

Abstract
Objective:
To quantify the effects of tip-back mechanics on the maxillary first molars and incisors.
Materials and Methods:
Sixteen subjects with Class II end-on malocclusion were treated with an intrusion arch to achieve distalization of the maxillary molar through tip-back mechanics. Lateral cephalograms were taken prior to molar tip-back (T1), after molar tip-back (T2), and after molar root uprighting (T3). Data were analyzed using the Friedman’s and Wilcoxon signed rank tests to evaluate differences in time points (P ≤ .016).
Results:
The maxillary first molar distalized 1.53 mm (P = .001) with 6.65° (P = .001) of distal tipping and 0.86 mm (P = .001) of extrusion at T2. Minor relapse of the first molar (mesial direction) was seen at T3. The maxillary incisors flared labially 0.4 mm, and the incisor root apex moved palatally 1.19 mm (P = .005) at T2. At T3, the incisor root apex moved palatally 1.5 mm (P = .003) from T1. An angular change from T1 of 3.31° (P = .008) and 3.53° (P = .014) was seen at T2 and T3, respectively, as a result of palatal root movement of the maxillary incisors.
Conclusions:
A significant amount of distalization of maxillary molars was attained at the crown level with tip-back mechanics. Palatal root angulation change was significant in the incisors with minimal anteroposterior movement of the incisal edge.
Keywords: Tip-back mechanics, 1 couple force system, Intrusion arch, Distalization
INTRODUCTION
Tip-back mechanics are an alternative to the conventional approach of maxillary molar intra-arch distalization for Class II correction. The advantage of this approach is that it circumvents the problem of anterior anchorage loss by delivering an intrusive force instead of a mesial force to the anterior teeth while distalizing the maxillary molars.1 This approach was introduced by Romeo and Burstone2 for the correction of second-order inclinations of a single molar or group of posterior teeth and also described as an option for the correction of Class II subdivision malocclusions.3 It has been reported that 2- to 3-mm of arch length can be gained with tip-back mechanics.2,4 Since its introduction, tip-back mechanics have been modified both in its applications and types of arch wire used. Nanda et al.1 introduced the Connecticut Intrusion Arch for the correction of deep bites and Class II malocclusions. Simultaneous intrusion of the maxillary incisors and tip-back of the maxillary molars was described in Class II deep bite subjects. Headgear was advocated to upright the maxillary molars after tip-back.
Instead of headgear, which heavily relies on patient’s compliance, root uprighting of the maxillary molars may be achieved by sequentially increasing the dimension and stiffness of the arch wires inserted into the molar tube while the intrusion arch remains actively attached. At the same time, the additional arch length gained after tip-back is maintained during the retraction of the anterior teeth with the aid of Class II elastics. In patients in whom molar distalization is planned but incisor intrusion is undesired, a larger anchorage unit is used.1 Specifically, to minimize the side effects of the intrusive force from the intrusion arch, the maxillary canines, first premolars, and second premolars are added to the maxillary incisor segment.
Although tip-back mechanics have anecdotally been reported as a treatment alternative for the correction of Class II malocclusions,1 limited evidence is available regarding the magnitude of molar distalization that may be achieved. In addition, the effect of a large anterior anchorage unit (from second premolar to the contralateral second premolar) in minimizing the anterior intrusive force is largely unknown. Hence, the purpose of this prospective clinical trial was to measure the amount of distalization of the maxillary first molars and the effects on the maxillary incisors and the large anterior anchorage unit with tip-back mechanics.
MATERIALS AND METHODS
Ethical approval from the Institutional review board (No. 11-016-1) of the University of Connecticut, School of Dental Medicine, was obtained for this prospective study. STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) statement guidelines for observational studies were followed. The clinical trial was conducted at the University of Connecticut orthodontic clinic from November 2010 to June 2014. The sample size of 17 subjects was determined after a power analysis based on the mean distalization values derived from a previous pilot study evaluating tip-back mechanics.5 To account for an attrition rate of 15%, the overall recruitment goal was 20 subjects. A total of 19 subjects were recruited based on the following inclusion criteria: (1) Angle Class II end on molar relationship bilaterally, (2) nonextraction treatment plan, and (3) 11–14 years of age. The exclusion criteria were (1) presence of any primary teeth, (2) missing or malformed permanent teeth (except third molars), and (3) failure to provide oral and written consent to be included in the research. Patients were recruited prior to placing maxillary bonded appliances and received a leveling and alignment phase before the first lateral cephalogram that was part of the study (T1) was acquired.
From the recruited 19 patients, two patients were excluded from the study since one molar had corrected to Class I relationship at the time that tip-back was supposed to be implemented (T1). Subsequently, during data analysis, the lateral cephalogram of one subject was distorted and had to be excluded. Data analysis was performed on 16 subjects (seven male and nine female) with mean age of 12.63 ± 1.1 years.
Tip-Back Mechanics and Guidelines
Patients were bonded in the maxilla with 0.022-inch self-ligating Carriere brackets (ClassOne Orthodontics, Carsbad, Calif), leveled and aligned until a 0.016 × 0.022-inch stainless-steel arch wire was placed. Tooth-positioning jigs were placed in the auxiliary tubes of the first maxillary molars during the pre–tip-back lateral cephalogram (T1). Maxillary first molars were cut off the 0.016 × 0.022-inch stainless-steel arch wire, leaving an anterior segment that included second premolar to the contralateral second premolar. However, five patients had blocked out or ectopically erupting canines; the anchorage unit included all premolars posteriorly and all incisors anteriorly bypassing the canines. A prefabricated 0.017 × 0.025-inch Connecticut intrusion arch (Ultimate Wireforms Inc, Bristol, Conn) was placed in the maxillary first molar tubes and tied anteriorly over all four maxillary incisor brackets, resulting in one-couple force system. The position of the V-bend was 3–5 mm mesial to the maxillary molars. The Connecticut intrusion arch was made of nickel titanium with a V bend calibrated to deliver an intrusive force of approximately 40–60 g.1 A clockwise moment of approximately 800–1200 gmm is generated on the maxillary molars for tip-back based on the average distance of the molar to the point of attachment on the lateral incisors (Figures 1 and 2a).
Figure 1.
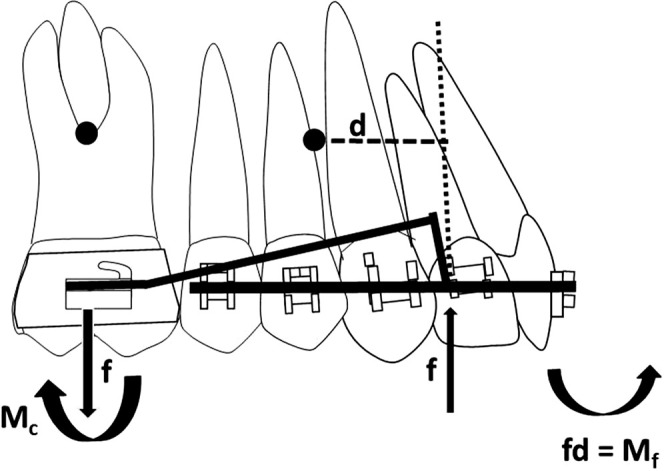
The intrusion arch exerts an intrusive force (f) on the anterior segment, extrusive force on the molar and clockwise moment of a couple (Mc). Counterclockwise moment of a force (Mf) is generated on the anterior anchorage unit as the intrusive force was anterior to the center of resistance of the anchorage unit.
Figure 2.
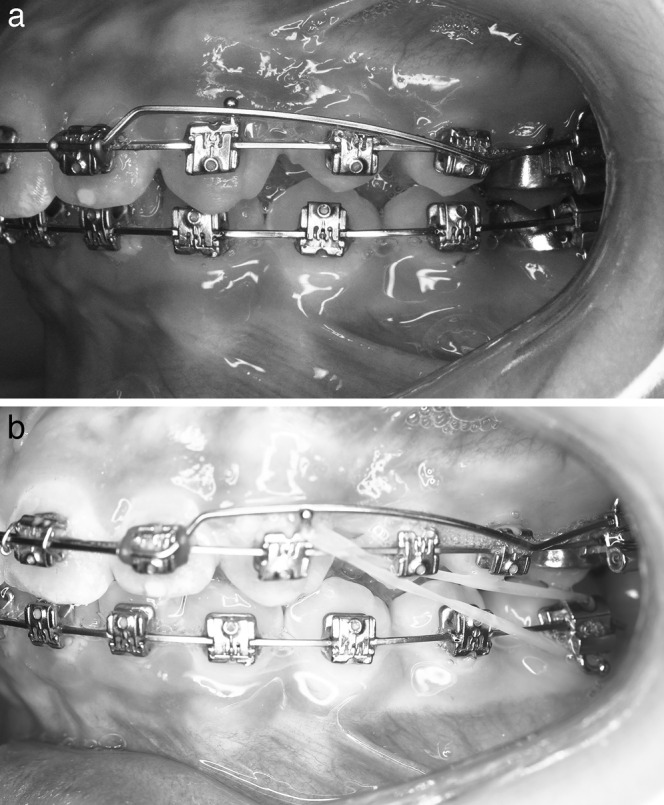
(a) Intraoral photographs at that start of study intervention (T1). (b) Photographs after completion of molar tip-back (T2).
Molar tip-back was completed when the Class I molar relationship was achieved clinically or when no additional tip-back of the molar was observed in two consecutive follow-up visits. This time point was determined by the study coordinator. At this point, a second lateral cephalometric radiograph (T2) was taken. During this same visit, a 0.017 × 0.025-inch nickel-titanium arch wire was placed from the maxillary first molar to the contralateral first molar, and the intrusion arch was maintained. The rationale to continue using the intrusion arch was to maintain the molar tip-back while the main arch wire uprighted the root. In addition, Class II elastics were used to retract the upper anterior teeth (Figure 2b). After 4 weeks, a 0.017 × 0.025-inch beta titanium arch wire was placed for 4 weeks, and later, a 0.017 × 0.025-inch stainless-steel arch wire was inserted and maintained for 4–6 weeks, when a third lateral cephalometric radiograph (T3) was taken.
Lateral Cephalometric Analysis
To distinguish between the right and left maxillary molars, tooth-positioning jigs (0.017 × 0.025-inch stainless steel) were placed in the molar auxiliary tubes during the acquisition of the lateral cephalograms at T1, T2, and T3 (Figure 3a–c). The jigs were bent at a 90° angle to the slot; the left jig was 10 mm in height and bent mesially, whereas the right jig was 5 mm in height and bent distally. The anteroposterior and vertical measurements of the maxillary molars on the lateral cephalogram were registered at the jigs’ insertion site on the molar auxiliary tube.6
Figure 3.

(a–c) Lateral cephalometric radiographs before molar tip-back (T1), after molar tip-back (T2), and after molar uprighting (T3).
To evaluate the maxillary dental changes, all of the radiographs were hand traced and superimposed from the described three time points.6 The maxillary superimpositions were performed on the internal palatal surfaces of the maxilla. After tracing the maxilla and teeth at T1, an x-axis was drawn by connecting the anterior nasal spine (ANS) and posterior nasal spine (PNS; Figure 4a,b). A y-axis was derived by drawing a line perpendicular to the x-axis, passing through sella turcica. After tracing maxillary structures at T2 and T3, the x-y coordinate system was transferred from T1 to T2 and T3 tracings while superimposing on the best fit of internal palatal surfaces of the maxilla. The linear and angular measurements for evaluating the molar and incisor changes are summarized in Figure 4a,b. Vertical and anteroposterior maxillary incisor changes were measured from the root apex, incisal edge, and centroid point. The centroid point was a constructed point 15 mm from the incisal edge along the long axis of the maxillary incisor. For the maxillary molars, the linear and vertical measurements were performed with the aid of tooth-positioning jigs measured at the entrance of molar tubes for both sides. The angular change of both molars was measured by drawing a line along the tooth-positioning jig extending to the x-axis. The average of linear, vertical, and angular changes of right and left molars was taken and statistical analysis performed.
Figure 4.

Occlusal view of bonded maxillary expander.
Statistical Analysis
Statistical analysis was performed using the SPSS software, version 17.0 (IBM Corporation, Armonk, NY). A reliability analysis was done by retracing all the radiographs by a single evaluator with a 4-week interval between tracings. The Shapiro-Wilk test for normality was conducted, and data were normally distributed. However, as the sample size was less than 30, Friedman’s tests were performed to determine whether there were significant changes between time points. Wilcoxon signed-rank test was conducted to distinguish where the differences were present among the evaluated variables. Bonferroni correction was performed to control the inflation of type I error (α = .05/3), and P value of ≤.016 was considered statistically significant.
RESULTS
Reliability analysis (intraclass correlation coefficient; ICC) indicated good reliability as the ICC Cronbach’s alpha ranged from .94 to .99 (Table 1). Table 2 displays the summary statistics of all variables examined in this study. Significant differences were evident anteroposteriorly for molar tip-back, incisor apex, and molar and incisor angular changes at T2 and T3 with reference to T1. Vertically, significant differences were observed in molar extrusion, centroid point of maxillary incisor at T2 and T3, and for incisal edge of maxillary incisor at T2 with reference to T1. The mean treatment time for molar tip-back phase was 5 ± 1.63 months (T2–T1) and molar uprighting phase (T3–T2) was 3.22 ± 0.77 months.
Table 1.
Intrarater Reliability: Intraclass Correlation Coefficient

Table 2.
Mean Values With Standard Deviations and 95% Confidence Intervals (CI) of Variables at T1, T2, and T3 Achieved With Tip-Back Mechanics With Mean Differencesa

Table 2.
(Continued)

Maxillary Molar Changes
Distalization of 1.53 ± 0.65 mm with 6.65° ± 5.6° of distal crown tipping was attained at T2. At T3, 0.1 ± 0.7 mm of distalization was lost as the molar tipped mesially by 1.84° ± 5.87°. Vertically, 0.86 ± 0.49 mm of molar extrusion was observed at T2 and 0.12 ± 0.58 mm of molar extrusion was lost at T3.
Maxillary Incisor Changes
The incisor root apex moved palatally by 1.19 ± 1.31 mm at T2 and moved further palatally to 1.5 ± 1.67 mm at T3. A minor anterior movement of the incisal edge at T2 returned to pretreatment position at T3. Palatal root torque was expressed in the maxillary incisors with an angular change from T1 of 3.31° ± 3.79° at T2 and 3.53° ± 5.31° at T3. Vertically, the incisal edge intruded by 0.97 ± 1 mm at T2, but the incisal edge extruded by 0.56 ± 0.85 mm at T3. The centroid point intruded by 0.78 ± 0.87 mm at T2, with 0.63 ± 0.82 mm of intrusion lost at the end of the uprighting phase (T3). The maxillary incisor apex intruded by 0.46 ± 0.76 mm after the tip-back phase (T2), and 0.31 ± 0.89 mm of intrusion was lost at T3.
DISCUSSION
The main objective of this study was to quantify the amount of maxillary molar distalization obtained with tip-back mechanics. The magnitude of distalization in our study was slightly less when compared with other buccal distalization methods7,8 as reported in a recent systematic review.9 Specifically, they found after analyzing numerous types of buccal distalization devices an average 2.6 mm of distal molar movement and 8.3° of angular change. However, very few studies have evaluated the relapse of the molar movement after distalization. Angelieri et al.10 reported 2.2 mm of molar distalization with pendulum appliance, but 1.1 mm of molar distalization was lost during the aligning and leveling phase after distalization. On the other hand, with tip-back mechanics, 1.43 mm of molar distalization was maintained at the end of the molar root uprighting phase. In the vertical dimension, tip-back mechanics were extrusive, and the amount of molar extrusion was comparable with other distalization appliances.9
Anchorage loss of the maxillary premolar and incisors has been the major drawback with most distalization appliances. A recent systematic review reported that the incisors flare labially by 1.8 mm with an angular change of 3.6°.9 The angular change of the incisors obtained in this study was similar to other studies, but the linear anterior displacement was minimal. The change in incisor angulation could be due to expression of palatal root torque of the maxillary incisors, whereas in the other studies, it was due to incisor flaring. In the vertical plane, transient intrusion of maxillary incisors was seen between T1 and T2, but most of the incisor intrusion relapsed at T3. On the other hand, maxillary incisor extrusion of 0.4 mm has been reported with distalization appliances.9
The results of the study suggest that the large anterior anchorage unit connected by a 0.016 × 0.022-inch stainless-steel arch wire may have successfully minimized anterior and vertical movement of the maxillary incisors. The maxillary first molar was minimally distalized without side effects on the anterior anchorage units, a finding that is not seen with other intra-arch distalization appliances. Based on the results of the study, tip-back mechanics appear marginally effective in the correction of an end-on Class II malocclusion.
To further describe the type of tooth movement achieved, we determined the center of rotation based on the linear and angular displacement of the maxillary first molars, as described by Baumrind et al.11 The center of rotation of the first molars was found 4 mm apical to the center of resistance (near the trifurcation of maxillary molar) resulting in distal crown and mesial root tipping. Based on this finding, distalization of maxillary molar with tip-back mechanics is not an effective method for gaining arch length to address crowding or overjet reduction. Tip-back mechanics may be indicated for uprighting tipped molars or a group of posterior teeth as originally described by Romeo and Burstone.2
Palatal root torque of maxillary incisors without anterior displacement of the maxillary incisor crowns was found in this study. Incisor third-order torque is least effectively attained with preadjusted edgewise appliances.12 In straight-wire mechanics, arch wire torsion of 22°–35° on a 0.019 × 0.022-inch stainless-steel wire is recommended to produce an effective torque moment of 5–20 Nmm.13
Isaacson et al.12 described the mechanics of achieving incisor torque either through the moment of a couple or the moment of a force. Since the intrusive force at the incisor bracket is not directed through the center of resistance of this anterior segment, a moment of the force is generated. Van Steenbergen et al.14 found 8°–9° of axial inclination change of the maxillary incisors with an intrusion arch when the anterior unit consisted only of the four anterior teeth. In our study, the magnitude of the moment of the force was likely higher since all teeth anterior to the first molars were included. Interestingly, we found that the amount of incisal inclination change was only 3.31°, suggesting that the large anterior segment of 10 teeth successfully prevented the labial movement of the incisor crowns; however, palatal root displacement as a result of the moment of the force was still expressed on the incisors roots. This finding is of interest; perhaps the cross-section of the wire in the anchorage unit may contribute to the changes observed in the incisors. Further in vitro studies are recommended to determine the three-dimensional forces and moments generated with tip-back mechanics to understand the biologic response, which can aid the clinician to predictably achieve incisor third-order corrections.
Some of the limitations of this lateral cephalometric study are inherent to 2D imaging such as errors in magnification, projection, landmark identification,15 and superimposition.11 To minimize the errors in landmark identification, tooth-positioning jigs were used to accurately locate the right and left maxillary molars. The lateral cephalograms were taken with the same cephalostat to minimize error due to the magnification. Although the head orientation was standardized while exposing the radiographs, minor projection errors were unavoidable, and the study results should be interpreted taking this factor into account. Another drawback with the study was a single rater measuring the radiographs twice; however, the reliability of the double measurements was very high, suggesting accuracy of the measurements. Despite these shortcomings, this prospective study provides evidence regarding the amount of molar distalization and type of molar movement attained with tip-back mechanics.
CONCLUSIONS
Tip-back mechanics distalized the maxillary first molars by 1.53 mm, and the type of tooth movement obtained was uncontrolled tipping with distal crown and mesial root movement. Slight mesial movement of the molar crown was observed during the uprighting phase. Based on the magnitude and type of movement obtained, tip-back mechanics may not be an effective method of distalization.
No unwarranted maxillary incisor flaring or intrusion was observed.
Expression of palatal root torque on maxillary incisors was a significant finding with tip-back mechanics.
ACKNOWLEDGMENTS
We thank Ultimate Wireforms Inc for providing the Connecticut intrusion arch wires (0.017 × 0.025-inch) for the study. Also, we thank Dr Achint Utreja for his statistical support.
REFERENCES
- 1.Nanda R, Marzban R, Kuhlberg A. The Connecticut intrusion arch. J Clin Orthod. 1998;32:708–715. [PubMed] [Google Scholar]
- 2.Romeo DA, Burstone CJ. Tip-back mechanics. Am J Orthod. 1977;72:414–421. doi: 10.1016/0002-9416(77)90354-2. [DOI] [PubMed] [Google Scholar]
- 3.Shroff B, Lindauer SJ, Burstone CJ. Class II subdivision treatment with tip-back moments. Eur J Orthod. 1997;19:93–101. doi: 10.1093/ejo/19.1.93. [DOI] [PubMed] [Google Scholar]
- 4.Braun S, Colgan J, Johnson BE. Altering mandibular arch length by tip back mechanics: a case report. Am J Orthod Dentofacial Orthop. 1994;106:555–560. doi: 10.1016/S0889-5406(94)70080-X. [DOI] [PubMed] [Google Scholar]
- 5.Faber ZT. Relationship of Tooth Movement to Measured Force Systems: A Prospective Analysis of the Treatment Effects of Orthodontic Intrusion Arches. SoDM Masters Theses. Paper 36. 2001 http://digitalcommons.uconn.edu/sodm_masters/36 . [Google Scholar]
- 6.Davoody AR, Posada L, Utreja A, et al. A prospective comparative study between differential moments and miniscrews in anchorage control. Eur J Orthod. 2013;35:568–576. doi: 10.1093/ejo/cjs046. [DOI] [PubMed] [Google Scholar]
- 7.Mavropoulos A, Karamouzos A, Kiliaridis S, Papadopoulos MA. Efficiency of noncompliance simultaneous first and second upper molar distalization: a three-dimensional tooth movement analysis. Angle Orthod. 2005;75:532–539. doi: 10.1043/0003-3219(2005)75[532:EONSFA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Mavropoulos A, Karamouzos A. Cephalometric changes following simultaneous first and second maxillary molar distalization using a non-compliance intraoral appliance. J Orofac Orthop. 2004;65:123–136. doi: 10.1007/s00056-004-0317-z. [DOI] [PubMed] [Google Scholar]
- 9.Antonarakis GS, Kiliaridis S. Maxillary molar distalization with noncompliance intramaxillary appliances in Class II malocclusion: a systematic review. Angle Orthod. 2008;78:1133–1140. doi: 10.2319/101507-406.1. [DOI] [PubMed] [Google Scholar]
- 10.Angelieri F, de Almeida RR, de Almeida MR, Fuziy A. Dentoalveolar and skeletal changes associated with the pendulum appliance followed by fixed orthodontic treatment. Am J Orthod Dentofacial Orthop. 2006;129:520–527. doi: 10.1016/j.ajodo.2005.12.003. [DOI] [PubMed] [Google Scholar]
- 11.Baumrind S, Miller D, Molthen R. The reliability of head film measurements: 3. Tracing superimposition. Am J Orthod. 1976;70:617–644. doi: 10.1016/0002-9416(76)90224-4. [DOI] [PubMed] [Google Scholar]
- 12.Isaacson RJ, Lindauer SJ, Rubenstein LK. Moments with the edgewise appliance: incisor torque control. Am J Orthod Dentofacial Orthop. 1993;103:428–438. doi: 10.1016/S0889-5406(05)81793-7. [DOI] [PubMed] [Google Scholar]
- 13.Archambault A, Lacoursiere R, Badawi H, et al. Torque expression in stainless steel orthodontic brackets: a systematic review. Angle Orthod. 2010;80:201–210. doi: 10.2319/080508-352.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Van Steenbergen E, Burstone C, Prahl-Andersen B, Aartman I. The relation between the point of force application and flaring of the anterior segment. Angle Orthod. 2005;75:730–735. doi: 10.1043/0003-3219(2005)75[730:TRBTPO]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Baumrind S, Frantz RC. The reliability of head film measurements: 1. Landmark identification. Am J Orthod. 1971;60:111–127. doi: 10.1016/0002-9416(71)90028-5. [DOI] [PubMed] [Google Scholar]