

Abstract
Objective:
To compare, through cone-beam computed tomography (CBCT), the root resorption and treatment efficiency of two different mini-implant-assisted modalities in intruding the maxillary incisors.
Materials and Methods:
Thirty-two adults who had deep bite and elongated maxillary incisors were randomly allocated to two groups: anterior mini-implant group (AMG) and posterior mini-implant group (PMG). In the AMG, approximately 40 g of force was applied per side with elastic chains from mini-implants placed between the lateral incisors and canines and in the PMG, with beta-titanium wires from mini-implants placed between the second premolars and first molars. This study was conducted on CBCT scans taken before intrusion and after 4 months of intrusion. Data were analyzed by means of a paired t-test, independent t-test, and Pearson’s correlation test.
Results:
One patient was excluded from the AMG due to mini-implant loosening. While the incisors showed a significant reduction in length and volume, this amount was greater in the AMG, especially in the central incisors (P < .05). Together with the mean intrusion rates of 0.62 and 0.39 mm/mo in the AMG and PMG respectively, the center of resistance of the incisors showed distal movement with labial tipping; these changes were greater in the PMG (P < .001). Volumetric root resorption was correlated with the amount of intrusion (P < .05).
Conclusions:
Intrusion anchoring from posterior mini-implants is preferred in cases of upright incisors, as the use of such mechanics directs the roots into the spongiosa where they undergo less root resorption and more labial tipping.
Keywords: Incisor intrusion, Cone-beam computed tomography, Mini-implant
INTRODUCTION
In recent years, the integration of mini-implants into intrusion mechanics has been proposed as an alternative technique to conventional mechanics, which have side effects on anchorage segments such as narrowing of the buccal segment1,2 and elongation and distal tipping of the posterior teeth.3,4
In published incisor intrusion studies, the mini-implants are located in the anterior region between the central incisors,5,6 the central and lateral incisors,7 or the laterals and canines.3,4,8,9 Though the effectiveness of anteriorly placed mini-implant-assisted intrusion mechanics have been investigated thoroughly, the information on root resorption of the incisors is limited, and no data has been published about incisor intrusion supported by posterior mini-implants.
Researchers have observed severe resorptive root damage from intrusive movements.10–12 Hence, a precise and unequivocal diagnostic method of imaging is needed to both prevent and monitor resorption, which is possible only by three-dimensional volumetric evaluation. Currently, cone-beam computed tomography (CBCT), as employed in rapid maxillary expansion and molar intrusion, is the leading tool for in vivo dental imaging in the field of root resorption research. However, no study using three-dimensional imaging techniques has been performed on root resorption and treatment efficacy as a consequence of incisor intrusion.
The purpose of this study was to compare, by means of CBCT, the amount of root resorption and treatment efficacy resulting from incisor intrusion supported by anterior vs posterior mini-implants.
MATERIALS AND METHODS
The study protocol was approved (10-5.1/13) by the Ethics Committee of the School of Medicine, Ege University, and written consent was obtained from the patients.
Included in the study were 32 adult subjects (20 female, 12 male) requiring maxillary incisor intrusion according to the following criteria: (a) overbite ≥5 mm, (b) Angle Class I or II discrepancy, (c) maxillary anterior crowding <5 mm, (d) maxillary incisors positioned below the functional occlusal plane, and (e) ≥5 mm of incisor display at rest. Patients were excluded if (a) the maxillary incisors had a history of any trauma or endodontic treatment, (b) the subject had any systemic disease or required periodic medication, or (c) the patient exhibited poor oral hygiene. Patients were allocated to two groups using RandList 1.2 (DatInf GmbH, Tübingen, Germany). The random number generator is based on the algorithm of Park and Miller with Bays-Durham correction at a 1:1 ratio.
Ten female and six male patients with a mean age of 19.31 ± 3.84 constituted the anterior mini-implant group (AMG), while the posterior mini-implant group (PMG) had 10 female and 6 male subjects with a mean age of 19 ± 3.48. An 0.018-inch Roth straight-wire appliance was bonded to the maxillary incisors. After being leveled and aligned, they were consolidated by figure-eight ligature ties of 0.017 × 0.025-inch stainless steel wires.
In the AMG, NeoAnchor Plus (Anchor Plus, Los Angeles, Calif) self-drilling mini-implants were inserted between the maxillary laterals and canines, and mini-implants of 1.4-mm diameter and length of 6 mm were chosen due to the limited interradicular space in the anterior segment. Elastic power chain (3M Unitek/ESPE, St Paul, Minn) was applied from the mini-implants to the archwire. In the PMG, the mini-implants were inserted between the second premolars and first molars. To minimize the disadvantage of the counterclockwise moment of mini-implant stability on the right side due to the planned intrusion mechanics and relying on the fact that the interradicular space was wider in this area, mini-implants of 1.6-mm diameter and 7-mm length were chosen. Burstone’s three-piece intrusion arch was modified, allowing the mini-implants to be integrated into this approach. One end of the 0.032-inch beta-titanium wire (TMA, Ormco, Orange, Calif) was slenderized so that it would fit through the hole in the mini-implant head while the other end was bent to be clinched to the anterior archwire. Force levels were adjusted at 40 g per side with force renewal at monthly intervals (Figure 1).
Figure 1.

Frontal and lateral views of the intrusive mechanics applied to the AMG and PMG.
CBCT scans were performed using Skyview volumetric scanner (Myray, Cefla Dental Group, Imola, Italy) with 10 mA, 90 kVp, and 300 µm of isotropic voxel size. Images were acquired before application of the intrusive force and after 4 months of intrusion.
CBCT data was saved in Digital Imaging and Communications in Medicine format and imported to Simplant 2011 software (Materialise Dental, Leuven, Belgium). To evaluate root resorption, linear and volumetric measurements were made between the cementoenamel junction and apex, followed by calculating percentages of respective root losses. To assess the efficiency of each intrusion modality, one angular and two linear measurements were carried out. The measurements were done in the sagittal slice, comprising the long axis of the tooth running through the incisal edge and apex. Sagittal sections were selected over axial or coronal sections because resorptions were delineated better in sagittal slices.13,14 The center of resistance (CR) of the central incisor was used to determine the amount of intrusion.15 The Cr determined on the preintrusion image was replicated onto the postintrusion image (Figure 2).
Figure 2.
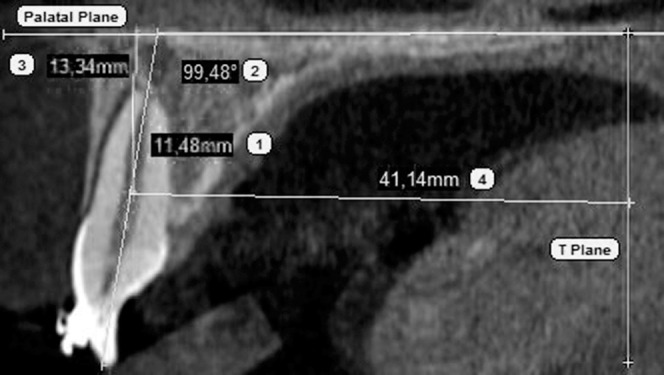
Linear and angular CBCT measurements: (1) 1 length, distance from apex to cementoenamel junction on long axis of the tooth (carried out for all the incisors); (2) 1-PP, angle between long axis of upper central incisor and palatal plane; (3) CR-PP, perpendicular distance from CR of the central incisor to palatal plane; (4) CR-T, perpendicular distance from CR of the central incisor to T plane (plane passing through posterior nasal spine and perpendicular to the palatal plane).
Because of incomplete tooth contour or teeth fused with the surrounding tissues after the initial automatic segmentation, further manual segmentation was carried out conservatively using the multiple-slice Edit tool for the axial, coronal, and sagittal slices with Add and Remove comments (Figure 3), making sure that only intact tooth morphology was present without surrounding structures (Figure 4). Additional segmentation was carried out to separate the root from the crown at the buccal cementoenamel junction with the incisal edge adjusted parallel to the floor (Figure 5).
Figure 3.

Manual segmentation in axial, coronal, and sagittal slices.
Figure 4.
Volumetric reconstruction after manual segmentation.
Figure 5.
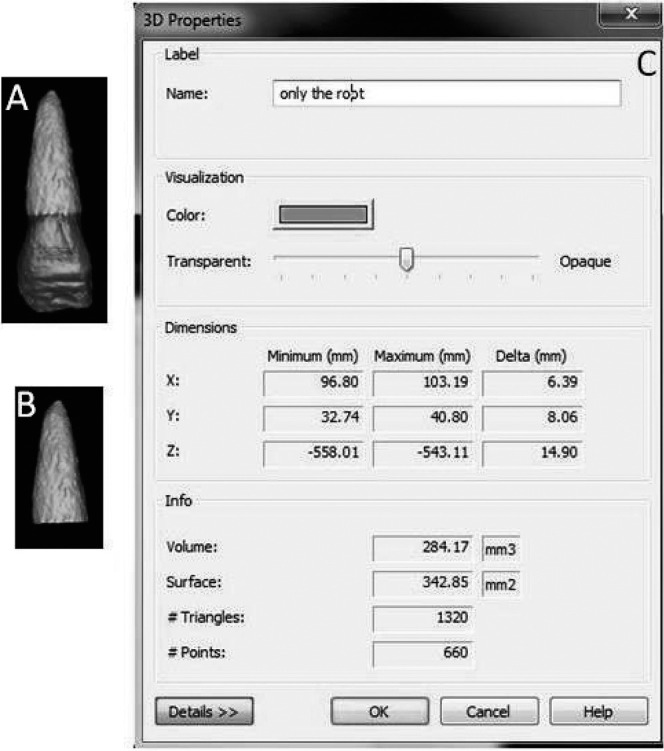
Volumetric measurements: (A) Reconstruction of whole tooth. (B) Separation of root from the crown. (C) Volume calculated.
According to the power analysis at the 0.05 level and 80% power (based on a 0.56-mm standard deviation and a 0.6-mm detectable group difference regarding intrusion rates3), the minimum sample size needed for each group was 14.
Statistical Analysis
To test reproducibility after 1 week, 20 images were reexamined using intraclass correlation coefficients. Normal distribution of pre- and postintrusion differences were observed by means of the Shapiro-Wilks test. The paired t-test was used for significance of mean changes within groups, and comparisons of mean changes in both groups were performed using an independent t-test. Also, to compare resorption between right and left incisors, an independent t-test was used. No statistically significant difference in resorption was observed, so the results were pooled. After this, percentages of length and volume losses were compared between the central and lateral incisors. Furthermore, the relationship between the amount of root resorption (124 teeth total) and available intrusion was analyzed with the Pearson correlation test. The data were analyzed using SPSS software (version 16.0, SPSS Inc, Chicago, Ill).
RESULTS
Thirty-one patients were included in the final assessment due to the loss of stability in one anterior mini-implant. High intraclass correlation coefficients were obtained with values of 0.994, 0.992, and 0.928 for angular, linear, and volumetric measurements, respectively.
Preintrusion and postintrusion volumetric, linear, and angular CBCT measurements are depicted in Table 1. Intragroup changes and intergroup differences due to treatment mechanics are presented in Table 2. All the incisors in both groups showed significant reduction in length and volume, with greater decreases in the AMG (P < .05), except for the right lateral incisor root volume (P > .05). When resorption percentages are considered, the central incisors displayed significantly more linear and volumetric decreases than did the laterals (P < .05, Table 3).
Table 1.
Preintrusion (T1) and Postintrusion (T2) CBCT Measurements of the Groups and Results of Statistical Assessmenta

Table 2.
Preintrusion (T1) and Postintrusion (T2) CBCT Measurement Changes and Intergroup Comparisonsa

Table 3.
Comparison of Central and Lateral Incisors With Regard to Their Linear and Volumetric Resorption Percentages

The incisors were intruded (decreased CR-PP), which was significantly greater in the AMG (P < .05). Also, the mean rates of intrusion were 0.62 mm/mo and 0.39 mm/mo, respectively, in the AMG and PMG. The CR of the incisors showed distal movement (decreased CR-T), with labial tipping (increased 1-PP) in both groups; these changes were greater in the PMG (P < .001). Volumetric root resorption exhibited a significant correlation with the amount of intrusion (P < .05, r = .416).
DISCUSSION
Since mini-implants reduce the need for complicated mechanics and eliminate the side effects of conventional methods, mini-implant-assisted incisor intrusion has gained popularity in recent years. In this context, it is important to weigh its intrusive ability against its possible side effects, as intrusion increases the chances of root resorption. In previous studies of root resorption occurring during maxillary incisor intrusion obtained with conventional methods and screened with periapical X-rays, resorption varied between 0.6 mm and 2.5 mm.16–20 Using utility arches, McFadden et al.18 found 0.84 mm of intrusion but 1.84 mm of resorption after termination of treatment (28.8 ± 7.4 months); Goel et al.19 observed 1.56 mm of root shortening for 1.60 mm of intrusion during a 4.32-month period. Using a Burstone intrusion arch, Costopoulos and Nanda16 observed 0.6 mm of resorption after 1.9 mm of apical movement of CR over 4.6 months with intrusive forces of 15 g per teeth. Also, Goerigk et al.20 reported similar results with 0.9 mm of resorption after 2.3 mm of intrusion in 4.3 months. However, Dermaut and De Munck17 reported far more root shortening, with resorptions of 2.8 mm (18%) after a mean CR intrusion of 3.6 mm after 6.7 months by a slightly modified Burstone technique, using an intrusive force of 25 g per tooth.
Applying intrusive forces of 100 g per side from the mini-implants placed between the laterals and centrals to the continuous archwire including also the buccal segments, Deguchi et al.7 measured 0.8 mm of root resorption after 6.6 months, with 3.6 mm of intrusion measured from the incisal edge. The present study revealed that loss of root length averaged between 0.85 mm and 1.19 mm in the AMG and between 0.70 mm and 0.83 mm in the PMG. Variations in the type (continuous or transient) and magnitude of force, duration of intrusion, and measuring methods in conventional radiographs can be responsible for the extent of root resorption observed, which at the same time leads to difficulty in comparing the above-mentioned studies with the present one. Furthermore, periapical radiographs to assess root loss present difficulties in landmark determination and standardization.21–24 Most importantly, since root resorption is a volume loss, three-dimensional quantitative methods would be much more precise in assessing root resorption than would two-dimensional methods.24–26 Unfortunately, no study has evaluated volumetrically the amount of root resorption occurring during incisor intrusion.
When volumetric measurements of root resorption were considered, root loss of each incisor was found to be significant, which held true for both groups. These decreases in volume were more in the AMG. In our opinion, this outcome was due to greater apical movement of the CR in the AMG, which is a known risk factor for resorption. This concept is reinforced by the significant correlation between the amount of root resorption and achieved intrusion. To our knowledge, only one other study17 has found a correlation between the amount of root resorption and magnitude of intrusion.
It should be emphasized that, while previous studies evaluated mostly the central incisors, the current study considered root resorption in the laterals as well. In our study, the centrals were subjected to more root resorption than were the lateral incisors in either groups, whereas Dermaut and De Munch17 found no difference between them. As suggested by De Vincenzo and Winn,27 close proximity of the roots to the cortical bone could account for greater resorption in the central incisors, because most of the patients in the present study had fairly retrusive incisors.
The literature includes only two studies3,4 using intrusion systems that incorporated only the four maxillary incisors with identically placed mini-implants as in the AMG. Since intrusion duration varies among those studies, it seems more reasonable to examine intrusion rates to compare treatment efficiency in the present study with previous ones. The rate of genuine intrusion measured from the CR of the incisors was 0.29 mm/mo in the Polat-Ozsoy et al.4 study and 0.35 mm/mo in Senisik and Turkkahraman’s.3 Intrusion rates in those studies with an intrusive force of 80 g–90 g were somewhat lower than that of the present study. This difference could be due to loosening of the mini-implant, resulting in lengthening of the intrusion period. While the mini-implant success rate was 90% in Senisik and Turkkahraman’s3 study, there is no information pertaining to this issue in that of Polat-Ozsoy et al.4 The intrusion rate of 0.39 mm/mo in our PMG could not be compared with any other study since no research was carried out using posteriorly located mini-implants.
More incisor flaring observed in the PMG may be related to the horizontal component of intrusive force, which was greater in this group. This horizontal component may have helped considerably decrease root resorption through further retraction of the incisor roots into the spongiosa, which can be preferable in cases with retrusive incisors. On the other hand, the larger vertical component of intrusive force in the AMG is responsible for greater intrusion rates than in the PMG.
When resorption percentages are considered, volumetric decreases are relatively smaller than length losses. Because of the root’s conical shape, volume loss in the apical region accounts for much smaller percentages compared with the whole root.
Although resorption occurred in all teeth, this degree of root resorption might be clinically irrelevant. Nonetheless, it could assume more importance if there had been additional loss of root material during the remaining span of orthodontic treatment, especially in the AMG.
Since we aimed to determine the amount of root resorption (entailing a great risk for root loss) attributable exclusively to intrusion, our observation period was fairly short in terms of treatment duration, which, incidentally, is an important shortcoming of this study.
CONCLUSIONS
The four maxillary incisors can be effectively intruded on sectional archwires with forces of 40 g per side from anteriorly or posteriorly located mini-implants.
The rates of both intrusion and root resorption were higher using the anteriorly placed, mini-implant-supported incisor intrusion method compared with intrusion rates resulting from the posteriorly placed mini-implants.
In patients demonstrating upright incisors, intrusion anchored from posterior mini-implants yielded more labial flaring and less root resorption than that anchored anteriorly.
Since both incisor intrusion and distalization are possible with mechanics anchoring from posterior mini-implants, usage of mini-implants in this manner presents an alternative to anterior mini-implants in deep-bite cases with premolar extraction. Further studies need to be conducted to observe the pros and cons of this approach.
REFERENCES
- 1.Burstone CJ. Biomechanics of deep overbite correction. Semin Orthod. 2001;7:26–33. [Google Scholar]
- 2.van Steenbergen E, Burstone CJ, Prahl-Andersen B, Aartman IH. Influence of buccal segment size on prevention of side effects from incisor intrusion. Am J Orthod Dentofacial Orthop. 2006;129:658–665. doi: 10.1016/j.ajodo.2004.06.039. [DOI] [PubMed] [Google Scholar]
- 3.Senisik NE, Turkkahraman H. Treatment effects of intrusion arches and mini-implant systems in deepbite patients. Am J Orthod Dentofacial Orthop. 2012;141:723–733. doi: 10.1016/j.ajodo.2011.12.024. [DOI] [PubMed] [Google Scholar]
- 4.Polat-Ozsoy O, Arman-Ozcirpici A, Veziroglu F, Cetinsahin A. Comparison of the intrusive effects of miniscrews and utility arches. Am J Orthod Dentofacial Orthop. 2011;139:526–532. doi: 10.1016/j.ajodo.2009.05.040. [DOI] [PubMed] [Google Scholar]
- 5.Ohnishi H, Yagi T, Yasuda Y, Takada K. A mini-implant for orthodontic anchorage in a deep overbite case. Angle Orthod. 2005;75:444–452. doi: 10.1043/0003-3219(2005)75[444:AMFOAI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Kim TW, Kim H, Lee SJ. Correction of deep overbite and gummy smile by using a mini-implant with a segmented wire in a growing Class II division 2 patient. Am J Orthod Dentofacial Orthop. 2006;130:676–685. doi: 10.1016/j.ajodo.2005.07.013. [DOI] [PubMed] [Google Scholar]
- 7.Deguchi T, Murakami T, Kuroda S, Yabuuchi T, Kamioka H, Takano-Yamamoto T. Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. Am J Orthod Dentofacial Orthop. 2008;133:654–660. doi: 10.1016/j.ajodo.2006.04.047. [DOI] [PubMed] [Google Scholar]
- 8.Upadhyay M, Nagaraj K, Yadav S, Saxena R. Mini-implants for en masse intrusion of maxillary anterior teeth in a severe Class II division 2 malocclusion. J Orthod. 2008;35:79–89. doi: 10.1179/146531207225022491. [DOI] [PubMed] [Google Scholar]
- 9.Polat-Ozsoy O, Arman-Ozcirpici A, Veziroglu F. Miniscrews for upper incisor intrusion. Eur J Orthod. 2009;31:412–416. doi: 10.1093/ejo/cjn122. [DOI] [PubMed] [Google Scholar]
- 10.Harris DA, Jones AS, Darendeliler MA. Am J Orthod Dentofacial Orthop. Vol. 130. Volumetric analysis of root resorption craters after application of controlled intrusive light and heavy orthodontic forces: a microcomputed tomography scan study; 2006. Physical properties of root cementum: part 8; pp. 639–647. [DOI] [PubMed] [Google Scholar]
- 11.Faltin RM, Faltin K, Sander FG, Arana-Chavez VE. Ultrastructure of cementum and periodontal ligament after continuous intrusion in humans: a transmission electron microscopy study. Eur J Orthod. 2001;23:35–49. doi: 10.1093/ejo/23.1.35. [DOI] [PubMed] [Google Scholar]
- 12.Han G, Huang S, Von den Hoff JW, Zeng X, Kuijpers-Jagtman AM. Root resorption after orthodontic intrusion and extrusion: an intraindividual study. Angle Orthod. 2005;75:912–918. doi: 10.1043/0003-3219(2005)75[912:RRAOIA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Lermen CA, Liedke GS, da Silveira HE, da Silveira HL, Mazzola AA, de Figueiredo JA. Comparison between two tomographic sections in the diagnosis of external root resorption. J Appl Oral Sci. 2010;18:303–307. doi: 10.1590/S1678-77572010000300019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.da Silveira HL, Silveira HE, Liedke GS, Lermen CA, Dos Santos RB, de Figueiredo JA. Diagnostic ability of computed tomography to evaluate external root resorption in vitro. Dentomaxillofac Radiol. 2007;36:393–396. doi: 10.1259/dmfr/13347073. [DOI] [PubMed] [Google Scholar]
- 15.Ng J, Major PW, Heo G, Flores-Mir C. True incisor intrusion attained during orthodontic treatment: a systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2005;128:212–219. doi: 10.1016/j.ajodo.2004.04.025. [DOI] [PubMed] [Google Scholar]
- 16.Costopoulos G, Nanda R. An evaluation of root resorption incident to orthodontic intrusion. Am J Orthod Dentofacial Orthop. 1996;109:543–548. doi: 10.1016/s0889-5406(96)70140-3. [DOI] [PubMed] [Google Scholar]
- 17.Dermaut LR, De Munck A. Apical root resorption of upper incisors caused by intrusive tooth movement: a radiographic study. Am J Orthod Dentofacial Orthop. 1986;90:321–326. doi: 10.1016/0889-5406(86)90088-0. [DOI] [PubMed] [Google Scholar]
- 18.McFadden WM, Engstrom C, Engstrom H, Anholm JM. A study of the relationship between incisor intrusion and root shortening. Am J Orthod Dentofacial Orthop. 1989;96:390–396. doi: 10.1016/0889-5406(89)90323-5. [DOI] [PubMed] [Google Scholar]
- 19.Goel P, Tandon R, Agrawal KK. A comparative study of different intrusion methods and their effect on maxillary incisors. J Oral Biol Craniofac Res. 2014;4:186–191. doi: 10.1016/j.jobcr.2014.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Goerigk B, Diedrich P, Wehrbein H. Intrusion of the anterior teeth with the segmented-arch technic of Burstone—a clinical study. Fortschr Kieferorthop. 1992;53:16–25. doi: 10.1007/BF02165141. [DOI] [PubMed] [Google Scholar]
- 21.Durack C, Patel S, Davies J, Wilson R, Mannocci F. Diagnostic accuracy of small volume cone beam computed tomography and intraoral periapical radiography for the detection of simulated external inflammatory root resorption. Int Endod J. 2011;44:136–147. doi: 10.1111/j.1365-2591.2010.01819.x. [DOI] [PubMed] [Google Scholar]
- 22.Patel S, Dawood A, Wilson R, Horner K, Mannocci F. The detection and management of root resorption lesions using intraoral radiography and cone beam computed tomography—an in vivo investigation. Int Endod J. 2009;42:831–838. doi: 10.1111/j.1365-2591.2009.01592.x. [DOI] [PubMed] [Google Scholar]
- 23.Sherrard JF, Rossouw PE, Benson BW, Carrillo R, Buschang PH. Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofacial Orthop. 2010;137:100–108. doi: 10.1016/j.ajodo.2009.03.040. [DOI] [PubMed] [Google Scholar]
- 24.Katona TR. Flaws in root resorption assessment algorithms: role of tooth shape. Am J Orthod Dentofacial Orthop. 2006;130:19–27. doi: 10.1016/j.ajodo.2006.06.012. [DOI] [PubMed] [Google Scholar]
- 25.Wang Y, He S, Yu L, Li J, Chen S. Accuracy of volumetric measurement of teeth in vivo based on cone beam computer tomography. Orthod Craniofac Res. 2011;14:206–212. doi: 10.1111/j.1601-6343.2011.01525.x. [DOI] [PubMed] [Google Scholar]
- 26.Chan EK, Darendeliler MA. Exploring the third dimension in root resorption. Orthod Craniofac Res. 2004;7:64–70. doi: 10.1111/j.1601-6343.2004.00280.x. [DOI] [PubMed] [Google Scholar]
- 27.DeVincenzo JP, Winn MW. Maxillary incisor intrusion and facial growth. Angle Orthod. 1987;57:279–289. doi: 10.1043/0003-3219(1987)057<0279:MIIAFG>2.0.CO;2. [DOI] [PubMed] [Google Scholar]