

Abstract
Objective:
To investigate the effects of flapless micro-osteoperforation and corticision on the rate of orthodontic tooth movement in rats.
Materials and Methods:
Forty-five 8-week-old male Sprague-Dawley rats were divided into the following groups: micro-osteoperforation and orthodontic force (MOP + F), corticision and orthodontic force (C + F), and orthodontic force only (F, control). The left maxillary first molars were pulled forward with a force of 50 g. Flapless surgical interventions were conducted in the MOP + F and C + F groups. The total duration of the experiment was 6 weeks. Alveolar bone density and the number of osteoclasts were evaluated using microcomputed tomography and histologic examination, respectively.
Results:
The tooth movement distance was significantly higher in both experimental groups than in the control group. Bone density and bone mineral density decreased in the MOP + F and C + F groups. The number of osteoclasts in the MOP + F and C + F groups was significantly higher than in the control group F.
Conclusion:
The two minimally invasive flapless surgical interventions increased bone remodeling and osteoclast activity and induced faster orthodontic tooth movement for at least 2 weeks in rats. No differences were observed between the outcome of flapless micro-osteoperforation and corticision in the rats.
Keywords: Micro-osteoperforation, Corticision, Orthodontic tooth movement
INTRODUCTION
Most patients prefer a short orthodontic treatment time. Methods such as local/systemic pharmaceutical administration as well as physical and mechanical stimulation have been reported to accelerate tooth movement.1,2 However, these methods might not be applicable to daily clinical practice because of their side effects and because their outcomes await validation.3–5 Over the past decade, the regional acceleratory phenomenon (RAP) induced by surgical trauma has received considerable emphasis for reducing the treatment time.6 Wilcko and colleagues6,7 have combined alveolar corticotomies with bone augmentation to accelerate tooth movement. However, the surgical trauma associated with this technique is considerably high, resulting in the limited application of this technique currently.
Researchers have attempted to identify minimally invasive surgical procedures for inducing RAP, and it could be induced by micro-osteoperforation8 and corticision.9 In previous studies, some showed no significant improvement after the surgical operations,10 whereas others showed significant acceleration in tooth movement.8,9,11 However, the results are not comparable because the surgical approaches used in these studies were different. Some researchers have performed mucoperiosteal flap elevation but some have not. In addition, mucoperiosteal flap surgery could induce RAP.12
The purpose of this study was to compare acceleration in tooth movement between micro-osteoperforation and corticision without flap elevation by measuring the movement distance, alveolar bone density changes, and number of osteoclasts.
MATERIALS AND METHODS
Forty-five 8-week-old male Sprague-Dawley rats (BioLASCO Taiwan Co, Ltd, Taipei, Taiwan) weighing 400–500 g were randomly divided into three groups—group 1: micro-osteoperforation + orthodontic force (MOP + F); group 2 : corticision + orthodontic force (C + F); and group 3 (control) : orthodontic force only (F).
Ethical approval for the complete study protocol was obtained from the Animal Center of Taipei Medical University (No. LAC-2014-0083). All rats were housed in the same room at constant room temperature (22°C ± 2°C), humidity (40%–70%), and a 12-hour:12-hour light–dark cycle. They were fed a standard diet of hard pellets and water.
Before orthodontic appliance delivery and surgery, a single dose of 25 mg/kg tiletamine-zolazepam (Zoletil 50, Virbac Inc, Carros, France) and 11.66 mg/kg xylazine (Rompum, Bayer Inc, Kyonggi-do, Korea) was used intraperitoneally to induce general anesthesia. In each rat, orthodontic force was applied using two incisors as anchorage to move the left maxillary first molar forward (Figure 1), and a closed-coil nickel-titanium spring (Sentalloy Coil Springs, Densply, Bohemia, NY, USA) was used to deliver a force of 50 g. A 0.008-inch stainless steel ligature wire was passed through the left maxillary first and second molars. To prevent the closed-coil spring from being dislodged, we tightly threaded the wire by using a pair of ligature wire tying pliers (YS-506, YDM Co, Tokyo, Japan). The other head of the closed-coil spring was threaded using a second stainless wire and activated to the left maxillary incisor. Before the wire was tied to the incisors, grooves of 0.5 mm depth were gingivally created on the distal and facial surfaces of the two incisors to prevent the wire from slipping off the incisors. For optimal reinforcement of the anchorage, the two maxillary incisors were ligated together with another wire. Furthermore, resin was applied to the two incisors. Finally, the mandibular incisors were cut with a disk to prevent appliance breakdown. The distance between the left maxillary incisor and the left maxillary first molar was measured weekly using a digital ruler with a precision of 0.01 mm when the rats were under anesthesia. The reduced distance between the upper left first molar and incisor was regarded as the distance by which the molar was moved forward. All measurements were conducted three times by the same investigator to eliminate bias, and the average value was calculated.
Figure 1.

Appliances used for molar protraction. (A) Intraoral view. (B) Occlusal view. (C) Lateral view.
Corticision was conducted on the line angle of the palatal vault 5 mm mesial to the left maxillary first molar (Figure 2). A blade (4 mm in length and 0.4 mm in width) was positioned on the gingiva at the incision. Subsequently, a hammer was used to gently push the blade through the cortical bone until it reached the cancellous bone. Rats in the MOP + F group received three small perforations measuring 0.25 mm in diameter and 0.25 mm in depth. These perforations were created using a ¼ round bur with a low-speed handpiece. The distance between the perforations was 1 mm. Similar to the perforations in the corticision group, the perforations were also positioned 5 mm mesial to the first molar.
Figure 2.

(A) Schematic of micro-osteoperforation and (B) corticision.
We used microcomputed tomography (micro-CT) to examine the alterations in the bone volume fraction (BV/TV), which is the ratio of the volume of mineralized tissue considered to be bone (BV) to the total tissue volume that is enclosed by the contours (TV), and the bone mineral density (BMD) at weeks 3 and 6 (T3 and T6, respectively).
The hemimaxillae were fixed in 10% formalin for 7 days to minimize tissue damage after removal of the mandibles and disposal of the soft tissue. Subsequently, all specimens were subjected to micro-CT scanning (SkyScan1176, Kontich, Belgium) at 65 kV and 385 µA. We used a standard hydroxyapatite for measurement of the same parameters at baseline. The region of interest (ROI) was mineralized tissue surrounding the left maxillary first and second molars (Figure 3). The ROI encircled a cross section at the middle of the roots of the left maxillary first and second molars. The bone density of the region was defined as BV/TV. In addition, the BMD was defined as the average mineral density of only those voxels considered to be bone.
Figure 3.

Micro-CT images depicting the ROI. (A) Lateral view of the left maxilla. A cross section was made at the middle of the roots (dotted line). (B) Axial view of the cross section. The bone density of the experimental side (left) was lower than that of the contralateral side (right). (C) The ROI encircled the roots of the first and the second molars, and the root images (dotted circled areas) were excluded.
After micro-CT scans, all hemimaxillae were decalcified in 10% EDTA (ethylenediaminetetraacetic acid) solution for 6 weeks. The samples were rinsed under tap water for 3 hours. A cross section was made at the middle of the roots. The specimens were embedded in paraffin wax to obtain a section with a thickness of 5 µm, and the sections were then stained with hematoxylin and eosin (H&E). According to previous studies,13,14 osteoclasts were morphologically identified as large multinucleated cells in close contact with alveolar bone on H&E staining (Figure 4). The area surrounding the mesiopalatal root of the left maxillary first molar was divided into mesial and distal halves, and osteoclasts in the mesial halves, that is, the compression sides, were counted.
Figure 4.

Osteoclasts were morphologically identified as large multinucleated cells on H&E staining. AB indicates alveolar bone; PDL, periodontal ligament; and TR, tooth root. Arrows: osteoclasts.
Statistically significant differences between the control and experimental groups were assessed using one-way analysis of variance. Post hoc Tukey tests were performed to identify the significant differences between the means. We used SAS version 9.4 software (SAS Institute Inc, Cary, NC, USA) or all statistical analyses. A value of P < .05 indicated a statistically significant difference.
RESULTS
The distance of orthodontic tooth movement in the C + F and MOP + F groups (Figure 5A) was increased compared with those in the F group at week 1 (T1); however, the differences were not statistically significant (P = .08). At week 2 (T2), the distance of tooth movement in the C + F (1.43 ± 0.38 mm) and MOP + F (1.39 ± 0.49 mm) groups was significantly greater (P = .02) than that in the F group (0.93 ± 0.49 mm). The distance of total tooth movement was greater in the two experimental groups than in the control group. When we compared the two different surgical approaches used in the experimental groups, no significant differences were observed in the weekly tooth movement between the MOP + F and C + F groups within 6 weeks. When we converted the distances to velocities, the velocities of orthodontic tooth movement were higher in the experimental groups than in the control group at T1 and T2; however, a significant difference was observed only at T2 (Figure 5B).
Figure 5.

(A) Distance of orthodontic tooth movement, P < .05, at T2. (B) Velocity of tooth movement (mm/week), P < .05, at T2.
The BV/TV decreased in the MOP + F (55.52 ± 15.52%) and C + F (58.07 ± 4.92%) groups at week 3 (T3) (Figure 6); however, the differences were not statistically significant compared with the BV/TV in the F group (60.56 ± 11.45%). At week 6 (T6), the data indicated that BV/TV decreased in all three groups, with statistically significant differences (P = .02) among the MOP + F (46.02 ± 5.60%), C + F (54.6 ± 9.21%), and F (59.48 ± 7.53%) groups.
Figure 6.

BV/TV and BMD (*P < .05). Our results showed that BV/TV decreased in the MOP + F and C + F groups compared with the F group at T3. Moreover, a statistically significant difference (P = .02) was observed between the MOP + F and F groups at T6. The BMD decreased significantly (P < .05) in the MOP + F and C + F groups at both time points.
Regarding the changes in BMD (Figure 6), we determined a significant decrease in BMD (P < .05) between both experimental groups and the control group at T3 and T6. However, when we compared the two surgical approaches, the changes in BMD were not significantly different between the MOP + F and C + F groups.
We also examined BV/TV and the BMD over the contralateral sides (the right side of the maxilla). The results indicated that the contralateral sides exhibited higher values than the experimental sides (Table 1). Furthermore, no differences were observed among the groups and between the two time points (T3 and T6). Thus, the orthodontic force with or without minor surgery on the left side of the maxilla did not influence the contralateral side.
Table 1.
BV/TV and BMD Over the Contralateral Side at 3 Weeks (T3) and 6 Weeks (T6) After Force Applicationa

The number of the osteoclasts was significantly higher (P < .05) in the MOP + F and C + F groups than in F group at T3 (Figure 7). At T6, no statistically significant differences were observed. From H&E stained sections, root resorption was more likely to occur in the F group than in the MOP + F and C + F groups (Figure 8) at T3 and T6. In addition, the severity of root resorption was higher at T6 than at T3 in all three groups.
Figure 7.
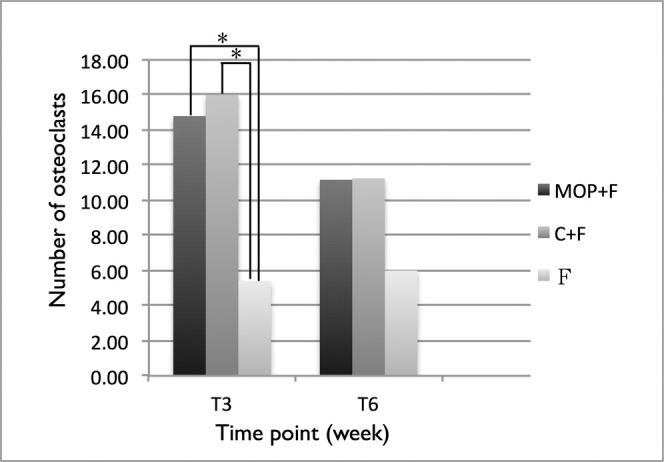
Number of osteoclasts. The number of osteoclasts increased significantly in the MOP + F and C + F groups at T3.
Figure 8.

Arrows indicating root resorption in H&E-stained sections. Upper row: T3; Lower row: T6.
DISCUSSION
The results of the present study reveal that the most significant difference in the orthodontic tooth movement distance occurred at week 2. This distance was 1.54 and 1.49 times faster in the C + F and MOP + F groups, respectively, compared with the F group. The amount of total tooth movement was 1.14 and 1.11 times greater in the MOP + F and C + F groups, respectively, compared with the F group at week 6. Furthermore, no significant difference was observed in tooth movement between the MOP + F and C + F groups at any time point throughout the experiment.
In a previous animal study by Teixeira et al.,11 orthodontic tooth movement on day 28 after three micro-osteoperforations with flap surgery in experimental rats was 2.13 times faster than in the control group. Baloul et al.8 reported that tooth movement was 1.3 times faster on day 42 after 10 micro-osteoperforations with flap elevation in rats. Cho et al.15 reported that the tooth movement distance increased to 4.41 times and 2.44 times in the maxilla and mandible, respectively, after applying 24 decortication dots with flap surgery in dogs. In the present study, the results showed that the tooth movement distance was 1.54 times and 1.11 times faster in the C + F group than in the control group at week 3 and week 6, respectively, and these values are less than those observed in previous studies. The possible reason for this discrepancy might be that the magnitude of the RAP is proportional to the magnitude of the insult.16 Our flapless surgical operations caused fewer injuries, leading to less tooth movement acceleration.
The peak tooth movement velocity was observed in all three groups at week 1 (T1), implying that this was the initial phase of orthodontics tooth movement.17 From T1 to T2, all three groups exhibited a decreased velocity of orthodontic tooth movement, implying a lag phase.17,18 However, this result is not consistent with that of Baloul et al.,8 who determined that only the control group (without decortication) exhibited a lag phase. They used rat models and applied an orthodontic force of 25 g to observe the effects of flap and multiple micro-osteoperforation surgery, inducing a more severe injury with a lighter force; therefore, a lag phase might not have appeared. Our result is consistent with that of Mostafa et al.,19 who reported that the experimental and control groups exhibited a similar orthodontic tooth movement pattern: initial, lag, and postlag phase. However, Mostafa et al. used 400 g of force, an unusually heavy force that might have induced a lag phase in their study on dogs. The results are consistent possibly because an orthodontic force of 50 g was applied in the present study. A heavy force for rats possibly caused the compression and hyalinization of the periodontal; ligament, inducing a lag phase in all three groups.
Rats subjected to both micro-osteoperforation and corticision showed significant declines (P < .05) in BMD at T3 and T6. Reduced bone mineralization may indicate a highly active bone catabolism. Furthermore, this indicates that the RAP occurred after the two surgical operations.
As per our histologic examination results, the osteoclast activity in the experimental groups was higher than that in the control group. Moreover, minor surgeries resulted in lesser root resorption than occurs in conventional orthodontic tooth movement. This phenomenon is notable but may require verification in future studies.
Some studies16,20,21 have concluded that the RAP occurs approximately 4 months after corticotomy. However, in the present study, the RAP was observed within 2 weeks after flapless micro-osteoperforation and corticision in rats. The limited duration of the RAP indicates that second or third surgical operations may be required for reinducing RAP and ensuring faster orthodontic tooth movement. Therefore, we may be required to conduct minor surgical operations only over limited mouth regions rather than the entire mouth, for example, large space closure, molar protraction, molar intrusion, wisdom teeth uprighting or protraction, unilateral arch expansion, and difficulty in moving the teeth.
Considering the differences in tissue structure, life cycle, and physiological responses for tooth movement between humans and rats, the optimal biomechanical force systems required for humans are unknown, and the optimal interval between each appointment warrants further explanation. Therefore, additional studies must be conducted to identify the effects of flapless micro-osteoperforation and corticision on humans.
CONCLUSIONS
The two minor flapless surgical operations increased bone remodeling and osteoclast activity and induced faster orthodontic tooth movement for at least 2 weeks in rats.
No obvious differences were observed between flapless micro-osteoperforation and corticision in rats.
ACKNOWLEDGMENT
We highly appreciate the valuable comments of the reviewers.
REFERENCES
- 1.Davidovitch Z, Finkelson MD, Steigman S, Shanfeld JL, Montgomery PC, Korostoff E. Electric currents, bone remodeling, and orthodontic tooth movement. II. Increase in rate of tooth movement and periodontal cyclic nucleotide levels by combined force and electric current. Am J Orthod. 1980;77:33–47. doi: 10.1016/0002-9416(80)90222-5. [DOI] [PubMed] [Google Scholar]
- 2.Leiker BJ, Nanda RS, Currier GF, Howes RI, Sinha PK. The effects of exogenous prostaglandins on orthodontic tooth movement in rats. Am J Orthod Dentofacial Orthop. 1995;108:380–388. doi: 10.1016/s0889-5406(95)70035-8. [DOI] [PubMed] [Google Scholar]
- 3.Yamaguchi M, Kasai K. Inflammation in periodontal tissues in response to mechanical forces. Arch Immunol Ther Exp (Warsz) 2005;53:388–398. [PubMed] [Google Scholar]
- 4.Sekhavat AR, Mousavizadeh K, Pakshir HR, Aslani FS. Effect of misoprostol, a prostaglandin E1 analog, on orthodontic tooth movement in rats. Am J Orthod Dentofacial Orthop. 2002;122:542–547. doi: 10.1067/mod.2002.126153. [DOI] [PubMed] [Google Scholar]
- 5.Krishnan V. Critical issues concerning root resorption: a contemporary review. World J Orthod. 2005;6:30–40. [PubMed] [Google Scholar]
- 6.Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J Periodontics Restorative Dent. 2001;21:9–19. [PubMed] [Google Scholar]
- 7.Wilcko WM, Ferguson DJ, Bouquot JE, Wilcko T. Rapid orthodontic decrowding with alveolar augmentation: case report. World J Orthod. 2003;4:197–205. [Google Scholar]
- 8.Baloul SS, Gerstenfeld LC, Morgan EF, Carvalho RS, Van Dyke TE, Kantarci A. Mechanism of action and morphologic changes in the alveolar bone in response to selective alveolar decortication-facilitated tooth movement. Am J Orthod Dentofacial Orthop. 2011;139(suppl):S83–S101. doi: 10.1016/j.ajodo.2010.09.026. [DOI] [PubMed] [Google Scholar]
- 9.Kim SJ, Park YG, Kang SG. Effects of corticision on paradental remodeling in orthodontic tooth movement. Angle Orthod. 2009;79:284–291. doi: 10.2319/020308-60.1. [DOI] [PubMed] [Google Scholar]
- 10.Safavi SM, Heidarpour M, Izadi SS, Heidarpour M. Effects of flapless bur decortications on movement velocity of dogs' teeth. Dent Res J. 2012;9:783–789. [PMC free article] [PubMed] [Google Scholar]
- 11.Teixeira CC, Khoo E, Tran J, et al. Cytokine expression and accelerated tooth movement. J Dent Res. 2010;89:1135–1141. doi: 10.1177/0022034510373764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yaffe A, Fine N, Binderman I. Regional accelerated phenomenon in the mandible following mucoperiosteal flap surgery. J Periodontol. 1994;65:79–83. doi: 10.1902/jop.1994.65.1.79. [DOI] [PubMed] [Google Scholar]
- 13.Wang L, Lee W, Lei DL, Liu YP, Yamashita DD, Yen SL. Tissue responses in corticotomy- and osteotomy-assisted tooth movements in rats: histology and immunostaining. Am J Orthod Dentofacial Orthop. 2009;136:770.e1–770.e11. doi: 10.1016/j.ajodo.2009.05.015. [DOI] [PubMed] [Google Scholar]
- 14.Iino S, Sakoda S, Ito G, Nishimori T, Ikeda T, Miyawaki S. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am J Orthod Dentofacial Orthop. 2007;131(448):e441–448. doi: 10.1016/j.ajodo.2006.08.014. [DOI] [PubMed] [Google Scholar]
- 15.Cho KW, Cho SW, Oh CO, Ryu YK, Ohshima H, Jung HS. The effect of cortical activation on orthodontic tooth movement. Oral Dis. 2007;13:314–319. doi: 10.1111/j.1601-0825.2006.01286.x. [DOI] [PubMed] [Google Scholar]
- 16.Cohen G, Campbell PM, Rossouw PE, Buschang PH. Effects of increased surgical trauma on rates of tooth movement and apical root resorption in foxhound dogs. Orthod Craniofac Res. 2010;13:179–190. doi: 10.1111/j.1601-6343.2010.01494.x. [DOI] [PubMed] [Google Scholar]
- 17.Pilon JJ, Kuijpers-Jagtman AM, Maltha JC. Magnitude of orthodontic forces and rate of bodily tooth movement. An experimental study. Am J Orthod Dentofacial Orthop. 1996;110:16–23. doi: 10.1016/s0889-5406(96)70082-3. [DOI] [PubMed] [Google Scholar]
- 18.van Leeuwen EJ, Maltha JC, Kuijpers-Jagtman AM. Tooth movement with light continuous and discontinuous forces in beagle dogs. Eur J Oral Sci. 1999;107:468–474. doi: 10.1046/j.0909-8836.1999.eos107608.x. [DOI] [PubMed] [Google Scholar]
- 19.Mostafa YA, Mohamed Salah Fayed M, Mehanni S, ElBokle NN, Heider AM. Comparison of corticotomy-facilitated vs standard tooth-movement techniques in dogs with miniscrews as anchor units. Am J Orthod Dentofacial Orthop. 2009;136:570–577. doi: 10.1016/j.ajodo.2007.10.052. [DOI] [PubMed] [Google Scholar]
- 20.Peter H, Buschang PMC, Ruso S. Accelerating tooth movement with corticotomies: is it possible and desirable? Semin Orthod. 2012;18:286–294. [Google Scholar]
- 21.Frost HM. The regional accelerated phenomenon. Orthop Clin North Am. 1981;12:725–726. [Google Scholar]