encompassing and broad that it was difficult to apply to a specific situation.
In response to participant critiques and suggested revisions synthesised with previous review of literature, this study developed a revised model of the Mandala of Health (Figure 3).
FIGURE 3.
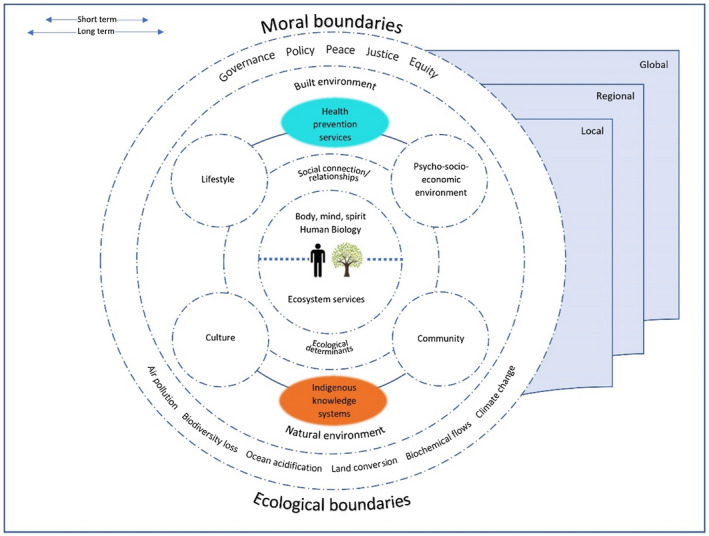
Revised Mandala of Health
The following section demonstrates participants interpretations of the Mandala of Health and subsequently recommendations for revision. Table 2 further clarifies how each enhancement of the Revised Mandala of Health was informed by participant responses and empirical literature.
TABLE 2.
Characteristics, participants perceptions and supporting literature focused on the Mandala of Health
| Characteristic of revised model | Participants perceptions of the original Mandala of Health | Supporting literature |
|---|---|---|
| Shared core of natural environment and human health, representing the co‐dependent relationship between these two components. | “this model has a weakness in the sense that it's got a person in the middle” (P7) |
Buse et al 4
|
| The broken lines throughout the model demonstrate the non‐linear relationships between all systems. | “the interactive nature of the systems that we're trying to deal with… seems to be missing from this.” (P7) |
VanLeeuwen et al 33
|
|
Explicitly labels EDoH and SDoH of health equally. |
“the last thing you want to do is have the ecological determinants here and the social determinants here and not talk. Not engage them.” (P3) |
Raworth 6 Jackson 57
|
| Embeds IKS as a cultural determinant of health to encourage engagement with the wider community |
“the two paradigms are quite difficult to reconcile at times.” (P2) “we have a lot to learn from Indigenous cultures” (P3) |
Ife & Tesoriero 58 Kingsley et al 25
|
| The term family changed to ‘social connections/relationship’ as it was considered too narrow for contemporary society. |
“I would probably make that change to family and friends…the social relationships.” (P9) “well I think in the 21st century, there's a range of questions to ask for what is family? How do you define family?” (P2) |
|
| Culture and community are on the same level and closer to the individual |
“I think we know that culture is deeply connected to an individual's experience in life and impacts and relates to health and wellbeing…an alternative framework would see that more closely connected to the individual, but their culture obviously applies cross society” (P2) |
Weir 23
|
| Top half is representing human systems, bottom half natural systems which is a praised feature of the original model. Adds in more detail of ecological boundaries (ie the biophysical environment). | “above the line you have essentially the social sciences, below the line you have the natural sciences. The whole model integrates the natural and social sciences which is what we have to do.” (P10) |
Hancock et al 1
|
| Includes policy and governance that influences every system | “I can't see policy. So much of policy can have flow on effect to the individual.” (P3) |
Patrick et al 5 World Health Organisation 21
|
| Lifestyle fully encompasses personal behaviour, activities and work | “the framework doesn't represent the extent to which personal behaviour is impacted by other societal forces.” (P2) |
|
| The term ‘sick‐care system’ changed to ‘health prevention services’ to be more inclusive of preventative healthcare/health promotion. | “If this is to be used for the purposes of health promotion, it would be good to highlight the things that actually contribute to that…what are the facilitators of it.” (P2) |
Patrick et al 18
|
| Time and geographical scales endeavours to demonstrate the multi‐dimensional and multi‐level spheres of health and the complex interactions between the determinants of health. |
“it's not just to be about the individual…it's on many levels and scales as well.” (P5) “you've got such a diverse multi‐scale focus of spatial, temporal, time lagged processes etc” (P8) |
Millennium Ecosystem Assessment 9 Prescott et al 3
|
| ‘Human‐made environment’ changed to ‘built environment’ to differentiate the built environment to the natural environment, as it was unclear of what constituted ‘human‐made’ environments in the original Mandala of Health. | “I just don't understand why human‐made environment is so prominent. Because ultimately humans influence everything. To separate out human‐made environments from the environment as a whole…is not that useful.” (P1) |
Hancock et al 1
|
| Addition of natural environment purposefully placed closer to the individual to capture the intimate relationship between them. |
The following quote describes the idea of ‘biosphere’ as seen in the original model: “It's all a construct of human aspects and there's just this ring around the outside that says environment or biosphere and it never sort of fully expressed that reciprocity or the fact that it's not just a vague undefined someone else's business settings for all human activity.” (P8) |
Steffen et al 2
|
The revised model's shared core of both human health and the health of natural ecosystems demonstrates the close interrelationship between them as compared to the original Mandala of Health model. Participants believed that the interactive nature of systems was missing in the original model, hence the authors used broken lines, as used in the Butterfly Model 39 to demonstrate this. Participants thought it would be beneficial to embed EDoH and SDoH to emphasise the equal importance of and the interconnection between these two fundamental determinants of health. EDoH include the life‐giving resources and processes of the natural environment, including but not limited to clean air, fertile soils, fresh water, marine aquatic systems, plants and animals. The term family was changed in the revised model as the definition of family has evolved to reflect anthropological approach to kinship which is not inclusive of other cultures. For example, a nuclear family structure is not a “natural” outcome for Indigenous kinship systems. 59
In the revised model, culture has moved from the outer ring to become closer to the individual as it is believed culture has equal influence as community has upon an individual's health and wellbeing. “Human‐made environment” as seen in the original model was found to be mis‐leading as it was believed that humans ultimately influence everything, including natural environments, so therefore every environment was “human‐made” as believed by participants.
Similar to any two‐dimensional model, it cannot portray the complexity of these interactions in their temporal and spatial domains. In particular, the relationships between elements of the figure do not fully capture the complex interactions that can occur among them. The revised model with time and geographical scales, endeavours to demonstrate the multi‐dimensional and multi‐level spheres.
4. DISCUSSION
The purpose of the study was to explore the application and relevance of conceptual socio‐ecological health models, such as the Mandala of Health, in guiding and facilitating dialogue to address the challenges of the Anthropocene for contemporary health promotion practice. Two of the key findings were the lack of attention to EDoH in health models as well as health promotion being criticised for being anthropocentric; that is the perspective that views humanity as the centre and core focus. 56
This study highlights the lack of both leadership and action regarding EDoH in the field of health promotion. Leadership is one of the five action areas for health promotion capacity building. 60 , 61 Capacity building allows health promotion to evolve and enhance its ability to address the underlying determinants of health. 60 In the context of the Anthropocene and the rapid ecological changes happening to the environment, capacity building is essential for health promotion to adapt and mitigate against the underlying causes of these environmental and health challenges that face the 21st century. 4
The lack of emphasis on EDoH compared to other determinants of health in health promotion as outlined by study participants is supported by literature. 1 , 62 The Ecological Determinant's of Health Framework expands the representation of humans to be part of a larger ecosystem in which survival depends on a balanced interrelationship and sustainable use of resources. 1 .Further exploration into the intersection of SDoH and EDoH is needed. For example, there is growing evidence of the socio‐economic disparities between those living in low income and marginalised communities and the possibility of them suffering from higher temperatures compared to those living in high income neighbourhoods. This could be a pathway for future research. Hancock and Spady 1 (p18) mention that “we need to revise our population health frameworks to become true socio‐ecological models that give greater weight to the EDoH and to interactions between them and the SDoH”. The revised model of the Mandala of Health developed in this study adds to the limited literature assessing current models exploring the Anthropocene. This research can encourage the development of innovative models that are better suited in designing sustainable solutions. However, conceptual models are to be treated as a tool that supports an understanding of a system that adapts to new understandings and different applications rather than a way to develop a theory and being a fixed paradigm. 63
Study participants identified culture as a major influencing factor on people and their environment. For example, facets of western culture (eg the use of cars as our predominant mode of transport, consumption of single‐use products and non‐recycling/throw‐aware culture of society) can negatively influence the natural environment and ultimately health. The sentiment of participants was there is a lack of understanding in health promotion about the importance of engaging with and learning from other cultures, specifically with Traditional Owners. Ife and Tesoriero 58 support this and identify the anthropocentric perspectives of western ideologies are barriers towards health promotion's ability to enact change in this domain. Furthermore, participants believed that incorporating IKS could assist with the lack of understanding among health experts regarding EDoH. There is much evidence regarding the value of Traditional Ecological Knowledge (TEK) and how it can contribute to conserving biodiversity and also provide solutions in reconciling the contrasting western and Indigenous paradigms. 64 , 65 TEK is defined as ‘a cumulative body of knowledge and beliefs, handed down through generations by cultural transmission, about the relationship of living beings (including humans) with one another and with their environment’ 66 (p3). Participants identified language as an inhibiting factor in engaging with other cultures. Perhaps this type of TEK, which is commonly shared by storytelling, arts and song, can be useful in enabling health promotion to evolve. 64 TEK is fluid and flexible, enabling itself to evolve with new understandings, contrasting to western knowledge systems that are accessible in written form and media in which context is often eliminated. 64 , 65
Although there are still challenges associated with incorporating these contrasting knowledge systems, future research could consider how health promotion practice can integrate IKS and cultural values. Further research could measure the health and environmental outcomes of health promotion practice which uses Indigenous understandings to address planetary health. This would help identify how health promotion practice might conflict with ecological sustainability goals and add to the much‐needed empirical research joining health, culture and the environment.
4.1. Strengths and limitations
It is important to recognise that the findings only provide a limited insight into such a complex discussion because of the qualitative nature of the study, small sample size and that the data were gathered from single interviews only. The study recruited more academics than practitioners, which was unintentional due to time restraints on response times, thus the results may not have been consistent with findings that might have been obtained from practitioners working in the field. As it was a low risk ethics approved, the sampling strategy was limited in its reach, for example, the study was unable to intentionally include people from Aboriginal and Torres Strait Islander backgrounds. Despite the inclusion of practitioners and academics with experience in culturally diverse communities, future research would benefit from a more deliberative approach to involving culturally and linguistically diverse participants. In summary, and nevertheless, the data collected does provide some new insights to the topic as a whole and creates a pathway for further research into this area.
5. CONCLUSION
This study has highlighted that there is room for improvement in Australian health promotion in terms of addressing EDoH and CDoH in theory and practice. It suggests the numerous challenges faced by health promoters in the context of the Anthropocene, but also the potential priorities and strategies to guide health promotion efforts in the future. The study has investigated the application and relevance of conceptual models, such as the Mandala of Health in the context of 21st century health issues and creates a pathway for future model development.
The paper highlights the view that, for too long humanity has not been effective in integrating or synergising efforts that meet the needs of humanity's health or the environment. The impacts being borne out of the Anthropocene era have shown those results. A paradigm shift in understanding our relationships with the environment and intrinsic connections to humans’ health is required. The determinants of health that are currently understood are found in disparate models. Thus, it is time to expand the dialogue and include more voices and perspectives in a collaborative, respectful manner. Using an established model such as the Mandala of Health has helped in leading the way to a more inclusive understanding of those determinants and a planetary health perspective. The current model proposed takes the understanding of EDoH and CDoH further and provides an opportunity for further dialogue and refinement to occur to benefit the promotion of health with due respect of the environment. If health promotion can better reflect the interrelationship between health and the natural environment, then health promotion can become an indispensable tool in offering solutions for anthropogenic environmental damage and better health outcomes for future generations to come. To strengthen this message even further future research could focus on other factors such as economic elements and have a larger sample size to validate these results.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ETHICS STATEMENT
Deakin University, Faculty of Health, Human research ethics committee (Project Number: HEAG‐H 46_2019).
Supporting information
Supplementary Material
ACKNOWLEDGEMENTS
The authors thank Dr Trevor Hancock for providing his insights into the making of the Mandala of Health framework during this study. The authors also thank the anonymous academics and practitioners for their willingness to participate in the study and the feedback they provided on the revised framework proposed in this paper. As non‐indigenous authors we acknowledge our role as advocates for the incorporation of Indigenous Knowledge Systems and for true self‐determination to be appropriately met in health promotion, the First Peoples of Australia must be included with full engagement in future research and practice on this topic or our words are meaningless.
Langmaid G, Patrick R, Kingsley J, Lawson J. Applying the Mandala of Health in the Anthropocene. Health Promot J Austral. 2021;32(S2):8–21. 10.1002/hpja.434
REFERENCES
- 1. Hancock T, Spady DW, Soskolne CL. Global Change and Public Health: addressing the ecological determinants of health: the report in brief. 2015.
- 2. Steffen W, Richardson K, Rockström J, et al. Planetary boundaries: Guiding human development on a changing planet. Science. 2015;347:1259855. 10.1126/science.1259855 [DOI] [PubMed] [Google Scholar]
- 3. Prescott SL, Logan AC. Prescott Susan, Logan Alan. Down to earth: planetary health and biophilosophy in the symbiocene epoch. Challenges. 2017;8(2):19. [Google Scholar]
- 4. Buse CG, Oestreicher JS, Ellis NR, et al. Public health guide to field developments linking ecosystems, environments and health in the Anthropocene. J Epidemiol Commun Health. 2017;72:420–5. [DOI] [PubMed] [Google Scholar]
- 5. Patrick R, Armstrong F, Hancock T, et al. Climate change and health promotion in Australia: navigating political, policy, advocacy and research challenges. Health Prom J Austr. 2019;30:295–8. 10.1002/hpja.278 [DOI] [PubMed] [Google Scholar]
- 6. Raworth K. A Doughnut for the Anthropocene: humanity's compass in the 21st century. Lancet Plan Health. 2017;1:e48–9. [DOI] [PubMed] [Google Scholar]
- 7. Berbés‐Blázquez M, González JA, Pascual U. Towards an ecosystem services approach that addresses social power relations. Curr Opin Environ Sustain. 2016;19:134–43. 10.1016/j.cosust.2016.02.003 [DOI] [Google Scholar]
- 8. Norgaard RB. Ecosystem services: from eye‐opening metaphor to complexity blinder. Ecol Econ. 2010;69:1219–27. [Google Scholar]
- 9. Millennium Ecosystem Assessment . Ecosystems and Human Well‐Being: synthesis. Washington, DC: Island Press; 2005. [Google Scholar]
- 10. Whitmee S, Haines A, Beyrer C, et al. Safeguarding human health in the Anthropocene epoch: report of The Rockefeller Foundation–Lancet Commission on planetary health. Lancet. 2015;386(10007):1973–2028 [DOI] [PubMed] [Google Scholar]
- 11. Houlden V, Weich S, Porto de Albuquerque J, et al. The relationship between greenspace and the mental wellbeing of adults: a systematic review. PLoS One. 2018;13(9):e0203000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Rojas‐Rueda D, Nieuwenhuijsen MJ, Gascon M, et al. Green spaces and mortality: a systematic review and meta‐analysis of cohort studies. Lancet Planetary Health. 2019;3:e469–e477. 10.1016/S2542-5196(19)30215-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Vandenberg M, van Poppel M, van Kamp I, et al. Visiting green space is associated with mental health and vitality: a cross‐sectional study in four European cities. Health Place. 2016;38:8–15. 10.1016/j.healthplace.2016.01.003 [DOI] [PubMed] [Google Scholar]
- 14. Kingsley J, Lawson J. Finding a unified understanding of nature. EcoHealth. 2015;12(4):551–2 [DOI] [PubMed] [Google Scholar]
- 15. Capaldi CA, Dopko RL, Zelenski JM. The relationship between nature connectedness and happiness: a meta‐analysis. Frontiers in Psychology. 2014;5:976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Albrecht G, Sartore GM, Connor L, et al. Solastalgia: the distress caused by environmental change. Austr Psychiatry. 2007;15(1_suppl):S95–S98. [DOI] [PubMed] [Google Scholar]
- 17. Horton R, Beaglehole R, Bonita R, et al. From public to planetary health: a manifesto. Lancet. 2014;383:8. [DOI] [PubMed] [Google Scholar]
- 18. Patrick R, Capetola T, Townsend M, et al. Health promotion and climate change: exploring the core competencies required for action. Health Promotion International. 2011;27:475–85. 10.1093/heapro/dar055 [DOI] [PubMed] [Google Scholar]
- 19. Health Promotion Journal of Australia . From the Editor. 2020. [cited 2020 Aug 4]. Available from: https://onlinelibrary.wiley.com/journal/22011617
- 20. International Union for Health Promotion and Education . IUHPE World Conference April 15. 2019. [cited 2020 Oct 1]. Available from; http://www.iuhpe2019.com
- 21. World Health Organisation . The Ottawa Charter for Health Promotion. World Health Organisation Regional Publication for Europe. 1986;1–7.
- 22. World Health Organisation . Closing the gap in a generation: health equity through action on the social determinants of health. 2008. Geneva. [DOI] [PubMed] [Google Scholar]
- 23. Weir JK. Country, native title and ecology. ANU E Press. 2012. [Google Scholar]
- 24. Lowitja Institute . Cultural determinants roundtable. 2014. www.lowitja.org.au/sites/default/files/docs/Cultural‐Determinants‐Roundtable‐Background‐Paper.pdf
- 25. Kingsley JY, Townsend M, Henderson‐Wilson C. Exploring Aboriginal people's connection to country to strengthen human‐nature theoretical perspectives. Adv Med Sociol. 2013;15:45–64. [Google Scholar]
- 26. Kellert SR. The Value of Life : Biological Diversity And Human Society. Washington, DC: Island Press; 1996. [Google Scholar]
- 27. Lawson J, Kingsley J. The language of Australian human‐ecological relationship: Identity, place and landscape. Brunn S, Kehrein R (eds) Handbook of the Changing World Language Map 2018. Springer, Cham; Journal Article 27/07/19. 2018. 1–16. 10.1007/978-3-319-73400-2_54-1 [DOI] [Google Scholar]
- 28. Burgess CP, Berry HL, Gunthorpe W, et al. Development and preliminary validation of the 'Caring for Country' questionnaire: measurement of an Indigenous Australian health determinant. Int J Equity Health. 2008;7(1):26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bamutaze Y. Revisiting socio‐ecological resilience and sustainability in the coupled mountain landscapes in Eastern Africa. Curr Opin Environ Sustain. 2015;14:257–65. 10.1016/j.cosust.2015.06.010 [DOI] [Google Scholar]
- 30. Kingsley J, Townsend M, Henderson‐Wilson C, et al. Developing an Exploratory Framework Linking Australian Aboriginal Peoples’ Connection to Country and Concepts of Wellbeing. International J Environ Res Public Health. 2013;10(2):678–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Hancock T, Perkins F. The mandala of health: a conceptual model and teaching tool. Health Promotion. 1985;24:8–10. [Google Scholar]
- 32. Seymour V. The human‐nature relationship and its impact on health: a critical review. Front Public Health. 2016;4:260. 10.3389/fpubh.2016.00260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. VanLeeuwen JA, Waltner‐Toews D, Abernathy T, et al. Evolving Models of Human Health Toward an Ecosystem Context. Ecosystem Health. 1999;5(3):204–19. [Google Scholar]
- 34. Travis JW, Callander MG. Wellness for helping professionals: creating compassionate cultures. Wellness Associates Publications. 1990.
- 35. Hancock T. Health, human development and the community ecosystem: three ecological models. Health Prom Int. 1993;8:41–7. 10.1093/heapro/8.1.41 [DOI] [Google Scholar]
- 36. Engel G. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. 10.1126/science.847460 [DOI] [PubMed] [Google Scholar]
- 37. Bronfenbrenner U. The Ecology of Human Development. Cambridge, Mass: Harvard University Press; 1979. [Google Scholar]
- 38. McLeroy KR, Bibeau D, Steckler A, et al. An ecological perspective on health promotion programs. Health Educ Q. 1988;15:351–77. [DOI] [PubMed] [Google Scholar]
- 39. Bormann F. ECOLOGY: a personal history. Ann Rev Energy Environ. 1996;21(1):1–29. [Google Scholar]
- 40. Coutts C, Forkink A, Weiner J. The portrayal of natural environment in the evolution of the ecological public health paradigm. Int J Environ Res Public Health. 2014;11:1005–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23:334–40. [DOI] [PubMed] [Google Scholar]
- 42. Bradshaw C, Atkinson S, Doody O. Employing a qualitative description approach in health care research. Global Qualit Nurs Res. 2017;4:2333393617742282. 10.1177/2333393617742282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Canadian Council on Social Determinants of Health . A Review of frameworks on the social determinants of health. 2015. [cited 2020 Oct 1]. Available from: http://ccsdh.ca/images/uploads/Frameworks_Report_English.pdf
- 44. Vitcu E, Lungu E, Vitcu L, et al. Multi‐stage maximum variation sampling in health promotion program evaluation. J Prevent Medi. 2007;15:5–18. [Google Scholar]
- 45. Creswell JW, Hanson WE, Clark VLP. Qualitative research designs. Counsel Psychol. 2007;35(2):236–64. [Google Scholar]
- 46. Charron DF. Ecohealth Research in Practice: Innovative Applications Of An Ecosystem Approach to Health. Ottawa: International Development Research Centre; 2012. [Google Scholar]
- 47. Nicholas C, Meghan C, Thomas G, et al. Key Methods in Geography. London, UK: , 3rd edn. Ringgold Inc; 2016. [Google Scholar]
- 48. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15:398–405. 10.1111/nhs.12048 [DOI] [PubMed] [Google Scholar]
- 49. Boyatzis RE. Transforming qualitative information: Thematic analysis and code development. Thousand Oaks, CA: Sage Publications Inc; 1998. [Google Scholar]
- 50. Crabtree BF, Miller WF. A template approach to text analysis: Developing and using codebooks. In: Crabtree BF, Miller WL, editors. Doing qualitative research. Thousand Oaks, CA: Sage Publications Inc; 1992. p. 93–109. [Google Scholar]
- 51. Sullivan‐Bolyai S, Bova C, Harper D. Developing and refining interventions in persons with health disparities: the use of Qualitative Description. Nurs Outlook. 2005;53:127–33. [DOI] [PubMed] [Google Scholar]
- 52. Johnson RB. Examining the validity structure of qualitative research. Education. 1997;118:282. [Google Scholar]
- 53. Marco CA, Larkin GL. Research ethics: ethical issues of data reporting and the quest for authenticity. Acad Emerg Med. 2000;7:691–4. 10.1111/j.1553-2712.2000.tb02049.x [DOI] [PubMed] [Google Scholar]
- 54. Barton H, Grant M. A health map for the local human habitat. J R Soc Prom Health. 2006;126:252–3. [DOI] [PubMed] [Google Scholar]
- 55. Sallis JF, Cervero RB, Ascher W, et al. An ecological approach to creating active living communities. Annu Rev Public Health. 2006;27:297–322. 10.1146/annurev.publhealth.27.021405.102100 [DOI] [PubMed] [Google Scholar]
- 56. Gagnon Thompson SC, Barton MA. Ecocentric and anthropocentric attitudes toward the environment. J Environ Psychol. 1994;14:149–57. 10.1016/S0272-4944(05)80168-9 [DOI] [Google Scholar]
- 57. Jackson SF. How can health promotion address the ecological determinants of health? Global Health Prom. 2017;24:3–4. 10.1177/1757975917747448 [DOI] [PubMed] [Google Scholar]
- 58. Ife J, Tesoriero F. Community development: community‐based alternatives in an age of globalisation. 3rd edn. Frenchs Forest, N.S.W.: Pearson Education; 2006. [Google Scholar]
- 59. Morphy F. Lost in translation?: Remote Indigenous households and definitions of the family. Family Matters. 2006;73: 23–31. [Google Scholar]
- 60. Department of Human Services . Integrated Health Promotion Resource Kit. 2003. [cited 2020 Apr 5]. Available from: https://www2.health.vic.gov.au/about/publications/policiesandguidelines/Integrated‐health‐promotion‐resource‐kit–‐Entire‐practice‐guide
- 61. Patrick R, Kingsley J. Exploring Australian health promotion and environmental sustainability initiatives. Health Prom J Austr. 2016;27:36–42. [DOI] [PubMed] [Google Scholar]
- 62. Meadows DH, Meadows DL, Randers J. Beyond the Limits: Global Collapse or a Sustainable Future. London: Earthscan Publications Ltd., 1992, p. xiv + 300. [Google Scholar]
- 63. Verburg PH, Dearing JA, Dyke JG, et al. Methods and approaches to modelling the Anthropocene. Glob Environ Change. 2016;39:328–40. 10.1016/j.gloenvcha.2015.08.007 [DOI] [Google Scholar]
- 64. Finn S, Herne M, Castille D. The value of traditional ecological knowledge for the environmental health sciences and biomedical research. Environ Health Perspect. 2017;125:1–9. 10.1289/EHP858 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Posey D. Cultural and Spiritual Values of Biodiversity. Nairobi, Kenya: Practical Action Publishing. 1999; p. 1. [Google Scholar]
- 66. Berkes F.Chapter 1: Traditional Ecological in Knowledge Perspective. International Development Research Centre, 1993, p. 1–9.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material